Submitted:
10 October 2024
Posted:
11 October 2024
You are already at the latest version
Abstract
Objective: To analyze the relationship and predictive value of Netrin-1 expression and ultrasonic blood flow parameters with the severity of cervical intraepithelial neoplasia (CIN). Methods: The receiver operating characteristic (ROC) curve analysis was used to evaluate the predictive value of Netrin-1 expression and ultrasonic blood flow parameters for the severity of cervical intraepithelial neoplasia. Results: FI, VI, and VFI levels increased sequentially, and the differences in levels between grade II, III patients, and the control group were statistically significant (P < 0.05). Netrin-1 was negatively correlated with ultrasonic blood flow parameters FI, VI, and VFI (r = -0.287, -0.309, -0.298, P < 0.05). The results of multifactorial logistic regression analysis showed that Netrin-1 positivity was a protective factor for CIN III lesions, while FI, VI, and VFI were risk factors for CIN III lesions. The AUC area of Netrin-1 was 0.712, with a sensitivity and specificity of 76.4% and 79.5%, respectively, which were higher than those of other indicators (P < 0.05). Conclusion: Netrin-1 is under-expressed in CIN patients, while ultrasonic blood flow parameters FI, VI, and VFI are over-expressed, and both are closely related to the severity of the patient's lesions. Netrin-1 is negatively correlated with ultrasonic blood flow parameters FI, VI, and VFI. Netrin-1 positivity is a protective factor for CIN III lesions, while FI, VI, and VFI are risk factors for CIN III lesions. The expression levels of both have a certain predictive guiding role in the early screening, diagnosis, and prevention of cervical cancer.
Keywords:
Netrin-1
; ultrasonic blood flow parameters
; cervical intraepithelial neoplasia
; severity
; predictive value
Introduction
Cervical intraepithelial neoplasia (CIN) is one of the precancerous lesions of cervical cancer, with a high malignant transformation rate, posing a potential threat to women's health [1]. Despite cervical cytological screening and cervical biopsy being commonly used diagnostic methods clinically, the accurate diagnosis of early CIN and assessment of disease severity still present challenges [2]. Netrin-1, as an important molecular signaling regulator, plays a crucial role in nervous system development [3]. Recent studies [4] have found that Netrin-1 expression levels are abnormal in various tumors and participate in tumorigenesis, development, and angiogenesis processes. However, the expression of Netrin-1 in cervical diseases and its relationship with disease severity have not been fully elucidated. Additionally, ultrasound blood flow parameters have important value in assessing tumor blood supply [5]. Through Doppler ultrasound examination and related software analysis, blood flow parameters such as flow index (FI), vascularization index (VI), and vascularization flow index (VFI) can be obtained to objectively evaluate tumor blood supply [6]. This study aims to explore the expression of Netrin-1 in CIN patients and analyze its correlation with ultrasonic blood flow parameters in disease severity assessment. Through retrospective analysis of clinical data of CIN patients and patients with chronic cervicitis, we attempt to validate whether Netrin-1 and ultrasonic blood flow parameters can serve as potential biomarkers and auxiliary diagnostic methods for early screening, diagnosis, and prevention of cervical cancer transformation. The results of this study are expected to provide new diagnostic and therapeutic insights for clinical practice, and offer more accurate evidence for early prevention and intervention of cervical cancer.
2. Materials and Methods
2.1. Clinical Data
A retrospective analysis was conducted on the clinical data of 115 patients with Cervical Intraepithelial Neoplasia (CIN) admitted to our hospital from January 2022 to January 2024, and they were included in the observation group (pathological examination showed 42 cases of CIN I, 39 cases of CIN II, and 34 cases of CIN III). Additionally, 37 patients with chronic cervicitis during the same period were selected as the control group. Inclusion criteria: all were clinically diagnosed with CIN or chronic cervicitis through relevant tests [7, 8]; aged 18 to 70 years, female; all underwent surgical treatment at our hospital; lesion tissues were obtained during surgery and confirmed by immunohistochemical staining pathology; no history of radiotherapy or chemotherapy before surgery and no history of hormone treatment within six months; complete and reliable clinical data available for analysis. Exclusion criteria: severe dysfunction of important organs; abnormalities in immune function, coagulation function, hematopoietic function, etc.; presence of malignant tumors; concomitant cognitive impairment, consciousness disorders; history of previous cervical surgery. The basic data including age, body mass index (BMI), and course of disease of the two groups were comparable (P > 0.05). After abnormal findings in cervical cytology examination, all patients underwent preoperative three-dimensional energy Doppler ultrasound examination, and pathological examination was performed on the lesion specimens obtained during surgery. This study has been approved by the hospital's Ethics Committee.
