
Submitted:
22 October 2024
Posted:
24 October 2024
You are already at the latest version
Abstract
A dysregulated immune response is associated with the excessive release of cytokines that can lead to systemic vasoplegia and vasoplegic shock with the development of multiorgan failure that is associated with an increased risk of dying. Under physiological circumstances, the endothelium and the glycocalyx are responsible for maintaining vascular tone, capillary permeability, hemostasis, and controlling inflammation. In hyperinflammation, the endothelium and glycocalyx become damaged due to the excessive production of certain toxic proteins, along with an overwhelming release of cytokines. It has been shown in both in vitro animal experiments and also in humans that extracorporeal hemoadsorption can reduce circulating levels of cytokines and may also remove toxic proteins that directly take part in endothelium and glycocalyx damage. The current review aims to summarize current knowledge and to put recent findings into context, and introduce the hypothesis of “endothelial protection with hemoadsorption” in critically ill patients.
Keywords:
sepsis
; septic shock
; hemoadsorption
; cytokines
; endothelium
; capillary leakage
1. Introduction
A dysregulated host immune response is the primary cause of severe organ dysfunction in hyperinflammatory conditions regardless of the insult, be it of an infectious (i.e.: sepsis) or non-infectious (i.e.: major surgery, trauma, etc.) origin [1]. As the body cannot control the overwhelming inflammatory response during this early course of the disease, extracorporeal blood purification in the form of hemoadsorption (HA) as an adjuvant therapy has been considered for almost two decades [2]. Both experimental animal data [3,4,5], a recent human study in healthy volunteers [6] and clinical studies in critically ill adults [7,8] and children [9,10] have shown that HA can effectively remove circulating cytokines, and hence could attenuate the dysregulated inflammatory response. Several clinical studies have reported rapid hemodynamic stabilization during HA, as indicated by a significant reduction in the need for vasopressor support and improved cardiovascular variables [11,12,13,14,15,16,17,18]. However, the exact pathophysiological link between reduced cytokine levels and hemodynamic improvement remains unclear.
Nevertheless, two of the latest meta-analyses found that cytokine adsorption may not have a significant effect on circulating cytokine levels (including IL-6) and may be associated with increased mortality in a subset of patients [19,20]. However, we should interpret these results with caution because the confidence in the evidence was low or very low in both studies.
The endothelium is a major determinant of circulatory function, platelet aggregation, and vascular tone [21]. Therefore, the current review aims to summarize, put recent findings into context, and introduce the hypothesis of “endothelial protection with HA” in critically ill patients.
2. The Endothelium and the Glycocalyx
The endothelium and its inner layer, the glycocalyx, are responsible for several essential physiological functions in maintaining homeostasis and adequate end-organ function. The glycocalyx is a web of membrane-bound glycoproteins and proteoglycans on the luminal side of the endothelium. These two structures act in concert to determine a number of vital functions for the circulatory system, including vascular permeability [22], coagulation, and inflammation - by preventing leukocytes and platelets from adhering to the vessel walls [23] and vascular tone - alongside with vascular smooth muscle [24].
