
Submitted:
31 October 2024
Posted:
04 November 2024
You are already at the latest version
Abstract
The present study aimed to evaluate the multivariate relationships between variables related to burnout and job stress in healthcare workers, evaluating if the relationship between these dimensions, the variables related to personal factors (age, seniority of service), and work–family balance factors (overwork related to unused vacation days, accumulated overtime hours) change when the worker is engaged in double-caregiving activities. Indeed, the twofold activities of home caregiving and caring at work might expose workers to challenging situations. To accomplish our aim, we carried out network analyses on data from 466 workers (77.90% females). Participants completed the Link Burnout Questionnaire (LBQ) and the Job Satisfaction Scale (OSI). Contrary to expectations, the variables related to work–life balance played a marginal role with respect to job satisfaction and burnout risk for the whole sample. In addition, no significant differences emerged between workers who reported dual- caregiving tasks, compared with those who did not. However, some peculiar aspects of the relationship between burnout and job satisfaction emerged in the two subsamples. The findings are discussed, highlighting a framework for understanding the interactions among the assessed variables.
Keywords:
double-duty caregiving
; burnout
; fulfilment
; job satisfaction
; work–life balance
; JD-R theory
; occupational health
; healthcare professionals
; network analysis
1. Introduction
1.1. Double Caregiving and Work–Life Balance in Healthcare
The concept of double caregiving [1,2] refers to how informal caregiving, combined with formal work in healthcare settings, can deteriorate caregivers’ mental and physical health, increasing stress, presenteeism, emotional exhaustion, and worsening job satisfaction and performance. Some studies [3,4,5,6] suggest that the risk of burnout in caregivers increases when they have to manage multiple roles and work–family conflict is prevalent, potentially increasing detachment and disengaged work-related behaviors instead of actually leaving their job (so-called “quiet quitting” [7]). These effects, including the risk of actually quitting the job, also occur in caregivers who benefit in terms of job satisfaction and personal well-being from work–life balance [5]. Furthermore, Gérain and Zech [6] found that informal caregivers experience higher levels of burnout than non-caregivers, especially in terms of emotional exhaustion. In particular, women with combined caregiving roles, older caregivers, and those engaged in triple caregiving have reported lower psychosocial well-being than those without family caregiving duties. Double caregivers have also been characterized by higher stress, greater family–work conflict, increased perceived stress and psychological distress, and overall worse psychosocial functioning [8]. Caregivers caring for children (with and without special needs) and individuals with chronic disabilities have shown a particularly high risk of burnout, increased family–work conflict, and a lower relationship quality with partners [6,8]. In healthcare workers, prolonged work–life imbalance contributes to burnout and dissatisfaction with work–life integration [9]. Conversely, a positive work–life balance is a predictor of reduced levels of burnout plus improved mental health and well-being [10,11,12,13].
During the Covid-19 pandemic, the phenomenon of burnout among double caregivers was further amplified. Parmar et al. [14] documented how double-shift caregivers, who were already balancing work and informal care, experienced a worsening of their condition during the pandemic. Emotional and physical overload increased significantly, and most caregivers reported a decline in their mental health and higher levels of anxiety. These results emphasize the need to recognize the crucial contribution of double caregivers and provide them with more support, especially during crises like Covid-19 [14]. Also, the conception of balance—or integration—between private life and work has changed dramatically [15]. In fact, work–life balance of health professionals was compromised with the recent pandemic, becoming an even more complex goal to define and achieve, especially for these workers who were on the frontlines of the Covid-19 emergency [16,17].
Recent studies [18] identified a positive relationship between work–life balance and job satisfaction, while others (involving nurses) focused on the impact of work–family conflict on life satisfaction [19] or on self-rated health outcomes [20]. Managing work and personal spheres can become even more challenging when one performs a job that requires care but also plays a caregiver role outside the professional field; thus, more attention from organizations is needed [2,14,21]. These ideas, among others, have been recently implemented in the Job Demands-Resources model (JD-R), wherein the multi-level complexity of occupational well-being is discussed and considered as constantly influenced by the dynamics of different aspects of people’s lives and their reciprocal interactions, always in a context of balance [22].
1.2. Burnout and Double Caregiving
According to the most widely accepted definition, burnout is a work-related syndrome that manifests through three degenerative aspects: the worker’s psychophysical exhaustion, cynical attitude towards users and colleagues (or depersonalization), and a decline in professional efficacy [23,24,25,26]. Over the last 2 decades, the concept of burnout has evolved and is now recognized as an organizational pathology that affects the entire service sector. This new perspective is based on the JD-R model, which views burnout as the result of an imbalance between job demands (e.g., pressing deadlines or inadequate work environments) and available resources (e.g., decision-making autonomy or perceived organizational support) [24,27].
In the frame of JD-R theory [28,29], job burnout is seen as the antithesis of work engagement, a state characterized by vigor (high mental energy), dedication (attribution of meaning to work), and absorption (deep concentration in work activities) [30,31,32,33,34,35,36]. Recently, the World Health Organization (WHO) included burnout in the ICD-11 as a non-medical condition [25,37], adopting the three dimensions of the model proposed by Maslach et al. [23,24,27] mentioned above.
Santinello and Negrisolo [38] and Borgogni et al. [39] proposed adding a fourth dimension to the traditional model called disillusion, already previously proposed by Edelwich and Brodsky in 1980 [35,40]. This stage of job burnout reflects the erosion of professional ideals and work-related expectations, emphasizing the importance of the meaning that work has for the individual, both socially and existentially. Disillusion is a dimension deeply embedded in the healthcare professions and deserves attention.
Regarding the factors that may influence the syndrome, recent studies focused on healthcare setting have identified, among others, a lack of support within healthcare organizations [41], job duties, skills, treatment received in the workplace, and opportunities for career advancement [42]. Research on burnout among healthcare professionals engaged in double-caregiving activities has highlighted several critical aspects that link work–life conflict and its impact on mental and physical health. Gérain and Zech [4] proposed a theoretical model for understanding informal caregiver burnout, adapting the concept of burnout, usually applied to work environments, to the context of informal caregiving and differentiating informal caregiver burnout from subjective burden, which refers to the subjective perception of care-related stress. The proposed model, which integrates the model of carer stress and burden and the JD-R model, is called the informal caregiving integrative model (ICIM), highlighting the main factors involved in caregiver burnout such as caregiver characteristics, the care setting, and the social environment [4].
Several authors have investigated the effects of the Covid-19 pandemic on the psychological health of healthcare workers. For example, it was found that burnout rates were higher among nurses during the pandemic, and that the major significant predictors were high stress levels and traumatic work experiences [43]. Moreover, Burrowes et al. [44] indicated that 59% of respondents experienced burnout weekly, and a substantial number considered leaving the profession within 5 years due to high stress and feeling undervalued. These findings reaffirm the importance of urgently intervening in organizational settings by implementing psychological support systems, mental health interventions for professionals, increased salaries, and flexible schedules [43,44,45].
1.3. Job Satisfaction in Healthcare Professionals
Job satisfaction can be defined as an experience of pleasure related to the accomplishment of something coveted [46]. Along with support from colleagues and work–life balance, job satisfaction is a key dimension of the overall well-being of healthcare professionals [47], and essential to promote so that the quality of healthcare services can also be ensured [47,48].
Several studies have investigated the relationship between job satisfaction and burnout among healthcare workers, suggesting the pivotal and protective role of organizational factors [49,50,51,52,53]. Other studies have found that job satisfaction is closely related to conflict resolution and relationships with colleagues, while salary, promotion opportunities, and interpersonal communication have emerged as significant sources of dissatisfaction [54,55,56].
Regarding the Covid-19 pandemic, a recent study that examined nurses’ burnout and job satisfaction revealed that an alarming 91.1% experienced high levels of burnout, significantly impacting their job satisfaction; it has been pointed out that demographic factors and job characteristics are crucial in influencing healthcare workers’ levels of burnout and overall job satisfaction [57]. To our knowledge, as argued thus far, there have been few studies involving the comparison of job satisfaction and the risk of burnout between those who have and those who do not have double-caregiving tasks in a healthcare context.
1.4. Study Aim
The aim of our study was to describe the multivariate relationships between burnout and job satisfaction dimensions in healthcare workers involved in double caregiving and compare them with those of health workers who did not have these tasks. In particular, we wanted to describe these dimensions in relation to personal (age, seniority of service) and work–family balance (unused vacation days, accumulated overtime hours) variables.
2. Materials and Methods
2.1. Research Design
This study was descriptive in nature and was conducted at two public hospital facilities in the province of Cagliari (Sardinia, Italy) as part of a program for the prevention of work-related stress and burnout risk of healthcare workers. Participants were recruited by a non-probabilistic sampling procedure. The data were collected between September 2023 and July 2024.
2.2. Assessment Instruments
The research protocol included two distinct sections. The first was related to the measurement of demographic variables (i.e., age, gender, informal or familiar caregiving activities) and social and professional features (i.e., organizational position, seniority of service, unused vacation days, accumulated overtime hours).
The second section included two assessment instruments standardized and validated in Italy. The Link Burnout Questionnaire (LBQ) [58] was administered to assess the workers’ job burnout and work engagement. This questionnaire is a self-assessment of 24 items evaluated with a 6-point scale (from 1 = “Never” to 6 = “Always”). The dimensions evaluated, with each bipolar and characterized by six items—three positive and three negative—were the following:
- psychophysical exhaustion–engagement (item e.g., “I feel physically exhausted by my work”, “Work makes me feel active and vital”; reliability α = 0.77);
- relational deterioration–involvement (item e.g., “I have the impression that most of my users do not follow my directions”, “I feel gratified by the relationship with my users”; α = 0.79);
- professional inefficacy–efficacy (item e.g., “I feel inadequate to deal with my users’ problems”, “At work, I seem to deal effectively with most of the problems”; α = 0.78); and
- disillusion–fulfilment (item e.g., “My expectations of this work have been frustrated”, “I still feel motivated by my professional ideals”; α = 0.85).