2.2. Methods
This study The protocol was approved by the ethics committee of Hebei Petro China Center Hospital, No.2975913. Informed consent was obtained from all study participants.. All the methods were carried out in accordance with the Declaration of Helsinki.
2.2.1. Immunohistochemical Staining
Paraffin tissue sections were set to a thickness of 4 μm, and staining was performed according to the instructions of the kit. During staining, the working concentration of Netrin-1 monoclonal antibody was diluted to 1:100. Pathological tissue sections were used as positive controls, while phosphate-buffered saline (PBS) was used instead of the primary antibody for negative controls. Positive cells were characterized by clear cell structure and staining in brown or tan. To semi-quantitatively evaluate the positive results of Netrin-1, the staining intensity of cells was divided into different grades (0 for no staining, 1 for pale yellow, 2 for tan, and 3 for brown). Additionally, the percentage of positive cells in the sample was assessed (0 for no positive cells, 1 for less than 25% positive cells, 2 for 25% to 50% positive cells, and 3 for more than 50% positive cells). The product of the staining intensity of cells and the percentage of positive cells was calculated, and if it reached or exceeded 2 points, it was considered as immunohistochemical positive (+), otherwise, it was negative (-).
2.2.2. Netrin-1 mRNA Expression Level in Pathological Tissues
Fluorescence quantitative PCR technology was used to detect the expression level of Netrin-1 mRNA in pathological tissues. Total RNA was extracted from tissue samples using Trizol (Sigma, USA). Reverse transcription reaction was performed, followed by PCR amplification, with β-actin as an internal reference. The PCR amplification conditions were set as follows: pre-denaturation at 95°C for 30 seconds, followed by 40 cycles of denaturation at 95°C for 5 seconds, and extension at 60°C for 35 seconds. The specific primer sequences are shown in Table 1 below. Finally, the expression level of Netrin-1 mRNA was calculated using the 2-△△Ct method.
2.2.3. Ultrasonography
A GE E8 Hitachi ultrasound diagnostic instrument was used for transvaginal cervical ultrasound examination in non-menstruating patients, with a probe frequency set at 5 to 10 MHz. Before the examination, patients were asked to empty their bladders and assume the lithotomy position. At the beginning of the ultrasound examination, routine disinfection of the external genitalia was performed, followed by covering the probe with a condom and applying coupling agent, then slowly inserting the probe into the patient's vagina until the vaginal fornix. The size, echo, continuity of the cervical endometrial line, and thickening of the cervix were recorded and observed. If a mass was found, its size, internal echo, and hemodynamic characteristics were further observed, and the blood flow index (FI), vascularization index (VI), and vascularization flow index (VFI) were calculated using VOCAL software at the site of strongest blood flow signal. All ultrasound examinations and blood flow data measurements were performed by the same professional physician. The cervix was scanned three times at the lesion site for each patient, and the average value was statistically analyzed.
2.3. Statistical Analysis
Data were processed using SPSS 20.0 software package. Measurement data were expressed as (), and t-test was used; count data were expressed as n (%), and chi-square test was used; Pearson method was used to analyze the correlation between Netrin-1 and ultrasound blood flow parameters FI, VI, and VFI; multiple-factor logistic regression analysis was used to analyze the factors affecting the severity of CIN; ROC curve analysis was used to assess the predictive value. P < 0.05 indicated statistical significance.
