
Submitted:
21 October 2024
Posted:
21 October 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Clinical microbiology studies and systematic reviews have largely concluded that SARS-CoV-2 RNA is rarely present in the urine of COVID-19 patients. Thus, wastewater surveillance has largely focused on human stool and defecation as the relevant matrix and behavior. But, the over-performance of wastewater testing during near-source surveillance, especially in settings where on-site defecation is presumed to be de minimis such as aircraft and non-residential schools, suggests the possibility of SARS-CoV-2 RNA input from a non-fecal source. To revisit the possibility of urine as an explanation, data was compiled from 45 studies reporting on SARS-CoV-2 RNA in the urine of 1,924 COVID-19 patients. In general, the reporting quality was low with most studies (86.7%) failing to report even basic details such as the volume of urine collected. Only 11 reported quantitative data and of these only a single study reported its experiments to the standards established for publication of quantitative PCR data. Taking the data at its face value, the pooled prevalence of urinary SARS-CoV-2 RNA shedding was 11.3% (95%CI: 8.4 - 14.3), which roughly agrees with previous analyses. However, the percentage of variability in the estimate attributable to heterogeneity between studies (I2 = 93.66%) warrants careful consideration. Notably, for the 8 studies reporting sufficient workflow information, the observed urinary RNA shedding prevalence was normally distributed (r2 = 1.00) as a function of the volume of urine being assayed in a single PCR reaction (i.e., the equivalent sample volume, ESV). The study achieving the highest ESV (83.3 µL of urine) detected SARS-CoV-2 RNA in urine sediments of 95.5% of COVID-19 patients. Conversely, during two studies achieving ESVs of only 2 µL and 11.7 µL of urine, SARS-CoV-2 RNA was not detected in the urine of 72 and 132 patients, respectively. For wastewater surveillance of COVID-19, these observations suggest the rarity of SARS-CoV-2 RNA in urine may be a methodological artifact. Further, the data on which rarity is presumed are of low quality. Beyond COVID-19, the findings demonstrate that clinical studies, by virtue of their design to answer clinically relevant questions, could produce datasets subject to large biases that make them less useful when assessing the feasibility of wastewater surveillance of infectious agents. Wastewater surveillance practitioners must carefully consider the appropriateness and limitations of clinical data considering the important differences between the methods and aims of the two disciplines. Given the great potential of wastewater testing, clinical and environmental microbiologist should collaborate to produce robust quantitative datasets for reliable feasibility assessments for both community and near-source public health surveillance.
Keywords:
environmental surveillance
; SARS-CoV-2
; urine
; wastewater surveillance
; public health
; equivalent sample volume
Pathogen Shedding and Wastewater Surveillance
The transmission of infectious agents from person to person is frequently initiated by the shedding of the agent (or its constituent parts) into the environment. Thus, the environment is a crucial venue for both the interruption of disease transmission and the observation of biological analytes associated with disease-causing microorganisms. To accomplish the first, in many places throughout the world human biological waste streams, including feces and urine, are collected from households via hydraulic systems and conveyed to wastewater treatment facilities. These engineered systems, by collecting and concentrating biological wastes from many people, afford an efficient opportunity for the second activity, the observation of biological analytes associated with disease, a subdiscipline of epidemiology known as environmental surveillance. Initial environmental surveillance efforts focused on enteric pathogens with an obvious link between fecal-associated transmission and presence in human sewage, such as Salmonella enterica[1] and poliovirus[2]. The historically prerequisite linkage between sewage as both a vehicle of transmission and a matrix for infectious disease surveillance was usurped in 2011 by the measurement of RNA from influenza A, a respiratory virus, in sewage in the Netherlands[3]. Now, the widespread application of environmental surveillance (also called wastewater surveillance or wastewater-based epidemiology) in response to the COVID-19 pandemic has firmly established sewage as a matrix for public health surveillance of a variety of respiratory pathogens, including SARS-CoV-2, influenza A, respiratory syncytial virus, and rhinoviruses[4,5]. Brendan Moore’s 1952 prediction concerning wastewater is prescient: “The methods used might be applied with advantage to… epidemiological studies of other infections in which the causative organism gains access to sewage” (emphasis mine)[6].
Since the body fluids from an infected individual are the means by which a biological analyte “gains access to sewage,” robust characterization of shedding dynamics is fundamental to the potential of wastewater surveillance for various infectious diseases. Traditionally, such characterizations have fallen under the purview of clinical microbiology. At the onset of the COVID-19 pandemic, clinical microbiologists measured the prevalence and abundance of SARS-CoV-2 RNA in different body fluids via RT-qPCR testing of clinical specimens[7,8]. These clinical data were then used to assess the feasibility and potential of COVID-19 wastewater surveillance and to estimate the prevalence of COVID-19 cases based on wastewater data[9,10]. The initial clinical data suggests that SARS-CoV-2 RNA in wastewater systems is most likely derived from feces and that shedding via urine is rare (circa 5%) among COVID-19 patients. Quantitative modeling of SARS-CoV-2 RNA emissions into sewers based on body fluid material balances premised on these data indicates community-level wastewater input is dominated by feces, but for near-source or building-level applications, urinary shedding, although rare, could contribute a detectable signal[11]. Most community-level SARS-CoV-2 wastewater surveillance presumes urinary inputs are negligible. Thus, fecal shedding dynamics and defecation behavior have been primary considerations for analyte input and quantitative links between wastewater data and caseload estimates[12].
Potential Role of a Non-Fecal Source in Near-Source Wastewater Surveillance
While neglecting urine may be reasonable at the community level, observations during near-source surveillance of COVID-19 invite scrutiny of a fecal-centric scenario. First are the observations of SARS-CoV-2 RNA in wastewater collected from commercial aircraft[13]. Not much is known about passenger bathroom behavior on such flights, but up to 36% of passengers report themselves as “likely to” defecate during long-haul flights[14]. But, during a study of 37 repatriation flights to Australia, 75% of flights with only a single incident COVID-19 case during arrival quarantine had SARS-CoV-2 RNA present in the wastewater[13]. The probability of observing 75% aircraft wastewater RNA positivity with a 36% likelihood of fecal shedding by a single onboard COVID-19 case is 2.5%, assuming a binomial distribution for the likelihood of defecating. Additional studies in the United Kingdom and the United States have observed 93% and 81% SARS-CoV-2 RNA positivity, respectively, in aircraft wastewater from arriving flights[15,16]. Because most aircraft wastewater systems discharge gray water from sinks overboard during flight via a drain mast, RNA detected in the aircraft wastewater must have entered via the lavatory toilets[17]. These observations suggest two possibilities – more passengers are defecating onboard than reported or there is a non-fecal route of RNA emission into lavatory toilets.
A fecal-centric wastewater input scenario for SARS-CoV-2 RNA is also worth revisiting, given observations during near-source surveillance of non-residential schools[18]. Again not much is known about the bathroom behavior of children at school, particularly whether or not school-age children defecate at school[19]. Nonetheless, wastewater from non-residential schools in a variety of settings has been consistently positive for SARS-CoV-2 RNA with up to 100% of samples from some sites containing RNA[20,21,22,23,24]. In one case, 67% of incident COVID-19 cases were associated with a RNA in the school wastewater[25]. The discrepancy between the consistent positivity of school wastewater and the assumed bathroom behavior of students indicates something is missing in our understanding of SARS-CoV-2 RNA input[26].
SARS-CoV-2 RNA in Urine: Literature Review and Data Extraction
Given the empirical observations during both aircraft and school wastewater surveillance of COVID-19, I hypothesized that previous conclusions about the presence of SARS-CoV-2 RNA in the urine of COVID-19 patients are potentially erroneous. To test this hypothesis, I sought to examine published datasets on SARS-CoV-2 RNA in urine with attention toward the prevalence and abundance of SARS-CoV-2 RNA in the urine of COVID-19 patients, the quality of the quantitative information as indicated by the reporting metrics, and the characteristics of the microbiological workflows used. To identify relevant literature, on 14 September 2023, I searched PubMed using the string “((SARS-CoV-2) AND (RNA)) AND (urine)”, which yielded 166 results. Inclusion criteria were primary literature or reviews published in the peer-reviewed literature and reporting SARS-CoV-2 RNA data in urine from two or more patients diagnosed with COVID-19 at the time of specimen testing. Importantly, the current analysis should not be interpreted to be a systematic review and meta-analysis but is instead a compilation of readily available data to characterize the strengths and limitations of wastewater surveillance as has been done previously for shedding pathways, caseload estimates, and feasibility[9,11]. Title, abstract, and full-text screening led to the exclusion of 83 studies that did not report data from urine, 7 publications reporting data for individual case reports, 4 studies of convalescent patients or patients never diagnosed with COVID-19, 3 method comparisons, 1 review of infectivity, 1 editorial, and 1 pre-print that duplicated a peer-reviewed manuscript. The remaining studies included 28 publications reporting primary datasets and 15 reviews. When a primary source from a review paper was not included in the literature identified by the PubMed search, I added it to the primary source list. The final analysis included 45 studies reporting primary data (28 from the initial PubMed search and 17 additional studies acquired from review papers).
Previous Reviews of SARS-CoV-2 RNA Shedding in Urine
As mentioned previously, early reviews of clinical datasets suggest that SARS-CoV-2 RNA in the urine of COVID-19 patients is rare[27,28]. Exact estimates of urinary shedding prevalence varied, with some meta-analyses finding no urine samples positive for RNA among COVID-19 patients, while others estimated positivity rates as high as 16.4%[29,30,31]. The majority of meta-analyses estimated urinary RNA shedding prevalence from 6 to 10% among COVID-19 patients, although when studies with patient sample sizes less than 9 were excluded, the prevalence decreased to as low as 1%[32,33,34,35,36]. Despite its rarity, some studies noted that urinary shedding of RNA could persist longer than respiratory shedding among some patients[37]. Important sources of uncertainty in the prevalence estimates include matrix effects associated with the difficulty of urine for PCR-based methods, methodological variation, and the low to moderate data quality in early clinical studies[27,29,33]. Notably, no single review or meta-analysis published to date included all the primary studies identified during the current literature search, which included several clinical studies published as late as 2022 and 2023, well after most of the previous reviews were published. Thus, the current review aims to add new insights and nuance to our understanding of SARS-CoV-2 RNA in urine and its implications for wastewater surveillance.