Job satisfaction was evaluated with a subscale of the Italian version of the Occupational Stress Indicator (OSI) [59]. This instrument is characterized by five scales:
- career satisfaction (six items; e.g., “The possibility of maturation or personal development that your job allows you”; reliability α = 0.77);
- satisfaction with the job itself (four items; e.g., “The type of work and the tasks that you are expected to perform”; α = 0.75);
- satisfaction with the setting and the organizational structure (five items; e.g., “The ways in which changes and innovations are implemented”; α = 0.81);
- satisfaction with organizational processes (four items; e.g., “The opportunity to participate in important decisions”; α = 0.76); and
- satisfaction with interpersonal relationships (three items; e.g., “Your relationships with others in the work environment”; α = 0.73).
The questions were headed by the sentence: “Rate your level of satisfaction” (evaluated with a Likert scale, from 1 = “Extremely unsatisfactory” to 6 = “Extremely satisfactory”).
2.3. Participants
A total of 466 health professionals took part in the assessment (mean age: 49.57, SD = 9.72; range: 25–67 years). Specifically, 363 (77.90%) participants were female; 103 (22.10%) were male. They reported the following organizational roles: executive physician (n = 77, 16.50%), nursing coordinator (n = 16, 3.50%), nurse (n = 199, 42.70%), obstetrician (n = 29, 6.30%), healthcare technician (n = 25, 5.40%), or socio-healthcare worker (n = 119, 25.60%). They were then divided into different occupational levels: direction (n = 12, 2.60%), coordination (n = 21, 4.70%), or subordinates (n = 432, 92.70%). The participants reported an average value of seniority service of 18.49 (SD = 11.09) years, an average value of unused vacation days of 24.52 (SD = 34.03), and an average value of accumulated overtime hours of 105.16 (SD = 172.73). A total of 202 participants (43.35%) reported that, outside of work, they performed a caregiving role (e.g., caring for relatives, elderly, children with disabilities or special health or educational needs).
2.4. Data Analysis
The descriptive features of the items and scales were inspected (mean, standard deviation, skewness, kurtosis). We applied the Pearson’s r linear coefficient of correlation between variables in order evaluate the bivariate linear relationships. Furthermore, we applied the Student’s t-test in order to explore the potential differences between the means regarding the group of workers that were/were not engaged in double-caregiving activities.
The complex relationships among variables were evaluated by the application of network analysis (NA), which can provide valuable insights into the complex interrelationships among psychological variables, individual features, and organizational specificities [60,61]. Indeed, NA allows for the handling of complex, high-dimensional data typical in psychological research, uncovering patterns that traditional statistical methods might miss.
We decided to include in the NA some variables related to sociodemographic and professional dimensions (age, seniority of service, unused vacation days, accumulated overtime hours) and the scales involved in the assessments applied (psychophysical exhaustion–engagement, relational deterioration–involvement, professional inefficacy–efficacy, disillusion–fulfilment, career satisfaction, satisfaction with the job itself, satisfaction with the setting and the organizational structure, satisfaction with organizational processes, satisfaction with interpersonal relationships). We decided not to include in the NA additional sociodemographic and occupational variables (e.g., gender, department, occupational category), as the group of participants did not appear to be balanced and stratified in relation to these variables.
The application of NA can aid in generating new hypotheses about the interplay of psychological factors, guiding future research directions [62]. It might be adequately applied in psychology due to its ability to effectively represent and analyze the complex, multidimensional, and dynamic nature of psychological data. It provides valuable insights that enhance our understanding of psychological and organizational processes, ultimately contributing to more effective interventions. For these reasons, NA is useful for exploratory data analysis, helping to uncover unexpected relationships [63]. NA is designed to capture and analyze these complex relationships, offering insights into how different elements influence each other. NA allows one to illustrate human behavior and psychological dimensions affected by a multitude of factors simultaneously; it can incorporate and analyze this multidimensionality effectively. Furthermore, the effective data representation and the application of graphical models allow one to depict variables as nodes and their interactions as edges (connections), providing a clear and intuitive visualization of complex relationships. This visual representation helps in identifying patterns, clusters, and central elements within psychological data, making complex data more understandable [60,61].
The computation of specific centrality measures allows the identification of key variables; distinctively, we could identify which variables (nodes) were most central or influential in the network. This was crucial to understanding which aspects/variables played pivotal roles in the psychological phenomena in focus. By identifying central nodes, interventions can be more precisely targeted to disturb maladaptive networks and promote positive changes.
Applying NA, each variable of the model is depicted as a node, as the connection-relating nodes are illustrated as edges [64]. Conventionally in the psychological context, blue edges designate positive relationships; red edges imply negative associations. Furthermore, the width of edges suggests their extent.
In this study, first, we estimated a network that involved the total sample of workers. Next, we applied NA by splitting the sample regarding the variable ‘double caregiving’, distinguishing the individuals that reported double-duty caregiving activities and individuals who did not report caregiving in their families. The analyses were applied with the JASP open-source software (release 0.18.3) [65].
2.5. Ethical Issues
This study was approved by the Ethical Committee at the Cagliari University, Italy (approval number 0166737 dated July 10, 2023), and was thus conducted in full agreement with the Ethical Principles of Psychologists and the Code of Conduct of the American Psychological Association (APA), joined into the Associazione Italiana di Psicologia (AIP) Code of Ethics. The research was carried out with informed and consenting workers; furthermore, according to Italian law, the project ensured the anonymity and privacy of all contributors.
3. Results
3.1. Results of the Overall Sample
To evaluate the linear correlations between continuous variables, the Pearson’s r coefficient was computed, considering the social and professional variables (age, seniority of service, number of unused vacation days, number of accumulated overtime hours), and the dimensions were assessed with burnout (LBQ) and job satisfaction (OSI) questionnaires (Table 1).
The findings highlighted a significant positive correlation between age and seniority of service (r = 0.684***), and between age and unused vacation days (r = 0.202***); there was a significant negative correlation between age and relational deterioration–involvement (r = -0.157***). Also, seniority of service showed a positive, significant correlation with unused vacation days (r = 0.177***). We also observed a positive, significant correlation between unused vacation days and accumulated overtime hours (r = 0.287***) and a negative correlation between satisfaction with interpersonal relationships and unused vacation days (r = -0.113*).
Psychophysical exhaustion–engagement correlated positively with all other scales of burnout and correlated negatively with all subscales of job satisfaction (Table 1). The same trend was confirmed for the other scales; specifically, the job satisfaction subscales correlated positively between the instruments and negatively with the burnout dimensions (Table 1).
We analyzed the data to explore the network structure of the variables, starting with the partial correlation matrix. The variables included in the NA were the following: age, seniority of service, unused vacation days, accumulated overtime hours, and the burnout (LBQ) and job satisfaction (OSI) dimensions. In this study, the network structure highlighted variations in relationships between the variables, according to the undirected edges (i.e., in which the nodes showed connecting lines, implying some mutual relationships without arrowheads to suggest the direction of influence). The NA was computed by the application of a pairwise Markov random field (PMRF), recognizing nodes that performed as ‘ties’ between others (i.e., the ties denote nodes that function as single links between two other nodes in this specific network). ‘Betweenness’ shows the number of shortest paths connecting any two variables.
The quantification of closeness refers to the manner in which a node indirectly is linked to other nodes (i.e., the computation applies the reciprocal of the sum of the smallest pathways from the considered node to different nodes). Closeness is figured as the inverted sum of the total length of all the shortest paths between a particular node and the remaining nodes in the network.
The evaluation of strength aims to identify the nodes that have dense direct links with others (i.e., estimated by the sum of all the absolute edge weights associated with a node). Strength quantifies the sum of the absolute weights of the edge [60,66]. Specifically, a standardized estimation by the extended Bayesian information criterion (EBIC) and the least absolute shrinkage and selection operator (LASSO) [61] were applied [62].
To reveal the importance of each node, centrality indices were considered (i.e., betweenness, closeness, strength, expected influence) [61]. Specifically, the nodes with elevated estimate of centrality indices were judged as the most important nodes in the network.
Betweenness assesses the number of times a node sits on the smallest pathway between two other nodes, relating the node to all the others in the network. The computation of the expected influence is considered to overwhelm the probable fallibility of usual centrality measures in networks with both positive and negative edges [66].
In order to improve the possibility to compare the role of each node, standardized z-scores for all indices were applied [63]. Thus, Zhang’s clustering coefficient was computed [67,68] to identify the locally unnecessary nodes in the network. Finally, we considered stability indices and weights by the application of a non-parametric bootstrap procedure, using 1,000 iterations [61,63]. We considered the accuracy and stability of coefficients, estimating the Centrality Stability coefficient that should not be below 0.25, and preferably above 0.5 [61].
The NA was carried out in different steps [61], initially regarding the total sample, then separately in relation to workers who provided caregiving and those who did not report providing caregiving.
The NA computation with our sample highlighted 13 nodes and 37/78 non-zero edges (sparsity: 0.526). In Table 2, we provide the z-standardized indices, highlighting the most influential nodes in the network; we computed centrality indices and Zhang’s clustering indices.
The graphical representation of these relationships is shown in Figure 1; the blue edges and red edges define, respectively, the positive and negative multivariate partialized relationships among variables. The stability of estimated centrality indices was assessed and is reported in Figure 2. Supplementary graphical outputs are reported in the Appendix.
