
Submitted:
24 October 2024
Posted:
24 October 2024
You are already at the latest version
Abstract
Foam rolling is widespread and deeply rooted in exercise practice. Optimal duration and role of this treatment still lack scientific consensus. Relatively novel foam rolling treatment that combines vibration during application targets different muscle characteristics that are not well understood. Studies exploring this combined treatment are scarce therefore the aim of this study was to investigate the acute effects of different duration vibration (15-s, 30-s and 60-s) foam rolling treatment on muscle skin temperature and surface muscle electromyography during Maximal Voluntary Isometric Contraction. Eighteen male subjects attended the research laboratory for three experimental sessions and performed four sets of three trials of maximal isometric heel rises. Repeated measures ANOVA determined that muscle skin temperature significant difference was only found for the 30-s treatment (p = 0.013 - 0.000). For surface muscle electromyography a 30-s treatment out of all three yielded the most significant results, between pretreatment set and post treatment set1 (p=0.01) small effect size (Cohen’s d= -0.33) and pretreatment set to post treatment set3 (p=0.01) small effect size (Cohen’s d= -0.30). All treatments did not produce significant difference during Maximal Voluntary Isometric Contraction heel rises. Future studies should investigate accute effects of longer duration treatment on changes in surface muscle temperature. Muscle activity could suggest that efficiency was improved taken into account of unchanged muscle strength, also downward trend of muscle activity caused by other two treatment durations could be of significance during rehabilitation process or during activites where this is a desired and indicated goal.
Keywords:
Self-myofascial release treatment
; foam rolling
; maximum voluntary isometric contraction
; vibration muscle treatment
1. Introduction
Foam rolling has been gaining more research focus in recent years and still there is a lack of guidelines in terms of optimal duration and role of this treatment. Physiotherapists and other practitioners commonly prescribe foam rolling as an intervention, but the mechanistic effects of this intervention are not known [1]. Widespread application of this treatment far outweighs the evidence found in current literature regarding proper and beneficial use. Individual applies its own bodyweight thus the applied direct mechanical pressure to the targeted soft tissue is performed by rolling the desired body part over the foam roller. In literature this is addressed as self-massage (self-myofascial release). Foam rolling treatment (FRt) may play an important role in variety of exercise-induced processes such as improvement of athletic performance, reduction in muscle pain, reduction in muscle, tendon, and fasciae inflammation, improving cellular circulation, influencing muscle mobility by changing range of motion, etc [2]. It has also been shown that the voluntary activation can be affected when applying mechanical pressure on a muscle tissue [3]. Therefore, the athletic performance and recovery protocols could be altered with muscle properties changes caused by the FRt [4].
Foam roller with vibration (Vibration foam roller treatment - VFRt) is a recent development. Electrical motor which is battery powered and inside of a foam roller is creating vibrations, most often with a range of frequency selection (Figure 1).
However, combining two treatments (i.e., rolling and vibration) at the same time in form of VFRt is creating a gap between the practice and science since clear evidence in favor of this treatment have not yet been established [4]. The potential beneficial role of vibration in this treatment could stem from the well-studied effects of vibration training/therapy. Highly supported by other whole body vibration (WBV) studies is the finding that increasing muscle strength is possible [5]. During maximal voluntary contraction frequency of motor unit excitation is 30 Hz [6]. For most effective muscle activation the optimal frequent range is from 30 Hz to 50 Hz and especially vibration training could induce greater improvements in muscle strength and power at elite athletes then in lower level athletes [7]. Where to place VFRt in a single training session or during the competition (e.g., pre-warmup, warm-up or pre-competition) is an important question as misplacing this treatment could have a significant impact on the muscle performance needed in the main part of training or during the high intensity or competitive activity [4].
Up to date, studies examining the effects of VFRt are scarce. First study to our knowledge regarding muscle temperature change was on a sample of twelve adolescent male squash players utilizing 60-s FRt and found no significant changes in quadriceps skin muscle temperature [1]. If thixotropy is one of the possible mechanisms through which acute effects are expressed during FRt or VFRt muscle temperature changes should be detectable and examined. Muscle’s contractile properties such as contraction time and force production may be affected by temperature changes [8]. Endothelial function was examined in a study on a sample of ten healthy young adults who performed SMR (FRt) and control trials on separate days in a randomized controlled crossover fashion and SMR proceeded in the order of adductors, hamstrings, quadriceps, iliotibial band and trapezius in duration of 20 repetitions per muscle group, plasma nitric oxide (NO) concentration were measured before and 30 minutes after both SMR and CON trials and the authors of the study found the plasma NO concentration significantly increased (from 20.4 ± 6.9 to 34.4 ± 17.2 µmol.L-1) after SMR using a foam roller (both p<0.05), but neither significantly differed after CON trials so external compression might be a major pathway of vasodilation induced by the increased release of NO [9]. Study on a sample of 20 healthy adult subjects performing isometric squat on a vibrating Galileo platform at a frequency of 26 Hz examined the blood volume in calf muscles and quadriceps muscle through the means of Doppler ultrasound imaging and found significant blood volume increase in the analyzed muscles [10]. Recent study utilizing two FRt protocols (2x1-min, 2x3-min) applied to the right anterior thigh of twenty healthy subjects found that local blood flow increased significantly from pre to post test (F(1,19) = 7.589, p = 0.013), being higher (∆ +9.7%) in the long-FRt condition than in the short-FR condition (∆ +2.8%), longer FRt durations seem to be more beneficial for perfusion which is of interest for exercise professionals designing warm-up and cool-down regimes [11]. Since time and energy of an individual as one of the main resources should be focused on beneficial procedures it becomes clear that FRt needs to be addressed if the aim is to improve any type of pre-warmup or warmup procedure.
Fourteen recreationally trained subjects were tested on two separate occasions in a randomized cross-over design to compare the effects of SS and self-massage (SM) with a roller massage for three sets of 30-s of the calf muscles on electromyography (EMG of soleus and tibialis anterior) characteristics [12], authors found that EMG values were not affected by either intervention. A study with the aim to determine the effects of applying a roller massager for 20-s and 60-s to the quadriceps muscles on knee-joint ROM and dynamic muscular performance on a sample of ten recreationally active men found that 20-s to 60-s of roller massage improved ROM and muscular efficiency (reduced VL-vastus lateralis EMG) during a lunge [13]. A recent study involved 21 male subjects who visited the laboratory on two separate days and were randomly assigned to either a VFR group (30 Hz) or a NVFR group, both interventions were performed for 3×1-min each, surface electromyography results were analyzed and showed no significant effects on the EMG values during MVIC [14].
So far researchers have used FRt durations ranging from 5-s to 3-min and others have used sets of treatment while the effect of treatment duration is not well studied [15]. Since thigh muscles seem to contribute marginally for the control of standing balance in healthy, young subjects [16], the role of plantar flexor muscles is important in many activities therefore they are set as a focus of interest in this study. When observed in exercise practice and in published data most common FRt duration is up to 1-min per muscle group. In terms with ecological validity the aim of this study was set to determine the acute effects of different duration VFRt in the range up to 60-s on surface muscle skin temperature (sMT) and surface muscle electromyography (sEMG) during MVIC (Fmax). Also the relationship between sEMG and MVIC as a measurement of efficiency will be investigated. As a methodological standpoint the general hypothesis was set as a negative one, the VFRt would reduce MsT and sEMG.
