
Submitted:
29 October 2024
Posted:
29 October 2024
You are already at the latest version
Abstract
Background: The increasing prevalence of Mycoplasma genitalium infections with macrolide resistance causing high azithromycin failure rates is a major concern internationally. In response to this challenge, diagnostics that simultaneously detect M. genitalium and genetic markers for macrolide resistance enable the therapy to be individually tailored, i.e. to implement resistance-guided therapy (RGT). Objectives: This study aimed to evaluate patient treatment outcomes of M. genitalium therapy guided by a macrolide-resistance assay in Bulgaria; Methods: Consecutively referred M. genitalium infection cases (n=17) were analyzed for macrolide-resistance mutations (MRMs) and specific antimicrobial treatment was recommended accordingly (MRMs-negative infections received azithromycin and MRMs-positive received moxifloxacin). Treatment outcome based on test-of-cure was recorded and treatment failure rates and time to microbiological cure were compared with treatment outcomes in patients treated before the implementation of RGT; Results: Among patients given RGT (n=17), the overall treatment failure rate was 1/17 (5.9%). This was significantly lower than the rate (47.6%) observed in patients treated pre-RGT (p=0.002). The time to microbiological cure was 29.4 days (CI 24.5 – 34.3) compared to 45.2 days (CI 36.5 – 53.7) pre-RGT (p=0.001); Conclusions: Implementation of M. genitalium diagnostics with macrolide-resistance detection improved treatment outcomes in Bulgaria with significantly lower treatment failure rates and reduced time to microbiological cure. In light of limited treatment options and concerns about their decreasing efficacy in response to misuse and overuse, diagnostic macrolide-resistance assay is critical to direct appropriate first-line treatment, to maintain the efficacy of antimicrobial treatment (antibiotic stewardship) and to minimize the spread of antimicrobial resistance.
Keywords:
Mycoplasma genitalium
; diagnostics
; macrolide-resistance assay
; resistance-guided therapy
; Bulgaria
1. Introduction
Mycoplasma genitalium causes non-gonococcal urethritis in men and cervicitis, pelvic inflammatory disease, and possibly infertility in women [1,2,3,4,5]. The appropriate diagnostic methods of M. genitalium are limited to nucleic acid amplification tests (NAATs), as culture is extremely slow (several months), challenging and insensitive [6]. In the routine practice, the use of NAATs leads to the initiation of antimicrobial therapy without antimicrobial susceptibility testing, since no viable isolates are available for the subsequent testing [7]. Due to an inherent mycoplasmas resistance to many antimicrobial classes, treatment options are scarce and the European M. genitalium guideline recommends azithromycin (0.5 g day 1, followed by 0.25 g days 2-5) as first-line treatment, and second-line treatment is moxifloxacin (400 mg per day, 7 days) [5]. For comparison, an increased azithromycin dose (1 g day 1, 0.5 g days 2–4) is used as the first-line treatment in Bulgaria, while the second-line moxifloxacin treatment is identical [8]. Treatment is becoming even more challenging due to increasing antimicrobial resistance, especially to macrolides. Multiple studies report a high prevalence of resistance and treatment failures across the globe [5,9,10,11]. Therefore, M. genitalium was recognized as an emerging global public health threat by US Centers for Disease Control and Prevention [12]. Addressing this threat requires regular updates on the extent of antimicrobial resistance and slowing its spread through optimized approaches for diagnostics and treatment (antimicrobial stewardship) until new antibiotics are developed [13]. An innovative approach in the diagnostics of M. genitalium involves simultaneous detection of both the pathogen and mutations associated with antimicrobial resistance. The additional information about resistance status allows the utilization of resistance-guided therapy (RGT) for prescribing antimicrobial that is most likely to treat the particular strain of infection. RGT of M. genitalium has been implemented in Australia, United Kingdom and Germany and demonstrated improvements in cure rate, treatment time and cost [14,15,16,17]. Furthermore, it grants a valuable tool helping to overcome the global threat of antibiotic resistance. In Bulgaria, high azithromycin failure rate (47.6%) has been observed and patients experience a lengthy time to cure, including multiple clinic visits and antibiotic courses [18]. An intervention to improve patient treatment outcomes in the context of the country’s widespread resistance and high first-line treatment failure rates became a necessity. Therefore, to guide first-line treatment, M. genitalium diagnostics with macrolide-resistance detection was implemented at the beginning of 2022.
This study aimed to evaluate patient treatment outcomes of M. genitalium therapy guided by a macrolide-resistance assay in Bulgaria by comparing (1) treatment failure rates and (2) mean time to microbiological cure before and after its implementation.
2. Materials and Methods
2.1. Study Design and Population
This was a prospective case study analysis of patients given macrolide RGT for M. genitalium infection between 1st January 2022 and 31st December 2022 at the National Center of Infectious and Parasitic Diseases in Sofia, Bulgaria. Testing was performed on referred attendees of the sexual health clinic “CheckPointSofia” for whom M. genitalium testing was indicated: presentation with symptoms and signs and/or risk factors for infection. The enrolled participants were patients, who were diagnosed with M. genitalium infection in 2022 and received specific antimicrobial treatment according to pathogen resistance status (resistance-guided therapy). Specifically, patients with M. genitalium infection in the absence of macrolide-resistance mutations (MRMs) received azithromycin (1 g day 1, 0.5 g days 2–4) and those with infection with the presence of MRMs were treated with moxifloxacin (400 mg per day, 7 days). Participants were asked to return for a test of cure (TOC) 21 days after completing the recommended antimicrobial therapy and to refrain from sexual activity until negative result. At the TOC, patients were assessed for therapy compliance and reinfection risk, and cases with non-adherence to the recommended dosing regimen and suspected reinfection were excluded. In case of treatment failure, patients were treated according to the recommendations of European M. genitalium guideline, i.e., moxifloxacin (400 mg per day, 7 days) for persistent M. genitalium infection in the presence of selected macrolide resistance after azithromycin treatment, and pristinamycin (1 g four times daily for 10 days) for persistent infection after moxifloxacin treatment [5].
