
Submitted:
31 October 2024
Posted:
31 October 2024
You are already at the latest version
Abstract
Background/Objectives: The University of Wisconsin (UW) solution is the gold standard for kidney preservation. The addition of quercetin (QE) to the preservation solution reduces damage to renal kidney tubular cells, and the addition of sucrose (Suc) is beneficial for kidney preservation. The aim of this study was to investigate the protective effects of QE and Suc and to evaluate whether their use improves mitigates ischemia-reperfusion (I/R) injury after simple cold storage (CS) in porcine kidneys. Methods: Kidney grafts were procured after 30 min of warm ischemia, followed by preservation under two conditions for 22 h: group 1, preserved with CS/UW solution (n = 4), and group 2, preserved with CS/UW solution containing QE (33.1 μM) and Suc (0.1 M; (n = 6). All grafts were evaluated using an ex- vivo isolated kidney- reperfusion model with oxygenated, diluted, autologous blood at room temperature. Results: At the end of reperfusion, creatinine phosphokinase and lactate dehydrogenase levels were significantly lower in group 2 than those in group 1. Additionally, group 2 had a significantly higher number more of anti-ERG-positive endothelial- cell nuclei than group 1 at the end of reperfusion. Conclusions: Our results suggest that the addition of QE and Suc to the UW solution can improve mitigate I/R injury to the donated kidney after CS.
Keywords:
kidney preservation
; quercetin
; sucrose
; cold storage
; ischemia-reperfusion injury
1. Introduction
A shortage of organ donors is a universal problem in transplantation. The University of Wisconsin (UW) solution has been the gold standard for preservation of the liver, kidneys, and pancreas since it was first developed by Belzer and Southard [1]. Quercetin (QE), a widely used flavonoid, has strong antioxidant [2], anti-inflammatory [3], and anti-apoptotic properties [4]. Some bioflavonoids reportedly attenuate tubular-cell injury of kidneys during cold preservation in EuroCollins and UW solutions [5]. In addition, the beneficial effects of these solutions may be due to their ability to prevent tissue edema during cold storage (CS). Sucrose (Suc) has exhibited beneficial effects as a supplement to such solutions [6]. The aim of this study was to investigate the protective effects of QE and Suc against CS-associated injury in porcine kidneys and to evaluate whether their use reduces ischemia-reperfusion (I/R) injury after simple CS. We discovered that their addition to the UW solution may prevent such CS-associated injury.
2. Materials and Methods
2.1. Animals
The Institutional Animal Ethics Committee of the Clinical Research Center, Asahikawa Medical University, Japan (permit no. R4-089) approved all experimental procedures. We used domestic pigs (male crossbreeds of Large-Yorkshire, Landrace, and Duroc hogs, 2–3 months old, 30 kg; Taisetsu Sanroku-Sya, Asahikawa, Japan) in this study.
Midazolam (0.3 mg/kg), medetomidine hydrochloride (0.06 mg/kg), and butorphanol tartrate (0.03 mg/kg) were injected into pigs’ femoral muscle for anesthetic induction. The peripheral ear vein was cannulated, and Ringer’s lactate solution was infused at a rate of 6.7–10 mL/kg/h. Thiamylal sodium (4.2 mg/kg) was intravenously injected, and intubation was performed. Anesthesia was maintained with propofol and oxygen (4 L/min). The internal jugular vein was subsequently infused with 6% (w/v) hydroxyethyl starch (33.3 mL/kg/h).
The pigs underwent midline laparotomy. The right common iliac artery was isolated, and a catheter was inserted to procure ~400 mL of autologous whole blood. The ureter, renal artery, and renal vein were identified, and the blood flow was cut off. We intravenously infused potassium chloride (2 mEq/kg) to induce cardiac arrest. The kidneys were kept under warm ischemic conditions for 30 min to simulate kidney donation after circulatory death (DCD). The kidney graft was retrieved and washed from the renal artery with 200 mL of each preservation solution at 4 °C as a back-table procedure. The kidney grafts were preserved under CS conditions for 22 hours at 4 °C.
2.2. Study design
After 30 min of warm-ischemia time, kidney grafts were preserved under one of two conditions for 22 hours: group 1, preserved with UW solution (n = 4) and Group 2, preserved with UW solution containing QE (33.1 μM) and Suc (0.1 M; n = 6).
2.3. Isolated ex-vivo reperfusion model
Kidney function was evaluated using an isolated kidney-reperfusion model. The grafts were reperfused with oxygenated, diluted, autologous blood at room temperature. The reperfusion parameters for the renal artery were set to 90–100 mmHg and ~20 mL/min. The reperfusion fluid was autologous whole blood containing 500 mL saline, 250 mL dextran, 60 mL calcium gluconate hydrate, 22 mL 8.5% bicarbonate, and heparin. Heparin levels were adjusted to an activated clotting time of 300 s. The hematocrit was maintained at ~10–12%. The oxygenator was regulated to achieve physio-logical blood-gas values (pO2, ~290–300 mmHg; pCO2, 10 mmHg).
2.4. Biochemistry
Blood urea nitrogen (BUN), creatinine (Cr), Cr phosphokinase (CPK), and lactate dehydrogenase (LDH) levels in the perfusate were measured every 60 min during reperfusion to determine the viability of the preserved kidney grafts by using standard biochemical methods. In addition, lactate levels were measured every 60 min during reperfusion by using a blood-gas analyzer (i-STAT 1 Analyzer; Abbott Japan LLC, Tokyo, Japan).
2.5. Histopathological Evaluation
A kidney wedge biopsy was performed immediately after laparotomy, before and after preservation, and 1 and 3 h after isolated ex-vivo reperfusion. The kidney tissue was fixed in 10% phosphate-buffered formalin and embedded in paraffin. Each sample was sectioned into 3-μm slices, dehydrated using ethanol, and subjected to hematoxylin-eosin staining.
ERG immunohistochemistry was performed to assess endothelial-cell damage in glomerular and peritubular capillary networks. Additionally, cluster of differentiation (CD)42b immunohistochemistry was performed to assess platelet aggregation in the glomerular tufts and around the renal tubules.
