
Submitted:
23 October 2024
Posted:
24 October 2024
You are already at the latest version
Abstract
Polycystic ovary syndrome (PCOS) is the predominant endocrine disorder among women of re-productive age and represents the leading cause of anovulatory infertility, which imposes a con-siderable health and economic burden. Currently, medications used to treat PCOS can lead to certain adverse reactions, such as affecting fertility and increasing the risk of venous thrombosis. Drug delivery systems utilizing nanomaterials, characterized by prolonged half-life, preci-sion-targeted delivery, enhanced bioavailability, and reduced toxicity, are currently being em-ployed in the management of PCOS. This innovative approach is gaining traction as a favored strategy for augmenting the therapeutic efficacy of medications. Consequently, this paper dis-cusses the roles of nanoparticles, nanocarriers, and targeted ligands within nanomaterial-based drug delivery systems, aiming to identify optimal methodologies for treating PCOS using nano-materials. Additionally, prospective research avenues concerning nanomaterial-based delivery systems in the context of PCOS, as well as the implications of existing insights on the advancement of novel therapies for PCOS, are highlighted.
Keywords:
PCOS
; nanoparticles
; novel drug delivery systems
1. Introduction
Polycystic ovary syndrome (PCOS) is a multifaceted condition identified by elevated androgen levels, menstrual irregularities, the presence of polycystic ovaries, and related metabolic and psychological consequences. PCOS is the most common endocrine condition impacting women of reproductive age, representing the leading cause of anovulatory infertility and a noteworthy factor contributing to the early development of type 2 diabetes mellitus (T2DM) and psychiatric issues[1]. Furthermore, demonstrate a greater incidence of pregnancy-related problems, such as early miscarriage, gestational diabetes, hypertension, and preeclampsia, along with a markedly elevated risk for endometrial cancer [2,3,4]. Research indicates that approximately 11-13% of women worldwide are affected by PCOS, leading to considerable healthcare and economic challenges [5,6,7]. Current effective management strategies for PCOS primarily focus on addressing metabolic function, reproductive health, hyperandrogenism, and psychological well-being. Common pharmacological treatments include metformin, clomiphene citrate, ethinylestradiol, and cyproterone acetate [8,9]. Nonetheless, these medications may carry potential adverse effects, such as hindering conception and raising the risk of venous thromboembolism [10].
In recent years, drug delivery methods utilizing nanomaterials have garnered significant attention due to their unique advantages, including nanoscale dimensions, controlled release of therapeutic agents, superior biocompatibility, remarkable optical and physical characteristics, and straightforward surface modification [11]. Recent findings indicate that nanomaterials can effectively transport conventional therapeutics to mitigate damage caused by inflammatory responses and address endocrine dysfunction, thereby reversing the pathological alterations associated with the progression of PCOS [12]. Hence, nanomaterials present substantial potential for enhancing the treatment of PCOS. This paper provides a comprehensive overview of the latest advancements in nanocarrier delivery strategies, targeting molecules, and drug release triggers, aiming to identify the most effective combinations of nanomaterial-based delivery systems for PCOS management. Furthermore, it will also explore future research directions pertaining to nanodelivery strategies. (Figure 1)
Figure 1(A): The pathophysiological mechanisms underlying polycystic ovary syndrome (PCOS) predominantly encompass hyperandrogenism, insulin resistance, inflammatory responses, and oxidative stress. Current therapeutic approaches for PCOS primarily consist of pharmacological interventions, lifestyle modifications, and psychotherapy. Figure 1(B): A diverse array of novel nanomaterials has been employed for the management of PCOS. This includes nanoparticles— natural medicine nanoparticles sourced from ginger, cinnamon, camellia, and aloe vera, as well as metal-based nanoparticles derived from silver, iron, and selenium— along with liposomes, nanotubes, quantum dots, and micelles. Figure 1(C): Oocytes and granulosa cells may serve as targeted ligands, playing a significant role in innovative drug delivery systems. Chitosan and mannose can provide a protective function for the ovaries by binding to oocytes. Moreover, copper and silver nanoparticles possess the capability to transit through granulated cells, thereby influencing ovarian functions.
2. The Pathophysiology of PCOS
High androgen levels, irregular menstrual cycles, and the presence of polycystic ovaries are the hallmarks of PCOS, a multifaceted disorder. The pathophysiological mechanisms underlying PCOS are complex and include dysfunctions within the hypothalamic-pituitary-ovarian (HPO) axis, influenced by hyperandrogenemia, insulin resistance (IR), impaired steroidogenesis, and adipose tissue accumulation [13]. These elements are interdependent; typically, the accumulation of body fat or an increased body mass index (BMI) exacerbates hyperandrogenemia and insulin resistance, suggesting that weight loss can be an effective treatment for PCOS. Additionally, adipose tissue formation stimulates the ovaries to release more androgens, further perpetuating hyperandrogenemia. Conversely, insulin resistance and hyperandrogenism contribute to obesity and T2DM, which can then disrupt menstrual cycles and potentially lead to reproductive issues, anxiety, or depression. The hypothalamic secretion of gonadotropin-releasing hormone (GnRH) in the HPO axis is essential for the regulation of both androgen production and insulin resistance. A disruption in GnRH secretion can result in decreased levels of follicle-stimulating hormone (FSH) and increased levels of luteinizing hormone (LH) [14]. Previous studies have indicated that insulin, in conjunction with LH, can enhance the generation of androgens within follicular membrane cells [15,16,17]. Moreover, excessive secretion of adrenocorticotropic hormone (ACTH) can lead to an overproduction of androgens by the adrenal cortex [18]. This state of hyperandrogenemia disrupts follicular maturation and ultimately hinders ovulation.
The underlying pathophysiological mechanisms of polycystic ovary syndrome (PCOS) remain inadequately explored. Current research indicates that hyperandrogenemia, IR, and hyperinsulinemia serve as primary contributors to female reproductive dysfunction [19,20,21,22,23,24]. Furthermore, inflammatory responses and oxidative stress can adversely influence oocyte quality and endothelial function, thereby facilitating the onset of PCOS [25].
2.1. Hyperandrogenism
Hyperandrogenemia presents as a systemic condition characterized by elevated androgen levels, commonly evident through symptoms such as hirsutism, acne, alopecia, central obesity, and acanthosis nigricans. In individuals diagnosed with PCOS, this condition may stem from impaired endogenous steroidogenesis in ovarian cells [26]. The androgens circulating in the bloodstream of women include dehydroepiandrosterone sulfate (DHEAS), testosterone (T), dihydrotestosterone, dehydroepiandrosterone (DHEA), and androstenedione (A) [27]. In the context of PCOS, there is an overproduction of DHEAS, T, DHEA, and A, which contributes to premature development of ovarian follicles, formation of numerous small antral follicles, and anovulation [15]. Additionally, heightened peripheral cortisol metabolism is posited as another contributor to hyperandrogenemia. Reduced cortisol levels disrupt negative feedback in the hypothalamic-pituitary-adrenal (HPA) axis, leading to an increase in the synthesis of ACTH by the pituitary gland and this stimulates adrenal steroidogenesis. [28]. Therefore, various pathways can lead to excessive androgen levels, resulting in hyperandrogenemia, which is one of the primary underlying causes of the pathophysiology of PCOS. Furthermore, hyperandrogenemia is posited to be one of the potential contributors to IR in PCOS patients. Research by Paolo et al. [29] indicated that individuals with a hyperandrogenic phenotype exhibited characteristics of insulin resistance. The administration of antiandrogenic pharmacological agents has been suggested to ameliorate insulin resistance in this population [30].
2.2. IR
Insulin serves diverse functions across multiple tissues to maintain equilibrium between nutrient availability and requirement. Under normal physiological circumstances, rising blood glucose levels trigger heightened insulin secretion, facilitating glucose uptake by peripheral tissues while simultaneously suppressing hepatic gluconeogenesis. When the capacity of insulin to fulfill these metabolic functions is compromised, compensatory hyperinsulinemia emerges, a phenomenon commonly referred to as insulin IR [31]. IR is notably prevalent among individuals with PCOS, with estimates suggesting that around 75% of PCOS patients develop IR [32]. This condition is intricately linked to metabolic disturbances associated with PCOS. Research from the 1990s posited that insulin engages its specific receptor in PCOS, thereby promoting not only ovarian and adrenal steroidogenesis but also the secretion of LH from the pituitary organ [33]. The hyperinsulinemia induced by tissue IR is fundamental to the pathophysiology of PCOS [34]. Furthermore, IR in PCOS patients impacts metabolic or mitogenic pathways in non-traditional insulin-responsive tissues such as the ovaries and the pituitary gland [35]. Additionally, the HPO axis is disrupted and the progression of PCOS is accelerated, as IR intensifies hyperandrogenemia, according to compelling evidence [35].
2.3. Inflammatory Response and Oxidative Stress
According to research, patients diagnosed with polycystic ovary syndrome (PCOS) demonstrate elevated levels of genetic and inflammatory markers. Investigations have demonstrated a substantial correlation between elevated concentrations of C-reactive protein (CRP), interleukin-18 (IL-18), tumor necrosis factor-alpha (TNF-α), interleukin-6 (IL-6), and ferritin in women with PCOS and control groups that are age- and BMI-matched. [36,37,38,39]. Additional contributing factors include elevated leukocyte counts, elevated concentrations of plasminogen activator inhibitor type 1 (PAI-1), heightened activity of the renin-angiotensin system (RAS), and augmented levels of free fatty acids (FFA). Within the context of PCOS, hyperandrogenemia incites an inflammatory response alongside IR, both of which amplify reactive oxygen species (ROS) production and subsequently facilitate oxidative stress [40].
Studies have shown that oxidative stress disrupts normal follicular development and maturation [41,42].An excess of ROS can harm both oocytes and granulosa cells in the follicle, compromising their integrity and posing a risk to fertility [43,44]. Oxidative stress is notably linked to pathological conditions associated with PCOS, including IR, hyperandrogenism, inflammatory responses, and obesity. Frank González et al. [45] have proposed that hyperglycemia may elevate ROS levels, resulting in a pro-inflammatory environment that triggers IR and hyperandrogenism in individuals with PCOS. Furthermore, Insulin resistance may be facilitated by compromised oxidative phosphorylation and mitochondrial dysfunction, which disrupt insulin signaling pathways and impede glucose metabolism [46,47]. In obese individuals, markers of antioxidant activity such as superoxide dismutase (SOD) and glutathione peroxidase (GSH-Px) are significantly diminished[48].
