Submitted:
09 October 2024
Posted:
10 October 2024
You are already at the latest version
Abstract
Background: Choline is an essential nutrient required for proper cell functioning. Due to its status as a precursor to acetylcholine, an important neurotransmitter connected to cognition and neuromuscular function, maintaining or enhancing choline levels is of interest. Supplementation with alpha-glycerylphosphorycholine (A-GPC) can maintain choline levels, but its ability to offer support towards cognition remains an area of ongoing research.
Methods: Using a randomized, double-blind, placebo-controlled, crossover approach, 20 resistance-trained males (31.3 ± 11.0 years, 178.6 ± 7.3 cm, 84.6 ± 11.4 kg, 15.4 ± 5.6 % fat) consumed either a placebo (PL), 630 mg A-GPC (HD), or 315 mg (LD) A-GPC (GeniusPure™, NNB Nutrition). After resting hemodynamic assessments, participants took their assigned dose and had cognitive assessments (Stroop, N-Back, and Flanker), visual analog scales, and hemodynamics evaluated 60 minutes after ingestion. All participants then warmed-up and completed vertical jumps and bench press throws before completing a bout of lower-body resistance exercise (6 x 10 repetitions using the Smith squat at a load of 70% 1RM). Venous blood was collected 5, 15, 30, and 60 minutes after completion of the squat protocol to evaluate changes in growth hormone and follow-up visual analog scales and cognitive measurements were evaluated 30 minutes after completing the exercise bout.
Results: When compared to PL, changes in Stroop total score were statistically greater after HD (13.0 ± 8.2 vs. 5.2 ± 9.0, p = 0.013, d = 0.61) and LD (10.8 ± 7.7 vs. 5.2 ± 9.0, p = 0.046, d = 0.48) administration in addition to significantly faster times in completing the Stroop test in the HD group when compared to PL (-0.12 ± 0.09s vs. -0.05 ± 0.09s, p = 0.021, d = 0.56). No significant differences between groups were found for the Flanker and N-Back assessments while a tendency was observed for HD to have faster reaction times when compared to PL during the Flanker test. No groups differences were realized for visual analog scales, physical performance, or growth hormone. Statistically significant changes in heart rate and blood pressure were observed in all groups, with all recorded values aligning within clinically accepted normative values.
Conclusions: HD and LD A-GPC supplementation significantly increased cognitive performance in a group of young, healthy males as measured by changes in the Stroop Total Score and completion time of the Stroop test. These results extend the previously published research which indicated that A-GPC can augment cognition in clinical populations to healthy individuals undergoing acute exercise stress.
Keywords:
cognition
; nootropic
; mental
; performance
1. Introduction
Choline has established itself as an important nutrient essential for proper functioning of many organs in the human body [1]. As part of it being a critical component of the neuronal phospholipid bilayer, choline is connected to signal transduction and methylation of DNA, histones, and neurons. Choline is a precursor of acetylcholine (ACh), a neurotransmitter involved in memory, attention, and skeletal muscle contraction [1]. As such, ACh is a key component of communication throughout the nervous system, thus creating its theorized connection to cognition while ACh also sits at the coalface between the nervous and muscular systems at the neuromuscular junction. Previous work has indicated that supplementation with alpha-glycerylphosphorylcholine (A-GPC), a choline-containing phospholipid, can increase choline levels, and in doing so may augment cognition, physical performance, and endogenous hormone production [2,3,4].
Due to A-GPC’s ability to increase choline levels [5] and other evidence that demonstrates disruption in cholinergic transmission leading to learning and memory deficits in times of reduced ACh availability [6], the interest in A-GPC supplementation to support cognition has been evident for several years. Currently, research findings are mixed regarding A-GPC’s potential to impact cognition [7,8]. When investigated in clinically compromised or healthy aged populations, A-GPC studies have indicated that A-GPC supplementation enhances memory and cognitive function and is an effective treatment for neurodegenerative disorders such as Alzheimer’s disease and dementia [1,9,10,11]. A-GPC has also been proposed to offer treatment support for traumatic brain and other cerebrovascular accidents [12]. Research in healthy populations, however, is scant and, to date, the majority of these studies have failed to highlight cognitive benefits in healthy individuals [13,14]. One of the initial studies exploring A-GPC for its ability to impact cognition used 32 healthy young volunteers who were administered an intramuscular injection of 1000 mg A-GPC or placebo for ten days before having cognition evaluated [15]. The authors reported A-GPC administration was able to antagonize memory and attention impairment induced by scopolamine. Unfortunately, the method of administration (intramuscular injection) in this study challenges its translation to larger segments of the population. A 2021 study by Tamura et al. [4] administered daily 400 mg doses of A-GPC or a placebo for 14 days to healthy volunteers who completed a scale to evaluate emotional states. After the treatment was administered, motivation levels were significantly improved while anxiety levels were not impacted. Two other studies in healthy individuals examined the potential for A-GPC to impact cognition. The first study was completed by Parker et al. [14] who used a randomized, double-blind, placebo-controlled, crossover design where they had 20 healthy men and women complete visual analog scales, a serial subtraction test, and a battery of physical performance tests after ingesting either 200 mg of A-GPC, 200 mg of caffeine, 400 mg of A-GPC, or a placebo. No statistically significant changes were observed in the serial subtraction test although the 200 mg dose of A-GPC scores were 18.1% and 10.5% faster than the caffeine and placebo groups, respectively. Additionally, Bunn and colleagues [13] acutely supplemented 21 college-aged males in a randomized, crossover manner to receive either a placebo or a combination of 500 mg A-GPC, 250 mg of uridine-5’-monophosphate, and 1,500 mg DHA). During each condition, participants had their cognition assessed using the ImPACT protocol along with vertical jump and maximal bench press repetitions. Results from this study also indicated that a single day of supplementation exerted no impact on their outcomes.
Other studies have also explored the potential for A-GPC to positively influence various indicators of muscular performance [3,5,14,16]. The results from these studies are currently mixed, which may be due to the length and amount of supplementation provided in each study. Three peer-reviewed studies are available that support the ability of A-GPC to augment exercise performance. Bellar et al. [3] supplemented 13 young, healthy males with either 600 mg A-GPC or placebo for six days and reported significant improvements in lower body force production. Another study involving young, healthy males required the participants to supplement with either a placebo, 250 mg A-GPC, or 500 mg A-GPC in a randomized, double-blind fashion for seven consecutive days [5]. Serum choline was increased along with significantly greater maximum velocity and maximum power values during a countermovement jump. Finally, Harrington et al. [17] reported that muscular power was improved in 30 male trained cyclists after seven days of supplementing with 300 mg of A-GPC, but the A-GPC was provided as part of a combination that also included BCAAs and citrulline, so the independent impact of A-GPC was not able to be clearly discerned from this study.
Three reports are available that outline findings after a single dose was delivered. In an abstract presented as part of a conference proceedings, Ziegenfuss et al. [16] used a randomized, double-blind, placebo-controlled, crossover approach with seven healthy men to examine the impact of consuming a single 600 mg dose of A-GPC 90 minutes prior to completing a bout of lower-body resistance exercise and reported that peak force production (p < 0.02) during a series of bench press throws was greater when A-GPC was provided while no changes in peak velocity or peak power were observed. Alternatively, no changes in vertical jump performance were reported in an abstract presented as part of a conference proceedings by Parker et al. [14] who supplemented 20 healthy men and women with either 200 mg of A-GPC, 200 mg of caffeine, 400 mg of A-GPC, or a placebo. Finally, Bunn and colleagues [13] acutely supplemented 21 college-aged males in a randomized, crossover manner to receive either a placebo or a combination of 500 mg A-GPC, 250 mg of uridine-5’-monophosphate, and 1,500 mg DHA) and reported that supplementation did not impact vertical jump performance or the maximal number of bench press repetitions completed.
A final area of interest has been in the ability of A-GPC to heighten endogenous production of growth hormone secondary to activation of the hypothalamic-pituitary axis. Kawamura et al. [2] supplemented eight healthy males with either 1000 mg A-GPC or a placebo in a randomized, double-blind, crossover fashion and reported that growth hormone levels were significantly increased 60 minutes after taking A-GPC. Another study was completed by Maldonado et al. [18] as part of a graduate thesis and has not been published in a peer-reviewed journal that required overweight adults to supplement with 1200 mg of A-GPC each day for eight weeks. No changes in growth hormone were identified in this study. Finally, Ziegenfuss et al. [16] reported a significantly greater area under the curve for growth hormone in response to a heavy bout of lower-body resistance exercise when a 600 mg dose of A-GPC was provided when compared to placebo. With the popularity of A-GPC being used in an acute fashion as part of various nutritional formulations ingested prior to workouts and competitions, more research is needed to examine the ability of A-GPC to impact cognition and exercise performance. Therefore, the purpose of this study was to evaluate the impact of two different doses of A-GPC on cognitive and physical performance in healthy resistance-trained individuals.
2. Materials and Methods
Overview of Research Design
All study participant recruitment and data collection were completed using a randomized, double-blind, placebo-controlled, crossover study design at the Center for Applied Health Sciences, a contract research organization in Canfield, OH (www.thecahs.com). Twenty-one healthy men with at least two years of resistance training experience were recruited to participate in this study protocol. Each study participant was required to complete four study visits whereby study visit 1 was a screening visit. Visit 1 required each participant to observe an overnight fast and have a medical history completed including assessments of their height, weight, body mass index, resting heart rate, and resting blood pressure in addition to providing a 24-hour dietary recall of their typical dietary intake, and routine blood work (i.e., CBC, CMP, lipid panel) to establish eligibility, and familiarization with the cognitive and exercise battery used in subsequent visits. The provided 24-hour dietary recall was reviewed for completeness with a research team member and a copy was provided back to the study participant to aid them in replicating their food and fluid intake prior to each subsequent study visit. Eligible participants were then scheduled for study visit 2 approximately 3 – 7 days after study visit 1. Prior to study visit 2 and each subsequent study visit, participants were instructed to replicate their food and fluid intake for 24 hours prior to each study visit, observe an overnight fast of at least 8 hours, refrain from exercise for 48 hours, and avoid caffeine, alcohol, and any foods that may impact choline levels for 24 hours prior to each visit. Upon arrival, participants had their body mass, heart rate, and blood pressure evaluated and confirmed their compliance with all pre-study procedures. Participants then donated their first venous blood sample and consumed their assigned test product in front of a research team member. Using a randomized, double-blind manner, study participants ingested during separate study visits (Visit 2 – 4) either a 315 mg dose (LD) of alpha-glycerophosphorylcholine (A-GPC) (delivered as 350 mg of 90% A-GPC, GeniusPure™, NNB Nutrition, Nanjing, China), a 630 mg dose (HD) of A-GPC (delivered as 700 mg of 90% A-GPC, GeniusPure™), or a resistant dextrin placebo.
