
Submitted:
31 October 2024
Posted:
04 November 2024
You are already at the latest version
Abstract
Background/Objectives: Chronic liver disease (CLD) is highly relevant in clinical practice due to its increasing incidence and associated mortality. We aimed to exhaustively characterize the multimorbidity in patients with CLD. Methods: Retrospective observational study of patients aged 18 years and older with a diagnosis of CLD in 2015 in the EpiChron Cohort (Spain). We analysed the prevalence of comorbidities according to sex and age, conducted a logistic regression analysis with CLD as the independent variable and each of the comorbidities as dependent variables to obtain odds ratios (OR) adjusted for age and sex, and performed an exploratory factor analysis to identify the presence of multimorbidity patterns. Results: 6836 adults had a diagnosis of CLD (mean age 61.6 years; 62.5% women), with an average of 13 co-existing chronic conditions. Arterial hypertension, lipid metabolism disorders, diabetes, obesity, and musculoskeletal diseases were the most frequent diseases. From the list of 110 chronic conditions analysed, 75 were systematically associated with CLD, including (OR, 95% confidence interval) chronic pancreatitis (41.2, 33.5-50.6), and inherited metabolic disorders (14.9, 11.8-18.8). Three multimorbidity patterns were identified in both men and women, and called cardiovascular, metabolic-geriatric, and mental-substance use, with some differences by sex. Conclusions: Multimorbidity is the norm in patients with CLD. Our results reveal that a comprehensive and integral approach based on person-centred care, which should take into account their entire spectrum of multimorbidity, is necessary during the care of this type of patients in clinical practice.
Keywords:
chronic liver disease
; multimorbidity
; comorbidity
; population-based study
1. Introduction
Chronic liver disease (CLD) is a common clinical condition consisting of a progressive deterioration of liver function related to a continuous process of inflammation, destruction and regeneration of the liver parenchyma [1]. This process can be due to a wide spectrum of etiologies including prolonged excessive alcohol consumption (alcoholic liver disease), metabolic alterations (non-alcoholic fatty liver disease), infections (chronic viral hepatitis), autoimmune diseases, genetic disorders, and hepatotoxic drugs, among others [2,3]. This severe damage causes the liver to lose its ability to repair itself, beginning with hepatosteatosis that leads to fibrosis, cirrhosis and, ultimately, the appearance of hepatocellular carcinoma [1,2].
Representing the fifth cause of death in the European Union, CLD is also responsible for high rates of disability and intensive use of healthcare services [3,4]. Its prevalence has experienced an increasing trend in recent decades. Approximately, 1.5 billion people suffer from CLD in the world [4,5], and its average prevalence in Europe is 0.83% [6]. According to data from the Global Burden of Disease Study, the age-standardized incidence rate of this disease was 20.7 cases per 100,000 inhabitants in 2015, which represents an increase of 13% since 2000 [4]. The epidemiology of CLD has undergone a change in recent years, reflecting, on the one hand, the implementation of large-scale hepatitis B vaccination and hepatitis C treatment programs and, on the other hand, the increasing prevalence of metabolic syndrome and excessive alcohol consumption [3].
The initial symptoms of CLD may initially be nonspecific, including fatigue, anorexia, and weight loss, or may manifest clinically with the development of complications such as esophageal varices, ascites, jaundice, hepatic encephalopathy, hepatorenal syndrome, hepatopulmonary syndrome, and coagulopathies [2,7]. Once diagnosed, the goal of CLD treatment is to stop disease progression and complications, which requires a multidisciplinary approach to correct the underlying cause, control portal hypertension, and treat individual signs of the disease. This requires a holistic and integrated approach by an interprofessional team including primary care physicians, specialists in gastroenterology, hepatology and nephrology, liver transplant teams if necessary, nutritionists to provide advice on diet, and social workers and community nurses [2].
The spectrum of symptoms and conditions of the patient with CLD is not limited to those caused by the disease itself; there may be many other coexisting diseases related to other pathophysiological mechanisms, both concordant and discordant. The coexistence of two or more chronic diseases in the same individual is known as multimorbidity [8]. Multimorbidity is currently the norm rather than the exception in clinical practices around the world, and it can result in interactions between diseases and between the drugs used to treat them, complicating the clinical management of chronic patients [9].
Comorbidity of CLD has already been studied in the literature; however, most studies focused on describing the specific comorbidities of some of the etiological diseases of CLD, such as alcoholic liver disease [10] and nonalcoholic fatty liver [11], or focus on its complications, such as ascites [12] and hepatocellular carcinoma [13]. Predictors of CLD have also been reported, including hypertension, insulin resistance, diabetes mellitus, and obesity. Most previous studies on the comorbidity of CLD were based on the calculation of disease prevalence rates or on regression models to calculate the likelihood of appearance of specific comorbidities based on the presence of CLD. No studies except for one has analyzed the existence of multimorbidity patterns in patients with CLD; however, it only focused on patients with hepatocellular carcinoma [13]. To the best of our knowledge, there is no study that has analyzed the complete multimorbidity spectrum of CLD as a whole.
The comprehensive analysis of multimorbidity in patients with CLD could help identify the most frequent and associated coexisting diseases, providing us with useful information for their early identification and diagnosis and even prevention, whereas the analysis of their multimorbidity patterns could help identify the profiles of patients susceptible to differentiated clinical management based on their specific pattern of coexisting diseases.
Our population study based on real-life data aimed to comprehensively analyze the comorbidity of CLD by means of the characterization of the most prevalent chronic comorbidities in these patients, the identification of those comorbidities systematically associated with CLD regardless of their prevalence, and the identification and clinical description of the existing multimorbidity patterns in patients with CLD.
2. Materials and Methods
2.1. Study Design and Population
We conducted a retrospective analytical observational study in the EpiChron Cohort, which integrates pseudonymized demographic and clinical information of all the users of the public health system of Aragón (Spain), who represent approximately 95% of its reference population (1.3 million inhabitants). The baseline characteristics of the EpiChron Cohort can be found elsewhere [14]. The conformation of this cohort for research on the epidemiology of multimorbidity and chronic diseases was favorably evaluated by the Research Ethics Committee of the Community of Aragón (CEICA; approval code PI17/0024). Given the epidemiological nature of the study, which used anonymized data that was presented only at an aggregate level, the obligation to obtain informed consent from the patients was waived by CEICA.
For this study, we selected as reference population all the people aged 18 years and older from the cohort who were registered as users of the public health system in 2015 and who were also registered during the previous year to have at least one year of complete information for their demographic and clinical characterization. Of these, we selected all the patients with a diagnosis of CLD recorded in their electronic health records for the study of their multimorbidity.
2.2. Variables and Data Sources
For all the patients included in the study, we analyzed their sex and age as of January 1, 2015, and all their chronic comorbidities registered in both primary and hospital care.
The diagnoses were initially coded using the International Classification of Primary Care, 1st edition (ICPC-1), in the case of primary care, and the International Classification of Diseases, 9th edition, Clinical Modification (ICD-9-CM), in the case of hospital care. We grouped these codes into broader mutually exclusive diagnostic categories called Expanded Diagnostic Clusters (EDCs) based on their clinical and diagnostic similarities using the Johns Hopkins Adjusted Clinical Groups (ACG®) [15]. The purpose of using this software was to transform the thousands of potential different codes into a more manageable list of 264 diagnoses that avoid duplicate diagnoses and facilitate the counting of diseases. From this list, only the 114 EDCs proposed as chronic in the study by Salisbury et al. [16] were taken into account. Chronic diseases were defined as those diseases that typically last six months or more, including past conditions that require current care, conditions with a high risk of recurrence, or past conditions that have ongoing implications for patient management. We grouped some diagnoses so that a total of 110 conditions were finally analyzed; the list of diseases used is presented as supplementary material (Table S1). Subjects with CLD were identified as those having the EDC code “GAS05: Chronic liver disease”.
All the information was gathered from patients’ electronic medical history of primary care, hospital discharge reports (through the Minimum Basic Data Set; CMBD), and clinical-administrative databases (user database, BDU).
