
Submitted:
01 November 2024
Posted:
01 November 2024
You are already at the latest version
Abstract
Delirium is the most common complication after major surgeries, with incidence rates ranging from 50% to 87%. Fortunately, postoperative delirium is preventable in up to 50% of patients, with the best preventive strategy being non-pharmacological interventions. However, these therapeutic approaches often face scalability challenges due to the complexity and high variability of their delivery, low patient engagement, and the existing clinical workforce constraints in the hospital setting. Cognitive stimulation is a non-pharmacological intervention with the potential to overcome the scalability and sustainability challenges of other non-pharmacological approaches, but evidence supporting its use is limited, especially in older adults at high risk for delirium. This narrative literature review examines evidence-based cognitive stimulation techniques being used as a non-pharmacological approach to prevent delirium in hospital settings.
Keywords:
delirium
; cognitive stimulation
; cognitive training
; cognitive rehabilitation
; cognitive prehabilitation
; geriatric
; prevention
Introduction
Delirium is an acute brain dysfunction affecting more than 11 million hospitalized older adults with an estimated annual cost of $150 billion.[1] These older adults have a higher risk of all-cause mortality (odds ratio ~ 4), stay an additional 2-4 days in the hospital, and are two times more likely to develop or experience worsening Alzheimer’s Disease and Related Dementias (ADRDs).[2,3,4,5,6,7] Delirium is the most common complication after major surgeries, with incidence rates ranging from 50% to 87%.[4,5,8] Delirium emerges from a complex interaction among predisposing vulnerability risk factors, such as prior cognitive impairment, and acute insults, such as undergoing major surgery.[9,10,11] Fortunately, postoperative delirium is preventable in up to 50% of patients, with the best preventive strategy being non-pharmacological interventions.[12,13,14,15] However, these therapeutic approaches often face scalability challenges due to the complexity and high variability of their delivery, low patient engagement, and the existing clinical workforce constraints in the hospital setting.[16,17]
Cognitive stimulation is a non-pharmacological intervention with the potential to overcome the scalability and sustainability challenges of other non-pharmacological approaches, but evidence supporting its use is limited, especially in older adults at high risk for delirium. Cognitive stimulation encompasses a variety of activities aimed at enhancing cognitive functions, including attention, memory, and executive function.[14,18] The rationale for utilizing cognitive stimulation as a preventive measure for delirium is based on several mechanisms. Cognitive stimulation helps build cognitive reserve, promotes neuroplasticity, enhances sensory engagement, and fosters social interaction.[19,20,21] Strategies for delivering cognitive stimulation includes traditional reality orientation[22,23] and workbooks[24] to brain-training applications and online games.[25,26] However, implementing cognitive stimulation in acute hospital settings faces several challenges, including limited resources, staffing issues, and a lack of training among nursing staff.[27] Additionally, conventional delivery of cognitive stimulation can often become repetitive, leading to decreased motivation and participant disengagement.[28] Incorporating games into cognitive stimulation therapy and using virtual reality (VR) to deliver such cognitive games has been shown to enhance cognitive functions[14,18] and increase participant engagement.[29,30,31,32,33,34] Thus, VR delivery of cognitive stimulation games is emerging as a potential solution to enhance patient engagement and overcome the scalability issues of the current delirium prevention approaches.
This narrative literature review examines evidence-based cognitive stimulation techniques being used as a non-pharmacological approach to prevent delirium in hospital settings. Of note is that the present review focuses on research published in the last 10 years. This review builds on prior important literature[35,36] by concentrating specifically on cognitive stimulation as a non-pharmacological intervention for preventing delirium.
Methods
We undertook a narrative literature review of peer-reviewed articles from January 2014 to September 2024 to identify and critically analyze research on cognitive stimulation (CS) as a non-pharmacological therapy for preventing or managing delirium. The methodology for this review conformed to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines (Figure 1). [37] The population of interest included adults > 18 years old who were admitted to the hospital and had cognitive stimulation as a part of CS exercise, cognitive pre-rehabilitation, or rehabilitation. We defined cognitive stimulation as any therapies or strategies directed at improving patient cognition or the domains of cognition. Examples of interventions included repeated tasks, games, skills, or questions, such as orientation exercises in both writing and/or verbal exercises delivered by health care professionals, family, computer software, or virtual reality. We sought to find studies comparing patients who received the intervention and those who did not and reported on our primary outcome of interest—delirium. The present narrative review included original research articles such as randomized-controlled trials (RCT), quasi-experimental trials (i.e., non-RCT), observational trials, and pre/post-intervention trials describing the application of cognitive stimulation in the hospital setting and reporting of delirium according to validated tools such as the CAM-ICU. [38] English-language publications were chosen to study adults in hospital settings.
Exclusion Criteria
The exclusion criteria were as follows: editorial, commentaries, abstracts, review articles, case reports, and letters with duplicate, incomplete, and unavailable data; participants with severe cognitive impairment and a history of severe sensory or motor impairment. For patients with terminal illnesses or a life expectancy of less than 6 months, where postoperative outcomes may be heavily influenced by factors other than the intervention being studied, pharmacological interventions for the prevention or treatment of delirium were excluded. Non-English articles were excluded. Articles focusing only on cognitive stimulations following hospital discharge (i.e., outpatients) were excluded as we sought to assess interventions applied in hospital settings.
Search Strategy
H.F. developed search strategies and reviewed them with a health sciences librarian. The search was conducted using PubMed (n=42), Scopus (n=40), and Web of Science (n=42) databases. Medical subject heading (MeSH) terms and keywords were used, including three key concepts: “Postoperative Delirium,” “Cognitive Stimulation,” and “Delirium in Older Adults.” Limitations included English-language articles. The initial search was conducted by the senior investigator (H.F.). Search results were managed using Covidence [39] and EndNote X9 software.
