
Submitted:
08 October 2024
Posted:
09 October 2024
You are already at the latest version
Abstract
Maintaining patient trust, providing quality care, and safeguarding patients' rights and safety, all of which require strong adherence to ethical principles. This study assessed the key differential factors influencing healthcare ethics (HCE) practice in two Ghanaian hospitals. This study employed an analytical cross-sectional design, utilizing simple random sampling to recruit 382 healthcare professionals. Bivariate analysis was conducted using Chi-square tests and T-tests, while Random Forest analysis was applied to identify variables of relative importance to HCE practice. The study found no significant differences in HCE knowledge or practices between the facilities. However, in both facilities, knowledge of HCE significantly influenced HCE practice, indicating that individuals with better knowledge of HCE were more likely to practice HCE. Further, the analysis identified age, knowledge, education, and facility type as the most relevant factors in general. In the sub-analysis, the key factors varied between facilities: for Facility A, age, knowledge, gender, and the intention to change profession were most relevant, while for Facility B, knowledge, education, gender, and age were the dominant factors. HCE training programs should be tailored to meet the unique needs of each facility to ensure effectiveness since factors influencing HCE may vary by facility.
Keywords:
knowledge
; practice gap
; healthcare ethics
; healthcare workers
; Ghanaian hospitals
1. Introduction
Healthcare delivery goes beyond clinical skills and knowledge; it extends to fulfilling ethical and legal expectations integral to medical practice [1]. Medical ethics form a cornerstone of healthcare delivery, guiding practitioners in their responsibilities toward patients, colleagues, and society [2]. Ethical principles, particularly autonomy, beneficence, non-maleficence, and justice, shape professional conduct in healthcare, ensuring patient dignity, respect, and fairness [3]. Compliance with these principles is crucial for maintaining trust, providing quality care, and safeguarding patients’ rights [4].
However, compliance with ethical standards remains a challenge as healthcare professionals navigate complex ethical dilemmas [5]. These challenges arise due to various factors, including competing personal, organizational, and professional values, as well as cultural diversity [6]. The rapidly evolving nature of medical technology and scientific advancements presents complex ethical and legal challenges in healthcare [7], necessitating strict adherence to ethical practices to safeguard patient care and uphold professional integrity. Moreover, global healthcare systems face increasingly complex ethical challenges that impact patient outcomes, necessitating consistent application of ethical principles by healthcare professionals [8].
In African healthcare systems, ethical challenges have become more pronounced, with an increase in legal complaints and litigation against healthcare professionals [9,10]. This rise in legal scrutiny highlights gaps in the knowledge and application of medical ethics among healthcare practitioners [11]. For instance, research from Nigeria reveals that many healthcare providers lack an adequate understanding of ethical principles, with their perceptions primarily based on undergraduate training and work experience [12]. Research in Ghana has shown that while many healthcare workers demonstrate good ethical knowledge and positive attitudes, there are gaps between knowledge and actual practice [13,14].
The persistence of paternalistic approaches to patient care further complicates ethical compliance, especially in contexts where healthcare professionals are blindly trusted without adequate checks on their ethical decision-making [15]. Despite these challenges, the ethical behavior of healthcare professionals is critical to the quality of healthcare delivery. Studies have shown that ethical sensitivity among healthcare workers is influenced by factors such as age, profession, and work experience [16]. Ethical lapses can jeopardize patient safety, compromise the reputation of healthcare providers, and lead to legal consequences [17]. In this context, Ghana has initiated measures to enhance compliance with medical ethics, concentrating on training programs that integrate local cultural competence and international ethical standards. Nurses in Ghana are guided by both the International Council of Nurses’ Code and local cultural practices when addressing ethical dilemmas [18]. Ghana has also focused on improving medical physics training, collaborating with international organizations to ensure practitioners meet global standards [19]. Nevertheless, knowledge gaps persist, particularly in the practical application of ethical principles in clinical settings.
Recent research has emphasized that multiple factors, such as knowledge, age, education, and gender, influence ethical practice among healthcare professionals [14,20]. However, knowledge remains the most crucial factor influencing ethical practice [21]. In Ghana, the absence of continuous professional development programs aimed at enhancing medical ethics knowledge has been identified as a critical issue. Therefore, this research aims to investigate the levels of awareness, comprehension, and adherence to medical ethics among healthcare professionals in Ghana and provide practical advice to the Ghana Medical Association, Nurses and Midwife Council, legislators, and healthcare organizations by analyzing some factors that impact ethical compliance. These findings could also assist in devising targeted interventions to improve ethical standards, enhance patient care outcomes, and promote a culture of ethical excellence in the Ghanaian healthcare system and beyond.
2. Materials and Methods
2.1. Study Settings
The study was carried out in two healthcare facilities (Facility A and B) in the Central region of Ghana. Central region is one of the 16 regions of Ghana. It is bordered by the Ashanti region and Eastern region to the north, the Western region to the west, Greater Accra to the east, and the Gulf of Guinea to the south. The current estimated population is 2,900,00, with a sex ratio of 48.6 males to 51.4 females and an annual growth rate of 2.1% [22]. The region has 20 districts, with Cape Coast Metropolitan Assembly as the administrative head, and Cape Coast as the regional capital. The region boasts 618 health facilities including 414 CHPS facilities, 132 health Centers and clinics, 25 maternity homes, 45 hospitals and polyclinics, and 1 regional hospital and teaching hospital, evenly distributed in the various districts of the region.
One of the facilities (Facility A) is a specialized secondary referral health facility, while the other is a government primary hospital. Both facilities are national health insurance accredited. They act as referral points for other hospitals, health centers, and clinics in the region and beyond. Facility A offers specialized care services; restorative, promotive, and rehabilitative healthcare by highly motivated, skilled, and client-focused staff in collaboration with stakeholders. Conversely, Facility B’s vision focuses on providing general services, such as the outpatient department (OPD), diagnostics, general surgery, obstetrics, and gynecological care, pediatric care as well as general preventive care.
2.2. Study Design
An analytical cross-sectional design was used to establish the relationship between two health facilities in relation to their knowledge and compliance with ethical practices and the association between socio-demographic factors and the practice of ethics at the health facility between March and May 2023.
