
Submitted:
24 October 2024
Posted:
25 October 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Despite the enormous efforts and funds spent to find an effective treatment for COVID-19, the results have been disappointing. In previous publications, we have demonstrated the remarkable effect of high-dose colchicine in inhibiting the cytokine storm and preventing multiorgan damage and death. However, this treatment is beneficial only after virus entry into the cell. The question of prophylaxis and entry prohibition should also be explored. We now demonstrate the prophylactic effect of bromhexine hydrochloride (BRH), an over-the-counter, non-invasive, effective, well-tolerated medicine, with proven safety, affordable, and inexpensive on 125 men and women. The effect of BRH is best when given continuously for prophylaxis during peaks in contagion in the wave of COVID-19. Then the probability of infection drops sharply, and if a disease does occur, it proceeds mildly. BRH is also effective when given by inhalation for post-exposure prophylaxis.When COVID-19 manifests itself clinically, the efficacy of BRH drops sharply because the virus is already in the cell. However, BRH inhalations are useful because they limit the spread of the virus and have an anti-inflammatory and possibly antiviral effect.
Keywords:
COVID-19
; Bromhexine
; TMPRSS2
; Prophylactics
Introduction
The COVID-19 pandemic has caused millions of human casualties and enormous financial damage to humanity. An enormous intellectual and financial resource has been thrown into finding a cure for COVID-19. A Google scholar search with the keyword COVID-19 shows 5 020 000 references, including 4 970 000 articles. The final result regarding the treatment of this disease is deplorable. The World Health Organization (WHO) offers for outpatient treatment three antiviral preparations (Paxlovid, Remdesivir and Molnupiravir) with a rather controversial effect [1,2,3,4].
In a number of articles, we have advocated that the strategy to combat coronavirus disease 2019 (COVID-19) is to block the “Severe acute respiratory syndrome coronavirus 2” (SARS-CoV-2) from entering the cell and to inhibit the hyperactivated nucleotide-binding oligomerization domain-like receptor containing pyrin domain 3 (NLRP3) inflammasome which is a central mediator of severe COVID-19 [5] causing the cytokine storm [CS], with subsequent multiorgan damage and death [3,4,6,7]. NLRP3 inflammasome is involved in COVID-19 respiratory manifestations, cardiovascular comorbidity and neurological symptoms [8].
We therefore also believe that antiviral agents cannot solve the problem, since there is no direct link between viral replication and hyperactivation of the NLRP3 inflammasome. [3,4,5,9,10,11,12,13,14].
Administration of antibodies blocking a given cytokine(s) is also doomed to failure because the cause of the CS, the hyperactivated NLRP3 inflammasome, continues to produce hypercytokinemia [3,4]. In a number of publications, we have demonstrated that blocking the NLRP3 inflammasome is possible with high but, safe doses of colchicine. If given on time, high doses of colchicine solve the CS problem [3,4,6,7,15,16,17,18,19,20].
It is well known that SARS-CoV-2 uses the Angiotensin-converting enzyme-2 (ACE2), which acts as a receptor for the virus S protein for host cell entry [21].
The lungs are the most susceptible organ to SARS-CoV-2 infection, because about 85% of the cells that express ACE2 in the lungs are type 2 alveolar epithelial cells. ACE2 is also present in the throat, heart, kidneys, intestines and other organs [22,23].
The principal SARS-CoV-2 cell entry (via plasma membrane/early endocytosis) is related with the androgen regulated cell-surface transmembrane protease serine subtype 2 (TMPRSS2). TMPRSS2 belongs to the very few trypsin-like proteases expressed in the human respiratory tract. TMPRSS2 plays a role in the proteolytic activation and invasion of the human airway epithelium by influenza A [24,25], it is the major activating protease for influenza B virus [26,27], as well as SARS-CoV and MERS viruses [28].
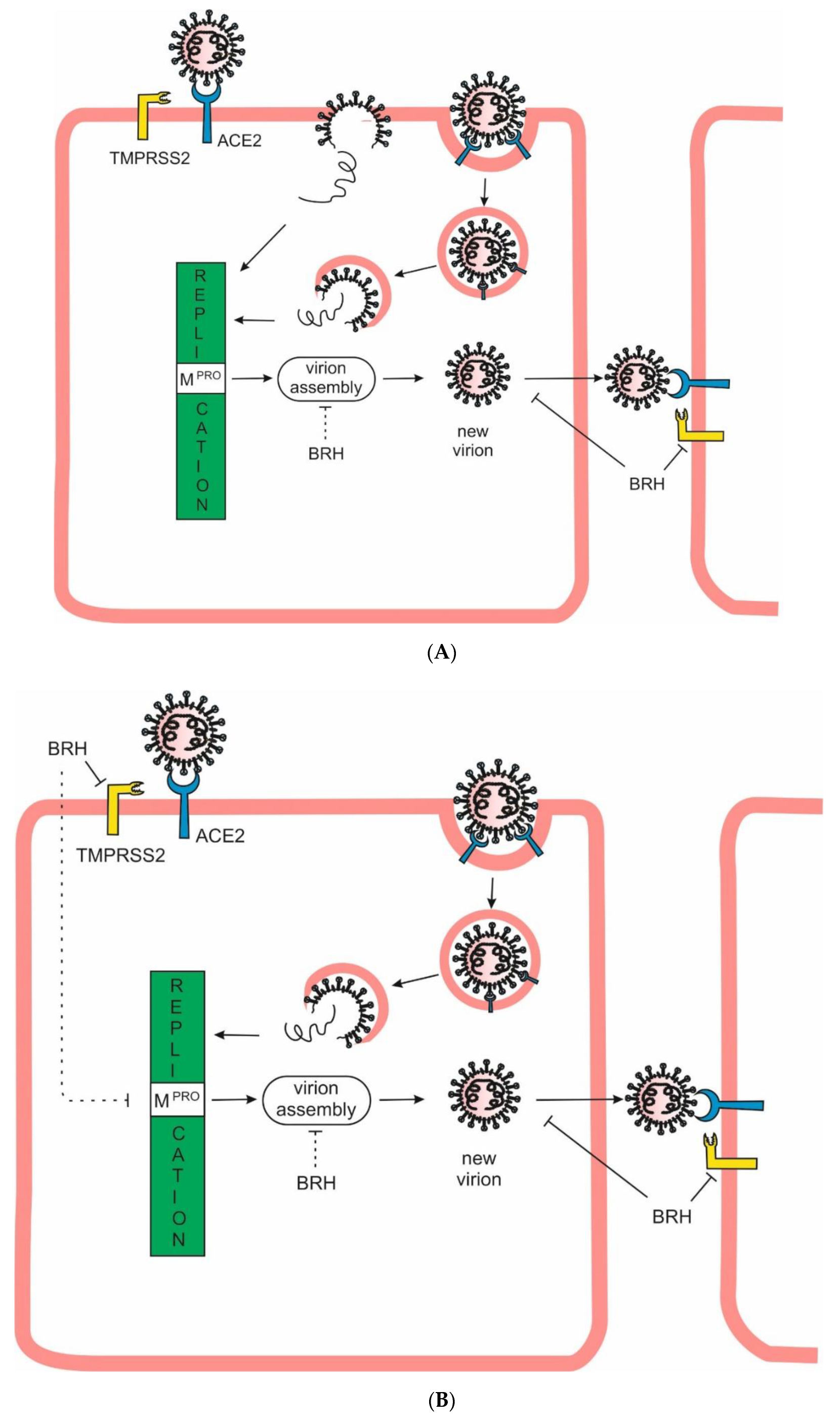
TMPRSS2 cleaves the spike protein leading to the fusion of the viral and host membranes (Entry via plasma membrane/Non-endocytosis/Early endocytosis/Cell surface entry). Binding of SARS-CoV-2 to ACE2, can result in uptake of virions into endosomes (Entry via endosomal pathway/Late endocytosis/Endosomal entry), where the S protein is activated by the pH-dependent cysteine protease cathepsin B/L [29,30,31,32] (Figure 1A). TMPRSS2 could act in both early and late endosome entry processes [21]. TMPRSS2 has been implicated in the regulation of the viral assembly in the Golgi apparatus and the release of the mature virus from the host plasma membrane [33,34,35,36]. TMPRSS2 is also responsible for the viral spread in the infected host. TMPRSS2 contributes to virus spread and immunopathology in the airways of murine models after coronavirus infection [21,28,37].