After supplement ingestion, participants then rested quietly for 60 minutes before having resting heart rate and blood pressure reassessed. From there, visual analog scales for mood, motivation to perform physical and mental tasks, alertness, and concentration were completed along with three assessments of cognitive function (Stroop, Flanker, and N-Back tests). Participants then completed a standardized warm-up and completed a series of body weight vertical jumps and bench press throws at 50% 1RM to evaluate lower-body and upper-body force, power, and velocity. Upon completion of the performance tests, a bout of lower-body resistance exercise (6 x 10 reps Smith Machine squats at 70% 1RM with 90 seconds of rest between each set) was performed which was followed with venous blood collection 5, 15, 30, and 60 minutes after completion of the lower-body resistance exercise protocol to evaluate changes in growth hormone. An additional battery of visual analog tests and cognitive function tests were completed 30 minutes after completion of the lower-body exercise protocol. The final heart rate and blood pressure was completed 60 minutes after completion of the exercise bout and this completed the study visit. Study participants were then scheduled to return for their two remaining study visits (identical to study visit 2) approximately 4 – 7 days after their previous study visit (see Figure 1 and Table 1).
Study Participants
Twenty-one healthy, resistance-trained men between the ages of 20 – 55 years were recruited for this study from a local suburban community in Ohio. Complete demographics of all study participants can be found in Table 2. All participants read and signed an IRB-approved informed consent form prior to participating in the study (WCG IRB, Puyallup, WA, Protocol # NNB-001-0123024, Approval date: 1/17/2024). To be deemed eligible, all study participants were required to be in good health as determined by review of their medical history and routine blood chemistries by the research team. Inclusion criteria indicated that all participants were between the ages of 20 – 55 years, had body mass index levels between 18.5 – 34.9 kg/m2 (inclusive) with a minimum body mass of 54.5 kg, were normotensive (systolic pressure < 140 mm Hg and diastolic pressure < 90 mm Hg) with a normal resting heart rate (<90 beats/min). Participants were required to replicate their previous 24-hour dietary intake, avoid exercise for 48 hours, refrain from alcohol, caffeine, and any foods or nutrients that may impact choline status for 24 hours, and not make any changes to their medications, diet, or supplementation during the study protocol. Finally, participants were instructed to fast for eight hours prior to each visit.
Participants were excluded from participating if they indicated they were currently a competitive athlete, had a history of psychiatric, hepatorenal, musculoskeletal, autoimmune, neurologic diseases or disorders as well as diabetes, asthma, gout, fibromyalgia, a clinical diagnosis of IBS/IBD, or a malignancy in the previous five years except for non-melanoma skin cancer. Participants with a prior history of gastrointestinal bypass surgery, chronic inflammatory condition or disease (e.g., rheumatoid arthritis, Crohn’s disease, ulcerative colitis, Lupus, HIV/AIDS, gastrointestinal or metabolic diseases that might impact nutrient absorption (e.g., short bowel syndrome, diarrheal illnesses, history of colon resection, gastro paresis, and inborn errors of metabolism) were excluded. Alcohol consumption (>2 standard alcoholic drinks per day or more than 10 drinks per week), current smoker, clinically significant abnormal laboratory results, concomitant use of corticosteroids or testosterone replacement therapy all resulted in study exclusion. Finally, participants who reported any current use of dietary supplements were required to maintain their current use throughout the study protocol. Individuals who were prescribed medications for anxiety or ADHD, a current allergy or sensitivity to any ingredient in the test formulation, or had participated in another clinical research trial in the previous 30 days were excluded.
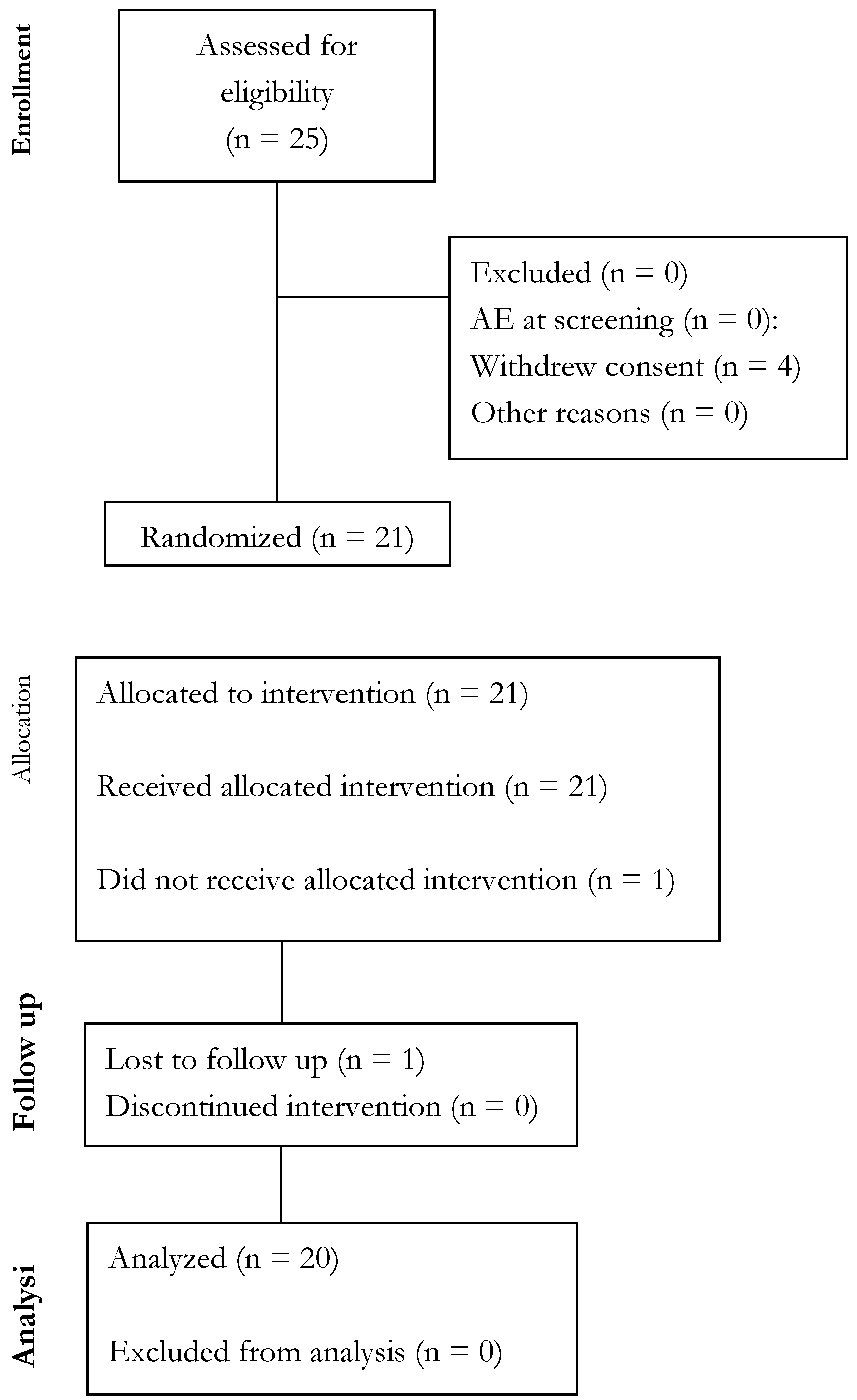
Figure 2.
Consolidated Standards of Reporting Trials (CONSORT) diagram.
Procedures
Anthropometrics
Using previously published methods [19,20], standing height was determined using a wall-mounted stadiometer and evaluated at study screening. Body mass was evaluated (±0.5 kg) using a Seca 767TM Medical Scale (Hamburg, Germany) and was measured at each visit). Seated resting heart rate and blood pressure were measured after resting quietly for approximately five minutes using an automated blood pressure cuff (Omron HEM-780, Japan) at screening and again during each study visit approximately one hour and 3.5 hours after supplement ingestion.
Body Composition
Body composition was assessed for descriptive purposes using an InBody 570 (InBody Co., Ltd., Cerritos, CA, USA) bioelectrical impedance analyzer following an 8-hour overnight fast for descriptive purposes. Prior to each analysis, participants voided their bladder, washed their hands, removed any additional clothing, all metal jewelry, and any other accessories before wiping both hands and both feet clean with cleansing wipes (InBody Tissue; InBody Co., Ltd., Cerritos, CA, USA) provided by the manufacturer before standing erect with both hands and feet in contact with the sensors. On each day the machine was used, the device was calibrated according to manufacturer guidelines and device specifications.
Dietary Intake and Physical Activity Monitoring
Outside of consuming their assigned supplementation dose at the beginning of each study visit, no other changes in dietary habits were prescribed as part of this study investigation. During study visit 1, all participants were instructed to complete a 24-hour dietary recall. This recall was reviewed with research team members for accuracy and omissions. This food record was then copied, and participants were instructed to replicate their food and fluid intake the day prior to study visits 2-4. The collected dietary records were analyzed for average daily energy and macronutrient intake by trained study investigators (Nutritionix, Washington DC). During each study visit, participants were asked by research team members the extent to which they were able to follow a similar eating pattern as previous visits and compliance was recorded. All study participants were required to refrain from exercise for 48 hours prior to each study visit. Outside of those limitations, no other physical activity restrictions were required as part of this study investigation.
