
Submitted:
24 October 2024
Posted:
25 October 2024
Read the latest preprint version here
Abstract
In this study we summarized our work on various aspects of colorectal adenocarcinomas, 1
focusing on tumor distribution (left- sided, right- sided, and rectal cancers), histologycal type, patient 2
age, gender and several factors affecting prognosis. These predictive and prognostic factors include 3
peritumoral budding, lymphovascular ant perineural invasion, lymph node metastasis, mismatch 4
repair status, and corellations with some frequently known mutations in colorectal adenocarcinomas, 5
detected using Next- Generation Sequencing (NGS) platform. This comprehensive approach allowed 6
us to explore how these factors interplay and influence the clinical outcome of patients with colorectal 7
adenocarcinoma. Additionaly, our findings contribute to the understanding of how genetic mutations 8
may correlate with histological features and prognostic markers, potentially guiding personalized 9
treatment strategies in the future. In our study, we do not claim to have exhausted the research on 10
the topic, and we fully recognized the need for more extensive and in-depth studies in this area of 11
tumor pathology.
Keywords:
colorectal adenocarcinoma
; left and right- sided
; histologic type
; peritumoral budding
; 13 lymphovascular and perineural invasion
; lymph node metastasis
; MMR status
; mutations
; NGS
1. Introduction
Cancers of colon and rectum are among the leading causes of morbidity and mortality worldwide. These cancers significantly contribute to the global burden of disease, with increasing incidence rates in many regions. [1] .
In the United States, it is estimated that there will be 152,810 new cases of colon and rectal cancers combined for both sexes. Additionally, the estimated number of deaths from these cancers in both sexes will be 53 010 in 2024. Colorectal cancer has now become a leading cause of death in men and the second leading cause in women under the age of 50.[2]
In Bulgaria, the estimated number of new cases of colorectal cancer was reported to be 5,096 with an estimated 2,079 deaths, making it the second most common cause of cancer mortality for both sexes in 2022.[3]
Based on data from the Global Cancer Observatory ( International Agency for Research on Cancer), the estimated number of new cases of colorectal cancer is projected to increase by approximately 61 % between 2022 and 2045. Similarly, the number of deaths from colorectal cancer is expexted to rise by approximately 77 % during the same period.[4] This alarming trend highlights the growing impact of colorectal cancer and underscores the need for enhanced prevention, early detection, and treatment strategies grounded in the principles of precision and personalized medicine. It further calls for the exploration of new widely- used predictive and prognostic biomarkers in this area of oncology, which could play a pivotal role in tailoring treatments and improving patient outcomes.
Recent understanding of colorectal carcinoma reveals that its etiology and development are influenced by a multitude of factors, such as diet [5] [6] [7] [8] [9] [10], lifestyle habits [11] [12] [13] [14] [15] [16] [17] , social and economic status [18] [19][20] and environmental exposures, and some of which can be modified and can be addressed through prevention strategies. However, other factors, like driver gene mutations and certain genetic predispositions, are not modifiable, highlighting the complexity of the disease.[21] [22] [23] [24] [25] [26]
Many studies emphasize several macroscopic, morphological, and histological characteristics of tumors that are closely related to patient prognosis and survival. These include primary tumor location(left- sided, right- sided or rectal tumors), tumor morphology, lymphatic and vascular invasion, neural invasion, host immune response, tumor budding(peri or intratumoral), poorly differentiated clusters and others. [27] [28] [29] [30] [31] [32] [33] [34] [26] [35] [36] [37][38][39] [40] [41][42] [43][44] [45][46][47][48][49][50][51] [52]
In our study, we focus on certain aspects of the aforementioned tumor characteristics, including some patients’ epidemiological data, primary tumor location, tumor histomorphology, perineural or intraneural invasion, lymph node status and tumor deposits, peritumoral budding, MMR status , and some of frequently observed mutations, assessing their prognostic and predictive role, as well as the possible interrelationships between them. This involves investigating the significance of these factors for disease progression and their influence on the selection of appropriate therapeutic regimens.
2. Materials and Methods
The study was conducted retrospectively, with 100 patients diagnosed between 2020 and 2023 with colorectal adenocarcinoma. These patients were selected from the archives of the Department of Clinical Pathology at "Georgi Stranski" University Hospital in Pleven- Bulgaria.
Patient selection:
Inclusion criteria:
In selecting patients for the study, we adhered to the following inclusion criteria:
- patients who provided informed consent to participate in the study;
- patients who had undergone resection of colon or rectum for primary adenocarcinoma.
The selection was carried out randomly. A small group of patients who had received preoperative radiation or chemotherapy was intentionally not excluded.
Exclusion criteria:
- presence of other histological tumor types or metastatic tumors of the colon or rectum;
- patient who declined to provide informed consent for participation.
The study was approved from the Ethics Committee of Medical University – Pleven prior to its commencement.
Methods
Assessment of peritumoral budding:
We used biopsy samples fixed in 10% buffered formalin, embedded in paraffin, cut at 4 µm, and stained with H&E.
Tumor buds were counted on H&E-stained slides according to the algorithm described by the International Tumor Budding Consensus Conference[47]:
Scanning 10 fields at a 10× objective to identify the invasive front of the tumor and the TB hotspot area.
Counting PTB in the hotspot area at a 20× objective, and dividing the result by the normalization factor to calculate the TB count at 0.785 mm² (in our study, the normalization factor was 0.810).
Tumor budding was graded as follows:
Bd1: Low – 0–4 tumor buds;
Bd2:Intermediate – 5–9 tumor buds;
Bd3: High – 10 or more tumor buds
Assessment of tumor MMR status:
IHC procedure
Tumor resection specimens from patients with colorectal adenocarcinoma were fixed in 10% buffered formalin for 24 to 36 hours at room temperature, dissected, and embedded in paraffin. A pathologist selected 5 µm thick parallel sections of representative invasive tumor tissue and normal mucosa, confirmed by H&E-stained slides.
Epitope retrieval was performed for 20 minutes at 97℃ using DAKO PT Link (Code PT100/PT101).
The tumor sections were stained with the following, ready to use antibodies (DAKO Denmark©):
MLH1: ES05 (Monoclonal mouse Anti- Human MutL Protein Homolog 1, (Ready to use; Ref.№ IR079 )
MSH2: FE11 (Monoclonal mouse Anti- Human MutS Protein Homolog 2 (Ready to use; Ref.№ IR085)
MSH6: EP49 (Monoclonal rabbit Anti- Human MutS Protein Homolog 6 (Ready to use; Ref.№ IR086)
PMS2: EP51 (Monoclonal rabbit Anti- Human Postmeiotic Segregation Increased 2 (Ready to use; Ref.№ IR087)
EnVision FLEX (K800021-2), High pH (Link), HRP. Rabbit/Mouse. High pH, Immunohistochemistry Visualization system kit was used.
Incubation time for all antibodies was 20 min. at room temperature.
A Dako Agilent Autostainer Link 48 slide stainer was used to perform the staining. External reagent negative controls were prepared as part of the manufacturer’s reagent kit. For internal positive controls, normal colonic mucosa, stromal cells, and stromal lymphocytes from the same slides containing the tumor were used.
The results were analyzed by a pathologist. The expression was categorized as follows:
Normal (Retained): Nuclear expression present in >10% of tumor cells, along with the retained expression in internal controls.
Negative (Loss): Absence of nuclear expression in tumor cells, with the retained expression of internal controls.
In our study, we did not aim to evaluate the subclonal expression of MMR proteins or use immunohistochemistry for the confirmation of peritutumoral budding.
Investigation of lymphovascular invasion- LVI:
Due to the relatively small sample size and the limited number of colorectal cancer patients with observed lymphatic and/or vascular invasion, we did not aim to separately analyze these two morphological characteristics. Additionally, we did not focus on distinguishing between intramural and extramural vascular invasion, despite existing evidence indicating their negative prognostic significance[53][54][55].
Assessment of perineural invasion- PNI:
The assessment of perineural invasion (PNI) is based on the identification of tumor cells within any of the three layers of the nerve sheath, following the definition by Liebig C. et al.[56]
NGS testing:
Genetic testing of tumor tissues was performed by NGS, with the TruSight Tumor 15 panel (Illumina. Inc.). Representative tumor tissue blocks, fixed in 10% neutral buffered formalin and embedded in paraffin (FFPE), were selected and cut into 5 µm sections, ensuring sufficient tumor content for analysis. DNA Extraction, quality and quantity assessment, and library preparation were carried out according manufacturer’s protocols. The sequencing platform used was the Illumina NextSeq 550 (Illumina. Inc.), following the manufacturer’s guidelines. Data analysis and result interpretation were conductefd by qualified medical bioinformatics and medical genetics personnel.
Statistical analysis
The results and other data, were recorded, and analyzed using IBM SPSS Statistics. The Chi-Square test was used to compare categorical data with values of p < 0.05 considered statistically significant. For parametric data, if the data did not follow a normal distribution, the Kruskal-Wallis test was employed. We used normalization to adjust the data within a specific range, ensuring that features or variables with different scales do not disproportionately influence the results of the analyses.
3. Results
- Epidemiological data
As mentioned above, in our study, a group of 100 patients was examined, with the following epidemiological characteristics- number and age distribution by sex - presented in Table 1 and Figure 1:

Table 1.
Distribution of patients by sex
| Sex | Number | % | Total |
| Female | 43 | 43 | 43 |
| Male | 57 | 57 | 57 |
| Total | 100 | 100 | 100 |
The age ranges were as follows: females ranged from 48 to 83 years old, and males fro 45 to 88 years old, with a median age 70 years for both sexes.
Tumor localization across different anatomical sites for the entire patient group is presented in Figure 2, along with the results normalized for sample sizes in Figure 3. There is no statistically significant association between tumor localization and sex. (: 2.95; p-value: 0.89; Df : 7)
After consolidating the tumor localizations, we formed groups of patients with left-sided, right-sided, and rectal localization of the primary tumor. After normalization, we obtained the following results- Figure 4.
- Tumor characteristics data
In the studied patient group, the results regarding some characteristics of the primary tumor are as follows: 1. Primary tumor localization and:
- Age
Figure 5 shows a box plot illustrating the distribution of the sample of studied patients based on the location of the primary tumor. Table 2. provides the median age of patients relative to tumor localization in the overall patient group, and differentiated by sex, as well as age ranges. Statistical analysis indicates no statistically significant differences in the distribution by sex(: 2.95; p-value: 0.938) and age(Kruskal-Wallis test statistic is approximately 3.25, p-value: 0.777) in relation to different tumor localizations.
Figure 5.
Age distribution by cancer localization
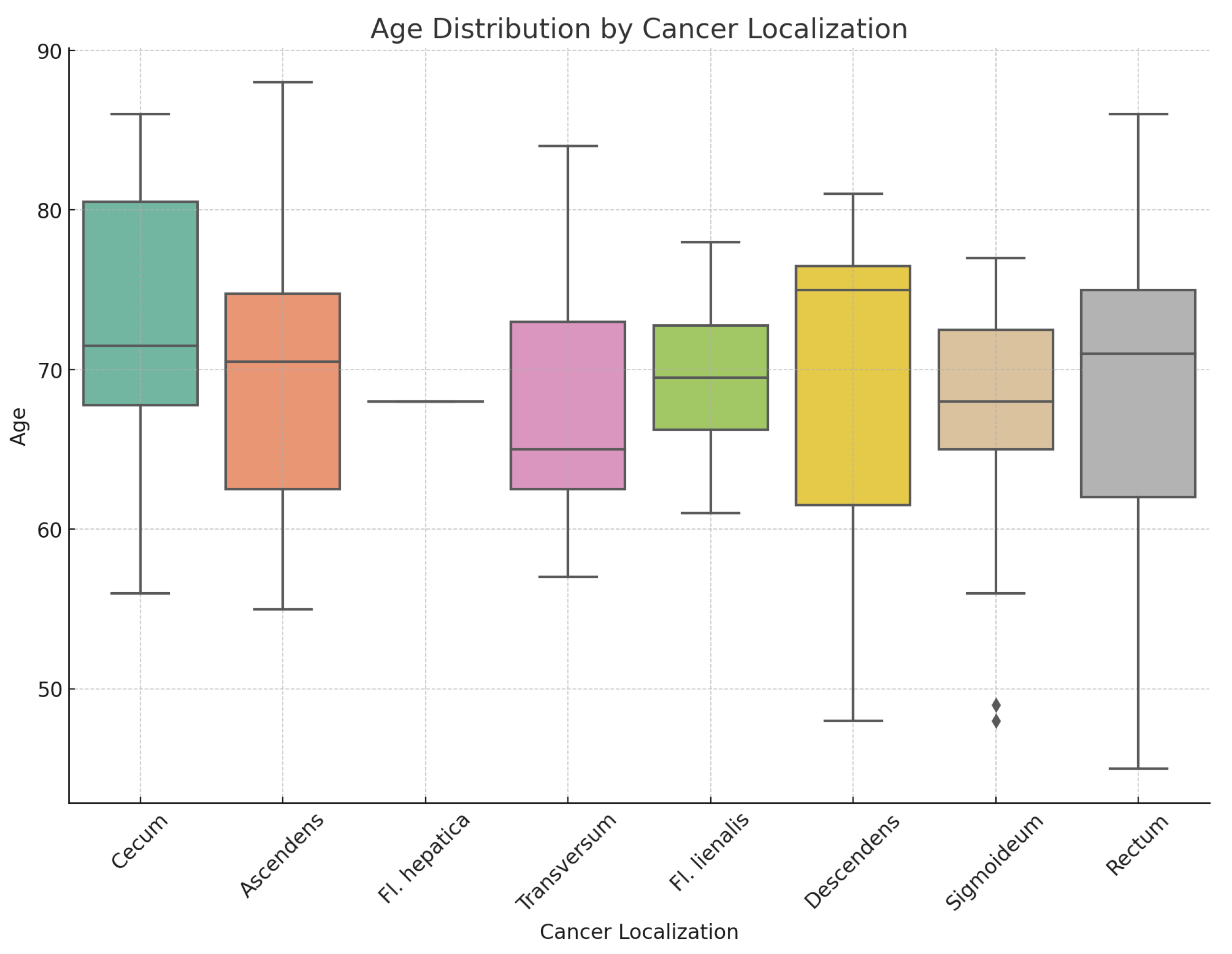
Table 2.
Distribution of patients by age and sex based on primary tumor localization.
| Median Age | Range | Total Patients | Median Males | Range Males | Total Males | Median Females | Range Females | Total Females | |
| Ascendens | 70.5 | 55 - 88 | 14 | 71.0 | 67 - 88 | 7 | 61.0 | 55 - 75 | 7.0 |
| Cecum | 71.5 | 56 - 86 | 16 | 71.5 | 57 - 86 | 10 | 71.5 | 56 - 83 | 6.0 |
| Descendens | 75.0 | 48 - 81 | 6 | 76.0 | 57 - 81 | 4 | 61.5 | 48 - 75 | 2.0 |
| Fl. hepatica | 68.0 | 68 - 68 | 1 | 68.0 | 68 - 68 | 1 | |||
| Fl. lienalis | 69.5 | 61 - 78 | 4 | 71.0 | 68 - 78 | 3 | 61.0 | 61 - 61 | 1.0 |
| Rectum | 71.0 | 45 - 86 | 29 | 72.5 | 45 - 86 | 16 | 68.0 | 57 - 77 | 13.0 |
| Sigmoideum | 68.0 | 48 - 77 | 19 | 68.0 | 57 - 77 | 9 | 68.5 | 48 - 76 | 10.0 |
| Transversum | 65.0 | 57 - 84 | 11 | 65.0 | 57 - 84 | 7 | 73.0 | 61 - 75 | 4.0 |
| Total | 70.0 | 45 - 88 | 100 | 70.0 | 45 - 88 | 57 | 70.0 | 48 - 83 | 43.0 |
Based on the different embryological origins of the right side of the colon (cecum, ascending colon, hepatic flexure, and the proximal two-thirds of the transverse colon) and its left side (splenic flexure, descending colon, and sigmoid colon), as well as extensive experimental and clinical data on differences in morphology, genetics, and clinical characteristics, we consolidated the primary tumor localizations into three groups: right colon, left colon, and rectum. This approach also facilitated the subsequent statistical analysis to some extent. Figure 6. and Figure 7. present the results concerning these three localization groups and their relationship with the age and sex of patients with colorectal carcinoma. The subsequent statistical analysis showed no statistically significant differences regarding the primary tumor localization, age, and sex of the patients.
The results of the Kruskal-Wallis tests are as follows:Females: The test statistic is 0.805 with a p-value of 0.669; Males: The test statistic is 0.418 with a p-value of 0.811.
- Histological subtype
The following bar chart displays the normalized proportions of histological subtypes as a grouped bar chart, with each localization group (Right Colon, Left Colon, and Rectum) represented in Figure 8. In summary, even with normalized proportions, there is no statistically significant relationship between localization and histological type:(: 19.937; p-value: 0.336; df=18). The statistical results of the chi-square test for the above indicators, separated by sex (not shown), also do not reveal any statistically significant differences.(Males: p-value: 0.685; Females: p-value: 0.380)
- Tumor Grade and Stage
The following two charts in Figure 9. and Figure 10*. illustrate the possible relationships between primary tumor localization in the Right colon, Left colon, and Rectum, and the corresponding tumor grade and stage. As seen from the charts and the results of the chi-square test, no statistically significant differences are found. Additionally, when analyzing these parameters separately by sex, no statistically significant differences are detected for either tumor grade(Males: p-value: 0.429, Df=6; Females: p-value: 0.096, Df=4) or stage(Males: p-value: 0.230, Df=8; Females: p-value: 0.154, Df=10).(*The ypT categories were added to their respective T groups).
However, when we compare tumor differentiation(G) and tumor stage(pT), the following expected results are obtained- Figure 11:
As expected, the chi-square test shows that the relationship between grade and stage is highly statistically significant.(: 42.69; p-value:0.00000565; Df=10)
- Lymph node status
The statistical analysis of the patient sample showed no statistically significant differences in the N status of patients with colorectal adenocarcinoma based on the localization of the primary tumor—Right colon, Left colon, or Rectum—for the entire patient group(: 11.811; p-value: 0.621; df=14). The same conclusions remain valid when analyzed separately by sex: Males: : 12.82; p-value: 0.382; df=12; Females: : 8.38; p-value: 0.869; df=14 Figure 12 represents the whole patient group.
When we compared lymph node status with the degree of tumor differentiation and tumor stage, the results indicated a lack of statistically significant differences once again, as is most clearly seen from the statistical analysis- Table 3.
- Important histological features of the tumor:
- Lymphatic and vascular invasion
In our study, due to the relatively small sample size and the limited number of colorectal cancer patients with observed lymphatic and/or vascular invasion, we did not aim to separately analyze these two morphological characteristics. We also did not focus on distinguishing between so-called intramural and extramural vascular invasion, despite evidence of their negative prognostic significance. For this reason, they will be considered together in the following brief section.
LVI and primary tumor localization: the following Figure 13 and Table 4 visually present the relationships between the localization of the primary tumor and lymphovascular invasion (LVI). The results of the chi-square test for the association between LVI status and localization are as follows: Chi-Square value: 2.38; df: 2; p-value: 0.304. The p-value is greater than 0.05, indicating that there is no statistically significant association between LVI status and localization.
LVI and histopatological subtype- Figure 14 shows the proportion of negative and positive statuses across different tumor histological subtypes. chi-square test The subsequent statistical analysis shows no statistically significant association between lymphovascular invasion (LVI) and histological subtype. The Monte Carlo approximation of the chi-square test for the association between LVI status and histological subtype yields the following results: Chi-Square value: 15.93; df: 9; Monte Carlo p-value: 0.068 However, the p-value is close to significance, suggesting a potential trend that may warrant further investigation.
LVI and tumor Grade and Stage- As we expected, there is a statistically significant association between lymphovascular invasion and tumor grade and stage. The results of the chi-square tests are shown in the following Table 5 and Figure 15.
- Perineural invasion
The assessment of perineural tumor invasion is based on the presence of tumor cells in any of the three layers of the nerves or tumor cells involving at least one-third of the nerve’s circumference.
