
Submitted:
02 November 2024
Posted:
05 November 2024
You are already at the latest version
Abstract
Congenital heart defects (CHD) are the most common congenital defect, occurring in approximately 1 in 100 live births and being a leading cause of perinatal morbidity and mortality. Of note, approximately 25% of these defects are classified as critical, requiring immediate postnatal care by pediatric cardiology and neonatal cardiac surgery teams. Consequently, early and accurate diagnosis of CHD is key to proper prenatal and postnatal monitoring in a tertiary care setting. In this scenario, fetal echocardiography is considered the gold standard imaging ultrasound method for the diagnosis of CHD. However, the availability of this examination in clinical practice remains limited due to the requirement for a qualified specialist in pediatric cardiology. Moreover, in light of the relatively low prevalence of CHD among at-risk populations (approximately 10%), ultrasound cardiac screening for potential cardiac anomalies during routine second-trimester obstetric ultrasound scans represents a pivotal aspect of diagnosing CHD. In order to maximize the accuracy of CHD diagnosis, the views of the ventricular outflow tract and the superior mediastinum were added to the four-chamber view of the fetal heart for routine ultrasound screening according to international guidelines. In this context, four-dimensional spatio-temporal image correlation software (4D-STIC) were developed in the beginning 2000s. Some of the advantages of 4D-STIC in fetal cardiac evaluation include the enrichment of anatomical details of fetal cardiac images in the absence of the pregnant woman and the ability to send volumes for analysis by an expert in fetal cardiology by an internet link. Sequentially, new technologies have been developed such as Fetal Intelligent Navigation Echocardiography (FINE), also known as "5D-heart", in which the nine fetal cardiac views recommended during a fetal echocardiogram are automatically generated from the acquisition of a cardiac volume. Furthermore, artificial intelligence (AI) has recently emerged as a promising technological innovation, offering the potential to warn of possible cardiac anomalies and thus increase the ability of non-cardiology specialists to the diagnose of CHD. In the early 2010s, the advent of 3D reconstruction software combined with high-definition printers enabled virtual and 3D physical reconstruction of the fetal heart. The 3D physical models may improve parental counseling of fetal CHD, maternal-fetal interaction in cases of blind pregnant women, and interactive discussion by multidisciplinary health teams. In addition, the 3D physical and virtual models can be an useful tool for teaching of cardiovascular anatomy and to optimize surgical planning, enabling simulation rooms for surgical procedures. Therefore, in this review the authors discuss advanced image technologies aiming that may optimize the prenatal diagnosis of CHD.
Keywords:
Fetal heart
; Congenital heart disease
; Ultrasonography
; Three-dimensional ultrasound
; Spatiotemporal Image Correlation
; Fetal Intelligent Navigation Echocardiography
; Artificial Intelligence
1. Introduction
Congenital heart defects (CHD) are the most frequent congenital malformations with an incidence of approximately 6-12:1000 live births [1,2,3,4]. Concerning mortality due to congenital defects, it is important to bear in mind that this is one of the main causes of perinatal mortality [5]. However, the rate of prenatal diagnosis of CHD remains low. It is known that more than 25% of CHD are classified as critical, which means that these cardiac defects will require immediate care in the postpartum period by pediatric cardiology teams and surgery or a neonatal cardiac surgical procedure [6]. Therefore, early and accurate diagnosis of CHD is essential for proper prenatal and birth follow-up in a tertiary service.
The gold standard method for diagnosing CHD is fetal echocardiography [7]. This examination is carried out in few centers due to the need for trained professionals and high-tech equipment. Furthermore, since only 10% of CHD come from high-risk groups, being crucial the screening during second trimester ultrasound scan. Currently, with the addition of the ventricular outflow tracts and the superior mediastinum (three-vessels and three vessels and trachea) views to the four-chamber view, has improved the accuracy of screening for CHD by almost 90% [7,8]. Despite the potential benefits of echocardiography in diagnosing CHD, the requirement for a qualified professional and high-tech equipment currently precludes its routine implementation in clinical practice. Accordingly, the majority of international guidelines advocate the referral of pregnant women for fetal echocardiography, contingent upon the risk profile of the population in light of the available evidence [9].
The advent of three-dimensional (3D) ultrasound in the early 1990s, and in particular, the four-dimensional (4D) spatio-temporal image correlation (STIC) software in the early 2000s, marked a significant turning point in the field of fetal imaging. This has enabled significant technological advancement in fetal heart assessment, particularly in the identification of atrioventricular and semilunar valve regions, as well as the delineation of interatrial and interventricular septum areas and volumes, cardiac chambers, and ventricular walls [10,11,12,13,14]. The advantages of STIC in fetal cardiac assessment include a reduced dependence on the operator's experience in obtaining diagnostic plans, a shorter examination time with the analysis of volumes conducted in the absence of the patient, and the capacity to transmit volumes for analysis to reference centers in fetal cardiology via an internet link [15]. It is possible to "navigate" within the cardiac structures by moving from one plane to another, thus enabling the cardiac anatomy to be detailed and diagnoses regarding cardiac malformations to be clarified [16,17,18].
In the early 2010s, the advent of 3D reconstruction software, coupled with the advent of high-definition printers, enabled the virtual and physical reconstruction of fetuses, as well as virtual navigation of fetal cavities using 3D ultrasound and magnetic resonance imaging (MRI) data. This has facilitated realistic visualizations of structures such as the upper airways in cases of cervical tumors, the urinary tract in cases of lower obstructions, and central nervous system malformations [19,20,21]. Furthermore, the use of physical 3D models has facilitated enhanced maternal-fetal interaction in cases of blind pregnancies, as well as more comprehensive parental understanding of fetal pathologies and interactive discussion by multidisciplinary medical teams [22,23]. With regard to the fetal heart, due to its specific aspect of movement, magnetic resonance imaging (MRI) data acquisition is still of low resolution, and 3D ultrasound using STIC software is still the preferred method.
The 3D physical model realistically reconstructs the 3D ultrasound image, providing a better understanding of fetal heart disease for parents [24,25]. Most CHD require immediate care in the postpartum period by a team of specialists, so that an early and accurate diagnosis permits the formulation of an appropriate birth plan and, in cases of critical heart disease, facilitates the referral of the pregnant woman to a center with specialized cardiac team resources for prenatal care and scheduled delivery. This approach has the potential to reduce morbidity and mortality. The utilization of physical and virtual 3D reconstructions facilitates comprehensive visualization of cardiac anatomy and morphology, facilitating interactive discourse between the multidisciplinary team (obstetricians, neonatologists, pediatric cardiologists, cardiac surgeons, specialist nurses) and enhanced comprehension of the anomaly by the parents [26,27,28].
Despite an increase in the number of ultrasound view included in the screening process for CHD, the prenatal diagnosis of cardiac malformations remains inadequate. This is due to the limited access to high-quality ultrasound images and the interpretation of images obtained by non-specialists, particularly in cases of high complexity. The recent developments in fetal heart imaging technologies and artificial intelligence (AI) have the potential to enhance the prenatal detection of CHD [29,30]. This review article will provide an overview of several of these imaging technologies.
2. Three-Dimensional Ultrasound and Saptiotemporal Image Correlation
The advent of fetal echocardiography approximately forty years ago has facilitated the study of embryonic development, morphology, biometry and fetal heart function. Since 2003, the 4D ultrasound with spatial-temporal image correlation (STIC) has enabled detailed digital assessment of the fetal heart. The STIC technology, initially described by De Vore et al. [10], enables the acquisition of cardiac volumes using a volumetric transducer over a single scan period of 7.5 to 15 seconds, with the acquisition of 150 images per second. The reconstruction of these images in 3D, correlated to time (STIC), allows the image of the fetal heart in motion to be presented with high definition (cinellop). This technology allows navigation through the valves, cavities, and vessels of the fetal heart, thereby facilitating the anatomical and functional detailed examination of the fetal heart [10,31]. Although the methodology is already familiar to practitioners, it is important to reiterate that in order to obtain high-quality cardiac volumes from the images used for the study of the fetal heart with STIC, it is recommended that the fetal spine be positioned at 6 o'clock (posterior dorsum) with an opening angle between 20o and 40o [32]. Therefore, unfavorable fetal statics, such as an anterior fetal dorsum and fetal movement during examination, can limit the accuracy of the image and pose a challenge to this technology, in a similar manner to two-dimensional (2D) ultrasound [33].
Furthermore, the assessment of cardiac volumes by STIC may be conducted with or without the patient (offline), as well as via the internet to tertiary centers (tele-STIC). Consequently, this technology has the potential to maximize cardiac screening by enabling remote access to fetal heart experts, thereby reducing costs and shortening distances. Fetal telemedicine has shown that it can improve prenatal parental counseling and cardiac screening by tele-medicine assisted or via a telemedicine link [34,35].
In this scenario, it is essential to highlight that 3D/4D spectral tissue imaging by reproducing a complete cardiac cycle allows the examiner in multiplanar and rendering modes to select the optimal image quality and observe detailed morphological and functional aspects of the fetal heart [36,37]. Additionally, the examiner has the option of transmitting the selected images to the experts via the Internet and being viable for obstetric ultrasound cardiac screening programs even by assisted ultrasound scanning of fetal heart [34,35,38,39].
By adjusting the brightness and color, STIC in rendering mode facilitates enhanced image clarity, thus enabling diagnoses of structural CHD, the measurement of area and volume of various fetal heart structures, including the interventricular septum, valves, and papillary muscles (Figure 1), and the assessment of cardiac function in fetuses at risk of heart failure (Figure 2) [14,40,41]. STIC technology is capable of reconstructing moving images and displaying them in a variety of modes, including STIC-M, inversion mode, Doppler (color Doppler/HDlive flow), B-flow, tomographic ultrasound imaging (TUI), HDlive Silhouette mode (Figure 3, Figure 4, Figure 5 and Figure 6) [42,43,44,45].
Advanced technologies have the potential to elucidate complex CHD such as anomalous venous return, vascular rings, heterotaxy syndromes, and conotruncal anomalies. These imaging techniques can provide a more realistic appearance of the cardiac structures, which is an invaluable asset in the diagnosis and management of these conditions [46,47,48,49]. An accurate fetal cardiac diagnosis will have a significant impact on a number of medical areas, including decision-making and/or cardiac surgical procedures in utero or postnatally, improved birth planning, parental counseling, and, in countries where it is permitted by law, the decision to terminate pregnancies in a safer and less traumatic manner [9,33].
Anomalous pulmonary venous return, in either its total or partial forms (Figure 7), is frequently misdiagnosed during the prenatal period. In this scenario, advanced fetal cardiovascular imaging technologies are useful tools for providing high-quality images with greater definition of the venous vessel walls and, consequently, of the drainage site as well as points of obstruction. Underdiagnosis of total anomalous pulmonary venous return (TAPVR) affects postnatal outcome, especially in obstructive forms (critical TAPVR), in which planned delivery and perinatal management are crucial to providing a better outcome [47,50,51]. Similarly, some umbilical vein anomalies (such as the agenesis of the ductus venosus and the persistence of the right umbilical vein) as well as systemic venous return anomalies (such as the agenesis of the portal vein and the interruption of the inferior vena cava) can be more accurately identified by 3D high-definition Doppler ultrasound. One of the most frequently encountered anomalies of the inferior vena cava (IVC) is the interruption of its intrahepatic segment at the suprarenal level. In such cases, the IVC flow typically returns to the right atrium via the azygos vein (or hemiazygos vein), which is associated with left heterotaxy or left atrial isomerism (also known as two morphologically left atria) (Figure 8) [46,52].
In general, persistence of the right umbilical vein (PRUV) is a benign anatomic variant, however, it could be associated with cardiac and extra cardiac anomalies (trisomy 18, monosomy X, genitourinary and central nervous system anomalies, septal and conotruncal anomalies) [53,54]. Extra-hepatic forms of PRUV are associated with agenesis of ductus venosus (ADV) and a poor prognosis [55]. In Indeed, ADV is associated with cardiac and extracardiac malformations, requiring a rigorous examination of the fetal anatomy and comprehensive testing for chromosomal anomalies, including trisomies 13, 21, 18, and monosomy X. The extrahepatic form of ADV is associated with a poorer prognosis and an elevated risk of hydrops [56,57]. In this scenario, the use of 3D color Doppler is beneficial for illustrating the spatial course of the vessels and the absence of flow through the DV (Figure 9). This can assist in predicting prognosis, identifying associated malformations, and providing parental guidance.
The advantages of 3D/4D ultrasound in the diagnosis of conotruncal anomalies, including simple transposition of the great arteries (TGA), aortic arch interruption, and double Taussig-Bing type right ventricle outflow tract, have been well-documented in the literature (Figure 10 and Figure 11) [58,59,60,61]. The automatic reconstruction of the outflow tracts from a 4D cardiac volume acquired from a standard four-chamber view facilitates the enhancement of the images of the ventricular outflow tracts, thereby improving the diagnostic accuracy. Moreover, TUI, inversion mode, HDlive Silhouette, HDlive flow, MV-Flow, LuminiFlow and other advanced imaging technologies utilizing 3D ultrasound have the capacity to enhance visualization of the outflow tracts, thereby facilitating a more accurate diagnosis of TGA (Figure 12). These tools allow for a more efficient examination and facilitates the reconstruction of the great arteries [58,59,60,61]. In cases of TGA with progression to restriction of the foramen ovale (FO), it may be necessary to perform an in utero opening of the foramen ovale and/or urgent postnatal ballon atrioseptostomy. Maximum velocity of pulmonary vein (a wave), FO flap mobility and FO diameter are important parameters to perform this evaluation [62]. Measurements of the area of the interatrial septum using 4D ultrasound with STIC have been performed in normal fetuses with the construction of reference curves, however the applicability in fetuses with CHD has not yet been validated (Figure 13) [63]. Future directions using these measurements in STIC to evaluate restrictive FO may be promising.
The most noteworthy distinction between Ebstein's anomaly (EA) and tricuspid dysplasia (TD) pertains to the anatomical characteristics of the tricuspid valve. In EA, the tricuspid valve cusps are attached to the right ventricular myocardium, resulting in a displacement of the usual tricuspid valve plane and atrialization of right ventricle. Conversely, in TD, the cusps are inserted normally at the level of the valve annulus, and regurgitation is caused by dysplasia with varying degrees of cusps deformation. Tricuspid regurgitation (TR) exists in EA and TD and in fetuses with severe TR, an increase in right ventricle pressure is observed with pulmonary insufficiency and progression to circular shunting. In these cases, blood circulates through the arterial ductus instead of going to the fetal body and placenta (Figure 14). The maternal use of anti-inflammatory drugs (indomethacin and/or ibuprofen) between 20 and 34 weeks has been shown to reduce mortality in EA and TD [64].
Regarding to vascular anomalies, STIC navigation with HDlive Silhouette, the post-processing inversion mode, high-resolution color Doppler such as HDlive flow, and Luminiflow techniques enable the detailed reconstruction of aortic and ductal arches with realistic images (Figure 15). In this scenario, anomalies of the laterality of the aortic arch and anomalies of the origin of the vessels and anomalies of the vascular ring can be more easily clarified (Video S1) [65,66,67,68].
Although cardiac tumors are rare, they can cause hemodynamic repercussions when there is obstruction to flow. Among fetal cardiac tumors, rhabdomyoma is the most prevalent. It is estimated that over 80% of rhabdomyomas are associated with tuberous sclerosis, which is linked to mutations in the TSC1 and TSC2 genes. These genes stimulate the production of hamartin and tuberin, thereby stimulating tumor proliferation. In cases of large masses with flow obstruction, myocardial dysfunction, and arrhythmias in fetuses that are not yet viable, some groups have been using mTOR inhibitors (Sirolimus) from 23 to 35 weeks of gestation with success [69,70,71]. Teratomas represent 15% of fetal cardiac tumors and are most frequently intrapericardial. They have the potential to grow rapidly and may be associated with large pericardial effusions, which can result in fetal hydrops [72]. In such cases, mortality is high, and aspiration of the pericardial effusion in utero is a crucial procedure. In this scenario, 3D ultrasound is particularly useful tool for identifying the type of tumor (Figure 16).
The cardiovascular score, which is based on a variety of parameters obtained from 2D Doppler ultrasound, enables the assessment of fetuses who are at risk of developing heart failure. Nevertheless, at the initial stages of myocardial dysfunction or even to provide detailed cardiac function assessment, 4D ultrasound with STIC can assist in the evaluation of STIC-M, tricuspid annular plane systolic excursion (TAPSE) and mitral annular plane systolic excursion (MAPSE), which are parameters that assess systolic dysfunction at an earlier stage than the filling fraction or the calculation of ejection fraction by virtual organ computer-aided analysis (VOCAL) (Figure 17 and Figure 18 / Videos S2 and S3). This can be beneficial in cases of diabetic fetuses, fetuses with vascular malformations such as Galen, tumors, as well as other conditions. Therefore, functional parameters (stroke volume, cardiac output and ejection fraction) can be assessed using the STIC with VOCAL. Each ventricular volume is measured at the end of diastole (maximum volume) and at the end of systole (minimum volume). The caliper is positioned inside the basal and apical ventricular regions. After six sequential plans, manually delineated for each ventricle, VOCAL provides the chamber volume and reconstructs its 3D image. Finally, stroke volume, cardiac output and ventricular ejection fraction values are calculated for each ventricle [73,74,75,76,77].