Venous Blood Collection
A single blood draw was performed at visit 1 for screening purposes and a series of five venous blood samples were collected at each study visit (visits 2-4). Whole blood and serum samples were collected using standard phlebotomy techniques at all study visits by a research nurse or phlebotomist. Whole blood samples were collected into K2-EDTA treated tubes and upon collection, each sample was slowly inverted ten consecutive times prior to immediate refrigeration. Serum samples were collected in serum separation tubes and allowed to clot for 30 minutes at room temperature prior to being centrifuged using a standard benchtop centrifuge for 15 minutes at 3,200 rpm. Samples were analyzed by a commercial diagnostic laboratory (Lab Corp) for complete blood counts, comprehensive metabolic panels, lipid panels, and growth hormone.
Supplementation Protocol
Using a Latin square to minimize order effects during this 3-way crossover, study participants were instructed to ingest either a resistant dextrin placebo, a low dose (LD: 315 mg) of A-GPC, or a high dose (HD: 630 mg) of A-GPC (GeniusPure™, 90% pure A-GPC, NNB Nutrition, Nanjing, China). All supplements were produced in non-transparent capsules that were similar color, size, and shape. All doses were administered by the research team at the beginning of each study visit and were consumed with approximately 12 fluid ounces of commercially bottled water. Third-party analysis confirmed purity and content as described A-GPC (batch # GP90-20230717, manufactured: 2023.07.17, re-test date: 2025.07.16, confirmed as 91.6%) and resistant dextrin (batch # 20230123, manufacture date: 2023.01.23, re-test date: 2025.01.22, confirmed 93.1%).
Visual Analog Scales
Visual analog scales (VAS) were completed 30 minutes prior to beginning the exercise protocol and 30 minutes after completing the exercise protocol to evaluate perceived changes in mood, motivation to perform physical and mental tasks, alertness, and concentration. Each VAS was 100 mm in length and anchored with “Worst Possible” or “Lowest Possible” and “Best Possible” or “Highest Possible”. These methods have been previously validated and determined to be reliable [21] and previously published [19,20,22,23].
Cognitive Performance
The Stroop test is a widely used test to evaluate multiple parameters of cognitive performance including attention, processing, cognitive flexibility and the ability to inhibit cognitive interference [24] in addition to working memory [25]. The Stroop test requires individuals to read words printed in a different color ink (for example, the word “green” could be printed in blue) and select the color of the ink they see instead of speaking the word they read [26]. All the participants were assessed using the congruent standard condition of the Stroop test for a duration of two minutes at each attempt/repetition. The outcome variables associated with the Stroop test were total score, accuracy, and average time per score.
The N-Back task is a widely used neurobehavioral assessment to evaluate working memory [27]. Briefly, this test requires participants to determine if the current stimulus repeats relative to the item that occurred ‘n’ times before its onset. The 1-back task was used in this study thus, this task would require participants to determine if the current stimulus is the same as the one before it. Stimuli were presented as a card with a colored shape for 1500 ms with a 500 ms intertrial interval. Participants had to respond as quickly as they could by striking an arrow on the keyboard corresponding to an appropriate response (e.g., either the color and shape matched, only the color or shape matched, or the color and shape did not match with the previous stimulus) [21,27]. An overall score, accuracy (correct responses as a percentage and number of correct responses out of the total number of attempts), total number of attempted responses, and reaction time (lumosity.com-Speed Match Overdrive) were used as part of analysis. Two separate tests were completed consecutively with approximately 45 seconds between each test. The two tests were averaged to achieve one value for the score, accuracy (absolute and percentage), and reaction time per attempt while the number of correct and attempted responses were totaled to provide a sum.
The Flanker Inhibitory Control and Attention Test measures attention and inhibitory control and assesses individuals’ ability to suppress responses that are inappropriate [33]. The test requires the participant to focus on a given stimulus while inhibiting attention to stimuli (shapes) flanking it. In doing so, the test evaluates speed and accuracy in responding to congruent stimuli, incongruent stimuli, and no stimuli. Scoring is reported as accuracy and reaction time within each stimuli condition (congruent, incongruent, none).
During each study visit, two repetitions of each cognitive test were completed and each test was administered approximately one hour and three hours after supplement ingestion. In total, each test was completed four times (eight times for the N-back) during each of the three separate study visits.
Exercise Performance
Upper body and lower body performance were evaluated approximately 90 minutes after supplement ingestion in alignment with previously completed data involving A-GPC supplementation [16]. Briefly, bench press throws were completed using a Tendo Power Analyzer (Lexington, SC) unit attached to the end of a standard 20-kg barbell throughout each repetition to evaluate upper body peak power, average power, average velocity, and peak force. For each repetition, a submaximal load (i.e., 50% of perceived 1RM) was performed on a Smith machine. Subjects laid flat on their backs on a bench with their feet on the ground and hands on the bar in a pronated grip. Grip width was standardized for all subjects and reproduced during follow up testing. The subjects lowered the bar (1-2 second eccentric action) until it lightly touched the chest slightly above the nipple line, and then explosively launched the bar vertically upwards. Using this approach, three sets of three repetitions with 90 seconds of rest between each set were completed and the highest average and peak power, peak velocity, and peak force were recorded. Prior to each test, two normal bench press repetitions were allowed prior to the bench press throws as an orientation. The position of the Tendo analyzer was standardized to minimize any deviations of the lanyard to minimize variability in the measurements. Previous studies have demonstrated the reliability of using a Tendo analyzer [28] for these outcomes and similar methodological approaches have been published previously to evaluate efficacy of various dietary supplements on these outcomes [29,30]. Lower body power was assessed via body weight jump squats while tethered to the Tendo power analyzer. A total of three countermovement jumps were completed. For each jump, subjects were required to hold a dowel on top of their shoulders and flex their knees eccentrically before executing the rapid vertical jump. Each jump was recorded for peak power and average power and peak velocity and force. The average of all three jumps was calculated and used for statistical analysis. Approximately 60-90 seconds of rest was given between sets. From these data, jump height was calculated [31,32] using algebraic substitution of the original formula: Jump height (cm) = average power in watts – (23 * body mass in kg) + (1,393/21.2).
Resistance Exercise Protocol
The resistance exercise protocol utilized in this study mirrored the approach utilized by Ziegenfuss et al. [16]. Herein and after completing all upper body and lower body performance assessments, study participants were guided through the completion of a lower-body resistance exercise protocol that was intended to stimulate endogenous hormone production [33,34]. The protocol commenced approximately two hours after consuming their assigned supplement and consisted of completing 6 sets of 10 repetitions at 70% 1RM using a squat movement on a Smith machine. A metronome was used (15 repetitions per minute) to ensure consistent cadence and time under tension. Approximately 90 seconds of rest was provided between each set of repetitions. A repetition was only counted if a full range of motion was utilized (thighs parallel to ground). All repetitions were supervised and counted by a study investigator / certified strength and conditioning specialist.
Serum and Whole Blood Analysis
For screening purposes, blood collected during study visit 1 was analyzed for comprehensive metabolic panels (e.g., glucose, blood urea nitrogen [BUN], creatinine, aspartate aminotransaminase [AST], alanine aminotransaminase [ALT], lactate dehydrogenase, total bilirubin, alkaline phosphatase [ALP], glomerular filtrate rate, sodium, potassium, total protein, albumin, and globulin), total white blood cell and red blood cell counts, and lipid panels (e.g., triglycerides [TG], total cholesterol [TC], LDL cholesterol, HDL cholesterol). All analyses were completed using automated clinical chemistry analyzers (LabCorp, Dublin, OH branch).
Growth hormone was measured in five venous blood samples across each supplementation period. In alignment with Figure 1 and to mimic the previous methods of Ziegenfuss et al. 2008 [16], growth hormone was assessed prior to supplementation and then 5, 15, 30, and 60 minutes after completing the lower-body resistance exercise protocol. The lower-body resistance exercise protocol didn’t begin until 60 minutes after supplementation ingestion and the exercise protocol itself took approximately 40 minutes to complete. As such, post-exercise growth hormone levels ended up being assessed 135, 145, 160, and 190 minutes after ingestion of the supplementation, which corresponded with the post-exercise time points identified above in this section. Serum samples were processed as indicated and analyzed individually by LabCorp.
Adverse Events
All adverse events (all local and systemic non-serious and serious) were monitored by the researchers and evaluated and assessed through reports coded using the Medical Dictionary for Regulatory Activities (MedDRA). In the event of an AE, the intensity of the AE would be graded according to the protocol-defined criteria based on the Common Terminology Criteria for Adverse Events (CTCAE) Version 5.0, 2017.
Statistical Analysis
A p-value of ≤ 0.05 was accepted as statistical significance, whereas p-values > 0.05 to ≤ 0.10 were accepted as a statistical trend. Normality of the frequency distributions were assessed using the Shapiro-Wilk test and log transformations were applied when the data (or a majority of the data) suggested non-normality. All data provided in tables and figures display raw (non-transformed) values. A one-way repeated measures ANOVA was used to assess differences between treatments for upper body performance, lower body performance, VAS variables, GH AUC, and change scores for cognitive testing. Change score/Delta values were computed by the differences in time points for the cognitive performance markers (30 min post exercise – 60 min post supplement ingestion). Mixed factorial ANOVAs were used to evaluate time and treatment main effects and time x treatment interaction effects for vital signs and growth hormone. When sphericity was violated, Greenhouse-Geiser adjustments were applied and LSD post-hoc comparisons were used to evaluate pairwise comparisons. Any values > 3SD or < -3SD were noted as outliers. Effect sizes using Cohen’s d (d) were calculated to evaluate the magnitude of the observed effect between groups (HD, LD, PL). A small effect size was ≥0.2, a medium effect ≥0.5, and a large effect ≥0.8. Analyses were conducted in GraphPad Prism, version 10.0.2.
