
Submitted:
17 October 2024
Posted:
18 October 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Influenza behavior depends on several characteristics: the agent itself, the host response, and environmental changes that determine seasonality, presentation, disease severity, lethality, and intensity of contagion. Vulnerable populations, such as the elderly, people with underlying diseases, and incomplete vaccination status, can influence disease presentation and epidemiology. These information changes are necessary for existing surveillance systems. Special surveillance of human and animal diseases is necessary, considering recent outbreaks and epidemic waves of viral diseases such as avian influenza. This study analyzed the impact of the COVID-19 pandemic on influenza vaccination coverage in Mexico and Central America. We used existing data and information in the countries and what was reported to WHO and UNICEF on administrative coverage of influenza vaccination reported by the countries, and the PAHO surveillance databases for influenza and other respiratory viruses. Influenza vaccine application varies in Central American countries and Mexico. Vaccination schedules have been adapted following WHO and PAHO recommendations, and considering the epidemiological, organizational conditions and financial realities of each country. Surveillance systems must be prepared for a possible “tridemic” in humans involving influenza, SARS-CoV-2 and respiratory syncytial virus (RSV). Influenza-associated disease was considerably affected during the COVID-19 pandemic. Given the preventive measures implemented, cases were unusually low during 2021-22, but cases increased sharply in 2022-23 caused by influenza A and influenza A H1N1 pdm09, with some isolated cases of influenza B.
Keywords:
immunization
; influenza
; influenza vaccine
; Central America
1. Introduction
Vaccination during the COVID-19 pandemic was negatively impacted in most countries, however, influenza vaccination, their policies and reporting systems were relevant due to fear of having the SARS-CoV2 and influenza run together. The Global Health Consortium, Global Health Department, Robert Stempel College of Public Health & Social Work, Florida International University, commissioned a series of four studies to analyze the impact of the COVID-19 pandemic on influenza vaccination coverage in Latin America focusing on Mexico and Central America, the Andean Region, the Southern Cone, and Brazil. The studies were presented at a seminar with immunization and influenza experts in mid-2023.
During the COVID-19 pandemic between 2020-21, the number of cases, hospitalizations, and deaths caused by influenza dropped considerably. This phenomenon was attributed to social isolation and strict preventive measurements implemented around the world [1] and continued during the second year of the pandemic. Underreport of morbidity and mortality associated with influenza has also been mentioned as a possible cause of this finding, nevertheless, several studies have demonstrated a real decrease in cases and deaths in the Americas and around the world, even though vaccination coverage was considerably impacted.
In Central America and Mexico, there was an effort to propel influenza vaccination during the pandemic to avoid an unnecessary demand for health services in case influenza disease increased simultaneously.
A technical advisory group on vaccine preventable diseases developed in July 202 [2] reviewed several documents on the advantages of influenza vaccination during the pandemic. These papers documented a possible protection of influenza vaccination against COVID-19 cases, and a positive effect in the elderly population, rates of hospitalization, prolonged hospital admissions, mechanical ventilation, intensive care need, and mortality when influenza vaccine was received close to SARS-CoV-2 disease.
Nevertheless, a decrease in the application of most biologics used rutinary in every country, including influenza vaccine, was documented in those years [1]. Implemented measures, temporary closure of vaccination centers, lack of transportation, fewer supplies, and even fear among population were among the mentioned causes [3].
2. Materials and Methods
In this report, we sought to analyze the impact of the COVID-19 pandemic on influenza vaccination coverage in Latin America, specifically in Central America and Mexico. The countries included in the research were: Belize, Costa Rica, El Salvador, Guatemala, Honduras, Mexico, Nicaragua, Panama.
The information analyzed corresponded to administrative coverage of influenza vaccination in the countries included in the study, during the years 2017 to 2023. These sources used corresponded to those officially reported by PAHO/WHO/UNICEF, corresponding to vaccination coverage and case reporting for the surveillance of influenza viruses and other respiratory viruses in the Americas.
3. Results
3.1. Possible Causes Affecting Influenza Immunization During the COVID-19 Pandemic
Respiratory viruses causing infection differ in genomic structure, severity, temporality, transmissibility, clinical symptoms, transmission, and susceptible populations [4]. Influenza virus is responsible for close to 36,500 deaths and 400,000 hospitalizations in Latin America and the Caribbean per year [1]. The SARS-CoV-2 emergency in 2020 lead national governments to implement a series of non-pharmacological strategies designed to generate social distancing, improve hand hygiene, and separation with the use of face masks. These measurements generated a reduction of influenza related cases and hospitalizations in North America, Central America, and the Caribbean [1,5,6] during the 2019-20 and 2020-21 seasons in the North Hemisphere, and 2021 in the Southern region.
The effectiveness of non-pharmacological measures to avoid transmission of disease depends on the characteristics of each virus [4]. Both coronavirus and influenza have similar methods of transmission, including direct contact, contact with contaminated surfaces, aerosol in case of COVID-19, and droplets (Table 1).
