
Submitted:
07 October 2024
Posted:
08 October 2024
You are already at the latest version
Abstract
Background: Studies on infectious endocarditis (IE) are mostly limited to institutions, which highlights the need for more comprehensive epidemiological studies. Objective: To verify the profile of deaths due IE and the relationship with deaths from other causes and conditions in Brazil and regions. Method: Study in database from the Brazilian Mortality Information System, from 2000 to 2019. Mentions of deaths due to IE, other causes and conditions were identified according to ICD-10. Cluster analysis was performed to verify the relationship between variables. Results: 52,055 deaths from IE were found, with a predominance of males, aged 60 to 79 years, in the Southeast, with deaths from the circulatory system most frequent. Three profiles were identified: 1 - age equal to or greater than 80 years, women, deaths due endocrine, circulatory and metabolic diseases, in the South and Southeast; 2 - also in the South and Southeast, age between 30 and 79 years, men, deaths due infectious and genitourinary diseases; 3 - 0 to 29 years, no genders differences, deaths due diseases of the respiratory system, in the North, Northeast and Central-West. Conclusion: Cluster analysis showed diversity in the profiles of deaths due IE, indicating heterogeneity in regions of the country.
Keywords:
Endocarditis
; epidemiological profile
; mortality
; upper-middle-income countries
; Brazil
1. Introduction
Infective endocarditis (IE) is defined as infection of the endocardium, intracardiac apparatus or valves [1]. Although it is a condition with low prevalence, it still has a significant fatality rate and is associated with serious complications such as heart failure, brain abscess and mycotic aneurysm [1]. The epidemiological profile of this infection varies according to the country of occurrence. In high-income countries, there is an association with degenerative valve diseases and involvement of middle-aged individuals [2,3]. In low-middle-income, low-income, and even some upper-middle-income countries, the main predisposing condition is still rheumatic fever with cardiac involvement, which is prevalent in individuals around the third decade of life [2,3]. Brazil and Argentina have demonstrated a reduction in the association between IE and rheumatic fever, which suggests positive results in prophylaxis [4,5]. Mortality due to IE is also unequal depending on the population and method used for the study. According to the literature, it can vary from 8% to 40% [6,7]. The incidence of complications is intrinsically associated with mortality, as well as with late diagnosis of the disease. Studies of Brazilian cohorts highlight acute renal failure, septic shock and heart failure as the main causes of death in patients with IE [5,8,9,10]. These studies refer to the presence of diseases such as diabetes mellitus and chronic kidney disease, and older age as factors for more reserved prognoses [5,8,9,10]. Knowledge about variables associated with death due to a disease contributes to understanding its evolution and prognosis. Studies on IE are mostly limited to institutions, highlighting the need for more comprehensive epidemiological studies, particularly in low- and middle-income countries. Thus, this study aimed to verify the frequency of deaths due to IE in Brazil and regions, and to analyze the profile of deaths due to infection through its relationship with other causes of death and sociodemographic variables, present in the Mortality Information System database, from 2000 to 2019.
2. Materials and Methods
This is an observational study of a time series of deaths with mention of IE, based on the individual database of the Mortality Information System (MIS), from the Department of Information and Informatics of the Unified Health System (DATASUS). This information was obtained through the microdatasus package in the R software [11]. The mentions of deaths due to IE were identified using the following codes, according to the 10th International Statistical Classification of Diseases and Related Health Problems (ICD-10) [12]: I 33 – Acute and Subacute Endocarditis; I 33.0 – Acute and Subacute Infective Endocarditis; I 33.9 – Unspecified Acute Infective Endocarditis; I 38 – Unspecified Valve Endocarditis; I39 – Endocarditis and Cardiac Valvular Disorders in Diseases classified elsewhere; I 39.0 – Mitral Valve Disorders in Diseases classified elsewhere; I 39.1 – Aortic Valve Disorders in Diseases classified elsewhere; I 39.2 – Tricuspid Valve Disorders in Diseases classified elsewhere; I 39.3 – Pulmonary Valve Disorders in Diseases classified elsewhere; I 39.4 – Multiple Valve Disorders in Diseases classified elsewhere; I 39.8 – Unspecified Valve Endocarditis in Diseases classified elsewhere.
Information on deaths, according to the codes mentioned, was extracted from the column corresponding to the “underlying cause” variable and from the columns related to the variables in lines A, B, C, D, and line II, available in the MIS database. Initially, the cause of death related to IE was investigated in the “underlying cause” variable. Only in cases where the cause of death due to IE was not identified in this variable, the search was performed in lines A, B, C, D, and line II. In this way, duplication of records was avoided in which the cause of death due to IE was present in both the “underlying cause” variable and in the other lines mentioned. Mentions of other causes of death that coexisted with the underlying cause or mention of IE for each individual were analyzed. These other causes were investigated both in the “underlying cause” variable and in lines A, B, C, D, and line II.
For the analysis, the mentions referring to other causes of death coexisting with deaths involving IE were classified according to the chapters of ICD-10: CHAPTER I: Some infectious and parasitic diseases; CHAPTER II: Neoplasms (Tumors); CHAPTER III: Diseases of the blood and hematopoietic organs and some immune disorders; CHAPTER IV: Endocrine, nutritional and metabolic diseases; CHAPTER V: Mental and behavioral disorders; CHAPTER VI: Diseases of the nervous system; CHAPTER VII: Diseases of the eye and adnexa; CHAPTER VIII: Diseases of the ear and mastoid process; CHAPTER IX: Diseases of the circulatory system; CHAPTER X: Diseases of the respiratory system; CHAPTER XI: Diseases of the digestive system; CHAPTER XII: Diseases of the skin and subcutaneous tissue; CHAPTER XIII: Diseases of the musculoskeletal system and connective tissue; CHAPTER XIV: Diseases of the genitourinary system; CHAPTER XV: Pregnancy, childbirth and the puerperium; CHAPTER XVI: Certain conditions originating in the perinatal period; CHAPTER XVII: Congenital malformations, deformities and chromosomal anomalies; CHAPTER XVIII: Symptoms, signs and abnormal findings of clinical and laboratory examinations, not classified elsewhere; CHAPTER XIX: Injuries, poisoning and certain other consequences of external causes; CHAPTER XX: External causes of morbidity and mortality; CHAPTER XXI: Factors influencing the state of health and contact with health services; CHAPTER XXII: Codes for special purposes. ICD-10 chapters whose mentions represented less than 5% of cases were excluded from the analysis.