Figure 1.
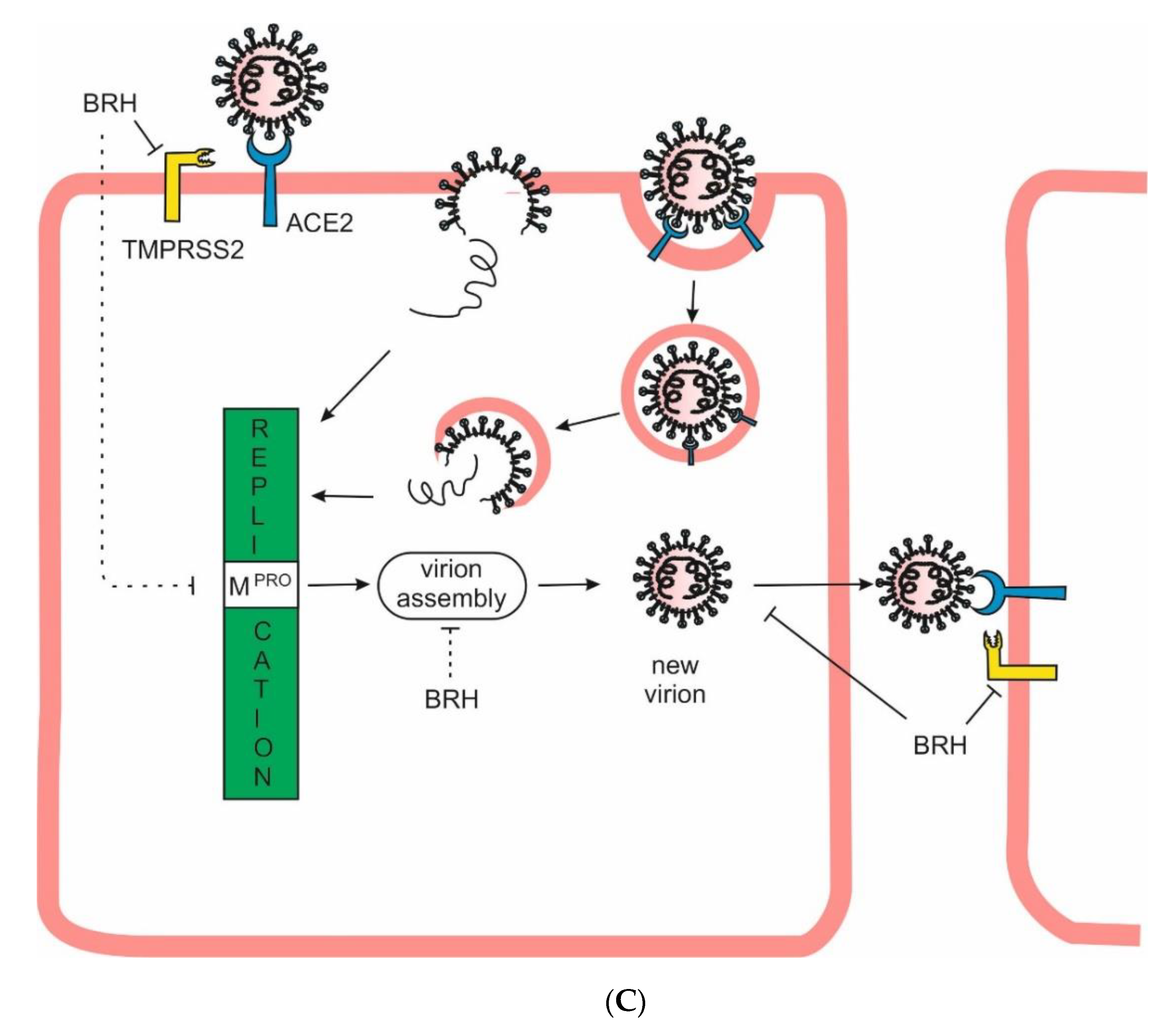
Effect of BRH administered at different time intervals. A The principal SARS-CoV-2 cell entry is related with TMPRSS2 (Entry via plasma membrane). The second way is through receptor-mediated endocytosis (Endosomal entry). B When BRH is taken prophylactically, the main route of viral entry is blocked due to the inhibition of TMPRSS2. BRH could theoretically also affect viral replication by inhibiting Mpro, virion assembly and spread. C When the disease occurs, the virus has already penetrated the cell and the effectiveness of BRH is greatly reduced. However, some positive effect of BRH remains with the blocking of virus spread and its anti-inflammatory and mucolytic properties.
Figure 1.
Effect of BRH administered at different time intervals. A The principal SARS-CoV-2 cell entry is related with TMPRSS2 (Entry via plasma membrane). The second way is through receptor-mediated endocytosis (Endosomal entry). B When BRH is taken prophylactically, the main route of viral entry is blocked due to the inhibition of TMPRSS2. BRH could theoretically also affect viral replication by inhibiting Mpro, virion assembly and spread. C When the disease occurs, the virus has already penetrated the cell and the effectiveness of BRH is greatly reduced. However, some positive effect of BRH remains with the blocking of virus spread and its anti-inflammatory and mucolytic properties.
Other mechanisms of entry have also been described. Despite the existence of alternate receptors (e.g., neuropilin-1, heparin sulfate) and entry mechanisms (antibody-mediated endocytosis, transcytosis of virions to adjacent cells), the distribution of ACE2 and TMPRSS2 are consistent predictors of SARS-CoV-2 tissue tropism [38,39]. Three major cell types co-express TMPRSS2 and ACE2 — type II pneumocytes, ileal absorptive enterocytes and nasal goblet secretory cells/nasal ciliated cells or both [40].
Since 1963 bromhexine hydrochloride (BRH), an over-the-counter, non-invasive, effective, well-tolerated medicine, with proven safety, affordable, available globally and at low costs, has a long history of use in respiratory tract disorders. The mucolytic cough suppressant BRH is known for its effectiveness as an expectorant and mucolytic agent and has been shown to have anti-inflammatory effects, thus reducing swelling and irritation in the respiratory tract [3,41].