Screening Methods and Data Extraction
Three reviewers (E.F. and N.D.) manually screened duplicate titles and abstracts for predetermined inclusion and exclusion criteria. Titles and abstracts lacking sufficient information for inclusion were reviewed in full-text form. A librarian (A.T.) resolved disagreements. Articles were chosen for full-text review after assessment of inclusion criteria for the study population, study comparison, and study outcomes. Subsequently, two investigators (H.F. and I.H.) independently reviewed full-text articles for final data extraction and analysis.
Data Synthesis
The findings were presented in a narrative format. We performed a narrative literature review due to the heterogeneity of interventions, outcomes, and study designs.
Results
Figure 1 depicts the PRISMA flow diagram. The search identified 124 articles. After an initial review of the titles and research origin, 70 duplicate articles were eliminated, leaving 54 articles for further consideration. After the title and abstract review, nine articles were removed for failure to meet inclusion criteria, leaving 43 publications for full-text review. After the full-text screening, 28 articles met the inclusion criteria. All 28 articles were reviewed using the standard extraction form, including the study sample, research methodology, research outcomes, and clinical implications, if available. Our literature search yielded twelve articles for in-depth analysis (Table 1).
Healthcare Professional-Led Cognitive Stimulation
We identified 8 studies ranging from feasibility studies to pre-and post-intervention studies to randomized clinical trials in which healthcare professionals delivered cognitive stimulation, including nurses, occupational therapists, and physical therapists. There were wide variations in the type of outcome reported about delirium (e.g., incidence, duration, density, delirium-free days). A randomized clinical trial (RCT) by Chen et al.[40] evaluated RAM-based cognitive stimulation therapy (CST) in 280 older postoperative patients with non-small cell lung cancer. Delirium screening was performed using the Nursing Delirium Screening Scale.[41] The study found that the incidence of postoperative delirium was significantly lower in the CST group (10.71%) compared to the control group (20.71%). Faustino et al.[42] conducted an RCT with 144 critically ill patients to assess non-pharmacological interventions, including reorientation, cognitive stimulation, sensory correction, environmental management, and sleep promotion. Delirium incidence density was measured using the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) tool.[38] The experimental group had a significantly lower incidence of delirium (1.3 × 10^−2 person-days) compared to the control group (2.3 × 10^−2 person-days), with a hazard ratio of 0.40 (95% CI: 0.17–0.95; P = 0.04). Felipe Martinez et al.[43] studied the impact of tailored interventions, including early mobilization, physical therapy, cognitive stimulation, and family involvement, on 227 adult ICU patients. Delirium was measured using the CAM-ICU tool.[38] The study found a significant reduction in delirium incidence, decreasing from 38% to 24%, with a relative risk of 0.62 (P = 0.02). Mudge et al.[44] examined the impact of a structured early rehabilitation program, including early physiotherapy, an individualized exercise program, nursing support for functional independence, and cognitive stimulation activities on 124 patients aged 65 and older. Delirium was identified according to chart review using validated methodology.[45] The author reported that the intervention group experienced a lower incidence of delirium than the control group (19.4% vs. 35.5%, P = 0.04). Álvarez et al.[46] conducted an RCT of 140 elderly ICU patients. Delirium screening was performed using the CAM-ICU.[38] The study results showed a reduced incidence of delirium (20% in the control group vs. 3% in the experimental group) after implementing an occupational therapy-led cognitive intervention protocol that included stimulation, rehabilitation, and training exercises (P = 0.001). Rivosecchi et al.[47] evaluated cognitive stimulation as part of a non-pharmacological delirium prevention bundle that included nursing education, music, reorientation, and sensory care per Pain, agitation, and delirium management guidelines.[48] Intensive Care Delirium Screening Checklist (ICDSC)[49] was utilized to screen delirium. The author and colleagues studied 230 patients in the pre-implementation phase and 253 in the post-implementation phase, reporting a decrease in delirium incidence from 15.7% in Phase I to 9.4% in Phase II (P = 0.04). Colombo et al.[50] reported a significant reduction in delirium occurrence, measured using CAM. [38] The study results showed delirium occurrence decreased from 36% in Phase I to 22% in Phase II following the introduction of a cognitive simulation protocol that included orientation, environmental, acoustic, and visual interventions (P = 0.020). This was controlled for dementia, APACHE II score, and mechanical ventilation. Şanlıtürk et al.[51] evaluated a two-stage intervention involving sensory stimulation and sleep hygiene in a pretest-posttest control trial with 92 COVID-19 ICU patients. Screening of delirium was performed using the CAM ICU tool.[38] They found a significant reduction in delirium, with 56% of the experimental group affected compared to 80% in the control group (P < 0.05).
Family Led Cognitive Stimulations
We found two studies in which a family member delivered cognitive stimulation. Mitchell et al.[52] conducted a single-center randomized controlled trial with 90 patients, examining a family-delivered intervention that included daily orientation, sensory checks, and cognitive stimulation through discussions about family life and reminiscing. They reported the intervention as feasible and acceptable despite a low recruitment rate of 28%. Munro et al. [53] conducted a three-arm RCT of 30 patients testing a family-led intervention via voice recordings and found an increase in mean delirium-free days (evaluated by CAM-ICU)[38] in the family voice recording group (1.9 days) vs the control group (1.6 days; P = 0.04).