2.2. Laboratory Testing
The routine diagnostics (standard care) were performed with Real-Time PCR (Mycoplasma genitalium Real-TM assay, Sacace Biotechnologies srl, Como, Italy), as per manufacturer instructions. The samples found positive for M. genitalium were further analyzed for MRMs by the ResistancePlus® MG assay (SpeeDx Pty. Ltd.). The latter uses propriety PCR technology to detect M. genitalium via the presence of MgPa gene and to detect any of the known mutations in the 23S rRNA gene associated with macrolide resistance (A2058G, A2059G, A2058C, A2059C and A2058T; E. coli numbering) [19]. Sanger sequencing of the 23S rRNA and parC genes, was performed on M. genitalium-positive samples for MRMs confirmation and determination of quinolone resistance-associated mutations (QRAMs), respectively [20,21]. In case of treatment failure, post-treatment M. genitalium-positive samples were examined for the presence of MRMs or QRAMs that are selected during azithromycin or moxifloxacin treatment, respectively.
2.3. Treatment Outcome
Treatment outcome was assessed by the treatment failure rate and the mean time to microbiological cure. Treatment failure rate was calculated as follows: numerator = number of participants with treatment failure at follow up (defined as M. genitalium positive at TOC, with or without persistent symptoms and no reinfection risk); denominator = all those treated according to macrolide-resistance assay. For both the denominator and numerator, only those who were followed up were included. Time to microbiological cure was defined as time (in days) to M. genitalium negative test from the first positive result. Mean time to microbiological cure was estimated with 95% CI.
To compare treatment outcomes before and after the implementation of M. genitalium diagnostics with macrolide-resistance detection, the treatment failure rate and the mean time to microbiological cure were compared with data from our previous M. genitalium therapy outcome study in which no macrolide-resistance assay was utilized (i.e., pre-RGT patient group) [18].
2.4. Statistical Analyses
First, the treatment failure rate as proportion and the mean time to microbiological cure with 95% confidence intervals (CI) were calculated, then Fisher’s exact test was used to compare treatment failure rates and Mann–Whitney U test to compare mean times (days) to microbiological cure. In the statistical analysis, p < 0.05 was considered significant.
2.5. Ethical Approval and Informed Consent
The study was conducted following the Declaration of Helsinki and was reviewed and approved by the institutional review board of the National Center of Infectious and Parasitic Diseases (IRB) 00006384. Written informed consent was obtained from all patients for personal data collection and microbiological sample testing.
3. Results
3.1. Selection of Cases, Treatment Outcomes and Demographic Characteristics
Twenty-two patients were diagnosed with M. genitalium during the study period (Figure 1). Four patients were ineligible as they did not receive first-line therapy according to the results of the macrolide-resistance assay. The causes for not following the macrolide RGT were syndromic management with doxycycline before establishing the diagnosis (n=3) and receiving a single-dose azithromycin with ceftriaxone for coinfection with gonorrhea (n = 1). Of the 18 enrolled participants, in 9 (50%) of the cases, no MRMs were detected and corresponding patients received azithromycin as first-line treatment. The remaining 9 cases were found to have MRMs and were treated with moxifloxacin accordingly. Of all the enrolled participants, 17 (94.5%) completed all aspects of the study and one participant with detected MRM and treated with moxifloxacin did not provide TOC samples (lost to follow-up, n=1). Overall, there were no treatment failures in those patients with MRMs-negative infections and who received azithromycin. Among the cases with detected MRMs, at TOC one case of treatment failure was observed. The case involved a patient with a persisting M. genitalium infection with no reinfection risk after moxifloxacin therapy. The patient was then successfully treated according to the European M. genitalium guideline recommendations (pristinamycin 1 g four times daily for 10 days) [5].
The median age of the patients with M. genitalium infection was 29 (age range 18–47); 14 (82.4%) were men and 3 (17.6%) were women. Twelve (85.7%) M. genitalium-positive males had symptomatic urethritis and 2 (14.3%) were asymptomatic contacts. Two (66.7%) of M. genitalium-positive females presented with cervicitis and mucopurulent discharge. The remaining one female was asymptomatic contact. The comparator group (pre-RGT patient group) consisted of cases with similar sample size and patient demographic characteristics from our previous M. genitalium therapy outcome study with no macrolide-resistance detection (Table 1) [18].
3.2. Macrolide and Quinolone Resistance Mutations (MRMs and QRAMs)
In 2022, macrolide resistance-associated 23S rRNA gene mutations were detected in 47% (8/17) of the cases by the ResistancePlus® MG assay. These results were then confirmed by 23S rRNA gene sequencing with further specification of the particular mutation at position A2058 or A2059 (E. coli numbering). The mutation A2059G (n = 7) was predominating, and the mutations A2058T and A2058G were found each in one case (Figure 2b). The distribution of the wild type and MRMs was similar in the pre-RGT and RGT groups, i.e., before and after the implementation of the M. genitalium diagnostics with macrolide-resistance detection; with overall macrolide resistance rate of 48% [18] and 47%, respectively (Figure 2a,b).
During the study period, QRAMs in the parC gene were detected in 18% of the cases. The possible resistance-associated ParC amino acid alterations were D87N (n = 2) and S83I (n = 1). The distribution of the wild type and QRAMs was similar in the pre-RGT and RGT groups, with an overall spread of possible quinolone resistance of 15% [8] and 18%, respectively (Figure 3a,b).
The spread of dual resistance (both MRMs and QRAMs present) was 9.5% and 11.7% among the pre-RGT [8,18] and RGT group, respectively (Figure 4).