2. Materials and Methods
2.1. Experimental Approach to the Problem
In this study a randomized cross-sectional design was used in a research laboratory setting. Each subject attended the research laboratory for three experimental sessions, only during the first session, anthropometrics and body composition measurements were collected using an anthropometer and InBody 720 body composition analyzer (Biospace, Korea) according to previously described procedures [17]. The flowchart of this study is shown in (Figure 2).
Subjects performed standardized general and specific warm up and four sets of three trials of maximal isometric heel rises. The first set of trials was used as a baseline labeled as Pretreatment initial set (PreTset), while the other three sets were performed after 1, 5 and 10-min of rest, labeled Posttreatment set 1, 2 and 3 (PostTset1, 2 and 3). Experimental sessions were done in a random order during which subjects performed three different duration vibration foam rolling treatment: 15 seconds labeled VFRt-15-s, 30 seconds VFRt-30-s and 60 seconds VFRt-60-s. All experimental sessions were applied at the same time of the day and were separated by one week. Ambient temperature in the research laboratory was controlled with AC units.
2.2. Subjects
Eighteen male adult amateur athletes from different sports volunteered to participate in this study. Subjects signed the written informed consent prior to beginning the study testing. The main inclusion criteria were that they were familiar with the foam rolling while the exclusion criteria were having the history of neural conditions and major muscular and/or tendon injury, or the use of any medicine during the last month that could affect the outcome of the findings. The main characteristics of the sample were age = 25.1 ± 4 years, height = 185.1 ± 6 cm, weight = 80.6 ± 7 kg, percent of body fat = 11.2 ± 3.9% and percent of skeletal muscle mass = 50.8 ± 2.4%. All subjects were instructed to refrain from performing any exercise at least 48-h prior to experimental testing session. Testing and treatment procedures were approved by the ethics board of the Faculty of Sport and Physical Education, University of Belgrade (number III47015) and the study was conducted in accordance with the Helsinki Declaration [18].
2.3. Procedures
General warm up protocol included the stationary bicycle lasting 5-min at 70 watts with individually adjusted sitting height to achieve full leg extension during cycling. During specific warm up subjects performed two sets of 10 standing heel raises with focus on fast concentric phase, this was followed with one set of 10 countermovement and one set of 10-15 quick ankle jumps. Upon completion of specific warm up subjects rested for 3-min after which were positioned in a testing position and performed three submaximal attempts to get familiar to the setting and instructions. The above described applied warm up protocol was the same as in the previously published study [4].
2.4. Electromyography and Temperature Outputs from MVIC Heel Rise
In this study a standardized test procedure and equipment were used to asses plantar flexor muscles [4,5,6,7,8,9,10,11,12,13,14,15,16,17,18,19] Custom-made construction with a fixed force transducer (tensile/compressive sensitivity 2 mV/n, Hottinger, Type S9, Darmstadt, Germany) was used for collecting data and the signal was acquisitioned and processed by software-hardware system (Isometrics Lite, ver. 3.1.1, Sport medical solutions, Belgrade, Serbia). The activity of the aforementioned muscle of both legs was measured on a premarked, preshaved and precleaned (Figure 3) spot using a sEMG wireless system (Trigno, Delsys, Boston, MA, USA) according to established procedure [20]. Clinically validated infrared thermometer (Microlife NC150, Microlife AG, Widnau, Switzerland) was used to measure sMT on a premarked spot on the calf muscle of both legs (gastrocnemius muscle medial head). Trial-to-trial reliability was checked for the PreTset and the calculated ICC values for sEMG and sMT (before general warm up) were 0.894 (95 % confidence interval 0.738-0.963) and 0.735 (95 % confidence interval 0.452-0.886). Calculated ICC value for sMT (after general and specific warm up and before PreTset) was 0.688 (95 % confidence interval 0.328-0.867). ICC value for MVIC during heel rises was 0.819 (95 % confidence interval 0.602-0.927).
In a seated position with hips and knees at 90° of flexion (Figure 4) subjects kept their back straight without leaning on the backrest during trials. With full feet were on the floor a wooden horizontal plate connected to the floor with perpendicularly positioned force transducer was placed over the thighs and was individually adjusted to firmly keep the feet on the ground, preventing the possibility of heel raise. On the researcher’s word Go a subject had to initiate the calf rise as strong and fast as possible. Three trials in each set were performed, separated with 2-min rest and the best of three trials was used for the analysis. The same testing protocol was repeated immediately after VFRt, after 5-min and after 10-min rest.
2.5. VFRt Protocol
Upon completion of PreTset subjects rested for 15-min prior to VFRt. A Wave roller (Thera Body, LA, USA), 30 x 13 cm (Figure 1) made of Hypo-allergenic EVA high-density foam was used for the VFRt. The vibration frequency was set at 29 Hz from the range of 5 preset frequencies. From the sitting position on the floor with legs extended subjects were using their bodyweight to press the calves over the roller. Subjects positioned one calf over the foam roller, while the other leg was crossed over the leg that rolls. To standardize the speed of rolling a metronome was used so each subject performed the same number of rolls (2 rolls per second). VFRt was self-administered for 15-s, 30-s and 60-s over subjects’ soleus and gastrocnemii muscles from proximal to distal portion of the calf (muscle belly and tendons) and then they switched legs and rolled for the same duration.
2.6. Variables
During MVIC testing three variables were examined: Fmax, sMT and sEMG. The Fmax was expressed in Newtons (N), sMT in degree Celsius (°C) and sEMG as RMS (root mean square) in microvolts (µV). For sMT and sEMG obtained values of both legs are calculated as average. Data from sEMG were collected during each MVIC trial. Collected sMT data was obtained during different time points: before general warm up (sMT-bfr-GW), immediately after general and specific warm up (sMT-aftr-GSW), immediately after PreTset (sMT-PreTset-1min), after 15-min of rest (sMT-PreTset-15min), immediately after PostTset1 (sMT-PostTset1-1min) and after 5-min of rest (sMT-PostTset1-5min).
2.7. Statistical Analysis
The basic descriptive statistics for mean, standard deviation (SD), coefficient of variation (cV%) were calculated for all the examined variables. The Shapiro-Wilk test was employed to assess the normality of data distribution prior to statistical analyses of VFRt effects. Variables showed normal data distribution, Fmax (p = 0.081 – 0.951), sMT-AVG (p = 0.054 – 0.073) and sEMG-AVG (p = 0.132 – 0.181) thereby the parametric statistic tests were used. The effects of self-administered VFRt on examined muscle outputs were established using the repeated measures ANOVA. The pairwise comparison was analyzed by Bonferroni post hoc test. To emphasize the effect size for the observed differences between and within treatments Cohen’s d was calculated and the results were interpreted using Cohen’s effect size classification [21]. The statistical significance was set at p < 0.05 and all statistical procedures were performed in the SPSS for Windows, Release 17.0 (Copyright © SPSS Inc., 1989-2002).
3. Results
The descriptive statistics for Fmax and repeated measure ANOVA results are presented in Table 1. The cV% values suggest homogeneous sample (10.4-16.8). The repeated measure ANOVA determined that any of the self-administered VFRt did not produce significant difference between the Fmax at PreTsets and PostTsets.
The descriptive statistics for sMT and repeated measure ANOVA results are presented in Table 2. The cV% values suggest homogeneous sample (0.8-1.7). The repeated measure ANOVA determined that there was no significant difference between any of the self-administered VFRt. A significant difference was only found for the VFRt-30-s and a detail view of the results is presented in the Table 3.
