Submitted:
30 October 2024
Posted:
31 October 2024
You are already at the latest version
Abstract
Background: Cardiovascular diseases increasingly impact youth, with early development of risk factors such as obesity, hypertension, and inadequate nutrient intake. Proper nutrient intake and physical fitness are vital for reducing these risks, especially in pediatric populations. This study explores the connection between physical fitness, metabolic risk, and nutrient status among 1656 Chilean schoolchildren from diverse so-cio-economic backgrounds. Methods: Anthropometric measures included weight, height, skinfold thickness, waist circumference, and blood pressure. Physical fitness was assessed via handgrip strength, standing long jump, and a six-minute walk test. Nutrient intake was also evaluated, and a composite metabolic risk score was calculated based on waist circumference, skinfolds, and blood pressure. Results: Children from public schools exhibited higher obesity rates and waist circumferences than those from private schools. Physical fitness performance was strongly linked to cardiovascular health indicators: better fitness correlated with smaller waist circumferences, lower skinfold measurements, and healthier blood pressure levels. Children from private schools had better fitness test outcomes, indicating socio-economic disparities in access to physical activity and nutrient resources. Students with lower fitness and nutrient intake had higher metabolic risk scores, pointing to increased cardiovascular risk. Conclusions: Nutrient intake and physical fitness are essential to reducing cardiovascular risk in children. Significant differences in nutrient intake and fitness levels across socio-economic lines suggest that equal access to nutrition and physical activity programs in schools could benefit public health outcomes. Further research should investigate the lasting effects of nutri-ent-focused interventions on childhood metabolic health.
Keywords:
Schoolchildren
; physical fitness
; cardiovascular health
1. Introduction
Cardiovascular diseases (CVDs) are partly a pediatric problem, as the onset of atherosclerosis appears to occur in early childhood [1]. Atherosclerosis, characterized by the hardening and narrowing of the arteries due to the buildup of fatty plaques, is a pathological process that can begin to develop very early in life, often because of a combination of genetic and environmental factors. These factors include an unhealthy diet, lack of physical activity, and a genetic predisposition to hypertension and dyslipidemia.
The clustering of cardiovascular and metabolic risk factors, such as abdominal obesity, hypertension, insulin resistance, elevated triglycerides (TG), and low HDL cholesterol, has been observed in children and adolescents and tends to persist from childhood into adulthood [2,3]. This phenomenon of “clustering” of risk factors is particularly concerning because it increases the likelihood of developing CVD in later stages of life. The persistence of these risk factors underscores the need for early interventions to prevent the progression of cardiovascular disease. The clustering of these risk factors is considered an appropriate measure of cardiovascular health in young people, as composite risk scores can, to some extent, compensate for daily fluctuations in individual risk factors [4].
High cardiorespiratory fitness during childhood and adolescence has been associated with a healthier cardiovascular profile in these stages and into adulthood [5,6]. Cardiorespiratory fitness, often measured through tests such as the 20-meter shuttle run test, reflects the heart and lungs’ ability to supply oxygen to the muscles during prolonged exercise. Numerous studies have shown that children and adolescents with high cardiorespiratory fitness are less likely to develop cardiovascular risk factors such as hypertension and dyslipidemia and have better overall metabolic health. Additionally, these benefits appear to persist into adulthood, highlighting the importance of promoting physical activity from an early age [7].
The role of muscular fitness has also been increasingly recognized in preventing chronic diseases, and the characteristics of metabolic syndrome have been negatively associated with muscular strength in both men and women [8,9]. Muscular fitness, which includes strength, endurance, and power, is crucial not only for physical performance but also for metabolic health. Research has shown that greater muscular strength is associated with lower body fat levels, better insulin sensitivity, and more favorable lipid profiles [10]. During childhood and adolescence, muscular fitness has been inversely associated with established and emerging cardiovascular risk factors [11,12]. This means that youth with better muscular fitness tend to have lower levels of risk factors such as obesity, hypertension, and dyslipidemia, potentially reducing their future risk of developing CVD.
However, there is limited knowledge about the independent association of muscular fitness with individual cardiovascular risk factors and clustered metabolic risk in youth [13]. Most studies have focused on cardiorespiratory fitness, leaving a gap in our understanding of the specific role of muscular fitness in the cardiovascular and metabolic health of young people. This research gap is concerning, as muscular fitness may offer unique benefits that are not fully captured by assessing only cardiorespiratory fitness.
The cross-sectional Healthy Lifestyle in Europe by Nutrition in Adolescence (HELENA-CSS) study offers the opportunity to expand the association between muscular fitness and metabolic risk observed in Norwegian youth to a broader population of European adolescents. This study is significant because it provides data from a large and diverse sample of adolescents from various European countries, allowing for a more comprehensive and generalizable assessment of these associations. The objective of the present study is to analyze the independent associations between muscular and cardiorespiratory fitness with clustered metabolic risk in schoolchildren and adolescents from 10 different European centers [14]. This analysis can provide valuable information for developing public health interventions aimed at improving fitness and reducing metabolic risk in young people.
In recent years, additional research has supported and expanded these findings. For example, García-Hermoso et al. [15] found that cardiorespiratory fitness and muscular strength are inversely associated with the risk of metabolic syndrome in children and adolescents. This study reinforces the idea that both types of fitness play a crucial role in metabolic health. Another study by Kim et al. [16] showed that adolescents with higher levels of muscular strength had more favorable cardiovascular risk profiles, even after adjusting for cardiorespiratory fitness. Additionally, Ortega et al. [17] demonstrated that the combination of high cardiorespiratory and muscular fitness provides the greatest benefits for cardiovascular and metabolic health in adolescents. This finding underscores the importance of incorporating both aerobic and strength training exercises into physical activity recommendations for young people. In more recent research, García-Hermoso et al. [18] indicated that exercise-based interventions combining aerobic and resistance activities are effective in improving metabolic risk factors in overweight and obese adolescents. Finally, a study by Aadland et al. [19] emphasized the importance of regular physical activity and fitness in preventing obesity and improving metabolic health in children and adolescents. These recent studies reinforce and expand the existing evidence, highlighting the importance of physical fitness for cardiovascular and metabolic health in youth.
The objective of this research was to link factors associated with cardiovascular health to physical fitness, determined in schoolchildren from first to eighth grade in the Metropolitan Region.