3. Results
3.1. Netrin-1 Fluorescence Quantitative PCR Expression Level and Immunohistochemical Staining Results
The expression level of Netrin-1 mRNA in the observation group was lower than that in the control group (P < 0.05). The expression level of Netrin-1 mRNA in patients with CIN I, II, and III decreased sequentially, with statistically significant differences compared to the control group (P < 0.05). Under the microscope, the positive expression rate of Netrin-1 protein in the observation group tissue was lower than that in the control group (P < 0.05). There were statistically significant differences in the positive expression rate of Netrin-1 protein in the pathological tissues of CIN I, II, and III patients (P < 0.05), as shown in Table 2.
3.2. Comparison of Ultrasound Blood Flow Parameters Levels in Patients with Different Degrees of Lesions
The ultrasound blood flow parameters FI, VI, and VFI in the observation group were all higher than those in the control group (P < 0.05). The levels of FI, VI, and VFI in patients with CIN I, II, and III in the observation group increased sequentially, and the differences between patients with CIN II, III and the control group were statistically significant (P < 0.05), as shown in Table 3.
3.3. Correlation between Netrin-1 and Ultrasound Blood Flow Parameters FI, VI, and VFI
Netrin-1 showed a negative correlation with ultrasound blood flow parameters FI, VI, and VFI (r=-0.287, -0.309, -0.298, P < 0.05), as shown in Figure 1.
3.4. Analysis of Factors Affecting the Severity of CIN
Using the occurrence of Grade III lesions in CIN patients as the dependent variable and Netrin-1 expression level, ultrasound blood flow parameters FI, VI, and VFI as independent variables, multiple logistic regression analysis was conducted. The results showed that Netrin-1 positivity was a protective factor for Grade III CIN lesions, while FI, VI, and VFI were risk factors for Grade III CIN lesions, as shown in Table 4.
3.5. Predictive Value of Different Indicators for CIN Grade III Lesions
4. Discussion
Currently, the methods for clinical treatment of CIN mainly include cervical conization or physical therapy, although these methods can partially inhibit the development of CIN, the overall efficacy of treatment is not high [9]. The condition of CIN often continues to deteriorate, and the risk of CIN grade III lesions developing into cervical cancer remains quite high [10]. Research [11] indicates that in endometrial diseases, endometrial invasion, neovascularization, and neural fiber proliferation all play important roles. Netrin-1 is a secreted protein with a molecular weight of 80 kD, its main function is to guide the growth and development of neuronal axons in specific directions through regulation by its receptors [12]. However, due to the diversity of its receptors, the action of Netrin-1 can be either attractive or repulsive [13]. Vascular and neural structures have anatomical similarities, and research [14] suggests that fluoxetine can upregulate the expression of HIF-1α-Netrin/VEGF cascade proteins, thereby promoting angiogenesis and improving long-term functional recovery after ischemic stroke. Furthermore, research [15] indicates that Netrin-1 can induce angiogenesis of endometrial lesions by interacting with CD146 in vascular endothelial cells, playing an important role in neurovascularization of endometriosis. Therefore, Netrin-1 not only promotes the proliferation of vascular endothelial cells but also promotes their migration and adhesion. In this study, we found that the expression of Netrin-1 was significantly increased in the cell membrane, cytoplasm, and cell-cell junctions of fibrous proliferative tissues. Compared with the control group, the positive expression rate of Netrin-1 protein in CIN patients in the observation group was significantly decreased, and with the worsening of the lesion, its expression rate showed a decreasing trend. This suggests that Netrin-1 may play an important protective role in the development of CIN, but its specific mechanism of action is unclear and requires further research for clarification. In addition, neurovascularization is crucial for the survival of metastatic tissues and metastatic tumors. Research [16] indicates that interleukin-1 (IL-1), a pro-inflammatory cytokine secreted by macrophages, may regulate the generation of neural cells by stimulating ectopic endometrial stromal cells. Recent studies [17] have also found that Netrin-1 can inhibit cell apoptosis by increasing the proportion of regulatory T cells and reducing the infiltration of T cells and macrophages, thereby reducing lung ischemia-reperfusion injury in mice. Therefore, we speculate that Netrin-1 may be involved in the physiological and pathological processes of vascular genesis and inflammatory response in CIN patients through different pathways. In conclusion, the treatment of CIN still faces challenges, and Netrin-1, as an important regulatory factor, may play a crucial protective role in the development of CIN. However, its specific mechanism is unclear and further research is needed for in-depth exploration.