We used a primary rabbit anti-ERG monoclonal antibody was used (clone EP111; Nichirei Bioscience Co., Ltd., Tokyo, Japan) and a rabbit anti-CD42b polyclonal anti-body (GeneID 2811; Proteintech Group, Inc., Rosemont, IL, US). EnVision-labeled polymer reagent (DAKO, Glostrup, Denmark) was used as the secondary antibody. ImageJ (National Institutes of Health, Bethesda, MD, US; https://imagej.nih.gov/ij/download.html) was used to quantify the anti-ERG- and CD42b-positive areas. The number of anti-ERG-positive endothelial-cell nuclei and the anti-CD42b-positive area were determined automatically in at least 10 randomly selected non-overlapping fields using the ImageJ software.
2.6. Gene expression
Quantitative reverse transcription-polymerase chain reactions were used to determine the gene-expression levels of endothelial-specific, inflammatory, and apoptotic proteins. Kidney-parenchyma biopsies were performed after laparotomy, before and after preservation, and 3 h after reperfusion. The samples were stored at -80 °C until analysis. Total RNA was extracted from snap-frozen biopsy specimens by using an miRNeasy Micro Kit (Qiagen, Valencia, CA, USA). RNA concentrations were deter-mined using a spectrophotometer (NanoDrop 2000; NanoDrop Technologies, Wilmington, DE, USA). Equal amounts of RNA were converted to complementary DNA by using the Transcriptor First Strand cDNA Synthesis Kit (Roche, Basel, Switzerland), and complementary DNA concentrations were measured using a LightCycler 480 System II (Roche). The relative expression level of the mRNA of interest was normalized to that of the housekeeping gene—glyceraldehyde-3-phosphate dehydrogenase (GAPDH). Data are presented as quantities relative to that of GAPDH. Table 1 summarizes the sense and antisense primer sequences.
2.7. Statistical Analyses
Values are presented as the mean ± standard deviation. Statistical analyses were performed using Microsoft Excel 2013 (Microsoft Corp., Redmond, WA, USA). The results were analyzed using Student’s t-test. P-values < 0.05 were considered statistically significant.
3. Results
3.1. BUN, Cr, CPK, LDH, And Lactate in the Perfusate Solution
No BUN-level differences were observed between the groups. At the end of reperfusion, the BUN levels in groups 1 and 2 were 4.30 ± 0.56 and 4.65 ± 1.01 mg/dL, respectively (P = 0.504; Figure 1A). Cr levels also did not differ between groups. At the end of reperfusion, the Cr levels in groups 1 and 2 were 0.45 ± 0.07 and 0.49 ± 0.45 mg/dL, respectively (P = 0.396; Figure 1B).
At 0, 1, and 2 h and at the end of reperfusion, CPK levels were lower in group 2 (313.16 ± 171.12, 391.00 ± 184.33, 449.33 ± 189.95, and 504.66 ± 200.33 IU/L, respectively) than those in group 1 (1249.75 ± 188.50, 1409.25 ± 204.43, 1490.25 ± 149.65, and 1504.00 ± 94.92 IU/L, respectively; all P < 0.001; Figure 1C).
At 0 and 1 h and at the end of reperfusion, the LDH levels were lower in group 2 than those in group 1 (154.16 ± 25.54 vs. 215.55 ± 35.42 (P =), 233.33 ± 61.90 vs. 411.00 ± 101.88 (P =), and 573.66 ± 151.52 vs. 836.00 ± 141.08 mg/dL (P =), respectively). The LDH levels at 2 h did not differ between the groups (420.50 ± 141.77 vs. 634.00 ± 166.12 mg/dL; P = 0.080; Figure 1D). No differences were observed in lactate levels between the groups. At the end of reperfusion, the lactate levels in groups 1 and 2 were 10.84 ± 0.86 and 10.38 ± 0.69 mg/dL, respectively (P = 0.40; Figure 1E).
3.2. Histological Observations During Reperfusion
3.2.1. Hematoxylin–Eosin Staining
At the end of reperfusion, we observed more vacuolation in the tubular epithelial cells in group 1 than that in group 2. In addition, the tubular epithelium exhibited more irregularity and exfoliation in group 1 than that in group 2. Group 1 also had more interstitial inflammation and hemorrhaging than group 2 (Figure 2).
3.2.2. ERG and CD42b Immunohistochemistry
At the end of reperfusion, group 2 had higher numbers of anti-ERG-positive endothelial-cell nuclei than group 1 (433.70 ± 151.69 [group 2] vs. 378.02 ± 119.29 [group 1] per field; P = 0.043; Figure 3). However, the anti-CD42b-positive areas at the end of reperfusion did not differ between the groups (22087.62 ± 14258.80 [group 1] vs. 17176.51 ± 10944.07 mg/dL [group 2]; P = 0.069; Figure 4).
3.3. Gene Expression
No differences in gene expression were observed between the groups. At the end of reperfusion, groups 1 and 2 did not differ in the expression of tumor necrosis factor-alpha (TNF-α; 0.2223 ± 0.0749 vs. 0.1423 ± 0.0579; P = 0.092; Figure 5A), interferon-gamma (IFN-γ) (0.0797 ± 0.0406 vs. 0.0447 ± 0.0183; P = 0.096; Figure 5B), or caspa-se-3 (0.4381 ± 0.1785 vs. 0.3269 ± 0.1156; P = 0.261; Figure 5C).
4. Discussion
Kidney transplantation is an established treatment for kidney failure. However, a shortage of kidney grafts has become a global problem. DCD and other donors have been used to expand the available donor pool [7,8]; however, an optimal preservation solution for grafts from marginal kidney donors, such as DCD, has not yet been developed.
CS is the easiest and most widely used preservation method for kidney trans-plants. However, prolonged CS can lead to postoperative complications, early graft dysfunction, and poor post-transplantation outcomes [9,10]. This is because ischemia during storage is associated with oxidative stress and apoptosis. Oxidative stress results from an imbalance between the production of reactive oxygen species (ROS), the level of antioxidants, and the effectiveness of repair processes [11]. ROS-mediated lipid peroxidation is hypothesized to be an important cause of cell-membrane damage during oxidative stress [12].