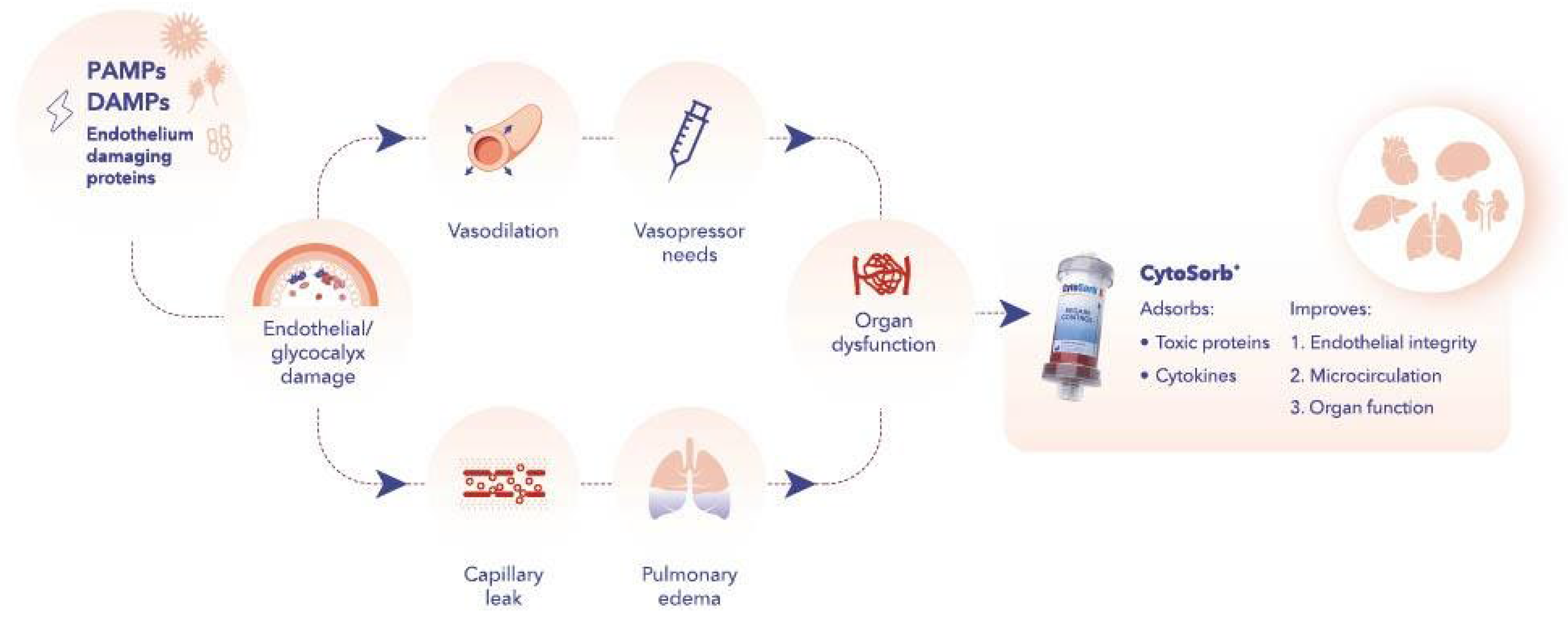
It has been shown that this function can be affected by several inflammatory conditions, including sepsis [25]. During hyperinflammation, the endothelium, its connecting adherents, and the glycocalyx become damaged due to the excessive production of inflammatory mediators, along with the overwhelming release of cytokines leading to increased capillary leakage, interstitial edema, and immuno-thrombosis that further amplifies the underlying hyperinflammation and the associated systemic vasoplegia [21,25]. This combination of increased capillary permeability and vasoplegia can be responsible for an absolute (into the tissues) and relative (into the dilated vessels) loss of circulating blood volume that explains the rationale and vital importance of early, adequate fluid resuscitation and vasopressor support (Figure 1).
On the one hand, resuscitation should begin immediately in septic shock to enhance hemodynamic stabilization, as stated as “Best Practice” by the most recent Surviving Sepsis Campaign Guidelines [26]. Even though fluids and vasopressors are the advised main resuscitation procedures, in themselves they do not reduce the inflammatory process. In fact, fluids can promote further amplification of the inflammatory response [27]. Therefore, attenuating the overwhelming inflammatory response following sepsis by extracorporeal removal of inflammatory mediators that can cause damage to the endothelium may mitigate endothelial dysfunction leading to organ failure.
3. Endothelium Protection with HA
Hemodynamic instability is the most important manifestation of vasoplegic shock, leading to inadequate microcirculatory perfusion, tissue oxygen deficit, and organ dysfunction. Therefore, maintaining an adequate microcirculation should be a primary goal of any therapeutic measure employed to improve the hemodynamic status [28]. Recent studies have shown that there is an array of cellular processes that contribute to endothelial damage during the course of septic shock [25,29].
One of the first animal models on this subject tested the efficacy of cytokine adsorption on coronary endothelial function in the setting of a “donation after cardiac death” scenario [30]. Healthy pig hearts were harvested after circulatory death and randomized into three groups: 1) controls, 2) four-hour hemoperfusion without HA, and 3) four-hour hemoperfusion with HA. Before microvascular assessments were performed, all hearts underwent 1 hour of reperfusion, and then laser-Doppler perfusion (LDP) was performed, and arteriolar perfusates were analyzed. In addition to 13 cytokines, the levels of markers of endothelial oxidative stress (nitrotyrosine and hydroxy-nonenal) as well as endothelial cell injury indicating adhesion molecules (CD54, CD106, CD31) were reduced, and LDP improved in the HA group. The authors concluded that HA prevented oxidative stress and ischemia-reperfusion injury of the endothelium in the coronary arterioles. Unfortunately, data were insufficient to provide a clear explanation of the results.