3. Diagnosis and Treatment of PCOS
3.1. Diagnosis of PCOS
In 1935, Stein et al. [49] first recognized what is currently termed PCOS in their study. Since that time, various diagnostic criteria for PCOS have emerged, sparking a contentious debate that persisted until 2003. During this year, 27 PCOS experts convened in Rotterdam to establish a consensus statement referred to as the "Rotterdam Criteria" [50,51]. These criteria expand the phenotypic characterization of PCOS to encompass any two of the three primary features: oligomenorrhea, hyperandrogenism, and a polycystic ovarian pattern observed via ultrasound. The scientific investigation of PCOS has been impeded by the coexistence of multiple classification systems, which has led to clinical ambiguity. Consequently, in 2012, experts advocated for the adoption of the broader 2003 Rotterdam Criteria, while also delineating subphenotypes within these criteria: (1) androgen excess coupled with ovarian dysfunction, (2) androgen excess accompanied by ovarian polycystic morphology (PCOM), (3) ovarian dysfunction and PCOM, and (4) concomitant androgen excess, ovarian dysfunction, and PCOM. To date, the Rotterdam criteria remain the most widely employed and endorsed standards for diagnosing PCOS, receiving unanimous support in the 2018 International Guidelines for the Assessment and Management of Evidence-Based PCOS [52]. The specific clinical relevance or natural progression of each phenotype remains elusive; however, recent investigations have indicated that reproductive and metabolic phenotypes are segregating through novel genetic discoveries [53]. Additionally, a review of metabolic profiles and phenotypes demonstrates that obesity exacerbates complications in the majority of analyses, despite the fact that androgenic phenotypes frequently correspond with more severe metabolic dysfunction. This introduces additional complexities [54,55]. The disease's diagnostic features are also contingent upon race and lifespan, complicating classification and natural progression. Nevertheless, the Rotterdam criteria continue to be the predominant choice among clinicians across various specialties [56].
Two of the following three manifestations: clinical or biochemical hyperandrogenemia, oligomenorrhea or amenorrhea, and polycystic ovaries, must be identified in order to diagnose PCOS using the Rotterdam criteria [57]. Clinical manifestations of hyperandrogenism include acne, hirsutism, and androgenetic alopecia, while biochemical indicators may indicate elevated levels of total, free, or bioavailable testosterone [58]. Oligomenorrhea is classified as menstrual intervals exceeding 35 days or experiencing 5-9 menstrual cycles annually. Amenorrhea refers to the cessation of menstruation for a period of three months or more [59]. A polycystic ovarian morphology is defined as the presence of 20 or more follicles per ovary, with a diameter spanning from 2-9 mm, and/or an ovarian volume exceeding 10 ml, as determined by ultrasound [60]. Additionally, the diagnosis of PCOS is exclusive, mandating that healthcare practitioners exclude other prevalent conditions presenting with similar clinical, biochemical, and morphologic features. These conditions encompass thyroid disorders, hyperprolactinemia, and non-classic congenital adrenal hyperplasia [61]. For instance, individuals with primary hypothyroidism may experience menstrual irregularities, infertility, and weight gain [62]. Laboratory evaluations indicate minor increases in free and total testosterone, free and total estradiol, prolactin, and LH [62]. Changes in ovarian morphology, such as a bilateral polycystic appearance, may also be evident on ultrasound [62].
3.2. Treatment of PCOS
The intricate pathogenesis and characterization of PCOS necessitate a multifaceted treatment approach. This aims to alleviate diagnosed symptoms and support patient well-being. An international survey identified obesity, menstrual irregularities, infertility, and excessive hair growth as critical health concerns for PCOS patients [63]. Consequently, therapeutic strategies should prioritize these issues. The 2023 International Evidence-Based Guidelines for the Evaluation and Management of PCOS designate oral contraceptives as the primary treatment option for addressing menstrual irregularities and androgen excess [5]. Current medications mainly target specific symptoms linked to PCOS, with no drugs explicitly approved for the syndrome itself. Effective treatments should address health risks, mitigate key pathophysiological processes, and cater to individual symptoms and needs. When applicable, interventions should aim to restore ovulatory cycles, enhance fertility, normalize menstrual cycle length, reduce clinical and biochemical hyperandrogenemia, improve insulin sensitivity, promote weight reduction, lower cardiometabolic risks, and enhance disease-specific quality of life.
Current pharmacological options for PCOS primarily include contraceptives, anti-androgens, and insulin sensitizers. However, these treatments carry potential side effects. For instance, combined contraceptives with androgenic progestins like norethindrone risk worsening hyperandrogenic symptoms [64]. Anti-androgenic drugs may lead to feminization of male fetuses [65]. Additionally, insulin sensitizers are predominantly indicated for T2DM but are commonly utilized for PCOS [66]. Adverse effects can manifest as treatment resistance, low adherence, or even treatment discontinuation. Therefore, there is a pressing need to improve the efficacy of the current therapeutic agents for PCOS and to investigate strategies to alleviate their associated side effects.
4. Nanomaterials in PCOS Treatment
Over the last thirty years, nanomedicines have progressed significantly in pharmacology. They have transformed how we deliver active pharmaceutical compounds [67,68]. Numerous effective nanotherapies emerged for various human diseases [69,70,71,72]. Recently, advancements in nanotechnology have been noted in treating polycystic ovary syndrome (PCOS). Nanocarriers serve as vehicles to transport drugs targeting these diseases. Presently, we utilize different nanocarriers for PCOS-related conditions. These include nanoparticles, liposomes, carbon nanotubes, quantum dots, and micelles. Their benefits, challenges associated with PCOS, and the methods for drug administration are outlined below. (Table 1)
4.1. Nanoparticle
4.1.1. Natural-Based Drug Nanoparticles
Natural medicines encompass a range of therapies derived from animal, plant, and mineral sources, all of which modern pharmacological research has validated for specific bioactive properties. Recent trends indicate a notable rise in plant-derived drugs due to their potential rehabilitative, therapeutic, and preventative roles in herbal medicine [73,74]. Arentz et al. [75] revealed dissatisfaction with Western medication among women with PCOS and their supplemental medication utilization rate of more than 70%, which suggests patient preference for complementary therapies. In addition, traditional medications associated with the treatment of PCOS disorders have side effects and are likely to be ineffective in some cases [76,77]. Various herbs have recently garnered attention for their applications in PCOS, providing multiple active compounds that may yield synergistic effects [78]. A substantial number of botanicals are known to contain pharmacologically active constituents that can have a beneficial impact on ovulatory function, obesity, insulin sensitivity, and hormonal levels, according to previous research [79]. For example, Maharjan et al. [80] demonstrated that Aloe barbadensis gel positively impacted PCOS in an animal model induced by letrozole, while chamomile extract facilitated normal follicular development in PCOS-affected rats [81]. Javad Heshmati et al.'s clinical trial suggested that curcumin might serve as a safe and effective adjunct therapy for alleviating hyperandrogenism and hyperglycemia linked to PCOS [82].
In recent years, the therapeutic applications of natural drug nanoparticles have emerged, with properties like surface charge and size distribution paralleling those of mammalian extracellular microbubbles [83,84]. These nanoparticles act as natural nanocarriers for vesicle transport and possess structural and functional biomolecules that enhance their clinical utility [85]. This positions such nanovesicles as viable candidates for developing next-generation biotherapeutics and drug delivery systems, addressing pressing clinical needs.
Curcumin, a phenolic compound that is acknowledged for its anti-inflammatory and antioxidant properties, has demonstrated efficacy in reducing hyperandrogenism, insulin resistance, and hyperglycemia in PCOS patients [86,87]. However, its clinical utility is limited by solubility issues and suboptimal pH stability. Researchers are increasingly focusing on biocompatible polymeric nanoparticles, like chitosan (CS), which are readily manageable and dissolve quickly [68,88,89]. While CS exhibits low water solubility, this limitation can be mitigated through chemical modifications [90,91,92]. Functionalizing CS allows for the encapsulation of various drug molecules, enhancing the pharmacokinetic profiles of these active substances [93]. As a cationic polysaccharide, CS-nanoparticles are advantageous for embedding diverse compounds, including antimicrobials, analgesics, and anti-inflammatory agents [94]. Raja et al. [95] successfully developed nanoparticles featuring curcumin-embedded arginine and N-acetylhistidine-modified CS, effectively inhibiting serum LH, prolactin, testosterone, and insulin levels in a rat model compared to controls. This research marks an encouraging initial stride toward leveraging nanoparticles as a potent delivery mechanism for curcumin in treating PCOS.
Ginger originates from the rhizome of Zingiber officinale, containing a variety of bioactive compounds, including phenols, terpenes, and volatile oils. The bioactive component, 6-gingerol, imparts a robust flavor while lowering insulin levels and enhancing insulin sensitivity [96]. Anil Kumar et al. [97] revealed that ginger-derived nanoparticles also combat insulin resistance, possibly by enhancing Foxa2 expression, thus mitigating IEC exosome-mediated insulin resistance.
Cinnamon belongs to a diverse genus utilized for centuries in culinary, spice, and medicinal contexts. All cinnamon species contain various minerals such as cinnamaldehyde, eugenol, manganese, iron, calcium, dietary fiber, and related compounds [98].Clinical and animal trials have examined cinnamon's therapeutic benefits for PCOS [99]. Evidence indicates that cinnamon restores the estrous cycle, lowers testosterone and insulin levels, and elevates LH levels in murine models of PCOS [100]. A clinical study by Borzoei et al. involving 84 overweight women with PCOS demonstrated that brief cinnamon supplementation positively impacts metabolic risk factors [101]. Koffi Kouame et al. [102] identified Cinnamomum cassia-derived silver nanoparticles (CcAgNPS) potentially enhancing renal function in diabetic rats through their antioxidant properties.
4.1.2. Metal Nanoparticles
Traditionally, researchers synthesized nanoparticles through physical and chemical means, which present several challenges. Recent studies have shifted focus toward innovative therapeutic nanoparticles like silver and selenium for PCOS treatment [105]. Silver nanoparticles show promise in treating inflammation and reducing inflammatory markers in PCOS-afflicted rats [106]. Such advancements signal a progressive approach, as alleviating inflammation could diminish symptoms often associated with elevated inflammatory cytokines in PCOS patients.
Current investigations predominantly utilize metal nanoparticles via natural compounds to maximize therapeutic benefits. Silver nanoparticles demonstrate impressive antibacterial properties, exhibiting activity against cinnamon extracts noted for anticancer and anti-inflammatory effects [102,107,108]. Research indicates that curcumin-loaded iron nanoparticles can effectively inhibit apoptosis in ovarian injury cells, thereby providing potential benefits for PCOS management [109]. Selenium nanoparticles have also shown effectiveness in PCOS treatment by reducing androgen synthesis and disrupting the excessive androgen cycle via diminished androgen receptor expression [110]. Additionally, selenium nanoparticles have been found to attenuate insulin sensitivity markers, sex hormone concentrations, inflammation, and mitochondrial function in PCOS models [111].