No macrolide or quinolone resistance was selected during azithromycin or moxifloxacin treatment, as no further MRMs or QRAMs emerged in the post-treatment positive samples (n=1) in comparison with the pre-treatment sample. Furthermore, the observed treatment failure case involved an infection with the same MRM and QRAM in the pre- and post-treatment samples (i.e., A2058T and S83I).
3.3. Treatment Failure Rate and Mean Time to Cure
Seventeen of 18 patients given RGT returned for TOC (94.4%), comprising 14 males and 3 females. Among those, the overall treatment failure rate was 1/17 (5.9%). This was significantly lower than the treatment failure rate (47.6%) observed in patients treated pre-RGT (p = 0.002) [18]. For patients given RGT who returned for TOC (n = 17), the mean time to microbiological cure was 29.4 days (CI 24.5 – 34.3) compared to 45.2 days (CI 36.5 – 53.7) in the pre-RGT group (p=0.001).
4. Discussion
Implementation of M. genitalium diagnostics with macrolide-resistance detection in Bulgaria improved patient treatment outcomes in a population where almost half of the
cases are macrolide-resistant. That was achieved by selecting the first-line antimicrobial according to a macrolide-resistance assay, that was performed as an addition to routine molecular diagnostics. The overall treatment failure rate observed in this study was 5.9%, which was significantly lower than the treatment failure rate (47.6%) in the Bulgarian patients group before the implementation of the resistance assay (p = 0.002). The mean time to microbiological cure was 29.4 days (CI 24.5 – 34.3) compared to 45.2 days (CI 36.5 – 53.7) (p=0.001) [18]. These results are consistent with other studies that have clinically demonstrated to improve patient cure rate and to reduce time to cure in the M. genitalium patient management. In Australia, the implementation of M. genitalium diagnostics with macrolide-resistance detection dramatically improved the cure rate to 93% in 2018 in comparison to 2013 (~40%) [14]. The preliminary rate of successful eradication from Germany (93.3%) was favorable for the continuation of the diagnostic strategy including macrolide-resistance detection [17]. In the United Kingdom treatment failure rate was significantly reduced (3%) compared to before the implementation of M. genitalium diagnostics with macrolide-resistance detection (27%) (p = 0.008) [16]. Furthermore, there was a trend of a shorter time to a negative TOC in male urethritis (55.1 [95% 43.7–66.4] vs. 85.1 [95% 64.1–106.0] days, p = 0.077) [16].
Among those patients who had MRMs-negative infections and received azithromycin, there were no treatment failures observed and accordingly no macrolide resistance was selected during treatment. Nevertheless, mycoplasmas have a high mutation rate and random MRMs may spontaneously emerge in a population of wild-type M. genitalium bacteria during the treatment of the infection [22]. A meta-analysis by Horner et al. found that an extended azithromycin regimen for M. genitalium (500 mg on day 1 followed by 250 mg on days 2–5; 1.5 g total oral dose) may be more effective than a 1 g of azithromycin single oral dose and is less likely to cause selection of macrolide resistance [23]. The absence of selected MRMs during azithromycin treatment in this study may indicate a lower selection rate using the increased azithromycin dose in Bulgaria (2.5 g total oral dose) compared to azithromycin 1 g single dose and azithromycin extended 1.5 g regimen [24].
Although the prevalence of reported macrolide resistance varies substantially between regions and countries [10], macrolide resistance has been rapidly increasing and is now above 50% in many countries around the globe [25]. Consequently, M. genitalium diagnostics with macrolide-resistance detection is encouraged in most international guidelines [5,26,27,28,29,30]. In this study, a high rate of macrolide resistance (47%) in M. genitalium infections was reported from Bulgaria in 2022. Similar high rates were also observed in the previous years in Bulgaria [8,18]. These high antimicrobial resistance rates in M. genitalium have emerged in Bulgaria in the context of no or very limited M. genitalium testing and no national M. genitalium antimicrobial resistance surveillance. Accordingly, no recommendations for patient management (diagnostics and treatment) exist yet in Bulgaria. In most settings macrolides, particularly an increased azithromycin dose (1 g day 1, 0.5 g days 2–4), have been preferred as empirical first-line treatment, and macrolide-resistance detection is performed only at the National Center of Infectious and Parasitic Diseases. The findings of the present study, including the high rate of macrolide resistance, clearly emphasize that routine macrolide-resistance detection before starting therapy for M. genitalium infections is imperative also in Bulgaria.
Among those patients who had MRMs-positive infections and received moxifloxacin, one case of treatment failure was observed. The case involved a persisting M. genitalium infection after moxifloxacin therapy with no reinfection risk. Molecular analysis revealed that it was caused by M. genitalium strain with dual resistance (both MRM and QRAM detected) and no macrolide or quinolone resistance selected during treatment (i.e., A2058T and S83I detected in the pre- and post-treatment samples). That finding poses a grave concern because no highly effective and accessible third-line treatment for M. genitalium infections is present. Accordingly, the European M. genitalium guideline recommends pristinamycin, minocycline or doxycycline, and none of these antimicrobials cure all M. genitalium cases (with observed cure rates of 75%, 70% and 40%, respectively) [5]. Furthermore, pristinamycin is expensive and is not available in many countries worldwide, including Bulgaria, and has to be explicitly imported by clinicians.