The variables analyzed included: (i) year range of registration (2000-2004, 2005-2009, 2010-2014, 2015-2019); (ii) age group (0 to 9, 10 to 29, 30 to 59, 60 to 79, 80 or older); (iii) gender (male, female); (iv) color/race (yellow, white, indigenous, brown, black); (v) marital status (single, married/consensual union, legally separated, widowed); (vi) education (none, 1 to 7 years, 8 to 11 years, 12 years or more); (vii) place of death (home, hospital/other health facility, others); and (viii) ICD-10 chapters. Missing data for the variables analyzed were treated by excluding cases, since incomplete records were not considered.
Statistical analyses included calculation of absolute frequencies and percentages for qualitative variables, as well as assessment of the association between variables and Brazilian regions using Pearson’s chi-square test. The proportions of each ICD-10 chapter were compared by region, using 95% confidence intervals (95%CI). For cluster analysis, due to computational cost, a representative data sample was performed in each year interval, drawing 5,000 observations per period, totaling 20,000 observations. Multiple Correspondence Analysis (MCA) was applied using the factoMineR package in R software [13], followed by hierarchical clustering based on the principal components of the MCA. Ward’s agglomeration method was used with Euclidean distance. The optimal number of clusters was determined automatically, and comparisons of the proportions of categories in the clusters were performed using the V test, based on the hypergeometric distribution [14]. The interpretation of the clusters was conducted using the metrics Cla/Mod (proportion of individuals belonging to a specific class (cluster)) and Mod/Cla (proportion of individuals who have a specific modality among those belonging to a class (cluster)). For a visual comparison of the characteristics among the identified clusters, a heat map was generated using the pheatmap package in R [15], with the application of a color scale that represented the frequency of the characteristics per cluster. All analyses were conducted in the R software, version 4.3.2, adopting a significance level of 5%.
Although the study used data from a public database, the research project was submitted to the Ethics and Research Committee of the Gafrée and Guinle University Hospital and approved, according to opinion number 7,051,294, on September 3, 2024.
3. Results
3.1. Analysis of the General Profile of Deaths Mentioning IE
Between 2000 and 2019, 52,055 mentions of deaths due to IE were recorded in Brazil. Approximately 50% of these deaths occurred in the Southeast region, followed by the Northeast and South regions, which recorded 19.06% and 15.76%, respectively. The North region recorded the lowest percentage, corresponding to 4.16% of the total (Table 1).
The age group with the highest percentage of deaths in Brazil was 60 to 79 years old, also predominant in the South and Southeast regions. In the North, Northeast and Central-West regions, the highest percentage of deaths occurred in younger age groups, between 30 and 59 years old. Males had the highest proportion of deaths both in Brazil and in all regions analyzed (Table 1).
Differences were also observed in the distribution of mentions of deaths due to IE in relation to race/color. In Brazil, as well as in the South, Southeast and Central-West regions, most deaths were recorded for individuals classified as white, while in the North and Northeast regions the race/color of brown predominated. Regarding marital status, the category “Married/Consensual Union” was the most frequent both in Brazil and in the five regions (Table 1).
Regarding education, the highest percentage of deaths occurred among individuals with 1 to 7 years of education, a trend consistently observed in the country and in the regions. When analyzing the place where deaths occurred, the records indicated that the highest percentage occurred in hospitals or other health establishments. However, the Central-West, South and Northeast regions stood out with the highest percentages of mentions of deaths due to IE occurring at home (Table 1).
In the period analyzed, in Brazil, the diseases mentioned together with deaths due to infective endocarditis were predominantly related to diseases of the circulatory system, with greater predominance in the Central-West (65.2%, 95% CI = 63.7-66.8%) and Northeast (64.5%, 95% CI = 63.5-65.4%) regions compared to the other regions (Figure 1). The most prevalent mentions, among the diseases of the circulatory system, were heart failure, cerebrovascular diseases and hypertensive diseases.
The chapter on infectious and parasitic diseases was the second most prevalent, with a predominance in the Southeast region (42.2%, 95% CI = 41.7-42.8%). The mention of unspecified septicemia stands out. Next, the group symptoms, signs and abnormal findings of clinical and laboratory tests, not classified elsewhere, was frequently mentioned, with emphasis on the North region (41.8%, 95% CI = 39.7-43.9%), with emphasis on cardiogenic shock (Figure 1). Diseases of the respiratory system were also mentioned with significant frequency, being less prevalent in the South region (20.5% (19.6-21.4%). Among these, the mention of respiratory failure stands out. Diseases of the genitourinary system presented a prevalence of 22.7% (95% CI = 22.4-23.1%) in Brazil, with a higher frequency of mentions in the Southeast region (24.3%, 95% CI = 23.8-24.8%) (Figure 1), particularly related to renal failure. External causes of morbidity and mortality were mainly represented by ICD-10 codes referring to abnormal reactions in patients or late complications resulting from surgical interventions, with mention of prosthesis implantation being the most relevant. The North region (17.3%, 95% CI = 15.7-18.8%) presented higher percentages compared to the Southeast and South regions. Finally, endocrine, nutritional and metabolic diseases were mentioned with greater prevalence in the Southeast region (9.1%, 95% CI = 8.8-9.4%), with emphasis on diabetes mellitus and malnutrition (Figure 1).
3.2. Analysis of Clusters with Mention of Deaths Due to IE
This analysis identified three groups with distinct profiles regarding the characteristics of individuals with mentions of death due to IE.
Cluster 1 showed a predominance of individuals aged 80 or over, who constituted 52.3% of this group and represented 72.8% of all individuals in this age group. Females were predominant, corresponding to 79.8% of the cluster and 34.7% of the total number of women analyzed. The white and yellow races, as well as the Southeast and South regions, were more represented in this Cluster compared to the general sample. The marital status of widower represented 81.8% of the cluster, corresponding to 91.9% of all widowers in the study. Individuals with no education and with 1 to 7 years of education were more represented in this cluster than in the general sample. Death at home corresponded to 13.7% of this group, involving 41.2% of all home deaths. Regarding deaths from other diseases, related to mentions of deaths due to IE, endocrine and metabolic diseases, and those of the circulatory and respiratory systems stood out (Figure 2).
