
Submitted:
29 October 2024
Posted:
31 October 2024
You are already at the latest version
Abstract
Multisensory spaces have been used across a number of health and social care contexts to promote well-being, engage the senses and promote inclusion by providing places where people can come together. Much of the existing research on such spaces focus on children or older adults with little investigation dedicated to spaces inclusive of both. Utilising multisensory spaces which bring together children and older adults can reduce costs and lead to opportunities for shared learning. We sought to identify empirical research which investigated the use of multisensory spaces for intergenerational participants. The Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines were used to guide this review. Five electronic databases (PsycINFO, CINAHL, Web of Science, Embase, Pubmed) were interrogated using search terms developed in collaboration with a specialist subject librarian around the concepts of ‘intergenerational’ and ‘multisensory’. Two authors independently applied the agreed upon eligibility criteria to the titles and abstracts of potential articles for inclusion. Once the final articles had been identified, the authors independently extracted data and assessed quality of the included studies. Data were subjected to narrative synthesis. Following review of 979 titles and abstracts, 3 articles were identified for inclusion. Quality appraisal rated these as between 3 to 6 out of a possible total of 7. Narrative synthesis identified three themes named as Independence, Connecting with others and Equitable multisensory space design. Multisensory spaces offer the potential to deliver care within health and social care contexts which caters to the needs of children and older adults. There is a need to co-create such spaces with service users and other stakeholders to ensure they adequately meet the needs of all.
Keywords:
intergenerational
; multisensory space
; scoping review
; health
; community
1. Introduction
The design and use of multisensory spaces (MSS), also referred to as multisensory environments (MSE), have garnered significant attention across education, health and social care and community services (1–3). MSS are environments specifically designed to stimulate the senses or promote a sense of relaxation and well-being (3,4). These spaces are increasingly recognised for their potential to enhance the well-being and quality of life for diverse populations, including children and older adults especially those with complex health, social, behavioural and emotional needs (5,6).
For children, MSS can provide an exciting and engaging environment that can support cognitive, behavioural and emotional development and regulation (7,8). Such spaces provide opportunities for experiential learning, sensory integration, and therapeutic interventions, especially beneficial for children who have experienced trauma, those with sensory processing disorders, autism spectrum disorders (ASD), and other developmental challenges (9–11). By engaging multiple senses simultaneously, these environments can foster attention, communication, and social interaction skills, thereby contributing to more effective learning and personal growth (7). A therapist working with high and low functioning children and adolescents with ASD in a controlled multisensory interactive room demonstrated statistically significant improvements in attention, inhibition and receptive communication (9). The authors suggest further comparative work is required with other environments and to determine whether findings are generalisabile to everyday life.
Older adults may face a different set of challenges, including physical and sensory decline, cognitive impairments, and social isolation (12–14). MSS can be employed to address some of these issues by creating experiences that stimulate cognitive function and improve quality of life (15,16). For individuals with dementia, multisensory stimulation can evoke positive memories, reduce agitation, and improve overall mood and behaviour (16–18). Furthermore, these spaces can serve as valuable tools in providing informal therapeutic settings, offering non-pharmacological interventions that enhance the quality of life for older adults (19). Snoezelen rooms have been widely used as MSE with older adults (20). These rooms utilise lights, music, colour and texture to stimulate the senses or create calming and relaxing environments (20). A study with 24 older adults with dementia compared a Snoezelen room with a landscaped garden and a communal living room (19). The authors reported positive effects on the well-being of participants but also on that of relatives, visitors and staff. More sadness was reported by participants during their time spent in the living room environment compared to both the garden and Snoezelen room (19).
The integration of MSS in health and social care facilities, and community settings which provide care to all underscores the importance of creating inclusive environments that cater to the needs of diverse individuals. A study exploring the use of Snoezelen on the autism symptoms of adolescents and adults (aged 16-35, Mean = 23.7 years) with ASD showed statistically significant differences between the control (no treatment) and intervention (Snoezelen) groups assessed using the Childhood Autism Rating Scale (10). MSS are increasingly recognised as providing benefits to both children and adults. This scoping review sought to explore and synthesise the existing evidence-base for the use of MSS for both children and older adults. Many studies have looked at either children or older adults, therefore we wished to explore this issue in relation to those which included both groups. Therefore this scoping review explores the applications and benefits of MSS for children and older adults. Through a comprehensive review of the international evidence, we aim to highlight the potential of these environments to support sensory, cognitive, behavioural, and emotional well-being for both cohorts.
2. Materials and Methods
2.1. Search Strategy
The authors conducted a thorough search of the existing literature to identify search terms for inclusion in this review. Further, we consulted with a specialist subject librarian to ascertain the best way to combine these terms and identify the most appropriate electronic databases to be used in this review. The search strategy was built around our research question and focused on two key themes, ‘intergenerational’ and ‘sensory spaces’ (see Table 1 for a list of search terms). All searches were undertaken in November 2023.