3. Fetal Intelligent Navigation Echocardiography (Fine) and Artificial Intelligence
The Fetal Intelligent Navigation Echocardiography (FINE) technique, referred to as “5D-Heart”, comprises the automated reconstruction of the 9 planes that have been standardized by fetal echocardiography. This is achieved by marking strategic cardiac anatomical points from the four-chamber view of the fetal heart. The software utilizes intelligent navigation to direct the examiner in the marking of seven points (the descending aorta, crux cordis, pulmonary valve, superior vena cava and transverse aorta) and subsequently, the 9 fetal echocardiography views are reproduced in sequence [78,79,80]. The FINE technique comprises the automated reconstruction of the 9 planes that have been standardized by fetal echocardiography. This is achieved by marking strategic cardiac anatomical points from the four-chamber view of the fetal heart (Figure 19). The software utilizes intelligent navigation to direct the examiner in the marking of seven points (the descending aorta, crux cordis, pulmonary valve, superior vena cava and transverse aorta) and subsequently, the nine fetal echocardiography views are reproduced in sequence. The diagnostic views and VIS-Assistance videoclips can be transmitted to experts in fetal cardiology [78,79,80,81].
Automatic applications including structure identification, automated measurements and providing alerts on probable diagnoses was added to the FINE technology. This recent AI software, designated HeartAssistTM (Samsung Co., Seoul, South Korea) is capable of recognize fetal heart structures and perform automatic (anatomical and functional) measurements, reducing examination time and minimizing measurement errors related to operator-examinator variations (Figure 20) [82,83,84].
The evidence concerning the potential benefits of AI in fetal cardiac ultrasound assessment, as demonstrated by HeartAssistTM, is encouraging. The current focus within the field of AI is the development of automated techniques for the detection of specific types of CHD, such as hypoplastic left heart syndrome, atrioventricular septal defect and tetralogy of Fallot (TOF). To exemplify, in TOF, fetuses with a pulmonary valve Z-score of less than -5.0 and a Z-score difference between the pulmonary and aortic valves of >5 have an increased risk of pulmonary flow dependence on ductal arch flow [85]. The measurements could be plotted in fetal Z scores against gestational age, biparietal diameter and femur length, helping us to categorize the diameters of the pulmonary valve and arteries.
Automating the measurement of cardiac structures using AI during the screening process provides an objective approach that can be performed in busy clinical environments, reduces operator variability and extends fetal heart screening by enabling non-specialists to be alerted to malformations. HeartAssistTM method is a potential method for automated fetal cardiac structure measurement. The establishment of reference curves of automated Z-scores of the fetal heart obtained by AI represents an encouraging avenue of research and the development of these automated techniques remains a work in progress [86].
4. Three-Dimensional Physical and Virtual Models of the Fetal Heart
The 4D ultrasound with STIC software provides the acquisition of cardiac volumes in multiplanar and rendering modes, enabling the offline navigation through the structures of the fetal heart. Physical and virtual 3D reconstruction of the fetal heart can be created from 3D ultrasound volumes (Figure 21 and Figure 22). This technology facilitates a more complete understanding of the anatomical changes associated with CHD, provides a platform for interactive discussion between the multidisciplinary medical team [87,88].
After acquire images of the fetal heart from 3D ultrasound (heart volumes), using tools from the Slicer 3D (Birmingham, UK) software, we may create different masks on each image in a sequence. Each mask corresponds to a particular structure. For example, a blue mask delineates a cavity or vessel within the fetus, thus defining the boundaries between structures. The program identifies all pixels in the sequence with a shade between the two values and selects them by creating an overlapping mask and assigning a color to each cardiac chamber or vessel. Once the segmentation is completed and the structures are properly separated in the masks, we proceed to generate the 3D physical model. From the 3D data generated, 3D physical models of the fetal heart can be printed on 3D printers [26].
In the process of creating virtual models of the fetal body, the 3D ultrasound or MRI mages of the fetal heart are exported to a 3D virtual navigation software named Elucis (Elucis software, Realize Medical, Ottawa, Canada). During the rendering process, the software calculates the lighting and shading effects according to the color and shape of the model, saving the images produced throughout the process (30 images for every second of movement). The aforementioned images will be employed to structure the navigation video and will be saved as an MP4 video [28].
The creation of 3D physical models of CHD can facilitate the enhancement of anatomical detail and contribute to the accuracy of diagnostic procedures. In addition, the use of 3D physical models can facilitate parental counselling, and may enhance therapeutic planning of cardiac diseases by a multidisciplinary team as it provides a more comprehensive understanding of the CHD [89,90,91]. Moreover, these 3D resin models can be employed in classes of cardiac anatomy. Virtual navigation has been utilized in other medical specialties for surgical training, and in fetal cardiology, it represents a promising tool due to its capacity to facilitate the training and planning of postnatal surgical procedures in virtual simulation rooms [27].
The utilization of virtual simulation rooms facilitates the participation of experts and students from disparate geographical locations, thereby reducing the physical distances that would otherwise be traversed. In this way, surgical procedures can be trained by the team before being actually performed, and a more experienced medical team can assist remotely [92].
5. Fetal Cardiac Magnetic Resonance Imaging
Fetal cardiac MRI is still limited by high fetal heart rates and the small size of fetal heart structures. The time required for the examination is also a limitation for the pregnant woman. On the other hand, unfavorable fetal statics is a major limitation for ultrasound, but not for MRI [93].
MRI is also capable of non-invasively assessing oxygenation through the calculation of both oxygen saturation and the hematocrit of the blood within a vessel, utilizing the T1 and T2 relaxation times. Fetal cardiac MRI has yielded significant insights into the circulatory systems. Fetal cardiac MRI may be useful when conventional fetal echocardiography is inconclusive, especially in vascular malformations, such as vascular rings, aortic anomalies and arteriovenous malformations (Galeno vein aneurism, coronary fistulas, hemangiomas) [94,95,96]. Fast sequences such as single-shot T2-weighted turbo spinecho (TSE) MR with half-Fourier reconstruction and steadystate free precession (SSFP) are the most used sequences for the assessment of fetal heart [97]. Bright-blood SSFP sequences provide optimal contrast between the cavities blood and myocardium [98] (Figure 24).
A study evaluated the clinical utility of fetal cardiac MRI in cases where conventional fetal echocardiography did not visualize all anatomic structures. Of a total of 31 fetuses, fetal cardiac MRI was helpful in management and/or parental counseling in 26 cases (84%). For aortic arch anatomy including signs of coarctation (20 cases), fetal cardiac MRI added diagnostic information in 16 cases (80%). In 4 fetuses with hypoplastic left heart syndrome (HLHS), fetal cardiac MRI helped delivery planning in 3 cases (75%) [99].
In a retrospective cohort study involving 431 singleton pregnancies (62 fetuses with CHD and 269 healthy fetuses), MRI cardiac axes were measured in both CHD and normal fetuses. The authors observed a good inter- and intraobserver reproducibility of fetal cardiac axes measured by echocardiography and MRI [100]. In other study, the authors assessed the contribution of fetal cardiac MRI to identify cardiovascular anomalies in fetuses with CHD. The authors identified 73 (60.3%) of cardiovascular anomalies in 31 fetuses with CHD. Fetal echocardiography was more sensitive for diagnosing cardiovascular anomalies compared to fetal MRI, but without significant differences [101].
A cohort study involving 13 fetuses (24 – 36 weeks of gestation) with CHD evaluated the image quality for slice-to-volume reconstruction of 4D balanced steady-state free precession (bSSFP) imaging of the fetal heart. Two radiologists evaluated slice-to-volume reconstruction image quality on a scale from 0 to 4 using 11 categories based on a segmental approach to defining cardiac anatomy and pathology. In 11 out of 13 cases, the average radiologist score of image quality across all categories was ≥ 3.0 [102] (Figure 25).
6. Conclusions
The application of advanced imaging techniques facilitates the acquisition of images with greater clarity, enabling the delineation or clarification of anatomical structures and the navigation of cardiac structures and vessels in real time and offline. Furthermore, these techniques can assist in the screening of CHD by non-specialists in fetal cardiology. In this scenario, the incorporation of advanced technology into the 2D ultrasound images of the fetal heart can enhance the prenatal detection of CHD. Automated measurements of the anatomical and functional structures of the fetal heart can reduce operator-dependent discrepancies. In addition to measurements, AI can assist in the identification of potential cardiovascular alterations. The prospective applications of 3D physical and virtual models of fetal cardiac structures and functions are promising tools for perinatal management of cardiovascular diseases.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Video S1. Sagittal view of aortic arch using STIC with Doppler in a case of coarctation of aorta. Observe the narrowing of the aortic isthmus. Video S2. How to obtain the measurement of mitral annular plane systolic excursion (MAPSE) using fetal STIC-M. Video S3. How to measure left ventricle (LV) systolic volume using STIC with virtual organ computer-aided analysis (VOCAL). The caliper is positioned inside the basal and apical ventricular regions. After six sequential plans, manually delineated for LV, VOCAL provides the ventricular chamber volume. Indeed, the stroke volume (SV), cardiac output (CO) and ejection fraction (EF) can be calculated for each ventricle by the measurement of the ventricular volume at the end of diastole and at the end of systole. Video S4. Virtual navigation in a case of transposition of the great arteries.
Acknowledgments
We acknowledge the financial support from Elucis software (Realize Medical, Ottawa Canada) which enable the process of printing 3D virtual models of fetal heart.
References
- Liu Y, Chen S, Zühlke L, Black GC, Choy MK, Li N; et al. Global birth prevalence of congenital heart defects 1970-2017: Updated systematic review and meta-analysis of 260 studies. Int J Epidemiol. 2019, 48, 455–463.
- Bouma BJ, Mulder BJ. Changing Landscape of Congenital Heart Disease. Circ Res. 2017, 120, 908–922.
- Hoffman JIE. The global burden of congenital heart disease. Cardiovasc J Afr. 2013, 24, 141–145.
- Khasawneh W, Hakim F, Abu Ras O, Hejazi Y, Abu-Aqoulah A. Incidence and patterns of congenital heart disease among Jordanian infants, a cohort study from a university tertiary center. Front Pediatr. 2020, 8, 219.
- Meller CH, Grinenco S, Aiello H, Córdoba A, Sáenz-Tejeira MM, Marantz P; et al. Congenital heart disease, prenatal diagnosis and management. Arch Argent Pediatr. 2020, 118, e149–e161.
- Oster ME, Lee KA, Honein MA, Riehle-Colarusso T, Shin M, Correa A. Temporal trends in survival among infants with critical congenital heart defects. Pediatrics. 2013, 131, e1502–e1508.
- Carvalho JS, Axt-Fliedner R, Chaoui R, Copel JA, Cuneo BF, Goff D; et al. ISUOG Practice Guidelines (updated): Fetal cardiac screening. Ultrasound Obstet Gynecol. 2023, 61, 788–803.
- Chaoui, R. The four-chamber view: Four reasons why it seems to fail in screening for cardiac abnormalities and suggestions to improve detection rate. Ultrasound Obstet Gynecol. 2003, 22, 3–10. [Google Scholar] [CrossRef]
- Donofrio MT, Moon-Grady AJ, Hornberger LK, Copel JA, Sklansky MS, Abuhamad A; et al. Diagnosis and treatment of fetal cardiac disease: A scientific statement from the American Heart Association. Circulation. 2014, 129, 2183–2242.
- Devore GR, Falkensammer P, Sklansky MS, Platt LD. Spatio-temporal image correlation (STIC): New technology for evaluation of the fetal heart. Ultrasound Obstet Gynecol. 2003, 22, 380–387.
- Vinãls F, Poblete P, Giuliano A. Spatio-temporal image correlation (STIC): A new tool for the prenatal screening of congenital heart defects. Ultrasound Obstet Gynecol. 2003, 22, 388–394.
- Gonçalves LF, Lee W, Chaiworapongsa T, Espinoza J, Schoen ML, Falkensammer P. Four-dimensional ultrasonography of the fetal heart with spatiotemporal image correlation. Am J Obstet Gynecol. 2003, 189, 1792–1802.
- Yagel S, Benachi A, Bonnet D, Dumez Y, Hochner-Celnikier D, Cohen SM; et al. Rendering in fetal cardiac scanning: The intracardiac septa and the coronal atrioventricular valve planes. Ultrasound Obstet Gynecol. 2006, 28, 266–274.
- Nardozza LM, Rolo LC, Araujo Júnior E, Hatanaka AR, Rocha LA, Simioni C; et al. Reference range for fetal interventricular septum area by means of four-dimensional ultrasonography using spatiotemporal image correlation. Fetal Diagn Ther. 2013, 33, 110–115.
- Vinãls F, Mandujano L, Vargas G, Giuliano A. Prenatal diagnosis of congenital heart disease using four-dimensional spatio-temporal image correlation (STIC) telemedicine via an Internet link: A pilot study. Ultrasound Obstet Gynecol. 2005, 25, 25–31.
- Espinoza J, Gonçalves LF, Lee W, Mazor M, Romero R. A novel method to improve prenatal venous connections using three- and four-dimensional ultrasonography and “inversion mode”. Ultrasound Obstet Gynecol. 2005, 25, 428–434.
- Liu J, Wang Y, Zhao H, Liu W. Spatio-temporal image correlation rendering mode visualizes the specific location and surrounding structure of ventricular septal defect. Clin Anat. 2019, 32, 408–420.
- Malho A, Ximenes RS, Bravo-Valenzuela NJ, Araujo Júnior E. Spatio-Temporal Image Correlation: Three-Dimensional Imaging for Fetal Cardiac Screening and Congenital Heart Disease Assessment. Arq Bras Cardiol. 2024;121(4):e20230580.
- Werner H, Lopes dos Santos JR, Fontes R, Belmonte S, Daltro P, Gasparetto E; et al. Virtual bronchoscopy for evaluating cervical tumors of the fetus. Ultrasound Obstet Gynecol. 2013, 41, 90–94.
- Werner H, Lopes J, Ribeiro G, Jésus NR, Santos GR, Alexandria HAF; et al. Three-dimensional virtual cystoscopy: Noninvasive approach for the assessment of urinary tract in fetuses with lower urinary tract obstruction. Prenat Diagn. 2017, 37, 1350–1352.
- Werner H, Ribeiro G, Lopes J, Sá RAM, Maia F, Castro P; et al. Virtual navigation for the improvement of parents counseling and the planning of fetal endoscopic myelomeningocele repair. Childs Nerv Syst. 2021, 37, 969–972.
- Werner H, Lopes J, Tonni G, Araujo Júnior E. Maternal-fetal attachment in blind women using physical model from three-dimensional ultrasound and magnetic resonance scan data: Six serious cases. J Matern Fetal Neonatal Med. 2016, 29, 2229–2232.
- Werner H, Castro P, Lopes J, Ribeiro G, Araujo Júnior E. Maternal-fetal physical model: Image fusion obtained by white light scanner and magnetic resonance imaging. J Matern Fetal Neonatal Med. 2022, 35, 4427–4430.
- Veronese P, Bertelli F, Cattapan C, Andolfatto M, Gervasi MT, Vida VL. Three-Dimensional Printing of Fetal Heart With d-Transposition of the Great Arteries From Ultrasound Imaging Data. World J Pediatr Congenit Heart Surg. 2021, 12, 291–292.
- Huang J, Shi H, Chen Q, Hu J, Zhang Y, Song H; et al. Three-Dimensional Printed Model Fabrication and Effectiveness Evaluation in Fetuses With Congenital Heart Disease or With a Normal Heart. J Ultrasound Med. 2021, 40, 15–28.
- Werner H, Lopes J, Ribeiro G, Raposo AB, Trajano E, Araujo Júnior E. Three-dimensional virtual traveling navigation and three-dimensional printing models of a normal fetal heart using ultrasonography data. Prenat Diagn. 2019, 39, 175–177.
- Bravo-Valenzuela NJ, Monteiro Pereira Leite MF, Lopes J, Arcoverde V, Ribeiro G, Araujo Júnior E; et al. Three-dimensional navigation inside a normal fetal heart in a virtual reality environment. J Clin Ultrasound. 2024 Aug 21. [CrossRef]
- Giffoni MC, Lopes J, Ribeiro G, Araujo Júnior E, Werner H. Fetal heart segmentation in a virtual reality environment. Int J Cardiovasc Imaging. 2024 Jun 4. [CrossRef]
- Taksøe-Vester CA, Mikolaj K, Petersen OBB, Vejlstrup NG, Christensen AN, Feragen A; et al. Role of artificial-intelligence-assisted automated cardiac biometrics in prenatal screening for coarctation of aorta. Ultrasound Obstet Gynecol. 2024, 64, 36–43.
- Pietrolucci ME, Maqina P, Mappa I, Marra MC, D' Antonio F, Rizzo G. Evaluation of an artificial intelligent algorithm (Heartassist™) to automatically assess the quality of second trimester cardiac views: A prospective study. J Perinat Med. 2023, 51, 920–924.
- Bennasar M, Martinez JM, Gomez O, Bartrons J, Olivella A, Puerto B; et al. Accuracy of four-dimensional spatiotemporal image correlation echocardiography in the prenatal diagnosis of congenital heart defects. Ultrasound Obstet Gynecol. 2010, 36, 458–464.
- Gonçalves LF, Espinoza J, Lee W, Nien K, Hong JS, Santolaya-Forgas J; et al. A new approach to fetal echocardiography: Digital casts of the fetal cardiac chambers and great vessels for detection of congenital heart disease. J Ultrasound Med. 2005, 24, 415–424.
- Barber N, Freud L. Advances in Fetal Cardiac Imaging and Intervention. CJC Pediatr Congenit Heart Dis. 2023, 3, 33–42.
- Vinãls F, Ascenzo R, Naveas R, Huggon I, Giuliano A. Fetal echocardiography at 11 + 0 to 13 + 6 weeks using four-dimensional spatiotemporal image correlation telemedicine via an Internet link: A pilot study. Ultrasound Obstet Gynecol. 2008, 31, 633–638.
- Sharma S, Parness IA, Kamenir SA, Ko H, Haddow S, Steinberg LG; et al. Screening fetal echocardiography by telemedicine: Efficacy and community acceptance. J Am Soc Echocardiogr. 2003(3):202-8.