Decrease in influenza cases during the pandemic have also been associated with displacement of respiratory viruses from their ecological niche due to circulation of SARS-CoV-2. Before 2020, influenza and rhinovirus were the most common circulating viruses. During the first wave of SARS-CoV-2, dynamics changed, and rhinovirus became the most common virus [7]. Rhinovirus can coexist with other respiratory viruses and interfere on influenza circulation due to inhibition of this virus replication in the upper respiratory airway after rhinovirus infection [8]. Also, SARS-CoV-2 circulation could delay influenza’s appearance for a period of time, and rhinovirus could block SARS-CoV-2 replication, probably because of an interferon mediated response that could also impact COVID-19 severity and burden of disease (Figure 1) [9].
3.2. Efficacy of Surveillance Systems on Epidemiology of Influenza During the COVID-19 Pandemic
Epidemics have affected humans throughout history [10]. Epidemiological surveillance of influenza represents one of the most important challenges for national health systems, since it has become the reference for modelling other possible pandemics, generate strategic plans, describe mechanisms of prevention and control, and create preparedness and responsiveness. Mexico and Central America had a plan implemented for the H1N1 Influenza pandemic back in 2009 and had a strategic reserve of drugs to treat this respiratory virus.
Surveillance systems implemented during the 2009 influenza pandemic proved to be invaluable in Central America and Mexico, enabling local responders to effectively identify and monitor syndromic respiratory pathogens like influenza. With the 2019 SARS-CoV-2 pandemic, these established surveillance mechanisms continued to play a crucial role, and despite the overload of work on healthcare providers, these systems remained sensitive and robust, facilitating detection and local characterization of the COVID-19 pandemic.
As shown in Table 2, the countries in Central America and Mexico have surveillance and registry of influenza-like illness (ILI) such as severe acute respiratory infections (SARI). All have virology diagnosis trough reverse transcription polymerase chain reaction (RT-PCR), and report to the Flu ID and Flu Net platforms (except for Panama) [11].
These surveillance systems generate valuable information used for public health analysis and decision-making, especially when analyzing preventive measures such as vaccination. They are trusted and have sufficient capacity to generate necessary information for this purpose.
Given the territorial and demographic characteristics of the country, Belize has a national surveillance system, using the World Health Organization (WHO) case definitions. Samples of the totality of cases are evaluated and informed to the population through the Belize Health Information System [11]. In 2020, Belize ran 1,078 tests.
The surveillance system in Costa Rica has their own definition for ILI and SARI but uses the WHO definition for acute respiratory infection (ARI). All SARI cases are tested, and a sample of 50 ILI patients are weekly analyzed, offering valuable follow-up information. For SIRI and ILI, Costa Rica uses the Pan American Health Organization (PAHO) surveillance system and their national digital medical record (EDUS). Results are reported online, and the system performed close to 4,700 tests in 2020 [11].
In El Salvador, it operates with an epidemiological system called VIGEPES using the WHO case definitions for ILI, ARI, and SARI. El Salvador uses sentinel surveillance sites in 3 to 4 places for ILI, and 1,238 sites for SARI. All cases are tested on these sites and reported online, and the country performed over 1,000 tests in 2020 [11].
Sentinel sites in Guatemala are used for ILI and SARI and ran 1,714 tests in 2020. The national surveillance is used for ARI cases. This country tests 40% or all SARI cases, and 60% of ILI diagnoses, with available online reports for the population. Guatemala uses the PAHO surveillance system called SIGSA 3, using the WHO operational definitions [11].
Honduras uses the WHO case definitions for their surveillance system. For ILI and SARI, sentinel sites test 21% and 100% of cases respectively, while ARI surveillance is national. For ILI and SARI, Honduras uses the PAHO surveillance system, but for ARI, they use their own program denominated SINAVIS [11]. Honduras performed 1,262 tests in 2020.
Mexico has a sensible and robust conventional and special surveillance system that tested 68,165 samples in 2020, using the WHO case definition for ARI cases. For ILI and SARI, they test 10% and 100% of cases respectively using sentinel spots, and national evaluation for ARI cases. They use their own systems: SISVER for ILI/SARI surveillance, and SUIVE for ARI cases [11].
The surveillance system in Nicaragua uses sentinel places for ILI and SARI cases using their own case definition. They test 100% of SARI cases, and three samples per week of ILI using six sentinel sites using a system called “Alerta”. In 2020, the system processed 3,639 samples. For ARI, they use the WHO operational definition trough a system denominated SIVE, with online reports of cases [11].
Panama uses WHO operational definitions for all three entities, using sentinel sites for SARI, and national samples for ILI and ARI. For ILI and SARI, a total of 100 cases are gathered per week in ten different sites, using online reports for communication of data [11]. Still, Panama ran less than 1,000 samples in 2020.
Reference laboratory characteristics in all eight countries and generated information is valuable to understanding the epidemiological surveillance capacity in respiratory diseases, especially influenza.
Central America and Mexico develop virologic surveillance using standardize RT-PCR. Only Belize and Nicaragua do not share samples with the WHO, but the total numbers shared during 2020 are coherent with influenza disease during the pandemic. Nevertheless, none of the countries has burden of disease information, and only Panama and Honduras have economic analysis of healthcare costs [12].
