
Submitted:
21 October 2024
Posted:
24 October 2024
You are already at the latest version
Abstract
Malaria remains a public health challenge in low- and middle-income countries (LMICs). Despite gains from strategies like Insecticide Treated Nets (ITNs) and Intermittent Preventive Treatment during pregnancy (IPTp), significant socioeconomic inequalities persist, particularly among pregnant women and children under five. This study analysed temporal and socioeconomic inequalities in malaria prevention in sub-Saharan Africa (SSA). Methods: Nationally representative Demographic Health Surveys from 10 SSA countries were used, comparing two time periods. Changes in ITN use by pregnant women and children under five, as well as IPTp coverage, were assessed. Inequalities based on socioeconomic status (SES) and residence were analysed using the Erreygers Normalized Concentration Index and Theil index.. Results: Results revealed significant variability in ITN use and IPTp coverage between and within countries. Eight countries showed improvements in ITN use during pregnancy, with Nigeria seeing a 173.9% increase over five years. Burkina Faso and Tanzania consistently reported high ITN use (~87%) in children under five. IPTp coverage increased in all countries except Kenya. Decomposition using the Theil index indicated that within-group inequalities, particularly based on SES and residence, were the primary drivers of disparities. Conclusion: To ensure progress toward universal health coverage, malaria prevention programs must prioritize vulnerable populations and be continuously evaluated.
Keywords:
Malaria prevention
; Pregnant women
; Under-five children
; Socioeconomic inequality
; Insecticide Treated Nets (ITNs)
; Intermittent Preventive Treatment (IPTp)
1. Introduction
Violence Malaria remains one of the most common diseases in Low-and Middle-income countries (LMICs). In 2022, the World Health Organisation reported that there were an estimated 249 million malaria cases and 608,000 malaria deaths globally, most of which occurred in LMICs [1]. The burden of malaria is most felt in the African region with 94% of all global malaria cases occurring in sub-Saharan Africa (SSA), and four countries Nigeria (27%), the Democratic Republic of the Congo (12%), Uganda (5%) and Mozambique (4%) accounting for almost half of all cases globally in 2022 [1]. Vulnerable populations such as pregnant women and children under the age of five in malaria endemic countries face heightened risk of malaria. In 2022 alone, 12.7 million malaria cases were reported among pregnant women across 33 SSA countries while a significant proportion of malaria deaths occurred among children under five years [1,2]. In the past two decades, however, significant gains have been made in the fight against malaria [3]. For instance, between 2000 and 2021, the global malaria mortality decreased by 32.6% while the global malaria incidence decreased by 21.1% [4]. These gains have been made possible by an increased coverage of malaria interventions such as insecticide treated nets (ITNs), in-door residual spraying (IRS), malaria treatment and chemoprevention [1].
Prior to 2008, malaria control interventions were targeted at pregnant women and children aged under five by prioritizing distribution of ITNs through routine vaccinations, antenatal clinics, social marketing of subsidized or free malaria commodities [5,6]. Equity in the distribution of malaria interventions distributed through these channels emerged as a concern as wealthy urban households who had better access to healthcare services relative to rural-poor households enjoyed better coverage by these malaria interventions [7,8]. This approach to distribution of malaria interventions changed with the call from the United Nations Secretary General for universal coverage with malaria interventions [9]. Consequently, in malaria endemic countries, there was a shift from targeted to mass ITN distribution through community delivery supported by routine services [3]. In addition, in 2004, in response to emerging parasite resistance, fast-acting artemisinin-based combination therapies (ACTs) replaced monotherapy as the recommended first-line treatment for uncomplicated malaria [10]. Through the support of the Global Fund and novel financing mechanisms such as the Affordable Medicines Facility-malaria, ACTs were made available in malaria endemic countries [11]. The involvement of community health workers, among other innovative distributional channels in malaria endemic countries reduced the inequality gap between the poorest and least poor in coverage with these malaria interventions [12].
Intermittent preventive treatment during pregnancy (IPTp), use of ITNs and effective case management of malaria and anaemia are the package of interventions recommended by WHO in areas with stable to high transmission of P.falciparum to tackle malaria in pregnancy [13]. Sulphadoxine-pyrimethamine is currently the most effective drug for IPTp in areas of high or seasonal transmission as it has been shown to lower placental infection rates, increase both maternal haemoglobin levels and the infants’ birth weight [14,15]. Intermittent preventive therapy with SP (IPTp-SP) for malaria in pregnancy is delivered to pregnant women as they attend antenatal clinics (ANC)[16]. Evidence suggests that despite high ANC attendance in most SSA countries, coverage with ITNs and IPTp-SP remains sub-optimally below the 80% target [17]. Evidence from meta-analysis of factors affecting the delivery, access and use of interventions to prevent malaria in pregnancy in SSA have identified socioeconomic status [18,19,20], education, knowledge and perceptions about malaria [21,22], number and timing of ANC visits [20,22], number of pregnancies and health system inadequacies [20,21] as factors that influence intervention coverage as well as access to ANC services.
Whilst available evidence suggests that progress has been made in malaria prevention, there are persistent inequalities in the uptake of malaria prevention strategies between the poorest and the richest [23,24]. Previous studies have evaluated inequalities in the coverage of malaria control interventions, mostly ITNs and outlined the role of socioeconomic status as one of the important predictors in the use and coverage of malaria control interventions [25,26]. Two previous studies assessed equity in coverage of a number of malaria control interventions across a number of malaria endemic African countries [3,7]. These studies provided mixed equity findings on the coverage of malaria control interventions. A dated study by Steketee et al. (2009) found that in 13 out of the 25 countries assessed, malaria treatment for febrile children and IPTp-SP for pregnant women were inequitable whilst ITN ownership was equitable [7]. Conversely, the study by Galactionova, Smith, de Savigny and Penny [3] which examined data from 30 malaria-endemic sub-Saharan African (SSA) countries using Demographic and Health and Malaria Indicator Survey data between 2005 and 2015 found that there were still wide inequities in the coverage of malaria interventions and their distribution by socioeconomic status within and across countries [3].
To our knowledge, previous studies examining inequalities in the utilization of malaria prevention interventions among pregnant women and children under-five have largely classified populations by socioeconomic status. However, there is sparse evidence that accounts for the diversity within these groups. This tends to obscure existing disparities and may limit the effectiveness of public interventions. Utilizing the most recent Demographic Health Survey (DHS) datasets from 10 SSA countries, the present study adds to existing evidence by; (1) analysing the trends in the uptake of malaria prevention interventions (ITNs use by pregnant women and children under 5, IPTp coverage in pregnancy) over time, (2) investigating the between-socioeconomic and residence group intertemporal inequalities in the uptake of these malaria prevention strategies, (3) examining the within-socioeconomic and residence group intertemporal inequalities in the uptake of these malaria prevention strategies, and, finally examining the contribution of between and within -group inequality to the overall inequality in ITN use and IPTp coverage.
By understanding trends in uptake of malaria prevention strategies as well as characterizing associated between and within group inequalities, this study can support evidence-based policy aimed at achieving equitable access to malaria prevention tools. Also, it can help align national malaria programs with global health goals, such as Universal Health Coverage (UHC), Sustainable Development Goal 3 (Good Health and Well-being), and Sustainable Development Goal 10 (Reduced inequalities).
2. Materials and Methods
2.1. Data
This study utilized publicly available nationally representative data from the Demographic Health Surveys (DHS). The countries studied were Mozambique (2011 & 2022/23), Burkina Faso (2010 & 2021), Tanzania (2015/16 & 2022), Côte d'Ivoire (2011/12 & 2021), Madagascar (2008/9 & 2021), Kenya (2014 & 2022), Rwanda (2014/15 & 2019/20), Nigeria (2013 & 2018), Uganda (2011 & 2016), and Cameroon (2011 & 2018). These countries were chosen based on two criteria; firstly, the availability of recent datasets and secondly, having the highest malaria incidence as reported by the 2023 World Health Organization Malaria report [27]. With the recommendation from DHS [28], the household member recode (PR), the individual recode file for women (IR) and the household recode (HR) file were merged for each country and each year, which resulted in 20 datasets that were appended into one file for final analysis.
2.2. Ethical Considerations
The secondary analysis in this study utilized publicly available Demographic and Health Survey (DHS) data from 10 sub-Saharan African countries. As such, no direct ethical approval was sought for this analysis. The original DHS data collection protocols were reviewed and approved by the respective national ethics review boards and the Institutional Review Board (IRB) of ICF International, ensuring the protection of participants' welfare and rights. The data are de-identified and publicly accessible, minimizing any risk to participants. Additionally, the data are governed by strict confidentiality protocols in accordance with the DHS Program's data use policies.
2.3. Study Variables
2.3.1. Outcome Variables
The outcome variables for this study were: ITN use by pregnant women, ITN use by children under five, and IPTp coverage. These variables were operationalized based on DHS guidance and their definition in previous studies as well as by virtue of being malaria interventions coverage indicators [27]. ITN use by pregnant women was defined as women aged 15-49 who, lived in a household with at least one insecticide-treated net (ITN), slept under an ITN the night before the survey [28,29]. The use of insecticide-treated nets (ITNs) by children under five was described as children living in households with at least one ITN who slept under it on the night prior to the survey [30].The third variable IPTp coverage, was defined as women aged 15 to 49 who had a live birth or stillbirth within two years before the survey and received three or more doses of Sulphadoxine-Pyrimethamine (SP) during their pregnancy [31,32].
For all countries, all these three outcome variables were computed, except for Rwanda where it was not possible to compute IPTp coverage due to data limitations. Regardless, Rwanda was included as it is one of the countries where malaria incidence has significantly declined in recent years. In 2022, the incidence rate was reduced to 76 cases per 1,000 people from 409 per 1,000 in 2016, marking a 39% decrease [27].
2.3.2. SES and Place of Residence
The Socioeconomic status (SES) and place of residence are key determinants that help in understanding disparities across different population groups. This study measured SES using the already computed wealth index in the DHS. Place of residence was determined using rural versus urban living.
2.4. Statistical Analysis
Data analysis was carried out using STATA 17. First, preliminary analysis was conducted to describe the sample and explore patterns of ITN use in pregnancy and under-fives as well as IPTp coverage. Consequently, Erreygers Normalized Concentration indices (ENCI) and Theil indices were computed to understand inequalities in the outcome measures. All the findings of this study ought to interpreted bearing in mind the differences in time periods between the two datasets for the various countries.
2.4.1. Erreygers Normalised Concentration Index (ENCI)
Inequalities in ITN use and IPTp coverage were first computed using the ENCI, a single summary measure which ranges from -1 to +1 [33]. A positive ENCI denotes that a health variable (ITN use and IPTp coverage) is more concentrated among wealthier socioeconomic groups and vice versa. An ENCI of zero denotes perfect equality.
The Erreygers normalized concentration index is calculated as shown below;
where:
μ is the mean of the health variable; (ITN use in under-fives, ITN use in pregnancy, IPTp Coverage).
b and a are the upper and lower bounds of the health variable, respectively.
C is the traditional concentration index.
The traditional concentration index is calculated as shown below:
where;
y is the health variable (ITN use in under-fives, ITN use in pregnancy, IPTp Coverage).
μ is the mean of y
is the fractional rank of individuals in the distribution of SES.
denotes the covariance between y and R
2.4.2. Theil Indices
Given that the ENCI was unable to demonstrate the extent to which inequality in ITN use in under-fives, ITN use in pregnancy, or IPTp Coverage is due to differences between and within SES and place of residence, this study computed Theil indices. This index, a Generalized Entropy index GE(2), permits the decomposition of inequality into its within-group and between-group components [34].
In this study, Theil indices were first calculated for the entire sample and then disaggregated by socioeconomic status (SES) and place of residence. Subsequently, the Theil indices were further decomposed to evaluate the contributions of both within-group and between-group components to the total inequality.
The GE(2) index ranges from 0 to infinity, where a value of 0 indicates perfect equality, and values above 0 signify increasing levels of inequality.
The GE(2) index is calculated as follows:
where;
is the outcome for individual is the mean of the outcome variable
is the total number of individuals.