In recent years, with the widespread application and development of Doppler ultrasound technology, its importance in the diagnosis and treatment of cervical lesions has gradually become prominent [18]. Compared to traditional two-dimensional imaging, Doppler ultrasound detection can visually display abnormal blood flow signals within lesion or cancerous tissues, aiding in accurately distinguishing the blood flow situation of lesions, cancerous tissues, and surrounding tissues [19]. Through computer software combined analysis, hemodynamic parameters such as FI, VI, and VFI can be directly obtained, which helps to better guide clinical treatment and analysis work. FI represents the total number of blood cells detected at the moment of three-dimensional scanning, VI represents the number of vessels detected at the lesion site, and VFI indicates the sum of all vascular information and blood cell counts detected at the lesion site [20]. In the early diagnosis of cervical dysplasia and carcinoma, vaginal ultrasound, as an intracavitary ultrasound technique, has a high image resolution and can accurately detect abnormal blood flow signals within lesion foci, possessing high clinical utility. Multiple studies [21, 22] have shown that in early cervical dysplasia and carcinoma, vaginal ultrasound can clearly display cervical layer structures, accurately analyze the infiltration of lesions or carcinomas and surrounding tissue conditions, and has high sensitivity. The results of this study showed that the Doppler ultrasound blood flow parameters FI, VI, and VFI values in the observation group were significantly higher than those in the control group. With the deepening of the lesion degree, FI, VI, and VFI values increased successively, indicating that compared with the control group, there is neoangiogenesis at the lesion site of CIN patients, and with the aggravation of the lesion degree, the number of neoangiogenesis increases, and blood flow perfusion enhances, which is consistent with previous related research results [23]. Pearson correlation analysis results showed that Netrin-1 was negatively correlated with FI, VI, and VFI values. Further Logistic multivariate analysis showed that Netrin-1 positivity was a protective factor for CIN grade III lesions, while FI, VI, and VFI were risk factors for CIN grade III lesions. In addition, this study also preliminarily explored the predictive value of Netrin-1 expression and Doppler ultrasound blood flow parameters for the severity of cervical intraepithelial neoplasia. According to clinical ROC curve research results, when the AUC area is greater than 0.7, it indicates certain predictive value, and when the AUC area is greater than 0.85, it suggests higher predictive value. The results of this study showed that the AUC areas of Netrin-1 were 0.732, with a sensitivity of 76.4% and a specificity of 79.5%, higher than other indicators, indicating that Netrin-1 expression has a certain predictive value for predicting the severity of cervical intraepithelial neoplasia. Therefore, closely monitoring the dynamic changes of this indicator is of great significance for predicting and guiding timely clinical interventions.
In summary, CIN patients exhibit low expression of Netrin-1 and high expression of Doppler ultrasound blood flow parameters FI, VI, and VFI, which are closely related to the severity of the patient's condition. Netrin-1 is negatively correlated with Doppler ultrasound blood flow parameters FI, VI, and VFI. Netrin-1 positivity is a protective factor for CIN grade III lesions, while FI, VI, and VFI are risk factors for CIN grade III lesions. The expression levels of both have a certain predictive and guiding role in early screening, diagnosis, treatment, and prevention of cervical cancer. It is worth noting that although this study has achieved some positive results in analyzing the relationship and predictive value of Netrin-1 expression and Doppler ultrasound blood flow parameters with the severity of CIN, the study itself still has some limitations, such as: ① Small sample size: The relatively small sample size included in this study may limit the reliability and generalizability of the results; ② Retrospective study design: This study used a retrospective analysis method, which may have information bias and incomplete data issues, and cannot rule out the influence of other potential factors; ③ Failure to consider other relevant factors: In addition to Netrin-1 and Doppler ultrasound blood flow parameters, there may be other factors affecting cervical intraepithelial neoplasia, such as viral infections, genetic factors, lifestyles, etc., but this study did not fully consider these factors, which may affect the interpretation and inference of the results to some extent. Therefore, although this study has made some progress, further research and validation are still needed to refine and confirm its results, and promote its application in clinical practice.
