
Submitted:
20 October 2024
Posted:
21 October 2024
You are already at the latest version
Abstract
Cerebral palsy is a group of nonprogressive conditions that affect movement and posture caused by damage to the central nervous system at an early stage of a child's development. Among this group of patients, there is a higher risk of the appearance and progression of neurogenic scoliosis, which unlike idiopathic scoliosis, progresses after skeletal maturity. The aim of the study was to analyze the association of comorbid factors with the risk of development and progression of neurogenic scoliosis. The study included 133 patients with cerebral palsy. The relationship between comorbidities in children with cerebral palsy and the risk of developing neurogenic scoliosis was demonstrated and proven.
Keywords:
cerebral palsy
; neurogenic scoliosis
; Cobb angle
; progression
; Gross Motor Function Classification System
1. Introduction
The Cerebral palsy is a syndrome of movement and postural abnormalities that result from nonprogressive damage to the central nervous system (CNS) early in a child’s development [1]. Cerebral palsy is estimated to occur in two to three cases per 1,000 live births; in the United States alone, it occurs in one in 323 children, while in Poland the figure is 2-2.5 per 1,000 live-born children [2,3]. In addition to movement and postural disorders, children with cerebral palsy are also accompanied by disorders of sensation, perception, cognition, communication and behavior, epilepsy or secondary musculoskeletal problems [1,2,4]. The most common adverse factors affecting brain damage at an early stage of its development are hypoxia, premature birth, intrauterine infections, low birth weight, Apgar scores below 5 points, multiple pregnancies, abnormalities of previous pregnancies or births, as well as premature rupture of fetal membranes or fetal malposition [1,4,5,6]. Children with cerebral palsy have an increased risk of the appearance and development of neurogenic scoliosis [7]. The incidence of neurogenic scoliosis among this group of patients is significantly higher than in the general population, averaging 20-25%, and depends on differences in age, the nature and severity of neurological dysfunction, and the degree of physical impairment [8,9,10,11]. Scoliosis is a musculoskeletal disorder caused by a three-plane deformation of the spine in the sagittal, transverse and frontal projections, which is often accompanied by a thoracic deformity [1,12]. Neurogenic scoliosis is a spinal deformity that often accompanies neuromuscular diseases and is closely related to them. It arises due to weakened control of the trunk muscles, as a result of their contracture or the resulting compensatory mechanisms that have deteriorated during the course of the disease [13]. According to the Scoliosis Research Society’s definition, neurogenic curvature is caused by disorders of the brain, spinal cord and muscular system. The structures are unable to maintain proper balance of the spine and trunk, resulting in asymmetries and deformities. The abnormal postural patterns that occur are due to brain damage, while secondary symptoms are caused by the activation of compensatory postural control mechanisms [13,14]. Along with the occurrence of torsion, pelvic obliquity, which is defined as a deviation of the pelvis from the horizontal plane, also often occurs. Abnormal curvature of the spine, hip contractures or a difference in the length of the lower extremities contribute to its formation. Among the categories attributed to pelvic obliquity, we can distinguish between supra-pelvic obliquity (of upper origin), resulting from disorders of the spine/back, caused by asymmetric retraction of the muscles connecting the trunk to the pelvis, and sub-pelvic obliquity (of lower origin), resulting from disorders of the hip joint and lower extremities, caused by asymmetric positioning of the hips, usually in flexion, adduction and internal rotation [13]. The curvature of the spine, along with the obliquity of the pelvis, causes imbalance and problems with maintaining a sitting position, which is especially important for people who move with the help of orthopedic devices such as a wheelchair. It contributes to the appearance of excessive pressure points on the body in the sitting position, resulting in pressure sores, bony deformities, and pain due to uneven loading of the trunk [13,15]. The classic form of neuromuscular spinal deformity is a longitudinal curvature at the level of the thoracolumbar spine up to the pelvis, causing it to be oblique [13,15] The degree of severity of scoliosis is determined by the amount of curvature of the spine, the angular amount of which is assessed using the Cobb angle and the angle of rotation of the trunk. Initially, the curvature may be low-grade, but over time, with progressive and established postural abnormalities, it can significantly change - worsen [1,12]. Changes in the structure, function and physiological position of the spine lead to asymmetric loading, which causes further degenerative changes, accelerated progression of muscle changes and postural collapse, and sometimes even changes in the respiratory or visceral system [16]. Factors contributing to the development of large spinal curvatures include severe neurological impairment, young age at the time of scoliosis onset, existing quadriplegia or severe spasticity affecting the entire body, accompanying comorbidities. Individuals who are able to move independently appear to be less susceptible to the development and progression of the disorder [10]. The risk of scoliosis also increases with the severity of co-occurring disorders involving incomplete or total body involvement, age, and level of psychomotor development as expressed by the Gross Motor Function Classification (GMFCS) scale [11]. It is also associated with a sedentary lifestyle, progressive degenerative changes, the appearance of muscular atrophy or decreased bone mineral density [8,9,10]. Severe scoliosis most often occurs in individuals with severe functional limitations, described using GMFCS classification levels 4 and 5 [10]. Patients with severe spasticity affecting the entire body are at the highest risk of developing scoliosis [10]. Regarding the different forms of cerebral palsy, according to studies, lateral curvature of the spine most often affects those with quadriplegia, followed by those with biplegia (diplegia) and hemiplegia [10,17]. In addition to paralysis, in some patients muscle hypertonia is a major factor in the appearance of torsion [13]. Then there is asymmetric control (disharmony) of the trunk muscles around the axis of the spine, which begins to progress over time due to inefficient compensatory muscle mechanisms [13]. In the early stages of the onset of scoliosis, it may be painless and the curvature may be hardly noticeable. Then, more visible changes in the alignment of individual body structures may turn out to be protraction of the head, protrusion of one of the shoulder blades, asymmetry of the hips, unequal waist angles or asymmetry of the level of shoulder alignment - one arm higher or lower than the other [18]. In the case of neuromuscular or neurological diseases, the goal is repeatedly not to reduce the angle of the curvature, but to avoid rapid progression of the curvature or to maintain it at the original level. The initial diagnosis consists of a screening