
Submitted:
28 October 2024
Posted:
29 October 2024
You are already at the latest version
Abstract
There is currently no clinically valid biomarker for predicting the growth and prognosis of abdominal aortic aneurysms (AAA). The most promising candidates with highest diagnostic values are plasma D-dimers and markers of activated neutrophils, i.e. myeloperoxidase (MPO) or cell-free DNA. So far, case-control studies on these markers were almost exclusively performed by using healthy individuals for control. To validate the value of these markers in the clinical setting of a vascular surgery department, we analysed the diagnostic and prognostic potential of plasma D-dimers and MPO in 177 AAA patients versus 138 non-AAA patients with different vascular diseases. Significantly elevated levels of D-dimers were recorded for AAA patients compared with non-AAA patients, although the difference between the two groups was significantly smaller than in other studies comparing AAA patients with healthy controls. Surprisingly, MPO levels were significantly higher in non-AAA patients than in AAA patients. After adjusting for the confounding factors sex, peripheral artery disease (PAD) and internal carotid stenosis in multivariate regression models, neither D-dimers nor MPO remained independent correlates of AAA. In contrast, D-dimer plasma levels correlated well with the maximal aortic diameter. Combined analysis of D-dimers and circulating cell-free DNA levels derived from a previous study, failed to improve the predictive values for the maximal aortic diameter. In conclusion, our data show that D-dimers and MPO are no suitable biomarkers for monitoring AAA in a real-world setting of mixed vascular surgery patients.
Keywords:
abdominal aortic aneurysm
; biomarker
; D-dimer
; Myeloperoxidase (MPO)
1. Introduction
AAA is a chronic disorder characterized by the weakening and progressive dilatation of the aorta with an increasing risk of rupture [1,2]. Identification of AAA by screening or incidental imaging at an early stage allows for a close surveillance and surgical intervention, when the diameter reaches a threshold of 55 mm in male or 50 mm in female patients [3]. However, not all aneurysms expand at the same rate and with the same physical evolution. Therefore, the diameter cannot always predict the rupture risk, which is why the additional use of a specific circulating biomarker would be of great clinical benefit [4]. The pathophysiology of AAA is associated with inflammation, formation of a large intra-luminal thrombus (ILT), and remodelling of the aortic wall. It thus offers numerous approaches for the use of circulating proteins as biomarkers for the prediction of the growth or prognosis of AAA [5,6,7]. Among the most studied and promoted candidates are D-dimers, which were found to be significantly increased in patients with AAA compared with healthy individuals and were associated with aneurysm growth [7,8,9,10]. D-dimers are cross-linked, fibrin-specific, degradation products, and elevation of D-dimer levels is a sensitive marker for thrombosis [11] and coagulation in clinical practice.
The ILT, which develops in 70-80% of AAA [12], may not only release D-dimers but be also a source of other circulating proteins that might be used as biomarkers. Particularly the accumulation of neutrophils in the ILT and their central role in creating an oxidative and proteolytic environment offers possibilities for monitoring the growth of AAA by using neutrophil-related factors [13,14,15]. One of the most abundant proteins in neutrophils, Myeloperoxidase (MPO), which is released when neutrophils are stimulated, has been demonstrated to be associated with AAA development and growth [6,14]. Multivariate regression models using myeloid activation markers and routine laboratory parameters have identified MPO and D-Dimer as strong independent correlates of AAA in a study with 41 AAA patients and 38 controls, recruited from general surgery, urology and ophthalmology departments [14]. A combined MPO/D-Dimer Score recently showed an improved performance in distinguishing AAA from peripheral artery disease (PAD) [16]. Moreover, MPO had the best prognostic value and higher baseline levels of MPO were associated with faster AAA growth in a study population of 65-year old men, invited for a AAA screening program [6].
Until now, the diagnostic and prognostic values of most circulating biomarkers (including D-dimers and MPO) was determined in comparison with healthy controls or with groups selected for age and sex (screening programs) or selected for specific vascular diseases (such as PAD) [8,10,14,16,17,18]. However, a robust biomarker should give reliable results under routine hospital conditions and be reasonably insensitive to pre-analytical procedures. The aim of our study therefore was to validate the diagnostic and prognostic values of D-dimers and MPO for AAA in a clinical real-world setting by using a mixed vascular surgery cohort for analysis. Because anticoagulant tube additives may affect the results of biomarker quantification, we additionally compared the plasma levels of D-dimers and MPO according to the additive that was used during blood collection.
2. Materials and Methods
2.1. Blood Samples and Pre-Analytics
The study was conducted according to the Code of Ethics of the World Medical Association (Declaration of Helsinki). Patients undergoing treatment at the Klinik für Gefäßchirurgie und endovaskuläre Chirurgie Heidelberg were enrolled for the Vascular Biobank Heidelberg (VBBH) between January 2014 and January 2024. Patients demographics were recorded by the Hospital Information System. Maximum aortic diameter of AAA patients was determined by computed tomography angiography scan (AAA patients) or ultrasound examination (other vascular patients). Peripheral venous blood was taken as part of a routine set of diagnostic tests on the day of their hos pitalization into lithium-heparin (Sarstedt, Germany, S-Monovette, Lithium-Heparin-Gel) or potassium-EDTA (Sarstedt, Germany, S-Monovette, EDTA KE) containing tubes, according to the standard operating procedures of the VBBH. All pa rticipants gave their written informed con sent to the study, which was approved by the ethical committee of the Uni versity of Heidelberg (S-025/2023) and (S-310/2013 “Etablierung einer humanen vaskulären Biomaterialbank (VBBH) an der Klinik für Gefäßchirurgie und endovaskuläre Chirurgie der Universitätsklinik Heidelberg), and amendments. The blood was processed for further studies within 4 h after venepuncture. Plasma was collected by centrifugation at 1200 g for 15 min. and aliquoted for storage at -80°C by the VBBH until analysis.
2.2. Diagnostic Study Design
Initially, 315 plasma samples were provided by the VBBH for analysis and included according to the following criteria: donors should be over 18 years old and give informed consent to the study. Exclusion criteria were: recent (<1 year) tumour and/or chemotherapy, systemic autoimmune or inflammatory disease. The complete case group consisted of 177 samples from patients who underwent early diagnostics or treatment for repair of their abdominal aortic aneurysm (AAA defined as a dilation of all three layers of the aorta; max. diameter ≥ 30 mm; penetrating aortic ulcer (PAU) and dissections of the abdominal aorta were not included), the control group consisted of 138 samples from patients without previous or present AAA (controls, defined by aortic max. diameter < 30 mm) who underwent treatment for other vascular diseases PAD, thrombendarterectomy of the internal carotid artery (ICA), other thrombendarterectomies, varicose veins, minor vascular interventions, other aortic diseases). When using the Lithium-Heparin plasma samples only, the groups consisted of 143 AAA and 89 control samples. As not all variables were measurable in all samples, the group sizes on which the calculations are based are explained in the figure legends. The patients’ characteristics are summarized in Table 1 and Supplementary Table 1.