SARS-CoV-2 RNA Urinary Shedding Prevalence Revisited
Based on primary data from 45 studies (Table S1), I estimated a pooled prevalence of SARS-CoV-2 shedding in urine on a per-patient basis (i.e., not by specimen). In studies where multiple specimens were collected from single patients, a patient was considered positive when any specimen tested positive for RNA. In studies where urine specimens were collected from a subset of patients, the shedding prevalence was recorded based on the number of unique patients tested (Table S1 column “patients sampled”). In studies reporting results stratified by multiple analytical methods (e.g., qPCR and dPCR, or qPCR and LAMP) or population immune status, the resulting prevalence was considered separately for each method or subpopulation. The pooled shedding prevalence (a proportion) was estimated using a Der Simonian-Laird binary random effects model executed in Open Meta Analyst software 12.11.4 (http://www.cebm.brown.edu/openmeta/)[38,39]. Among the 1,924 patients included in the included studies, 173 tested positive for SARS-CoV-2 RNA in their urine (Figure S1). The pooled estimate of the SARS-CoV-2 urinary shedding prevalence among COVID-19 patients in the 45 included studies is 11.3% (95% CI: 8.4 - 14.3).
While the shedding prevalence estimated here is not meaningfully different from previously published estimates, one feature of the analysis is striking – the inter-study heterogeneity, as assessed via the I2 statistic. The I2 statistic describes the percentage of variability in the pooled estimate that is due to heterogeneity rather than random chance. In this case, the I2 statistic is 93.66% (p < 0.001), suggesting most of the variability in SARS-CoV-2 RNA urinary shedding prevalence is attributable to clinical and methodological diversity between studies. Considering these two sources of variation between studies offers the opportunity to develop new hypotheses concerning the status of SARS-CoV-2 RNA in urine.
Clinical Diversity: Study Population
One potential source of the heterogeneity in the prevalence of SARS-CoV-2 RNA urinary shedding is the various subpopulations of COVID-19 patients that have been under study. Of the 45 studies included in the current analysis, 26 described the study population as COVID-19 patients. Presumably, such patients were symptomatic and diagnosed with COVID-19, although fully specified inclusion criteria are missing in most studies. Notably, five studies included no precise description of the relevant study population. Only one study stratified between symptomatic and asymptomatic patients[40]. The authors reported asymptomatic patients exhibited higher SARS-CoV-2 RNA loads than symptomatic patients and found that 1 in 15 asymptomatic patients had RNA in their urine, while none of the 45 symptomatic patients did[40]. Only three studies sampled urine from children, with one study consisting of a neonate and their mother[41,42,43]. Only the neonate tested positive for SARS-CoV-2 RNA in their urine[41], while among the 15 children in the other two studies, none had RNA detected in their urine[42,43]. Although the sample size is limited, these preliminary results suggest that urinary shedding among children with COVID-19 is possibly rarer than the pooled estimate from all studies.
Perhaps the most important subpopulation is those with severe COVID-19. Four studies tested urine samples from patients with severe or very severe disease or intensive care unit (ICU) patients[44,45,46,47]. The prevalence of urinary RNA shedding among these patients was none (n = 2)[45], 7.4% (n = 81)[46], 16.3% (n = 135)[47], and 95.5% (n = 22)[44]. For patients with long-term COVID-19 symptoms, Tejerina et al. found that 13.8% of patients had SARS-CoV-2 RNA detected in their urine[48]. The results from these few studies do not demonstrate a systematic bias relative to the pooled estimate. In four studies that included patients with both severe and non-severe disease, urinary shedding results were also mixed. Fang et al. found that among 32 ICU or non-ICU patients, none had SARS-CoV-2 RNA detected in their urine[49]. Similarly, another study documented low urinary shedding prevalence among severe and non-severe COVID-19 patients, with only a single patient’s urine testing positive for RNA[50]. Conversely, in a study of 60 patients, the 8 with SARS-CoV-2 RNA detected in their urine had more severe COVID-19, including 4 deaths among the 8[51]. While another study found significantly higher urinary shedding of SARS-CoV-2 RNA among severe patients (11 of 23) compared to patients with mild disease (4 of 30). A single study found urinary RNA shedding prevalence among immunocompetent patients (1 in 98) was significantly lower than among immunosuppressed patients (20 in 25), suggesting that immune status could be associated with urinary shedding of SARS-CoV-2 RNA[52]. Nonetheless, among the immunocompetent population, these studies do not substantiate a definitive relationship between COVID-19 severity and the presence of SARS-CoV-2 RNA in urine among the general population.
Such mixed results are consistent with observations of SARS-CoV-2 RNA in other body fluids. Several individual studies have observed higher virus loading in respiratory tissues or plasma for patients with severe COVID-19 and comorbidities[50,53,54,55]. However, systematic reviews have not established a definitive link between RNA loading and disease severity among symptomatic patients or between symptomatic versus asymptomatic patients[56,57]. Even for patients experiencing acute kidney injury, SARS-CoV-2 RNA in urine was not associated with renal complications[46]. If severe COVID-19 were, in fact, associated with higher SARS-CoV-2 RNA concentrations, assuming equivalent workflows, a consistently higher detection rate in urine among severe patients would be expected. However, the evidence is mixed. This suggests that study population alone does not explain the heterogeneity in the pooled estimate of SARS-CoV-2 RNA urinary shedding prevalence.
Methodological Diversity: Sample Type Equivalent Sample Volume
Since the diversity of the subpopulations does not adequately explain the heterogeneity of urinary shedding prevalence between studies, methodological diversity between studies should also be carefully considered including sample type, analytical system, and the equivalent sample volume achieved by the microbiological workflow. Collectively, the 45 studies include 3,202 urine samples collected from 1,924 unique patients. Only 13.3% of studies (6/45) reported the volume of urine collected during sampling from each subject. Most studies interrogated liquid urine during the RNA testing. However, 8 studies performed testing of urine sediment obtained by centrifuging the urine sample, discarding the supernatant, and finally resuspending the pellet for RNA extraction. Urine positivity for SARS-CoV-2 RNA among these 8 studies ranged from 1.7% (1/60)[40] to as high as 95% (21/22)[44]. Notably, no study analyzing urine sediment reported the absence of urinary shedding among all COVID-19 patients. Three urine sediment studies produced RNA positivity rates greater than the pooled estimate (95%[44]; 28.3%[58]; 16.3%[47]), while four produced prevalence estimates less than the pooled estimate (7.5%[59]; 5.7%[53]; 2.7%[60]; 1.7%[40]). The last study used two different testing methods, RT droplet digital PCR (RT-ddPCR) produced a 27.1% positivity rate (29/107) while RT-qPCR produced a 0.9% positivity rate (1/107) from the same samples[61]. Together, the studies analyzing urine sediment do not demonstrate a consistent departure from the pooled estimate of the prevalence of urinary RNA shedding. However, the findings from Shinde et al. raise another important consideration for methodological diversity – the analytical system.
Methodological Diversity: Analytical System
The vast majority (86.7%) of studies examining SARS-CoV-2 RNA in the urine of COVID-19 patients made use of one-step RT-qPCR employing assays targeting the E, RdRP, S, N, ORF1ab, and ORF1b genes. Seven studies (15.6%) did not report what assay was used. Urinary shedding prevalence among these studies ranged from 0% (20 studies totaling 425 patients) to as high as 95.5%[44]. One study made use of two-step RT qPCR along with SYBR Green dye, rather than a Taqman probe, to detect SARS-CoV-2 RNA in urine from 5/5 patients[62]. Interestingly, Baj et al. also made use of SYBR Green dye (with a one-step RT-qPCR) to detect RNA in urine sediments from 95.5% of patients (21/22)[44]. Conversely, no RNA was detected in the urine of 5 patients in another study utilizing RT-qPCR with SYBR Green dye[63]. One study made use of an anchor-primer PCR assay targeting the N gene to detect SARS-CoV-2 RNA in urine from 36.4% patients (4/11)[64]. A single study comparing RT-qPCR to RT-LAMP found the use of RT-LAMP double the prevalence of RNA in urine from 2/100 patients to 4/100 patients, although the prevlance still remained low[65]. Three studies used RT-ddPCR to test urine from COVID-19 patients. One study testing urine exclusively by RT-ddPCR found SARS-CoV-2 RNA in urine from 1 of 2 patients[66]. Results from comparative studies of RT-qPCR and RT-ddPCR were mixed from two studies. In one, RT-ddPCR increased the RNA positivity in urine sediment by 26.2% among 107 patients[61] while another failed to detect SARS-CoV-2 RNA in urine from 14 patients by either RT-qPCR or RT-ddPCR[67]. Overall, the results among analytical systems and assays are mixed with no clear evidence of systematic bias associated with a particular method. There is anecdotal evidence to suggest that in some cases droplet digital PCR or RT-qPCR with SYBR Green dye could yield significantly higher prevalence of SARS-CoV-2 RNA in urine.
Although excluded from the current analysis, two papers raise interesting points for PCR-based analysis of body fluids, such as urine, which are known to harbor compounds that can inhibit PCR amplification. A methodological investigation of RT-qPCR and RT-dPCR for testing urine found that the reverse transcription step was more vulnerable to inhibitory compounds than the PCR step and that matrix effects explained more variation in Cq values for RT-qPCR than mastermix diversity[68]. The authors also found that when testing urine seeded with SARS-CoV-2 RNA, the overall inhibitory effects varied by urine donor with urine from two donors inhibiting RT-qPCR while urine from another did not[68]. Meanwhile, during a retrospective analysis of urine sediments from Italy, 13 urine sediment samples tested negative by qPCR while 6/13 were positive for SARS-CoV-2 RNA via hemi-nested PCR[69]. Critically, none of the 45 studies in the current analysis reported the use of inhibition controls to assess the potential inhibitory effects of urine, which is a serious limitation when interpreting the current datasets.
Methodological Diversity: Equivalent Sample Volume
Another important, and as yet overlooked, source of methodological diversity in the studies of SARS-CoV-2 RNA in urine is the equivalent sample volume (ESV) achieved by the testing workflow. The ESV is the sample volume of the original matrix (in this case urine) that is interrogated in a single PCR reaction[70]. The ESV encodes the material balance of the multi-step workflows often used to process biological samples during PCR testing. In the case of the 45 studies of urine in the current analysis the diversity of workflows included studies using centrifugation to obtain urine sediments, studies that diluted prior to RNA extraction, studies that concentrated urine prior to extraction, and the majority of studies that directly extracted some volume of urine in a workflow used for other fluids such as nasal swab eluate. The ESV allows all these workflows to be considered within a single frame. In the absence of inhibition, greater ESV equates to more sample tested per reaction and increased analytical sensitivity. However, as previously discussed, the inhibitory effects of urine could result in a non-linear relationship between ESV and sensitivity. Only 8 of 45 studies (17.8%) reported the volumetric information required to estimate the ESV achieved by their workflow (Table S1). Each ESV was calculated per Equation S1 using the volumes summarized in Table S2. As shown in Figure 1A, the resulting ESVs range from 2 µL to 83.3 µL of urine per PCR reaction with an average of 29.0 µL ± 28.1 µL (standard deviation). Interestingly, the SARS-CoV-2 RNA prevalence in urine observed during each study is normally distributed as a function of the natural log of the ESV (r2 = 1.00, Figure 1B). Among 5 studies with ESV < 23 µL of urine, SARS-CoV-2 RNA was not detected in the urine of 227 patients. Whereas, for the studies achieving ESV > 39.9 µL, RNA was detected in the urine of 21.8% of 133 patients. Although the number of studies is limited, this implicates the ESV as a potential explanatory variable for the heterogeneity in urinary SARS-CoV-2 RNA positivity rates between studies.