3. Results
Compliance & Adverse Events (AEs)
Weekly compliance checks by the research study team revealed >95% compliance to the supplementation (data not shown) regimen. A summary table of adverse events (AEs) is provided (Table 3). Ten participants experienced AEs that were mild to moderate in nature during this study. There were no differences in proportions of reported adverse events (p > 0.05) between treatments. Given that all but one AE were experienced on visit 2 (i.e., the first testing visit) and proportional across study products, it is determined that most AEs were due to the study design procedures (e.g., IV insertions/blood draw and workout stress) rather than the study product consumed.
Body Mass & Hemodynamics
Body mass values tended to be different across the study protocol with PL reporting significantly lower body mass values (84.4 ± 11.4 kg) than HD (85.0 ± 11.5 kg, p = 0.025, d = 0.54). Significant changes within groups occurred for hemodynamic variables. All measured outcomes remained within clinically accepted values for healthy, exercise individuals (Table 4).
Cognitive Performance
Cognitive performance was evaluated using the Stroop color matching, Flanker, and N-back test. Delta scores were computed to assess changes in Stroop performance and analyzed using one way ANOVA. Using this approach, a statistically significant difference in Stroop total score (p = 0.016) was observed using one way ANOVA. LSD post-hoc comparisons revealed that Stroop total score (Figure 3) increased to a statistically significant greater degree in HD (13.0 ± 8.2; p = 0.013, d = 0.61) and LD (10.8 ± 7.7; p = 0.046, d = 0.48) when compared to PL (5.2 ± 9.0). A statistically significant difference was also observed with the time required per score in the Stroop test (p = 0.030; Figure 4). Following this, LSD post-hoc comparisons revealed that HD resulted in significantly faster responses when compared to PL (HD: -0.12 ± 0.09s vs. PL: -0.05 ± 0.09s, p = 0.021, d = 0.56). A trend was observed for LD to be faster (-0.10 ± 0.08s) than PL (p = 0.072, d = 0.42). Additionally, one way ANOVA for Stroop Accuracy indicated a statistical trend for differences between (p = 0.073). LSD post-hoc comparisons indicated that HD had significantly greater accuracy than LD (HD: 0.28 ± 0.85% vs. LD: -0.58 ± 0.90%, p = 0.005, d = 0.72). No statistically significant changes between groups (p > 0.05) were observed for measurements taken in Flanker Compatible Accuracy (p = 0.376, Flanker Incompatible Accuracy (p = 0.754), Flanker Incompatible Reaction Time (p = 0.467), Flanker None Accuracy (p = 0.214), and N-Back tests (Table 5). Statistically different reaction times were observed for the Flanker Compatible Reaction Time whereby HD exhibited statistically faster reaction times than PL (-51.2 ± 53.9 ms vs. -13.0 ± 51.6 ms, p = 0.018, d = 0.58).
Visual Analog Scales
As seen in Table 6, no significant differences between groups were identified 60 minutes after supplement ingestion for mood (p = 0.649), motivation to perform physical tasks (p =0.320), motivation to perform mental tasks (p = 0.664), alertness (p = 0.197), and concentration (p = 0.385). A trend (16.7%; p = 0.054, d = 0.47) was identified for HD to be greater than PLA. When VAS was evaluated again 30 minutes after completion of the exercise bout, no significant differences between groups for mood (p = 0.649), motivation to perform physical tasks (p =0.320), motivation to perform mental tasks (p = 0.664), alertness (p = 0.197), and concentration (p = 0.385).
Physical Performance
Table 7 provides the data for the upper-body and lower-body performance tests. Using oneway ANOVA, no significant differences in bench press average power (p = 0.198), peak power (p = 0.168), peak velocity (0.296), or peak force (p = 0.159) were observed. To fully examine potential differences between the three groups, LSD comparisons were completed and peak force production in HD was found to be significantly greater than PL (p = 0.043, d = 0.49). Peak power values tended to be greater in HD (p = 0.071, d = 0.43), and LD tended to be greater than PL (p = 0.073, d = 0.44).
Lower-body performance was evaluated using vertical jumps. Using oneway ANOVA, a statistically significant difference was observed for peak force produced (p = 0.050) with LSD post-hoc comparisons indicating that LD was greater than HD (p = 0.027, d = 0.54) and LD tended to be greater than PL (p = 0.085, d = 0.41). Peak power (p = 0.085) tended to be different between groups with forced LSD post-hoc comparisons indicating that peak power values tended to be greater with LD than HD (p = 0.071, d = 0.43) and LD tended to be greater than PL (p = 0.068, d = 0.43). No differences were observed between groups using oneway ANOVA for average power (p = 0.954) and peak velocity (p = 0.160). Forced LSD post-hoc comparisons indicated a tendency for HD to be greater than PL (p = 0.091, d = 0.40).
Growth Hormone
As seen below in Table 8, the group x time interaction for growth hormone was not significant (p=0.174) while the main effect of group (p < 0.001) and time were statistically significant (p < 0.001). The main effect of group was further decomposed by completing individual one way ANOVA at each individual timepoints. No significant differences were observed between groups using one way ANOVA for each individual timepoint (0 min: p = 0.366; 5 min: p = 0.069; 15 min: p = 0.362; 30 min: p = 0.318; 60 min: p = 0.447). Factorial ANOVAs with repeated measures on time were completed to evaluated changes within each group from its respective baseline value. In the HD and LD groups, observed growth hormone levels were increased at all post-exercise timepoints when compared to their respective baseline values. The PLA group was different 5 min (p = 0.005) and 15 min (p = 0.013) but was not different from baseline 30 min (p = 0.158) and 60 min (p = 0.283) post-exercise. Area under the curve (AUC) calculations were and one way ANOVA indicated no significant differences were found between the three groups (HD: 380 ± 279, LD: 414 ± 273, PL: 351 ± 272 ng/mL/min, p = 0.438).
4. Discussion
Choline availability can have widespread physiological impact by way of impacting acetylcholine status across the body and facilitating other intracellular communication. A-GPC supplementation has been documented in studies to positively influence choline levels [5,35] and exert influence over mood [4], cognition [1,9,12], and physical performance [3,5]. The primary findings from the current study highlight the statistically significant improvement in Stroop total score when participants supplemented with both HD and LD when compared to PL (Figure 3). Additionally, outcomes revealed that HD spent significantly less time (they completed the test faster) on the test when compared to PL (Figure 4). Forced post-hocs also revealed that HD exhibited faster responses times during the Flanker test when compared to PL (Table 5). Finally, although faster, HD exhibited decreased accuracy when compared to LD, but accuracy was similar when compared to PL (Table 5). These results are meaningful because they represent the first time that A-GPC supplementation has been documented to increase parameters of cognitive performance in a young, healthy cohort. Previous investigations using this population were unable to identify such changes [13,14] while studies involving older and clinically compromised populations [1] have reported on the ability of A-GPC to positively impact cognitive performance. The reasons for why these outcomes deviate from previous studies involving healthy populations are not entirely known. The current study and the two other investigations using single doses of oral ingestion both used robust randomized, double-blind, crossover, placebo-controlled study designs and made acute assessments of physical and cognitive performance. The Stroop color and matching test is a clinically validated and popular assessment of selective attention, cognitive flexibility, processing speed, and inhibition while the other investigations used the ImPACT [13] and serial subtraction [14] tests. The higher A-GPC dosage (HD: 630 mg) during the present study was higher than the dosages provided during both the Parker (200 mg and 400 mg) and Bunn (500 mg) investigations [13,14], which may have impacted the outcomes, but the lower dose (LD: 315 mg) also exerted some positive influence, which somewhat rebuts this as an explanation for our outcomes. It is worth mentioning that the A-GPC delivered as part of the Bunn investigation was combined with two other ingredients (UMP and DHA), which further challenges one’s ability to compare the results of these investigations. Collectively, each of these studies used young, healthy cohorts (20 – 30 years) and completed measurements within a similar time frame of administration (30 – 90 minutes after ingestion). Another difference may be the manufacturing method utilized for the A-GPC provided in the current investigation versus the other investigations. The A-GPC used in the present study (GeniusPure, NNB Nutrition) is commercially produced at a higher purity rate in a manner that is free of soy and other common allergens. The extent to which commercial production methods may have impacted the bioavailability or absorption kinetics is not currently known.
The present study also examined the potential impact of A-GPC’s ability to augment physical performance using a study approach that closely mimicked the study design previously utilized by Ziegenfuss et al. [16]. Using this approach, peak force produced during the vertical jumps was different between groups with post-hoc comparisons indicating that LD was greater than HD (p = 0.0.27, d = 0.54) and tended to be greater than PL (p = 0.085, d = 0.41) (Table 7). A trend was observed for vertical jump peak power using oneway ANOVA (p = 0.085) and forced LSD post-hocs with LD exhibiting a tendency to be greater than PL (p = 0.068, d = 0.43) and HD (p = 0.071, d = 0.43). Changes in upper-body performance were similar between all three groups using oneway ANOVA (Table 7) but forced post-hocs indicated a statistically significant difference was present between HD and PL (p = 0.043, d = 0.49). These results align somewhat with the previous studies examining physical performance changes in a young, healthy cohort [3,5,16]. Briefly, Bellar et al. [3] reported statistically significant improvements in peak force production while Marcus et al. [5] reported greater peak power production when A-GPC was provided. In addition, and in alignment with the present study, Ziegenfuss et al. [16] measured a series of upper-body and lower-body outcomes and reported significant increases in upper-body force versus placebo and a statistical trend for A-GPC to be greater than PL. Both the Bellar and Marcus studies dosed orally for six and seven days, respectively, while Ziegenfuss delivered single oral doses as what was completed in the present study. Thus, it seems plausible that if a longer supplementation protocol was followed in the present study that force and power production may have been further augmented to yield even stronger outcomes in the present study related to performance. Future research should examine this as a possibility.