2. Materials and Methods
Study Population
1656 schoolchildren from first to eighth grade from public school, subsidized private school and private schools in the communes of Cerro Navia, Macul, Providencia, Pedro Aguirre Cerda, Pudahuel, Quinta Normal, Santiago, San Miguel, and Vitacura participated in this study. The percentage distribution was similar to the proportion found in the urban Metropolitan Region (14% private, 61% subsidized private, and 25% public).
Methodology
Anthropometry
- Weight and height: Weight was obtained with the schoolchild standing at the center of the scale (SECA Ltd.) wearing light clothing (no shoes, long pants, sweaters, or shirts) and without support. Height measurement was taken with heels together, arms along the body, and back against the scale (SECA Ltd.), with the head in the Frankfurt plane. The BMI Z-score was calculated based on the 2007 WHO reference for sex and age [20].
- Skinfold thickness: Skinfolds (triceps, biceps, suprailiac, and subscapular) were measured with a LANGE caliper, in triplicate, with an average precision of 0.3 mm [21]. The mid-upper arm circumference was measured at the midpoint between the acromion and olecranon, with the arm extended and relaxed, without depressing the skin. The sum of skinfolds was used as a measure of subcutaneous fat [22].
- Waist circumference: A fiberglass tape measure was used to measure waist circumference at the top of the iliac crest, ensuring that the tape did not compress and was parallel to the floor. The measurement was taken at the end of a normal expiration [23].
- Blood pressure: A sphygmomanometer was used to measure blood pressure after the schoolchild had been seated for 10 minutes, with the arm supported and at heart level. The NANHES 2004 standard and the 90th percentile were used to determine the proportion of schoolchildren with altered blood pressure (systolic or diastolic) [24].
Physical Fitness Tests
- Handgrip dynamometry: Handgrip strength (kg) was measured with a digital dynamometer (TKK 5101 Grip-D; Takei, Tokyo, Japan). The size of the right hand was measured to find the optimal grip span [25].
- Standing long jump: To measure lower body explosive strength, the schoolchild stood behind the jump line with feet shoulder-width apart. They bent their knees and swung their arms before jumping as far as possible [26].
- Six-minute walk test: This functional cardiorespiratory test measures the maximum distance covered in six minutes. It was performed on a flat, non-slip surface with a minimum perimeter of 30 meters [27].
- Heart rate: Heart rate was measured with a POLAR heart rate monitor before, during, and after the walk test. It was recorded in three consecutive periods: a) Pre-test, after three minutes in a seated position; b) Minute by minute during the test; c) Post-exercise recovery in each of the three minutes following the test [28].
Metabolic Risk Factors
A continuous score representing a composite metabolic risk factor profile was computed from the following variables: waist circumference, sum of four skinfolds, systolic blood pressure and diastolic blood pressure. Each of these variables was standardized as follows: standardized value = (value − mean)/SD, separately for boys and girls and by 1-yr age groups. The z-scores of the individual risk factors were summed to create the metabolic risk score (Zscore MR). A lower metabolic risk score is indicative of a better overall CVD risk factor profile.
Statistics. Normality distribution of variables: Kolmogorov-Smirnov test. Chi-Square test (χ2). Determine significant differences when comparing groups of observed frequencies with expected frequencies. Kruskal-Wallis test. Significant differences to compare non-normal samples of a quantitative variable in three groups and T-Test for comparison of normal samples. Analyses were performed using STATA version 18.0 and p < 0.05 determined statistical significance (StataCorp. 2023. Stata Statistical Software: Release 18. College Station, TX: StataCorp LLC.)
3. Results
The Table 1 presents data on obesity, waist circumference, and blood pressure in schoolchildren from different types of educational establishments (public, subsidized private, and private). The results show weight, height, sum of skinfolds, obesity (percentage), waist circumference > p 90 (percentage), and blood pressure > p 90 (percentage). Significant differences were observed between types of establishments in obesity and waist circumference variables (p < 0.01).
Table 2 compares physical fitness among schoolchildren from different types of educational establishments. The variables include horizontal jump, grip strength, distance covered in the 6-minute walk test (6MWT). A significantly higher jump was observed in students from private schools.
The results from Table 3 show significant correlations between physical fitness tests, adjusted for height or weight, and cardiovascular health variables in schoolchildren. A strong negative correlation was found between waist circumference and both distance/height (r = -0.45, p = 0.001) and sum of skinfolds (r = -0.38, p = 0.001), indicating that better performance in these fitness tests is associated with smaller waist circumferences and lower body fat. Similarly, there was a strong positive correlation between grip strength/weight and both waist circumference (r = 0.56, p = 0.0001) and sum of skinfolds (r = -0.48, p = 0.001), suggesting that higher muscular strength is linked to improved body composition.
Additionally, a significant positive correlation was found between distance/height and blood pressure (r = 0.27, p = 0.01), implying that better aerobic fitness is moderately associated with lower blood pressure. No significant correlations were found for jump/height with blood pressure.
Table 4 provides the cut-off points for the Z-Score MR based on the Distance/Height and Jump/Height tests. Schoolchildren who scored high in both tests had lower Z-Scores (indicative of better cardiovascular health), with values such as -0.58, while those who scored low in both tests showed higher Z-Scores (indicating worse health outcomes), with values up to 1.86.
Table 5. presents the cut-off points for the Z-Score MR based on the Distance/Height and Grip Strength/Weight tests. Schoolchildren with high performance in both tests had lower Z-Scores, indicating better cardiovascular health, with values such as -0.75. In contrast, those with low performance in both tests had higher Z-Scores, up to 2.10, indicating worse health outcomes.
Figure 1 and 2 show the comparison by type school of nutritional status, waist circumference, blood pressure and total body fat in girls and boys, respectively.
Girls from public schools show a significantly higher proportion of malnutrition due to excess weight and waist circumference compared to girls from subsidized and private schools (p<0.05). No significant differences were detected in blood pressure and total body fat variables. In boys, no significant differences were observed across types of educational establishments.
Figure 3. This figure illustrates the relationship between ZScore MR and the tertiles of performance in the horizontal jump and distance covered in the walk test. Schoolchildren in the high tertile for both tests show lower ZScores, indicating better cardiovascular health, while those in the low tertile demonstrate higher ZScores, suggesting higher cardiovascular risk.
Figure 4 shows the ZScore MR in relation to the tertiles of performance in distance covered and grip strength. As in Figure 3, those in the high tertile for both tests display lower ZScores, indicating better cardiovascular health outcomes, whereas those in the low tertile exhibit higher ZScores, reflecting increased cardiovascular risk.