The UW solution, commonly used for preservation, has limitations in the prevention of oxidative injury; however, the addition of antioxidants has yielded improved cell survival [13]. New preservation techniques that can resolve these problems, im-prove organ quality, and decrease severe complications are receiving increasing inter-est. To this end, various new organ-preservation strategies have been examined [3].
QE is an excellent in-vitro antioxidant and the most potent ROS scavenger in the flavonoid family [14]. The inhibition of nuclear factor kappa-light-chain-enhancer of activated B cells (NF-κB) activation, which is required for tissue repair, has been suggested to prevent apoptosis associated with kidney I/R injury [15,16]. Kinaci et al. re-ported that NF-κB expression was significantly decreased by QE treatment in an I/R rat model [4]. Thus, QE treatment reduced kidney I/R injury by reducing apoptosis. The levels of enzymes such as superoxide dismutase, catalase, and glutathione peroxidase reportedly become insufficient during I/R associated with abundant ROS formation [17,18]. Inal et al. reported that the levels of these enzymes in the renal cortex of the I/R group were significantly lower than those in the control group, but that the difference was not significant [17]. These results suggest that QE exerts a protective effect against ROS production during renal I/R.
Considering its metabolism in the organs and the stability of its effects, the ideal QE concentration in a rat model of cold preservation and orthotopic transplantation of the liver was determined as 33.1 μM [19]. Kato et al. showed that aspartate aminotransferase and alanine aminotransferase levels were significantly lower in the group treated with UW containing QE and Suc than those in the group treated with UW alone after orthotopic liver transplantation in rats [19]. In addition, Gochi et al. used a QE concentration of 33.1 µM in a porcine model of kidney autologous trans-plantation and revealed lower lipid-peroxidation levels and renal resistance when QE and Suc were combined as a machine-perfusion solution for hypothermic oxygenated perfusion [20]. Because QE is less expensive than other flavonoid compounds, it is considered suitable for clinical applications from an economic perspective.
In this study, the protective effects of a preservation solution containing QE and Suc during CS were demonstrated using early kidney-function tests. Soares et al. evaluated the effects of alprostadil in an experimental model of I/R injury in rat kidney tissue and reported that CPK levels in the alprostadil-treated group were significantly lower than those in the vehicle-treated group [21].
Ahlenstiel et al. measured the LDH release in cultured kidney tubular cells and reported that the addition of bioflavonoids to preservation solutions significantly reduced cell injury during CS [5,22]. Our study revealed that the addition of GE and Suc to the UW solution yielded significantly higher CPK and LDH levels than the UW solution alone during reperfusion.
Kidney transplantation is associated with a high likelihood of endothelial injury in allografts [23]. Given its intimate contact with the blood, the endothelium is the primary affected structure during I/R injury. The resulting tubular and endothelial dam-age, particularly in the peritubular capillary network, induces microvascular rarefaction. Jansen et al. discovered that renal I/R injury in mice led to increased platelet activation in the immediate proximity of necrotic cell casts [24]. ERG immunohistochemical experiments revealed that group 2 had significantly more endothelial cells during reperfusion than group 1. CD42b immunohistochemical experiments revealed a great-er degree of platelet aggregation during reperfusion in group 1 than that in group 2, although no significant difference was observed. These results indicate that the addition of QE and Suc to the UW solution can mitigate I/R injury.
IFN-γ, which is associated with macrophage activation and neutrophil recruitment, may amplify the immune response following kidney reperfusion, mediating the early I/R injury phase [25,26]. Additionally, early TNF-α expression in kidney tissue contributes to neutrophil infiltration and injury after renal I/R [27]. Yang et al. showed that caspase-3 is a pivotal regulator of microvascular endothelial-cell apoptosis, kidney fibrosis, and microvascular injury after I/R [28]. In this study, IFN-γ, TNF-α, and caspase-3 levels were lower in group 2 than those in group 1, although these differences were not. These results also suggest that the addition of QE and Suc to the UW solution alleviated I/R injury.
This study has several limitations. First, owing to the small sample, we could not exclude surgical bias from our experiments. This bias should be reduced by increasing the number of samples in future studies, stabilizing surgical procedures. Second, the protective effect was limited by the short I/R period used in this study. Further studies are required to investigate the mechanisms of action of QE and Suc in the UW solution by using transplantation models.
5. Conclusions
We investigated the utility of the flavonoids QE and Suc in kidney transplantation by using a reperfusion model in CS. Our results suggest that the addition of QE and Suc to the UW solution may be effective to prevent CS-associated injury in DCD kidneys, with QE possibly exerting this beneficial action by suppressing oxidative stress, and may enhance kidney-transplantation outcomes.
Author Contributions
Conceptualization, N.M.; methodology, N.M. and H.O.; validation, D.I., A.T., Y.S., Y.O. and N.M.; formal analysis, H.O., Y.S. and Y.O.; investigation, H.D. and M.I.; data curation, H.O., Y.S. and Y.O.; writing—original draft preparation, D.I. and A.T.; writing—review and editing, H.O., Y.N. and N.M.; supervision, N.M.; project administration, N.M.; All authors have read and agreed to the published version of the manuscript.
Funding
No funding was received to assist with the preparation of this manuscript.
Institutional Review Board Statement
The animal study protocol was approved by the Institutional Animal Ethics Committee of the Clinical Research Center, Asahikawa Medical University, Japan (protocol code R4-089).
Informed Consent Statement
Not applicable.
Data Availability Statement
The authors confirm that the data supporting the findings of this study are available within the article and its supplementary materials.
Acknowledgments
We would like to thank Editage (www.editage.com) for English language editing.
Conflicts of Interest
The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; in the decision to publish the results.