Software-Based Cognitive Stimulation
E.A. Alvarez et al. [54] feasibility study evaluated software, including modules for time-spatial re-orientation, cognitive stimulation, early mobilization, sensorial support use promotion, sleep hygiene, and pain management optimization. The clinical feasibility assessment showed that 83.3% of the 30 enrolled hospitalized patients (76±8 years) completed the 5-day protocol of software usage during hospitalization. Delirium was measured using the CAM-ICU tool.[38] Software use was associated with a decrease in delirium incidence of 5 of 32 (15.6%) at baseline to 2 of 30 (6.6%) after its implementation.
Virtual reality-based cognitive stimulation
Faisal et al.[55] developed a prototype VR platform, "ReCognitionVR," designed for immersive cognitive stimulation games. Initial testing included a 20-minute VR session with healthy older volunteers,[56] followed by a pilot trial with low-risk older surgical patients. [55] Preliminary findings showed that the VR games were feasible, safe, and well-accepted, with all patients completing the sessions and achieving a mean System Usability Scale (SUS) score of 92 (SD = 8) without safety concerns. Game performance was assessed through metrics like the percentage of balloons popped and completion time, but no significant differences were found between groups. Due to the small sample size, the study did not observe any differences in delirium occurrence.
Discussion
Delirium emerges from a complex interaction among predisposing vulnerability risk factors, such as prior cognitive impairment, and acute insults, such as undergoing major surgery.[9,10,11] Fortunately, delirium is preventable in up to 50% of patients, with the best preventive strategy being non-pharmacological interventions.[12,13,14,15] However, these therapeutic approaches often face scalability challenges due to the complexity and high variability of their delivery, low patient engagement, and the existing clinical workforce constraints in the hospital setting.[16,17] Cognitive stimulation is a non-pharmacological intervention with the potential to overcome the scalability and sustainability challenges of other non-pharmacological approaches, but evidence supporting its use is limited, especially in older patients at high risk for delirium. This paper reviewed cognitive stimulation therapy for the prevention and treatment of delirium. Considering the number of studies included in this paper, there is a clear need for additional research on applying cognitive stimulation therapy in the hospital setting.
We identified only ten studies that evaluated cognitive stimulation for delirium prevention but exhibited significant bias, warranting caution in their clinical application (Table 2). Healthcare professional-led cognitive stimulation demonstrated a variable reduction in delirium, as evidenced by three RCTs,[40,42,46] three pre- and post-intervention studies, [43,47,51], and one study using a chart-based identification method of delirium.[44] One study focused solely on the feasibility of implementing a prevention program and did not report on delirium-related outcomes.[50,52,53]
Family-led cognitive stimulation for hospitalized patients is under-utilized and under-reported, warranting further investigation. It presents an alternative to healthcare professional-led cognitive stimulation, which faces challenges such as limited resources, staffing issues, and insufficient training among nursing staff.[27] Feasibility studies on family-led cognitive stimulation included in this review,[52,53] while not sufficiently powered to assess delirium outcomes, can aid in developing protocols for future randomized controlled trials. For instance, Mitchell et al. provided a sample size estimate of 596 for achieving 80% power at a significance level of (P = 0.05).[52]
Conventional strategies used for cognitive stimulation in the ambulatory setting range from traditional reality orientation[22,23] and workbooks[24] to brain-training applications and online games.[25,26] Healthcare professionals and family-led conventional cognitive stimulation can often become repetitive, decreasing motivation and participant disengagement.[28] Incorporating games into cognitive stimulation therapy and using virtual reality (VR) to deliver such cognitive games has been shown to enhance cognitive functions[14,18] and increase participant engagement.[29,30,31,32,33,34] Thus, VR delivery of cognitive stimulation games is emerging as a potential solution to enhance patient engagement and overcome the scalability issues of the current delirium prevention approaches. This review identified one study on software-based cognitive stimulation and two studies on VR-based cognitive stimulation, all exhibiting small sample sizes and a high risk of bias. Consequently, the efficacy of these interventions for delirium prevention and management remains inconclusive. In a feasibility study by Alvarez et al.,[54] software-based re-orientation and cognitive stimulation correlated with a reduction in delirium incidence from 15.6% (5 of 32) at baseline to 6.6% (2 of 30) post-implementation. Faisal et al.[55] assessed VR-based cognitive stimulation games for older surgical patients, finding them safe, feasible, and acceptable, though delirium outcomes were not reported.
Limitations
This narrative review has several limitations. Firstly, it focused exclusively on peer-reviewed literature published in English, potentially omitting relevant studies in other languages and unpublished work. Secondly, it excluded other reviews, case reports, and commentaries. Thirdly, the included studies were assessed to have a critical, serious, or high risk of bias, which restricts the ability to draw definitive conclusions regarding the effects of cognitive stimulation. Fourthly, most of the studies were pilot or feasibility studies, making it premature to determine their impact on delirium outcomes. Lastly, the review may be constrained by the specific databases searched, with potentially relevant studies not indexed in these sources.
Conclusion
Cognitive stimulation for delirium prevention in a hospital setting is a relatively new area of research and warrants further exploration. In addition, implementing cognitive stimulation in hospital settings faces several challenges. VR delivery of cognitive stimulation games is emerging as a potential solution to enhance patient engagement and overcome the scalability issues of the current delirium prevention approaches. However, insufficient evidence is available supporting its use. In turn, the authors are conducting a study to evaluate VR-based cognitive stimulation games to prevent delirium in older adults in the hospital setting. Larger, multi-center trials to evaluate VR-based cognitive intervention protocols are needed to examine the effects on delirium outcomes in a hospital setting.
Funding Disclosures
All authors have no financial disclosures or any conflict of interest.
