
Submitted:
15 October 2024
Posted:
16 October 2024
You are already at the latest version
Abstract
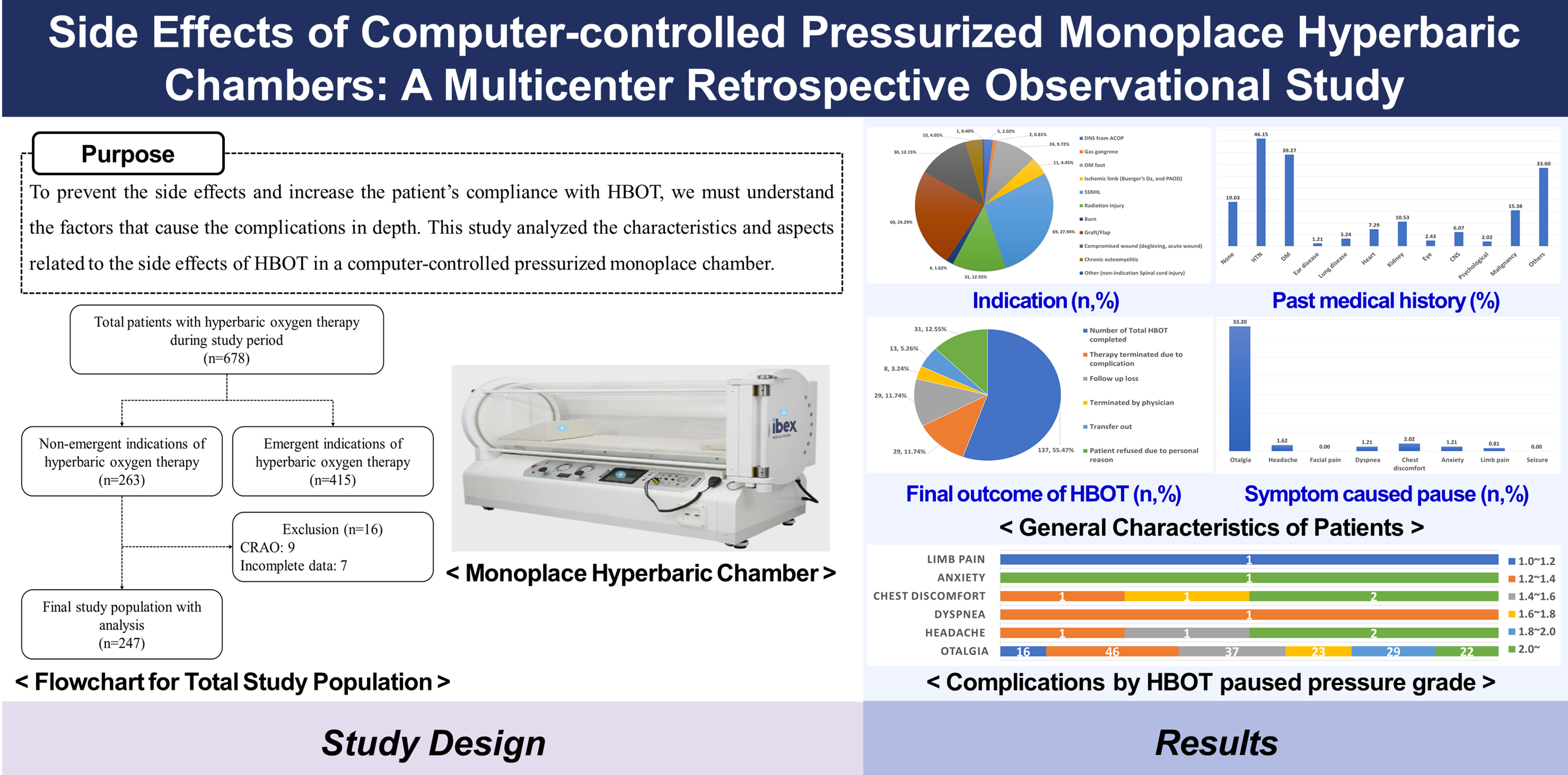
Hyperbaric oxygen therapy (HBOT) involves inhaling nearly 100% oxygen in a pressurized environment and is commonly used to treat various diseases and injuries. Despite its well-known safety, HBOT is associated with complications, with frequent middle ear barotrauma (MEB) and oxygen toxicity. Understanding the characteristics and risk factors associated with these complications is critical for improving patient’s compliance and treatment outcomes. This retrospective multicenter study aimed to analyze the characteristics and factors associated with complications during HBOT using a computer-controlled pressurized monoplace hyperbaric chamber. We conducted a retrospective observational study across two tertiary hospitals in Korea, involving patients who received HBOT from October 2017 to June 2020. Data were extracted from electronic medical records and hyperbaric chamber logs, including patient demographics, medical history, HBOT indications, and details of complications. Statistical analyses, including chi-square and t-tests, were used to compare variables. A total of 247 patients (mean age: 59.35 ± 15.05 years, 63.56% male) were included. The most common indications for HBOT were sudden sensorineural hearing loss (27.94%) and post-graft/flap (24.29%). Hypertension (46.15%) and diabetes mellitus (39.27%) were the most frequent comorbidities. Otalgia was the most prevalent side effect (33.20%), followed by chest discomfort (2.02%) and headache (1.62%). A significant proportion of patients (11.74%) terminated HBOT due to complications, with most pauses occurring at pressures between 1.2 to 1.4 ATA (26.67%). Complications, particularly otalgia, significantly impact patient compliance with HBOT. The incidence of complications varies by pressure level during treatment, suggesting the need for tailored strategies to minimize complications. This study highlights the importance of patient monitoring and education to improve the safety and efficacy of HBOT in monoplace chambers.