4.2. Liposome
Liposomes represent self-assembled, spherical systems featuring lipid bilayers composed of one or more phospholipids [112]. These structures are both non-toxic and biodegradable, providing a versatile delivery mechanism for various pharmaceuticals [113]. They are capable of transporting a variety of substances, such as proteins, nucleic acids, and small molecules, which are hydrophobic and hydrophilic. By stabilizing compounds, liposomes enhance the therapeutic efficacy of drugs, overcome cellular uptake barriers, and facilitate the bio-distribution of drugs to target sites while mitigating systemic toxicity [114]. Resveratrol, a natural polyphenol, can enhance reproductive health, yet its application is restricted by low bioavailability. DMU-212, a methoxy derivative of resveratrol, demonstrates enhanced bioavailability as a result of its lipophilic properties. Researchers developed a liposomal version of DMU-212 (lipDMU-212) and demonstrated that lipDMU-212 substantially increases the secretion of estradiol and progesterone in a dose-dependent manner [115]. This finding indicates potential benefits of lipDMU-212 in treating conditions linked to estrogen deficiency and hyperandrogenism, such as PCOS.
4.3. Nanotubes
Carbon nanotubes are a new generation of materials that are extensively employed in biomedical applications due to their unique structure, attractive properties (e.g., size and aspect ratio of covering surface area to length), electrical, mechanical, and thermal properties [116]. Compared to other nanocarriers, carbon nanotubes can be easily modified to bind bioactive compounds and ligands for targeting. Therefore, the application of carbon nanotube-based nanomedicine is very attractive and promising. Miey Park et al. [117] reported that carbon nanotubes can exert a role in insulin resistance by reducing fasting blood glucose and improving serum biomarker levels associated with oxidative stress and inflammation. Carbon nanotubes are employed for diagnostic applications in addition to drug delivery. Human fetuin A (HFA) is a biomarker associated with PCOS insulin resistance as well as the inflammatory process of T2DM. Esther Sánchez-Tirado et al. [118] used magnetic multi-walled carbon nanotubes (m-MWCNTs) as nanocarriers to measure HFA, and the results showed that the performance of this assay was significantly superior to that reported by ELISA kits and chronoimpedance immunosensors. The study by Pradeep K Jha et al. [119] found that multi-walled carbon nanotubes are capable of loading silver nanoparticles and may be used in the diagnosis of infertility in the future. Furthermore, the toxicity of carbon nanotubes is an issue that must not be disregarded. Jianbin Zhao et al. [120] discovered that prolonged exposure to multi-walled carbon nanotubes (MWCNTs) adversely impacts the growth and development of X. tropicalis and presents a possible reproductive concern. At the same time, MWCNTs in humans may also inhibit progesterone secretion from ovarian granulosa cells, possibly by inhibiting steroid acute regulatory protein expression [121].
4.4. Quantum Dots
Quantum dots exhibit remarkable photostability and high brightness, significantly surpassing other fluorescent dyes. They find application in various immunoassays involving antibodies. Kunal Sarkar et al. [122] reported a pegylated graphene oxide quantum dot (GOQD)-based nanodrug delivery platform. This platform facilitates the sustained release of metformin, potentially because GOQD-PEG can restore glucose uptake and alleviate insulin resistance in an in vitro model of insulin resistance. Additionally, quantum dots can integrate with nanoparticles, producing multisensing effects [123]. Generally, in mammalian systems, quantum dots penetrate cell membranes and regulate substance transport across the cell barrier. This largely transpires via mechanisms like as clathrin-mediated endocytosis, caveolae-mediated endocytosis, and micropinocytosis [125,126,127]. Recent findings reveal that quantum dots can sensitively detect and localize unique markers for ovarian cancer metastasis, enabling precise treatment strategies [128]. A study by Vimal Singh et al. [129] demonstrated the safety and non-toxicity of carbon quantum dots in both mice and cervical cells, supporting their viability for biomedical applications.
4.5. Micelles
Micelles, extensively used molecular assemblies, have drawn considerable attention in contemporary medicine due to their remarkable stability. Polymeric micelles demonstrate reduced drug immunogenicity and prolonged half-life compared to traditional micelles [130]. Co-delivery micelles may enhance chemotherapy efficacy while somewhat mitigating reproductive toxicity and fertility damage [131]. Micellar nanoparticles arise from the self-assembly of surfactants or amphiphilic polymers in aqueous conditions, functioning as targeted drug delivery vehicles. Research by Maryam Nazarian et al. [132] indicated that curcumin and nano-membicellated curcumin (NMC) effectively reduce chlorpyrifos-induced reproductive toxicity, likely by lessening oxidative damage and inflammatory responses. Interestingly, another study indicated that NMC might diminish oocyte quality and impact embryonic development [133]. Notably, a newly developed siRNA nanoparticle, self-assembled micellar inhibitory RNA (SAMiRNA), shows promise in treating androgenetic alopecia linked to hyperandrogenism [134]. Oral insulin, a potential treatment for PCOS patients, encounters low bioavailability due to enzyme instability and malabsorption. Micelles offer great potential as a novel drug delivery method for oral insulin, demonstrating greater sensitivity to glucose levels and rapid responses to glucose fluctuations [135].
5. Targeted Ligands in Nanomaterial-Based Drug Delivery Systems for PCOS
Certain drug delivery carriers mentioned above lack targeting capabilities; thus, it is essential to engineer targeting ligands on the surfaces of these nanocarriers to enhance the nanoparticles' targeting qualities. These targeting ligands can be mainly classified into two categories based on the different receptors recognized by the targeting ligands, including ligands targeting oocytes and granulosa cells.
5.1. Oocyte
The ovarian follicle consists of oocytes encased in somatic cells. It serves as the foundational functional unit of female reproduction [136]. Anovulatory infertility frequently occurs in women with PCOS. High-quality oocytes correlate with effective embryonic development and the likelihood of a successful pregnancy [137]. Follicle development is strictly controlled by pituitary gonadotropins, namely follicle-stimulating hormone (FSH) and luteinizing hormone (LH), as well as intraovarian regulatory elements such as steroids, growth factors, and cytokines [138]. PCOS can negatively impact the ovarian microenvironment. Pro-inflammatory cytokines, including TNFα, IL-1β, and IL-6, disrupt oocyte maturation, while a chronic inflammatory state leads to ongoing oxidative stress in the ovaries, causing negative implications for pregnancy. Recent studies have explored nanomaterial-based drug delivery systems aimed at enhancing oocyte functionality in relation to fertility [133,139,140]. Researchers have employed active agents to modify the surfaces of nanocarriers, such as chitosan [141]. Chitosan, a natural polysaccharide, finds applications across diverse sectors, including pharmaceuticals and medicine [142,143,144,145]. Chitosan nanoparticles (ChNPs) exhibit significant potential as nanocarriers due to their ability to regulate drug release, minimize dosage and side effects, and enhance drug stability, potency, and bioavailability [146]. Bilirubin-grafted chitosan-coated nanoparticles can lower intracellular ROS and Ca2+ levels, effectively safeguarding oocyte quality and facilitating oocyte maturation, all while preserving the fertilization capacity and developmental potential of mature oocytes. Furthermore, reports indicate that the mannose binding site may influence the recognition and fertilization capabilities of oocytes, positioning it as a potential vehicle for targeted drug or molecule delivery to oocytes [147].
5.2. Granulosa Cells
Granulosa cells, together with oocytes, form the follicle within the ovary [148]. These cells proliferate pre-ovulation and are critical for the healthy development of oocytes and the fertilization process that follows [149]. In PCOS patients, excessive androgens can induce metabolic disturbances in granulosa cells, contributing to ovarian dysfunction [148]. Various copper nanoparticles enhance the functionality of ovarian granulosa cells, modulating the secretion of progesterone, testosterone, and estradiol, offering therapeutic benefits for reproductive disorders [150]. Intriguingly, a study involving bovine ovarian granulosa cells revealed that silver nanoparticles may trigger apoptosis and oxidative stress, consequently impairing ovarian cell function and viability [151].
6. Outlook
Polycystic Ovary Syndrome (PCOS) represents the most prevalent condition among infertile women. Nanomaterials show potential to alleviate certain therapeutic constraints related to PCOS. They can prolong the half-life of medications, enhance drug bioavailability, and facilitate targeted delivery to specific cells. This approach may extend the therapeutic window, minimize adverse effects, and improve drug efficacy for PCOS treatment. This review consolidates recent advancements in nanomaterial-based drug delivery systems for PCOS management. We categorize and describe the various nanoparticles employed in PCOS therapy, focusing on natural drug nanoparticles and metallic nanoparticles. Additionally, we outline various nanocarriers relevant to PCOS, such as liposomes, carbon nanotubes, quantum dots, and micelles. Finally, we suggest potential targeting ligands for these nanomaterials.
Currently, research into novel drug delivery systems for PCOS is still nascent, indicating significant opportunities for exploration. Most studies predominantly emphasize the bioavailability and targeting capabilities of nanoparticles, while investigations into nanoparticle toxicity and elimination in the context of PCOS remain scarce, warranting further inquiry. Moreover, comprehensive studies examining the mechanisms and therapeutic impacts of nanoparticles in PCOS are essential for advancing nanomaterial-based drug delivery from laboratory settings to clinical applications. Additionally, further in-depth investigations regarding similar nanoparticle types are needed.
Author Contributions
Writing—original draft preparation, M.S. and L.X.; collecting the literature, Z.L., X.L. and Y.S.; investigation, S.Z., Z.W. and X.Z.; writing—review and editing, D.Q. and R.Z. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Natural Science Foundation of China (82374425, 82160923, 82460974); Applied Basic Research Programs of Science and Technology Commission Foundation of Yunnan Province (202301AS070053); Key Laboratory of Traditional Chinese Medicine for Prevention and Treatment of Neuropsychiatric Diseases, Yunnan Provincial Department of Education; Scientific Research Projects for High-level Talents of Yunnan University of Chinese Medicine (2019YZG01); Young Top-Notch Talent in 10,000 Talent Program of Yunnan Province (YNWR-QNBJ-2019-235); Yunnan Province Innovation Team of Prevention and Treatment for Brain Diseases With Acupuncture and Tuina (202405AS350007); Yunnan Key Laboratory of Dai and Yi Medicines ,Yunnan University of Chinese Medicine (2024SS24007).