The higher edge is represented by the positive partial coefficient between age and seniority of service, which are moreover positioned in a marginal position in the network. Also, we noted that the variables related to the overwork conditions (node 3—unused vacation days; and node 4—accumulated overtime hours) are placed in a marginal position in the network. The central position might be identified for node 8 (disillusion–fulfilment).
Node 8 (disillusion–fulfilment) and node 10 (satisfaction with the job itself) might be considered the “bridges” among burnout and job satisfaction dimensions.
The stronger positive index of strength is shown by node 12 (satisfaction with organizational processes). The strong values of expected influences are observed in relation to node 11 (satisfaction with the setting and the organizational structure), node 12 (satisfaction with organizational processes), and node 9 (career satisfaction). The node with high redundance in the network is number 11 (satisfaction with the setting and the organizational structure).
Based on the values shown in Table 2 with reference to the total sample and in particular to the betweenness centrality measure, it can be seen that the relational deterioration–involvement (node 6) and age (node 1) were the variables with the highest values and are therefore central in relation to the entire network.
As for closeness, it can be observed that the data on unused vacation days (node 3), accumulated overtime hours (node 4), and seniority (node 2) were also quite inflated per standardized negative values—and were less central nodes that had a limited impact on the network, while it can be said the opposite for the index of the disillusion–fulfilment dimension (node 8).
Regarding strength, unused vacation days and accumulated overtime hours remained marginal nodes in the network; they appear to have few direct links with the other nodes. However, satisfaction with organizational processes (node 12) appears to have dense direct links with the other nodes.
Regarding expected influence (i.e., how much a node is able to influence the others in both a direct and indirect sense), a small influence of the variables accumulated overtime hours (node 4) and satisfaction with the job itself (node 10) can be observed; conversely, the highest influence can be seen for career satisfaction, satisfaction with the organizational setting and structure, and satisfaction with the organizational processes (respectively nodes 9, 11, and 12).
Going further into the relationships between the individual nodes of the evaluated psychological dimensions (Figure 1), we noted: the inverse relationship between node 5 (psychophysical exhaustion–engagement) and node 13 (satisfaction with interpersonal relationships); the inverse relationship between node 9 (career satisfaction) and node 8 (disillusion–fulfilment), and the inverse relationship between node 7 (professional inefficacy–efficacy) and node 10 (satisfaction with the job itself).
3.2 Results of the Subsample Comparison
In order to explore and deepen the potential features that might characterize workers that did/did not engage in double-caregiving activities, we chose to compare the means of these two groups initially by the application of a Student’s t-test, regarding the means of variables considered in our NA. Table 3 shows there was a significant difference only in relation to the variable seniority of service, which was higher for workers that reported double-duty caregiving activities. For all the other variables assessed, we did not observe any significant difference between the two groups.
Then, NA was applied, distinguishing the variable double caregiving per “yes” or “no”. Specifically, we set the double-caregiving activity as a ‘yes/no’ as a splitting variable; we applied this new analysis by using the same statistical setting mentioned previously to try to reveal the multivariate relationships among the variables in the two groups of workers.
For group 1 (double caregiving “yes”), we obtained 13 nodes, with 34 non-zero edges out of 78 (sparsity: 0.564); for group 2 (double caregiving “no”), we observed 13 nodes, with 38 non-zero edges out of 78 (sparsity: 0.513).
Table 4 illustrates the standardized centrality and clustering measures per variable in relation to each group; the graphical representations of the two networks are reported in Figure 3.
Consistently, with the results obtained by the application of the Student’s t-test comparison between the means of the two groups (see Table 3), the networks of the two groups appear similar. In order to carry out a network comparison, we considered the weight matrix of both networks, and we applied Pearson’s linear correlations on them as a measure of similarity [69,70]. The obtained coefficients ranged from 0.840 to 1.000, highlighting the similarity between the two networks.
As previously emphasized, the variables related to age, seniority of service (nodes 1 and 2, respectively), and overwork (node 3—unused vacation days; node 4—accumulated overtime hours) were in marginal positions in the network. Moreover, the central position in both networks is held by node 5 (psychophysical exhaustion–engagement) and node 8 (disillusion–fulfilment).
The Zhang’s clustering coefficient (per the total sample of workers) for individuals involved or not involved in double-duty caregiving converged in designating node 11 (satisfaction with the setting and the organizational structure) as having higher redundance in the network, possibly since the other nodes, its neighbors’ (9—career satisfaction; 12—satisfaction with organizational processes; and 13—satisfaction with interpersonal relationships), tended to be powerfully associated with each other [67].
In group 2 (double caregiving “no”), the positive association between nodes 5 (psychophysical exhaustion–engagement) and 8 (disillusion–fulfilment), between nodes 5 (psychophysical exhaustion–engagement) and 7 (professional inefficacy–efficacy), and between nodes 9 (career satisfaction) and 12 (satisfaction with organizational processes) were stronger than in group 1.
Observing in detail the two networks in Figure 2, we highlight in the group of workers that reported double-caregiving activities (group 1), there was a strong negative relationship between nodes 5 (psychophysical exhaustion–engagement) and 10 (satisfaction with the job itself). Furthermore, in group 1, we found a strong negative association between nodes 8 (disillusion–fulfilment) and 13 (satisfaction with interpersonal relationships) that were not present in group 2.
In group 1, the positive association between nodes 11 (satisfaction with the setting and the organizational structure) and 12 (satisfaction with organizational processes) was stronger than in group 2. Also in group 1, the negative association between nodes 5 (psychophysical exhaustion–engagement) and 13 (satisfaction with interpersonal relationships) was weaker than the same association in group 2.
In group 1, the negative association between nodes 8 (disillusion–fulfilment) and 12 (satisfaction with the organizational processes) was less intense than the association in group 2. Also in group 1, the negative association between nodes 7 (professional inefficacy–efficacy) and 10 (satisfaction with the job itself) appeared stronger than the association in group 2. Finally, in group 1, the negative association between nodes 6 (relational deterioration–involvement) and 10 (satisfaction with the job itself) was weaker than the association in group 2.
4. Discussion
4.1. Overall Sample
Our findings on the relationship between job satisfaction and job burnout dimensions can provide valuable insights regarding occupational and organizational health in healthcare contexts. Contrary to what we expected and what was found in other studies [3,4,5,6], the stressor variables per work–family balance (especially unused vacation days and accumulated overtime hours) played a very marginal role in influencing the relationship between the nodes of both burnout and job satisfaction dimensions. The explanation of this (i.e., counter-intuitive) result can be facilitated by the subsample comparison analysis (double caregiving yes/no) presented below (Paragraph 4.2).
The relationship between disillusion–fulfilment and satisfaction with the job itself suggests the importance of the preservation of vocational ideals within the context of healthcare roles and the recognition of health workers’ expectations towards their work [52,53]. Also, the centrality of the disillusion–fulfilment dimension emerged, especially its relationship with career satisfaction, like in recent research on the subject [71], satisfaction with organizational processes, and with interpersonal relationships. These findings emphasize the importance of cultivating motivational and vocational aspects of the health professions, besides the importance of relationships with colleagues and users/patients, which deserve further attention in the research.
The inverse relationship between psychophysical exhaustion–engagement and satisfaction with interpersonal relationships reminded us of the value of the emotional dimension in workplace relationships for occupational well-being, satisfaction, and other organizational nature outcomes [72,73,74,75,76]. Finally, the relationship between professional inefficacy–efficacy and satisfaction with the job itself pertains to being able to effectively read the specific problems of one’s own context and feeling competent, as well as translating into a better service what to do with the perception of one’s own job as a source of satisfaction. In the context of the JD-R model [22], perceived professional efficacy can be considered a resource and, in this sense, a motivating factor, in turn promoting involvement and well-being, mitigating the burden of excessive job demands through a better management of these. Moreover, in the frame of self-determination theory [77,78], regarding the need for competence, a worker who feels a high level of success and mastery in their job experiences greater intrinsic motivation and therefore greater job satisfaction.
4.2. Comparison of Subsamples
The results of our NA showed no significant differences in terms of risk of burnout and job satisfaction between the group of healthcare professionals with a double-caregiving role and those without. This result is partially echoed, for example, in a study by Boumans and Dorant [1], where no significant differences were found in job satisfaction and motivation among healthcare professionals with a double-caregiving role; still, the latter were found to experience greater emotional exhaustion and lower psychophysical well-being. This result was also found in other qualitative studies [2]. However, in the groups we compared, the dimensions of disillusion–fulfilment and psychophysical exhaustion–engagement played a central role: this finding gains meaning in relation to the caring profession that our participants shared.
An interesting finding, observable from the network and arrangement of variables, is the marginal position of the sociodemographic variables, which did not show a significant weight in the relationship with the other variables investigated. The common redundancy of the dimension of satisfaction with organizational setting and structure could highlight the importance attached by our participants to the workplace and these specific aspects, which stand as predictors of distress [79].
It is also interesting to note that for the healthcare professionals who did not have dual-care duties, the positive relationships between psychophysical exhaustion–engagement and disillusion–fulfilment, between psychophysical exhaustion–engagement and professional inefficacy–efficacy, and between career satisfaction and satisfaction with organizational processes were more intense compared to the non-double carers. Perhaps the non-caregivers are more vulnerable, as their work can be the main source from which they derive well-being and on which motivation and perceived efficacy are modulated, increasing, for them, the risk of experiencing psychophysical exhaustion. Instead, double caregiving could be a protective factor against the more damaging effects of burnout on vocational ideals and perceived professional efficacy, as it could allow for the development of a greater capabilities and resilience, which are personal resources [79]. The double caregiving role could give the opportunity to find meaning outside of the work sphere, therefore not constituting an "additional burden" for the double caregiver. Playing an informal caregiving role could also paradoxically constitute a kind of detachment from the frustrations related to the professional sphere, whereas non-double caregivers may focus mainly on the professional domain and experience greater identification with the formal caregiving role and struggle more in dealing with stressors, despite identification with one’s work as being considered a characteristic of engagement [79]. In the context of JD-R theory, in fact, this result might be argued for by considering that people have specific personal and professional resources and can interpret a greater workload or personal demands as challenges and feel more motivated or turn them into resources. Perhaps a double-caregiving role can both protect healthcare professionals from the risk of burnout and also exacerbate it. In any case, this result, which is at odds with previous studies on dual carers [3,4,5,6] requires further research.