Keywords:
Hyperbaric oxygen therapy
; Complications
; Monoplace hyperbaric chamber
1. Introduction
Hyperbaric oxygen therapy (HBOT) requires inhaling near 100% oxygen in an elevated pressure environment above 1.4 atmospheres absolute (ATA) [1]. Most studies report that the effect of HBOT requires pressure between 2.0 ATA and 3.0 ATA to obtain the clinical benefit [2]. There are two kinds of hyperbaric chambers. A monoplace chamber treats one patient per session, and a multiplace chamber can treat two or more patients together [3]. In Korea, HBOT is applied to the indications that are approved by the Korean National Health Insurance Service, which are the following: acute carbon monoxide poisoning, gas embolism, central retinal artery occlusion, decompression sickness, acute cyanide poisoning, tissue necrosis after radiation therapy, diabetic foot ulcer, after flap or graft, after amputation surgery, sudden sensorineural hearing loss, peripheral artery occlusion diseases (including Buerger’s disease), thermal burn, refractory osteomyelitis, intracranial abscess, gas gangrene, and hemorrhagic anemia [4]. Emergent diseases, such as acute carbon monoxide poisoning, arterial gas embolism, and decompression sickness, need prompt HBOT and only screen for the absolute contraindications of HBOT [5]. For non-emergent diseases, such as diabetic foot ulcers, ischemic wounds, chronic osteomyelitis, and sudden sensorineural hearing loss (SSNHL), HBOT is recommended after thorough assessments and adequate patient education to prevent the complications [6]. HBOT is known to be safe compared to other therapies, and the incidence of complications is low [7]. Barotrauma and oxygen toxicity are possible complications of HBOT. During the treatment, barotrauma may occur when the compression starts to meet the therapeutic pressure [8].
Middle ear barotrauma (MEB) is the most common side effect of HBOT [9]. When pressure increases in the hyperbaric chamber, the tympanic membrane may be injured from the pressure difference. To prevent tympanic membrane injury, the Eustachian tube must be opened to equalize the inner and outer ear pressure [10]. According to previous studies, the incidence of MEB ranges from 8.9% to 65%, which depends on the skills of the hyperbaric chamber operator, the patient’s underlying conditions, and adequate patient education [11]. MEB may cause otalgic pain, decrease or loss of hearing, and rupture of the tympanic membrane [12]. The severity can be graded using the modified TEED scale and ranges from symptoms with no ontological signs (Grade 0) to a rupture of the tympanic membrane (Grade 5). If the injury is not severe, the tympanic membrane heals quickly with the pause of HBOT. The tympanic membrane may require weeks or months to recover, and permanent hearing loss may occur in severe cases. The incidence of sinus and pulmonary barotrauma is rare [13].
Compared to MEB, oxygen toxicity due to HBOT does not occur often. The most critical oxygen toxicity-related side effect involves the central nervous system (CNS) and a seizure. Oxygen toxicity may also involve complications on the eye and lungs, which recover by stopping oxygen breathing in most cases [14]. Dr. Hadanny and his colleagues retrospectively reviewed 2,334 patients who received HBOT from June 2010 to December 2014. Only one patient experienced oxygen toxicity-related seizures. Eight patients experienced myopia. The study only involved the patients who were treated in the multiplace chamber. In the multiplace chamber, two or more patients are treated together. Therefore, the rate and time required to increase the pressure in the chamber to the therapeutic range cannot be determined for individual patients [15].
The complications of HBOT may determine the patient’s compliance with the completion of the treatment [16]. The treatment protocol for HBOT may vary by institution and nation. However, the protocol requires a minimum of 90 minutes of staying in the hyperbaric chamber for repetitive treatment sessions, depending on the indication [17]. Thus, establishing a strategy to prevent complications is essential. To prevent the complications and increase the patient’s compliance with HBOT, we must understand the factors that cause the complications in depth. This study analyzed the characteristics and aspects related to the complications of HBOT in a computer-controlled pressurized monoplace chamber.
2. Materials and Methods
This retrospective multicenter observational study includes patients from two tertiary-care academic hospitals, including hyperbaric facilities, Wonju Severance Christian Hospital (Wonju, Republic of Korea) and Inha University Hospital (Incheon, Republic of Korea). We retrieved the electronic data of how each hyperbaric treatment proceeded in the computer-controlled pressurized monoplace chamber (IBEX M2, IBEX Medical Systems, Seoul, Korea). The data included a real-time recording of treated and paused time and pressure changes. We matched the electronic records from the chamber and the electronic medical records with the patient’s hospital identification number. The Institutional Review Board of Wonju Severance Christian Hospital approved our study protocol(approval number: CR320074) and registered with Korea’s Clinical Research Information Service (CRIS: KCT0005974). The informed consent was waived for this study because it is a retrospective and observational study, and we conducted the study procedures under the Helsinki Declaration. The patient records and information were anonymized before analysis.