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- Xing:, L. : Xu, J.; Wei, Y.; Chen, Y.; Zhuang, H.; Tang, W.; Yu, S.; Zhang, J.; Yin, G.; Wang, R.; et al. Depression in polycystic ovary syndrome: Focusing on pathogenesis and treatment. Front Psychiatry 2022, 13, 1001484. [Google Scholar] [CrossRef]
- Johnson, J.E.; Daley, D.; Tarta, C.; Stanciu, P.I. Risk of endometrial cancer in patients with polycystic ovarian syndrome: A meta-analysis. Oncol Lett 2023, 25, 168. [Google Scholar] [CrossRef] [PubMed]
- Hanna, F.; Wu, P.; Heald, A.; Fryer, A. Diabetes detection in women with gestational diabetes and polycystic ovarian syndrome. Bmj 2023, 382, e071675. [Google Scholar] [CrossRef] [PubMed]
- Mills, G.; Badeghiesh, A.; Suarthana, E.; Baghlaf, H.; Dahan, M.H. Polycystic ovary syndrome as an independent risk factor for gestational diabetes and hypertensive disorders of pregnancy: a population-based study on 9.1 million pregnancies. Hum Reprod 2020, 35, 1666–1674. [Google Scholar] [CrossRef]
- Teede, H.J.; Tay, C.T.; Laven, J.; Dokras, A.; Moran, L.J.; Piltonen, T.T.; Costello, M.F.; Boivin, J.; Redman, L.M.; Boyle, J.A.; et al. Recommendations from the 2023 International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome†. Hum Reprod 2023, 38, 1655–1679. [Google Scholar] [CrossRef] [PubMed]
- Riestenberg, C.; Jagasia, A.; Markovic, D.; Buyalos, R.P.; Azziz, R. Health Care-Related Economic Burden of Polycystic Ovary Syndrome in the United States: Pregnancy-Related and Long-Term Health Consequences. J Clin Endocrinol Metab 2022, 107, 575–585. [Google Scholar] [CrossRef]
- Yadav, S.; Delau, O.; Bonner, A.J.; Markovic, D.; Patterson, W.; Ottey, S.; Buyalos, R.P.; Azziz, R. Direct economic burden of mental health disorders associated with polycystic ovary syndrome: Systematic review and meta-analysis. Elife 2023, 12. [Google Scholar] [CrossRef]
- Melin, J.; Forslund, M.; Alesi, S.; Piltonen, T.; Romualdi, D.; Spritzer, P.M.; Tay, C.T.; Pena, A.; Witchel, S.F.; Mousa, A.; et al. The impact of metformin with or without lifestyle modification versus placebo on polycystic ovary syndrome: a systematic review and meta-analysis of randomized controlled trials. Eur J Endocrinol 2023, 189, S37–s63. [Google Scholar] [CrossRef]
- Fonseka, S.; Wijeyaratne, C.N.; Gawarammana, I.B.; Kalupahana, N.S.; Rosairo, S.; Ratnatunga, N.; Kumarasiri, R. Effectiveness of Low-dose Ethinylestradiol/Cyproterone Acetate and Ethinylestradiol/Desogestrel with and without Metformin on Hirsutism in Polycystic Ovary Syndrome: A Randomized, Double-blind, Triple-dummy Study. J Clin Aesthet Dermatol 2020, 13, 18–23. [Google Scholar]
- Teede, H.J.; Tay, C.T.; Laven, J.; Dokras, A.; Moran, L.J.; Piltonen, T.T.; Costello, M.F.; Boivin, J.; L, M.R.; J, A.B.; et al. Recommendations from the 2023 International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. Fertil Steril 2023, 120, 767–793. [Google Scholar] [CrossRef]
- Diez-Pascual, A.M.; Rahdar, A. Functional Nanomaterials in Biomedicine: Current Uses and Potential Applications. ChemMedChem 2022, 17, e202200142. [Google Scholar] [CrossRef] [PubMed]
- Yan, S.; Gao, Z.; Ding, J.; Chen, S.; Wang, Z.; Jin, W.; Qu, B.; Zhang, Y.; Yang, L.; Guo, D.; et al. Nanocomposites based on nanoceria regulate the immune microenvironment for the treatment of polycystic ovary syndrome. J Nanobiotechnology 2023, 21, 412. [Google Scholar] [CrossRef] [PubMed]
- Siddiqui, S.; Mateen, S.; Ahmad, R.; Moin, S. A brief insight into the etiology, genetics, and immunology of polycystic ovarian syndrome (PCOS). J Assist Reprod Genet 2022, 39, 2439–2473. [Google Scholar] [CrossRef] [PubMed]
- Dumesic, D.A.; Meldrum, D.R.; Katz-Jaffe, M.G.; Krisher, R.L.; Schoolcraft, W.B. Oocyte environment: follicular fluid and cumulus cells are critical for oocyte health. Fertil Steril 2015, 103, 303–316. [Google Scholar] [CrossRef] [PubMed]
- Andrade, V.H.; Mata, A.M.; Borges, R.S.; Costa-Silva, D.R.; Martins, L.M.; Ferreira, P.M.; Cunha-Nunes, L.C.; Silva, B.B. Current aspects of polycystic ovary syndrome: A literature review. Rev Assoc Med Bras (1992) 2016, 62, 867–871. [Google Scholar] [CrossRef]
- Nelson-Degrave, V.L.; Wickenheisser, J.K.; Hendricks, K.L.; Asano, T.; Fujishiro, M.; Legro, R.S.; Kimball, S.R.; Strauss, J.F., 3rd; McAllister, J.M. Alterations in mitogen-activated protein kinase kinase and extracellular regulated kinase signaling in theca cells contribute to excessive androgen production in polycystic ovary syndrome. Mol Endocrinol 2005, 19, 379–390. [Google Scholar] [CrossRef]
- Willis, D.; Mason, H.; Gilling-Smith, C.; Franks, S. Modulation by insulin of follicle-stimulating hormone and luteinizing hormone actions in human granulosa cells of normal and polycystic ovaries. J Clin Endocrinol Metab 1996, 81, 302–309. [Google Scholar] [CrossRef]
- da Silva, B.B.; Lopes-Costa, P.V.; Rosal, M.A.; Pires, C.G.; dos Santos, L.G.; Gontijo, J.A.; Alencar, A.P.; de Jesus Simões, M. Morphological and morphometric analysis of the adrenal cortex of androgenized female rats. Gynecol Obstet Invest 2007, 64, 44–48. [Google Scholar] [CrossRef]
- Chun, S. Relationship between early follicular serum estrone level and other hormonal or ultrasonographic parameters in women with polycystic ovary syndrome. Gynecol Endocrinol 2020, 36, 143–147. [Google Scholar] [CrossRef]
- Kumariya, S.; Ubba, V.; Jha, R.K.; Gayen, J.R. Autophagy in ovary and polycystic ovary syndrome: role, dispute and future perspective. Autophagy 2021, 17, 2706–2733. [Google Scholar] [CrossRef]
- Calcaterra, V.; Verduci, E.; Cena, H.; Magenes, V.C.; Todisco, C.F.; Tenuta, E.; Gregorio, C.; De Giuseppe, R.; Bosetti, A.; Di Profio, E.; et al. Polycystic Ovary Syndrome in Insulin-Resistant Adolescents with Obesity: The Role of Nutrition Therapy and Food Supplements as a Strategy to Protect Fertility. Nutrients 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Sanchez-Garrido, M.A.; Tena-Sempere, M. Metabolic dysfunction in polycystic ovary syndrome: Pathogenic role of androgen excess and potential therapeutic strategies. Mol Metab 2020, 35, 100937. [Google Scholar] [CrossRef] [PubMed]
- McCartney, C.R.; Campbell, R.E.; Marshall, J.C.; Moenter, S.M. The role of gonadotropin-releasing hormone neurons in polycystic ovary syndrome. J Neuroendocrinol 2022, 34, e13093. [Google Scholar] [CrossRef] [PubMed]
- Palomba, S.; Piltonen, T.T.; Giudice, L.C. Endometrial function in women with polycystic ovary syndrome: a comprehensive review. Hum Reprod Update 2021, 27, 584–618. [Google Scholar] [CrossRef]
- Doh, E.; Mbanya, A.; Kemfang-Ngowa, J.D.; Dohbit, S.; Tchana-Sinou, M.; Foumane, P.; Donfack, O.T.; Doh, A.S.; Mbanya, J.C.; Sobngwi, E. The Relationship between Adiposity and Insulin Sensitivity in African Women Living with the Polycystic Ovarian Syndrome: A Clamp Study. Int J Endocrinol 2016, 2016, 9201701. [Google Scholar] [CrossRef]
- Diamanti-Kandarakis, E. Polycystic ovarian syndrome: pathophysiology, molecular aspects and clinical implications. Expert Rev Mol Med 2008, 10, e3. [Google Scholar] [CrossRef]
- Burger, H.G. Androgen production in women. Fertil Steril 2002, 77 Suppl 4, S3–5. [Google Scholar] [CrossRef]
- Tsilchorozidou, T.; Honour, J.W.; Conway, G.S. Altered cortisol metabolism in polycystic ovary syndrome: insulin enhances 5alpha-reduction but not the elevated adrenal steroid production rates. J Clin Endocrinol Metab 2003, 88, 5907–5913. [Google Scholar] [CrossRef]
- Moghetti, P.; Tosi, F.; Bonin, C.; Di Sarra, D.; Fiers, T.; Kaufman, J.M.; Giagulli, V.A.; Signori, C.; Zambotti, F.; Dall'Alda, M.; et al. Divergences in insulin resistance between the different phenotypes of the polycystic ovary syndrome. J Clin Endocrinol Metab 2013, 98, E628–637. [Google Scholar] [CrossRef]
- Armanini, D.; Andrisani, A.; Bordin, L.; Sabbadin, C. Spironolactone in the treatment of polycystic ovary syndrome. Expert Opin Pharmacother 2016, 17, 1713–1715. [Google Scholar] [CrossRef]