Cluster 2 concentrated individuals between 30 and 79 years old, representing more than 90% of the individuals in the cluster. Males were predominant, constituting 68.4% of the cluster and 66.7% of the total number of male individuals studied. The white and yellow races also had greater representation in Cluster 2 in relation to the general sample. The South and Southeast regions were more represented, corresponding to 22.3% and 62.2% of the cluster, respectively, covering 70.4% and 61.1% of the individuals in these regions. The married and separated marital statuses were more represented in this Cluster. Only individuals with no education were underrepresented in this group. Hospital death was highly prevalent, constituting 95% of the group and 55% of all deaths. Infectious and genitourinary diseases were significant, composing 41.8% and 26.2% of the cluster, respectively, and covering 57.7% and 61.4% of the total cases of these diseases. External causes were also frequent (Figure 2).
Cluster 3 was characterized by younger age groups. Individuals aged 0 to 9 years represented 4.5% of the cluster, with 100% of cases in this age group present in this cluster. The age group of 10 to 29 years represented 31.3% of the cluster, including 98.2% of all individuals in this age group. The cluster showed balance between the genders. The brown and black races were the most represented. The North, Northeast and Central-West regions were the most evident in comparison to the total sample, with the Northeast region being predominant, equivalent to 38.9% of the group. The single marital status constituted 74.3% of the cluster, corresponding to 74.6% of all single individuals analyzed. Regarding the other diseases related to IE, respiratory diseases stood out in comparison to Cluster 2 and the total sample (Figure 2).
4. Discussion
The study showed a significant number of deaths due to IE, 52,055 mentions, in Brazil for the period studied. Mortality due to IE is quite diverse worldwide and, particularly in Latin America, there is a shortage of studies with population-based databases. The EIRA 3 study, a prospective multicenter study on IE, in Argentina, in 2018, showed continued high mortality when compared with the results of previous studies, EIRA 1 in 1993 and EIRA 2 in 2002 [16]. A 17-year prospective population-based study conducted in Italy also showed an increasing trend in mortality due to IE [17]. Thus, the number of deaths found in the present study appears to still reflect the trend of high mortality from the disease.
The distribution of the frequency of deaths in Brazilian regions was similar to the study carried out by Oliveira et al., which used the DATASUS database, specifically on hospital procedures of the Unified Health System, to obtain data on morbidity and mortality due to valve IE, in Brazil, from 2018 to 2021. The authors report higher morbidity and mortality values in the Southeast and the lowest values in the North region [18]. The predominance of deaths due to IE in the Southeast can be explained by the higher population density and the more robust quality of mortality records in this region [19,20]. This result was similar to the study by David et al., who investigated mortality due to IE, using the MIS, between 2012 and 2021, and found a higher frequency of deaths in this region, 53.5% [21]. The difference in the quality of records between the states of the federation can also influence the interpretation of regional results. The North region has a lower correspondence in the SIM in relation to the civil registry, as was demonstrated in relation to the 2010 Census [20]. Thus, in this region, where a lower percentage of deaths due to IE was observed, it is possible that there is underreporting of cases or even a lower prevalence of the disease.
The results on the epidemiological profile of deaths due to IE were consistent with those described in the literature. It was predominant in men over 60 years of age [2,3,4,5,6,7,8,9]. This data suggests a relationship between advanced age and fatal outcomes due to IE. The relationship between aging and greater vulnerability to endocardial infection has already been documented, thus, there is a tendency for deaths to be concentrated in populations with a higher prevalence of IE, according to gender and age [2,3,4,5,7,8,9].
The regional differences in deaths according to race/color, found in the study, follow the demographic distribution of Brazil, with a predominance of whites in the Center-South and brown/blacks in the North and Northeast [19,20]. The study showed a higher percentage of deaths in married individuals/consensual unions and with less education, from 1 to 7 years, for the entire country. In fact, Melo et al. in an ecological epidemiological study, with analysis of cases reported in the Notifiable Diseases Information System - SINAN, on deaths due to acute and subacute IE, in the northeast of the country, from 2010 to 2019, showed a strong positive correlation with the male gender; brown race/color; education of 8 to 11 years of study; age range between 65 and 75 years, and among married individuals [22]. This corroborates the influence of socioeconomic factors, such as education, on mortality due to infection.
Regarding the places where deaths occurred, the records showed a higher percentage of deaths occurring in hospitals or other health units. This result is expected since treatment for IE is usually performed with the patient hospitalized, to receive intravenous medication. A population-based study in Finland also demonstrated that 89.5% of deaths due to IE occurred in a hospital or other health unit and 8.6% at home [23]. A higher frequency of deaths at home was observed in the Central-West, South and Northeast regions. No study was found in the literature that demonstrated causes related to death due to IE at home, but it is possible that this outcome is due to complications of the disease, such as embolic phenomena and heart failure. In part, there may also be a relationship with the lack of hospital infrastructure for hospitalizations and adequate treatment in more complicated cases, in which surgery is necessary.
Deaths due to circulatory system diseases were the most frequent causes, along with deaths due to IE, especially heart failure, cerebrovascular diseases and hypertension. Causes due to infectious diseases appeared as the second most frequent, particularly septicemia. Studies that analyzed risk factors, trends and evolution of deaths due to IE invariably reported causes such as heart failure and sepsis/septicemia/septic shock [17,24,25,26]. The study carried out by Ahtela et al., in Finland, reported the registration of septicemia as the underlying cause of death in 11.5% of cases and another infectious disease in 2.8%, in deaths that mentioned IE. The authors also reported cardiovascular diseases as the main underlying non-infectious causes of death, with coronary artery disease and cerebrovascular disease as the main contributors [23]. These results found in the literature corroborate what was shown in this investigation.