References
- Southard, J.H.; Belzer, F.O. Organ preservation. Annu Rev Med 1995, 46, 235–247. [CrossRef]
- Liu, C.M.; Zheng, Y.L.; Lu, J.; Zhang, Z.F.; Fan, S.H.; Wu, D.M.; Ma, J.Q. Quercetin protects rat liver against lead-induced oxidative stress and apoptosis. Environ Toxicol Pharmacol 2010, 29, 158–166. [CrossRef]
- Zielińska, M.; Kostrzewa, A.; Ignatowicz, E.; Budzianowski, J. The flavonoids, quercetin and isorhamnetin 3-O-acylglucosides diminish neutrophil oxidative metabolism and lipid peroxidation. Acta Biochim Pol 2001, 48, 183–189.
- Kinaci, M.K.; Erkasap, N.; Kucuk, A.; Koken, T.; Tosun, M. Effects of quercetin on apoptosis, NF-κB and NOS gene expression in renal ischemia/reperfusion injury. Exp Ther Med 2012, 3, 249–254. [CrossRef]
- Ahlenstiel, T.; Burkhardt, G.; Köhler, H.; Kuhlmann, M.K. Bioflavonoids attenuate renal proximal tubular cell injury during cold preservation in Euro-Collins and University of Wisconsin solutions. Kidney Int 2003, 63, 554–563. [CrossRef]
- Kumano, K.; Wang, W.; Endo, T. [Effects of osmotic agents for cold kidney preservation.] Nihon Hinyokika Gakkai Zasshi 1994, 85, 925–931. [CrossRef]
- Bertuzzo, V.R.; Cescon, M.; Odaldi, F.; Di Laudo, M.; Cucchetti, A.; Ravaioli, M.; Del Gaudio, M.; Ercolani, G.; D'Errico, A.; Pinna, A.D. Actual risk of using very aged donors for unselected liver transplant candidates: a European single-center experience in the MELD era. Ann Surg 2017, 265, 388–396. [CrossRef]
- Flores, A.; Asrani, S.K. The donor risk index: a decade of experience. Liver Transpl 2017, 23, 1216–1225. [CrossRef]
- Hoyer, D.P.; Paul, A.; Gallinat, A.; Molmenti, E.P.; Reinhardt, R.; Minor, T.; Saner, F.H.; Canbay, A.; Treckmann, J.W.; Sotiropoulos, G.C.; Mathé, Z. Donor information based prediction of early allograft dysfunction and outcome in liver transplantation. Liver Int 2015, 35, 156–163. [CrossRef]
- Agopian, V.G.; Petrowsky, H.; Kaldas, F.M.; Zarrinpar, A.; Farmer, D.G.; Yersiz, H.; Holt, C.; Harlander-Locke, M.; Hong, J.C.; Rana, A.R.; Venick, R.; McDiarmid, S.V.; Goldstein, L.I.; Durazo, F.; Saab, S.; Han, S.; Xia, V.; Hiatt, J.R.; Busuttil, R.W. The evolution of liver transplantation during 3 decades: analysis of 5347 consecutive liver transplants at a single center. Ann Surg 2013, 258, 409–421. [CrossRef]
- Elahi, M.M.; Kong, Y.X.; Matata, B.M. Oxidative stress as a mediator of cardiovascular disease. Oxid Med Cell Longev 2009, 2, 259–269. [CrossRef]
- Kaçmaz, A.; Polat, A.; User, Y.; Tilki, M.; Ozkan, S.; Sener, G. Octreotide: a new approach to the management of acute abdominal hypertension. Peptides 2003, 24, 1381–1386. [CrossRef]
- Salahudeen, A.K.; Huang, H.; Patel, P.; Jenkins, J.K. Mechanism and prevention of cold storage-induced human renal tubular cell injury. Transplantation 2000, 70, 1424–1431. [CrossRef]
- Heijnen, C.G.M.; Haenen, G.R.M.M.; Oostveen, R.M.; Stalpers, E.M.; Bast, A. Protection of flavonoids against lipid peroxidation: the structure activity relationship revisited. Free Radic Res 2002, 36, 575–581. [CrossRef]
- Seok, Y.M.; Kim, J.; Park, M.J.; Boo, Y.C.; Park, Y.K.; Park, K.M. Wen-pi-tang-Hab-Wu-ling-san attenuates kidney fibrosis induced by ischemia/reperfusion in mice. Phytother Res 2008, 22, 1057–1063. [CrossRef]
- Spandou, E.; Tsouchnikas, I.; Karkavelas, G.; Dounousi, E.; Simeonidou, C.; Guiba-Tziampiri, O.; Tsakiris, D. Erythropoietin attenuates renal injury in experimental acute renal failure ischaemic/reperfusion model. Nephrol Dial Transplant 2006, 21, 330–336. [CrossRef]