References
- Bowden, S.J., et al., Risk factors for human papillomavirus infection, cervical intraepithelial neoplasia and cervical cancer: an umbrella review and follow-up Mendelian randomisation studies. BMC Med, 2023. 21(1): p. 274. [CrossRef]
- Chen, Y., et al., Human papillomavirus infection and cervical intraepithelial neoplasia progression are associated with increased vaginal microbiome diversity in a Chinese cohort. BMC Infect Dis, 2020. 20(1): p. 629. [CrossRef]
- Cassier, P.A., et al., Netrin-1 blockade inhibits tumour growth and EMT features in endometrial cancer. Nature, 2023. 620(7973): p. 409-416. [CrossRef]
- Gao, R., et al., Macrophage-derived netrin-1 drives adrenergic nerve-associated lung fibrosis. J Clin Invest, 2021. 131(1). [CrossRef]
- Panova, I.E., E.V. Samkovich, and P.A. Nechiporenko, [Doppler ultrasound in the assessment of blood supply to choroidal melanoma: parallels with contrast angiography and histography]. Vestn Oftalmol, 2023. 139(1): p. 27-34. [CrossRef]
- Sakuragi, T., et al., Relationship between placental hemodynamics and placental histological analysis in third trimester. J Obstet Gynaecol Res, 2023. 49(2): p. 560-567. [CrossRef]
- Burness, J.V., J.M. Schroeder, and J.B. Warren, Cervical Colposcopy: Indications and Risk Assessment. Am Fam Physician, 2020. 102(1): p. 39-48.
- Shroff, S., Infectious Vaginitis, Cervicitis, and Pelvic Inflammatory Disease. Med Clin North Am, 2023. 107(2): p. 299-315.
- Kalliala, I., et al., Incidence and mortality from cervical cancer and other malignancies after treatment of cervical intraepithelial neoplasia: a systematic review and meta-analysis of the literature. Ann Oncol, 2020. 31(2): p. 213-227. [CrossRef]
- Loopik, D.L., et al., The Natural History of Cervical Intraepithelial Neoplasia Grades 1, 2, and 3: A Systematic Review and Meta-analysis. J Low Genit Tract Dis, 2021. 25(3): p. 221-231. [CrossRef]
- Soler, M., et al., Thermal Ablation Treatment for Cervical Precancer (Cervical Intraepithelial Neoplasia Grade 2 or Higher [CIN2+]). Methods Mol Biol, 2022. 2394: p. 867-882.
- Luo, Y., S. Liao, and J. Yu, Netrin-1 in Post-stroke Neuroprotection: Beyond Axon Guidance Cue. Curr Neuropharmacol, 2022. 20(10): p. 1879-1887. [CrossRef]
- Ziegon, L. and M. Schlegel, Netrin-1: A Modulator of Macrophage Driven Acute and Chronic Inflammation. Int J Mol Sci, 2021. 23(1). [CrossRef]
- Claro, V. and A. Ferro, Netrin-1: Focus on its role in cardiovascular physiology and atherosclerosis. JRSM Cardiovasc Dis, 2020. 9: p. 2048004020959574. [CrossRef]
- Vásquez, X., P. Sánchez-Gómez, and V. Palma, Netrin-1 in Glioblastoma Neovascularization: The New Partner in Crime? Int J Mol Sci, 2021. 22(15).
- Bellina, M. and A. Bernet, [Netrin-1, a novel antitumoral target]. Med Sci (Paris), 2022. 38(4): p. 351-358.
- Lu, X., et al., Engineered exosomes enriched in netrin-1 modRNA promote axonal growth in spinal cord injury by attenuating inflammation and pyroptosis. Biomater Res, 2023. 27(1): p. 3. [CrossRef]
- Li, J., et al., Ultrasonographic diagnosis in rare primary cervical cancer. Int J Gynecol Cancer, 2021. 31(12): p. 1535-1540. [CrossRef]
- Zhang, P., Q. Zhou, and Z. Zeng, Combination of serum FOXR2 and transvaginal three-dimensional power Doppler ultrasonography in the diagnosis of uterine lesions. Adv Clin Exp Med, 2023. [CrossRef]
- Wang, Y., et al., The Application Value of Three-Dimensional Power Doppler Ultrasound in Fetal Growth Restriction. Evid Based Complement Alternat Med, 2022. 2022: p. 4087406. [CrossRef]
- Saidman, J.M., et al., Importance of Doppler ultrasound in vaginal foreign body: case report and review of the literature. J Ultrasound, 2022. 25(2): p. 409-412. [CrossRef]
- Pozzati, F., et al., Clinical and ultrasound characteristics of vaginal lesions. Int J Gynecol Cancer, 2021. 31(1): p. 45-51. [CrossRef]
- Nam, M., et al., Comparable Plasma Lipid Changes in Patients with High-Grade Cervical Intraepithelial Neoplasia and Patients with Cervical Cancer. J Proteome Res, 2021. 20(1): p. 740-750. [CrossRef]
Figure 1.