BRH is rapidly absorbed from the gastrointestinal tract, however, its first-pass metabolism in the liver is high and bioavailability when taken orally is only 20% [29]. BRH application by inhalation could circumvent the first pass effect. BRH is orally readily bioavailable, and thus, a more frequent and higher oral dose could have a stronger and longer term inactivation of the TMPRSS2 enzyme [29].
The active demethylated metabolite of BRH, ambroxol, is a potent inducer of surfactant synthesis in AT2 cells [42,43]. BRH can prevent influenza infection [44], inhibiting TMPRSS2 [45].
BRH has a selective inhibitory effect on TMPRSS2, thus inhibiting the SARSCoV-2 entry into the cell [21,46]. Other authors suggest that BRH exerts its anti-SARS-CoV-2 activity by inhibition of cathepsin rather than TMPRSS2 [47,48], but in both cases, BRH blocked the entry of SARS-CoV-2 into cells. In addition, BRH demonstrated an antiviral effect by inhibiting the cysteine protease 3Clpro/Mpro, respectively disrupting the viral replication [49,50].
BRH has been effective in controlling SARS-CoV and MERS infections [27].
There is conflicting data about the role of BRH in the prevention and treatment of COVID-19. In sum, there is no convincing evidence for the effect of BRH as a prophylactic treatment for COVID-19 [29,31,41,45,51,52,53,54,55].
In this study, we attempt to demonstrate the potent prophylactic effect of BRH, which preventing the viral penetration into host cells protects against infection with COVID-19 or promotes its mild course.
Aim of the Study
The main purpose of the study was to record the patient reported outcome (covid infections vs no-covid infection), among people, using BRH as a prophylactic agent during the peak waves of contagion between 2021 and 2022.
For context, at the end of 2020, an official announcement by prof. Dr. Vanyo Mitev within the faculty of Medicine, Medical-University of Sofia, supported the use of bromhexine as a way to prohibit SARS-2-COV entry into the cells and prevent infection. This call was reflected in media in 2021 https://www.bgonair.bg/a/36-sutreshen-blok/246992-akad-mitev-lekuvayte-kovid-19-s-bromheksin-i-kolhitsin , with many of the clinics and attending doctors heeding it.
Materials and Methods
This is a retrospective, questionnaire-based study of patient and staff experiences with BRH prophylactic treatment during COVID-19 peaks in contagion in the outbreaks during 2021 and 2022.
Recruitment and Procedure
The study focused on both patients and staff within the clinics of the Medical University of Sofia, Bulgaria between January 2021 and December 2022. Patients attending routine check-ups once yearly, were given instructions for BRH prophylactic use during the pandemic. At attendance, previous exposure to COVID was ascertained, and at the end of 2022, patients were asked to fill-in a questionnaire survey.
For staff, a standard operating procedure (SOP) was distributed on the prophylactic use of BRH when dealing with patients and medical students. In January 2021 staff reported on previous COVID-19 infections, and at the end of 2022 filled-out the same questionnaire as patients.
All subjects were given the same standardized questionnaire where we recorded overall medication intake during COVID-19, specific sections on if and how BRH was applied prophylactically, daily number of tablets, duration of prophylactic use in days. A question asking if the subjects had had a COVID-19 diagnosis confirmed during this time period, and the severity of symptoms. A minimum of 10 days continuous intake of BRH tablets was considered “prophylactic”. Further questions on vaccination status were included, as well as “post-COVID-19” symptoms.
Data on Height, weight, age was also collected, allowing for BMI calculation.
Outcomes
The main outcome of interest was defined as “confirmed subsequent infection with COVID-19”, after BRH addition as a prophylactic agent.
Secondary outcomes included severity of symptoms and “post- COVID-19” symptoms for the subsequent 30 days. A total of 13 post- COVID-19 symptoms were included in the questionnaire:
- Fatigue, or up unexplainable tiredness
- Constant fatigue, despite rest
- Finding it “difficult to breathe”
- Chest discomfort (such as tightness, or as if pricked by a needle)
- Coughing fits
- Increased heart-rate without exertion
- Increased body temperature
- Muscle or joint pain
- Headache
- Impaired cognitive reasoning, function, or concentration abilities
- Difficulty sleeping/lower quality of sleep
- Loss of sense of smell.
- Hair-loss
Statistical Analysis
Both groups were analyzed together as “responders”
Patient responses were recorded and coded into excel for descriptive statistical analysis with MedCalc Statistical Software version 22.0.0 (MedCalc Software bvba, Ostend, Belgium; http://www.medcalc.org; 2024).
Paired samples T-test was used to ascertain differences in COVID-19 infection before and after BRH prophylactic treatment in all patients. Further stratification on infection rate was done for “non-vaccinated” and “vaccinated” individuals. Independent samples t-test was used to analyze the mean secondary infection rate among these individuals.
Patients were subject to further subgroup analysis, based on daily dose and duration of prophylactic treatment: no more than 10 days; no more than 20 days; no more than 30 days; continuous intake for over 30 days. One-way ANOVA was used to analyze subgroups.
Results
Baseline Responder Characteristics
A total of 376 responses were received, with 125 responses of confirmed cases of prophylactic usage of BRH extracted from them them. Mean and median ages for the 125 included responders were 56.46 and 58 years, respectively. Mean BMI of responders was 25.59. Duration of BRH intake varied among responders, as well as daily doses (Table 1). Majority of responders reported taking BRH prophylactically at least 20 to 30 days per year (2021 and 2022), with the mean duration showing 47.52 days, and the median 30 days. Detailed prophylactic regimens available in supplementary table S1. Only 20% of responders reported being vaccinated.
Reported Comorbidities
The number of comorbidities reported was low with a median of 1 comorbidity per patient. 64 (51.2%) responders reported they had no comorbidities, and among the remaining 61 responders, the highest recorded comorbidity was hypertension with 49 counts (Figure 1). Among responders, 35.2% (n = 47) had one comorbidity, 6.4% (n = 8) had 2; 4% (n = 5) had 3 comorbidities, and only 1 patient reported four concomitant comorbidities.
Responders varied greatly in age with the highest number of people observable in the age brackets <40 years and >75 years (Table 2). Elderly patients (defined as patients 65%) showed a higher share of comorbidities, with patients aged 75% having a comorbidity prevalence of 12.8%. Another observable trend is the increase in BMI. The highest recorded BMI was for patients aged 65-69 years, and in general, as age increases, so do the underlying risk-factors such as increased BMI and presence of comorbidities. This confirms that elderly patients are at higher risk of COVID-19 mortality. Despite the low average BMI recorded for the patient population, 23 cases of obesity (defined as a BMI >30) were recorded, corresponding to a prevalence of 18.4%.
COVID-19 Status
At the time of recruitment 63.41% (n = 78) reported a previously confirmed COVID-19 diagnosis. At follow-up and upon BRH inclusion, the percentage with a subsequent infection fell to 11.2% (n = 11). This represents a statistically significant difference of 52.28% in subsequent infection cases (p < 0.0001).
Vaccination coverage was low in the sample with 27 individuals reporting being vaccinated (21.6%). Out of those, 12 responders confirmed they had been vaccinated prior to their first infection (9.6%), with the corresponding 15 responders being vaccinated after their first COVID-19 infection (12%).