examination, which includes a visual assessment of the child’s figure to determine asymmetry of the indentation of the waist angles, inequality regarding the level of the shoulders or lateral deviation of the trunk in relation to the pelvis. This assessment is supported by special measuring tools such as the Bunnel scoliometer or inclinometer, which help evaluate objectively the symmetry of the vertical alignment of specific body points and the angle of rotation [19]. The Bunnel scoliometer is a plastic device used to measure the angle of rotation of the trunk, having a tube filled with liquid, similar to a level, in which the pointer moves, and a recess in the center of the lower edge for placement on the spinous process of the vertebrae of the spine. It is a reliable tool recommended for screening to diagnose scoliosis, which is placed perpendicular to the long axis of the spine in a non-invasive and pressure-free manner. During the examination, the patient is asked to position his feet hip-width apart and his limbs straight at the knee joints. The patient then bends forward to make the asymmetrical alignment of the spinal segments more apparent, as well as the presence of a rib hump or lumbar shaft. The angle of rotation of the trunk is measured at the point of greatest asymmetry of the spine or at different levels of the spine. When the spine is symmetrical, then the scale indicates 0 degrees. Among the occurring ranges of trunk rotation, we can distinguish: 0-3 degrees - physiological asymmetry of the trunk, 4-6 degrees - the need for repeated examinations after 3-4 months, and rotation >7 degrees - indicating suspected scoliosis, in which case an X-ray and a visit to an orthopedist are recommended [20]. Performing a radiographic examination (in anterior-posterior projection) is used to determine the amount of curvature (Cobb angle) and allows monitoring the progression of an already diagnosed postural defect [20]. Determining the value of the Cobb angle makes it possible to assess the level of progression of scoliosis and to decide on treatment. The most common division indicating the severity of curvature is the four-stage division, according to which the 1st degree of curvature is up to 30 degrees, the 2nd degree 31-60 degrees, the 3rd 61-90 degrees and the 4th 91 degrees and above [18]. The degree of multiple curvature scoliosis is judged by the value of the greatest curvature, usually the primary curvature. Scoliosis is diagnosed when the angle of curvature is at least 10 degrees, while if the angle is less than 10 degrees and structural changes are not noticeable, then this posture is referred to as “scoliotic posture” [18,21]. Children with neurogenic scoliosis face daily problems with sitting, pressure sores, cardiopulmonary dysfunction, gastrointestinal dysfunction and pain sensations. Early diagnosis and recognition of a postural defect is important because of the faster initiation of therapy aimed at correcting already existing disorders and preventing the progression of the curvature, thus avoiding deterioration of functioning in the child’s daily life and the appearance or increase of pain [9]. In the programming of conservative treatment, the most important goal is to prevent the development and perpetuation of mobility restrictions and abnormal posture, for example, during sitting or inappropriate joint alignment, caused by spasticity or excessive contractures [14]. In order to properly carry out the therapy process, it is necessary to be guided by knowledge of the causes of the resulting disorder, regarding the development of compensatory antigravity mechanisms in the patient and the presence of substitute postural patterns in order to prevent them [14]. In the course of comprehensive rehabilitation of children with cerebral palsy, various types of orthopedic supplies are used to correct postural defects or compensate for structural or functional abnormalities, including orthoses, prostheses or assistive devices such as canes, crutches and wheelchairs. In the case of hip dislocation, which is a fairly common problem in children with cerebral palsy, orthoses such as the SWASH (Standing, Walking and Sitting Hip Orthosis) are used. These orthoses, by firmly stabilizing the pelvis and lower extremities, aim to reduce excessive adduction and internal rotation movements that most often lead to hip dislocation [14]. Bracing used to slow the progression of scoliosis improves sitting balance and allows trunk support, which provides better head and neck control and increases upper limb function. According to studies, it has been proven that orthoses can slow the progression of curvature, especially in younger patients whose curvature angle is less than 40 degrees [9]. In addition to the orthoses used, a method based on optimizing the sitting position can also be used to correct posture [15]. It has been noted that the placement of a 3-point side cushion system results in a more symmetrical trunk position and corrects the angle of curvature by 35% in non-ambulatory patients with cerebral palsy and neurogenic scoliosis [15]. In the treatment of children with cerebral palsy, therapeutic aids such as botulinum toxin BTX-A are also frequently used. Among the short-term benefits of using these adjunctive agents in a child’s therapy are a reduction in pain and associated discomfort and improved function, for example, in terms of upper limb motility, while long-term benefits include preventing the formation of permanent contractures and accompanying increased pain, as well as allowing muscle growth and more normal development of muscle function [14]. Although conservative treatment methods can slow the progression of scoliosis, surgery remains the definitive form of management for neurogenic scoliosis. Therefore, conservative treatment is often used as preparatory therapy for surgery [15]. Operative intervention in these patients mainly aims to stabilize and reduce the scoliotic curve, thus improving sitting, positioning and reducing the level of pain sensation. Indications for this method of treatment may include a curvature measuring 30 degrees or more, a curvature that impairs the ability to sit, a thoracic deformity that limits the patient’s respiratory function, or very severe pain [15]. Among the surgical methods of treating neurogenic scoliosis, we can distinguish posterior spondylodesis, which is the most common type of surgical treatment of scoliosis and is usually prescribed for patients whose spinal curvature is more than 50 degrees Cobb, shows great progression or results in functional or physiological disorders [15]. Surgical procedures used to reduce spasticity in patients with cerebral palsy include selective dorsal rhizotomy (SDR) and intrathecal baclofen therapy (ITB) pump implantation. Dorsal rhizotomy is a procedure performed before puberty, usually in the age range of 4 to 10 years in children with the ability to walk (mainly GMFCS levels I, II, III). As for the baclofen pump, on the other hand, it finds its use mainly in adolescents or adults with limited or no walking ability (GMFCS IV-V) [10]. Knowledge of the prevalence and characteristics of neurogenic scoliosis among patients with cerebral palsy is crucial for planning comprehensive health care, conducting regular screening for faster diagnosis, creating special scoliosis surveillance programs for children with cerebral palsy, and analyzing the risk in individual patients [9].