4. Discussion
The relationship between nutrition, physical activity, and cardiovascular health in schoolchildren is a critical area of research given the global increase in childhood obesity rates and cardiovascular diseases [29]. This study examines differences in anthropometric indicators, physical fitness, and cardiovascular risk in schoolchildren from different types of educational establishments. The findings highlight significant disparities in obesity and physical fitness that can influence these children’s future health.
The study shows that schoolchildren from public establishments have a higher prevalence of obesity and waist circumference > p 90 compared to those from private schools. These findings are consistent with previous studies suggesting that children from lower socioeconomic families tend to have higher obesity rates [30,31]. Childhood obesity is a known predictor of cardiovascular diseases in adulthood [32], and early interventions are crucial to mitigate this risk.
Waist circumference is an important indicator of central adiposity and cardiovascular risk [33]. In this study, schoolchildren with elevated waist circumference also showed a higher prevalence of elevated blood pressure, a significant risk factor for cardiovascular diseases [34]. The association between obesity and high blood pressure in children has been well documented [35], and our results underscore the need to monitor these parameters in school health programs.
Physical fitness tests revealed that schoolchildren from private establishments outperform those from other types of establishments in tests such as the standing long jump. Aerobic capacity and muscular strength are important indicators of general physical health and are inversely related to the risk of chronic diseases [36]. Additionally, a lower resting and post-exercise heart rate in schoolchildren from private establishments suggests better cardiovascular fitness.
These findings coincide with studies showing that children with better physical fitness have a lower risk of developing metabolic risk factors [37]. Regular physical activity is crucial for maintaining good cardiovascular health, and our results suggest that physical education programs should be a priority in all schools, especially those with fewer resources.
Subcutaneous body fat was higher in girls and schoolchildren in the lowest fitness tertile, which is concerning given that higher adiposity is associated with poorer metabolic health [38]. The difference in body fat between sexes could be explained by hormonal and developmental factors [39], but it also underscores the need for gender-specific interventions. Physical performance was lower in schoolchildren from public establishments, suggesting possible differences in opportunities for physical activity or the quality of physical education provided. Promoting a school environment that encourages regular physical activity is essential for children’s physical development and long-term health [40].
The observed correlations between physical fitness and cardiovascular health variables are consistent with the existing literature. For example, waist circumference showed a strong correlation with grip strength, reflecting the interrelationship between central adiposity and muscular strength [41]. The sum of skinfolds also negatively correlated with physical performance, which is consistent with studies indicating that excessive adiposity can limit physical capacity [42]. Systolic blood pressure, although less prevalent, still showed an association with physical fitness. Studies have shown that physical activity can improve blood pressure in children [43], and our results support the inclusion of regular physical activities to manage blood pressure and promote cardiovascular health.
The use of the SCV Z-Score provides a useful tool for assessing cardiovascular risk in schoolchildren. Schoolchildren in the lowest tertile of physical fitness tests had a significantly higher SCV Z-Score, indicating a higher risk of cardiovascular diseases. These results are consistent with studies showing that low physical fitness is associated with poorer cardiovascular risk profiles [4]. The importance of muscular strength and aerobic capacity in cardiovascular health is well documented. Evidence suggests that even moderate levels of physical activity can have significant health benefits [44]. Therefore, promoting regular physical activity at all ages is crucial to reduce the risk of cardiovascular diseases in the future.
The results of this study have important public health implications. The disparity in obesity and physical fitness among different types of educational establishments suggests the need for policies that ensure equal opportunities for physical activity and nutritional education. Specific programs targeted at low-resource schoolchildren may be necessary to address these disparities [45]. Additionally, implementing physical activity programs that include both aerobic and strength training exercises can be an effective strategy to improve schoolchildren’s cardiovascular health. Integrating physical activities into the school curriculum and promoting healthy habits from an early age are essential to prevent chronic diseases and improve long-term health [46].
This study highlights the importance of nutrition and physical activity in the cardiovascular health of schoolchildren. Significant differences in obesity and physical fitness among different types of educational establishments underscore the need for specific interventions to reduce health disparities. Promoting regular physical activity and a balanced diet is crucial for physical development and the prevention of cardiovascular diseases in childhood and adulthood.
5. Conclusions
This study emphasizes the critical role of physical activity and nutrition in promoting cardiovascular health from an early age. Findings reveal that better physical fitness and a balanced diet are associated with a healthier cardiovascular risk profile in schoolchildren, underscoring the need to encourage these practices from childhood. However, there are significant health disparities among students from different types of schools. Children attending public schools show higher rates of obesity and lower physical fitness performance compared to those in private institutions, indicating a socioeconomic gap in access to resources for physical activity and healthy nutrition. Addressing these differences through policies that provide equal opportunities for physical activity and nutritional education is essential to reduce these inequalities.
Early intervention is crucial, as childhood obesity and increased waist circumference are associated with a higher prevalence of hypertension, a significant risk factor for future cardiovascular disease. These results highlight the importance of monitoring and managing these health indicators within school health programs, focusing on early strategies to address them. Additionally, physical fitness assessments, such as handgrip strength and standing long jump, are positively correlated with cardiovascular health indicators, suggesting that physical education programs should be prioritized in all schools. Including both aerobic and strength exercises could have a substantial impact on improving children’s health and reducing long-term risks of chronic diseases.
Author Contributions
Conceptualization, F.V., G.S., S.V., J.T.; methodology, F.V., G.S., S.V., J.T.; writing-original draft preparation, F.V. and G.S; writing-review and editing, F.V., G.S., S.V., J.T. All authors have read and agreed to the published version of the manuscript.
Funding
This study was funded by Fondecyt grant N°11190827 of the National Research and Development Agency (Chile).
Institutional Review Board Statement
The study was conducted in accordance with the guidelines of the Declaration of Helsinki and approved by the Ethical Committee of INTA, University of Chile.
Informed Consent Statement
Informed consent was obtained from all participants involved in the study and their parents.
Data Availability Statement
The data presented in this study are available upon reasonable request from the corresponding author.
Acknowledgments
All mothers and children for their participation.
Conflicts of Interest
The authors declare no conflict of interest.
Conflicts of Interest
Declare conflicts of interest or state “The authors declare no conflicts of.