Similar reasoning might be applied to the dimensions related to satisfaction: Caregivers who are not dual carers and who have a greater focus on their work environment and its stability might derive more satisfaction from an organization that functions efficiently and thus supports their professional development. Double caregivers, on the other hand, who have to manage a double role, might consider other aspects more important than career opportunities, such as work flexibility and organizational support, thus considering aspects strictly related to organizational processes less crucial to their well-being and work–life balance. These findings also require further research.
The same aspects can be discussed by looking more specifically at the differences that emerged between the two groups, such as the negative relationship between disillusion–fulfilment and satisfaction with interpersonal relationships that subsisted only for double caregivers. This result highlights the relevance of the socio-relational aspect in nurturing and protecting the vocational aspects of these workers, who, being busy juggling professional and informal responsibilities, might find the quality of relationships between coworkers and users more influential on their occupational well-being. However, despite the fact that in general—for both groups—positive relationships at work were associated with less psychophysical exhaustion–engagement; for those with a double caring role, the protective function of the relational factor was less impactful for this specific dimension of burnout. Similar aspects have emerged in qualitative analyses like Detaille et al.’s [2]. Moreover, relational deterioration–involvement seemed to have less of an impact on satisfaction with the job itself in the group of double caregivers, possibly due to, as argued earlier, greater resilience or greater entrenchment of the satisfaction that can be drawn from the caring role in general, or the presence of more developed coping strategies for dealing with relational stress.
Also, for the double caregivers, feeling ineffective had a more pronounced impact on satisfaction with the job itself than the other group of colleagues. This may have been due to some kind of conflict between their formal and informal roles, which, on the other hand, may not subsist in those who do not perform the double caring role, since the perception of efficacy can be limited to the work context, thus having less impact on this type of satisfaction. Also, the double caregivers seemed to be less sensitive to the effects of experienced disillusion–fulfilment on satisfaction with organizational processes, probably finding their purpose in other aspects of their existence or professional context, as previously discussed. These results also need additional investigation.
Finally, when healthcare professionals reported they were satisfied with their organizational setting and structure, they also tended to be satisfied with the processes taking place, although this effect emerged more significantly for those with the double-caring role, and a functional organization could allow these people to better address and balance. This finding is in line with JD-R theory in relation to job design [79].
4.3. Practical Implications
The results of this study allowed us to outline some possible lines of intervention for the promotion of job satisfaction and the prevention of burnout risk in health workers, which can be considered (albeit with different nuances) as valid for those with dual-caring duties as for those without this role. Regarding the dimension of disillusion–fulfilment, to date little-studied [71], and its relationship with the different dimensions of job satisfaction, it becomes evident how important it is to promote organizational actions that nurture the sense of importance and vocational work motivation of care workers, regardless of whether they have double-caregiving tasks.
Regarding psychophysical exhaustion–engagement, some studies [72,73,74,75,76] have proposed training interventions aimed at enhancing emotional intelligence among health professionals, with these interventions being a valuable strategy to ensure these health workers’ health is protected, reduce burnout levels, and improve the quality of care of services and their relationships with patients and colleagues.
Moreover, in healthcare organizations, satisfaction with the setting and the organizational structure is a central aspect of occupational well-being. Work environments and occupational roles should be individual-appropriate to avoid high levels of distress and inspire the greater involvement of staff and leaders to define ergonomic and structural aspects. Such collaboration can be a protective factor and allow for more efficient adjustments and better adaptation of planned activities; they can help in planning interventions and/or discussing issues together around how innovations and changes within a company are introduced, following an approach of greater involvement of the staff, implicitly knowing which process improvements can take place, and how [43,44,45].
Concerning the relationship between professional inefficacy–efficacy and satisfaction with the job itself, we recommend promoting a greater perception of professional effectiveness through interventions aimed at improving self-efficacy, autonomy, psychological capital, and self-determination. Finally, it is certainly important to consider specific and particular conditions of health workers with more burdensome family circumstances (e.g., those with dual-caregiving duties) and to promote organizational and work actions that enable these people to manage their work–life balance in a sustainable way.
4.4. Study Limitations
This study had several limitations, including this study’s mainly descriptive nature, given the still under-explored phenomenon in relation to the specific dimensions assessed, the profession of the participants, and the specific cultural context; thus, we consider our conducted analyses preliminary. Regarding the characteristics of the sample, for a more accurate reading of the results, it is worth noting that most of the participants reported nursing as their job and identified with the female gender, although these variables were not specifically included in the network; similarly, more than 90% of our participants reported no coordinating role, so subsequent research could focus more on health directors or managers, including those who have an administrative role in hospital facilities.
Future research on work–life balance, as well as on the specific topic of double-duty caregiving, could also take into account the variables excluded in this study (reasons given in Section 2.4), such as gender and occupational category, or other more specific categories, such as any restorative activity carried out during extra-work hours, which could deepen this area of research.
Another aspect for further investigation which could not be evaluated here as a single ‘macro-factor’ could be some kind of strain variable, which might be analyzed as a composite variable, consisting of similar data—or additionally—to those collected in this study, like unused vacation days, accumulated overtime hours, and seniority of service. Moreover, adding a specific measure of double-duty caregiving and work–life balance—or, better, work–life integration—through dedicated instruments, here missing, could lead to more accurate interpretations. Finally, regarding the relationships discussed above, in addition to understanding whether they are replicable in similar studies involving healthcare professionals, they clearly need to be further explored also in qualitative terms to better investigate their nature.
5. Conclusions
Given our findings and the theoretical framework of the present study, with reference to work–life balance and JD-R theory, some concluding remarks can be made. Irrespective of whether one has a dual-caring role or not, an organization that is functionally structured such that process-design involves more of the employees could be a context capable of promoting and facilitating the development of personal and job resources aimed at better balancing private life and work. In public healthcare, greater care for ergonomics and settings could significantly improve the occupational well-being and job satisfaction of healthcare workers, while at the same time enabling better management of stressors, resulting in a more caring and respectful environment for workers’ needs, expectations, and values. Regardless of the domain from which the demands come, a more sustainable organization of work can in fact be helpful in mitigating the perceived conflict between life and work, and vice versa, reducing the risk of burnout and promoting professional fulfilment, as well as higher levels of engagement and, given the particular times and the current Italian socioeconomic context, lower levels of turnover. Finally, the role of dual caregiving in managing the work–family interface appears complex and multifaceted. In fact, it cannot simply be considered as an additional demand for this type of healthcare worker, but perhaps has nuances of a vocational nature that can be linked to the self-actualizing aspects of the different healthcare professions. Indeed, it might paradoxically constitute a personal resource that can modulate the relationship between the burnout risk and job satisfaction of healthcare workers. For this reason, it should be properly considered in the organization and management of the work–family interface of healthcare workers.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Ethics Committee of the University of Cagliari (approval number 0166737 dated July 10, 2023) for studies involving humans.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data are available within the article. For more information, please contact the corresponding author.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Boumans, N.P.G.; Dorant, E. Double-duty Caregivers: Healthcare Professionals Juggling Employment and Informal Caregiving. A Survey on Personal Health and Work Experiences. J. Adv. Nurs. 2014, 70, 1604–1615. [Google Scholar] [CrossRef] [PubMed]