A very similar approach was applied in two further in vitro experiments. In both studies, the authors retrieved HA cartridges after their use in hyperinflamed patients and washed out the cellular elements of blood components and non-adsorbed plasma proteins. Adsorbed proteins were then detached by rinsing the cartridges with acetonitrile. The proteins were identified with high-performance liquid chromatography and lyophilized, then resuspended to form different elutions. Endothelial cell cultures were then treated with this elution, and measurements were performed. This way, Denzinger et al. [31] were able to identify 39 protein fractions, of which 3 fractions had a detrimental effect on the endothelial cells by inhibiting cell proliferation, increasing cell death, and inducing cell apoptosis. Piskovatska et al. [32] found similar results and also identified a concentration-dependent harm. They showed that the majority (83; 65.4%) of the isolated proteins were in the molecular weight range below 60 kDa and reported that the higher the protein concentration in the elute, the lower the percentage of viable cells in the culture. In fact, at the highest concentration, cell death was similar to treated cells with highly toxic hydrogen peroxide (H2O2). The authors also investigated the effects of these proteins on “wound healing” by scarring the endothelial cell culture and evaluating regeneration (i.e.: healing). In the control cultures, scars disappeared within 24 hours, while the addition of the elute, even at the lowest concentration, prevented endothelial regeneration. The authors concluded that HA allowed for broad-spectrum removal of a wide range of molecules that cause endothelial damage.
David et al. [33] treated human umbilical vein endothelial cells (HUVECs) in vitro with serum obtained from a septic shock patient receiving HA therapy. Serum samples were collected before and after 24 hours of HA, and their effects on the HUVECs were investigated and then compared to treating HUVECs with serum from a healthy control. Morphological changes were measured by immunofluorescent immunochemistry, and functional changes (i.e. capillary permeability) were measured with transendothelial resistance (TER). Treatment with the serum obtained before HA resulted in a substantial disruption of the endothelial cellular junctions and a drop in TER compared to controls. When HUVECs were treated with the serum collected after HA therapy, disruption did not take place, and TER remained significantly higher. The authors suggested that HA might have cleared substances responsible for the loss of endothelial integrity caused by the septic serum. However, one cannot exclude that the results were due to the natural course of the disease, i.e.: the collected blood at time zero behaved differently from the blood collected 24 hours later, and changes were not necessarily the direct effect of HA. Nevertheless, the results are intriguing and render the need for further clinical studies.
4. Other Potential Inflammatory Markers that Could Damage the Glycocalyx
Several inflammatory markers are routinely measured in everyday clinical practice to aid decision making in diagnosis and treatment. Most of these have been shown to be effectively adsorbed by HA.
In a recent clinical-experimental study Drost et al. found that interleukin - IL-6 was strongly associated with glycocalyx damage and correlated both with glycocalyx dimensions and circulating biomarkers [34]. Exposure of endothelial cells to 5% serum from COVID-19 or sepsis patients resulted in a significant decrease in glycocalyx height, which was attenuated by co-incubation with tocilizumab. In 219 COVID-19 patients a previously identified proteomic glycocalyx signature correlated with IL-6 (p<0.0001). These data suggest that IL-6 may significantly drive endothelial damage in COVID-19 and bacterial sepsis. A recent observation in human volunteers found that HA effectively removes IL-6 [6]. Therefore, it is a logical assumption that reducing circulating levels of IL-6 could have some effects on endothelial protection.
One of the most frequently used and investigated inflammatory biomarkers is procalcitonin (PCT). Although PCT has routinely been used as a diagnostic inflammatory marker worldwide for 25 years, it has also been suggested to mediate the underlying disease process [35]. In their study, Nylen et al. used an E. coli peritonitis model in hamsters and administered exogenous PCT to one group of septic animals, which significantly increased mortality compared to non-treated septic animals (93% vs. 43%, p=0.02). On the other hand, pretreating the animals with PCT antiserum almost completely prevented mortality compared to the septic controls (6% vs. 62%, p=<0.003). A recent observational clinical study combined with in vitro and in vivo experiments provides further strong support to the hypothesis that PCT, in fact, has a direct damaging effect on the endothelium [36]. The authors found that, on the one hand, elevated PCT levels were associated with microvascular dysfunction and increased capillary leakage in patients undergoing cardiac surgery, as indicated by a 1.4-fold increase in endothelial and 2.3-fold increase in pulmonary capillary permeability (both p values, 0.001). Furthermore, the authors’ in vitro and in vivo experiments provided evidence that these effects were due to the direct effects of PCT on the endothelium by destabilizing VE-cadherin and also that inhibiting PCT’s action with olcegepant reduced capillary leakage. As available data indicate that HA can rapidly and significantly decrease circulating PCT concentrations [12,13,37,38,39], supports the hypothesis that reducing PCT levels with HA may inhibit the action of PCT on the endothelium, which could help to preserve vascular integrity.