In our study, regarding this tumor characteristic, we observed the following results as shown in Figure 16 and Table 6. There are no statistically significant associations between PNI and any of the variables: primary tumor localization, tumor histological subtype, tumor grade, or tumor stage (all p-values > 0.05).
- Immune response
In our study, we focused on evaluating the peritumoral stromal inflammatory reaction at the invasive tumor front, specifically assessing the immune response of the so-called "Crohn-like" type. Our interest lay in investigating the presence or absence of interactions between this immune reaction and other prognostic factors such as tumor budding, MMR status, mutational status, and primary tumor localization, among others. For practical purposes, we conducted a semi-quantitative assessment of the peritumoral stromal inflammatory reaction, categorizing it into three levels: Absent, Moderate, and Marked inflammatory response. After data processing, we obtained the following results:
-Immune response and primary tumor localization- Figure 17:
The Right Colon has the highest percentage of marked reactions (56.1%), while absent reactions are relatively low.
The Left Colon shows a more balanced distribution, with the majority of cases presenting marked reactions (48%).
The Rectum is unique in having the highest percentage of moderate reactions (55.2%) and the lowest percentage of marked reactions (13.8%).
Results from the Chi-Square test: value: 14.05; (dof): 4; p-value: 0.007. The p-value is statistically significant (below the typical threshold of 0.05). This suggests that there is a strong indication that the distribution of peritumoral stromal immune reactions is not uniform across the three tumor localizations (Right Colon, Left Colon, and Rectum). In other words, the type or intensity of the immune response differs significantly depending on the tumor’s primary location.
-Immune response and histological subtype
The chart compares the average peritumoral stromal reaction for each histological subtype. Each point represents the average immune response (from absent to marked) within each histological type- Figure 18:
As shown in the chart, adenocarcinomas NOS with an additional tumor component (such as Synchronous- Cecum- mucinous + Rectum- Adenocarcinoma NOS, Adenocarcinoma NOS + intra- and extracellular mucin production, or MiNEN with an exception) exhibit a marked immune response. Speculatively, this could be due to the tumor heterogeneity and the higher immunogenicity of these tumors.
The results from the Chi-square test are: value: 18.76; p-value: 0.4067; Degrees of freedom (dof): 18 These results show no statistically significant association between histological type and the peritumoral stromal reaction. This suggests that while some histological subtypes may show a pronounced immune response, there isn’t a consistent or significant pattern across the different histological subtypes studied.
-Immune response and tumor grade and stage
In the following Table 7—the relationships between tumor grade and peritumoral stromal immune reaction, as well as tumor stage and peritumoral stromal immune reaction, are presented. The Chi-square tests conducted for these two characteristics show no statistically significant results for either variable, indicating no strong association between tumor grade or tumor stage and the intensity of the peritumoral stromal immune reaction:
1. Tumor Grade (G1, G2, G3) vs. Peritumoral strormal immune reaction (Normalized): Chi-square value (): 0.185; p-value: 0.996; Degrees of freedom (dof): 4.
2. Tumor Stage (T1, T2, T3, T4) vs. Peritumoral stromal immune reaction (Normalized): Chi-square value (): 0.685; p-value: 0.995; Degrees of freedom (dof): 6.
This suggests that the immune response in the tumor’s surrounding stroma does not significantly correlate with the differentiation (grade) or progression (stage) of the tumor in this particular cohort.
-Immune response and lymph node status
The chi-square test results for the relationship between peritumoral stromal immune reaction and lymph node status are as follows:
Chi-square value: 14.47; p-value: 0.416; Degrees of Freedom: 14.
These results indicate that there is no significant association between peritumoral stromal immune reaction and lymph node status, as the p-value is greater than 0.05. This suggests that variations in the immune reaction in the tumor stroma do not correlate significantly with whether lymph node involvement is present or not.
-Immune response and lymphovascular (LVI) and perineural invasion (PNI)
The following Figure 20 shows the correlation between peritumoral stromal immune reaction and lymphovascular and perineural invasion. As seen from the results of the chi-square tests, there is no statistically significant association between these three examined parameters.
1. Peritumoral stromal immune reaction vs. lymphovascular invasion (LVI):
Chi-square value: 2.23; p-value: 0.327; Degrees of freedom: 2.
2. Peritumoral stromal immune reaction vs. perineural invasion (PNI):
Chi-square value: 3.08; p-value: 0.214; Degrees of freedom: 2.
The lack of a significant correlation suggests that the peritumoral stromal immune reaction does not directly influence lymphovascular or perineural invasion in the context of the cases studied. These results can be interpreted to mean that the immune reaction in the tumor stroma is not a primary predictor of tumor invasiveness in these aspects.
- Tumor budding
In our study, when assessing tumor budding, we followed the classical scheme described by the International Tumor Budding Consensus Conference (ITBCC) . During the evaluation, we also encountered cases with zero budding, which were included in Bd1 group.
After evaluating the tumor budding, we obtained the following results:
- Peritumoral budding and primary tumor localization- Right colon, Left colon, Rectum:
In the following Figure 20, the relationship between peritumoral budding Bd1 = (Bd0 + Bd1), Bd2, and Bd3 and the primary tumor localization (Right colon, Left colon, Rectum) is illustrated. As seen in the graph, all grades of peritumoral budding are more prevalent in the right colon, followed by the left colon and rectum. Notably, the Bd1 group in the rectum shows a higher value compared to the left colon.
The subsequent statistical analysis did not reveal statistically significant differences among these groups. The results of the Kruskal-Wallis test indicate: Test statistic: 3.37; p-value: 0.185.
- Peritumoral budding and histological subtype:
In Figure 21, we can observe the distribution of peritumoral budding across different histological tumor subtypes. The results of the Kruskal-Wallis test for the peritumoral budding groups (Bd1, Bd2, Bd3) across these histological types are as follows: Test statistic: 7.39, p-value: 0.597. These results indicate that there is no statistically significant difference in peritumoral budding across the different histological subtypes, suggesting that the subtype does not have a meaningful impact on the distribution of tumor budding grades for the studied cohort of patients.
The undifferentiated tumors, along with adenocarcinoma NOS that include other tumor components such as mucinous and poorly cohesive types, exhibit the highest average peritumoral budding grade (Bd3). This suggests the correlation between these tumor types and more aggressive behavior.
- Peritumoral budding and tumor grade and stage:
The results for peritumoral budding grades and tumor Grade and Stage are shown in the next Table 8
The results of the chi-square tests for the association between peritumoral budding and both tumor grade and tumor stage are as follows: and both tumor grade and tumor stage:
1. Tumor grade vs. Peritumoral budding: Chi-square value: 14.39; p-value: 0.0255; Degrees of freedom: 6. This result indicates that there is a statistically significant association between peritumoral budding and tumor grade, as the p-value is below 0.05.
2. Tumor stage vs. Peritumoral budding: Chi-square value: 7.36; p-value: 0.691; Degrees of freedom: 10.
This result suggests that there is no statistically significant association between peritumoral budding and tumor stage, as the p-value is much higher than 0.05.
-Peritumoral budding and lymphovascular invasion(LVI) and lymph node status:
The analysis of the association between peritumoral budding and lymphovascular invasion indicates a statistically significant correlation between the two, as illustrated in Figure 22. The results from the chi-square test are as follows:
Chi-square value: 8.59; p-value: 0.0137; Degrees of freedom: 2
These results suggest that there is a meaningful relationship between peritumoral budding and lymphovascular invasion, implying that higher levels of budding may be associated with an increased likelihood of lymphovascular spread in colorectal cancer. This finding highlights the importance of assessing both peritumoral budding and lymphovascular invasion in the prognostic evaluation of tumors.
On the other hand, the analysis of the association between peritumoral budding and lymph node status shows a lack of statistical significance in this group:
Chi-square value: 19.93; p-value: 0.132; Degrees of freedom: 14.
These results indicate that there is no significant relationship between peritumoral budding and lymph node status in this cohort.
-Peritumoral budding and perineural invasion(PNI)
The chi-square test results for the association between peritumoral budding and perineural invasion (PNI) are as follows:
Chi-square value: 5.59; p-value: 0.061; Degrees of freedom: 2
These results suggest a marginally non-significant association, as the p-value is slightly above the common threshold of 0.05. This indicates that while there may be some correlation between peritumoral budding and PNI, it does not achieve statistical significance.
3. Important prognostic and predictive biomarkers of Colorectal carcinoma (CRC)
-MMR status and primary tumor localization:
The following Table 9 presents the results of MMR status in colorectal carcinomas within the studied cohort. As illustrated in the corresponding Figure 23, the findings can be summarized as follows:
1. dMMR (Deficient mismatch repair): Right-sided tumors dominate: A significant majority of tumors in the dMMR group are localized in the right colon, approximately 89%. This strong association suggests that dMMR status is more prevalent in right-sided colon cancer. Left-sided and rectal tumors are rare: There are very few left-sided tumors and no rectal tumors associated with dMMR, indicating a distinct localization pattern.
2. pMMR (Proficient mismatch repair): Even distribution: Tumors in the pMMR group are more evenly distributed across all localization groups (right, left, rectum), suggesting that pMMR tumors do not have a strong preference for a specific side. Common rectal tumors: Rectal tumors are notably common in the pMMR group, accounting for nearly 35% of cases. This highlights a significant presence of rectal cancer in patients with proficient MMR. Relatively frequent left-sided tumors: Left-sided tumors are also observed more frequently in the pMMR group compared to dMMR, reinforcing the variability in tumor location based on MMR status.
-Statistical analysis:
The chi-square test results confirm a statistically significant association between MMR status and tumor localization (right, left, rectum):
Chi-square value: 20.28; p-value: 0.000039; Degrees of freedom: 2. These results indicate a strong correlation between MMR status and the localization of colorectal tumors.
-MMR status and sex:
For both sexes, the pattern for dMMR is as follows:
-Right Colon: dMMR is most prevalent in the right colon for both males and females. There are 8 cases for males and 8 cases for females localized in the right colon.
-Left Colon: There is only 1 case of dMMR for both males and females in the left colon, showing a much lower prevalence compared to the right colon.
-Rectum: dMMR is absent in the rectum for both males and females. In summary, dMMR is predominantly found in the right colon in both males and females, with very few cases in the left colon and none in the rectum.
-Chi-square value: 0.16; p-value: 0.689; Degrees of Freedom: 1
These results indicate that there is no statistically significant association between MMR status and sex.
-MMR status and histological subtype:
The results for MMR status, histological subtype, and tumor localization are presented in the next crosstab- Table 10. The key findings for dMMR are as follows:
Adenocarcinoma NOS: All 8 cases of dMMR-associated Adenocarcinoma NOS are located in the right colon.
Medullary: Both cases of Medullary tumors are located in the right colon.
MiNEN: The single case of MiNEN is also found in the right colon.
Mucinous: Most dMMR-associated Mucinous cases (4 out of 6) are found in the right colon, with 2 in the left colon.
Serrated adenocarcinoma: The single case is located in the right colon.
No dMMR-associated tumors were found in the rectum.
The results of the chi-square test for statistical significance for MMR status vs histological subtype and tumor localization are as follows:
Chi-square value: 36.72; p-value: 0.0467; Degrees of freedom: 24.
There is a statistically significant association between MMR status, histological subtype, and tumor localization, as the p-value is slightly below 0.05.
When we examined the relationship between MMR status and histological subtype separately, the following results from the chi-square test were obtained:
Chi-square value: 27.87; p-value: 0.001;Degrees of Freedom: 9.
This indicates that there is a statistically significant association between MMR status and histological subtype, as the p-value is well below the 0.05 threshold.
-MMR status and peritumoral stromal immune reaction
Our results indicated a lack of statistically significant association between MMR status and peritumoral stromal immune reaction. This suggests that the immune response in the peritumoral stroma does not appear to be influenced by the MMR status of the tumors in the studied cohort.
Chi-square value: 4.18; p-value: 0.1239; Degrees of freedom: 2.
-MMR status and lymph node status:
The next chart visualizing the relationship between MMR status (dMMR and pMMR) and lymph node status- Figure 24.
-MMR status and lymphovascular invasion (LVI) and perineural invasion (PNI) The statistical analysis indicates a lack of statistical significance for the association between MMR status and both lymphovascular invasion (LVI) and perineural invasion (PNI). This suggests that MMR status may not play a significant role in predicting these specific invasive behaviors in the tumors analyzed.
1. MMR Status vs LVI: Chi-square value: 0.24 p-value: 0.63; Degrees of freedom: 1.
2. MMR Status vs PNI: Chi-square value: 0.19; p-value: 0.66; Degrees of Freedom: 1.
In a Table 11, patients with dMMR and the corresponding MLH1, PMS2, MSH6, and MSH2 abnormalities identified through immunohistochemistry (IHC) are shown, along with the NGS-analyzed mutations in key genes and their combinations. In the last col- umn, we have indicated cases where further investigation for Lynch syndrome is war- ranted. In cases with a suspicion of Lynch syndrome, no additional tests were conducted in our research to confirm the diagnosis. The research team declared a refusal to influence specific diagnostic or therapeutic decisions.
- Gene mutations identified by NGS
In our study, we utilized the "TruSight Tumor 15" panel from Illumina for Next-Generation Sequencing (NGS). This panel is designed to detect mutations across 15 key genes associated with various cancers, which include: AKT1, BRAF, EGFR, ERBB2(HER2), FOXL2, GNA11, GNAQ, KIT, KRAS, MET, NRAS, PDGFRA, PIK3CA, RET, TP53.
The results obtained from NGS are as follows:
-Observed mutations by sex:
-Proportions of gene mutations by sex:
Females: TP53 is the most frequent mutation, appearing in about 67.4% of cases. KRAS follows with a proportion of 34.9%. Other gene mutations include BRAF (18.6%), PIK3CA (9.3%), and NRAS (4.7%).
Males: TP53 is also the most common, but slightly less frequent than in females, at 57.9%. KRAS appears in 38.6% of cases. Other gene mutations include PIK3CA (12.3%), BRAF (15.8%), and NRAS (3.5%).
Both sexes show a higher prevalence of TP53 mutations, but females have a slightly higher proportion. PIK3CA mutations appear more often in males compared to females.
The two-proportion Z-test for each gene mutation between males and females are as follows:
AKT1: Z-Statistic: 0.202; p-value: 0.840;
TP53: Z-Statistic: 0.974; p-value: 0.330;
KRAS: Z-Statistic: -0.381; p-value: 0.703;
BRAF: Z-Statistic: 0.371; p-value: 0.711;
PIK3CA: Z-Statistic: -0.471; p-value: 0.637;
NRAS: Z-Statistic: 0.289; p-value: 0.773;
All p-values are greater than the common significance level of 0.05, indicating no statistically significant differences in the proportions of any gene mutation between males and females.
-Observed mutations vs primary tumor localization:
The distributions of gene mutations by count and frequency in relation to tumor localization are presented in the Table 12 and Figure 25 below. These visualizations illustrate the variations in mutation prevalence across different tumor sites.
The chi-square test results for the association between gene mutations and localizations are as follows: Chi-square value: 22.59; p-value: 0.012; Degrees of freedom: 10. The p-value (0.012) is less than 0.05, indicating that there is a statistically significant association between gene mutations and localization. This suggests that the distribution of gene mutations differs significantly across the Right colon, Left colon, and Rectum.
Based on the statistical analysis, there is a significant association between gene mutations and localization:
1. Right colon:
Tumors located in the Right colon tend to exhibit the highest number of mutations overall (42), with a variety of gene mutations such as TP53, KRAS, BRAF, PIK3CA, and AKT1. BRAF and KRAS mutations are more frequent here compared to other locations. The high presence of mutations like BRAF in the right colon aligns with known patterns in colorectal cancer, and they indicates a sporadic pathway rather than Lynch syndrome.
2. Left colon:
The left colon tumors have fewer total mutations (25) compared to the right colon. The dominant mutations here include TP53 and KRAS, with PIK3CA also present but at a lower frequency. The mutations in the left colon tend to align more with classic genetic alterations seen in colorectal cancer. The lower count of BRAF mutations in this area differentiates it from the right colon.
3. Rectum:
The rectal carcinomas has 29 total mutations, with a higher frequency of TP53 mutations. Unlike the right colon, the rectum does not show any BRAF mutations, which is a key distinction. This suggests that the genetic profile of rectal cancers in this dataset differs significantly from right-sided colorectal cancers, which often exhibit BRAF mutations. The presence of KRAS and NRAS mutations indicates a different mutation spectrum in the rectum, which might be more associated with sporadic colorectal cancers rather than hereditary syndromes like Lynch.
-Mutations across tumor histological subtype:
The only gene mutation showing a significant association with histological type is BRAF. This suggests that the presence of BRAF mutations may vary depending on the histological subtype. The Table 13 displays the results of the Chi-square test comparing mutated genes with histological subtypes.
-Mutations across tumor grade and stage:
The performed chi-square test for gene mutations in relation to tumor grade and stage yielded the following results:
Tumor grade vs gene mutations:
AKT1 Chi-Square: 0.360; DOF: 2; p-value: 0.835.
TP53 Chi-Square: 5.194; DOF: 2; p-value: 0.074.
KRAS Chi-Square: 0.102; DOF: 2; p-value: 0.950.
BRAF Chi-Square: 12.070; DOF: 2; p-value: 0.002.
PIK3CA Chi-Square: 0.509; DOF: 2; p-value: 0.775.
NRAS Chi-Square: 0.761; DOF: 2; p-value: 0.684.
BRAF shows a statistically significant association with tumor grade.
G2 is the grade with the highest frequency of mutations, particularly TP53 and KRAS. G3 shows TP53 as the most frequent mutation, with a slight increase in BRAF mutations. G4 has the fewest mutations overall.
Tumor stage vs gene mutations:
AKT1 Chi-Square: 1.591; DOF: 5; p-value: 0.902.
TP53 Chi-Square: 4.116; DOF: 5; p-value: 0.533.
KRAS Chi-Square: 1.814; DOF: 5; p-value: 0.874.
BRAF Chi-Square: 6.304; DOF: 5; p-value: 0.278.
PIK3CA Chi-Square: 3.742; DOF: 5; p-value: 0.587.
NRAS Chi-Square: 11.929; DOF: 5; p-value: 0.036.
NRAS shows a statistically significant association with tumor stage.
Stages pT1 and pT2: These early stages demonstrate limited mutations, with TP53 and KRAS mutations appearing occasionally.
Stages pT3 and pT4: In these advanced stages, TP53 and KRAS mutations become more frequent. Additionally, mutations in BRAF and PIK3CA are observed in some cases, indicating a shift toward a more aggressive tumor profile.
Lymph node status and lymphovascular invasion vs gene mutations:
Lymph node status vs gene mutations:
Negative lymph node status: TP53 (27 cases) and KRAS (18 cases) are the most frequent mutations. BRAF appears in 10 cases.
Positive lymph node status: TP53 is the most common (34 cases), followed by KRAS (19 cases) and PIK3CA (8 cases).
Lymphovascular invasion vs gene mutations:
Negative Lymphovascular Invasion: TP53 (38 cases) and KRAS (28 cases) are prominent. BRAF and PIK3CA mutations are also present but less frequent.
Positive Lymphovascular Invasion: TP53 remains frequent (24 cases), but KRAS drops to 9 cases. BRAF is seen in 9 cases, and PIK3CA appears in 5 cases.
The results of the performed chi-square test indicate significant associations between specific gene mutations and both lymph node status and lymphovascular invasion in colorectal cancer:
TP53 Mutations: There is a notable association with both lymph node status and lymphovascular invasion.
Chi-square: 7.423; Dof: 2; p-value: 0.024 (significant association).
BRAF Mutations: A significant association with lymphovascular invasion was also observed for BRAF mutations.
Chi-square: 4.853; Dof: 1; p-value: 0.028 (significant association).
Analyses for gene mutations versus peritumoral budding, stromal immune reaction, and perineural invasion:
1. Peritumoral budding vs gene mutations:
Bd1(Bd0 + Bd1): TP53 and KRAS mutations are most frequent, with moderate occurrences of BRAF and PIK3CA.
Bd2: Similar frequency for TP53, with KRAS and BRAF appearing less frequently.