The chapter on symptoms, signs, and abnormal findings of clinical and laboratory tests includes symptoms, signs, and abnormal findings of clinical tests or other diagnostic investigation procedures, in addition to ill-defined conditions for which there is no diagnosis classified elsewhere [12]. This chapter was the third most frequent in deaths from IE. It is very likely that it is related to tests requested to investigate the disease, in which there was doubt about the diagnosis, since the conditions and signs or symptoms included in the categories of this chapter, according to ICD-10, consist of: “cases for which a more precise diagnosis cannot be reached; signs or symptoms existing at the time of the first consultation that are shown to be of a transient nature and whose causes cannot be determined; provisional diagnoses attributed to a patient who does not return for a consultation for further investigation of the diagnosis or for care; cases referred to other locations for investigation or treatment before the diagnosis was made; cases for which it was not possible to establish a more precise diagnosis for any other reason; some symptoms for which additional information is provided and which in themselves represent important problems in medical care” [12].
Mentions of deaths due to diseases of the respiratory system, genitourinary system, and endocrine, nutritional, and metabolic diseases should be related to complications and comorbidities that increase the risk of IE, such as renal failure and diabetes mellitus [27]. Indeed, when analyzing these chapters, the most frequent mentions for each of them were, respectively, respiratory failure, renal failure, and diabetes mellitus.
Abnormal reactions in patients or late complications resulting from surgical interventions, from the chapter on external causes of morbidity and mortality of ICD-10, mentioned prosthesis implantation as the most relevant and was the sixth most frequent chapter. This finding points to deaths that occurred after treatment with surgical intervention and probably indicates patients at higher risk. They were found mainly in the North region of the country, where there is less hospital infrastructure, when compared to other regions, such as the Southeast and South.
The method, through Multiple Correspondence Analysis, made it possible to identify 3 different profiles of individuals who had IE involved in their deaths.
The first profile identified was that of older individuals, aged 80 or over, predominantly female, widowed, white or yellow, with little or no education, with a higher frequency of deaths at home, in which endocrine and metabolic diseases, circulatory system and respiratory diseases stood out, with a greater representation in the Southeast and South regions of the country. This profile is consistent in its characteristics regarding age, gender, marital status, race/color, place of predominance of deaths and is related to the regions of the country identified. The states of the South and Southeast concentrate older populations, with a predominance of white race [19]. Among the older population, females are more frequent, due to the greater survival of women in relation to men. The probability of deaths at home increases in older individuals who live alone. The highest frequency here was of individuals who were widowed. The causes of death related to mentions of deaths due to IE, in this profile, are also common in this age group. As previously reported, mentions of diabetes mellitus, heart failure and respiratory failure were the most frequent in chapters that include endocrine and metabolic diseases, and those of the circulatory and respiratory systems.
The second profile was characterized by people of intermediate age, from 30 years old to older people, over 60 years old but under 80, with a predominance of men, married and separated, also of white or yellow race/color, with a higher level of education, deaths in hospitals, with a greater representation of deaths that were mentioned as infectious and genitourinary diseases, and external causes. This profile also had a greater representation of the South and Southeast regions. Thus, it is possible to deduce that this second identified profile complements the first profile, based on deaths that occur in individuals with different characteristics, but within the same region. The age range in this profile precedes that of the first profile, therefore, it has characteristics such as a predominance of males, higher level of education, with deaths in hospitals, in individuals whose status predominated as married and separated. Mentions of deaths concomitant with mentions of IE are also relevant in this profile, since deaths due to infectious diseases, renal failure and mentions of prosthesis implants, more frequently described in the ICD-10 chapters, may be present as complications of IE.
The third profile differed from the others in several aspects. It was defined by much younger individuals, between 0 and 29 years of age, and 100% of the population of individuals who died from IE, between 0 and 9 years of age, were in this group. There was no predominance of one of the genders, the most represented race/color was brown and black, the marital status was single, the mention of deaths due to diseases of the respiratory system were the most frequent and the most representative region in this profile was the Northeast. This profile, like the others, has concordance between its characteristics. The Northeast region has a younger population of individuals than the Southeast and South, and is represented by individuals who declare themselves to be brown and black, more frequently [19]. Individuals in this age group are mostly single. As for the mentions of deaths due to other causes in IE, it would not be common to find a high frequency of ICD-10 chapters involving chronic diseases. Therefore, it is reasonable to admit that respiratory system diseases have the greatest representation for this profile, in which the most frequent mention was respiratory failure.
The limitations of this investigation are related to the quality of the records reported in the database. Despite this, these databases provide information on a large number of individuals, in the real world, that would be difficult to reach in another type of study.
5. Conclusions
The frequency of deaths with mention of infective endocarditis, in Brazil and regions, over a 20-year period, was significant, particularly in the Southeast region.
In general, in Brazil, deaths due to infection were characterized in male individuals, over 60 years old, married, with low education and more frequently occurring in hospitals. The most frequent mentions of other causes of death, attached to the mention of infective endocarditis, were those related to the chapter on diseases of the circulatory system, particularly heart failure, cerebrovascular diseases and hypertensive diseases.
The identification of death profiles allowed a better understanding of the different characteristics in the regions of the country, which differentiate them from a general profile. Two profiles identified in the South and Southeast regions complement each other, with individuals aged 80 or over and deaths due to endocrine and metabolic diseases, circulatory and respiratory systems, and individuals of intermediate age up to 79 years, with infectious and genitourinary diseases, and external causes. The third profile made it possible to understand peculiarities for the Northeast, North and Central West of the country, with young individuals, whose deaths mentioning infective endocarditis were related to deaths due to diseases of the respiratory system.
Author Contributions
The authors contributed to the article as follows. João Vitor Fazzio de Andrade Cordeiro - conception, planning, data analysis, interpretation of results and writing of the paper. Leticia Martins Raposo - conception, planning, performance of statistical analysis, data analysis, writing of the paper and review of the text. Paulo Henrique Godoy - conception, planning, data analysis, interpretation of results, writing of the paper and review of the text.
Funding
This research did not receive external funding. However, the first author, who is an undergraduate medical student, receives a scientific initiation scholarship, which supports his dedication to research. This scholarship comes from the Scientific Initiation Program of the Brazilian Hospital Services Company (EBSERH), through the Teaching and Research Management of the Gaffrée e Guinle University Hospital (HUGG), in partnership with the National Council for Scientific and Technological Development (CNPq). This scholarship was awarded through Public Notice No. 06/2024.