- Inal, M.; Altinişik, M.; Bilgin, M.D. The effect of quercetin on renal ischemia and reperfusion injury in the rat. Cell Biochem Funct 2002, 20, 291–296. [CrossRef]
- Ahmad, N.; Pratt, J.R.; Potts, D.J.; Lodge, J.P.A. Comparative efficacy of renal preservation solutions to limit functional impairment after warm ischemic injury. Kidney Int 2006, 69, 884–893. [CrossRef]
- Kato, F.; Gochi, M.; Kawagoe, T.; Yotsuya, S.; Matsuno, N. The protective effects of quercetin and sucrose on cold preservation injury in vitro and in vivo. Organ Biology 2020, 27, 207–215. [CrossRef]
- Gochi, M.; Kato, F.; Toriumi, A.; Kawagoe, T.; Yotsuya, S.; Ishii, D.; Otani, M.; Nishikawa, Y.; Furukawa, H.; Matsuno, N. A novel preservation solution containing quercetin and sucrose for porcine kidney transplantation. Transplant Direct 2020, 6, e624. [CrossRef]
- Soares, B.L.F.; de Freitas, M.A.L.; Montero, E.F.S.; Pitta, G.B.B.; Miranda, F., Jr. Alprostadil attenuates inflammatory aspects and leucocytes adhesion on renal ischemia and reperfusion injury in rats. Acta Cir Bras 2014, 29 Suppl 2, 55–60. [CrossRef]
- Ahlenstiel, T.; Burkhardt, G.; Köhler, H.; Kuhlmann, M.K. Improved cold preservation of kidney tubular cells by means of adding bioflavonoids to organ preservation solutions. Transplantation 2006, 81, 231–239. [CrossRef]
- Cardinal, H.; Dieudé, M.; Hébert, M.J. Endothelial dysfunction in kidney transplantation. Front Immunol 2018, 9, 1130. [CrossRef]
- Jansen, M.P.B.; Emal, D.; Teske, G.J.D.; Dessing, M.C.; Florquin, S.; Roelofs, J.J.T.H. Release of extracellular DNA influences renal ischemia reperfusion injury by platelet activation and formation of neutrophil extracellular traps. Kidney Int 2017, 91, 352–364. [CrossRef]
- Kinsey, G.R.; Li, L.; Okusa, M.D. Inflammation in acute kidney injury. Nephron Exp Nephrol 2008, 109, e102–e107. [CrossRef]
- Dong, X.; Swaminathan, S.; Bachman, L.A.; Croatt, A.J.; Nath, K.A.; Griffin, M.D. Resident dendritic cells are the predominant TNF-secreting cell in early renal ischemia-reperfusion injury. Kidney Int 2007, 71, 619–628. [CrossRef]
- Donnahoo, K.K.; Meng, X.; Ayala, A.; Cain, M.P.; Harken, A.H.; Meldrum, D.R. Early kidney TNF-alpha expression mediates neutrophil infiltration and injury after renal ischemia-reperfusion. Am J Physiol 1999, 277, R922–R929. [CrossRef]
- Yang, B.; Lan, S.; Dieudé, M.; Sabo-Vatasescu, J.P.; Karakeussian-Rimbaud, A.; Turgeon, J.; Qi, S.; Gunaratnam, L.; Patey, N.; Hébert, M.J. Caspase-3 is a pivotal regulator of microvascular rarefaction and renal fibrosis after ischemia-reperfusion injury. J Am Soc Nephrol 2018, 29, 1900–1916. [CrossRef]
Figure 1.
Laboratory results. (a) Blood urea nitrogen (BUN; mg/dL); (b) Creatinine (Cr; mg/dL); (c) Cr phosphokinase (CPK; IU/L); (d) Lactate dehydrogenase (LDH; mg/dL); and (e) lactate (mg/dL) levels (mean ± standard deviation) in the perfusate solution before, and 1, 2, and 3 h after reperfusion.
Figure 1.
Laboratory results. (a) Blood urea nitrogen (BUN; mg/dL); (b) Creatinine (Cr; mg/dL); (c) Cr phosphokinase (CPK; IU/L); (d) Lactate dehydrogenase (LDH; mg/dL); and (e) lactate (mg/dL) levels (mean ± standard deviation) in the perfusate solution before, and 1, 2, and 3 h after reperfusion.
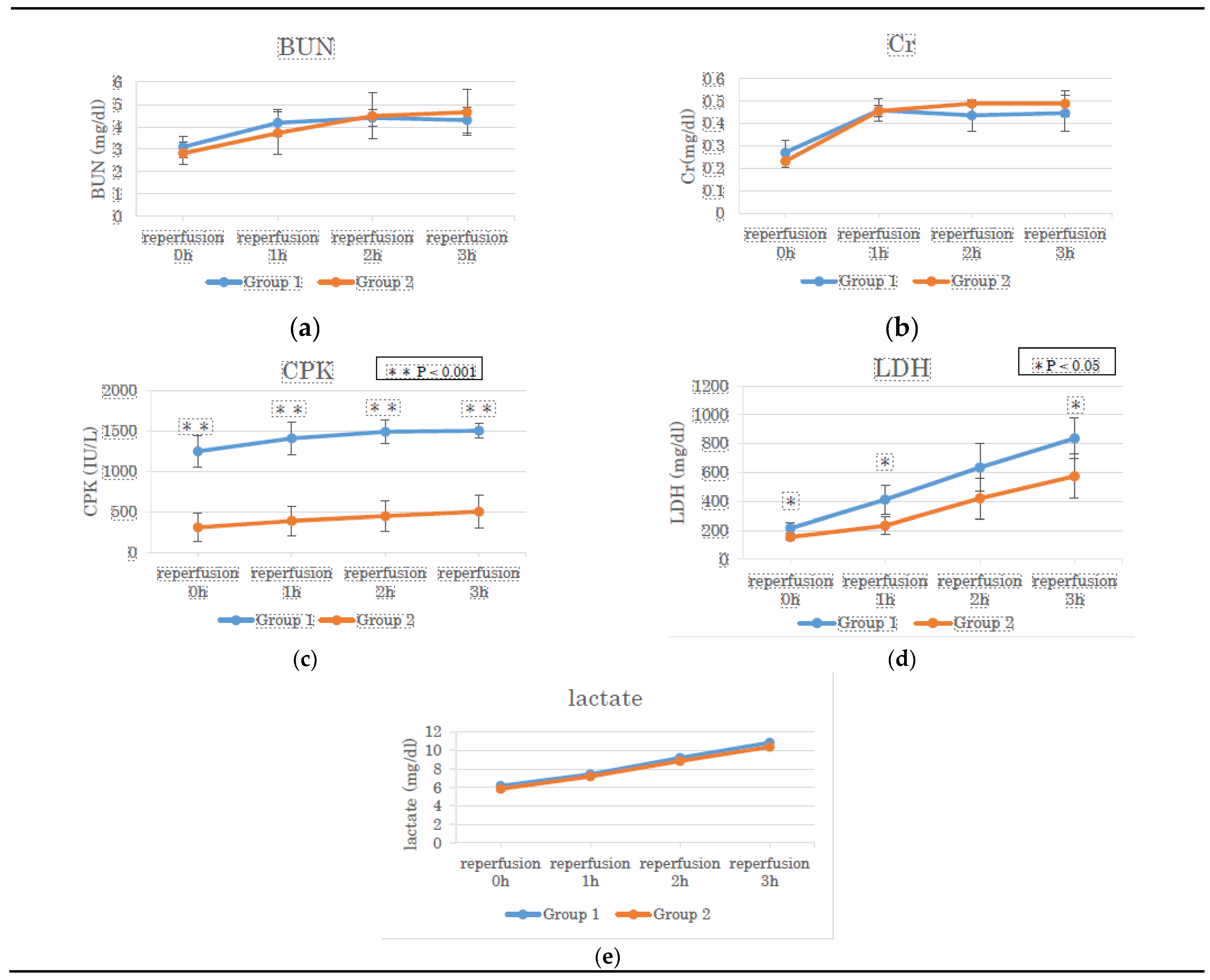
Figure 2.