2.2. Information Sources
Five databases were employed in this review and included Pubmed, CINAHL complete, Embase, PsychInfo (1806 to present), and Web of Science (core collection). These databases were selected due to their comprehensive coverage of the evidence base and relevance to the research question.
2.3. Eligibility Criteria
We sought to include only empirical studies which focused on the investigation of sensory spaces for intergenerational participants i.e. those which included both children and older adults. We defined older adults as those over 65 years of age. Included studies had to be peer reviewed and published in the English language. We excluded any review articles, unpublished dissertations, opinion articles and conference abstracts. Articles which focused on specialist populations (e.g. offenders or psychiatric in-patients) and education settings (mainstream and additional needs settings), were also excluded.
2.4. Selection Process
Our searches identified a total of 1847 possible articles for inclusion from the five selected databases: PubMed (n=452), Web of Science (n=343), Embase (n=642), PsycINFO (n=249) and CINAHL (n=161). These were imported into Covidence (21), an online systematic reviewing tool, where 868 duplicates were removed. The eligibility criteria were applied to the titles and abstracts of the remaining articles (n=979) and (n=958) were removed. Twenty-one articles were retrieved for full text review. Following review of the full texts, 18 further articles were excluded. The reasons for exclusion included articles only focusing on children or only on adults or those which focused on specialist populations and contexts (e.g., psychiatric hospitals). Therefore, this review included 3 studies that were carried forward for analysis. See Figure 1 for the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) (22) flowchart.
2.5. Data Extraction
The authors of this study independently screened and extracted data from all included articles. A standardised data extraction tool was used to ensure key areas of interest were identified in each article and to allow for consistency. Discrepancies of judgements were discussed until consensus was reached. The data extraction tool included information on author name, date of publication, country of origin, study aim, study design, participants, measurements and key findings. A summary of characteristics of the included studies can be found in Table 2.
2.6. Quality Assessment
The mixed methods assessment tool (MMAT) (23) was used to assess the methodological quality of included articles. The MMAT comprises two initial screening questions which seek to determine whether the article includes a clear research question and whether data collection can address this question. The reviewer then decides which of five possible research designs the article uses, before answering five questions relating to that design. Questions are answered as ‘yes’, ‘no’ or ‘can’t tell’ with only ‘yes’ receiving a point. Each study can be rated out of a possible 7 points. See Table 3 for a summary of the quality appraisal of articles included in this review.
2.7. Data Analysis
Due to the diverse nature of study designs found among the included papers the authors chose to conduct a narrative synthesis (24) of study findings. A narrative synthesis seeks to identify common themes across included studies to highlight core areas of work.
3. Results
3.1. Characteristic of Included Studies
Studies included in this review were published between 2020 and 2023 and utilised a qualitative approach (25), a pre post-test design (26), and mixed methods (3). They were conducted in Canada (25), Russia (26) and New Zealand (3). Participants comprised school children, healthcare professionals, parents, older adults, disabled adults and support persons. Malysheva et al (26) sought to explore physiological changes in school children, youths and older adults after walking in a park. Litwin et al (25) sought to co-design a paediatric procedures room in a hospital, while Wilkinson et al (3) explored the experiences of disabled users of a multisensory room (See Table 2 for characteristics of included studies).
3.2. Quality Appraisal of Included Studies
Quality appraisal using the MMAT showed that Litwin et al’s (25) work had been conducted to a high standard, scoring 6 out of a possible 7. The main criticism of this paper was the failure to provide sufficient illustrative quotes to determine whether their interpretation was adequately supported. Malysheva et al (26) scored 4 out of 7 due to a lack of explanation of their analysis, approach to recruitment and underrepresentation of younger children. Wilkinson et al (3) scored 3 out of 7 due to a lack of explanation for their choice of a mixed methods design and lack of integration of their qualitative and quantitative findings.
3.3. Narrative Synthesis
3.3.1. Independecne
The need for children and older adults to exist in safe spaces which fostered a sense of autonomy was a common theme across all three included studies. Wilkinson et al (3) and Litwin et al (25) found that self-determination and control were important components of MSS. This was both in relation to the individual’s ability to adapt and interact with and exert some control of the space, but also in their ability to choose to engage in whatever aspect of the environment they desired. Participants wanted spaces in which they felt safe, secure and respected. Malysheva et al (26) found that mental capacity, and visual and auditory memory improved in older people in their study, following a walk in the park. Improved cognitive functioning has implications for independence among older adults and children and young people alike.