- Yeo L, Romero R, Jodicke C, Kim SK, Gonzalez JM, Oggè G; et al. Simple targeted arterial rendering (STAR) technique: A novel and simple method to visualize the fetal cardiac outflow tracts. Ultrasound Obstet Gynecol 2011, 37, 549–556.
- Rocha LA, Rolo LC, Barros FS, Nardozza LM, Moron AF, Araujo Júnior E. Assessment of Quality of Fetal Heart Views by 3D/4D Ultrasonography Using Spatio-Temporal Image Correlation in the Second and Third Trimesters of Pregnancy. Echocardiography. 2015, 32, 1015–1021.
- Espinoza J, Lee W, Comstock C, Romero R, Yeo L, Rizzo G; et al. Collaborative study on 4-dimensional echocardiography for the diagnosis of fetal heart defects: The COFEHD study. J Ultrasound Med. 2010, 29, 1573–1580.
- Adriaanse BM, Tromp CH, Simpson JM, Van Mieghem T, Kist WJ, Kuik DJ; et al. Interobserver agreement in detailed prenatal diagnosis of congenital heart disease by telemedicine using four-dimensional ultrasound with spatiotemporal image correlation. Ultrasound Obstet Gynecol. 2012, 39, 203–209.
- Rolo LC, Nardozza LM, Araujo Júnior E, Hatanaka AR, Rocha LA, Simioni C; et al. Reference ranges of atrioventricular valve areas by means of four-dimensional ultrasonography using spatiotemporal image correlation in the rendering mode. Prenat Diagn. 2013, 33, 50–55.
- Rolo LC, Pietrolucci ME, Araujo Júnior E, Barros FS, Nardozza LM, Martina WP; et al. Viewing rate and reproducibility of papillary muscle areas in foetal atrioventricular valves using spatio-temporal image correlation in the rendering mode in congenital heart disease. J Matern Fetal Neonatal Med. 2015, 28, 1375–1380.
- Lei W, Ying Z, Ailu C, Xiaoguang W. Evaluation of normal fetal ductus venosus using B-flow imaging with spatiotemporal image correlation and traditional color Doppler echocardiography. Echocardiography. 2015, 32(2):325–331.
- Qin Y, Zhang Y, Zhou X, Wang Y, Sun, W, Chen L; et al. Four-dimensional echocardiography with spatiotemporal image correlation and inversion mode for detection of congenital heart disease. Ultrasound Med Biol. 2014, 40, 1434–1441.
- Rizzo G, Capponi A, Vendola M, Pietrolucci ME, Arduini D. Role of tomographic ultrasound imaging with spatiotemporal image correlation for identifying fetal ventricular septal defects. J. Ultrasound Med. 2008, 27, 1071–1075.
- Malho AS, Bravo-Valenzuela NJ, Ximenes R, Peixoto AB, Araujo Júnior E. Antenatal diagnosis of congenital heart disease by 3D ultrasonography using spatiotemporal image correlation with HDlive Flow and HDlive Flow silhouette rendering modes. Ultrasonography. 2022, 41, 578–596.
- Tie HX, Ma B, Zhang DC, Li TG. Prenatal diagnosis of fetal inferior vena cava malformation using HDlive flow combined with spatiotemporal image correlation. Echocardiography. 2022, 39, 685–690.
- Li TG, Ma B, Gao YH, Zhang RH, Li PL, Da ZQ. Prenatal diagnosis of total anomalous pulmonary venous connection using 2D and HDlive flow combined with spatiotemporal image correlation. Echocardiography. 2022, 39, 1269–1275.
- Karmegaraj B, Kumar S, Srimurugan B, Sudhakar A, Simpson JM, Vaidyanathan B. 3D/4D spatiotemporal image correlation (STIC) fetal echocardiography provides incremental benefit over 2D fetal echocardiography in predicting postnatal surgical approach in double-outlet right ventricle. Ultrasound Obstet Gynecol. 2021, 57, 423–430.
- Magioli Bravo-Valenzuela NJ, Malho AS, Nieblas CO, Castro PT, Werner H, Araujo Júnior E. Evolution of Fetal Cardiac Imaging over the Last 20 Years. Diagnostics (Basel). 2023, 13, 3509.
- Seale AN, Carvalho JS, Gardiner HM, Mellander M, Roughton M, Simpson J; et al. Total anomalous pulmonary venous connection: Impact of prenatal diagnosis. Ultrasound Obstet Gynecol. 2012, 40, 310–318.
- Bravo-Valenzuela NJM, Peixoto AB, Araujo Júnior E. Prenatal diagnosis of total anomalous pulmonary venous connection: 2D and 3D echocardiographic findings. J Clin Ultrasound. 2021, 49, 240–247.
- Yagel S, Kivilevitch Z, Cohen SM, Valsky DV, Messing B, Shen O, Achiron R. The fetal venous system, part I: Normal embryology, anatomy, hemodynamics, ultrasound evaluation and Doppler investigation. Ultrasound Obstet Gynecol. 2010, 35, 741–750.
- Wolman I, Gull I, Fait G, Amster R, Kupferminc MJ, Lessing JB, et al Persistent right umbilical vein: Incidence and significance. Ultrasound Obstet Gynecol. 2002, 19, 562–564. [CrossRef]
- Weichert J, Hartge D, Germer U, Axt-Fliedner R, Gembruch U. Persistent right umbilical vein: A prenatal condition worth mentioning? Ultrasound Obstet Gynecol. 2011, 37, 543–548.
- Lide B, Lindsley W, Foster MJ, Hale R, Haeri S. Intrahepatic persistent right umbilical vein and associated outcomes: A systematic review of the literature. J Ultrasound Med. 2016, 35, 1–5.
- Strizek B, Zamprakou A, Gottschalk I, Roethlisberger M, Hellmund A, Müller A; et al. Prenatal diagnosis of agenesis of ductus venosus: A retrospective study of anatomic variants, associated anomalies and impact on postnatal outcome. Ultraschall Med. 2019, 40, 333–339.
- Pacheco D, Brandão O, Montenegro N, Matias A. Ductus venosus agenesis and fetal malformations: What can we expect? – a systematic review of the literature. J Perinat Med. 2019, 47, 1–11.
- Turan S, Turan OM, Desai A, Harman CR, Baschat AA. First-trimester fetal cardiac examination using spatiotemporal image correlation, tomographic ultrasound and color Doppler imaging for the diagnosis of complex congenital heart disease in high-risk patients. Ultrasound Obstet Gynecol. 2014, 44, 562–567.
- Rizzo G, Capponi A, Cavicchioni O, Vendola M, Pietrolucci ME, Arduini D. Application of automated sonography on 4-dimensional volumes of fetuses with transposition of the great arteries. J Ultrasound Med. 2008, 27, 771–776.
- Shih JC, Shyu MK, Su YN, Chiang YC, Lin CH, Lee CN. 'Big-eyed frog' sign on spatiotemporal image correlation (STIC) in the antenatal diagnosis of transposition of the great arteries. Ultrasound Obstet Gynecol. 2008, 32, 762–768.
- Araujo Júnior E, Tonni G, Bravo-Valenzuela NJ, Da Silva Costa F, Meagher S. Assessment of Fetal Congenital Heart Diseases by 4-Dimensional Ultrasound Using Spatiotemporal Image Correlation: Pictorial Review. Ultrasound Q. 2018, 34, 11–17.
- Gottschalk I, Walter A, Menzel T, Weber EC, Wendt S, Sreeram N; et al. D-Transposition of the great arteries with restrictive foramen ovale in the fetus: The dilemma of predicting the need for postnatal urgent balloon atrial septostomy. Arch Gynecol Obstet. 2024, 309, 1353–1367.
- Pontes ALS, Chagas CC, Bravo-Valenzuela NJ, Peixoto AB, Mappa I, Rizzo G; et al. Fetal heart foramen ovale area by three-dimensional ultrasound using stic in the rendering mode: Reference range and applicability in congenital heart diseases. Int J Cardiovasc Imaging. 2023, 39, 531–539.
- Freud LR, Wilkins-Haug LE, Beroukhim RS, LaFranchi T, Phoon CK, Glickstein JS; et al. Effect of In Utero Non-Steroidal Anti-Inflammatory Drug Therapy for Severe Ebstein Anomaly or Tricuspid Valve Dysplasia (NSAID Therapy for Fetal Ebstein anomaly). Am J Cardiol. 2021, 141, 106–112.
- Hirano Y, Masuyama H, Hayata K, Eto E, Nobumoto E, Hiramatsu Y. Prenatal Diagnosis of Interrupted Aortic Arch: Usefulness of Three-Vessel and Four-Chamber Views. Acta Med Okayama. 2016, 70, 485–491.
- Hata T, Koyanagi A, Yamanishi T, Bouno S, Takayoshi R, Miyagi Y; et al. Success rate of five fetal cardiac views using HDlive Flow with spatiotemporal image correlation at 18-21 and 28-31 weeks of gestation. J Perinat Med. 2020 Mar 3:/j/jpme.ahead-of-print/jpm-2019-0434/jpm-2019-0434.xml. [CrossRef]
- Pappalardo E, Gulino FA, Ettore C, Cannone F, Ettore G. Body Stalk Anomaly Complicated by Ectopia Cordis: First-Trimester Diagnosis of Two Cases Using 2- and 3-Dimensional Sonography. J Clin Med. 2023, 12, 1896.
- Zhang S, Wang N, Qu P, Shu X, Mi Y, Gao X. Prenatal echocardiography diagnosis of a novel combination of bilateral ductus arteriosus and cardiovascular anomalies: A case report and literature review. Front Cardiovasc Med. 2024, 11, 1389759.
- Pluym ID, Sklansky M, Wu JY, Afshar Y, Holliman K, Devore GR; et al. Fetal cardiac rhabdomyomas treated with maternal sirolimus. Prenat Diagn. 2020, 40, 358–364.
- Maász A, Bodó T, Till Á, Molnár G, Masszi G, Labossa G; et al. Three-Year Follow-Up after Intrauterine mTOR Inhibitor Administration for Fetus with TSC-Associated Rhabdomyoma. Int J Mol Sci. 2023, 24, 12886.
- Qaderi S, Javinani A, Blumenfeld YJ, Krispin E, Papanna R, Chervenak FA; et al. Mammalian target of rapamycin inhibitors: A new-possible approach for in-utero medication therapy. Prenat Diagn. 2024, 44, 88–98.
- Kamil D, Geipel A, Schmitz C, Breuer J, Herberg U, Knöpfle G; et al. Fetal pericardial teratoma causing cardiac insufficiency: Prenatal diagnosis and therapy. Ultrasound Obstet Gynecol. 2006, 28, 972–973.
- Messing B, Cohen SM, Valsky DV, Rosenak D, Hochner-Celnikier D, Savchev S; et al. Fetal cardiac ventricle volumetry in the second half of gestation assessed by 4D ultrasound using STIC combined with inversion mode. Ultrasound Obstet Gynecol. 2007, 30, 142–151.
- Simioni C, Nardozza LM, Araujo Júnior E, Rolo LC, Zamith M, Caetano AC; et al. Heart stroke volume, cardiac output, and ejection fraction in 265 normal fetus in the second half of gestation assessed by 4D ultrasound using spatio-temporal image correlation. J Matern Fetal Neonatal Med. 2011, 24, 1159–1167.
- Tedesco GD, de Souza Bezerra M, Barros FS, Martins WP, Nardozza LM, Carrilho MC; et al. Reference Ranges of Fetal Cardiac Biometric Parameters Using Three-Dimensional Ultrasound with Spatiotemporal Image Correlation M Mode and Their Applicability in Congenital Heart Diseases. Pediatr Cardiol. 2017, 38, 271–279.
- Bravo-Valenzuela NJ, Peixoto AB, Mattar R, Melo Júnior JF, da Silva Pares DB, Araujo Júnior E. Fetal Cardiac Function and Ventricular Volumes Determined by Three-Dimensional Ultrasound Using STIC and VOCAL Methods in Fetuses from Pre-gestational Diabetic Women. Pediatr Cardiol. 2020, 41, 1125–1134.
- Tanis JC, Mohammed N, Bennasar M, Martinez JM, Bijnens B, Crispi F; et al. Online versus offline spatiotemporal image correlation (STIC) M-mode for the evaluation of cardiac longitudinal annular displacement in fetal growth restriction. J Matern Fetal Neonatal Med. 2018 Jul;31(14):1845-1850.
- Yeo L, Romero R. Fetal Intelligent Navigation Echocardiography (FINE): A Novel Method for Rapid, Simple, and Automatic Examination of the Fetal Heart. Ultrasound Obstet Gynecol. 2013, 42, 268–284.
- Carrillo MC, Rolo LC, Tonni G, Araujo Júnior E. Evaluation of the quality of standard fetal heart views using the FAST, STAR and FINE four-dimensional ultrasound techniques in congenital heart disease screening. Echocardiography. 2020, 37, 114–123.
- Yeo L, Romero R. Color and power Doppler combined with Fetal Intelligent Navigation Echocardiography (FINE) to evaluate the fetal heart. Ultrasound Obstet Gynecol. 2017, 50, 476–491.
- Yeo L, Romero R. Intelligent navigation to improve obstetrical sonography. Ultrasound Obstet Gynecol. 2016, 47, 403–409.
- Rizzo G, Pietrolucci ME, Capponi A, Mappa I. Exploring the role of artificial intelligence in the study of the foetal heart. Int J Cardiovasc Imaging. 2022, 38, 1017–1019.
- Wu H, Wu B, Lai F, Liu P, Lyu G, He S; et al. Application of Artificial Intelligence in Recognising the Anatomical Structure of Fetal Heart Standard Section. Comput Math Methods Med. 2023, 2023, 5650378.
- Pietrolucci ME, Maqina P, Mappa I, Marra MC, D'Antonio F, Rizzo G. Evaluation of an artificial intelligent algorithm (Heart Assist™) to automatically assess the quality of second trimester cardiac views: A prospective study. J Perinat Med. 2023, 51, 920–924.
- Rodenbarger A, Thorsson T, Stiver C, Jantzen D, Chevenon M, Yu S; et al. Third trimester predictors of interventional timing and accuracy of fetal anticipatory guidance in tetralogy of Fallot: A multi-center study. Prenat Diagn. 2020, 40, 870–877.
- Ungureanu A, Marcu AS, Patru CL, Ruican D, Nagy R, Stoean R; et al. Learning deep architectures for the interpretation of first-trimester fetal echocardiography (LIFE) - a study protocol for developing an automated intelligent decision support system for early fetal echocardiography. BMC Pregnancy Childbirth. 2023, 23, 20.
- Nieblas CO, Bravo-Valenzuela NJ, Araujo Júnior E, Werner H. Fetal transposition of the great arteries: 3D virtual and physical models from ultrasound datasets. Int J Cardiovasc Imaging. 2024, 40, 1157–1158.
- Pires GDV, Nieblas CO, Bravo-Valenzuela NJ, Araujo Júnior E, Castro PT, Werner H. Ebstein anomaly: 3D virtual and physical models from obstetrical ultrasound data. Echocardiography. 2024, 41, e15806.
- Acar P, Hadeed K, Dulac Y. Advances in 3D echocardiography: From foetus to printing. Arch Cardiovasc Dis. 2016, 109, 84–86.
- Chen SA, Ong CS, Hibino N, Baschat AA, Garcia JR, Miller JL. 3D printing of fetal heart using 3D ultrasound imaging data. Ultrasound Obstet Gynecol. 2018, 52, 808–809.
- Aly DM, Shah S. Three-Dimensional Echocardiography Derived Printing: A Review of Workflow, Current, and Future Applications. Curr Cardiol Rep. 2023, 25, 597–605.
- Werner H, Ribeiro G, Arcoverde V, Lopes J, Velho L. The use of metaverse in fetal medicine and gynecology. Eur J Radiol. 2022, 150, 110241.
- Lloyd DFA, Pushparajah K, Simpson JM, van Amerom JFP, van Poppel MPM, Schulz A; et al. Three-dimensional visualisation of the fetal heart using prenatal MRI with motion-corrected slice-volume registration: A prospective, single-centre cohort study. Lancet. 2019, 393, 1619–1627.
- Lloyd DFA, van Poppel MPM, Pushparajah K, Vigneswaran TV, Zidere V, Steinweg J; et al. Analysis of 3-Dimensional Arch Anatomy, Vascular Flow, and Postnatal Outcome in Cases of Suspected Coarctation of the Aorta Using Fetal Cardiac Magnetic Resonance Imaging. Circ Cardiovasc Imaging. 2021, 14, e012411.
- Zhang X, Zhu M, Dong SZ. Utility of fetal cardiovascular magnetic resonance imaging in assessing the fetuses with complete vascular ring. Front Pediatr. 2023, 11, 1159130.
- Ulm B, Muin D, Scharrer A, Prayer D, Dovjak G, Kasprian G. Prenatal ultrasound and magnetic resonance evaluation and fetal outcome in high-risk fetal tumors: A retrospective single-center cohort study over 20 years. Acta Obstet Gynecol Scand. 2020, 99, 1534–1545.
- Prayer, D. Fetal MRI. Top Magn Reson Imaging. 2011, 22, 89. [Google Scholar] [CrossRef]
- Manganaro L, Savelli S, Di Maurizio M, Francioso A, Fierro F, Tomei A; et al. Fetal MRI of the cardiovascular system: Role of steady-state free precession sequences for the evaluation of normal and pathological appearances. Radiol Med. 2009, 114, 852–870.
- Salehi D, Fricke K, Bhat M, Arheden H, Liuba P, Hedström E. Utility of fetal cardiovascular magnetic resonance for prenatal diagnosis of complex congenital heart defects. JAMA Netw Open. 2021, 4, e213538.
- Liu K, Zhu M, Zhang YQ, Chen LJ, Dong SZ. Utility of fetal cardiac magnetic resonance imaging in assessing the cardiac axis in fetuses with congenital heart disease. Pediatr Radiol. 2023, 53, 910–919.