Disease associated with influenza was considerably affected during the COVID-19 pandemic. For example, in the Americas, the respiratory season of 2019-20 was ended abruptly and almost no activity of influenza was documented in 2020-21. Given the preventive measures implemented, cases where unusually low during 2021-22, but cases rose intensively in 2022-23 caused by influenza A, and influenza A H1N1 pdm09, with some isolated cases of influenza B.
In North America, including Mexico, similar behavior of influenza was documented, with non-typified cases of influenza A and influenza B during the last weeks of the season. For Central America and the Caribbean, the situation was similar, with fewer influenza B cases, but with longer circulation times of influenza A during 2021-22 [12].
Epidemiologic surveillance systems of these eight countries give sufficient and trusted information, enough to help with decision making and to generate evidence for public health policies. These systems can always be improved and enriched with better analysis of already available information. Nevertheless, not all information is available due to underreporting in several countries.
Regarding the epidemiological surveillance indicators for influenza in the countries, all use SARI, ILI, and have National Center of Influenza, RT-PCR for surveillance an external quality evaluation program. The countries had the last evaluation between 2020 (El Salvador, Nicaragua) and 2021 (Belize, Costa Rica, Honduras, Mexico, and Panama) except Guatemala, where there is no data. The eight countries carried out Flu ID reports and for Flu Net except for Panama. As of the information reported for the year 2023, all countries reported to Flu Net.
Influenza behavior depends on several characteristics: the agent itself, host response, and environmental changes that determine seasonality, presentation, disease severity, lethality, and intensity of contagion. Vulnerable populations like the elderly, people with underlying conditions, and incomplete vaccination status, can influence the presentation of disease and epidemiology. These information changes are necessary for surveillance systems that are in place.
Up to 80% of modern emerging diseases are of zoonotic origin, like those documented with influenza, SARS-CoV-2, and other respiratory viruses. Special surveillance of human and animal diseases is necessary, considering recent outbreaks and epidemic waves of viral diseases such as avian influenza. Even though human-to-human transmission of these recent zoonotic diseases has not shown to be efficient, preparation and response for prevention and control are imperative.
Surveillance systems need to be prepared for a possible “tridemic” in humans that include influenza, SARS-CoV-2, and Respiratory Syncytial Virus (RSV) disease. Early detection, evaluation, analysis of learned lessons, and self-evaluation of applied interventions, need to be taken into consideration by local systems.
3.3. Influenza Vaccination in Central America and Mexico Before and After the COVID-19 Pandemic
Influenza vaccine is not included in national vaccination programs of many countries, but in the region of the Americas, it is included in most countries.1 Application varies in Central American countries and Mexico. Immunization schedules have been adapted following the WHO and PAHO recommendations, and considering epidemiological conditions, organizations, and financial realities for each country.
Belize, Guatemala, and Mexico apply influenza vaccine with the northern hemisphere formulation between October and February, while Costa Rica, El Salvador, Honduras, Nicaragua, and Panama, use the southern hemisphere formulation [13]
Based on epidemiological characteristics and the availability of economic resources [14], countries decide if trivalent (one antigen against influenza B and two against influenza A) or tetravalent (two antigens against influenza A and B) vaccines are used. In 2022, Costa Rica, El Salvador, and Panama used tetravalent vaccine [15,16], while Belize, Guatemala, Honduras, Mexico, and Nicaragua used trivalent vaccine in their national vaccination campaign.
According to the epidemiological situation and availability of resources in each country, prioritization of risk groups is used based on recommendations of the Technical Advisory Group (TAG) of PAHO and the Strategic Advisory Group of Experts on Immunization (SAGE-WHO), which prioritize pregnant women, children, elderly, people with underlying diseases, and healthcare workers [2].
Information regarding vaccine coverage against influenza varies among countries, depending on their policies to provide vaccination and their definition of high-risk groups. Report systems and frequency with which information is updated are also different among regions. Considering these variations, information available in Central America and Mexico is not complete. Vaccine coverage information is based on annual reports that countries make to PAHO, WHO, and UNICEF [17], and that are available in the PAHO database [18], WHO [19], and the “Immunization of the Americas” document from PAHO between 2018-22 [3,20,21,22].
Vaccination against influenza in pregnant women has been a priority in American countries, especially after the influenza A H1N1 pandemic in 2009. All countries have pregnant individuals as a priority group. Available information shows that El Salvador, Honduras, and Mexico had steady coverage during 2020, while Panama increased coverage that year. Nevertheless, in 2021, Guatemala, Honduras, and Panama experienced a decrease in vaccines applied in this group. Comparing 2021 data with 2018 in Costa Rica, a decrease in coverage among pregnant women, children, and the elderly was observed, while there was an increase among healthcare workers, a trend that continued in 2022 and 2023 (Table 3).
Vaccination in children experienced a decrease in coverage in many countries during 2021, with a partial recovery in countries like Belize and El Salvador. For the years 2022 and 2023, none of the countries reported optimal vaccination coverage.