3.3.2. Connecting with Others
The importance of having spaces where people could come together for a range of purposes from recreation, to consultation, treatment and to socialise was readily apparent. In addition to the physiological benefits of spending time walking in a park (26), the act of being around and interacting with other park users can enhance social connections and create a sense of community. A multisensory space in a hospital must serve multiple purposes due to the shortage of available space and the needs and range of likely users. Litwin et al (25) highlight that such spaces should contain areas that are age appropriate and flexible to enable people to come and go as needed whilst also accommodating the wide array of equipment that may be required. Wilkinson et al’s (3) community space was designed to allow social connection between disabled users of all ages with users describing how much they enjoyed the opportunity to chat with others. These interactions were seen as important for enhancing users’ wellbeing whilst also providing respite for family carers.
3.3.3. Equitable Multisensory Spaces
Participants in both Litwin et al (25) and Wilkinson et al’s (3) research discussed the importance of inclusive and adaptable multisensory spaces which were welcoming to users and carers alike. Participants in Wilkinson’s et al (3) study highlighted issues of accessibility in relation to individuals with conditions which limited their physical capabilities. For example, a space which could only be accessed via stairs excluded those who utilised assistive walking aids. Explicit or implicit rules of the multisensory space could create barriers or facilitate equitable treatment of users (3). This might occur through a lack of clarity around expectations of users (e.g. who was responsible for setting-up the space and for ensuring this was ready for new users or whether users were aware that they could alter features within the spaces and interact with lighting and sound etc), or through procedural difficulties in gaining access to the booking system (3).
4. Discussion
This scoping review sought to identify and synthesise the evidence for the use of multisensory spaces that are inclusive of children and older adults. Much research has been conducted which examines the use of such spaces for children or older adults, but little has sought to include both groups. Given the financial pressures facing health and social care organisations which cater to multiple groups across the lifespan (27–29), multisensory spaces which serve diverse stakeholders are increasingly required. Three studies were identified which included both groups indicating that this is an under researched area which requires further exploration. Quality appraisal of the included studies rated Litwin et al’s (25) qualitative research highest (6 out of 7), followed by Malysheva et al’s (26) experimental design (4 out of 7) and Wilkinson et al’s (3) mixed methods research (3 out of 7). The lower quality scores related mainly to a lack of justification of study methodology. Research conducted in this field is still in its infancy, all three studies were published in the previous four years, with future research efforts developing more robust investigative methods.
Narrative analysis identified three key themes across the included studies. Children and older adults may have their independence curtailed due to a perception that they lack the capacity to make informed decisions (30,31). This can be particularly difficult for older adults who have led independent lives up to the point where illness or injury limits their choices (32). Children’s independence may be limited due to their age, protective guardians or environmental constraints (e.g. inability to travel). However, both groups require independence to live happy and meaningful lives which promote a sense of agency and autonomy (33,34). Multisensory spaces can provide opportunities for children and older adults to make safe choices about their activities, friendship groups and levels of participation which can be adapted to their varied and changing needs. Such spaces need to be flexible and adaptable to meet these needs and require the involvement of all stakeholders in their creation.
The theme of connecting with others shows the value participants in the included studies placed on being social with a range of individuals. Older adults and children who may be disabled or who are excluded from other settings, e.g., school, can experience social isolation which is detrimental to their health and well-being (34,35). Spaces which can bring people together are increasingly recognised as crucial to a healthy and well-functioning society and fundamental to community empowerment (10,19,36). It was also acknowledged that multisensory spaces were required to serve as places for treatment, counselling or where privacy was required, which emphasises the usefulness of such spaces to social prescribing, a key component in individualised care and support plans. This approach connects individuals to activities and services in their community that meets their practical, social and emotional needs, in an effort to positively affect their health and wellbeing. In such instances connection with health and social care professionals and other users would take place as a subset of activities within the larger multisensory space.
The creation and management of multisensory spaces which are equitable for all would seem to constitute a basic tenant of the design process. However, older buildings which lack lifts/elevators or those which fail to provide ramps for wheelchair users exclude these individuals. Despite globally recognised legislation e.g. United Nations Convention on the Rights of Person’s with Disability (37), United Nations Convention on the Rights of Children (38), Americans with Disabilities Act 1990 (39), the Equality Act 2010 UK (40), Disability Discrimination Act 1992 Australia (41), many buildings and services lack access for people of all ages with physical impairments. Governments and organisations providing services should be held to account for failing to follow legislation which has existed for over thirty years. It is beholden on any organisation which seeks to engage with the public to ensure that they enable everyone irrespective of age or disability. Creating multisensory spaces that are accessible, easy to reserve and which provide clear and understandable guidance on their use would aid in equitable provision.