- Goncalves LF, Lindblade CL, Cornejo P, Patel MC, McLaughlin ES, Bardo DME. Contribution of fetal magnetic resonance imaging in fetuses with congenital heart disease. Pediatr Radiol. 2022, 52, 513–526.
- Rubert NC, Jategaonkar G, Plasencia JD, Lindblade CL, Bardo DME, Goncalves LF. Four-dimensional fetal cardiac imaging in a cohort of fetuses with suspected congenital heart disease. Pediatr Radiol. 2023, 53, 198–209.
Figure 1.
Measurement of interventricular septum volume (IVS) using 3D ultrasound with STIC and virtual-organ computer aided analysis (VOCAL) in a fetus from a diabetic mother at 25 weeks of gestation. IVS volume=0.144 cm3.
Figure 1.
Measurement of interventricular septum volume (IVS) using 3D ultrasound with STIC and virtual-organ computer aided analysis (VOCAL) in a fetus from a diabetic mother at 25 weeks of gestation. IVS volume=0.144 cm3.

Figure 2.
Left ventricle diastolic volume using STIC with virtual organ computer-aided analysis (VOCAL) in a fetus at 30 weeks of gestation. LV volume=1.3cm3.
Figure 2.
Left ventricle diastolic volume using STIC with virtual organ computer-aided analysis (VOCAL) in a fetus at 30 weeks of gestation. LV volume=1.3cm3.
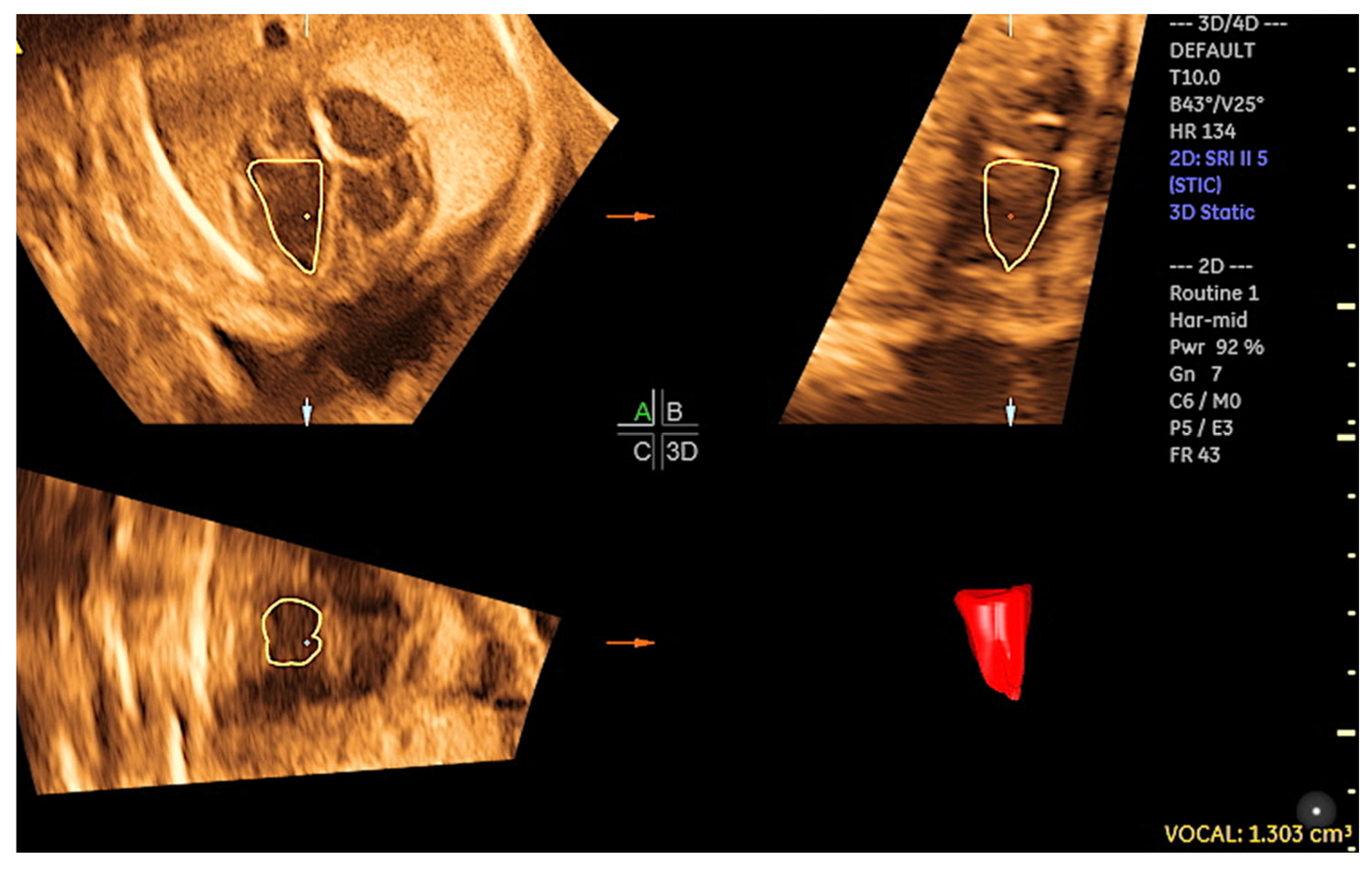
Figure 3.
Evaluation of the tricuspid annular movement using fetal STIC-M (5.4mm). TAPSE: tricuspid annular plane systolic excursion; RV: right ventricle.
Figure 3.
Evaluation of the tricuspid annular movement using fetal STIC-M (5.4mm). TAPSE: tricuspid annular plane systolic excursion; RV: right ventricle.
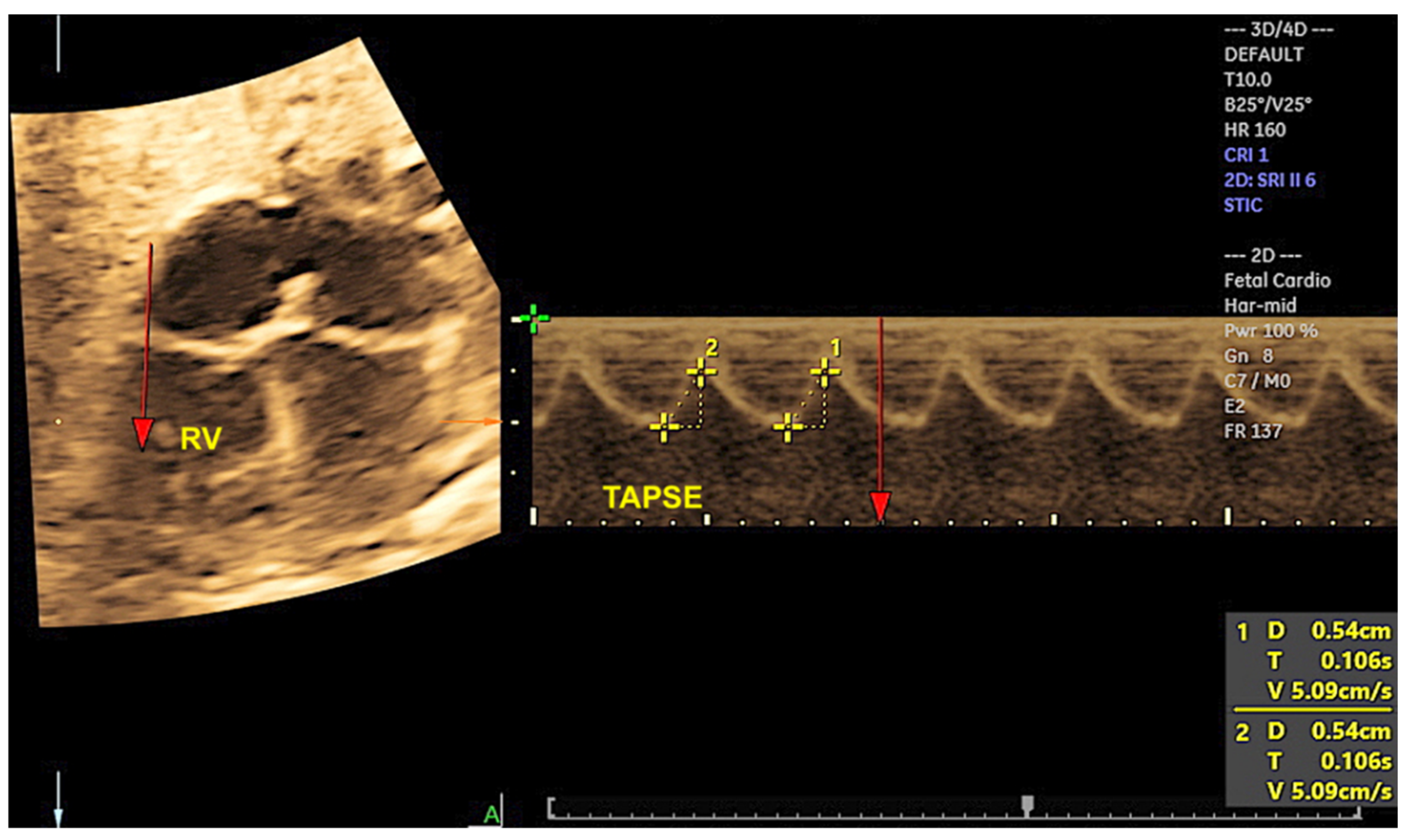
Figure 4.
Three-dimensional ultrasound with STIC and HDlive mode, providing the reconstruction of the left ventricular outflow tract in a case of transposition of great arteries. Observe the pulmonary artery (P) arising from the left ventricle (LV). RV: right ventricle.
Figure 4.
Three-dimensional ultrasound with STIC and HDlive mode, providing the reconstruction of the left ventricular outflow tract in a case of transposition of great arteries. Observe the pulmonary artery (P) arising from the left ventricle (LV). RV: right ventricle.
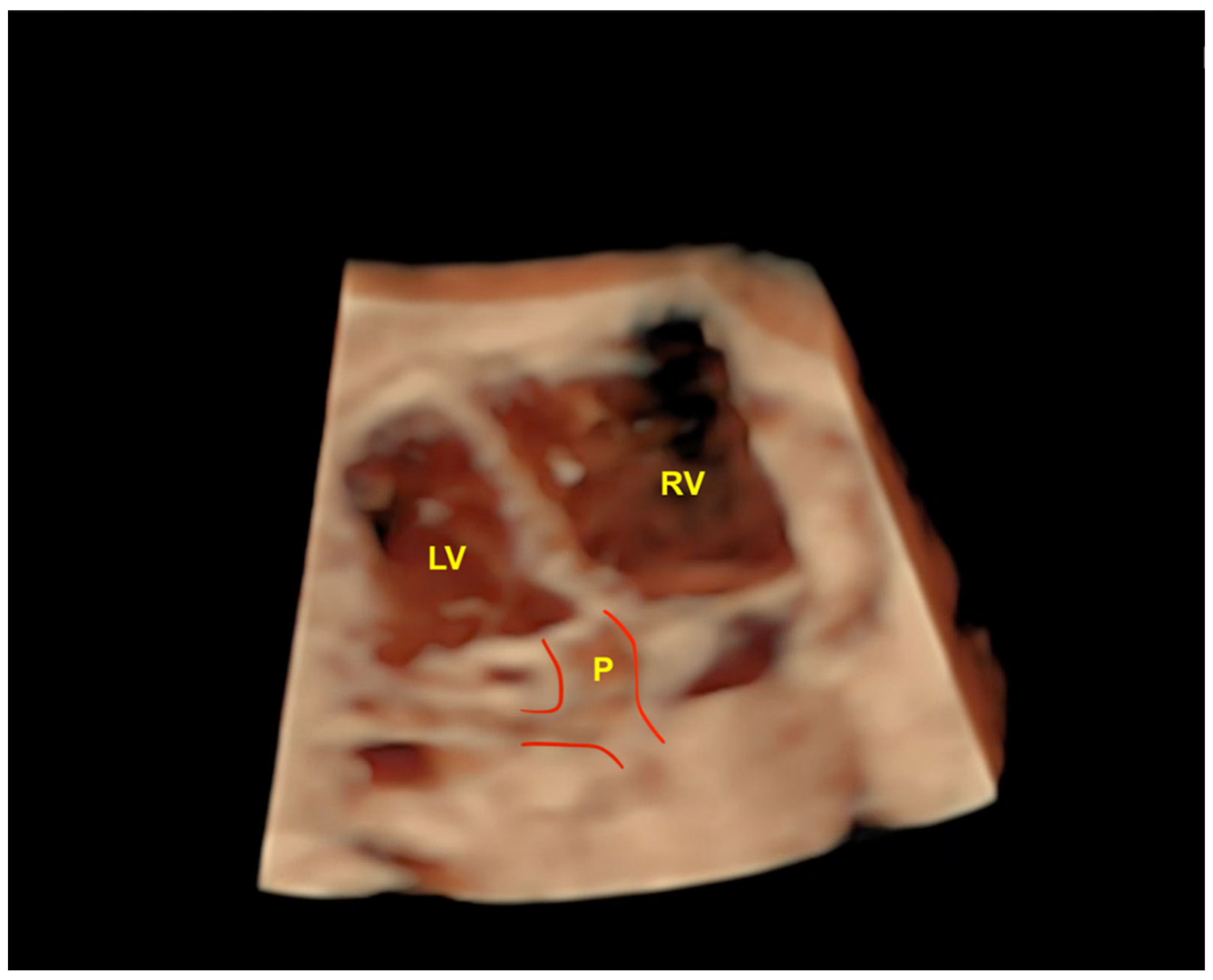
Figure 5.
Tomographic ultrasound imaging (TUI) in the rendering mode enables the visualization of sequential axial planes in the case of inlet ventricular septal defect (VSD) (yellow arrows).
Figure 5.
Tomographic ultrasound imaging (TUI) in the rendering mode enables the visualization of sequential axial planes in the case of inlet ventricular septal defect (VSD) (yellow arrows).
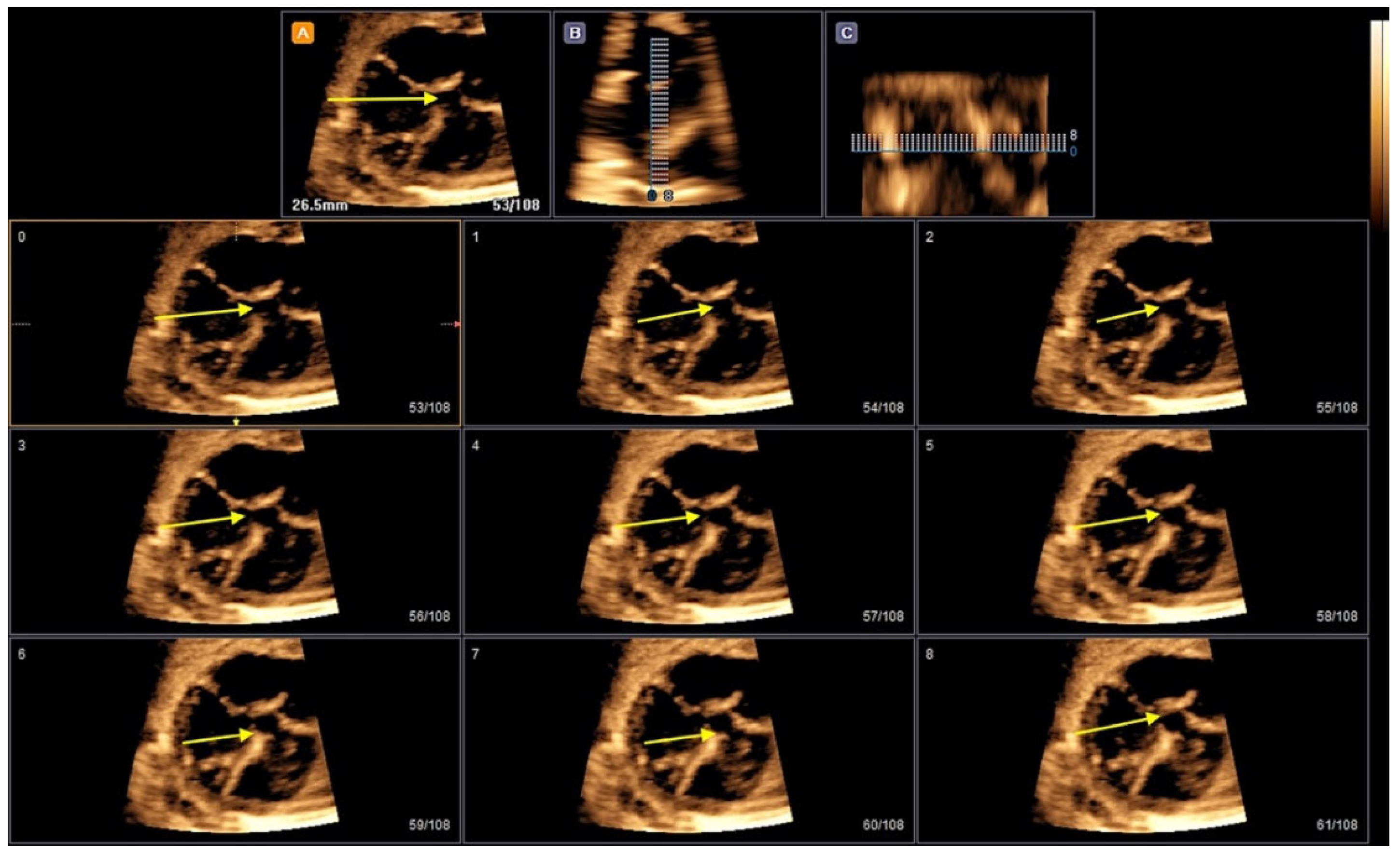
Figure 6.