- Detaille, S.I.; De Lange, A.; Engels, J.; Pijnappels, M.; Hutting, N.; Osagie, E.; Reig-Botella, A. Supporting Double Duty Caregiving and Good Employment Practices in Health Care Within an Aging Society. Front. Psychol. 2020, 11, 535353. [Google Scholar] [CrossRef] [PubMed]
- Häusler, N.; Bopp, M.; Hämmig, O. Informal Caregiving, Work-Privacy Conflict and Burnout among Health Professionals in Switzerland—A Cross-Sectional Study. Swiss Med. Wkly. 2017. [Google Scholar] [CrossRef]
- Gérain, P.; Zech, E. Informal Caregiver Burnout? Development of a Theoretical Framework to Understand the Impact of Caregiving. Front. Psychol. 2019, 10. [Google Scholar] [CrossRef]
- Williams, K.; Eggett, D.; Patten, E.V. How Work and Family Caregiving Responsibilities Interplay and Affect Registered Dietitian Nutritionists and Their Work: A National Survey. PLoS ONE 2021, 16, e0248109. [Google Scholar] [CrossRef] [PubMed]
- Gérain, P.; Zech, E. Do Informal Caregivers Experience More Burnout? A Meta-Analytic Study. Psychology, Health & Medicine 2021, 26, 145–161. [Google Scholar] [CrossRef]
- Boy, Y.; Sürmeli, M. Quiet quitting: A significant risk for global healthcare. Journal of Global Health 2023, 13, 03014. [Google Scholar] [CrossRef]
- DePasquale, N.; Davis, K.D.; Zarit, S.H.; Moen, P.; Hammer, L.B.; Almeida, D.M. Combining Formal and Informal Caregiving Roles: The Psychosocial Implications of Double- and Triple-Duty Care. GERONB 2016, 71, 201–211. [Google Scholar] [CrossRef]
- Schwartz, S.P.; Adair, K.C.; Bae, J.; Rehder, K.J.; Shanafelt, T.D.; Profit, J.; Sexton, J.B. Work-Life Balance Behaviours Cluster in Work Settings and Relate to Burnout and Safety Culture: A Cross-sectional Survey Analysis. BMJ Quality & Safety 2019, 28(2), 142–150. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; Hasan, O.; Dyrbye, L.N.; Sinsky, C.; Satele, D.; Sloan, J.; West, C.P. Changes in Burnout and Satisfaction With Work-Life Balance in Physicians and the General US Working Population Between 2011 and 2014. Mayo Clinic Proceedings 2015, 90, 1600–1613. [Google Scholar] [CrossRef]
- Shanafelt, T.D.; West, C.P.; Sinsky, C.; Trockel, M.; Tutty, M.; Wang, H.; Carlasare, L.E.; Dyrbye, L.N. Changes in Burnout and Satisfaction With Work-Life Integration in Physicians and the General US Working Population Between 2011 and 2020. Mayo Clinic Proceedings 2022, 97, 491–506. [Google Scholar] [CrossRef] [PubMed]
- Bodendieck, E.; Jung, F.U.; Conrad, I.; Riedel-Heller, S.G.; Hussenoeder, F.S. The Work-Life Balance of General Practitioners as a Predictor of Burnout and Motivation to Stay in the Profession. BMC Prim. Care 2022, 23, 218. [Google Scholar] [CrossRef] [PubMed]
- Volk, J.O.; Schimmack, U.; Strand, E.B.; Reinhard, A.; Hahn, J.; Andrews, J.; Probyn-Smith, K.; Jones, R. Work-Life Balance Is Essential to Reducing Burnout, Improving Well-Being. J Am Vet Med Assoc 2024, 262, 950–957. [Google Scholar] [CrossRef] [PubMed]
- Parmar, J.; L’Heureux, T.; Lobchuk, M.; Penner, J.; Charles, L.; St. Amant, O.; Ward-Griffin, C.; Anderson, S. Double-Duty Caregivers Enduring COVID-19 Pandemic to Endemic: “It’s Just Wearing Me down”. PLoS ONE 2024, 19, e0298584. [Google Scholar] [CrossRef] [PubMed]
- Chan, X.W.; Shang, S.; Brough, P.; Wilkinson, A.; Lu, C. Work, Life and COVID -19: A Rapid Review and Practical Recommendations for the post-pandemic Workplace. Asia Pac J Human Res 2023, 61, 257–276. [Google Scholar] [CrossRef]
- Ayar, D.; Karaman, M.A.; Karaman, R. Work-Life Balance and Mental Health Needs of Health Professionals During COVID-19 Pandemic in Turkey. Int J Ment Health Addiction 2022, 20, 639–655. [Google Scholar] [CrossRef]
- Mahfouz, M.S.; Osman, S.A.; Mohamed, B.A.; Saeed, E.A.M.; Ismaeil, M.I.H.; Elkhider, R.A.A.; Orsud, M.A. Healthcare Professionals’ Experiences During the COVID-19 Pandemic in Sudan: A Cross-Sectional Survey Assessing Quality of Life, Mental Health, and Work-Life-Balance. Int J Public Health 2023, 68, 1605991. [Google Scholar] [CrossRef]
- Thro, P.D.; Prasain, G.P. Work-Life Balance—Its Impact on Job Satisfaction among the Healthcare Workers in Senapati District, Manipur. SDMIMD 2024, 119–129. [Google Scholar] [CrossRef]
- El Keshky, M.E.S.; Sarour, E.O. The Relationships between Work-Family Conflict and Life Satisfaction and Happiness among Nurses: A Moderated Mediation Model of Gratitude and Self-Compassion. Front. Public Health 2024, 12, 1340074. [Google Scholar] [CrossRef]
- Pien, L.-C.; Cheng, W.-J.; Chou, K.-R.; Lin, L.-C. Effect of Work–Family Conflict, Psychological Job Demand, and Job Control on the Health Status of Nurses. IJERPH 2021, 18, 3540. [Google Scholar] [CrossRef]
- Mitra, L.G.; Sharma, J.; Walia, H.S. Improving Work–Life Balance and Satisfaction to Improve Patient Care. Indian J Crit Care Med 2024, 28, 326–328. [Google Scholar] [CrossRef] [PubMed]
- Demerouti, E.; Bakker, A.B. Job Demands-Resources Theory in Times of Crises: New Propositions. Organizational Psychology Review 2023, 13, 209–236. [Google Scholar] [CrossRef]
- Maslach, C.; Leiter, M.P.; Schaufeli, W.B. Measuring burnout. In The Oxford Handbook of Organizational Well-Being; Cooper, C.L., Cartwright, S., Eds.; Oxford University Press: Oxford, UK, 2009; pp. 86–108. [Google Scholar]
- Schaufeli, W.B. Burnout: A short socio-cultural history. In Burnout, Fatigue, Exhaustion; Neckel, S., Schaffner, A., Wagner, G., Eds.; Palgrave Macmillan: Cham, Switzerland, 2017a; pp. 105–127. [Google Scholar]
- Nadon, L.; De Beer, L.T.; Morin, A.J.S. Should Burnout Be Conceptualized as a Mental Disorder? Behav. Sci. 2022, 12, 82. [Google Scholar] [CrossRef]
- Schaufeli, W.B. Burnout: A Critical Overview. In Organizational Stress and Well-Being; Lapierre, L.M., Cooper, C., Eds.; Cambridge University Press: Cambridge, UK, 2023; pp. 214–259. [Google Scholar]
- Schaufeli, W.B. Applying the Job Demands-Resources Model. Organ. Dyn. 2017b, 46, 120–132. [Google Scholar] [CrossRef]
- Hu, Q.; Schaufeli, W.B.; Taris, T.W. How Are Changes in Exposure to Job Demands and Job Resources Related to Burnout and Engagement? A Longitudinal Study among Chinese Nurses and Police Officers. Stress and Health 2017, 33, 631–644. [Google Scholar] [CrossRef] [PubMed]
- Rattrie, L.T.B.; Kittler, M.G.; Paul, K.I. Culture, Burnout, and Engagement: A Meta-Analysis on National Cultural Values as Moderators in JD-R Theory. Applied Psychology 2020, 69, 176–220. [Google Scholar] [CrossRef]
- Schaufeli, W.B. Work Engagement. What Do We Know and Where Do We Go? Rom. J. Appl. Psychol. 2012, 14, 3–10. [Google Scholar]
- Schaufeli, W.B.; Bakker, A.B. Defining and measuring work engagement: Bringing clarity to the concept. In Work Engagement: A Handbook of Essential Theory and Research; Bakker, A.B., Leiter, M.P., Eds.; Psychology Press: London, UK, 2010; pp. 10–24. [Google Scholar]
- Hakanen, J.J.; Ropponen, A.; Schaufeli, W.B.; De Witte, H. Who Is Engaged at Work?: A Large-Scale Study in 30 European Countries. J Occup Environ Med 2019, 61, 373–381. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Bakker, A.B.; Van Rhenen, W. How Changes in Job Demands and Resources Predict Burnout, Work Engagement, and Sickness Absenteeism. J Organ Behavior 2009, 30, 893–917. [Google Scholar] [CrossRef]
- Hakanen, J.J.; Schaufeli, W.B. Do Burnout and Work Engagement Predict Depressive Symptoms and Life Satisfaction? A Three-Wave Seven-Year Prospective Study. J Affec Disord 2012, 141, 415–424. [Google Scholar] [CrossRef] [PubMed]
- Nonnis, M.; Pirrone, M.P.; Cuccu, S.; Agus, M.; Pedditzi, M.L.; Cortese, C.G. Burnout Syndrome in Reception Systems for Illegal Immigrants in the Mediterranean. A Quantitative and Qualitative Study of Italian Practitioners. Sustainability 2020, 12, 5145. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Bakker, A.B. Work Engagement: A Critical Assessment of the Concept and Its Measurement. In Handbook of Positive Psychology Assessment; Tuch, W.R., Bakker, A.B., Tay, L., Gander, F., Eds.; Hogrefe: Göttingen, Germany, 2022; pp. 273–295. [Google Scholar]
- World Health Organization (WHO). International Classification of Diseases (ICD-11). Available online: https://icd.who.int/browse11/l-m/en#/http://id.who.int/icd/entity/129180281 (accessed on 25 September 2024).