4.1. Strengths and Limitations of This Review
Prior to creating our list of search terms we ran a number of preparatory searches using recognised terms from the literature. These were then taken to a specialist subject librarian for further refinement. Data extraction and quality appraisal were independently conducted by two reviewers using standardised data extraction and quality appraisal tools. All decisions regarding the application of inclusion and exclusion criteria were discussed and agreed upon before moving on to the next stage of the process. Due to resource constraints it was not possible to include articles published in languages other than English. It is therefore possible that some important papers have been omitted.
4.2. Implications for Practice
Designing inclusive spaces for children and older adults presents significant challenges given their competing demands and interests. Multi-functional spaces are increasing in demand as service budgets are reduced and providers are asked to do more with less. It is important to ensure that children, young people, older adults and their families, staff and stakeholders alike are all involved in the design of spaces to ensure they are useful and sustainable.
Funding should be prioritised to MSS that can address the needs of multiple user groups. Not only will this save on costs it also offers opportunity for intergenerational learning and cooperation which could bring benefit to both the young and old. Whilst it is inevitable that the young and old will not wish to spend all of their time together, MSS which are designed for, and cater to, both groups can allow opportunity to bring these groups together to their mutual benefit.
Partnership working between community organisations, health and social care and academia, which includes service user participation, could ensure MSS are created which are evidence-based and meet the needs of service users and organisations. Input from all stakeholders is required and should be respected if MSS are to adequately address the needs of those people for whom they are designed. It is important to ensure that such spaces are co-designed to ensure that service users’ needs and wants are considered so that designs can maximise their sense of safety, connection and belonging, encourage meaningful and respectful interactions, and promote dignity and autonomy. It is only through their inclusion and the establishment of a sense of ownership that MSS will be used to their full potential.
4.3. Suggestions for Future Research
There is a dearth of research on the creation of MSS for both children and older adults. What research is available has not been rigorously evaluated and lacks in some aspects of methodological quality. The current review found only 3 studies, none of which employed a randomised controlled trial design to test for the effectiveness of MSS on important outcomes. Future research should conduct rigorous examination of the impact of MSS on key stakeholder outcomes.
To create truly inclusive spaces a co-design approach should be undertaken with all those who will use the spaces, e.g., children, young people and their families, older adults, carers and other health and social care professionals. This will help ensure any such space can adequately address the needs of all. Pre design consultations should be undertaken with children, older adults and other stakeholders when organisations seek to create a MSS and should become standard practice if meaningful and sustainable solutions are to be delivered.
5. Conclusions
Multisensory spaces have the potential to improve the wellbeing of children and older adults across a range of health and social care settings. When designed well, they offer flexible use for sensory stimulation, assessment and treatment, relaxation and social connection which can meet the needs of varied users. To ensure uptake, such spaces should be co-designed with the people who they are created for. Flexible multisensory spaces can also be utilised by health and social care practitioners to deliver care and provide services within community settings which are comfortable and familiar to their clients. They also offer the potential to operate as hubs of wellbeing which bring together clients and health and social care practitioners to work collectively to improve care delivery and enhance community empowerment.
Author Contributions
ML and MT were responsible for conceptualisation of the review question and aim. Both authors contributed to the design of the methodology, collecting the data, and performing the analysis. ML was a major contributor in writing the manuscript, ML and MT reviewed and approved the final manuscript.
Funding
This work was supported by Development Trusts NI (DTNI) and funded by the Department of Levelling Up Housing and Communities, Community Ownership Fund. For the purpose of open access, the authors have applied a Creative Commons Attribution (CC BY) licence to any Author Accepted Manuscript version arising from this submission.
Institutional Review Board Statement
Not applicable.
Data Availability Statement
Data is available from the corresponding author upon request.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results”.