2.3. Analysis of D-dimers and Myeloperoxidase (MPO) Concentrations in Plasma Samples
Concentrations of D-dimers and MPO in plasma samples were measured by ELISA (Human D-dimer ELISA Kit, Human Myeloperoxidase instant Kit; Thermo Fisher Scientific; Germany) by following the instructions of the manufacturer. Samples were diluted 1: 500 000 for D-dimer analysis and 1:50 for MPO analysis. Signal intensity (absorbance) was measured by a TECAN multiplate reader at 450 nm. A reference of 620 nm was used for reading MPO signal intensities.
2.4. Statistical Analysis
The sample size of the diagnostic study was calculated based on previously published data on concentrations of D-dimers and MPO in blood plasma [6,14,18,19]. With 150 cases, a power of 83 % to show a sensitivity and specificity of at least 0.6 for the marker D-dimers should be achieved. The evaluation on which the power calculation is based tests the union of the two null hypotheses “H¬1, Sens: Sensitivity ≤ 0.6” and “H¬1, Spec: Specificity ≤ 0.6” at the one-sided significance level of 2.5 %. As this is an intersection union test, the significance level does not need to be adjusted for multiple testing. The concentration of D-dimers was assumed to be log-normally distributed, with medians (IQR) reported in the literature of 1.3 µg/ml (1.68 µg/ml) for AAA patients and 0.47 µg/ml (0.49 µg/ml) for patients without AAA [14,19]. Microsoft Excel was used for data processing. GraphPad Prism 10 software was used for plot preparation, descriptive statistics and for statistical analysis. Data distribution was tested for normality by using the Kolmogorov-Smirnov Test, the Shapiro–Wilk test or the D’Agostino and Pearson test and appropriate parametric or non-parametric tests were used for further analysis. Multiple group comparisons were carried out using a Kruskal-Wallis test ANOVA or ordinary one-way ANOVA to analyse non-parametric and parametric data, respectively. The box plots show the minimum and the maximum with all data points. The AUC was calculated using ROC to further characterize the biomarker potential and obtain information on specificity and sensitivity. All specific tests used and P-value ranges are indicated in the figure legends. Univariate and multivariate analyses were performed using a logistic regression model. P values for regression coefficients were calculated by Wald tests. Variables that showed statistical significance with p-values < 0.0001 in the univariate analysis were included in the multivariate analysis. The odds ratio (OR) was reported with a 95% CI.
3. Results
3.1. Pre-analytic Parameters (Anti-Coagulant, Storage Time) Affecting the Measurements
Because the plasma samples had been provided from a biobank where they had been collected with different anti-coagulants and stored for different time periods, we first determined whether these pre-analytic parameters affect the D-dimer and MPO measurements. The anti-coagulant that was used in blood sampling tubes appeared to affect the concentrations of both D-dimers and MPO. The median overall D-dimer concentration was significantly higher in EDTA-samples (1.608 µg/ml) than in heparin samples (1.309 µg/ml) with a difference of 0.2995 µg/ml (Figure 1A). In contrast, the median MPO concentration was significantly lower in EDTA-samples (6.08 ng/ml) than in heparin samples (28.21 ng/ml) with a difference of 22.12 ng/ml (Figure 1B). Statistical analysis by Kruskal Wallis test revealed no significant difference of D-dimer and MPO concentrations between heparin samples that were stored for different lengths of time, although there was a trend for a minimal loss of D-Dimers over eight years (Supplementary Figure S1). We therefore decided to only use the heparin samples for further analysis.
3.2. Diagnostic Value of D-dimers
The heparin plasma levels of D-dimers were significantly increased in AAA patients (median 1.38 µg/ml) compared to controls (median 1.18 µg/ml), P = 0.0065, resulting in a small difference of only 0.2 µg/ml between the medians (Figure 2A). Consequently, ROC analysis revealed a low AUC of 0.598 (Figure 2B). A diagnostic logistic regression model was developed including the following parameters: sex, ICA stenosis, PAD, diabetes, COPD, and previous stroke. After backward elimination, only sex (odds ratio 2.61 and 95% CI [1.02-6.72]), ICA stenosis (odds ratio 45.29 and 95% and CI [18.34-128.3]) and PAD (odds ratio 8.08 and CI [3.27-20.78]) had a significant independent importance for AAA diagnosis, whereas D-dimers had no significant independent importance for AAA diagnosis (odds ratio 0.93 and CI [0.6092-1.343], p-value 0.737) (Supplementary Table S2). Accordingly, the ROC analysis for D-dimers increased to an AUC of 0.8995 after adjusting for sex, ICA stenosis and PAD. In summary, in our study, D-dimers were not suitable for discriminating AAA patients from patients with other vascular diseases.
3.3. Diagnostic value of Myeloperoxidase (MPO)
The heparin plasma levels of MPO were significantly higher in non-AAA patients (median 29,3 ng/ml) than in AAA patients (median 26,9 ng/ml), P = 0.0287, resulting in a small difference of 2.4 ng/ml between the medians (Figure 3A). Consequently, ROC analysis revealed a low AUC of 0.587 (Figure 3B). The diagnostic logistic regression model used for D-dimers was also applied for adjusting MPO. After backward elimination, only sex (odds ratio 2.598 and 95% CI [1.01-6.71]), ICA stenosis (odds ratio 46.43 and 95% and CI [18.95-130.3]) and PAD (odds ratio 8.09 and CI [3.28-20.78]) had a significant independent importance for AAA diagnosis, whereas MPO had no significant independent importance for AAA diagnosis (odds ratio 1.0001 and CI [0.99-1.01], p-value 0.638) (Supplementary Table S2). Accordingly, the ROC analysis for MPO increased to an AUC of 0.90 after adjusting for sex, ICA stenosis and PAD. In summary, in our study, MPO was not suitable for discriminating AAA patients from patients with other vascular diseases.
3.4. Correlation of Plasma Factors with the Maximal Aortic Diameter and Prognostic Values of D-Dimers and MPO for AAA Progression
A subset of the samples used in this study had already been used in a previous study to investigate the diagnostic value of cell-free DNA for monitoring AAA (Dihlmann et al., under review). To determine the correlation across plasma levels of D-dimers, MPO and cell-free DNA with the maximal aortic diameter, a Spearman r correlation matrix was performed (Figure 4A and Supplementary Tables S4 and S5). The strongest correlation with the maximal aortic diameter was found with cell-free single stranded (ss) DNA (r = 0.32, P = 0.0006). The correlation with D-dimer concentrations was r = 0.19, P = 0.0024. The correlation between the maximum aortic diameter and MPO was not significant (r = - 0.035, P = 0.3041). Of note, height and weight of the patients did also correlate well with the maximum aortic diameter (r = 0.23, P < 0.0001 and r = 0.21, P = 0.0010 respectively).