STIC with HDlive Silhouette mode in a case of coarctation of aorta. Note the discrepancy of the great arteries due to the small aorta. Ao: aorta; PA: pulmonary artery; VC: superior vena cava.
Figure 6.
STIC with HDlive Silhouette mode in a case of coarctation of aorta. Note the discrepancy of the great arteries due to the small aorta. Ao: aorta; PA: pulmonary artery; VC: superior vena cava.
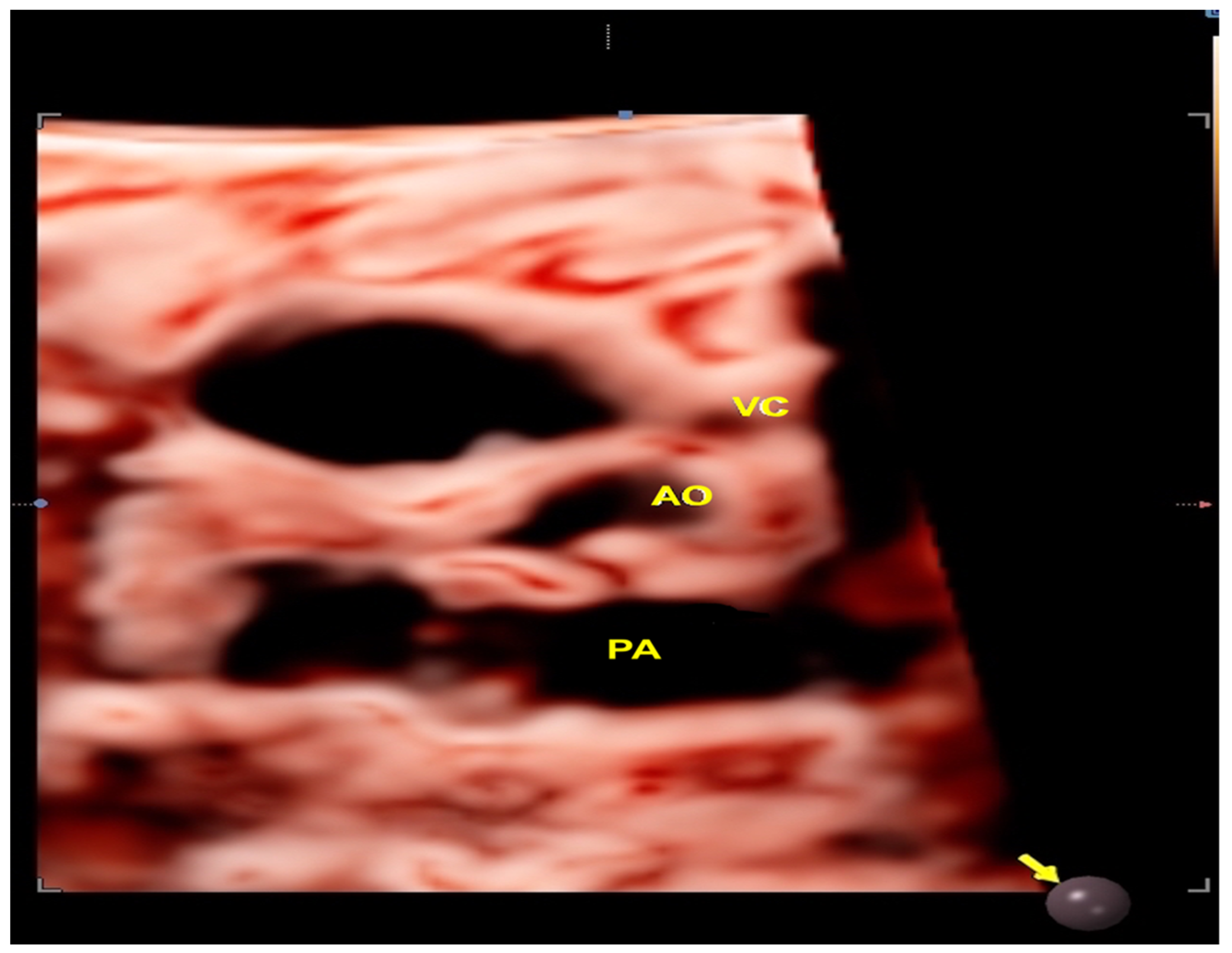
Figure 7.
(A) Three-dimensional ultrasound with Surface Realistic Vue (SRV) imaging in a case of partial anomalous pulmonary vein return with ventricular septal defect (VSD). Note that 2 of the pulmonary veins return to the right atrium (red arrows). Virtual light source position, 10 o’clock. (B) STIC with color Doppler of a case of total anomalous pulmonary vein return (type infradiaphragmatic). The right (RPV) and left pulmonary veins (LPV) drain (white arrows) into a collecting vein (COL) and subsequently into a vertical vein (VV), which achieves the right atrium (RA) via the inferior vena cava (IVC). LV: left ventricle; LA: left atrium; RA: right atrium; RV: right ventricle; **VSD: ventricular septal defect; PV: pulmonary vein; T: tricuspid valve; M: mitral valve.
Figure 7.
(A) Three-dimensional ultrasound with Surface Realistic Vue (SRV) imaging in a case of partial anomalous pulmonary vein return with ventricular septal defect (VSD). Note that 2 of the pulmonary veins return to the right atrium (red arrows). Virtual light source position, 10 o’clock. (B) STIC with color Doppler of a case of total anomalous pulmonary vein return (type infradiaphragmatic). The right (RPV) and left pulmonary veins (LPV) drain (white arrows) into a collecting vein (COL) and subsequently into a vertical vein (VV), which achieves the right atrium (RA) via the inferior vena cava (IVC). LV: left ventricle; LA: left atrium; RA: right atrium; RV: right ventricle; **VSD: ventricular septal defect; PV: pulmonary vein; T: tricuspid valve; M: mitral valve.
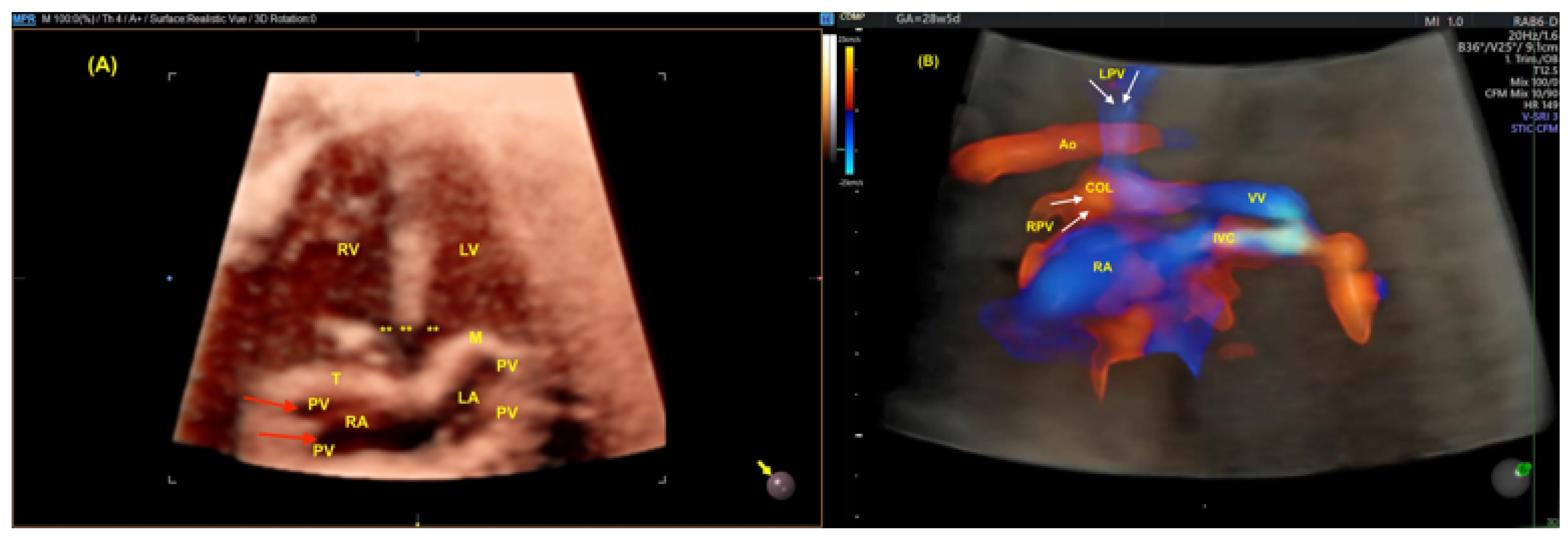
Figure 8.
Three-dimensional ultrasound with STIC and HDlive mode in a case of left heterotaxy. Observe that the venous vessel (hemiazygos) is located posterior (near to the fetal spine) to the arterial vessel (aorta) at the upper abdomen view. Ao; aorta; Hz: hemiazygos vein; L: fetal left side; R: fetal right side.
Figure 8.
Three-dimensional ultrasound with STIC and HDlive mode in a case of left heterotaxy. Observe that the venous vessel (hemiazygos) is located posterior (near to the fetal spine) to the arterial vessel (aorta) at the upper abdomen view. Ao; aorta; Hz: hemiazygos vein; L: fetal left side; R: fetal right side.
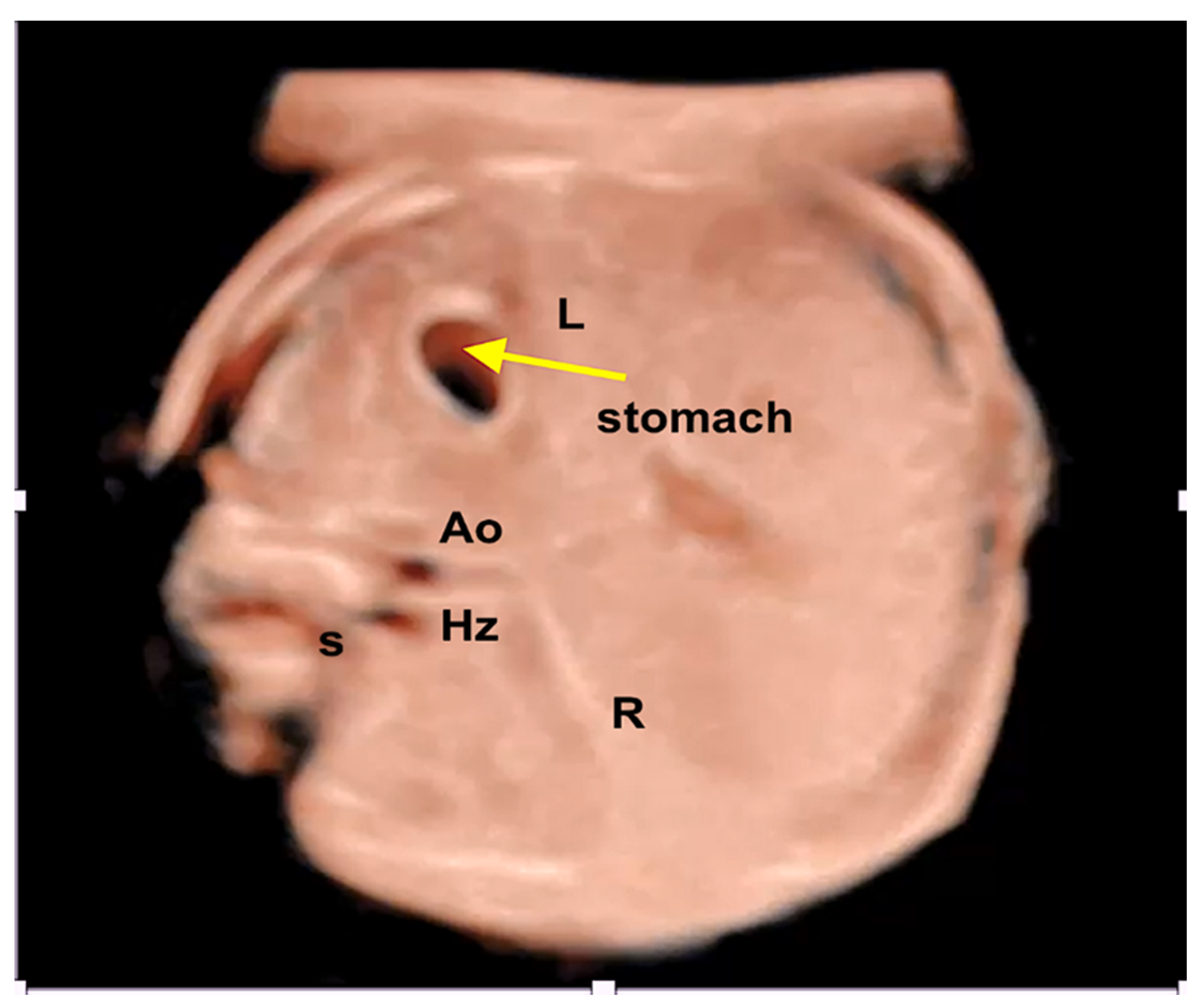
Figure 9.
Extra-hepatic form of agenesis of ductus venosus (DV) using three-dimensional ultrasound with STIC. Note the high-resolution color Doppler showing the absence of flow through the DV (red arrow). IVC: inferior vena cava; DV: ductus venosus; RA: right atrium.
Figure 9.
Extra-hepatic form of agenesis of ductus venosus (DV) using three-dimensional ultrasound with STIC. Note the high-resolution color Doppler showing the absence of flow through the DV (red arrow). IVC: inferior vena cava; DV: ductus venosus; RA: right atrium.
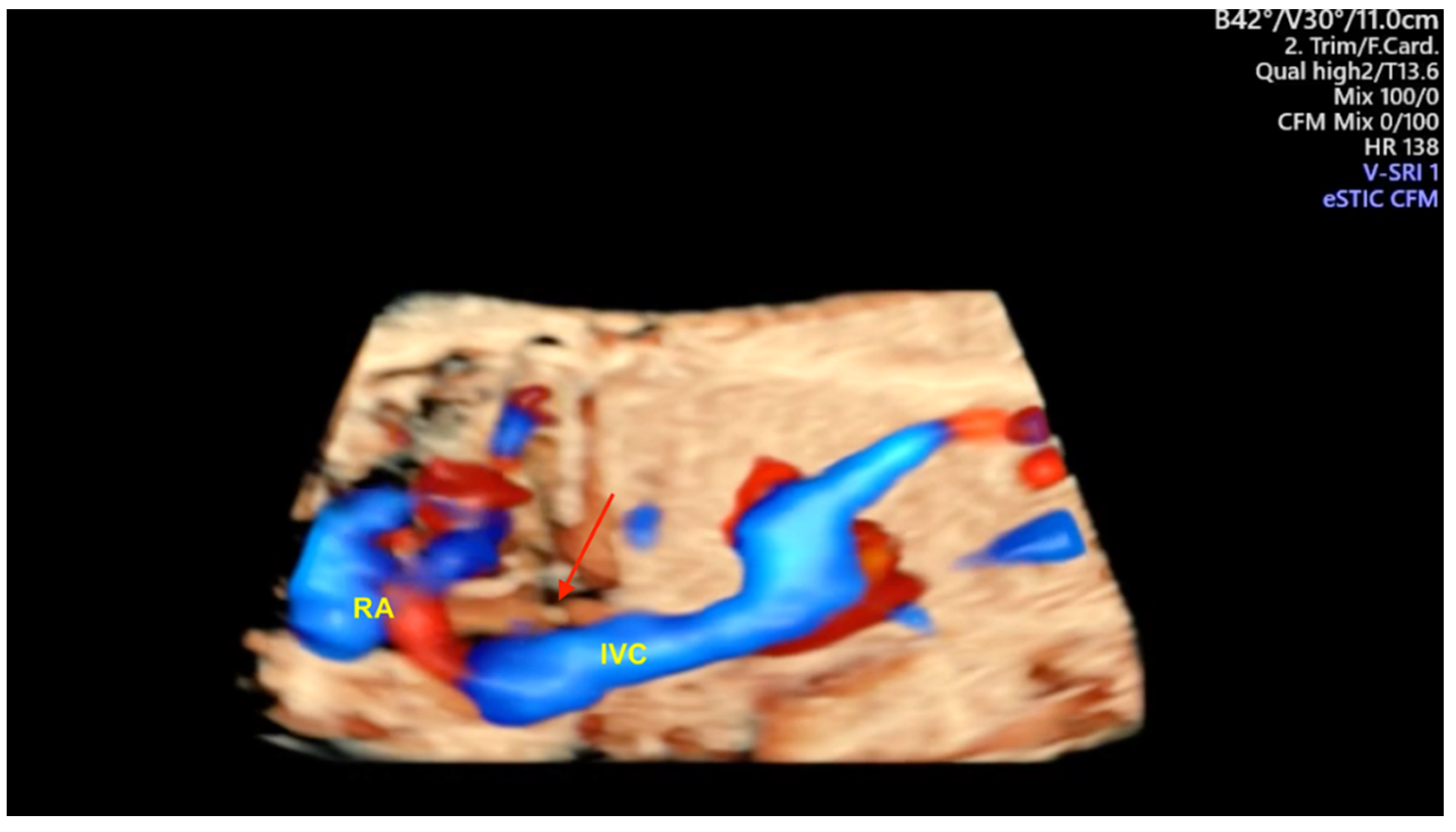
Figure 10.
Three-dimensional ultrasound with STIC enabling the reconstruction of the ventricular outflow tracts in a case of double outflow of right ventricle type Taussig- Bing. Note the great arteries arising from the right ventricle (RV) in a parallel relationship. Ao: aorta; PA: pulmonary artery.
Figure 10.
Three-dimensional ultrasound with STIC enabling the reconstruction of the ventricular outflow tracts in a case of double outflow of right ventricle type Taussig- Bing. Note the great arteries arising from the right ventricle (RV) in a parallel relationship. Ao: aorta; PA: pulmonary artery.