- ROOT, H.F. Insulin Resistance and Bronze Diabetes. New England Journal of Medicine 1929, 201, 201–206. [Google Scholar] [CrossRef]
- Moghetti, P.; Tosi, F. Insulin resistance and PCOS: chicken or egg? J Endocrinol Invest 2021, 44, 233–244. [Google Scholar] [CrossRef] [PubMed]
- Dunaif, A. Insulin resistance and the polycystic ovary syndrome: mechanism and implications for pathogenesis. Endocr Rev 1997, 18, 774–800. [Google Scholar] [CrossRef] [PubMed]
- Diamanti-Kandarakis, E.; Dunaif, A. Insulin resistance and the polycystic ovary syndrome revisited: an update on mechanisms and implications. Endocr Rev 2012, 33, 981–1030. [Google Scholar] [CrossRef] [PubMed]
- Nestler, J.E.; Jakubowicz, D.J.; de Vargas, A.F.; Brik, C.; Quintero, N.; Medina, F. Insulin stimulates testosterone biosynthesis by human thecal cells from women with polycystic ovary syndrome by activating its own receptor and using inositolglycan mediators as the signal transduction system. J Clin Endocrinol Metab 1998, 83, 2001–2005. [Google Scholar] [CrossRef] [PubMed]
- Xiong, Y.L.; Liang, X.Y.; Yang, X.; Li, Y.; Wei, L.N. Low-grade chronic inflammation in the peripheral blood and ovaries of women with polycystic ovarian syndrome. Eur J Obstet Gynecol Reprod Biol 2011, 159, 148–150. [Google Scholar] [CrossRef]
- Boulman, N.; Levy, Y.; Leiba, R.; Shachar, S.; Linn, R.; Zinder, O.; Blumenfeld, Z. Increased C-reactive protein levels in the polycystic ovary syndrome: a marker of cardiovascular disease. J Clin Endocrinol Metab 2004, 89, 2160–2165. [Google Scholar] [CrossRef]
- Rudnicka, E.; Kunicki, M.; Suchta, K.; Machura, P.; Grymowicz, M.; Smolarczyk, R. Inflammatory Markers in Women with Polycystic Ovary Syndrome. Biomed Res Int 2020, 2020, 4092470. [Google Scholar] [CrossRef]
- Kelly, C.C.; Lyall, H.; Petrie, J.R.; Gould, G.W.; Connell, J.M.; Sattar, N. Low grade chronic inflammation in women with polycystic ovarian syndrome. J Clin Endocrinol Metab 2001, 86, 2453–2455. [Google Scholar] [CrossRef]
- Awonuga, A.O.; Camp, O.G.; Abu-Soud, H.M. A review of nitric oxide and oxidative stress in typical ovulatory women and in the pathogenesis of ovulatory dysfunction in PCOS. Reprod Biol Endocrinol 2023, 21, 111. [Google Scholar] [CrossRef]
- Immediata, V.; Ronchetti, C.; Spadaro, D.; Cirillo, F.; Levi-Setti, P.E. Oxidative Stress and Human Ovarian Response-From Somatic Ovarian Cells to Oocytes Damage: A Clinical Comprehensive Narrative Review. Antioxidants (Basel) 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Wang, L.Y.; Wang, D.H.; Zou, X.Y.; Xu, C.M. Mitochondrial functions on oocytes and preimplantation embryos. J Zhejiang Univ Sci B 2009, 10, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Shaeib, F.; Khan, S.N.; Ali, I.; Thakur, M.; Saed, M.G.; Dai, J.; Awonuga, A.O.; Banerjee, J.; Abu-Soud, H.M. The Defensive Role of Cumulus Cells Against Reactive Oxygen Species Insult in Metaphase II Mouse Oocytes. Reprod Sci 2016, 23, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Banerjee, J.; Shaeib, F.; Maitra, D.; Saed, G.M.; Dai, J.; Diamond, M.P.; Abu-Soud, H.M. Peroxynitrite affects the cumulus cell defense of metaphase II mouse oocytes leading to disruption of the spindle structure in vitro. Fertil Steril 2013, 100, 578–584. [Google Scholar] [CrossRef]
- González, F.; Rote, N.S.; Minium, J.; Kirwan, J.P. Reactive oxygen species-induced oxidative stress in the development of insulin resistance and hyperandrogenism in polycystic ovary syndrome. J Clin Endocrinol Metab 2006, 91, 336–340. [Google Scholar] [CrossRef]
- Ruegsegger, G.N.; Creo, A.L.; Cortes, T.M.; Dasari, S.; Nair, K.S. Altered mitochondrial function in insulin-deficient and insulin-resistant states. J Clin Invest 2018, 128, 3671–3681. [Google Scholar] [CrossRef]
- Lewis, M.T.; Kasper, J.D.; Bazil, J.N.; Frisbee, J.C.; Wiseman, R.W. Quantification of Mitochondrial Oxidative Phosphorylation in Metabolic Disease: Application to Type 2 Diabetes. Int J Mol Sci 2019, 20. [Google Scholar] [CrossRef]
- Zuo, T.; Zhu, M.; Xu, W. Roles of Oxidative Stress in Polycystic Ovary Syndrome and Cancers. Oxid Med Cell Longev 2016, 2016, 8589318. [Google Scholar] [CrossRef]
- Stein, I.F.; Leventhal, M.L. Amenorrhea associated with bilateral polycystic ovaries. American Journal of Obstetrics and Gynecology 1935, 29, 181–191. [Google Scholar] [CrossRef]
- Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome (PCOS). Hum Reprod 2004, 19, 41–47. [CrossRef]
- Revised 2003 consensus on diagnostic criteria and long-term health risks related to polycystic ovary syndrome. Fertil Steril 2004, 81, 19–25. [CrossRef]
- Teede, H.J.; Misso, M.L.; Costello, M.F.; Dokras, A.; Laven, J.; Moran, L.; Piltonen, T.; Norman, R.J. Recommendations from the international evidence-based guideline for the assessment and management of polycystic ovary syndrome. Hum Reprod 2018, 33, 1602–1618. [Google Scholar] [CrossRef] [PubMed]
- Dapas, M.; Lin, F.T.J.; Nadkarni, G.N.; Sisk, R.; Legro, R.S.; Urbanek, M.; Hayes, M.G.; Dunaif, A. Distinct subtypes of polycystic ovary syndrome with novel genetic associations: An unsupervised, phenotypic clustering analysis. PLoS Med 2020, 17, e1003132. [Google Scholar] [CrossRef] [PubMed]
- Moran, L.J.; Norman, R.J.; Teede, H.J. Metabolic risk in PCOS: phenotype and adiposity impact. Trends Endocrinol Metab 2015, 26, 136–143. [Google Scholar] [CrossRef] [PubMed]
- Yang, R.; Yang, S.; Li, R.; Liu, P.; Qiao, J.; Zhang, Y. Effects of hyperandrogenism on metabolic abnormalities in patients with polycystic ovary syndrome: a meta-analysis. Reprod Biol Endocrinol 2016, 14, 67. [Google Scholar] [CrossRef] [PubMed]
- Wang, R.; Mol, B.W. The Rotterdam criteria for polycystic ovary syndrome: evidence-based criteria? Hum Reprod 2017, 32, 261–264. [Google Scholar] [CrossRef]
- Williams, T.; Mortada, R.; Porter, S. Diagnosis and Treatment of Polycystic Ovary Syndrome. Am Fam Physician 2016, 94, 106–113. [Google Scholar]
- Azziz, R. Polycystic Ovary Syndrome. Obstet Gynecol 2018, 132, 321–336. [Google Scholar] [CrossRef]
- Pereira, K.; Brown, A.J. Secondary amenorrhea: Diagnostic approach and treatment considerations. Nurse Pract 2017, 42, 34–41. [Google Scholar] [CrossRef]
- Neven, A.C.H.; Laven, J.; Teede, H.J.; Boyle, J.A. A Summary on Polycystic Ovary Syndrome: Diagnostic Criteria, Prevalence, Clinical Manifestations, and Management According to the Latest International Guidelines. Semin Reprod Med 2018, 36, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Kyritsi, E.M.; Dimitriadis, G.K.; Kyrou, I.; Kaltsas, G.; Randeva, H.S. PCOS remains a diagnosis of exclusion: a concise review of key endocrinopathies to exclude. Clin Endocrinol (Oxf) 2017, 86, 1–6. [Google Scholar] [CrossRef] [PubMed]
- de-Medeiros, S.F.; Yamamoto, M.M.W.; de-Medeiros, M.A.S.; Barbosa, J.S.; Norman, R.J. Should Subclinical Hypothyroidism Be an Exclusion Criterion for the Diagnosis of Polycystic Ovary Syndrome? J Reprod Infertil 2017, 18, 242–250. [Google Scholar] [PubMed]
- Gibson-Helm, M.; Teede, H.; Dunaif, A.; Dokras, A. Delayed Diagnosis and a Lack of Information Associated With Dissatisfaction in Women With Polycystic Ovary Syndrome. J Clin Endocrinol Metab 2017, 102, 604–612. [Google Scholar] [CrossRef] [PubMed]
- Ehrmann, D.A. Polycystic ovary syndrome. N Engl J Med 2005, 352, 1223–1236. [Google Scholar] [CrossRef] [PubMed]
- Teede, H.J.; Tay, C.T.; Laven, J.J.E.; Dokras, A.; Moran, L.J.; Piltonen, T.T.; Costello, M.F.; Boivin, J.; Redman, L.M.; Boyle, J.A.; et al. Recommendations From the 2023 International Evidence-based Guideline for the Assessment and Management of Polycystic Ovary Syndrome. J Clin Endocrinol Metab 2023, 108, 2447–2469. [Google Scholar] [CrossRef] [PubMed]
- Du, Q.; Yang, S.; Wang, Y.J.; Wu, B.; Zhao, Y.Y.; Fan, B. Effects of thiazolidinediones on polycystic ovary syndrome: a meta-analysis of randomized placebo-controlled trials. Adv Ther 2012, 29, 763–774. [Google Scholar] [CrossRef] [PubMed]
- Baker, S.; Satish, S. Endophytes: toward a vision in synthesis of nanoparticle for future therapeutic agents. Int. J. Bio-Inorg. Hybd. Nanomat 2012, 1, 67–77. [Google Scholar]