The overall GE(2) index is then decomposed into within-group and between-group components as shown:
where;
represents within-group inequality and,
represents between-group inequality
The within-group and between-group contributions to overall inequality in health outcomes (ITN use in under-fives, ITN use in pregnancy, IPTp Coverage) were calculated as follows:
3. Results
3.1. Descriptive Statistics
Table 1 presents the proportions of ITN use in pregnancy, ITN use by under-fives and IPTp coverage. Results demonstrated a general trend of improvement in ITN use during pregnancy over time in most countries, although there were notable exceptions such as Kenya and Rwanda where slight decreases were observed. Nigeria saw a dramatic increase in ITN use during pregnancy from 29.82% in 2013 to 81.67% in 2018, and such a huge increase was also observed in Cameroon and Côte d'Ivoire indicating a strong push for malaria prevention. For ITN use by under-fives, Nigeria registered the lowest prevalence (31.48% in 2013) but this dramatically improved to 80% in 2018. Cameroon also demonstrated strong improvements over time, with more than a 20 percentage point increase in under-five ITN use. Burkina Faso and Tanzania both showed consistently high levels of ITN use by under-fives, both countries achieving approximately 87% by 2021/2022.
With regards to IPTp coverage, the reported prevalences are much lower compared to those of ITN use in pregnancy and by under-fives. The highest prevalences reported were in Burkina Faso (56.68%, 2021), Cameroon (32.54%, 2018), and Madagascar (30.96%, 2021). Burkina Faso had the highest increase in IPTp coverage, going from 40.95% in 2010 to 56.68% in 2021 while Madagascar saw a remarkable rise in IPTp coverage from 1.93% in 2008/09 to 30.96% by 2021. Kenya on the other hand, experienced a decline in IPTp coverage, from 10.55% in 2014 to 6.45% in 2022, highlighting a potential issue in malaria prevention during pregnancy.
In general, Burkina Faso consistently showed high and improving prevalences in all three areas (ITN use in pregnancy, ITN use by under-fives, and IPTp coverage), positioning it as a strong performer in malaria prevention. Nigeria also exhibited the most remarkable improvement, particularly in ITN use in pregnancy and among under-fives, with significant increases between 2013 and 2018. However, Kenya and Rwanda showed slight declines or stagnation in key indicators, signalling potential areas for concern and further investigation into barriers to prevention efforts.
3.2. Concentration Indices and Curves
As shown in Table 2, it is evident that Nigeria and Côte d'Ivoire had the largest concentration of ITN use in pregnancy among the poor with Côte d'Ivoire ENCI value decreased from -0.117 in 2011/12 to -0.216 in 2021. Nigeria observed a notable shift from pro-rich inequality (0.067 in 2013) to significant pro-poor inequality in 2018 (-0.156, p = 0.000) suggesting a redistribution of ITN use towards poorer populations. Rwanda and Kenya on the other hand, show persistent pro-rich inequality in ITN use during pregnancy, with Rwanda's inequality increasing slightly over time.
As shown in Table 3, Cameroon and Mozambique show the highest levels of pro-rich inequality in IPTp coverage in the most recent years, with Cameroon (2018) having the highest ENCI overall. Additionally, Cameroon, Mozambique, Nigeria, Côte d'Ivoire, and Madagascar, saw an increase in ENCI over two study periods, indicating a growing concentration of IPTp coverage among wealthier women.
From Table 4, it is observed that Côte d'Ivoire and Nigeria experienced the largest shifts toward pro-poor outcomes, with Côte d'Ivoire (2021) showing the strongest pro-poor concentration of ITN use among under-fives. For Côte d'Ivoire, the ENCI became more negative over time, shifting from -0.090 in 2011/12 to -0.183 in 2021 while for Nigeria the ENCI moved dramatically from 0.060 (pro-rich inequality) in 2013 to -0.139 (pro-poor inequality) in 2018, reflecting a redistribution of ITN use to poorer households. Kenya, Mozambique, and Rwanda consistently exhibit pro-rich inequality, although in Kenya, this inequality has been reduced over time.
The Lorenz curves in Figure 1 illustrate the distribution of ITN use in pregnancy, ITN use by under-fives, and IPTp coverage by SES across SSA in two different years per country. In general, the curves for IPTp coverage, are well below the line of equality, indicating a pro-rich distribution. That is, of all the three interventions, IPTp coverage is mostly concentrated among wealthier households pointing to the need to improve access to and utilization of IPTp in poor populations.
3.3. Theil Indices for ITN Use in Pregnancy, ITN Use by Under-Fives Distinguished by Place of Residence
Table 5, shows major improvements in equity for ITN use and IPTp coverage in Mozambique, Côte d’Ivoire, Nigeria, Uganda, and Cameroon, with substantial reductions in Theil indices over time, particularly for rural areas. In Mozambique, inequality in ITN use in pregnancy decreased significantly from 0.215 (urban) and 0.444 (rural) in 2011 to 0.164 (urban) and 0.221 (rural) in 2022/23, indicating reduced inequality across both urban and rural settings. For IPTp coverage, inequality increased dramatically, especially in rural areas, rising from 0.674 in 2011 to 1.874 in 2022/23, suggesting that rural women are now facing significantly more unequal access to IPTp services.
With ITN use by under-fives, inequality decreased over time, with urban areas moving from 0.236 to 0.099, and rural areas from 0.345 to 0.189 in 2022/23, indicating better distribution of ITN use among children. For Côte d'Ivoire, inequality in the use of ITNs in pregnancy decreased significantly from 0.429 (urban) and 0.295 (rural) in 2011/12 to 0.172 (urban) and 0.096 (rural) in 2021, showing much greater equity in ITN distribution by 2021. Similarly, for IPTp coverage inequality fell drastically from 5.161 (urban) and 7.592 (rural) to 0.940 and 1.207, respectively, reflecting improved equity in IPTp coverage. With ITN use by under-fives, both urban and rural areas show reduced inequality, with urban GE(2) dropping from 0.407 to 0.186 and rural GE(2) from 0.285 to 0.090.
For Nigeria, inequality in ITN use in pregnancy significantly reduced, with urban GE(2) falling from 0.891 to 0.179 and rural GE(2) from 1.273 to 0.093 by 2018, indicating much greater equality in ITN use. IPTp coverage reported a dramatic decrease in inequality, with urban GE(2) dropping from 6.905 to 1.880 and rural GE(2) from 7.281 to 2.848, indicating a more equal distribution of IPTp coverage by 2018. Similarly, with ITN use by under-fives, inequality decreased sharply, with both urban and rural areas seeing significant improvements in access for both groups.
3.4. Theil Indices for ITN Use in Pregnancy, ITN Use by Under-Fives Distinguished by SES
Analyzing the Theil indices by SES (as shown in Table 6), shows an improved equity in ITN use in pregnancy, IPTp coverage, and ITN use by under-fives across several countries, particularly Mozambique, Nigeria, Burkina Faso, Tanzania, Côte d’Ivoire, and Cameroon, where inequality decreased significantly across the three socioeconomic classes. Of these countries, Nigeria demonstrated a dramatic improvement in ITN use and IPTp coverage for all groups, especially the poor, by 2018. Conversely, Kenya and Rwanda saw increases in inequality in malaria prevention, with poorer groups facing higher inequality. Of the three malaria prevention interventions, IPTp coverage generally exhibits the highest levels of inequality across most countries and years, but the trend shows improvement over time, especially among poor groups.
3.5. Decomposition of Theil Indices by Place of Residence
The largest reductions in overall inequality in ITN use in pregnancy were reported in Cameroon (improved by 0.375 points), Côte d'Ivoire (improved by 0.208 points), and Mozambique (improved by 0.154 points). Conversely, Kenya and Rwanda recorded slight increases in overall inequality in ITN use in pregnancy (Table 7). For ITN use by under-fives, Mozambique, Côte d'Ivoire and Cameroon, the overall inequality reduced over time meaning that these countries made significant progress in reducing inequality in ITN access for this population. For IPTp coverage, Madagascar (21 points), Nigeria (4.74 points), and Mozambique (3.49 points) had the highest decreases in overall inequality suggesting improving equity in access to IPTp coverage. On the other hand, Kenya observed the largest increase in overall inequality for IPTp coverage, with an increase of 2.987 points. This indicates a widening gap in access to IPTp services, with advantaged groups increasingly benefiting more than disadvantaged groups by 2022.
Regarding the contribution of within and between-group components to the overall inequality, between-group inequality contributed very little to the overall inequality in all countries, with within-group inequality being the dominant factor across the board. Cameroon had the largest increase in the between-group contribution for IPTp coverage (+1.74%), indicating widening gaps between different population groups. Mozambique and Nigeria also saw increases in between-group contributions, though to a lesser extent. Burkina Faso had minimal between-group inequality in both years, indicating that most inequality in IPTp coverage is driven by within-group differences. Mozambique also reported a major decrease in within-group inequality (-3.498 points), reflecting a large improvement in equity for IPTp coverage within groups.
Madagascar had the largest decrease in within-group inequality (-21.099 points), with almost all inequality coming from disparities within population groups (e.g., urban groups, rural groups). This signals a significant improvement in equity for IPTp coverage within the two groups over time. Lastly, Kenya experienced a worsening within-group inequality, with the within-group contribution rising by +2.985 points. This means that inequality worsened within people of the same place of residence, contributing to the overall increase in inequality for IPTp coverage.
3.6. Decomposition of Theil Indices by SES
Table 8 shows the decomposition of Theil indices by SES. it is observed that Cameroon had the largest decrease in overall inequality for ITN use in pregnancy (-0.375), while Rwanda had a slight increase in inequality for ITN use in pregnancy (+0.039). Nigeria saw the largest decrease in overall inequality for ITN use among under-fives (-0.908), while Tanzania had a smaller decrease (-0.073), indicating less change over time. Madagascar had the largest decrease in overall inequality for IPTp coverage (-21.099), showing a dramatic improvement in equity, while Kenya had the largest increase in inequality for IPTp coverage (+2.987), indicating worsening access disparities.
Côte d'Ivoire saw the largest increase in between-group inequality for ITN use in pregnancy, with the contribution from between-group disparities rising by 5.94%. This indicates that inequality between socioeconomic classes became more pronounced over time. Cameroon experienced the largest decrease in within-group inequality for ITN use in pregnancy, with the contribution of within-group disparities decreasing by 0.371 points. This suggests improved equity within socioeconomic groups, although overall inequality still remains.
On ITN use by under-fives, Cameroon demonstrated the largest decrease in between-group inequality for ITN use by under-fives, with the contribution of between-group disparities reducing to 0% by 2018. This indicates a reduction in disparities between socioeconomic classes. Mozambique had the largest increase in between-group inequality for IPTp coverage, with the contribution from between-group disparities increasing by 2.22%. This indicates that differences between socioeconomic groups became more prominent over time.
Lastly, Madagascar reported the largest decrease in within-group inequality for IPTp coverage, with the within-group contribution dropping by 21.104 points. This represents a dramatic improvement in equity within SES groups. Across all countries, the majority of the inequality in ITN use in pregnancy, ITN use by under-fives, and IPTp coverage is driven by within- socioeconomic group disparities rather than between-group differences. The within-group contributions are highest (often at 100%) in most countries, indicating that disparities within people of the same socioeconomic class are the main source of inequality.
4. Discussion
The aim of this study was to examine the temporal and socioeconomic inequalities associated with three critical malaria prevention interventions: ITN use during pregnancy, ITN use among children under five, and IPTp coverage across 10 Sub-Saharan African countries. Drawing on DHS surveys from two different time points per country, this analysis explored how the distribution of these interventions changed over time and the extent to which socioeconomic status (SES) and place of residence influenced access to these essential malaria intervention tools. Our study findings highlighted considerable variability in the proportions of ITN use during pregnancy, ITN use by children under five, and IPTp coverage both across the 10 countries and over time. While countries like Nigeria and Burkina Faso demonstrated remarkable progress, others, such as Kenya and Rwanda, experienced stagnation or even declines in key indicators, reflecting a nuanced landscape of malaria prevention efforts. This variation aligns with previous research that has documented the uneven success of national malaria programs, largely due to differing levels of healthcare infrastructure, resource allocation, and the effectiveness of implementation strategies [35]. Burkina Faso's consistent high coverage in both ITN use and IPTp, even in rural areas, underscores the importance of sustained and targeted interventions. Such improvements parallel findings from Bhatt, et al. [36], who emphasized that large-scale distribution of malaria prevention tools, combined with effective public health campaigns, can lead to significant reductions in malaria transmission and improve overall health outcomes in vulnerable populations [36].