The electronic medical records (EMR) included the following general characteristics: age, sex, HBOT indication, past medical history, including hypertension (HTN), diabetes mellitus (DM), otologic, pulmonary including asthma, chronic obstructive pulmonary disease (COPD), and pneumothorax, cardiovascular, renal, ophthalmic, cerebrovascular, psychological, and any malignant diseases, mental status at the initial treatment, and the outcome of completed HBOT session. From the EMR, we also collected the patient’s clinical characteristics associated with HBOT, including a symptom that caused to pause of the treatment, HBOT session outcome at the initial trial, pressure at which the HBOT session paused with time-paused in minutes, and pressure at which the HBOT session terminated.
We selected specific statistical methods depending on the properties of the variables. Mean and standard deviation or median and range are used for continuous variables. Frequency and percentage are used for categorical variables. A chi-square test was used to compare categorical variables, and two-sample t-tests or Mann-Whitney U tests were used to compare continuous variables. Normal distribution was analyzed using Student’s t-test. A p-value of <0.05 was considered statistically significant. We used SAS (version 9.4; SAS Institute, Inc., Cary, NC, USA) for all statistical analyses.
3. Results
3.1. Characteristics of Study Subjects
This multicenter retrospective registry-based observation study involved two tertiary university academic hospitals. Yonsei University Wonju Severance Christian Hospital (Wonju, Gangwon, Republic of Korea) included patients who received hyperbaric oxygen therapy (HBOT) from October 2016 to June 2020. Inha University Hospital (Incheon, Republic of Korea) included patients who received HBOT from October 2017 to June 2020. The total number of patients treated with HBOT in the monoplace chamber was 678, including 263 non-emergent indication patients. Among 263 cases, we excluded nine central retinal artery occlusion cases, with a specific treatment protocol requiring the pause during the compression time for vision check, and seven patients with incomplete data (Figure 1).
The general characteristics of the subjects were analyzed. The average age was 59.35±15.05. One hundred fifty-seven patients (63.56%) were male. SSNHL had sixty-nine cases (27.94%), the most frequent. Post-graft/flap was sixty patients (24.29%), and post-radiation therapy-induced tissue necrosis was thirty-one (12.55%), second and third in the order. Hypertension (114, 46.15%) was the most frequent past medical history, and diabetes mellitus (97, 39.27%) was the second. One hundred thirty-seven patients (55.47%) completed the planned number of HBOT from the initial diagnosis. Twenty-nine patients (11.74%) terminated the HBOT due to complications during the treatment. The most common side effect from the HBOT was otalgia (82, 33.20%). Other complications were chest discomfort (5, 2.02%), headache (4, 1.62%), dyspnea (3, 1.21%), anxiety (3, 1.21%), and limb pain (2, 0.81%). One hundred sixty-two patients (65.59%) completed the HBOT at initial treatment without pause, thirty-five patients (14.17%) had a pause during treatment, and fifty patients (20.24%) terminated the treatment (Table 1).
3.2. Demographic & Clinical Differences Between Groups by HBOT Pressure Grade
Among the initial trials, the most frequently paused pressure occurred in the 1.2 to 1.4 grade (48, 26.67%), and the median time for patients to pause compression during treatment was 3 [2-5] minutes after the starting treatment. The next most common stoppage occurred in the 1.4 to 1.6 grade (38, 21.11%) and the 1.8 to 2.0 grade (29, 16.11%) in that order. In addition, among the initial trials, the most frequently terminated pressure occurred above the 2.0 grade (15, 30.00%), and the median time for all patients to discontinue treatment was 1 [1-1] minute after starting treatment. The next most terminations occurred in the 1.4 to 1.6 grade (10, 20.00%) and the 1.8 to 2.0 grade (10, 20.00%) in that order. (Table 2).
3.3. Demographic & Clinical Differences Between Groups by HBOT Termination Pressure Grade
Demographic and clinical differences were analyzed for the group that completed treatment without intermediate termination and the group that was classified into three groups based on the pressure grade where treatment was completed (Table 3). There was a statistically significant difference in the proportion of SSNHL patients between groups (p=0.047). Additionally, there was a statistically significant difference between groups in patients who complained of otalgia, one of the complications (p<0.001).
3.4. Complications by HBOT Pressure Grade
Otalgia was the most common side effect across various pressure grades: 1.0 to 1.2 (16, 19.51%), 1.2 to 1.4 (46, 56.10%), 1.4 to 1.6 (37, 45.12%), 1.6 to 1.8 (23, 28.05%), 1.8 to 2.0 (29, 35.37%), and above 2.0 (22, 26.83%) (Table 4).
3.5. Demographic & Clinical Differences in the Otalgia Group
Significant differences were found in the proportion of compromised wound patients between groups that completed treatment without intermediate termination and groups divided into three pressure grades in middle age (p=0.013). Among patients who complained of otalgia, there was a significant difference among those with a history of brain disease (p=0.006) (Table 5).
4. Discussion
This study aimed to analyze the characteristics and factors related to the complications of HBOT in a computer-controlled pressurized monoplace chamber. HBOT patients were asked to stay in the monoplace chamber for 90 minutes, and their compliance with treatment completion was examined. We discuss the implications of these findings, focusing on the most common complications, their incidence, and the potential factors contributing to these outcomes.