3.3. Statistical Analysis
For the comprehensive analysis of the multimorbidity of patients with CLD, we conducted a three-phase analysis. First, we carried out a descriptive analysis of the demographic and clinical characteristics of the study population. For the identification of the most frequent comorbidities, we analyzed the prevalence of each comorbidity in the total population and stratified by sex and age (i.e., 18-44, 45-65, and >65 years), which was presented as frequencies and percentages.
Secondly, for the identification of those comorbidities systematically associated with CLD, we performed logistic regression models to calculate the risk of occurrence of each comorbidity (dependent variable) based on the presence or absence of CLD (independent variable). As a result, we obtained odds ratios (ORs) accompanied by their 95% confidence intervals (95% CI), which were calculated as unadjusted crude ORs and as age- and sex-adjusted ORs. For the comparison of adjusted ORs, we used the Bonferroni correction method for multiple comparisons (for a total of 85 disease comparisons with at least five cases in both men and women), establishing statistical significance at p <0.00059.
Finally, for the analysis of the existence of associations among diseases in the form of multimorbidity patterns in patients with CLD, we carried out an exploratory factor analysis. This technique allowed us to reduce the number of explanatory variables in the data set to a smaller number of latent variables, which can be interpreted as groups of variables (in our case diseases) that share a common underlying causal factor. This analysis was carried out in each sex and age group. To increase the clinical relevance of the results and facilitate their interpretation, we only included in the analysis those comorbidities with a prevalence greater than 5%. Each comorbidity was represented in the analysis as a binary variable indicating present (1) or absence (0), which allowed for the construction of a tetrachoric correlation matrix. To extract the factors, we used the main factor method, and to facilitate its interpretation, we applied an oblique rotation of the factors (Oblimin). To choose the number of factors (i.e., patterns) to extract, we used scree plots of the eigenvalues from the correlation matrix ordered in descending order. This visualization allowed us to identify the inflection point, which indicates the optimal number of factors to extract. This statistical criterion was accompanied by the clinical assessment of the different results.
In each pattern, we included those chronic diseases with a loading factor or factor score (a value that ranges between -1 and 1, representing the strength of association of each diagnosis within each pattern) equal to or greater than 0.30, allowing each disease to be in more than one pattern. To determine the degree of suitability of the sample to use factor analysis, we performed the Kaiser–Meyer–Olkin (KMO) test; the value of this parameter varies between 0 and 1, with values closer to 1 representing greater goodness of fit.
Once the patterns in each subpopulation were obtained, and to facilitate their clinical interpretation, we named the patterns based on the composition of diseases and the names already described in the bibliography with the help of two clinical care specialists in family and community medicine from the research group.
All statistical analyzes were carried out in Stata (Version 12.0, StataCorp LLC, College Station, TX, US) and R (Version 3.6.3, The R Foundation for Statistical Computing, Vienna, Austria).
3. Results
Of the 954,168 people aged 18 years or older in the EpiChron Cohort in 2015 (505,313 women and 448,855 men; mean age of 52.3 years), 6836 people had an active diagnosis of CLD in their electronic medical record (mean age of 61.6 years; 62.5% women; Table 1). These data translate into a prevalence of CLD in adults of 0.51% in women and 0.95% in men, 95% of cases accumulating in people over 40 years of age. Multimorbidity was present in 99% of people with CLD, who showed a high burden of comorbidity with an average of 13 chronic conditions.
3.1. Most Prevalent Chronic Conditions in Patients with CLD
Some cardiometabolic diseases such as arterial hypertension, lipid metabolism disorders, diabetes and obesity, and musculoskeletal diseases like arthritis were among the most frequent diseases in the population with CLD (Table 1). These conditions were also some of the most prevalent in the overall cohort. Although these diseases had a similar behavior in the different population groups studied, there were some relevant differences, such as the high prevalence of disorders related to substance use in men from an early age, as well as depression and cancer (Table 2).
3.2. Chronic Conditions Associated with the Presence of CLD
From the original list of 110 conditions analyzed, 75 were associated with CLD, being their prevalence higher than expected (Table 3). The most systematically associated comorbidity was chronic pancreatitis (adjusted OR 41.2), followed by inherited metabolic disorders, and hemophilia.
3.2. Multimorbidity Patterns in Patients with CLD
Regarding the exploratory factor analysis, unacceptable values below 0.50 were obtained for the KMO parameter in the different age and sex strata, indicating that these samples were not suitable for conducting an analysis of this type [17]. Moreover, the Heywood phenomenon occurred in some cases, which is sometimes related to the existence of collinearity between variables [18]. Consequently, we carried out the analyses stratified only by sex, so that multimorbidity patterns were determined in men and women, but not in the different age intervals. When the analyses were carried out stratified by sex this type of phenomenon did not occur, and acceptable sample adequacy indices were obtained (KMO of 0.76 in men and 0.65 in women).
To choose the number of patterns to extract in each analysis, we based our decision in the sedimentation graphs presented in Figure 1, in which the inflection point of the eigenvalues occurred between three and six factors in both sexes, but not in a clear way. Therefore, this criterion was complemented by the assessment of two clinicians of the team, who chose the optimal number of patterns based on the clinical interpretation of the different possible alternatives, always looking for the model with greater parsimony that explained the greatest degree of variance with the minimum number of variables.
Finally, we decided to extract three factors in each sex, resulting in three patterns of multimorbidity in both men (Figure 2) and women (Figure 3). These patterns were named Cardiovascular, Metabolic-Geriatric, and Mental-Substance use in both men and women, although they showed slight differences in their composition depending on sex.
The Cardiovascular pattern included cardiovascular diseases such as congestive heart failure, arrhythmia, anemia, and ischemic disease, as well as chronic obstructive pulmonary disease (COPD) and other respiratory disorders, and cerebrovascular disease. In the case of men, cancer was also added to this pattern.
The Metabolic-Geriatric pattern presented with chronic metabolic conditions such as diabetes, obesity, and lipid metabolism disorder (in men also gout), which were joined by conditions that seem more typical of advanced age like glaucoma, deafness, cataracts, and arthritis (also osteoporosis in women).
The Mental-substance use pattern was composed by substance use, depression, sleep disorders, and neuritis (also anxiety in women).
4. Discussion
In this study, we observed that multimorbidity is the norm rather than the exception in patients with CLD, which is frequently accompanied by other diseases, like arterial hypertension, lipid metabolism disorders, diabetes, obesity, and musculoskeletal diseases, with some relevant differences between sexes, such as the higher prevalence in men of disorders related to substance use from an early age, as well as of depression and cancer. This multimorbidity seems to cluster in three different multimorbidity patterns (Cardiovascular, Metabolic-Geriatric, and Mental-Substance use) in both men and women, although with slight differences in their composition depending on sex.
The prevalence rates of CLD obtained in our study are similar and consistent with the average prevalence of CLD described in the European Union, which is around 0.83% [6], and with the fact that excessive alcohol consumption, one of the most common etiologies of CLD, is more common in men than in women [19].
The prevalence rate of multimorbidity is higher than those observed in previous articles reporting multimorbidity rates of 80% and a lower number of comorbidities [11,20]; this is probably due to the fact that our study exhaustively analyzed all possible chronic conditions, and it was not based on a limited number of them. It has been demonstrated that the risk and severity of non-alcoholic liver disease increase with the number of components of metabolic syndrome present, and obesity is considered as the biggest risk factor for it [11]. Similar results were observed in people with non-alcoholic liver disease in Russia; almost 80% had at least two metabolic comorbidities, with the most common ones being overweight/ obesity (81%), hypercholesterolemia (75%), and type 2 diabetes (17%) [11]. In a population-based study in Sweden, high blood pressure was more prevalent (33%) than type 2 diabetes (29%) and obesity (24%). In the Manitoba Follow-up Study, hypertension, insulin resistance/ diabetes mellitus, and obesity were reported as greatest predictors of the appearance of CLD [21]. However, the majority of studies focused on describing the specific comorbidities of some of the etiological diseases of CLD, such as alcoholic liver disease [10] and nonalcoholic fatty liver [11], or on its complications, such as ascites [12] and hepatocellular carcinoma [13].