- Jaybhaye, S.V. Antimicrobial activity of silver nanoparticles synthesized from waste vegetable fibers. Materials Today: Proceedings 2015, 2, 4323–4327. [Google Scholar] [CrossRef]
- Ndayishimiye, J.; Kumeria, T.; Popat, A.; Falconer, J.R.; Blaskovich, M.A.T. Nanomaterials: The New Antimicrobial Magic Bullet. ACS Infect Dis 2022, 8, 693–712. [Google Scholar] [CrossRef]
- Tang, L.; Zhang, A.; Zhang, Z.; Zhao, Q.; Li, J.; Mei, Y.; Yin, Y.; Wang, W. Multifunctional inorganic nanomaterials for cancer photoimmunotherapy. Cancer Commun (Lond) 2022, 42, 141–163. [Google Scholar] [CrossRef]
- Tang, J.; Ouyang, Q.; Li, Y.; Zhang, P.; Jin, W.; Qu, S.; Yang, F.; He, Z.; Qin, M. Nanomaterials for Delivering Antibiotics in the Therapy of Pneumonia. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef] [PubMed]
- Li, L.; Wang, Z.; Guo, H.; Lin, Q. Nanomaterials: a promising multimodal theranostics platform for thyroid cancer. J Mater Chem B 2023, 11, 7544–7566. [Google Scholar] [CrossRef] [PubMed]
- Chu, W.K.; Cheung, S.C.M.; Lau, R.A.W.; Benzie, I.F.F. Bilberry (Vaccinium myrtillus L.). In Herbal Medicine: Biomolecular and Clinical Aspects, Benzie, I.F.F., Wachtel-Galor, S., Eds.; CRC Press/Taylor & Francis Copyright © 2011 by Taylor and Francis Group, LLC.: Boca Raton (FL), 2011. [Google Scholar]
- Al-Romaiyan, A.; King, A.J.; Persaud, S.J.; Jones, P.M. A novel extract of Gymnema sylvestre improves glucose tolerance in vivo and stimulates insulin secretion and synthesis in vitro. Phytother Res 2013, 27, 1006–1011. [Google Scholar] [CrossRef] [PubMed]
- Arentz, S.; Abbott, J.A.; Smith, C.A.; Bensoussan, A. Herbal medicine for the management of polycystic ovary syndrome (PCOS) and associated oligo/amenorrhoea and hyperandrogenism; a review of the laboratory evidence for effects with corroborative clinical findings. BMC Complement Altern Med 2014, 14, 511. [Google Scholar] [CrossRef]
- Group, T.A.E.A.-S.r.P.C.W. Consensus on women's health aspects of polycystic ovary syndrome (PCOS)†. Human Reproduction 2011, 27, 14–24. [Google Scholar] [CrossRef]
- Tang, T.; Lord, J.M.; Norman, R.J.; Yasmin, E.; Balen, A.H. Insulin-sensitising drugs (metformin, rosiglitazone, pioglitazone, D-chiro-inositol) for women with polycystic ovary syndrome, oligo amenorrhoea and subfertility. Cochrane Database Syst Rev 2010, Cd003053. [Google Scholar] [CrossRef]
- Zeng, L.H.; Rana, S.; Hussain, L.; Asif, M.; Mehmood, M.H.; Imran, I.; Younas, A.; Mahdy, A.; Al-Joufi, F.A.; Abed, S.N. Polycystic Ovary Syndrome: A Disorder of Reproductive Age, Its Pathogenesis, and a Discussion on the Emerging Role of Herbal Remedies. Front Pharmacol 2022, 13, 874914. [Google Scholar] [CrossRef]
- Moini Jazani, A.; Nasimi Doost Azgomi, H.; Nasimi Doost Azgomi, A.; Nasimi Doost Azgomi, R. A comprehensive review of clinical studies with herbal medicine on polycystic ovary syndrome (PCOS). Daru 2019, 27, 863–877. [Google Scholar] [CrossRef]
- Maharjan, R.; Nagar, P.S.; Nampoothiri, L. Effect of Aloe barbadensis Mill. formulation on Letrozole induced polycystic ovarian syndrome rat model. J Ayurveda Integr Med 2010, 1, 273–279. [Google Scholar] [CrossRef]
- Farideh, Z.Z.; Bagher, M.; Ashraf, A.; Akram, A.; Kazem, M. Effects of chamomile extract on biochemical and clinical parameters in a rat model of polycystic ovary syndrome. J Reprod Infertil 2010, 11, 169–174. [Google Scholar]
- Heshmati, J.; Moini, A.; Sepidarkish, M.; Morvaridzadeh, M.; Salehi, M.; Palmowski, A.; Mojtahedi, M.F.; Shidfar, F. Effects of curcumin supplementation on blood glucose, insulin resistance and androgens in patients with polycystic ovary syndrome: A randomized double-blind placebo-controlled clinical trial. Phytomedicine 2021, 80, 153395. [Google Scholar] [CrossRef] [PubMed]
- Zhang, M.; Viennois, E.; Xu, C.; Merlin, D. Plant derived edible nanoparticles as a new therapeutic approach against diseases. Tissue Barriers 2016, 4, e1134415. [Google Scholar] [CrossRef] [PubMed]
- Mu, J.; Zhuang, X.; Wang, Q.; Jiang, H.; Deng, Z.B.; Wang, B.; Zhang, L.; Kakar, S.; Jun, Y.; Miller, D.; et al. Interspecies communication between plant and mouse gut host cells through edible plant derived exosome-like nanoparticles. Mol Nutr Food Res 2014, 58, 1561–1573. [Google Scholar] [CrossRef] [PubMed]
- Wang, Q.; Zhuang, X.; Mu, J.; Deng, Z.B.; Jiang, H.; Zhang, L.; Xiang, X.; Wang, B.; Yan, J.; Miller, D.; et al. Delivery of therapeutic agents by nanoparticles made of grapefruit-derived lipids. Nat Commun 2013, 4, 1867. [Google Scholar] [CrossRef] [PubMed]
- Shen, W.; Qu, Y.; Jiang, H.; Wang, H.; Pan, Y.; Zhang, Y.; Wu, X.; Han, Y.; Zhang, Y. Therapeutic effect and safety of curcumin in women with PCOS: A systematic review and meta-analysis. Front Endocrinol (Lausanne) 2022, 13, 1051111. [Google Scholar] [CrossRef] [PubMed]
- Akter, T.; Zahan, M.S.; Nawal, N.; Rahman, M.H.; Tanjum, T.N.; Arafat, K.I.; Moni, A.; Islam, M.N.; Uddin, M.J. Potentials of curcumin against polycystic ovary syndrome: Pharmacological insights and therapeutic promises. Heliyon 2023, 9, e16957. [Google Scholar] [CrossRef] [PubMed]
- Tiwari, P.M.; Vig, K.; Dennis, V.A.; Singh, S.R. Functionalized Gold Nanoparticles and Their Biomedical Applications. Nanomaterials (Basel) 2011, 1, 31–63. [Google Scholar] [CrossRef]
- Muzzarelli, C.; Stanic, V.; Gobbi, L.; Tosi, G.; Muzzarelli, R.A. Spray-drying of solutions containing chitosan together with polyuronans and characterisation of the microspheres. Carbohydrate Polymers 2004, 57, 73–82. [Google Scholar] [CrossRef]
- Gao, Y.; Xu, Z.; Chen, S.; Gu, W.; Chen, L.; Li, Y. Arginine-chitosan/DNA self-assemble nanoparticles for gene delivery: In vitro characteristics and transfection efficiency. International journal of pharmaceutics 2008, 359, 241–246. [Google Scholar] [CrossRef]
- Jayakumar, R.; Prabaharan, M.; Reis, R.; Mano, J. Graft copolymerized chitosan—present status and applications. Carbohydrate Polymers 2005, 62, 142–158. [Google Scholar] [CrossRef]
- Jayakumar, R.; Nwe, N.; Tokura, S.; Tamura, H. Sulfated chitin and chitosan as novel biomaterials. International journal of biological macromolecules 2007, 40, 175–181. [Google Scholar] [CrossRef] [PubMed]
- Shelma, R.; Sharma, C.P. In vitro and in vivo evaluation of curcumin loaded lauroyl sulphated chitosan for enhancing oral bioavailability. Carbohydrate Polymers 2013, 95, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Cheung, R.C.; Ng, T.B.; Wong, J.H.; Chan, W.Y. Chitosan: An Update on Potential Biomedical and Pharmaceutical Applications. Mar Drugs 2015, 13, 5156–5186. [Google Scholar] [CrossRef] [PubMed]
- Raja, M.A.; Maldonado, M.; Chen, J.; Zhong, Y.; Gu, J. Development and Evaluation of Curcumin Encapsulated Self-assembled Nanoparticles as Potential Remedial Treatment for PCOS in a Female Rat Model. Int J Nanomedicine 2021, 16, 6231–6247. [Google Scholar] [CrossRef] [PubMed]
- Mao, Q.Q.; Xu, X.Y.; Cao, S.Y.; Gan, R.Y.; Corke, H.; Beta, T.; Li, H.B. Bioactive Compounds and Bioactivities of Ginger (Zingiber officinale Roscoe). Foods 2019, 8. [Google Scholar] [CrossRef]
- Kumar, A.; Sundaram, K.; Teng, Y.; Mu, J.; Sriwastva, M.K.; Zhang, L.; Hood, J.L.; Yan, J.; Zhang, X.; Park, J.W.; et al. Ginger nanoparticles mediated induction of Foxa2 prevents high-fat diet-induced insulin resistance. Theranostics 2022, 12, 1388–1403. [Google Scholar] [CrossRef]
- Gu, D.T.; Tung, T.H.; Jiesisibieke, Z.L.; Chien, C.W.; Liu, W.Y. Safety of Cinnamon: An Umbrella Review of Meta-Analyses and Systematic Reviews of Randomized Clinical Trials. Front Pharmacol 2021, 12, 790901. [Google Scholar] [CrossRef]
- Novakovic, S.; Jakovljevic, V.; Jovic, N.; Andric, K.; Milinkovic, M.; Anicic, T.; Pindovic, B.; Kareva, E.N.; Fisenko, V.P.; Dimitrijevic, A.; et al. Exploring the Antioxidative Effects of Ginger and Cinnamon: A Comprehensive Review of Evidence and Molecular Mechanisms Involved in Polycystic Ovary Syndrome (PCOS) and Other Oxidative Stress-Related Disorders. Antioxidants (Basel) 2024, 13. [Google Scholar] [CrossRef]