Another potential biomarker of interest is the soluble urokinase-type plasminogen activator receptor (suPAR) [40]. This molecule, expressed in various immune cell membranes, is associated with innate and adaptive immunity: endothelial cells, macrophages, neutrophils, and activated T-cells [41]. It is released into body fluids during inflammatory stimulation and has been associated with endothelial dysfunction, especially in patients with nephrotic syndrome [42,43]. Roca et al., in an observational cross-sectional study in patients with nephrotic syndrome, reported a significant correlation between suPAR and vascular cell adhesion molecule-1 (VCAM-1) and syndecan-1, two established biomarkers of endothelial and glycocalyx injury [42]. The results of a more recent study by Nusshag et al. not only support the relevance of suPAR as a new diagnostic biomarker but, more importantly, strengthen the concept that suPAR is a direct pathophysiological driver involved in sepsis-induced AKI [43]. Furthermore, in this polymicrobial murine sepsis model, they found pronounced ultrastructural kidney damage, impaired kidney function, and poor survival associated with high blood sugar levels. In a case series of COVID-19 patients and in a kidney transplanted patient it was shown that suPAR can be adsorbed by HA [41,44], indicating a potential protective role of HA also in this context.
The third potential biomarker exhibiting mediator properties is high mobility group box-1 (HMGB-1). HMGB-1, circulating histones and glycans such as heparan sulfate, are considered damage-associated molecular patterns (DAMPs) [45]. Among them, HMGB-1 and histones have been extensively studied because they significantly mediate lethal systemic inflammation, complement and coagulation activation, endothelial injury, and organ dysfunction in various critical illnesses, such as sepsis [46], acute liver failure [47], pancreatitis [48], multiple trauma [49] and severe COVID-19 [50]. Effective adsorption of HMGB-1 by HA has recently been shown by Gruda et al. [51]. Subsequently, Weber et al. found that 6-hrs HA significantly decreased circulating histone levels in the blood of 22 humans with multiple injuries [52].
In summary, these early mechanistic data look promising and can help inform the design of future studies investigating the potential of active mediator removal by HA as a novel approach to protect endothelial integrity, and contribute to circulatory recovery in critically ill patients. It is also important to note that although there are several HA devices on the market, all of the preclinical and clinical studies on this topic to date used CytoSorb (CytoSorbents Corporation, Monmouth Junction, NJ, USA), hence it can only be speculated about the potential performance of other devices in this regard, something that should also be considered when future research is planned.
5. Clinical Implications
Endothelial protection by HA in critically ill patients could have important clinical implications. Efficient removal of toxic substances that impair endothelial integrity may help sustain endothelial function in support of organ function. Better microcirculatory flow and perfusion could also lead to faster hemodynamic stabilization and improved tissue oxygen uptake. Improved macro- and microcirculation performance with hemodynamic stabilization could also reduce excessive fluid administration and prolonged vasopressor support, which have been associated with unfavorable outcomes [28,53,54].
6. Limitations and Future Perspectives
Despite the above detailed promising results, clinical data, well-designed prospective studies are still lacking. In human case reports and case series, authors report that HA therapy resulted in improved microcirculatory flow, assessed in the sublingual region in septic shock patients that was also associated with hemodynamic stabilization, improvement of metabolic acidosis, and overall sequential organ failure assessment (SOFA) scores [8,55]. Such studies suggest that sublingual microcirculatory monitoring may provide a useful diagnostic tool for evaluating endothelial and microcirculatory function to guide the use and timing of HA using microcirculatory improvement as a clinical target for resuscitation [56].