2.3. Population
The target population of the study included medical doctors and nurses who were permanent staff at the two selected health facilities in the central region. These cadres of staff were selected due to their continuous and physical contact with health service seekers. They typically have more contact hours with patients/clients compared to any other workers at the health facility. One cannot seek healthcare services without having contact with these health workers. Nurses are the first point of contact at the hospital. They provide OPD services by taking history and offering nursing care, diagnostic care, medication administration, health assessment, and promotion services. On the other hand, medical doctors tend to have more contact. They provide diagnostic and treatment services, perform physical examinations, prescribe medications, perform surgeries, and offer preventive care services. The study included only those who have worked for more than a year, and permanent staff available during data collection. However, health workers who were on contract, on rotation, and those who refused to participate in the study were excluded from participation.
2.4. Sampling and Sample Size
A simple random sampling technique was used to select the respondents from the sampling frame, the list of nurses and medical doctors in the two health facilities. As only medical doctors and nurses were the target population for the two health facilities, it was relatively simple to sample and for that matter, the complete enumeration was the rational choice to enable the study to gather an adequate sample size for the study. Out of the total sample of 419 nurses and medical doctors from the two health facilities, 382 were available and agreed to participate in the study.
2.5. Data Collection Tool
Data was collected using a structured questionnaire that was developed. The structured questionnaire contained both close-ended and open-ended questions. The questionnaire was developed based on the objectives and adapted from pre-existing instruments [23,24]. The final drafted tool was structured into three sections. The first section questioned the respondents about their personal and demographic information. The second section had questions that assessed the level of knowledge of the respondents on medical ethics. The third section consisted of questions that determined the respondents’ level of practice of medical ethics. The questionnaires were self-administered, and a high level of discretion was maintained to protect the identity and views of the respondents.
2.5.1. Knowledge of Healthcare Ethics
The knowledge of healthcare ethics was assessed using nine items, each rated on a four-point Likert scale. The nine items yielded a Cronbach’s alpha of 0.6, indicating moderate internal consistency [25]. A sample item included, “There is no need for the health practitioner to seek informed consent from patients,” with responses ranging from “strongly disagree” to “strongly agree.” To enhance variability, items were coded from 1 to 4 with higher scores indicating a higher level of correct knowledge. For instance, for the sample item, responses of “strongly disagree” were coded as 4. The composite score was calculated by summing the scores of all nine items. In our sample, the maximum observed composite score was 33, and the minimum was 17.
2.5.2. Practise of Healthcare Ethics
We assessed healthcare ethics practice among professionals using eight items, with responses rated on a four-point scale from “never” to “always.” A Cronbach’s alpha of 0.60 was estimated for the reliability of the eight items. One of the items included was, “Consciously or unconsciously, I sometimes found myself using my mobile phone for non-medical or administrative purposes while on duty.” Similar to the knowledge assessment in healthcare ethics, responses were coded to indicate adherence, with higher scores representing greater adherence. Specifically, responses indicating a higher level of adherence were coded as 4, while those indicating lower adherence were coded as 1. For the sample item, for instance, responses of “Never” were coded as 4, and “Always” as 1. We calculated the composite score by summing the scores for all items, which was then used in subsequent analysis. In this sample, the minimum practice score was 16, and the maximum score was 30.
2.5.3. Demographics
We collected information on participants’ gender, age, marital status, educational level, and intention to change profession. Personality was assessed by asking the question, “How introverted or extroverted are you?” In this context, an introvert is defined as someone who is shy and quiet and prefers to spend time alone or with one or two people, while an extrovert is characterized as an outgoing person who enjoys talking to and being with many people. Participants responded with, “I would say that I am predominantly...”
2.6. Data Collection Procedure
Data collection only began after ethical clearance was approved by the Ghana Health Service Ethics Review Committee. Data collection was conducted at the hospital premises after obtaining permission from the heads of the two facilities. The questionnaire was given to qualified persons and they were supposed to be collected after two weeks; however, it took between 4 to 5 weeks before almost all the questionnaires distributed to the health workers were retrieved. The response rate was 94.6% and a few refused to return them since they withdrew from the study with no reason given to the research team. Data collection spanned from the 4th of March to the 31st of May 2023.
2.7. Statistical Analysis
First, we report the sample count and percentages for the overall sample and by facility. This is followed by a bivariate analysis. Specifically, the Chi-square test was conducted for the categorical variables. The T-test was used for the continuous variables to assess facility differences. Random Forest, a machine learning regression method, was used to analyze factors that influence the practice of HCE. Random Forest is known to provide more robust results, especially where the sample size is relatively small, and also captures complex interactions and nonlinear relationships compared to other regression methods [26,27,28,29,30]. The percentage increase in mean squared error (%IncMSE) and the increase in node purity (IncNodePurity) were employed to assess variable importance in predicting HCE. The %IncMSE evaluates model accuracy when a variable is permuted, with higher values indicating greater variable importance [31]. The IncNodePurity assesses how much the model error increases when a variable is randomly permuted. The results from the Random Forest analysis were plotted to improve the interpretation of the order of variable importance.
3. Results
Facility A represents 55% of our sample, while Facility B represents the rest. Females constitute the majority (58.4%) in the gender domain. Approximately 63.4% (n = 242) of our sample hold a diploma or lower qualification. Most of them identify as extroverts (55%), with the rest being introverts. Roughly 64% and 65% of our sample were unmarried and expressed no desire to switch professions, respectively. The mean age of our sample was estimated at 28 with a standard deviation (SD) of 5.37. A mean of 26.3 (SD = 2.83) and 23.50 (SD = 2.94) was also observed for the scores of participant’s knowledge and practice of healthcare ethics, respectively. Except for age and educational level, there were no statistically significant differences between Facility A and B for the majority of the variables examined in the study. Table 1 highlights the details.
3.1. Influence of HCE Knowledge on HCE Practise
3.2. Key Influencing Factors of Healthcare Ethics Practice
The mean Residual Sum of Squares (RSS) for the general dataset, Facility A, and Facility B is estimated at [insert values] respectively. Table 2 presents the results of the Random Forest analysis conducted on the entire dataset (general) and separately by facility (Facility A and Facility B) in the practice of healthcare ethics. The Random Forest analysis highlights knowledge, age, and education as key factors influencing the practice of healthcare ethics.