- Santinello, M.; Negrisolo, A. Quando Ogni Passione è Spenta. La Sindrome del Burnout nelle Professioni Sanitarie; Mc Graw Hill: Milan, Italy, 2009; pp. 5–34. [Google Scholar]
- Borgogni, L.; Consiglio, C.; Alessandri, G.; Schaufeli, W.B. “Don’t Throw the Baby out with the Bathwater!” Interpersonal Strain at Work and Burnout. Eur J Work Organ Psychol 2012, 21, 875–898. [Google Scholar] [CrossRef]
- Edelwich, J.; Brodsky, A. Burnout: Stages of Disillusionment in the Helping Professions; Kluwer Academic Plenum Publishers: Dordrecht, The Netherlands, 1980; pp. 7–48. [Google Scholar]
- Tanios, M.; Haberman, D.; Bouchard, J.; Motherwell, M.; Patel, J. Analyses of Burn-out among Medical Professionals and Suggested Solutions—A Narrative Review. J Hosp Manag Health Policy 2022, 6. [Google Scholar] [CrossRef]
- Zhang, M.; Li, S.; Han, D.; Wu, Y.; Zhao, J.; Liao, H.; Ma, Y.; Yan, C.; Wang, J. Association of Job Characteristics and Burnout of Healthcare Workers in Different Positions in Rural China: A Cross-Sectional Study. Int J Public Health 2023, 68, 1605966. [Google Scholar] [CrossRef]
- Izdebski, Z.; Kozakiewicz, A.; Białorudzki, M.; Dec-Pietrowska, J.; Mazur, J. Occupational Burnout in Healthcare Workers, Stress and Other Symptoms of Work Overload during the COVID-19 Pandemic in Poland. IJERPH 2023, 20, 2428. [Google Scholar] [CrossRef]
- Burrowes, S.A.B.; Casey, S.M.; Pierre-Joseph, N.; Talbot, S.G.; Hall, T.; Christian-Brathwaite, N.; Del-Carmen, M.; Garofalo, C.; Lundberg, B.; Mehta, P.K.; et al. COVID-19 Pandemic Impacts on Mental Health, Burnout, and Longevity in the Workplace among Healthcare Workers: A Mixed Methods Study. J Interprof Educ Pract 2023, 32, 100661. [Google Scholar] [CrossRef] [PubMed]
- Antao, H.S.; Sacadura-Leite, E.; Correia, A.I.; Figueira, M.L. Burnout in Hospital Healthcare Workers after the Second COVID-19 Wave: Job Tenure as a Potential Protective Factor. Front. Psychol. 2022, 13, 942727. [Google Scholar] [CrossRef] [PubMed]
- Spector, P.E. Job Satisfaction: Application, Assessment, Causes, and Consequences; SAGE Publications Inc.: Thousand Oaks, CA, USA, 1997. [Google Scholar]
- Caraballo-Arias, Y.; Feola, D.; Milani, S. The Science of Joy: Happiness among Healthcare Workers. Curr Opin Epidemiol Public Health 2024. [Google Scholar] [CrossRef]
- Negri, L.; Cilia, S.; Falautano, M.; Grobberio, M.; Niccolai, C.; Pattini, M.; Pietrolongo, E.; Quartuccio, M.E.; Viterbo, R.G.; Allegri, B.; et al. Job Satisfaction among Physicians and Nurses Involved in the Management of Multiple Sclerosis: The Role of Happiness and Meaning at Work. Neurol Sci 2022, 43, 1903–1910. [Google Scholar] [CrossRef]
- De Simone, S.; Vargas, M.; Servillo, G. Organizational Strategies to Reduce Physician Burnout: A Systematic Review and Meta-Analysis. Aging Clin Exp Res 2021, 33, 883–894. [Google Scholar] [CrossRef]
- Srivastava, S.; Misra, R.; Madan, P. ‘The Saviors Are Also Humans’: Understanding the Role of Quality of Work Life on Job Burnout and Job Satisfaction Relationship of Indian Doctors. Journal of Health Management 2019, 21, 210–229. [Google Scholar] [CrossRef]
- Barili, E.; Bertoli, P.; Grembi, V.; Rattini, V. Job Satisfaction among Healthcare Workers in the Aftermath of the COVID-19 Pandemic. PLoS ONE 2022, 17, e0275334. [Google Scholar] [CrossRef]
- Keller, E.; Widestrom, M.; Gould, J.; Fang, R.; Davis, K.G.; Gillespie, G.L. Examining the Impact of Stressors during COVID-19 on Emergency Department Healthcare Workers: An International Perspective. IJERPH 2022, 19, 3730. [Google Scholar] [CrossRef] [PubMed]
- Selič-Zupančič, P.; Klemenc-Ketiš, Z.; Onuk Tement, S. The Impact of Psychological Interventions with Elements of Mindfulness on Burnout and Well-Being in Healthcare Professionals: A Systematic Review. J. Multidiscip. Healthc. 2023, 16, 1821–1831. [Google Scholar] [CrossRef] [PubMed]
- Khamlub, S.; Harun-Or-Rashid, M.; Sarker, M.A.B.; Hirosawa, T.; Outavong, P.; Sakamoto, J. Job Satisfaction of Health-Care Workers at Health Centers in Vientiane Capital and Bolikhamsai Province, Lao PDR. Nagoya J Med Sci 2013, 75, 233–241. [Google Scholar]
- Deshmukh, N.; Raj, P.; Chide, P.; Borkar, A.; Velhal, G.; Chopade, R. Job Satisfaction Among Healthcare Providers in a Tertiary Care Government Medical College and Hospital in Chhattisgarh. Cureus 2023, 15(6). [Google Scholar] [CrossRef]
- Karaferis, D.; Aletras, V.; Niakas, D.N. Job Satisfaction of Primary Healthcare Professionals: A Cross-Sectional Survey in Greece: Job Satisfaction in Greek Primary Care. Acta Biomed 2023, 94, e2023077. [Google Scholar] [CrossRef]
- Galanis, P.; Moisoglou, I.; Katsiroumpa, A.; Vraka, I.; Siskou, O.; Konstantakopoulou, O.; Meimeti, E.; Kaitelidou, D. Increased Job Burnout and Reduced Job Satisfaction for Nurses Compared to Other Healthcare Workers after the COVID-19 Pandemic. Nursing Reports 2023, 13, 1090–1100. [Google Scholar] [CrossRef]
- Santinello, M. Link Burnout Questionnaire — LBQ; Giunti, O.S., Ed.; Organizzazioni Speciali: Firenze, Italia, 2007. [Google Scholar]
- Cooper, L.C.; Sloan, S.J.; Williams, S. OSI: Occupational Stress Indicator. Adattamento Italiano a cura di Saulo Sirigatti e Cristina Stefanile; 2002.
- Borsboom, D.; Deserno, M.K.; Rhemtulla, M.; Epskamp, S.; Fried, E.I.; McNally, R.J.; Robinaugh, D.J.; Perugini, M.; Dalege, J.; Costantini, G.; et al. Network Analysis of Multivariate Data in Psychological Science. Nat Rev Methods Primers 2021, 1, 58. [Google Scholar] [CrossRef]
- Epskamp, S.; Borsboom, D.; Fried, E.I. Estimating Psychological Networks and Their Accuracy: A Tutorial Paper. Behav Res 2018, 50, 195–212. [Google Scholar] [CrossRef]
- Epskamp, S.; Fried, E.I. A Tutorial on Regularized Partial Correlation Networks. Psychological Methods 2018, 23, 617–634. [Google Scholar] [CrossRef] [PubMed]
- Hevey, D. Network Analysis: A Brief Overview and Tutorial. Health Psychol Behav Med 2018, 6, 301–328. [Google Scholar] [CrossRef] [PubMed]
- Epskamp, S.; Cramer, A.O.J.; Waldorp, L.J.; Schmittmann, V.D.; Borsboom, D. Qgraph : Network Visualizations of Relationships in Psychometric Data. J. Stat. Soft. 2012, 48. [Google Scholar] [CrossRef]
- AA.VV. (2024). JASP 0.18.3 software [Software]. https://jasp-stats.org/.
- Robinaugh, D.J.; Millner, A.J.; McNally, R.J. Identifying Highly Influential Nodes in the Complicated Grief Network. J. Abnorm. Psychol. 2016, 125, 747–757. [Google Scholar] [CrossRef] [PubMed]
- Costantini, G.; Perugini, M. Generalization of Clustering Coefficients to Signed Correlation Networks. PLoS ONE 2014, 9, e88669. [Google Scholar] [CrossRef]
- Zhang, B.; Horvath, S. A General Framework for Weighted Gene Co-Expression Network Analysis. Stat Appl Genet Mol Biol 2005, 4. [Google Scholar] [CrossRef]
- Jiang, Y.; Li, M.; Fan, Y.; Di, Z. Characterizing Dissimilarity of Weighted Networks. Sci Rep 2021, 11, 5768. [Google Scholar] [CrossRef] [PubMed]
- Tantardini, M.; Ieva, F.; Tajoli, L.; Piccardi, C. Comparing Methods for Comparing Networks. Sci Rep 2019, 9, 17557. [Google Scholar] [CrossRef]
- Nonnis, M.; Agus, M.; Corona, F.; Aru, N.; Urban, A.; Cortese, C.G. The Role of Fulfilment and Disillusion in the Relationship between Burnout and Career Satisfaction in Italian Healthcare Workers. Sustainability 2024, 16, 893. [Google Scholar] [CrossRef]
- Dugan, J.W.; Weatherly, R.A.; Girod, D.A.; Barber, C.E.; Tsue, T.T. A Longitudinal Study of Emotional Intelligence Training for Otolaryngology Residents and Faculty. JAMA Otolaryngol Head Neck Surg 2014, 140, 720. [Google Scholar] [CrossRef]
- Shahid, R.; Stirling, J.; Adams, W. Promoting Wellness and Stress Management in Residents through Emotional Intelligence Training. Adv. Med. Educ. Pract. 2018, 9, 681–686. [Google Scholar] [CrossRef] [PubMed]
- Foji, S.; Vejdani, M.; Salehiniya, H.; Khosrorad, R. The Effect of Emotional Intelligence Training on General Health Promotion among Nurse. J Edu Health Promot 2020, 9, 4. [Google Scholar] [CrossRef]
- Sharp, G.; Bourke, L.; Rickard, M.J.F.X. Review of Emotional Intelligence in Health Care: An Introduction to Emotional Intelligence for Surgeons. ANZ Journal of Surgery 2020, 90, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Bhattacharjee, A.; Ali, A.; Basu, A. Effectiveness Of Emotional Intelligence Training Programs For Healthcare Providers In Kolkata. EATP 2024, 3784–3757. [Google Scholar] [CrossRef]
- Deci, E.L.; Ryan, R.M. Self-Determination Theory. In P. A. M. Van Lange, A.W. Kruglanski, & E. T. Higgins (Eds.), Handbook of Theories of Social Psychology: Volume 1; SAGE Publications Ltd.: London, UK, 2012; pp. 416–436. [Google Scholar] [CrossRef]
- Deci, E.L.; Olafsen, A.H.; Ryan, R.M. Self-Determination Theory in Work Organizations: The State of a Science. Annu. Rev. Organ. Psychol. Organ. Behav. 2017, 4, 19–43. [Google Scholar] [CrossRef]
- Bakker, A.B.; Demerouti, E.; Sanz-Vergel, A. Job Demands–Resources Theory: Ten Years Later. Annu. Rev. Organ. Psychol. Organ. Behav. 2023, 10, 25–53. [Google Scholar] [CrossRef]
Figure 1.