2. Materials and Methods
A questionnaire survey was conducted, targeting parents or legal guardians of children with cerebral palsy. It was conducted at the Department of Orthopedics and Traumatology and the Center for Technically Assisted Rehabilitation, the W. Degi Orthopedic and Rehabilitation Clinical Hospital, the Treatment and Rehabilitation Center “Always Together” and the Special School Complex No. 103 in Poznan. The purpose of its conduct was to obtain answers to information on the specificity of the disorders occurring and to assess the methods of improvement used in children with cerebral palsy according to the opinion of their parents. The criterion for inclusion in the survey was the presence of a parent or legal guardian of a child with cerebral palsy. The study was conducted between April 2023 and October 2023.
All the information obtained and the medical data on the patients’ conditions were obtained from previously collected hospital medical records and during an interview with the patients’ parents. The patients were examined in the ward. The acquisition of collected patient data was preceded by the consent of the patients’ legal guardians.
The present study was approved by the Bioethics Committee No. 311/23 on 6.04.2023. Due to the successful application for the research experiment, mandatory liability insurance was purchased for the entity conducting the medical experiment (policy number: COR395955).
There were 133 children in the study group, ranging in age from 3 to 17 years, where the median age was 9. The mean age in the study group was 9.7, while the standard deviation was 3.8. Among the study group there were also children born prematurely. The group included 77 premature babies, that is, babies born before 37 weeks of gestation. Extremely extreme preterm infants (babies born between 22 and 27 weeks’ gestation) were 20, while extreme preterm infants (babies born between 28 and 31 weeks’ gestation inclusive) were 27. The average age of birth of the babies fell at 34 weeks’ gestational age. The standard deviation was equal to 5.4.
Analyzing birth weight, 18 patients had extremely low birth weight, that is, less than 1000g. Extremely low birth weight, that is, above 1000g and below 1500g presented 23 patients. Low birth weight, that is, above 1499g and below 2500g, had 35 patients. The average birth weight of the patients was 2213g (min. 530g, max. 4500g). The standard deviation value was equal to 993.6g.
Among the 133-patient group, 9 patients were GMFCS level I, 55 patients GMFCS level II, 18 patients GMFCS level III, 22 patients GMFCS level IV and 29 patients GMFCS level V (Gross Motor Function Classification System).
In the study group, there were 24 patients who developed hip dislocation and 23 patients who developed hip dysplasia. The incidence of hip dislocation varied according to the patient’s GMFCS level. Hip dislocation occurred in: 4 patients with GMFCS 2, 1 patient with GMFCS 3, 6 patients with GMFCS 4, and 13 patients with GMFCS 5. There were no hip dislocations among the study group of patients with GMFCS 1. Pearson’s linear correlation coefficient was 0.4.
The data of the child, the mother and the influence of external factors on the child’s health were evaluated in the patient group of the survey. Parents’ opinions on the physiotherapeutic methods used in the treatment of children with cerebral palsy were also surveyed. Questions directed at obtaining the child’s data included the child’s gender, current weight and height, the child’s weight at birth, what week the child was born, fetal, perinatal and postnatal risk factors, and the child’s Apgar scale score. The Apgar scale is a 10-point scale that assesses a newborn’s vital functions and is performed at 1 and 5 minutes of life. Such parameters as skin coloration, heart rate, reflexes, muscle tone and respiration are evaluated. For each activity the baby can get 0-2, then the points are added up. A certain number of summed points indicates successively: 10-8 very good condition of the body, not requiring treatment; 4-7 medium condition; and 0-3 severe, life-threatening condition of the child. The corresponding groups of scale values were assigned to 3 groups, where group 1 meant a score of 0 to 3 points, group 2 meant 4 to 7 points received, and group 3 meant 8 to 10 points on the Apgar scale. Responses were also obtained regarding the child’s nutritional status (whether the patient has problems eating solid foods) or the presence of eating disorders, the time of diagnosis of cerebral palsy, the level of GMFCS, the form of cerebral palsy or the presence of comorbidities or other disorders. On the other hand, questions directed at obtaining the mother’s data included her age at delivery and the current age range she is in. Questions about the child’s therapy methods mainly concerned the frequency of rehabilitation performed and the use of specific kinesitherapy and physical therapy methods.
3. Results
Statistica version 13.3 software was used for statistical analysis. To enable more accurate analysis of the data obtained, some of the responses were coded accordingly and a nominal scale was used. Responses to the yes/no survey questions were assigned in such a way that a value of 0 meant a negative answer, while a value of 1 was assigned to a positive answer. Responses regarding the most effective physical therapy and kinesitherapy methods according to parents’ opinions were also coded appropriately to allow the most common answers given by parents of children with cerebral palsy to be shown.
Spearman rank order correlations were used to test the relationship between Apgar scale scores and age of diagnosis of cerebral palsy. Statistically significant values were the results if p<0.05. The p-value was 0.001421, which means that there is a relationship between the Apgar scale scores the patient received at birth and the age of diagnosis of cerebral palsy.

Table 1.
Study of the relationship between Apgar scores and age of diagnosis of cerebral palsy.
| Korelacja porządku rang Spearmana | ||||
|---|---|---|---|---|
| N Ważnych |
R Spearman |
t(N-2) | p-Value | |
| Apgar score & time of diagnosis of CP | 133 | 0,273912 | 3,259739 | 0,001421 |
Note: p-value less than 0.05 (statistically significant) are in bold; R – Spearman rank correlation coefficient.
To analyze the relationship between GMFCS level and the incidence of neurogenic scoliosis, the Mann-Whitney U Test was used. The analysis assumed a statistical significance coefficient of a=0.05, and the results were statistically significant when p<0.05.According to the test, the p-value was 0.144726, which indicated that there was no relationship between the two factors studied.
Table 2.