Among the entirety of vaccinated individuals, the probability of COVID-19 infection, prior to BRH prophylactic intake was 48.15%, with 13 total cases of COVID-19 out of 27 vaccinated individuals. During the follow-up interview, only 1 patient reported having a secondary infection (3.7%), corresponding to a 44.45% decrease in re-infection likelihood (p = 0.002). It is worth noting that this single patient had a BMI of 42, 3 comorbidities, and had his vaccine after his first COVID-19 infection, thus can be considered a very “high-risk” patient.
Among unvaccinated individuals (n = 98), infection rate prior to BRH infection was reported at 66.32% (n = 65). Upon BRH inclusion, this percentage went down to 13.26% (n=13), representing a statistically significant difference of -53.06% (p < 0.0001) – Table 3.
To differentiate the effect-estimate of antibodies on infection likelihood, two separate groups were further stratified – unvaccinated with a prior infection (n = 65), vs unvaccinated without a prior infection (n = 33). Among the 65 non-vaccinated with possible antibodies, receiving BRH prophylactic treatment, the rate of subsequent re-infection was 13.8% (n = 9). Among the 33 unvaccinated without antibodies, subsequent infection rate was 12.2% (n = 4). The difference was statistically insignificant (p = 0.9248) between the two groups.
Duration of Prophylactic Treatment and Outcomes
One-way ANOVA analysis confirmed that duration of prophylactic treatment is related to improved outcomes and lower re-infection likelihood. Patients taking BRH for more than 30 days had a significantly lower re-infection rate than patients taking it no more than 10 days. As the duration of prophylactic intake of BRH increased, so did the infection likelihood correspondingly fall among these patients. Although no statistical significance was confirmed for the group taking BRH for no longer than 20 days, their reinfection rate was still lower than group 1, and higher than group 3 (difference of -19.04%, and + 10.44%, respectively)
Within the subgroup of 21 patients taking BRH for more than a month, 13 were unvaccinated (with 1 having a prior infection), while 8 had been vaccinated, noting a positive effect, which lacked the sample size to confirm statistically this trend.
Analysis of Secondary Outcomes
Out of all 125 responders, 13 replied they haven’t had post-COVID-19 symptoms, 104 left that part of the questionnaire blank, and only 8 filled-in questionnaires confirmed the presence of post- COVID-19 symptoms (3 male, 5 female). These 8 patients had the following characteristics: Average BMI 25.56, all had been vaccinated prior to their first infection, no infection after initiating BRH therapy, none of them had been hospitalized due to COVID-19 infection, none of them were active or previous smokers, and only 3 had a comorbidity, with that comorbidity being Hypertension for all 3. On average, the number of post- COVID-19 symptoms were 5, however, there didn’t seem to be a discernable connection between the severity of their post- COVID-19 experience and any recognized risk-factors (Supplementary Table S2). All 8 responders had a duration of BRH prophylaxis less than 20 days.
Discussion
Game of Time
While for colchicine the dosage is important – just the right dose [game of dosage], for BRH not the dose, but the of duration of administration is decisive – just the right duration [game of time].
When predicting the effectiveness of BRH the question of when and how it should be applied comes to the forefront. This stems from the fact that the peak of SARS-CoV-2 load is reached before or simultaneously with the onset of symptoms. Thus, when the first symptoms appear, the viral load is already at its maximum [56].
Therefore, even if the treatment with BRH starts from the first day of symptom onset, the virus has already penetrated the cells, significantly reducing the efficacy of BRH, especially if not inhaled [3,6,15].
The second issue of note is what precisely is the optimal duration of prophylactic administration, that can reduce the likelihood of re-infection. In our study, the median duration of BRH intake was 30 days. The one-way ANOVA analysis clearly indicated that increasing the duration of prophylactic intake results in lower re-infection likelihood. A further beneficial effect was observed for vaccinated individuals. Although both sets of individuals – vaccinated and unvaccinated experienced lower reinfection likelihood, the presence of vaccine-induced antibodies seemed to enhance the beneficial effect. Our data indicates that individuals with antibodies, who maintain a minimum of 30 days of intake, have virtually negligent odds of reinfection. These findings are consistent with what is known about the innate immune response and antibody dynamics during COVID-19 infection. Specific antibodies to the S-glycoprotein of SARS-2-COV result only after exposure, where IgM antibodies that form within a week of infection last only 12 weeks, while IgG antibodies last longer [57]. A functioning immune response has also humoral components, whereby even if small viral quantities manage to enter the cells, they are swiftly dealt with. Our study did not account for the number of contacts (i.e., their social activity) these responders have had during the study period; this presents a possible limitation to the study. Other limitation can be outlined in the way the study was conducted. Patient reported outcomes suffer from a high-risk of bias and prone to missing information, as evidenced by the lack of information on post- COVID-19 symptoms. Despite this, it is worth noting that the presence of post- COVID-19 symptoms in our sample did not show any connection to the established risk factors such as – age, sex, presence of comorbidities [63].
Benefits of Prophylaxis with BRH
Нypothesis
BRH is most effective when taken prophylactically, because it blocks in advance the entrance of the SARS-CoV-2 to the cell (Figure 1B). Prevention is best done before the next COVID-19 wave with BRH tablets, for a minimum of 1 month.
Reasoning
Our results demonstrate that when you encounter the virus, there is a high probability that you will not get sick. When the virus has penetrated the cell, the chief concern is what will be the reaction of the NLRP3 inflammasome. Complications can occur only with its hyperreaction, the reasons for which are unknown. In NLRP3 inflammasome hyperreactivity, high doses of colchicine resolve the problem. It is characteristic of our cases that if they get sick, the disease is mild.
Benefits of Post-Exposure Prophylaxis with BRH
Нypothesis
When someone has been in contact with an infected or sick person, BRH inhalations should be started immediately. If the BRH inhalations are undertaken immediately after contact, the probability that the infection not progress is high. The timing and the mode of administration are crucial [3]. The outcome of the competition, whether the virus will enter the cell before BRH is able to block TMPRSS2, will determine whether or not an infected person will become ill.
Reasoning
Benefits of using BRH as post-exposure prophylaxis show that the incidence of symptomatic COVID-19 was significantly lower in individuals who received BRH than in those who received the placebo, with a relative risk reduction of 50%. The hospitalization rate, death, and medication side effects did not vary significantly between the BRH and placebo arms [51]. A lower frequency symptomatic SARS-CoV-2 infection among medical personnel taking BRH (8 mg three times a day) compared to controls was reported [59]. The small sample size was the main limitation of that study, but the trend is true. We are confident that with inhaled BRH the result would have been better.
Benefits of Using BRH as a Remedy
Нypothesis
When the first symptoms of COVID-19 appear, the virus has already entered the cell. As we noted above, the viral load is already at its maximum [56]. This greatly limits the prophylactic effect of BRH. However, as TMPRSS2 is responsible for the viral assembly and spread [21,28,33,34,35,36,37,38] the immediate inhalation of BRH may help limit contamination. A probable effect on viral replication (inhibition of Mpro) is also possible (Figure 1C) [49,50].
In addition, BRH is an effective expectorant and mucolytic agent having anti-inflammatory effects, thus reducing swelling and irritation in the respiratory tract, helping to relieve cough, lassitude, congestion, and dyspnea specific to COVID-19 [41]. These cardinal respiratory symptoms were remarkably less in COVID-19 patients who received BRH treatment than the standard group [31].