References
- Dinu Roman Szabo M, Dumitras A, Mircea DM, Doroftei D, Sestras P, Boscaiu M, et al. Touch, feel, heal. The use of hospital green spaces and landscape as sensory-therapeutic gardens: a case study in a university clinic. Front Psychol. 2023;14(November):1–20. [CrossRef]
- Cuturi LF, Cappagli G, Yiannoutsou N, Price S, Gori M. Informing the design of a multisensory learning environment for elementary mathematics learning. J Multimodal User Interfaces [Internet]. 2022;16(2):155–71. Available from. [CrossRef]
- Wilkinson A, Calder A, Elliott B, Rodger R, Mulligan H, Hale L, et al. Disabled People or Their Support Persons’ Perceptions of a Community Based Multi-Sensory Environment (MSE): A Mixed-Method Study. Int J Environ Res Public Health. 2023;20(19). [CrossRef]
- Putrino D, Ripp J, Herrera JE, Cortes M, Kellner C, Rizk D, et al. Multisensory, Nature-Inspired Recharge Rooms Yield Short-Term Reductions in Perceived Stress Among Frontline Healthcare Workers. Front Psychol. 2020;11(November):1–6. [CrossRef]
- Cameron A, Burns P, Garner A, Lau S, Dixon R, Pascoe C, et al. Making Sense of Multi-Sensory Environments: A Scoping Review. Int J Disabil Dev Educ [Internet]. 2020;67(6):630–56. Available from. [CrossRef]
- Strøm BS, Ytrehus S, Grov EK. Sensory stimulation for persons with dementia: A review of the literature. J Clin Nurs. 2016;25(13–14):1805–34. [CrossRef]
- Unwin KL, Powell G, Jones CRG. A sequential mixed-methods approach to exploring the experiences of practitioners who have worked in multi-sensory environments with autistic children. Res Dev Disabil [Internet]. 2021;118(April):104061. Available from. [CrossRef]
- Unwin KL, Powell G, Jones CRG. The use of Multi-Sensory Environments with autistic children: Exploring the effect of having control of sensory changes. Autism. 2022;26(6):1379–94. [CrossRef]
- Basadonne I, Cristofolini M, Mucchi I, Recla F, Bentenuto A, Zanella N. Working on cognitive functions in a fully digitalized multisensory interactive room: A new approach for intervention in autism spectrum disorders. Brain Sci. 2021;11(11). [CrossRef]
- Novakovic N, Milovancevic MP, Dejanovic SD, Aleksic B. Effects of Snoezelen—Multisensory environment on CARS scale in adolescents and adults with autism spectrum disorder. Res Dev Disabil [Internet]. 2019;89(July 2018):51–8. Available from. [CrossRef]
- Lotan M, Gold C. Meta-analysis of the effectiveness of individual intervention in the controlled multisensory environment (Snoezelen®) for individuals with intellectual disability. J Intellect Dev Disabil. 2009;34(3):207–15. [CrossRef]
- Fakoya OA, McCorry NK, Donnelly M. Loneliness and social isolation interventions for older adults: a scoping review of reviews. BMC Public Health [Internet]. 2020 Dec 14;20(1):129. Available from: https://bmcpublichealth.biomedcentral.com/articles/10.1186/s12889-020-8251-6. [CrossRef]
- Pu L, Pan D, Wang H, He X, Zhang X, Yu Z, et al. A predictive model for the risk of cognitive impairment in community middle-aged and older adults. Asian J Psychiatr [Internet]. 2023;79(December 2022):103380. Available from. [CrossRef]
- Liu CJ, Chang PS, Griffith CF, Hanley SI, Lu Y. The Nexus of Sensory Loss, Cognitive Impairment, and Functional Decline in Older Adults: A Scoping Review. Gerontologist. 2022;62(8):E457–67. [CrossRef]
- Vazini Taher A, Khalil Ahmadi M, Zamir P. Effects of multi-sensory stimulation on cognition function, depression, anxiety and quality of life in elderly persons with dementia. Int J Sport Stud [Internet]. 2015;5(3):355–60. Available from: http:www.ijssjournal.com.
- Helbling M, Grandjean ML, Srinivasan M. Effects of multisensory environment/stimulation therapy on adults with cognitive impairment and/or special needs: A systematic review and meta-analysis. Spec Care Dent. 2024;44(2):381–420. [CrossRef]
- Griffiths S, Dening T, Beer C, Tischler V. Mementos from Boots multisensory boxes – Qualitative evaluation of an intervention for people with dementia: Innovative practice. Dementia. 2019;18(2):793–801. [CrossRef]
- Sánchez A, Marante-Moar MP, Sarabia C, De Labra C, Lorenzo T, Maseda A, et al. Multisensory Stimulation as an Intervention Strategy for Elderly Patients with Severe Dementia: A Pilot Randomized Controlled Trial. Am J Alzheimers Dis Other Demen. 2016;31(4):341–50. [CrossRef]
- Cox H. Multisensory Environments for Leisure Promoting Well-being in Nursing Home Residents With Dementia. J Gerontol Nurs. 2004;37–46.
- Schofield P. A pilot study into the use of a multisensory environment (Snoezelen) within a palliative day-care setting. Int J Palliat Nurs. 2003;9(3):124–30. [CrossRef]
- Veritas Health Innovation. Covidence systematic review software [Internet]. Melbourne; 2023. Available from: www.covidence.org.
- Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. Int J Surg. 2021;88:1–11.
- Hong QN, Pluye P, Fàbregues S, Bartlett G, Boardman F, Cargo M, et al. Mixed Methods Appraisal Tool (MMAT), Version 2018. [Internet]. Canadian Intellectual Property Office, Industry Canada. 2018. Available from: http://mixedmethodsappraisaltoolpublic.pbworks.com/w/file/fetch/127916259/MMAT_2018_criteria-manual_2018-08-01_ENG.pdf%0Ahttp://mixedmethodsappraisaltoolpublic.pbworks.com/.