3.3. Order of Influencing Factors of Healthcare Ethics
Illustratively, Figure 2, Figure 3 and Figure 4 visualize the order of importance (highest from the top and decrease below) in the prediction of healthcare ethics in the overall sample and by facility. On the %IncMSE side, indicating a variable’s importance in predicting the outcome, age, knowledge, and education were systematically identified as the top three crucial variables. On the IncNodePurity (improving the homogeneity) side, age, knowledge, and facility were identified.
While age, knowledge, and gender are the order of importance for Facility A (Figure 3), age was not identified among the first three important influencing factors for Facility B (Figure 4). However, it was identified as the second most important variable in enhancing homogeneity. Furthermore, although education and marital status were deemed the least influential factors in Facility A, the intention to change profession and personality were considered the least relevant factors in predicting HCE practice. Overall, the importance order of variables differed between Facility A and Facility B, highlighting variations in the factors affecting healthcare ethics practice at each facility.
Knowledge was consistently the most important factor, particularly in Facility B, where it had the highest % of IncMSE (33.3) and IncNodePurity (299.9) values. Gender also showed a notable influence, especially in Facility A, with a %IncMSE of 17 and the highest IncNodePurity of 96.3. Variables such as personality and intention to change profession also demonstrated a moderate influence across all three analysis domains. Generally, the strengths in both %IncMSE and IncNodePurity for Facility A and Facility B differed by variable.
4. Discussion
This study determined the knowledge and practice of healthcare ethics at two healthcare facilities. It identified key influencing factors such as age, education, knowledge, and gender. The study contributed to understanding how both institutional and personal factors shape healthcare workers’ ethical behavior.
Healthcare ethics (HCE) guides professionals in making decisions that prioritize patient care. HCE knowledge lays the foundation for understanding key principles such as autonomy, beneficence, and justice in complex medical situations [3]. Although the study reveals no statistically significant difference in HCE knowledge between Facility A and Facility B, the factors influencing their ethical practices may differ, suggesting a need for facility-specific ethics education programs to bridge the gap between knowledge and practice. This finding aligns with a study by Mortell [32] which suggests that knowledge alone does not always translate into ethical practice. While knowledge is a crucial factor, particularly evident in Facility B where it had a relatively high impact on HCE practice, it must be supported by ongoing ethical education and practical training. Sustained ethics training programs that go beyond theory are essential, ensuring that healthcare workers are equipped to translate knowledge into action in real-world scenarios.
Thomas et al. [33] emphasize that professional education plays a pivotal role in shaping ethical behavior, as healthcare professionals with higher levels of training are better equipped to recognize and address ethical dilemmas. Furthermore, Sultana & Kitchlew [34] emphasize that the workplace environment, including relationships, communication, and organizational climate, significantly impacts the institutionalization of ethics. Ethical challenges often require more than theoretical knowledge, highlighting the need for experiential learning in ethics. Therefore, ethics training must evolve to incorporate hands-on, experiential learning opportunities, fostering a culture of ethical decision-making within healthcare institutions.
Research indicates that demographic factors influence ethical healthcare practices. Age, gender, and education impact ethical practices in healthcare, influencing decision-making and behavior among professionals [35,36]. This study also reveals that age and education are important factors in predicting the practice of healthcare ethics. Age is particularly important in Facility A, where it ranks as the top factor. The study shows a similar direction to research conducted by Kirilmaz, Akbolat & Kahraman [16], which mentioned that older healthcare professionals tend to demonstrate higher levels of ethical behavior, possibly due to greater experience in handling complex situations that require ethical decision-making. Healthcare institutions should harness the experience of older professionals by integrating mentorship opportunities that enhance the ethical practices of younger staff. Gender is also identified as a significant influencing factor, particularly in Facility A. Our study is consistent with previous studies [37] and also demonstrates that ethical practices may be influenced by gender. Women in healthcare may be more likely to emphasize ethical considerations related to patient care, possibly due to differences in empathy and communication styles compared to their male counterparts [37]. Implementing gender-sensitive ethics training could harness these strengths, fostering a more inclusive and empathetic approach to ethical practice.
Education is another variable that significantly impacts HCE practice, especially in Facility B, where it was ranked among the top three influencing factors. Higher levels of education have been linked to better ethical practice in numerous studies [38,39]. Healthcare professionals with advanced degrees are more likely to have received thorough training in ethical principles, enabling them to navigate ethical challenges more effectively. Advanced educational opportunities and continual professional development are essential, as they sharpen ethical decision-making skills and enhance overall healthcare delivery. González-Blázquez et al. [40] note that healthcare workers who receive ethics training as part of their higher education are better equipped to handle ethical dilemmas, highlighting the importance of integrating ethics into professional training programs. Regular updates to ethics courses and consideration of regional and disciplinary differences are recommended to enhance ethical healthcare practice [40]. Ethics education should be integrated into all stages of professional development to guarantee a consistent and comprehensive approach to ethical practice among healthcare professionals. This implies that a dynamic, evolving ethics curriculum is vital, ensuring that professionals stay current with emerging ethical challenges in healthcare.
Personality traits, such as extroversion and introversion, may impact how healthcare workers interact with patients and colleagues, ultimately influencing their ethical behavior [41]. For instance, extroverts, due to their socially outgoing nature, may engage more deeply in patient-centered care, emphasizing ethical principles like autonomy and beneficence through active communication and empathy. In contrast, introverts may approach interactions with greater reservation, leading to more reflective and considered ethical decision-making, though their methods of patient advocacy may differ. These insights suggest that ethics training programs could benefit from a personalized approach, tailoring learning experiences that leverage the distinct strengths of different personality types to enhance ethical practice. Moreover, it is anticipated that employees who plan to remain in their profession will demonstrate a stronger commitment to acting in accordance with their professional codes of conduct [42] compared to those who intend to change careers. While personality traits and the intention to stay in a profession are relevant factors, our study suggests that they may not be as significant in influencing healthcare ethics practice as other factors, such as educational background, age, type of institution, and gender.