Moreover, the trends observed in Kenya and Rwanda, where some indicators either stagnated or declined, suggest that barriers such as unequal healthcare access, geographic disparities, and perhaps lapses in policy implementation could be hindering progress. These results emphasize the need for more context-specific interventions that address the unique challenges faced by different countries and regions within them. This study thus contributes to the growing body of literature indicating that while significant strides have been made in malaria prevention, persistent inequalities, particularly related to socioeconomic status and place of residence, continue to impede universal access to life-saving interventions [37]
The concentration indices (ENCI) for ITN use during pregnancy present a complex picture of socioeconomic inequality in access to malaria prevention interventions. In countries such as Côte d'Ivoire and Nigeria, the results indicate a clear shift toward pro-poor inequality, meaning that ITN use was more concentrated among poorer populations over time. This shift suggests that national malaria programs in these countries have successfully implemented targeted interventions aimed at increasing ITN coverage among disadvantaged groups. Such outcomes align with findings from Talipouo, et al. [38], who reported that well-planned distribution campaigns can significantly improve ITN access in low-income communities [38].
However, the results also highlight persistent pro-rich inequality in other countries, notably Rwanda and Kenya, where wealthier households are still more likely to benefit from ITN use during pregnancy. This disparity is concerning because it suggests that despite overall improvements in ITN distribution, the poorest women, who are at the highest risk for malaria-related complications during pregnancy, are not receiving adequate protection. The increase in pro-rich inequality in Kenya over time is particularly troubling, as it implies that gains made in ITN distribution are disproportionately benefiting wealthier populations. This finding echoes the concerns raised by Sumari, et al. [39], who emphasized the need for more tailored interventions that specifically target vulnerable populations to close these gaps in access [39]. Without such targeted efforts, the most disadvantaged groups will continue to face barriers to accessing essential malaria prevention tools, which could undermine broader efforts to reduce malaria prevalence and mortality among pregnant women.
In contrast, the concentration indices for IPTp coverage show a more concerning picture of entrenched inequality across most countries studied. The results revealed a consistent pro-rich bias, meaning that wealthier women were more likely to access IPTp services compared to their poorer counterparts. This inequality was particularly pronounced in Cameroon, Mozambique, and Nigeria, where ENCI values indicated increasing inequality over time. The concentration of IPTp services among wealthier women in these countries is concerning, especially given the global emphasis on ensuring universal access to IPTp during pregnancy as part of comprehensive malaria prevention strategies. The results are consistent with previous studies, such as Kalu, et al. [40] and Ochieng, et al. [41], which found that malaria prevention services, including IPTp, are often more accessible to higher socioeconomic groups, particularly in urban areas where healthcare infrastructure is more developed [40,41]
The persistence of these inequalities in IPTp coverage suggests that systemic barriers, such as inadequate healthcare infrastructure in rural areas, financial constraints, and limited awareness of IPTp benefits, continue to hinder access for poorer women. These findings underscore the need for more inclusive malaria prevention policies that specifically address these barriers. For example, improving access to healthcare services in rural and remote areas, subsidizing IPTp for low-income women, and enhancing community outreach programs could help reduce these disparities [42].While countries such as Burkina Faso and Madagascar showed slight reductions in IPTp inequality, the overall low coverage of IPTp remains a significant public health challenge. As noted by Chen, et al. [43], scaling up IPTp services is essential to reducing the risk of malaria-related complications during pregnancy, particularly in underserved areas where women are most at risk [43]. The findings of this study reinforce the urgency of addressing these inequalities by prioritizing interventions that target low-income and rural populations, where the need for IPTp is greatest.
For ITN use among children under five, the concentration indices revealed stark disparities across the countries studied. In some countries, such as Côte d'Ivoire and Nigeria, there were significant shifts towards pro-poor ITN use, reflecting successful efforts to redistribute ITNs to poorer households. This shift is an encouraging sign that malaria prevention strategies in these countries are beginning to reach the most vulnerable populations, particularly children under five, who are at the greatest risk of severe malaria and death. The pro-poor trend in these countries aligns with findings from earlier studies, such as Maghendji-Nzondo, Nzoughe, Lemamy, Kouna, Pegha-Moukandja, Lekoulou, Mbatchi, Toure-Ndouo and Lekana-Douki [35], which highlighted the positive impact of targeted ITN interventions on improving access for disadvantaged households [35]. These results suggest that when malaria prevention campaigns are designed to prioritize equity, they can achieve meaningful improvements in ITN coverage among poorer populations, helping to protect children from the worst outcomes of malaria.
However, the analysis also showed that pro-rich inequality persists in countries like Kenya, Mozambique, and Rwanda, where wealthier households continue to have better access to ITNs for their children. This inequality is particularly concerning in countries with high malaria burdens, where children under five are especially vulnerable to severe malaria and related mortality. The continued concentration of ITN use among wealthier households in these countries suggests that malaria prevention campaigns have not been equally effective across all socioeconomic groups. This may be due to several factors, including geographic disparities in healthcare access, differences in awareness and education about ITNs [44], and financial barriers that prevent poorer families from acquiring sufficient ITNs. These findings are consistent with previous research, such as Talipouo, Ngadjeu, Doumbe-Belisse, Djamouko-Djonkam, Sonhafouo-Chiana, Kopya, Bamou, Awono-Ambene, Woromogo and Kekeunou [38], which emphasized the importance of prioritizing ITN distribution in the poorest and most rural communities to achieve more equitable health outcomes [38] .
Theil indices for ITN use in pregnancy, ITN use by children under five, and IPTp coverage revealed critical insights into the unequal distribution of malaria prevention services based on place of residence. In countries such as Mozambique, Côte d'Ivoire, and Nigeria, the analysis showed higher levels of inequalities in rural populations compared to their urban counterparts, particularly concerning IPTp coverage. This disparity in access to malaria prevention services between rural and urban areas has been well-documented in earlier studies, such as Assele, et al. [45], which identified rural residence as a significant determinant of limited access to essential health services, including malaria prevention tools [45]. The higher inequality in rural areas highlights the challenges faced by these communities, such as poor healthcare infrastructure, geographical barriers, and limited access to information on malaria prevention interventions [24].
However, a deeper examination through the decomposition of the Theil indices revealed that within-group inequality, rather than between-group inequality, was the predominant driver of overall disparities in most countries. This meant that while differences between rural and urban areas exist, the more significant issue lay within these groups, where the distribution of malaria prevention interventions is highly uneven. For instance, within both rural and urban populations, there are subgroups perhaps distinguished by income, education, or other socioeconomic factors that experienced vastly different levels of access to ITN use and IPTp coverage. This within-group inequality is a critical finding, as it suggests that targeting broad rural or urban populations without addressing these internal disparities may not be sufficient to reduce overall inequality. These results are in line with findings from Imboumy-Limoukou, et al. [46], who also emphasized the importance of addressing intra-group disparities to achieve more equitable health outcomes [46].
Theil indices by socioeconomic status (SES) further underscored the disparities in ITN use and IPTp coverage across different income groups. In countries like Nigeria, Burkina Faso, and Côte d'Ivoire, the data shows significant improvements, with overall inequality decreasing over time. These countries have made strides in reducing disparities in access to malaria prevention tools, likely due to targeted programs that have successfully reached the poorest households. In contrast, countries like Kenya and Rwanda have seen an increase in inequality, particularly regarding IPTp coverage. This trend is concerning, as it indicates that efforts to scale up malaria prevention interventions in these countries may not be reaching the most disadvantaged populations. Such findings are consistent with the observations of Maghendji-Nzondo, Nzoughe, Lemamy, Kouna, Pegha-Moukandja, Lekoulou, Mbatchi, Toure-Ndouo and Lekana-Douki [35], who documented similar patterns of increasing inequality in access to healthcare services in these countries [35]. The growing inequality in IPTp coverage, especially in Kenya and Rwanda, points to systemic barriers that disproportionately affect poorer women, such as financial constraints, inadequate healthcare infrastructure in rural areas, and lack of awareness about the benefits of IPTp [2,47].
Importantly, the persistence of within-group inequality among lower socioeconomic groups suggests that even within the poorest populations, there are subgroups that face more significant barriers to accessing malaria prevention interventions. These within-group disparities indicate that not all poor households are equally disadvantaged as some may still have relatively better access to services than others, due to factors like proximity to healthcare facilities, education, or community support networks. These finding highlighted the need for more targeted and finely-tuned interventions that address the unique challenges faced by different subgroups within the poorest populations. As argued by multiple authors, simply categorizing populations by socioeconomic status without recognizing the heterogeneity within these groups may obscure the true nature of health disparities and hinder the effectiveness of public health interventions [48,49,50]. Policies aimed at reducing inequality in malaria prevention must therefore consider the diverse needs of subpopulations within broader socioeconomic categories, ensuring that the most marginalized individuals receive adequate attention.
The decomposition of Theil indices by both place of residence and SES provides further insights into the complex nature of inequality in malaria prevention. Across most countries, between-group inequality whether between rural and urban areas or between different SES groups contributed very little to the overall inequality. Instead, within-group inequalities remained the primary driver of disparities in ITN use and IPTp coverage. These findings are crucial, as they suggest that while geographic and socioeconomic differences are important, the most significant inequalities are found within these larger population categories. This trend echoes the conclusions of Imboumy-Limoukou, Maghendji-Nzondo, Sir-Ondo-Enguier, Niemczura De Carvalho, Tsafack-Tegomo, Buekens, Okouga, Mouinga-Ondeme, Kwedy Nolna and Lekana-Douki [46], who emphasized that addressing disparities within population subgroups is essential for improving equity in access to malaria prevention services [46]. Focusing solely on broad categories like "rural" or "poor" may miss the difference and deeply ingrained inequalities that exist within these groups, which can perpetuate health disparities despite efforts to increase overall coverage.
However, for IPTp coverage specifically, the increase in between-group inequality observed in countries like Cameroon and Mozambique highlights a troubling trend of growing disparities between socioeconomic classes. This suggests that while overall IPTp coverage may be improving, wealthier women are benefiting disproportionately, exacerbating inequalities between the rich and poor. Addressing this issue will require more than just expanding IPTp services; it will necessitate a concerted effort to reduce socioeconomic inequalities by ensuring that the poorest and most vulnerable women have equal access to these life-saving interventions. These findings are a clear reminder that achieving equity in malaria prevention requires not only increasing coverage but also ensuring that the benefits of these interventions are distributed fairly across all population groups. Without addressing both within-group and between-group inequalities, the goal of universal access to malaria prevention tools will remain elusive [51].
To address these persistent disparities, it is essential for malaria prevention efforts to focus on expanding ITN access in underserved areas, particularly rural and low-income communities where the need is greatest [52].This could involve strengthening community-based distribution programs, improving healthcare infrastructure in remote areas, and increasing education and awareness campaigns that target vulnerable populations. Without concerted efforts to close these gaps, the benefits of ITN distribution will remain unevenly distributed, and the most disadvantaged children will continue to face an elevated risk of malaria-related illness and death [53]. Overall, the findings from the concentration indices of ITN use in pregnancy, IPTp coverage, and ITN use among children under five highlight the critical importance of addressing socioeconomic inequalities in malaria prevention efforts. While some countries have made notable progress in reducing these disparities, others continue to struggle with pro-rich inequality, which limits the effectiveness of malaria prevention strategies. Addressing these inequalities will require a coordinated effort to design and implement more inclusive policies that prioritize the needs of the poorest and most vulnerable populations. By doing so, countries can improve access to life-saving malaria prevention tools and reduce the burden of malaria on pregnant women and young children across Sub-Saharan Africa.