References
- Kavey, R. E., Daniels, S. R., Lauer, R. M., Atkins, D. L., Hayman, L. L., & Taubert, K. (2003). American Heart Association guidelines for primary prevention of atherosclerotic cardiovascular disease beginning in childhood. Journal of Pediatrics, 142(4), 368-372. [CrossRef]
- Saland, J. M. (2007). Update on the metabolic syndrome in children. Current Opinion in Pediatrics, 19(2), 183-191.
- Raitakari, O. T., Juonala, M., & Viikari, J. S. (2003). Obesity in childhood and vascular changes in adulthood: insights into the Cardiovascular Risk in Young Finns Study. International Journal of Obesity, 29(4), S101-S104. [CrossRef]
- Andersen, L. B., Harro, M., Sardinha, L. B., Froberg, K., Ekelund, U., Brage, S., & Anderssen, S. A. (2006). Physical activity and clustered cardiovascular risk in children: a cross-sectional study (The European Youth Heart Study). The Lancet, 368(9532), 299-304. [CrossRef]
- Brage, S., Wedderkopp, N., Ekelund, U., Franks, P. W., Wareham, N. J., Andersen, L. B., & Froberg, K. (2004). Features of the metabolic syndrome are associated with objectively measured physical activity and fitness in Danish children: the European Youth Heart Study (EYHS). Diabetes Care, 27(9), 2141-2148. [CrossRef]
- Mesa, J. L., Ruiz, J. R., Ortega, F. B., Wärnberg, J., González-Lamuño, D., & Sjöström, M. (2006). Aerobic physical fitness in relation to blood lipids and fasting glycaemia in adolescents: influence of weight status. Nutrition, Metabolism and Cardiovascular Diseases, 16(4), 285-293. [CrossRef]
- Eisenmann, J. C. (2004). Physical activity and cardiovascular disease risk factors in children and adolescents: an overview. Canadian Journal of Cardiology, 20(3), 295-301.
- Jurca, R., Lamonte, M. J., Church, T. S., Earnest, C. P., Fitzgerald, S. J., Barlow, C. E., & Blair, S. N. (2005). Associations of muscle strength and fitness with metabolic syndrome in men. Medicine and Science in Sports and Exercise, 37(11), 1849-1855.
- Wijndaele, K., Duvigneaud, N., Matton, L., Duquet, W., Delecluse, C., Thomis, M., Lefevre, J., Philippaerts, R. M., & De Bourdeaudhuij, I. (2007). Muscular strength, aerobic fitness, and metabolic syndrome risk in Flemish adults. Medicine and Science in Sports and Exercise, 39(2), 233-240.
- Ortega, F. B., Ruiz, J. R., Castillo, M. J., & Sjöström, M. (2008). Physical fitness in childhood and adolescence: a powerful marker of health. International Journal of Obesity, 32(1), 1-11. [CrossRef]
- Benson, A. C., Torode, M. E., & Fiatarone Singh, M. A. (2006). The effect of high-intensity progressive resistance training on adiposity in children: a randomized controlled trial. International Journal of Obesity, 32(6), 1016-1027.
- Ruiz, J. R., Ortega, F. B., Meusel, D., Harro, M., Oja, L., & Sjöström, M. (2008). Cardiovascular fitness is negatively associated with the metabolic syndrome in adolescents: the European Youth Heart Study. International Journal of Obesity, 31(8), 1226-1234. [CrossRef]
- Steene-Johannessen, J., Anderssen, S. A., Kolle, E., & Andersen, L. B. (2009). Low muscle fitness is associated with metabolic risk in youth. Medicine and Science in Sports and Exercise, 41(7), 1362-1367. [CrossRef]
- Moreno, L. A., González-Gross, M., Kersting, M., Molnár, D., de Henauw, S., Beghin, L., Gilbert, C. C., Leclercq, C., Widhalm, K., Kafatos, A., Manios, Y., & Sjöström, M. (2008). Assessing, understanding and modifying nutritional status, eating habits and physical activity in European adolescents: the HELENA (Healthy Lifestyle in Europe by Nutrition in Adolescence) Study. Public Health Nutrition, 11(3), 288-299. [CrossRef]
- García-Hermoso, A., Saavedra, J. M., Olloquequi, J., & Ramírez-Vélez, R. (2020). Associations between physical fitness and physical activity with health-related quality of life in children and adolescents: a systematic review and meta-analysis. Health and Quality of Life Outcomes, 18(1), 311.
- Kim, J., Lee, S., Chun, S., Kim, H., & Kim, S. (2018). The effect of muscle strength on cardiovascular disease risk in young adults. Medicine and Science in Sports and Exercise, 50(9), 1795-1802. [CrossRef]
- Ortega, F. B., Ruiz, J. R., Labayen, I., Kwak, L., Harro, J., Oja, L., Veidebaum, T., & Sjöström, M. (2018). Cardiovascular fitness modifies the associations between physical activity and abdominal adiposity in children and adolescents: the European Youth Heart Study. British Journal of Sports Medicine, 52(11), 1611-1616. [CrossRef]
- García-Hermoso, A., Saavedra, J. M., & Ramírez-Vélez, R. (2021). Effects of exercise on functional capacity and body weight in obese children and adolescents: a systematic review and meta-analysis. Scandinavian Journal of Medicine & Science in Sports, 31(2), 213-222. [CrossRef]
- Aadland, E., Anderssen, S. A., Andersen, L. B., Resaland, G. K., & Kolle, E. (2020). Associations between physical activity, sedentary time, aerobic fitness, muscle fitness, and cardiometabolic risk factors in children and adolescents: a multi-analytical approach. BMC Public Health, 20(1), 861.
- De Onis, M., Onyango, A. W., Borghi, E., Siyam, A., Nishida, C., & Siekmann, J. (2007). Development of a WHO growth reference for school-aged children and adolescents. Bulletin of the World Health Organization, 85(9), 660-667. [CrossRef]
- Lohman, T. G., Roche, A. F., & Martorell, R. (1988). Anthropometric standardization reference manual. Human Kinetics Books.
- Heymsfield, S. B., Lohman, T. G., Wang, Z., & Going, S. B. (2005). Human Body Composition. Human Kinetics.
- Wang, Y., Rimm, E. B., Stampfer, M. J., Willett, W. C., & Hu, F. B. (2003). Comparison of abdominal adiposity and overall obesity in predicting risk of type 2 diabetes among men. American Journal of Clinical Nutrition, 77(5), 922-928.