Bd3: Highest occurrence of TP53, followed by KRAS, BRAF, and some PIK3CA mutations.
2. Stromal immune reaction vs gene mutations:
Absent: TP53 and KRAS mutations are common, with minimal BRAF and PIK3CA.
Moderate: TP53 and KRAS are frequent, with a presence of BRAF but fewer PIK3CA mutations.
Marked: TP53 remains frequent, with higher occurrences of BRAF and PIK3CA.
3. Perineural invasion vs gene mutations:
Negative: TP53 and KRAS mutations are most frequent; BRAF and PIK3CA appear less frequently.
Positive: TP53 remains common, and there is an increase in PIK3CA mutations compared to negative cases.
The summary of the performed chi-square test for the associations reveals significant findings:
TP53 and peritumoral budding: Chi-Square = 6.071; p-value = 0.048; DOF = 2. This indicates a statistically significant association between TP53 mutations and peritumoral budding, suggesting that the presence of TP53 mutations may influence the tumor’s invasive characteristics, potentially impacting prognosis and treatment options.
NRAS and stromal immune reaction: Chi-square = 7.645; p-value = 0.022; DOF = 2. The significant association between NRAS mutations and the stromal immune reaction indicates that NRAS may play a role in the immune landscape surrounding tumors, which could have implications for therapeutic strategies.
These results highlight the importance of genetic profiling in colorectal cancer, as understanding the relationships between specific mutations and clinical features can help inform prognosis and treatment decisions.
MMR status (pMMR and dMMR) versus gene mutations:
Lastly, in this section, we will examine the association between gene mutations and MMR status. In Table 14, the results of the MMR status in relation to the mutations of individual genes are presented. This table highlights the correlation between the MMR (mismatch repair) status and specific gene mutations, which can provide insights into the genetic landscape of colorectal cancer.
Only KRAS and BRAF mutations show significant associations with MMR status:
KRAS: Chi-square: 7.739; p-value: 0.005; Dof: 1.
BRAF: Chi-square: 34.204; p-value: <0.001; Dof: 1.
These results indicate a strong relationship between these specific mutations and the MMR status of colorectal tumors. The significant p-values suggest that the presence of KRAS and BRAF mutations is associated with specific MMR status groups, which may have implications for treatment decisions and prognostic outcomes.
4. Discussion
1.Patient demographics:
Age and Sex Distribution The cohort consists of 100 patients, with a slight male predominance (57%). The median age of diagnosis is 70 years, consistent with global CRC demographics where incidence increases with age . Studies like those by Siegel et al. confirm this age range, reporting similar median ages in CRC populations globally[2]. Notably, the analysis indicated no statistically significant association between sex and tumor localization (: 2.95, p-value: 0.938), aligning with the findings of Kishiki et al., who also found no gender-specific localization preference[57].
2.Tumor localization and its clinical implications. In this cohort, right-sided colon cancers are predominant, consistent with observations that right-sided tumors often feature distinct molecular profiles, such as dMMR status. The study reports that 89% of dMMR cases occur in right-sided tumors, supporting findings from Yahagi et al., which highlight the prevalence of genetic anomalies like BRAF mutations in this localization[50]. The statistically significant correlation between MMR status and tumor localization (: 20.28, p-value: 0.000039) confirms the distinct biological behavior observed in right-sided CRCs.
3.Tumor grade and stage
Most tumors in the cohort are of moderate grade (G2), with advanced stages (T3/T4) being common. There is a significant correlation between tumor grade and lymphovascular invasion (LVI) (: 17.33; p-value: 0.00017), supporting the hypothesis that higher grades are associated with more aggressive behavior. These results align with Saito et al., who also identified higher rates of LVI in advanced CRC grades[48]. The study found no significant relationship between tumor budding and overall stage (p > 0.05), a result that mirrors findings by Benedix et al., who noted that tumor budding’s impact varies based on additional factors like tumor localization and genetic mutations[21].
4.Lymphovascular invasion (LVI) and perineural invasion (PNI)
Lymphovascular invasion (LVI) and perineural invasion (PNI) LVI was detected in 26% of cases, showing significant association with higher tumor grades and stages (p < 0.05) . This aligns with the work of Des Guetz et al., who identified LVI as a reliable marker for predicting poor prognosis and increased metastasis risk in CRC patients [58]. However, PNI did not exhibit statistically significant correlations with tumor grade, stage, or localization (all p-values > 0.05). This reflects findings from studies like Lee et al., who reported the inconsistent prognostic value of PNI across CRC cases[59].
5.Lymph node status and tumor stage
Correlation lymph node involvement increased with tumor stage, notably in T3 and T4 stages, a pattern consistent with established CRC literature that underscores the role of lymphatic spread in tumor progression. Lugli et al. highlight the importance of lymph node evaluation, stating that node positivity is one of the strongest indicators of disease progression. The lack of a statistically significant association between tumor budding and lymph node status (p-value: 0.132) suggests that lymph node involvement is influenced by multiple histological and molecular factors beyond peritumoral budding.
6. Mutations
Mutations and MMR status: Genetic analysis identified several key mutations, including KRAS, BRAF, and TP53. The majority of BRAF mutations were in right-sided tumors, in line with the literature on sporadic CRC cases. dMMR were prevalent in 89% of right-sided cases, reinforcing their role as biomarkers for this subtype. This matches findings by Boland and Goel, who confirm the diagnostic and therapeutic significance of MSI and MMR status in CRC management[60].
7. Comparison with other studies
Tumor budding and immune microenvironment Tumor budding was significantly correlated with higher tumor grades in this cohort, validating its role as a marker for aggressive tumor behavior. Lugli et al. noted similar patterns, emphasizing the association between tumor budding and adverse clinical outcomes[47]. Additionally, the immune response, correlate with better prognosis, consistent with Saito et al., who demonstrated the prognostic value of immune engagement in MSI-H cases[48].
8. Pathological implications of mutations in CRC
The study highlights the prognostic significance of mutations like KRAS, BRAF, and TP53. KRAS mutations, found in various tumor stages and locations, are known to confer resistance to anti-EGFR therapies, necessitating alternative treatment strategies . BRAF mutations, predominantly in right-sided cancers, are associated with poor prognosis and necessitate targeted approaches, echoing findings from Kopetz et al[61]. BRAF mutations in colorectal cancer (CRC) have been associated with a higher likelihood of metastatic disease, highlighting the aggressive nature of this subtype. Research by Domingo et al. emphasizes that BRAF-mutated CRC is characterized by distinct biological behaviors and poorer prognostic outcomes. These mutations are often linked to a more advanced stage at diagnosis and a tendency for early metastasis, particularly to the liver and peritoneum[62]. TP53 mutations are frequently observed across various tumor stages and localizations in colorectal cancer (CRC), highlighting their significant role in tumor progression. These mutations contribute to the molecular complexity and heterogeneity of CRC, influencing both the biological behavior of tumors and their responses to therapies[63].
5. Conclusions
Our team leaves the opportunity for the esteemed audience to draw their own conclusions.
Author Contributions
The contributions of the individual authors in this study are as follows: Krasimir Petrov: conceptualization, methodology, software, resources, validation, investigation, data curation, writing, project administration. Ivan Ivanov: conceptualization, methodology, software, resources, validation, investigation, data curation, supervision. Savelina Popovska: conceptualization, methodology, supervision, project administration, funding acquisition. Tatyana Betova: investigation. Zornica Kamburova: NGS testing -methodology, validation, formal analysis, investigation, data curation. All authors have read and agreed to the published version of the manuscript.
Funding
The implementation of the present study is thanks to the funding of the Project BG05M2OP001-1.002-0010-C01, “Center for Competence in Personalized Medicine, 3D and Telemedicine, Robotic and Minimal Invasive Surgery” funded by the Operational Program“Science and Education for Smart Growth,”co-funded by the European Union through the European Structural and Investment Funds”.
Institutional Review Board Statement
“The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of Medical University- Pleven, protocol № 50/ 05. 2020 and ON: 635- KENID/ 11. 06. 2020
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data from this study is available on the Science Data Bank website: https://www.scidb.cn. Interested parties may access the data by submitting a request to the authors of the study.
Acknowledgments
The research team extends its gratitude to Zornica Petrova, a biologist, Kristina Ignatova, a histological laboratory technician, and Vladislav Nankov, a Master’s student in Translational Oncology, for their tireless work and professionalism. Their contributions were invaluable to the success of this study.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CRC | Colorectal cancer |
| PNI | Perineural invasion |
| LVI | Lymphovascular invasion |
| MMR | Mismatch repair |
| NGS | Next generation sequencing |
References
- Ferlay, J.e.a. Global Cancer Observatory: Cancer Today. 2024. Available online: http://gco.iarc.who.int/media/globocan/factsheets/cancers/8-colon-fact-sheet.pdf (accessed on 23 September 2024).
- Siegel, R.L.; Giaquinto, A.N.; Jemal, A. Cancer Statistics, 2024. CA: A Cancer Journal for Clinicians 2024, 74, 12–49. [Google Scholar] [CrossRef] [PubMed]
- European Cancer Information System. 2024. Available online: https://ecis.jrc.ec.europa.eu/explorer.php?/0-0/1-BG/2-All/4-1,2/3-All/6-0,85/5-2022,2022/7-7/CEstByCancer/X0_8-3/CEstRelativeCanc/X1_8-3/X1_9-AE27/CEstBySexByCancer/X2_8-3/X2_-1-1 (accessed on 23 September 2024).
- Cancer Tomorrow. 2024. Available online: https://gco.iarc.who.int/tomorrow/en/dataviz/tables?mode=cancer&group_populations=1 (accessed on 23 September 2024).
- Bouvard, V.; Loomis, D.; Guyton, K.Z.; Grosse, Y.; Ghissassi, F.E.; Benbrahim-Tallaa, L.; Guha, N.; Mattock, H.; Straif, K. Carcinogenicity of Consumption of Red and Processed Meat. The Lancet Oncology 2015, 16, 1599–1600. [Google Scholar] [CrossRef] [PubMed]
- Christakos, S.; Dhawan, P.; Porta, A.; Mady, L.J.; Seth, T. Vitamin D and Intestinal Calcium Absorption. Molecular and Cellular Endocrinology 2011, 347, 25–29. [Google Scholar] [CrossRef]
- Aleksandrova, K.; Boeing, H.; Jenab, M.; Bas Bueno-de-Mesquita, H.; Jansen, E.; Van Duijnhoven, F.J.; Fedirko, V.; Rinaldi, S.; Romieu, I.; Riboli, E.; et al. Metabolic Syndrome and Risks of Colon and Rectal Cancer: The European Prospective Investigation into Cancer and Nutrition Study. Cancer Prevention Research 2011, 4, 1873–1883. [Google Scholar] [CrossRef]
- Zhong, Y.; Zhu, Y.; Li, Q.; Wang, F.; Ge, X.; Zhou, G.; Miao, L. Association between Mediterranean Diet Adherence and Colorectal Cancer: A Dose-Response Meta-Analysis. The American Journal of Clinical Nutrition 2020, 111, 1214–1225. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Schwedhelm, C.; Hoffmann, G.; Knüppel, S.; Laure Preterre, A.; Iqbal, K.; Bechthold, A.; De Henauw, S.; Michels, N.; Devleesschauwer, B.; et al. Food Groups and Risk of Colorectal Cancer. International Journal of Cancer 2018, 142, 1748–1758. [Google Scholar] [CrossRef]
- Veettil, S.K.; Wong, T.Y.; Loo, Y.S.; Playdon, M.C.; Lai, N.M.; Giovannucci, E.L.; Chaiyakunapruk, N. Role of Diet in Colorectal Cancer Incidence: Umbrella Review of Meta-analyses of Prospective Observational Studies. JAMA Network Open 2021, 4, e2037341. [Google Scholar] [CrossRef]
- Lynch, B.M. Sedentary Behavior and Cancer: A Systematic Review of the Literature and Proposed Biological Mechanisms. Cancer Epidemiology, Biomarkers & Prevention 2010, 19, 2691–2709. [Google Scholar] [CrossRef]
- Botteri, E.; Iodice, S.; Bagnardi, V.; Raimondi, S.; Lowenfels, A.B.; Maisonneuve, P. Smoking and Colorectal Cancer: A Meta-analysis. JAMA 2008, 300, 2765. [Google Scholar] [CrossRef]
- Fedirko, V.; Tramacere, I.; Bagnardi, V.; Rota, M.; Scotti, L.; Islami, F.; Negri, E.; Straif, K.; Romieu, I.; La Vecchia, C.; et al. Alcohol Drinking and Colorectal Cancer Risk: An Overall and Dose–Response Meta-Analysis of Published Studies. Annals of Oncology 2011, 22, 1958–1972. [Google Scholar] [CrossRef]
- Galeone, C.; Turati, F.; La Vecchia, C.; Tavani, A. Coffee Consumption and Risk of Colorectal Cancer: A Meta-Analysis of Case–Control Studies. Cancer Causes & Control 2010, 21, 1949–1959. [Google Scholar] [CrossRef]
- Liang, P.S.; Chen, T.Y.; Giovannucci, E. Cigarette Smoking and Colorectal Cancer Incidence and Mortality: Systematic Review and Meta-analysis. International Journal of Cancer 2009, 124, 2406–2415. [Google Scholar] [CrossRef] [PubMed]
- LoConte, N.K.; Brewster, A.M.; Kaur, J.S.; Merrill, J.K.; Alberg, A.J. Alcohol and Cancer: A Statement of the American Society of Clinical Oncology. Journal of Clinical Oncology 2018, 36, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Mctiernan, A.; Friedenreich, C.M.; Katzmarzyk, P.T.; Powell, K.E.; Macko, R.; Buchner, D.; Pescatello, L.S.; Bloodgood, B.; Tennant, B.; Vaux-Bjerke, A.; et al. Physical Activity in Cancer Prevention and Survival: A Systematic Review. Medicine & Science in Sports & Exercise 2019, 51, 1252–1261. [Google Scholar] [CrossRef]
- Toma, M.; Beluşică, L.; Stavarachi, M.; Apostol, P.; Spandole, S.; Radu, I.; Cimponeriu, D. Rating the environmental and genetic risk factors for colorectal cancer. Journal of medicine and life 2012, 5, 152. [Google Scholar]
- Goy, J.; Rosenberg, M.W.; King, W.D. Health risk behaviors: examining social inequalities in bladder and colorectal cancers. Annals of Epidemiology 2008, 18, 156–162. [Google Scholar] [CrossRef]
- Egeberg, R.; Halkjær, J.; Rottmann, N.; Hansen, L.; Holten, I. Social inequality and incidence of and survival from cancers of the colon and rectum in a population-based study in Denmark, 1994–2003. European Journal of Cancer 2008, 44, 1978–1988. [Google Scholar] [CrossRef]
- Benedix, F.; Kube, R.; Meyer, F.; Schmidt, U.; Gastinger, I.; Lippert, H. Comparison of 17,641 Patients With Right- and Left-Sided Colon Cancer: Differences in Epidemiology, Perioperative Course, Histology, and Survival. Diseases of the Colon & Rectum 2010, 53, 57–64. [Google Scholar] [CrossRef]
- Bonilla, C.E.; Montenegro, P.; O’Connor, J.M.; Hernando-Requejo, O.; Aranda, E.; Pinto Llerena, J.; Llontop, A.; Gallardo Escobar, J.; Díaz Romero, M.D.C.; Bautista Hernández, Y.; et al. Ibero-American Consensus Review and Incorporation of New Biomarkers for Clinical Practice in Colorectal Cancer. Cancers 2023, 15, 4373. [Google Scholar] [CrossRef]
- Patel, J.; Fong, M.; Jagosky, M. Colorectal Cancer Biomarkers in the Era of Personalized Medicine. Journal of Personalized Medicine 2019, 9, 3. [Google Scholar] [CrossRef]
- Patel, A.; Gulhati, P. Molecular Landscape and Therapeutic Strategies against Colorectal Cancer. Cancers 2024, 16, 1551. [Google Scholar] [CrossRef] [PubMed]
- Alfahed, A. Molecular Pathology of Colorectal Cancer: The Saudi Situation in Perspective. Saudi Medical Journal 2023, 44, 836–847. [Google Scholar] [CrossRef] [PubMed]
- Cai, X.; Gu, D.; Chen, M.; Liu, L.; Chen, D.; Lu, L.; Gao, M.; Ye, X.; Jin, X.; Xie, C. The Effect of the Primary Tumor Location on the Survival of Colorectal Cancer Patients after Radical Surgery. International Journal of Medical Sciences 2018, 15, 1640–1647. [Google Scholar] [CrossRef]
- Alexander, P.G.; McMillan, D.C.; Park, J.H. The Local Inflammatory Response in Colorectal Cancer – Type, Location or Density? A Systematic Review and Meta-Analysis. Cancer Treatment Reviews 2020, 83, 101949. [Google Scholar] [CrossRef] [PubMed]
- Almangush, A.; Youssef, O.; Pirinen, M.; Sundström, J.; Leivo, I.; Mäkitie, A.A. Does Evaluation of Tumour Budding in Diagnostic Biopsies Have a Clinical Relevance? A Systematic Review. Histopathology 2019, 74, 536–544. [Google Scholar] [CrossRef]
- Almangush, A.; Karhunen, M.; Hautaniemi, S.; Salo, T.; Leivo, I. Prognostic Value of Tumour Budding in Oesophageal Cancer: A Meta-Analysis. Histopathology 2016, 68, 173–182. [Google Scholar] [CrossRef] [PubMed]
- Benedix, F.; Schmidt, U.; Mroczkowski, P.; Gastinger, I.; Lippert, H.; Kube, R. Colon Carcinoma – Classification into Right and Left Sided Cancer or According to Colonic Subsite? – Analysis of 29 568 Patients. European Journal of Surgical Oncology (EJSO) 2011, 37, 134–139. [Google Scholar] [CrossRef]
- Benson, A.B.; Hunt, S.; Nurkin, S. NCCN Guidelines Index Table of Contents Discussion, 2024.
- Blank, A.; Schenker, C.; Dawson, H.; Beldi, G.; Zlobec, I.; Lugli, A. Evaluation of Tumor Budding in Primary Colorectal Cancer and Corresponding Liver Metastases Based on H&E and Pancytokeratin Staining. Frontiers in Medicine 2019, 6, 247. [Google Scholar] [CrossRef]
- Breivik, J.; Lothe, R.A.; Meling, G.I.; Rognum, T.O.; Børresen-Dale, A.L.; Gaudernack, G. Different Genetic Pathways to Proximal and Distal Colorectal Cancer Influenced by Sex-Related Factors. International Journal of Cancer 1997, 74, 664–669. [Google Scholar] [CrossRef]
- Bufill, J.A. Colorectal Cancer: Evidence for Distinct Genetic Categories Based on Proximal or Distal Tumor Location. Annals of Internal Medicine 1990, 113, 779. [Google Scholar] [CrossRef]
- Coleman, W.B.; Tsongalis, G.J. (Eds.) Molecular Pathology: The Molecular Basis of Human Disease, second edition ed.; Academic Press: Amsterdam, 2018. [Google Scholar]
- Deb, B.; Jacob, S. Predictive Power of Tumour Budding for Lymph Node Metastasis in Colorectal Carcinomas: A Retrospective Study. Indian Journal of Medical Research 2019, 150, 635. [Google Scholar] [CrossRef] [PubMed]
- Ettarh, R. Colorectal Cancer Biology: From Genes to Tumor; BoD–Books on Demand, 2012.