In one of the earliest case reports in a patient treated with severe acute respiratory distress syndrome (ARDS), HA appeared to decrease capillary leakage and alveolar fluid accumulation, as evidenced by improved respiratory function, a significantly reduced need for fluid resuscitation, and achievement of a negative fluid balance shortly after therapy initiation [57]. In a recent multicenter study in critically ill COVID-19 patients with respiratory failure requiring extracorporeal membrane oxygenation (ECMO) support who were also treated with HA, Hayanga et al. reported higher survival rates compared with the global experience in such patients treated with ECMO alone [58]. Results of a recent retrospective study on 124 septic patients suggest that HA therapy is associated with a reduced positive fluid balance and reduction in vasopressor needs that may, in part, be attributable to potential positive effects on endothelial integrity [59]. Finally, a recent systematic review and meta-analysis found that HA in ARDS patients resulted in a reduction in vasopressor requirements and a decrease in CRP levels as well as a significant improvement in oxygenation, potentially corresponding to improvements in endothelial function and lower fluid balance [60].
7. Conclusions
There is robust data that hyperinflammation contributes to endothelial damage, which in turn, triggers the deleterious pathophysiological cascade of lost endothelial function leading to vasoplegia, resulting in tissue hypoperfusion, organ failure, and ultimately death. Hemoadsorption is capable of removing circulating cytokines, inflammatory mediators, and additional toxic proteins responsible for endothelial damage, thereby potentially exerting endothelial protection and improving micro- and macrocirculatory function. Whether these mechanistic effects translate into palpable clinical benefits is a question for future research.
Funding
This project was partially funded by the Hungarian National Research, Development and Innovation Office, Grant No.: K 138816.
Competing Interests Statement (even if there are none)
ZM received honoraria for lectures and consultations from CytoSorbents Europe; CI received lecture honoraria and travel reimbursement from CytoSorbents Europe GmbH over the last five years; JB and MP have no conflict of interest related to this topic.
References
- Singer, M., et al., The Third International Consensus Definitions for Sepsis and Septic Shock (Sepsis-3). JAMA, 2016. 315(8): p. 801-10.10.1001/jama.2016.0287. [CrossRef]
- Ronco, C. and R. Bellomo, History and Development of Sorbents and Requirements for Sorbent Materials. Contrib Nephrol, 2023. 200: p. 2-7.10.1159/000529569. [CrossRef]
- Kellum, J.A., et al., Understanding the inflammatory cytokine response in pneumonia and sepsis: results of the Genetic and Inflammatory Markers of Sepsis (GenIMS) Study. Arch Intern Med, 2007. 167(15): p. 1655-63.10.1001/archinte.167.15.1655. [CrossRef]
- Peng, Z.Y., M.J. Carter, and J.A. Kellum, Effects of hemoadsorption on cytokine removal and short-term survival in septic rats. Crit Care Med, 2008. 36(5): p. 1573-7.10.1097/CCM.0b013e318170b9a7. [CrossRef]
- Song, M., et al., Cytokine removal with a novel adsorbent polymer. Blood Purif, 2004. 22(5): p. 428-34.10.1159/000080235. [CrossRef]
- Jansen, A., et al., CytoSorb hemoperfusion markedly attenuates circulating cytokine concentrations during systemic inflammation in humans in vivo. Crit Care, 2023. 27(1): p. 117.10.1186/s13054-023-04391-z. [CrossRef]
- Dilken, O., et al., Successful Reduction of Creatine Kinase and Myoglobin Levels in Severe Rhabdomyolysis Using Extracorporeal Blood Purification (CytoSorb(R)). Blood Purif, 2020. 49(6): p. 743-747.10.1159/000505899. [CrossRef]