All this plus its very low side effects are arguments for using BRH in the treatment regimen for COVID-19. However, it must be strongly emphasized that after the penetration of SARS-CoV-2 into the cell, it is not the replication of the virus that leads to disease aggravation, but the abnormal reaction of the NLRP3 inflammasome.
Results
Several trials have been conducted to determine BRH efficacy, however, its usefulness remains controversial [29,31,41,45,51,52,53,54,55].
In our experience, administration of inhaled BRH is beneficial in both outpatient and inpatient settings [3]. This will be more or less effective, but in no case decisive to avoid possible complications. As we have already noted, only inhibition of the hyperactivated NLRP3 inflammasome can save the patient from CS, multiorgan damage and death. BRH is most effective when given prophylactically over the course of a month during the peak of another COVID-19 wave or by inhalation as post-exposure prophylaxis.
Many hopes were placed on the TMPRSS2 inhibitor Camostat Mesylate (CM), previously used for treatment of pancreatitis and reflux oesophagitis, now for the treatment of COVID-19 [21].
A large number of prestigious clinical trials have been launched to investigate the effectiveness of CM in COVID-19: Denmark (CamoCO-19, NCT04321096), USA (RECOVER, NCT04470544, NCT04353284, NCT04524663, NCT04374019), UK (NCT04455815), Mexico (NCT04530617), Israel (COSTA, NCT04355052), Germany (NCT04338906), South Korea (NCT04521296) and Japan (NCT04451083).
Conclusions
BRH significantly reduces the likelihood of COVD-19 infection, with this effectiveness being more pronounced in individuals with antibodies.
Our study suggests that vaccines and BRH have complementary mechanisms that allow for a higher degree of protection in 2 possible ways: firstly, BRH inhibits viral cell entry, second to that, if the virus still manages to gain entry, patient with S-glycoprotein specific antibodies are able to swiftly deal with the infection before peak cell load.
Based on our experience since 2020, we are convinced that the ideal way to deal with the COVID-19 pandemic is as follows: mass prophylaxis with BRH/ambroxol during another COVID-19 wave; when in contact with a sick or infectious person - immediate inhalations with BRH/ambroxol; in case of illness - high doses of colchicine and inhaled BRH/ambroxol. This will effectively cut hospital admissions and reduce treatment to the outpatient setting.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org.
Acknowledgements
The work was funded by Project BG-RRP-2.004-0004-C01 financed by Bulgarian National Science Fund. The research is financed by the Bulgarian National Plan for Recovery and Resilience.
References
- Morgenstern, J. Paxlovid evidence: Still very little reason to prescribe. First10EM 2024. [Google Scholar] [CrossRef]
- Sax, P. The Rise and Fall of Paxlovid—HIV and ID Observations. NEJM Journal Watch. 2024. Available online: https://blogs.jwatch.org (accessed on 3 June 2024).
- Mitev, V. Comparison of treatment of COVID-19 with inhaled bromhexine, higher doses of colchicine and hymecromone with WHO-recommended paxlovid, molnupiravir, remdesivir, anti-IL-6 receptor antibodies and baricitinib. Pharmacia 2023, 70, 1177–1193. [Google Scholar] [CrossRef]
- Mitev, V. Colchicine—The Divine Medicine against COVID-19. J. Pers. Med. 2024, 14, 756. [Google Scholar] [CrossRef] [PubMed]
- Freeman, T.L.; Swartz, T.H. Targeting the NLRP3 Inflammasome in Severe COVID-19. Front. Immunol 2020, 11, 1518. [Google Scholar] [CrossRef]
- Mitev, V.; Mondeshki, T.; Marinov, K.; Bilukov, R. ; Colchicine, bromhexine, and hymecromone as part of COVID19 treatment - cold, warm, hot. In Current Overview on Disease and Health Research; Khan , BA, Ed.; BP International: London, UK, 2023; Volume 10, pp. 106–13. [Google Scholar]
- Tiholov, R.; Lilov, A.I.; Georgieva, G.; Palaveev, K.R.; Tashkov, K.; Mitev, V. Effect of increasing doses of colchicine on thetreatment of 333 COVID-19 inpatients. Immun Inflamm Dis. 2024, 12, e1273. [Google Scholar] [CrossRef]
- Ni, Z.; Bin, D.; Li-li, X. ; The NLRP3 inflammasome and COVID-19: Activation, pathogenesis and therapeutic strategies. Cytokine Growth Factor Rev. 2021, 61, 2–15. [Google Scholar]
- Fu, L.; Wang, B.; Yuan, T.; Chen, X.; Ao, Y.; Fitzpatrick, T. ; Peiyang, Li.; Yiguo, Z.; Yi-Fan, L.; Qibin, D.; et al. Clinical characteristics of coronavirus disease 2019 (COVID-19) in China: A systematic review and meta-analysis. Journal of Infection 2020, 80, 656–665. [Google Scholar] [CrossRef]
- Fung, S.Y.; Yuen, K.S.; Ye, Z.; Chan, C.P.; Jin, D.Y. A tug-of-war between severe acute respiratory syndrome coronavirus 2 and host antiviral defence: lessons from other pathogenic viruses. Emerging Microbes Infections 2020, 9, 558–570. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersal,l R. S.; Manson, J.J. COVID-19: consider cytokine storm syndromes and immunosuppression. The Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Zhang, C,; Wu, Z.; Li, J.W.; Zhao, H.; Wang, G.Q. Cytokine release syndrome in severe COVID-19: interleukin-6 receptor antagonist tocilizumab may be the key to reduce mortality. Int. J. Antimicrob. Agents 2020, 55, 105954. [Google Scholar] [CrossRef]
- Zhao, M. Cytokine storm and immunomodulatory therapy in COVID-19: role of chloroquine and anti-IL-6 monoclonal antibodies. Int. J. Antimicrob. Agents 2020, 55, 105982. [Google Scholar] [CrossRef] [PubMed]
- Zhao, N.; Di, B.; Xu, L.L. The NLRP3 inflammasome and COVID-19: Activation, pathogenesis and therapeutic strategies. Cytokine Growth Factor Rev. 2021, 61, 2–15. [Google Scholar] [CrossRef]
- Mondeshki, T.; Bilyukov, R.; Tomov, T.; Mihaylov, M.; Mitev, V. Complete, rapid resolution of severe bilateral pneumonia and acute respiratory distress syndrome in a COVID-19 patient: role for a unique therapeutic combination of inhalations with bromhexine, higher doses of colchicine, and hymecromone. Cureus 2022, 14, e30269. [Google Scholar] [CrossRef] [PubMed]