- Felton, J.; Cheng, K.; Shang, A.C.; Hu, S.; Larabee, S.M.; Drachenberg, C.B.; Raufman, J.P. Two Sides to Colon Cancer: Mice Mimic Human Anatomical Region Disparity in Colon Cancer Development and Progression. Journal of Cancer Metastasis and Treatment 2018, 4, 51. [Google Scholar] [CrossRef]
- Fujiyoshi, K.; Väyrynen, J.P.; Borowsky, J.; Papke, D.J.; Arima, K.; Haruki, K.; Kishikawa, J.; Akimoto, N.; Ugai, T.; Lau, M.C.; et al. Tumour Budding, Poorly Differentiated Clusters, and T-cell Response in Colorectal Cancer. EBioMedicine 2020, 57, 102860. [Google Scholar] [CrossRef] [PubMed]
- Galon, J.; Costes, A.; Sanchez-Cabo, F.; Kirilovsky, A.; Mlecnik, B.; Lagorce-Pagès, C.; Tosolini, M.; Camus, M.; Berger, A.; Wind, P.; et al. Type, Density, and Location of Immune Cells within Human Colorectal Tumors Predict Clinical Outcome. Science (New York, N.Y.) 2006, 313, 1960–1964. [Google Scholar] [CrossRef]
- Galon, J.; Pagès, F.; Marincola, F.M.; Thurin, M.; Trinchieri, G.; Fox, B.A.; Gajewski, T.F.; Ascierto, P.A. The Immune Score as a New Possible Approach for the Classification of Cancer. Journal of Translational Medicine 2012, 10, 1. [Google Scholar] [CrossRef]
- Haddad, T.S.; Lugli, A.; Aherne, S.; Barresi, V.; Terris, B.; Bokhorst, J.M.; Brockmoeller, S.F.; Cuatrecasas, M.; Simmer, F.; El-Zimaity, H.; et al. Improving Tumor Budding Reporting in Colorectal Cancer: A Delphi Consensus Study. Virchows Archiv 2021, 479, 459–469. [Google Scholar] [CrossRef] [PubMed]
- J Ross, P.; Srikandarajah, K.; de Naurois, J.; Guy’s Cancer Centre, Guy’s and St Thomas’ NHS Foundation Trust, Management Offices, 4th Floor Bermondsey Wing, Great Maze Pond, London SE1 9RT. Right versus Left-Sided Colon Cancer: Is It Time to Consider These as Different Diseases? AIMS Medical Science 2018, 5, 303–315. [Google Scholar] [CrossRef]
- Jäger, T.; Neureiter, D.; Fallaha, M.; Schredl, P.; Kiesslich, T.; Urbas, R.; Klieser, E.; Holzinger, J.; Sedlmayer, F.; Emmanuel, K.; et al. The Potential Predictive Value of Tumor Budding for Neoadjuvant Chemoradiotherapy Response in Locally Advanced Rectal Cancer. Strahlentherapie Und Onkologie: Organ Der Deutschen Rontgengesellschaft ... [et Al] 2018, 194, 991–1006. [Google Scholar] [CrossRef] [PubMed]
- Jurescu, A.; Dema, A.; Văduva, A.; Gheju, A.; Vita, O.; Barna, R.; Lăzureanu, C.; Cornianu, M.; Tăban, S.; Dută, C.; et al. Poorly Differentiated Clusters and Tumor Budding Are Important Prognostic Factors in Colorectal Carcinomas. Bosnian Journal of Basic Medical Sciences 2021. [Google Scholar] [CrossRef]
- Kang, G.; Pyo, J.S.; Kim, N.Y.; Kang, D.W. Clinicopathological Significances and Prognostic Role of Intratumoral Budding in Colorectal Cancers. Journal of Clinical Medicine 2022, 11, 5540. [Google Scholar] [CrossRef]
- Lugli, A.; Kirsch, R.; Ajioka, Y.; Bosman, F.; Cathomas, G.; Dawson, H.; El Zimaity, H.; Fléjou, J.F.; Hansen, T.P.; Hartmann, A.; et al. Recommendations for Reporting Tumor Budding in Colorectal Cancer Based on the International Tumor Budding Consensus Conference (ITBCC) 2016. Modern Pathology 2017, 30, 1299–1311. [Google Scholar] [CrossRef] [PubMed]
- Saito, K.; Okuyama, T.; Miyazaki, S.; Oi, H.; Mitsui, T.; Noro, T.; Takeshita, E.; Ono, Y.; Urahashi, T.; Tajima, H.; et al. Tumor Budding as a Predictive Marker of Relapse and Survival in Patients With Stage II Colon Cancer. In Vivo 2022, 36, 1820–1828. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, S.; Guha, R.; Mukherjee, S.; Kundu, S.; Chakrabarti, S. Evaluation And Applicability Of Tumour Budding And Poorly Differentiated Clusters As Additional Prognostic Markers In Colorectal Cancers. Preprint, In Review, 2022. [CrossRef]
- Yahagi, M.; Okabayashi, K.; Hasegawa, H.; Tsuruta, M.; Kitagawa, Y. The Worse Prognosis of Right-Sided Compared with Left-Sided Colon Cancers: A Systematic Review and Meta-analysis. Journal of Gastrointestinal Surgery 2016, 20, 648–655. [Google Scholar] [CrossRef]
- Zhang, L.; Zhao, Y.; Dai, Y.; Cheng, J.N.; Gong, Z.; Feng, Y.; Sun, C.; Jia, Q.; Zhu, B. Immune Landscape of Colorectal Cancer Tumor Microenvironment from Different Primary Tumor Location. Frontiers in Immunology 2018, 9, 1578. [Google Scholar] [CrossRef]
- IARC. In WHO Classification of Tumours Editorial Board. Digestive System Tumours, 5th ed.; WHO Classification of Tumours Series; International Agency for Researchon Cancer, 2019; Volume 1.
- Knijn, N.; van Exsel, U.E.; de Noo, M.E.; Nagtegaal, I.D. The value of intramural vascular invasion in colorectal cancer–a systematic review and meta-analysis. Histopathology 2018, 72, 721–728. [Google Scholar] [CrossRef] [PubMed]
- Chand, M.; Siddiqui, M.R.; Swift, I.; Brown, G. Systematic review of prognostic importance of extramural venous invasion in rectal cancer. World journal of gastroenterology 2016, 22, 1721. [Google Scholar] [CrossRef]
- Kirsch, R.; Messenger, D.E.; Riddell, R.H.; Pollett, A.; Cook, M.; Al-Haddad, S.; Streutker, C.J.; Divaris, D.X.; Pandit, R.; Newell, K.J.; et al. Venous invasion in colorectal cancer: impact of an elastin stain on detection and interobserver agreement among gastrointestinal and nongastrointestinal pathologists. The American journal of surgical pathology 2013, 37, 200–210. [Google Scholar] [CrossRef]
- Liebig, C.; Ayala, G.; Wilks, J.A.; Berger, D.H.; Albo, D. Perineural invasion in cancer: a review of the literature. Cancer: Interdisciplinary International Journal of the American Cancer Society 2009, 115, 3379–3391. [Google Scholar] [CrossRef]
- Kishiki, T.; Kuchta, K.; Matsuoka, H.; Kojima, K.; Asou, N.; Beniya, A.; Yamauchi, S.; Sugihara, K.; Masaki, T. The Impact of Tumor Location on the Biological and Oncological Differences of Colon Cancer: Multi-institutional Propensity Score-Matched Study. The American Journal of Surgery 2019, 217, 46–52. [Google Scholar] [CrossRef]
- Des Guetz, G.; Schischmanoff, O.; Nicolas, P.; Perret, G.Y.; Morere, J.F.; Uzzan, B. Does Microsatellite Instability Predict the Efficacy of Adjuvant Chemotherapy in Colorectal Cancer? A Systematic Review with Meta-Analysis. European Journal of Cancer (Oxford, England: 1990) 2009, 45, 1890–1896. [Google Scholar] [CrossRef]
- Lee, G.; Malietzis, G.; Askari, A.; Bernardo, D.; Al-Hassi, H.; Clark, S. Is Right-Sided Colon Cancer Different to Left-Sided Colorectal Cancer? – A Systematic Review. European Journal of Surgical Oncology (EJSO) 2015, 41, 300–308. [Google Scholar] [CrossRef] [PubMed]
- Boland, C.R.; Goel, A. Microsatellite Instability in Colorectal Cancer. Gastroenterology 2010, 138, 2073–2087.e3. [Google Scholar] [CrossRef] [PubMed]
- Kopetz, S.; Lonardi, S.; McDermott, R.S.; Aglietta, M.; Hendlisz, A.; Morse, M.; Leach, J.W.; Neyns, B.; Chan, E.; Chen, F.; et al. Concordance of DNA Mismatch Repair Deficient (dMMR)/Microsatellite Instability (MSI) Assessment by Local and Central Testing in Patients with Metastatic CRC (mCRC) Receiving Nivolumab (Nivo) in CheckMate 142 Study. Journal of Clinical Oncology 2017, 35, 3548–3548. [Google Scholar] [CrossRef]
- Domingo, E.; Camps, C.; Kaisaki, P.J.; Parsons, M.J.; Mouradov, D.; Pentony, M.M.; Makino, S.; Palmieri, M.; Ward, R.L.; Hawkins, N.J.; et al. Mutation Burden and Other Molecular Markers of Prognosis in Colorectal Cancer Treated with Curative Intent: Results from the QUASAR 2 Clinical Trial and an Australian Community-Based Series. The Lancet Gastroenterology & Hepatology 2018, 3, 635–643. [Google Scholar] [CrossRef]
- Michel, M.; Kaps, L.; Maderer, A.; Galle, P.R.; Moehler, M. The role of p53 dysfunction in colorectal cancer and its implication for therapy. Cancers 2021, 13, 2296. [Google Scholar] [CrossRef]
Figure 1.
Age distribution by sex: t- test: t: 2.18; p: 0.0318; Df: 90.15
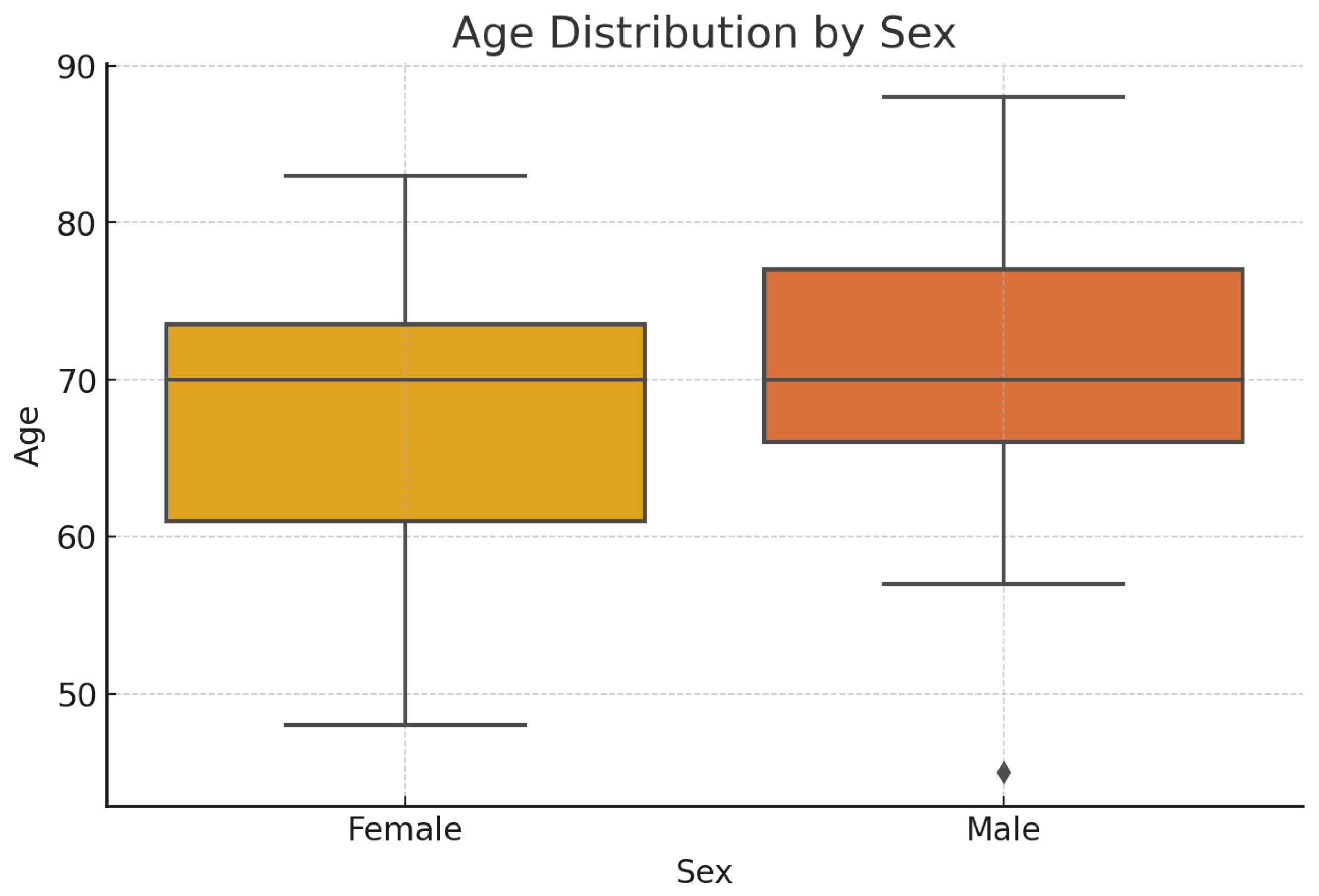
Figure 2.
Tumor localization distribution for the whole patient group(count)
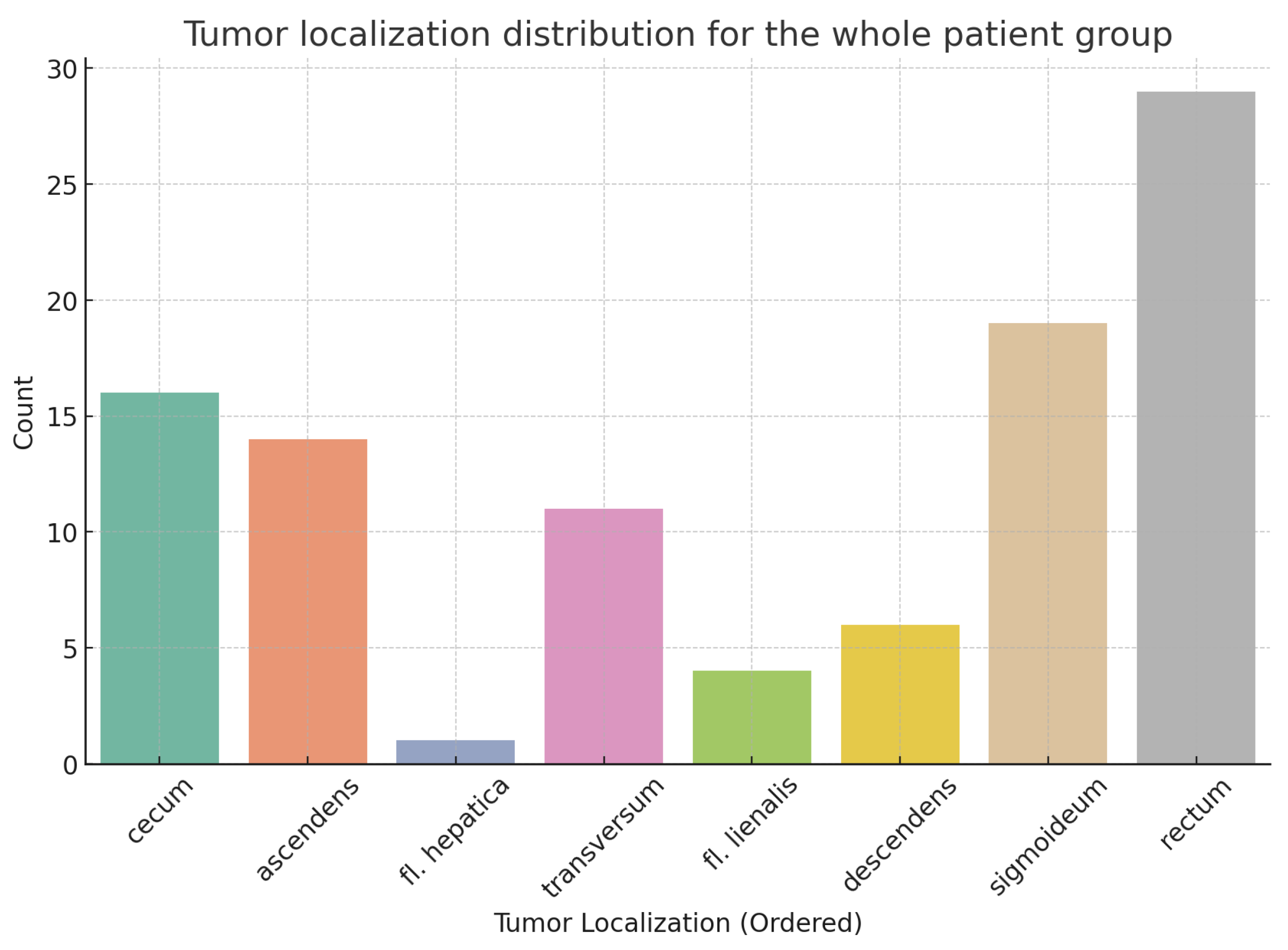
Figure 3.
Normalized tumor localization distribution by sex
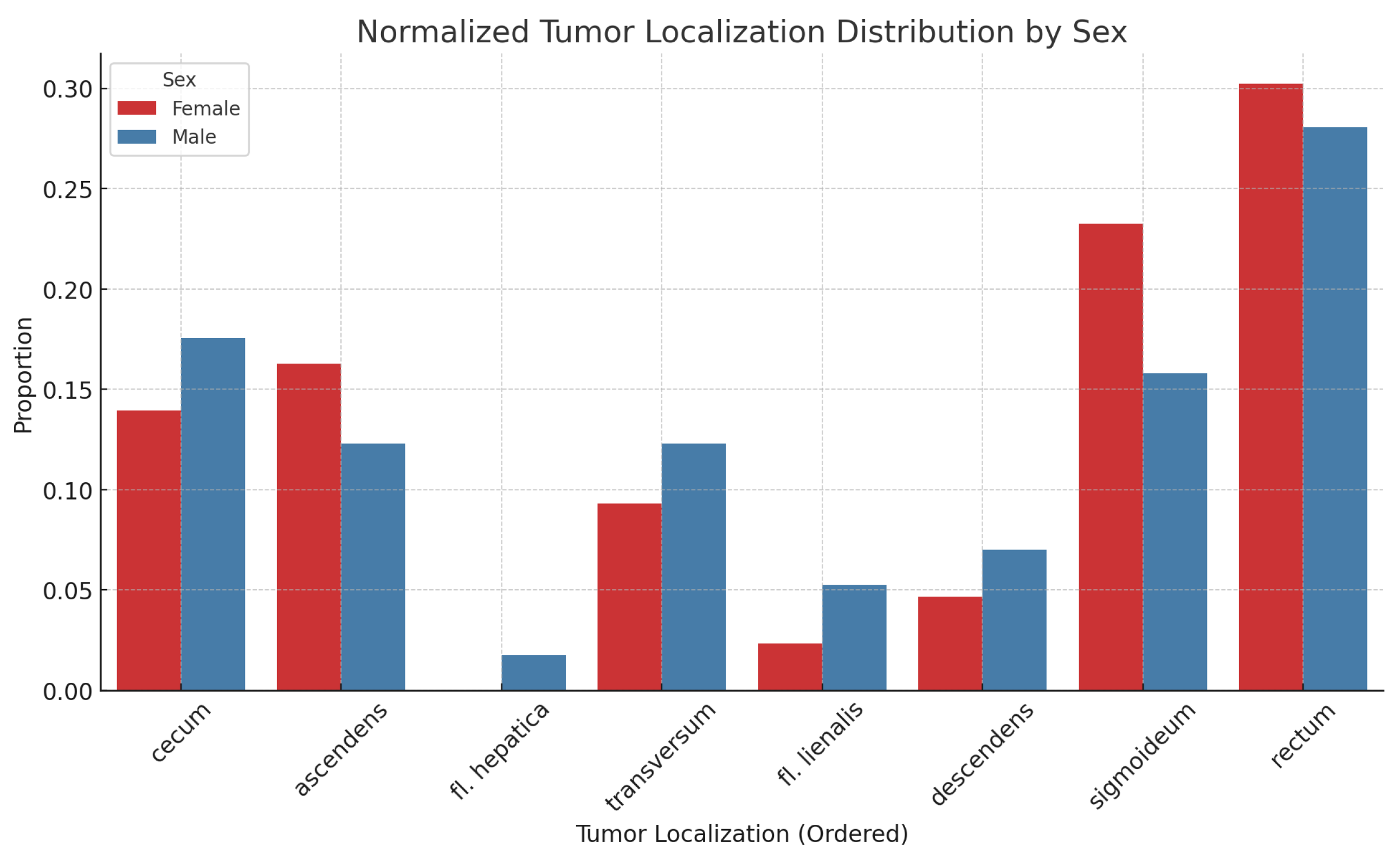
Figure 4.