Study of the relationship between GMFCS levels and the incidence of neurogenic scoliosis.
| Test U Manna-Whitneya (z poprawką na ciągłość) Względem zmiennej: skolioza neurogenna. Zaznaczone wyniki są istotne z p <,05000 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sum.rang Grupa 1 |
Sum.rang Grupa 2 |
U | Z | p | Z popraw. |
p-Value | N ważn. Grupa 1 |
N ważn. Grupa 2 |
2*1str. dokł. p |
||
| GMFCS | 7064,500 | 1846,500 | 1069,500 | -1,39250 | 0,163771 | -1,45842 | 0,144726 | 109 | 24 | 0,163869 | |
Note: p-value less than 0.05 (statistically significant) are in bold.
To test the existence of a relationship between the incidence of neurogenic scoliosis in a patient with cerebral palsy and hip dysplasia, the Chi-square Test was used, where the value was statistically significant if p<0.05. The p-value obtained was 0.0217 and thus statistically significant, proving that there is a relationship between the incidence of hip dysplasia and the incidence of neurogenic scoliosis in the study group. On the other hand, in the case of the relationship between the incidence of neurogenic scoliosis and hip dysplasia, also using the Chi-square Test, the p-value was 0.1176, so the existence of a relationship between the two factors was not demonstrated.
Table 3.
Study of the relationship between the presence of neurogenic scoliosis and the presence of hip dysplasia.
Table 3.
Study of the relationship between the presence of neurogenic scoliosis and the presence of hip dysplasia.
| Kolumna1 | Kolumna2 | ||
|---|---|---|---|
| Chi-kwadrat (df=1) | 5,27 | p = ,0217 |
In order to confirm the hypothesis that there is a relationship between BMI value and the incidence of hip dislocation, the Mann-Whitney U Test was again used. The analysis assumed a statistical significance coefficient of a=0.05, hence the results were statistically significant if p<0.05. The value of the difference was p=0.000977, which proved that the results were statistically significant and there was a relationship between BMI value and the incidence of hip dislocation.
Table 4.
Study of the relationship between BMI value and the incidence of hip dislocation.
| Test U Manna-Whitneya (z poprawką na ciągłość) Względem zmiennej: podwichnięcie bioder. Zaznaczone wyniki są istotne z p <,05000 | |||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Sum.rang Grupa 1 |
Sum.rang Grupa 2 |
U | Z | p | Z popraw. |
p-Value | N ważn. Grupa 1 |
N ważn. Grupa 2 |
2*1str. dokł. p |
||
| BMI | 7867,000 | 1044,000 | 744,0000 | 3,296957 | 0,000977 | 3,297007 | 0,000977 | 109 | 24 | 0,000782 | |
Note: p-value less than 0.05 (statistically significant) are in bold.
In order to verify which of the kinesiotherapy methods used in the child’s therapy to date were the most effective, the data was sorted and calculated accordingly. The most common answer given by the respondents was SI therapy, which was considered to be the therapy that caused the greatest effect in the child’s therapy, according to the child’s existing needs at the time. However, as for the methods used in the child’s therapy in the field of physical therapy, the most frequently mentioned method was hydrotherapy, which, according to the parents’ opinion, had a very positive effect on the relaxation of spastic muscles.
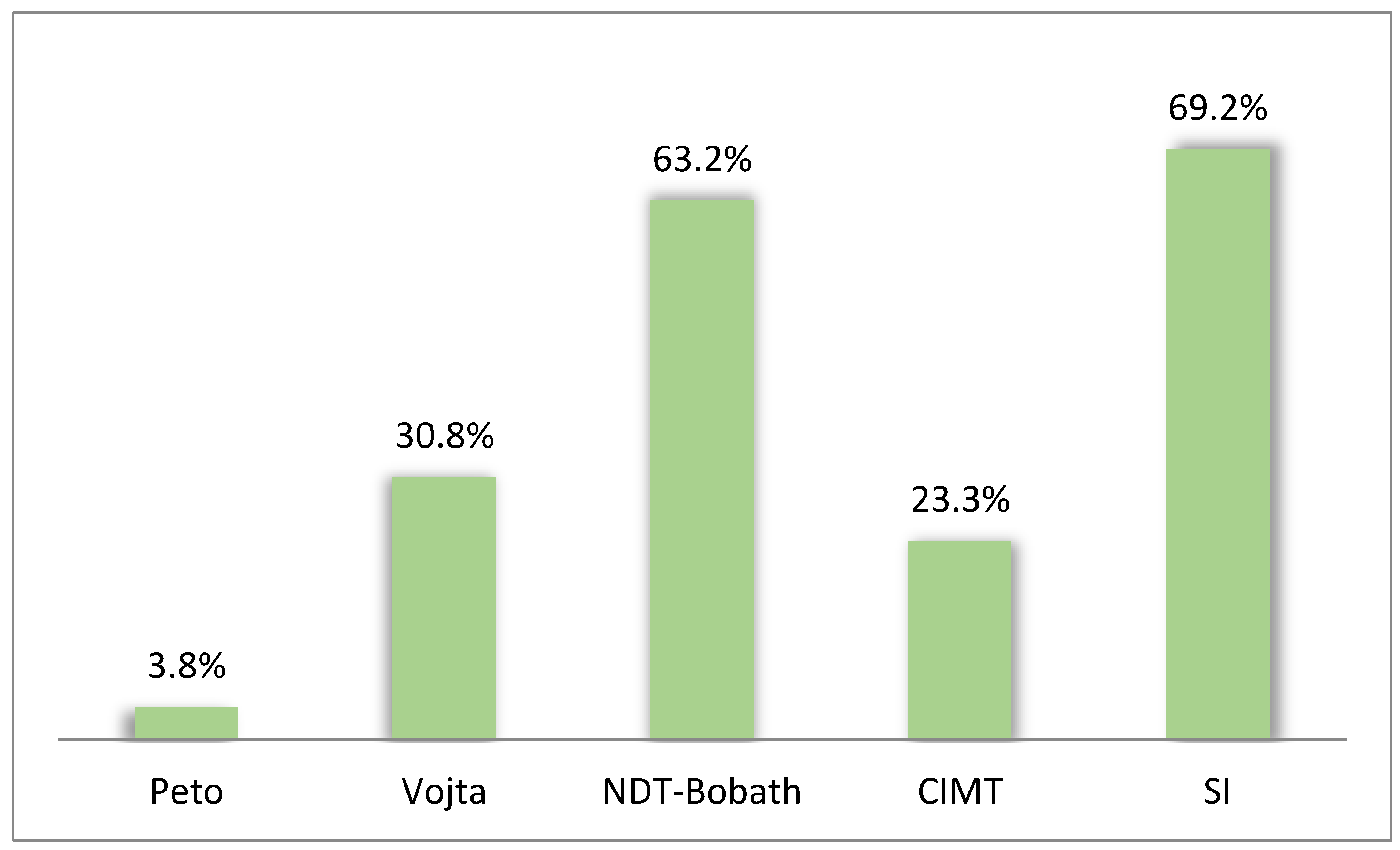
The most common methods in the field of physiotherapy used in the treatment of children with cerebral palsy were, in turn, SI therapy (69.2%), NDT-Bobath Method (63.2%), Vojta Method (30.8%), CIMT (23.3%), Peto Method (3.8%).