Variations in healthcare settings can significantly impact the factors influencing ethical practices among professionals. One of the key contributions of this study is its identification of differences between the two facilities regarding the factors that influence healthcare ethics (HCE) practice. While age, knowledge, and gender are the most important factors in Facility A, Facility B places a stronger emphasis on knowledge, age, and education. This suggests that different healthcare settings may require tailored approaches to ethics training and professional development. These findings align with studies by White, Jordens, and Kerridge [43], suggesting that one-size-fits-all approaches to ethics education in healthcare are insufficient. Each healthcare facility has its own unique culture, patient demographics, and institutional challenges, all of which can affect the ethical behavior of healthcare professionals. Thus, ethics programs should be carefully designed to meet the distinct needs of each healthcare facility, ensuring that ethical practices align with the specific institutional contexts in which healthcare professionals operate.
5. Conclusion and Implications for Practice
This study offers valuable insights into the factors influencing healthcare ethics practice in two healthcare facilities. Knowledge, age, education, and gender were found to be the most significant predictors of ethical behavior, with variations between facilities. The findings highlight the need for tailored ethics training programs that consider the unique characteristics of each healthcare facility. Ongoing education and practical training in healthcare ethics are crucial in ensuring that healthcare professionals can apply ethical principles in their practice, ultimately leading to improved patient care and outcomes.
Author Contributions
Conceptualization, P.O.A. and F.K.; methodology, P.O.A. and F.K.; Software, P.O.A. and F.A.; validation, P.O.A., F.K. and F.A; formal analysis, F.A. and P.O.A.; investigation, F.K. and J.F.A-D.; resources, P.O.A., F.K. and F.A.; writing—original draft preparation, P.O.A., F.K., F.A and J.F.A-D.; writing—review and editing, P.O.A., F.A. and E.M.; supervision, E.M.; project administration, P.O.A. and E.M. All authors have read and agreed to the published version of the manuscript
Funding
This research received no external funding
Informed Consent Statement
This study was approved by Ghana Health Service Ethics Review Committee.
Data Availability Statement
Data used in this study are available on request
Acknowledgments
We would like to express our sincere gratitude to all participating hospitals for their invaluable support and collaboration in this study. A special thanks to the healthcare professionals who generously shared their time, insights, and experiences. Your participation and dedication were essential to the success of this research.
Conflicts of Interest
The authors declare no conflict of interest
References
- Unnikrishnan, B.; Kanchan, T.; Kulkarni, V.; Kumar, N.; Papanna, M.K.; Rekha, T.; Mithra, P. Perceptions and practices of medical practitioners towards ethics in medical practice–A study from coastal South India. Journal of Forensic and Legal Medicine 2014, 22, 51–56. [Google Scholar] [CrossRef] [PubMed]
- Faden, R.R.; Kass, N.E.; Goodman, S.N.; Pronovost, P.; Tunis, S.; Beauchamp, T.L. An ethics framework for a learning health care system: a departure from traditional research ethics and clinical ethics. Hastings Center Report 2013, 43, S16–S27. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, A.; Ali, H.S.; Mahmoud, M.A. Prioritizing Well-being of Patients through Consideration of Ethical Principles in Healthcare Settings: Concepts and Practices. Systematic Reviews in Pharmacy 2020, 11, 643–648. [Google Scholar]
- Quitio Arevalo, C.M.; Guambuguete, J.I. Principios éticos del cuidado enfermero en seguridad. relatos de pacientes dados de alta. Hospital Alfredo Noboa Montenegro octubre 2019–febrero 2020. bachelor’s thesis, Universidad Estatal de Bolìvar: Carrera de Enfermeria.
- Jones-Bonofiglio, K. Health care ethics through the lens of moral distress; Springer: Cham, 27 Aug 2020. [Google Scholar]
- Wesarat, P.O.; Mathew, J. Linking ethical standards for healthcare professionals with Indian cultural values. Asia Pacific Journal of Health Management 2021, 16, 49–58. [Google Scholar]
- Hall, M.A.; Bobinski, M.A.; Orentlicher, D.; Cohen, I.G.; Bagley, N.; Sawicki, N.N. Health Care Law and Ethics: [Connected EBook]; Aspen Publishing, 19 Feb 2024. [Google Scholar]
- Mousavi, S. Global Ethical Principles in Healthcare Networks, Including Debates on Euthanasia and Abortion. Cureus 2024, 16. [Google Scholar] [CrossRef]
- Pepper, M.S.; Slabbert, M.N. Is South Africa on the verge of a medical malpractice litigation storm? South African Journal of Bioethics and Law 2011, 4, 29–35. [Google Scholar]
- Moodley, K.; Kabanda, S.M.; Kleinsmidt, A.; Obasa, A.E. COVID-19 underscores the important role of Clinical Ethics Committees in Africa. BMC Medical Ethics 2021, 22, 1–9. [Google Scholar]
- Srivastav, S. Medico-Legal Practices and Doctor-Patient Relationship in India’s Evolving Healthcare Landscape. Healthcare Administration and Managerial Training in the 21st Century 2024 (pp. 107-146). IGI Global.
- Monsudi, K.F.; Oladele, T.O.; Nasir, A.A.; Ayanniyi, A.A. Medical ethics in sub-Sahara Africa: closing the gaps. African Health Sciences 2015, 15, 673–681. [Google Scholar] [CrossRef]
- Coleman, A.M. Baseline Survey of knowledge, attitude, and practice of healthcare ethics, in healthcare practitioners of a tertiary healthcare institution in Ghana, a Sub-Saharan Country. Bangladesh Journal of Bioethics 2023, 14, 7–12. [Google Scholar] [CrossRef]
- Asare, P.; Ansah, E.W.; Sambah, F. Ethics in healthcare: Knowledge, attitude, and practices of nurses in the Cape Coast Metropolis of Ghana. PloS one 2022, 17, e0263557. [Google Scholar] [CrossRef]
- Ofosu-Poku, R. Perspective Chapter: Who Is Making Decisions? An open letter to healthcare professionals in the developing world. In Suggestions for Addressing Clinical and Non-Clinical Issues in Palliative Care; 2021; Volume 325. [Google Scholar]
- Kirilmaz, H.; Akbolat, M.; Kahraman, G. Research about the ethical sensitivity of healthcare professionals. International Journal of Health Sciences 2015, 3, 73–82. [Google Scholar] [CrossRef]
- Kadakia, E. Navigating the Complexities of Medical Error and Its Ethical Implications. Doctoral dissertation, Temple University. Libraries.