The descriptive statistics for sEMG and repeated measure ANOVA results are presented in Table 4. The cV% values suggest homogeneous sample (22.6-34.2). A detailed repeated measure ANOVA analysis found significant difference between VFRt-15-s and VFRt-60-s on a PostTset2 level, medium effect size (Cohen’s d 0.45) and between VFRt-30-s and VFRt-60on a level PostTset3, medium effect size (Cohen’s d=0.60). Within VFRt-15-s a significant difference was found only between PostTset1and PostTset3 (p=0.02). A VFRt-30-s out of all three yielded the most significant results, between PreTset and PostTset1 (p=0.01) small effect size (Cohen’s d= -0.33) and PreTset to PostTset3 (p=0.01) small effect size (Cohen’s d= -0.30). Within VFRt-60-s a significant difference was found between PostTset1 and PostTset3 (p=0.008). Relative difference (%) between initial testing (PreTset) and PostTset of each VFRt is presented in (Figure 5). A decreasing trend of the results is visible for VFRt-15-s and VFRt-60-s although not statistically significant. For VFRt-30-s a positive trend of the results is visible, statistically significant at level PostTset1 and PostTset3.
4. Discussion
The aim of this study was to investigate the acute effects of different duration self-administered vibration foam rolling treatment (15-s, 30-s and 60-s) on sMT and sEMG of plantar flexors during MVIC. Results of this study indicate that any of the here applied VFRt did not affect the Fmax. Regarding sMT results suggest that only VFRt-30-s affected the plantar flexors in a negative way. Also, interesting finding is that only the VFRt-30-s affected plantar flexors sEMG causing a significantly elevated activity. The other two applied VFRt induced a decrease in sEMG but without significance.
The results of this study in terms of acute effects on Fmax are consistent with the findings from the study where higher vibration frequency and duration was applied, three sets of 60-s foam rolling at a frequency of 48 Hz for the calf muscles [22,23]. In contrast, a study which used a similar setup for isometric testing to our study except the treatment and testing were done on one leg and also for the same muscle group as in our study, applied self-massage with a roller stick (no vibration) for three sets of 30-s led to a significantly greater force (8.2%) production relative to static stretching and to a small increase in MVIC of about 4%, 10-min after the intervention [12]. Three sets of 30-s vibration foam rolling treatment at 28 Hz on hamstring and quadriceps muscles found that vibration rolling was effective in increasing quadriceps isokinetic muscle strength by 2-fold [24]. Lower activation of the vastus medialis during maximal voluntary contraction and elevated parasympathetic responses after myofascial release treatment was reported relative to sham ultrasound, authors suggest that massage may induce a transient loss of muscle strength or a change in the muscle fiber tension-length relationship [25]. Future research should focus on providing a clear understanding of mechanisms involved in changes of muscle strength properties during and after implementation of this self-treatment since many are proposed but with consensus so far.
Increased muscle contractile capacity occurs with higher muscle temperature after acute bouts of passive heating, also enhanced voluntary and involuntary fast force contraction properties are apparent [26]. Passive heating suggests that increased muscle temperature is more effective on fast contraction force (e.g., RFD and time to peak torque) and a probable mechanism responsible for this is the release of the Ca2+ into the myoplasm which results in the binding of Ca2+ to troponin C unblocking the sites between the actin and myosin heads (cross-bridges formation), subsequently producing force development [26]. Regardless of its implementation in the field of sport or rehabilitation, VFRt is not a passive technique, similar acute effects could be expected and are of importance for exercise practice. The findings of our study are the first to our knowledge to present the acute effects of different duration VFRt on surface muscle temperature. The findings in our study regarding no change during 60-s treatment are in agreement with the findings of the study of [1]. The other finding in our study concerning that a VFRt-30-s produced statistically significant and decreasing results of sMT is somewhat surprising. It was to be expected that longer duration, thus friction should induce greater changes in sMT. Increases in blood flow, and subsequently in muscle fluid, in response to passive heating may also increase the rate of cross-bridge formation and the muscle shortening velocity besides increasing muscle stiffness, causing a positive effect on RFD [26]. It is to be expected that the same mechanism could be responsible during VFRt. Local muscle blood flow increases linearly with muscle temperature [27] and can rise by 61% after heat exposure [28]. FRt could be one of the interventions among others to prevent the detrimental effects of limb immobilization on skeletal muscle health. Daily exposure to heat stress results in increased heat shock protein expression, maintains mitochondrial respiratory capacity and attenuates atrophy in skeletal muscle and may serve as an effective therapeutic strategy [29]. While no single therapeutic intervention may offer the physical, physiological and mental benefits of exercise, exercise mimetic strategies have the potential to provide at least some like benefits, especially for sedentary and clinical population [30]. Passive heating may offer exercise mimetic hypertrophy and neuromuscular adaptations that could resultantly increase the quality of life and decrease healthcare costs [31]. Future studies should investigate longer duration VFRt and utilize other sensitive devices for detecting muscle temperature changes during and after VFRt.
The main finding of our study regarding changes in sEMG is the differentiation of one duration treatment that led to elevated acute effects 20-min after and that was VFRt-30-s. This finding is the first to our knowledge in published literature to yield such statistically significant results. Within VFRt-15-s and VFRt-60-s a significant difference was found between PostTset1 and PostTset3 which could suggest that fatigue did occur but the findings of VFRt-30-s and no changes in Fmax suggest otherwise. Even though VFRt-15-s and VFRt-60-s caused an insignificant decrease in relationship to baseline (pretest) sEMG this finding could be interpreted as improved muscle efficiency since for the unchanged Fmax values muscles exhibited lower activity after treatment. Such finding is in agreement with the finding of the study where foam rolling treatment in duration of 2-min during three consecutive days caused a decrease in sEMG during same submaximal task (50 % of MVC), authors interpreted this finding as improved muscle efficiency [32]. In terms of improved efficiency, the results of this study are in agreement with the findings of [13]. The authors of that study concluded that while performing the same motoric task (lunge) lower EMG activity was recorded of the muscle Vastus lateralis therefore the muscle efficiency was improved. The same authors also state that foam rolling is an active process since during treatment the recorded surface EMG activity was 7 % and 8 % of MVIC for muscles Biceps femoris and Vastus lateralis. Cocontractions are a normal human response to a potential unpleasant or during unpleasant situation such as FRt [33]. In contrast, a study on 14 subjects during which the effects of static streching and foam rolling (roller massager) were compared, both treatments for three sets of 30-s, the recorded values of surface EMG activity of muscles soleus and tibialis anterior showed no significant difference [12]. In agreement with previously mentioned study are the results of the study done on 21 male active subjects (mean age 25.2 ± 3.8) where the effects of VFR (30 Hz) and FR were compared in terms of surface EMG and the results showed no significant difference between two treatments during MVIC testing [14].