The prevalence of QRAMs is increasing worldwide [10], and the reported QRAM rates range from less than 5% in northern Europe up to around 20% in southern Europe [25]. However, scientific evidence indicates that not all QRAMs cause quinolone resistance in vitro, and the association between mutations and treatment failure is not well established (24). Accordingly, the most significant QRAM (i.e., S83I) leads to moxifloxacin failure in only 60% of the treated patients, but the absence of the S83I is highly predictive of moxifloxacin cure (96.4%; 95% CI, 93.7 to 98.2) [31]. That suggests that incorporating the detection of quinolone resistance in M. genitalium diagnostics would not be as successful in determining the first-line treatment, but rather in individualizing the TOC [32,33]. Furthermore, a novel therapeutic approach (i.e., resistance-guided sequential therapy) has shown higher cure rates and lower selection of resistance in populations with high prevalence of macrolide and quinolone resistance [14,15]. That approach comprises sequential therapy by pretreating with doxycycline and selecting the second antimicrobial with a macrolide-resistance assay. In this study, a high prevalence of QRAMs (18%) in M. genitalium infections was demonstrated in Bulgaria in 2022. In the country, a widespread prevalence of QRAMs was likewise observed in the previous years [8]. However, the current study reports the first verified case of moxifloxacin treatment failure. Nevertheless, because of the lack of consistency in the association of QRAMs with the treatment outcomes, the detection of quinolone resistance in Bulgaria is not indicated outside of scientific research. Resistance-guided sequential therapy appears to be a viable approach among Bulgarian patients to delay further emergence and spread of antimicrobial resistance. Ultimately, novel effective and affordable antimicrobials for the treatment of M. genitalium infections are essential.
The main limitation of this study was the small sample size from one sexual health clinic in Sofia, Bulgaria. However, given the reported high rate of treatment failures in Bulgaria [18], the study results provide necessary information about preliminary monitoring of treatment outcomes after the implementation of macrolide-resistance assay until further data with more samples become available. Another limitation was that patients were recommended treatment according to ResistancePlus® MG assay results, which is slightly less sensitive than the gold standard of Sanger sequencing [34,35]. Nevertheless, the confirmatory 23S rRNA sequencing performed in the study showed that all eligible participants were correctly allocated for the appropriate treatment by the ResistancePlus assay. A further concern is the increased cost of the M. genitalium diagnostics when incorporating the macrolide-resistance assay. In this regard, a recent study in Australia showed that this diagnostic approach is cost-effective for M. genitalium infections, supporting its adoption as a national management strategy [36].
5. Conclusions
Implementation of M. genitalium diagnostics with macrolide-resistance detection improved treatment outcomes in Bulgaria with significantly lower treatment failure rates and reduced time to microbiological cure. In light of limited treatment options and concerns about their decreasing efficacy in response to misuse and overuse, diagnostic macrolide-resistance assay is critical to direct appropriate first-line treatment, to maintain the efficacy of antimicrobial treatment (antibiotic stewardship) and to minimize the spread of antimicrobial resistance.
Author Contributions
Conceptualization, I.P. and V.L.; methodology, I.P.; software, V.M.; validation, M.M., V.M. and I.P.; formal analysis, M.M.; investigation, E.B.; resources, E.B.; data curation, I.P.; writing—original draft preparation, I.P.; writing—review and editing, M.M., E.B., V.M and V.L.; visualization, I.P.; supervision, V.L.; project administration, I.P. and V.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board of the National Center of Infectious and Parasitic Diseases 00006384.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data are available upon reasonable request from the author for correspondence (I.P.)
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Sonnenberg P, Ison CA, Clifton S, Field N, Tanton C, Soldan K, et al. Epidemiology of Mycoplasma genitalium in British men and women aged 16–44 years: evidence from the third National Survey of Sexual Attitudes and Lifestyles (Natsal-3). Int J Epidemiol. 2015, 44, 1982–1994. [Google Scholar] [CrossRef] [PubMed]
- Edouard S, Tissot-Dupont H, Dubourg G, Bernard A, Fournier P, Ravaux I, et al. Mycoplasma genitalium, an agent of reemerging sexually transmitted infections. Apmis. 2017, 125, 916–920. [Google Scholar] [CrossRef] [PubMed]
- Taylor-Robinson D, Jensen JS. Mycoplasma genitalium: from Chrysalis to multicolored butterfly. Clin Microbiol Rev. 2011, 24, 498–514. [Google Scholar] [CrossRef]
- Lis R, Rowhani-Rahbar A, Manhart LE. Mycoplasma genitalium infection and female reproductive tract disease: a meta-analysis. Clin Infect Dis. 2015, 61, 418–426. [Google Scholar] [CrossRef]
- Jensen JS, Cusini M, Gomberg M, Moi H, Wilson J, Unemo M. 2021 European guideline on the management of Mycoplasma genitalium infections. J Eur Acad Dermatology Venereol. 2022, 36, 641–650. [Google Scholar] [CrossRef]
- Jensen JS, Hansen HT, Lind K. Isolation of Mycoplasma genitalium strains from the male urethra. J Clin Microbiol. 1996, 34, 286–291. [Google Scholar] [CrossRef]
- Wihlfahrt K, Günther V, Mendling W, Westermann A, Willer D, Gitas G, et al. Sexually Transmitted Diseases—An Update and Overview of Current Research. Diagnostics. 2023, 13, 1656. [Google Scholar] [CrossRef]
- Philipova I, Hadad R, Levterova V, Kantardjiev T, Unemo M. Mycoplasma genitalium antimicrobial (azithromycin and moxifloxacin) resistance and treatment outcome in Sofia, Bulgaria, 2018-2021. J Eur Acad Dermatology Venereol. 2023 Mar 27;n/a(n/a). [CrossRef]
- Lau A, Bradshaw CS, Lewis D, Fairley CK, Chen MY, Kong FYS, et al. The efficacy of azithromycin for the treatment of genital Mycoplasma genitalium: a systematic review and meta-analysis. Clin Infect Dis. 2015, 61, 1389–1399. [Google Scholar] [CrossRef]
- Machalek DA, Tao Y, Shilling H, Jensen JS, Unemo M, Murray G, et al. Prevalence of mutations associated with resistance to macrolides and fluoroquinolones in Mycoplasma genitalium: a systematic review and meta-analysis. Lancet Infect Dis. 2020, 20, 1302–1314, Available from: https://www.sciencedirect.com/science/article/pii/S1473309920301547. [Google Scholar] [CrossRef]
- Li Y, Le W-J, Li S, Cao Y-P, Su X-H. Meta-analysis of the efficacy of moxifloxacin in treating Mycoplasma genitalium infection. Int J STD AIDS. 2017, 28, 1106–1114. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Antibiotic resistance threats in the United States, 2019. US Department of Health and Human Services, Centres for Disease Control and Prevention; 2019.