- Dou, L.; Zheng, Y.; Li, L.; Gui, X.; Chen, Y.; Yu, M.; Guo, Y. The effect of cinnamon on polycystic ovary syndrome in a mouse model. Reprod Biol Endocrinol 2018, 16, 99. [Google Scholar] [CrossRef]
- Borzoei, A.; Rafraf, M.; Asghari-Jafarabadi, M. Cinnamon improves metabolic factors without detectable effects on adiponectin in women with polycystic ovary syndrome. Asia Pac J Clin Nutr 2018, 27, 556–563. [Google Scholar] [CrossRef]
- Kouame, K.; Peter, A.I.; Akang, E.N.; Moodley, R.; Naidu, E.C.; Azu, O.O. Histological and biochemical effects of Cinnamomum cassia nanoparticles in kidneys of diabetic Sprague-Dawley rats. Bosn J Basic Med Sci 2019, 19, 138–145. [Google Scholar] [CrossRef] [PubMed]
- Yahya, R.; Al-Rajhi, A.M.H.; Alzaid, S.Z.; Al Abboud, M.A.; Almuhayawi, M.S.; Al Jaouni, S.K.; Selim, S.; Ismail, K.S.; Abdelghany, T.M. Molecular Docking and Efficacy of Aloe vera Gel Based on Chitosan Nanoparticles against Helicobacter pylori and Its Antioxidant and Anti-Inflammatory Activities. Polymers (Basel) 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Hosen, M.E.; Rahman, M.A.; Rahman, M.S.; Akash, S.; Khalekuzzaman, M.; Alsahli, A.A.; Bourhia, M.; Nafidi, H.A.; Islam, M.A.; Zaman, R. Synthesis of Silver Nanoparticles Using Camellia sinensis Leaf Extract: Promising Particles for the Treatment of Cancer and Diabetes. Chem Biodivers 2024, 21, e202301661. [Google Scholar] [CrossRef] [PubMed]
- Javid-Naderi, M.J.; Mahmoudi, A.; Kesharwani, P.; Jamialahmadi, T.; Sahebkar, A. Recent advances of nanotechnology in the treatment and diagnosis of polycystic ovary syndrome. Journal of Drug Delivery Science and Technology 2023, 79, 104014. [Google Scholar] [CrossRef]
- Alwan, S.H.; Al-Saeed, M.H. Silver Nanoparticles Biofabricated from Cinnamomum zeylanicum Reduce IL-6, IL-18, and TNF-ɑ in Female Rats with Polycystic Ovarian Syndrome. Int J Fertil Steril 2023, 17, 80–84. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Gao, P.; Du, J.; Zhao, X.; Wong, K.K.Y. Long-term anti-inflammatory efficacy in intestinal anastomosis in mice using silver nanoparticle-coated suture. J Pediatr Surg 2017, 52, 2083–2087. [Google Scholar] [CrossRef] [PubMed]
- Girigoswami, A.; Yassine, W.; Sharmiladevi, P.; Haribabu, V.; Girigoswami, K. Camouflaged Nanosilver with Excitation Wavelength Dependent High Quantum Yield for Targeted Theranostic. Sci Rep 2018, 8, 16459. [Google Scholar] [CrossRef] [PubMed]
- Fatemi Abhari, S.M.; Khanbabaei, R.; Hayati Roodbari, N.; Parivar, K.; Yaghmaei, P. Curcumin-loaded super-paramagnetic iron oxide nanoparticle affects on apoptotic factors expression and histological changes in a prepubertal mouse model of polycystic ovary syndrome-induced by dehydroepiandrosterone - A molecular and stereological study. Life Sci 2020, 249, 117515. [Google Scholar] [CrossRef]
- Abdallah, A.B.E.; El-Ghannam, M.A.; Hasan, A.A.; Mohammad, L.G.; Mesalam, N.M.; Alsayed, R.M. Selenium Nanoparticles Modulate Steroidogenesis-Related Genes and Improve Ovarian Functions via Regulating Androgen Receptors Expression in Polycystic Ovary Syndrome Rat Model. Biol Trace Elem Res 2023, 201, 5721–5733. [Google Scholar] [CrossRef]
- Rabah, H.M.; Mohamed, D.A.; Mariah, R.A.; Abd El-Khalik, S.R.; Khattab, H.A.; AbuoHashish, N.A.; Abdelsattar, A.M.; Raslan, M.A.; Farghal, E.E.; Eltokhy, A.K. Novel insights into the synergistic effects of selenium nanoparticles and metformin treatment of letrozole - induced polycystic ovarian syndrome: targeting PI3K/Akt signalling pathway, redox status and mitochondrial dysfunction in ovarian tissue. Redox Rep 2023, 28, 2160569. [Google Scholar] [CrossRef]
- Dymek, M.; Sikora, E. Liposomes as biocompatible and smart delivery systems - the current state. Adv Colloid Interface Sci 2022, 309, 102757. [Google Scholar] [CrossRef] [PubMed]
- Fan, Y.; Marioli, M.; Zhang, K. Analytical characterization of liposomes and other lipid nanoparticles for drug delivery. J Pharm Biomed Anal 2021, 192, 113642. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, D.; Cavaco-Paulo, A.; Nogueira, E. Design of liposomes as drug delivery system for therapeutic applications. Int J Pharm 2021, 601, 120571. [Google Scholar] [CrossRef] [PubMed]
- Józkowiak, M.; Kobylarek, D.; Bryja, A.; Gogola-Mruk, J.; Czajkowski, M.; Skupin-Mrugalska, P.; Kempisty, B.; Spaczyński, R.Z.; Piotrowska-Kempisty, H. Steroidogenic activity of liposomal methylated resveratrol analog 3,4,5,4'-tetramethoxystilbene (DMU-212) in human luteinized granulosa cells in a primary three-dimensional in vitro model. Endocrine 2023, 82, 681–694. [Google Scholar] [CrossRef] [PubMed]
- Prajapati, S.K.; Malaiya, A.; Kesharwani, P.; Soni, D.; Jain, A. Biomedical applications and toxicities of carbon nanotubes. Drug Chem Toxicol 2022, 45, 435–450. [Google Scholar] [CrossRef] [PubMed]
- Park, M.; Sharma, A.; Kang, C.; Han, J.; Tripathi, K.M.; Lee, H.J. N-Doped Carbon Nanorods from Biomass as a Potential Antidiabetic Nanomedicine. ACS Biomater Sci Eng 2022, 8, 2131–2141. [Google Scholar] [CrossRef] [PubMed]
- Sánchez-Tirado, E.; González-Cortés, A.; Yáñez-Sedeño, P.; Pingarrón, J.M. Magnetic multiwalled carbon nanotubes as nanocarrier tags for sensitive determination of fetuin in saliva. Biosens Bioelectron 2018, 113, 88–94. [Google Scholar] [CrossRef]
- Jha, P.K.; Jha, R.K.; Rout, D.; Gnanasekar, S.; Rana, S.V.S.; Hossain, M. Potential targetability of multi-walled carbon nanotube loaded with silver nanoparticles photosynthesized from Ocimum tenuiflorum (tulsi extract) in fertility diagnosis. J Drug Target 2017, 25, 616–625. [Google Scholar] [CrossRef]
- Zhao, J.; Luo, W.; Xu, Y.; Ling, J.; Deng, L. Potential reproductive toxicity of multi-walled carbon nanotubes and their chronic exposure effects on the growth and development of Xenopus tropicalis. Sci Total Environ 2021, 766, 142652. [Google Scholar] [CrossRef]
- Qu, Y.; Yang, B.; Jiang, X.; Ma, X.; Lu, C.; Chen, C. Multiwalled Carbon Nanotubes Inhibit Steroidogenesis by Disrupting Steroidogenic Acute Regulatory Protein Expression and Redox Status. J Nanosci Nanotechnol 2017, 17, 914–925. [Google Scholar] [CrossRef]
- Sarkar, K.; Chatterjee, A.; Bankura, B.; Bank, S.; Paul, N.; Chatterjee, S.; Das, A.; Dutta, K.; Chakraborty, S.; De, S.; et al. Efficacy of pegylated Graphene oxide quantum dots as a nanoconjugate sustained release metformin delivery system in in vitro insulin resistance model. PLoS One 2024, 19, e0307166. [Google Scholar] [CrossRef] [PubMed]
- Bagheri, E.; Ansari, L.; Abnous, K.; Taghdisi, S.M.; Ramezani, P.; Ramezani, M.; Alibolandi, M. Silica-Quantum Dot Nanomaterials as a Versatile Sensing Platform. Crit Rev Anal Chem 2021, 51, 687–708. [Google Scholar] [CrossRef] [PubMed]
- Shan, Y.; Hao, X.; Shang, X.; Cai, M.; Jiang, J.; Tang, Z.; Wang, H. Recording force events of single quantum-dot endocytosis. Chem Commun (Camb) 2011, 47, 3377–3379. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.Y.; Chang, Q.; Sun, Z.X.; Liu, J.; Deng, X.; Liu, Y.; Cao, A.; Wang, H. Fate of CdSe/ZnS quantum dots in cells: Endocytosis, translocation and exocytosis. Colloids Surf B Biointerfaces 2021, 208, 112140. [Google Scholar] [CrossRef] [PubMed]
- Hunt, N.J.; Lockwood, G.P.; Le Couteur, F.H.; McCourt, P.A.G.; Singla, N.; Kang, S.W.S.; Burgess, A.; Kuncic, Z.; Le Couteur, D.G.; Cogger, V.C. Rapid Intestinal Uptake and Targeted Delivery to the Liver Endothelium Using Orally Administered Silver Sulfide Quantum Dots. ACS Nano 2020, 14, 1492–1507. [Google Scholar] [CrossRef] [PubMed]
- Le, N.; Zhang, M.; Kim, K. Quantum Dots and Their Interaction with Biological Systems. Int J Mol Sci 2022, 23. [Google Scholar] [CrossRef] [PubMed]
- Díaz-García, D.; Díaz-Sánchez, M.; Álvarez-Conde, J.; Gómez-Ruiz, S. Emergence of Quantum Dots as Innovative Tools for Early Diagnosis and Advanced Treatment of Breast Cancer. ChemMedChem 2024, 19, e202400172. [Google Scholar] [CrossRef]