Surprisingly, 75 conditions of the original list of 110 were associated with CLD in our study, and their prevalence was higher than expected. This could be due to the multifactorial etiology of CLD and to the fact that the liver represents an important organ with many functions [2], whose alteration and damage could in turn be the cause of many other chronic disorders. In fact, among the conditions that showed a higher degree of association with CLD, we observed conditions that are both possible causes (e.g., inherited metabolic disorders, chronic viral infection, substance use, autoimmune diseases, diabetes, obesity [2,3]) and potential consequences (e.g., coagulation disorders, thrombosis, gastroesophageal reflux, chronic renal/respiratory failure) of CLD [2,22].
Although the relationship between CLD and comorbidities has been studied, there are not many studies that analyze the association of these comorbidities in the form of patterns. As well as we have observed the presence of three patterns, Mu et al. identified three main comorbidity patterns in patients with hepatocellular carcinoma, which included: 1) cirrhosis, hepatitis B, portal hypertension, and ascites; 2) hypertension, diabetes mellitus, coronary heart disease and cerebral infarction; and 3) hypoproteinemia, electrolyte disorders, gastrointestinal bleeding, and hemorrhagic anemia [13].
Of the three patterns analyzed, the Cardiovascular pattern has been widely described in the literature and is one of the most consistent in the general population [23,24]. Although it had not been specifically described in patients with CLD, it is one of the main cause of hospital admissions [12] and death in patients with non-alcoholic fatty liver disease [25,26]. In Germany, it was observed that among hospital admissions of CLD patients, diagnosis of respiratory diseases with infection had the highest mortality rate of 21.6% followed by cerebrovascular disease with a rate of 15.5% [12]. The development of these cardiovascular complications are related to obesity [12,25]. It is thought that the hyperdynamic circulation in cirrhosis provides some protection against overt heart failure, atherosclerosis, and ischemic events, but peripheral arterial disease, acute myocardial infarction, and heart failure were predictors of mortality in the CirCom study [22].
The Metabolic-Geriatric pattern is also one of the most consistently described in the general population [23], and in the specific case of CLD it makes sense that there is a profile of patients with this type of multimorbidity, since the metabolic syndrome and the disease of the associated fatty liver disease is one of the most common causes of CLD [11,27]. We observed that this pattern was mainly composed of obesity, diabetes and lipid metabolism disorder (due to low HDL and high triglycerides), that are considered metabolic risk factors of CLD, and diabetes is a predictor of severe outcomes [27]. Non-alcoholic fatty liver disease is recognized as the hepatic manifestation of the metabolic syndrome that represents a cluster of metabolic abnormalities, such as hyperlipidemia, glucose intolerance, obesity, and systemic hypertension [11], comorbidities that we found associated to CLD. The fact that this pattern is associated with geriatric or aging diseases could be due to the fact that older CLD patients are precisely those who have had this metabolic etiology, and not the one related to excessive consumption of alcohol and related factors that may cause these patients to have a lower life expectancy [28]. However, due to the technique used (factor analysis), which groups diseases and not people, it is not possible to know the average age of the patients of this multimorbidity pattern to corroborate this hypothesis.
The Mental-substance use pattern was composed by substance use, depression, sleep disorders, and neuritis has been previously described in the literature, but mainly in young and adult men, while in women a mental pattern with anxiety and depression is usually observed but not associated with substance use [23,24]. As in the previous case, this pattern of multimorbidity makes clinical sense since it would represent another of the most frequent etiologies of CLD: alcoholic liver disease due to excessive alcohol consumption [10,22]. Knowing that this pattern is also associated with problems such as depression and sleep disorders is important in order to characterize the specific needs of these patients [29] and proactively seek their appearance and diagnosis to prevent worsening health outcomes. In many cases, depression is associated to stigmatization in patients with liver disease, and it is associated to a lack of social support, and a decrease in the tendency to seek health care [29]. In the development of CirCom score, Jepsen et al. considered that mental disease could be a predictor of mortality due to its association with substance abuse and suicide risk, but they observed that schizophrenia was indeed an adverse prognostic factor, but depression and bipolar disorder were not associated with mortality [22]. They did not find other studies that have examined the prognostic impact of psychiatric diseases in cirrhosis [22].
The negatives outcomes of CLD patients are not only due to their comorbidities and clinical complexity, but also to biological (i.e., ageing, frailty, multimorbidity, mental disease, dependency, malnutrition) and non-biological (i.e., socioeconomic, behavioral, environmental, cultural) variables [30]. Lifestyle factors, including smoking, alcohol, physical inactivity, adiposity [26], and poor diet [25], played a key role in the incidence of CLD as well as to their complications. That is the reason why promotion of lifestyle interventions among CLD patients in early stage of disease course is necessary, in order to prevent cardiovascular risk factors [25], transitions to metabolic complications and death [26]. Also, social factors like limitations in daily living due to their disease, loneliness, low income, stigmatisation, and isolation, play an important role in the evolution of these disease decreasing the quality of life of these patients [29]. Patients highlighted the need for information to understand and manage CLD, and awareness and support from healthcare professionals to better cope with the disease [29]. An interprofessional team that provides a holistic and integrated approach is needed for a CLD patient to achieve the best possible outcomes. The earlier signs and symptoms of a complication are identified, the better is the prognosis and outcome [2].
One of the most important limitations of our study was related to its cross-sectional design, which did not allow the establishment of causal relationships between the existence of CLD and the comorbidities analyzed, nor to study the order of appearance or time of progression of the diseases within each multimorbidity pattern. Furthermore, it was not possible to analyze variables of interest for the interpretation of the results, such as the socioeconomic and educational level of the patients, genetic variables, or information on lifestyles (e.g., physical activity, consumption of alcohol, tobacco), which were not available in the EpiChron Cohort. On the other hand, the factor analysis presented limitations for the study of the different sex and age strata, and the analysis had to be done stratified only by sex. Lastly, given the multifactorial etiology of CLD, it would be interesting to carry out future studies that include various subanalyses according to the origin of the disease (e.g., alcoholism, fatty liver, viral infection) to know whether this influences the formation and composition of multimorbidity patterns.
One of the main strengths of this study lies in its population-based nature, since all cases of CLD in the reference population were analyzed. Furthermore, we exhaustively analysed the comorbidity of CLD based on the analysis of virtually all chronic diseases (and not only the most relevant or frequent ones) contained in the clinical history and recorded by a professional (and not self-referred by the patients or from surveys).
5. Conclusions
Multimorbidity is the norm in patients with CLD, who have indeed a huge disease burden. Our study revealed that, although the majority of the most prevalent diseases in these patients are also among the most prevalent in the general population, there are other diseases that, although much less prevalent, are systematically associated with CLD, such as chronic pancreatitis, coagulation disorders, and inherited metabolic disorders. Our study also revealed the existence of three differentiated multimorbidity patterns in women and men with CLD, named as cardiovascular, metabolic-geriatric, and mental-substance use. These results, which should be validated in other contexts, indicate that the care of these patients in clinical practice should follow a comprehensive and integral approach that takes into account all their comorbidity, in order to provide them with person-centred care instead of just disease-centred care.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: List of 110 chronic conditions or Expanded Diagnostic Clusters (EDC) included and analyzed in the study.
Author Contributions
Conceptualization, A.G.-M. and A.M.-J.; methodology, B.P.-P., C.L.-B., and A.G.-M.; software, B.P.P.; formal analysis, A.G.-M. and B.P.-P.; investigation, A.G.-M. and B.P.-P.; resources, A.G.-M.; data curation, B.P.-P. and C.L.-B.; writing—original draft preparation, A.M.-J. and A.G.-M.; writing—review and editing, B.P.-P., C.L.-B., B.C.-M, E. L., A.S.-M, L.G.-F.; visualization, A.G.-M.; supervision, A.G.-M.; project administration, A.M.-J.; funding acquisition, A.G.-M. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Carlos III Institute of Health, Ministry of Science and Innovation (Spain), through the Network for Research on Chronicity, Primary Care, and Health Promotion (RICAPPS), awarded for the call for the creation of Health Outcomes-Oriented Cooperative Research Networks (grant number RD21/0016/0019). This research was also funded by Gobierno de Aragón (grant number B01_23R) and funded by European Union’s Next Generation EU funds. The APC was funded by RICAPPS (RD21/0016/0019).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Clinical Research Ethics Committee of the Community of Aragón (CEICA; protocol code PI17/0024, approved on February 15, 2017).