- Sakalauskienė G V, Radzevičienė A. Antimicrobial Resistance: What Lies Beneath This Complex Phenomenon? Diagnostics. 2024, 14, 2319. [Google Scholar] [CrossRef] [PubMed]
- Read TRH, Fairley CK, Murray GL, Jensen JS, Danielewski J, Worthington K, et al. Outcomes of resistance-guided sequential treatment of Mycoplasma genitalium infections: a prospective evaluation. Clin Infect Dis. 2019, 68, 554–560. [Google Scholar] [CrossRef] [PubMed]
- Durukan D, Read TRH, Murray G, Doyle M, Chow EPF, Vodstrcil LA, et al. Resistance-Guided Antimicrobial Therapy using doxycycline–moxifloxacin and doxycycline–2.5 g azithromycin for the treatment of Mycoplasma genitalium infection: Efficacy and tolerability. Clin Infect Dis. 2020, 71, 1461–1468. [Google Scholar] [CrossRef] [PubMed]
- Conway RJH, Cook S, Malone C, Bone S, Hassan-Ibrahim MO, Soni S. Resistance-guided treatment of Mycoplasma genitalium infection at a UK sexual health centre. Int J STD AIDS. 2021, 32, 758–765. [Google Scholar] [CrossRef]
- Dumke R, Spornraft-Ragaller P. Antibiotic Resistance and Genotypes of Mycoplasma genitalium during a Resistance-Guided Treatment Regime in a German University Hospital. Antibiotics 2021, 10, 962. [Google Scholar] [CrossRef]
- Philipova I, Levterova V, Simeonovski I, Kantardjiev T. Azithromycin treatment failure and macrolide resistance in Mycoplasma genitalium infections in Sofia, Bulgaria. Folia medica (Plovdiv). 2022, 64, 422–429. [Google Scholar] [CrossRef]
- Tabrizi SN, Tan LY, Walker S, Twin J, Poljak M, Bradshaw CS, et al. Multiplex assay for simultaneous detection of Mycoplasma genitalium and macrolide resistance using PlexZyme and PlexPrime technology. PLoS One. 2016, 11, e0156740. [Google Scholar]
- Jensen JS, Bradshaw CS, Tabrizi SN, Fairley CK, Hamasuna R. Azithromycin treatment failure in Mycoplasma genitalium-positive patients with nongonococcal urethritis is associated with induced macrolide resistance. Clin Infect Dis. 2008, 47, 1546–1553. [Google Scholar] [CrossRef]
- Deguchi T, Maeda S-I, Tamaki M, Yoshida T, Ishiko H, Ito M, et al. Analysis of the gyrA and parC genes of Mycoplasma genitalium detected in first-pass urine of men with non-gonococcal urethritis before and after fluoroquinolone treatment. J Antimicrob Chemother. 2001, 48, 742–744. [Google Scholar] [CrossRef]
- Twin J, Jensen JS, Bradshaw CS, Garland SM, Fairley CK, Min LY, et al. Transmission and selection of macrolide resistant Mycoplasma genitalium infections detected by rapid high resolution melt analysis. PLoS One. 2012, 7, e35593. [Google Scholar]
- Horner P, Ingle SM, Garrett F, Blee K, Kong F, Muir P, et al. Which azithromycin regimen should be used for treating Mycoplasma genitalium? A meta-analysis. Sex Transm Infect. 2018, 94, 14–20. [Google Scholar] [CrossRef] [PubMed]
- Read TRH, Fairley CK, Tabrizi SN, Bissessor M, Vodstrcil L, Chow EPF, et al. Azithromycin 1.5 g over 5 days compared to 1g single dose in urethral Mycoplasma genitalium: impact on treatment outcome and resistance. Clin Infect Dis. 2017, 64, 250–256. [Google Scholar] [CrossRef] [PubMed]
- Jensen JS, Unemo M. Antimicrobial treatment and resistance in sexually transmitted bacterial infections. Nat Rev Microbiol. 2024, 1–16. [Google Scholar] [CrossRef]
- Public Health Agency of Canada. Mycoplasma genitalium guide: key information and resources. [Internet]. Government of Canada. 2023. Available from: https://www.canada.ca/en/public-health/services/infectious-diseases/sexual-health-sexually-transmitted-infections/canadian-guidelines/mycoplasma-genitalium.html#Key_information.
- Wada K, Hamasuna R, Sadahira T, Araki M, Yamamoto S. UAA-AAUS guideline for M. genitalium and non-chlamydial non-gonococcal urethritis. J Infect Chemother. 2021, 27, 1384–1388. [Google Scholar] [CrossRef]
- Workowski KA. Sexually transmitted infections treatment guidelines, 2021. MMWR Recomm Reports. 2021, 70. [CrossRef]
- Fifer H, Saunders J, Soni S, Sadiq ST, FitzGerald M. British Association for Sexual Health and HIV national guideline for the management of infection with Neisseria gonorrhoeae (2019). London: British Association for Sexual Health and HIV; 2019.
- The Australasian STI management guidelines. Mycoplasma genitalium [Internet]. The Australasian Sexual and Reproductive Health Alliance (ASHA). 2021. Available from: https://sti.guidelines.org.au/sexually-transmissible-infections/mycoplasma-genitalium/.