Author Contributions
Emman Fatima (E.F.), Ian Hill (I.H.), Noah Dover (N.D.), and Hina Faisal (H.F.) contributed to all aspects of the manuscript, including study conception, design, acquisition, analysis, and interpretation of data, drafting the article. In addition, H.F. contributed to editing, revising, and writing an article's final draft.
Funding
None.
Acknowledgments
We thank Amy Taylor, MLS, AHIP, Medical librarian at Houston Methodist Education Institute, Houston Methodist Hospital, for her guidance in research strategy, pulling articles from databases, and transferring them to Covidence.
References
- Leslie, D.L.; Marcantonio, E.R.; Zhang, Y.; Leo-Summers, L.; Inouye, S.K. One-Year Health Care Costs Associated With Delirium in the Elderly Population. Arch. Intern. Med. 2008, 168, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Goldberg TE, Chen C, Wang Y, et al. Association of Delirium With Long-term Cognitive Decline: A Meta-analysis. JAMA Neurology 2020, 77, 1373–81. [Google Scholar] [CrossRef] [PubMed]
- Witlox, J.; Eurelings, L.S.M.; de Jonghe, J.F.M.; Kalisvaart, K.J.; Eikelenboom, P.; van Gool, W.A. Delirium in Elderly Patients and the Risk of Postdischarge Mortality, Institutionalization, and Dementia. JAMA 2010, 304, 443–451. [Google Scholar] [CrossRef]
- Khan, B.A.; Perkins, A.J.; Gao, S.; Hui, S.L.; Campbell, N.L.; Farber, M.O.; Chlan, L.L.; Boustani, M.A. The Confusion Assessment Method for the ICU-7 Delirium Severity Scale: A Novel Delirium Severity Instrument for Use in the ICU. Crit. Care Med. 2017, 45, 851–857. [Google Scholar] [CrossRef]
- Collaborative GMR. Delirium is prevalent in older hospital inpatients and associated with adverse outcomes: results of a prospective multi-centre study on World Delirium Awareness Day. BMC Medicine 2019;17:229.
- Thein, M.Z.A.; Pereira, J.V.; Nitchingham, A.; Caplan, G.A. A call to action for delirium research: Meta-analysis and regression of delirium associated mortality. BMC Geriatr. 2020, 20, 325. [Google Scholar] [CrossRef]
- Alzheimer's disease facts and figures. Alzheimers Dement 2024;20:3708-821.
- Popp, J.; Kukreja, D.; Günther, U. Delirium in the elderly: Current problems with increasing geriatric age. Indian J. Med Res. 2015, 142, 655–661. [Google Scholar] [CrossRef] [PubMed]
- Kwak, MJ. Delirium in Frail Older Adults. Ann Geriatr Med Res 2021;25:150-9.
- Al Farsi, R.S.; Al Alawi, A.M.; Al Huraizi, A.R.; Al-Saadi, T.; Al-Hamadani, N.; Al Zeedy, K.; Al-Maqbali, J.S. Delirium in Medically Hospitalized Patients: Prevalence, Recognition and Risk Factors: A Prospective Cohort Study. J. Clin. Med. 2023, 12, 3897. [Google Scholar] [CrossRef]
- Wang, X.; Yu, D.; Du, Y.; Geng, J. Risk factors of delirium after gastrointestinal surgery: A meta-analysis. J. Clin. Nurs. 2023, 32, 3266–3276. [Google Scholar] [CrossRef]
- Hshieh TT, Yue J, Oh E, et al. Effectiveness of multicomponent nonpharmacological delirium interventions: a meta-analysis. JAMA Intern Med 2015;175:512-20.
- Marra, A.; Ely, E.W.; Pandharipande, P.P.; Patel, M.B. The ABCDEF Bundle in Critical Care. Crit. Care Clin. 2017, 33, 225–243. [Google Scholar] [CrossRef]
- Tobar, E.; Alvarez, E.; Garrido, M. Cognitive stimulation and occupational therapy for delirium prevention. Rev. Bras. de Ter. Intensiv. 2017, 29, 248–252. [Google Scholar] [CrossRef]
- Hshieh, T.T.; Yang, T.; Gartaganis, S.L.; Yue, J.; Inouye, S.K. Hospital Elder Life Program: Systematic Review and Meta-analysis of Effectiveness. Am. J. Geriatr. Psychiatry 2018, 26, 1015–1033. [Google Scholar] [CrossRef]
- Costa DK, White MR, Ginier E, et al. Identifying Barriers to Delivering the Awakening and Breathing Coordination, Delirium, and Early Exercise/Mobility Bundle to Minimize Adverse Outcomes for Mechanically Ventilated Patients: A Systematic Review. Chest 2017;152:304-11.
- Morandi, A.; Piva, S.; Ely, E.W.; Myatra, S.N.M.; Salluh, J.I.; Amare, D.; Azoulay, E.; Bellelli, G.; Csomos, A.; Fan, E.; et al. Worldwide Survey of the “Assessing Pain, Both Spontaneous Awakening and Breathing Trials, Choice of Drugs, Delirium Monitoring/Management, Early Exercise/Mobility, and Family Empowerment” (ABCDEF) Bundle. Crit. Care Med. 2017, 45, e1111–e1122. [Google Scholar] [CrossRef]
- Gibbor, L.; Yates, L.; Volkmer, A.; Spector, A. Cognitive stimulation therapy (CST) for dementia: a systematic review of qualitative research. Aging Ment. Heal. 2021, 25, 980–990. [Google Scholar] [CrossRef]
- Woods, B.; Rai, H.K.; Elliott, E.; Aguirre, E.; Orrell, M.; Spector, A. Cognitive stimulation to improve cognitive functioning in people with dementia. Cochrane Database Syst. Rev. 2023, 2023. [Google Scholar] [CrossRef]
- Park, D.C.; Bischof, G.N.; Dc, P. The aging mind: neuroplasticity in response to cognitive training. Dialog- Clin. Neurosci. 2013, 15, 109–119. [Google Scholar] [CrossRef]
- Stern, Y. How Can Cognitive Reserve Promote Cognitive and Neurobehavioral Health? Archives of Clinical Neuropsychology 2021;36:1291-5.