SARS-CoV-2 RNA Urinary Abundance Revisited
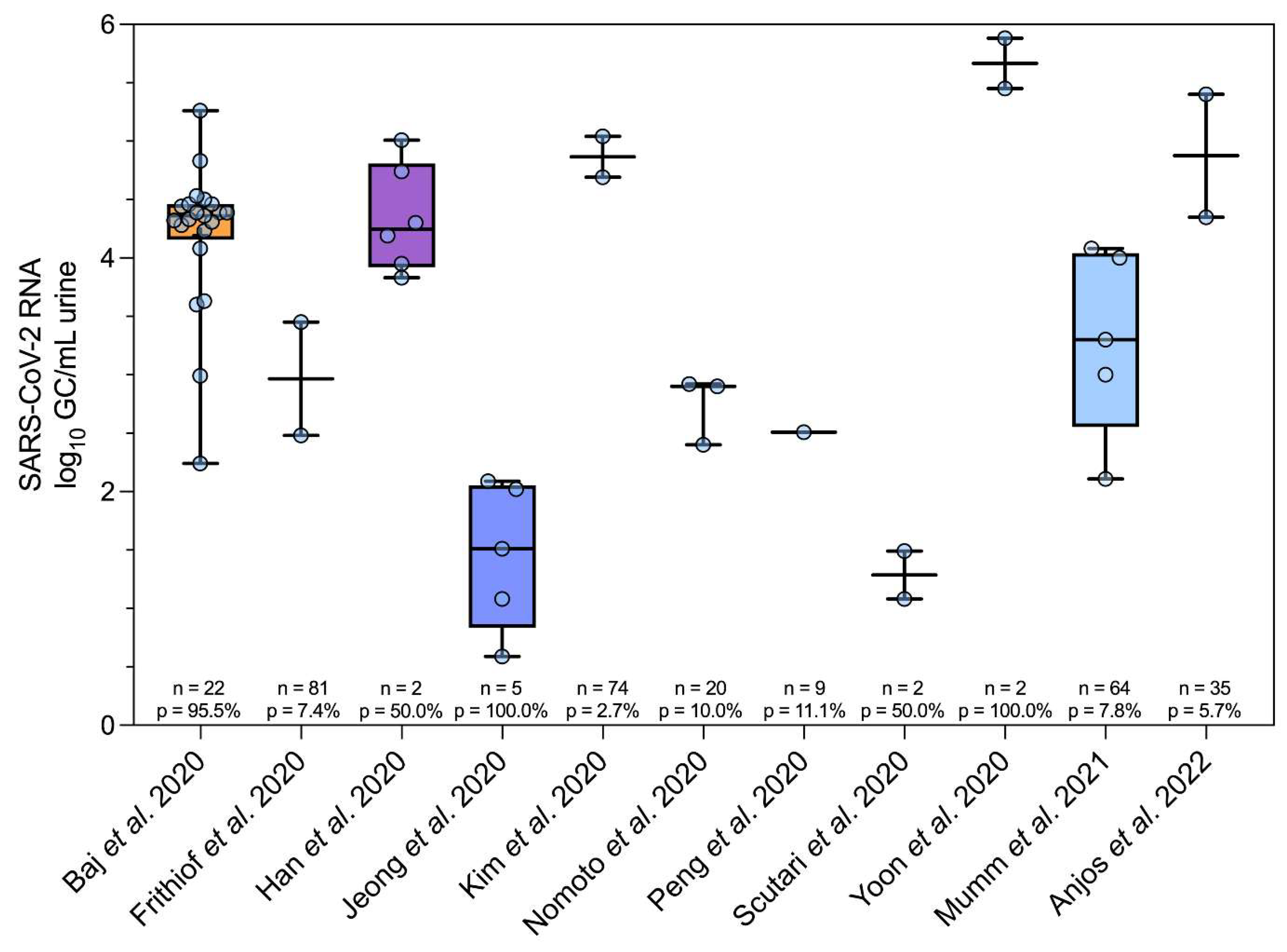
In addition to urinary RNA shedding prevalence among COVID-19 patients, the abundance of SARS-CoV-2 RNA in urine (count per unit volume) is also a key component in estimating the expected loading into wastewater[11]. Of the 45 studies included in the current analysis, only 11 reported quantitative data produced via RT-qPCR[41,44,46,53,60,62,71,72,73,74] or RT-ddPCR[66]. Translating RT-qPCR data from Cq values to quantitative results is non-trivial and requires the use of precisely quantified standards and careful experimentation to create calibration curves. Erroneous calibration curves or defective control materials can lead to the production of biased or imprecise quantitative data[75]. To safeguard against the publication of low-quality data, standards such as the Minimum Information for Publication of Quantitative Real-Time PCR Experiments (MIQE) and digital MIQE have been proposed[76,77]. Only Baj et al. published their quantitative data for SARS-CoV-2 RNA in urine to the MIQE standard[44]. The remaining 10 publications failed to report the required calibration curve metrics or workflow descriptions adequate to replicate the author’s calculations. Nonetheless, the quantitative data were extracted from figures provided in the 11 studies using WebPlotDigitizer v 4.7 MacOS 64-bit (Apple Silicon, https://automeris.io/v4/), resulting in a dataset of 51 observations, as shown in Figure 2. The abundance of SARS-CoV-2 RNA in urine among these studies ranged from 0.59 log10 to 5.88 log10 GC/mL of urine with a mean of 3.68 log10 GC/mL (95%CI: 3.33 - 4.04). The mean observed here is comparable to that reported for a urine dataset of 15 observations by Crank et al. (3.34 log10 GC/mL, 95% CI: 2.33 - 4.36)[11]. However, as shown in Figure S2 A, the maximum in the dataset from the current study is approximately 1.7 log10 GC/mL lower than that used to estimate wastewater input from urine previously[11]. Conversely, the mode observed for SARS-CoV-2 RNA log10 GC/mL in the current analysis (4.5) is 1.5 log10 GC/mL higher than the Crank et al. dataset[11]. Overall, despite the inclusion of 36 additional observations, the SARS-CoV-2 RNA counts in urine compiled here are roughly consistent with those used in a previous loading analysis and indicate the density of SARS-CoV-2 RNA in urine on a volumetric basis is, on average, one to two orders of magnitude lower than the density in stool on a per mass basis[11,12,78].
Additional Evidence for SARS-CoV-2 Constituents in Urine
Human urine contains both DNA and RNA, although usually at low concentrations and low quality due to fragmentation[79]. Previously, much of the interest in these nucleic acids has been driven by the potential use of urine as a diagnostic matrix for diseases such as colon cancer[80]. In the case of COVID-19, angiotensin-coverting enzyme 2 (ACE2), the receptor for SARS-CoV-2 is highly expressed in the kidneys and thus acute kidney injury (AKI) can be associated with COVID-19[81]. Using single-cell RNA sequencing, one study has reported evidence of SARS-CoV-2 virions directly infecting urinary bladder cells and found SARS-CoV-2 RNA in urothelial cells[82]. There is also some evidence to suggest the potential presence of infectious SARS-CoV-2 virions in urine. One study reported the isolation of infectious SARS-CoV-2 from the urine of a COVID-19 patient[83] while another reported that ferrets inoculated with urine became infected[62]. In addition to nucleic acids, urine from COVID-19 patients has also been found to possess a unique protein signature that could be useful for predicting severe outcomes[84,85]. SARS-CoV-2 nucleocapsid (N) protein or its constituent peptides were detected in 33% of urine samples from COVID-19 patients[86] and urinary N has been associated with risk of AKI among ICU patients[87]. Another study detected SARS-CoV-2 spike protein in the urine of 25.3% of patients testing positive for COVID-19 via nasopharyngeal swab[88].Together these observations further substantiate the plausibility of SARS-CoV-2 RNA being present in the urine of COVID-19 patients.
Implications for Wastewater Surveillance of Infectious Disease (631 words)
The success for COVID-19 is now spurring the expansion of wastewater surveillance for a variety of infectious agents such as influenza, norovirus, rhinovirus, respiratory syncytial virus, and arboviruses[5,89,90,91,92]. Quantitative models premised on human shedding data are being utilized to examine the technical feasibility and performance characteristics of wastewater testing[9,93,94,95]. Accurate characterization of analyte shedding patterns is critical to avoid erroneous feasibility assessments. Typically, the production of such data falls under the purview of clinical microbiology, although such information remains limited even for well-known viruses[96]. However, it is important to recognize that the aims of clinical microbiology and environmental microbiology can diverge in ways that are crucial for the production, interpretation, and application of the resulting data. In the case of clinical microbiology, during investigations of novel infectious agents, such as SARS-CoV-2, primary interests are body fluids most useful for diagnostic testing and shedding routes relevant to transmission. These interests inform studies where an equivalent workflow is applied to a variety of body fluids to produce a dataset that is primarily comparative in nature – sputum versus stool versus urine or plasma versus sputum.
For SARS-CoV-2, many of the published studies of urine applied workflows that achieved exceptionally low ESVs of urine. While these workflows might suffice for fluids where the loading is high, such as those from the respiratory tract or saliva, in the case of urine there is compelling evidence to suggest that the “rarity” of urinary shedding is in fact a methological artifact. Among the studies of SARS-CoV-2 RNA in urine, 83.3 µL was the highest ESV achieved with a resulting positivity of 95.5% among COVID-19 patients[44]. Even still, this volume is miniscule compared to the mean daily production volume of 1,500 mL per person that is discharged into wastewater collection systems each day[97]. The workflows applied during wastewater surveillance programs achieve ESVs orders of magnitude higher than those reported for urine. Additionally, the methodological reporting in many studies of SARS-CoV-2 RNA in urine does not comply with best practices for producing reliable quantitative data and is of low quality. For example, no study assessed the inhibitory effects of urine or the process recovery via proper controls. It is likely worth revisiting the question of SARS-CoV-2 RNA presence and density in urine with methods designed to achieve ESVs relevant for wastewater surveillance and with attention to proper controls and quantitative reliability. Such studies of stool have already produced interesting revisions of SARS-CoV-2 RNA shedding prevalence and abundance in feces[12,78].