Informed Consent Statement
Patient consent was waived by CEICA due to the epidemiological nature of the study, which used anonymized data that was presented only at an aggregate level.
Data Availability Statement
The data used in this study cannot be publicly shared because of restrictions imposed by the Aragon Health Sciences Institute (IACS) and asserted by the CEICA due to the existence of potentially identifying patient information. The authors who accessed the data received permission from IACS to utilize the data for this specific study, thus implying its exclusive use by the researchers appearing in the project protocol approved by the CEICA. Potential collaborations should be addressed to the Principal Investigator of the EpiChron Research Group, Antonio Gimeno-Miguel, at agimenomi.iacs@aragon.es. Requests for the data set used in this study should be addressed to CEICA at ceica@aragon.es.
Acknowledgments
The authors acknowledge the funding and support received by Institute of Health Carlos III (RD21/0016/0019) and Gobierno de Aragón (B01_23R).
Conflicts of Interest
The authors declare no conflicts of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- EuroStemCell. Enfermedad hepática crónica: ¿Cómo puede ayudar la medicina regenerativa? | Eurostemcell [Internet]. 2020 [cited 2022 Mar 20]. Available from: https://www.eurostemcell.org/es/enfermedad-hepatica-cronica-como-puede-ayudar-la-medicina-regenerativa.
- Sharma A, Nagalli S. Chronic Liver Disease. 2023 Jul 3. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan–.
- Moon AM, Singal AG, Tapper EB. Contemporary Epidemiology of Chronic Liver Disease and Cirrhosis. Clinical Gastroenterology and Hepatology. 2020;18:2650–66. [CrossRef]
- James SL, Abate D, Abate KH, Abay SM, Abbafati C, Abbasi N, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. The Lancet. 2018;392:1789–858. [CrossRef]
- Cheemerla S, Balakrishnan M. Global Epidemiology of Chronic Liver Disease. Clinical Liver Disease. 2021;17:365–70. [CrossRef]
- Pimpin L, Cortez-Pinto H, Negro F, Corbould E, Lazarus JV, Webber L, et al. Burden of liver disease in Europe: Epidemiology and analysis of risk factors to identify prevention policies. Journal of Hepatology. 2018;69:718–35. [CrossRef]
- Abbas Z, Shazi L. Pattern and profile of chronic liver disease in acute on chronic liver failure. Hepatol Int. 2015;9:366–72. [CrossRef]
- Van Den Akker M, Buntinx F, Knottnerus JA. Comorbidity or multimorbidity: what’s in a name? A review of literature. European Journal of General Practice. 1996;2:65–70. [CrossRef]
- Marengoni A, Onder G. Guidelines, polypharmacy, and drug-drug interactions in patients with multimorbidity. BMJ. 2015;350:h1059–h1059. [CrossRef]
- Grissa D, Nytoft Rasmussen D, Krag A, Brunak S, Juhl Jensen L. Alcoholic liver disease: A registry view on comorbidities and disease prediction. Rzhetsky A, editor. PLoS Comput Biol. 2020;16:e1008244. [CrossRef]
- Maev IV, Samsonov AA, Palgova LK, Pavlov CS, Shirokova E, Starostin KM. Real-world comorbidities and treatment patterns among patients with non-alcoholic fatty liver disease receiving phosphatidylcholine as adjunctive therapy in Russia. BMJ Open Gastroenterol. 2019;6:e000307. [CrossRef]
- Gu W, Hortlik H, Erasmus H-P, Schaaf L, Zeleke Y, Uschner FE, et al. Trends and the course of liver cirrhosis and its complications in Germany: Nationwide population-based study (2005 to 2018). The Lancet Regional Health - Europe. 2022;12:100240. [CrossRef]
- Mu X-M, Wang W, Jiang Y-Y, Feng J. Patterns of Comorbidity in Hepatocellular Carcinoma: A Network Perspective. IJERPH. 2020;17:3108. [CrossRef]
- Prados-Torres A, Poblador-Plou B, Gimeno-Miguel A, Calderón-Larrañaga A, Poncel-Falcó A, Gimeno-Feliú LA, et al. Cohort Profile: The Epidemiology of Chronic Diseases and Multimorbidity. The EpiChron Cohort Study. International Journal of Epidemiology. 2018;47:382–384e. [CrossRef]
- The Johns Hopkins University. Johns Hopkins ACG® System [Internet]. 2022 [cited 2022 Jul 25]. Available from: https://www.hopkinsacg.org/.
- Salisbury C, Johnson L, Purdy S, Valderas JM, Montgomery AA. Epidemiology and impact of multimorbidity in primary care: a retrospective cohort study. Br J Gen Pract. 2011;61:e12–21. [CrossRef]
- Dziuban CD, Shirkey EC. When is a correlation matrix appropriate for factor analysis? Some decision rules. Psychological Bulletin. 1974;81:358–61. [CrossRef]
- Cooperman AW, Waller NG. Heywood you go away! Examining causes, effects, and treatments for Heywood cases in exploratory factor analysis. Psychological Methods. 2022;27:156–76. [CrossRef]
- Mäkelä P, Gmel G, Grittner U, Kuendig H, Kuntsche S, Bloomfield K, et al. Drinking patterns and their gender differences in Europe. Alcohol and Alcoholism. 2006;41:i8–18. [CrossRef]
- Patel PJ, Hayward KL, Rudra R, Horsfall LU, Hossain F, Williams S, et al. Multimorbidity and polypharmacy in diabetic patients with NAFLD: Implications for disease severity and management. Medicine. 2017;96:e6761. [CrossRef]
- Uhanova J, O’Brien M, Minuk G, Tate R. Chronic Liver Disease and Metabolic Comorbidities in Healthy Young Males Followed for 65 Years: The Manitoba Follow-up Study. Clinical Gastroenterology and Hepatology. 2021;19:2417-2424.e2. [CrossRef]
- 22. Jepsen P. Comorbidity in cirrhosis. WJG. 2014;20:7223. [CrossRef]
- Prados-Torres A, Calderón-Larrañaga A, Hancco-Saavedra J, Poblador-Plou B, Van Den Akker M. Multimorbidity patterns: a systematic review. Journal of Clinical Epidemiology. 2014;67:254–66. [CrossRef]
- Ioakeim-Skoufa I, Poblador-Plou B, Carmona-Pírez J, Díez-Manglano J, Navickas R, Gimeno-Feliu LA, et al. Multimorbidity Patterns in the General Population: Results from the EpiChron Cohort Study. IJERPH. 2020;17:4242. [CrossRef]
- Colaci C, Gambardella ML, Maria Scarlata GG, Boccuto L, Colica C, Luzza F, et al. Dysmetabolic comorbidities and non-alcoholic fatty liver disease: a stairway to metabolic dysfunction-associated steatotic liver disease. Hepatoma Res. 2024;10:16. [CrossRef]
- Pang Y, Han Y, Yu C, Kartsonaki C, Guo Y, Chen Y, et al. The role of lifestyle factors on comorbidity of chronic liver disease and cardiometabolic disease in Chinese population: A prospective cohort study. The Lancet Regional Health - Western Pacific. 2022;28:100564. [CrossRef]
- Jarvis H, Craig D, Barker R, Spiers G, Stow D, Anstee QM, et al. Metabolic risk factors and incident advanced liver disease in non-alcoholic fatty liver disease (NAFLD): A systematic review and meta-analysis of population-based observational studies. Singal A, editor. PLoS Med. 2020;17:e1003100. [CrossRef]
- Morgan M. The prognosis and outcome of alcoholic liver disease. 1994;2:335–43.