The present study also sought to examine changes in perception of affect (mood, motivation, etc.) and growth hormone changes in response to an intense, acute bout of lower-body resistance exercise. Using visual analog scales, perceptions of mood, alertness, concentration, and motivation towards physical and mental exercise were assessed and no changes were observed between any groups. The working hypothesis for these measurements suggested that the known increases in choline which occur with A-GPC supplementation may have improved these outcomes, particularly when surrounded by a challenging acute bout of exercise. Moreover, Tamura et al. [4] previously showed that 14 days of 400 mg of A-GPC given orally can positively impact mood, but no changes in these variables were observed in the present study. Thus it seems prudent to suggest that future studies should examine if longer dosing protocols would demonstrate changes in these outcomes. Circulating growth hormone levels were also evaluated after A-GPC supplementation as it has been shown in previous studies to increase growth hormone levels [2,16,36]. In contrast to the results provided by Ziegenfuss et al. [16], no differences in growth hormone concentrations were observed in the present study. While our observed changes in growth hormone align with previous investigations that reported on growth hormone changes after acute bouts of resistance exercise [37,38], the lack of changes secondary to A-GPC delivery was somewhat unexpected considering the similar dosages used and the study design replication that was employed to the Ziegenfuss study [16]. A ceiling effect surrounding growth hormone response is evident in this literature, which may have impacted any potential for A-GPC to further augment this response. Whether or not differences existed within the A-GPC remains to be seen and future studies using prolonged supplementation regimens of higher doses should be completed to continue to explore the ability of A-GPC to function as a growth hormone secretagogue
The current paper has a few key strengths to highlight starting with the randomized, double-blind, placebo-controlled, crossover study design used to examine the measured outcomes. In addition, the current study also provides insight into any dose-response outcomes which may occur with A-GPC supplementation. Other key strengths lie with the completion of both cognitive and physical performance outcomes after one dose of supplementation. A few limitations should also be highlighted for the reviewer to consider when evaluating the findings. We only recruited males into this study to best align our outcomes with the current literature and as result more research involving females should be completed to establish how well these results hold true for females. A full discovery of pairwise comparisons using LSD approaches was completed for primary and secondary outcomes to clearly understand all potential differences. It is acknowledged and should be considered by the reader that using more rigorous correction for pairwise comparisons may have impacted our final outcomes. Another key limitation was the single dose delivered as part of this study design. While results after a single dose have obvious value, being able to understand how the findings from our current study design are impacted by longer supplementation regimens would also be of interest, particularly if longer doses are also considered.
5. Conclusions
In conclusion, a single 630 mg dose of A-GPC was shown from the present study to positively impact total Stroop test scores and processing speed and tended to impact some conditions of the Flanker test while a lower dose demonstrated tendencies for improved performance when compared to placebo.
Supplementary Materials
No supplementary materials are available with this article.
Author Contributions
The author of this Study design, preparation of manuscript report.
Funding
Funding was provided by Nanjing Nutrabuilding Bio-tech Co. (NNB Nutrition, Nanjing, China) through a restricted grant to The Center for Applied Health Sciences. Outside of initial discussions, the sponsor played no part in designing the study. Further, the sponsor had no part in collecting the data, analyzing the data, or preparing the manuscript for publication.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of WCG IRB (Puyallup, WA) on 30 September 2022 (NNB-001-012024, Approval date: 1/17/2024) for human studies.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study by the contract research organization, the Center for Applied Health Sciences, in alignment with IRB guidelines and the Declaration of Helsinki.
Data Availability Statement
The data that support the findings of this study are available by reasonable request from the author upon permission from the sponsor (NNB Nutrition).
Acknowledgments
The author would like to thank the study participants for their participation in the study and the staff at the Center for Applied Health Sciences for conducting the study. Unblinded data analysis was completed by the Center for Applied Health Sciences and provided in a statistical report to the author. Publication of these results should not be considered as an endorsement of any product used in this study by the author, the Center for Applied Health Sciences, or Lindenwood University.
Conflicts of Interest
The author (CK) serves as a paid scientific advisor for the sponsor of this study (NNB Nutrition). A conflict-of-interest management plan was developed and followed by Lindenwood University which requires that the author was not involved in consenting of any human participants, data collection, or analysis of the data prior to unblinding. All data collection and statistical analysis was completed at the Center for Applied Health Sciences (Canfield, OH).
References
- Kansakar, U.; Trimarco, V.; Mone, P.; Varzideh, F.; Lombardi, A.; Santulli, G. Choline Supplements: An Update. Front Endocrinol (Lausanne) 2023, 14, 1148166. [CrossRef]
- Kawamura, T.; Okubo, T.; Sato, K.; Fujita, S.; Goto, K.; Hamaoka, T.; Iemitsu, M. Glycerophosphocholine Enhances Growth Hormone Secretion and Fat Oxidation in Young Adults. Nutrition 2012, 28, 1122–1126. [CrossRef]
- Bellar, D.; LeBlanc, N.R.; Campbell, B. The Effect of 6 Days of Alpha Glycerylphosphorylcholine on Isometric Strength. J Int Soc Sports Nutr 2015, 12, 42. [CrossRef]
- Tamura, Y.; Takata, K.; Matsubara, K.; Kataoka, Y. Alpha-Glycerylphosphorylcholine Increases Motivation in Healthy Volunteers: A Single-Blind, Randomized, Placebo-Controlled Human Study. Nutrients 2021, 13, 2091. [CrossRef]
- Marcus, L.; Soileau, J.; Judge, L.W.; Bellar, D. Evaluation of the Effects of Two Doses of Alpha Glycerylphosphorylcholine on Physical and Psychomotor Performance. J Int Soc Sports Nutr 2017, 14, 39. [CrossRef]
- Carlsson, A. Brain Neurotransmitters in Aging and Dementia: Similar Changes across Diagnostic Dementia Groups. Gerontology 1987, 33, 159–167. [CrossRef]
- Pennisi, M.; Lanza, G.; Cantone, M.; D’Amico, E.; Fisicaro, F.; Puglisi, V.; Vinciguerra, L.; Bella, R.; Vicari, E.; Malaguarnera, G. Acetyl-L-Carnitine in Dementia and Other Cognitive Disorders: A Critical Update. Nutrients 2020, 12, 1389. [CrossRef]
- Hudson, S.; Tabet, N. Acetyl-L-Carnitine for Dementia. Cochrane Database Syst Rev 2003, 2003, CD003158. [CrossRef]
- Parnetti, L.; Amenta, F.; Gallai, V. Choline Alphoscerate in Cognitive Decline and in Acute Cerebrovascular Disease: An Analysis of Published Clinical Data. Mech Ageing Dev 2001, 122, 2041–2055. [CrossRef]
- Passeri, M.; Cucinotta, D.; Bonati, P.A.; Iannuccelli, M.; Parnetti, L.; Senin, U. Acetyl-L-Carnitine in the Treatment of Mildly Demented Elderly Patients. Int J Clin Pharmacol Res 1990, 10, 75–79.
- Rai, G.; Wright, G.; Scott, L.; Beston, B.; Rest, J.; Exton-Smith, A.N. Double-Blind, Placebo Controlled Study of Acetyl-l-Carnitine in Patients with Alzheimer’s Dementia. Curr Med Res Opin 1990, 11, 638–647. [CrossRef]
- Barbagallo Sangiorgi, G.; Barbagallo, M.; Giordano, M.; Meli, M.; Panzarasa, R. Alpha-Glycerophosphocholine in the Mental Recovery of Cerebral Ischemic Attacks. An Italian Multicenter Clinical Trial. Ann N Y Acad Sci 1994, 717, 253–269. [CrossRef]
- Bunn, J.A.; Crossley, A.; Timiney, M.D. Acute Ingestion of Neuromuscular Enhancement Supplements Do Not Improve Power Output, Work Capacity, and Cognition. J Sports Med Phys Fitness 2018, 58, 974–979. [CrossRef]
- Parker, A.G.; Gordon, J.; Thornton, A.; Byars, A.; Lubker, J.; Bartlett, M.; Byrd, M.; Oliver, J.; Simbo, S.; Rasmussen, C.; et al. The Effects of IQPLUS Focus on Cognitive Function, Mood and Endocrine Response before and Following Acute Exercise. Journal of the International Society of Sports Nutrition 2011, 8, 16. [CrossRef]
- Canal, N.; Franceschi, M.; Alberoni, M.; Castiglioni, C.; De Moliner, P.; Longoni, A. Effect of L-Alpha-Glyceryl-Phosphorylcholine on Amnesia Caused by Scopolamine. Int J Clin Pharmacol Ther Toxicol 1991, 29, 103–107.
- Ziegenfuss, T.; Landis, J.; Hofheins, J. Acute Supplementation with Alpha-Glycerylphosphorylcholine Augments Growth Hormone Response to, and Peak Force Production during, Resistance Exercise. Journal of the International Society of Sports Nutrition 2008, 5, P15. [CrossRef]
- Harrington, R.N. Effects of Branched Chain Amino Acids, l-Citrulline, and Alpha-Glycerylphosphorylcholine Supplementation on Exercise Performance in Trained Cyclists: A Randomized Crossover Trial. J Int Soc Sports Nutr 2023, 20, 2214112. [CrossRef]
- Maldonado, W.G. The Effects of α-GPC Supplementation on Growth Hormone, Fat Loss, and Body Composition in Overweight Adults.