Limitations and Strengths
This study is not without limitations. First, this study utilized data from cross-sectional surveys, hence it is impossible to draw causal links between ITN use and IPTp coverage and SES/residence status. Second, while the study offered the opportunity to situate temporal trends of the outcomes at two time periods, the same cannot be said of individual level changes. Third, the Theil indices while offering policy relevant insights into between and within group inequalities it is more sensitive to changes at the extremes of socioeconomic distribution compared to other indices like the Gini coefficient and as such, it may overstate inequalities in cases where extremes are not representative of the larger population. Additionally, the Theil index has a lower bound of zero and this may mask nuances in relatively equal distributions as small variations in inequality are harder to detect compared to other measures [54].
Despite these limitations, this study has multiple strengths. First, because of utilizing high quality, nationally representative, and most-recent cross-country DHS datasets, findings from this study are robust and can be generalized across multiple contexts in SSA. Second, this study utilized both the ENCI and Theil indices in examining inequalities. This comprehensive approach offers multidimensional inequality insights. When combined, ENCI and the Theil index allow researchers to simultaneously assess inequalities in health outcomes (via the ENCI) and wealth distribution inequalities (via the Theil index), providing insights into whether health inequalities are driven primarily by economic factors or other social determinants [33,34,55].This allows for a more nuanced understanding of inequalities which is critical in policy decisions.
5. Conclusions
This study has provided valuable insights into the temporal inequalities in the uptake of malaria prevention strategies among pregnant women and children under five across 10 Sub-Saharan African countries. The findings highlight that while some progress has been made in expanding access to malaria prevention strategies, the benefits are still not equitably distributed across different SES and residence status groups. Generally, pregnant women and children in the poor households and those in rural areas continue to face barriers in accessing and utilizing preventive interventions. Temporal analysis reveals that although inequality may have reduced in some areas, in other contexts like Kenya and Rwanda, inequalities are widening which demands urgent targeted and sustained policy efforts if these countries are looking to make progress towards the Sustainable Development Goals.
Addressing these disparities is crucial for achieving universal health coverage and reducing malaria-related morbidity and mortality in the region. Policymakers must prioritize interventions that not only increase the overall coverage of malaria prevention strategies but also ensure that they identify and reach the most vulnerable populations living in both rural and urban areas and across the various SES groups. Lastly, continuous monitoring and evaluation of inequality trends over time, coupled with inclusive health policies, will be essential to ensure that no woman or child is left behind in the fight against malaria in Sub-Saharan Africa.
Author Contributions
D.O. conceptualized the study and was also responsible for assembly of data, data analysis, drafting methods/results/conclusion sections and overall editing. A.T.L contributed to data analysis and drafted the discussion section. R.O. reviewed methods/results section and drafted the introduction section. P.B supported data analysis/results section write up and led overall editing of the manuscript. P.C. and O.A. provided technical oversight during the conceptualization of the study and offered strategic guidance throughout the research process. All authors reviewed and approved the various drafts of the manuscript and contributed to the final version.
Funding
This study did not receive any external funding. The authors contributed their own time and resources to conduct the research. The article processing charge (APC) was covered by the International Journal of Environmental Research and Public Health.
Institutional Review Board Statement
This study used secondary analysis based on publicly available Violence Against Children (VACS) datasets. Even so, ethics approval was obtained from the Human Research Ethics Committee (HREC) at the University of Cape Town (HREC REF: 282/2022).
Data Availability Statement
Datasets are available at http://www.dhsprogram.com .
Acknowledgments
We extend our sincere gratitude to the University of Cape Town's Health Economics Unit for their invaluable support and contributions to this research. A special thanks goes to A/Prof. Olufunke Alaba for securing an opportunity for us to publish this work free-of-cost. The authors would also like to express their appreciation to the Demographic and Health Survey (DHS) for providing access to the data.
Conflicts of Interest
No competing interests.
References
- World Health Organisation. World malaria report 2023; eneva: World Health Organization; 2023. Licence: CC BY-NC-SA 3.0 IGO, 2023. [Google Scholar]
- Berchie, G.O.; Doe, P.F.; Azu, T.D.; Agyeiwaa, J.; Owusu, G.; Boso, C.M.; Yeboa, N.K.; Agyare, D.F.; Aboh, I.K.; Nabe, B. Uptake and Effectiveness of Intermittent Preventive Treatment with Sulfadoxine-Pyrimethamine during Pregnancy in Africa: A Scoping Review. Diseases 2024, 12, 203. [Google Scholar] [CrossRef] [PubMed]
- Galactionova, K.; Smith, T.A.; de Savigny, D.; Penny, M.A. State of inequality in malaria intervention coverage in sub-Saharan African countries. BMC medicine 2017, 15, 1–11. [Google Scholar] [CrossRef] [PubMed]
- GBD 2021 Causes of Death Collaborators. Global burden of 288 causes of death and life expectancy decomposition in 204 countries and territories and 811 subnational locations, 1990-2021: a systematic analysis for the Global Burden of Disease Study 2021. 2021.
- Willey, B.A.; Paintain, L.S.; Mangham, L.; Car, J.; Schellenberg, J.A. Strategies for delivering insecticide-treated nets at scale for malaria control: a systematic review. Bulletin of the World Health Organization 2012, 90, 672–684. [Google Scholar] [CrossRef]
- O'Connell, K.A.; Gatakaa, H.; Poyer, S.; Njogu, J.; Evance, I.; Munroe, E.; Solomon, T.; Goodman, C.; Hanson, K.; Zinsou, C. Got ACTs? Availability, price, market share and provider knowledge of anti-malarial medicines in public and private sector outlets in six malaria-endemic countries. Malaria journal 2011, 10, 1–14. [Google Scholar] [CrossRef]
- Steketee, R.W.; Eisele, T.P. Is the scale up of malaria intervention coverage also achieving equity? PLoS One 2009, 4, e8409. [Google Scholar] [CrossRef]
- Webster, J.; Lines, J.; Bruce, J.; Schellenberg, J.R.A.; Hanson, K. Which delivery systems reach the poor? A review of equity of coverage of ever-treated nets, never-treated nets, and immunisation to reduce child mortality in Africa. The Lancet Infectious Diseases 2005, 5, 709–717. [Google Scholar] [CrossRef]
- United Nations. Secretary-General announces ‘Roll Back Malaria Partnership’ on World Malaria Day. New York: United Nations Secretary-General (SG/SM/11531); 2008. Available online: https://press.un.org/en/2008/sgsm11531.doc.htm (accessed on 8 October).
- World Health Organization. Guidelines for the treatment of malaria; World Health Organization: 2006.
- Gelband, H.; Seiter, A. A global subsidy for antimalarial drugs. Defining and Defeating the Intolerable Burden of Malaria III: Progress and Perspectives: Supplement to Volume 77 (6) of American Journal of Tropical Medicine and Hygiene 2007.
- Gwatkin, D.R. Trends in health inequalities in developing countries. The Lancet Global Health 2017, 5, e371–e372. [Google Scholar] [CrossRef]
- World Health Organization. A strategic framework for malaria prevention and control during pregnancy in the African region; World Health Organization. Regional Office for Africa: 2004.
- Challis, K.; Osman, N.; Cotiro, M.; Nordahl, G.; Dgedge, M.; Bergström, S. Impact of a double dose of sulphadoxine–pyrimethamine to reduce prevalence of pregnancy malaria in southern Mozambique. Tropical Medicine & International Health 2004, 9, 1066–1073. [Google Scholar]
- Shulman, C.; Dorman, E.; Cutts, F.; Kawuondo, K.; Bulmer, J.; Peshu, N.; Marsh, K. Intermittent sulphadoxine-pyrimethamine to prevent severe anaemia secondary to malaria in pregnancy: a randomised placebo-controlled trial. The Lancet 1999, 353, 632–636. [Google Scholar] [CrossRef]
- Anchang-Kimbi, J.K.; Achidi, E.A.; Apinjoh, T.O.; Mugri, R.N.; Chi, H.F.; Tata, R.B.; Nkegoum, B.; Mendimi, J.-M.N.; Sverremark-Ekström, E.; Troye-Blomberg, M. Antenatal care visit attendance, intermittent preventive treatment during pregnancy (IPTp) and malaria parasitaemia at delivery. Malaria Journal 2014, 13, 1–9. [Google Scholar] [CrossRef]
- World Health Organization. World malaria report 2010; World Health Organization: 2010.
- Holtz, T.H.; Patrick Kachur, S.; Roberts, J.M.; Marum, L.H.; Mkandala, C.; Chizani, N.; Macheso, A.; Parise, M.E. Use of antenatal care services and intermittent preventive treatment for malaria among pregnant women in Blantyre District, Malawi. Tropical Medicine & International Health 2004, 9, 77–82. [Google Scholar]
- Kiwuwa, M.S.; Mufubenga, P. Use of antenatal care, maternity services, intermittent presumptive treatment and insecticide treated bed nets by pregnant women in Luwero district, Uganda. Malaria Journal 2008, 7, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Bouyou-Akotet, M.K.; Mawili-Mboumba, D.P.; Kombila, M. Antenatal care visit attendance, intermittent preventive treatment and bed net use during pregnancy in Gabon. BMC Pregnancy and Childbirth 2013, 13, 1–6. [Google Scholar] [CrossRef]
- Mubyazi, G.; Bloch, P.; Kamugisha, M.; Kitua, A.; Ijumba, J. Intermittent preventive treatment of malaria during pregnancy: a qualitative study of knowledge, attitudes and practices of district health managers, antenatal care staff and pregnant women in Korogwe District, North-Eastern Tanzania. Malaria journal 2005, 4, 1–10. [Google Scholar] [CrossRef]
- Ndyomugyenyi, R.; Neema, S.; Magnussen, P. The use of formal and informal services for antenatal care and malaria treatment in rural Uganda. Health policy and planning 1998, 13, 94–102. [Google Scholar] [CrossRef]
- Carrasco-Escobar, G.; Fornace, K.; Benmarhnia, T. Mapping socioeconomic inequalities in malaria in Sub-Sahara African countries. Scientific reports 2021, 11, 15121. [Google Scholar] [CrossRef]
- Apeagyei, A.E.; Patel, N.K.; Cogswell, I.; O’Rourke, K.; Tsakalos, G.; Dieleman, J. Examining geographical inequalities for malaria outcomes and spending on malaria in 40 malaria-endemic countries, 2010–2020. Malaria Journal 2024, 23, 206. [Google Scholar] [CrossRef]
- Taylor, C.; Florey, L.; Ye, Y. Equity trends in ownership of insecticide-treated nets in 19 sub-Saharan African countries. Bulletin of the World Health Organization 2017, 95, 322. [Google Scholar] [CrossRef]
- Njau, J.D.; Stephenson, R.; Menon, M.; Kachur, S.P.; McFarland, D.A. Exploring the impact of targeted distribution of free bed nets on households bed net ownership, socio-economic disparities and childhood malaria infection rates: analysis of national malaria survey data from three sub-Saharan Africa countries. Malaria journal 2013, 12, 1–15. [Google Scholar] [CrossRef]
- World Health Organization. World Malaria Report 2023; 2023; p. 283.
- Croft, T.N.; Marshall, A.M.; Allen, C.K.; Arnold, F.; Assaf, S.; Balian, S. Guide to DHS statistics. Rockville: ICF 2018, 645, 292–303. [Google Scholar]
- van Eijk, A.M.; Hill, J.; Alegana, V.A.; Kirui, V.; Gething, P.W.; ter Kuile, F.O.; Snow, R.W. Coverage of malaria protection in pregnant women in sub-Saharan Africa: a synthesis and analysis of national survey data. Lancet Infect. Dis. 2011, 11, 190–207. [Google Scholar] [CrossRef] [PubMed]
- Kebede, W.; Tolcha, A.; Soboksa, N.E.; Negassa, B.; Kanno, G.G.; Aregu, M.B. Utilization of insecticide-treated nets in households for Under-5 children and associated factors in east Mesekan District, Gurage zone, Southern Ethiopia. Environmental Health Insights 2023, 17, 11786302231164287. [Google Scholar] [CrossRef] [PubMed]
- Florey, L. Preventing malaria during pregnancy in sub-Saharan Africa: determinants of effective IPTp delivery. 2013.