Whole body vibration in a study where 45 Hz frequency was applied during isometric squat for five sets of 1-min the recorded surface EMG revealed that H-reflex and M-wave amplitude was decreased comparing to baseline measurement and remained decreased for 20-min after the vibration treatment [34]. On the sample of 11 subjects during 2-min FRt of quadriceps muscle H reflex value was found to returne to baseline values after two minutes of rest after cessation of treatment thus allowing the activation of deep mechanoreceptors to decrease and normal production of force [35]. In contrast [36], the findings of the study suggest that FRt of plantar flexor muscles did not change the relationship of H/M waves as a measure of spine excitability independent of gender. When interpreting sEMG activity one should approach with caution. A plausible explanation could be found in the study of [37], which offers an interpretation that EMG amplitude is a poor determinant of neural activation. Larger subject sample size could provide more valid findings of this study. Also, research has shown that differences in muscle architecture can influence EMG amplitude, even when the muscle is activated at a similar intensity [38]. For small muscles, the relationship between force and the EMG signal tend to be linear, whereas in bigger muscles that need a better motor recruitment, the same relationship tends to not be linear, because the amplitude variations of the muscle electric signal do not correspond to the force variations [39]. In a study with a purpose to evaluate a possible linear relationship between the RMS value of the EMG signal and the contraction force of the rectus femoris, vastus medialis, lateralis, biceps femoris, semitendinosus, and brachial biceps muscles on a sample of 24 female university students that practice physical activity regularly results showed that a linear relationship with the required torque was found between the contraction force and the RMS value of the EMG signal in females for the analyzed muscles [40].
5. Conclusions
Data from our study suggest that short duration application up to one minute, of self-administered myofascial release treatment with a vibrating foam roller (VFRt) presents a safe technique for plantar flexor muscle strength properties. Specifically in terms of maximal muscle force production that remained unchanged after any of the three here administered durations. Application of this short duration treatment did not provide any meaningful detectable surface muscle temperature changes that could be of practical importance at this moment. Future studies should investigate accute effects of longer duration treatment on changes in surface muscle temperature. Our findings regarding surface EMG changes indicate that the use of VFRt-30s should be implemented if the desired outome of this treatment is the elevated muscle activity. Although the VFRt-15s and VFRt-60s caused the downward trend of muscle activity, when taken into consideration together with the finding of unchanged muscle strength it can be concluded that muscle efficiency was improved which is of practical importance in the field of sport, recreation and esspecialy rehabilitation. Also, a downward trend of muscle activity caused by these two treatment durations could be of significance during rehabilitation process for certain conditions where it is beneficial in terms of health to decrease the muscle activity.
Author Contributions
Conceptualization, A.B., M.D. and M.Ć.; Methodology, A.B. and M.D.; Validation, A.B.; Formal analysis, A.B. and M.D.; Investigation, A.B. and G.J.; Resources, A.B.; Writing—original draft preparation, A.B.; Writing—review and editing, A.B. and M.Ć.; Visualization, A.B., I.R. and D.J.; Supervision, M.D.; Project administration, A.B. All authors have read and agreed to the published version of the manuscript.
Institutional Review Board Statement
Testing and treatment procedures were approved by the ethics board of the Faculty of Sport and Physical Education, University of Belgrade (number III47015).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
Authors state that there are no conflicts of interest, including financial, consultant, institutional, and other relationships that might have led to bias and that the present study complies with the current laws of the country in which it was performed.
References
- Murray, A.; Jones, T.; Horobeanu, C.; Turner, P.; Sproule, J. Sixty Seconds of Foam Rolling Does Not Affect Functional Flexibility or Change Muscle Temperature in Adolescent Athletes. Int J Sports Phys Ther, 2016, 11, 765–776. [Google Scholar] [PubMed]
- Wiewelhove, T.; Döweling, A.; Schneider, C.; Hottenrott, L.; Meyer, T.; Kellmann, M.; Pfeiffer, M.; Ferrauti, A. A meta-analysis of the effects of foam rolling on performance and recovery. Front Physiol 2019. [Google Scholar] [CrossRef] [PubMed]
- Cavanaugh, T.; Döweling, A.; Young, D.; Quigley, J.; Hodgson, D. , Whitten, H.; Behm, G. An acute session of roller massage prolongs voluntary torque development and diminishes evoked pain. Eur. J Appl. Physiol, 2017, 117, 109–117. [Google Scholar] [CrossRef] [PubMed]
- Borisavljević, A.; Kukić, F.; Janković, G.; Ćosić, M.; Dopsaj, M. Acute effects of vibration foam rolling on the explosive strength properties of the plantar flexors during maximal isometric contraction. IES 2023. [Google Scholar] [CrossRef]
- Esmaeilzadeh, S.; Akpinar, M.; Polat, S.; Yildiz, A.; Oral, A. The effects of two different frequencies of whole-body vibration on knee extensors strength in healthy young volunteers: a randomized trial. J Musculoskelet Neuronal Interact, 2015, 15, 333–340. [Google Scholar]
- Silva, E.; Nubi, M.; Vaamonde, D.; Fernandez, J.; Garcia-Manso, M.; Lancho, L. Effects of different frequencies of whole body vibration on muscular performance. Biol. Sport, 2006, 23, 124–132. [Google Scholar]
- Luo, J.; McNamara, B.; Moran, K. The Use of Vibration Training to Enhance Muscle Strength and Power. Sports medicine (Auckland, N.Z.), 2005, 35. [Google Scholar] [CrossRef]
- Ranatunga, W.; Sharpe, B.; Turnbull, B. Contractions of a human skeletal muscle at different temperatures. J Physiol, 1987, 390, 383–395. [Google Scholar] [CrossRef]
- Okamoto, T.; Masuhara, M.; Ikuta, K. Acute effects of self-myofascial release using a foam roller on arterial function. J Strength Cond Res, 2014, 28, 69–73. [Google Scholar] [CrossRef] [PubMed]
- Kerschan-Schindl, K.; Grampp, S.; Henk, C.; Resch, H.; Preisinger, E.; Fialka-Moser, V.; Imhof, H. Whole-body vibration exercise leads to alterations in muscle blood volume. Clin Physiol, 2001, 21, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Schroeder, J.; Wilke, J.; Hollander, K. Effects of Foam Rolling Duration on Tissue Stiffness and Perfusion: A Randomized Cross-Over Trial. J Sports Sci Med, 2021, 20, 626–634. [Google Scholar] [CrossRef] [PubMed]