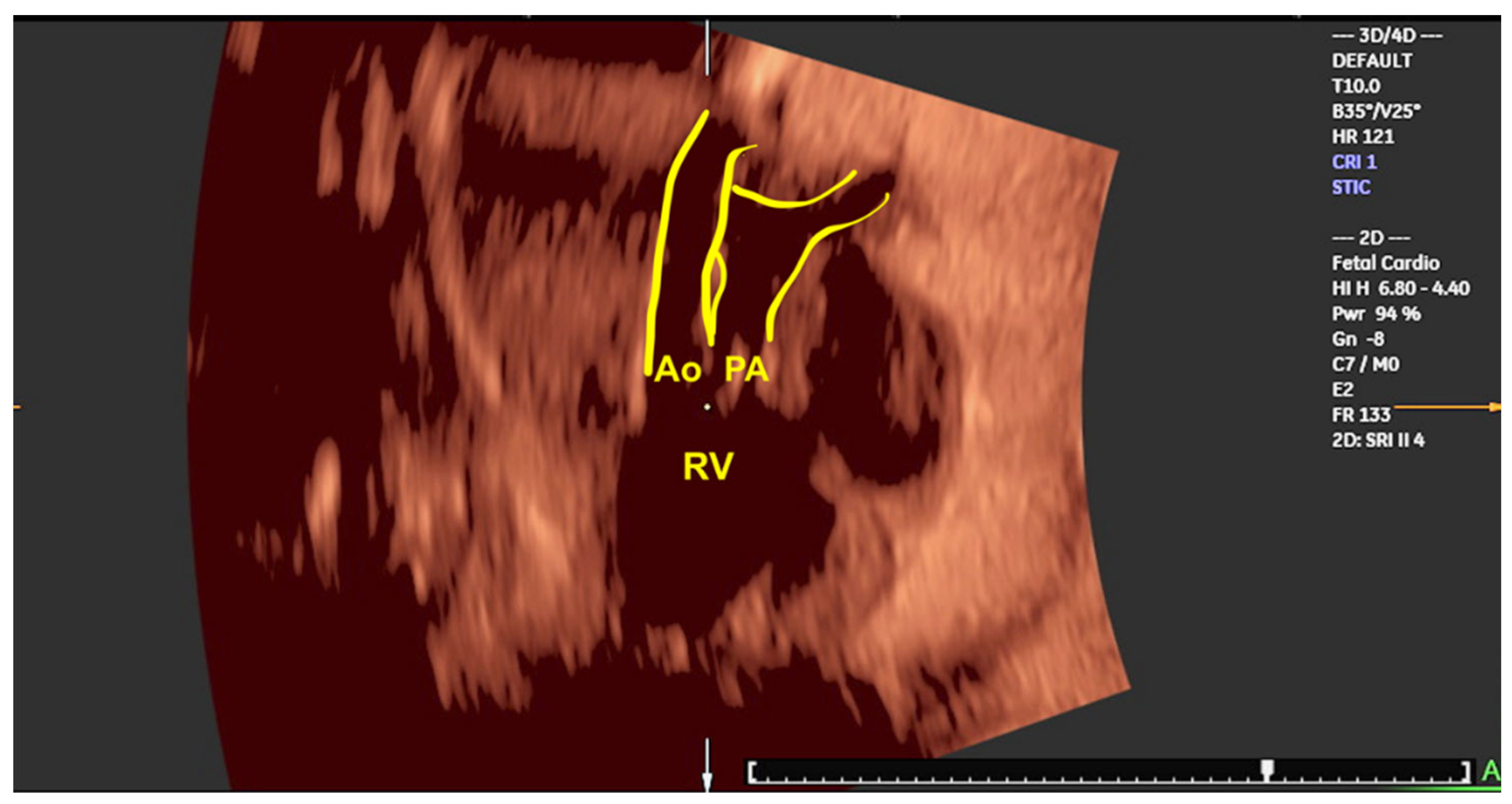
Figure 11.
Tomographic ultrasound imaging (TUI) in the rendering mode in a case of Tetralogy of Fallot and in (B) double outflow of right ventricular (DORV). The RV hypertrophy (yellow arrows) could be observed using this technology (A). Note the great arteries in a parallel relationship (red arrows) in a fetus with DORV type Taussig-Bing using color Doppler(B). DORV: double outflow of right ventricle; Ao; aorta; P: pulmonary artery.
Figure 11.
Tomographic ultrasound imaging (TUI) in the rendering mode in a case of Tetralogy of Fallot and in (B) double outflow of right ventricular (DORV). The RV hypertrophy (yellow arrows) could be observed using this technology (A). Note the great arteries in a parallel relationship (red arrows) in a fetus with DORV type Taussig-Bing using color Doppler(B). DORV: double outflow of right ventricle; Ao; aorta; P: pulmonary artery.
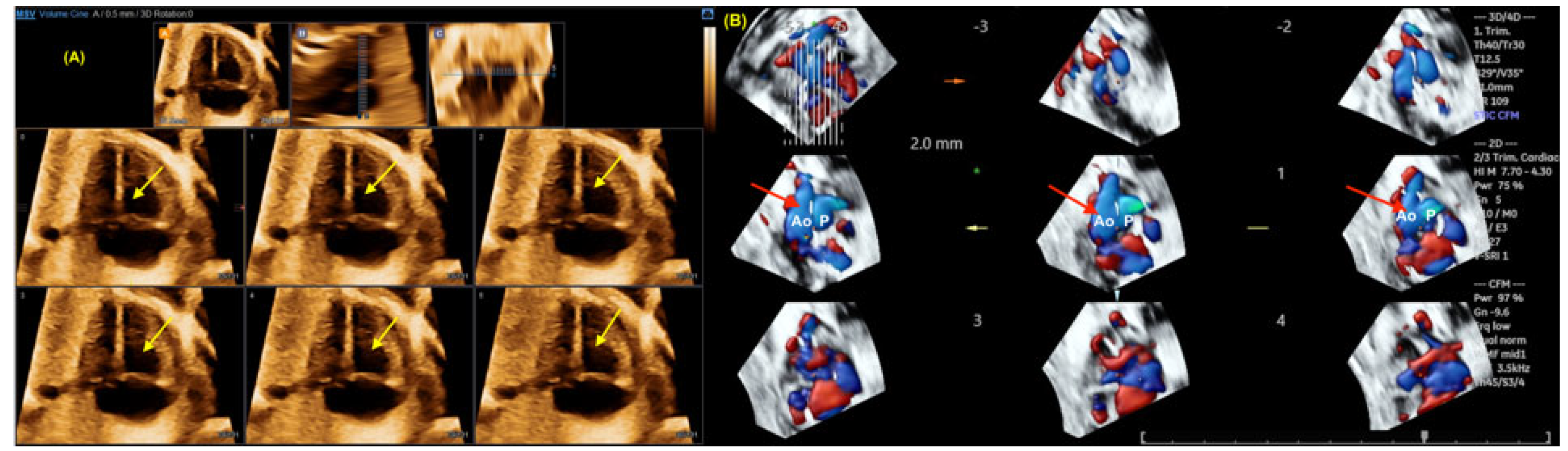
Figure 12.
The reconstruction of the ventricular outflow tracts in a case of transposition of great arteries (TGA) using STIC with color Doppler (A) and HDlive Silhouette. In Image A, it is evident that the aorta (Ao) arises from the right ventricle (RV). In Image B, the pulmonary artery (PA) is unequivocally identified as originating from the left ventricle (LV). The two arteries are observed to be in parallel relationship, with the aorta located anteriorly to the PA.
Figure 12.
The reconstruction of the ventricular outflow tracts in a case of transposition of great arteries (TGA) using STIC with color Doppler (A) and HDlive Silhouette. In Image A, it is evident that the aorta (Ao) arises from the right ventricle (RV). In Image B, the pulmonary artery (PA) is unequivocally identified as originating from the left ventricle (LV). The two arteries are observed to be in parallel relationship, with the aorta located anteriorly to the PA.
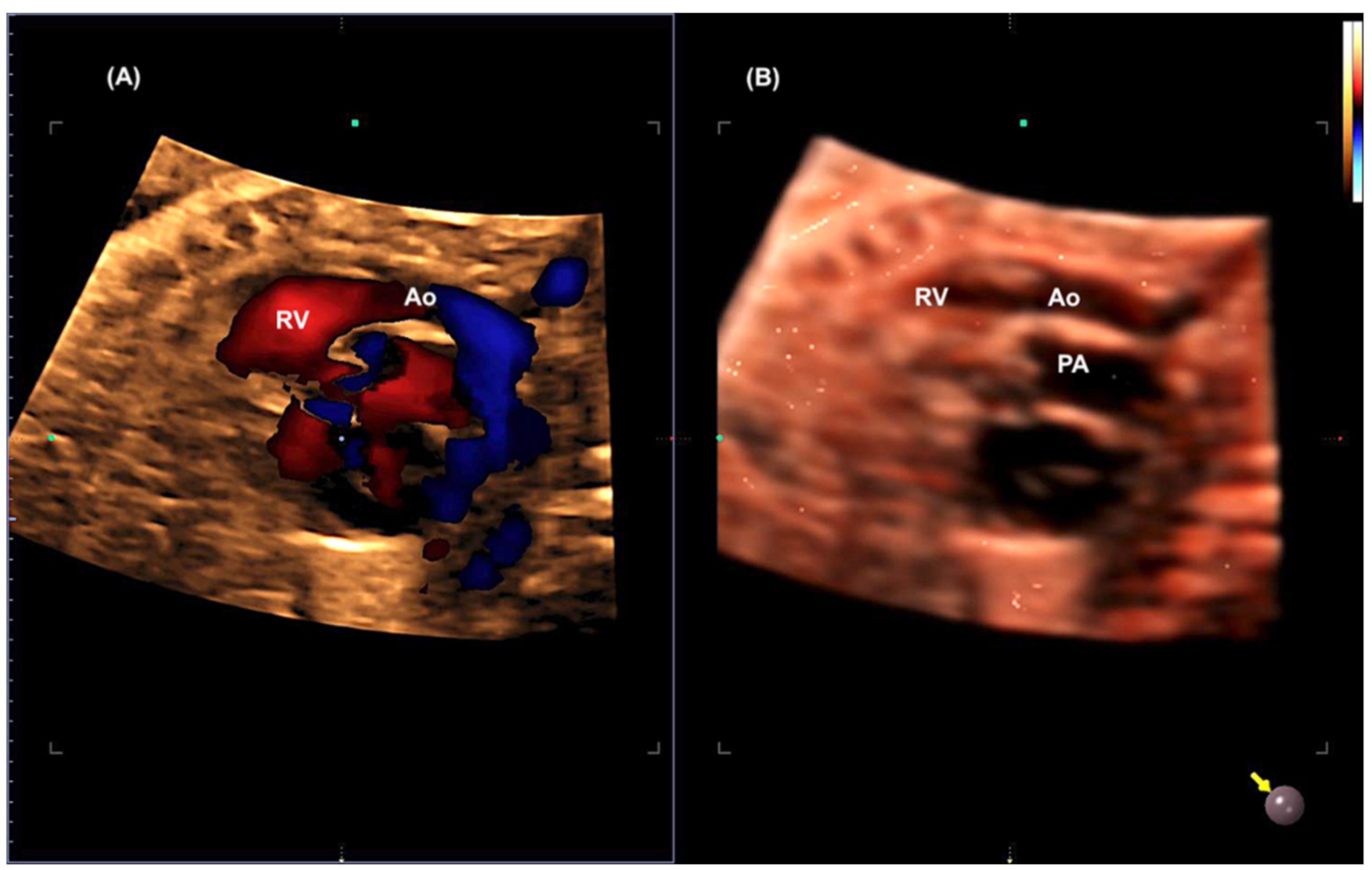
Figure 13.
Measurement of the area of the foramen ovale (FO) using 3D ultrasound with STIC in the rendering mode.
Figure 13.
Measurement of the area of the foramen ovale (FO) using 3D ultrasound with STIC in the rendering mode.
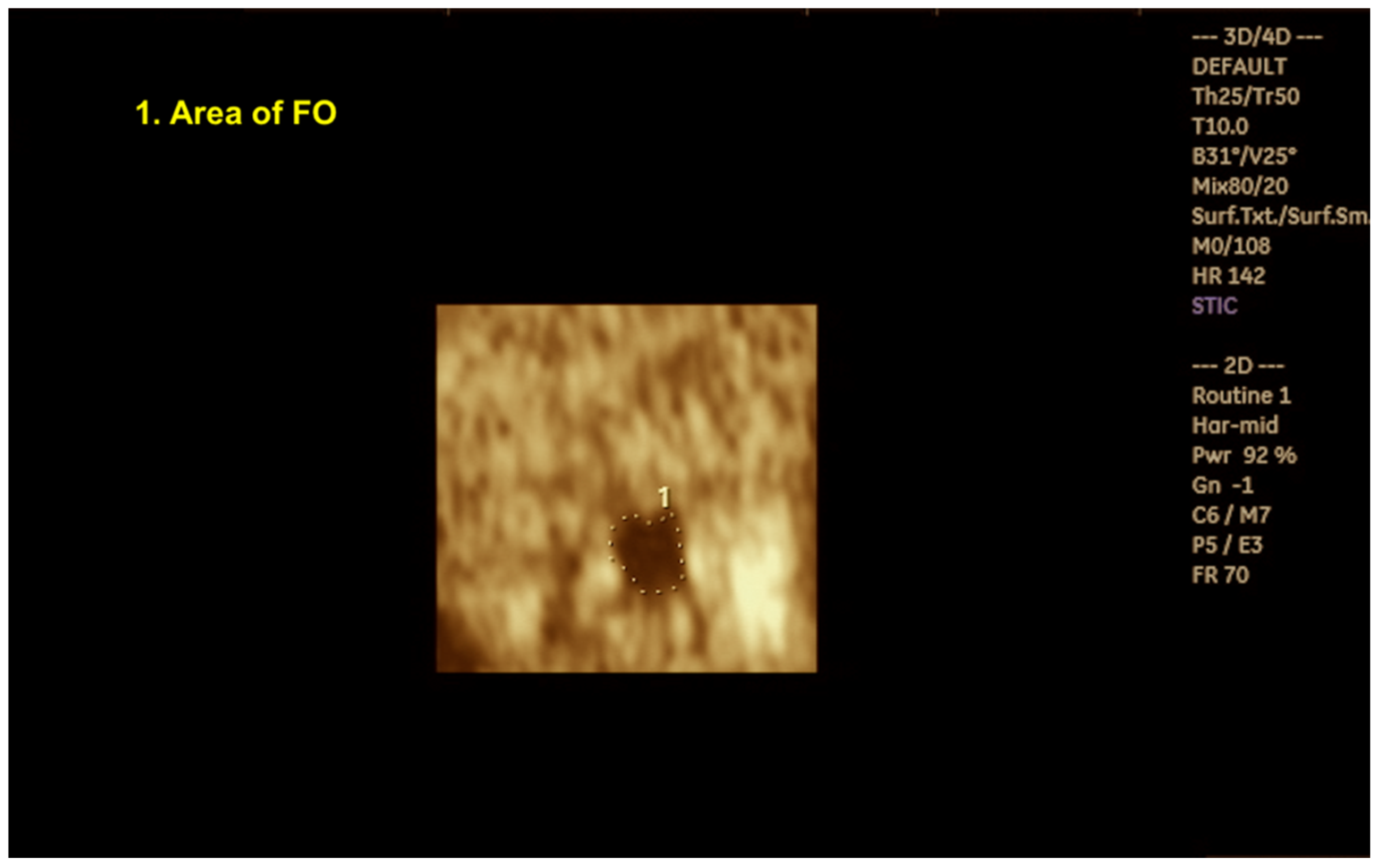
Figure 14.
Three-dimensional with STIC in the rendering mode (A) and HDlive mode (B) of a fetus with Ebstein anomaly at 30 weeks of gestation.
Figure 14.
Three-dimensional with STIC in the rendering mode (A) and HDlive mode (B) of a fetus with Ebstein anomaly at 30 weeks of gestation.
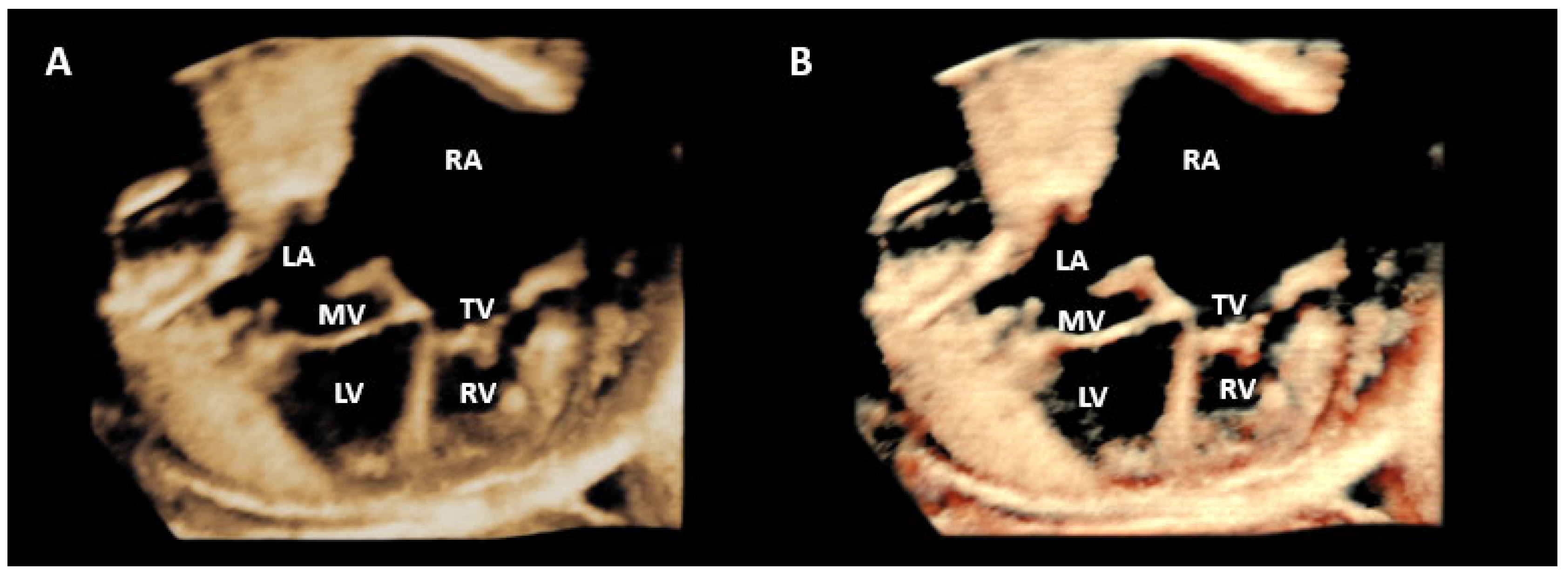
Figure 15.