The feasibility of wastewater surveillance, especially near-source surveillance in places such as schools and long-haul aircraft, hinges on the accurate characterization of shedding of the relevant analytes[11,98]. For example, in the case of aircraft wastewater surveillance, whether or not passengers shed SARS-CoV-2 RNA in urine makes a significant difference in both the number of aircraft that must be tested and in the likelihood of detecting a novel infectious agent via such a system[17,99]. Whether or not such a system is fiscally and technically feasible could hinge entirely on the question of urine. Moving forward, clinical and environmental microbiologist should collaborate to produce shedding route datasets that are appropriate for use in wastewater surveillance. In the meantime, wastewater surveillance practitioners should take extra care when adopting and applying clinical datasets to ensure that the caveats and limitations are thoroughly understood and incorporated into any subsequent analyses.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
References
- Wilson, W.J. Isolation of Enteric Bacilli from Sewage and Water and Its Bearing on Epidemiology. Br Med J 1933, 2, 560–562. [Google Scholar] [CrossRef]
- Paul, J.R.; Trask, J.D.; Gard, S. II. POLIOMYELITIC VIRUS IN URBAN SEWAGE. J. Exp. Med. 1940, 71, 765–777. [Google Scholar] [CrossRef] [PubMed]
- Heijnen, L.; Medema, G. Surveillance of Influenza A and the Pandemic Influenza A (H1N1) 2009 in Sewage and Surface Water in the Netherlands. J. Water Health 2011, 9, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Wastewater-Based Disease Surveillance for Public Health Action; National Academies Press: Washington, DC, USA, 2023. [CrossRef]
- Boehm, A.B.; Hughes, B.; Duong, D.; Chan-Herur, V.; Buchman, A.; Wolfe, M.K.; White, B.J. Wastewater Concentrations of Human Influenza, Metapneumovirus, Parainfluenza, Respiratory Syncytial Virus, Rhinovirus, and Seasonal Coronavirus Nucleic-Acids during the COVID-19 Pandemic: A Surveillance Study. Lancet Microbe 2023, 4, e340–e348. [Google Scholar] [CrossRef] [PubMed]
- Moore, B.; Perry, C.E.L.; Chard, S.T. A Survey by the Sewage Swab Method of Latent Enteric Infection in an Urban Area. Epidemiol. Infect. 1952, 50, 137–156. [Google Scholar] [CrossRef]
- Wölfel, R.; Corman, V.M.; Guggemos, W.; Seilmaier, M.; Zange, S.; Müller, M.A.; Niemeyer, D.; Jones, T.C.; Vollmar, P.; Rothe, C.; Hoelscher, M.; Bleicker, T.; Brünink, S.; Schneider, J.; Ehmann, R.; Zwirglmaier, K.; Drosten, C.; Wendtner, C. Virological Assessment of Hospitalized Patients with COVID-2019. Nature 2020, 581, 465–469. [Google Scholar] [CrossRef]
- He, X.; Lau, E.H.Y.; Wu, P.; Deng, X.; Wang, J.; Hao, X.; Lau, Y.C.; Wong, J.Y.; Guan, Y.; Tan, X.; Mo, X.; Chen, Y.; Liao, B.; Chen, W.; Hu, F.; Zhang, Q.; Zhong, M.; Wu, Y.; Zhao, L.; Zhang, F.; Cowling, B.J.; Li, F.; Leung, G.M. Temporal Dynamics in Viral Shedding and Transmissibility of COVID-19. Nat. Med. 2020, 26, 672–675. [Google Scholar] [CrossRef]
- Hart, O.E.; Halden, R.U. Computational Analysis of SARS-CoV-2/COVID-19 Surveillance by Wastewater-Based Epidemiology Locally and Globally: Feasibility, Economy, Opportunities and Challenges. Sci. Total Environ. 2020, 730, 138875. [Google Scholar] [CrossRef]
- Ahmed, W.; Angel, N.; Edson, J.; Bibby, K.; Bivins, A.; O’Brien, J.W.; Choi, P.M.; Kitajima, M.; Simpson, S.L.; Li, J.; Tscharke, B.; Verhagen, R.; Smith, W.J.M.; Zaugg, J.; Dierens, L.; Hugenholtz, P.; Thomas, K.V.; Mueller, J.F. First Confirmed Detection of SARS-CoV-2 in Untreated Wastewater in Australia: A Proof of Concept for the Wastewater Surveillance of COVID-19 in the Community. Sci. Total Environ. 2020, 728, 138764. [Google Scholar] [CrossRef]
- Crank, K.; Chen, W.; Bivins, A.; Lowry, S.; Bibby, K. Contribution of SARS-CoV-2 RNA Shedding Routes to RNA Loads in Wastewater. Sci. Total Environ. 2022, 806, 150376. [Google Scholar] [CrossRef]
- Arts, P.J.; Kelly, J.D.; Midgley, C.M.; Anglin, K.; Lu, S.; Abedi, G.R.; Andino, R.; Bakker, K.M.; Banman, B.; Boehm, A.B.; Briggs-Hagen, M.; Brouwer, A.F.; Davidson, M.C.; Eisenberg, M.C.; Garcia-Knight, M.; Knight, S.; Peluso, M.J.; Pineda-Ramirez, J.; Diaz Sanchez, R.; Saydah, S.; Tassetto, M.; Martin, J.N.; Wigginton, K.R. Longitudinal and Quantitative Fecal Shedding Dynamics of SARS-CoV-2, Pepper Mild Mottle Virus, and crAssphage. mSphere 2023, 8, e00132–23. [Google Scholar] [CrossRef] [PubMed]
- Ahmed, W.; Bivins, A.; Simpson, S.L.; Bertsch, P.M.; Ehret, J.; Hosegood, I.; Metcalfe, S.S.; Smith, W.J.; Thomas, K.V.; Tynan, J. Wastewater Surveillance Demonstrates High Predictive Value for COVID-19 Infection on Board Repatriation Flights to Australia. Environ. Int. 2022, 158, 106938. [Google Scholar] [CrossRef] [PubMed]
- Jones, D.L.; Rhymes, J.M.; Wade, M.J.; Kevill, J.L.; Malham, S.K.; Grimsley, J.M.S.; Rimmer, C.; Weightman, A.J.; Farkas, K. Suitability of Aircraft Wastewater for Pathogen Detection and Public Health Surveillance. Sci. Total Environ. 2023, 856, 159162. [Google Scholar] [CrossRef] [PubMed]
- Farkas, K.; Williams, R.; Alex-Sanders, N.; Grimsley, J.M.S.; Pântea, I.; Wade, M.J.; Woodhall, N.; Jones, D.L. Wastewater-Based Monitoring of SARS-CoV-2 at UK Airports and Its Potential Role in International Public Health Surveillance. PLOS Glob. Public Health 2023, 3, e0001346. [Google Scholar] [CrossRef]
- Morfino, R.C. Notes from the Field: Aircraft Wastewater Surveillance for Early Detection of SARS-CoV-2 Variants — John F. Kennedy International Airport, New York City, August–September 2022. MMWR Morb. Mortal. Wkly. Rep. 2023, 72. [Google Scholar] [CrossRef]
- Bivins, A.; Morfino, R.; Franklin, A.; Simpson, S.; Ahmed, W. The Lavatory Lens: Tracking the Global Movement of Pathogens via Aircraft Wastewater. Preprints May 9, 2023. [CrossRef]
- Hassard, F.; Lundy, L.; Singer, A.C.; Grimsley, J.; Cesare, M.D. Innovation in Wastewater Near-Source Tracking for Rapid Identification of COVID-19 in Schools. Lancet Microbe 2021, 2, e4–e5. [Google Scholar] [CrossRef]
- Hassard, F.; Singh, S.; Coulon, F.; Yang, Z. Can Wastewater Monitoring Protect Public Health in Schools? Lancet Reg. Health Am. 2023, 20. [Google Scholar] [CrossRef]
- Wolken, M.; Sun, T.; McCall, C.; Schneider, R.; Caton, K.; Hundley, C.; Hopkins, L.; Ensor, K.; Domakonda, K.; Kalvapalle, P.; Persse, D.; Williams, S.; Stadler, L.B. Wastewater Surveillance of SARS-CoV-2 and Influenza in preK-12 Schools Shows School, Community, and Citywide Infections. Water Res. 2023, 231, 119648. [Google Scholar] [CrossRef]
- Crowe, J.; Schnaubelt, A.T.; SchmidtBonne, S.; Angell, K.; Bai, J.; Eske, T.; Nicklin, M.; Pratt, C.; White, B.; Crotts-Hannibal, B.; Staffend, N.; Herrera, V.; Cobb, J.; Conner, J.; Carstens, J.; Tempero, J.; Bouda, L.; Ray, M.; Lawler, J.V.; Campbell, W.S.; Lowe, J.-M.; Santarpia, J.; Bartelt-Hunt, S.; Wiley, M.; Brett-Major, D.; Logan, C.; Broadhurst, M.J. Assessment of a Program for SARS-CoV-2 Screening and Environmental Monitoring in an Urban Public School District. JAMA Netw. Open 2021, 4, e2126447. [Google Scholar] [CrossRef]