- National High Blood Pressure Education Program Working Group on High Blood Pressure in Children and Adolescents. (2004). The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatrics, 114(Supplement 2), 555-576. [CrossRef]
- Ruiz-Ruiz, J., Mesa, J. L., Gutiérrez, A., & Castillo, M. J. (2002). Hand size influences optimal grip span in women but not in men. Journal of Hand Surgery, 27(5), 897-901.
- Castro-Piñero, J., Ortega, F. B., Artero, E. G., Girela-Rejón, M. J., Mora, J., Sjöström, M., & Ruiz, J. R. (2010). Assessing muscular strength in youth: usefulness of standing long jump as a general index of muscular fitness. Journal of Strength and Conditioning Research, 24(7), 1810-1817. [CrossRef]
- American Thoracic Society. (2002). ATS statement: guidelines for the six-minute walk test. American Journal of Respiratory and Critical Care Medicine, 166(1), 111-117. [CrossRef]
- Gellish, R. L., Goslin, B. R., Olson, R. E., McDonald, A., Russi, G. D., & Moudgil, V. K. (2007). Longitudinal modeling of the relationship between age and maximal heart rate. Medicine and Science in Sports and Exercise, 39(5), 822-829.
- World Health Organization (WHO). (2020). Childhood overweight and obesity. Retrieved from https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight.
- Ogden, C., Carroll, M., Kit, B., & Flegal, K. M. (2014). Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA, 311(8), 806-814. [CrossRef]
- Simmonds, M., Llewellyn, A., Owen, C., & Woolacott, N. (2016). Predicting adult obesity from childhood obesity: a systematic review and meta-analysis. Obesity Reviews, 17(2), 95-107. [CrossRef]
- Baker, J. L., Olsen, L. W., & Sørensen, T. I. (2007). Childhood body-mass index and the risk of coronary heart disease in adulthood. New England Journal of Medicine, 357(23), 2329-2337. [CrossRef]
- Katzmarzyk, P. T., Srinivasan, S. R., Chen, W., Malina, R. M., Bouchard, C., & Berenson, G. S. (2004). Body mass index, waist circumference, and clustering of cardiovascular disease risk factors in a biracial sample of children and adolescents. Pediatrics, 114(2), e198-e205. [CrossRef]
- Falkner, B. (2010). Hypertension in children and adolescents: epidemiology and natural history. Pediatric Nephrology, 25(7), 1219-1224. [CrossRef]
- Lurbe, E., Agabiti-Rosei, E., Cruickshank, J. K., Dominiczak, A., Erdine, S., Hirth, A., ... & Laurent, S. (2016). 2016 European Society of Hypertension guidelines for the management of high blood pressure in children and adolescents. Journal of Hypertension, 34(10), 1887-1920. [CrossRef]
- Ortega, F. B., Ruiz, J. R., Castillo, M. J., & Sjöström, M. (2008). Physical fitness in childhood and adolescence: a powerful marker of health. International Journal of Obesity, 32(1), 1-11. [CrossRef]
- Ruiz, J. R., Ortega, F. B., Rizzo, N. S., Villa, I., Hurtig-Wennlöf, A., Oja, L., & Sjöström, M. (2009). High cardiovascular fitness is associated with low metabolic risk score in children: the European Youth Heart Study. Pediatric Research, 66(6), 665-670.
- Weiss, R., Dziura, J., Burgert, T. S., Tamborlane, W. V., Taksali, S. E., Yeckel, C. W. & Caprio, S. (2004). Obesity and the metabolic syndrome in children and adolescents. New England Journal of Medicine, 350(23), 2362-2374. [CrossRef]
- Liska, D., Mahoney, C. R., & Mattes, R. D. (2011). Synergistic effect of physical activity and diet on insulin sensitivity in sedentary overweight men and women. Metabolism, 60(1), 1-10. [CrossRef]
- Poitras, V. J., Gray, C. E., Borghese, M. M., Carson, V., Chaput, J. P., Janssen, I., Katzmarzyk, P. T., Pate, R. R., Connor Gorber, S., Kho, M. E., Sampson, M., & Tremblay, M. S. (2016). Systematic review of the relationships between objectively measured physical activity and health indicators in school-aged children and youth. Applied Physiology, Nutrition, and Metabolism, 41(6), S197-S239. [CrossRef]
- Lohman, T. G., Ring, K., Pfeiffer, K., Camhi, S., Arredondo, E., Pratt, C., Himes, J. H., & Going, S. (2006). Relationships among fitness, body composition, and physical activity. Medicine and Science in Sports and Exercise, 38(6), 1232.
- Higgins, J. P., & Hales, D. (2001). Adiposity and its relationship to physical activity in children and youth. Journal of Pediatrics, 139(6), 826-834. [CrossRef]
- Garcia-Hermoso, A., Saavedra, J. M., Escalante, Y., & Sanchez-Lopez, M. (2013). Effects of exercise on resting blood pressure in obese children: a meta-analysis of randomized controlled trials. Obesity Reviews, 14(11), 919-928. [CrossRef]
- Janssen, I., & LeBlanc, A. G. (2010). Systematic review of the health benefits of physical activity and fitness in school-aged children and youth. International Journal of Behavioral Nutrition and Physical Activity, 7(1), 40. [CrossRef]
- Sallis, J. F., Floyd, M. F., Rodríguez, D. A., & Saelens, B. E. (2012). Role of built environments in physical activity, obesity, and cardiovascular disease. Circulation, 125(5), 729-737. [CrossRef]
- Pate, R. R., Davis, M. G., Robinson, T. N., Stone, E. J., McKenzie, T. L., & Young, J. C. (2006). Promoting physical activity in children and youth: a leadership role for schools: a scientific statement from the American Heart Association Council on Nutrition, Physical Activity, and Metabolism (Physical Activity Committee) in collaboration with the Councils on Cardiovascular Disease in the Young and Cardiovascular Nursing. Circulation, 114(11), 1214-1224. [CrossRef]
Figure 1.
Nutritional status indicators by tertiles in girls according to educational establishment.
Figure 1.
Nutritional status indicators by tertiles in girls according to educational establishment.