- Halperin, I.; Aboodarda, J.; Button, C.; Andersen, L. , Behm, G. Roller massager improves range of motion of plantar flexor muscles without subsequent decreases in force parameters. Int J Sports Phys Ther, 2014, 9, 92–102. [Google Scholar] [PubMed]
- Bradbury-Squires, J.; Noftall, C.; Sullivan, M.; Behm, G.; Power, E.; Button, C. Roller-massager application to the quadriceps and knee-joint range of motion and neuromuscular efficiency during a lunge. J Athl Train, 2015, 50, 133–140. [Google Scholar] [CrossRef] [PubMed]
- Reiner, M.; Glashüttner, C.; Bernsteiner, D.; Tilp, M.; Guilhem, G.; Morales-Artacho, A.; Konrad, A. A comparison of foam rolling and vibration foam rolling on the quadriceps muscle function and mechanical properties. Eur J Appl Physiol, 2021, 121, 1461–1471. [Google Scholar] [CrossRef] [PubMed]
- Phillips, J.; Diggin, D.; King, L.; Sforzo, A. Effect of Varying Self-myofascial Release Duration on Subsequent Athletic Performance. J Strength Cond Res, 2021, 35, 746–753. [Google Scholar] [CrossRef]
- Dos Anjos, F.; Pinto, P.; Cerone, L.; Gazzoni, M.; Vieira, M. Is the attenuation effect on the ankle muscles activity from the EMG biofeedback generalized to - or compensated by - other lower limb muscles during standing? J Electromyogr Kinesiol, 2022, 67. [Google Scholar] [CrossRef]
- Dopsaj, M.; Kukić, F.; Đorđević-Nikić, M.; Koropanovski, N.; Radovanović, D.; Miljuš, D.; Subošić, D.; Tomanić, M.; Dopsaj, V. Indicators of Absolute and Relative Changes in Skeletal Muscle Mass during Adulthood and Ageing. Int J Environ Res Public Health, 2020, 17. [Google Scholar] [CrossRef] [PubMed]
- Williams, R. The Declaration of Helsinki and public health. Bull World Health Organ, 2008, 86, 650–652. [Google Scholar] [CrossRef]
- Majstorović, N.; Nešić, G.; Grbić, V.; Savić, Z.; Živković, M.; Aničić, Z.; Marković, S.; Dopsaj, M. Reliability of a simple novel field test for the measurement of plantar flexor muscle strength. Rev. Bras. Med. Esporte, 2021, 27. [Google Scholar] [CrossRef]
- Hermens, H.; Freriks, B.; Disselhorst-Klug, C.; Rau, G. Development of recommendations for SEMG sensors and sensor placement procedures. J Electromyogr Kinesiol, 2000, 10. [Google Scholar] [CrossRef]
- Sullivan, M.; Feinn, R. Using Effect Size—or Why the P Value Is Not Enough. J Grad Med Educ, 2012, 4. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Sato, S.; Kiyono, R.; Yoshida, R.; Murakami, Y.; Yasaka, K.; Yahata, K.; Konrad, A. Acute Effect of Vibration Roller With and Without Rolling on Various Parts of the Plantar Flexor Muscle. Front Physiol, 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, M.; Sato, S.; Kiyono, R.; Yoshida, R.; Yasaka, K.; Yahata, K.; Konrad, A. Comparison Between Foam Rolling With and Without Vibration on Passive and Active Plantar Flexor Muscle Properties. J Strength Cond Res, 2021, 1. [Google Scholar] [CrossRef] [PubMed]
- Lee, L.; Chu, H.; Lyu, J.; Chang, D.; Chang, J. Comparison of vibration rolling, nonvibration rolling, and static stretching as a warm-up exercise on flexibility, joint proprioception, muscle strength, and balance in young adults. J Sports Sci, 2018, 36, 2575–2582. [Google Scholar] [CrossRef] [PubMed]
- Arroyo-Morales, M.; Olea, N.; Martínez, M.; Hidalgo-Lozano, A.; Ruiz-Rodríguez, C. , Díaz-Rodríguez, L. Psychophysiological effects of massage-myofascial release after exercise: a randomized sham-control study. J Altern Complement Med, 2008, 14, 1223–1229. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, P.; Trajano, S.; Stewart, B.; Minett, M. Potential role of passively increased muscle temperature on contractile function. Eur J Appl Physiol, 2022, 122. [Google Scholar] [CrossRef] [PubMed]
- Pearson, J. , Low, A.; Stöhr, E.; Kalsi, K.; Ali, L.; Barker, H.; González-Alonso, J. Hemodynamic responses to heat stress in the resting and exercising human leg: insight into the effect of temperature on skeletal muscle blood flow. Am J Physiol Regul Integr Comp Physiol, 2011, 300, 663–673. [Google Scholar] [CrossRef] [PubMed]
- Heinonen, I.; Brothers, M.; Kemppainen, J.; Knuuti, J.; Kalliokoski, K.; Crandall, G. Local heating, but not indirect whole body heating, increases human skeletal muscle blood flow. J Appl Physiol, 1985, 111, 818–824. [Google Scholar] [CrossRef]
- Hafen, S.; Abbott, K.; Bowden, J.; Lopiano, R.; Hancock, R.; Hyldahl, D. Daily heat treatment maintains mitochondrial function and attenuates atrophy in human skeletal muscle subjected to immobilization. J Appl Physiol, 1985, 127, 47–57. [Google Scholar] [CrossRef]
- Fan, W.; Evans, M. Exercise Mimetics: Impact on Health and Performance. Cell Metab, 2017, 25. [Google Scholar] [CrossRef]
- Hunt, P.; Minett, M.; Gibson, R.; Kerr, K. Stewart, B. Could Heat Therapy Be an Effective Treatment for Alzheimer's and Parkinson's Diseases? A Narrative Review. Front Physiol, 2019, 10. [Google Scholar] [CrossRef]
- Macgregor, L.; Fairweather, M.; Bennett, R.; Hunter, A. The Effect of Foam Rolling for Three Consecutive Days on Muscular Efficiency and Range of Motion. Sports Med Open, 2018, 4. [Google Scholar] [CrossRef] [PubMed]
- Chambers, J.; Cham, R. Slip-related muscle activation patterns in the stance leg during walking. Gait Posture, 2007, 25, 565–572. [Google Scholar] [CrossRef] [PubMed]
- Harwood, B.; Scherer, J.; Brown, E.; Cornett, M.; Kenno, A. , Jakobi, M. Neuromuscular responses of the plantar flexors to whole-body vibration. Scand J Med Sci Sports, 2017, 27, 1569–1575. [Google Scholar] [CrossRef] [PubMed]
- MacDonald, Z.; Penney, D.; Mullaley, E.; Cuconato, L. , Drake, D.; Behm, G.; Button, C. An acute bout of self-myofascial release increases range of motion without a subsequent decrease in muscle activation or force. J Strength Cond Res, 2013, 27, 812–821. [Google Scholar] [CrossRef]
- Nakamura, M.; Konrad, A.; Ryosuke, K.; Sato, S.; Yahata, K.; Yoshida, R.; Murakami, Y.; Sanuki, F.; Wilke, J. Sex Differences in the Mechanical and Neurophysiological Response to Roller Massage of the Plantar Flexors. J Sports Sci Med, 2021, 20, 665–671. [Google Scholar] [CrossRef]
- Martinez-Valdes, E.; Negro, F.; Falla, D.; De Nunzio, M.; Farina, D. Surface electromyographic amplitude does not identify differences in neural drive to synergistic muscles. J Appl Physiol, 2018, 124, 1071–1079. [Google Scholar] [CrossRef]
- Vieira, M.; Bisi, C.; Stagni, R.; Botter, A. Changes in tibialis anterior architecture affect the amplitude of surface electromyograms. J Neuroeng Rehabil, 2017, 14. [Google Scholar] [CrossRef]
- Basmajian, V. Muscles Alive—their functions revealed by electromyography. Postgrad Med J, 1963, 39, 162. [Google Scholar]
- Fukuda, Y.; Echeimberg, O.; Pompeu, E.; Lucareli, G.; Garbelotti, S.; Gimenes, O.; Apolinário, A. Root Mean Square Value of the Electromyographic Signal in the Isometric Torque of the Quadriceps, Hamstrings and Brachial Biceps Muscles in Female Subject. J App Res, 2010, 10, 32–39. [Google Scholar]
Figure 1.
Theragun Wave roller (https://www.therabody.com/us/en-us/wave-roller-us.html).
Figure 1.
Theragun Wave roller (https://www.therabody.com/us/en-us/wave-roller-us.html).

Figure 2.
Flow chart of the study design.