Figure 1.
Most frequently used methods in therapy of children with cerebral palsy according to parents’ opinions.
Figure 1.
Most frequently used methods in therapy of children with cerebral palsy according to parents’ opinions.
4. Discussion
The incidence of neurogenic scoliosis in children with cerebral palsy increases as the level of motor functioning decreases, i.e., as the level of GMFCS increases [22]. Based on a study conducted on a group of 11 patients with cerebral palsy, a similar relationship can be observed. A greater Cobb angle occurred in patients with a higher GMFCS level, that is, with an increase in the level of locomotor disability. Risk factors for scoliosis growth and progression are an initial high Cobb angle, a Cobb angle of ≥ 30 degrees at age 10, and GMFCS level V [22]. More severe scoliosis is much more common in sedentary children, who often do not move independently [22]. In a study of 206 patients (86 girls and 120 boys), recruited from the Norwegian Cerebral Palsy Quality and Surveillance Registry, severe scoliosis was found among 80 of the 206 patients and the distribution regarding its prevalence at different GMFCS levels was as follows: GMFCS level V - 62%, level IV - 19%, level III - 6%. The rate of scoliosis progression increased significantly faster and much more effectively in patients with GMFCS level V, compared to patients with GMFCS level IV. Among the 50 children with GMFCS III, 20% had a curvature angle of ≥ 10 degrees and 6% of ≥ 40 degrees. Of the 47 GMFCS IV-level children, 47% of patients had a curvature angle of ≥ 10 degrees, while 19% of patients had a curvature angle of ≥ 40 degrees. Among the 109 GMFCS V patients, there were 82% of children with a curvature of ≥ 10 degrees and as many as 62% with a curvature angle of ≥ 40 degrees [22].
Based on clinical and radiographic findings in a prospective registry study in the Swedish Cerebral Palsy Patient Surveillance Program, which aims to monitor and prevent hip dislocations, contractures and deformities in children with cerebral palsy, the frequency and severity of scoliosis also increased with GMFCS level, from 0.1% in children with GMFCS I to 42-55% in children with GMFCS V. More frequent scoliosis was observed in younger patients with higher GMFCS levels, while the incidence of scoliosis increased with age and the level of large motor development expressed on the GMFCS scale. Among children at 10 years of age, moderate or severe scoliosis was seen in: about 1% of patients with GMFCS I-II, 5% with GMFCS III, 10% with GMFCS IV, and 30% with GMFCS V. After 10 years, the percentages of patients with moderate or severe scoliosis were, respectively: 5%, 30%, 45%, 80%, showing that the incidence and progression of scoliosis increases with age [11]. Among the study group, it could also be observed that a higher Cobb angle of scoliosis is definitely more common in older children than in younger ones, which may indicate an upward trend in the angle of lateral curvature of the spine with age. However, in order to observe the changes and confirm the hypothesis, it would be necessary to conduct further studies in this direction, over a longer period of time and with the inclusion of a larger number of patients.
The rate of scoliosis progression in a study on the relationship of the level of the Functional Large Motor Classification Scale (GMFCS) and hip dysplasia to the pattern and progression of scoliosis in children with cerebral palsy, in the group of patients with GMFCS I-III was 5.8%, with GMFCS IV was 5.6%, while in the group of patients with GMFCS V was 12.5% (percentage progression per year based on a linear curve progression model) [23].
The authors of the study noted an increase in the prevalence and severity of scoliosis with increasing GMFCS levels and age [9]. In a study based on 7200 measurements, a group of 666 children with cerebral palsy between the ages of 4 and 18 were surveyed during annual health care program examinations [9]. Based on the results collected, a trend was also noted for the number of children with cerebral palsy and neurogenic scoliosis to increase with the level of GMFCS [9]. The majority of children with moderate to severe scoliosis, and with a curvature of more than 20° were at GMFCS levels III-V, while all operated scoliosis predominated among children with GMFCS IV-V. The risk of progression of neurogenic scoliosis among the patients studied also increased with age. Among children at GMFCS levels IV-V, it was about 50% at age 18. However, there is no statistically significant relationship between the risk of scoliosis progression and the subtype of cerebral palsy [9].
The present survey study did not show a similar relationship between the GMFCS level of a patient with cerebral palsy and the presence of neurogenic scoliosis. This may be due to the lack of X-rays among the patients surveyed or the lack of regular screening, whereby postural abnormalities can be detected through visual assessment of the patient and measurements with a scoliometer, and then radiography can be ordered for further diagnosis. Parents of children with cerebral palsy at GMFCS levels 4 and 5 often focus attention on other comorbid disorders associated with cerebral palsy that, at any given time, create greater difficulties for the child in daily functioning, hence scoliosis may become a secondary concern. Spastic patients were the larger group in the survey. According to a cohort study of 292 patients with cerebral palsy, the frequency and severity of neurogenic scoliosis were associated with dystonic movement disorders [24]. Severe spinal curvature, in which the Cobb angle was >40°, was more likely in patients with dystonia than with spasticity [24]. This is further supported by the fact that spasticity facilitates stabilization of body segments and an antigravity effect, resulting in the maintenance of an upright trunk position [25].