- Grønkjær LL, Lauridsen MM. Quality of life and unmet needs in patients with chronic liver disease: A mixed-method systematic review. JHEP Reports. 2021;3:100370. [CrossRef]
- Lenti MV, Ballesio A, Croce G, Brera AS, Padovini L, Bertolino G, et al. Comorbidity and multimorbidity in patients with cirrhosis, hospitalised in an internal medicine ward: a monocentric, cross-sectional study. BMJ Open. 2024;14:e077576. [CrossRef]
Figure 1.
Scree plots used to determine the optimal number of factors (i.e., multimorbidity patterns) to extract in women and men with chronic liver disease. The inflection point of the curve indicates the approximate optimal number of factors to extract, a decision that was complemented by clinical judgment.
Figure 1.
Scree plots used to determine the optimal number of factors (i.e., multimorbidity patterns) to extract in women and men with chronic liver disease. The inflection point of the curve indicates the approximate optimal number of factors to extract, a decision that was complemented by clinical judgment.
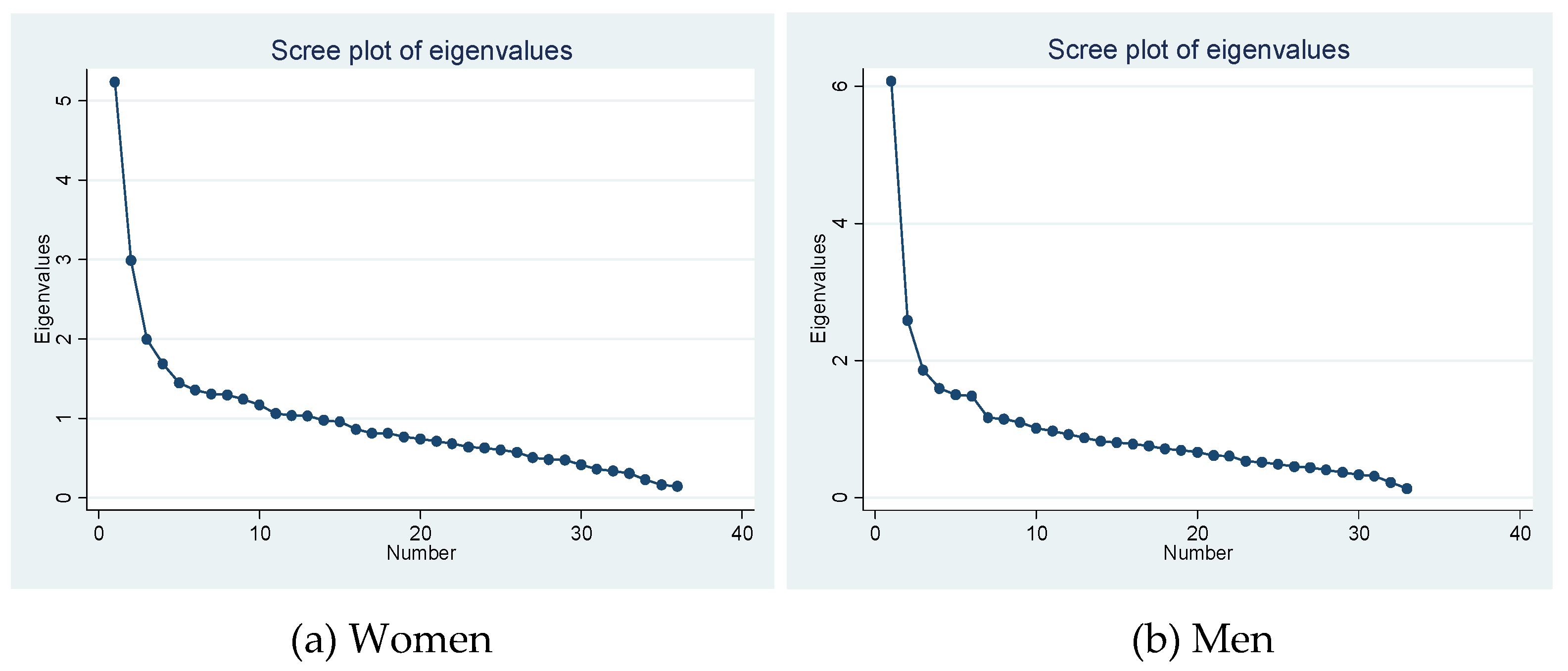
Figure 2.
Multimorbidity patterns in adult men with chronic liver disease in the EpiChron Cohort. COPD: Chronic obstructive pulmonary disease. Dis.: disorders. The Y axis represents the loading factor (between 0-1) of each disease within its respective pattern. Only those diseases with loading factors ≥0.30 are represented.
Figure 2.
Multimorbidity patterns in adult men with chronic liver disease in the EpiChron Cohort. COPD: Chronic obstructive pulmonary disease. Dis.: disorders. The Y axis represents the loading factor (between 0-1) of each disease within its respective pattern. Only those diseases with loading factors ≥0.30 are represented.
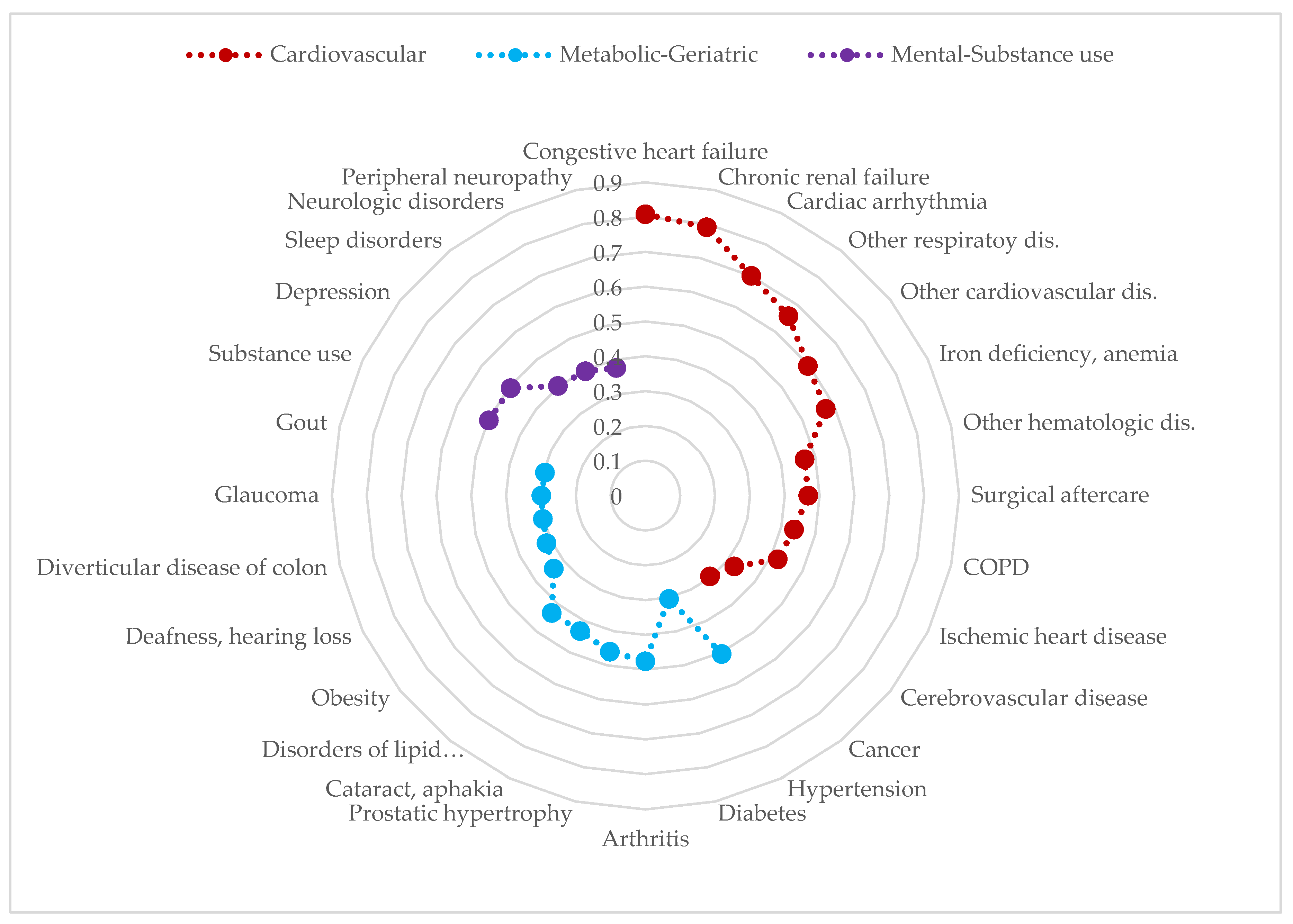
Figure 3.