- Hassard, F.; Vu, M.; Rahimzadeh, S.; Castro-Gutierrez, V.; Stanton, I.; Burczynska, B.; Wildeboer, D.; Baio, G.; Brown, M.R.; Garelick, H.; Hofman, J.; Kasprzyk-Hordern, B.; Majeed, A.; Priest, S.; Denise, H.; Khalifa, M.; Bassano, I.; Wade, M.J.; Grimsley, J.; Lundy, L.; Singer, A.C.; Cesare, M.D. Wastewater Monitoring for Detection of Public Health Markers during the COVID-19 Pandemic: Near-Source Monitoring of Schools in England over an Academic Year. PLoS ONE 2023, 18, e0286259. [Google Scholar] [CrossRef]
- Kim, S.; Boehm, A.B. Wastewater Monitoring of SARS-CoV-2 RNA at K-12 Schools: Comparison to Pooled Clinical Testing Data. PeerJ 2023, 11, e15079. [Google Scholar] [CrossRef] [PubMed]
- Lopez Marin, M.A.; Zdenkova, K.; Bartackova, J.; Cermakova, E.; Dostalkova, A.; Demnerova, K.; Vavruskova, L.; Novakova, Z.; Sykora, P.; Rumlova, M.; Bartacek, J. Monitoring COVID-19 Spread in Selected Prague’s Schools Based on the Presence of SARS-CoV-2 RNA in Wastewater. Sci. Total Environ. 2023, 871, 161935. [Google Scholar] [CrossRef] [PubMed]
- Fielding-Miller, R.; Karthikeyan, S.; Gaines, T.; Garfein, R.S.; Salido, R.A.; Cantu, V.J.; Kohn, L.; Martin, N.K.; Wynn, A.; Wijaya, C.; Flores, M.; Omaleki, V.; Majnoonian, A.; Gonzalez-Zuniga, P.; Nguyen, M.; Vo, A.V.; Le, T.; Duong, D.; Hassani, A.; Tweeten, S.; Jepsen, K.; Henson, B.; Hakim, A.; Birmingham, A.; Hoff, P.D.; Mark, A.M.; Nasamran, C.A.; Rosenthal, S.B.; Moshiri, N.; Fisch, K.M.; Humphrey, G.; Farmer, S.; Tubb, H.M.; Valles, T.; Morris, J.; Kang, J.; Khaleghi, B.; Young, C.; Akel, A.D.; Eilert, S.; Eno, J.; Curewitz, K.; Laurent, L.C.; Rosing, T.; Knight, R.; Baer, N.A.; Barber, T.; Castro-Martinez, A.; Chacón, M.; Cheung, W.; Crescini, E.S.; Eisner, E.R.; Vargas, L.F.; Hakim, A.; Hobbs, C.; Lastrella, A.L.; Lawrence, E.S.; Matteson, N.L.; Gangavarapu, K.; Ngo, T.T.; Seaver, P.; Smoot, E.W.; Tsai, R.; Xia, B.; Aigner, S.; Anderson, C.; Belda-Ferre, P.; Sathe, S.; Zeller, M.; Andersen, K.G.; Yeo, G.W.; Kurzban, E. Safer at School Early Alert: An Observational Study of Wastewater and Surface Monitoring to Detect COVID-19 in Elementary Schools. Lancet Reg. Health Am. 2023, 19. [Google Scholar] [CrossRef] [PubMed]
- Castro-Gutierrez, V.; Hassard, F.; Vu, M.; Leitao, R.; Burczynska, B.; Wildeboer, D.; Stanton, I.; Rahimzadeh, S.; Baio, G.; Garelick, H.; Hofman, J.; Kasprzyk-Hordern, B.; Kwiatkowska, R.; Majeed, A.; Priest, S.; Grimsley, J.; Lundy, L.; Singer, A.C.; Cesare, M.D. Monitoring Occurrence of SARS-CoV-2 in School Populations: A Wastewater-Based Approach. PLoS ONE 2022, 17, e0270168. [Google Scholar] [CrossRef]
- Jones, D.L.; Baluja, M.Q.; Graham, D.W.; Corbishley, A.; McDonald, J.E.; Malham, S.K.; Hillary, L.S.; Connor, T.R.; Gaze, W.H.; Moura, I.B.; Wilcox, M.H.; Farkas, K. Shedding of SARS-CoV-2 in Feces and Urine and Its Potential Role in Person-to-Person Transmission and the Environment-Based Spread of COVID-19. Sci. Total Environ. 2020, 749, 141364. [Google Scholar] [CrossRef]
- Johnson, H.; Garg, M.; Shantikumar, S.; Thachil, J.; Rai, B.; Aboumarzouk, O.M.; Hashim, H.; Philip, J. COVID-19 (SARS-CoV-2) in Non-Airborne Body Fluids: A Systematic Review & Meta-Analysis. Turk. J. Urol. 2021, 47, 87–97. [Google Scholar] [CrossRef]
- Böger, B.; Fachi, M.M.; Vilhena, R.O.; Cobre, A.F.; Tonin, F.S.; Pontarolo, R. Systematic Review with Meta-Analysis of the Accuracy of Diagnostic Tests for COVID-19. Am. J. Infect. Control 2021, 49, 21–29. [Google Scholar] [CrossRef]
- Bwire, G.M.; Majigo, M.V.; Njiro, B.J.; Mawazo, A. Detection Profile of SARS-CoV-2 Using RT-PCR in Different Types of Clinical Specimens: A Systematic Review and Meta-Analysis. J. Med. Virol. 2021, 93, 719–725. [Google Scholar] [CrossRef]
- Morone, G.; Palomba, A.; Iosa, M.; Caporaso, T.; De Angelis, D.; Venturiero, V.; Savo, A.; Coiro, P.; Carbone, D.; Gimigliano, F.; Iolascon, G.; Paolucci, S. Incidence and Persistence of Viral Shedding in COVID-19 Post-Acute Patients With Negativized Pharyngeal Swab: A Systematic Review. Front. Med. 2020, 7, 562. [Google Scholar] [CrossRef]
- Roshandel, M.R.; Nateqi, M.; Lak, R.; Aavani, P.; Sari Motlagh, R.; F Shariat, S.; Aghaei Badr, T.; Sfakianos, J.; Kaplan, S.A.; Tewari, A.K. Diagnostic and Methodological Evaluation of Studies on the Urinary Shedding of SARS-CoV-2, Compared to Stool and Serum: A Systematic Review and Meta-Analysis. Cell. Mol. Biol. Noisy--Gd. Fr. 2020, 66, 148–156. [Google Scholar] [CrossRef]
- Brönimann, S.; Rebhan, K.; Lemberger, U.; Misrai, V.; Shariat, S.F.; Pradere, B. Secretion of Severe Acute Respiratory Syndrome Coronavirus 2 in Urine. Curr. Opin. Urol. 2020, 30, 735–739. [Google Scholar] [CrossRef] [PubMed]
- Chan, V.W.-S.; Chiu, P.K.-F.; Yee, C.-H.; Yuan, Y.; Ng, C.-F.; Teoh, J.Y.-C. A Systematic Review on COVID-19: Urological Manifestations, Viral RNA Detection and Special Considerations in Urological Conditions. World J. Urol. 2021, 39, 3127–3138. [Google Scholar] [CrossRef] [PubMed]
- Mishra, C.; Meena, S.; Meena, J.K.; Tiwari, S.; Mathur, P. Detection of Three Pandemic Causing Coronaviruses from Non-Respiratory Samples: Systematic Review and Meta-Analysis. Sci. Rep. 2021, 11, 16131. [Google Scholar] [CrossRef] [PubMed]
- Kashi, A.H.; De la Rosette, J.; Amini, E.; Abdi, H.; Fallah-Karkan, M.; Vaezjalali, M. Urinary Viral Shedding of COVID-19 and Its Clinical Associations: A Systematic Review and Meta-Analysis of Observational Studies. Urol. J. 2020, 17, 433–441. [Google Scholar] [CrossRef]
- Trypsteen, W.; Van Cleemput, J.; Snippenberg, W.v.; Gerlo, S.; Vandekerckhove, L. On the Whereabouts of SARS-CoV-2 in the Human Body: A Systematic Review. PLoS Pathog. 2020, 16, e1009037. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-Analysis in Clinical Trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef]
- Wallace, B.C.; Dahabreh, I.J.; Trikalinos, T.A.; Lau, J.; Trow, P.; Schmid, C.H. Closing the Gap between Methodologists and End-Users: R as a Computational Back-End. J. Stat. Softw. 2012, 49, 1–15. [Google Scholar] [CrossRef]
- Hasanoglu, I.; Korukluoglu, G.; Asilturk, D.; Cosgun, Y.; Kalem, A.K.; Altas, A.B.; Kayaaslan, B.; Eser, F.; Kuzucu, E.A.; Guner, R. Higher Viral Loads in Asymptomatic COVID-19 Patients Might Be the Invisible Part of the Iceberg. Infection 2021, 49, 117–126. [Google Scholar] [CrossRef]
- Han, M.S.; Seong, M.-W.; Heo, E.Y.; Park, J.H.; Kim, N.; Shin, S.; Cho, S.I.; Park, S.S.; Choi, E.H. Sequential Analysis of Viral Load in a Neonate and Her Mother Infected With Severe Acute Respiratory Syndrome Coronavirus 2. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2020, 71, 2236–2239. [Google Scholar] [CrossRef]