Table 1 presented the general characteristics of patients treated with the monoplace chamber for non-emergent indications In this study, the most frequent indicator in patients who received HBOT was sudden sensorineural hearing loss (SSNHL). In 2012, the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) published treatment guidelines for SSNHL [18], revised in 2019. In these revised guidelines, HBOT was subdivided into ‘optional’ levels that can be combined with steroids as initial and salvage therapy [19]. Most of the patients had hypertension and diabetes mellitus in their past medical history. In addition, the most common complication from the HBOT was otalgia. This high incidence aligns with previous studies that reported that otalgia was a common side effect due to pressure changes in hyperbaric chambers [11]. Although there were no complications such as facial pain or seizures in this study, there were differences between this study and other previous studies. Skevas et al. reported that negative pressure gradients caused inflammation on the mucosal surface of the paranasal sinuses and bone cavities, compressing the paranasal space and causing congestion and edema, which was accompanied by facial pain, which was relieved when the pressure disappeared [20]. Seizure rarely occurs at typical clinical treatment pressures (2 ATA to 3 ATA) and is difficult to predict individually. Heyboer 3rd et al. reported that seizure incidence is approximately 1 in about 2,000 treatments [21], and Hadanny et al. also reported a low incidence of seizures in multiplace chambers [15].
Table 2 indicates the distribution of treatment pauses and terminations across different pressure grades, which provided valuable information. Most pauses occurred in the 1.2 to 1.4 ATA range, with a median pause time of 3 minutes. Terminations were more frequent at pressures above 2.0 ATA. Gill and Bell noted that not all patients respond similarly to the same pressure, so an individualized treatment approach is more important than adjusting protocols based on generalized data [22]. Understanding these pressure-related trends can guide modifications in HBOT protocols to minimize complications and improve patient outcomes.
Table 3 highlighted demographic and clinical differences between groups based on the pressure at which treatment was paused or terminated. For instance, SSNHL patients showed a statistically significant difference in treatment outcomes, particularly at higher pressures (above the 2.0 grade). Hadanny et al. reported that it was particularly critical given that the median pause time in the 1.2 to 1.4 ATA range was manageable. However, higher pressures above 2.0 ATA correlate with more frequent treatment terminations due to complications [23]. Additionally, Rozbicki et al. emphasized the importance of timely initiation and careful pressure management in improving hearing outcomes in patients with SSNHL, noting that higher pressures are often associated with increased complications, including barotrauma and oxygen toxicity [24]. This finding may suggest that SSNHL patients are more susceptible to pressure-related complications, necessitating tailored protocols for this subgroup.
Moreover, patients' compliance with HBOT is significantly influenced by the occurrence of complications. Table 4 describes complications according to HBOT pressure grade; otalgia was the most common side effect of treatment pauses or termination across various pressure grades. The most common reason for otalgia would be considered to be due to failure in equalizing. Hwang et al. proposed the developed algorithm, which determined and equalized the unbalanced pressure of a subject based on their tympanic admittance and was evaluated in conjunction with conventional HBOT in an experiment involving 100 subjects [25]. Even if treatment was paused at a pressure level of 2.0 or higher, the possibility of undiagnosed claustrophobia or panic attacks might be presumed to be the cause of headache complaints. Miller et al. noted that claustrophobia might be managed with coaching and anxiolytic medications, and intolerance of a monoplace chamber may warrant referral to the closest multiplace chamber facility [26]. Managing and mitigating these complications could be essential to increase patient compliance and complete HBOT sessions.
5. Conclusions
This study underscores the importance of recognizing and addressing the complications associated with HBOT in monoplace chambers. Middle ear barotrauma is the most prevalent complication, highlighting the need for effective pressure equalization techniques and patient education. While oxygen toxicity is rare, monitoring remains critical. Tailoring HBOT protocols based on patient demographics and clinical characteristics, especially for conditions like SSNHL, can enhance treatment safety and efficacy. Future studies should focus on preventive strategies and protocol optimization to reduce complications and improve patient adherence to HBOT.
Author Contributions
Conceptualization, Y.-S.L.; methodology, J.-H.P. and Y.-S.L.; validation, S.K.; formal analysis, H.-Y.L., S.K. and Y.-S.L.; investigation, J.-H.P., T.-K.A., Y.-H.S., and Y.-S.C..; data curation, S.K., T.-K.A., Y.-H.S., H.K., and Y.-S.C.; writing—original draft preparation, H.-Y.L. and S.K.; writing—review and editing, H.-Y.L. and Y.-S.L.; project administration, J.-H.P., H.K., and Y.-S.L.; funding acquisition, H.K.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was carried out with approval from the Research Ethics Committee of Yonsei University Wonju Severance Christian Hospital (IRB approval number: CR320074) and registered with the Clinical Research Information Service (CRIS) operated by the Korea Disease Control and Prevention Agency (CRIS trial registration number: KCT0005974).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.
Acknowledgments
We thank the medical staff for managing the treatment of patients receiving hyperbaric oxygen therapy.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Jain, K.K.; Baydin, S.A. Textbook of hyperbaric medicine, 6th ed.; Springer; 2017.
- Mathieu, D.; Marroni, A.; Kot, J. Tenth European Consensus Conference on Hyperbaric Medicine: recommendations for accepted and non-accepted clinical indications and practice of hyperbaric oxygen treatment. Diving Hyperb Med, 2017, 47(1), 24-32.
- Moon, R.E.; Bakker, D.; Barnes, R.; Bennett, M.; Camporesi, E.; Cianci, P. Hyperbaric oxygen therapy indications. 14th ed.; North Palm Beach: Best Publishing Company, FL, USA, 2017.