- Donkor, N.T.; Andrews, L.D. Ethics, culture and nursing practice in Ghana. International nursing review 2011, 58, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Amuasi, J.H.; Kyere, A.K.; Schandorf, C.; Fletcher, J.J.; Boadu, M.; Addison, E.K.; Hasford, F.; Sosu, E.K.; Sackey, T.A.; Tagoe, S.N.; Inkoom, S. Medical physics practice and training in Ghana. Physica medica 2016, 32, 826–830. [Google Scholar] [CrossRef]
- Tafesse, N.; Samuel, A.; Geta, A.; Desalegn, F.; Gebru, L.; Tadele, T.; Genet, E.; Abate, M.; Jemal, K. Clinical ethical practice and associated factors in healthcare facilities in Ethiopia: a cross-sectional study. BMC Medical Ethics 2022, 23, 61. [Google Scholar] [CrossRef]
- Shahbaz, F.; Tarar, A.Z.; Farooq, M.W.; Majeed, F.; Riaz, A.; Imran, M.; Saleem, J.; Ullah, S.; Haider, N.; Tahir, M.N. Assessing medical doctors’ knowledge about medical ethics in health practices: A cross-sectional survey in Lahore, Pakistan. International Journal of Health Sciences 2023, 7, 960–973. [Google Scholar] [CrossRef]
- Ghana Statistical Service. In Population and Housing Census 2021. Available from: https://census2021.statsghana.gov.gh.
- Baatiema, L. The knowledge-practice gap: Evidence-based practice for acute stroke care in Ghana. Doctoral dissertation, Australian Catholic University.
- Bhardwaj, A.; Chopra, M.; Mithra, P.; Singh, A.; Siddiqui, A.; Rajesh, D.R. Current Status of Knowledge, Attitudes, and Practices towards Healthcare Ethics Among Doctors and Nurses from Northern India-A Multicentre Study. Pravara Medical Review 2014, 6. [Google Scholar]
- Koo, T.K.; Li, M.Y. A guideline for selecting and reporting intraclass correlation coefficients for reliability research. Journal of chiropractic medicine 2016, 15, 155–163. [Google Scholar] [CrossRef]
- Petkovic, D.; Altman, R.; Wong, M.; Vigil, A. Improving the explainability of Random Forest classifier–user-centered approach. InPacific Symposium on Biocomputing. Pacific Symposium on Biocomputing 2018 (Vol. 23, p. 204). NIH Public Access.
- Hastie, T.; Tibshirani, R.; Friedman, J.H.; Friedman, J.H. The elements of statistical learning: data mining, inference, and prediction; Springer: New York, Aug 2009. [Google Scholar]
- Statnikov, A.; Wang, L.; Aliferis, C.F. A comprehensive comparison of random forests and support vector machines for microarray-based cancer classification. BMC bioinformatics 2008, 9, 1–0. [Google Scholar] [CrossRef]
- Boulesteix, A.L.; Janitza, S.; Kruppa, J.; König, I.R. Overview of random forest methodology and practical guidance with emphasis on computational biology and bioinformatics. Wiley Interdisciplinary Reviews: Data Mining and Knowledge Discovery 2012, 2, 493–507. [Google Scholar] [CrossRef]
- Wang, H.; Yang, F.; Luo, Z. An experimental study of the intrinsic stability of random forest variable importance measures. BMC bioinformatics 2016, 17, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, S.; Egert, B.; Neumann, S.; Steinbeck, C. Building blocks for automated elucidation of metabolites: Machine learning methods for NMR prediction. BMC bioinformatics 2008, 9, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Mortell, M. Theory-practice-ethics: Is there a gap? A unique concept to reflect on. Acta Scientific Women’s Health 2019, 2, 1–2. [Google Scholar]
- Thomas, K.; Smith, J.; Phillips, J.D.; Falkenheimer, S. Solving Ethical Dilemmas in International Healthcare Professional Education: A Case Study Using a Revised Ethical Model. Christian Journal for Global Health 2018, 5, 29–34. [Google Scholar] [CrossRef]
- Sultana, K.; Kitchlew, N. Ethical Leadership and Institutionalization of Ethics: Intervening Role of Personal Factors. InAcademy of Management Proceedings 2021 (Vol. 2021, No. 1, p. 15215). Briarcliff Manor, NY 10510: Academy of Management.
- Gierczyk, M.; Harrison, T. The effects of gender on the Ethical Decision-making of Teachers, Doctors and Lawyers.
- Bhuyan, B.; Kumar, S.; Choudhury, S.; Kashyap, K. Impact of demographic factors on the ethical conduct of physicians in India. Indian Journal of Public Health 2020, 11, 589. [Google Scholar] [CrossRef]
- Etherington, C.; Boet, S. Why gender matters in the operating room: recommendations for a research agenda. British Journal of Anaesthesia 2018, 121, 997–999. [Google Scholar] [CrossRef]
- May, D.R.; Luth, M.T. The effectiveness of ethics education: A quasi-experimental field study. Science and engineering ethics 2013, 19, 545–568. [Google Scholar] [CrossRef]
- Banait, S.H.; Jain, J.Y.; Bokariya, P.R.; Khan, S.H. Effectiveness of healthcare ethics training in the undergraduate medical curriculum: A quasi-experimental study from rural India. Indian J Med Ethics 2022. [Google Scholar] [CrossRef]
- González-Blázquez, F.J.; Ruiz-Hontangas, A.; López-Mora, C. Bioethical knowledge in students and health professionals: a systematic review. Frontiers in Medicine 2024, 11, 1252386. [Google Scholar] [CrossRef]
- Anwar, S.; Shah, N. Impact of personality traits on ethical behavior. The Government-Annual Research Journal of Political Science 2018, 6. [Google Scholar]
- Niazazari, K.; Enayati, T.; Behnamfar, R.; Kahroodi, Z. Relationship between Professional Ethics and Job Commitment. Iran J Nurs. 2014, 27, 34–42. [Google Scholar] [CrossRef]
- White, K.L.; Jordens, C.F.; Kerridge, I. Contextualising professional ethics: The impact of the prison context on the practices and norms of health care practitioners. Journal of Bioethical Inquiry 2014, 11, 333–345. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Influence of HCE Knowledge on HCE Practise.