- Jiehao, C.; Jin, X.; Daojiong, L.; Zhi, Y.; Lei, X.; Zhenghai, Q.; Yuehua, Z.; Hua, Z.; Ran, J.; Pengcheng, L.; Xiangshi, W.; Yanling, G.; Aimei, X.; He, T.; Hailing, C.; Chuning, W.; Jingjing, L.; Jianshe, W.; Mei, Z. A Case Series of Children With 2019 Novel Coronavirus Infection: Clinical and Epidemiological Features. Clin. Infect. Dis. 2020, 71, 1547–1551. [Google Scholar] [CrossRef]
- Liu, P.; Cai, J.; Jia, R.; Xia, S.; Wang, X.; Cao, L.; Zeng, M.; Xu, J. Dynamic Surveillance of SARS-CoV-2 Shedding and Neutralizing Antibody in Children with COVID-19. Emerg. Microbes Infect. 2020, 9, 1254–1258. [Google Scholar] [CrossRef] [PubMed]
- Baj, A.; Azzi, L.; Dalla Gasperina, D.; Genoni, A.; Tamborini, A.; Gambarini, C.; Carcano, G.; Grossi, P.; Sessa, F. Pilot Study: Long-Term Shedding of SARS-CoV-2 in Urine: A Threat for Dispersal in Wastewater. Front. Public Health 2020, 8, 569209. [Google Scholar] [CrossRef] [PubMed]
- Couturier, A.; Ferlicot, S.; Chevalier, K.; Guillet, M.; Essig, M.; Jauréguiberry, S.; Collarino, R.; Dargelos, M.; Michaut, A.; Geri, G.; Roque-Afonso, A.-M.; Zaidan, M.; Massy, Z.A. Indirect Effects of Severe Acute Respiratory Syndrome Coronavirus 2 on the Kidney in Coronavirus Disease Patients. Clin. Kidney J. 2020, 13, 347–353. [Google Scholar] [CrossRef] [PubMed]
- Frithiof, R.; Bergqvist, A.; Järhult, J.D.; Lipcsey, M.; Hultström, M. Presence of SARS-CoV-2 in Urine Is Rare and Not Associated with Acute Kidney Injury in Critically Ill COVID-19 Patients. Crit. Care Lond. Engl. 2020, 24, 587. [Google Scholar] [CrossRef] [PubMed]
- Tong, Y.; Bao, A.; Chen, H.; Huang, J.; Lv, Z.; Feng, L.; Cheng, Y.; Wang, Y.; Bai, L.; Rao, W.; Zheng, H.; Wu, Z.; Qiao, B.; Zhao, Z.; Wang, H.; Li, Y. Necessity for Detection of SARS-CoV-2 RNA in Multiple Types of Specimens for the Discharge of the Patients with COVID-19. J. Transl. Med. 2020, 18, 411. [Google Scholar] [CrossRef]
- Tejerina, F.; Catalan, P.; Rodriguez-Grande, C.; Adan, J.; Rodriguez-Gonzalez, C.; Muñoz, P.; Aldamiz, T.; Diez, C.; Perez, L.; Fanciulli, C.; Garcia de Viedma, D. Post-COVID-19 Syndrome. SARS-CoV-2 RNA Detection in Plasma, Stool, and Urine in Patients with Persistent Symptoms after COVID-19. BMC Infect. Dis. 2022, 22, 211. [Google Scholar] [CrossRef]
- Fang, Z.; Zhang, Y.; Hang, C.; Ai, J.; Li, S.; Zhang, W. Comparisons of Viral Shedding Time of SARS-CoV-2 of Different Samples in ICU and Non-ICU Patients. J. Infect. 2020, 81, 147–178. [Google Scholar] [CrossRef]
- Zheng, S.; Fan, J.; Yu, F.; Feng, B.; Lou, B.; Zou, Q.; Xie, G.; Lin, S.; Wang, R.; Yang, X.; Chen, W.; Wang, Q.; Zhang, D.; Liu, Y.; Gong, R.; Ma, Z.; Lu, S.; Xiao, Y.; Gu, Y.; Zhang, J.; Yao, H.; Xu, K.; Lu, X.; Wei, G.; Zhou, J.; Fang, Q.; Cai, H.; Qiu, Y.; Sheng, J.; Chen, Y.; Liang, T. Viral Load Dynamics and Disease Severity in Patients Infected with SARS-CoV-2 in Zhejiang Province, China, January-March 2020: Retrospective Cohort Study. BMJ 2020, 369, m1443. [Google Scholar] [CrossRef]
- Perrella, A.; Brita, M.; Coletta, F.; Cotena, S.; De Marco, G.; Longobardi, A.; Sala, C.; Sannino, D.; Tomasello, A.; Perrella, M.; Russo, G.; Tarsitano, M.; Chetta, M.; Della Monica, M.; Orlando, V.; Coscioni, E.; Villani, R. SARS-CoV-2 in Urine May Predict a Severe Evolution of COVID-19. J. Clin. Med. 2021, 10, 4061. [Google Scholar] [CrossRef]
- Mendes-Correa, M.C.; Salomão, M.C.; Ghilardi, F.; Tozetto-Mendoza, T.R.; Santos Villas-Boas, L.; de Paula, A.V.; Paiao, H.G.O.; da Costa, A.C.; Leal, F.E.; Ferraz, A. de B. C.; Sales, F.C.S.; Claro, I.M.; Ferreira, N.E.; Pereira, G.M.; da Silva, A.R.J.; Freire, W.; Espinoza, E.P.S.; Manuli, E.R.; Romano, C.M.; de Jesus, J.G.; Sabino, E.C.; Witkin, S.S. SARS-CoV-2 Detection and Culture in Different Biological Specimens from Immunocompetent and Immunosuppressed COVID-19 Patients Infected with Two Different Viral Strains. Viruses 2023, 15. [Google Scholar] [CrossRef]
- Anjos, D.; Fiaccadori, F.S.; Servian, C.d.P.; da Fonseca, S.G.; Guilarde, A.O.; Borges, M.A.S.B.; Franco, F.C.; Ribeiro, B.M.; Souza, M. SARS-CoV-2 Loads in Urine, Sera and Stool Specimens in Association with Clinical Features of COVID-19 Patients. J. Clin. Virol. Plus 2022, 2, 100059. [Google Scholar] [CrossRef] [PubMed]
- Maltezou, H.C.; Raftopoulos, V.; Vorou, R.; Papadima, K.; Mellou, K.; Spanakis, N.; Kossyvakis, A.; Gioula, G.; Exindari, M.; Froukala, E.; Martinez-Gonzalez, B.; Panayiotakopoulos, G.; Papa, A.; Mentis, A.; Tsakris, A. Association Between Upper Respiratory Tract Viral Load, Comorbidities, Disease Severity, and Outcome of Patients With SARS-CoV-2 Infection. J. Infect. Dis. 2021, 223, 1132–1138. [Google Scholar] [CrossRef]
- Fajnzylber, J.; Regan, J.; Coxen, K.; Corry, H.; Wong, C.; Rosenthal, A.; Worrall, D.; Giguel, F.; Piechocka-Trocha, A.; Atyeo, C.; Fischinger, S.; Chan, A.; Flaherty, K.T.; Hall, K.; Dougan, M.; Ryan, E.T.; Gillespie, E.; Chishti, R.; Li, Y.; Jilg, N.; Hanidziar, D.; Baron, R.M.; Baden, L.; Tsibris, A.M.; Armstrong, K.A.; Kuritzkes, D.R.; Alter, G.; Walker, B.D.; Yu, X.; Li, J.Z. SARS-CoV-2 Viral Load Is Associated with Increased Disease Severity and Mortality. Nat. Commun. 2020, 11, 5493. [Google Scholar] [CrossRef]
- Dadras, O.; Afsahi, A.M.; Pashaei, Z.; Mojdeganlou, H.; Karimi, A.; Habibi, P.; Barzegary, A.; Fakhfouri, A.; Mirzapour, P.; Janfaza, N.; Dehghani, S.; Afroughi, F.; Dashti, M.; Khodaei, S.; Mehraeen, E.; Voltarelli, F.; Sabatier, J.-M.; SeyedAlinaghi, S. The Relationship between COVID-19 Viral Load and Disease Severity: A Systematic Review. Immun. Inflamm. Dis. 2022, 10, e580. [Google Scholar] [CrossRef]
- Zuin, M.; Gentili, V.; Cervellati, C.; Rizzo, R.; Zuliani, G. Viral Load Difference between Symptomatic and Asymptomatic COVID-19 Patients: Systematic Review and Meta-Analysis. Infect. Dis. Rep. 2021, 13, 645–653. [Google Scholar] [CrossRef]
- Zhang, L.; Tian, M.; Song, Y.; Liang, W.; Li, X.; Tong, Y.; Wang, H. Urinary SARS-CoV-2 RNA Is an Indicator for the Progression and Prognosis of COVID-19. Diagn. Basel Switz. 2021, 11. [Google Scholar] [CrossRef]
- Wang, W.; Xu, Y.; Gao, R.; Lu, R.; Han, K.; Wu, G.; Tan, W. Detection of SARS-CoV-2 in Different Types of Clinical Specimens. JAMA 2020, 323, 1843–1844. [Google Scholar] [CrossRef]
- Kim, J.-M.; Kim, H.M.; Lee, E.J.; Jo, H.J.; Yoon, Y.; Lee, N.-J.; Son, J.; Lee, Y.-J.; Kim, M.S.; Lee, Y.-P.; Chae, S.-J.; Park, K.R.; Cho, S.-R.; Park, S.; Kim, S.J.; Wang, E.; Woo, S.; Lim, A.; Park, S.-J.; Jang, J.; Chung, Y.-S.; Chin, B.S.; Lee, J.-S.; Lim, D.; Han, M.-G.; Yoo, C.K. Detection and Isolation of SARS-CoV-2 in Serum, Urine, and Stool Specimens of COVID-19 Patients from the Republic of Korea. Osong Public Health Res. Perspect. 2020, 11, 112–117. [Google Scholar] [CrossRef]
- Shinde, M.; Lavania, M.; Rawal, J.; Chavan, N.; Shinde, P. Evaluation of Droplet Digital qRT-PCR (Dd qRT-PCR) for Quantification of SARS CoV-2 RNA in Stool and Urine Specimens of COVID-19 Patients. Front. Med. 2023, 10, 1148688. [Google Scholar] [CrossRef]