- Mondeshki, T.; Bilyukov, R.; Mitev, V. Effect of an Accidental Colchicine Overdose in a COVID-19 Inpatient With Bilateral Pneumonia and Pericardial Effusion. Cureus 2023, 15, e35909. [Google Scholar] [CrossRef] [PubMed]
- Mitev, V. What is the lowest lethal dose of colchicine? Biotechnol. Biotechnol. Equip.. 2023, 37, 2288240. [Google Scholar] [CrossRef]
- Lilov, A.; Palaveev, K.; Mitev, V. High Doses of Colchicine Act As “Silver Bullets” Against Severe COVID-19. Cureus 2024, 16, e54441. [Google Scholar] [CrossRef]
- Mondeshki, T.; Mitev, V. High-Dose Colchicine: Key Factor in the Treatment of Morbidly Obese COVID-19 Patients. Cureus 2024, 16, e58164. [Google Scholar] [CrossRef]
- Bulanov, D.; Yonkov, A.; Arabadzhieva, E.; Mitev, V. Successful Treatment With High-Dose Colchicine of a 101-Year-Old Patient Diagnosed With COVID-19 After an Emergency Cholecystectomy. Cureus 2024, 16, e63201. [Google Scholar] [CrossRef]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Krüger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell 2020, 181, 271–280. [Google Scholar] [CrossRef]
- Zhang, H.; Penninger, J.M.; Li, Y.; Zhong, N.; Slutsky, A.S. Angio-tensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 receptor: molecular mechanisms and potential therapeutic target. Intensive Care Med. 2020, 46, 586–90. [Google Scholar] [CrossRef]
- Gheblawi, M.; Wang, K.; Viveiros, A.; Nguyen, Q.; Zhong, J.C.; Turner, A.J. ; Raizada, M, K,; Grant, M.B.; Oudit, G.Y. Angiotensin-converting enzyme 2: SARS-CoV-2 receptor and regulator of the renin-angiotensin system: Celebrating the 20th anniversary of the discovery of ACE2. Circ. Res 2020, 126, 1456–74. [Google Scholar] [CrossRef] [PubMed]
- Böttcher, E.; Matrosovich, T.; Beyerle, M. ; Klenk, H-D.; Garten, W.; Matrosovich, M.. Proteolytic activation of influenza viruses by serine proteases TMPRSS2 and HAT from human airway epithelium. J Virol 2006, 80, 9896–9898. [Google Scholar] [CrossRef] [PubMed]
- Sakai, K.; Ami, Y.; Nakajima, N.; Nakajima, K.; Kitazawa, M.; Anraku, M.; Takayama, I.; Sangsriratanakul, N.; Komura, M.; Sato, Y.; et al. TMPRSS2 independency for haemagglutinin cleavage in vivo differentiates influenza B virus from influenza A virus. Sci Rep 2016, 6, 29430. [Google Scholar] [CrossRef] [PubMed]
- Limburg, H.; Harbig, A.; Bestle, D.; Stein, D. A.; Moulton, H. M.; Jaeger, J.; Janga, H.; Hardes, K.; Koepke, J. Schulte, L. TMPRSS2 is the major activating protease of influenza A virus in primary human airway cells and influenza B virus in human type II pneumocytes. J Virol. 2019, 93, e00649–19. [Google Scholar] [CrossRef] [PubMed]
- Shen, L. W.; Mao, H. J.; Wu, Y. L.; Tanaka, Y.; Zhang, W. TMPRSS2: A potential target for treatment of influenza virus and coronavirus infections. Biochimie 2017, 142, 1–10. [Google Scholar] [CrossRef]
- Iwata-Yoshikawa, N.; Okamura, T.; Shimizu, Y.; Hasegawa, H.; Takeda, M.; Nagata, N. TMPRSS2 contributes to virus spread and immunopathology in the airways of murine models after coronavirus infection. J Vvirol, 2019, 93, 10–1128. [Google Scholar] [CrossRef]
- Depfenhart, M.; De Villiers, D.; Lemperle, G.; Meyer, M.; Di Somma, S. Potential new treatment strategies for COVID-19: is there a role for bromhexine as add-on therapy? Intern Emerg Med 2020, 15, 801–812. [Google Scholar] [CrossRef]
- V’kovski, P.; Kratzel, A.; Steiner, S.; Stalder, H.; Thiel, V. Coronavirus biology and replication: implications for SARS-CoV-2. Nat Rev Microbiol 2021, 19, 155–170. [Google Scholar] [CrossRef]
- Ansarin, K.; Tolouian, R.; Ardalan, M.; Taghizadieh, A.; Varshochi, M.; Teimouri, S.; Vaezi, T.; Valizadeh, H.; Saleh, P.; Safiri, S. Effect of bromhexine on clinical outcomes and mortality in COVID-19 patients: A randomized clinical trial. BioImpacts 2020, 10, 209–215. [Google Scholar] [CrossRef]
- Zhao, M M.; Yang, WL.; Yang, F.Y.; Zhang, L.; Huang, W-J,; Hou, W.; Fan, C-F.; Jin, R-H.; Feng, Y-M.; Wang Y-C.; et al. Cathepsin L plays a key role in SARS-CoV-2 infection in humans and humanized mice and is a promising target for new drug development. Signal Transduct Target Ther 2021, 6, 134. [CrossRef]
- Ou, X.; Liu, Y.; Lei, X.; Li, P.; Mi, D.; Ren, L.; Guo, L. , Guo, R.; Chen, T.; Hu, J.; et al. Characterization of spike glycoprotein of SARS-CoV-2 on virus entry and its immune cross-reactivity with SARS-CoV. Nat Commun 2020, 11, 1620. [Google Scholar] [CrossRef] [PubMed]
- Shen, L.W.; Mao, H.J.; Wu, Y.L.; Tanaka, Y.; Zhang, W. TMPRSS2: A potential target for treatment of influenza virus and coronavirus infections. Biochimie 2017, 142, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Maggio, R.; Corsini, G.U. Repurposing the mucolytic cough suppressant and TMPRSS2 protease inhibitor bromhexine for the prevention and management of SARS-CoV-2 infection. Pharmacol. Res. 2020, 157, 104837. [Google Scholar] [CrossRef]
- Markus, D.; Gottfried, L.; Markus, M.; Marina, R.; Dario, B.; Danielle de, V. A SARS-CoV-2 prophylactic and treatment; A counter argument against the sole use of chloroquine. Am J Biomed Sci. 2020, 248–351. [Google Scholar]
- Shirato, K.; Kawase, M.; Matsuyama, S. Wild-type human coronaviruses prefer cell-surface TMPRSS2 to endosomal cathepsins for cell entry. Virology 2018, 517, 9–15. [Google Scholar] [CrossRef] [PubMed]
- Zhou, Y.; Vedantham, P.; Lu, K.; Agudelo, J.; Carrion, R.; Nunneley, J.W.; Barnard, D.; Pöhlmann, S.; McKerrow, J.H.; Renslo, A.R.; et al. Protease inhibitors targeting coronavirus and filovirus entry. Antiviral Res. 2015, 116, 76–84. [Google Scholar] [CrossRef]
- Atyeo, N.; Perez, P.; Matuck, B.; Byrd, K.M.; Warner, B.M. The Mouth as a Site of SARS-CoV-2 Infection. Curr Oral Health Rep 2024, 11, 167–176. [Google Scholar] [CrossRef]
- Jackson, C.B.; Farzan, M.; Chen, B.; Choe, H. Mechanisms of SARS-CoV-2 entry into cells. Nat Rev Mol Cell Biol 2022, 23, 3–20. [Google Scholar] [CrossRef]
- Ghayour, A.E.; Nazari, S.; Keramat, F.; Shahbazi, F.; Eslami-Ghayour, A. Evaluation of the efficacy of N-acetylcysteine and bromhexine compared with standard care in preventing hospitalization of outpatients with COVID-19: a double blind randomized clinical trial. Rev Clín Esp. (English Edition). 2024, 224, 86–95. [Google Scholar]