Multimorbidity patterns in adult women with chronic liver disease in the EpiChron Cohort. COPD: Chronic obstructive pulmonary disease. Dis.: disorders. The Y axis represents the loading factor (between 0-1) of each disease within its respective pattern. Only those diseases with loading factors ≥0.30 are represented.
Figure 3.
Multimorbidity patterns in adult women with chronic liver disease in the EpiChron Cohort. COPD: Chronic obstructive pulmonary disease. Dis.: disorders. The Y axis represents the loading factor (between 0-1) of each disease within its respective pattern. Only those diseases with loading factors ≥0.30 are represented.
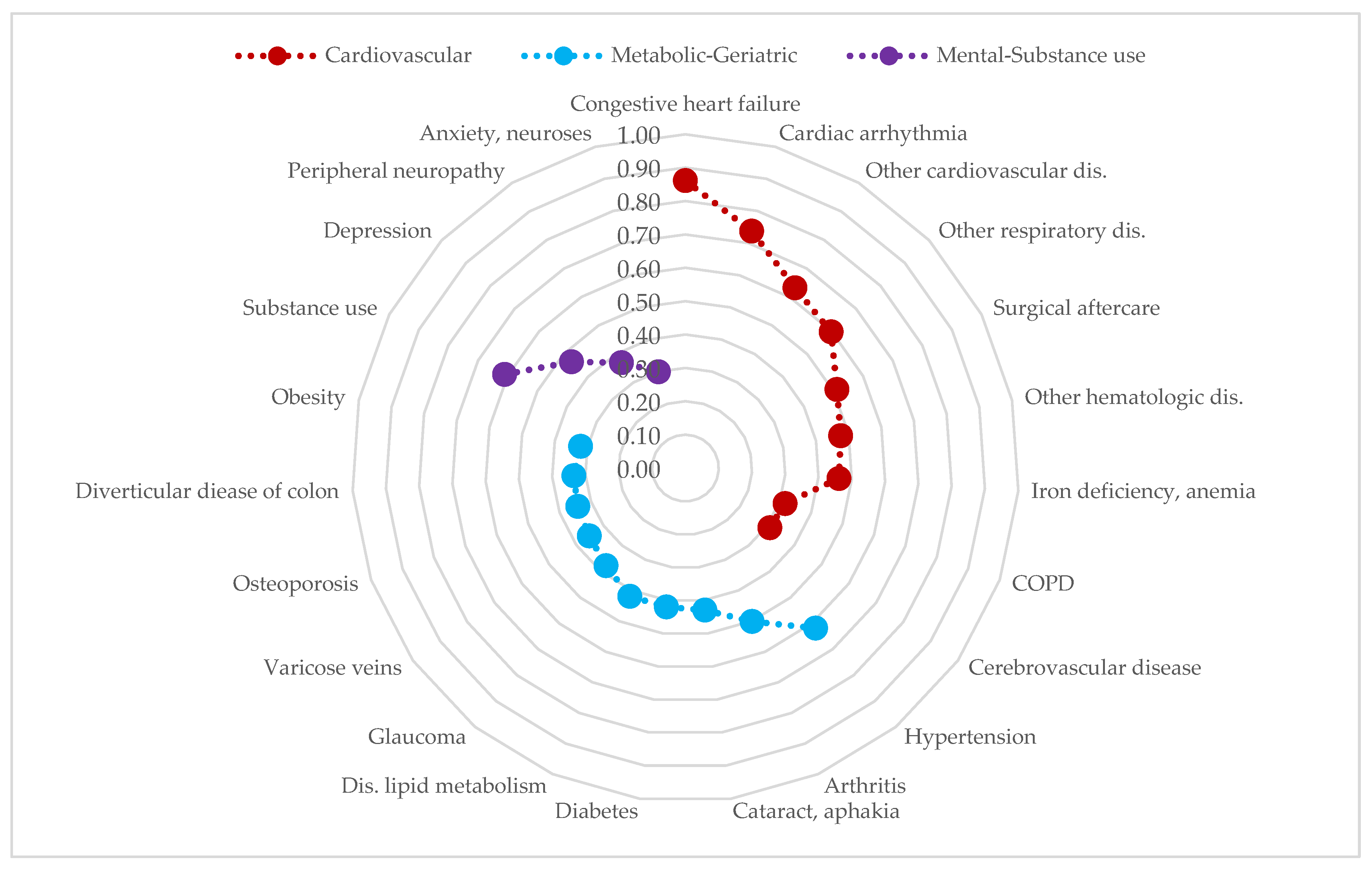

Table 1.
Demographic and clinical characteristics of the adult population with chronic liver disease in the EpiChron Cohort (Aragon, Spain).
Table 1.
Demographic and clinical characteristics of the adult population with chronic liver disease in the EpiChron Cohort (Aragon, Spain).
| Sex (n, %) | Women (2563; 37.5%) | Men (4273; 62.5%) | Total (6836; 100%) |
| Age (n, %) | |||
| 18-39 years | 142 (5.54) | 236 (5.52) | 378 (5.53) |
| 40-64 years | 1170 (45.7) | 2375 (55.6) | 3545 (51.9) |
| ≥65 years | 1251 (48.8) | 1662 (38.9) | 2913 (42.6) |
| Mean age (s.e1), years | 63.3 (0.29) | 60.6 (0.21) | 61.6 (0.17) |
| Multimorbidity2 (%) | 99.6 | 99.1 | 99.3 |
| Number of chronic diseases, mean (s.d.3) | 14.1 (7.31) | 12.5 (7.21) | 13.1 (7.29) |
| Most prevalent chronic diseases (EDC4, %) | Arterial hypertension (49.9) | Arterial hypertension (49.9) | Arterial hypertension (48.0) |
| Disorders of lipid metabolism (42.3) | Disorders of lipid metabolism (41.3) | Disorders of lipid metabolism (41.3) | |
| Arthritis (28.2) | Diabetes (28.8) | Diabetes (26.9) | |
| Varicose veins (26.9) | Substance abuse (24.3) | Obesity (19.7) | |
| Depression (24.7) | Obesity (17.6) | Arthritis (19.1) | |
| Diabetes (24.1) | Cancer (17.5) | Substance abuse (17.6) | |
| Obesity (23.4) | COPD5 (14.6) | Depression (16.5) | |
| Osteoporosis (19.0) | Arthritis (13.7) | Cancer (16.0) | |
| Iron deficiency, anemia (17.4) | Cardiac arrhythmia (13.3) | Varicose veins (15.2) | |
| Hypothyroidism (16.3) | Iron deficiency, anemia (12.7) | Iron deficiency, anemia (14.4) |
1 Standard error; 2 Defined as the presence of two or more chronic diseases, including chronic liver disease; 3 Standard deviation; 4 Expanded Diagnostic Clusters; 5 Chronic obstructive pulmonary disease.
Table 2.
Prevalence of the most common chronic comorbidities in adult patients with chronic liver disease in the EpiChron Cohort stratified by sex and age.
Table 2.