Institutional Review Board Statement
Although the study used data from a public database, the research project was submitted to the Ethics and Research Committee of the Gafrée and Guinle University Hospital and approved, according to opinion number 7,051,294, on September 3, 2024.
Informed Consent Statement
“Not applicable.”
Data Availability Statement
The data used for investigation comes from a public database, which can be accessed by any citizen through the DATASUS website: https://datasus.saude.gov.br/.
Acknowledgments
We would like to thank EBSERH/HUGG and CNPq for encouraging research for undergraduate medical students through the scientific initiation scholarship.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Delgado, V.; Ajmone Marsan, N.; de Waha, S.; Bonaros, N.; Brida, M.; Burri, H.; Caselli, S.; Doenst, T.; Ederhy, S.; Erba, P. A.; Foldager, D.; Fosbøl, E. L.; Kovac, J.; Mestres, C. A.; Miller, O. I.; Miro, J. M.; Pazdernik, M.; Pizzi, M. N.; Quintana, E.; Rasmussen, T. B.; Ristić, A. D.; Rodés-Cabau, J.; Sionis, A.; Zühlke, L. J.; Borger, M. A.; ESC Scientific Document Group. 2023 ESC Guidelines for the Management of Endocarditis: Developed by the Task Force on the Management of Endocarditis of the European Society of Cardiology (ESC) Endorsed by the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2023, 44 (39), 3948–4042. [CrossRef]
- Ambrosioni, J.; Hernandez-Meneses, M.; Téllez, A.; Pericàs, J.; Falces, C.; Tolosana, J. M.; Vidal, B.; Almela, M.; Quintana, E.; Llopis, J.; Moreno, A.; Miro, J. M.; Hospital Clinic Infective Endocarditis Investigators. The Changing Epidemiology of Infective Endocarditis in the Twenty-First Century. Curr. Infect. Dis. Rep. 2017, 19 (5), 21. [CrossRef]
- Bin Abdulhak, A. A.; Baddour, L. M.; Erwin, P. J.; Hoen, B.; Chu, V. H.; Mensah, G. A.; Tleyjeh, I. M. Global and Regional Burden of Infective Endocarditis, 1990–2010: A Systematic Review of the Literature. Glob. Heart 2014, 9 (1), 131–143. [CrossRef]
- Ferreiros, E.; Nacinovich, F.; Casabé, J. H.; Modenesi, J. C.; Swieszkowski, S.; Cortes, C.; Arazi, H. C.; Kazelian, L.; Varini, S. Epidemiologic, Clinical, and Microbiologic Profile of Infective Endocarditis in Argentina: A National Survey. The Endocarditis Infecciosa en la República Argentina–2 (EIRA-2) Study. Am. Heart J. 2006, 151 (2), 545–552. [CrossRef]
- Damasco, P. V.; Ramos, J. N.; Correal, J. C.; Potsch, M. V.; Vieira, V. V.; Camello, T. C.; Pereira, M. P.; Marques, V. D.; Santos, K. R.; Marques, E. A.; Castier, M. B.; Hirata, R. Jr.; Mattos-Guaraldi, A. L.; Fortes, C. Q. Infective Endocarditis in Rio de Janeiro, Brazil: A 5-Year Experience at Two Teaching Hospitals. Infection 2014, 42 (5), 835–842. [CrossRef]
- Rajani, R.; Klein, J. L. Infective Endocarditis: A Contemporary Update. Clin. Med. (Lond.) 2020, 20(1), 31–35. [CrossRef]
- Cresti, A.; Baratta, P.; De Sensi, F.; Aloia, E.; Sposato, B.; Limbruno, U. Clinical Features and Mortality Rate of Infective Endocarditis in Intensive Care Unit: A Large-Scale Study and Literature Review. Anatol. J. Cardiol. 2024, 28(1), 44–54.
- Damasco, P. V.; Correal, J. C. D.; Cruz-Campos, A. C. D.; Wajsbrot, B. R.; Cunha, R. G. da; Fonseca, A. G. da; et al. Epidemiological and Clinical Profile of Infective Endocarditis at a Brazilian Tertiary Care Center: An Eight-Year Prospective Study. Rev. Soc. Bras. Med. Trop. 2019, 52, e2018375. [CrossRef]
- Jorge, M. S.; Rodrigues, A. J.; Vicente, W. V. A.; Evora, P. R. B. Cirurgia de Endocardite Infecciosa. Análise de 328 Pacientes Operados em um Hospital Universitário Terciário. Arq. Bras. Cardiol. 2023, 120(3), e20220608. [CrossRef]
- Bezerra, R. L.; Salgado, L. S.; Silva, Y. M. da; Figueiredo, G. G. R.; Bezerra Filho, R. M.; Machado, E. L. G.; et al. Epidemiological Profile of Patients with Infective Endocarditis at Three Tertiary Centers in Brazil from 2003 to 2017. Int. J. Cardiovasc. Sci. 2022, 35(4), 467–475. [CrossRef]
- Saldanha, R. de F.; Bastos, R. R.; Barcellos, C. Microdatasus: Pacote para Download e Pré-processamento de Microdados do Departamento de Informática do SUS (DATASUS). Cad. Saúde Pública 2019, 35(9), e00032419. [CrossRef]
- Wells, R. H. C.; Bay-Nielsen, H.; Braun, R.; Israel, R. A.; Laurenti, R.; Maguin, P.; Taylor, E. CID-10: Classificação Estatística Internacional de Doenças e Problemas Relacionados à Saúde; EDUSP: São Paulo, 2011.
- Lê, S.; Josse, J.; Husson, F. FactoMineR: An R Package for Multivariate Analysis. J. Stat. Softw. 2008, 25(1), 1–18. [CrossRef]
- Piron, M.; Lebart, L.; Morineau, A. Statistique Exploratoire Multidimensionnelle; DUNOD: Paris, France, 1995; 439 pp.
- Kolde, Raivo; Kolde, Maintainer Raivo. Package ‘pheatmap’. R package, v. 1, n. 7, p. 790, 2015. || pheatmap Package Documentation. https://cran.r-project.org/web/packages/pheatmap/index.html (accessed 01-10-2024).