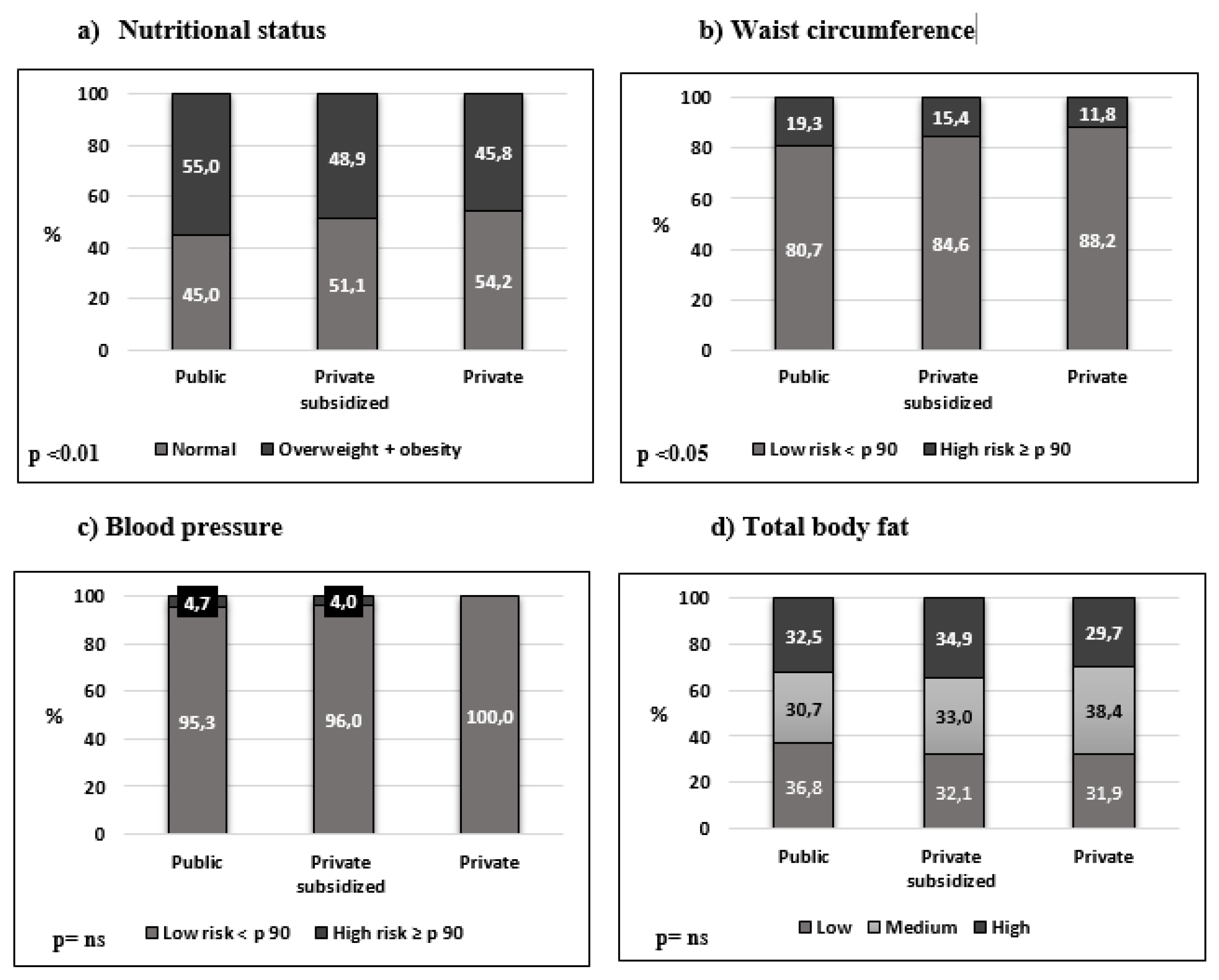
Figure 2.
Nutritional status indicators by tertiles in boys according to educational establishment.
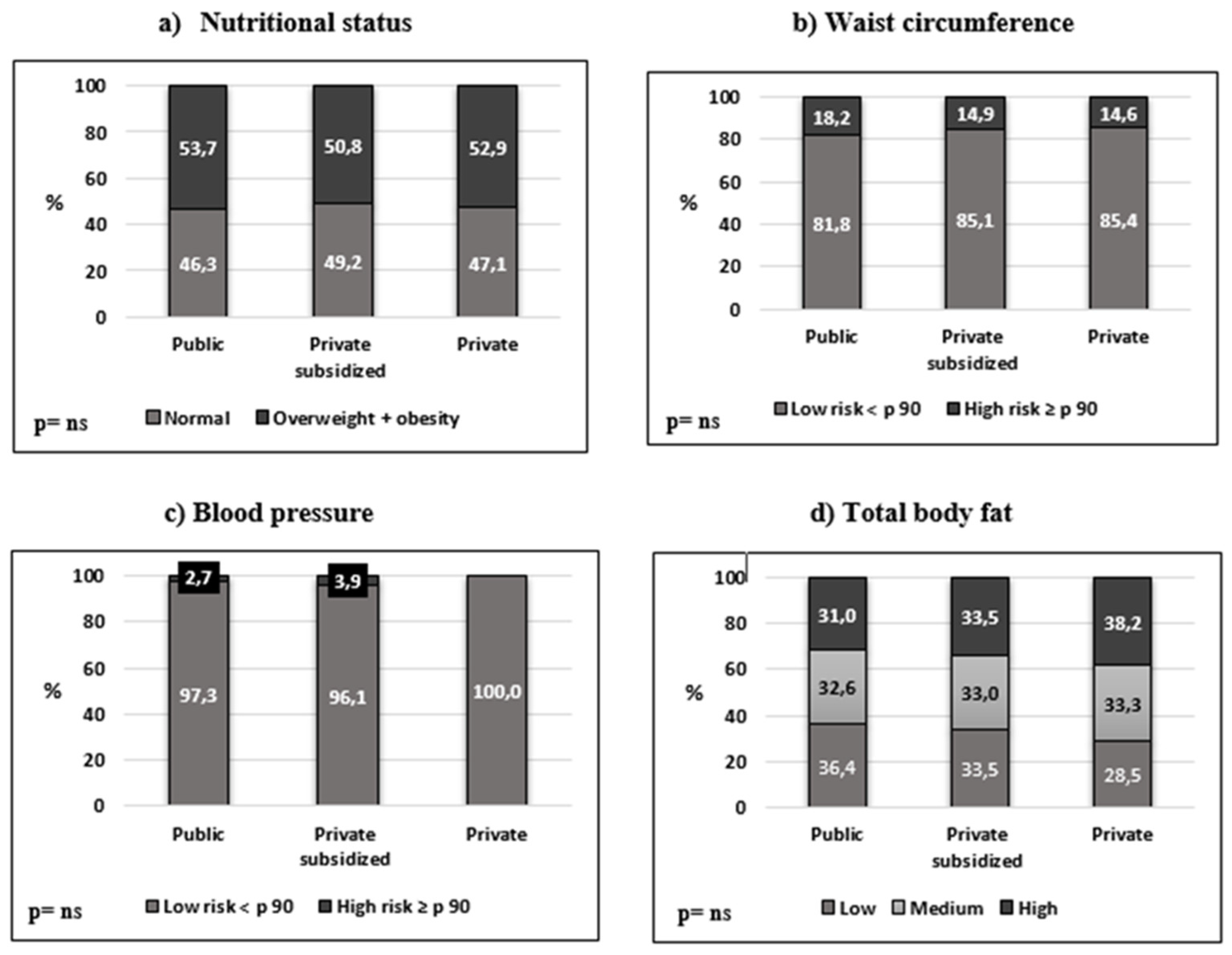
Figure 3.