- Murray GL, Bodiyabadu K, Vodstrcil LA, Machalek DA, Danielewski J, Plummer EL, et al. parC variants in Mycoplasma genitalium: trends over time and association with moxifloxacin failure. Antimicrob Agents Chemother. 2022, 66, e00278–22. [Google Scholar]
- Sweeney EL, Bradshaw CS, Murray GL, Whiley DM. Individualised treatment of Mycoplasma genitalium infection—incorporation of fluoroquinolone resistance testing into clinical care. Lancet Infect Dis. 2022, 22, e267–70. [Google Scholar] [CrossRef]
- Manhart LE, Jensen JS. Quinolone Resistance–Associated Mutations in Mycoplasma genitalium: Not Ready for Prime Time. Sex Transm Dis. 2020, 47, 199. [Google Scholar] [CrossRef]
- Tabrizi SN, Su J, Bradshaw CS, Fairley CK, Walker S, Tan LY, et al. Prospective evaluation of ResistancePlus MG, a new multiplex quantitative PCR assay for detection of Mycoplasma genitalium and macrolide resistance. J Clin Microbiol. 2017, 55, 1915–1919. [Google Scholar] [CrossRef]
- Le Roy C, Pereyre S, Hénin N, Bébéar C. French prospective clinical evaluation of the Aptima Mycoplasma genitalium CE-IVD assay and macrolide resistance detection using three distinct assays. J Clin Microbiol. 2017, 55, 3194–3200. [Google Scholar] [CrossRef]
- Adawiyah R Al, Bradshaw CS, Vodstrcil LA, Fairley CK, Zhang L, Ong JJ. Cost-effectiveness of resistance-guided therapy for Mycoplasma genitalium in Australia. Sci Rep. 2024, 14, 12856. [Google Scholar] [CrossRef]
Figure 1.
Selection of cases and outcomes of M. genitalium therapy guided by diagnostics with macrolide-resistance detection from Bulgaria, 2022.
Figure 1.
Selection of cases and outcomes of M. genitalium therapy guided by diagnostics with macrolide-resistance detection from Bulgaria, 2022.
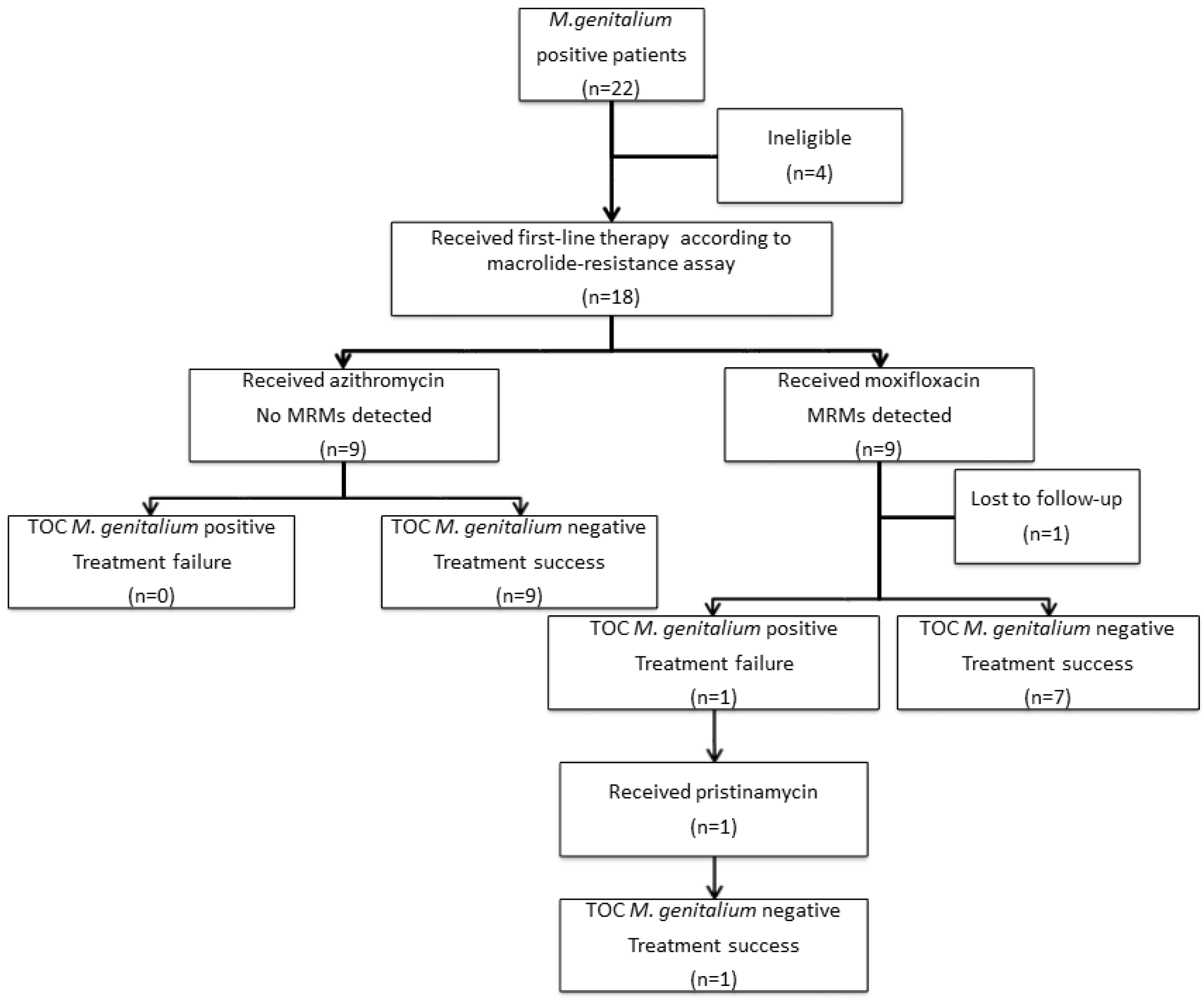
Figure 2.
Distribution of wild type and different MRMs in M. genitalium positive cases: (a) before the implementation of the M. genitalium diagnostics with macrolide-resistance detection, n=21 (pre-RGT group) [18]; (b) after the implementation of the M. genitalium diagnostics with macrolide-resistance detection, n=18 (RGT current study group).