Prevalence of the most common chronic comorbidities in adult patients with chronic liver disease in the EpiChron Cohort stratified by sex and age.
| Women aged 18-39 years (n=142) | Men aged 18-39 years (n=236) | |||||
| Mean number of chronic diseases: 9.2 | Mean number of chronic diseases: 7.3 | |||||
| EDC1 | Comorbidity | N (%) | EDC | Comorbidity | N (%) | |
| CAR11 | Dis.2 of lipid metabolism | 27 (19.0) | CAR11 | Dis. of lipid metabolism | 61 (25.7) | |
| NUT03 | Obesity | 21 (14.8) | PSY02 | Substance use | 38 (16.0) | |
| SKN02 | Dermatitis and eczema | 21 (14.8) | NUT03 | Obesity | 37 (15.6) | |
| HEM02 | Iron deficiency, anemia | 20 (14.1) | ALL03 | Allergic rhinitis | 34 (14.3) | |
| ALL03 | Allergic rhinitis | 18 (12.7) | SKN02 | Dermatitis and eczema | 30 (12.6) | |
| END05 | Other endocrine dis. | 18 (12.7) | ASMA | Asthma | 24 (10.1) | |
| PSY01 | Anxiety, neuroses | 17 (12.0) | DIAB | Diabetes | 20 (8.44) | |
| SKN13 | Disease of hair | 15 (10.6) | HTA | Arterial hypertension | 18 (7.59) | |
| END04 | Hypothyroidism | 14 (9.86) | MUS14 | Low back pain | 18 (7.59) | |
| MUS14 | Low back pain | 14 (9.86) | PSY09 | Depression | 13 (5.48) | |
| Women aged 40-64 years (n=1170) | Men aged 40-64 years (n=2375) | |||||
| Mean number of chronic diseases: 12.2 | Mean number of chronic diseases: 11.1 | |||||
| EDC | Comorbidity | N (%) | EDC | Comorbidity | N (%) | |
| CAR11 | Dis. of lipid metabolism | 482 (41.2) | CAR11 | Dis. of lipid metabolism | 989 (41.6) | |
| HTA | Arterial hypertension | 366 (31.3) | HTA | Arterial hypertension | 934 (39.3) | |
| NUT03 | Obesity | 282 (24.1) | PSY02 | Substance use | 722 (30.4) | |
| PSY09 | Depression | 280 (23.9) | DIAB | Diabetes | 561 (23.6) | |
| GSU08 | Varicose veins | 275 (23.5) | NUT03 | Obesity | 419 (17.6) | |
| MUS03 | Arthritis | 208 (17.8) | PSY09 | Depression | 315 (13.3) | |
| DIAB | Diabetes | 190 (16.2) | CANCER | Cancer | 274 (11.5) | |
| END04 | Hypothyroidism | 188 (16.1) | SKN02 | Dermatitis and eczema | 259 (10.9) | |
| PSY19 | Sleep disorders | 164 (14.0) | PSY19 | Sleep disorders | 258 (10.8) | |
| END05 | Other endocrine dis. | 158 (13.5) | RES04 | COPD3 | 248 (10.4) | |
| Women aged ≥65 years (n=1251) | Men aged ≥65 years (n=1662) | |||||
| Mean number of chronic diseases: 16.5 | Mean number of chronic diseases: 15.4 | |||||
| EDC | Comorbidity | N (%) | EDC | Comorbidity | N (%) | |
| HTA | Arterial hypertension | 908 (72.5) | HTA | Arterial hypertension | 1059 (63.7) | |
| CAR11 | Dis. of lipid metabolism | 574 (45.8) | CAR11 | Dis. of lipid metabolism | 714 (43.0) | |
| MUS03 | Arthritis | 512 (40.9) | DIAB | Diabetes | 649 (39.0) | |
| DIAB | Diabetes | 417 (33.3) | CANCER | Cancer | 470 (28.3) | |
| GSU08 | Varicose veins | 402 (32.1) | GUR04 | Prostatic hypertrophy | 414 (24.9) | |
| END02 | Osteoporosis | 362 (28.9) | CAR09 | Cardiac arrhythmia | 405 (24.4) | |
| PSY09 | Depression | 339 (27.1) | MUS03 | Arthritis | 374 (22.5) | |
| NUT03 | Obesity | 294 (23.5) | RES04 | COPD | 374 (22.5) | |
| HEM02 | Iron deficiency, anemia | 285 (22.8) | HEM02 | Iron deficiency, anemia | 326 (19.6) | |
| EYE06 | Cataract, aphakia | 266 (21.2) | ADM02 | Surgical aftercare | 315 (19.0) | |
1 Expanded Diagnostic Clusters, 2 Disorder, 3 Chronic Obstructive Pulmonary Disease.
Table 3.
Chronic diseases systematically associated with the presence of chronic liver disease in the adult population of the EpiChron Cohort.
Table 3.
Chronic diseases systematically associated with the presence of chronic liver disease in the adult population of the EpiChron Cohort.
| EDC1 | Comorbidity | Crude OR2 (95% CI)3 |
p value | Adjusted OR4 (95% CI) |
p value |
|---|---|---|---|---|---|
| GAS12 | Chronic pancreatitis | 66.1 (53.9-81.0) | <0.001 | 41.2 (33.5-50.6) | <0.00001 |
| GTC02 | Inherited metabolic disorders | 22.9 (18.2-28.8) | <0.001 | 14.9 (11.8-18.8) | <0.00001 |
| HEM07 | Hemophilia, coagulation disorder | 21.6 (17.0-27.5) | <0.001 | 14.0 (11.0-17.9) | <0.00001 |
| HEM06 | Deep vein thrombosis | 21.4 (16.8-27.3) | <0.001 | 13.4 (10.5-17.1) | <0.00001 |
| INF04 | HIV5 | 14.4 (12.4-16.7) | <0.001 | 13.3 (11.4-15.4) | <0.00001 |
| CAR10 | Generalized atherosclerosis | 20.1 (17.1-23.6) | <0.001 | 12.2 (10.3-14.4) | <0.00001 |
| PSY13 | Adjustment disorder | 14.0 (10.4-18.9) | <0.001 | 11.0 (8.14-14.9) | <0.00001 |
| PSY02 | Substance use | 13.9 (13.1-14.8) | <0.001 | 10.6 (9.93-11.3) | <0.00001 |
| GAS08 | Gastroesophageal reflux | 15.1 (13.4-17.1) | <0.001 | 10.0 (8.85-11.3) | <0.00001 |
| RHU01 | Autoimmune, connective tissue dis. | 12.5 (10.0-15.6) | <0.001 | 8.55 (6.84-10.7) | <0.00001 |
| REN01 | Chronic renal failure | 10.8 (9.68-12.0) | <0.001 | 7.74 (6.91-8.67) | <0.00001 |
| PSY20 | Major depression | 7.38 (5.14-10.6) | <0.001 | 7.01 (4.87-10.1) | <0.00001 |
| CAR07 | Cardiomyopathy | 11.7 (9.46-14.5) | <0.001 | 6.66 (5.37-8.26) | <0.00001 |
| RES13 | Chronic respiratory failure | 10.3 (8.09-13.1) | <0.001 | 6.40 (5.02-8.15) | <0.00001 |
| RES06 | Sleep apnea | 10.3 (8.79-12.1) | <0.001 | 6.17 (5.25-7.25) | <0.00001 |
| ADM02 | Surgical aftercare | 8.97 (8.34-9.66) | <0.001 | 6.02 (5.58-6.49) | <0.00001 |
| REN06 | End stage renal disease | 9.78 (6.80-14.1) | <0.001 | 5.67 (3.94-8.16) | <0.00001 |
| RES11 | Respiratory disorders, other | 7.22 (6.65-7.84) | <0.001 | 4.55 (4.19-4.95) | <0.00001 |