Normalized simplified tumor localization groups: Right colon, Left colon, and Rectum
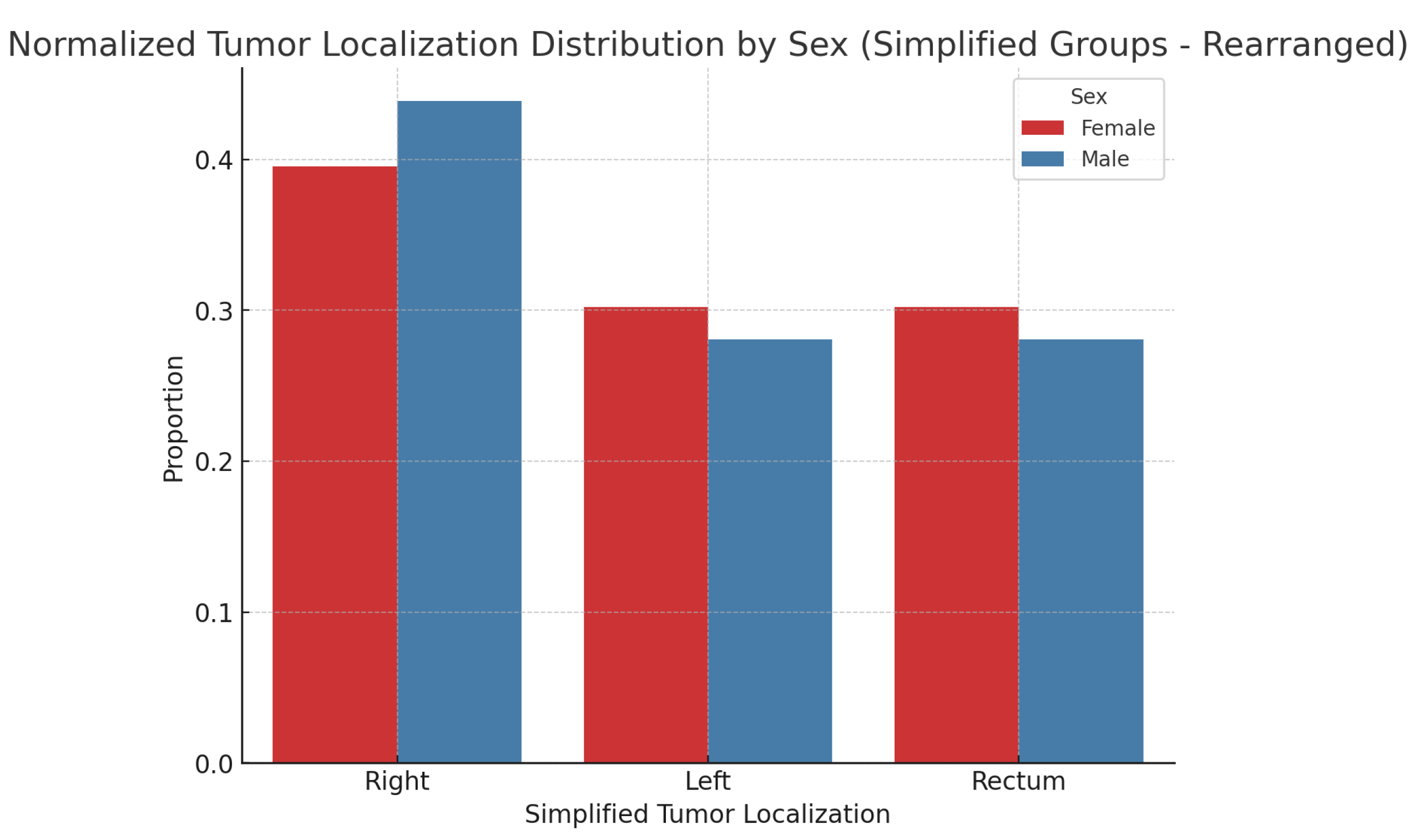
Figure 6.
Age distributions across the right colon, left colon, and rectum-females

Figure 7.
Age distributions across the right colon, left colon, and rectum-males
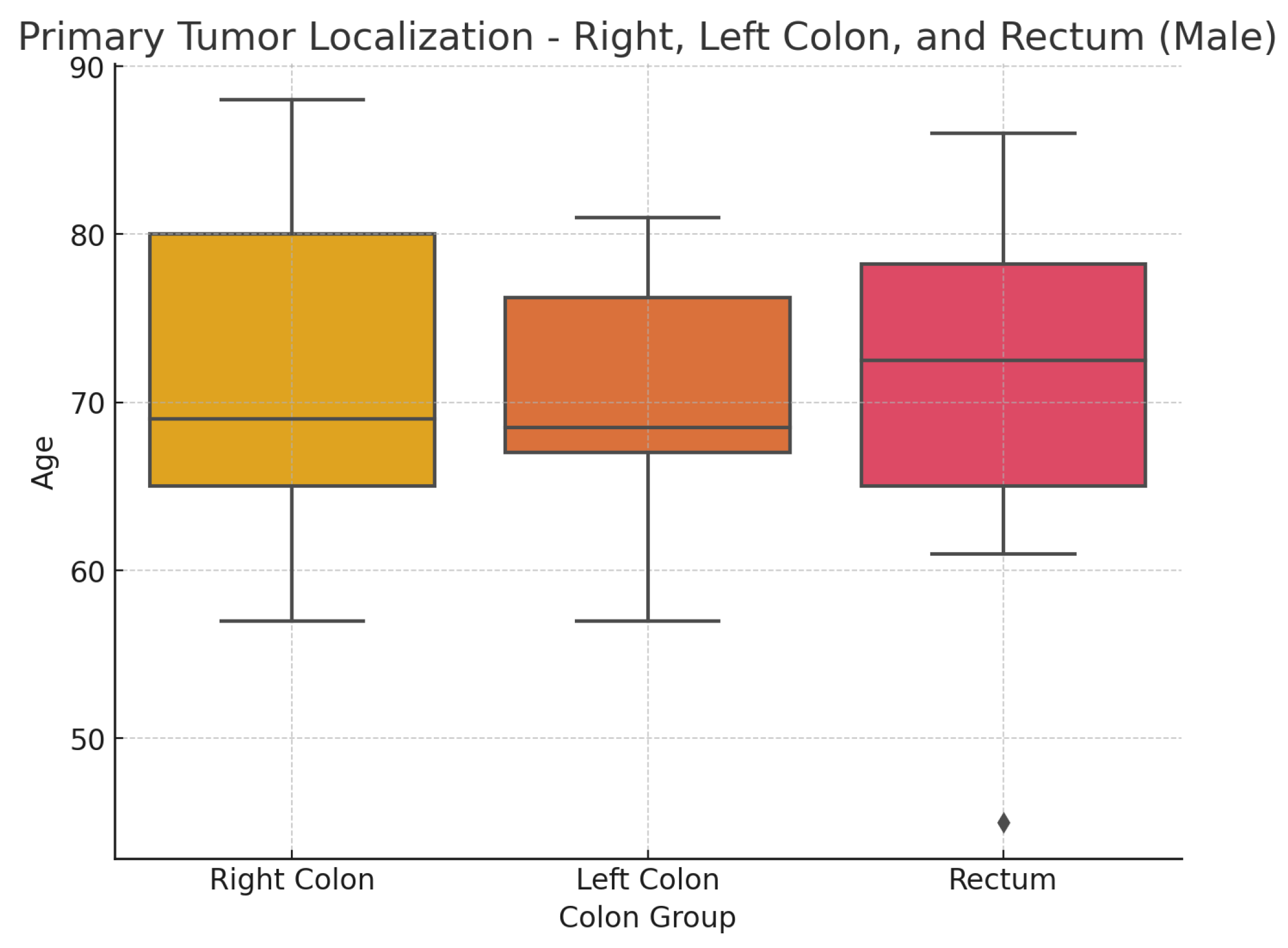
Figure 8.
Proportional distribution of histological subtypes by localization group (normalized)
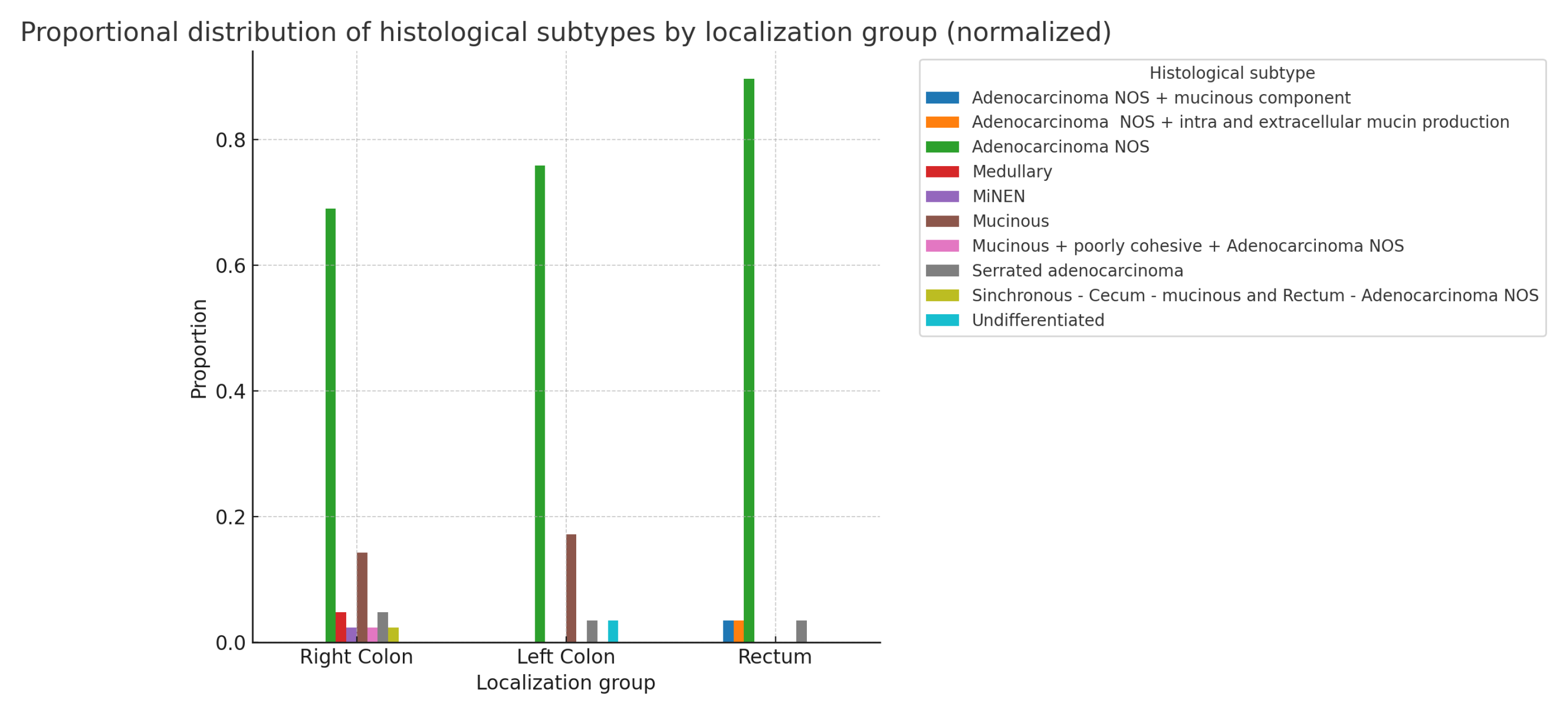
Figure 9.
Proportional distribution of grade by localization groups(: 9.107; p-value: 0.168; Df=6)
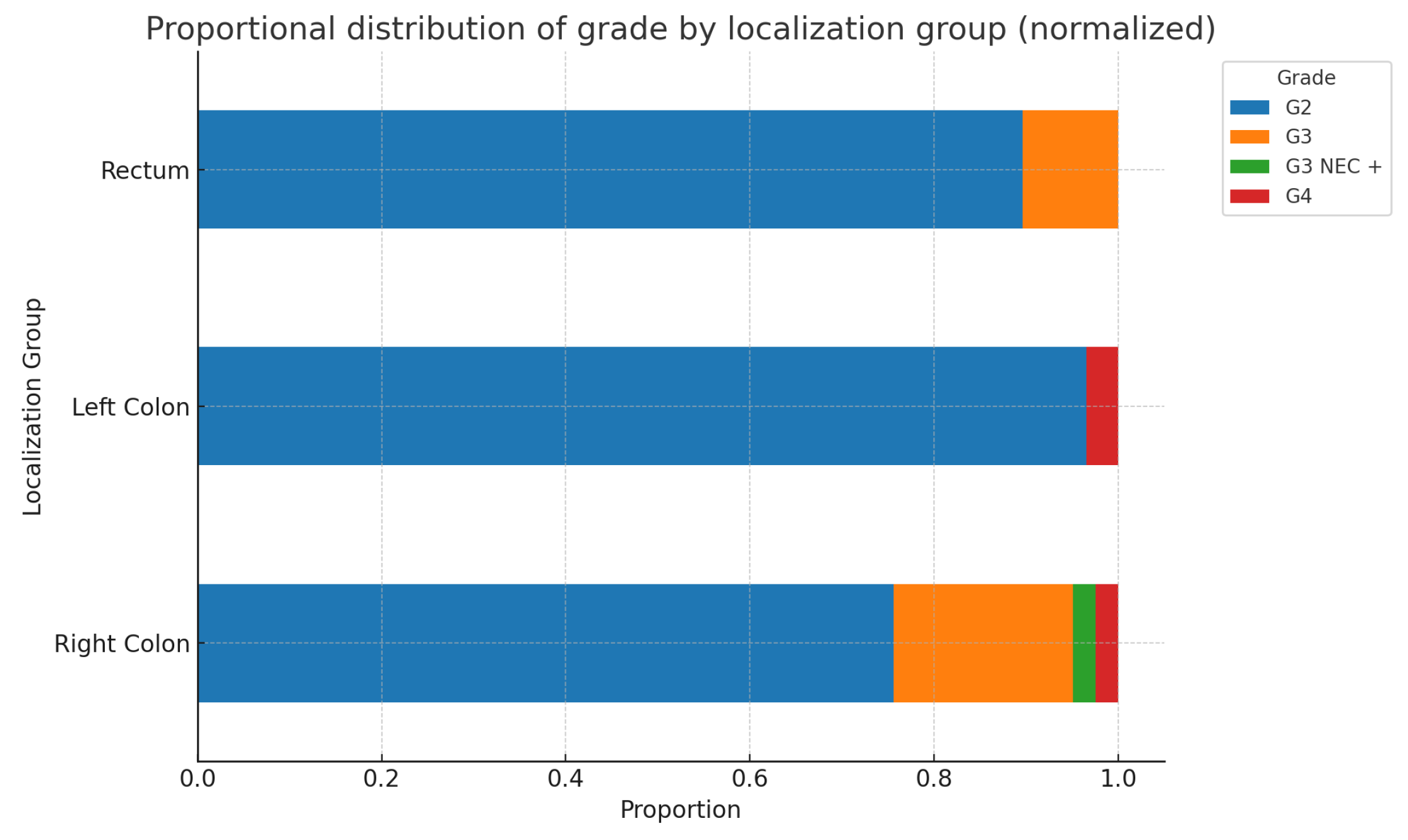
Figure 10.
Proportional distribution of stage by localization groups(: 15.248; p-value: 0.123; Df=10)
Figure 10.
Proportional distribution of stage by localization groups(: 15.248; p-value: 0.123; Df=10)
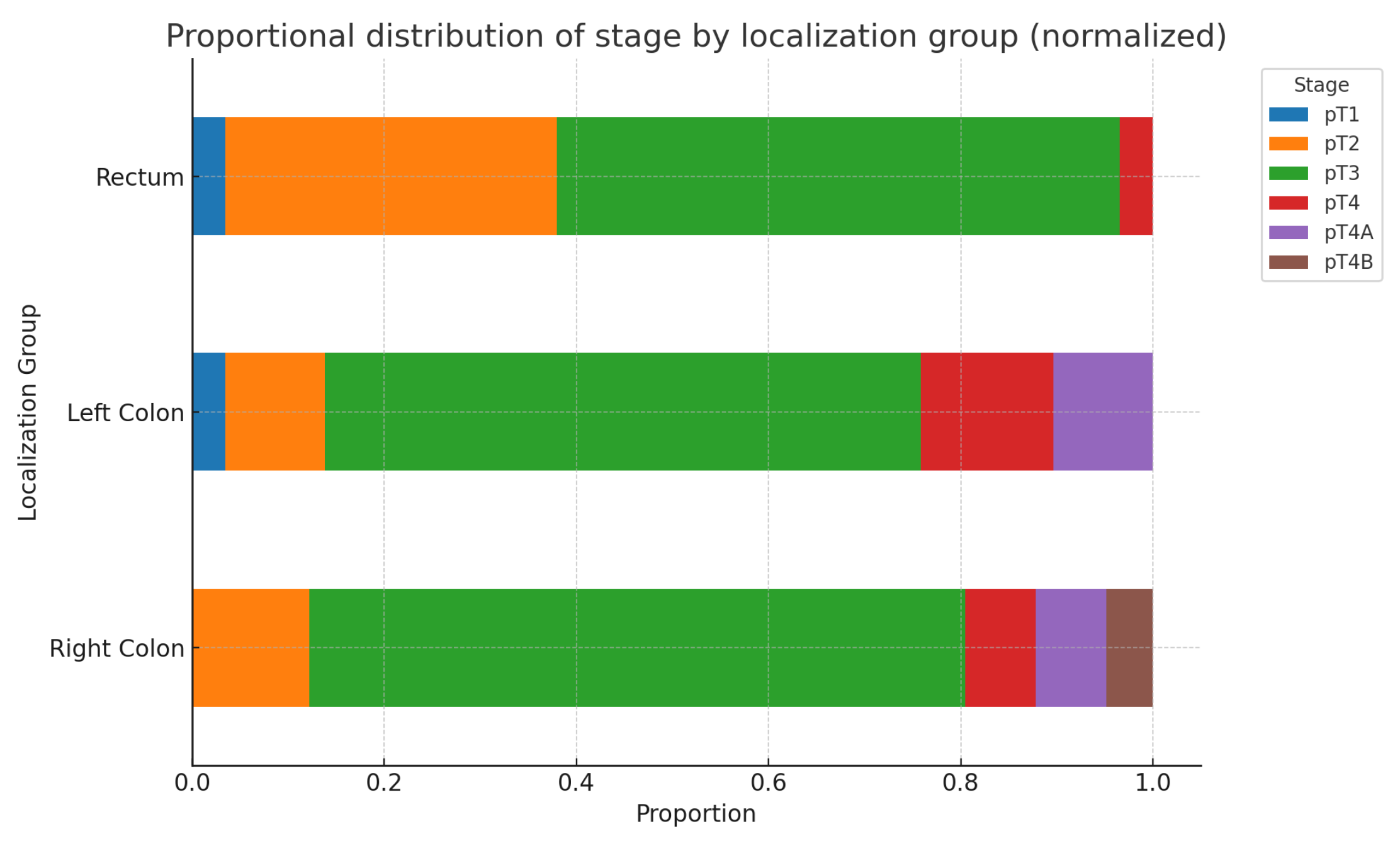
Figure 11.