Figure 2.
Distribution of wild type and different MRMs in M. genitalium positive cases: (a) before the implementation of the M. genitalium diagnostics with macrolide-resistance detection, n=21 (pre-RGT group) [18]; (b) after the implementation of the M. genitalium diagnostics with macrolide-resistance detection, n=18 (RGT current study group).
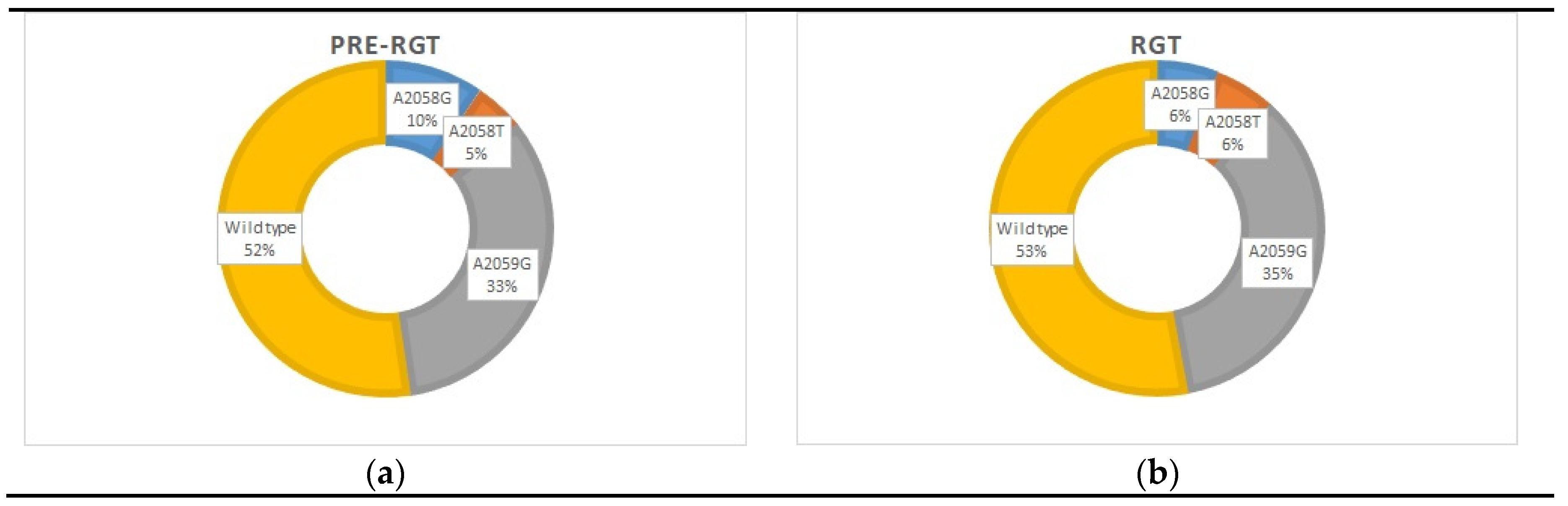
Figure 3.
Distribution of wild type and different QRAMs in M. genitalium positive cases: (a) before the implementation of the M. genitalium diagnostics with macrolide-resistance detection, n=21 (pre-RGT group) [8]; (b) after the implementation of the M. genitalium diagnostics with macrolide-resistance detection, n=18 (RGT current study group).
Figure 3.
Distribution of wild type and different QRAMs in M. genitalium positive cases: (a) before the implementation of the M. genitalium diagnostics with macrolide-resistance detection, n=21 (pre-RGT group) [8]; (b) after the implementation of the M. genitalium diagnostics with macrolide-resistance detection, n=18 (RGT current study group).
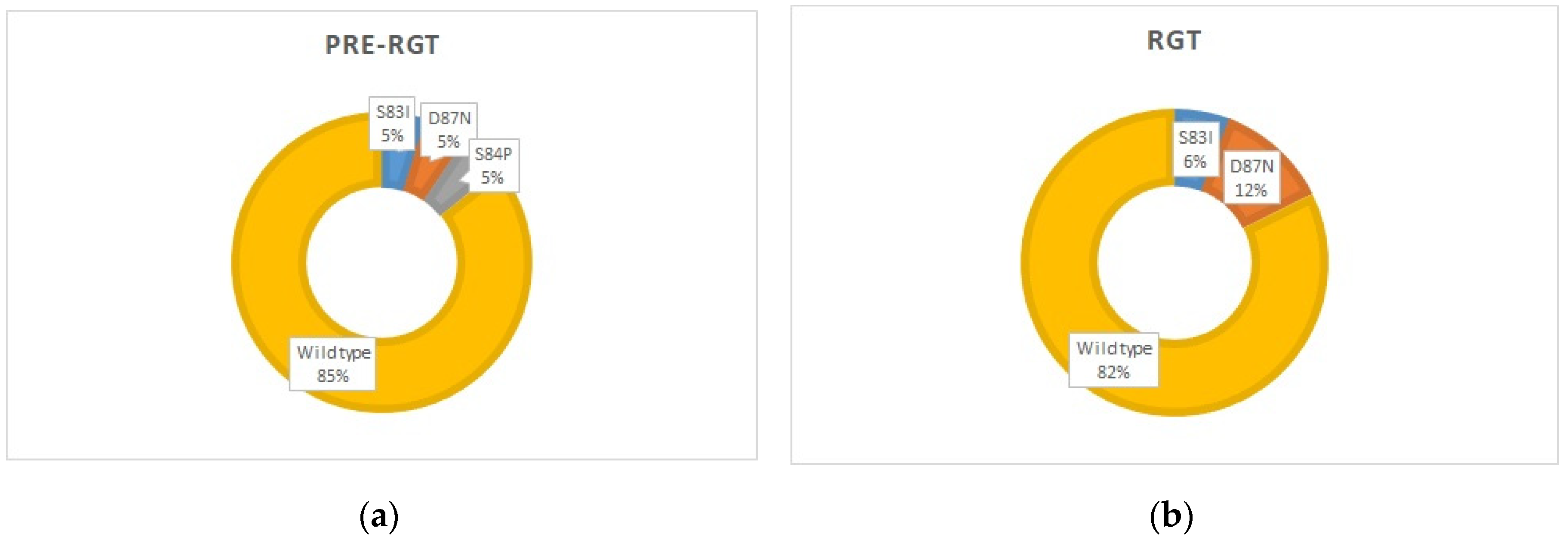
Figure 4.