- Lee, S.M.; Heo, T.; Kim, K.W.; Kim, H. Current status and development direction of hyperbaric medicine in Korea. J Korean Med Assoc, 2022, 65(4), 232-238. [CrossRef]
- Weaver, L.K.; Hopkins, R.O.; Chan, K.J.; Churchill, S.; Elliott, C.G.; Clemmer, T.P.; Orme, J.F.Jr.; Thomas, F.O.; Morris, A.H. Hyperbaric oxygen for acute carbon monoxide poisoning. New Engl J Med, 2002, 347(14), 1057-1067. [CrossRef]
- Hart, G.B. Indications and contraindications for hyperbaric-oxygen therapy. J Am Med Assoc, 1976, 236(16), 1892-1892.
- Klingmann, C.; Gonnermann, A.; Dreyhaupt, J.; Vent, J.; Praetorius, M.; Plinkert, P.K. Decompression illness reported in a survey of 429 recreational divers. Aviat Space Environ Med, 2008, 79(2), 123-128. [CrossRef]
- Tibbles, P.M.; Edelsberg, J.S. Hyperbaric-oxygen therapy. New Engl J Med, 1996, 334(25), 1642-1648.
- Vahidova, D.; Sen, P.; Papesch, M.; Zein-Sanchez, M.P.; Mueller, P.H.J. Does the slow compression technique of hyperbaric oxygen therapy decrease the incidence of middle-ear barotrauma?. J Laryngol Otol, 2006, 120(6), 446-449. [CrossRef]
- Miyazawa, T.; Ueda, H.; Yanagita, N. Eustachian tube function and middle ear barotrauma associated with extremes in atmospheric pressure. Ann Otol Rhinol Laryngol Suppl, 1996, 105(11), 887-892. [CrossRef]
- Yamamoto, Y.; Noguchi, Y.; Enomoto, M.; Yagishita, K.; Kitamura, K. Otological complications associated with hyperbaric oxygen therapy. Eur Arch Otorhinolaryngol Suppl, 2016, 273, 2487-2493. [CrossRef]
- Becker, G.D.; Parell, G.J. Barotrauma of the ears and sinuses after scuba diving. Eur Arch Otorhinolaryngol Suppl, 2001, 258, 159-163. [CrossRef]
- O'Neill, O.J.; Weitzner, E.D. The O'Neill grading system for evaluation of the tympanic membrane: A practical approach for clinical hyperbaric patients. Undersea Hyperb Med, 2015, 42(3).
- Skeik, N.; Porten, B.R.; Isaacson, E.; Seong, J.; Klosterman, D.L.; Garberich, R.F.; Alexander, J.Q.; Rizvi, A.; Manunga J.M.Jr.; Cragg, A.; Graber, J.; Alden, P., Sullivan, T. Hyperbaric oxygen treatment outcome for different indications from a single center. Ann Vasc Surg, 2015, 29(2), 206-214. [CrossRef]
- Hadanny, A.; Meir, O.; Bechor, Y.; Fishlev, G.; Bergan, J.; Efrati, S. Seizures during hyperbaric oxygen therapy: retrospective analysis of 62,614 treatment sessions. Undersea Hyperb Med, 2016, 43(1).
- Zhang, Y.; Zhou, Y.; Jia, Y.; Wang, T.; Meng, D. Adverse effects of hyperbaric oxygen therapy: a systematic review and meta-analysis. Front Med, 2023, 10, 1160774. [CrossRef]
- Mathieu, D. (Ed.). Handbook on hyperbaric medicine. Springer, Dordrecht, The Netherlands, Springer, 2006; p. 812.
- Stachler, R.J.; Chandrasekhar, S.S.; Archer, S.M.; Rosenfeld, R.M.; Schwartz, S.R.; Barrs, D.M.; Brown, S.R.; Fife, T.D.; Ford, P., Ganiats, T.G.; Hollingsworth, D.B.; Lewandowski, C.A., Montano, J.J.; Saunders, J.E.; Tucci, D.L.; Valente, M.; Warren, B.E.; Yarechuk, K.L.; Robertson, P.J. Clinical practice guideline: sudden hearing loss. Otolaryngol Head Neck Surg, 2012, 146(3_suppl), S1-S35.
- Chandrasekhar, S.S.; Tsai Do, B.S.; Schwartz, S.R.; Bontempo, L.J.; Faucett, E.A.; Finestone, S.A.; Hollingsworth, D.B.; Kelly, D.M.; Kmucha, S.T.; Moonis, G.; Poling, G.L.; Roberts, J.K.; Stachler, R.J.; Zeiter, D.M.; Corrigan, M.D., Nnacheta, L.C.; Satterfield, L. Clinical practice guideline: sudden hearing loss (update). Otolaryngol Head Neck Surg, 2019, 161(1_suppl), S1-S45.
- Skevas, T.; Baumann, I.; Bruckner, T.; Clifton, N.; Plinkert, P.K.; Klingmann, C. Medical and surgical treatment in divers with chronic rhinosinusitis and paranasal sinus barotrauma. Eur Arch Otorhinolaryngol Suppl, 2012, 269, 853-860. [CrossRef]
- Heyboer 3rd, M.; Jennings, S.; Grant, W.D.; Ojevwe, C.; Byrne, J.; Wojcik, S.M. Seizure incidence by treatment pressure in patients undergoing hyperbaric oxygen therapy. Undersea Hyperb Med, 2014, 41(5), 379-385.