ZScore MR vs. high, medium and low tertiles of horizontal jump (m) and distance covered in the walk test (m).
Figure 3.
ZScore MR vs. high, medium and low tertiles of horizontal jump (m) and distance covered in the walk test (m).
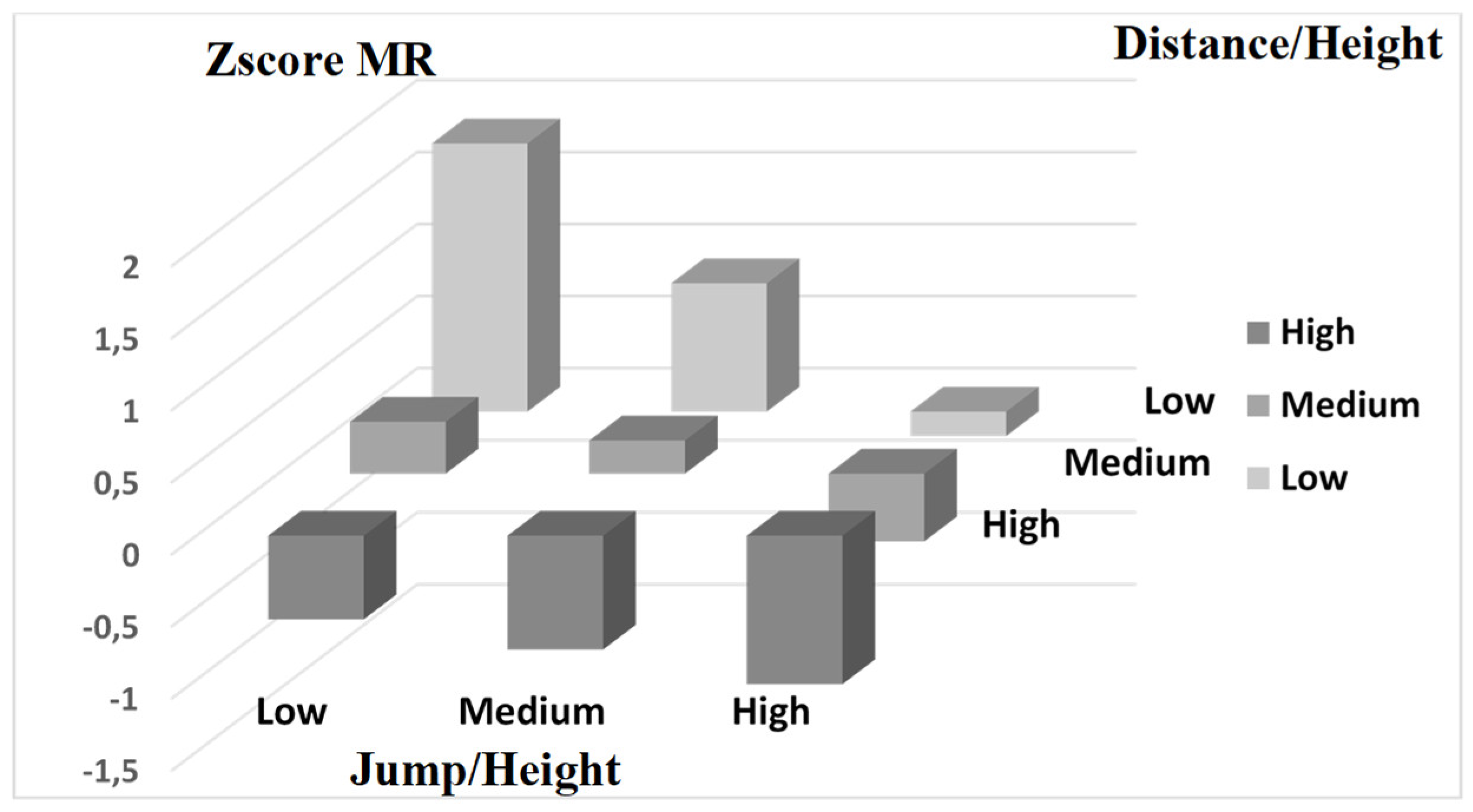
Figure 4.
ZScore MR vs. high, medium and low tertiles of distance (m) and grip strength (kg).