Rates of dual resistance (both MRMs and QRAMs present) before and after the implementation of the M. genitalium diagnostics with macrolide-resistance detection (pre-RGT group, n=21 [8,18] and RGT group, n=17).
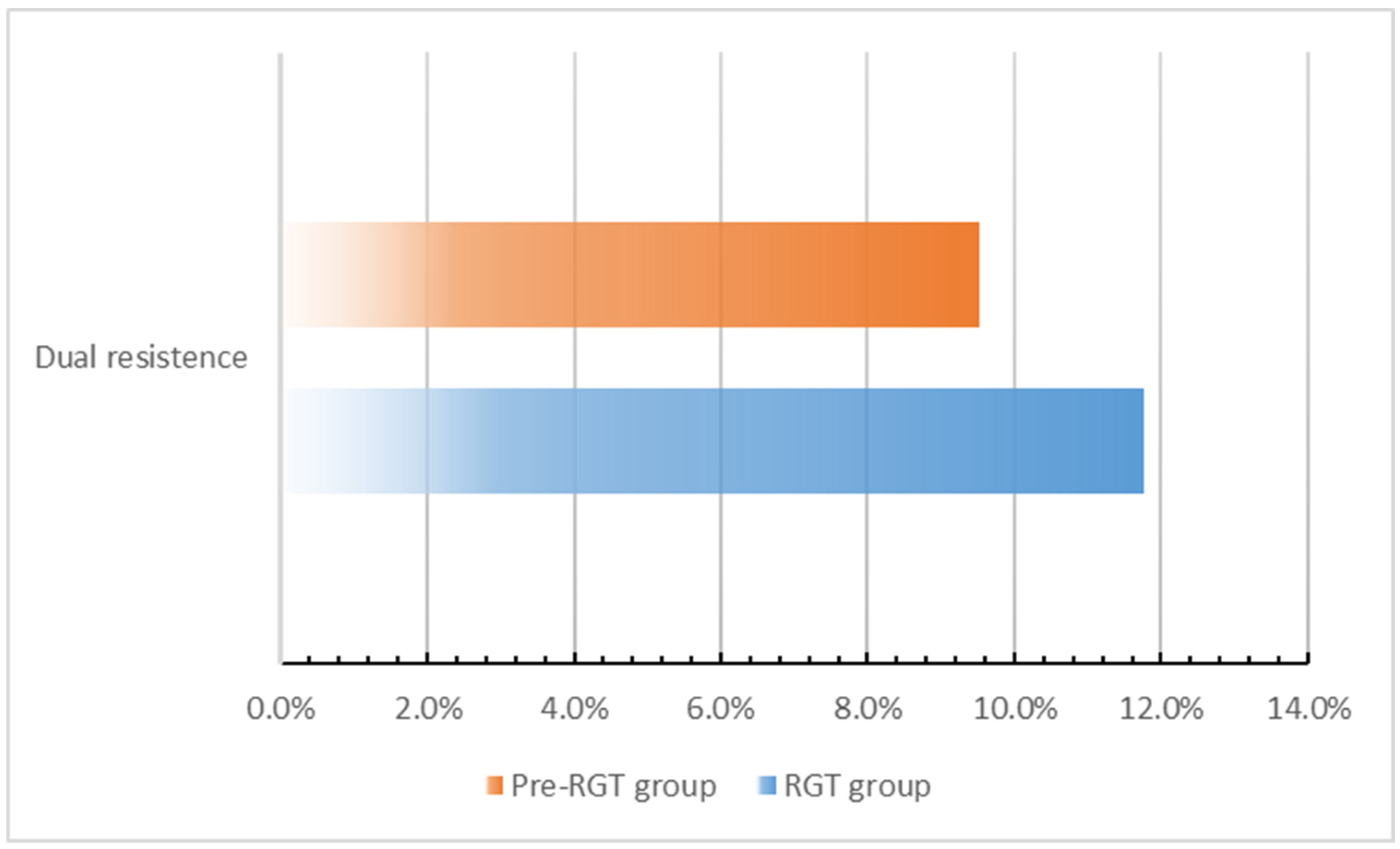

Table 1.
Characteristics of the patients before (pre-RGT group) and after (RGT current study group) the implementation of M. genitalium diagnostics with macrolide-resistance detection.
Table 1.
Characteristics of the patients before (pre-RGT group) and after (RGT current study group) the implementation of M. genitalium diagnostics with macrolide-resistance detection.
| pre-RGT group [18], n (%) |
RGT, n (%) | |||
| Male (n = 18) | Female (n = 3) | Male (n = 14) | Female (n = 3) | |
| Median age (range) | 32 (22-49) | 28 (23-33) | 29 (18-47) | 29 (23-34) |
| Presentation | ||||
| Symptomatic | 15 (83.3) | 1 (33.3) | 12 (85.7) | 2 (66.7) |
| Asymptomatic contact | 3 (16.7) | 2 (66.7) | 2 (14.3) | 1 (33.3) |
| Specimen | ||||
| First-void urine | 14 (77.8) | 0 (0) | 7 (50) | 0 (0) |
| Urogenital swab | 4 (22.2) | 3 (100) | 5 (35.7) | 3 (100) |
| Extra-genital swab | 0 (0) | 0 (0) | 2 (14.3) | 0 (0) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