- Avellana, P. M.; Aurelio, M. G.; Swieszkowski, S.; Nacinovich, F.; Kazelian, L.; Spennato, M.; Gagliardi, J. A. Infective Endocarditis in Argentina: Results of the EIRA 3 Study. Rev. Argent. Cardiol. 2018, 86(1), 19–27.
- Cresti, A.; Chiavarelli, M.; Scalese, M.; Nencioni, C.; Valentini, S.; Guerrini, F.; D’Aiello, I.; Picchi, A.; De Sensi, F.; Habib, G. Epidemiological and Mortality Trends in Infective Endocarditis: A 17-Year Population-Based Prospective Study. Cardiovasc. Diagn. Ther. 2017, 7(1), 27–35.
- Oliveira, J. M.; Freitas, R. B.; Quirino, R. L.; Gomes, J. H.; Paula, B. P. Levantamento da Morbimortalidade por Endocardite de Valva no Brasil: Análise das Complicações da Doença e os Desafios do Diagnóstico e Terapêutica para a Melhora do Paciente. Braz. J. Health Rev. 2023, 6(6), 32590–32603.
- Instituto Brasileiro de Geografia e Estatística (IBGE). Censo Demográfico 2022: Resultados Gerais. Available online: https://www.ibge.gov.br/ (accessed on 18 September 2024).
- Diógenes, V. H. D.; Pinto Júnior, E. P.; Gonzaga, M. R.; Queiroz, B. L.; Lima, E. E. C.; Costa, L. C. C. da; et al. Differentials in Death Count Records by Databases in Brazil in 2010. Rev. Saúde Pública 2022, 56, 92. [CrossRef]
- David, L. E. S.; Cirilo, L. M.; Borges, P. V. B.; Souza, R. A. O.; Chalegre, M. C. T.; Silva, L. M. F.; Lima, L. C. S. Avaliação do Perfil Epidemiológico da Mortalidade por Endocardite Infecciosa no Brasil entre 2012 e 2021. In Anais do XXIII Congresso Brasileiro de Infectologia, Outubro de 2023; The Brazilian Journal of Infectious Diseases, 2023; Vol. 27, Supplement 1, Paper e8828. [CrossRef]
- Melo, S. N. de; Torres, B. R. S.; Nascimento, M. M. G. do; Júnior, A. F. da S. X.; Rodrigues, W. G.; Lima, R. B. de S.; Souza, N. S. S. de; Menezes, L. E. de F. B. Caracterização do Perfil Epidemiológico da Mortalidade por Endocardite Infecciosa na Região Nordeste de 2010–2019. Rev. Eletrônica Acervo Saúde 2021, 13(9), e8828. [CrossRef]
- Ahtela, E.; Oksi, J.; Sipilä, J.; Rautava, P.; Kytö, V. Occurrence of Fatal Infective Endocarditis: A Population-Based Study in Finland. BMC Infect. Dis. 2019, 19(1), 987. [CrossRef]
- Costa, M. A. C. da; Wollmann Jr, D. R.; Campos, A. C. L.; Cunha, C. L. P. da; Carvalho, R. G. de; Andrade, D. F. de; et al. Índice de Risco de Mortalidade por Endocardite Infecciosa: Um Modelo Logístico Multivariado. Braz. J. Cardiovasc. Surg. 2007, 22(2), 192–200. [CrossRef]
- Marques, A.; Cruz, I.; Caldeira, D.; Alegria, S.; Gomes, A. C.; Broa, A. L.; et al. Risk Factors for In-Hospital Mortality in Infective Endocarditis. Arq. Bras. Cardiol. 2020, 114(1), 1–8. [CrossRef]
- Muñoz, P.; Kestler, M.; De Alarcon, A.; Miro, J. M.; Bermejo, J.; Rodríguez-Abella, H.; Fariñas, M. C.; Cobo Belaustegui, M.; Mestres, C.; Llinares, P.; Goenaga, M.; Navas, E.; Oteo, J. A.; Tarabini, P.; Bouza, E.; Spanish Collaboration on Endocarditis-Grupo de Apoyo al Manejo de la Endocarditis Infecciosa en España (GAMES). Current Epidemiology and Outcome of Infective Endocarditis: A Multicenter, Prospective, Cohort Study. Medicine (Baltimore) 2015, 94(43), e1816. [CrossRef]
- Sousa, C.; Pinto, F. J. Endocardite Infecciosa: Ainda Mais Desafios que Certezas. Arq. Bras. Cardiol. 2022, 118(5), 976–988. [CrossRef]
Figure 1.
Deaths due to other diseases mentioned together with deaths due to IE, according to the chapters of ICD-10, in Brazil and regions, from 2000 to 2019.
Figure 1.
Deaths due to other diseases mentioned together with deaths due to IE, according to the chapters of ICD-10, in Brazil and regions, from 2000 to 2019.