It has been noted that there is a correlation between hip dysplasia and co-occurring neurogenic scoliosis. During a 5-year study based on data from the Swedish Cerebral Palsy Surveillance Program in children from southern Sweden, out of 337 patients, scoliosis was found with present pelvic malalignment in the form of pelvic obliquity in 38 children [26]. The symptoms of hip dysfunction present also included asymmetric hip inversion, which was present in 45 children. Also, an increase in GMFCS level had an impact on the occurrence of pelvic obliquity. 29% of patients had pelvic obliquity in combination with mild scoliosis, with moderate scoliosis and pelvic obliquity there were already 43% of patients, while the highest number, 60% of patients, were with severe scoliosis. In the studies conducted, pelvic obliquity also tended to occur on the opposite side to the convexity of the spinal curvature, and to occur on the side with the greatest hip joint displacement and reduced hip inversion range [26,27].
In a study conducted on a population of 656 patients, including 524 patients with scoliosis and pelvic obliquity, it was noted that, the presence of pelvic obliquity often co-occurs with spinal curvature. They speculated the fact that individual scoliotic curves appear as compensatory mechanisms for the pelvic obliquity present. Knowledge of this subject is particularly important for planning spinal or pelvic correction surgery, as this procedure can negatively disrupt the compensatory relationship between pelvic parameters and lumbar spine deformity [27].
Deficiencies in body weight, body fat or muscle tissue can have an impact on the development of joint abnormalities in the normal function of the hip joint, among others [28]. However, the direct influence on hip dislocation in a study conducted in a group of 18 patients with cerebral palsy in Stockholm, was not body weight, but the occurrence of spasticity in the patients, which is the most important variable affecting joint dislocation, time spent standing in a brace was found to be the second most important variable [28]. This is explained by the fact that the main cause of hip dislocation is a change caused by spastic muscle forces acting on the femoral head in the acetabulum [28]. These forces can be stronger when the child is in a standing orthosis (the Standing Shell), in which he or she is strapped in and the knee and pelvic joints cannot move. Muscle force can be focused on the hip joint and cause hip dislocation [28]. The present study showed that the higher the BMI value, the higher the incidence of hip dislocation in children with cerebral palsy, indicating that not only malnutrition, but also excessive body weight may be related to hip dislocation.
Younger patients with cerebral palsy have a higher risk of postoperative complications. Patient malnutrition and comorbidities are also factors contributing to the increased risk of complications. Because of recent doubts about conservative treatment, which involves the use of orthotic devices, botulinum toxin or adductor surgery, and the effective results of surgical treatment in patients with severe cerebral palsy, hip reconstruction surgery is an acceptable and often unavoidable form of patient treatment [29]. Surgical treatment of the hip joint in patients with cerebral palsy makes it possible to improve the function of independent walking and correct contracted structures, provides lasting treatment results and brings significant pain relief, as well as functional improvement among patients [30].
Risk factors for scoliosis progression in spastic patients include a high angle of spinal curvature before the age of 15 (angle ≥ 40 degrees), total body occupation or being in a supine position only [31]. Severe scoliosis is more likely in patients with intractable epilepsy, poor large motor functional assessment scores, limb spasticity and a history of previous hip surgery [32]. Among children with cerebral palsy, those with moderate to severe spasticity involving most of the body have a higher risk of hip dislocation, scoliosis, hip and spine surgery rates and mortality. Injection of botulinum toxin BTX-A, which is designed to reduce muscle tension by inactivating the neuromuscular plaque, in children with cerebral palsy according to a study conducted in Taiwan using information from the Taiwan National Insurance Health Research Database, did not significantly reduce hip dislocation and scoliosis, while it is further considered a safe treatment for spasticity, which can positively affect patient function [14,33].
The present study proves the existence of a relationship between Apgar scale scores at birth and the age of diagnosis of cerebral palsy. In a study conducted at the Department of Pediatric Cardiology and General Pediatrics at the Medical University of Warsaw, it was noted that a low Apgar score, which assesses a newborn’s vital functions at birth, measured immediately after birth and 5 minutes after birth may indicate an increased risk of cerebral palsy. Among the patients studied, 70% had reduced Apgar scores immediately after birth, while 36% of the newborns still had reduced scores 5 minutes after birth. It was also found that there was no significant association between scores obtained just after birth and the incidence of cerebral palsy among this group of patients. However, low Apgar scores 5 minutes after birth had an impact on the increased risk of developing cerebral palsy among patients. Birth factors resulting in the award of a low score can cause damage to the nervous system, which subsequently increases the risk of developing cerebral palsy [3]. In a cohort study on the relationship of cerebral palsy with Apgar scale scores in low- and normal-birth-weight infants, based on the results of pooled data from the Norwegian Childhood Cerebral Palsy Registry, it was found that an increased risk of cerebral palsy was also seen among normal-birth-weight infants with low Apgar scale scores 5 minutes after birth, but to a lesser extent among low-birth-weight infants [34]. Also, a strong association between low Apgar scores with death and increased risk of cerebral palsy was found in a population-based cohort study conducted in Norway, in which Apgar scores at the first and fifth minutes ranged from 0 to 3, the risk of neonatal death and cerebral palsy was increased 642-fold and 145-fold, respectively, compared with scores of 7 to 10. Among the group of patients who scored 0-3 on the Apgar scale 5 minutes after birth and survived beyond 1 year of age, 6.8% received services for cerebral palsy at 8 to 12 years of age. Based on the results, it can be seen how important the Apgar scale score is for the early identification of infants at increased risk of serious disorders [35].
The study showed that of the methods most frequently mentioned in the responses of those surveyed and one of the most popular physiotherapy methods to supplement the therapy of children with cerebral palsy was hydrotherapy. This method has positive applications in the treatment of this group of patients. Hydrotherapy interventions should be used as a complementary method of treatment and rehabilitation along with other conventional rehabilitation methods. Such a combination positively influences the development of large motor skills and brings joy among children to physical activity [36]. Hydrotherapy, thanks to the buoyancy properties of water and the reduction of gravity, has an effect on relieving pressure in the joints, which positively affects the quality of exercises performed during therapy. It is also used to alleviate sensory system disorders, as well as to reduce muscle tissue tension. With the use of this method as a complementary therapy in the rehabilitation of patients, a significant improvement in gait, improvement in cardiovascular function during exercise or improvement in static and dynamic balance from a seated position is also noted [37].