| ALL06 | Disorders of the immune system | 6.02 (5.22-6.94) | <0.001 | 4.36 (3.78-5.03) | <0.00001 |
| NUR17 | Paralytic syndromes, other | 6.60 (5.13-8.48) | <0.001 | 4.10 (3.18-5.27) | <0.00001 |
| CAR05 | Congestive heart failure | 5.24 (4.80-5.72) | <0.001 | 3.86 (3.52-4.25) | <0.00001 |
| GSU15 | Alimentary, excretory surgic. openings | 6.44 (4.59-9.03) | <0.001 | 3.77 (2.69-5.30) | <0.00001 |
| REN04 | Nephritis, nephrosis | 5.18 (4.09-6.56) | <0.001 | 3.74 (2.95-4.74) | <0.00001 |
| RHU03 | Arthropathy | 5.74 (3.68-8.98) | <0.001 | 3.71 (2.37-5.80) | <0.00001 |
| REN05 | Renal disorders, other | 5.08 (4.22-6.11) | <0.001 | 3.66 (3.04-4.40) | <0.00001 |
| PSY08 | Personality disorders | 3.42 (2.81-4.16) | <0.001 | 3.34 (2.75-4.07) | <0.00001 |
| CAR16 | Cardiovascular disorders, other | 5.06 (4.69-5.47) | <0.001 | 3.22 (2.98-3.48) | <0.00001 |
| GAS10 | Diverticular disease of colon | 4.72 (4.27-5.22) | <0.001 | 3.18 (2.87-3.52) | <0.00001 |
| HEM02 | Iron deficiency, anemias | 3.68 (3.44-3.94) | <0.001 | 3.08 (2.87-3.30) | <0.00001 |
| HEM08 | Hematologic disorders, other | 4.54 (4.20-4.90) | <0.001 | 2.93 (2.70-3.17) | <0.00001 |
| CAR06 | Cardiac valve disorders | 4.42 (3.94-4.97) | <0.001 | 2.87 (2.55-3.24) | <0.00001 |
| INF01 | Tuberculosis infection | 3.09 (2.56-3.73) | <0.001 | 2.83 (2.34-3.42) | <0.00001 |
| DIAB | Diabetes | 4.31 (4.08-4.55) | <0.001 | 2.72 (2.57-2.88) | <0.00001 |
| EYE13 | Diabetic retinopathy | 4.24 (3.58-5.01) | <0.001 | 2.69 (2.27-3.18) | <0.00001 |
| GSU11 | Peripheral vascular disease | 4.50 (3.80-5.32) | <0.001 | 2.62 (2.21-3.10) | <0.00001 |
| RES04 | COPD6 | 4.34 (4.03-4.68) | <0.001 | 2.54 (2.34-2.74) | <0.00001 |
| CAR09 | Cardiac arrhythmia | 3.75 (3.49-4.04) | <0.001 | 2.38 (2.21-2.57) | <0.00001 |
| REC03 | Chronic ulcer of the skin | 3.37 (2.99-3.79) | <0.001 | 2.31 (2.04-2.61) | <0.00001 |
| NUR07 | Seizure disorder | 2.64 (2.27-3.07) | <0.001 | 2.28 (1.96-2.65) | <0.00001 |
| EYE03 | Retinal disorders (excl. diabetic retinopathy) | 3.20 (2.08-4.93) | <0.001 | 2.21 (1.43-3.41) | 0.00033 |
| CANCER | Cancer | 3.26 (3.06-3.48) | <0.001 | 2.09 (1.96-2.24) | <0.00001 |
| GUR09 | Renal calculi | 2.91 (2.58-3.29) | <0.001 | 1.99 (1.76-2.25) | <0.00001 |
| NUT03 | Obesity | 2.62 (2.46-2.78) | <0.001 | 1.99 (1.87-2.11) | <0.00001 |
| HEM01 | Hemolytic anemia | 1.82 (1.32-2.52) | 0.00030 | 1.90 (1.37-2.63) | 0.00012 |
| NUR21 | Neurologic disorders, other | 2.47 (2.27-2.68) | <0.001 | 1.86 (1.71-2.03) | <0.00001 |
| NUR03 | Peripheral neuropathy, neuritis | 2.14 (1.94-2.36) | <0.001 | 1.85 (1.68-2.04) | <0.00001 |
| NUR19 | Developmental disorder | 0.85 (0.64-1.13) | 0.272 | 1.85 (1.38-2.47) | 0.00003 |
| GAS02 | Inflammatory bowel disease | 2.25 (1.78-2.85) | <0.001 | 1.80 (1.42-2.28) | <0.00001 |
| HTA | Hypertension | 3.27 (3.11-3.43) | <0.001 | 1.79 (1.70-1.89) | <0.00001 |
| RHU02 | Gout | 3.38 (3.05-3.75) | <0.001 | 1.77 (1.59-1.97) | <0.00001 |
| RES08 | Pulmonary embolism | 2.71 (2.04-3.60) | <0.001 | 1.76 (1.32-2.33) | 0.00010 |
| GAS09 | Irritable bowel syndrome | 2.05 (1.77-2.37) | <0.001 | 1.69 (1.46-1.96) | <0.00001 |
| MUS14 | Low back pain | 2.11 (1.95-2.29) | <0.001 | 1.68 (1.55-1.83) | <0.00001 |
| HEM03 | Thrombophlebitis | 2.33 (2.06-2.64) | <0.001 | 1.66 (1.47-1.89) | <0.00001 |
| PSY01 | Anxiety, neuroses | 1.73 (1.57-1.91) | <0.001 | 1.64 (1.48-1.82) | <0.00001 |
| PSY09 | Depression | 2.02 (1.90-2.16) | <0.001 | 1.64 (1.53-1.75) | <0.00001 |
| NUR24 | Dementia | 2.00 (1.73-2.32) | <0.001 | 1.58 (1.36-1.85) | <0.00001 |
| IHD | Ischemic heart disease | 2.74 (2.50-3.00) | <0.001 | 1.55 (1.41-1.70) | <0.00001 |
| END04 | Hypothyroidism | 1.63 (1.50-1.77) | <0.001 | 1.54 (1.41-1.68) | <0.00001 |
| END02 | Osteoporosis | 1.74 (1.60-1.89) | <0.001 | 1.50 (1.37-1.65) | <0.00001 |
| END05 | Other endocrine disorders | 1.57 (1.44-1.72) | <0.001 | 1.50 (1.38-1.64) | <0.00001 |
| PSY07 | Schizophrenia, affective psychosis | 1.90 (1.59-2.25) | <0.001 | 1.50 (1.26-1.78) | <0.00001 |
| NUR05 | Cerebrovascular disease | 2.24 (2.02-2.48) | <0.001 | 1.39 (1.25-1.54) | <0.00001 |
| MUS13 | Cervical pain syndromes | 1.67 (1.45-1.92) | <0.001 | 1.35 (1.17-1.56) | 0.00003 |
| PSY19 | Sleep disorders | 1.88 (1.75-2.02) | <0.001 | 1.35 (1.26-1.45) | <0.00001 |
| SKN12 | Psoriasis | 1.71 (1.51-1.94) | <0.001 | 1.34 (1.18-1.52) | <0.00001 |
| GSU08 | Varicose veins of lower extremities | 1.58 (1.48-1.68) | <0.001 | 1.30 (1.21-1.40) | <0.00001 |
| CAR11 | Disorders of lipid metabolism | 2.25 (2.14-2.36) | <0.001 | 1.27 (1.21-1.34) | <0.00001 |
| SKN02 | Dermatitis and eczema | 0.89 (0.82-0.96) | 0.00168 | 1.23 (1.14-1.33) | <0.00001 |
| EYE06 | Cataract, aphakia | 1.84 (1.70-1.99) | <0.001 | 1.17 (1.07-1.27) | 0.00029 |
| MUS03 | Arthritis | 1.82 (1.71-1.93) | <0.001 | 1.17 (1.10-1.25) | <0.00001 |
1 Expanded Diagnostic Cluster; 2 Non-adjusted Odds ratios; 3 95% confidence interval; 4 Age- and sex-adjusted Odds ratios; 5 Human immunodeficiency virus; 6 Chronic Obstructive Pulmonary Disease. Only those comorbidities with a statistically significant age- and sex-adjusted Odds ratio are presented in the table ordered from highest to lowest based on the value of the Odds ratio.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