Proportional distribution of G2, G3, and G4 within each stage
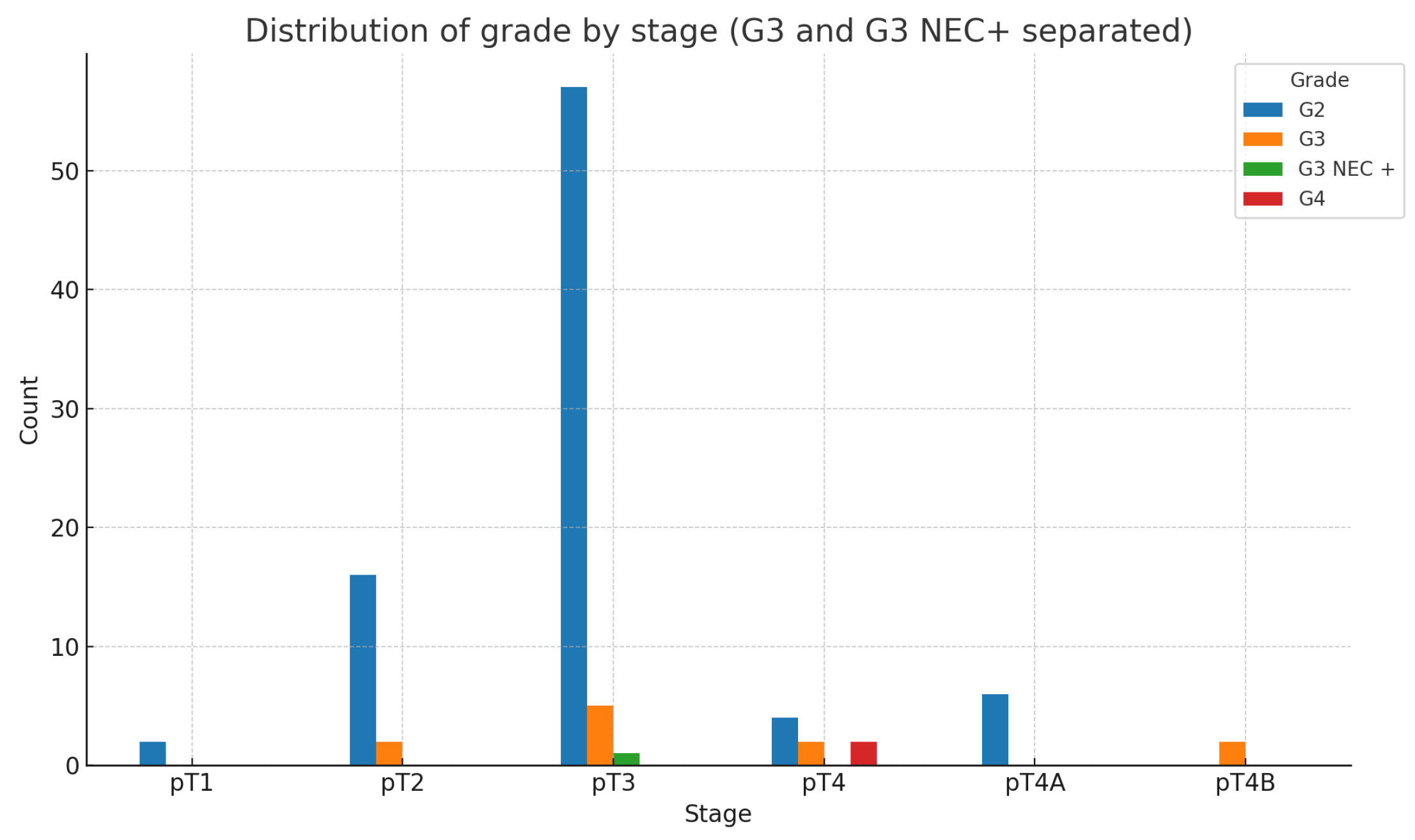
Figure 12.
N status and tumor localization- Right colon, Left colon, and Rectum(whole group count)
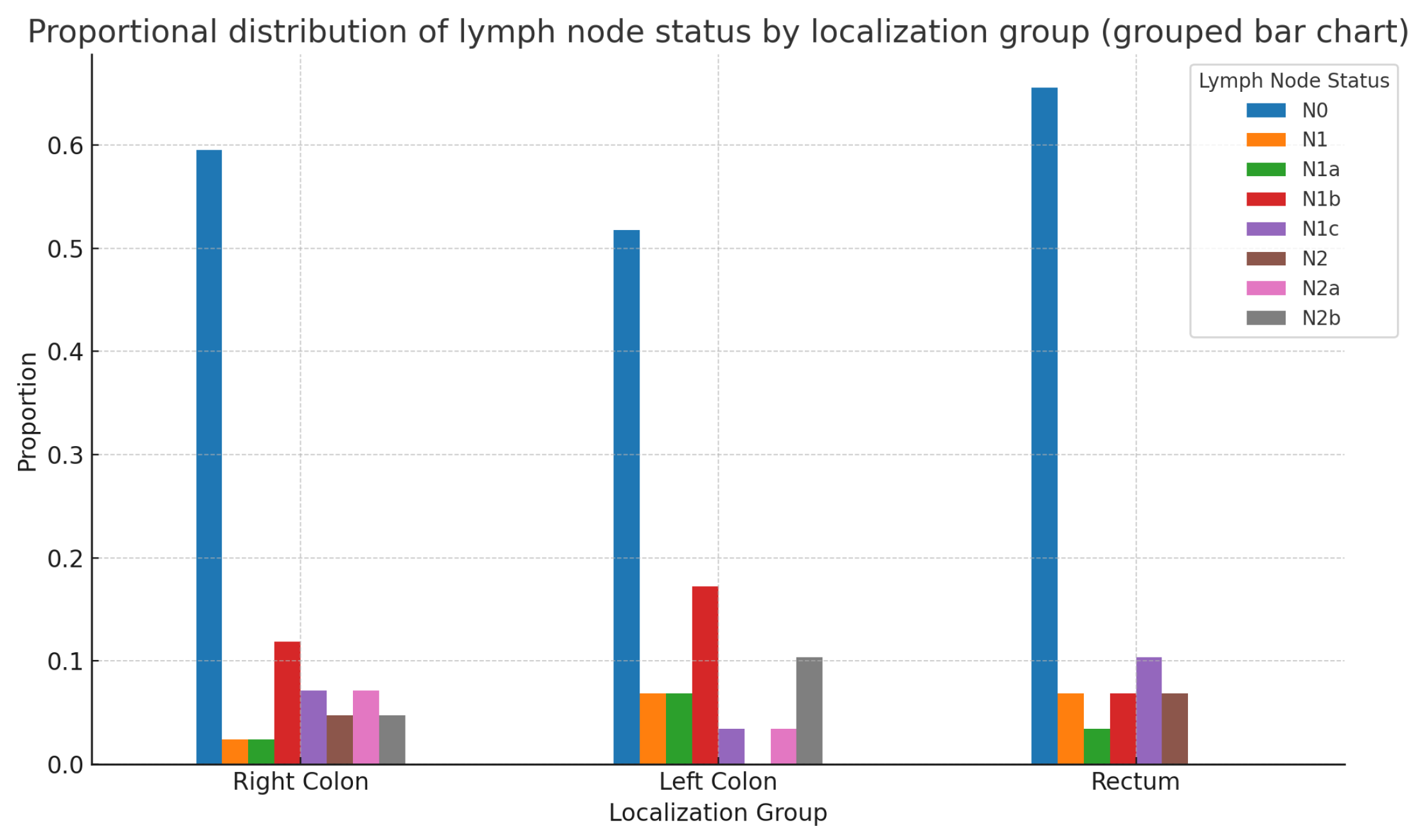
Figure 13.
LVI distribution for Right colon, Left colon, and Rectum

Figure 14.
Proportional LVI Distribution by Histological Subtype
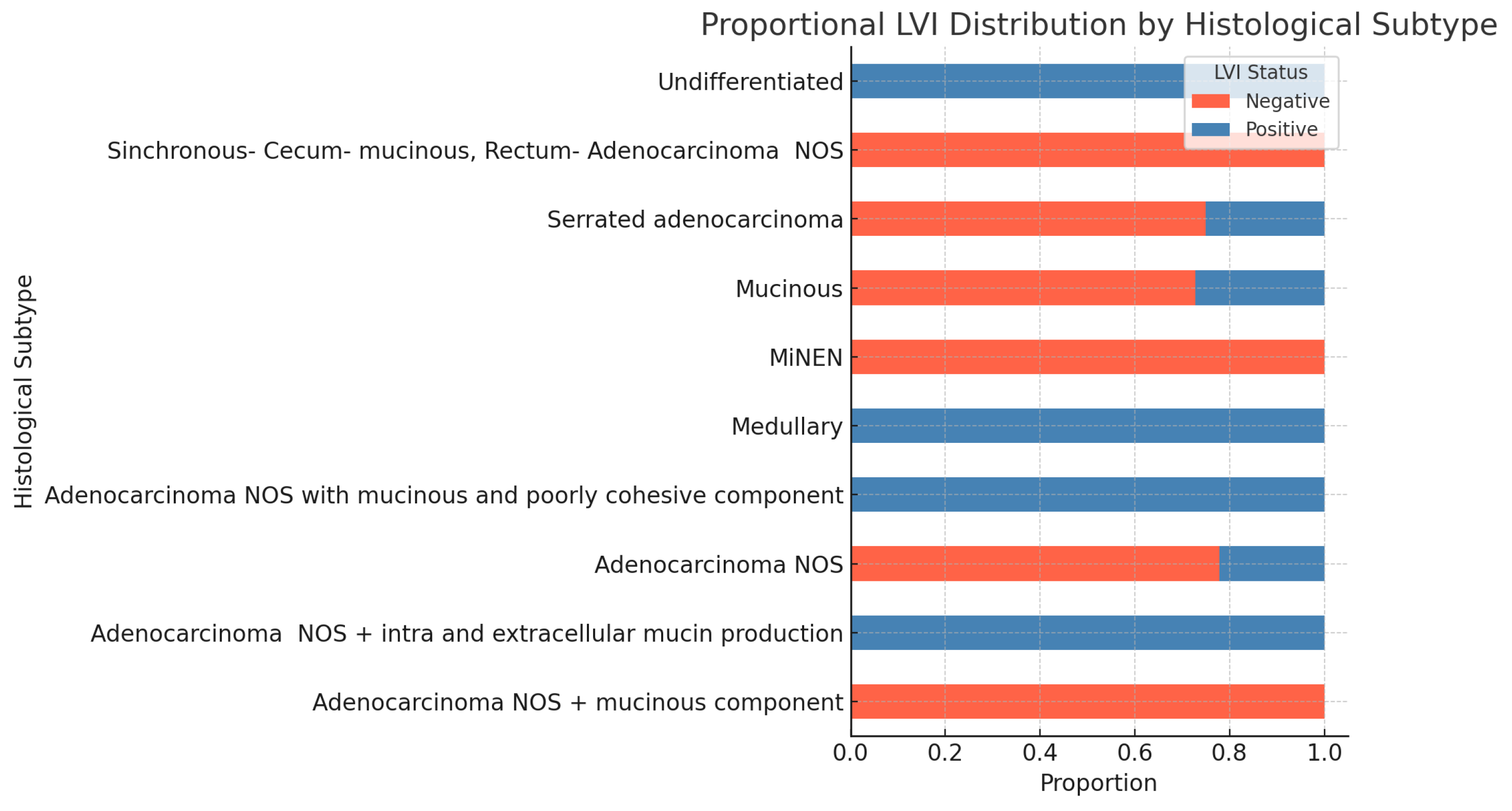
Figure 15.
Proportional distribution of LVI status across both tumor grade and tumor stage
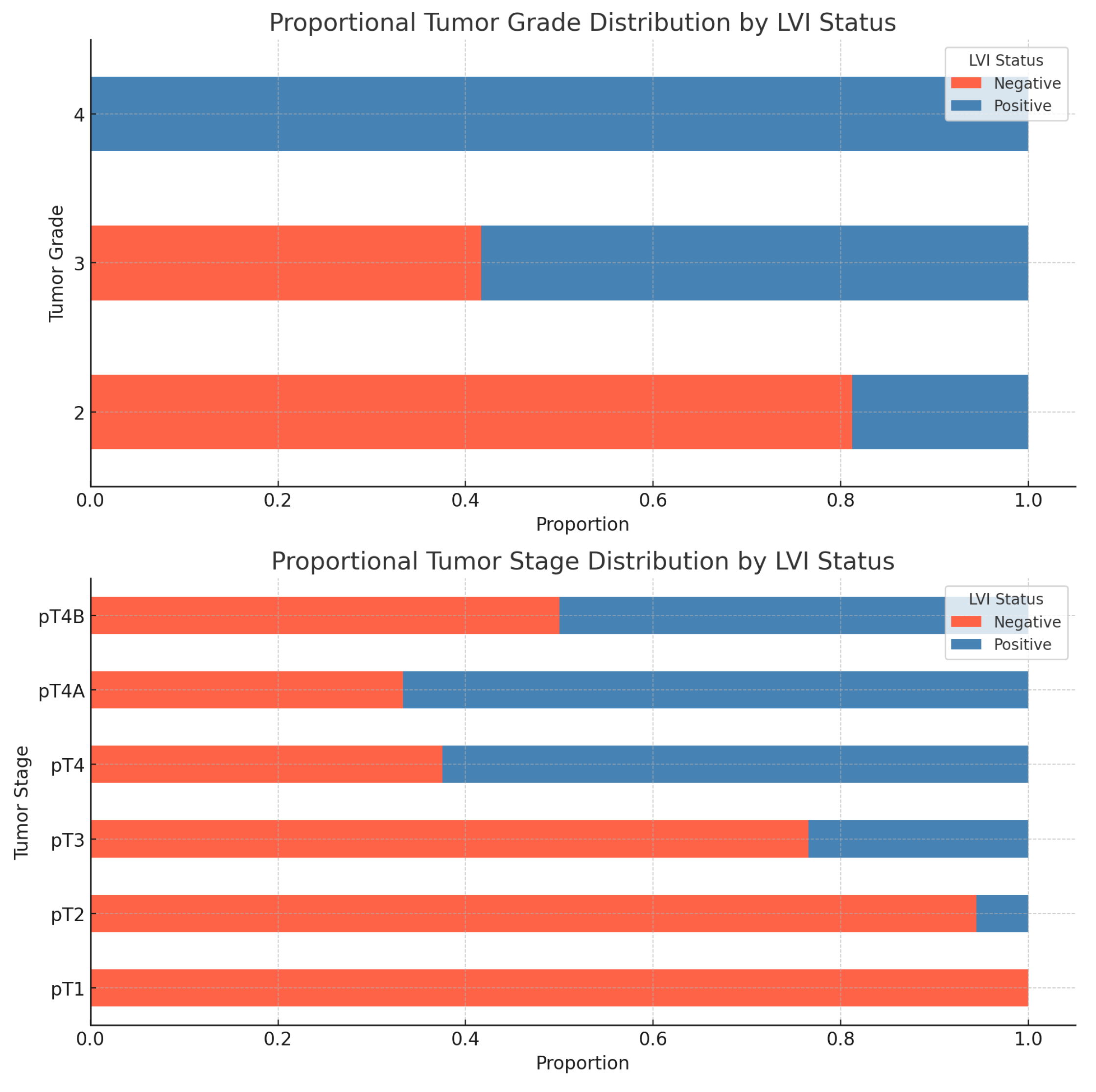
Figure 16.
Proportional distribution of Perineural Invasion (PNI) across the following variables: Primary tumor localization, Histological subtype, Tumor grade, Tumor stage.
Figure 16.
Proportional distribution of Perineural Invasion (PNI) across the following variables: Primary tumor localization, Histological subtype, Tumor grade, Tumor stage.
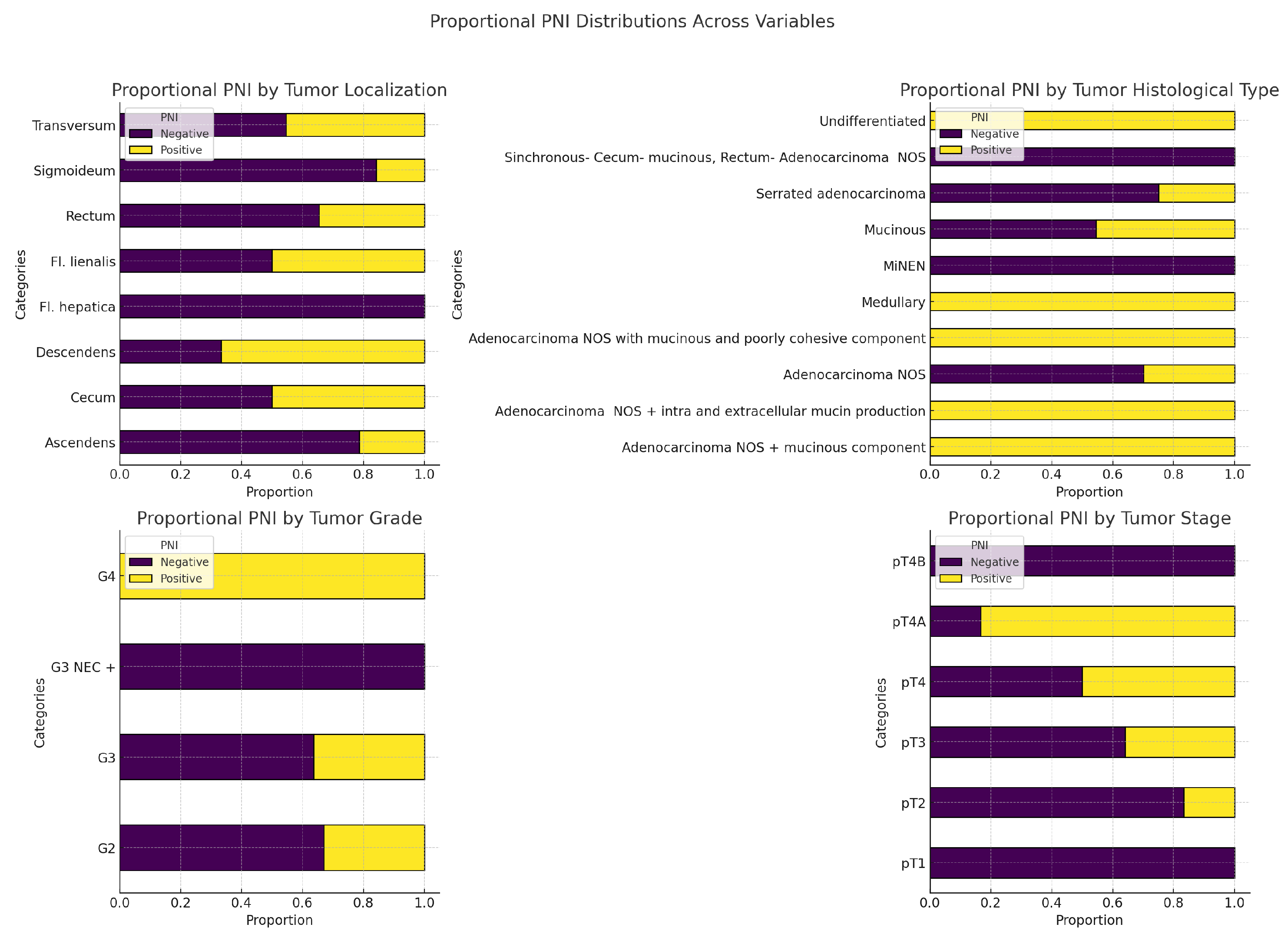
Figure 17.