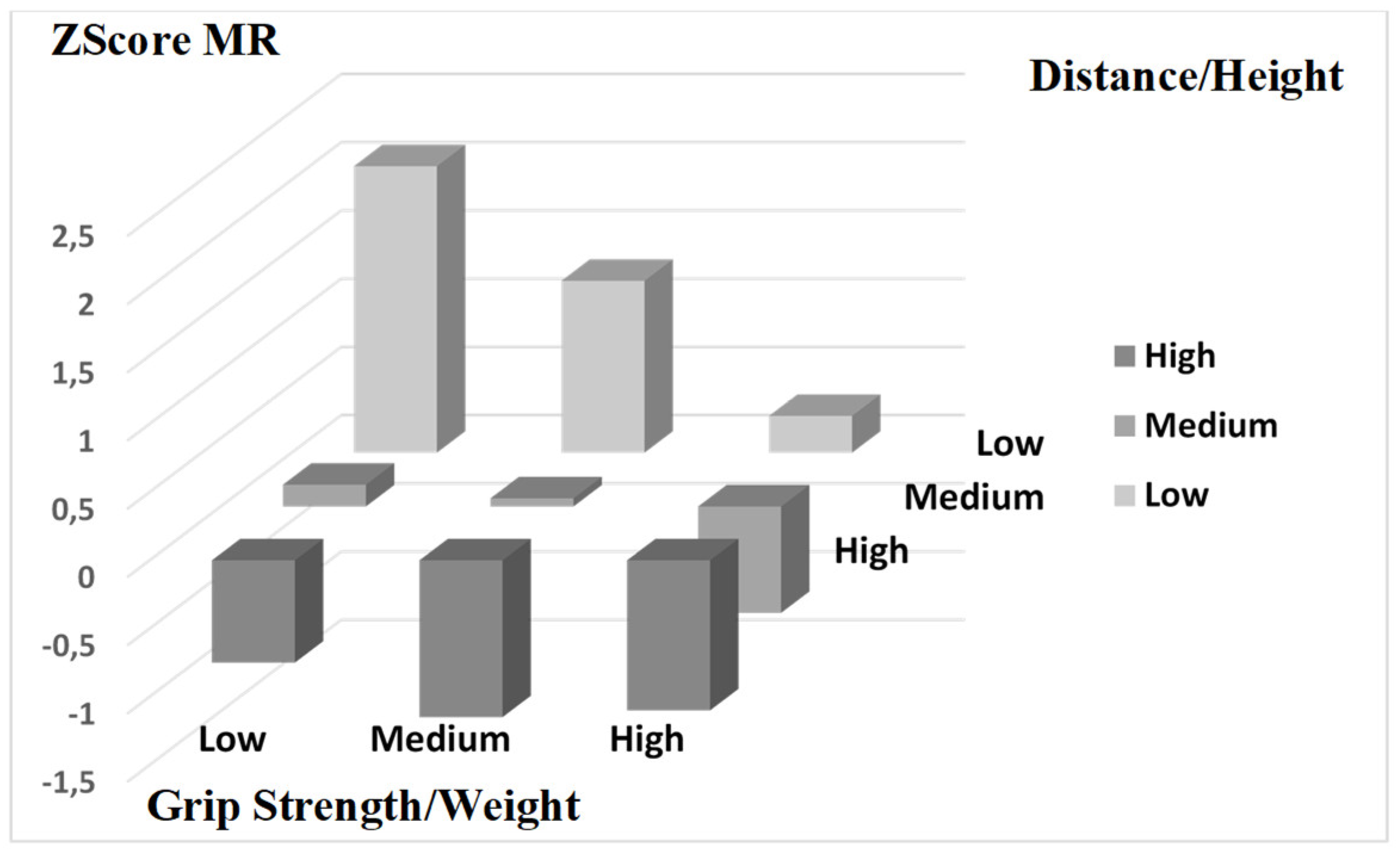

Table 1.
Obesity and proportion of schoolchildren with waist circumference and blood pressure > percentile 90.
Table 1.
Obesity and proportion of schoolchildren with waist circumference and blood pressure > percentile 90.
| Types of educational establishment |
Weight | Height | Sum of skinfolds | Obesity (%) | Waist circumference > p 90 (%) | Blood pressure > p 90 (%) |
|
|---|---|---|---|---|---|---|---|
|
Public school (n=486) |
40.6±15 | 139.4±14.1 | 52.4±23.6 | 23.7 | 21.0 | 3.7 | |
| Private subsidized school (n=1012) | 40.7±13.9 | 141.9±14.6 | 51.5 ± 23 | 18.4 | 15.9 | 3.9 | |
|
Private school (n=158) |
|||||||
| 39.7±11.9 | 141.6±13.6 | 49.6±23.8 | 14.6 | 12.7 | --- | ||
| p< 0.01* | p<0.01* | ||||||
* χ2.
Table 2.
Physical fitness and heart rate by types of educational establishment.
| Types of educational establishment |
Horizontal jump (m)* |
Grip strength (k) |
Distance 6-minute test (m) |
|---|---|---|---|
|
Public school (n=486) |
1.2 ± 0.3 | 16.6 ± 6.7 | 643.6 ± 65 |
|
Private subsidized school (n=1012) |
1.2 ± 0.3 | 17.6 ± 6.9 | 654.2 ± 64 |
|
Private school (n=158) |
1.6 ± 0.3 | 17.0 ± 6.4 | 636.4 ± 36 |
| *Kuskal-Wallis p <0.001 | |||
Table 3.
Correlations between physical fitness tests (adjusted for height or weight) and variables related to cardiovascular health.
Table 3.
Correlations between physical fitness tests (adjusted for height or weight) and variables related to cardiovascular health.
| Variable | Distance/ Height |
Jump/ Height |
Grip strength/ Weight |
|---|---|---|---|
| Waist circumference | -0.45 | 0.13 | 0.56 |
| p | 0.001 | 0.0001 | 0.0001 |
| Sum of skinfolds | -0.38 | -0.43 | -0.48 |
| p | 0.001 | 0.001 | 0.001 |
| Blood pressure | 0.27 | --- | --- |
| p | 0.01 | ||
Table 4.
Cut-off points for Z-Score MR (y-axis) for the categories high, medium and low categories of the Distance/Height (z-axis) and Jump/Height (x-axis) tests. Adjusted for sex and tanner stage.
Table 4.
Cut-off points for Z-Score MR (y-axis) for the categories high, medium and low categories of the Distance/Height (z-axis) and Jump/Height (x-axis) tests. Adjusted for sex and tanner stage.
| Variable | Low | Medium | High | Distance/Height |
| High | -0.58 | -0.79 | -1.03 | |
| Medium | 0.36 | 0.23 | -0.47 | |
| Low | 1.86 | 0.89 | -0.17 | |
| Jump/Height | ||||
Table 5.
Cut-off points for Z-Score MR (y-axis) for the categories high, medium and low categories of the Distance / Size (z-axis) and Grip Strength / Weight (x-axis) tests. Adjusted for sex and tanner stage.
Table 5.
Cut-off points for Z-Score MR (y-axis) for the categories high, medium and low categories of the Distance / Size (z-axis) and Grip Strength / Weight (x-axis) tests. Adjusted for sex and tanner stage.
| Variable | Low | Medium | High | Distance/Height |
|---|---|---|---|---|
| High | -0.75 | -1.15 | -1.1 | |
| Medium | 0.16 | 0.06 | -0.78 | |
| Low | 2.1 | 1.26 | 0.27 | |
| Grip strength/Weight |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