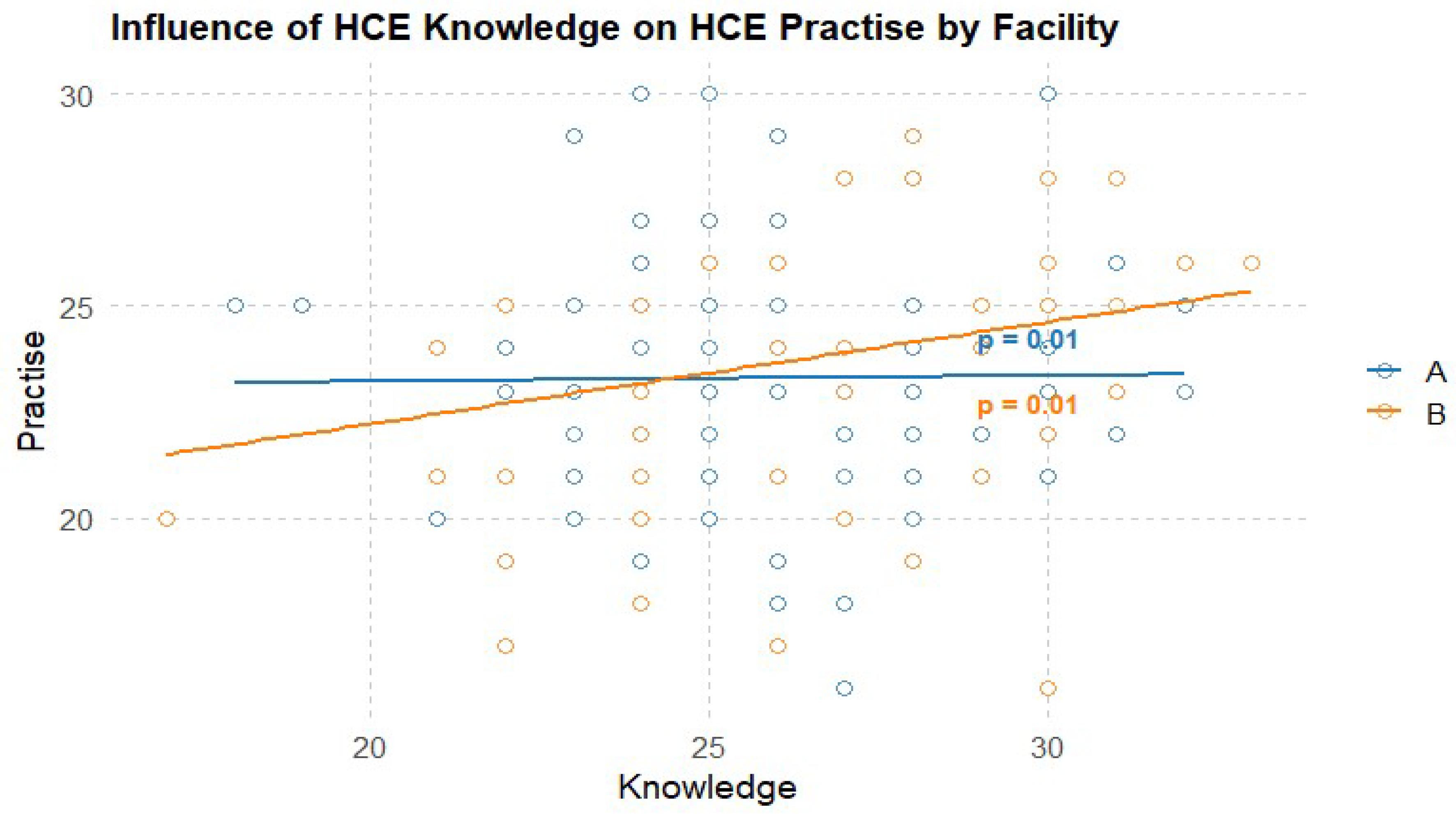
Figure 2.
Order of Influencing Factors of Healthcare Ethics in Overall Sample.
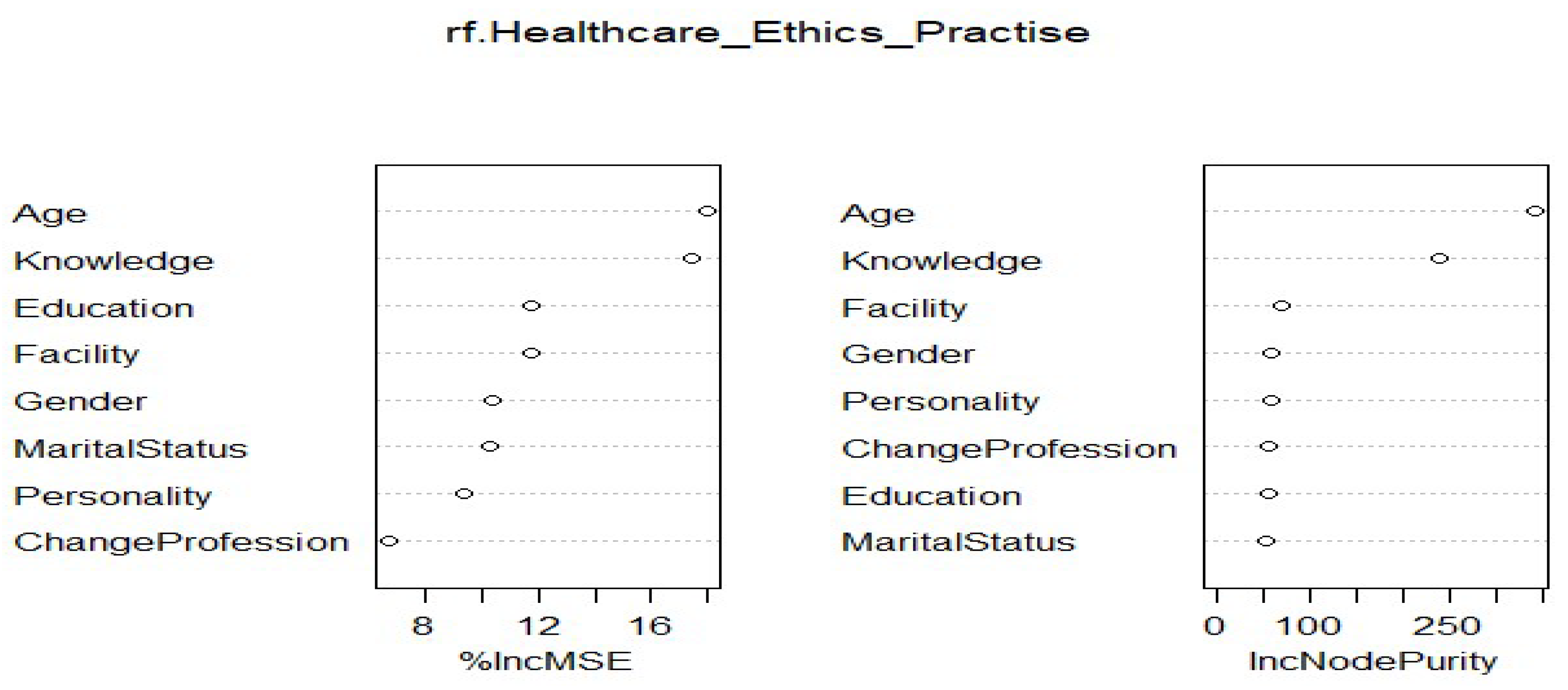
Figure 3.