- Gill, A.Á.; Bell, C.N. Hyperbaric oxygen: its uses, mechanisms of action and outcomes. QJM, 2004, 97(7), 385-395. [CrossRef]
- Hadanny, A.; Abbott, S.; Suzin, G.; Bechor, Y.; Efrati, S. Effect of hyperbaric oxygen therapy on chronic neurocognitive deficits of post-traumatic brain injury patients: retrospective analysis. BMJ open, 2018, 8(9), e023387. [CrossRef]
- Rozbicki, P.; Usowski, J.; Krzywdzińska, S.; Jurkiewicz, D.; Siewiera, J. Assessing the Effectiveness of Different Hyperbaric Oxygen Treatment Methods in Patients with Sudden Sensorineural Hearing Loss. Audiol Res, 2024, 14(2), 333-341. [CrossRef]
- Hwang, L.; Song, M.; Lee, Y.; Shin, T.M. Methods for preventing middle ear barotrauma in computer-controlled pressurization of monoplace hyperbaric chambers. Undersea Hyperb Med, 2019, 46(2). [CrossRef]
- Miller, R.S.; Weaver, L.K.; Bahraini, N.; Churchill, S.; Price, R.C.; Skiba, V.; Caviness, J.; Mooney, S.; Hetzell, B.; Liu, J.; Deru, K.; Ricciardi, R.; Francisco, S.; Close, N.C.; Surrett, G.W.; Bartos, C.; Margaret, R.; Brenner, L.A.; HOPPS Trial Team. Effects of hyperbaric oxygen on symptoms and quality of life among service members with persistent postconcussion symptoms: a randomized clinical trial. JAMA Intern Med, 2015, 175(1), 43-52.
Figure 1.
Flowchart for the total study population.


Table 1.
General characteristics of patients treated with monoplace chamber for non-emergent indications.
Table 1.
General characteristics of patients treated with monoplace chamber for non-emergent indications.
| Variables | Total patients (n=247) |
|---|---|
| Age, yr (M±S.D) | 59.35±15.05 |
| Male, n(%) | 157 (63.56) |
| Indication | |
| DNS from ACOP | 5 (2.02) |
| Gas gangrene | 2 (0.81) |
| DM foot | 24 (9.72) |
| Ischemic limb (Buerger’s Dz, and PAOD) | 11 (4.45) |
| SSNHL | 69 (27.94) |
| Radiation injury | 31 (12.55) |
| Burn | 4 (1.62) |
| Graft/Flap | 60 (24.29) |
| Compromised wound (degloving, acute wound) | 30 (12.15) |
| Chronic osteomyelitis | 10 (4.05) |
| Other (non-indication Spinal cord injury) | 1 (0.40) |
| Past Medical Hx., n(%) | |
| None | 47 (19.03) |
| HTN | 114 (46.15) |
| DM | 97 (39.27) |
| Ear disease | 3 (1.21) |
| Lung (asthma, COPD, Pneumothorax) | 8 (3.24) |
| Heart | 18 (7.29) |
| Kidney | 26 (10.53) |
| Eye | 6 (2.43) |
| CNS | 15 (6.07) |
| Psychological | 5 (2.02) |
| Malignancy | 38 (15.38) |
| Others | 83 (33.20) |
| Mental Status, n(%) | |
| Alert | 242 (97.98) |
| Verbal | 5 (2.02) |
| Final outcome of completed HBOT session, n(%) | |
| Number of Total HBOT completed | 137 (55.47) |
| Therapy terminated due to complication | 29 (11.74) |
| Follow up loss | 29 (11.74) |
| Terminated by physician | 8 (3.24) |
| Transfer out | 13 (5.26) |
| Patient refused due to personal reason | 31 (12.55) |
| Symptom caused treatment pause | |
| Otalgia | 82 (33.20) |
| Headache | 4 (1.62) |
| Facial pain | - |
| Dyspnea | 3 (1.21) |
| Chest discomfort | 5 (2.02) |
| Anxiety | 3 (1.21) |
| Limb pain | 2 (0.81) |
| Seizure | - |
| HBOT outcome at initial treatment | |
| Completed without pause | 162 (65.59) |
| Completed with pause | 35 (14.17) |
| Treatment terminated | 50 (20.24) |
* M – mean, S.D – standard deviation, DNS - delayed neuropsychiatric sequelae, ACOP - acute carbon monoxide poisoning, DM – diabetes mellitus, Dz – disease, PAOD - peripheral arterial disease, SSNHL - sudden sensorineural hearing loss, HBOT – hyperbaric oxygen therapy, Hx. – history, HTN – hypertension, COPD – chronic obstructive pulmonary disease, CNS - central nervous system.
Table 2.
Distribution of the delayed treatment time by paused or terminated pressure.
| Pressure (kPa) |
Frequency (n, %) |
Delayed treatment time (minute) | |||
|---|---|---|---|---|---|
| Minimum | Maximum | Median [IQR] | |||
| Treatment paused pressure (n=180) |
1.0~1.2 | 17 (9.44) | 1 | 8 | 2 [1-3] |
| 1.2~1.4 | 48 (26.67) | 1 | 15 | 3 [2-5] | |
| 1.4~1.6 | 38 (21.11) | 1 | 13 | 2 [1-4] | |
| 1.6~1.8 | 23 (12.78) | 1 | 14 | 1 [1-2] | |
| 1.8~2.0 | 29 (16.11) | 1 | 7 | 2 [1-2] | |
| 2.0~ | 25 (13.89) | 1 | 10 | 3 [2-5] | |
| Treatment terminated pressure (n=50) |
1.0~1.2 | 1 (2.00) | 1 | 1 | 1 [1-1] |
| 1.2~1.4 | 9 (18.00) | 1 | 9 | 2 [1-4] | |
| 1.4~1.6 | 10 (20.00) | 1 | 4 | 1 [1-1] | |
| 1.6~1.8 | 5 (10.00) | 1 | 1 | 2 [1-2] | |
| 1.8~2.0 | 10 (20.00) | 1 | 4 | 3 [2-7] | |
| 2.0~ | 15 (30.00) | 1 | 9 | 1 [1-1] | |
* Available for several responses in each pressure section
Table 3.