- Popay J, Roberts H, Sowden A, Petticrew M, Arai L, Rodgers M, et al. Guidance on the Conduct of Narrative Synthesis in Systematic Reviews. A Prod from ESRC Methods Program. 2006;(April 2006):211–9.
- Litwin S, Clarke L, Copeland J, Tyrrell J, Tait C, Mohabir V, et al. Designing a Child-, Family-, and Healthcare Provider–Centered Procedure Room in a Tertiary Care Children’s Hospital. Heal Environ Res Des J. 2023;16(3):195–209. [CrossRef]
- Malysheva E, Skripnikova E, Logina T. Age-related peculiarities of changes in functional state of a person in the recreation areas. BIO Web Conf. 2020;22:01028. [CrossRef]
- Emmerson C, Frayne C, Goodman A. How much would it cost to increase UK health spending to the European Union average? The Institute for Fiscal Studies. 2002.
- Ansah JP, Chiu CT. Projecting the chronic disease burden among the adult population in the United States using a multi-state population model. Front Public Heal. 2023;10. [CrossRef]
- Ogugua, J. Muonde, M. Maduka, C. Olorunsogo, T. Omotayo, O. Demographic shifts and healthcare: A review of aging populations and systemic challenges. Int J Sci Res Arch. 2024;11(1):383–95.
- Hudson K. Practitioners’ views on involving young children in decision making: Challenges for the children’s rights agenda. Aust J Early Child. 2012;37(2):4–9. [CrossRef]
- Bollig G. Ageism and Lack of Shared Decision-Making is a Problem in Healthcare and Geriatrics. Int J Clin Stud Med Case Reports. 2024;35(4):1–4. [CrossRef]
- Langmann E. Vulnerability, ageism, and health: is it helpful to label older adults as a vulnerable group in health care? Med Heal Care Philos. 2023;26(1):133–42.
- Cerino A. The importance of recognising and promoting independence in young children: the role of the environment and the Danish forest school approach. Educ 3-13 [Internet]. 2023;51(4):685–94. Available from. [CrossRef]
- Banerjee D, Rabheru K, de Mendonca Lima CA, Ivbijaro G. Role of Dignity in Mental Healthcare: Impact on Ageism and Human Rights of Older Persons. Am J Geriatr Psychiatry [Internet]. 2021;29(10):1000–8. Available from. [CrossRef]
- Kwan C, Gitimoghaddam M, Collet JP. Effects of social isolation and loneliness in children with neurodevelopmental disabilities: A scoping review. Brain Sci. 2020;10(11):1–36. [CrossRef]
- Park G, Nanda U, Adams L, Essary J, Hoelting M. Creating and Testing a Sensory Well-Being Hub for Adolescents with Developmental Disabilities. J Inter Des. 2020;45(1):13–32. [CrossRef]
- United Nations. Convention on the rights of persons with disabilities. Treaty Ser [Internet]. 2006;2515:3. Available from: http://www.un.org/disabilities/.
- United Nations. The United Nations convention on the rights of the chid. Vol. 1577. 1989.
- Americans with Disabilities Act. of 1990, 42 U.S.C. 12101 (1990). https://www.ada.gov/pubs/adastatute08.htm.
- Equality Act [Internet]. UK; 2010. Available from: https://www.legislation.gov.uk/ukpga/2010/15/contents.
- Disability Discrimination Act [Internet]. Australia; 1992. Available from: https://www.legislation.gov.au/C2004A04426/latest/text.
Figure 1.
Prisma flowchart of article selection.