Estimated Network Model with the Total Sample.
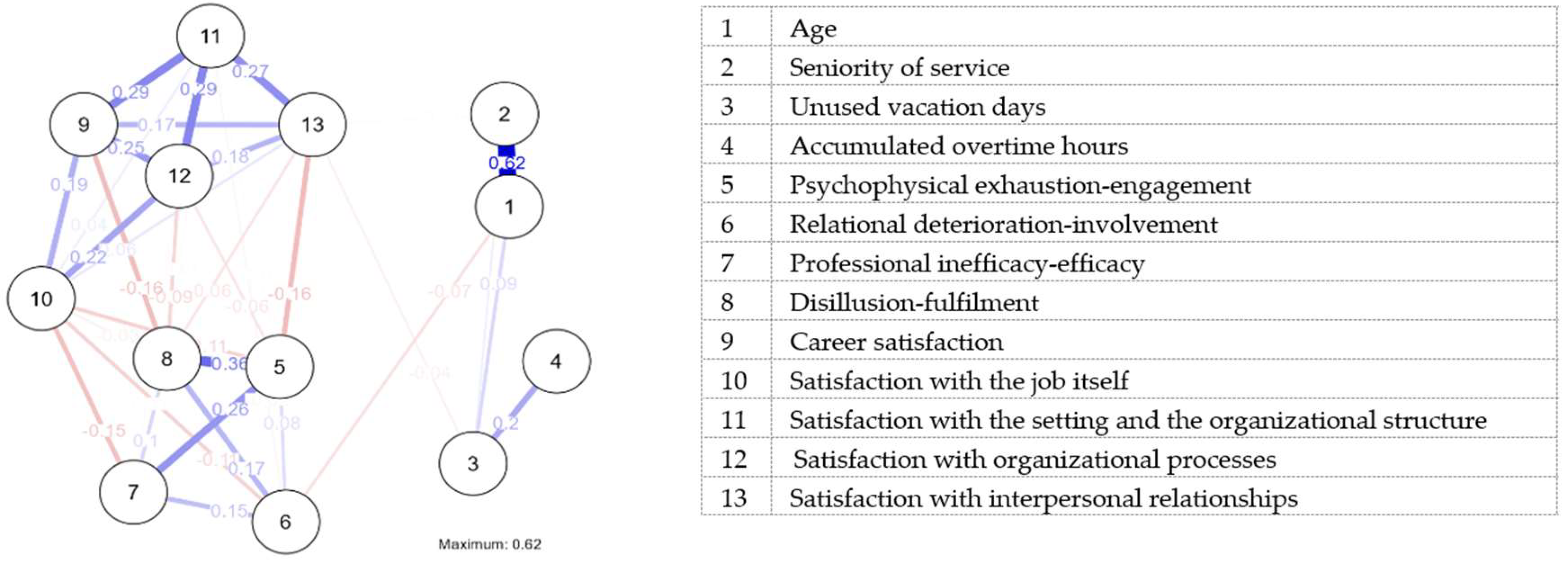
Figure 2.
Estimated Network Plots for the Two Groups.
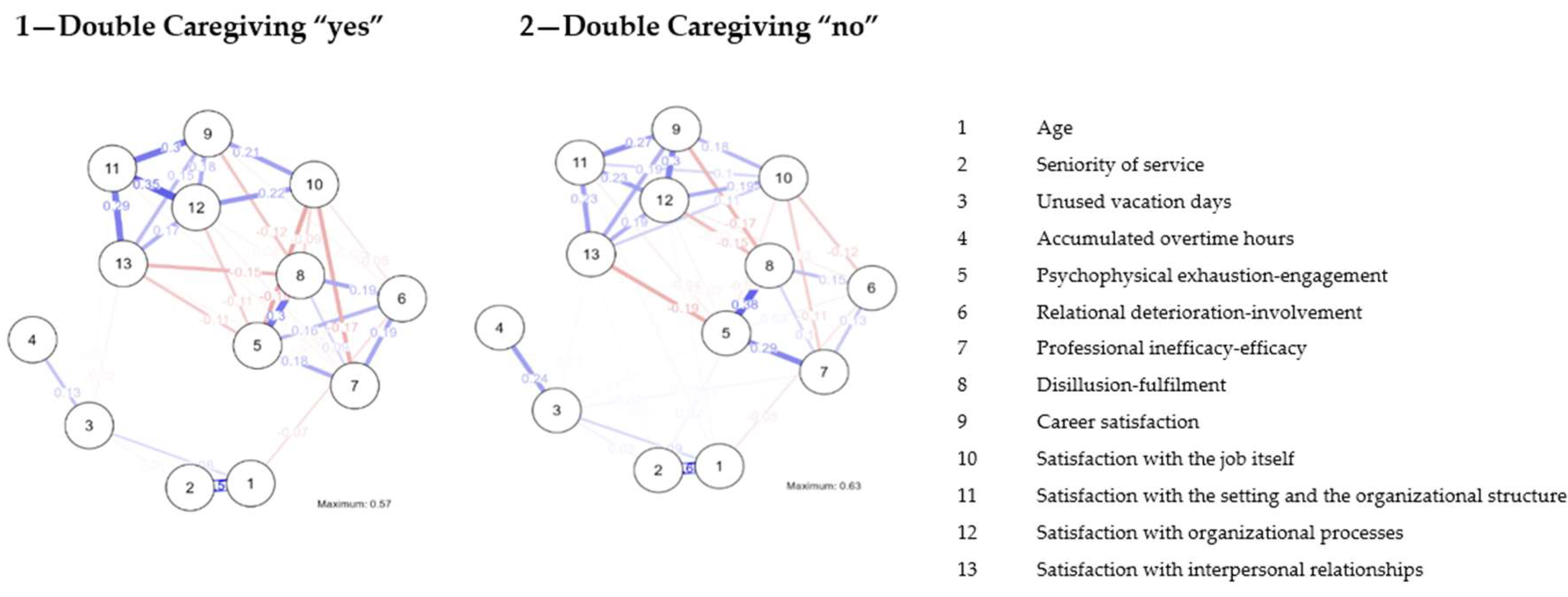

Table 1.
Pearson’s Correlations.
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | ||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Age | R | — | |||||||||||||||||||||||||
| p-value | — | ||||||||||||||||||||||||||
| 2. Seniority of service | R | 0.684 | *** | — | |||||||||||||||||||||||
| p-value | < .001 | — | |||||||||||||||||||||||||
| 3. Unused vacation days | R | 0.202 | *** | 0.177 | *** | — | |||||||||||||||||||||
| p-value | < .001 | < .001 | — | ||||||||||||||||||||||||
| 4. Accumulated overtime hours | R | -0.002 | 0.034 | 0.287 | *** | — | |||||||||||||||||||||
| p-value | 0.960 | 0.465 | < .001 | — | |||||||||||||||||||||||
| 5. Psychophysical exhaustion-engagement | R | -0.053 | -0.004 | 0.057 | 0.058 | — | |||||||||||||||||||||
| p-value | 0.249 | 0.927 | 0.217 | 0.212 | — | ||||||||||||||||||||||
| 6. Relational deterioration-involvement | R | -0.157 | *** | -0.089 | -0.014 | -0.022 | 0.537 | *** | — | ||||||||||||||||||
| p-value | < .001 | 0.054 | 0.771 | 0.636 | < .001 | — | |||||||||||||||||||||
| 7. Professional inefficacy-efficacy | R | 0.001 | -0.041 | 0.048 | -0.037 | 0.652 | *** | 0.500 | *** | — | |||||||||||||||||
| p-value | 0.998 | 0.381 | 0.298 | 0.428 | < .001 | < .001 | — | ||||||||||||||||||||
| 8. Disillusion-fulfilment | R | -0.056 | 0.021 | 0.002 | 0.026 | 0.778 | *** | 0.563 | *** | 0.598 | *** | — | |||||||||||||||
| p-value | 0.228 | 0.647 | 0.959 | 0.578 | < .001 | < .001 | < .001 | — | |||||||||||||||||||
| 9. Career Satisfaction | R | 0.053 | -0.023 | -0.064 | -0.045 | -0.660 | *** | -0.460 | *** | -0.500 | *** | -0.720 | *** | — | |||||||||||||
| p-value | 0.252 | 0.624 | 0.168 | 0.332 | < .001 | < .001 | < .001 | < .001 | — | ||||||||||||||||||
| 10. Satisfaction with the Job itself | R | 0.020 | 0.066 | -0.048 | -0.032 | -0.679 | *** | -0.513 | *** | -0.581 | *** | -0.669 | *** | 0.756 | *** | — | |||||||||||
| p-value | 0.670 | 0.157 | 0.303 | 0.491 | < .001 | < .001 | < .001 | < .001 | < .001 | — | |||||||||||||||||
| 11. Satisfaction with the setting and the Organizational Structure | R | 0.065 | -0.026 | -0.080 | -0.016 | -0.646 | *** | -0.456 | *** | -0.479 | *** | -0.664 | *** | 0.832 | *** | 0.704 | *** | — | |||||||||
| p-value | 0.161 | 0.570 | 0.086 | 0.734 | < .001 | < .001 | < .001 | < .001 | < .001 | < .001 | — | ||||||||||||||||
| 12. Satisfaction with Organizational Processes | R | 0.083 | 0.029 | -0.027 | -0.039 | -0.693 | *** | -0.464 | *** | -0.540 | *** | -0.714 | *** | 0.842 | *** | 0.768 | *** | 0.835 | *** | — | |||||||
| p-value | 0.074 | 0.530 | 0.561 | 0.404 | < .001 | < .001 | < .001 | < .001 | < .001 | < .001 | < .001 | — | |||||||||||||||
| 13. Satisfaction with Interpersonal Relationships | R | 0.005 | -0.055 | -0.113 | * | -0.023 | -0.696 | *** | -0.384 | *** | -0.520 | *** | -0.688 | *** | 0.796 | *** | 0.699 | *** | 0.804 | *** | 0.801 | *** | — | ||||
| p-value | 0.907 | 0.234 | 0.015 | 0.629 | < .001 | < .001 | < .001 | < .001 | < .001 | < .001 | < .001 | < .001 | — |
* p < .05, ** p < .01, *** p < .001
Table 2.