- La Monica, M.B.; Raub, B.; Ziegenfuss, E.J.; Hartshorn, S.; Grdic, J.; Gustat, A.; Sandrock, J.; Ziegenfuss, T.N. Acute Effects of Naturally Occurring Guayusa Tea and Nordic Lion’s Mane Extracts on Cognitive Performance. Nutrients 2023, 15, 5018. [CrossRef]
- La Monica, M.B.; Raub, B.; Malone, K.; Hartshorn, S.; Grdic, J.; Gustat, A.; Sandrock, J. Methylliberine Ingestion Improves Various Indices of Affect but Not Cognitive Function in Healthy Men and Women. Nutrients 2023, 15, 4509. [CrossRef]
- Jonides, J.; Schumacher, E.H.; Smith, E.E.; Lauber, E.J.; Awh, E.; Minoshima, S.; Koeppe, R.A. Verbal Working Memory Load Affects Regional Brain Activation as Measured by PET. Journal of Cognitive Neuroscience 1997, 9, 462–475. [CrossRef]
- Lopez, H.L.; Cesareo, K.R.; Raub, B.; Kedia, A.W.; Sandrock, J.E.; Kerksick, C.M.; Ziegenfuss, T.N. Effects of Hemp Extract on Markers of Wellness, Stress Resilience, Recovery and Clinical Biomarkers of Safety in Overweight, But Otherwise Healthy Subjects. Journal of Dietary Supplements 2020, 17, 561–586. [CrossRef]
- Ziegenfuss, T.N.; Kedia, A.W.; Sandrock, J.E.; Raub, B.J.; Kerksick, C.M.; Lopez, H.L. Effects of an Aqueous Extract of Withania Somnifera on Strength Training Adaptations and Recovery: The STAR Trial. Nutrients 2018, 10, 1807. [CrossRef]
- Jensen, A.R.; Rohwer, W.D. The Stroop Color-Word Test: A Review. Acta Psychologica 1966, 25, 36–93. [CrossRef]
- Kane, M.J.; Engle, R.W. Working-Memory Capacity and the Control of Attention: The Contributions of Goal Neglect, Response Competition, and Task Set to Stroop Interference. Journal of Experimental Psychology: General 2003, 132, 47–70. [CrossRef]
- Scarpina, F.; Tagini, S. The Stroop Color and Word Test. Front. Psychol. 2017, 8. [CrossRef]
- Wang, H.; He, W.; Wu, J.; Zhang, J.; Jin, Z.; Li, L. A Coordinate-Based Meta-Analysis of the n-Back Working Memory Paradigm Using Activation Likelihood Estimation. Brain Cogn 2019, 132, 1–12. [CrossRef]
- Stock, M.S.; Beck, T.W.; DeFreitas, J.M.; Dillon, M.A. Test-Retest Reliability of Barbell Velocity during the Free-Weight Bench-Press Exercise. J Strength Cond Res 2011, 25, 171–177. [CrossRef]
- Hoffman, J.R.; Ratamess, N.A.; Kang, J.; Rashti, S.L.; Faigenbaum, A.D. Effect of Betaine Supplementation on Power Performance and Fatigue. J Int Soc Sports Nutr 2009, 6, 7. [CrossRef]
- Ziegenfuss, T.N.; Cesareo, K.; Raub, B.; Kedia, A.W.; Sandrock, J.E.; Kerksick, C.M.; Ferrando, A.A.; Lopez, H.L. Effects of an Amylopectin-Chromium Complex Plus Whey Protein on Strength and Power After Eight Weeks of Resistance Training. JEN 2021, 4. [CrossRef]
- Beckenholdt, S.E.; Mayhew, J.L. Specificity among Anaerobic Power Tests in Male Athletes. J Sports Med Phys Fitness 1983, 23, 326–332.
- Stone, M.H.; Byrd, R.; Tew, J.; Wood, M. Relationship between Anaerobic Power and Olympic Weightlifting Performance. J Sports Med Phys Fitness 1980, 20, 99–102.
- Kraemer, W.J.; Ratamess, N.A. Hormonal Responses and Adaptations to Resistance Exercise and Training. Sports Med 2005, 35, 339–361. [CrossRef]
- Kraemer, W.J.; Ratamess, N.A.; Nindl, B.C. Recovery Responses of Testosterone, Growth Hormone, and IGF-1 after Resistance Exercise. J Appl Physiol (1985) 2017, 122, 549–558. [CrossRef]
- Gatti, G.; Barzaghi, N.; Acuto, G.; Abbiati, G.; Fossati, T.; Perucca, E. A Comparative Study of Free Plasma Choline Levels Following Intramuscular Administration of L-Alpha-Glycerylphosphorylcholine and Citicoline in Normal Volunteers. Int J Clin Pharmacol Ther Toxicol 1992, 30, 331–335.
- Ceda, G.P.; Ceresini, G.; Denti, L.; Marzani, G.; Piovani, E.; Banchini, A.; Tarditi, E.; Valenti, G. Alpha-Glycerylphosphorylcholine Administration Increases the GH Responses to GHRH of Young and Elderly Subjects. Horm Metab Res 1992, 24, 119–121. [CrossRef]
- Kraemer, W.J.; Marchitelli, L.; Gordon, S.E.; Harman, E.; Dziados, J.E.; Mello, R.; Frykman, P.; McCurry, D.; Fleck, S.J. Hormonal and Growth Factor Responses to Heavy Resistance Exercise Protocols. J Appl Physiol (1985) 1990, 69, 1442–1450. [CrossRef]
- Gonzalez, A.M.; Hoffman, J.R.; Townsend, J.R.; Jajtner, A.R.; Boone, C.H.; Beyer, K.S.; Baker, K.M.; Wells, A.J.; Mangine, G.T.; Robinson, E.H.; et al. Intramuscular Anabolic Signaling and Endocrine Response Following High Volume and High Intensity Resistance Exercise Protocols in Trained Men. Physiol Rep 2015, 3, e12466. [CrossRef]
Figure 1.
Timeline Schematic of Study Design and Procedures.
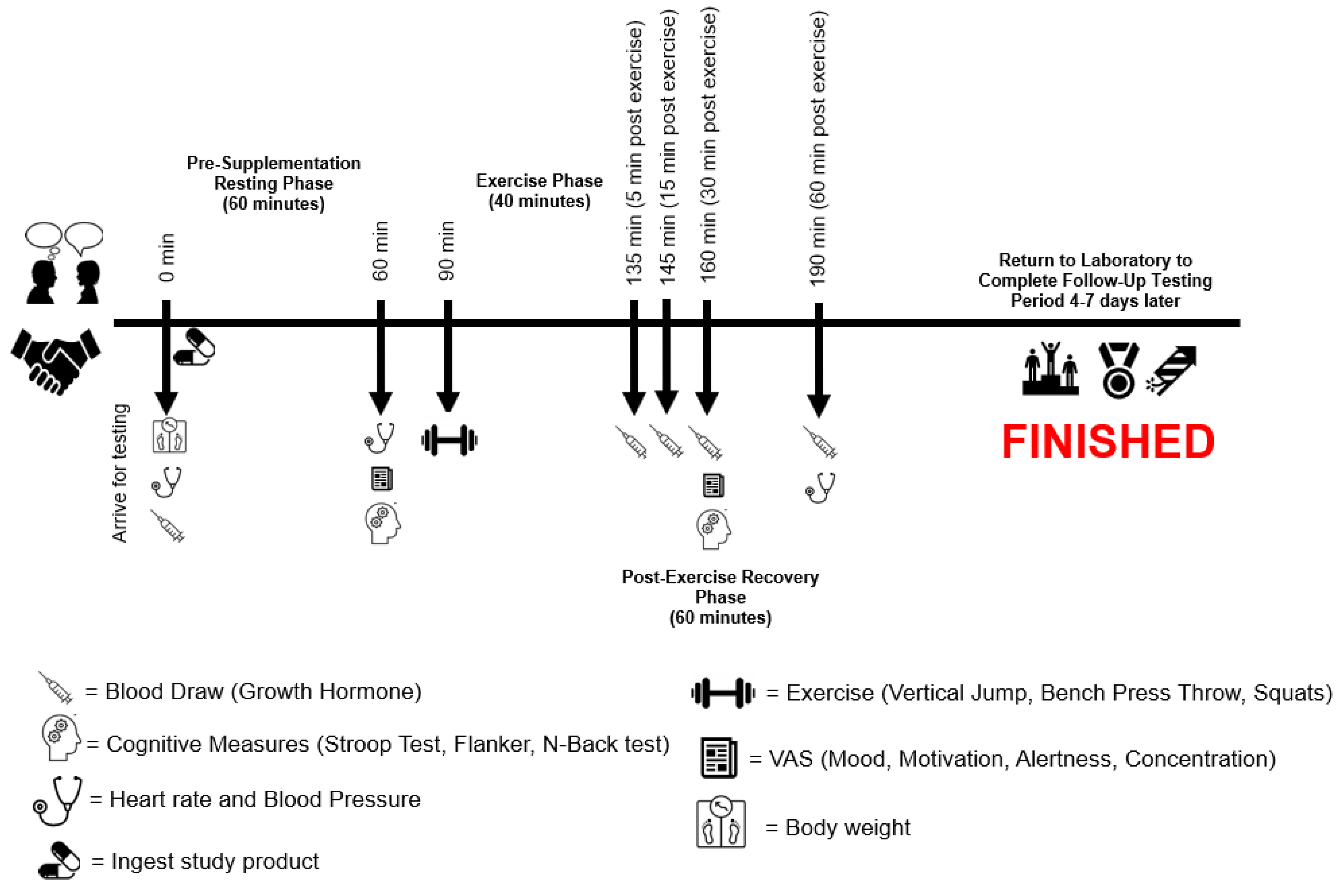
Figure 3.
Delta Stroop Total Score. * = Different than PL (p < 0.05).