- Martin, M.K.; Venantius, K.B.; Patricia, N.; Bernard, K.; Keith, B.; Allen, K.; Godfrey, A.; Rogers, T.; Damazo, K.T.; Dathan, B.M. Correlates of uptake of optimal doses of sulfadoxine-pyrimethamine for prevention of malaria during pregnancy in East-Central Uganda. Malaria Journal 2020, 19, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Erreygers, G. Correcting the concentration index. J. Health Econ. 2009, 28, 504–515. [Google Scholar] [CrossRef]
- Conceição, P.; Ferreira, P. The young person's guide to the Theil index: Suggesting intuitive interpretations and exploring analytical applications. 2000.
- Maghendji-Nzondo, S.; Nzoughe, H.; Lemamy, G.J.; Kouna, L.C.; Pegha-Moukandja, I.; Lekoulou, F.; Mbatchi, B.; Toure-Ndouo, F.; Lekana-Douki, J.B. Prevalence of malaria, prevention measures, and main clinical features in febrile children admitted to the Franceville Regional Hospital, Gabon. Parasite 2016, 23. [Google Scholar] [CrossRef]
- Bhatt, S.; Weiss, D.; Cameron, E.; Bisanzio, D.; Mappin, B.; Dalrymple, U.; Battle, K.; Moyes, C.; Henry, A.; Eckhoff, P. The effect of malaria control on Plasmodium falciparum in Africa between 2000 and 2015. Nature 2015, 526, 207–211. [Google Scholar] [CrossRef]
- Degarege, A.; Fennie, K.; Degarege, D.; Chennupati, S.; Madhivanan, P. Improving socioeconomic status may reduce the burden of malaria in sub Saharan Africa: A systematic review and meta-analysis. PloS one 2019, 14, e0211205. [Google Scholar] [CrossRef]
- Talipouo, A.; Ngadjeu, C.S.; Doumbe-Belisse, P.; Djamouko-Djonkam, L.; Sonhafouo-Chiana, N.; Kopya, E.; Bamou, R.; Awono-Ambene, P.; Woromogo, S.; Kekeunou, S. Malaria prevention in the city of Yaoundé: knowledge and practices of urban dwellers. Malaria Journal 2019, 18, 1–13. [Google Scholar]
- Sumari, D.; Dillip, A.; Ndume, V.; Mugasa, J.P.; Gwakisa, P.S. Knowledge, attitudes and practices on malaria in relation to its transmission among primary school children in Bagamoyo district, Tanzania. MalariaWorld Journal 2016, 7. [Google Scholar]
- Kalu, G.O.; Francis, J.M.; Ibisomi, L.; Chirwa, T.; Kagura, J. Factors associated with the uptake of Intermittent Preventive Treatment (IPTp-SP) for malaria in pregnancy: Further analysis of the 2018 Nigeria Demographic and Health Survey. PLOS Global Public Health 2023, 3, e0000771. [Google Scholar] [CrossRef]
- Ochieng, W.; Munsey, A.; Kinyina, A.; Assenga, M.; Onikpo, F.; Binazon, A.; Adeyemi, M.; Alao, M.; Aron, S.; Nhiga, S. Antenatal care services in Benin and Tanzania 2021/2022: an equity analysis study. BMJ public health 2024, 2. [Google Scholar] [CrossRef] [PubMed]
- Gizaw, Z.; Astale, T.; Kassie, G.M. What improves access to primary healthcare services in rural communities? A systematic review. BMC Primary Care 2022, 23, 313. [Google Scholar] [CrossRef] [PubMed]
- Chen, I.; Clarke, S.E.; Gosling, R.; Hamainza, B.; Killeen, G.; Magill, A.; O’Meara, W.; Price, R.N.; Riley, E.M. “Asymptomatic” malaria: a chronic and debilitating infection that should be treated. PLoS medicine 2016, 13, e1001942. [Google Scholar] [CrossRef] [PubMed]
- Baciu, A.; Negussie, Y.; Geller, A.; Weinstein, J.N.; National Academies of Sciences, E.; Medicine. The root causes of health inequity. In Communities in action: Pathways to health equity; National Academies Press (US): 2017.