- Spector A, Davies S, Woods B, Orrell M. Reality orientation for dementia: a systematic review of the evidence of effectiveness from randomized controlled trials. Gerontologist 2000;40:206-12.
- Taulbee, L.R.; Folsom, J.C. Reality Orientation for Geriatric Patients. Psychiatr. Serv. 1966, 17, 133–135. [Google Scholar] [CrossRef]
- Orrell, M.; Yates, L.; Leung, P.; Kang, S.; Hoare, Z.; Whitaker, C.; Burns, A.; Knapp, M.; Leroi, I.; Moniz-Cook, E.; et al. The impact of individual Cognitive Stimulation Therapy (iCST) on cognition, quality of life, caregiver health, and family relationships in dementia: A randomised controlled trial. PLOS Med. 2017, 14, e1002269. [Google Scholar] [CrossRef]
- Al-Thaqib, A.; Al-Sultan, F.; Al-Zahrani, A.; Al-Kahtani, F.; Al-Regaiey, K.; Iqbal, M.; Bashir, S. Brain Training Games Enhance Cognitive Function in Healthy Subjects. Med Sci. Monit. Basic Res. 2018, 24, 63–69. [Google Scholar] [CrossRef]
- Tapia, J.L.; Puertas, F.J.; Duñabeitia, J.A. Digital Therapeutics for Insomnia: Assessing the Effectiveness of a Computerized Home-Based Cognitive Stimulation Program. J. Integr. Neurosci. 2023, 22, 34. [Google Scholar] [CrossRef]
- Parker, A.M.; Aldabain, L.; Akhlaghi, N.; Glover, M.; Yost, S.; Velaetis, M.; Lavezza, A.; Mantheiy, E.; Albert, K.; Needham, D.M. Cognitive Stimulation in an Intensive Care Unit: A Qualitative Evaluation of Barriers to and Facilitators of Implementation. Crit. Care Nurse 2021, 41, 51–60. [Google Scholar] [CrossRef]
- Kallio, E.-L.; Öhman, H.; Kautiainen, H.; Hietanen, M.; Pitkälä, K. Cognitive Training Interventions for Patients with Alzheimer’s Disease: A Systematic Review. J. Alzheimer's Dis. 2017, 56, 1349–1372. [Google Scholar] [CrossRef]
- Barnes DE, Yaffe K, Belfor N, et al. Computer-based cognitive training for mild cognitive impairment: results from a pilot randomized, controlled trial. Alzheimer Dis Assoc Disord 2009;23:205-10.
- Brugada-Ramentol, V.; Bozorgzadeh, A.; Jalali, H. Enhance VR: A Multisensory Approach to Cognitive Training and Monitoring. Front. Digit. Heal. 2022, 4, 916052. [Google Scholar] [CrossRef]
- Green, C.S.; Bavelier, D. Action video game modifies visual selective attention. Nature 2003, 423, 534–537. [Google Scholar] [CrossRef]
- Lee, H.K.; Kent, J.D.; Wendel, C.; Wolinsky, F.D.; Foster, E.D.; Merzenich, M.M.; Voss, M.W. Home-Based, Adaptive Cognitive Training for Cognitively Normal Older adults: Initial Efficacy Trial. Journals Gerontol. Ser. B 2020, 75, 1144–1154. [Google Scholar] [CrossRef]
- Lumsden, J.; A Edwards, E.; Lawrence, N.S.; Coyle, D.; Munafò, M.R. Gamification of Cognitive Assessment and Cognitive Training: A Systematic Review of Applications and Efficacy. JMIR Serious Games 2016, 4, e11. [Google Scholar] [CrossRef]
- Man, D.W.K.; Poon, W.S.; Lam, C. The effectiveness of artificial intelligent 3-D virtual reality vocational problem-solving training in enhancing employment opportunities for people with traumatic brain injury. Brain Inj. 2013, 27, 1016–1025. [Google Scholar] [CrossRef]
- Deemer, K.; Zjadewicz, K.; Fiest, K.; Oviatt, S.; Parsons, M.; Myhre, B.; Posadas-Calleja, J. Effect of early cognitive interventions on delirium in critically ill patients: a systematic review. Can. J. Anaesth. 2020, 67, 1016–1034. [Google Scholar] [CrossRef]
- Johnson, G.U.; Towell-Barnard, A.; McLean, C.; Ewens, B. Delirium prevention and management in an adult intensive care unit through evidence-based nonpharmacological interventions: A scoping review. Collegian 2024, 31, 232–251. [Google Scholar] [CrossRef]
- Liberati A, Altman DG, Tetzlaff J, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol 2009;62:e1-34.
- Miranda F, Gonzalez F, Plana MN, Zamora J, Quinn TJ, Seron P. Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) for the diagnosis of delirium in adults in critical care settings. Cochrane Database Syst Rev 2023;11:Cd013126.
- Covidence systematic review software, Veritas Health Innovation, Melbourne, Australia. Available at www.covidence.org.