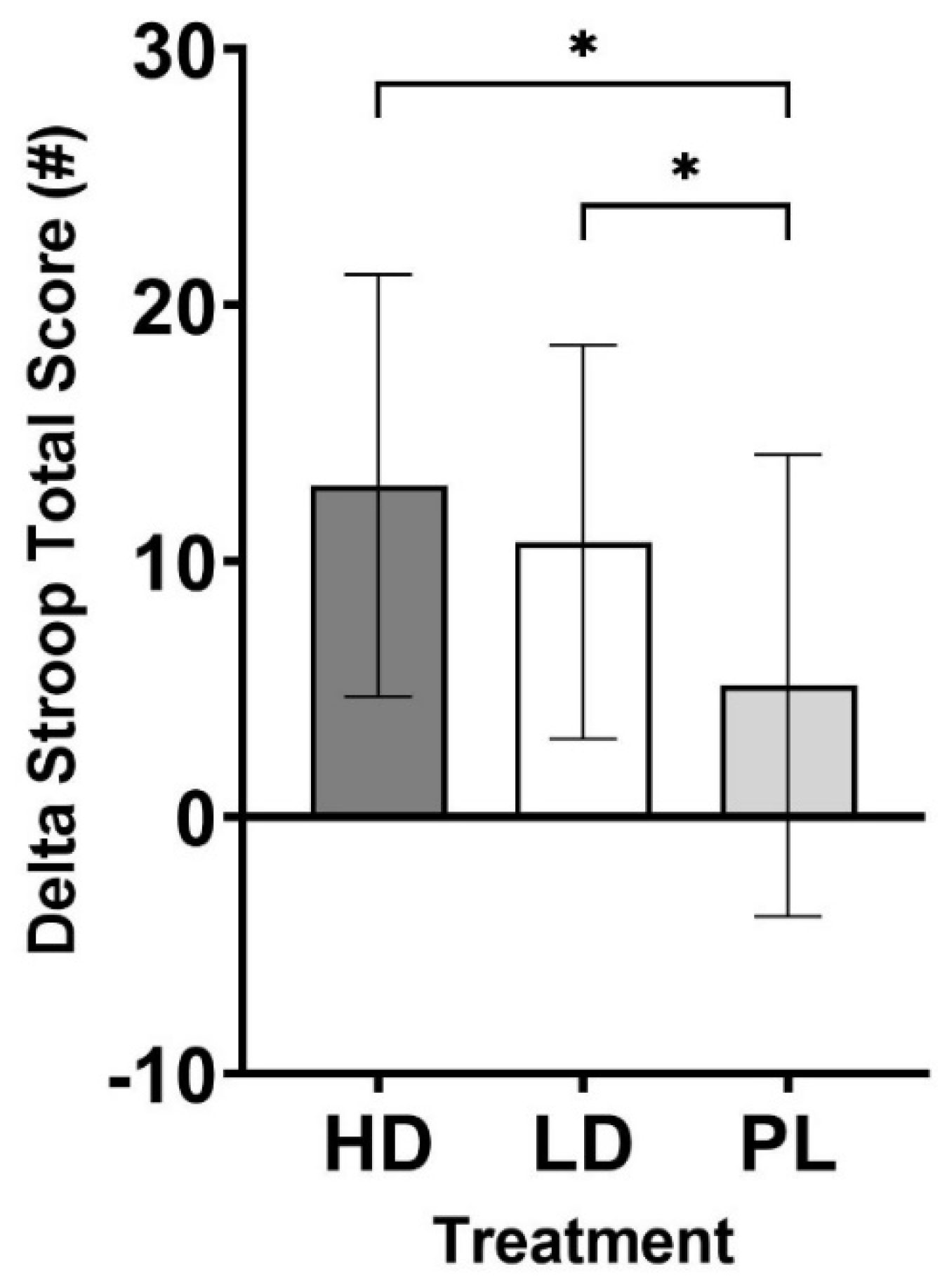
Figure 4.
Delta Time Per Score. * = Different than PL (p < 0.05).
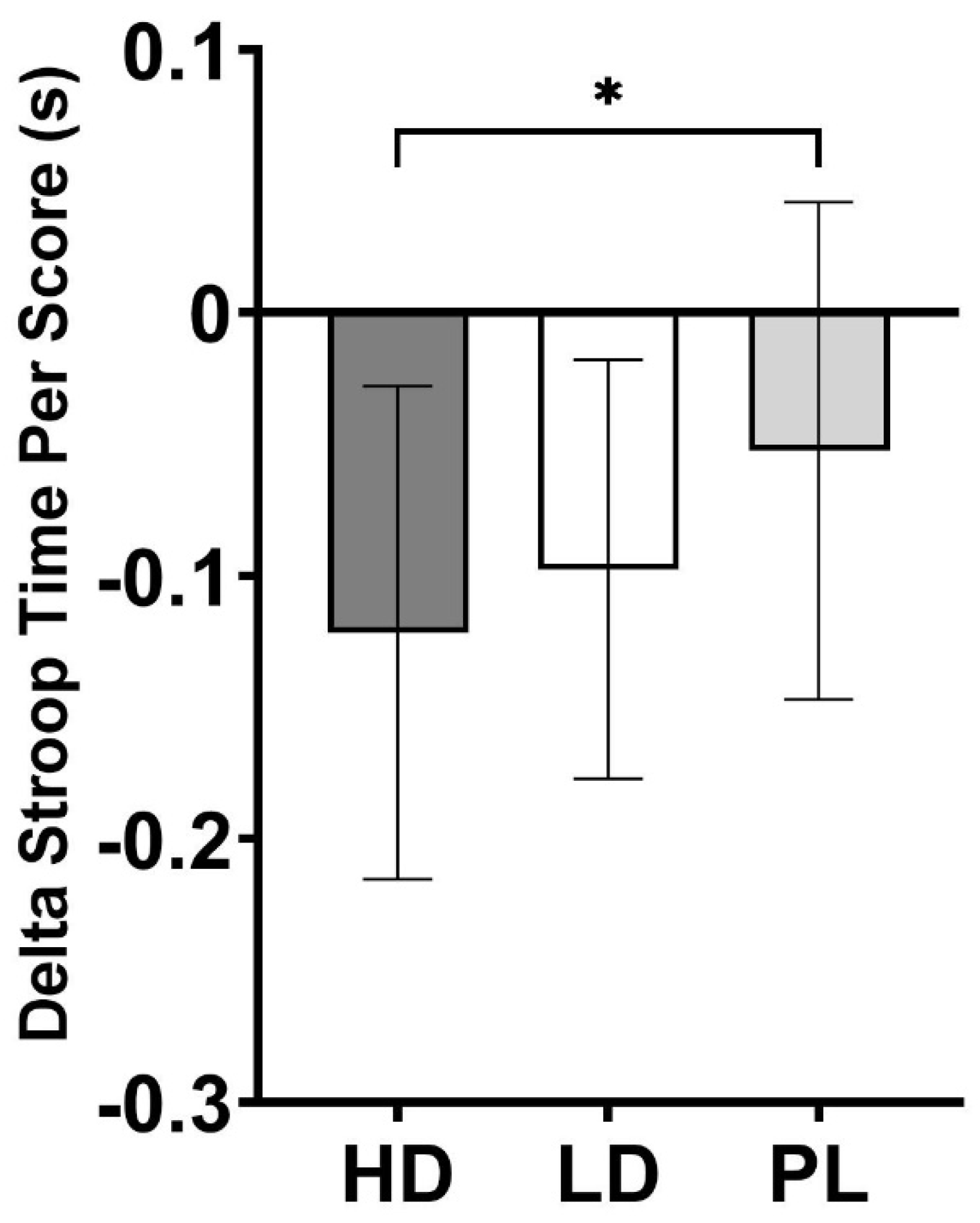

Table 1.
Overview of Study Design.
| Procedure | Visit 1 (Screen) |
Visit 2 (Day 1) |
Visit 3 (Day 8) |
Visit 4 (Day 15) |
|---|---|---|---|---|
| Informed Consent | X | |||
| Inclusion/Exclusion Criteria | X | |||
| Medical History | X | |||
| Height, weight, and BMI | X | X | X | X |
| 24-hr Dietary recall | X | |||
| CBC, CMP, Lipid Panel | X | |||
| Vitals (HR and BP) | X | |||
| Body Composition | X | |||
| Upper Body Exercise Performance | X | X | X | |
| Lower Body Exercise Performance | X | X | X | |
| Resistance Exercise Protocol | X | X | X | |
| Cognitive performance | X | X | X | X |
| Growth hormone | X | X | X | |
| Visual Analog Scales | X | X | X | |
| Vitals (HR and BP) Post-Exercise | X | X | X | |
| 24 hr Diet Records/Analysis/Repeat | X | X | X | |
| Protocol Compliance | X | X | X | |
| Dispense Test Product | X | X | X | |
| Adverse Events Monitoring | X | X | X | X |
Table 2.
Study Participant Characteristics (n=20).
| Variable | Mean ± SD |
|---|---|
| Age (years) | 31.3 ± 11.0 |
| Height (cm) | 178.6 ± 7.3 |
| Weight (kg) | 84.6 ± 11.4 |
| Body Mass Index (kg/m2) | 26.4 ± 2.5 |
| Body Fat (%) | 15.4 ± 5.6 |
| Systolic Blood Pressure (mm Hg) | 120.7 ± 12.1 |
| Diastolic Blood Pressure (mm Hg) | 72.3 ± 9.0 |
| Resting Heart Rate (bpm) | 63.4 ± 8.7 |
| White Blood Cell Count (x103/µL) | 5.3 ± 1.4 |
| Red Blood Cell Count (x106/µL) | 5.3 ± 0.4 |
| Hemoglobin (g/dL) | 15.8 ± 0.7 |
| Hematocrit (%) | 46.5 ± 2.1 |
| Glucose (mg/dL) | 90.0 ± 9.8 |
| Blood Urea Nitrogen (mg/dL) | 16.8 ± 5.3 |
| Creatinine (mg/dL) | 1.1 ± 0.2 |
| BUN/Creatinine ratio | 91.8 ± 16.9 |
| eGFR (mL/min/1.73) | 14.7 ± 3.5 |
| Sodium (mmol/L) | 140.8 ± 1.9 |
| Potassium (mmol/L) | 4.5 ± 0.4 |
| Chloride (mmol/L) | 103.1 ± 2.0 |
| CO2 (mmol/L) | 23.9 ± 1.5 |
| Calcium (mg/dL) | 9.5 ± 0.3 |
| Total Protein (g/dL) | 7.1 ± 0.4 |
| Albumin (g/dL) | 4.7 ± 0.2 |
| Globulin (g/dL) | 2.4 ± 0.3 |
| Albumin/Globulin ratio | 2.0 ± 0.3 |
| Bilirubin (mg/dL) | 0.6 ± 0.3 |
| Alkaline Phosphatase (IU/L) | 69.3 ± 14.4 |
| AST (IU/L) | 23.5 ± 5.7 |
| ALT (IU/L) | 25.7 ± 7.0 |
| Total Chol (mg/dL) | 162.0 ± 25.3 |
| Triglycerides (mg/dL) | 102.4 ± 112.1 |
| HDL (mg/dL) | 50.0 ± 10.6 |
| VLDL (mg/dL) | 18.6 ± 16.8 |
| LDL (mg/dL) | 93.4 ± 21.1 |
| LDL/HDL | 1.9 ± 0.4 |
| Total/HDL | 3.5 ± 1.0 |
Table 3.