Clinical difference between groups by HBOT termination pressure grade
| Variables | Pressure grade | p-value | |||
|---|---|---|---|---|---|
| No terminated (n=197) |
1.0~1.2 (n=1) |
1.2~2.0 (n=34) |
2.0~ (n=15) |
||
| Age, yr [IQR] | 60 [47-70] | 64 [64-64] | 61.5 [54-72] | 61 [53-69] | 0.868 |
| Male, n(%) | 129 (65.48) | 0 | 20(58.82) | 8 (53.33) | 0.345 |
| Indication, n(%) | |||||
| DNS from ACOP | 4 (2.03) | 0 | 1 (2.94) | 0 | 0.681 |
| Gas gangrene | 2 (1.02) | 0 | 0 | 0 | 1.000 |
| DM foot | 21 (10.66) | 0 | 3 (8.82) | 0 | 0.629 |
| Ischemic limb | 10 (5.08) | 0 | 1 (2.94) | 0 | 1.000 |
| SSNHL | 51 (25.89) | 1(100.00) | 9 (26.47) | 8 (53.33) | 0.047* |
| Radiation injury | 27 (13.71) | 0 | 3 (8.82) | 1 (6.67) | 0.738 |
| Burn | 3 (1.52) | 0 | 0 | 1 (6.67) | 0.316 |
| Graft/Flap | 47 (22.22) | 0 | 9 (26.47) | 4 (26.67) | 0.911 |
| Compromised wound | 24 (12.18) | 0 | 6 (17.65) | 0 | 0.337 |
| Chronic osteomyelitis | 8 (4.06) | 0 | 1 (2.94) | 1 (6.67) | 0.679 |
| Other | 0 | 0 | 1 (2.94) | 0 | 0.202 |
| Past Medical Hx., n(%) | |||||
| None | 38 (19.29) | 0 | 5 (14.71) | 4 (26.67) | 0.680 |
| HTN | 91 (46.19) | 1 (100.00) | 18 (52.94) | 4 (26.67) | 0.462 |
| DM | 83 (42.13) | 0 | 11 (32.35) | 3 (20.00) | 0.203 |
| Ear disease | 2 (1.02) | 0 | 1 (2.94) | 0 | 0.494 |
| Lung | 6 (3.05) | 0 | 2 (5.88) | 0 | 0.613 |
| Heart | 14 (7.11) | 0 | 3 (8.82) | 1 (6.67) | 0.900 |
| Kidney | 22 (11.17) | 0 | 3 (8.82) | 1 (6.67) | 1.000 |
| Eye | 6 (3.05) | 0 | 0 | 0 | 0.731 |
| Brain | 10 (5.08) | 0 | 5 (14.71) | 0 | 0.161 |
| Psychological | 4 (2.03) | 0 | 1 (2.94) | 0 | 0.681 |
| Maignancy | 34 (17.26) | 0 | 3 (8.82) | 1 (6.67) | 0.476 |
| Others | 62 (31.47) | 0 | 14 (41.18) | 6 (40.00) | 0.568 |
| Complication, n(%) | |||||
| Otalgia | 32 (16.24) | 1 (100.00) | 33 (97.06) | 15 (100.0) | <0.001*** |
| Headache | 3 (1.52) | 0 | 1 (2.94) | 0 | 0.598 |
| Dyspnea | 3 (1.52) | 0 | 0 | 0 | 1.000 |
| Chest discomfort | 3 (1.52) | 0 | 0 | 0 | 1.000 |
| Anxiety | 3 (1.52) | 0 | 0 | 0 | 1.000 |
| Limb pain | 2 (1.02) | 0 | 0 | 0 | 1.000 |
* p<0.05,** p<0.01,***p<0.001, * IQR – interquartile range, DNS - delayed neuropsychiatric sequelae, ACOP - acute carbon monoxide poisoning, DM – diabetes mellitus, SSNHL - sudden sensorineural hearing loss, Hx. – history, HTN – hypertension.
Table 4.
Complications by HBOT pressure grade.