- Chen, C.-Y.; Ding, H.; Wang, S.-S. Effectiveness of Roy Adaptation Model-Based Cognitive Stimulation Therapy in Elderly Patients with Non-Small Cell Lung Cancer Undergoing Curative Resection. Tohoku J. Exp. Med. 2024, 263, 27–34. [Google Scholar] [CrossRef]
- Gaudreau, J.-D.; Gagnon, P.; Harel, F.; Roy, M.-A. Impact on delirium detection of using a sensitive instrument integrated into clinical practice. Gen. Hosp. Psychiatry 2005, 27, 194–199. [Google Scholar] [CrossRef]
- Faustino, T.N.; Suzart, N.A.; Rabelo, R.N.d.S.; Santos, J.L.; Batista, G.S.; de Freitas, Y.S.; Saback, D.A.; Sales, N.M.M.D.; Barreto, B.B.; Gusmao-Flores, D. Effectiveness of combined non-pharmacological interventions in the prevention of delirium in critically ill patients: A randomized clinical trial. J. Crit. Care 2022, 68, 114–120. [Google Scholar] [CrossRef]
- Martínez, F.; Donoso, A.M.; Marquez, C.; Labarca, E. Implementing a Multicomponent Intervention to Prevent Delirium Among Critically Ill Patients. Crit. Care Nurse 2017, 37, 36–46. [Google Scholar] [CrossRef]
- Mudge, A.M.; Giebel, A.J.; Cutler, A.J. Exercising Body and Mind: An Integrated Approach to Functional Independence in Hospitalized Older People. J. Am. Geriatr. Soc. 2008, 56, 630–635. [Google Scholar] [CrossRef]
- Inouye, S.K.; Leo-Summers, L.; Zhang, Y.; Bogardus, S.T.; Leslie, D.L.; Agostini, J.V. A Chart-Based Method for Identification of Delirium: Validation Compared with Interviewer Ratings Using the Confusion Assessment Method. J. Am. Geriatr. Soc. 2005, 53, 312–318. [Google Scholar] [CrossRef]
- Álvarez, E.A.; Garrido, M.A.; Tobar, E.A.; Prieto, S.A.; Vergara, S.O.; Briceño, C.D.; González, F.J. Occupational therapy for delirium management in elderly patients without mechanical ventilation in an intensive care unit: A pilot randomized clinical trial. J. Crit. Care 2017, 37, 85–90. [Google Scholar] [CrossRef]
- Rivosecchi, R.M.; Kane-Gill, S.L.; Svec, S.; Campbell, S.; Smithburger, P.L. The implementation of a nonpharmacologic protocol to prevent intensive care delirium. J. Crit. Care 2016, 31, 206–211. [Google Scholar] [CrossRef]
- Barr, J.; Fraser, G.L.; Puntillo, K.; Ely, E.W.; Gélinas, C.; Dasta, J.F.; Davidson, J.E.; Devlin, J.W.; Kress, J.P.; Joffe, A.M.; et al. Clinical Practice Guidelines for the Management of Pain, Agitation, and Delirium in Adult Patients in the Intensive Care Unit. Crit. Care Med. 2013, 41, 263–306. [Google Scholar] [CrossRef]
- Bergeron, N.; Dubois, M.-J.; Dumont, M.; Dial, S.; Skrobik, Y. Intensive Care Delirium Screening Checklist: evaluation of a new screening tool. Intensiv. Care Med. 2001, 27, 859–864. [Google Scholar] [CrossRef]
- Colombo, R.; Corona, A.; Praga, F.; Minari, C.; Giannotti, C.; Castelli, A.; Raimondi, F. A reorientation strategy for reducing delirium in the critically ill. Results of an interventional study.. 2012, 78, 1026–1033. [Google Scholar]
- Şanlıtürk, D.; Kaplan, V.; Dörtkardeş, N. Preventive Effect of Cognitive Stimulation and Sleep Hygiene on Delirium in COVID-19 Intensive Care Patients. J. Turk. Sleep Med. 2023, 10, 206–215. [Google Scholar] [CrossRef]
- Mitchell, M.L.; Kean, S.; Rattray, J.E.; Hull, A.M.; Davis, C.; Murfield, J.E.; Aitken, L.M. A family intervention to reduce delirium in hospitalised ICU patients: A feasibility randomised controlled trial. Intensiv. Crit. Care Nurs. 2017, 40, 77–84. [Google Scholar] [CrossRef] [PubMed]
- Munro, C.L.; Cairns, P.; Ji, M.; Calero, K.; Anderson, W.M.; Liang, Z. Delirium prevention in critically ill adults through an automated reorientation intervention – A pilot randomized controlled trial. Hear. Lung 2017, 46, 234–238. [Google Scholar] [CrossRef] [PubMed]
- A Alvarez, E.; Garrido, M.; Ponce, D.P.; Pizarro, G.; A Córdova, A.; Vera, F.; Ruiz, R.; Fernández, R.; Velásquez, J.D.; Tobar, E.; et al. A software to prevent delirium in hospitalised older adults: development and feasibility assessment. Age and Ageing 2020, 49, 239–245. [Google Scholar] [CrossRef]
- Faisal, H.; Masud, F.N.; Junhyoung, K.; Podell, K.; Xu, J.; Boncyk, C.; Taffet, G.E.; Boustani, M.A. Virtual reality-based cognitive exercise games in geriatric surgical patients: A pilot trial. J. Am. Geriatr. Soc. 2024. [Google Scholar] [CrossRef]
- Faisal, H.; Lim, W.; Dattagupta, A.; Lin, P.; Gupta, R.; Lai, E.C.; Xu, J.; Wong, S.T.; Masud, F.N. Usability and Tolerability of Virtual Reality-Based Cognitive Stimulation in Healthy Elderly Volunteers—A Feasibility Clinical Trial. Games Heal. J. 2024. [Google Scholar] [CrossRef]
Figure 1.