Order of Influencing Factors of HealthCare Ethics in Facility A.
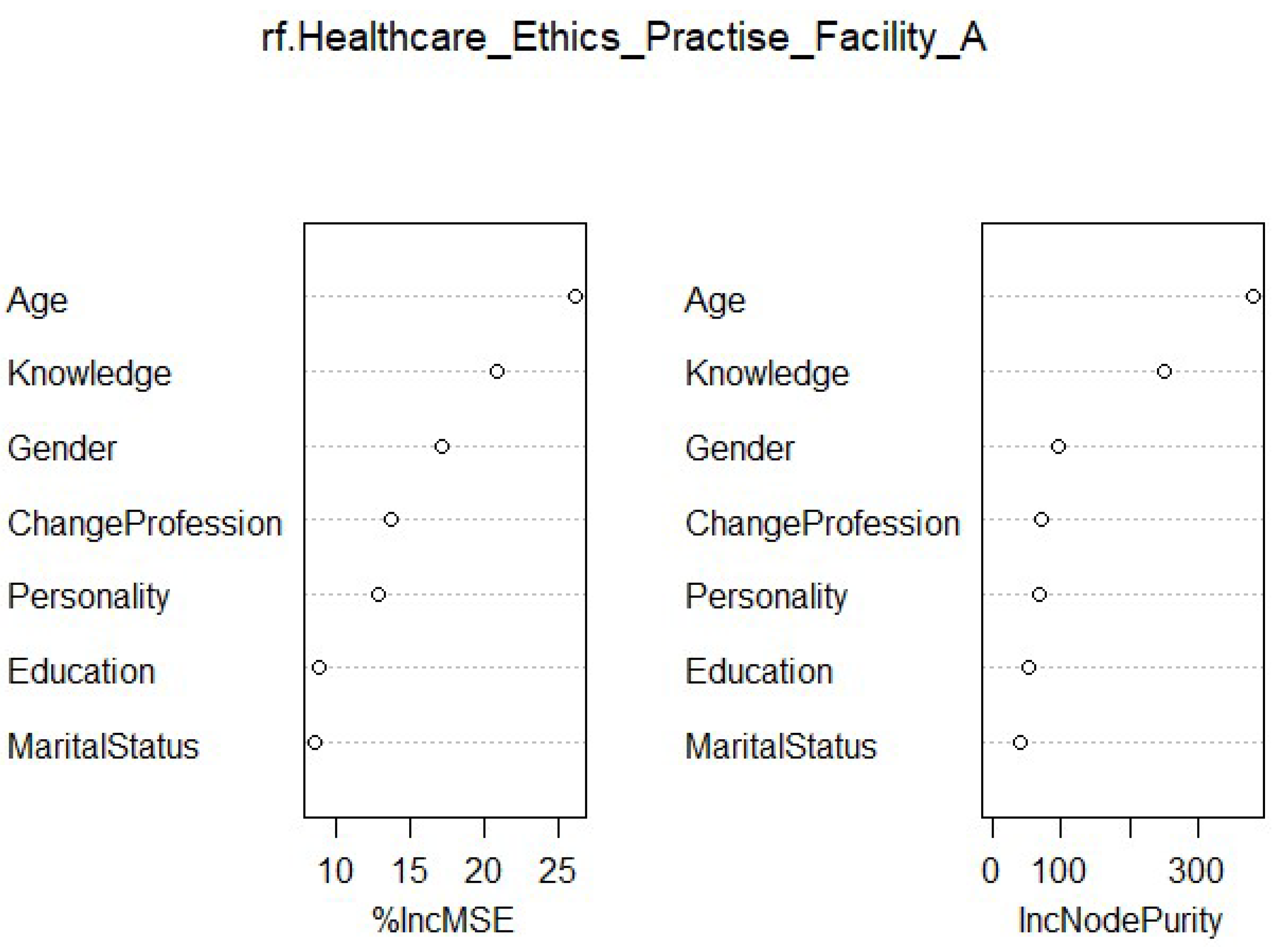
Figure 4.
Order of Influencing Factors of HealthCare Ethics in Facility B.