(A) Reconstruction of aortic arch using STIC with inversion mode in a case of Coarctation of aorta. Observe the narrowing of the aortic isthmus (yellow arrow). (B) Aortic and duct arches imaging in a fetal with normal heart. (B) Sagittal view of the fetal heart at with a normal heart showing aortic and ductal arches using LumiFlow. Ao: aorta; BCT: brachiocephalic trunk; LCC: left common carotid; LSCA: left subclavian artery.
Figure 15.
(A) Reconstruction of aortic arch using STIC with inversion mode in a case of Coarctation of aorta. Observe the narrowing of the aortic isthmus (yellow arrow). (B) Aortic and duct arches imaging in a fetal with normal heart. (B) Sagittal view of the fetal heart at with a normal heart showing aortic and ductal arches using LumiFlow. Ao: aorta; BCT: brachiocephalic trunk; LCC: left common carotid; LSCA: left subclavian artery.
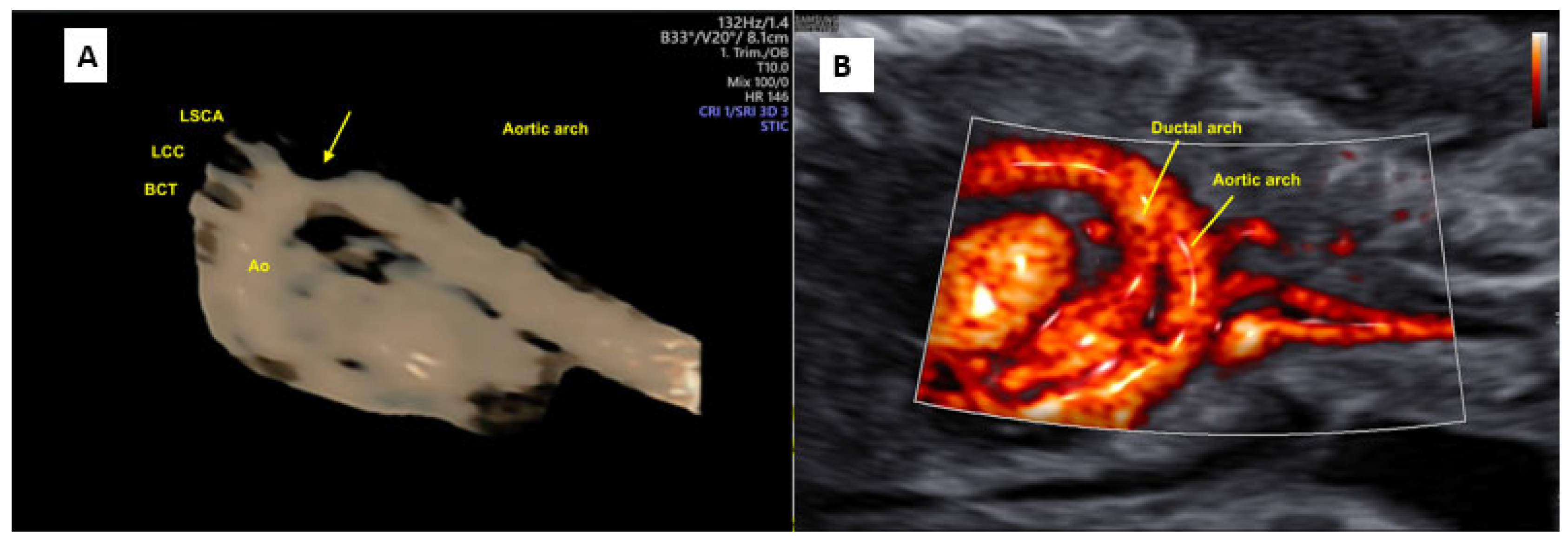
Figure 16.
Large masses (**) in the ventricular septum and both ventricles, mainly in the left ventricle, in a case of Rhabdomyomas with a reduction in the size of the masses after prenatal therapy with Sirolimus. LV: left ventricle; LA: left atrium; RA: right atrium; RV: right ventricle; T: tricuspid valve.
Figure 16.
Large masses (**) in the ventricular septum and both ventricles, mainly in the left ventricle, in a case of Rhabdomyomas with a reduction in the size of the masses after prenatal therapy with Sirolimus. LV: left ventricle; LA: left atrium; RA: right atrium; RV: right ventricle; T: tricuspid valve.
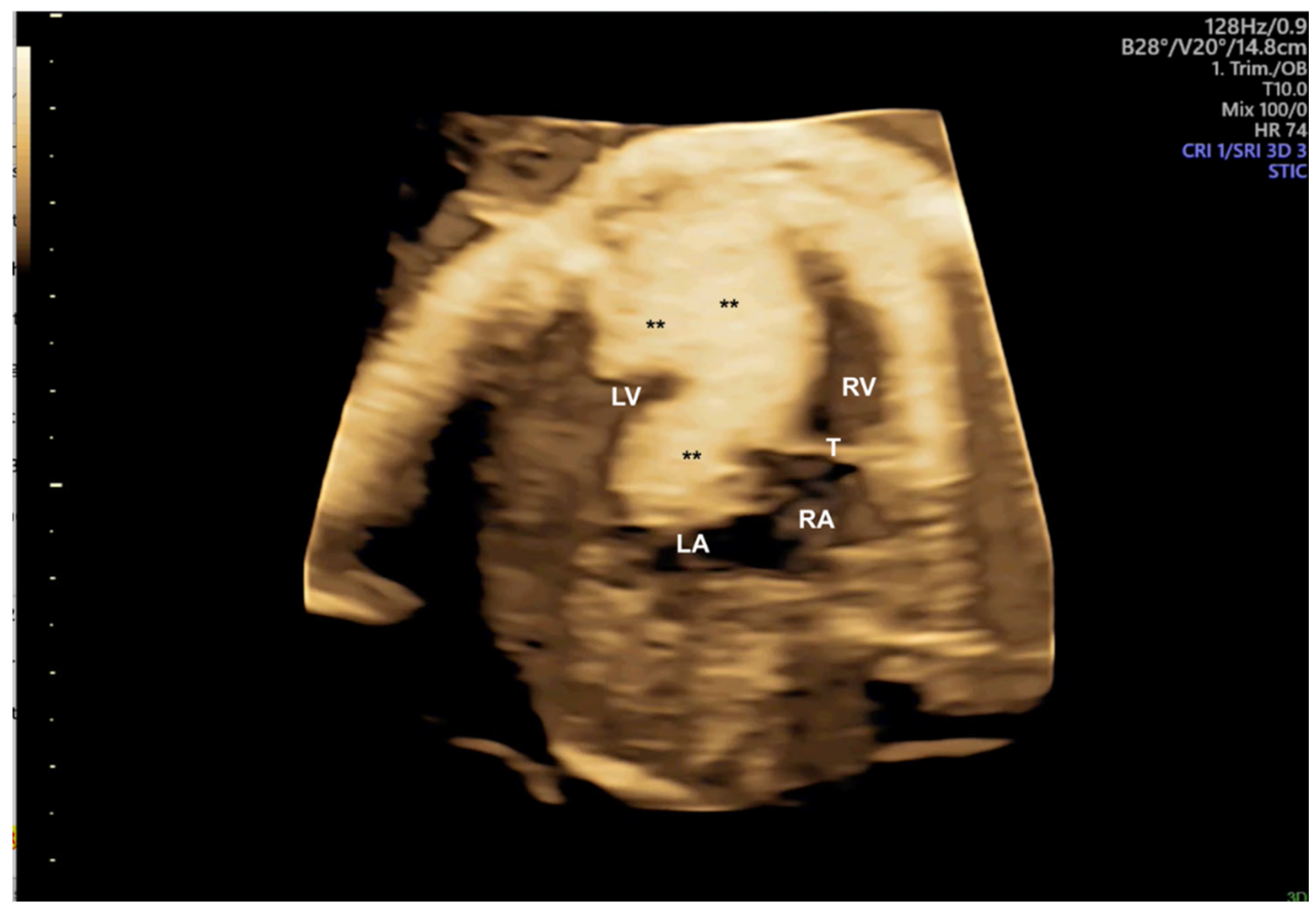
Figure 17.
STIC-M enabling the measurement of mitral annular plane systolic excursion (MAPSE) using fetal STIC-M (5.4mm). MAPSE: MITRAL annular plane systolic excursion; LV: left ventricle.
Figure 17.
STIC-M enabling the measurement of mitral annular plane systolic excursion (MAPSE) using fetal STIC-M (5.4mm). MAPSE: MITRAL annular plane systolic excursion; LV: left ventricle.
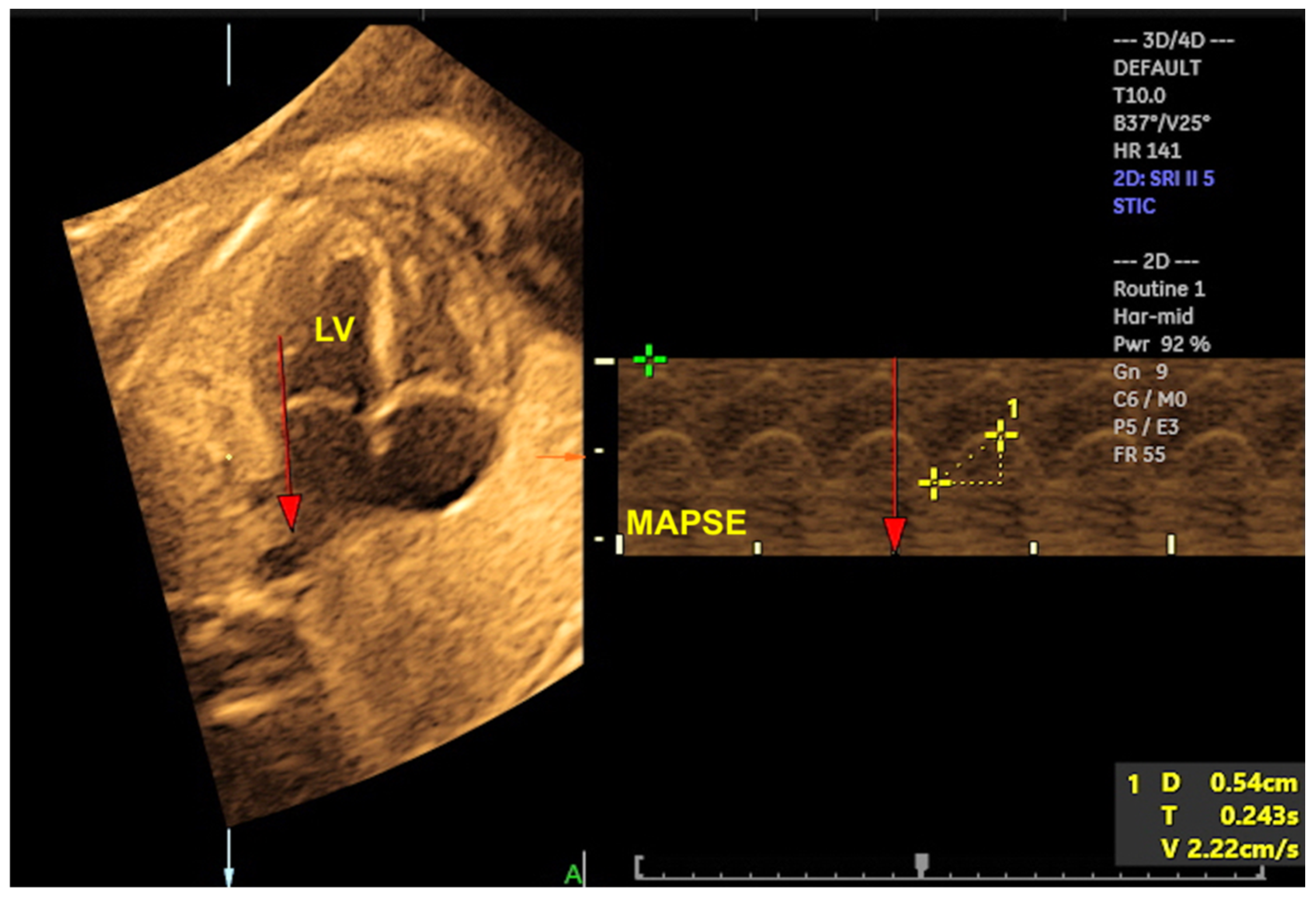
Figure 18.
Three-dimensional reconstruction of the left ventricle (LV) using of STIC with virtual organ computer-aided analysis (VOCAL) in a fetus at 22 weeks of gestation.
Figure 18.
Three-dimensional reconstruction of the left ventricle (LV) using of STIC with virtual organ computer-aided analysis (VOCAL) in a fetus at 22 weeks of gestation.
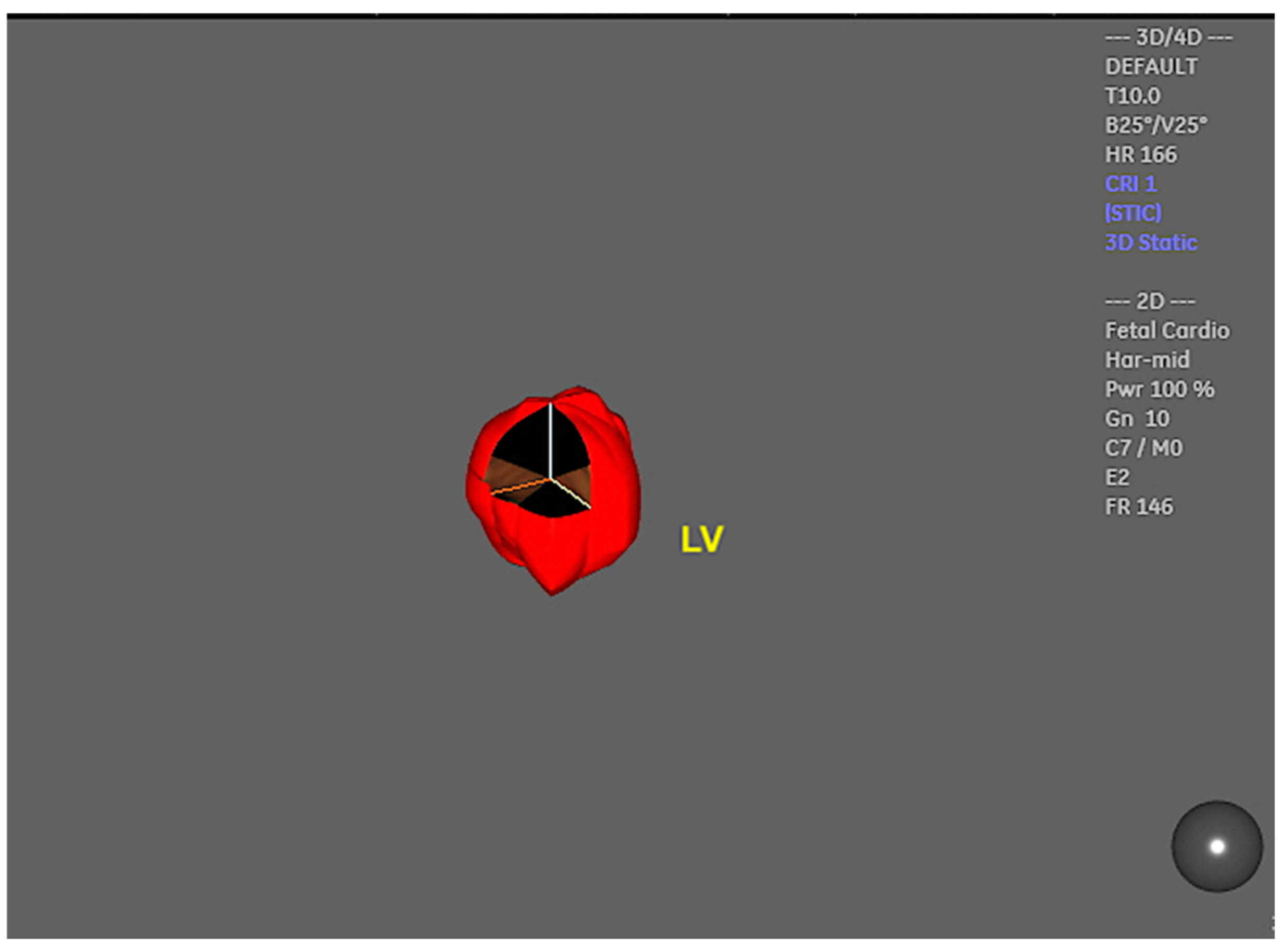
Figure 19.
FINE navigation (known as “5D-Heart”) in (A) a case of a malalignment type ventricular septal defect (**, yellow arrows) and in (B) a case of complete atrioventricular septal defect (AVSD). In case (A) observe: the overriding of the aorta (Ao). In case (B), the four-chamber, the five-chamber and LV outflow tract (LVOT) views (yellow arrows) draw attention to this diagnosis. ***common AV valve; VSD: ventricular septal defect; ASD: primum atrial septal defect; GN: LVOT with a “goose neck” shape.