Summary of Adverse Events.
| Treatment | HD | LD | PL |
|---|---|---|---|
| Severity | |||
| Mild | 2 | ||
| Moderate | 2 | 2 | 4 |
| Severe | |||
| Relationship to Study Treatment (Product) | |||
| Unlikely | 1 | 1 | 1 |
| Possible | 1 | 3 | 3 |
| Probable | |||
| Relationship to Test Article (Procedural) | |||
| Unlikely | |||
| Possible | |||
| Probable | 2 | 4 | 4 |
| Body Systems and AEs | |||
| Gastrointestinal | |||
| Emesis (regurgitate) | 1 | 2 | |
| Nausea | 1 | 1 | 1 |
| Retching (dry heaving) | 1 | ||
| Nervous | |||
| Cephalalgia (headache) | 1 | ||
| Cardiovascular | |||
| Presyncope (lightheaded) | 3 | 2 | |
| Total Number of Adverse Events Experienced During Study | 3 | 5 | 5 |
| Total Number of Subjects Experiencing AEs: n (%) | 2/20 (10%) | 4/21 (19%) | 4/20 (20%) |
Table 4.
Hemodynamics.
| 0 min Post-Ingestion | 60 min Post Ingestion | 30 min Post Exercise | ||
|---|---|---|---|---|
| Systolic Blood Pressure (mm Hg) | HD | 121.1 ± 10.3 | 121.1 ± 11.4 | 116.4 ± 12.1 |
| LD | 120.1 ± 9.3 | 120.4 ± 7.9 | 115.3 ± 11.6 | |
| PL | 123.1 ± 10.7 | 121.0 ± 9.8 | 116.9 ± 12.3 | |
| Diastolic Blood Pressure (mm Hg) | HD | 74.9 ± 8.0 | 74.6 ± 7.4 | 73.5 ± 8.3 |
| LD | 72.5 ± 8.6 | 77.5 ± 8.5† | 71.9 ± 8.3† | |
| PL | 73.6 ± 7.2 | 76.8 ± 7.1 | 71.1 ± 7.0† | |
| Heart Rate (beats/min) | HD | 62.6 ± 11.4 | 58.9 ± 10.2† | 72.6 ± 12.0† |
| LD | 62.7 ± 8.7 | 60.7 ± 8.6 | 74.1 ± 8.6† | |
| PL | 61.3 ± 10.4 | 59.5 ± 9.7 | 74.2 ± 12.4† |
† = different than 0 min Post-Ingestion (p < 0.05).
Table 5.
Cognitive Performance.
| HD | LD | PL | p | |
|---|---|---|---|---|
| Stroop Total Score | 13.0 ± 8.2** | 10.8 ± 7.7** | 5.2 ± 9.0 | 0.016 |
| Stroop Accuracy | 0.29 ± 0.85‡ | -0.58 ± 0.90 | -0.16 ± 1.35 | 0.073 |
| Stroop Time Per Score (s) | -0.12 ± 0.09** | -0.10 ± 0.08* | -0.05 ± 0.09 | 0.030 |
| Flanker Compatible Accuracy (%) | -1.24 ± 3.1 | -0.16 ± 2.57 | 0.00 ± 2.26 | 0.376 |
| Flanker Compatible Reaction Time (ms) | -51.2 ± 53.9** | -13.0 ± 97.2 | -13.0 ± 51.6 | 0.126 |
| Flanker Incompatible Accuracy (%) | -0.63 ± 2.97 | 0.00 ± 3.03 | -0.78 ± 1.99 | 0.754 |
| Flanker Incompatible Reaction Time (ms) | -39.2 ± 60.1 | -18.2 ± 107 | -14.1 ± 48.8 | 0.467 |
| Flanker None Accuracy (%) | -1.25 ± 2.19 | -0.39 ± 3.07 | 0.23 ± 0.76 | 0.214 |
| Flanker None Reaction Time (ms) | -34.1 ± 56.3# | -11.5 ± 89.4 | -19.4 ± 73.4 | 0.165 |
| N-Back Score (au) | 853 ± 1973 | 828 ± 1455 | 1486 ± 2328 | 0.490 |
| N-Back Correct (#) | 7.2 ± 7.5 | 5.2 ± 5.3 | 6.5 ± 7.0 | 0.617 |
| N-Back Attempted (#) | 9.2 ± 8.5 | 6.2 ± 5.4 | 7.5 ± 6.6 | 0.395 |
| N-Back Accuracy (%) | -1.7 ± 2.5 | -0.5 ± 2.2 | -0.4 ± 3.0 | 0.241 |
| N-Back Time Per Score (ms) | -81.7 ± 107 | -71.7 ± 81.5 | -67.4 ± 55.4 | 0.951 |
All values are reported and analyzed as delta scores (30 min post-exercise – 60 min post-ingestion of assigned supplement). p = Oneway ANOVA. * = Trend vs. PL (p < 0.10). ** = Significantly different than PL (p < 0.05). # = Trend vs. LD (p < 0.10). ‡ = Significantly different than LD (p < 0.05).
Table 6.
Visual Analog Scales.
| 60 min Post-Ingestion | p | 30 min Post-Exercise | p | ||
|---|---|---|---|---|---|
| Mood | HD | 7.2 ± 1.2 | 0.649 | 7.1 ± 1.3 | 0.189 |
| LD | 7.3 ± 1.4 | 7.0 ± 1.7 | |||
| PL | 7.1 ± 1.3 | 6.5 ± 1.8 | |||
| Motivation Towards Physical Exercise | HD | 6.6 ± 1.6 | 0.320 | 5.7 ± 2.4 | 0.546 |
| LD | 6.9 ± 1.4 | 5.4 ± 2.5 | |||
| PL | 6.4 ± 1.4 | 5.1 ± 2.6 | |||
| Motivation Towards Mental Exercise | HD | 6.8 ± 1.7 | 0.664 | 6.3 ± 1.9 | 0.182 |
| LD | 6.9 ± 1.6 | 6.6 ± 2.1 | |||
| PL | 6.6 ± 1.7 | 5.7 ± 2.2 | |||
| Alertness | HD | 7.2 ± 1.3 | 0.197 | 6.3 ± 2.2 | 0.860 |
| LD | 6.7 ± 2.3 | 6.3 ± 2.6 | |||
| PL | 6.2 ± 2.5 | 6.1 ± 2.6 | |||
| Concentration | HD | 7.2 ± 1.3 | 0.385 | 6.5 ± 1.7 | 0.942 |
| LD | 7.2 ± 1.4 | 6.5 ± 2.1 | |||
| PL | 6.9± 1.5 | 66. ± 1.8 |
p = p-value of one-way ANOVA.
Table 7.
Physical Performance.
| HD | LD | PL | p | |
|---|---|---|---|---|
| Bench Press Average Power (watts) | 509 ± 94 | 527 ± 107 | 506 ± 101 | 0.198 |
| Bench Press Peak Power (watts) | 913 ± 192# | 909 ± 213 | 864 ± 202 | 0.168 |
| Bench Press Peak Velocity (m/s) | 1.36 ± 0.22 | 1.38 ± 0.23 | 1.35 ± 0.23 | 0.296 |
| Bench Press Peak Force (N) | 898 ± 168** | 915 ± 210* | 869 ± 193 | 0.159 |
| Vertical Jump Average Power (watts) | 1572 ± 263 | 1569 ± 286 | 1573 ± 278 | 0.954 |
| Vertical Jump Peak Power (watts) | 7309 ± 2719# | 8403 ± 4363* | 7546 ± 3555 | 0.085 |
| Vertical Jump Peak Velocity (m/s) | 3.45 ± 0.44* | 3.42 ± 0.45 | 3.37 ± 0.45 | 0.160 |
| Vertical Jump Peak Force (N) | 2899 ± 1155‡ | 3080 ± 1060* | 2916 ± 1192 | 0.050 |
p = Oneway ANOVA. * = Trend vs. PL (p < 0.10). ** = Significantly different than PL (p < 0.05). # = Trend vs. LD (p < 0.10). ‡ = Significantly different than LD (p < 0.05).
Table 8.
Growth Hormone (ng/mL).
| Time | HD | LD | PL | p | |
|---|---|---|---|---|---|
| 0 min | 0.58 ± 1.38 | 0.72 ± 2.12† | 0.35 ± 0.59† | Group | <0.001 |
| 5 min | 9.82 ± 6.72† | 14.00 ± 12.66† | 11.63 ± 11.46† | Time | < 0.001 |
| 15 min | 9.61 ± 7.27† | 11.81 ± 10.51† | 10.60 ± 11.72† | Group x Time | 0.174 |
| 30 min | 5.99 ± 4.86† | 7.94 ± 6.43† | 8.93 ± 14.03† | ||
| 60 min | 2.73 ± 3.01 | 3.04 ± 2.42† | 3.99 ± 6.62† |
† = Different than 0 min (p < 0.05).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