- Assele, V.; Ndoh, G.E.; Nkoghe, D.; Fandeur, T. No evidence of decline in malaria burden from 2006 to 2013 in a rural Province of Gabon: implications for public health policy. BMC public health 2015, 15, 1–8. [Google Scholar] [CrossRef]
- Imboumy-Limoukou, R.K.; Maghendji-Nzondo, S.; Sir-Ondo-Enguier, P.N.; Niemczura De Carvalho, J.; Tsafack-Tegomo, N.P.; Buekens, J.; Okouga, A.P.; Mouinga-Ondeme, A.; Kwedy Nolna, S.; Lekana-Douki, J.-B. Malaria in children and women of childbearing age: infection prevalence, knowledge and use of malaria prevention tools in the province of Nyanga, Gabon. Malaria journal 2020, 19, 1–8. [Google Scholar] [CrossRef]
- Dahab, R.; Sakellariou, D. Barriers to accessing maternal care in low income countries in Africa: a systematic review. Int. J. Environ. Res. Public Health 2020, 17, 4292. [Google Scholar] [CrossRef]
- Kabudula, C.W.; Houle, B.; Collinson, M.A.; Kahn, K.; Tollman, S.; Clark, S. Assessing changes in household socioeconomic status in rural South Africa, 2001–2013: a distributional analysis using household asset indicators. Social indicators research 2017, 133, 1047–1073. [Google Scholar] [CrossRef]
- Ataguba, J.E.-O.; McIntyre, D. Who benefits from health services in South Africa? Health Economics, Policy and Law 2013, 8, 21–46. [Google Scholar] [CrossRef]
- Alaba, O.; Chola, L. Socioeconomic inequalities in adult obesity prevalence in South Africa: a decomposition analysis. Int. J. Environ. Res. Public Health 2014, 11, 3387–3406. [Google Scholar] [CrossRef]
- Saddiq, A.; Saleh, J.-E.A.; Wondimagegnehu, A.; Mpazanje, R.; Audu, B.M. Universal Access to Malaria Prevention, Diagnosis and Treatment as a Strategy toward Disease Control and Elimination: A Critical Look at Northeastern Nigeria. Open Access Library Journal 2019, 6, 1–12. [Google Scholar] [CrossRef]
- Naserrudin, N.A.; Lin, P.Y.P.; Monroe, A.; Baumann, S.E.; Adhikari, B.; Miller, A.C.; Sato, S.; Fornace, K.M.; Culleton, R.; Cheah, P.Y. Disentangling the intersection of inequities with health and malaria exposure: key lessons from rural communities in Northern Borneo. Malaria Journal 2023, 22, 343. [Google Scholar] [CrossRef]
- Ahorlu, C.S.; Adongo, P.; Koenker, H.; Zigirumugabe, S.; Sika-Bright, S.; Koka, E.; Tabong, P.T.-N.; Piccinini, D.; Segbaya, S.; Olapeju, B. Understanding the gap between access and use: a qualitative study on barriers and facilitators to insecticide-treated net use in Ghana. Malaria journal 2019, 18, 1–13. [Google Scholar] [CrossRef]
- Jenkins, S.P.; Van Kerm, P. The measurement of economic inequality. 2011.
- Wagstaff, A.; O'Donnell, O.; Van Doorslaer, E.; Lindelow, M. Analyzing health equity using household survey data: a guide to techniques and their implementation; World Bank Publications: 2007.
Figure 1.
Erregyers Normalised Concentration Curves for ITN use and IPTp coverage in 10 countries in SSA, various years.
Figure 1.
Erregyers Normalised Concentration Curves for ITN use and IPTp coverage in 10 countries in SSA, various years.
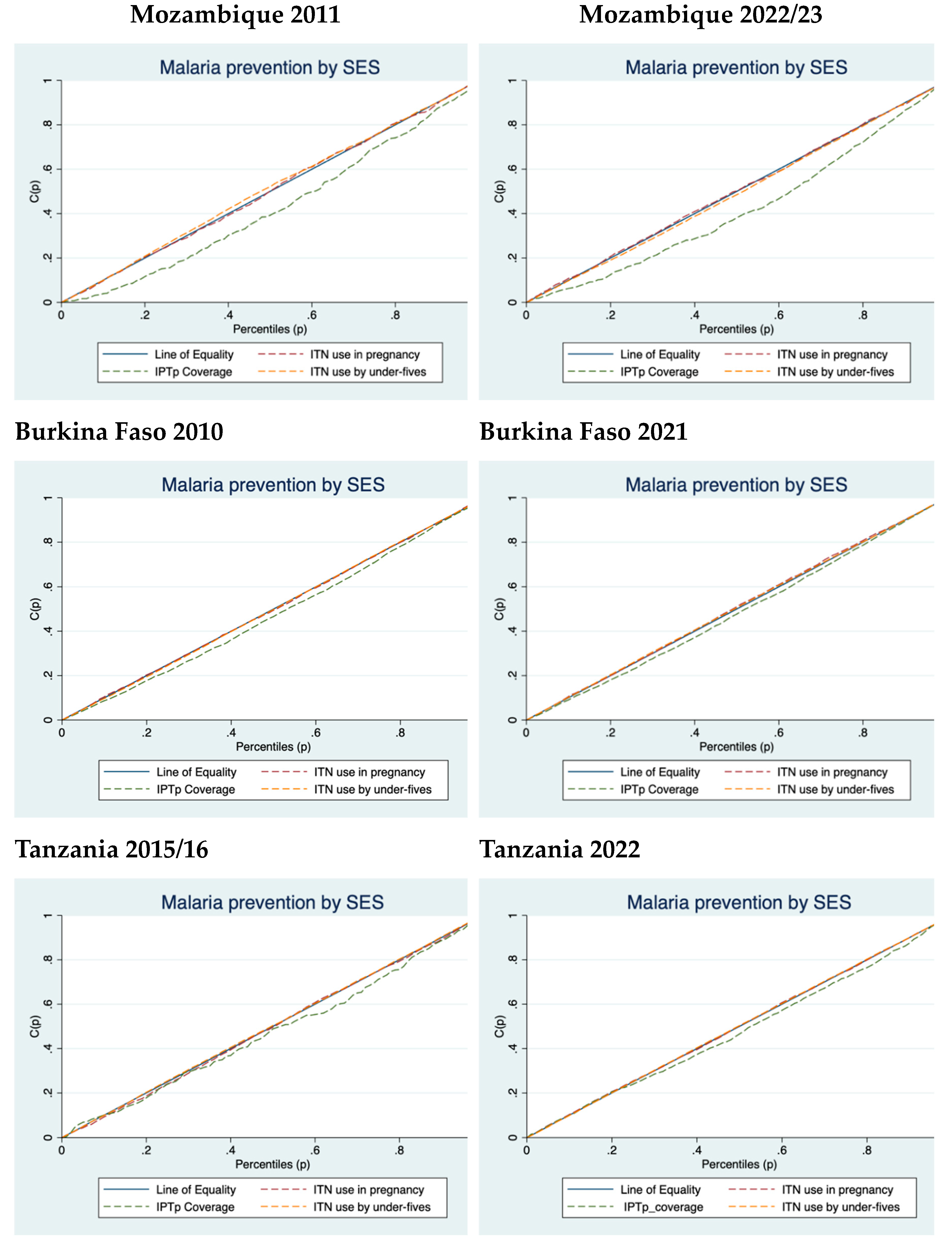
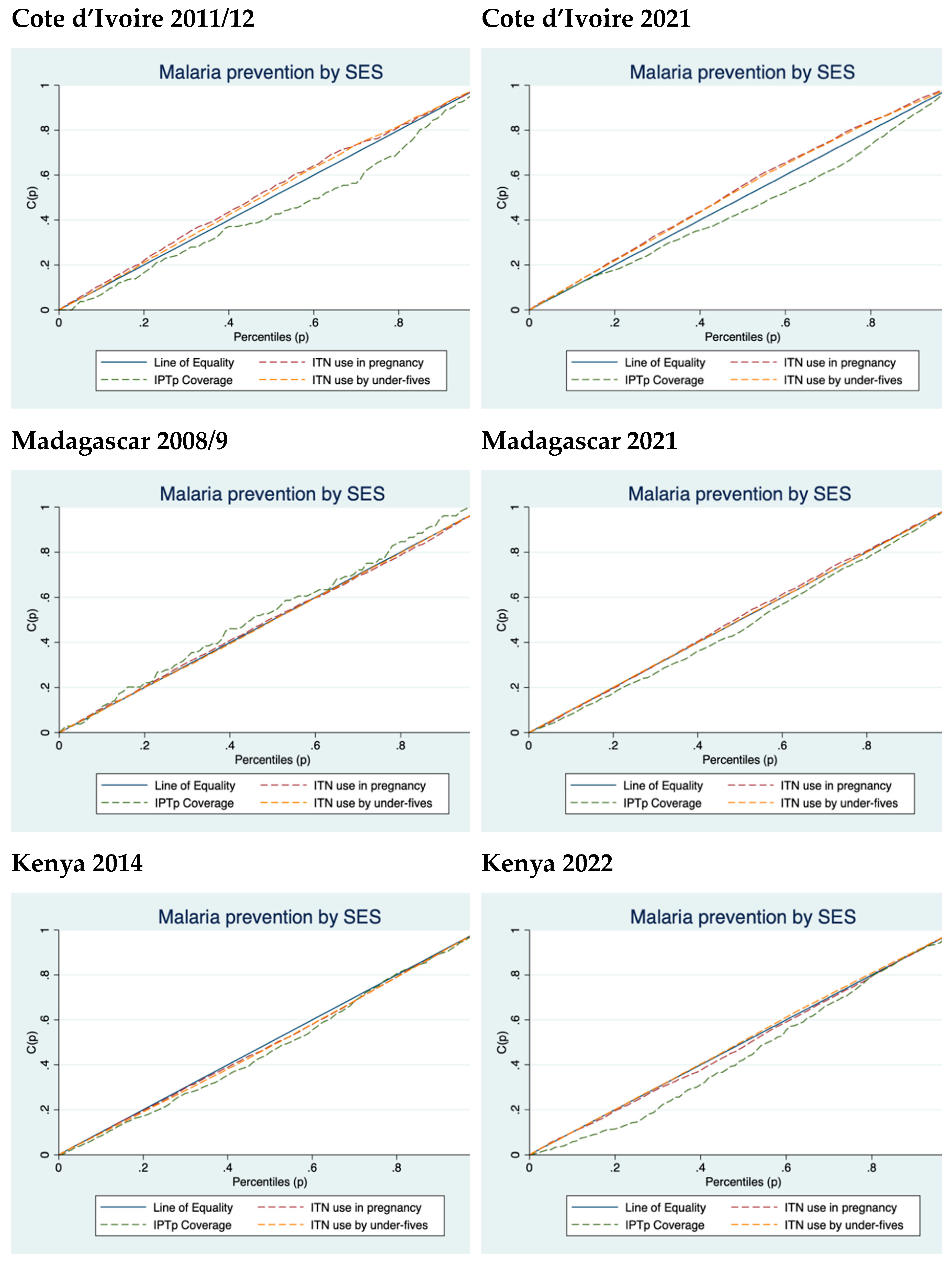
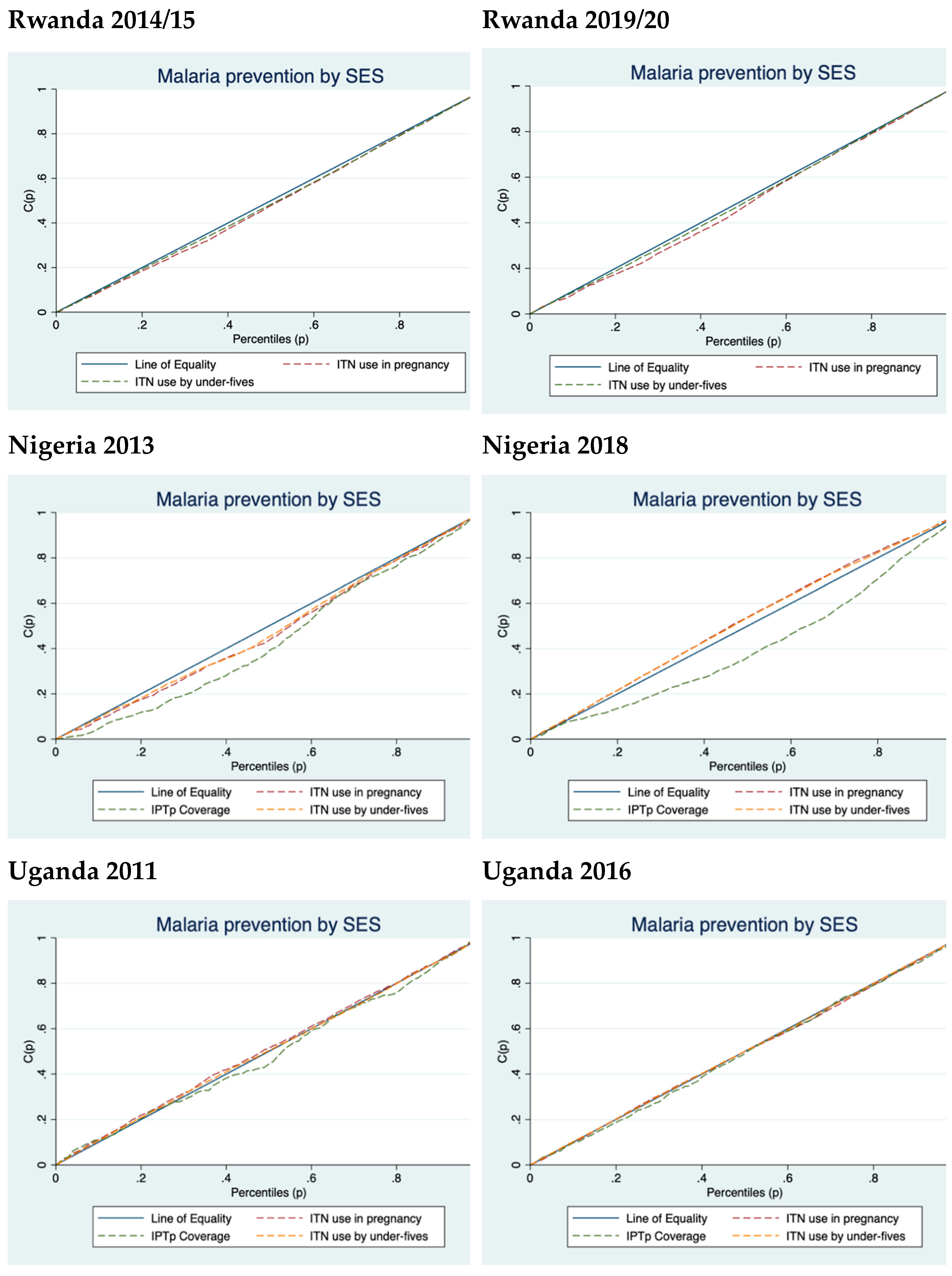
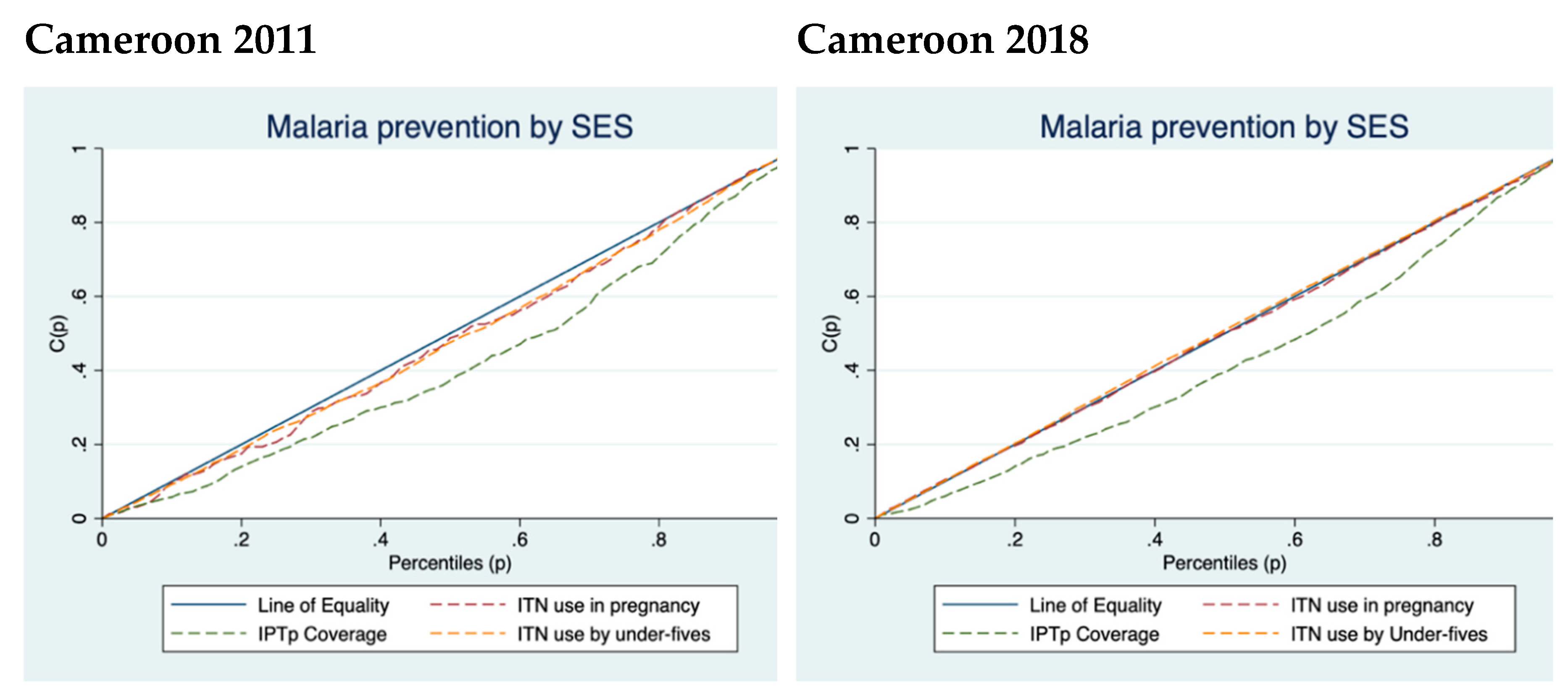

Table 1.
The proportions ITN use in pregnancy, ITN use by children under-5 and IPTp coverage for 10 countries in SSA, various years.
Table 1.