Except for Mexico and Panama, in 2020 most countries suffered a decrease in vaccination coverage against influenza among the elderly. By 2021, El Salvador and Mexico recovered to pre-pandemic numbers, while Honduras and Panama had constant drop in vaccination coverage. During 2022, an increase in coverage was observed for most countries. However, some of these countries experienced a decrease in 2023, such as Honduras and Panama.
Information regarding vaccine coverage in groups with chronic underlying diseases is not available in several countries. Honduras and Nicaragua reported maximum coverage in this group, with no variation between 2020-21. Mexico and Nicaragua continue to be the countries with ideal and constant coverage in the region for the years 2022-23
Vaccination among healthcare workers remains constant in most countries between 2019-20. Nevertheless, by 2021, Belize, Guatemala, Honduras, and Panama reported a decrease in vaccine coverage when compared with 2020. For 2022-23, an increase in coverage for this population is observed in most countries. However, Belize, Guatemala and Panama are the countries with low coverage for these years.
However, there is a big question regarding influenza vaccination coverage. Countries do not procure the number of vaccines according to the number of people in the defined groups they should vaccinate, purchases are always lower than that of in need of being vaccinated. Hence, we believe countries are reporting administrative coverages, meaning the percentage of vaccines applied of those defined for that specific group from the total procured doses.
Central America and Mexico differ in the characteristics of the vaccine used, time of the year for vaccination, and definition of risk groups. We present the available information on the characteristics of vaccination in each country and the reported vaccine coverage among risk groups between 2017-23.
In Belize, before the COVID-19 pandemic, an important effort to establish public health policies and adequate vaccine coverage, and between October and June, Belize used the northern hemisphere vaccine formulation. Coverages were severely compromised during the pandemic, except for vaccination in children, that in 2021, numbers were similar to pre-pandemic data.
Costa Rica has tried to improve national public policies. Influenza vaccination is scheduled every year beginning in May-July with the southern hemisphere formulation.
There are national policies for influenza vaccination in El Salvador, with application of the southern hemisphere formulation starting April to May. The number of doses has increased through the years, nevertheless, a decrease of vaccination in children and elderly in 2020 was documented.
In 2018, Guatemala used the southern hemisphere vaccine in April-June, and the Northern hemisphere one in November-December to continue with this formulation thereafter. Available information regarding coverage does not allow a thorough analysis of high-risk groups or their behavior in time, except for vaccination in children, where a decrease was observed during the pandemic years.
Using the southern hemisphere formulation, Honduras applies close to 1.5 million vaccines per year, with a discrete increase in available doses when compared 2018 and 2021.
Influenza vaccine coverage in Mexico also suffered changes during the COVID-19 pandemic. A slight decrease in coverage in pregnant women and children was documented in 2020. By 2021, vaccination coverage in pregnant women reached similar numbers than in the pre-pandemic period and continued similar for the years 2022-23. High coverage has been described in healthcare workers and people with underlying diseases. Likewise, children and the elderly population have had optimal coverage.
Nicaragua reported steady vaccine coverage in people with underlying conditions and healthcare personnel, while during pregnancy, the number dropped when compared with pre-pandemic reports. This country has no record of coverage for the group of children, but it shows 100% coverage in population groups with chronic diseases and health workers.
Panama has a national vaccination policy that controls recommendations for influenza vaccine. With a decrease in number of available doses when compared 2018 with 2021, Panama also observed a decline in coverage among children and healthcare workers. A slight increase in applied doses to pregnant women and the elderly was documented after the COVID-19 pandemic. But for the years 2022-23, the country showed an increase in coverage for priority groups.
3.4. Access to Influenza Vaccine in Central America and Mexico
The region of the Americas is identified by the WHO as the region with more influenza vaccine doses applied around the world, with more than 300 million doses used only in this region [1]. Between Central American countries and Mexico, around 40 million doses are estimated to be applied annually. Acquisition of vaccines for the region can be achieved by direct production, PAHO Revolving Fund (RF) for Vaccines, direct purchases from producers, and donations. In 2019, six American countries reported local production of influenza vaccine. During the pandemic, several initiatives were presented to reinforce local production [23] towards becoming a self-sufficient region. Nevertheless, this goal has not been achieved at this time.
Most countries in the region procure vaccines through the PAHO-RF regardless of the formulation used or the specific characteristics of the vaccine (trivalent vs. tetravalent). The objective is to ensure quality, lower costs, and homogeneity between countries regardless of the number of vaccines applied [14]. During the COVID-19 pandemic, the RF played a major role trying to keep equity among countries and a continuous offer of supplies and vaccines, including influenza vaccine [24].
Countries can also celebrate direct agreements with influenza vaccine producers, ensuring WHO vaccine standards and prices close to those offered by the RF. For example, most influenza vaccines with southern hemisphere formulation are produced in the American region, opening the possibility for countries to acquire the vaccine trough the RF, direct purchase, or a combination of both. Several countries can also access vaccines through donations.
4. Discussion
Vaccination is a complex and priority process in need of new strategies and mechanisms for the continuous improvement of programs and public policies. Each vaccination program has differences among countries, nevertheless, they all have a core health system based on the prevention of diseases with sensitive epidemiological surveillance systems able to generate information that public policies can and should use for decision making regarding vaccination.