For modelling the prognostic values of the different plasma biomarkers, a simple linear regression analysis was performed, demonstrating an association of the max. aortic diameter with D-Dimers (P = 0.039) and plasma ssDNA (P = 0.0025) (Figure 4B). Plasma levels of MPO, dsDNA and mtDNA revealed no significant association with the max. aortic diameter in simple regression analysis P values = 0.956, 0.138, and 0.408, respectively). Finally, using D-Dimers and ssDNA in combination did not improve the prognostic value to predict AAA growth (R squared in a multiple linear regression model using the two parameters: 0.083).
4. Discussion
The association of D-dimers plasma levels with AAA has been well documented [7,8,9,10]. Moreover, a combination of plasma D-Dimers and MPO was recently suggested to be used for a diagnostic and prognostic AAA score [14] and to distinguish AAA from PAD [16]. We here aimed to investigate the diagnostic and prognostic utility of D-Dimers and MPO for monitoring AAA in a real-world setting of a typical vascular surgery patient cohort at a university hospital. Accordingly, we compared a group of patients who came to the hospital for surgical treatment or outpatient control of an AAA with a control group of patients with different vascular diseases (non-AAA group).
Because ultrasound screening and CT scans are already well-established non-invasive methods for the diagnostic detection and surveillance of an AAA, additional circulating biomarkers, used for diagnostic and prognostic use, should be as specific as possible and thus stand out not only from healthy individuals but also from patients with other vascular diseases, such as PAD, carotid stenosis, varicose veins, or others. According to our study results, the difference of the median plasma D-Dimer levels between patients with AAA and the control group of non-AAA patients was very low and not suitable for additional diagnostic purposes. With a median D-Dimer level of 1.38 µg/ml our AAA-group displayed very similar results to those previously published (0.8 µg/ml [8], 1.30 µg/ml [14,19], 1.27 µg/ml [16], > 1.006 µg/ml[10]. In contrast, the median D-Dimer level in our non-AAA group (1.18 µg/ml) was much higher than that reported for healthy individuals (0.47 µg/ml [14], 0.38 µg/ml [16], < 0.5 µg/ml[10]) or patients with PAD only (0.58 µg/ml [16], 0.28 [8]). Consequently, the area under the ROC curve was very low in our study resulting in a sensitivity of 60.14% and a weak specificity of 43.06%. At 80% sensitivity, the specificity fell to less than 40%. Considering our own results shown here and studies by others [20], we are aware that the choice of anticoagulant supplement (EDTA, Heparin, Citrate, other) during blood sampling affects the measurement of D-dimers. Here, the median D-dimer levels in EDTA plasma samples were significantly higher than in Heparin plasma samples, although both groups contained similar amounts of samples from AAA and non-AAA patients. However, this does not explain the smaller differences between the AAA and control groups using the Heparin samples, only. After adjusting for sex, PAD and ICA stenosis, D-Dimer plasma levels were no longer independent markers for AAA prediction in the study presented here, in contrast to sex, PAD and ICA stenosis which remained independent. This indicates that a great proportion of the D-Dimers found in plasma resulted from diseases other than AAA. In line with previous data [8,16], subgroup analysis of our study cohort revealed a trend for increased D-dimer levels in patients with AAA plus PAD compared with patients with PAD only (without AAA), which was not statistically significant (Supplemental Figure S2a). In contrast, accompanying AAA in patients with ICA stenosis did not increase the median D-dimer levels, whereby the group of patients with AAA and ICA stenosis was very small (Supplemental Figure S2b).
The second marker that was tested here showed even weaker results. The plasma MPO levels of non-AAA patients were higher than that of patients with AAA which clearly calls into question the suitability of MPO as a biomarker for AAA. MPO is a lysosomal protein stored in azurophilic granules of neutrophils, which can be released into the extracellular space during degranulation. The release of MPO is part of the neutrophil defence mechanism to kill pathogens that cannot be phagocytosed, but it can also be detrimental to the host by inducing tissue damage and exacerbating inflammation [21]. Elevated plasma MPO levels are frequently detected in patients with atherosclerosis, cardiovascular, respiratory, autoimmune and neurogenerative diseases and cancer, and correlate with disease severity [21,22,23,24,25]. The association of increased MPO plasma levels with aortic aneurysm has been documented in several studies, using healthy donors for comparison [6,14,16,26]. In contrast, one study found decreased serum MPO levels associated significantly with the risk for peripheral atherosclerosis disease and AAA compared with those in healthy donors [27]. In general, the measured values of our study group were significantly higher as those published earlier (median in AAA (here): 26,87 ng/ml vs. 13.3 ng/ml in AAA and 7.7 ng/ml in healthy donors [14]; 3.01 ng/ml in AAA and 2.79 ng/ml in non-AAA donors from a screening study [6]). This could be due to the different anticoagulants used for the blood collection, which resulted in lower readings of samples drawn with EDTA blood collection tubes. In this study, the median plasma MPO levels in samples from EDTA tubes were less than a quarter as high as those from heparin tubes. Regardless, even when we compared a homogeneous group with samples from heparin tubes only, we could not demonstrate an association of plasma MPO level with aortic diameter or the occurrence of AAA. Finally, the combination with the ssDNA content in plasma examined in a previous study also improved neither the diagnostic nor the prognostic value of the D-dimer or MPO levels in plasma.
5. Conclusions
In summary, we conclude that neither D-Dimer nor MPO plasma levels, nor a combination of both or with cell-free DNA plasma levels are suitable for use as biomarkers for the monitoring and/or prognostics of AAA in a real-world setting of a vascular surgery department.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Supplemental Figure S1: Effects of the storage time on the median plasma concentration of D-dimers and MPO; Supplemental Figure S2: Comparison of D-dimers plasma levels (Heparin samples) between subgroups (excluding patients with PAU or thoracic aortic dissection); Supplemental Figure S3: Comparison of Plasma-D dimer levels between Patients with AAA and controls (excluding patients with PAU or thoracic aortic dissection). Supplemental Table S1: Patient and control blood parameters; Supplemental table S2: Multiple logistic regression of D-dimers, adjusted for sex, ICA stenosis, PAD (Heparin plasma only), Supplemental Table S3: Multiple logistic regression of MPO, adjusted for sex, ICA stenosis, PAD MPO (Heparin plasma only); Supplemental Table S4: Correlation of maximal aortic diameter with continuous variables (Heparin plasma only). Supplemental Table S5: One-tailed P values of spearman correlation, maximal aortic diameter with other variables (Heparin plasma only).
Funding
This research was funded by “Verein der Heidelberger Stiftung Chirurgie”, grant number 2023/586 to K.P. and A.S.P.”