- Jeong, H.W.; Kim, S.-M.; Kim, H.-S.; Kim, Y.-I.; Kim, J.H.; Cho, J.Y.; Kim, S.-H.; Kang, H.; Kim, S.-G.; Park, S.-J.; Kim, E.-H.; Choi, Y.K. Viable SARS-CoV-2 in Various Specimens from COVID-19 Patients. Clin. Microbiol. Infect. Off. Publ. Eur. Soc. Clin. Microbiol. Infect. Dis. 2020, 26, 1520–1524. [Google Scholar] [CrossRef]
- Chan, J.F.-W.; Yuan, S.; Kok, K.-H.; To, K.K.-W.; Chu, H.; Yang, J.; Xing, F.; Liu, J.; Yip, C.C.-Y.; Poon, R.W.-S.; Tsoi, H.-W.; Lo, S.K.-F.; Chan, K.-H.; Poon, V.K.-M.; Chan, W.-M.; Ip, J.D.; Cai, J.-P.; Cheng, V.C.-C.; Chen, H.; Hui, C.K.-M.; Yuen, K.-Y. A Familial Cluster of Pneumonia Associated with the 2019 Novel Coronavirus Indicating Person-to-Person Transmission: A Study of a Family Cluster. The Lancet 2020, 395, 514–523. [Google Scholar] [CrossRef] [PubMed]
- Xu, T.; Wang, J.; Hu, B.; Zhang, G.; Zhou, W.; Zheng, M.; Shen, B.; Sun, B.; Zhang, Y.; Chen, Y.; Yu, J.; Liang, M.; Pan, J.; Chen, C.; Chen, H.; Jiang, M.; Xu, L.; Qu, J.; Chen, J.-F. Identification of the RNase-Binding Site of SARS-CoV-2 RNA for Anchor Primer-PCR Detection of Viral Loading in 306 COVID-19 Patients. Brief. Bioinform. 2021, 22, 1215–1224. [Google Scholar] [CrossRef] [PubMed]
- García-Bernalt Diego, J.; Fernández-Soto, P.; Muñoz-Bellido, J.L.; Febrer-Sendra, B.; Crego-Vicente, B.; Carbonell, C.; López-Bernús, A.; Marcos, M.; Belhassen-García, M.; Muro, A. Detection of SARS-CoV-2 RNA in Urine by RT-LAMP: A Very Rare Finding. J. Clin. Med. 2022, 11, 158. [Google Scholar] [CrossRef] [PubMed]
- Scutari, R.; Piermatteo, L.; Ciancio Manuelli, M.; Iannetta, M.; Salpini, R.; Bertoli, A.; Alteri, C.; Saccomandi, P.; Bellocchi, M.C.; Malagnino, V.; Teti, E.; Sforza, D.; Siragusa, L.; Grande, M.; Sarmati, L.; Svicher, V.; Andreoni, M.; Ceccherini-Silberstein, F. Long-Term SARS-CoV-2 Infection Associated with Viral Dissemination in Different Body Fluids Including Bile in Two Patients with Acute Cholecystitis. Life Basel Switz. 2020, 10. [Google Scholar] [CrossRef] [PubMed]
- Yu, F.; Yan, L.; Wang, N.; Yang, S.; Wang, L.; Tang, Y.; Gao, G.; Wang, S.; Ma, C.; Xie, R.; Wang, F.; Tan, C.; Zhu, L.; Guo, Y.; Zhang, F. Quantitative Detection and Viral Load Analysis of SARS-CoV-2 in Infected Patients. Clin. Infect. Dis. 2020, 71, 793–798. [Google Scholar] [CrossRef]
- Whale, A.S.; von der Heide, E.K.; Kohlenberg, M.; Brinckmann, A.; Baedker, S.; Karalay, O.; Fernandez-Gonzalez, A.; Busby, E.J.; Bustin, S.A.; Hauser, H.; Missel, A.; O’Sullivan, D.M.; Huggett, J.F.; Pfaffl, M.W.; Nolan, T. Digital PCR Can Augment the Interpretation of RT-qPCR Cq Values for SARS-CoV-2 Diagnostics. Methods San Diego Calif 2022, 201, 5–14. [Google Scholar] [CrossRef]
- Amendola, A.; Canuti, M.; Bianchi, S.; Kumar, S.; Fappani, C.; Gori, M.; Colzani, D.; Kosakovsky Pond, S.L.; Miura, S.; Baggieri, M.; Marchi, A.; Borghi, E.; Zuccotti, G.; Raviglione, M.C.; Magurano, F.; Tanzi, E. Molecular Evidence for SARS-CoV-2 in Samples Collected from Patients with Morbilliform Eruptions since Late 2019 in Lombardy, Northern Italy. Environ. Res. 2022, 215 Pt 1, 113979. [Google Scholar] [CrossRef]
- Crank, K.; Papp, K.; Barber, C.; Wang, P.; Bivins, A.; Gerrity, D. Correspondence on “The Environmental Microbiology Minimum Information (EMMI) Guidelines: qPCR and dPCR Quality and Reporting for Environmental Microbiology. ” Environ. Sci. Technol. 2023, 57, 20448–20449. [Google Scholar] [CrossRef]
- Mumm, J.-N.; Ledderose, S.; Ostermann, A.; Rudelius, M.; Hellmuth, J.C.; Münchhoff, M.; Munker, D.; Scherer, C.; Volz, Y.; Ebner, B.; Giessen-Jung, C.; Lampert, C.; Vilsmaier, T.; Schneider, S.; Gapp, M.; Milger-Kneidinger, K.; Behr, J.; von Bergwelt-Baildon, M.; Keppler, O.T.; Stief, C.; Magistro, G.; Staehler, M.; Rodler, S. Dynamics of Urinary and Respiratory Shedding of Severe Acute Respiratory Syndrome Virus 2 (SARS-CoV-2) RNA Excludes Urine as a Relevant Source of Viral Transmission. Infection 2022, 50, 635–642. [Google Scholar] [CrossRef]
- Nomoto, H.; Ishikane, M.; Katagiri, D.; Kinoshita, N.; Nagashima, M.; Sadamasu, K.; Yoshimura, K.; Ohmagari, N. Cautious Handling of Urine from Moderate to Severe COVID-19 Patients. Am. J. Infect. Control 2020, 48, 969–971. [Google Scholar] [CrossRef]
- Peng, L.; Liu, J.; Xu, W.; Luo, Q.; Chen, D.; Lei, Z.; Huang, Z.; Li, X.; Deng, K.; Lin, B.; Gao, Z. SARS-CoV-2 Can Be Detected in Urine, Blood, Anal Swabs, and Oropharyngeal Swabs Specimens. J. Med. Virol. 2020, 92, 1676–1680. [Google Scholar] [CrossRef] [PubMed]
- Yoon, J.G.; Yoon, J.; Song, J.Y.; Yoon, S.-Y.; Lim, C.S.; Seong, H.; Noh, J.Y.; Cheong, H.J.; Kim, W.J. Clinical Significance of a High SARS-CoV-2 Viral Load in the Saliva. J. Korean Med. Sci. 2020, 35. [Google Scholar] [CrossRef] [PubMed]
- Bivins, A.; Kaya, D.; Bibby, K.; Simpson, S.L.; Bustin, S.A.; Shanks, O.C.; Ahmed, W. Variability in RT-qPCR Assay Parameters Indicates Unreliable SARS-CoV-2 RNA Quantification for Wastewater Surveillance. Water Res. 2021, 203, 117516. [Google Scholar] [CrossRef] [PubMed]
- Huggett, J.F.; Foy, C.A.; Benes, V.; Emslie, K.; Garson, J.A.; Haynes, R.; Hellemans, J.; Kubista, M.; Mueller, R.D.; Nolan, T.; Pfaffl, M.W.; Shipley, G.L.; Vandesompele, J.; Wittwer, C.T.; Bustin, S.A. The Digital MIQE Guidelines: Minimum Information for Publication of Quantitative Digital PCR Experiments. Clin. Chem. 2013, 59, 892–902. [Google Scholar] [CrossRef] [PubMed]
- Bustin, S.A.; Benes, V.; Garson, J.A.; Hellemans, J.; Huggett, J.; Kubista, M.; Mueller, R.; Nolan, T.; Pfaffl, M.W.; Shipley, G.L.; Vandesompele, J.; Wittwer, C.T. The MIQE Guidelines: Minimum Information for Publication of Quantitative Real-Time PCR Experiments. Clin. Chem. 2009, 55, 611–622. [Google Scholar] [CrossRef]
- Liu, P.; Sablon, O.; Wang, Y.; Hilton, S.P.; Khalil, L.; Ingersoll, J.M.; Truell, J.; Edupuganti, S.; Alaaeddine, G.; Naji, A.; Monarrez, E.; Wolfe, M.; Rouphael, N.; Kraft, C.; Moe, C.L. Longitudinal Fecal Shedding of SARS-CoV-2, Pepper Mild Mottle Virus, and Human Mitochondrial DNA in COVID-19 Patients. Front. Med. 2024, 11. [Google Scholar] [CrossRef]
- Janovičová, Ľ.; Kmeťová, K.; Tóthová, Ľ.; Vlková, B.; Celec, P. DNA in Fresh Urine Supernatant Is Not Affected by Additional Centrifugation and Is Protected against Deoxyribonuclease. Mol. Cell. Probes 2023, 68, 101900. [Google Scholar] [CrossRef]
- Su, Y.-H.; Wang, M.; Brenner, D.E.; Ng, A.; Melkonyan, H.; Umansky, S.; Syngal, S.; Block, T.M. Human Urine Contains Small, 150 to 250 Nucleotide-Sized, Soluble DNA Derived from the Circulation and May Be Useful in the Detection of Colorectal Cancer. J. Mol. Diagn. 2004, 6, 101–107. [Google Scholar] [CrossRef]
- Wang, M.; Xiong, H.; Chen, H.; Li, Q.; Ruan, X.Z. Renal Injury by SARS-CoV-2 Infection: A Systematic Review. Kidney Dis. 2020, 7, 100–110. [Google Scholar] [CrossRef]
- Cheung, M.D.; Erman, E.N.; Liu, S.; Erdmann, N.B.; Ghajar-Rahimi, G.; Moore, K.H.; Edberg, J.C.; George, J.F.; Agarwal, A. Single-Cell RNA Sequencing of Urinary Cells Reveals Distinct Cellular Diversity in COVID-19-Associated AKI. Kidney360 2022, 3, 28–36. [Google Scholar] [CrossRef]