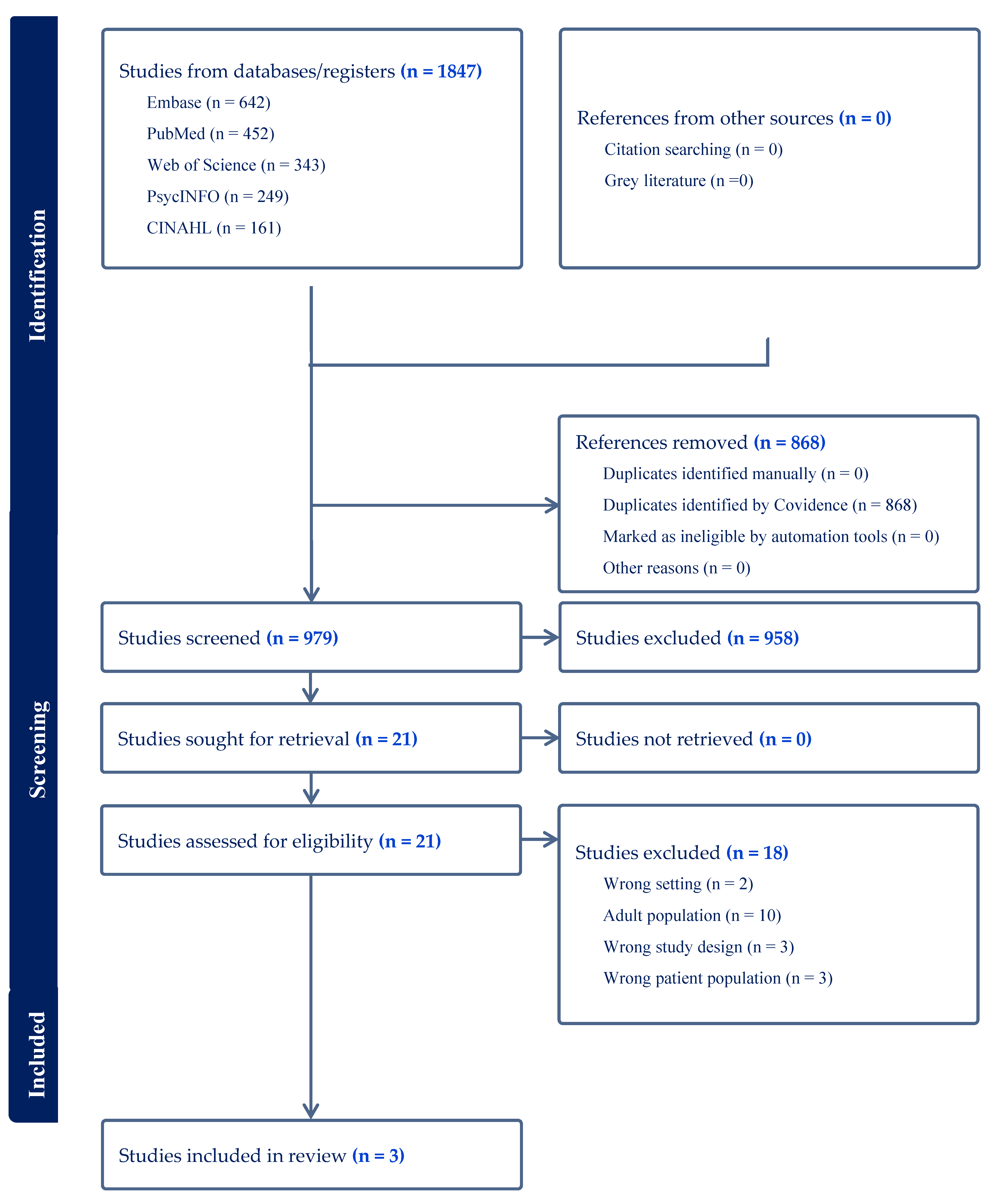

Table 1.
Search terms employed in this review.
| Intergenerational | Sensory spaces |
|---|---|
| Intergen* OR Child* OR Adolescen* OR “Young adult*” OR Adult* OR “older adult*” OR elderly |
“sensory room*” OR “sensory space*” OR “sensory environment*” OR “multi-sensory environment*” OR “quiet room*” |
Table 2.
Characteristics of included studies.
| Author and Country of Origin | Aim(s) | Design | Participants |
Measures employed or interview questions | Findings |
|---|---|---|---|---|---|
| Litwin et al (2023) Canada |
To co-design new paediatric procedure room prototypes with children, caregivers, and healthcare providers |
Qualitative design employing observation, semi-structured interviews and co-design workshops. | n=11 children and youth; n=38 physicians; n=8 youth and parent advisors | Not provided | 1 Control: Helathcare professionals and patients need to be able to control features in the environment; 2 Privacy: Spaces must be designed with features to help patients feel safe, secure, and respected during procedures; 3 Evidence-based pain-reduction and distraction methods: Positive distraction tools available for all patients. Distractions must be age appropriate and flexible to suit individual needs; 4 Sensory environment: Patients and healthcare providers should be able to modify sensory stimuli in the room; 5 Human factors organization of the space and equipment: Rooms must enable the seamless flow of people and storage of equipment; 6 Equitable spatial design: Create a space that is inclusive for all patients and families; 7 The journey: experience of a medical procedure begins prior to arriving at the hospital. |
| Malysheva et al (2020) Russia |
To study the physiological effects of staying in park areas in people of different ages. | Pre-post-test experimental design | n=20 children aged 14-15 years; n=20 students aged 18-20 years; n=11 older people aged 69-76 years |
Respiratory rate (RR), respiratory minute volume (RMV), maximal pulmonary ventilation (MPV) were recorded with a spirograph. Anfimov’s table technique used to assess attention. Auditory memory test (word recall task). Blood pressure, heart rate and hemodynamics. | Students made fewer mistakes, the number of selected symbols, the capacity of visual memory, the speed of information processing increase, but their attention span decreased. After a walk in the park, their levels of state anxiety decreased. In older people mental capacity slightly improved, which showed itself in an increase in intellectual efficiency, accuracy in completing tasks, as well as an improved visual and auditory memory, though attention span decreased. There was a positive effect on hemodynamic parameters in elderly people. |
| Wilkinson et al (2023) New Zealand |
To explore disabled users’ experiences of the MSE that they operate and support with a view to expanding access to MSE-type environments within the metropolitan area. Given the paucity of evidence internationally and nationally of the benefits of community-based MSEs, it was deemed relevant to understand who uses the MSE and their perceptions of it. | Mixed methods employing an electronic survey and semi-structured interviews. | n=104 survey responses, n=74 parents, n=15 MSE room users, n=12 support persons. Age < 4 n=45, 5-21 n=32, >21 n=19. n=14 Interviews, disabled adult MSE users n=3 males, n=5 females aged 20-70 years; child MSE users n=5 males, n=3 females aged 1-11 years old. |