The most common methods used in the therapy of children with cerebral palsy also turned out to be the SI method, the NDT-Bobath method and the Vojta method, among others. The aim of the aforementioned methods is to support normal development and strive to achieve the greatest possible independence for the patient. It has been noted that Sensory Integration (SI) therapy has positive effects in improving gait, balance, and gross motor functions. Improvements in the senses of vision, touch and prioception improve mobility and maintain correct posture, and are much needed in learning new motor skills. With therapy, it is possible to improve gait pattern, postural stability or postural control [38]. Training based on the NDT-Bobath method also has an impact on correct posture and balance maintenance. The results of a study conducted at Pamukkale University, School of Physiotherapy and Rehabilitation in Turkey, showed that this therapy improved the functional motor level among patients with hemiparesis, making the patients’ gait faster and safer than before the therapy [39]. The Vojta method also has an impact on the development of motor skills and performance of daily activities [40]. All of these measures enable functional independence and participation in social life, which definitely improves patients’ quality of life.
5. Conclusions
1. There is a relationship between the Apgar scale scores received by the patient just after birth and the age of diagnosis of cerebral palsy.
2. There is no relationship between the level of psychomotor development expressed on the GMFCS scale and the incidence of neurogenic scoliosis in children with cerebral palsy.
3. There is a relationship between the incidence of neurogenic scoliosis and hip dysplasia.
4. There is a relationship between the child’s BMI value and the incidence of hip dislocation in patients with cerebral palsy.
5. According to parents, the most effective method from the field of kinesitherapy used in the therapy of patients turns out to be SI therapy, which is a therapy that supports the development of patients with cerebral palsy, while thanks to it parents notice satisfactory results.
6. The most effective method from the field of physical therapy, which is used in the therapy of patients with cerebral palsy, turns out to be hydrotherapy. It has a positive impact on the effects of the child’s therapy according to the parents’ opinion.
7. Among the most frequently mentioned methods commonly used in the therapy of children with cerebral palsy, special attention can be paid to SI therapy, which, as a method that aids children’s development, accounted for 69.2% of respondents’ answers. Other methods used in therapies with children with cerebral palsy were the NDT-Bobath Method (63.2%), the Vojta Method (30.8%), CIMT (23.3%) and the Peto Method (3.8%).
Author Contributions
Conceptualization, Marta Rosik and Roksana Malak; Data curation, Dorota Sikorska; Formal analysis, Marta Rosik; Funding acquisition, Włodzimierz Samborski and Przemysław Daroszewski; Investigation, Marta Rosik; Methodology, Marta Rosik; Project administration, Roksana Malak; Resources, Włodzimierz Samborski; Software, Dorota Sikorska; Supervision, Włodzimierz Samborski and Roksana Malak; Validation, Włodzimierz Samborski, Przemysław Daroszewski and Roksana Malak; Visualization, Marta Rosik; Writing–original draft, Włodzimierz Samborski and Roksana Malak; Writing–review & editing, Włodzimierz Samborski, Dorota Sikorska and Roksana Malak. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by Bioethics Committee (consent reference number 2023/23 on the 9th of March 2024) Poznań University of Medical Sciences, Poznań, Poland.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Włodzisław Kuliński, Krzysztof Zeman (red.) przy współpracy Teresy Orlik. Fizjoterapia w Pediatrii, PZWL; Warszawa: 2014.
- Vitrikas K, Dalton H, Breish D. Cerebral Palsy: An Overview. Am Fam Physician. 2020 Feb 15;101(4):213-220. [PubMed]
- Milewska, Agnieszka, et al. “Analiza czynników ryzyka mózgowego porażenia dziecięcego.” Nowa Pediatria 4 (2011): 79-84.
- Graham HK, Rosenbaum P, Paneth N, et al. Cerebral palsy. Nat Rev Dis Primers. 2016 Jan 7;2:15082. [CrossRef] [PubMed] [PubMed Central]
- Krigger, KW. Cerebral palsy: an overview. Am Fam Physician. 2006 Jan 1;73(1):91-100. [PubMed]
- Sadowska M, Sarecka-Hujar B, Kopyta I. Analysis of Selected Risk Factors Depending on the Type of Cerebral Palsy. Brain Sci. 2021 Oct 30;11(11):1448. [CrossRef] [PubMed] [PubMed Central]
- Madigan RR, Wallace SL. Scoliosis in the institutionalized cerebral palsy population. Spine (Phila Pa 1976). 1981 Nov-Dec;6(6):583-90. [CrossRef] [PubMed]
- Sawin PD, Menezes AH. Neuromuscular scoliosis: diagnostic and therapeutic considerations. Semin Pediatr Neurol. 1997 Sep;4(3):224-42. [CrossRef] [PubMed]
- Persson-Bunke M, Hägglund G, Lauge-Pedersen H, Wagner P, Westbom L. Scoliosis in a total population of children with cerebral palsy. Spine (Phila Pa 1976). 20 May 2012 ;37(12):E708-13. [CrossRef] [PubMed]
- Koop, SE. Scoliosis in cerebral palsy. Dev Med Child Neurol. 2009 Oct;51 Suppl 4:92-8. [CrossRef] [PubMed]
- Hägglund, Gunnar, et al. “Incidence of scoliosis in cerebral palsy: a population-based study of 962 young individuals.” Acta Orthopaedica 89.4 (2018): 443-447.
- Kasperczyk, T. Wady postawy ciała, diagnostyka i leczenie, Wyd. FHU Kasper, Kraków, 2002.
- Vialle R, Thévenin-Lemoine C, Mary P. Neuromuscular scoliosis. Orthop Traumatol Surg Res. 2013 Feb;99(1 Suppl):S124-39. Epub 2013 Jan 19. [CrossRef] [PubMed]
- Małgorzata Domagalska-Szopa, Andrzej Szopa. Postępowanie usprawniające w mózgowym porażeniu dziecięcym, Edra Urban & Partner; Wrocław: 2023.