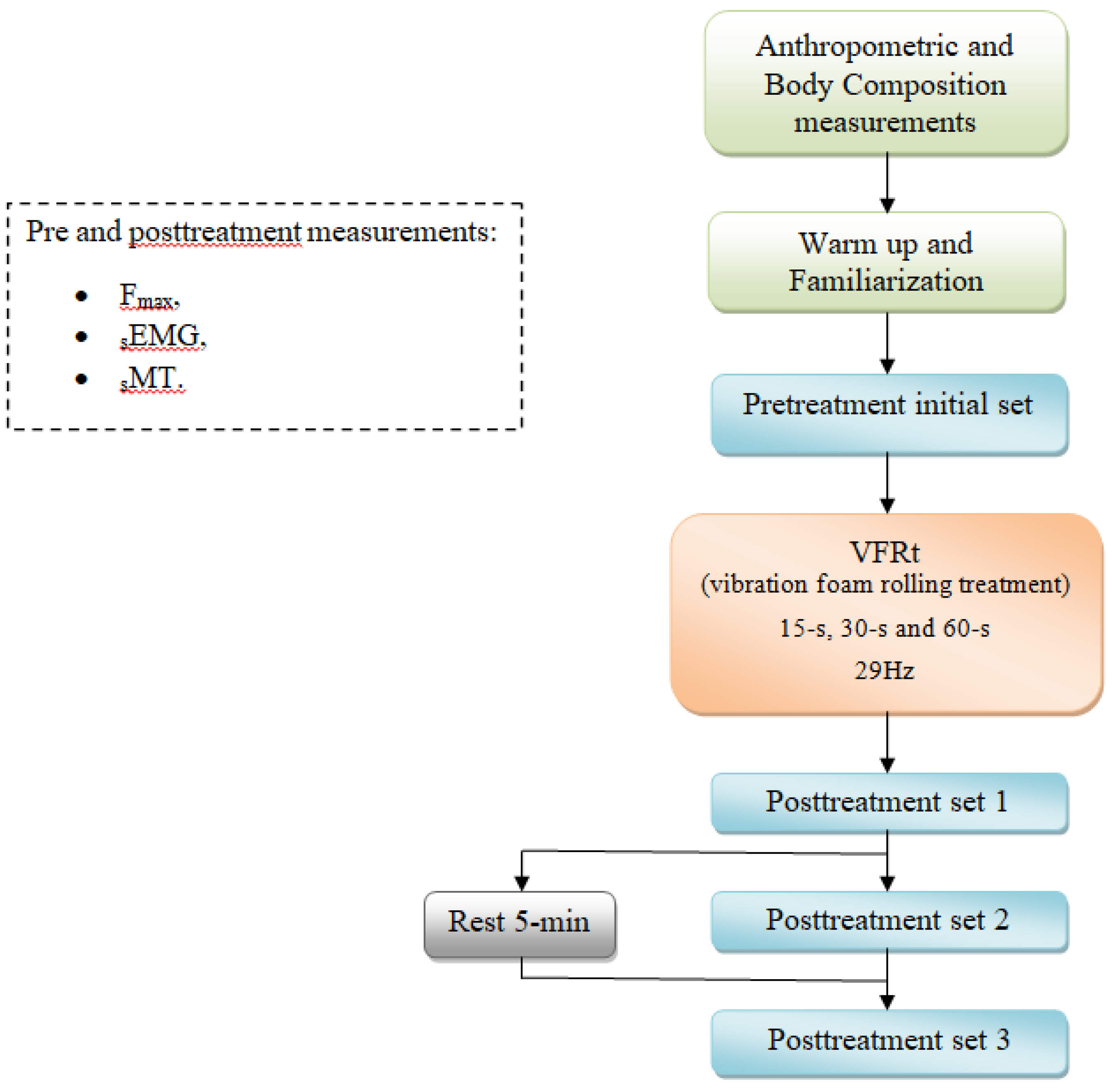
Figure 3.
sEMG electrodes spot.
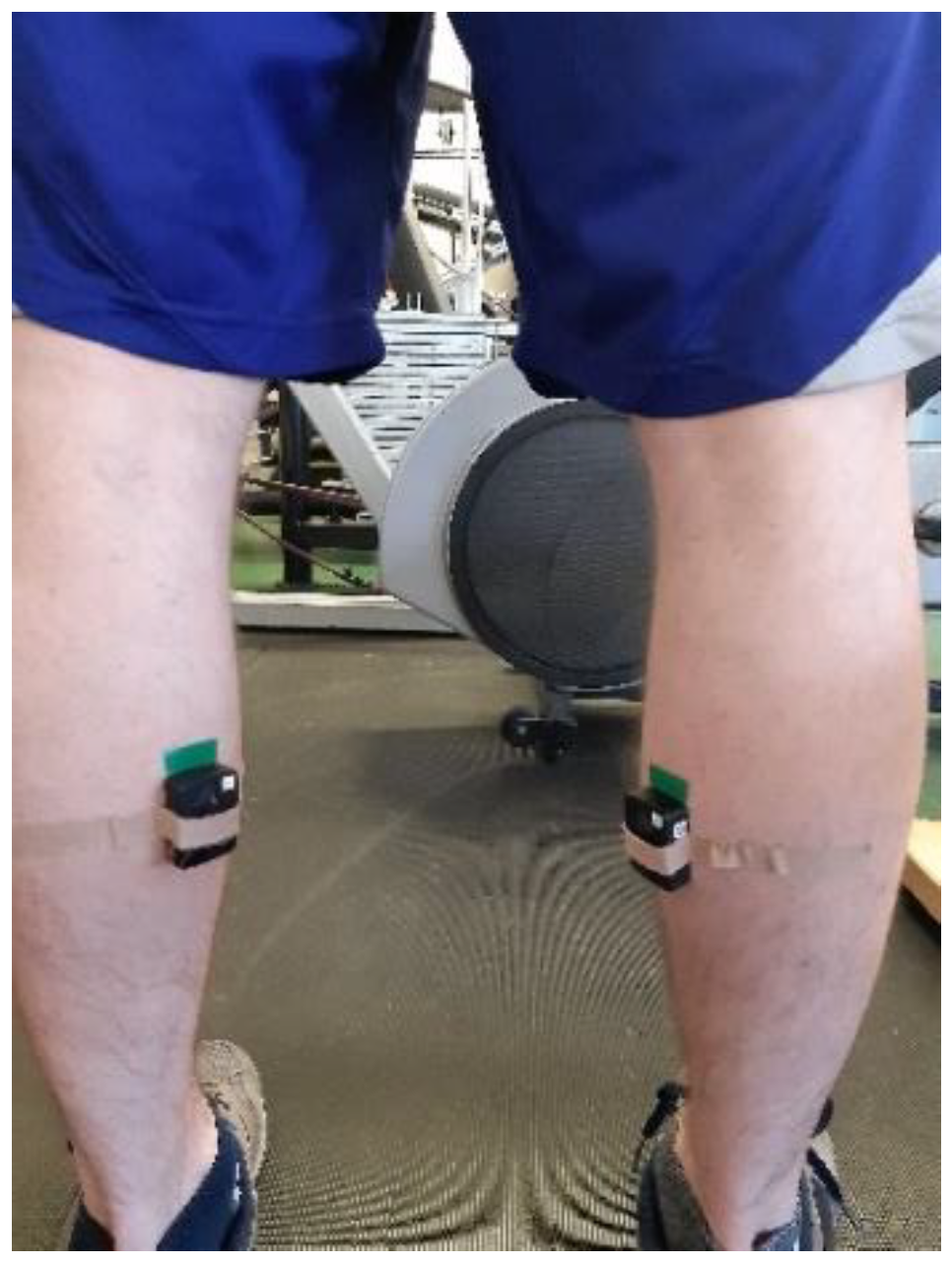
Figure 4.