- Sun, J.; Zhu, A.; Li, H.; Zheng, K.; Zhuang, Z.; Chen, Z.; Shi, Y.; Zhang, Z.; Chen, S.-B.; Liu, X.; Dai, J.; Li, X.; Huang, S.; Huang, X.; Luo, L.; Wen, L.; Zhuo, J.; Li, Y.; Wang, Y.; Zhang, L.; Zhang, Y.; Li, F.; Feng, L.; Chen, X.; Zhong, N.; Yang, Z.; Huang, J.; Zhao, J.; Li, Y.-M. Isolation of Infectious SARS-CoV-2 from Urine of a COVID-19 Patient. Emerg. Microbes Infect. 2020, 9, 991–993. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.; Song, L.; Zheng, N.; Shi, J.; Wu, H.; Yang, X.; Xue, N.; Chen, X.; Li, Y.; Sun, C.; Chen, C.; Tang, L.; Ni, X.; Wang, Y.; Shi, Y.; Guo, J.; Wang, G.; Zhang, Z.; Qin, J. A Urinary Proteomic Landscape of COVID-19 Progression Identifies Signaling Pathways and Therapeutic Options. Sci. China Life Sci. 2022, 65, 1866–1880. [Google Scholar] [CrossRef] [PubMed]
- Wendt, R.; Thijs, L.; Kalbitz, S.; Mischak, H.; Siwy, J.; Raad, J.; Metzger, J.; Neuhaus, B.; Leyen, H.v.d.; Dudoignon, E.; Mebazaa, A.; Spasovski, G.; Milenkova, M.; Canevska-Talevska, A.; Czerwieńska, B.; Wiecek, A.; Peters, B.; Nilsson, Å.; Schwab, M.; Rothfuss, K.; Lübbert, C.; Staessen, J.A.; Beige, J. A Urinary Peptidomic Profile Predicts Outcome in SARS-CoV-2-Infected Patients. eClinicalMedicine 2021, 36. [Google Scholar] [CrossRef] [PubMed]
- Chavan, S.; Mangalaparthi, K.K.; Singh, S.; Renuse, S.; Vanderboom, P.M.; Madugundu, A.K.; Budhraja, R.; McAulay, K.; Grys, T.E.; Rule, A.D.; Alexander, M.P.; O’Horo, J.C.; Badley, A.D.; Pandey, A. Mass Spectrometric Analysis of Urine from COVID-19 Patients for Detection of SARS-CoV-2 Viral Antigen and to Study Host Response. J. Proteome Res. 2021, 20, 3404–3413. [Google Scholar] [CrossRef] [PubMed]
- Tampe, D.; Hakroush, S.; Bösherz, M.-S.; Franz, J.; Hofmann-Winkler, H.; Pöhlmann, S.; Kluge, S.; Moerer, O.; Stadelmann, C.; Ströbel, P.; Winkler, M.S.; Tampe, B. Urinary Levels of SARS-CoV-2 Nucleocapsid Protein Associate With Risk of AKI and COVID-19 Severity: A Single-Center Observational Study. Front. Med. 2021, 8. [Google Scholar] [CrossRef]
- George, S.; Pal, A.C.; Gagnon, J.; Timalsina, S.; Singh, P.; Vydyam, P.; Munshi, M.; Chiu, J.E.; Renard, I.; Harden, C.A.; Ott, I.M.; Watkins, A.E.; Vogels, C.B.F.; Lu, P.; Tokuyama, M.; Venkataraman, A.; Casanovas-Massana, A.; Wyllie, A.L.; Rao, V.; Campbell, M.; Farhadian, S.F.; Grubaugh, N.D.; Dela Cruz, C.S.; Ko, A.I.; Berna Perez, A.Z.; Akaho, E.H.; Moledina, D.G.; Testani, J.; John, A.R.; Ledizet, M.; Mamoun, C.B. Evidence for SARS-CoV-2 Spike Protein in the Urine of COVID-19 Patients. Kidney360 2021, 2, 924–936. [Google Scholar] [CrossRef]
- Markt, R.; Stillebacher, F.; Nägele, F.; Kammerer, A.; Peer, N.; Payr, M.; Scheffknecht, C.; Dria, S.; Draxl-Weiskopf, S.; Mayr, M.; Rauch, W.; Kreuzinger, N.; Rainer, L.; Bachner, F.; Zuba, M.; Ostermann, H.; Lackner, N.; Insam, H.; Wagner, A.O. Expanding the Pathogen Panel in Wastewater Epidemiology to Influenza and Norovirus. Viruses 2023, 15, 263. [Google Scholar] [CrossRef]
- Kilaru, P.; Hill, D.; Anderson, K.; Collins, M.B.; Green, H.; Kmush, B.L.; Larsen, D.A. Wastewater Surveillance for Infectious Disease: A Systematic Review. Am. J. Epidemiol. 2023, 192, 305–322. [Google Scholar] [CrossRef]
- Keshaviah, A.; Diamond, M.B.; Wade, M.J.; Scarpino, S.V.; Ahmed, W.; Amman, F.; Aruna, O.; Badilla-Aguilar, A.; Bar-Or, I.; Bergthaler, A.; et al. . Wastewater Monitoring Can Anchor Global Disease Surveillance Systems. Lancet Glob. Health 2023, 11, e976–e981. [Google Scholar] [CrossRef]
- Lee, W.L.; Gu, X.; Armas, F.; Leifels, M.; Wu, F.; Chandra, F.; Chua, F.J.D.; Syenina, A.; Chen, H.; Cheng, D.; Ooi, E.E.; Wuertz, S.; Alm, E.J.; Thompson, J. Monitoring Human Arboviral Diseases through Wastewater Surveillance: Challenges, Progress and Future Opportunities. Water Res. 2022, 223, 118904. [Google Scholar] [CrossRef]
- Chen, W.; Bibby, K. Model-Based Theoretical Evaluation of the Feasibility of Using Wastewater-Based Epidemiology to Monitor Monkeypox. Environ. Sci. Technol. Lett. 2022, 9, 772–778. [Google Scholar] [CrossRef]
- Chen, W.; Bibby, K. Making Waves: Establishing a Modeling Framework to Evaluate Novel Targets for Wastewater-Based Surveillance. Water Res. 2023, 245, 120573. [Google Scholar] [CrossRef] [PubMed]
- Chen, W.; Bibby, K. A Model-Based Framework to Assess the Feasibility of Monitoring Zika Virus with Wastewater-Based Epidemiology. ACS EST Water 2023, 3, 1071–1081. [Google Scholar] [CrossRef]
- Lowry, S.A.; Wolfe, M.K.; Boehm, A.B. Respiratory Virus Concentrations in Human Excretions That Contribute to Wastewater: A Systematic Review and Meta-Analysis. J. Water Health 2023, 21, 831–848. [Google Scholar] [CrossRef]
- Rauch, W.; Brockmann, D.; Peters, I.; Larsen, T.A.; Gujer, W. Combining Urine Separation with Waste Design: An Analysis Using a Stochastic Model for Urine Production. Water Res. 2003, 37, 681–689. [Google Scholar] [CrossRef]
- Vo, V.; Harrington, A.; Chang, C.-L.; Baker, H.; Moshi, M.A.; Ghani, N.; Itorralba, J.Y.; Tillett, R.L.; Dahlmann, E.; Basazinew, N.; Gu, R.; Familara, T.D.; Boss, S.; Vanderford, F.; Ghani, M.; Tang, A.J.; Matthews, A.; Papp, K.; Khan, E.; Koutras, C.; Kan, H.-Y.; Lockett, C.; Gerrity, D.; Oh, E.C. Identification and Genome Sequencing of an Influenza H3N2 Variant in Wastewater from Elementary Schools during a Surge of Influenza A Cases in Las Vegas, Nevada. Sci. Total Environ. 2023, 872, 162058. [Google Scholar] [CrossRef]
- St-Onge, G.; Davis, J.T.; Hébert-Dufresne, L.; Allard, A.; Urbinati, A.; Scarpino, S.V.; Chinazzi, M.; Vespignani, A. Optimization and Performance Analytics of Global Aircraft-Based Wastewater Surveillance Networks. medRxiv August 4, 2024, p 2024.08.02.24311418. [CrossRef]
Figure 1.
(A) Equivalent sample volume (ESV, µL of urine) achieved by the workflows reported in 8 studies measuring SARS-CoV-2 RNA in the urine of COVID-19 patients. (B) SARS-CoV-2 RNA urinary shedding prevalence among COVID-19 patients is normally distributed as a function of the natural log of the ESV (r2 = 1.00).
Figure 1.
(A) Equivalent sample volume (ESV, µL of urine) achieved by the workflows reported in 8 studies measuring SARS-CoV-2 RNA in the urine of COVID-19 patients. (B) SARS-CoV-2 RNA urinary shedding prevalence among COVID-19 patients is normally distributed as a function of the natural log of the ESV (r2 = 1.00).
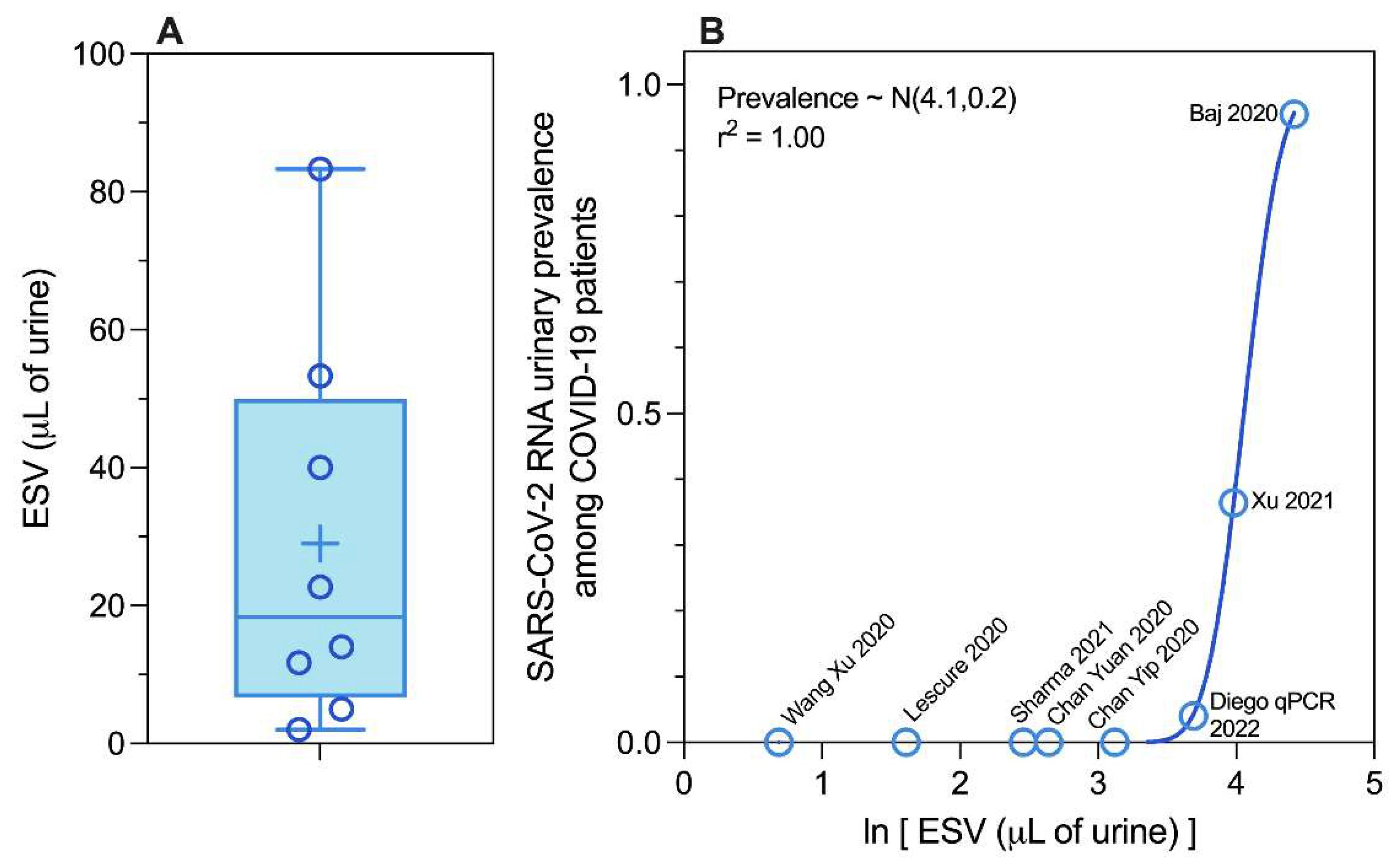
Figure 2.
SARS-CoV-2 RNA abundance in urine as observed during 11 studies analyzing urine from COVID-19 patients, including the number of patients sampled (n) and the urinary prevalence of RNA observed (p) during each study.
Figure 2.
SARS-CoV-2 RNA abundance in urine as observed during 11 studies analyzing urine from COVID-19 patients, including the number of patients sampled (n) and the urinary prevalence of RNA observed (p) during each study.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