Total Sample Network Analysis: Centrality and Clustering Measures per Variable, Expressed as Standardized Values (Z-Scores)
Table 2.
Total Sample Network Analysis: Centrality and Clustering Measures per Variable, Expressed as Standardized Values (Z-Scores)
| Centrality measures per variable | Clustering measure per variable | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Betweenness | Closeness | Strength | Expected Influence | Zhang | ||||||
| 1 | Age | 1.641 | -0.679 | -0.008 | 0.753 | -1.475 | |||||
| 2 | Seniority of service | -0.949 | -0.957 | -0.436 | 0.776 | -0.475 | |||||
| 3 | Unused vacation days | 0.408 | -1.605 | -1.527 | -0.634 | -0.879 | |||||
| 4 | Accumulated overtime hours | -0.949 | -2.068 | -2.119 | -1.007 | -1.835 | |||||
| 5 | Psychophysical exhaustion-engagement | -0.085 | 0.696 | 0.889 | -0.355 | -0.281 | |||||
| 6 | Relational deterioration-involvement | 2.011 | 0.981 | -0.669 | -0.981 | 0.107 | |||||
| 7 | Professional inefficacy-efficacy | -0.949 | 0.642 | -0.461 | -0.412 | 0.801 | |||||
| 8 | Disillusion-fulfilment | 0.901 | 1.019 | 0.721 | -0.706 | -0.166 | |||||
| 9 | Career satisfaction | -0.209 | 0.526 | 0.985 | 1.180 | 0.898 | |||||
| 10 | Satisfaction with the job itself | -0.332 | 0.486 | 0.389 | -1.370 | 0.075 | |||||
| 11 | Satisfaction with the setting and the organizational structure | -0.949 | 0.204 | 0.519 | 1.638 | 1.593 | |||||
| 12 | Satisfaction with organizational processes | -0.702 | 0.247 | 1.135 | 1.294 | 0.874 | |||||
| 13 | Satisfaction with interpersonal relationships | 0.161 | 0.507 | 0.583 | -0.178 | 0.763 | |||||
Table 3.
Student’s T-Test Comparison of Means in Two Groups (Workers That Did/Did Not Provide Caregiving).
Table 3.
Student’s T-Test Comparison of Means in Two Groups (Workers That Did/Did Not Provide Caregiving).
| Variables | t | df | p | Cohen’s d | Group | Mean | Standard Deviation | |
|---|---|---|---|---|---|---|---|---|
| 1 | Age | 1.128 | 464 | 0.260 | 0.105 | 1 – Double caregiving yes | 50.158 | 8.783 |
| 2 – Double caregiving no | 49.133 | 10.388 | ||||||
| 2 | Seniority of service | 2.617 | 464 | 0.009 | 0.245 | 1 – Double caregiving yes | 20.015 | 10.428 |
| 2 – Double caregiving no | 17.319 | 11.454 | ||||||
| 3 | Unused vacation days | 1.771 | 463 | 0.077 | 0.166 | 1 – Double caregiving yes | 27.713 | 35.252 |
| 2 – Double caregiving no | 22.087 | 32.914 | ||||||
| 4 | Accumulated overtime hours | -0.548 | 456 | 0.584 | -0.052 | 1 – Double caregiving yes | 100.111 | 156.760 |
| 2 – Double caregiving no | 109.039 | 184.263 | ||||||
| 5 | Psychophysical exhaustion-engagement | -0.843 | 464 | 0.400 | -0.079 | 1 – Double caregiving yes | 19.421 | 6.189 |
| 2 – Double caregiving no | 19.909 | 6.199 | ||||||
| 6 | Relational deterioration-involvement | 1.166 | 464 | 0.244 | 0.109 | 1 – Double caregiving yes | 16.158 | 3.705 |
| 2 – Double caregiving no | 15.758 | 3.657 | ||||||
| 7 | Professional inefficacy-efficacy | -0.988 | 464 | 0.323 | -0.092 | 1 – Double caregiving yes | 14.847 | 5.293 |
| 2 – Double caregiving no | 15.330 | 5.178 | ||||||
| 8 | Disillusion-fulfilment | 0.092 | 464 | 0.927 | 0.009 | 1 – Double caregiving yes | 14.094 | 4.285 |
| 2 – Double caregiving no | 14.057 | 4.345 | ||||||
| 9 | Career satisfaction | -0.927 | 464 | 0.354 | -0.087 | 1 – Double caregiving yes | 10.554 | 2.782 |
| 2 – Double caregiving no | 10.795 | 2.779 | ||||||
| 10 | Satisfaction with the job itself | 0.291 | 464 | 0.771 | 0.027 | 1 – Double caregiving yes | 20.411 | 7.628 |
| 2 – Double caregiving no | 20.208 | 7.317 | ||||||
| 11 | Satisfaction with the setting and the organizational Structure | -0.405 | 464 | 0.686 | -0.038 | 1 – Double caregiving yes | 15.916 | 5.685 |
| 2 – Double caregiving no | 16.125 | 5.408 | ||||||
| 12 | Satisfaction with organizational processes | -1.741 | 464 | 0.082 | -0.163 | 1 – Double caregiving yes | 13.302 | 4.897 |
| 2 – Double caregiving no | 14.125 | 5.177 | ||||||
| 13 | Satisfaction with interpersonal relationships | 0.002 | 464 | 0.999 | 0.001 | 1 – Double caregiving yes | 17.569 | 8.142 |
| 2 – Double caregiving no | 17.568 | 7.669 |
Table 4.
Centrality and Clustering Measures per Variable, Expressed as Standardized Z-Scores Values in Two Groups. (1—Double Caregiving “yes”; 2—Double Caregiving “no”)
Table 4.
Centrality and Clustering Measures per Variable, Expressed as Standardized Z-Scores Values in Two Groups. (1—Double Caregiving “yes”; 2—Double Caregiving “no”)
| 1 – Double caregiving yes | 2 – Double caregiving no | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Centrality | Clustering | Centrality | Clustering | ||||||||||
| Variable | Betweenness | Closeness | Strength | Expected influence | Zhang | Betweenness | Closeness | Strength | Expected influence | Zhang | |||
| 1 | Age | 1.853 | -0.484 | -0.165 | 0.646 | -1.705 | 1.572 | -0.752 | 0.022 | 0.910 | -1.280 | ||
| 2 | Seniority of service | -0.865 | -0.743 | -0.610 | 0.646 | -0.313 | -0.761 | -0.955 | -0.357 | 0.859 | -0.742 | ||
| 3 | Unused vacation days | 0.166 | -1.623 | -1.720 | -0.717 | -1.244 | 0.124 | -1.643 | -1.431 | -0.495 | -0.851 | ||
| 4 | Accumulated overtime hours | -0.865 | -2.097 | -2.123 | -0.923 | -1.820 | -0.761 | -1.927 | -2.015 | -1.130 | -1.577 | ||
| 5 | Psychophysical exhaustion-engagement | -0.584 | 0.977 | 0.963 | -0.550 | 0.128 | 0.124 | 0.762 | 0.778 | -0.320 | -0.528 | ||
| 6 | Relational deterioration-involvement | 2.134 | 1.051 | -0.283 | 0.025 | 0.636 | 1.814 | 0.996 | -0.994 | -1.721 | -0.327 | ||
| 7 | Professional inefficacy-efficacy | 0.072 | 0.754 | -0.228 | -0.580 | 0.744 | -0.681 | 0.602 | -0.473 | -0.260 | 0.525 | ||
| 8 | Disillusion-fulfilment | 0.541 | 1.039 | 0.681 | -0.705 | 0.108 | 1.572 | 1.136 | 0.808 | -0.802 | -0.353 | ||
| 9 | Career Satisfaction | -0.865 | 0.255 | 0.710 | 1.013 | 0.771 | -0.118 | 0.530 | 1.183 | 1.278 | 1.063 | ||
| 10 | Satisfaction with the job itself | -0.022 | 0.577 | 0.556 | -1.620 | -0.002 | -0.761 | 0.594 | 0.292 | -0.838 | 0.500 | ||
| 11 | Satisfaction with the setting and the organizational structure | -0.865 | 0.003 | 0.661 | 1.780 | 1.176 | -0.761 | -0.035 | 0.553 | 1.200 | 1.524 | ||
| 12 | Satisfaction with organizational processes | -0.584 | 0.015 | 1.048 | 1.317 | 0.674 | -0.761 | 0.417 | 1.107 | 1.156 | 1.113 | ||
| 13 | Satisfaction with interpersonal relationships | -0.115 | 0.277 | 0.511 | -0.331 | 0.848 | -0.600 | 0.274 | 0.527 | 0.163 | 0.934 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