Vaccination cannot be an isolated program from other interventional strategies or control of diseases. The 2019 WHO World Strategy against Influenza for 2019-30 has core elements so that every country can be prepared to face the risk of a new influenza pandemic.
Lessons learned by all health systems during the COVID-19 pandemic are relevant. Such an unprecedented event highlighted the strengths but also the weaknesses of health systems around the world. Even though in most countries, vaccination was a well-received strategy, it showed resistance among people, doubt, and a growing antivaccine force that affected vaccination campaigns. Nevertheless, there is a need to increase vaccination coverage against influenza in Central America and Mexico.
The objectives and priority actions of the World Strategy against Influenza are to strengthen national surveillance capacities, prevention, preparedness, treatment, and response; and to elaborate better instruments to prevent, detect, and control influenza disease using vaccines, antivirals, and effective treatments available in all countries [25].
This World Strategy contemplates all actions necessary to prepare and plan for influenza season, and the possibility of a future pandemic caused by influenza. Priority inclusion of vaccine processes is necessary, not only in the operations side, but in research and innovation.
It is important to emphasize the urge for immunization programs to be separated from political decisions and become programs that endure and get stronger with time. It is essential to gradually establish a legal framework to provide vaccination policies and ensure adequate finance for their proper implementation.
Most countries in the PAHO region, particularly Central America and Mexico, carry out campaigns of massive vaccination, to reach identified priority groups. Influenza vaccine is not always offered in public health systems, and unlike other vaccines, it is only available during pre-defined high-risk epidemiological periods, that vary in every sub-region.
Before the COVID-19 pandemic, vaccination was mainly offered at health entities and mobile units to reach places of dense people concentration. For example, Honduras used to increase vaccination hours at day and night to improve possibilities for the working force and their families.
In 2020-21, several strategies to maintain vaccine coverage were implemented, such as vaccination in institutions with prolonged working hours, isolated vaccine areas to avoid possible contact with COVID-19 patients, mobile units to visit communities, drive-through vaccination spots, and vaccines offered during other healthcare services [1]. For this purpose, countries adapted their health systems, using social and community leaders, and created health promotion campaigns through massive advertising [3]. Some countries continue to strengthen vaccination campaigns to achieve optimal protection coverage in the population.
Central America and Mexico vaccination programs have a great history of success. Elimination of vaccine-preventable diseases has been accomplished in the region several times before, so the use of adequate resources in each country and region is not the current challenge to improve vaccine coverage.
There are important elements that could help improve the influenza vaccine in the region. Adequate training before, during, and after vaccine campaigns to healthcare providers is necessary, so they can understand the importance of immunization and encourage communities and high-risk populations. Skills to guide and inform the general public and help in case of hesitancy or doubt could avoid misinformation and improve vaccine acceptance. The COVID-19 pandemic has made evident the growing infodemic problem that people around the world is exposed to.
One of the biggest challenges for Central America and Mexico is to improve and maintain vaccination coverage, prioritize national immunization programs, and guarantee human and economic necessary resources. An alliance between public, social, private, academic, and religious sectors among other could help in this process.
Author Contributions
C.E.T and F.B-P, conceptualized the revision and made substantial contributions and edits. C.R-M, L.S-I, and C.R-M wrote the original first draft. R.T.V and H.B.C provided comments on the manuscript and adjusted the final manuscript. All authors participated in the draft revisions and in approving the final draft for submission. The authors accept responsibility for the decision to submit the article for publication.
Funding
This research was developed by the Global Health Consortium, Department of Global Health, Robert Stempel College of Public Health & Social Work Florida International University (Project ID 800017326).
Informed Consent Statement
Not applicable.
Data Availability Statement
Data are contained in the article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Vicari AS, Olson D, Vilajeliu A, et al. Seasonal Influenza Prevention and Control Progress in Latin America and the Caribbean in the Context of the Global Influenza Strategy and the COVID-19 Pandemic. Am J Trop Med Hyg 2021; 105(1): 93-101. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8274756/. [CrossRef]
- Organización Panamericana de la Salud. Reunión del Grupo Técnico Asesor (GTA) sobre Enfermedades Prevenibles por Vacunación. Las vacunas nos acercan, 14 al 16 de julio del 2021. https://www.paho.org/es/documentos/xxvi-reunion-grupo-tecnico-asesor-gta-sobre-enfermedades-prevenibles-por-vacunacion.
- Organización Panamericana de la Salud. Inmunización en las Américas. Resumen 2020. 2020. https://iris.paho.org/handle/10665.2/55370.