- Han, S.; Mallampalli, R. K. The role of surfactant in lung disease and host defense against pulmonary infections. Annals of the American Thoracic Society 2015, 12, 765–774. [Google Scholar] [CrossRef]
- Plomer, M.; de Zeeuw, J. More than expectorant: new scientific data on ambroxol in the context of the treatment of bronchopulmonary diseases. MMW-Fortschritte der Medizin 2017, 159, 22–33. [Google Scholar] [CrossRef] [PubMed]
- Garten, W.; Braden, C.; Arendt, A.; Peitsch, C.; Baron, J.; Lu, Y.; Pawletko, K.; Hardes, K.; Steinmetzer, T.; Böttcher-Friebertshäuser, E. Influenza virus activating host proteases: Identification, localization and inhibitors as potential therapeutics. Eur J Cell Biol. 2015, 94, 375–83. [Google Scholar] [CrossRef] [PubMed]
- Fu, Q.; Zheng, X.; Zhou, Y.; Tang, L.; Chen, Z.; Ni, S. Re-recognizing bromhexine hydrochloride: pharmaceutical properties and its possible role in treating pediatric COVID-19. Eur J Clin Pharmacol. 2021, 77, 77,261–263. [Google Scholar] [CrossRef] [PubMed]
- Lucas, J.M.; Heinlein, C.; Kim, T.; Hernandez, S.A.; Malik, M.S.; True, L.D.; Morrissey, C.; Corey, E.; Montgomery, B.; Mostaghel, E.; et al. The androgen-regulated protease TMPRSS2 activates a proteolytic cascade involving components of the tumor microen-vironment and promotes prostate cancer metastasis. Cancer Discovery 2014, 4, 1310–1325. [Google Scholar] [CrossRef]
- Lee, J.; Lee, J.A.; Kim, H. J.; Ko, M.; Jee, Y.; Kim, S. TMPRSS2 and RNA-dependent RNA polymerase are effective targets of therapeutic intervention for treatment of COVID-19 caused by SARS-CoV-2 variants (B. 1.1. 7 and B. 1.351). Microbiol Spectr. 2021, 9, e0047221. [Google Scholar] [CrossRef]
- Wettstein, L.; Kirchhoff, F.; Münch, J. The Transmembrane Protease TMPRSS2 as a Therapeutic Target for COVID-19 Treatment. Int. J. Mol. Sci. 2022, 23, 1351. [Google Scholar] [CrossRef]
- Bahadoram, S.; Keikhaei, B.; Bahadoram, M.; Mahmoudian-Sani, R.; Hassanzadeh, S.; Saeedi-Boroujeni, A.; Alikhani, K. Bromhexine is a potential drug for COVID-19; From hypothesis to clinical trials. Vopr Virusol 2022, 67, 126–132. [Google Scholar] [CrossRef]
- Huynh, T.; Wang, H.; Luan, B. In silico exploration of the molecular mechanism of clinically oriented drugs for possibly inhibiting SARS-CoV-2’s main protease. J. Phys. Chem. Lett. 2020, 11, 4413–4420. [Google Scholar] [CrossRef]
- Tolouian ,R.; Moradi, O.; Mulla, Z.D.; Ziaie, S.; Haghighi, M.; Esmaily, H.; Amini, H.; Hassanpour, R.; Poorheidar, E.; Kouchek, M.; et al. Bromhexine for post-exposure COVID-19 prophylaxis: A randomized, double-blind, placebo-controlled trial. Jundishapur J. Microbiol 2022, 15, e130198. [Google Scholar]
- Tolouian, R.; Mulla, Z.D. Controversy with bromhexine in COVID-19; where we stand. Immunopathologia Persa 2021, 7, e12. [Google Scholar] [CrossRef]
- Tolouian, R.; Mulla, Z.D.; Jamaati, H.; Babamahmoodi, A.; Marjani, M.; Eskandari, R.; Dastan, F.J. Effect of bromhexine in hospitalized patients with COVID-19. JIM 2021, 71, 691–699. [Google Scholar] [CrossRef] [PubMed]
- Méndez, M.L.; Antón Sanz, C.; Cárdenas García, A.D.R.; Bravo Malo, A.; Torres Martínez, F.J.; Martín Moros, J.M.; Real Torrijos, M.; Vendrell Covisa, J.F.J.; Guzmán Sierra, O.; Molina Barcena, V.; et al. Efficacy of bromhexine versus standard of care in reducing viral load in patients with mild-to-moderate COVID-19 disease attended in primary care: A randomized open-label trial. J Clin Med. 2022, 12, 142. [Google Scholar] [CrossRef]
- Cuerdo, A.R.M.; Ogbac, M.K.; Tamayo, J.E. Effect of Bromhexine among COVID-19 Patients - A Meta-Anaylsis. ERJ Open Res. 2022, 8, 104. [Google Scholar]
- He, X.; Lau, E. H.; Wu, P.; Deng, X.; Wang, J.; Hao, X. . & Leung, G. M. Temporal dynamics in viral shedding and transmissibility of COVID-19. Nature medicine 2020, 26, 672–675. [Google Scholar]
- Boechat JL, Chora I, Morais A, Delgado L. The immune response to SARS-CoV-2 and COVID-19 immunopathology - Current perspectives. Pulmonology. 2021, 27, 423–437.
- Mikhaylov, E.N.; Lyubimtseva, T.A.; Vakhrushev, A.D.; Stepanov, D.; Lebedev, D.S.; Vasilieva, E.Y.; . Konradi, A.O.; Shlyakhto, E. V. Bromhexine hydrochloride prophylaxis of COVID-19 for medical personnel: A randomized open-label study. Interdiscip Perspect Infect Dis. 2022, 4693121. [Google Scholar] [CrossRef]
- Tobback, E.; Degroote, S.; Buysse, S.; Delesie, L.; Van Dooren, L.; Vanherrewege, S.; Barbezange, C.; Hutse, V. ; Romano, M,.;Thomas, I.; et a;. Efficacy and safety of camostat mesylate in early COVID-19 disease in an ambulatory setting: a randomized placebo-controlled phase II trial. Int J Infect Dis 2022, 122, 628–635. [Google Scholar] [CrossRef]
- Khan, U.; Mubariz, M.; Khlidj, Y.; Nasirk M., M.; Ramadan, S.; Saeed, F.; Muhammad, A.; Abuelazm, M. Safety and Efficacy of Camostat Mesylate for Covid-19: a systematic review and Meta-analysis of Randomized controlled trials. BMC Infect Dis 2024, 24, 709. [Google Scholar] [CrossRef]
- Kinoshita, T.; Shinoda, M.; Nishizaki, Y.; Shiraki, K.; Hirai, Y.; Kichikawa, Y.; Tsushima, K.; Shinkai, M.; Komura, N.; Yoshida, K.; et al. A multicenter, double-blind, randomized, parallel-group, placebo-controlled study to evaluate the efficacy and safety of camostat mesilate in patients with COVID-19 (CANDLE study). BMC Med 2022, 20, 342. [Google Scholar]
- Chupp, G.; Spichler-Moffarah, A.; Søgaard, O.S.; Esserman, D.; Dziura, J.; Danzig, L.; Chaurasia, R.; Patra, K.P.; Salovey, A.; Nunez, A.; et al. Placebo-controlled Trial of Oral Camostat Mesylate for Early Treatment of COVID-19 Outpatients Showed Shorter Illness Course and Attenuation of Loss of Smell and Taste. medRxiv 01.28.22270035. 2022. [Google Scholar]
- Tsampasian V, Elghazaly H, Chattopadhyay R, et al. Risk Factors Associated With Post−COVID-19 Condition: A Systematic Review and Meta-analysis. JAMA Intern Med. 2023, 183, 566–580. [Google Scholar] [CrossRef]
Figure 1.