Hematoxylin–eosin staining at the end of reperfusion. (a) Group 1; (b) Group 2.
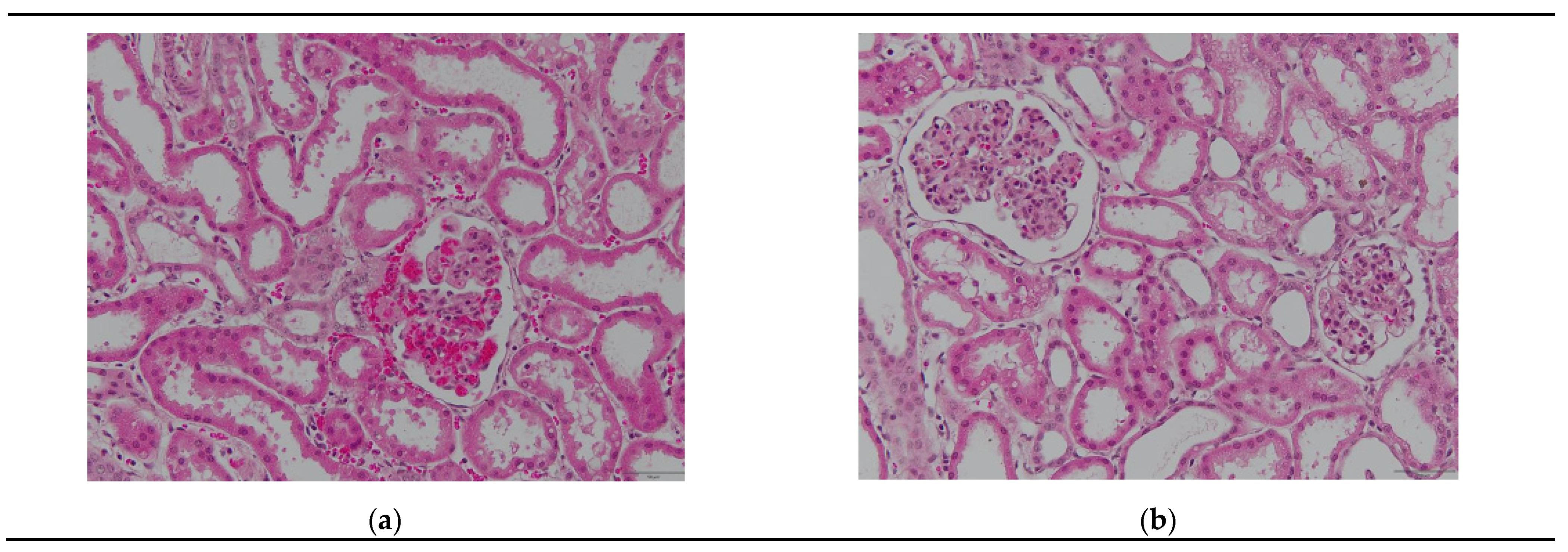
Figure 3.
ERG immunohistochemistry at the end of reperfusion. (a) Group 1; (b) Group 2; (c) Quantification of anti-ERG-positive area in groups 1 and 2.
Figure 3.
ERG immunohistochemistry at the end of reperfusion. (a) Group 1; (b) Group 2; (c) Quantification of anti-ERG-positive area in groups 1 and 2.