Immune stromal reaction and primary tumor localization
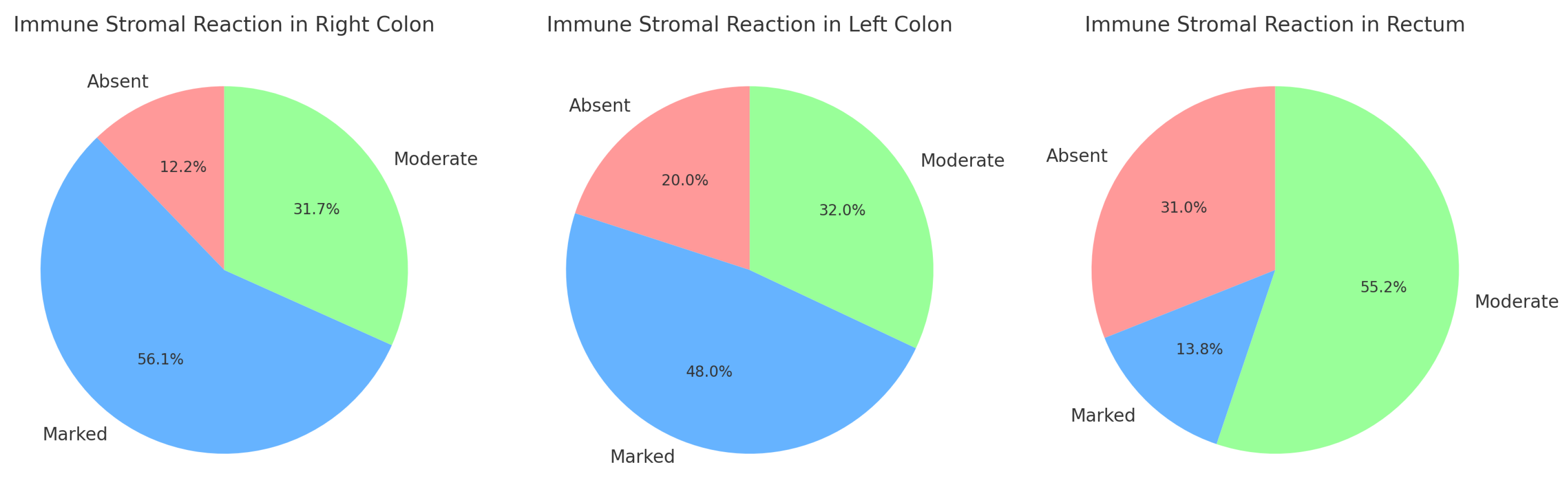
Figure 18.
Average peritumoral stromal reaction by histological subtype
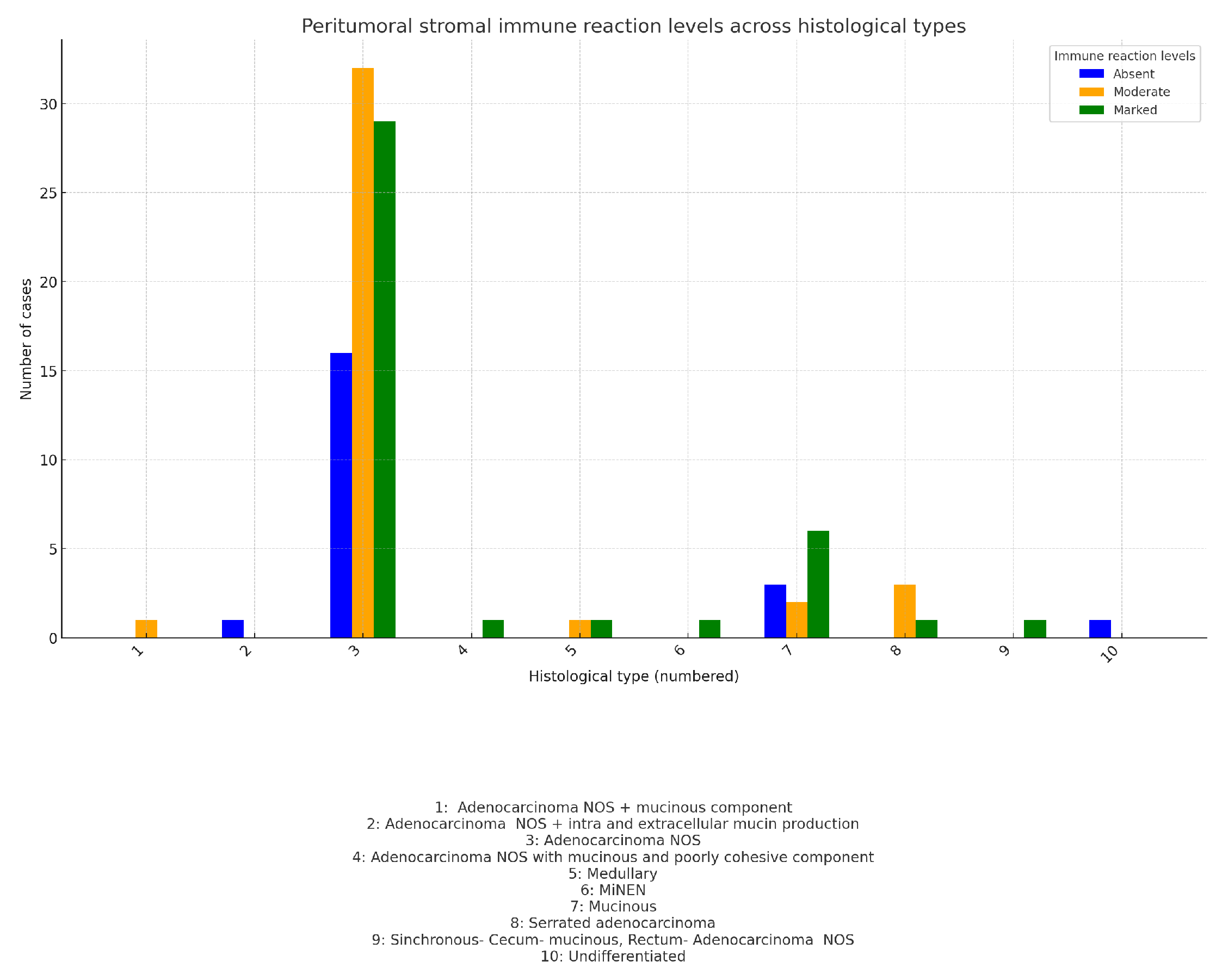
Figure 19.
Peritumoral stromal immune reaction vs lymphovascular invasion (LVI) and perineural invasion (PNI)
Figure 19.
Peritumoral stromal immune reaction vs lymphovascular invasion (LVI) and perineural invasion (PNI)
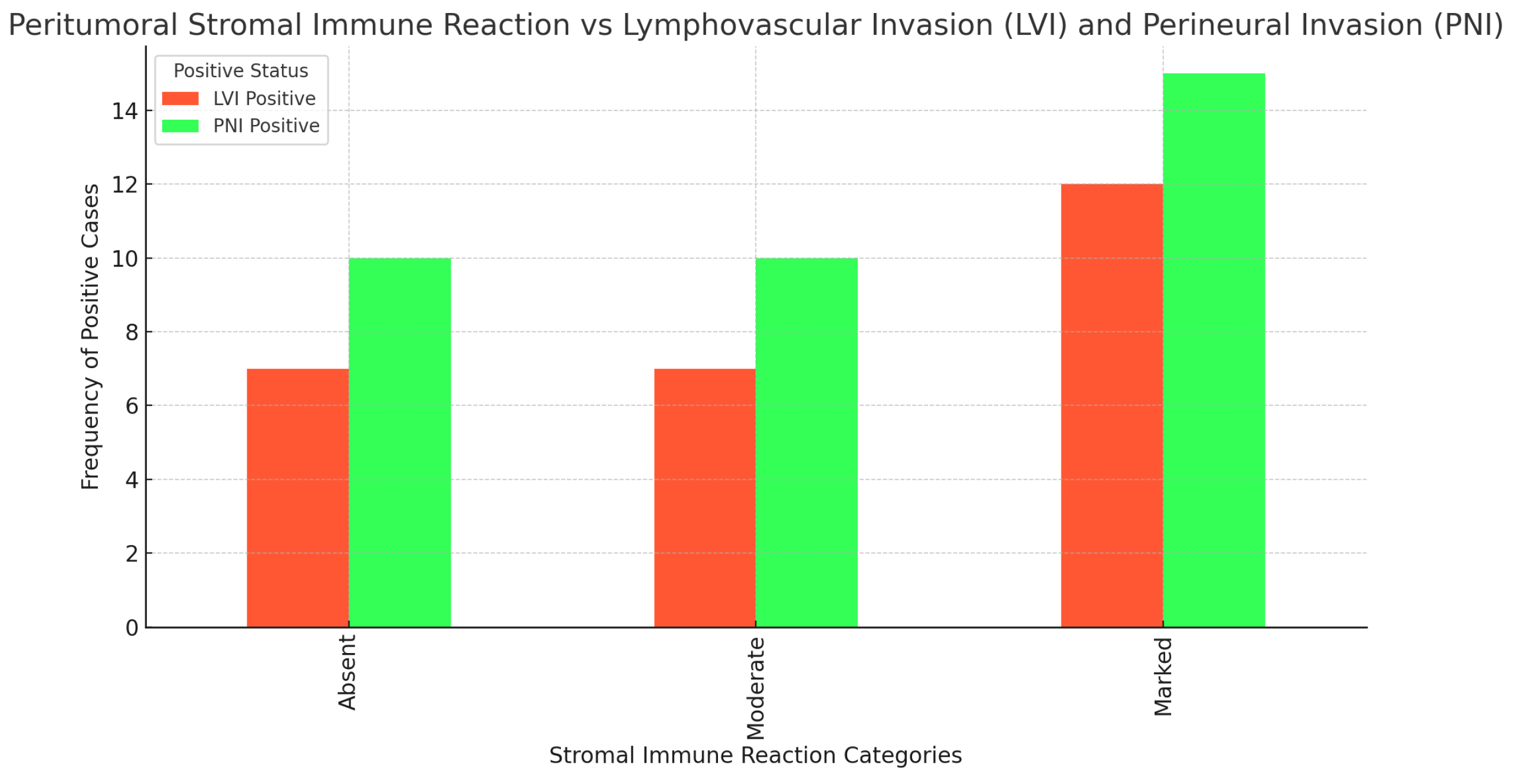
Figure 20.
Peritumoral budding distribution across tumor localizations (Bd0+Bd1 Combined)
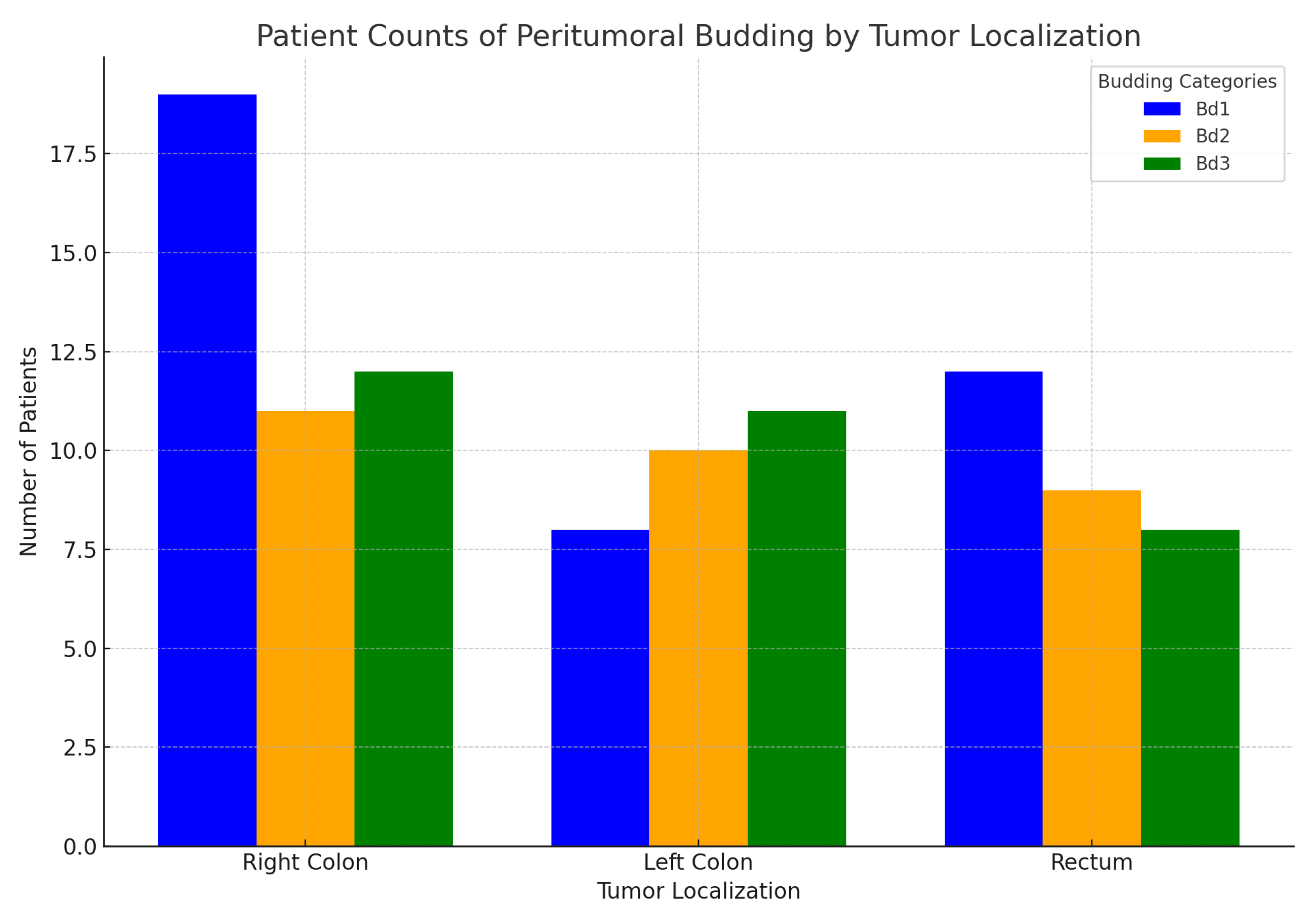
Figure 21.
Peritumoral budding distribution across tumor histological subtypes
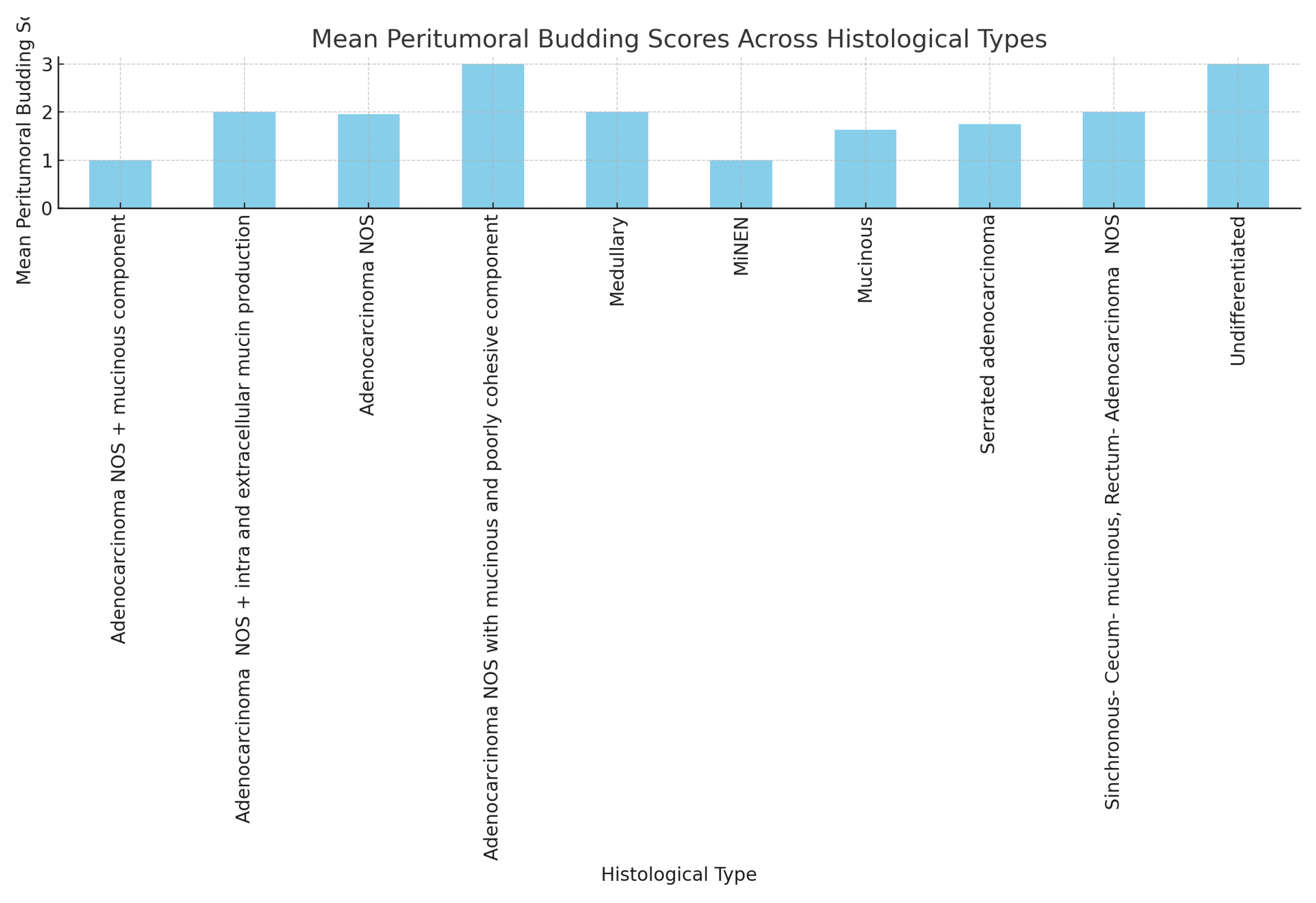
Figure 22.
Peritumoral budding and LVI
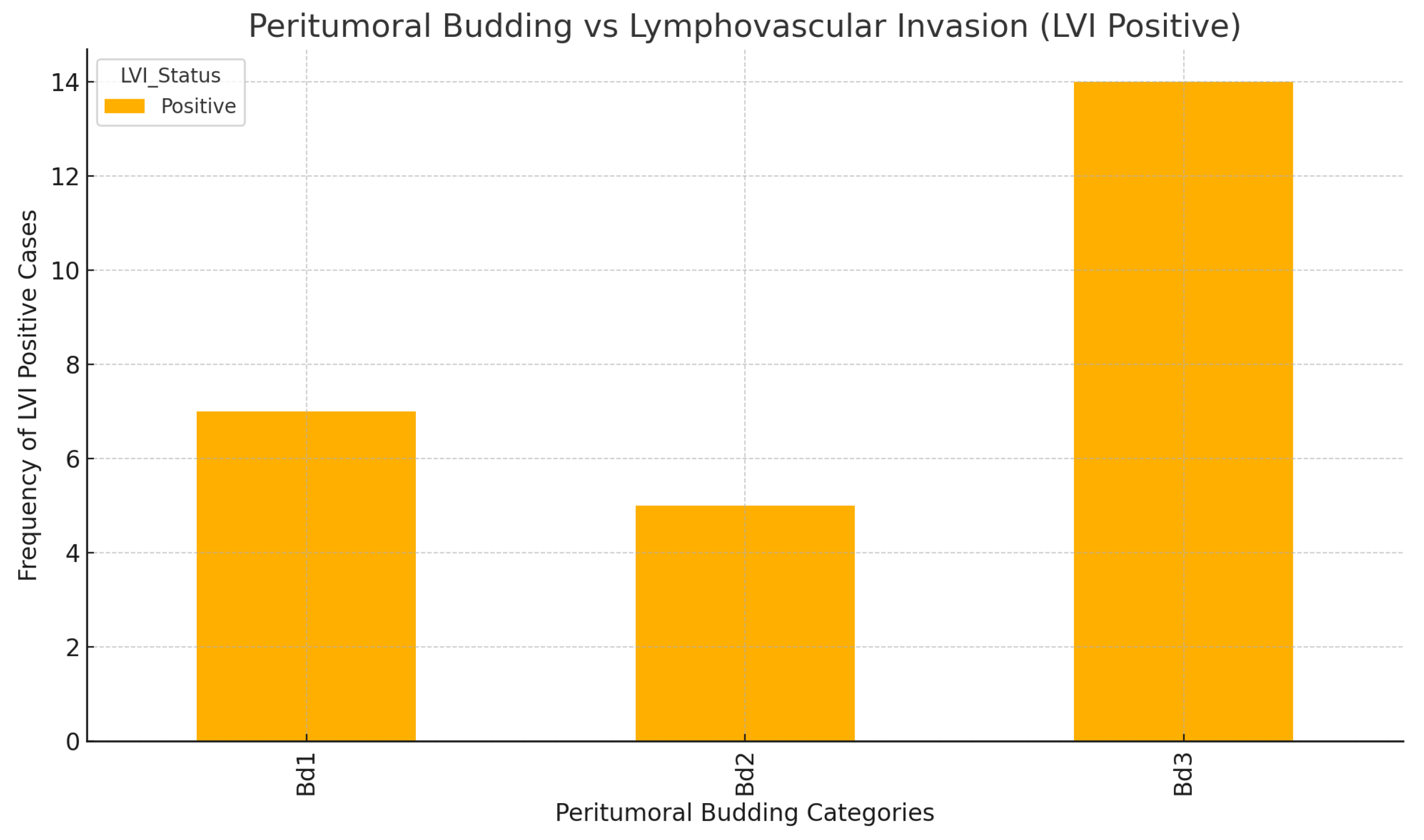
Figure 23.