The assessment of outputs during MVIC.
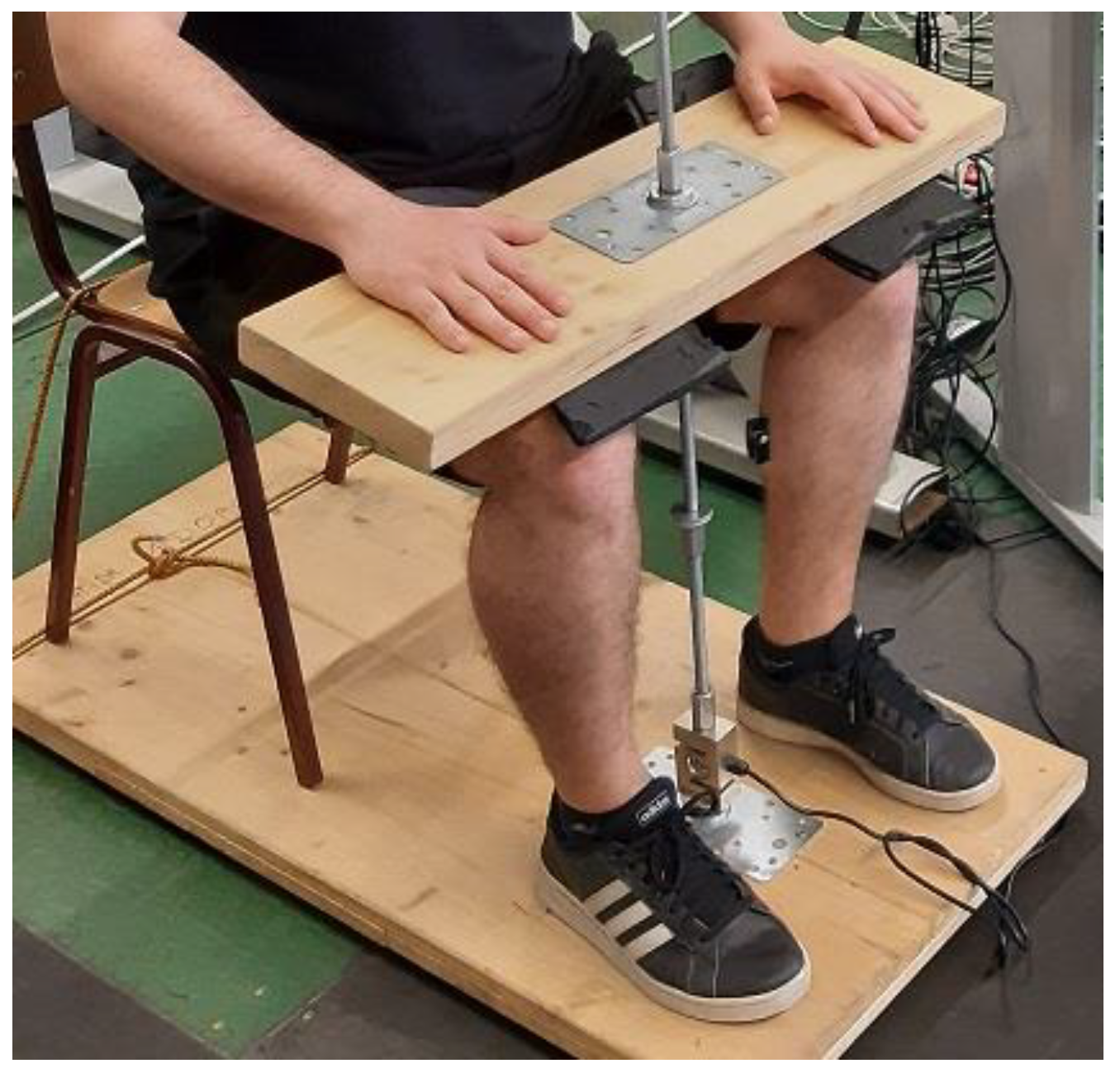
Figure 5.
Relative difference (%) between pretreatment and posttreatment set of each VFRt for sEMG.
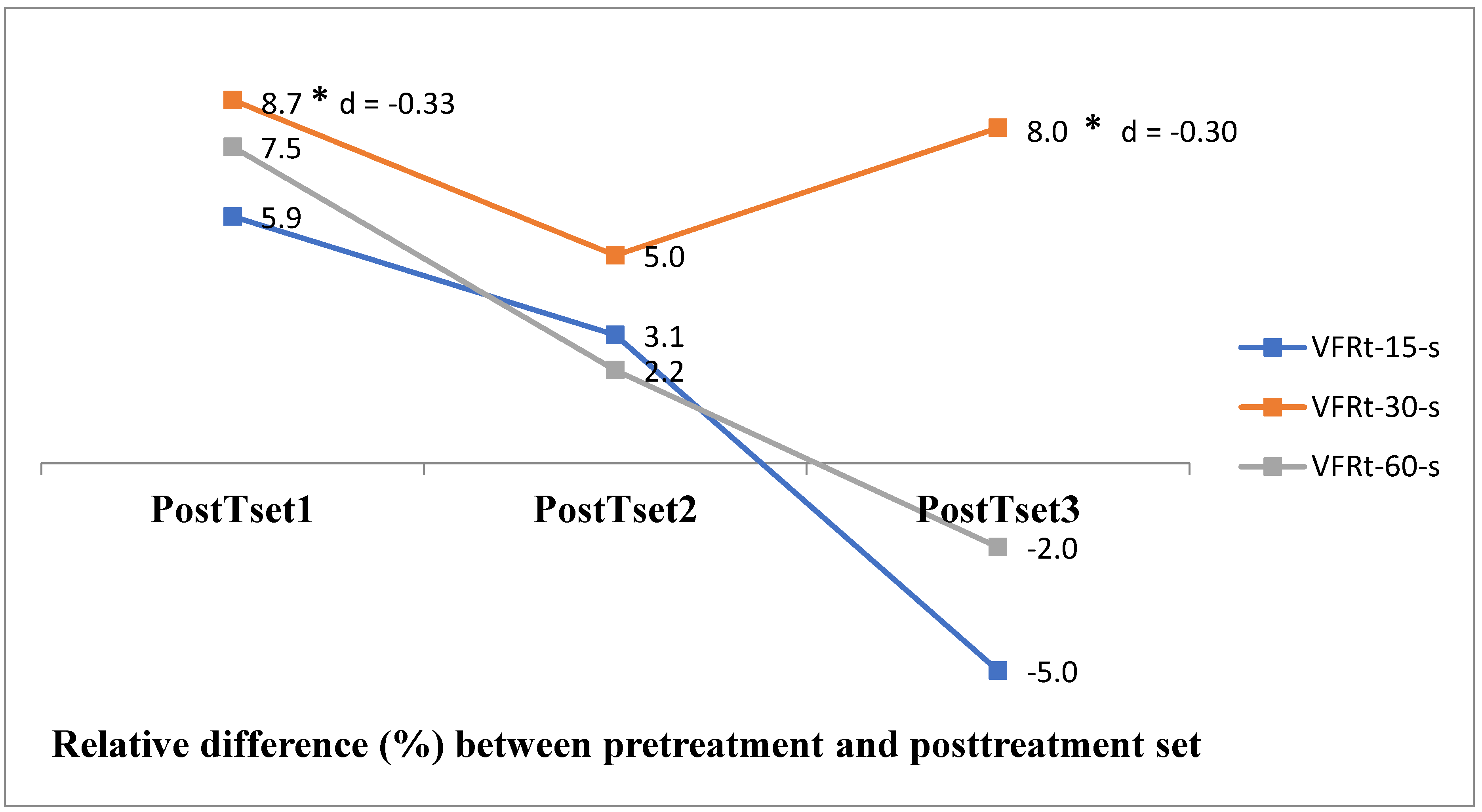

Table 1.