- Zuccari, S., et al., Changes in Cytokines, Haemodynamics and Microcirculation in Patients with Sepsis/Septic Shock Undergoing Continuous Renal Replacement Therapy and Blood Purification with CytoSorb. Blood Purif, 2020. 49(1-2): p. 107-113.10.1159/000502540. [CrossRef]
- Bottari, G., et al., Impact of CytoSorb and CKRT on hemodynamics in pediatric patients with septic shock: the PedCyto study. Front Pediatr, 2023. 11: p. 1259384.10.3389/fped.2023.1259384. [CrossRef]
- Bottari, G., et al., Hemoperfusion with Cytosorb in pediatric patients with septic shock: A retrospective observational study. Int J Artif Organs, 2020. 43(9): p. 587-593.10.1177/0391398820902469. [CrossRef]
- Friesecke, S., et al., Extracorporeal cytokine elimination as rescue therapy in refractory septic shock: a prospective single-center study. J Artif Organs, 2017. 20(3): p. 252-259.10.1007/s10047-017-0967-4. [CrossRef]
- Hawchar, F., et al., Hemoadsorption in the critically ill-Final results of the International CytoSorb Registry. PLoS One, 2022. 17(10): p. e0274315.10.1371/journal.pone.0274315. [CrossRef]
- Hawchar, F., et al., Extracorporeal cytokine adsorption in septic shock: A proof of concept randomized, controlled pilot study. J Crit Care, 2019. 49: p. 172-178.10.1016/j.jcrc.2018.11.003. [CrossRef]
- Kogelmann, K., et al., First Evaluation of a New Dynamic Scoring System Intended to Support Prescription of Adjuvant CytoSorb Hemoadsorption Therapy in Patients with Septic Shock. J Clin Med, 2021. 10(13): p. 2939.10.3390/jcm10132939. [CrossRef]
- Kogelmann, K., et al., Hemoadsorption by CytoSorb in septic patients: a case series. Crit Care, 2017. 21(1): p. 74.10.1186/s13054-017-1662-9. [CrossRef]
- Rugg, C., et al., Hemoadsorption with CytoSorb in Septic Shock Reduces Catecholamine Requirements and In-Hospital Mortality: A Single-Center Retrospective 'Genetic' Matched Analysis. Biomedicines, 2020. 8(12): p. 539.10.3390/biomedicines8120539. [CrossRef]
- Brouwer, W.P., S. Duran, and C. Ince, Improved Survival beyond 28 Days up to 1 Year after CytoSorb Treatment for Refractory Septic Shock: A Propensity-Weighted Retrospective Survival Analysis. Blood Purif, 2021. 50(4-5): p. 539-545.10.1159/000512309. [CrossRef]
- Brouwer, W.P., et al., Hemoadsorption with CytoSorb shows a decreased observed versus expected 28-day all-cause mortality in ICU patients with septic shock: a propensity-score-weighted retrospective study. Crit Care, 2019. 23(1): p. 317.10.1186/s13054-019-2588-1. [CrossRef]
- Heymann, M., R. Schorer, and A. Putzu, The Effect of CytoSorb on Inflammatory Markers in Critically Ill Patients: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Crit Care Med, 2023. 51(12): p. 1659-73.10.1097/CCM.0000000000006007. [CrossRef]
- Becker, S., et al., Efficacy of CytoSorb(R): a systematic review and meta-analysis. Crit Care, 2023. 27(1): p. 215.https://doi.org/10.1159/000528706. [CrossRef]
- Vincent, J.L., C. Ince, and P. Pickkers, Endothelial dysfunction: a therapeutic target in bacterial sepsis? Expert Opin Ther Targets, 2021. 25(9): p. 733-748.10.1080/14728222.2021.1988928. [CrossRef]
- Jacob, M., et al., The endothelial glycocalyx affords compatibility of Starling's principle and high cardiac interstitial albumin levels. Cardiovasc Res, 2007. 73(3): p. 575-86.10.1016/j.cardiores.2006.11.021. [CrossRef]
- Reitsma, S., et al., Endothelial glycocalyx structure in the intact carotid artery: a two-photon laser scanning microscopy study. J Vasc Res, 2011. 48(4): p. 297-306.10.1159/000322176. [CrossRef]
- Villalba, N., S. Baby, and S.Y. Yuan, The Endothelial Glycocalyx as a Double-Edged Sword in Microvascular Homeostasis and Pathogenesis. Front Cell Dev Biol, 2021. 9: p. 711003.10.3389/fcell.2021.711003. [CrossRef]
- Joffre, J., et al., Endothelial Responses in Sepsis. Am J Respir Crit Care Med, 2020. 202(3): p. 361-370.10.1164/rccm.201910-1911TR. [CrossRef]