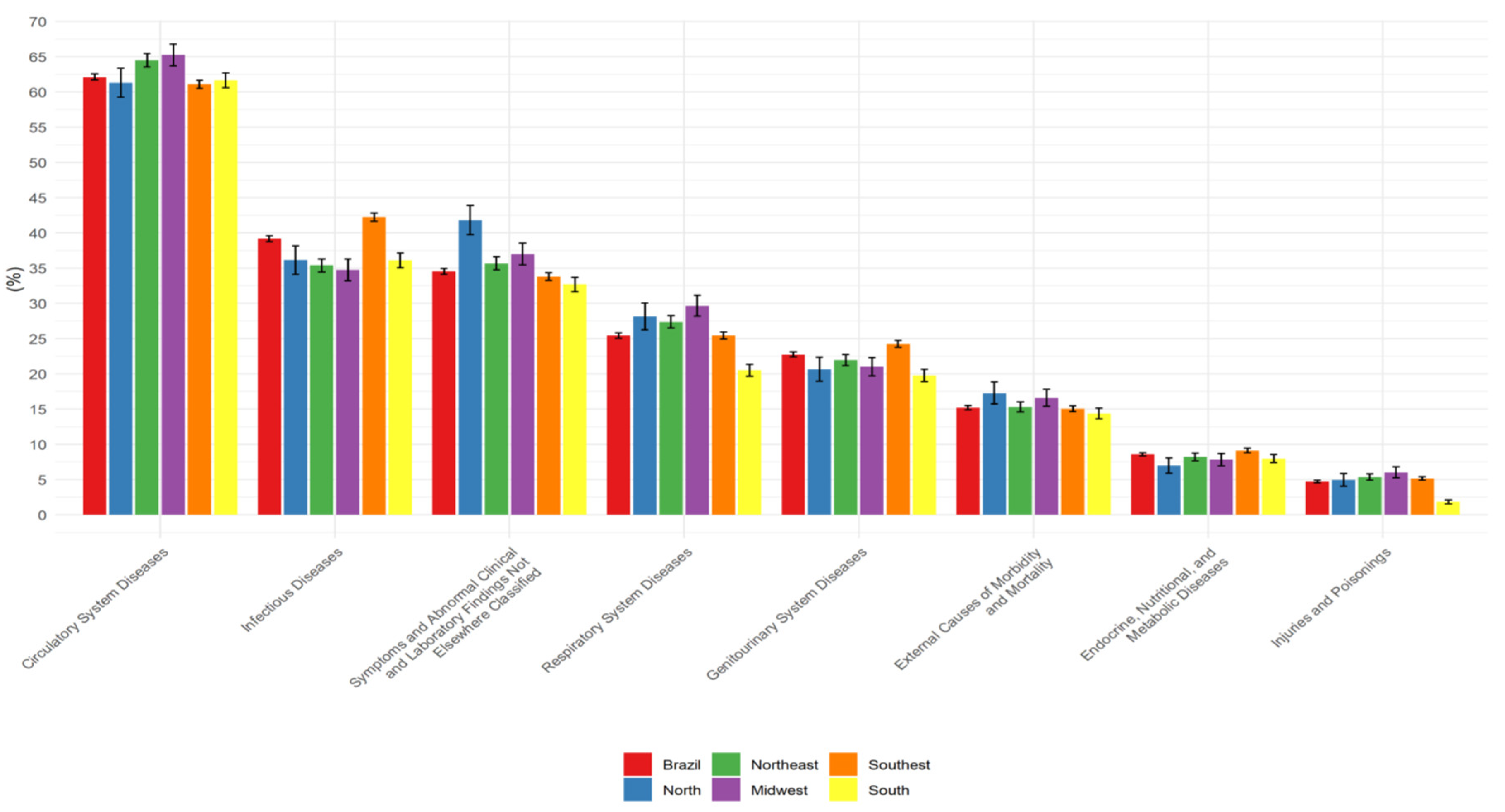
Figure 2.
Profiles of deaths with mention of EI, grouped by characteristics, according to the clusters identified by Multiple Correspondence Analysis.
Figure 2.
Profiles of deaths with mention of EI, grouped by characteristics, according to the clusters identified by Multiple Correspondence Analysis.
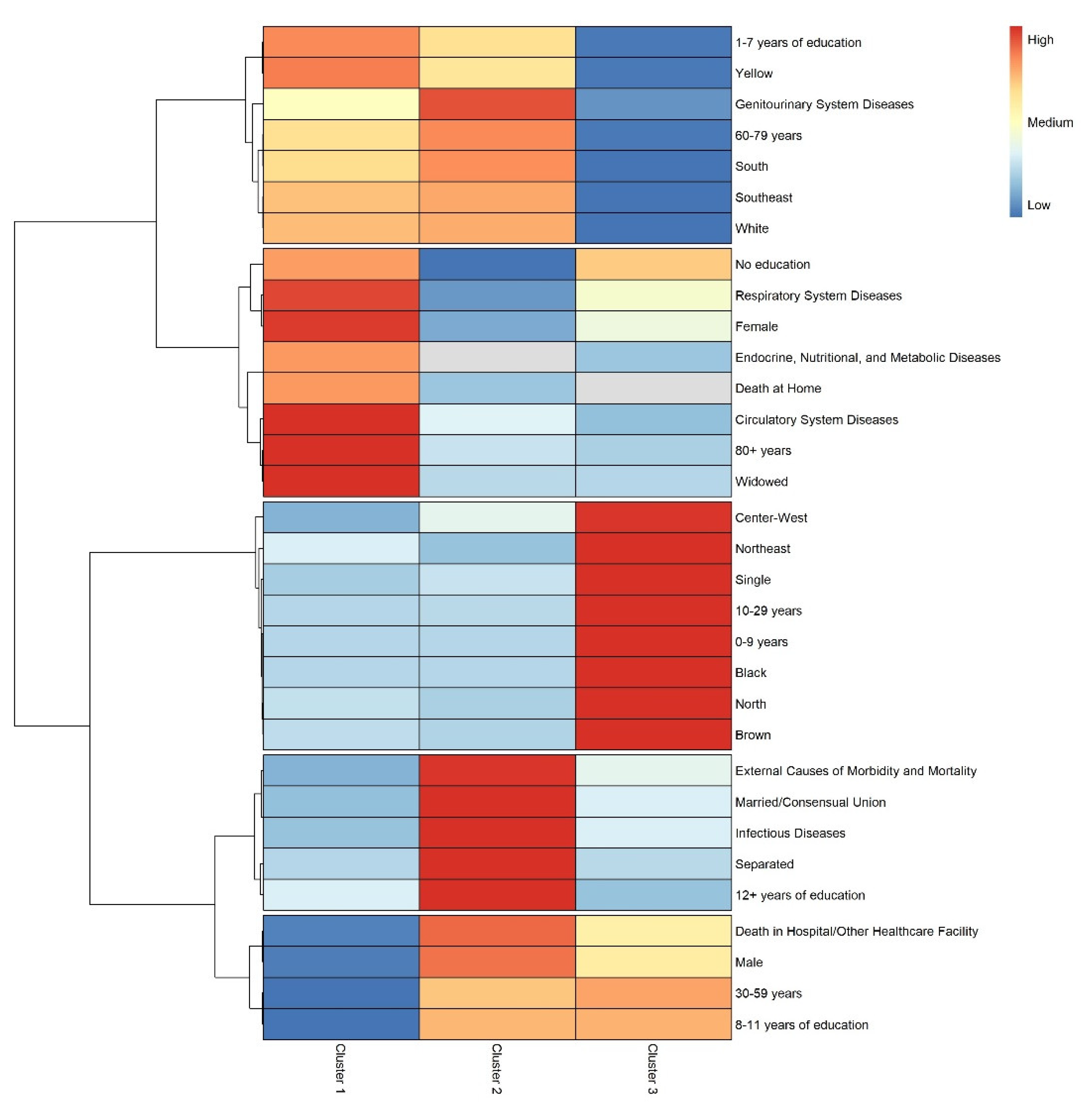

Table 1.