PRISMA flowchart of study selection.
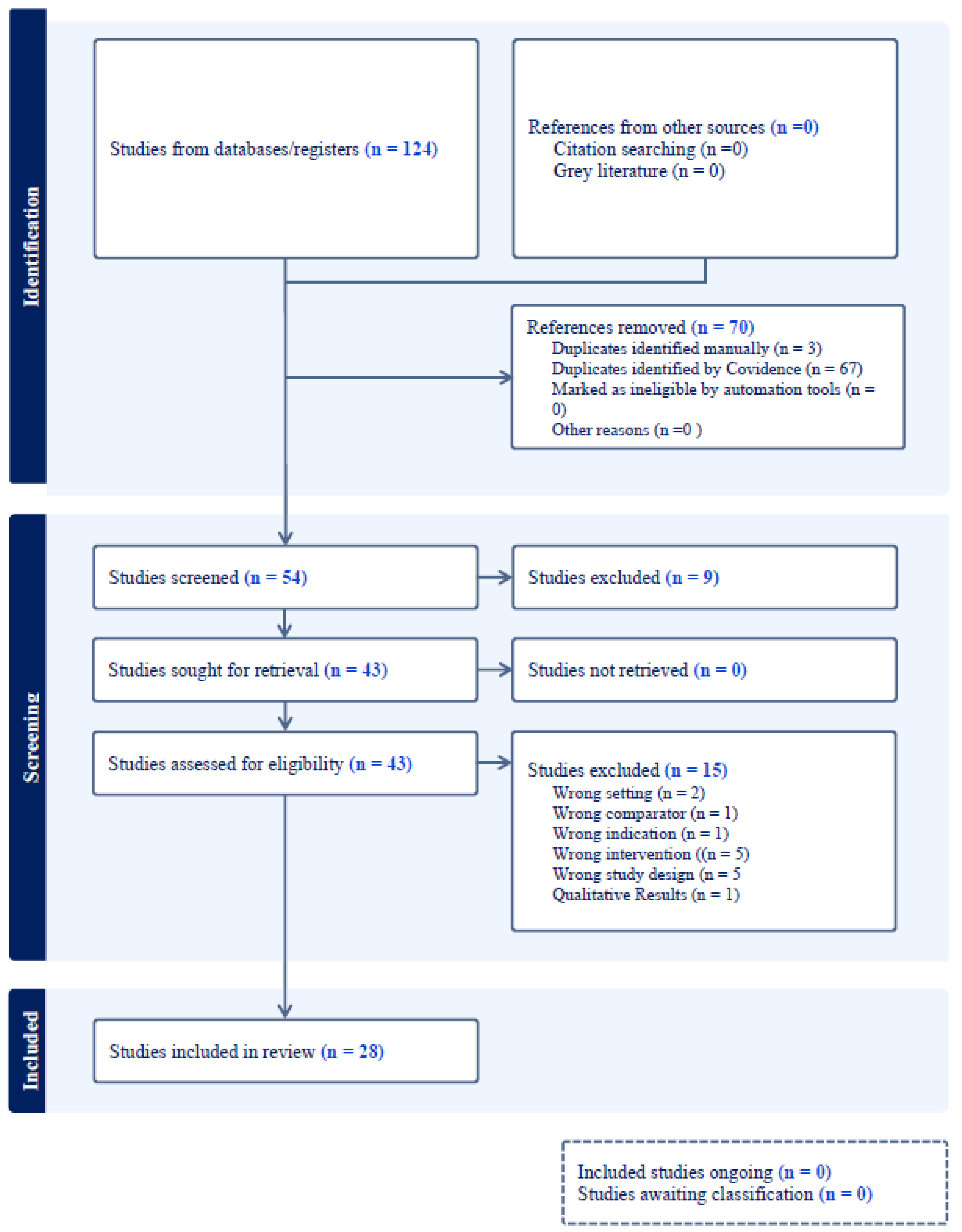

Table 1.
Study Summary.