- Evans, L., et al., Surviving sepsis campaign: international guidelines for management of sepsis and septic shock 2021. Intensive Care Med, 2021. 47(11): p. 1181-1247.10.1007/s00134-021-06506-y. [CrossRef]
- Kusza, K., et al., Ringer's lactate solution enhances the inflammatory response during fluid resuscitation of experimentally induced haemorrhagic shock in rats. Arch Med Sci, 2018. 14(3): p. 655-670.10.5114/aoms.2017.69771. [CrossRef]
- Ince, C., Hemodynamic coherence and the rationale for monitoring the microcirculation. Crit Care, 2015. 19 Suppl 3(Suppl 3): p. S8.10.1186/cc14726. [CrossRef]
- Zarbock, A., et al., Sepsis-associated acute kidney injury: consensus report of the 28th Acute Disease Quality Initiative workgroup. Nat Rev Nephrol, 2023. 19(6): p. 401-417.10.1038/s41581-023-00683-3. [CrossRef]
- Saemann, L., et al., Cytokine Adsorber Use during DCD Heart Perfusion Counteracts Coronary Microvascular Dysfunction. Antioxidants (Basel), 2022. 11(11): p. 2280.10.3390/antiox11112280. [CrossRef]
- Denzinger, M., et al., Bioassay for Endothelial Damage Mediators Retrieved by Hemoadsorption. Sci Rep, 2019. 9(1): p. 14522.10.1038/s41598-019-50517-1. [CrossRef]
- Piskovatska, V., et al., Proteins Adsorbed during Intraoperative Hemoadsorption and Their In Vitro Effects on Endothelium. Healthcare (Basel), 2023. 11(3): p. 310.10.3390/healthcare11030310. [CrossRef]
- David, S., et al., Effect of extracorporeal cytokine removal on vascular barrier function in a septic shock patient. J Intensive Care, 2017. 5: p. 12.10.1186/s40560-017-0208-1. [CrossRef]
- Drost, C.C., et al., Interleukin-6 drives endothelial glycocalyx damage in COVID-19 and bacterial sepsis. Angiogenesis, 2024.10.1007/s10456-024-09916-w. [CrossRef]
- Nylen, E.S., et al., Mortality is increased by procalcitonin and decreased by an antiserum reactive to procalcitonin in experimental sepsis. Crit Care Med, 1998. 26(6): p. 1001-6.10.1097/00003246-199806000-00015. [CrossRef]
- Brabenec, L., et al., Targeting Procalcitonin Protects Vascular Barrier Integrity. Am J Respir Crit Care Med, 2022. 206(4): p. 488-500.10.1164/rccm.202201-0054OC. [CrossRef]
- Mehta, Y., et al., Modulating the Inflammatory Response With Hemadsorption (CytoSorb) in Patients Undergoing Major Aortic Surgery. J Cardiothorac Vasc Anesth, 2021. 35(2): p. 673-675.10.1053/j.jvca.2020.06.028. [CrossRef]
- Akil, A., et al., Combined Use of CytoSorb and ECMO in Patients with Severe Pneumogenic Sepsis. Thorac Cardiovasc Surg, 2021. 69(3): p. 246-251.10.1055/s-0040-1708479. [CrossRef]
- Öveges, N., et al., Early cytokine adsorption in septic shock (ACESS-trial): results of a proof concept, pilot study, in ISICEM. 2018, Crit Care: Brussels. p. P113.
- Cyrille, N.B., P.A. Villablanca, and H. Ramakrishna, Soluble urokinase plasminogen activation receptor--An emerging new biomarker of cardiovascular disease and critical illness. Ann Card Anaesth, 2016. 19(2): p. 214-6.10.4103/0971-9784.179588. [CrossRef]
- Vicka, V., et al., Kinetics of SuPAR hemoadsorption in critical COVID-19 patients on renal replacement therapy. BMC Nephrol, 2022. 23(1): p. 371.10.1186/s12882-022-03003-2. [CrossRef]
- Roca, N., et al., Relationship between soluble urokinase-type plasminogen activator receptor and serum biomarkers of endothelial activation in patients with idiopathic nephrotic syndrome. Clin Kidney J, 2021. 14(2): p. 543-549.10.1093/ckj/sfz173. [CrossRef]
- Nusshag, C., et al., suPAR links a dysregulated immune response to tissue inflammation and sepsis-induced acute kidney injury. JCI Insight, 2023. 8(7): p. e165740.10.1172/jci.insight.165740. [CrossRef]
- Schenk, H., et al., Removal of focal segmental glomerulosclerosis (FSGS) factor suPAR using CytoSorb. J Clin Apher, 2017. 32(6): p. 444-452.10.1002/jca.21538. [CrossRef]