Correlation between Netrin-1 and Ultrasound Blood Flow Parameters FI, VI, and VFI.
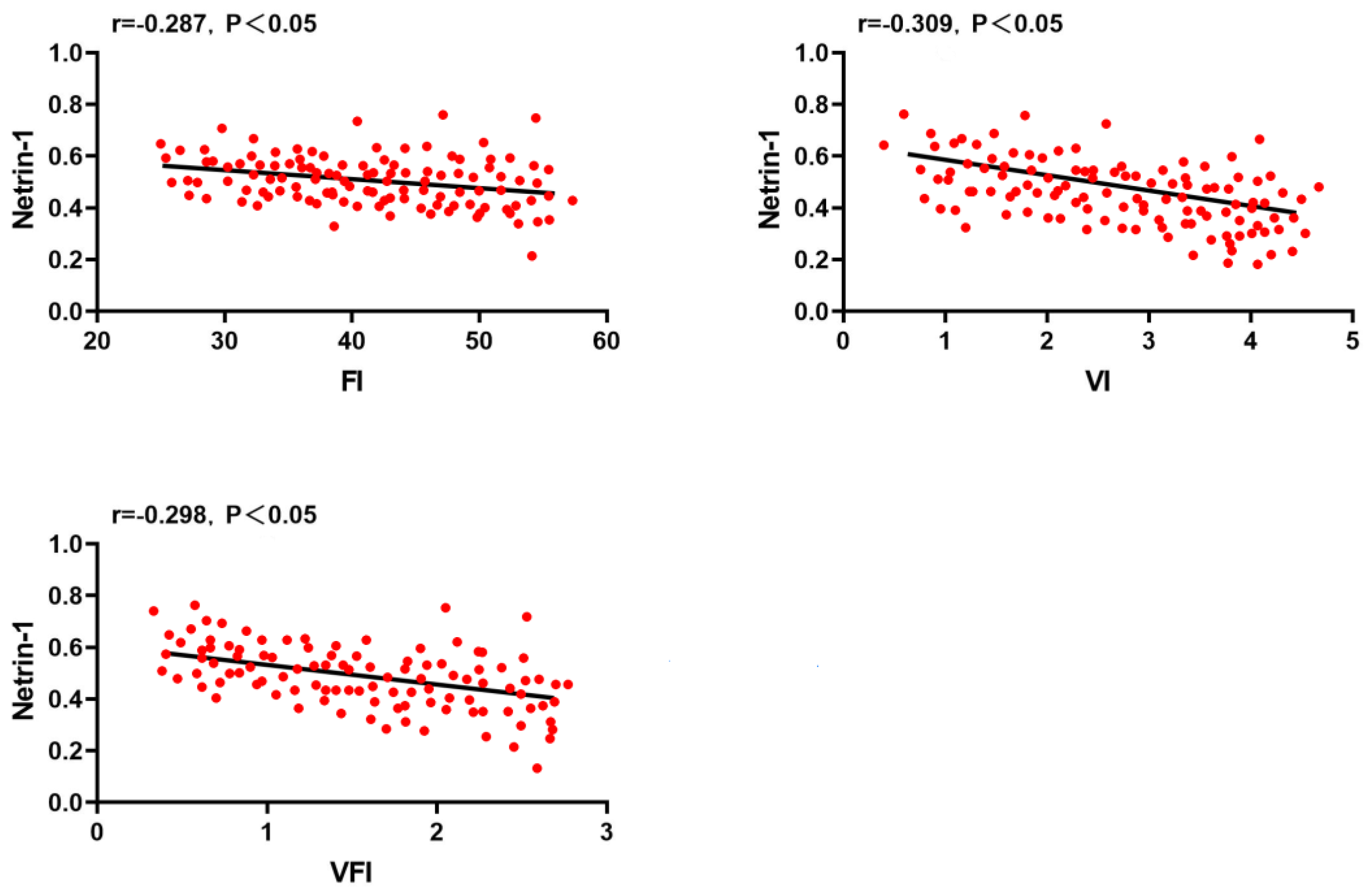
Figure 2.