| Study | Purpose/intervention | Design, age, sample size | Outcomes and outcome measures | Results | Conclusion |
|---|---|---|---|---|---|
| Healthcare Professional-led cognitive stimulation | |||||
|
Chen et al. (2024) [40] |
To investigate the effects of a Royal Adaptation Model (RAM)-based cognitive stimulation therapy (CST) on older patients with primary non-small cell lung cancer (NSCLC) undergoing curative resection | Single-center Randomized controlled trial (RCT) Age > 65 years n=280 |
Delirium prevalence/incidence using the Nursing Delirium Screening Scale. [41] |
Incidence of delirium: 20.71 % in the control group Vs. 10.71% in the RAM-based CST group (P=0.032) | RAM-based CST in elderly NSCLC patients undergoing curative resection yielded reduced delirium incidence. |
| Faustino et al. (2022) [42] |
To evaluate the effectiveness of combined non-pharmacological interventions (periodic reorientation, cognitive stimulation, correction of sensory deficits) in preventing delirium in critically ill patients | Single-center RCT Age >18 years n= 144 |
Delirium incidence density using the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) tool. [38] | Incidence density of delirium: (2.3 × 10−2 person-days) in control group Vs. (1.3 × 10−2 person-days) in the intervention group. | Combined non-pharmacological interventions reduced delirium in critically ill patients compared to standard care. |
| Martinez et al. (2017) [43] |
To assess the effectiveness of a tailored multicomponent intervention (early mobilization for preventing the incidence of delirium among critically ill patients. | A before-and-after study Age> 18 years n=227 |
Delirium incidence using CAM-ICU tool. [38] | Incidence of delirium: Reduced from 38% to 24% (relative risk, 0.62; 95% CI, 0.40-0.94; P = .02) | Multicomponent strategy successfully reduced delirium. Early participation of the whole team, shared leadership, and the provision of concrete tasks were key to the intervention's success. |
| Mudge et al. (2008) [44] | To evaluate the effect of a structured, multi-component, early rehabilitation program on delirium of older acute medical inpatients. |
Prospective controlled trial Age ≥ 65 years n=124 |
Incidence of delirium. Delirium was identified according to chart review using validated methodology. [45] | Incidence of delirium: 35.5% in control group Vs. 19.4% in the intervention group (P=0.19) | In the intervention group, there was a reduction in delirium. |
| Alvarez et al. (2017) [46] |
To determine the impact of occupational therapy (OT) -led cognitive intervention protocol on the incidence, duration, and severity of delirium in older ICU patients | Pilot study, RCT Age>60 years n=140 |
Delirium incidence and duration using the CAM ICU tool.[38] | Incidence of delirium: 20% in the control group Vs 3 % in the treatment group (P=0.01) Duration of delirium: lower in the treatment group (IRR, 0.15; 95% CI, 0.12 to 0.19; P<0.001): Control group (IRR, 6.7; 95% CI, 5.2 to 8.3; P<0.001). |
A combination of early OT and cognitive intervention strategies decreases the incidence and duration of delirium. |
| Rivosecchi et al. (2016) [47] |
To assess whether an evidence-based non-pharmacologic protocol could further decrease the duration of delirium in patients in a medical ICU that already implements a sedation and mobility protocol. [47] | Prospective, pre-post intervention QI project. (n=483). Phase I: baseline data collection before protocol implementation (n=230). Phase II: development and implementation of non-pharmacologic protocol |
Incidence and duration of delirium in phase 1 vs 2, using the Intensive Care Delirium Screening Checklist (ICDSC). [49] |
Phase I Vs. Phase II delirium incidence (15.7% Vs. 9.4%; P=0.04). Median duration of delirium in Phase I (20 hours) and Phase II (16 hours), (50.6% reduction; P<0.001) |
Nonpharmacologic strategies reduce risk and duration of delirium in the ICU, even if a mobilization protocol and sedation algorithm are already in place. |
| Colombo et al. (2012)50 | To assess the efficacy of the cognitive stimulation protocol (orientation, environmental, acoustic, and visual interventions) on delirium in medical and surgical ICU patients | Two-stage prospective- observational study. Age > 18 years Phase 1: observational (n=170) phase II interventional (n=144) |
Delirium occurrence using the CAM-ICU tool.[38] |
Delirium occurrence was lower (36% in phase I vs 22% in phase II, P=0.02). |
A reorientation strategy was associated with a reduced incidence of delirium. |
| Şanlıtürk et al. (2023)51 | To evaluate the effect of two-stage intervention (sensory stimulation and sleep hygiene) on delirium in Coronavirus disease-2019 (COVID-19) patients | Pre-test/post-test control group and trial model. Age>18 years n=92 |
Delirium incidence using CAM-ICU tool.[38] | Incidence of delirium: 80% in control group Vs. 56% in the intervention group (P<0.05) |
The sensory stimulation and sleep hygiene intervention based on the nursing model effectively reduced the incidence of delirium in critically ill COVID-19 patients. |
| Family-led cognitive stimulations | |||||
| Mitchell et al. (2017) [52] | To evaluate the feasibility and acceptability of a family-delivered intervention (orientation or memory clues, sensory checks, and therapeutic or cognitive stimulation) to reduce delirium in hospitalized ICU patients. | Single-center Feasibility RCT Age ≥16 years n=61 |
Retention of family members, feasibility, and acceptability of the intervention |
No family member withdrew from the intervention group, and one withdrew from the control group. Low recruitment rate (28%) | The feasibility of recruiting and retaining family members participants; nurse supportive of interventions |
| Munro et al. (2017) [53] | To determine if recorded audio-orienting messages (automated orientation messages in a family member's voice) reduce the risk of delirium in critically ill adults. | Prospective RCT Age> 18 years n=30 |
Delirium-free days evaluated by CAM-ICU. [38] | Mean delirium-free days: 1.9 in the family voice group, 1.6unknownvogroup, and 1.6 in the control group (P =0.04) | Participants exposed to recorded voice messages from family members had more delirium-free days. |
| Software-based & Virtual-Reality (VR)-based cognitive stimulation | |||||
| E A. Alvarez et al. (2020) [54] | To determine the clinical feasibility assessment of software by older adults | Feasibility study Age> 75 years n=30 |
Delirium incidence using the CAM -ICU tool. [38] |
Software use was associated with a decrease in delirium incidence of 5 of 32 (15.6%) at baseline to 2 of 30 (6.6%) after its implementation. |
Use of software to improve the delivery of non-pharmacological interventions may prevent delirium. |
| Faisal et al. (2024) [55] | To determine VR-based cognitive stimulation games' safety, feasibility, and acceptability for preventing delirium in older surgical patients. | Pilot trial Age ≥ 60 years n=30 |
Safety, feasibility, and acceptability. Delirium incidence using the CAM tool. [38] |
ReCognitionVR-based cognitive games were safe, feasible, and mean Mean System Usability Scale (SUS) score of 92 (SD = 8) |
The study did not observe any differences in delirium occurrence due to the small sample size. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