- Rumpret, M., et al., Inhibitory pattern recognition receptors. J Exp Med, 2022. 219(1).10.1084/jem.20211463. [CrossRef]
- Li, L. and Y.Q. Lu, The Regulatory Role of High-Mobility Group Protein 1 in Sepsis-Related Immunity. Front Immunol, 2020. 11: p. 601815.10.3389/fimmu.2020.601815. [CrossRef]
- Yang, R., et al., HMGB1 and Extracellular Histones Significantly Contribute to Systemic Inflammation and Multiple Organ Failure in Acute Liver Failure. Mediators Inflamm, 2017. 2017: p. 5928078.10.1155/2017/5928078. [CrossRef]
- Shen, X. and W.Q. Li, High-mobility group box 1 protein and its role in severe acute pancreatitis. World J Gastroenterol, 2015. 21(5): p. 1424-35.10.3748/wjg.v21.i5.1424. [CrossRef]
- Abrams, S.T., et al., Circulating Histones Are Mediators of Trauma-associated Lung Injury. American Journal of Respiratory and Critical Care Medicine, 2013. 187(2): p. 160-169.10.1164/rccm.201206-1037OC. [CrossRef]
- Shaw, R.J., et al., Circulating histones play a central role in COVID-19-associated coagulopathy and mortality. Haematologica, 2021. 106(9): p. 2493-2498.10.3324/haematol.2021.278492. [CrossRef]
- Gruda, M.C., et al., Broad adsorption of sepsis-related PAMP and DAMP molecules, mycotoxins, and cytokines from whole blood using CytoSorb(R) sorbent porous polymer beads. PLoS One, 2018. 13(1): p. e0191676.10.1371/journal.pone.0191676. [CrossRef]
- Weber, B., et al., Effects of Circulating HMGB-1 and Histones on Cardiomyocytes-Hemadsorption of These DAMPs as Therapeutic Strategy after Multiple Trauma. J Clin Med, 2020. 9(5): p. 1421.10.3390/jcm9051421. [CrossRef]
- Malbrain, M.L., et al., Fluid overload, de-resuscitation, and outcomes in critically ill or injured patients: a systematic review with suggestions for clinical practice. Anaesthesiol Intensive Ther, 2014. 46(5): p. 361-80.10.5603/AIT.2014.0060. [CrossRef]
- Russell, J.A., Vasopressor therapy in critically ill patients with shock. Intensive Care Med, 2019. 45(11): p. 1503-1517.10.1007/s00134-019-05801-z. [CrossRef]
- Duran, S., et al., Sublingual Microcirculatory Evaluation of Extracorporeal Hemoadsorption with CytoSorb(R) in Abdominal Sepsis: A Case Report. Blood Purif, 2022. 51(7): p. 634-638.10.1159/000518903. [CrossRef]
- Duranteau, J., et al., The future of intensive care: the study of the microcirculation will help to guide our therapies. Crit Care, 2023. 27(1): p. 190.10.1186/s13054-023-04474-x. [CrossRef]
- Traeger, K., et al., Cytokine Reduction in the Setting of an ARDS-Associated Inflammatory Response with Multiple Organ Failure. Case Rep Crit Care, 2016. 2016: p. 9852073.10.1155/2016/9852073. [CrossRef]
- Hayanga, J.W.A., et al., Extracorporeal hemoadsorption in critically ill COVID-19 patients on VV ECMO: the CytoSorb therapy in COVID-19 (CTC) registry. Crit Care, 2023. 27(1): p. 243.10.1186/s13054-023-04517-3. [CrossRef]
- Kogelmann, K., et al., Impact of CytoSorb Hemoadsorption Therapy on Fluid Balance in Patients with Septic Shock. J Clin Med, 2024. 13(1): p. 294.10.3390/jcm13010294. [CrossRef]
- Szigetvary, C.E., et al., Hemoadsorption as Adjuvant Therapy in Acute Respiratory Distress Syndrome (ARDS): A Systematic Review and Meta-Analysis. Biomedicines, 2023. 11(11): p. 3068.10.3390/biomedicines11113068. [CrossRef]
Figure 1.
Hyperinflammation caused endothelial damage and protection with hemoadsorption. Legend: PAMPs, pathogen associated molecular patterns; DAMP, damage associated molecular patterns. See explanation in text.
Figure 1.
Hyperinflammation caused endothelial damage and protection with hemoadsorption. Legend: PAMPs, pathogen associated molecular patterns; DAMP, damage associated molecular patterns. See explanation in text.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