- Leung NHL. Transmissibility and transmission of respiratory viruses. Nat Rev Microbiol 2021; 19(8): 528-45. Epub 2021 Mar 22. [CrossRef]
- Nasrullah A, Gangu K, Garg I, Javed A, Shuja H, Chourasia P, et al. Trends in Hospitalization and Mortality for Influenza and Other Respiratory Viruses during the COVID-19 Pandemic in the United States. Vaccines (Basel) 2023; 11(2): 412. [CrossRef]
- Doroshenko A, Lee N, MacDonald C, Zelyas N, Asadi L, Kanji JN. Decline of Influenza and Respiratory Viruses With COVID-19 Public Health Measures: Alberta, Canada. Mayo Clin Proc 2021; 96(12): 3042-52. [CrossRef]
- Kiseleva I, Ksenafontov A. COVID-19 Shuts Doors to Flu but Keeps Them Open to Rhinoviruses. Biology (Basel) 2021; 10(8). [CrossRef]
- Wu A, Mihaylova VT, Landry ML, Foxman EF. Interference between rhinovirus and influenza A virus: a clinical data analysis and experimental infection study. Lancet Microbe 2020; 1(6): e254-e62. [CrossRef]
- Dee K, Goldfarb DM, Haney J, Amat J Ar, Herder V, Meredith S, et al. Human Rhinovirus Infection Blocks Severe Acute Respiratory Syndrome Coronavirus 2 Replication Within the Respiratory Epithelium: Implications for COVID-19 Epidemiology. J Infect Dis 2021; 224(1): 31-8. [CrossRef]
- Moriyama M, Hugentobler WJ, Iwasaki A. Seasonality of Respiratory Viral Infections. Annu Rev Virol 2020; 7(1): 83-101. [CrossRef]
- Pan American Health Organization. Influenza and Other Respiratory Viruses: Surveillance in the Americas 2021. 2022. https://iris.paho.org/handle/10665.2/56544.
- World Health Organization. FluNet Summary. 2024. https://www.who.int/tools/flunet/flunet-summary.
- Organización Panamericana de la Salud. Vacuna contra la influenza. 2023. https://www.paho.org/es/vacuna-contra-influenza.
- Organización Panamericana de la Salud. Precios Vacunas del Fondo Rotatorio de la OPS 2023. https://www.paho.org/es/documentos/precios-vacunas-fondo-rotatorio-ops-2023.
- Ministerio de Salud. Republica de Costa Rica. Lineamiento para la Jornada de Vacunación con Influenza Estacional 2022 en los establecimientos de salud de la Caja Costarricense del Seguro Social. 2022. https://www.cendeisss.sa.cr/wp/wp-content/uploads/2022/07/Lineamiento-Influenza-2022.pdf.
- Influenza puede causar enfermedad grave en grupos de riesgo; vacúnese. 2021. https://lawebdelasalud.com/influenza-puede-causar-enfermedad-grave-en-grupos-de-riesgo-vacunese/.
- Organización Panamericana de la Salud - iris Institucional Repository for Information Sharing. Preguntas frecuentes: Formulario conjunto para la notificación de datos sobre inmunización y estimaciones de la OMS y el UNICEF sobre la cobertura nacional de inmunización. 2020. https://iris.paho.org/handle/10665.2/52556.
- Organización Panamericana de la Salud. Cobertura de vacunación contra influenza 2018. https://ais.paho.org/imm/InfluenzaCoverageMap.asp.
- UNICEF. Immunization coverage estimates dashboard. 2023. https://data.unicef.org/resources/immunization-coverage-estimates-data-visualization/.
- Organización Panamericana de la Salud. Inmunización en las Américas, Resumen 2018. 2018. https://www.paho.org/es/node/59921.
- Organización Panamericana de la Salud. Inmunización en las Américas, Resumen 2019. 2019. https://www.paho.org/es/documentos/inmunizacion-americas-resumen-2019.
- Organización Panamericana de la Salud. Inmunización en las Américas. Resumen 2021. 2021. https://www.paho.org/es/documentos/inmunizacion-americas-resumen-2021#:~:text=Resumen%202021,-.
- Sparrow E, Wood JG, Chadwick C, Newall AT, Torvaldsen S, Moen A, et al. Global production capacity of seasonal and pandemic influenza vaccines in 2019. Vaccine 2021; 39(3): 512-20. [CrossRef]
- Organización Panamericana de la Salud. La compra conjunta como parte de la preparación y respuesta frente a pandemias: Potenciar los fondos rotatorios de la OPS para fortalecer la equidad en la salud y la resiliencia. 2022. https://iris.paho.org/handle/10665.2/56956.
- Organización Panamericana de la Salud. Estrategia Mundial contra la Gripe 2019-2030. 2019. https://www.paho.org/es/documentos/estrategia-mundial-contra-gripe-2019-2030#:~:text=La%20Estrategia%20Mundial%20contra%20la,y%20el%20control%20de%20la.
Figure 1.
Interaction between respiratory viruses. Adapted from COVID-19 Shuts Doors to Flu but Keeps Them Open to Rhinoviruses. Kiseleva I, Ksenafontov A. Biology (Basel). 2021;10(8). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8389621/.
Figure 1.
Interaction between respiratory viruses. Adapted from COVID-19 Shuts Doors to Flu but Keeps Them Open to Rhinoviruses. Kiseleva I, Ksenafontov A. Biology (Basel). 2021;10(8). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8389621/.