Author Contributions
Conceptualization, Karola Passek and Susanne Dihlmann; Formal analysis, Hans Siegrist, Karola Passek and Susanne Dihlmann; Funding acquisition, Andreas Peters, Karola Passek and Dittmar Böckler; Investigation, Hans Siegrist, Anja Spieler and Susanne Dihlmann; Methodology, Anja Spieler and Susanne Dihlmann; Resources, Andreas Peters and Dittmar Böckler; Supervision, Susanne Dihlmann; Visualization, Hans Siegrist and Susanne Dihlmann; Writing – original draft, Susanne Dihlmann; Writing – review & editing, Hans Siegrist, Andreas Peters and Karola Passek.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the University of Heidelberg, Germany (protocol code S-045/2023 from 23.03.2023).” for studies involving humans. The Ethics Committee of the University of Heidelberg, Germany discussed the research project at its meeting on 13.02.2023. The additional information requested was received on 07.03.2023. The Ethics Committee has no objections to the conduct of the study.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All data required for interpretation can be found in the manuscript and the supplements. The underlying raw data of the measurements will be provided by the corresponding author upon reasonable request.
Acknowledgments
The authors would like to thank Samuel Kilian, Institute for Medical Biometry and Informatics (IMBI), Heidelberg, Germany for his extensive advice on carrying out the statistical analysis.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Davis, F.M.; Daugherty, A.; Lu, H.S. Updates of Recent Aortic Aneurysm Research. Arterioscler Thromb Vasc Biol 2019, 39, e83–e90. [Google Scholar] [CrossRef] [PubMed]
- Golledge, J.; Moxon, J.V.; Singh, T.P.; Bown, M.J.; Mani, K.; Wanhainen, A. Lack of an effective drug therapy for abdominal aortic aneurysm. J Intern Med 2020, 288, 6–22. [Google Scholar] [CrossRef] [PubMed]
- Moll, F.L.; Powell, J.T.; Fraedrich, G.; Verzini, F.; Haulon, S.; Waltham, M.; van Herwaarden, J.A.; Holt, P.J.; van Keulen, J.W.; Rantner, B.; et al. Management of abdominal aortic aneurysms clinical practice guidelines of the European society for vascular surgery. Eur J Vasc Endovasc Surg 2011, 41 Suppl 1, S1–S58. [Google Scholar] [CrossRef]
- Kurvers, H.; Veith, F.J.; Lipsitz, E.C.; Ohki, T.; Gargiulo, N.J.; Cayne, N.S.; Suggs, W.D.; Timaran, C.H.; Kwon, G.Y.; Rhee, S.J.; et al. Discontinuous, staccato growth of abdominal aortic aneurysms. J Am Coll Surg 2004, 199, 709–715. [Google Scholar] [CrossRef] [PubMed]
- Groeneveld, M.E.; Meekel, J.P.; Rubinstein, S.M.; Merkestein, L.R.; Tangelder, G.J.; Wisselink, W.; Truijers, M.; Yeung, K.K. Systematic Review of Circulating, Biomechanical, and Genetic Markers for the Prediction of Abdominal Aortic Aneurysm Growth and Rupture. J Am Heart Assoc 2018, 7. [Google Scholar] [CrossRef]
- Memon, A.A.; Zarrouk, M.; Agren-Witteschus, S.; Sundquist, J.; Gottsater, A.; Sundquist, K. Identification of novel diagnostic and prognostic biomarkers for abdominal aortic aneurysm. Eur J Prev Cardiol 2020, 27, 132–142. [Google Scholar] [CrossRef]
- Nana, P.; Dakis, K.; Brodis, A.; Spanos, K.; Kouvelos, G. Circulating Biomarkers for the Prediction of Abdominal Aortic Aneurysm Growth. J Clin Med 2021, 10. [Google Scholar] [CrossRef]
- Cai, H.; Pan, B.; Xu, J.; Liu, S.; Wang, L.; Wu, K.; Yang, P.; Huang, J.; Wang, W. D-Dimer Is a Diagnostic Biomarker of Abdominal Aortic Aneurysm in Patients With Peripheral Artery Disease. Front Cardiovasc Med 2022, 9, 890228. [Google Scholar] [CrossRef]
- Golledge, J.; Muller, R.; Clancy, P.; McCann, M.; Norman, P.E. Evaluation of the diagnostic and prognostic value of plasma D-dimer for abdominal aortic aneurysm. Eur Heart J 2011, 32, 354–364. [Google Scholar] [CrossRef]
- Sundermann, A.C.; Saum, K.; Conrad, K.A.; Russell, H.M.; Edwards, T.L.; Mani, K.; Bjorck, M.; Wanhainen, A.; Owens, A.P. , 3rd. Prognostic value of D-dimer and markers of coagulation for stratification of abdominal aortic aneurysm growth. Blood Adv 2018, 2, 3088–3096. [Google Scholar] [CrossRef]
- Ariens, R.A.; de Lange, M.; Snieder, H.; Boothby, M.; Spector, T.D.; Grant, P.J. Activation markers of coagulation and fibrinolysis in twins: heritability of the prethrombotic state. Lancet 2002, 359, 667–671. [Google Scholar] [CrossRef] [PubMed]
- Harter, L.P.; Gross, B.H.; Callen, P.W.; Barth, R.A. Ultrasonic evaluation of abdominal aortic thrombus. J Ultrasound Med 1982, 1, 315–318. [Google Scholar] [CrossRef] [PubMed]
- Piechota-Polanczyk, A.; Jozkowicz, A.; Nowak, W.; Eilenberg, W.; Neumayer, C.; Malinski, T.; Huk, I.; Brostjan, C. The Abdominal Aortic Aneurysm and Intraluminal Thrombus: Current Concepts of Development and Treatment. Front Cardiovasc Med 2015, 2, 19. [Google Scholar] [CrossRef] [PubMed]