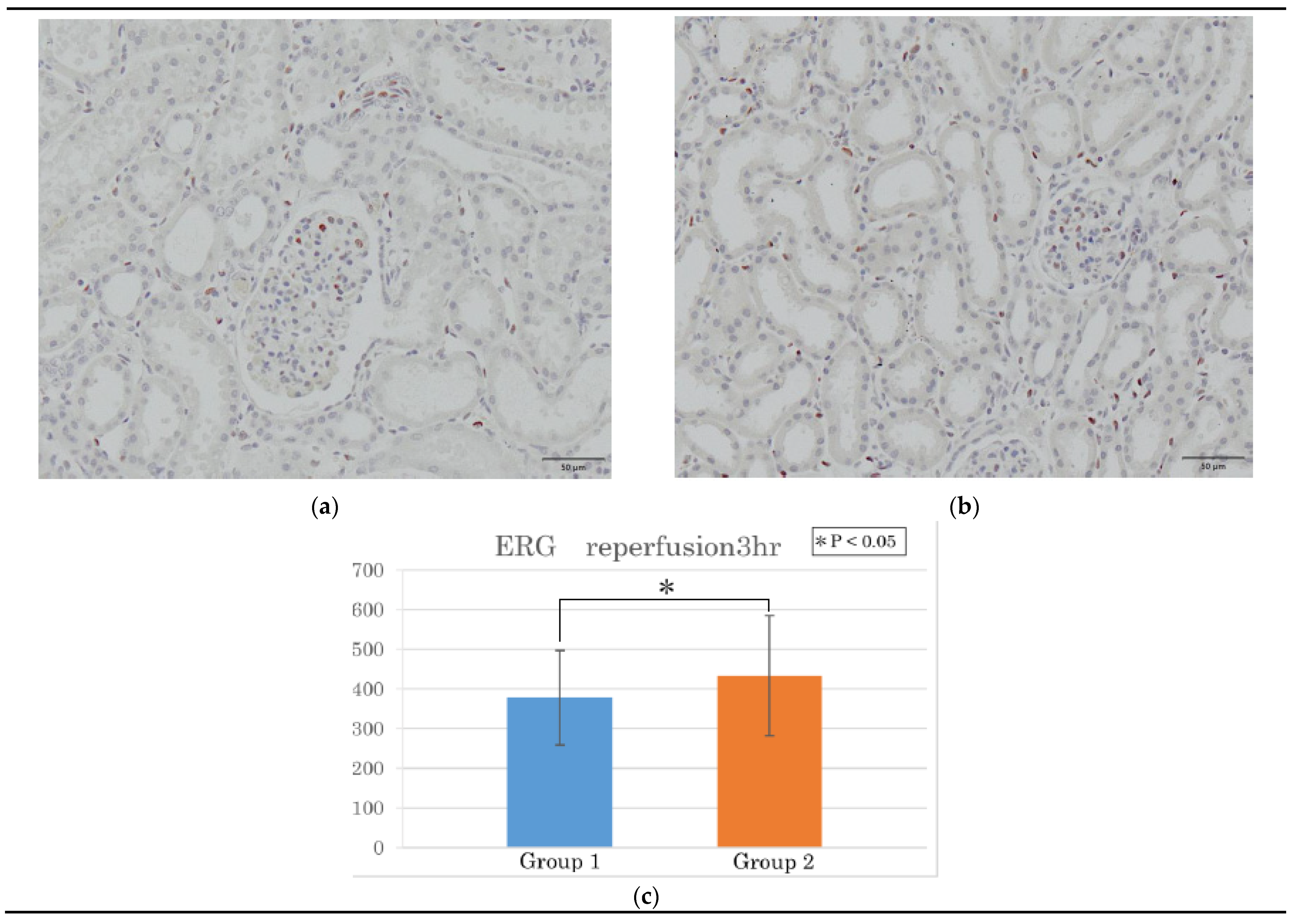
Figure 4.
Cluster of differentiation (CD)42b immunohistochemistry at the end of reperfusion. (a) Group 1; (b) Group 2; (c) Quantification of anti-CD42b-positive area in groups 1 and 2.
Figure 4.
Cluster of differentiation (CD)42b immunohistochemistry at the end of reperfusion. (a) Group 1; (b) Group 2; (c) Quantification of anti-CD42b-positive area in groups 1 and 2.
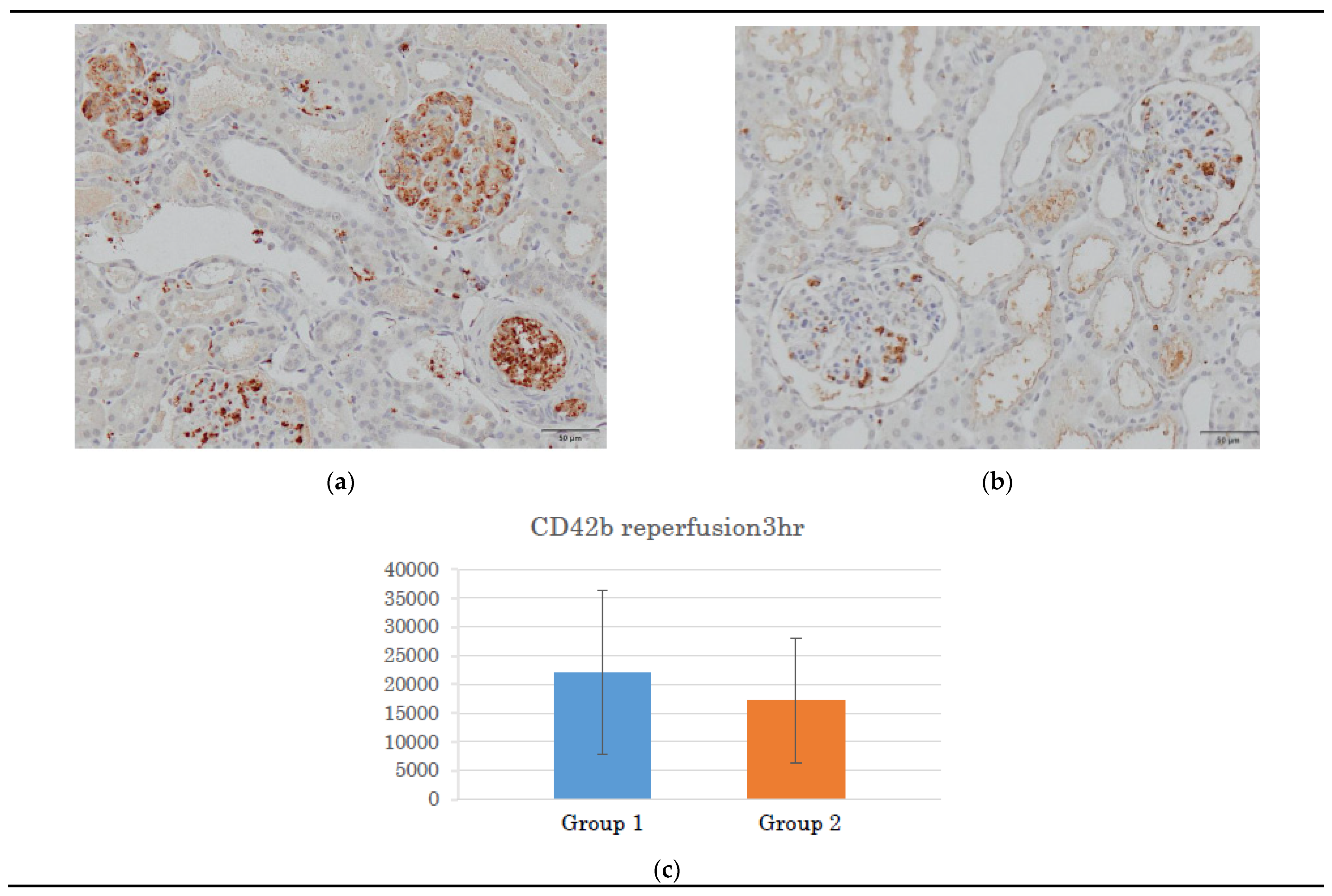
Figure 5.