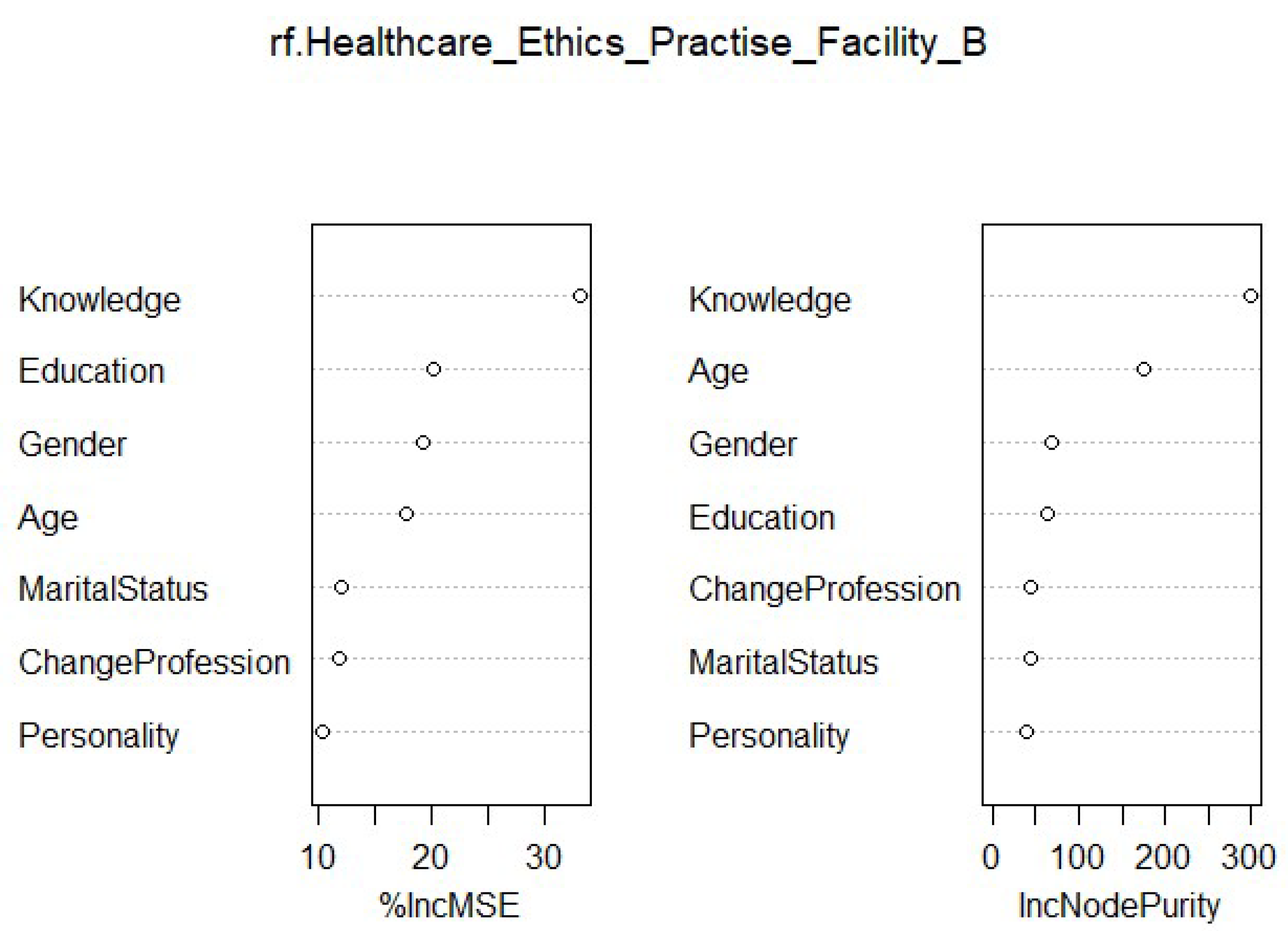

Table 1.
Description of Study Variables Overall and by Facility.
| Total Sample | Facility A (n= 210) |
Facility B (n=172) | X2 P value | ||||
|---|---|---|---|---|---|---|---|
| n | % | N | % | N | % | ||
| Gender | 0.41 | ||||||
| Man | 159 | 41.62 | 83 | 39.52 | 76 | 44.18 | |
| Woman | 223 | 58.38 | 127 | 60.48 | 96 | 55.82 | |
| Education Level | 0.03 | ||||||
| Diploma and below | 242 | 63.35 | 144 | 68.57 | 98 | 56.97 | |
| Above Diploma | 140 | 36.65 | 66 | 31.43 | 74 | 43.03 | |
| Personality | 0.22 | ||||||
| Introvert | 172 | 45.03 | 101 | 48.1 | 71 | 41.28 | |
| Extrovert | 210 | 54.97 | 109 | 51.9 | 101 | 58.72 | |
| Intention to change profession | 0.71 | ||||||
| Yes | 135 | 35.34 | 72 | 34.29 | 63 | 36.63 | |
| No | 247 | 64.66 | 138 | 65.71 | 109 | 63.37 | |
| Marital Status | 0.02 | ||||||
| Yes | 139 | 36.4 | 65 | 74 | 43.02 | ||
| No | 243 | 63.6 | 145 | 98 | 56.98 | ||
| Mean | SD | Mean | SD | Mean | SD | T-Test P value | |
| Age | 28.30 | 5.37 | 27.80 | 5.22 | 29.00 | 5.47 | 0.02 |
| Knowledge of HCE | 26.30 | 2.83 | 26.30 | 2.67 | 26.30 | 2.67 | 0.98 |
| Practice of HCE | 23.50 | 2.94 | 23.30 | 2.87 | 23.7 | 3.01 | 0.16 |
HCE, Healthcare ethics, SD, Standard Deviation.
| General | Facility A | Facility B | ||||
|---|---|---|---|---|---|---|
| Variable | %IncMSE | IncNodePurity | %IncMSE | IncNodePurity | %IncMSE | IncNodePurity |
| Age | 18.02 | 341.438 | 26.179 | 379.897 | 17.854 | 174.785 |
| Knowledge | 17.449 | 238.554 | 20.888 | 250.651 | 33.264 | 299.882 |
| Education | 11.773 | 56.529 | 8.943 | 52.882 | 20.206 | 64.906 |
| Personality | 9.31 | 59.79 | 12.811 | 67.6444 | 10.288 | 40.824 |
| Gender | 10.327 | 60.25711 | 17.105 | 96.327 | 19.358 | 67.862 |
| Intention to Change Profession | 6.642 | 57.304 | 13.781 | 70.4688 | 11.795 | 43.803 |
| Marital Status | 10.267 | 54.022 | 8.557 | 40.911 | 12.016 | 43.377 |
| Facility | 11.735 | 71.329 | NA | NA | NA | NA |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