- Cloake T, Gardner A. The management of scoliosis in children with cerebral palsy: a review. J Spine Surg. 2016 Dec;2(4):299-309. [CrossRef] [PubMed] [PubMed Central]
- McAviney J, Roberts C, Sullivan B,. The prevalence of adult de novo scoliosis: A systematic review and meta-analysis. Eur Spine J. 2020 Dec;29(12):2960-2969. Epub 2020 May 22. [CrossRef] [PubMed]
- Koop SE, Lonstein JE, Winter RB, Denis F. The Natural History of Spine Deformity in Cerebral Palsy. Scoliosis Research Society Annual Meeting, September 1991.
- Dariusz, Białoszewski; et al. (red). Fizjoterapia w Ortopedii, PZWL; Warszawa: 2015.
- Kobylińska M, Malak R, Majewska K, Kędzia A, Samborski W. Assessment of anterior-posterior spinal curvatures in children suffering from hypopituitarism. BMC Endocr Disord. 2019 Dec 11;19(1):137. [CrossRef] [PubMed] [PubMed Central]
- Kobylińska M, Malak R, Majewska K, Fechner B, Samborski W, Kędzia A. Angle of trunk rotation in children suffering from growth hormone deficiency. Pediatria Polska - Polish Journal of Paediatrics. 2023;98(1):30-35. [CrossRef]
- Suken, A. Shah, MD Pediatric Orthopaedic and Scoliosis Surgery Department of Orthopaedics 1600 Rockland Road, PO Box 269 Wilmington, DE 19899 302-651-5904.
- Vinje, Svend, Terje Terjesen, and Thomas Kibsgård. “Scoliosis in children with severe cerebral palsy: a population-based study of 206 children at GMFCS levels III–V.” European Spine Journal 32.11 (2023): 4030-4036.
- Garg, Sumeet, et al. “The relationship of gross motor functional classification scale level and hip dysplasia on the pattern and progression of scoliosis in children with cerebral palsy.” Spine Deformity 1.4 (2013): 266-271.
- 24. Willoughby KL, Ang SG, Thomason P, Rutz E, Shore B, Buckland AJ, Johnson MB, Graham HK. Epidemiology of scoliosis in cerebral palsy: A population-based study at skeletal maturity. J Paediatr Child Health. 2022 Feb;58(2):295-301. Epub 2021 Aug 28. Erratum in: J Paediatr Child Health. 2022 Apr;58(4):743. doi: 10.1111/jpc.15943. PMID: 34453468; PMCID: PMC9291795. [CrossRef] [PubMed] [PubMed Central]
- Manikowska, Faustyna, Marek Jóźwiak, and Maciej Idzior. “Wpływ nasilenia spastyczności na możliwości funkcjonalne dziecka z mózgowym porażeniem.” Neurologia Dziecięca 18.36 (2009): 31-35.
- Hägglund, G. Association between pelvic obliquity and scoliosis, hip displacement and asymmetric hip abduction in children with cerebral palsy: a cross-sectional registry study. BMC Musculoskelet Disord. 2020 Jul 14;21(1):464. [CrossRef] [PubMed] [PubMed Central]
- Radcliff, Kristen E., et al. “Is pelvic obliquity related to degenerative scoliosis?.” Orthopaedic surgery 5.3 (2013): 171-176.
- Dalén, Ylva, et al. “Effects of standing on bone density and hip dislocation in children with severe cerebral palsy.” Advances in Physiotherapy 12.4 (2010): 187-193.
- Kraus, Manuel Johannes, Reinald Brunner, and Erich Rutz. Risk profile of bony intervention for hip displacement in our youngest cohort of children with cerebral palsy. Diss. Medizinische Fakultät der Universität Basel, 2019.
- Houdek MT, Watts CD, Wyles CC, Trousdale RT, Milbrandt TA, Taunton MJ. Total Hip Arthroplasty in Patients with Cerebral Palsy: A Cohort Study Matched to Patients with Osteoarthritis. J Bone Joint Surg Am. 2017 Mar 15;99(6):488-493. [CrossRef] [PubMed]
- Saito, Naoto, et al. “Natural history of scoliosis in spastic cerebral palsy.” The Lancet 351.9117 (1998): 1687-1692.
- Bertoncelli, Carlo M., et al. “Risk factors for developing scoliosis in cerebral palsy: a cross-sectional descriptive study.” Journal of child neurology 32.7 (2017): 657-662.
- Lin, Ching-Yueh, et al. “Long-term effect of botulinum toxin A on the hip and spine in cerebral palsy: A national retrospective cohort study in Taiwan.” PLoS One 16.7 (2021): e0255143.
- Lie, Kari Kveim, Else-Karin Grøholt, and Anne Eskild. “Association of cerebral palsy with Apgar score in low and normal birthweight infants: population based cohort study.” Bmj 341 (2010).
- Moster, Dag, et al. “The association of Apgar score with subsequent death and cerebral palsy: a population-based study in term infants.” The Journal of pediatrics 138.6 (2001): 798-803.
- Khalaji, Masoud, et al. “The effect of hydrotherapy on health of cerebral palsy patients: An integrative review.” Iranian Rehabilitation Journal 15.2 (2017): 173-180.
- Bairaktaridou, Aikaterini, et al. “The effect of hydrotherapy on the functioning and quality of life of children and young adults with cerebral palsy.” Int J Adv ResMed 3 (2021): 21-4.
- Warutkar VB, Krishna Kovela R. Review of Sensory Integration Therapy for Children With Cerebral Palsy. Cureus. 2022 Oct 26;14(10):e30714. [CrossRef] [PubMed] [PubMed Central]
- Tekin, Fatih, et al. “Effectiveness of Neuro-Developmental Treatment (Bobath Concept) on postural control and balance in Cerebral Palsied children.” Journal of back and musculoskeletal rehabilitation 31.2 (2018): 397-403.
- Senthilkumar, S., and P. Swarnakumari. “A study on Vojta therapy approach to improve the motor development of cerebral palsy children.” Int J Med Sci 4.1&2 (2011): 39-45.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