- Zagrapan, B.; Eilenberg, W.; Prausmueller, S.; Nawrozi, P.; Muench, K.; Hetzer, S.; Elleder, V.; Rajic, R.; Juster, F.; Martelanz, L.; et al. A Novel Diagnostic and Prognostic Score for Abdominal Aortic Aneurysms Based on D-Dimer and a Comprehensive Analysis of Myeloid Cell Parameters. Thromb Haemost 2019, 119, 807–820. [Google Scholar] [CrossRef]
- Klopf, J.; Brostjan, C.; Neumayer, C.; Eilenberg, W. Neutrophils as Regulators and Biomarkers of Cardiovascular Inflammation in the Context of Abdominal Aortic Aneurysms. Biomedicines 2021, 9. [Google Scholar] [CrossRef]
- Zagrapan, B.; Klopf, J.; Celem, N.D.; Brandau, A.; Rossi, P.; Gordeeva, Y.; Szewczyk, A.R.; Liu, L.; Ahmadi-Fazel, D.; Najarnia, S.; et al. Diagnostic Utility of a Combined MPO/D-Dimer Score to Distinguish Abdominal Aortic Aneurysm from Peripheral Artery Disease. J Clin Med 2023, 12. [Google Scholar] [CrossRef]
- Folsom, A.R.; Yao, L.; Alonso, A.; Lutsey, P.L.; Missov, E.; Lederle, F.A.; Ballantyne, C.M.; Tang, W. Circulating Biomarkers and Abdominal Aortic Aneurysm Incidence: The Atherosclerosis Risk in Communities (ARIC) Study. Circulation 2015, 132, 578–585. [Google Scholar] [CrossRef]
- Vele, E.; Kurtcehajic, A.; Zerem, E.; Maskovic, J.; Alibegovic, E.; Hujdurovic, A. Plasma D-dimer as a predictor of the progression of abdominal aortic aneurysm. J Thromb Haemost 2016, 14, 2298–2303. [Google Scholar] [CrossRef]
- Eilenberg, W.; Zagrapan, B.; Bleichert, S.; Ibrahim, N.; Knobl, V.; Brandau, A.; Martelanz, L.; Grasl, M.T.; Hayden, H.; Nawrozi, P.; et al. Histone citrullination as a novel biomarker and target to inhibit progression of abdominal aortic aneurysms. Transl Res 2021, 233, 32–46. [Google Scholar] [CrossRef]
- Favresse, J.; Lippi, G.; Roy, P.M.; Chatelain, B.; Jacqmin, H.; Ten Cate, H.; Mullier, F. D-dimer: Preanalytical, analytical, postanalytical variables, and clinical applications. Crit Rev Clin Lab Sci 2018, 55, 548–577. [Google Scholar] [CrossRef]
- Rizo-Tellez, S.A.; Sekheri, M.; Filep, J.G. Myeloperoxidase: Regulation of Neutrophil Function and Target for Therapy. Antioxidants (Basel) 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Baldus, S.; Heeschen, C.; Meinertz, T.; Zeiher, A.M.; Eiserich, J.P.; Munzel, T.; Simoons, M.L.; Hamm, C.W.; Investigators, C. Myeloperoxidase serum levels predict risk in patients with acute coronary syndromes. Circulation 2003, 108, 1440–1445. [Google Scholar] [CrossRef] [PubMed]
- Brennan, M.L.; Penn, M.S.; Van Lente, F.; Nambi, V.; Shishehbor, M.H.; Aviles, R.J.; Goormastic, M.; Pepoy, M.L.; McErlean, E.S.; Topol, E.J.; et al. Prognostic value of myeloperoxidase in patients with chest pain. N Engl J Med 2003, 349, 1595–1604. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.J.; Hazen, S.L. Myeloperoxidase and cardiovascular disease. Arterioscler Thromb Vasc Biol 2005, 25, 1102–1111. [Google Scholar] [CrossRef] [PubMed]
- Zhu, A.; Ge, D.; Zhang, J.; Teng, Y.; Yuan, C.; Huang, M.; Adcock, I.M.; Barnes, P.J.; Yao, X. Sputum myeloperoxidase in chronic obstructive pulmonary disease. Eur J Med Res 2014, 19, 12. [Google Scholar] [CrossRef]
- Brandau, A.; Ibrahim, N.; Klopf, J.; Hayden, H.; Ozsvar-Kozma, M.; Afonyushkin, T.; Bleichert, S.; Fuchs, L.; Watzinger, V.; Nairz, V.; et al. Association of Lipoproteins with Neutrophil Extracellular Traps in Patients with Abdominal Aortic Aneurysm. Biomedicines 2022, 10. [Google Scholar] [CrossRef]
- Pradhan-Palikhe, P.; Vikatmaa, P.; Lajunen, T.; Palikhe, A.; Lepantalo, M.; Tervahartiala, T.; Salo, T.; Saikku, P.; Leinonen, M.; Pussinen, P.J.; et al. Elevated MMP-8 and decreased myeloperoxidase concentrations associate significantly with the risk for peripheral atherosclerosis disease and abdominal aortic aneurysm. Scand J Immunol 2010, 72, 150–157. [Google Scholar] [CrossRef]
Figure 1.
Influence of the anticoagulants (EDTA or Heparin) used during blood sampling on the measured plasma levels of D-dimers (a) and MPO (b). Graphs of boxplots show the interquartile range, medians and maximal and minimal values. Sample sizes, medians and P-values for group comparison (based on Mann Whitney tests) are given in the tables below the boxplots.
Figure 1.
Influence of the anticoagulants (EDTA or Heparin) used during blood sampling on the measured plasma levels of D-dimers (a) and MPO (b). Graphs of boxplots show the interquartile range, medians and maximal and minimal values. Sample sizes, medians and P-values for group comparison (based on Mann Whitney tests) are given in the tables below the boxplots.
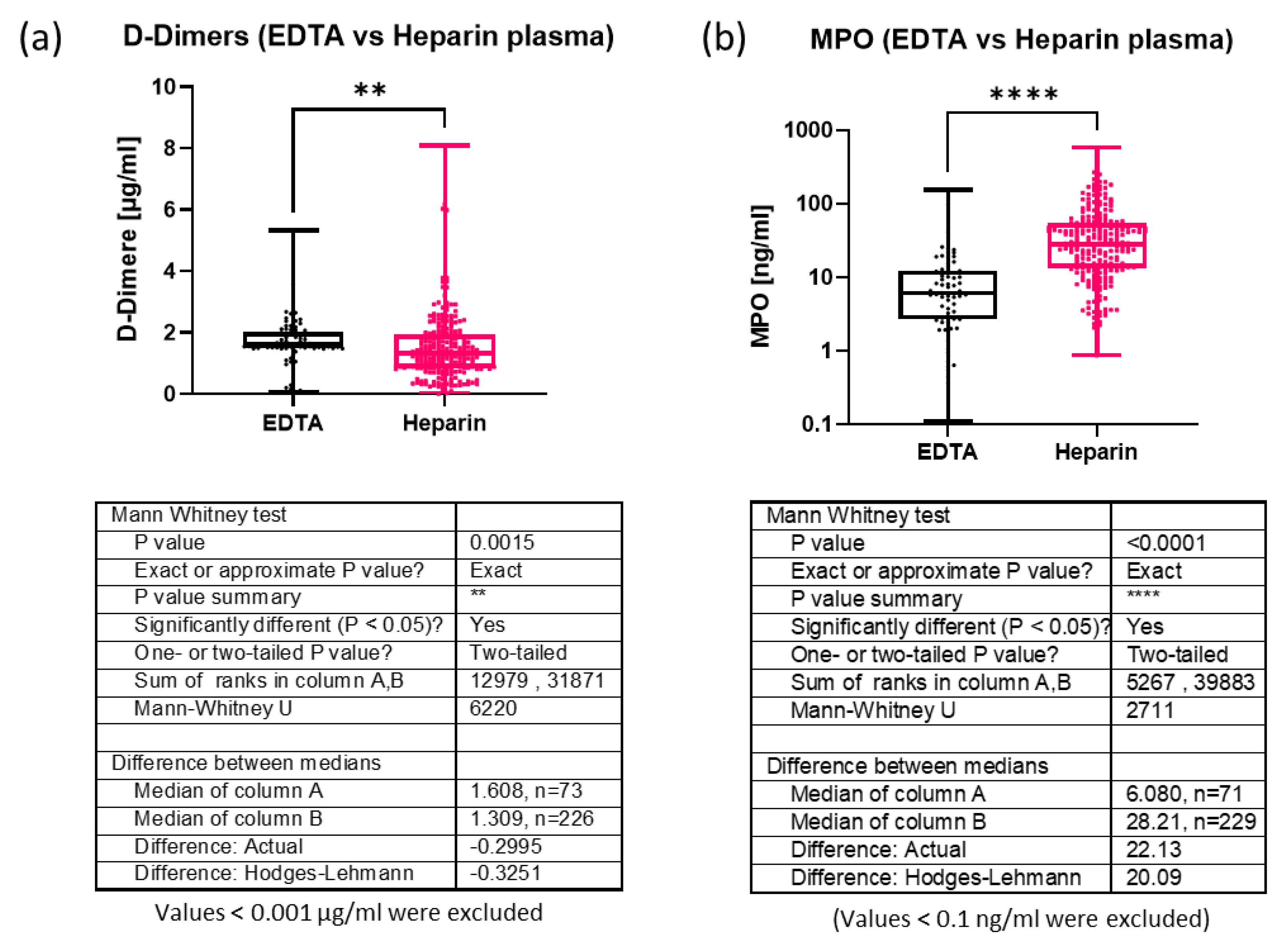
Figure 2.