ROC curves for predicting CIN Grade III lesions using different indicators. Note: A (Netrin-1); B (FI); C (VI); D (VFI).
Figure 2.
ROC curves for predicting CIN Grade III lesions using different indicators. Note: A (Netrin-1); B (FI); C (VI); D (VFI).
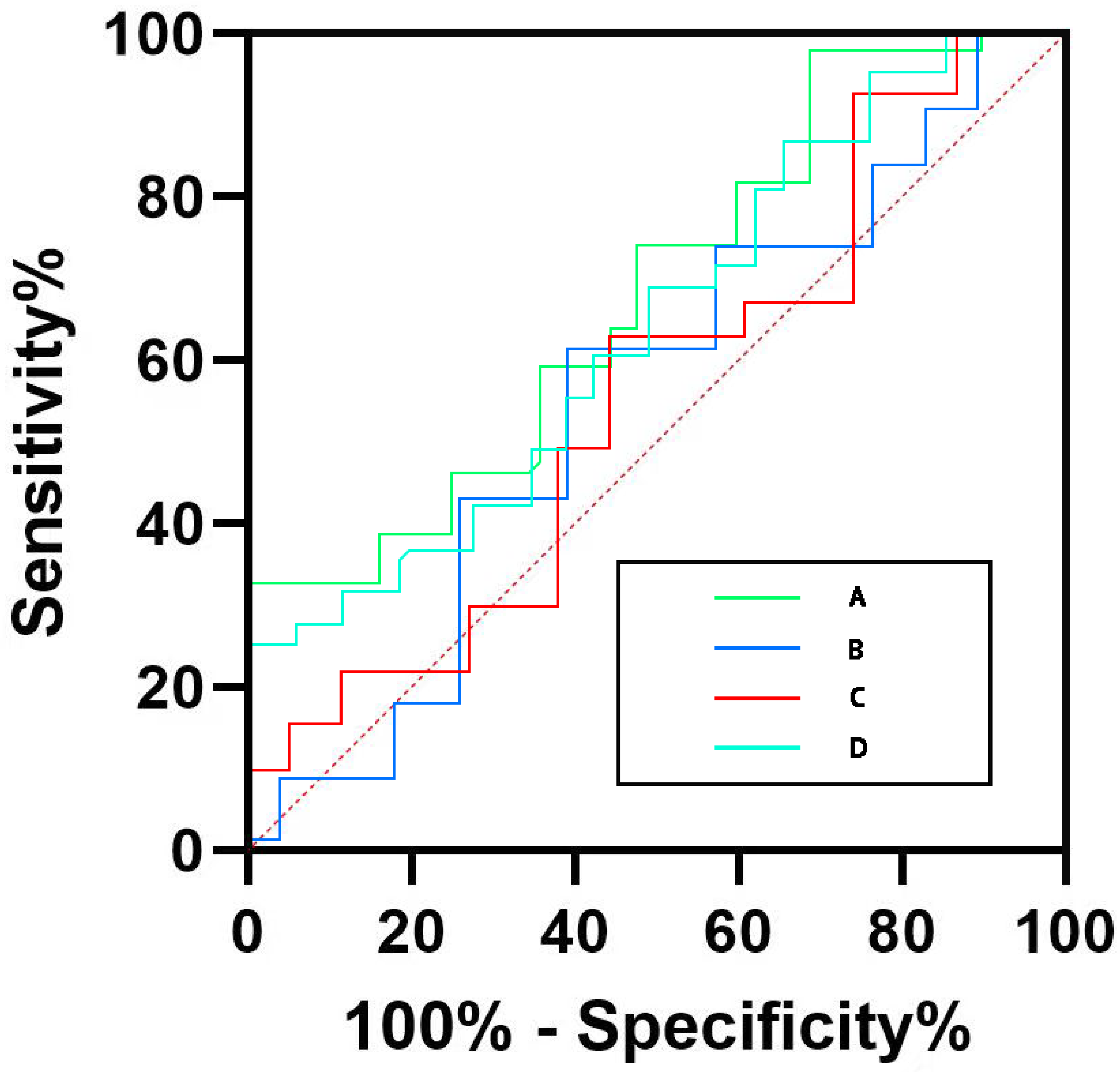

Table 1.