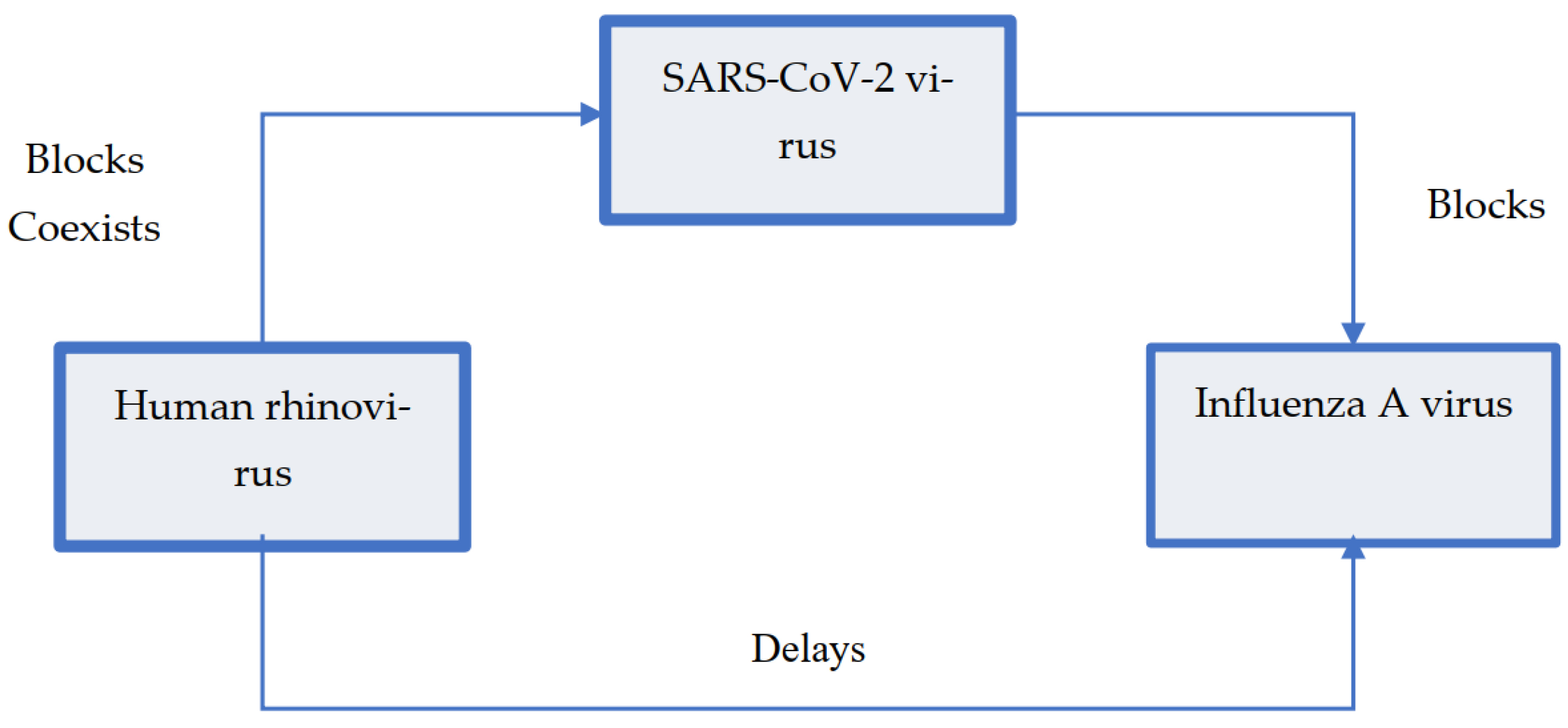

Table 1.
Transmissibility variables, ways of transmission, and effectivity of non-pharmacological measurements. (Abbreviations: SAR, Secondary attack rate).
Table 1.
Transmissibility variables, ways of transmission, and effectivity of non-pharmacological measurements. (Abbreviations: SAR, Secondary attack rate).
| Variables | SARS-CoV-2 | Influenza Virus |
|---|---|---|
| Transmissibility | ||
| Basic reproduction number (R0) | 0.5-8.0 | 1.0-21.0 |
| Household SAR (%) | 0-38.2 | 1.4-38.0 |
| Ways of transmission | ||
| Direct contact transmission | Yes | Yes |
| Fomite transmission | Yes | Yes |
| Airway transmission | Yes | Yes - main source of transmission |
| Aerosol transmission | Yes | Yes |
| Effectivity of non-pharmacological | ||
| Handwash | Yes | Yes |
| Face mask | Yes (within the house) | Yes |
| Surface cleanse | Limited | Limited |
| Close spaces ventilation | Yes | Yes |
Table 2.