Comparison of D-dimers plasma levels (Heparin samples) between AAA patients and controls. (a) Boxplots show the interquartile range, medians and maximal and minimal values. Sample sizes, medians and P-values for group comparison (based on Mann Whitney tests) are given in the table next to the graph. (b) ROC analysis of D-Dimer plasma levels in AAA patients against the non-AAA patients (controls) without adjustment. The area under the curve, sample size, 95% confidence interval and P value are given in the table below the graphs. (c) ROC analysis of D-Dimer plasma levels in AAA patients against the non-AAA patients (controls) after adjustment for sex, PAD and stenosis of the internal carotid artery (ICA). The area under the curve, sample size 95% confidence interval, P value, negative predictive value and positive predictive value are given in the table below the graphs.
Figure 2.
Comparison of D-dimers plasma levels (Heparin samples) between AAA patients and controls. (a) Boxplots show the interquartile range, medians and maximal and minimal values. Sample sizes, medians and P-values for group comparison (based on Mann Whitney tests) are given in the table next to the graph. (b) ROC analysis of D-Dimer plasma levels in AAA patients against the non-AAA patients (controls) without adjustment. The area under the curve, sample size, 95% confidence interval and P value are given in the table below the graphs. (c) ROC analysis of D-Dimer plasma levels in AAA patients against the non-AAA patients (controls) after adjustment for sex, PAD and stenosis of the internal carotid artery (ICA). The area under the curve, sample size 95% confidence interval, P value, negative predictive value and positive predictive value are given in the table below the graphs.
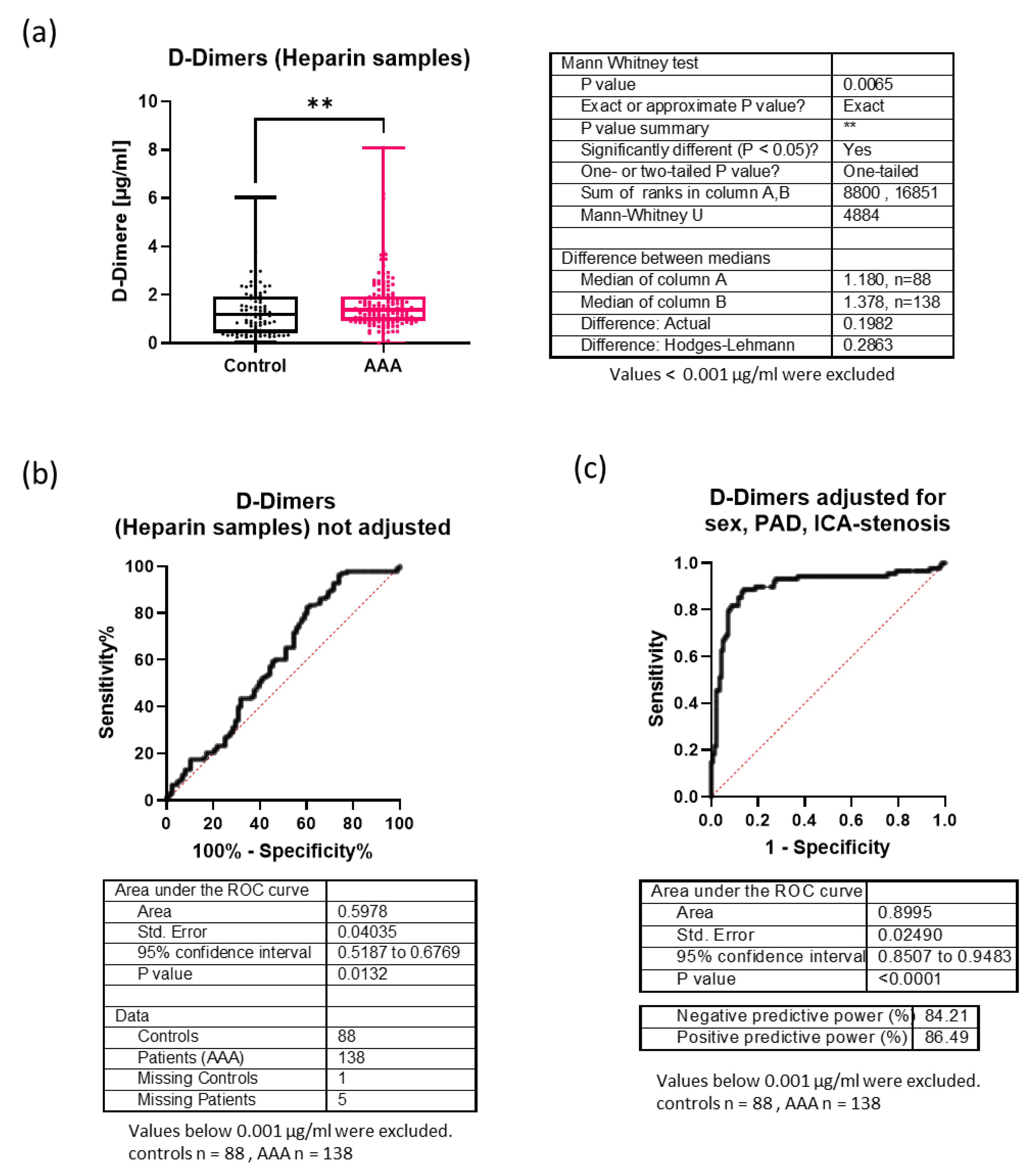
Figure 3.