Descriptive and repeated measure ANOVA indicators for Fmax.
| Testing | Experimental session | ||||
| PreTset | Fmax _15-s | Fmax_30-s | Fmax_60-s | Wilks' Lambda | p |
| Mean ± SD | 3569 ± 373 | 3651 ± 484 | 3672 ± 620 | 0.93 | 0.57 |
| cV% | 10.4 | 13.2 | 16.8 | ||
| VFRt-15-s | VFRt-30-s | VFRt-60-s | |||
| PostTset1 | 3513 ± 366 | 3585 ± 441 | 3593 ± 571 | 0.94 | 0.61 |
| 10.4 | 12.3 | 15.9 | |||
| PostTset2 | 3509 ± 421 | 3560 ± 474 | 3574 ± 537 | 0.96 | 0.74 |
| 12.0 | 13.3 | 15.0 | |||
| PostTset3 | 3506 ± 368 | 3607 ± 557 | 3570 ± 588 | 0.94 | 0.63 |
| 10.5 | 15.4 | 16.4 | |||
| Wilks' Lambda | 0.94 | 0.85 | 0.84 | ||
| p | 0.82 | 0.48 | 0.46 | ||
Table 2.
Descriptive and repeated measure ANOVA indicators for sMT.
| Testing | Experimental session | ||||
| sMT-bfr-GW | sMT_15-s | sMT_30-s | sMT_60-s | Wilks' Lambda | p |
| Mean ± SD | 35.62 ± 0.32 | 35.72 ± 0.49 | 35.81 ± 0.48 | 0.85 | 0.24 |
| cV% | 0.9 | 1.4 | 1.3 | ||
| sMT-aftr-GSW | 35.42 ± 0.61 | 35.80 ± 0.42 | 35.86 ± 0.40 | 0.48 | 0.21 |
| 1.7 | 1.2 | 1.1 | |||
| sMT-PreTset-1min | 35.82 ± 0.39 | 35.95 ± 0.22 | 35.91 ± 0.34 | 0.87 | 0.28 |
| 1.1 | 0.6 | 0.9 | |||
| sMT-PreTset-15min | 35.71 ± 0.33 | 35.54 ± 0.43 | 35.75 ± 0.33 | 0.82 | 0.16 |
| 0.9 | 1.2 | 0.9 | |||
| VFRt-15-s | VFRt-30-s | VFRt-60-s | |||
| sMT-PostTset1-1min | 35.65 ± 0.27 | 35.50 ± 0.42 | 35.72 ± 0.28 | 0.78 | 0.11 |
| 0.8 | 1.2 | 0.8 | |||
| sMT-PostTset1-5min | 35.63 ± 0.27 | 35.51 ± 0.41 | 35.71 ± 0.28 | 0.80 | 0.14 |
| 0.8 | 1.2 | 0.8 | |||
| Wilks' Lambda | 0.52 | 0.39 | 0.64 | ||
| p | 0.06 | 0.003* | 0.11 | ||
| *. The mean difference is significant at the 0.05 level. | |||||
Table 3.
Repeated measure ANOVA indicators for sMT in VFRt-30-s.
| Pairwise Comparisons | ||||||
| sMT(°C) | Mean Diff. (I-J) | Std. Error | Sig.b | 95% Confidence Interval for Differenceb | ||
| Lower Bound | Upper Bound | |||||
| sMT-bfr-GW | sMT-aftr-GSW | -0.08 | 0.07 | 1.00 | -0.33 | 0.18 |
| sMT-PreTset-1min | -0.23 | 0.10 | 0.49 | -0.56 | 0.10 | |
| sMT-PreTset-15min | 0.18 | 0.12 | 1.00 | -0.23 | 0.59 | |
| sMT-PostTset1-1min | 0.22 | 0.09 | 0.34 | -0.08 | 0.51 | |
| sMT-PostTset1-5min | 0.21 | 0.09 | 0.33 | -0.07 | 0.50 | |
| sMT-aftr-GSW | sMT-PreTset-1min | -0.15 | 0.07 | 0.67 | -0.39 | 0.09 |
| sMT-PreTset-15min | 0.26 | 0.11 | 0.38 | -0.10 | 0.61 | |
| sMT-PostTset1-1min | 0.293* | 0.07 | 0.013* | 0.04 | 0.54 | |
| sMT-PostTset1-5min | 0.290* | 0.07 | 0.011* | 0.05 | 0.53 | |
| sMT-PreTset-1min | sMT-PreTset-15min | 0.410* | 0.09 | 0.004* | 0.10 | 0.72 |
| sMT-PostTset1-1min | 0.446* | 0.07 | 0.000* | 0.20 | 0.69 | |
| sMT-PostTset1-5min | 0.443* | 0.07 | 0.000* | 0.21 | 0.68 | |
| sMT-PreTset-15min | sMT-PostTset1-1min | 0.04 | 0.10 | 1.00 | -0.31 | 0.39 |
| sMT-PostTset1-5min | 0.03 | 0.10 | 1.00 | -0.32 | 0.38 | |
| sMT-PostTset1-1min | sMT-PostTset1-5min | 0.00 | 0.01 | 1.00 | -0.03 | 0.02 |
| Based on estimated marginal means | ||||||
| *. The mean difference is significant at the 0.05 level. | ||||||
| b. Adjustment for multiple comparisons: Bonferroni. | ||||||
Table 4.
Descriptive and repeated measure ANOVA indicators for sEMG.
| Testing | Experimental session | ||||
| PreTset | sEMG_15-s | sEMG_30-s | sEMG_60-s | Wilks' Lambda | p |
| Mean ± SD | 276.84 ± 84.74 | 255.35 ± 69.02 | 239.80 ± 76.66 | 0.75 | 0.18 |
| cV% | 30.6 | 27.0 | 32.0 | ||
| VFRt-15-s | VFRt-30-s | VFRt-60-s | |||
| PostTset1 | 293.13 ± 88.13 | 277.48 ± 62.79 | 257.90 ± 81.20 | 0.67 | 0.09 |
| 30.1 | 22.6 | 31.5 | |||
| PostTset2 | 285.29 ± 91.80 | 268.01 ± 67.37 | 245.13 ± 83.77 | 0.52 | 0.02* |
| 32.2 | 25.1 | 34.2 | |||
| PostTset3 | 263.14 ± 88.71 | 275.79 ± 65.44 | 234.00 ± 71.89 | 0.36 | 0.002* |
| 33.7 | 23.7 | 30.6 | |||
| Wilks' Lambda | 0.47 | 0.27 | 0.42 | ||
| p | 0.03* | 0.002* | 0.002* | ||
| *. The mean difference is significant at the 0.05 level. | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