Epidemiologic surveillance indicators of influenza per country.
| Country | SARI surveillance | ILI surveillance | National Center of Influenza | RT-PCR surveillance | External quality evaluation program | Last evaluation year | Flu ID report | Flu Net report |
|---|---|---|---|---|---|---|---|---|
| Belize | Yes | Yes | Yes | Yes | Yes | 2021 | Yes | Yes |
| Costa Rica | Yes | Yes | Yes | Yes | Yes | 2021 | Yes | Yes |
| El Salvador | Yes | Yes | Yes | Yes | Yes | 2020 | Yes | Yes |
| Guatemala | Yes | Yes | Yes | Yes | Yes | No data | Yes | Yes |
| Honduras | Yes | Yes | Yes | Yes | Yes | 2021 | Yes | Yes |
| Mexico | Yes | Yes | Yes | Yes | Yes | 2021 | Yes | Yes |
| Nicaragua | Yes | Yes | Yes | Yes | Yes | 2020 | Yes | Yes |
| Panama | Yes | Yes | Yes | Yes | Yes | 2021 | Yes | No |
Table 3.
Influenza vaccine coverage for key groups in Central America and Mexico between 2017-2023. Data originate from World Health Organization WHO, https://immunizationdata.who.int/global/wiise-detail-page/influenza-vaccination-coverage. (July 18, 2024).
Table 3.
Influenza vaccine coverage for key groups in Central America and Mexico between 2017-2023. Data originate from World Health Organization WHO, https://immunizationdata.who.int/global/wiise-detail-page/influenza-vaccination-coverage. (July 18, 2024).
| Countries | Year | ||||||
|---|---|---|---|---|---|---|---|
| 2017 (%) | 2018 (%) | 2019 (%) | 2020 (%) | 2021 (%) | 2022 (%) | 2023 (%) | |
| Influenza vaccine coverage in pregnant women | |||||||
| Belize | 8 | 48 | 72 | No data | 6 | 5 | 8 |
| Costa Rica | 72 | 73 | No data | No data | 69 | No data | 82 |
| El Salvador | 61 | 78 | 48 | 49 | 60 | 100 | 87 |
| Guatemala | 23 | No data | No data | 16 | 10 | 14 | 16 |
| Honduras | 78 | 82 | 85 | 84 | 63 | 60 | 67 |
| Mexico | 62 | 81 | No data | 78 | 88 | 88 | 81 |
| Nicaragua | 51 | 91 | 98 | No data | 89 | 87 | 98 |
| Panama | 58 | 64 | 63 | 73 | 58 | 79 | 93 |
| Influenza vaccine coverage in children | |||||||
| Belize | 73 | 70 | 83 | 54 | 85 | 41 | 43 |
| Costa Rica | 32 | 77 | No data | No data | 66 | 45 | 43 |
| El Salvador | 62 | 66 | 57 | 39 | 54 | 65 | 65 |
| Guatemala | 2 | 100 | 1 | 10 | 4 | 8 | 13 |
| Honduras | No data | No data | 62 | 53 | 47 | 38 | 47 |
| Mexico | 84 | 88 | 91 | 87 | 82 | 83 | 86 |
| Nicaragua | No data | No data | No data | No data | No data | No data | No data |
| Panama | 69 | 57 | 71 | 61 | 27 | 33 | 31 |
| Influenza vaccine coverage in elderly | |||||||
| Belize | 2 | 41 | 36 | 6 | 2 | 1 | 3 |
| Costa Rica | 92 | 99 | No data | No data | 61 | No data | 56 |
| El Salvador | 35 | No data | 42 | 37 | 45 | 57 | 64 |
| Guatemala | No data | No data | No data | No data | 3 | 3 | 5 |
| Honduras | 88 | 79 | 68 | 56 | 45 | 100 | 73 |
| Mexico | 94 | 94 | 94 | 94 | 95 | 95 | 95 |
| Nicaragua | No data | No data | No data | No data | 96 | 97 | No data |
| Panama | 100 | 100 | 83 | 99 | 18 | 67 | 65 |
| Influenza vaccine coverage in chronic conditions | |||||||
| Belize | No data | No data | No data | No data | 2 | 4 | 1 |
| Costa Rica | No data | 79 | No data | No data | No data | No data | No data |
| El Salvador | No data | No data | No data | No data | No data | No data | No data |
| Guatemala | 100 | No data | No data | No data | 25 | 33 | 53 |
| Honduras | 100 | 100 | 100 | 100 | 100 | 100 | No data |
| Mexico | 100 | 99 | 99 | 100 | 100 | 100 | 100 |
| Nicaragua | No data | 100 | 100 | 100 | 100 | 100 | 100 |
| Panama | No data | No data | No data | No data | 100 | 100 | No data |
| Influenza vaccine coverage in health personnel | |||||||
| Belize | No data | 78 | 46 | 12 | 3 | 1 | 1 |
| Costa Rica | 88 | 72 | No data | No data | 88 | No data | No data |
| El Salvador | 61 | 84 | 100 | 100 | 100 | 100 | 99 |
| Guatemala | 74 | 90 | No data | 47 | 32 | 34 | 47 |
| Honduras | 100 | 100 | 85 | 82 | 59 | 88 | 91 |
| Mexico | 100 | 100 | 100 | 100 | 100 | 95 | 100 |
| Nicaragua | 88 | 100 | 96 | 100 | 100 | 100 | 100 |
| Panama | 92 | 94 | 95 | 89 | 42 | 53 | 70 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