The proportions ITN use in pregnancy, ITN use by children under-5 and IPTp coverage for 10 countries in SSA, various years.
| Country | Year | ITN use in pregnancy % [95% CI] |
% change in ITN use in pregnancy | ITN use by under-fives % [95% CI] |
% change in ITN use in under-fives | IPTp coverage % [95% CI] |
% change in IPTp coverage |
|---|---|---|---|---|---|---|---|
| Mozambique | 2011 | 61.07 [56.60;65.53] | +18.80 | 65.15 [62.77;67.53] | +19.63 | 9.63 [8.16;11.11] | +159.40 |
| 2022/3 | 72.55 [67.70;77.39] | 77.94 [75.42;80.45] | 24.98 [22.75;27.21] | ||||
| Burkina Faso | 2010 | 76.65 [73.40;79.89] | +8.39 | 76.99 [75.20;78.77] | +13.46 | 40.95 [38.79;43.10] | +38.41 |
| 2021 | 83.08 [80.37;85.79] | 87.35 [86.16;88.54] | 56.68 [54.21;59.14] | ||||
| Tanzania | 2015/16 | 74.40 [70.69;78.11] | +13.74 | 76.71 [74.67;78.75] | +13.86 | 7.87 [6.71;9.03] | +299.87 |
| 2022 | 84.62 [81.24;88.00] | 87.34 [86.20;88.49] | 31.47 [29.13;33.81] | ||||
| Côte d'Ivoire | 2011/12 | 57.11 [52.11;62.12] | +36.89 | 59.61 [56.79;62.41] | +29.56 | 8.16 [6.64;9.67] | +322.18 |
| 2021 | 78.18 [74.49;81.88] | 77.23 [74.72;79.73] | 34.45 [31.70;37.20] | ||||
| Madagascar | 2008/09 | 75.86 [71.94;79.78] | +1.78 | 80.38 [78.46;82.31] | +5.54 | 1.93 [1.36;2.49] | +1504.15 |
| 2021 | 77.21 [73.81;80.62] | 84.83 [83.20;86.46] | 30.96 [28.80;33.11] | ||||
| Kenya | 2014 | 76.30 [72.93;79.67] | -1.85 | 80.97 [79.72;82.20] | -1.52 | 10.55 [9.25;11.85] | -38.86 |
| 2022 | 74.89 [71.29;78.49] | 79.74 [78.36;81.12] | 6.45 [5.68;7.22] | ||||
| Nigeria | 2013 | 29.82 [26.82;32.81] | +173.88 |
31.48 [29.16;33.80] | +153.97 | 7.02 [6.17;7.88] | +136.75 |
| 2018 | 81.67 [79.67;83.68] | 79.95 [78.70;81.19] | 16.62 [15.51;17.72] | ||||
| Uganda | 2011 | 71.14 [66.79;75.48] | +11.12 | 71.58 [69.42;73.74] | +14.64 | 10.57 [9.07;12.07] | +57.24 |
| 2016 | 79.05 [76.53;81.57] | 82.06 [80.79;83.32] | 17.40 [16.16;18.63] | ||||
| Cameroon | 2011 | 46.44 [39.86;53.01] | +67.44 | 51.17 [47.80;83.32] | +56.65 | 12.13 [10.90;13.36] | +168.26 |
| 2018 | 77.76 [74.04;81.48] | 80.16 [78.22;82.10] | 32.54 [30.26;34.83] | ||||
| Rwanda | 2014/15 | 87.72 [85.31;90.12] | -6.76 | 86.69 [85.48;87.90] | -3.20 | - | - |
| 2019/20 | 81.79 [78.13;85.46] | 83.92 [82.42;85.43] | - |
Table 2.
Erreygers Normalized Concentration indices (ENCI) for ITN use in pregnancy for 10 countries in SSA, various years.
Table 2.
Erreygers Normalized Concentration indices (ENCI) for ITN use in pregnancy for 10 countries in SSA, various years.
| Country | Year | ENCI | p-values | Robust standard errors |
|---|---|---|---|---|
| Mozambique | 2011 | -0.003 | 0.934 | 0.040 |
| 2022/3 | 0.000 | 0.995 | 0.040 | |
| Burkina Faso | 2010 | -0.003 | 0.914 | 0.029 |
| 2021 | -0.023 | 0.334 | 0.024 | |
| Tanzania | 2015/16 | -0.006 | 0.862 | 0.035 |
| 2022 | -0.008 | 0.761 | 0.027 | |
| Côte d'Ivoire | 2011/12 | -0.117 | 0.003 | 0.040 |
| 2021 | -0.216 | 0.000 | 0.028 | |
| Madagascar | 2008/09 | -0.002 | 0.950 | 0.031 |
| 2021 | -0.049 | 0.108 | 0.030 | |
| Kenya | 2014 | 0.069 | 0.009 | 0.026 |
| 2022 | 0.052 | 0.063 | 0.028 | |
| Rwanda | 2014/15 | 0.109 | 0.000 | 0.026 |
| 2019/20 | 0.122 | 0.001 | 0.036 | |
| Nigeria | 2013 | 0.067 | 0.010 | 0.026 |
| 2018 | -0.156 | 0.000 | 0.018 | |
| Uganda | 2011 | -0.037 | 0.330 | 0.038 |
| 2016 | 0.025 | 0.248 | 0.022 | |
| Cameroon | 2011 | 0.090 | 0.148 | 0.061 |
| 2018 | 0.020 | 0.543 | 0.034 |
Table 3.
Erreygers Normalized Concentration indices (ENCI) for IPTp coverage for 10 countries in SSA, various years.
Table 3.
Erreygers Normalized Concentration indices (ENCI) for IPTp coverage for 10 countries in SSA, various years.
| Country | Year | ENCI | p-values | Robust standard errors |
|---|---|---|---|---|
| Mozambique | 2011 | 0.043 | 0.001 | 0.011 |
| 2022/3 | 0.149 | 0.000 | 0.018 | |
| Burkina Faso | 2010 | 0.084 | 0.000 | 0.017 |
| 2021 | 0.082 | 0.000 | 0.021 | |
| Tanzania | 2015/16 | 0.016 | 0.113 | 0.010 |
| 2022 | 0.033 | 0.085 | 0.019 | |
| Côte d'Ivoire | 2011/12 | 0.035 | 0.004 | 0.012 |
| 2021 | 0.117 | 0.000 | 0.019 | |
| Madagascar | 2008/09 | -0.003 | 0.611 | 0.005 |
| 2021 | 0.062 | 0.001 | 0.019 | |
| Kenya | 2014 | 0.016 | 0.080 | 0.009 |
| 2022 | 0.019 | 0.005 | 0.008 | |
| Nigeria | 2013 | 0.026 | 0.000 | 0.006 |
| 2018 | 0.115 | 0.000 | 0.010 | |
| Uganda | 2011 | 0.012 | 0.329 | 0.012 |
| 2016 | 0.008 | 0.454 | 0.011 | |
| Cameroon | 2011 | 0.080 | 0.000 | 0.012 |
| 2018 | 0.178 | 0.000 | 0.019 |
Table 4.
Erreygers Normalized Concentration indices (ENCI) for IPTp coverage for 10 countries in SSA, various years.
Table 4.
Erreygers Normalized Concentration indices (ENCI) for IPTp coverage for 10 countries in SSA, various years.
| Country | Year | ENCI | p-values | Robust standard errors |
|---|---|---|---|---|
| Mozambique | 2011 | -0.059 | 0.006 | 0.022 |
| 2022/3 | 0.054 | 0.006 | 0.020 | |
| Burkina Faso | 2010 | 0.003 | 0.843 | 0.014 |
| 2021 | -0.022 | 0.020 | 0.010 | |
| Tanzania | 2015/16 | 0.052 | 0.003 | 0.018 |
| 2022 | 0.009 | 0.381 | 0.011 | |
| Côte d'Ivoire | 2011/12 | -0.090 | 0.000 | 0.021 |
| 2021 | -0.183 | 0.000 | 0.014 | |
| Madagascar | 2008/09 | 0.020 | 0.148 | 0.014 |
| 2021 | -0.005 | 0.642 | 0.012 | |
| Kenya | 2014 | 0.086 | 0.000 | 0.010 |
| 2022 | 0.027 | 0.006 | 0.010 | |
| Rwanda | 2014/15 | 0.068 | 0.000 | 0.011 |
| 2019/20 | 0.080 | 0.000 | 0.013 | |
| Nigeria | 2013 | 0.060 | 0.002 | 0.019 |
| 2018 | -0.139 | 0.000 | 0.011 | |
| Uganda | 2011 | 0.010 | 0.535 | 0.016 |
| 2016 | 0.010 | 0.300 | 0.010 | |
| Cameroon | 2011 | 0.083 | 0.014 | 0.034 |
| 2018 | -0.044 | 0.009 | 0.017 |
Table 5.
Theil indices for subgroups for ITN use and IPTp coverage distinguished by place of residence for 10 countries in SSA, various years.
Table 5.
Theil indices for subgroups for ITN use and IPTp coverage distinguished by place of residence for 10 countries in SSA, various years.
| Country | Year | ITN use in pregnancy | IPTp coverage | ITN use by under-fives | |||
|---|---|---|---|---|---|---|---|
| Urban GE(2) |
Rural GE(2) |
Urban GE(2) |
Rural GE(2) |
Urban GE(2) |
Rural GE(2) |
||
| Mozambique | 2011 | 0.215 | 0.444 | 0.326 | 0.674 | 0.236 | 0.345 |
| 2022/3 | 0.164 | 0.221 | 1.005 | 1.874 | 0.099 | 0.189 | |
| Burkina Faso | 2010 | 0.171 | 0.138 | 0.552 | 0.694 | 0.159 | 0.134 |
| 2021 | 0.120 | 0.090 | 0.331 | 0.390 | 0.088 | 0.067 | |
| Tanzania | 2015/16 | 0.145 | 0.164 | 4.386 | 7.084 | 0.130 | 0.162 |
| 2022 | 0.094 | 0.103 | 1.077 | 1.639 | 0.077 | 0.080 | |
| Côte d'Ivoire | 2011/12 | 0.429 | 0.295 | 5.161 | 7.592 | 0.407 | 0.285 |
| 2021 | 0.172 | 0.096 | 0.940 | 1.207 | 0.186 | 0.090 | |
| Madagascar | 2008/09 | 0.136 | 0.166 | 22.53 | 22.26 | 0.093 | 0.131 |
| 2021 | 0.187 | 0.127 | 1.083 | 1.008 | 0.086 | 0.086 | |
| Kenya | 2014 | 0.113 | 0.186 | 4.080 | 4.300 | 0.095 | 0.141 |
| 2022 | 0.151 | 0.159 | 6.467 | 7.657 | 0.139 | 0.118 | |
| Nigeria | 2013 | 0.891 | 1.273 | 6.905 | 7.281 | 0.834 | 1.145 |
| 2018 | 0.179 | 0.093 | 1.880 | 2.848 | 0.179 | 0.106 | |
| Uganda | 2011 | 0.097 | 0.209 | 5.272 | 4.777 | 0.148 | 0.205 |
| 2016 | 0.109 | 0.137 | 2.689 | 2.363 | 0.089 | 0.113 | |
| Cameroon | 2011 | 0.426 | 0.645 | 2.579 | 4.279 | 0.383 | 0.488 |
| 2018 | 0.159 | 0.178 | 0.733 | 1.443 | 0.138 | 0.126 | |
| Rwanda | 2014/15 | 0.046 | 0.079 | - | - | 0.045 | 0.086 |
| 2019/20 | 0.058 | 1.275 | - | - | 0.066 | 0.107 | |
Note: Data for IPTp coverage was not available for Rwanda.
Table 6.
Theil indices for subgroups for ITN use and IPTp coverage distinguished by SES for 10 countries in SSA, various years.
Table 6.