- Singh, V.; Kashyap, S.; Yadav, U.; Srivastava, A.; Singh, A.V.; Singh, R.K.; Singh, S.K.; Saxena, P.S. Nitrogen doped carbon quantum dots demonstrate no toxicity under in vitro conditions in a cervical cell line and in vivo in Swiss albino mice. Toxicol Res (Camb) 2019, 8, 395–406. [Google Scholar] [CrossRef] [PubMed]
- Yoshizawa, M.; Catti, L. Aromatic micelles: toward a third-generation of micelles. Proc Jpn Acad Ser B Phys Biol Sci 2023, 99, 29–38. [Google Scholar] [CrossRef]
- Wu, M.; Xue, L.; Guo, Y.; Dong, X.; Chen, Z.; Wei, S.; Yi, X.; Li, Y.; Zhang, J.; Zhou, S.; et al. Microenvironmentally Responsive Chemotherapeutic Prodrugs and CHEK2 Inhibitors Self-Assembled Micelles: Protecting Fertility and Enhancing Chemotherapy. Adv Mater 2023, 35, e2210017. [Google Scholar] [CrossRef]
- Nazarian, M.; Aramjoo, H.; Roshanravan, B.; Samarghandian, S.; Farkhondeh, T. Protective Effects of Curcumin and Nanomicelle Curcumin on Chlorpyrifos-induced Oxidative Damage and Inflammation in the Uterus, Ovary and Brain of Rats. Curr Pharm Biotechnol 2024. [Google Scholar] [CrossRef] [PubMed]
- Roshanfekr Rad, M.; Nejati, V.; Razi, M.; Najafi, G. Nano-micelle Curcumin; A Hazardous and/or Boosting Agent? Relation with Oocyte In-vitro Maturation and Pre-implantation Embryo Development in Rats. Iran J Pharm Res 2020, 19, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Yun, S.I.; Lee, S.K.; Goh, E.A.; Kwon, O.S.; Choi, W.; Kim, J.; Lee, M.S.; Choi, S.J.; Lim, S.S.; Moon, T.K.; et al. Weekly treatment with SAMiRNA targeting the androgen receptor ameliorates androgenetic alopecia. Sci Rep 2022, 12, 1607. [Google Scholar] [CrossRef] [PubMed]
- Yang, H.; Sun, X.; Liu, G.; Ma, R.; Li, Z.; An, Y.; Shi, L. Glucose-responsive complex micelles for self-regulated release of insulin under physiological conditions. Soft Matter 2013, 9, 8589–8599. [Google Scholar] [CrossRef]
- Orisaka, M.; Mizutani, T.; Miyazaki, Y.; Shirafuji, A.; Tamamura, C.; Fujita, M.; Tsuyoshi, H.; Yoshida, Y. Chronic low-grade inflammation and ovarian dysfunction in women with polycystic ovarian syndrome, endometriosis, and aging. Front Endocrinol (Lausanne) 2023, 14, 1324429. [Google Scholar] [CrossRef]
- Da Broi, M.G.; Giorgi, V.S.I.; Wang, F.; Keefe, D.L.; Albertini, D.; Navarro, P.A. Influence of follicular fluid and cumulus cells on oocyte quality: clinical implications. J Assist Reprod Genet 2018, 35, 735–751. [Google Scholar] [CrossRef]
- Orisaka, M.; Miyazaki, Y.; Shirafuji, A.; Tamamura, C.; Tsuyoshi, H.; Tsang, B.K.; Yoshida, Y. The role of pituitary gonadotropins and intraovarian regulators in follicle development: A mini-review. Reprod Med Biol 2021, 20, 169–175. [Google Scholar] [CrossRef]
- El-Naby, A.A.H.; Ibrahim, S.; Hozyen, H.F.; Sosa, A.S.A.; Mahmoud, K.G.M.; Farghali, A.A. Impact of nano-selenium on nuclear maturation and genes expression profile of buffalo oocytes matured in vitro. Mol Biol Rep 2020, 47, 8593–8603. [Google Scholar] [CrossRef]
- Aghaz, F.; Vaisi-Raygani, A.; Khazaei, M.; Arkan, E.; Sajadimajd, S.; Mozafari, H.; Rahimi, Z.; Pourmotabbed, T. Co-encapsulation of tertinoin and resveratrol by solid lipid nanocarrier (SLN) improves mice in vitro matured oocyte/ morula-compact stage embryo development. Theriogenology 2021, 171, 1–13. [Google Scholar] [CrossRef]
- Xi, H.; Huang, L.; Qiu, L.; Li, S.; Yan, Y.; Ding, Y.; Zhu, Y.; Wu, F.; Shi, X.; Zhao, J.; et al. Enhancing oocyte in vitro maturation and quality by melatonin/bilirubin cationic nanoparticles: A promising strategy for assisted reproduction techniques. Int J Pharm X 2024, 8, 100268. [Google Scholar] [CrossRef]
- Pramanik, S.; Sali, V. Connecting the dots in drug delivery: A tour d'horizon of chitosan-based nanocarriers system. Int J Biol Macromol 2021, 169, 103–121. [Google Scholar] [CrossRef] [PubMed]
- Moraru, C.; Mincea, M.M.; Frandes, M.; Timar, B.; Ostafe, V. A Meta-Analysis on Randomised Controlled Clinical Trials Evaluating the Effect of the Dietary Supplement Chitosan on Weight Loss, Lipid Parameters and Blood Pressure. Medicina (Kaunas) 2018, 54. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Gómez, C.P.; Cecilia, J.A. Chitosan: A Natural Biopolymer with a Wide and Varied Range of Applications. Molecules 2020, 25. [Google Scholar] [CrossRef] [PubMed]
- Guzmán, E.; Ortega, F.; Rubio, R.G. Chitosan: A Promising Multifunctional Cosmetic Ingredient for Skin and Hair Care. Cosmetics 2022, 9, 99. [Google Scholar] [CrossRef]
- Jafernik, K.; Ładniak, A.; Blicharska, E.; Czarnek, K.; Ekiert, H.; Wiącek, A.E.; Szopa, A. Chitosan-Based Nanoparticles as Effective Drug Delivery Systems-A review. Molecules 2023, 28. [Google Scholar] [CrossRef] [PubMed]
- Rosano, G.; Caille, A.M.; Gallardo-Ríos, M.; Munuce, M.J. D-Mannose-binding sites are putative sperm determinants of human oocyte recognition and fertilization. Reprod Biomed Online 2007, 15, 182–190. [Google Scholar] [CrossRef] [PubMed]
- Liao, B.; Qi, X.; Yun, C.; Qiao, J.; Pang, Y. Effects of Androgen Excess-Related Metabolic Disturbances on Granulosa Cell Function and Follicular Development. Front Endocrinol (Lausanne) 2022, 13, 815968. [Google Scholar] [CrossRef]
- Zhang, C.H.; Liu, X.Y.; Wang, J. Essential Role of Granulosa Cell Glucose and Lipid Metabolism on Oocytes and the Potential Metabolic Imbalance in Polycystic Ovary Syndrome. Int J Mol Sci 2023, 24. [Google Scholar] [CrossRef]
- Sirotkin, A.V.; Radosová, M.; Tarko, A.; Martín-García, I.; Alonso, F. Effect of morphology and support of copper nanoparticles on basic ovarian granulosa cell functions. Nanotoxicology 2020, 14, 683–695. [Google Scholar] [CrossRef]
- Tabandeh, M.R.; Samie, K.A.; Mobarakeh, E.S.; Khadem, M.D.; Jozaie, S. Silver nanoparticles induce oxidative stress, apoptosis and impaired steroidogenesis in ovarian granulosa cells of cattle. Anim Reprod Sci 2022, 236, 106908. [Google Scholar] [CrossRef]
Figure 1.
Nanomaterials and Targeted Ligands in PCOS Therapy.
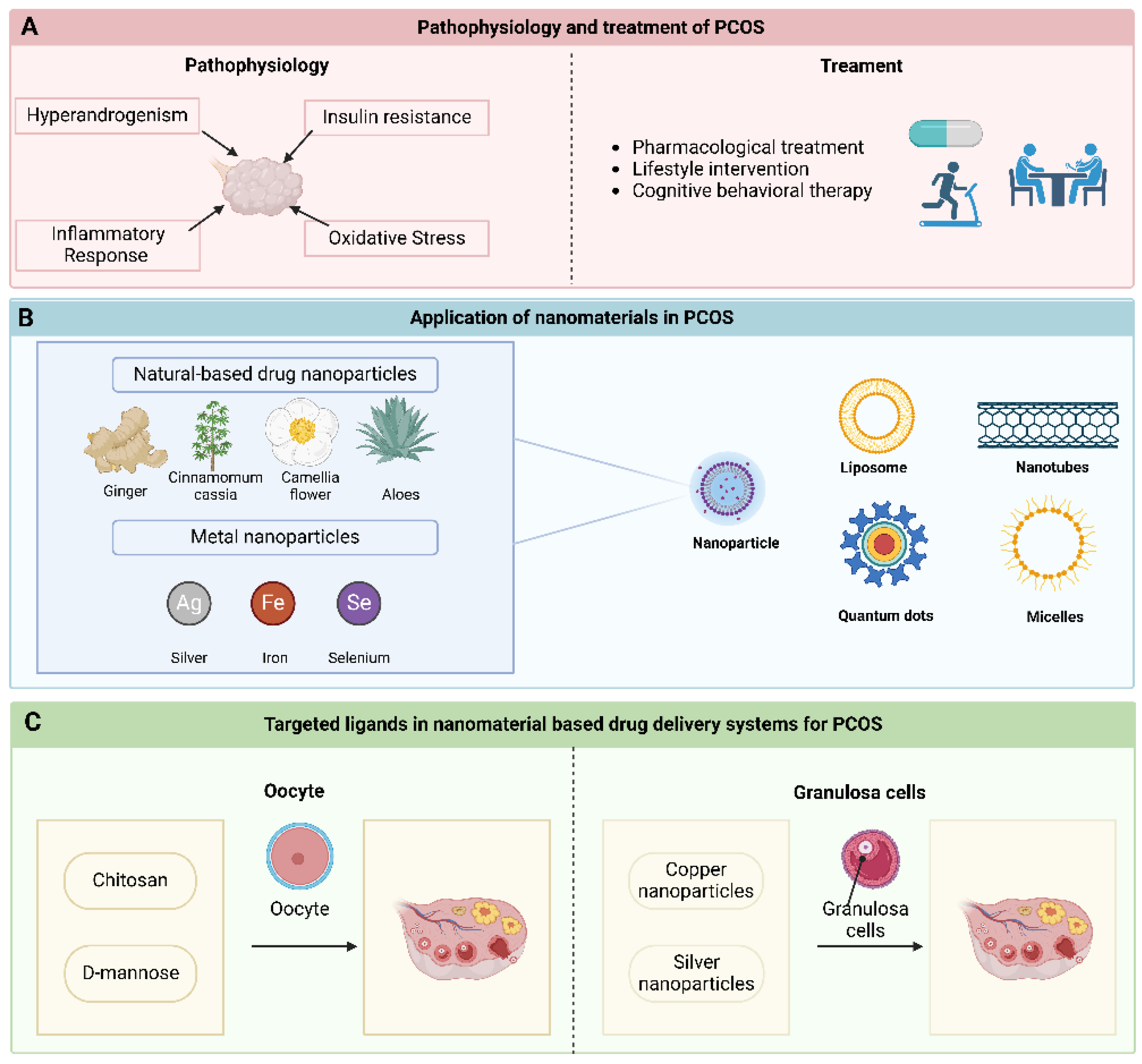

Table 1.
Nanocarriers for PCOS treatment.
| Number | Nanocarrier | Key Ingredient | Therapeutic Agent | Research object | Mechanism | Reference |
|---|---|---|---|---|---|---|
| 1 | Chitosan nanoparticles | Chitosan | Curcumin | Rat | Reduce the levels of serum luteinizing hormone , prolactin, testosterone and insulin | [95] |
| 2 | Ginger nanoparticles | Lipid | Ginger | Mice | Elevated the expression of forkhead transcription factor (Foxa2) to mitigate insulin resistance induced by intestinal epithelial cell (IEC) exosomes. | [97] |
| 3 | Silver nanoparticles | Silver | Cinnamomum cassia | Rat | Antioxidant | [102] |
| 4 | Silver nanoparticles | Silver | Cinnamomum zeylanicum | Rat | Reduce the levels of inflammatory markers such as IL-6, IL-18, and TNF - α | [106] |
| 5 | Iron nanoparticles | Iron oxide | Curcumin | Mice | Inhibition of ovarian injury cell apoptosis and dehydroepiandrosterone induced cell apoptosis | [109] |
| 6 | Selenium nanoparticles | Chitosan | Selenium dioxide | Rat | Reduce androgen synthesis and block the vicious cycle caused by excessive androgen secretion by reducing the expression of androgen receptors | [110] |
| 7 | Selenium nanoparticles | Chitosan | Selenium dioxide | Rat | Upregulation of PI3K and Akt gene expression reduces insulin sensitivity, lipid profile, sex hormone levels, inflammation, oxidative stress, and mitochondrial functional markers | [111] |
| 8 | Liposomes | Glycerol phospholipid | Methoxy derivatives of resveratrol (DMU-212) | Ovarian granulosa cells | Increase the secretion of estradiol and progesterone | [115] |
| 9 | Carbon nanotubes | Silkworm powder | Nitrogen doped carbon nanorods (N-CNR) | Mice | Reduce fasting blood glucose and improve serum biomarker levels associated with oxidative stress and inflammation | [117] |
| 10 | Quantum dot | Polyethylene glycol (PEG) | Metformin | Hepg2 cells | Restore glucose uptake and reverse insulin resistance | [122] |
| 11 | Micelle | / | Curcumin | Rat | Reduced oxidative damage and inflammatory response | [132] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