Comparison of MPO plasma levels (Heparin samples) between AAA patients and controls. (a) Boxplots show the interquartile range, medians and maximal and minimal values. Sample sizes, medians and P-values for group comparison (based on Mann Whitney tests) are given in the table next to the graph. (b) ROC analysis of MPO plasma levels in AAA patients against the non-AAA patients (controls) without adjustment. The area under the curve, sample size, 95% confidence interval and P value are given in the table below the graphs. (c) ROC analysis of MPO plasma levels in AAA patients against the non-AAA patients (controls) after adjustment for sex, PAD and stenosis of the internal carotid artery (ICA). The area under the curve, sample size 95% confidence interval, P value, negative predictive value and positive predictive value are given in the table below the graphs.
Figure 3.
Comparison of MPO plasma levels (Heparin samples) between AAA patients and controls. (a) Boxplots show the interquartile range, medians and maximal and minimal values. Sample sizes, medians and P-values for group comparison (based on Mann Whitney tests) are given in the table next to the graph. (b) ROC analysis of MPO plasma levels in AAA patients against the non-AAA patients (controls) without adjustment. The area under the curve, sample size, 95% confidence interval and P value are given in the table below the graphs. (c) ROC analysis of MPO plasma levels in AAA patients against the non-AAA patients (controls) after adjustment for sex, PAD and stenosis of the internal carotid artery (ICA). The area under the curve, sample size 95% confidence interval, P value, negative predictive value and positive predictive value are given in the table below the graphs.
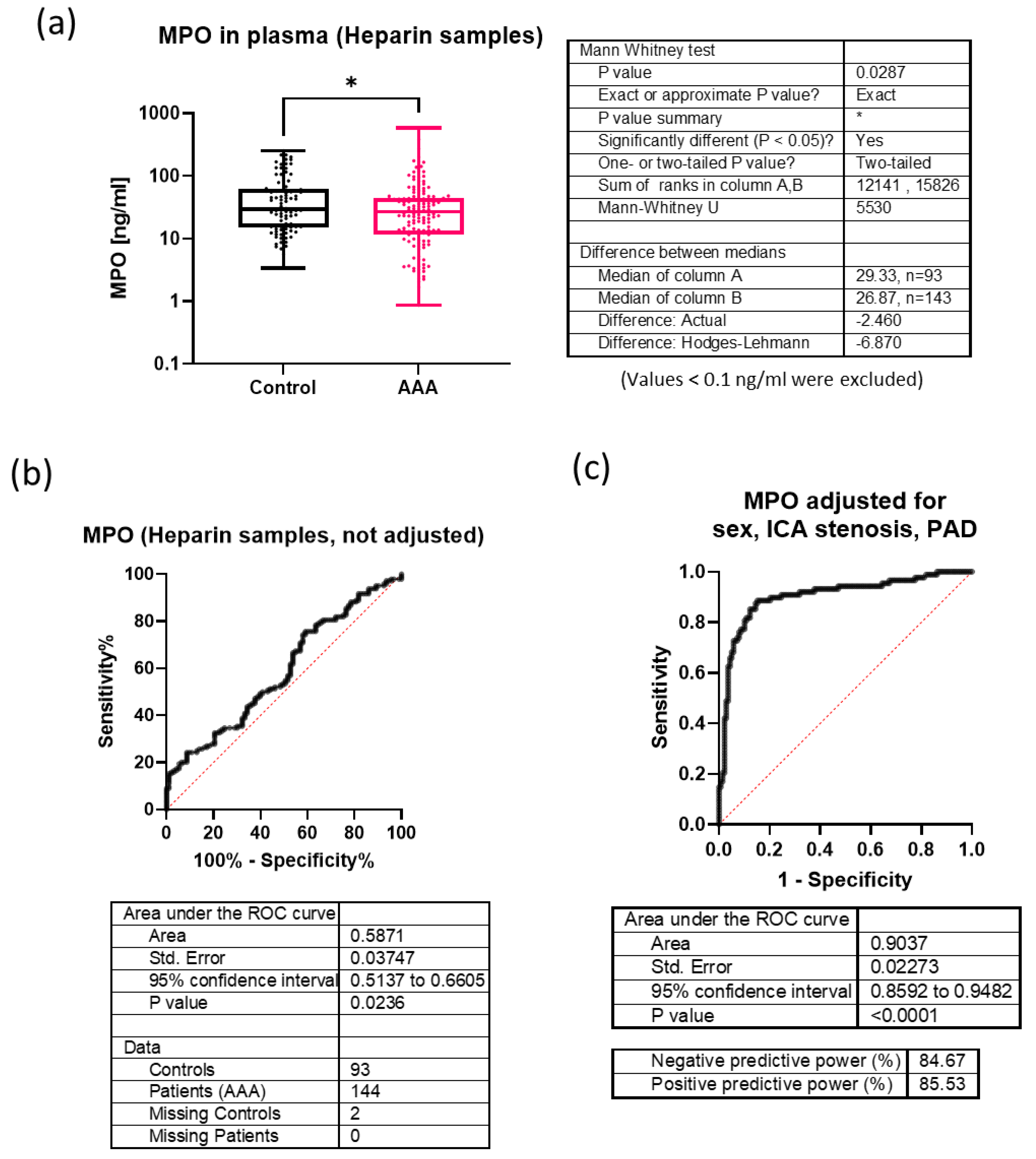
Figure 4.
Correlation of different circulating plasma parameters and patient demographics with the maximal aortic diameter. (a) Correlation matrix of the age, weight, height, BMI, plasma levels of ssDNA (single stranded DNA), dsDNA (double stranded DNA), mtDNA (mitochondrial DNA) copy number, MPO and D-dimers with the maximal aortic diameter of patients with and without AAA. Shown are the spearman correlation coefficients for each pair of parameters. (b) Graphs illustrating simple linear regression models for D-Dimers plasma levels (left panel) or ssDNA plasma levels (right panel) and the maximal aortic diameter of patients with and without AAA.
Figure 4.
Correlation of different circulating plasma parameters and patient demographics with the maximal aortic diameter. (a) Correlation matrix of the age, weight, height, BMI, plasma levels of ssDNA (single stranded DNA), dsDNA (double stranded DNA), mtDNA (mitochondrial DNA) copy number, MPO and D-dimers with the maximal aortic diameter of patients with and without AAA. Shown are the spearman correlation coefficients for each pair of parameters. (b) Graphs illustrating simple linear regression models for D-Dimers plasma levels (left panel) or ssDNA plasma levels (right panel) and the maximal aortic diameter of patients with and without AAA.