Theil indices for subgroups for ITN use and IPTp coverage distinguished by SES for 10 countries in SSA, various years.
| Country | Year | ITN use in pregnancy | IPTp coverage | ITN use by under-fives | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Poor GE(2) | Middle GE(2) | Rich GE(2) | Poor GE(2) | Middle GE(2) | Rich GE(2) | Poor GE(2) | Middle GE(2) | Rich GE(2) | ||
| Mozambique | 2011 | 0.374 | 0.277 | 0.374 | 6.964 | 5.116 | 3.970 | 0.269 | 0.257 | 0.345 |
| 2022/3 | 0.190 | 0.226 | 0.194 | 2.315 | 1.714 | 0.994 | 0.179 | 0.162 | 0.130 | |
| Burkina Faso | 2010 | 0.141 | 0.153 | 0.145 | 0.791 | 0.654 | 0.551 | 0.146 | 0.132 | 0.140 |
| 2021 | 0.094 | 0.086 | 0.110 | 0.445 | 0.365 | 0.313 | 0.065 | 0.068 | 0.083 | |
| Tanzania | 2015/16 | 0.167 | 0.120 | 0.173 | 6.688 | 7.531 | 5.287 | 0.142 | 0.162 | 0.158 |
| 2022 | 0.104 | 0.078 | 0.109 | 1.584 | 1.458 | 1.320 | 0.074 | 0.080 | 0.083 | |
| Côte d'Ivoire | 2011/12 | 0.268 | 0.369 | 0.450 | 7.923 | 9.047 | 4.405 | 0.280 | 0.283 | 0.432 |
| 2021 | 0.063 | 0.153 | 0.285 | 1.335 | 1.187 | 0.684 | 0.071 | 0.147 | 0.258 | |
| Madagascar | 2008/09 | 0.155 | 0.203 | 0.149 | 20.80 | 24.32 | 23.30 | 0.127 | 0.120 | 0.117 |
| 2021 | 0.119 | 0.137 | 0.161 | 1.201 | 0.815 | 0.922 | 0.084 | 0.089 | 0.087 | |
| Kenya | 2014 | 0.184 | 0.164 | 0.120 | 4.664 | 3.289 | 4.114 | 0.153 | 0.112 | 0.095 |
| 2022 | 0.186 | 0.106 | 0.146 | 8.606 | 5.975 | 6.331 | 0.120 | 0.094 | 0.150 | |
| Nigeria | 2013 | 1.403 | 0.852 | 1.047 | 10.06 | 4.841 | 6.422 | 1.244 | 0.800 | 0.961 |
| 2018 | 0.072 | 0.121 | 0.226 | 3.649 | 2.465 | 1.541 | 0.085 | 0.125 | 0.215 | |
| Uganda | 2011 | 0.163 | 0.204 | 0.197 | 5.365 | 4.259 | 4.671 | 0.173 | 0.245 | 0.186 |
| 2016 | 0.130 | 0.185 | 0.104 | 2.482 | 2.394 | 2.338 | 0.104 | 0.126 | 0.103 | |
| Cameroon | 2011 | 0.650 | 0.542 | 0.445 | 4.851 | 3.796 | 2.281 | 0.527 | 0.426 | 0.375 |
| 2018 | 0.171 | 0.199 | 0.150 | 1.566 | 1.120 | 0.649 | 0.113 | 0.146 | 0.143 | |
| Rwanda | 2014/15 | 0.127 | 0.044 | 0.045 | - | - | - | 0.100 | 0.081 | 0.052 |
| 2019/20 | 0.184 | 0.094 | 0.076 | - | - | - | 0.128 | 0.087 | 0.078 | |
Table 7.
Decomposition of Theil indices by place of residence.
| Country | Year | ITN use in pregnancy | IPTp coverage | ITN use by under-fives | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Overall inequality GE(2) |
(%Contr) | (%Contr) | Overall inequality GE(2) |
(%Contr) | (%Contr) | Overall inequality GE(2) |
(%Contr) | (%Contr) | ||
| Mozambique | 2011 | 0.353 | 0.009 (2.55%) | 0.344 (97.45%) | 5.01 | 0.021 (0.42%) | 4.989 (99.58%) | 0.301 | 0.002 (0.33%) | 0.300 (99.67%) |
| 2022/3 | 0.199 | 0.000 (0%) | 0.199 (100%) | 1.517 | 0.026 (1.71%) | 1.491 (98.29) | 0.151 | 0.002 (1.32%) | 0.149 (98.68%) | |
| Burkina Faso | 2010 | 0.145 | 0.000 (0%) | 0.145 (100%) | 0.659 | 0.001 (0.15%) | 0.658 (99.85) | 0.140 | 0.000 (0%) | 0.140 (100%) |
| 2021 | 0.099 | 0.000 (0%) | 0.099 (100%) | 0.372 | 0.001 (0%) | 0.372 (100%) | 0.073 | 0.000 (0%) | 0.073 (100%) | |
| Tanzania | 2015/16 | 0.159 | 0.000 (0%) | 0.159 (100%) | 6.202 | 0.021 (0.34%) | 6.181 (99.66%) | 0.153 | 0.000 (0%) | 0.153 (100%) |
| 2022 | 0.101 | 0.000 (0%) | 0.101 (100%) | 1.449 | 0.010 (0.69%) | 1.439 (99.31%) | 0.080 | 0.000 (0%) | 0.080 (100%) | |
| Côte d'Ivoire | 2011/12 | 0.334 | 0.003 (0.60%) | 0.332 (99.40%) | 6.555 | 0.016 (0.24%) | 6.539 (99.76%) | 0.321 | 0.002 (0.62%) | 0.319 (99.38%) |
| 2021 | 0.126 | 0.002 (1.59%) | 0.124 (98.41%) | 1.088 | 0.004 (0.37%) | 1.084 (99.63%) | 0.123 | 0.003 (1.63%) | 0.121 (98.37%) | |
| Madagascar | 2008/09 | 0.160 | 0.000 (0%) | 0.160 (100%) | 22.12 | 0.000 (0%) | 22.12 (100%) | 0.122 | 0.000 (0%) | 0.122 (100%) |
| 2021 | 0.136 | 0.001 (0%) | 0.136 (100%) | 1.021 | 0.000 (0%) | 1.021 (100%) | 0.086 | 0.000 (0%) | 0.086 (100%) | |
| Kenya | 2014 | 0.158 | 0.002 (0.67%) | 0.157 (99.37%) | 4.227 | 0.000 (0%) | 4.227 (100%) | 0.124 | 0.001 (0.81%) | 0.123 (99.19%) |
| 2022 | 0.156 | 0.000 (0%) | 0.156 (100%) | 7.214 | 0.003 (0%) | 7.212 (100%) | 0.125 | 0.000 (0%) | 0.125 (100%) | |
| Nigeria | 2013 | 0.148 | 0.007 (4.73%) | 1.141 (95.27%) | 7.152 | 0.000 (0%) | 7.152 (100%) | 1.036 | 0.005 (0.48%) | 1.031 (99.52%) |
| 2018 | 0.116 | 0.002 (1.72%) | 0.114 (98.28%) | 2.412 | 0.016 (0.66%) | 2.396 (99.34%) | 0.128 | 0.001 (0.78%) | 0.127 (99.22%) | |
| Uganda | 2011 | 0.182 | 0.003 (1.65%) | 0.179 (98.35%) | 4.879 | 0.001 (0.02%) | 4.878 (99.98) | 0.189 | 0.000 (0%) | 0.189 (100%) |
| 2016 | 0.131 | 0.000 (0%) | 0.131 (100%) | 2.417 | 0.000 (0%) | 2.417 (100%) | 0.108 | 0.000 (0%) | 0.108 (100%) | |
| Cameroon | 2011 | 0.544 | 0.006 (1.10%) | 0.538 (98.90%) | 3.411 | 0.025 (0.73%) | 3.386 (99.27%) | 0.440 | 0.002 (0.45%) | 0.438(99.55%) |
| 2018 | 0.169 | 0.000 (0%) | 0.169 (100%) | 1.051 | 0.026 (2.47%) | 1.025 (97.53%) | 0.132 | 0.000 (0%) | 0.132 (100%) | |
| Rwanda | 2014/15 | 0.071 | 0.000 (0%) | 0.071 (100%) | - | - | - | 0.075 | 0.000 (0%) | 0.075 (100%) |
| 2019/20 | 0.109 | 0.001 (0.92%) | 0.108 (99.08%) | - | - | - | 0.096 | 0.000 (0%) | 0.096 (100%) | |
Note: Data for IPTp coverage was not available for Rwanda.
Table 8.
Decomposition of Theil indices by SES.
| Country | Year | ITN use in pregnancy | IPTp coverage | ITN use by under-fives | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Overall inequality GE(2) |
(%Contr) | (%Contr) | Overall inequality GE(2) |
(%Contr) | (%Contr) | Overall inequality GE(2) |
(%Contr) | |||
| Mozambique | 2011 | 0.353 | 0.001 (0.28%) | 0.352 (99.72%) | 5.010 | 0.024 (0.48%) | 4.986 (99.52%) | 0.300 | 0.001 (0%) | 0.300 (100%) |
| 2022/3 | 0.200 | 0.000 (0%) | 0.200 (100%) | 1.517 | 0.041 (2.70%) | 1.476 (97.30%) | 0.151 | 0.000 (0%) | 0.151 (100%) | |
| Burkina Faso | 2010 | 0.145 | 0.000 (0%) | 0.145 (100%) | 0.659 | 0.004 (0.61%) | 0.655 (99.39%) | 0.140 | 0.000 (0%) | 0.140 (100%) |
| 2021 | 0.099 | 0.000 (0%) | 0.099 (100%) | 0.372 | 0.002 (0.54%) | 0.370 (99.46%) | 0.073 | 0.000 (0%) | 0.073 (100%) | |
| Tanzania | 2015/16 | 0.159 | 0.001 (0.63%) | 0.158 (99.37%) | 6.202 | 0.008 (0.13%) | 6.194 (99.87%) | 0.152 | 0.000 (0%) | 0.152 (100%) |
| 2022 | 0.100 | 0.000 (0%) | 0.100 (100%) | 1.449 | 0.002 (0.07%) | 1.448 (99.93%) | 0.079 | 0.000 (0%) | 0.079 (100%) | |
| Côte d'Ivoire | 2011/12 | 0.334 | 0.004 (1.20%) | 0.330 (98.80%) | 6.555 | 0.042 (0.64%) | 6.513 (99.36%) | 0.321 | 0.003 (0.93%) | 0.318 (99.07%) |
| 2021 | 0.126 | 0.008 (7.14%) | 0.117 (92.86%) | 1.088 | 0.019 (1.84%) | 1.068 (98.16%) | 0.123 | 0.006 (4.88%) | 0.117 (95.12%) | |
| Madagascar | 2008/09 | 0.160 | 0.000 (0%) | 0.160 (100%) | 22.13 | 0.002 (0.05%) | 22.12 (99.95%) | 0.122 | 0.000 (0%) | 0.122 (100%) |
| 2021 | 0.136 | 0.000 (0%) | 0.136 (100%) | 1.022 | 0.006 (0.59%) | 1.016 (99.41%) | 0.086 | 0.000 (0%) | 0.086 (100%) | |
| Kenya | 2014 | 0.158 | 0.001 (5.07%) | 0.157 (94.93%) | 4.227 | 0.007 (0.17%) | 4.220 (99.83%) | 0.124 | 0.001 (0.81%) | 0.123 (99.19%) |
| 2022 | 0.156 | 0.001 (0%) | 0.156 (100%) | 7.214 | 0.011 (0.17%) | 7.202 (99.83%) | 0.124 | 0.000 (0%) | 0.124 (100%) | |
| Nigeria | 2013 | 1.147 | 0.010 (0.87%) | 1.137 (99.13%) | 7.152 | 0.038 (0.52%) | 7.115 (99.48%) | 1.036 | 0.007 (0.68%) | 1.029 (99.32%) |
| 2018 | 0.116 | 0.004 (4.31%) | 0.111 (95.69%) | 2.412 | 0.050 (2.07%) | 2.362 (97.93%) | 0.128 | 0.004 (2.34%) | 0.125 (97.66%) | |
| Uganda | 2011 | 0.181 | 0.000 (0%) | 0.181 (100%) | 4.879 | 0.003 (0.06%) | 4.876 (99.94%) | 0.190 | 0.001 (0%) | 0.190 (100%) |
| 2016 | 0.130 | 0.000 (0%) | 0.130 (100%) | 2.417 | 0.000 (0%) | 2.417 (100%) | 0.108 | 0.000 (0%) | 0.108 (100%) | |
| Cameroon | 2011 | 0.544 | 0.004 (0.74%) | 0.540 (99.26%) | 3.411 | 0.045 (2.32%) | 3.366 (98.68%) | 0.440 | 0.002 (0.68%) | 0.437 (99.32%) |
| 2018 | 0.169 | 0.000 (0%) | 0.169 (100%) | 1.051 | 0.034 (3.24%) | 1.017 (96.76%) | 0.131 | 0.000 (0%) | 0.131 (100%) | |
| Rwanda | 2014/15 | 0.071 | 0.002 (2.82%) | 0.069 (97.18%) | _ | _ | _ | 0.076 | 0.001 (1.32%) | 0.075 (98.68%) |
| 2019/20 | 0.110 | 0.003 (2.73%) | 0.107 (97.27%) | _ | _ | _ | 0.096 | 0.001 (1.04%) | 0.095 (98.96%) | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