| Symptom caused treatment pause | Treatment paused pressure (kPa) | ||||||
|---|---|---|---|---|---|---|---|
| 1.0~1.2 | 1.2~1.4 | 1.4~1.6 | 1.6~1.8 | 1.8~2.0 | 2.0~ | ||
| Otalgia (n=82) |
n,% | 16 (19.51) | 46 (56.10) | 37 (45.12) | 23 (28.05) | 29 (35.37) | 22 (26.83) |
| p-value | <0.001*** | <0.001*** | <0.001*** | <0.001*** | <0.001*** | <0.001*** | |
| Headache (n=4) |
n,% | 0 | 1 (25.00) | 1 (25.00) | 0 | 0 | 2 (50.00) |
| p-value | 1.000 | 0.581 | 0.490 | 1.000 | 1.000 | 0.052 | |
| Dyspnea (n=3) |
n,% | 0 | 1 (33.33) | 0 | 0 | 0 | 0 |
| p-value | 1.000 | 0.479 | 1.000 | 1.000 | 1.000 | 1.000 | |
| Chest discomfort (n=5) |
n,% | 0 | 1 (20.00) | 0 | 1 (20.00) | 0 | 2 (40.00) |
| p-value | 1.000 | 1.000 | 1.000 | 0.389 | 1.000 | 0.081 | |
| Anxiety (n=3) |
n,% | 0 | 0 | 0 | 0 | 0 | 1 (33.33) |
| p-value | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | 0.275 | |
| Limb pain (n=2) |
n,% | 1 (50.00) | 0 | 0 | 0 | 0 | 0 |
| p-value | 0.133 | 1.000 | 1.000 | 1.000 | 1.000 | 1.000 | |
* p<0.05,** p<0.01,***p<0.001.
Table 5.
Demographic & clinical differences in the otalgia group by HBOT termination pressure grade in the otalgia group.
Table 5.
Demographic & clinical differences in the otalgia group by HBOT termination pressure grade in the otalgia group.
| Variables | Pressure grade | p-value | ||||||
|---|---|---|---|---|---|---|---|---|
| No terminated (n=32) |
1.0~1.2 (n=1) |
1.2~1.4 (n=9) |
1.4~1.6 (n=10) |
1.6~1.8 (n=5) |
1.8~2.0 (n=10) |
2.0~ (n=10) |
||
| Age, yr [IQR] | 59.5 [56.5~71.5] |
64 [64-64] |
57 [48~76] |
59 [53~62] |
63 [62~68] |
64 [56~73] |
61 [53~69] |
0.861 |
| Male, n(%) | 17 (53.13) | 0 | 5(55.56) | 7 (70.00) | 3 (60.00) | 5 (50.00) | 8 (53.33) | 0.943 |
| Indication, n(%) | ||||||||
| DNS from ACOP | 3 (9.38) | 0 | 0 | 0 | 0 | 1(10) | 0 | 0.804 |
| Gas gangrene | 0 | 0 | 0 | 0 | - | |||
| DM foot | 6 (18.75) | 0 | 0 | 0 | 1 (20.00) | 2((20) | 0 | 0.219 |
| Ischemic limb | 1 (3.13) | 0 | 0 | 1 | 0 | 0 | 0 | 0.706 |
| SSNHL | 7 (21.88) | 1 (100.00) | 2 (22.22) | 3 (30.00) | 1 (20.00) | 3(30) | 8(53.33) | 0.288 |
| Radiation injury | 3 (9.38) | 0 | 0 | 2 (20.00) | 0 | 1(10) | 1(15) | 0.853 |
| Burn | 0 | 0 | 0 | 0 | 0 | 0 | 1(6.67) | 0.610 |
| Graft/Flap | 10 (31.25) | 0 | 5 (55.56) | 2 (20.00) | 0 | 2(20) | 4(26.67) | 0.445 |
| Compromised wound | 2 (6.25) | 0 | 1 | 2 (20.00) | 3 (60.00) | 0 | 0 | 0.013* |
| Chronic osteomyelitis | 0 | 0 | 1 (11.11) | 0 | 0 | 0 | 1(6.67) | 0.288 |
| Other | 0 | 0 | 0 | 0 | 0 | 1(10) | 0 | 0.427 |
| Past Medical Hx., n(%) | ||||||||
| None | 3 (9.38) | 0 | 1 (11.11) | 2 (20.00) | 1 (20.00) | 1(10) | 4(26.67) | 0.684 |
| HTN | 19 (59.38) | 1 (100.00) | 6 (66.67) | 4 (40.00) | 3 (60.00) | 5(50) | 4(26.67) | 0.313 |
| DM | 19 (59.38) | 0 | 2 (22.22) | 2 (20.00) | 3 (60.00) | 4(40) | 3(20) | 0.055 |
| Ear disease | 0 | 0 | 0 | 0 | 0 | 1(10) | 0 | 0.427 |
| Lung | 0 | 0 | 1 (11.11) | 1 (10.00) | 0 | 0 | 0 | 0.186 |
| Heart | 5 (15.63) | 0 | 0 | 1 (10.00) | 2 (40.00) | 0 | 1(6.67) | 0.307 |
| Kidney | 7 (21.88) | 0 | 0 | 1 (10.00) | 2 (40.00) | 0 | 1(6.67) | 0.213 |
| Eye | 2 (6.25) | 0 | 0 | 0 | 0 | 0 | 0 | 1.000 |
| Brain | 0 | 0 | 1 (11.11) | 2 (20.00) | 2 (40.00) | 0 | 0 | 0.006** |
| Psychological | 0 | 0 | 0 | 0 | 0 | 1(10) | 0 | 0.427 |
| Maignancy | 5 (15.63) | 0 | 0 | 2 (20.00) | 0 | 1(10) | 1(6.67) | 0.822 |
| Others | 13 (40.63) | 0 | 3 (33.33) | 5 (50.00) | 2 (40.00) | 4(40) | 6(40) | 0.995 |
* p<0.05,** p<0.01,***p<0.001, * IQR – interquartile range, DNS - delayed neuropsychiatric sequelae, ACOP - acute carbon monoxide poisoning, DM – diabetes mellitus, SSNHL - sudden sensorineural hearing loss, Hx. – history, HTN – hypertension.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