Survey collected data on: (i) indication of whether the respondent was the MSE room user (participant) or completing the e-survey on behalf of a room user (support person); (ii) participant demographics (age, gender, ethnicity, region where they resided, who (if anyone) accompanied the room user to the MSE, mode of transport, and frequency and length of SCMSE room use); (iii) barriers to access; and iv) reported participant disability via the Washington Group Short Set on Functioning (WG-SS) Demographics: age, gender, ethnicity. Interview guide: Can you share your thoughts along with some examples of your experiences of using the multisensory room? Prompts: Reasons for using the room, benefits, or barriers, if you could change anything in the room what might it be and why? Could you share your thoughts about your equipment preferences? Prompts: What equipment do you enjoy using and why? Is there other equipment that you would like added or removed from the multisensory room? Please explain. Talk me though what is involved for you (and your support persons) in getting ready and then getting to the multisensory room. Prompts: Transport, the path of travel from the building entrance to the multisensory room Talk me through what is involved for you (and your support persons) in the return journey, from the multisensory room to home. Can you share your experiences and some examples about the accessibility of information about the multisensory room. Prompts: Can you tell us about how you found out about the multisensory room (i.e., who referred you and why?). What information was available (e.g., online, brochures)? Did the information available meet your needs (i.e., was there enough information or too much)? Where and how did you go about finding further information if you needed to? Is there anything that could be done differently to enhance the information about the multisensory room? Who accompanies them to the room. Understanding the impairments, they experience/sensory systems affected |
Survey findings: Overall, 131 participants responded to the e-survey, representing a response rate of 8.8%. Most of the child room users were male; conversely, most of the adult users were female. The types of limitations, as per the WSS-GS, of the room users included: Seeing (n = 2), Hearing (n = 1), Walking (n = 6), Concentration (n = 10), Self-care (n = 14), and Communication (n = 9). Frequency of room use was every two weeks n=8, Monthly n=20, 2-4 times a year n=25, one a year or less n=51. Barriers to MSE access included booking system n=11, distance to MSE n=4, time constraints n=6, location of front desk n=3, MSE too overwhelming n=2, staff shortages n=5, upstairs location n=8, other n=4. Qualitative themes: 1 Self-determination - Choice and control, individualisation, independence, and safety ; 2 Enhancing wellbeing opportunities - MSE created opportunities for social connection with others, influenced the room user’s behaviour and mood, and provided respite and a space to extend therapy; 3 Engagement in the MSE - Environmental factors, such as the room design, the role of the MSE staff, and implicit room rules, either facilitated or created challenges; 4 Accessibility - participants predominantly described external environmental barriers (such as the MSE being upstairs), rather than internal barriers (i.e., lack of time) to access. |
Table 3.
Quality Assessment using the MMAT.
| First Author & Year | Q1 | Q2 | Q3 | Q4 | Q5 | Q6 | Q7 | Explanation |
|---|---|---|---|---|---|---|---|---|
| Litwin et al (2023) | Y | Y | Y | Y | Y | N | Y | Insufficient illustrative quotations. |
| Malysheva et al (2020) | Y | Y | Y | N | Y | CT | CT | School children recruited only represented those aged 14-15 years. No detail provided on recruitment or statistical analysis. |
| Wilkinson et al (2023) | Y | Y | N | N | N | N | Y | No rationale given for using a mixed methods design, lack of synthesis of qualitative and quantitative methods, no explanation of divergence between quantitative and qualitative findings. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