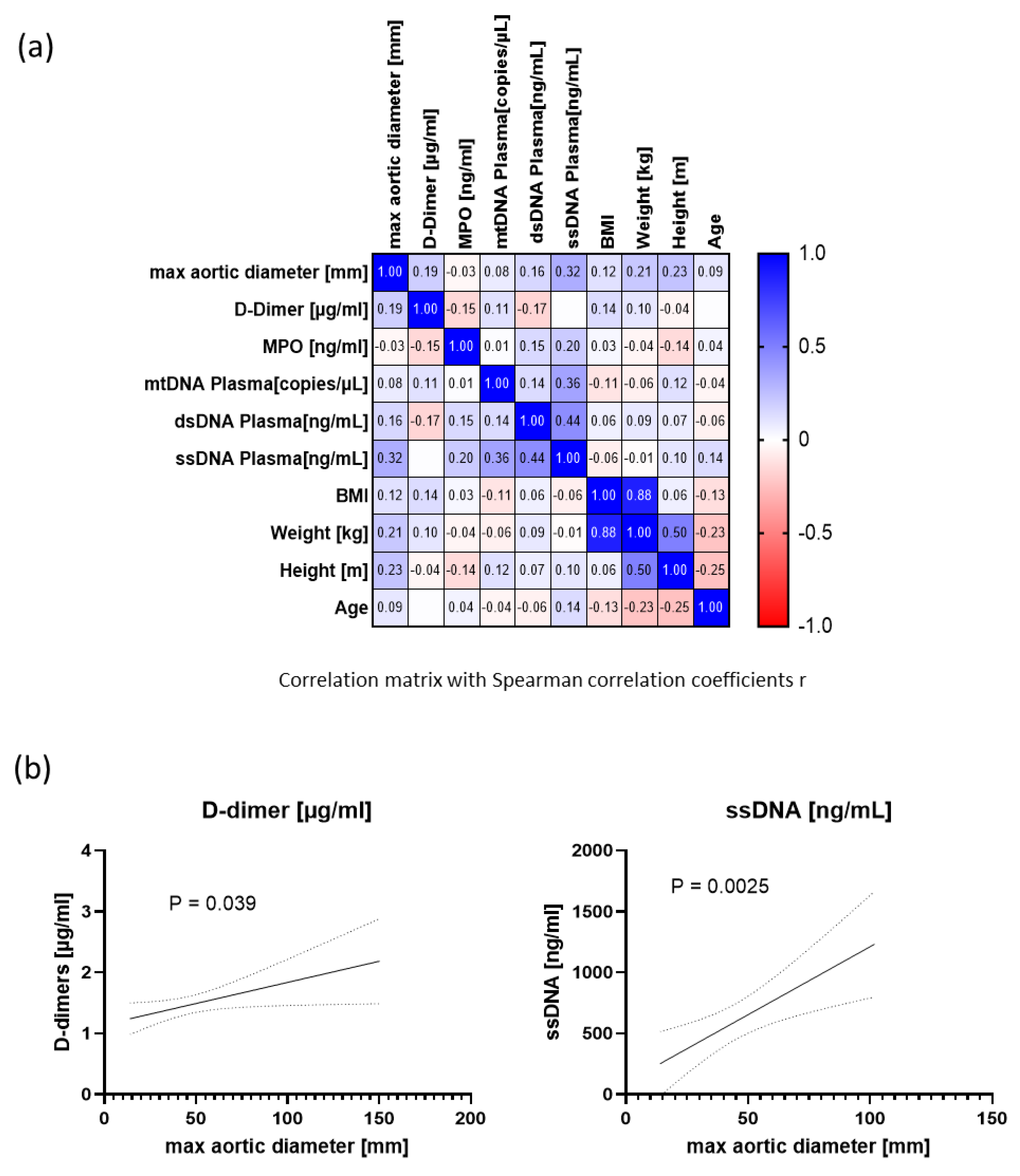

Table 1.
Patient and control demographics and co-morbidities.
| Characteristic | AAA (N = 177) Median (Range) |
Non-AAA (N = 138) Median (Range) |
P-value |
|---|---|---|---|
| age (years) | 71.00 (46-89) | 70.00 (29-85) | 0.9377 |
| Body mass index (kg/m2) | 27.29 (17.67-41.03) | 25.95 (19.14-42.97) | 0.0342 |
| max. aortic diameter (mm)# | 58.00 (30–150) | 19.00 (14-93) | <0.0001 |
|
N (%) |
N (%) |
||
| Sex | |||
| female | 25 (13.97%) | 49 (36.03%) | < 0.0001 |
| male | 154 (86.03%) | 87 (63.97%) | |
| Smoker status | |||
| current + ever | 137 (76.54%) | 83 (61.48%) | 0.0024 |
| never | 39 (21.87%) | 52 (38.52%) | |
| unknown | 3 (1.68%) | 1 (0.74%) | |
| Hypertension | 155 (86.59%) | 121 (89.63%) | 0.486 |
| Antihypertensive therapy | 149 (83.24%) | 110 (81.48%) | 0.7646 |
| Hypertriglyceridemia* | 58 (34.73%) | 42 (34.15%) | >0.9999 |
| Hypercholesterinaemia** | 160 (95.81%) | 122 (99.19%) | 0.1442 |
| Lipid-lowering therapy | 145 (81.01%) | 113 (83.70%) | 0.5555 |
| ICA stenosis | 8 (4.60%) | 83 (63.36%) | <0.0001 |
| PAD | 21 (11.73%) | 59 (43.70%) | <0.0001 |
| Antiplatelet therapy | 137 (76.54%) | 110 (81.48%) | 0.3311 |
| Coronary heart disease | 96 (53.63%) | 58 (42.96%) | 0.0685 |
| Myocardial infarction | 40 (22.35%) | 18 (13.33%) | 0.0556 |
| Stroke | 15 (8.38%) | 26 (19.26%) | 0.0064 |
| Diabetes | 31 (17.32%) | 42 (31.11%) | 0.0047 |
| Metformin therapy | 21 (11.73%) | 23 (17.04%) | 0.1922 |
| COPD | 21 (11.73%) | 8 (5.93%) | 0.1140 |
| Chronic kidney disease | 27 (15.08%) | 27 (18.52%) | 0.4457 |
| AAA family history | 12 | 0 | |
| no family history | 18 | ||
| unknown | 149 |
AAA: abdominal aortic aneurysm; ICA. Internal carotid artery; PAD: peripheral artery disease; COPD: chronic obstructive pulmonary disease; IQR: Interquartile range; #available for all AAA and 109 non-AAA; non-AAA include patients with dilative aorta due to PAU (n = 4) or dissections of the thoracic aorta (n = 4); *TAG > 150 mg/dl; **total cholesterol > 100 mg/dl.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