Reverse transcription-polymerase chain reaction. (a) TNF-α; (b) IFN-γ; and (c) caspase-3 value after laparotomy, before and after preservation, and 3 h after reperfusion. Values are ex-pression levels relative to that of GAPDH. CS, cold storage.
Figure 5.
Reverse transcription-polymerase chain reaction. (a) TNF-α; (b) IFN-γ; and (c) caspase-3 value after laparotomy, before and after preservation, and 3 h after reperfusion. Values are ex-pression levels relative to that of GAPDH. CS, cold storage.
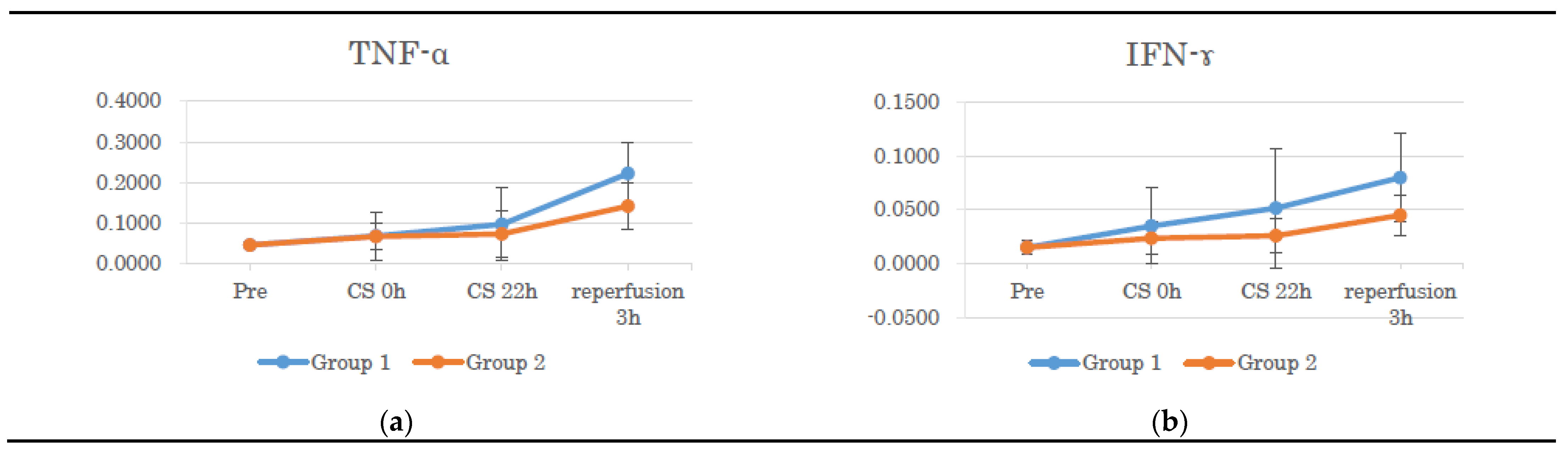
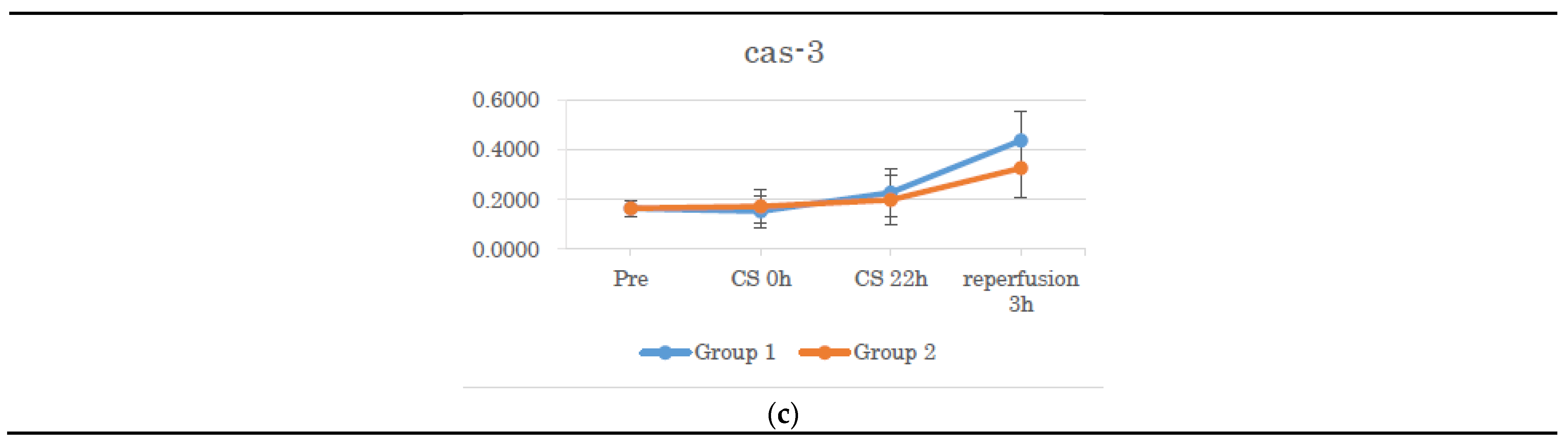

Table 1.
PCR primers.
| Primer | Forward | Reverse |
|---|---|---|
| GAPDH | AGGAGTAAGAGCCCCTGGAC | GTGTGTTGGGGGATCGAGT |
| TNF-α | TTGTCGCTACATCGCTGAAC | CCAGTAGGGCGGTTACAGAC |
| IFN-γ | TTCAGCTTTGCGTGACTTTG | TGCATTAAAATAGTCCTTTAGGATCG |
| Caspase-3 | GAATGGCATGTCGATCTGGT | TTGTGAAGGTCTCCCTGAGATT |
GAPDH: glyceraldehyde-3-phosphate dehydrogenase; IFN-γ: interferon-gamma; TNF-α: tumor necrosis factor-alpha.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