Recorded cases of comorbidities.
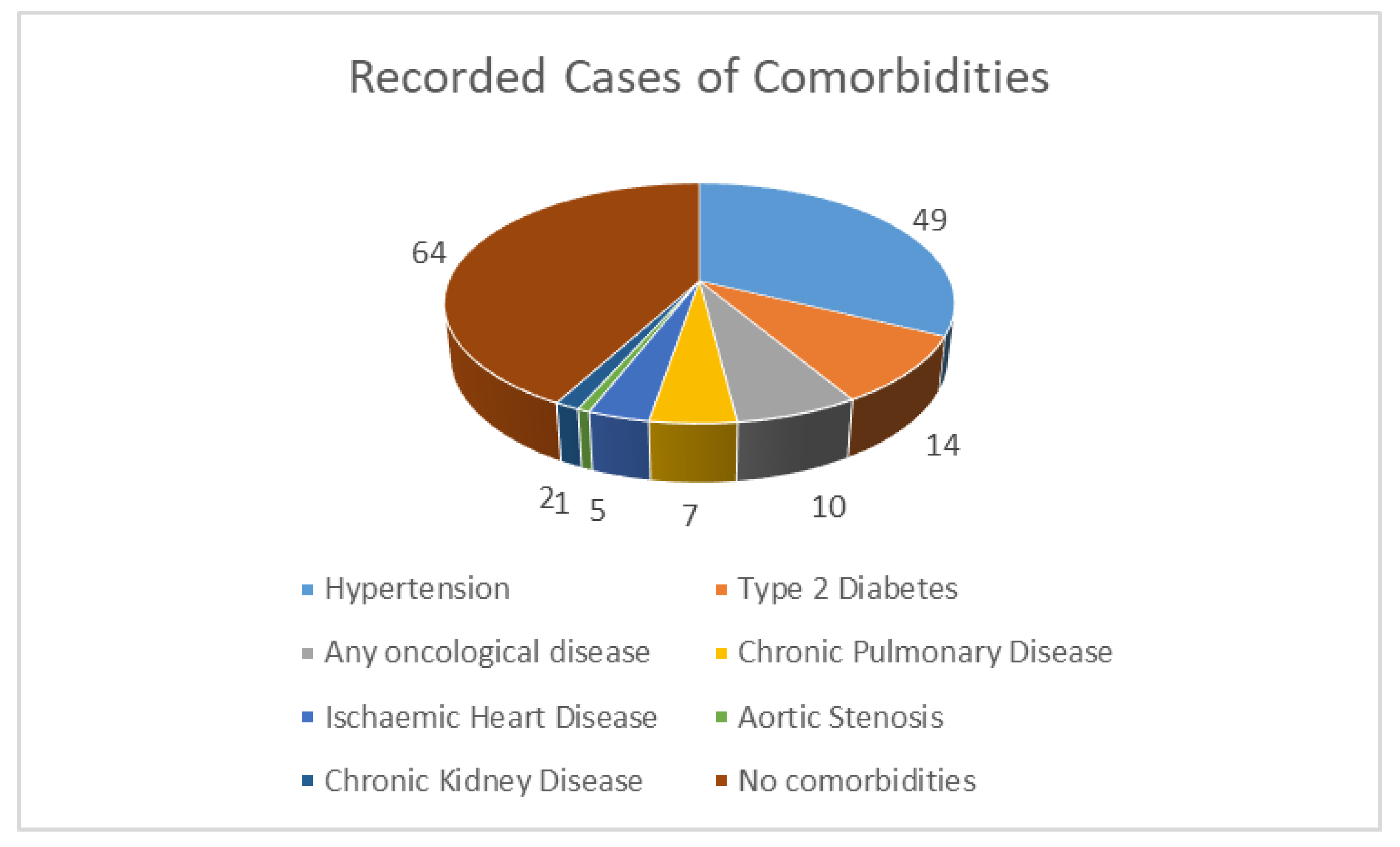

Table 1.
Baseline characteristics of patients.
| Mean (95% CI) | Median | Lowest | Highest | |
|---|---|---|---|---|
| Age | 56.46 years (53.23-59.69) | 58 years | 16 years | 98 years |
| BMI | 25.59 (24.53-26.64) | 24.25 | 14.52 | 45.91 |
| Number of Comorbidities | 1.33 (1.15-1.52) | 1 | 1 | 4 |
| Duration of bromehexine intake | 47.51 days (38.04-56.99) | 30 days | 10 days | 365 days |
| Daily bromhexine intake | 41.15 mg (37.82-44.48) | 48 mg | 8 mg | 128 mg. |
| Vaccination rate | 20% | |||
Table 2.
Age distribution among responders.
| Age group | Number | Average BMI | Number who reported comorbidities | % in group with comorbidity (% from total) |
|---|---|---|---|---|
| < 40 | 24 people | 21.96 | 5 people | 20.83% (4%) |
| 40 – 44 | 7 people | 21.37 | 1 person | 14.28% (0.8%) |
| 45 – 49 | 9 people | 25.17 | 1 person | 11.11% (0.8%) |
| 50 – 54 | 16 people | 26.46 | 7 people | 43.75% (5.6%) |
| 55 – 59 | 9 people | 27.89 | 7 people | 77.77% (5.6%) |
| 60 – 64 | 11 people | 24.94 | 4 people | 36.36% (3.2%) |
| 65 – 69 | 15 people | 29.39 | 8 people | 53.33% (6.4%) |
| 70 – 74 | 11 people | 26.33 | 8 people | 72.72% (6.4%) |
| 75 + | 23 people | 26.14 | 16 people | 69.56% (12.8%) |
| Total | 125 people | 25.59 | 57 people | 45.6 % |
Table 3.
Infection percentages among vaccinated and unvaccinated responders.
| Infection % prior to BRH | Infection % after BRH inclusion | |
| Vaccinated (n = 27) | 48.15% (n = 13) | 3.7% (n = 1) |
| Unvaccinated (n = 98) | 66.32% (n = 65) | 13.26% (n = 13) |
| Overall (n = 125) | 62.4% (n = 78) | 11.2% (n =14) |
Table 4.
ANOVA analysis of reinfection likelihood, stratified by duration of prophylactic treatment.
Table 4.
ANOVA analysis of reinfection likelihood, stratified by duration of prophylactic treatment.
| Factor | N | Mean reinfection rate | SD | Different (p < 0.05) than factor | |
| 1. | No more than 10 days | 18 | 0.3333 (33.33%) | 0.4851 | 3, 4 |
| 2. | No more than 20 days | 42 | 0.1429 (14.29%) | 0.3542 | - |
| 3. | No more than 30 days | 26 | 0.03846 (3.84%) | 0.1961 | 1 |
| 4. | 30 days or more | 39 | 0.02564 (2.56%) | 0.1601 | 1 |
| F- ratio | 4.927 | ||||
| Significance level | P = 0.003 | ||||
| Levene Statistic | 20.202 | ||||
| Significance | P < 0.001 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