MMR status and primary tumor localization
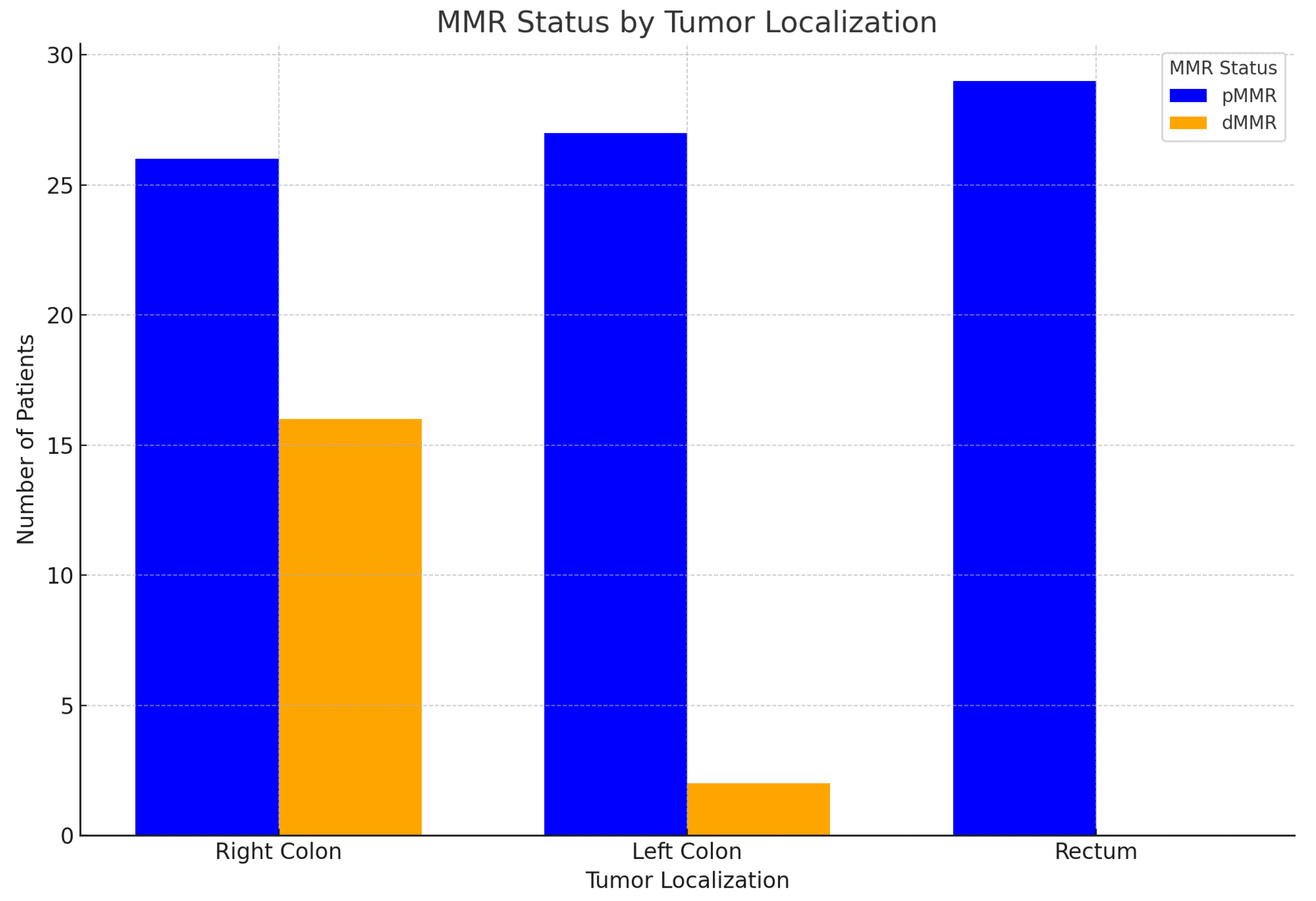
Figure 24.
MMR status and lymph node status: Chi-square value: 4.94; p-value: 0.667; Degrees of freedom: 7- there is no statistically significant association
Figure 24.
MMR status and lymph node status: Chi-square value: 4.94; p-value: 0.667; Degrees of freedom: 7- there is no statistically significant association
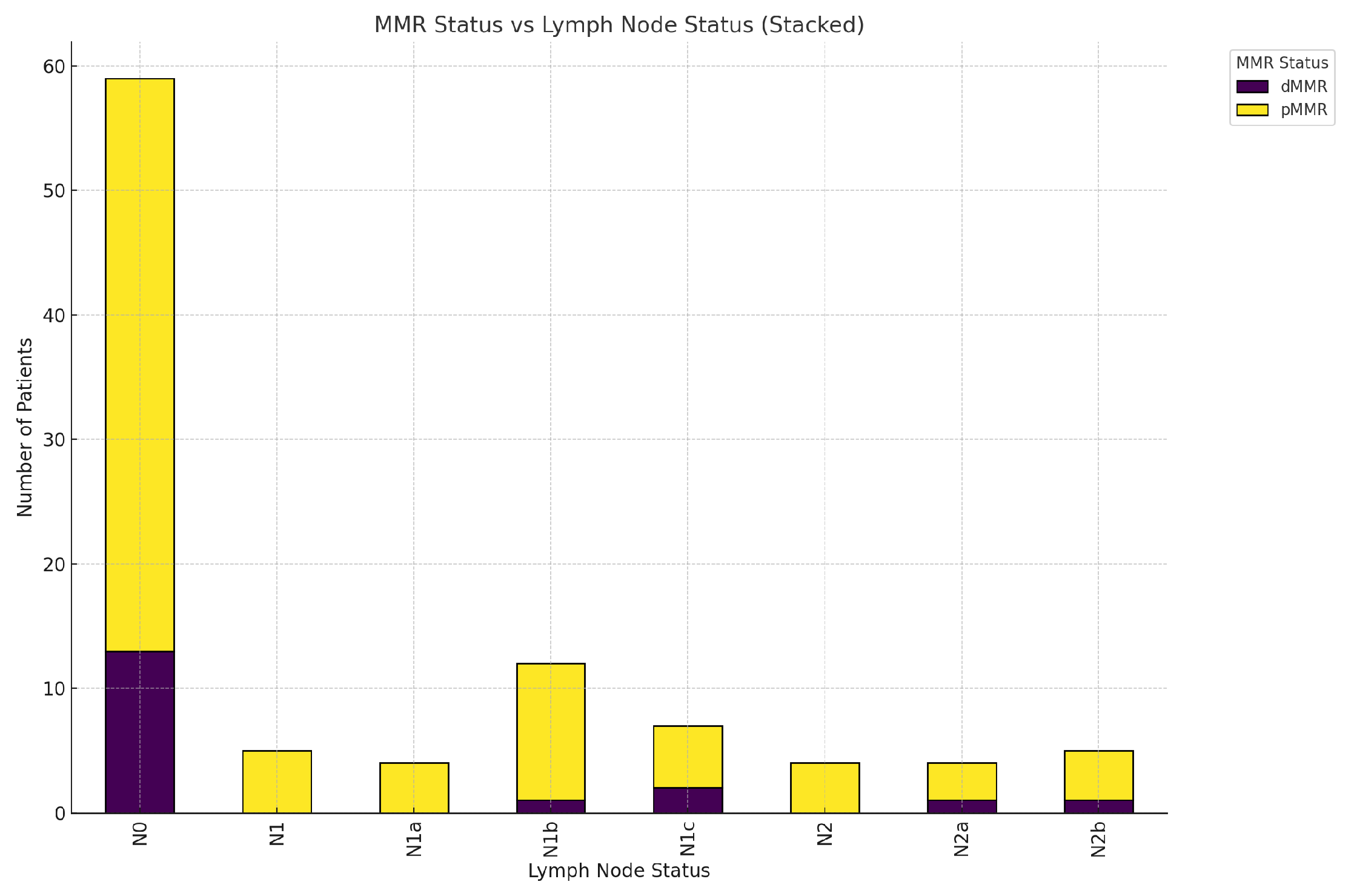
Figure 25.
Mutated genes distribution by primary tumor localization- Right colon, Left colon, and Rectum
Figure 25.
Mutated genes distribution by primary tumor localization- Right colon, Left colon, and Rectum
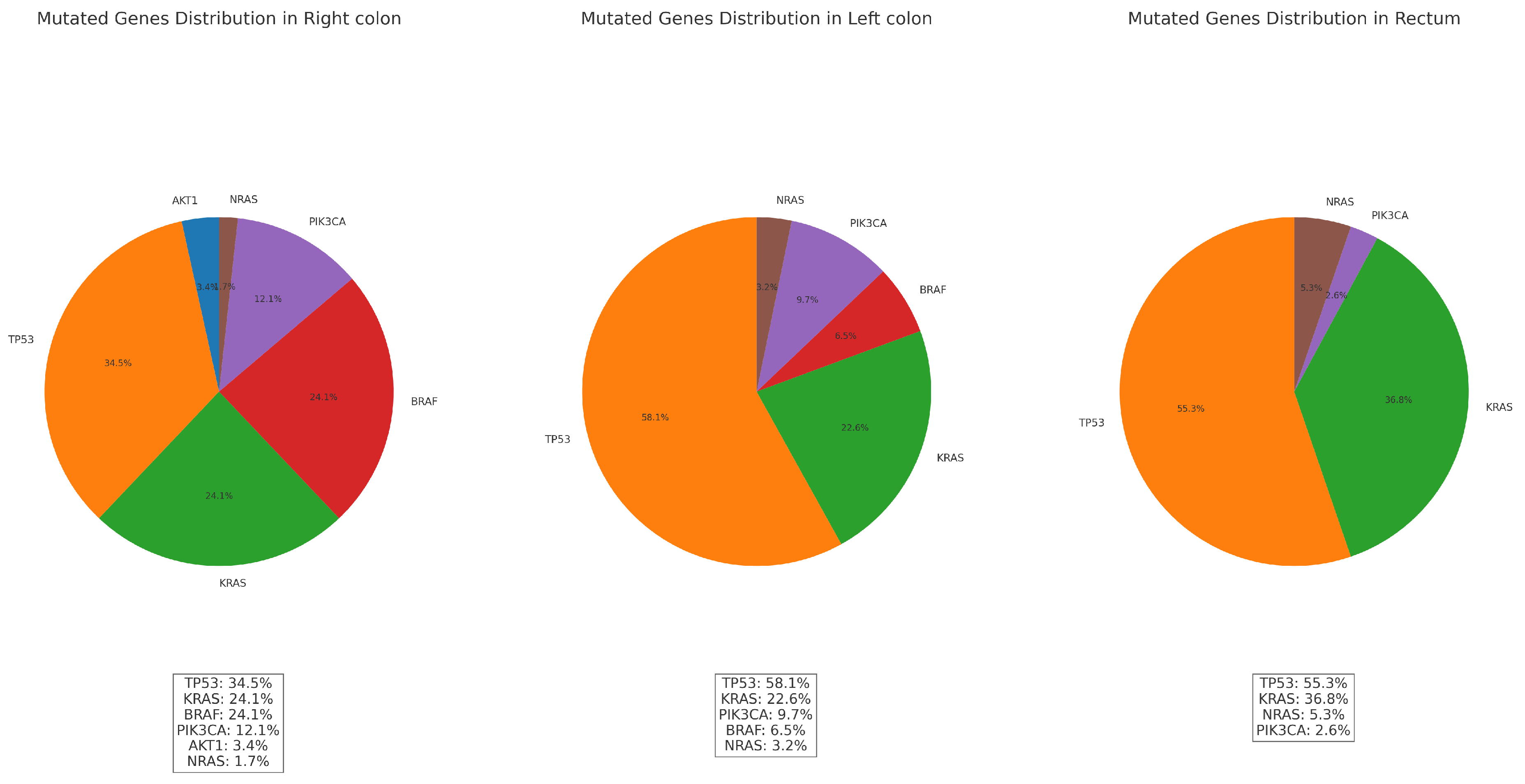
Table 3.
Chi-Square test results for lymph node status vs. tumor grade and tumor stage
| Chi- square test | Grade | Stage |
| Chi-square value | 16.945 | 36.590 |
| Dof | 14 | 35 |
| p- value | 0.259 | 0.395 |
Table 4.
LVI count by localization group
| LVI count by localization | Negative | Positive |
|---|---|---|
| Right colon | 28 | 14 |
| Left colon | 22 | 7 |
| Rectum | 24 | 5 |
| Total | 74 | 26 |
Table 5.
Chi-square test results for LVI and tumor Grade and Stage
| Chi- square value | Grade | Stage |
|---|---|---|
| value | 17.33 | 16.13 |
| df | 2 | 5 |
| p- value | 0.00017 | 0.006 |
Table 6.
Results of the chi-square tests for the association between Perineural Invasion (PNI) and Localization, Histological subtype, Grade, and Stage.
Table 6.
Results of the chi-square tests for the association between Perineural Invasion (PNI) and Localization, Histological subtype, Grade, and Stage.
| Localization | Histological subtype | Grade | Stage | |
|---|---|---|---|---|
| value | 1.46 | 7.31 | 2.15 | 2.46 |
| p- value | 0.984 | 0.605 | 0.542 | 0.783 |
| Df | 7 | 9 | 3 | 5 |
Table 7.
Results for tumor grade and tumor stage and peritumoral stromal immune reaction(count)
| Tumor grade | Absent | Moderate | Marked |
| G2 | 18 | 35 | 32 |
| G3 | 2 | 3 | 7 |
| G4 | 1 | 1 | 1 |
| Tumor stage | |||
| T1 | 1 | 1 | 0 |
| T2 | 3 | 9 | 6 |
| T3 | 13 | 23 | 28 |
| T4 | 4 | 6 | 6 |
Table 8.
Results for tumor grade and tumor stage and peritumoral budding- Bd1(Bd0+ Bd1), Bd2, Bd3
| Tumor grade | Bd1 | Bd2 | Bd3 |
| G2 | 35 | 3 | 1 |
| G3+G3 NEC | 29 | 1 | 0 |
| G4 | 21 | 8 | 2 |
| Tumor stage | |||
| T1 | 1 | 0 | 1 |
| T2 | 7 | 5 | 6 |
| T3 | 24 | 22 | 18 |
| T4 | 4 | 1 | 3 |
| T4A | 1 | 2 | 3 |
| T4B | 2 | 0 | 0 |
Table 9.
MMR status and primary tumor localization
| MMR status/ Localization | Right | Left | Rectum |
| dMMR | 16 | 2 | 0 |
| pMMR | 26 | 27 | 29 |
Table 10.
MMR status, histological subtype, and primary tumor localization
| MMR Status | Histological Type | Right | Left | Rectum |
|---|---|---|---|---|
| dMMR | Adenocarcinoma NOS | 8 | 0 | 0 |
| Medullary | 2 | 0 | 0 | |
| MiNEN | 1 | 0 | 0 | |
| Mucinous | 4 | 2 | 0 | |
| Serrated adenocarcinoma | 1 | 0 | 0 | |
| pMMR | Adenocarcinoma NOS + mucinous component | 0 | 0 | 1 |
| Adenocarcinoma NOS + intra and extracellular mucin production | 0 | 0 | 1 | |
| Adenocarcinoma NOS | 21 | 22 | 26 | |
| Adenocarcinoma NOS with mucinous and poorly cohesive component | 1 | 0 | 0 | |
| Mucinous | 2 | 3 | 0 | |
| Serrated adenocarcinoma | 1 | 1 | 1 | |
| Sinchronous- Cecum- mucinous + Rectum- Adenocarcinoma NOS | 1 | 0 | 0 | |
| Undifferentiated | 0 | 1 | 0 |
Table 11.
dMMR status with corresponding MLH1, PMS2, MSH6, and MSH2 status, main gene mutations, and mutated gene combinations and their relation to Lynch syndrome.
Table 11.
dMMR status with corresponding MLH1, PMS2, MSH6, and MSH2 status, main gene mutations, and mutated gene combinations and their relation to Lynch syndrome.
| Patient | MMR | MLH1 | PMS2 | MSH6 | MSH2 | BRAF gene mutations |
Mutated genes and combinations | Suspicion for Lynch Syndrome |
| 10 | dMMR | neg | neg | pos | pos | BRAF | BRAF+ TP53 | Not Suspected |
| 16 | dMMR | neg | neg | pos | pos | BRAF | BRAF+ TP53 | Not Suspected |
| 19 | dMMR | neg | neg | neg | pos | BRAF | BRAF+ TP53 | Not Suspected |
| 20 | dMMR | neg | neg | pos | pos | BRAF | BRAF+ TP53 | Not Suspected |
| 33 | dMMR | neg | neg | pos | pos | BRAF | BRAF | Not Suspected |
| 52 | dMMR | neg | neg | pos | pos | BRAF | BRAF+PIK3CA | Not Suspected |
| 56 | dMMR | neg | neg | pos | pos | BRAF | BRAF | Not Suspected |
| 58 | dMMR | neg | neg | pos | pos | BRAF | BRAF | Not Suspected |
| 60 | dMMR | neg | neg | pos | pos | TP53 | Suspected | |
| 65 | dMMR | pos | pos | neg | neg | No Result | Suspected | |
| 67 | dMMR | pos | pos | neg | pos | PIK3CA + TP53+ KRAS | Not Suspected | |
| 75 | dMMR | neg | pos | pos | neg | No Result | Suspected | |
| 84 | dMMR | neg | neg | pos | pos | BRAF | BRAF | Not Suspected |
| 88 | dMMR | neg | neg | pos | pos | BRAF | BRAF + AKT1 | Not Suspected |
| 92 | dMMR | neg | neg | pos | pos | NRAS + TP53 | Suspected | |
| 94 | dMMR | neg | neg | pos | pos | BRAF | BRAF+PIK3CA | Not Suspected |
| 95 | dMMR | neg | neg | pos | pos | BRAF | BRAF+ TP53 | Not Suspected |
| 96 | dMMR | neg | neg | pos | pos | PIK3CA | Suspected |
Table 12.
Mutations and primary tumor localization (*For 12 of the studied patients, there is a lack of data regarding the mutational profile due to insufficient material, technical reasons, and other factors.)
Table 12.
Mutations and primary tumor localization (*For 12 of the studied patients, there is a lack of data regarding the mutational profile due to insufficient material, technical reasons, and other factors.)
| Localization | Total Mutations | AKT1 | TP53 | KRAS | BRAF | PIK3CA | NRAS |
| Right colon | 42 | 2 | 20 | 14 | 14 | 7 | 1 |
| Left colon | 25 | 0 | 18 | 7 | 2 | 3 | 1 |
| Rectum | 29 | 0 | 21 | 14 | 0 | 1 | 2 |
Table 13.
Chi- square test results for mutations vs histological subtype
| Gene | Chi-square value | p-value | Dof |
| AKT1 | 0.61 | 1.0 | 9 |
| TP53 | 7.49 | 0.586 | 9 |
| KRAS | 10.982 | 0.277 | 9 |
| BRAF | 20.292 | 0.016 | 9 |
| PIK3CA | 10.988 | 0.277 | 9 |
| NRAS | 1.245 | 0.999 | 9 |
Table 14.
MMR status in relation to the mutations
| MMR status | AKT1 | TP53 | KRAS | BRAF | PIK3CA | NRAS |
| dMMR | 1 | 8 | 1 | 12 | 4 | 1 |
| pMMR | 1 | 54 | 36 | 5 | 7 | 3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