Primer Sequences.
| - | - | Primer Sequences |
|---|---|---|
| Netrin-l | Upstream | 5ˊ- AAGCCTATCACCCACCGGAAG - 3ˊ 3、 |
| Downstream | 5ˊ- GCGCCACAGGAATCTTGATGG | |
| β-actin | Upstream | 5ˊ- AGAGGGAAATCGTGCGTGAC |
| Downstream | 5ˊ- CAATCGTGACCTGGCCGT - 3ˊ |
Table 2.
Netrin-1 Fluorescence Quantitative PCR Expression Level and Immunohistochemical Staining Results [, n (%)].
Table 2.
Netrin-1 Fluorescence Quantitative PCR Expression Level and Immunohistochemical Staining Results [, n (%)].
| Group | n | Netrin-1 mRNA | Netrin-1 Protein Expression | |
| + | - | |||
| Control | 37 | 0.62±0.25 | 29 (78.38) | 8 (21.62) |
| Observation | 115 | 0.38±0.14a | 32 (27.83)a | 83 (72.17) |
| I | 42 | 0.47±0.13a | 18 (42.86)a | 24 (57.14) |
| II | 39 | 0.34±0.13ab | 10 (25.64)a | 29 (74.36) |
| III | 34 | 0.29±0.10ab | 4 (11.76)ab | 30 (88.24) |
Note: Compared with the control group, aP < 0.05; compared with the I group, bP < 0.05; compared with the II group, cP < 0.05.
Table 3.
Comparison of Ultrasound Blood Flow Parameters Levels in Patients with Different Degrees of Lesions ().
Table 3.
Comparison of Ultrasound Blood Flow Parameters Levels in Patients with Different Degrees of Lesions ().
| Group | n | FI (dB) | VI (%) | VFI (dB) |
| Control | 37 | 33.51±3.13 | 0.81±0.13 | 0.64±0.28 |
| Observation | 115 | 38.65±4.24a | 1.85±0.77a | 1.27±0.53a |
| I | 42 | 34.49±3.28 | 0.87±0.14 | 0.81±0.32 |
| II | 39 | 39.07±4.13ab | 1.73±0.65ab | 1.32±0.55ab |
| III | 34 | 43.59±5.22abc | 3.18±1.14abc | 1.78±0.60abc |
Note: Compared with the control group, aP < 0.05; compared with the I group, bP < 0.05; compared with the II group, cP < 0.05.
Table 4.
Analysis of Factors Affecting the Severity of CIN.
| Factor | β | S.E. | Wald X² | P | OR (95%CI) |
| Netrin-1 | 0.301 | 0.129 | 5.526 | 0.020 | 0.745 (0.574~0.957) |
| FI | 0.363 | 0.167 | 4.879 | 0.031 | 1.441 (1.038~1.976) |
| VI | 0.254 | 0.121 | 4.517 | 0.035 | 1.287 (1.023~1.625) |
| VFI | 0.356 | 0.133 | 12.569 | 0.011 | 1.423 (1.091~1.844) |
Table 5.
Predictive Value of Different Indicators for CIN Grade III Lesions.
| Indicator | AUC | 95%CI | Sensitivity (%) | Specificity (%) |
| Netrin-1 | 0.732 | 0.318~0.826 | 76.4 | 79.5 |
| FI | 0.676 | 0.549~0.931 | 70.9 | 74.5 |
| VI | 0.631 | 0.439~0.816 | 72.4 | 73.8 |
| VFI | 0.704 | 0.523~0.767 | 72.6 | 76.6 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