Deaths due to infective endocarditis, in Brazil and regions, according to sociodemographic variables, from 2000 to 2019.
Table 1.
Deaths due to infective endocarditis, in Brazil and regions, according to sociodemographic variables, from 2000 to 2019.
| Characteristics | Brazil 52.0551 |
North 2.1681 |
Northeast 9.9221 |
Midwest 3.6451 |
Southeast 28.1141 |
South 8.2061 |
p-value2 |
|---|---|---|---|---|---|---|---|
| Age group (years) | <0,001 | ||||||
| 0 to 9 | 1.492 (2.9%) | 150 (6.9%) | 355 (3.6%) | 95 (2.6%) | 756 (2.7%) | 136 (1.7%) | |
| 10 to 29 | 4.210 (8.1%) | 400 (18.5%) | 1.509 (15.2%) | 316 (8.7%) | 1.596 (5.7%) | 389 (4.7%) | |
| 30 to 59 | 19.003 (36.5%) | 897 (41.4%) | 3.887 (39.2%) | 1.528 (41.9%) | 9.939 (35.4%) | 2.752 (33.5%) | |
| 60 to 79 | 20.135 (38.7%) | 580 (26.8%) | 2.997 (30.2%) | 1.322 (36.3%) | 11.531 (41.0%) | 3.705 (45.1%) | |
| 80 or more | 7.215 (13.9%) | 141 (6.5%) | 1.174 (11.8%) | 384 (10.5%) | 4.292 (15.3%) | 1.224 (14.9%) | |
| Gender | <0,001 | ||||||
| Female | 23.593 (45.3%) | 937 (43.2%) | 4.644 (46.8%) | 1.637 (44.9%) | 12.896 (45.9%) | 3.479 (42.4%) | |
| Male | 28.462 (54.7%) | 1.231 (56.8%) | 5.278 (53.2%) | 2.008 (55.1%) | 15.218 (54.1%) | 4.727 (57.6%) | |
| Race/Color | <0,001 | ||||||
| Yellow | 336 (0.7%) | 7 (0.3%) | 22 (0.2%) | 17 (0.5%) | 263 (1.0%) | 27 (0.3%) | |
| White | 30.908 (63.6%) | 604 (29.0%) | 2.963 (33.0%) | 1.761 (50.7%) | 18.491 (70.4%) | 7.089 (91.2%) | |
| Indigenous | 83 (0.2%) | 27 (1.3%) | 9 (0.1%) | 22 (0.6%) | 15 (0.1%) | 10 (0.1%) | |
| Brown | 13.702 (28.2%) | 1.307 (62.7%) | 5.179 (57.7%) | 1.443 (41.5%) | 5.419 (20.6%) | 354 (4.6%) | |
| Black | 3.546 (7.3%) | 138 (6.6%) | 804 (9.0%) | 232 (6.7%) | 2.083 (7.9%) | 289 (3.7%) | |
| Unknown | 3.480 | 85 | 945 | 170 | 1.843 | 437 | |
| Marital Status | <0,001 | ||||||
| Single | 12.534 (26.2%) | 761 (39.9%) | 3.260 (38.0%) | 948 (28.8%) | 6.162 (23.4%) | 1.403 (18.1%) | |
| Married/Consensual union | 23.873 (49.9%) | 876 (45.9%) | 3.920 (45.7%) | 1.613 (49.1%) | 13.153 (49.9%) | 4.311 (55.5%) | |
| Legally separated | 3.121 (6.5%) | 78 (4.1%) | 296 (3.5%) | 243 (7.4%) | 1.992 (7.6%) | 512 (6.6%) | |
| Widowed | 8.338 (17.4%) | 192 (10.1%) | 1.097 (12.8%) | 483 (14.7%) | 5.028 (19.1%) | 1.538 (19.8%) | |
| Unknown | 4.189 | 261 | 1.349 | 358 | 1.779 | 442 | |
| Education Level | <0,001 | ||||||
| None | 3.750 (10.4%) | 228 (13.7%) | 1.126 (17.6%) | 368 (13.6%) | 1.561 (8.1%) | 467 (8.0%) | |
| 1 to 7 years | 20.353 (56.7%) | 864 (51.8%) | 3.388 (53.0%) | 1.496 (55.1%) | 10.888 (56.5%) | 3.717 (63.6%) | |
| 8 to 11 years | 7.746 (21.6%) | 418 (25.1%) | 1.290 (20.2%) | 587 (21.6%) | 4.320 (22.4%) | 1.131 (19.4%) | |
| 12 years or more | 4.037 (11.2%) | 158 (9.5%) | 583 (9.1%) | 263 (9.7%) | 2.505 (13.0%) | 528 (9.0%) | |
| Unknown | 16.169 | 500 | 3.535 | 931 | 8.840 | 2.363 | |
| Place of Death | <0,001 | ||||||
| Home | 3.027 (5.8%) | 94 (4.3%) | 735 (7.4%) | 273 (7.5%) | 1.310 (4.7%) | 615 (7.5%) | |
| Hospital/Other healthcare facility | 48.378 (93.0%) | 2.047 (94.6%) | 9.014 (91.0%) | 3.316 (91.0%) | 26.554 (94.5%) | 7.447 (90.9%) | |
| Others | 604 (1.2%) | 23 (1.1%) | 152 (1.5%) | 53 (1.5%) | 241 (0.9%) | 135 (1.6%) | |
| Unknown | 46 | 4 | 21 | 3 | 9 | 9 | |
| 1n (%); 2Chi-squared test of independence | |||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