Figure 19.
FINE navigation (known as “5D-Heart”) in (A) a case of a malalignment type ventricular septal defect (**, yellow arrows) and in (B) a case of complete atrioventricular septal defect (AVSD). In case (A) observe: the overriding of the aorta (Ao). In case (B), the four-chamber, the five-chamber and LV outflow tract (LVOT) views (yellow arrows) draw attention to this diagnosis. ***common AV valve; VSD: ventricular septal defect; ASD: primum atrial septal defect; GN: LVOT with a “goose neck” shape.
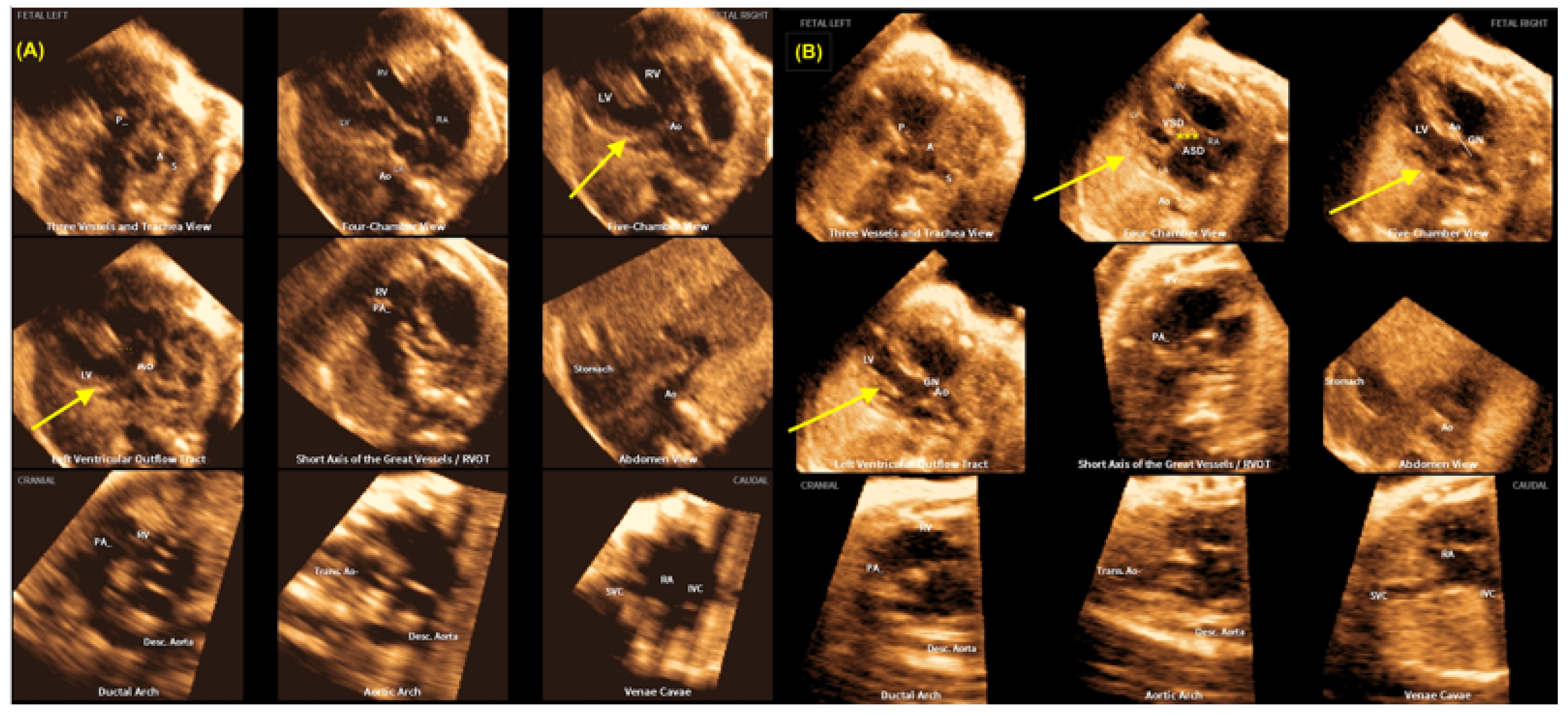
Figure 20.
Automatic measurement of the fetal the cardiac axis (40.30) using Artificial Intelligence (‘Learning Machine’) in a normal heart using Fetal Intelligent Navigation Echocardiography (FINE), also known as “5D Heart”. LV: left ventricle; LA: left atrium; RA: right atrium; RV: right ventricle; A or Ao: aorta; P or PA: pulmonary artery; S: superior vena cava; IVC: inferior vena cava; Desc: descending; Trans: transverse.
Figure 20.
Automatic measurement of the fetal the cardiac axis (40.30) using Artificial Intelligence (‘Learning Machine’) in a normal heart using Fetal Intelligent Navigation Echocardiography (FINE), also known as “5D Heart”. LV: left ventricle; LA: left atrium; RA: right atrium; RV: right ventricle; A or Ao: aorta; P or PA: pulmonary artery; S: superior vena cava; IVC: inferior vena cava; Desc: descending; Trans: transverse.
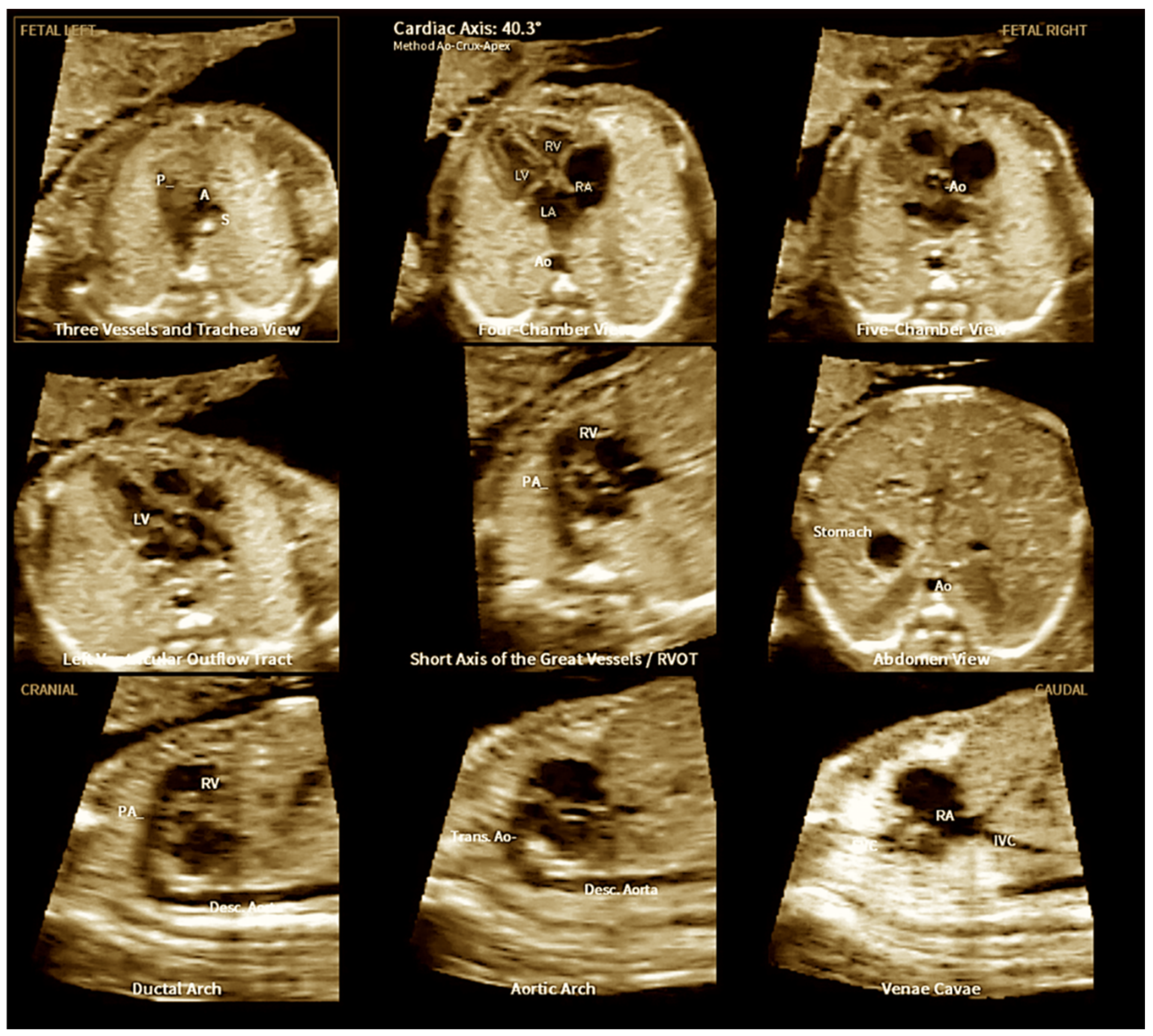
Figure 21.
3D physical model of a fetus with transposition of great arteries (TGA). RV: right ventricle; Ao: aorta; LV: left ventricle; P: pulmonary artery.
Figure 21.
3D physical model of a fetus with transposition of great arteries (TGA). RV: right ventricle; Ao: aorta; LV: left ventricle; P: pulmonary artery.
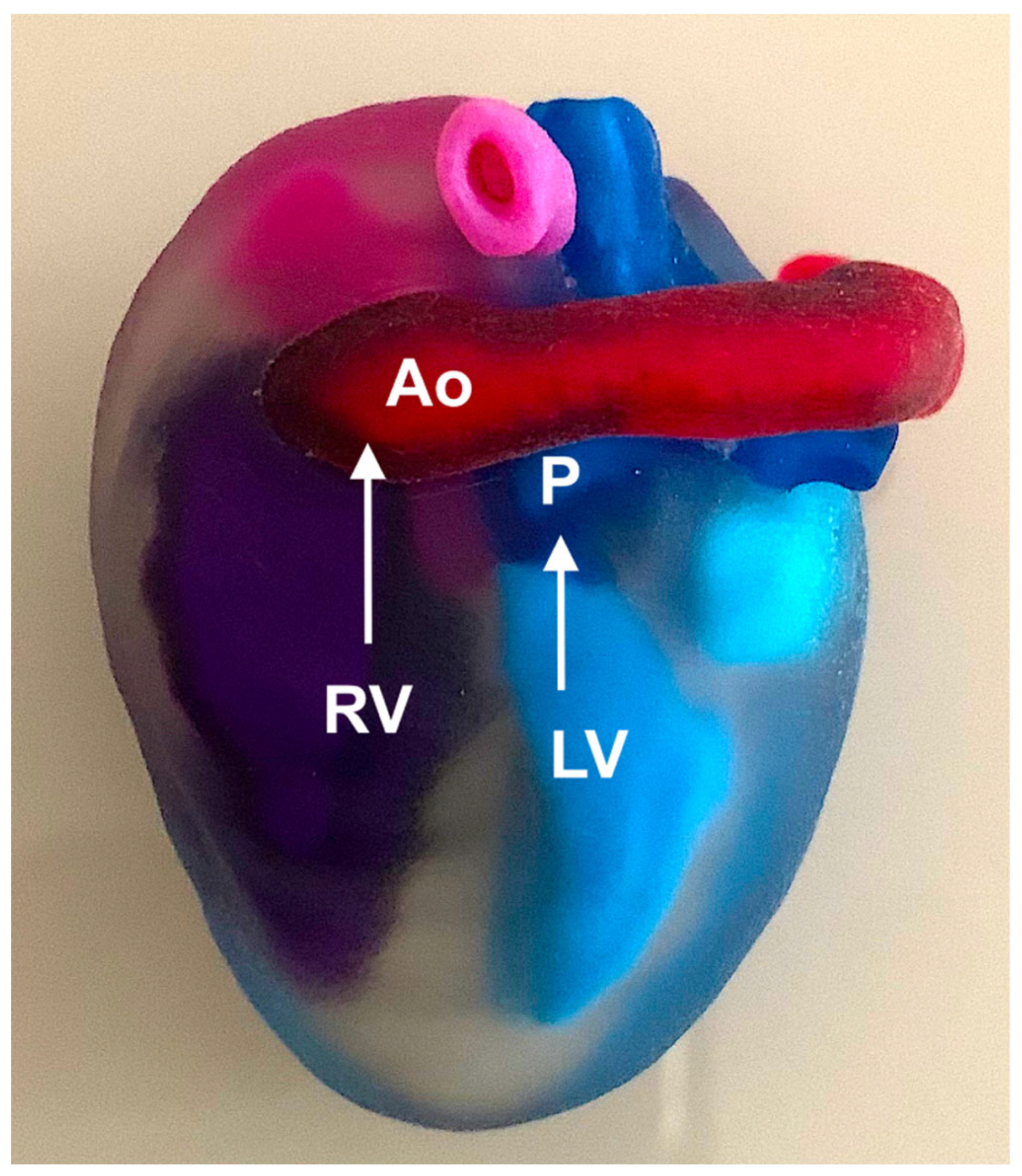
Figure 22.
Three-dimensional (3D) virtual model of fetal heart in a fetus with transposition of the great arteries (TGA) and in a fetus with Ebstein anomaly. RA: right atrium; RV: right ventricle; LA: left atrium; T: tricuspid valve; M: mitral valve; LV: left ventricle; Ao: aorta; P: pulmonary artery. .
Figure 22.
Three-dimensional (3D) virtual model of fetal heart in a fetus with transposition of the great arteries (TGA) and in a fetus with Ebstein anomaly. RA: right atrium; RV: right ventricle; LA: left atrium; T: tricuspid valve; M: mitral valve; LV: left ventricle; Ao: aorta; P: pulmonary artery. .
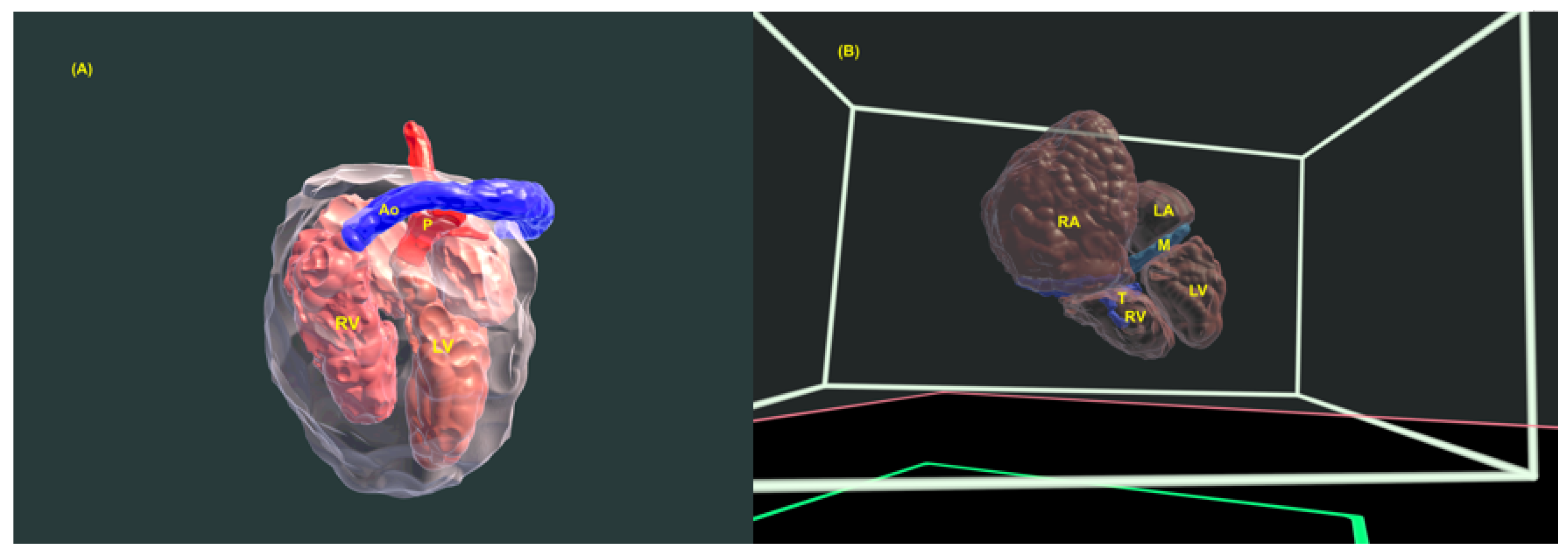
Figure 23.
Following the acquisition of images of the fetal heart with Tetralogy of Fallot from 3D ultrasound (heart volumes) using tools from the Slicer 3D software (Birmingham, UK), the cardiac structures were segmented, with each cavity identified by a different color (right and left atrium, right and left ventricles, aorta, pulmonary artery, vena cava and pulmonary veins). Thereafter, a raw file format was generated. Based on the aforementioned 3D data, physical 3D models of the fetal heart can be printed on 3D printers. Ao: aorta; LA: left atrium; P: pulmonary artery; RA: right atrium; LV: left ventricle; RV: right ventricle; VSD: ventricular septal defect.
Figure 23.
Following the acquisition of images of the fetal heart with Tetralogy of Fallot from 3D ultrasound (heart volumes) using tools from the Slicer 3D software (Birmingham, UK), the cardiac structures were segmented, with each cavity identified by a different color (right and left atrium, right and left ventricles, aorta, pulmonary artery, vena cava and pulmonary veins). Thereafter, a raw file format was generated. Based on the aforementioned 3D data, physical 3D models of the fetal heart can be printed on 3D printers. Ao: aorta; LA: left atrium; P: pulmonary artery; RA: right atrium; LV: left ventricle; RV: right ventricle; VSD: ventricular septal defect.
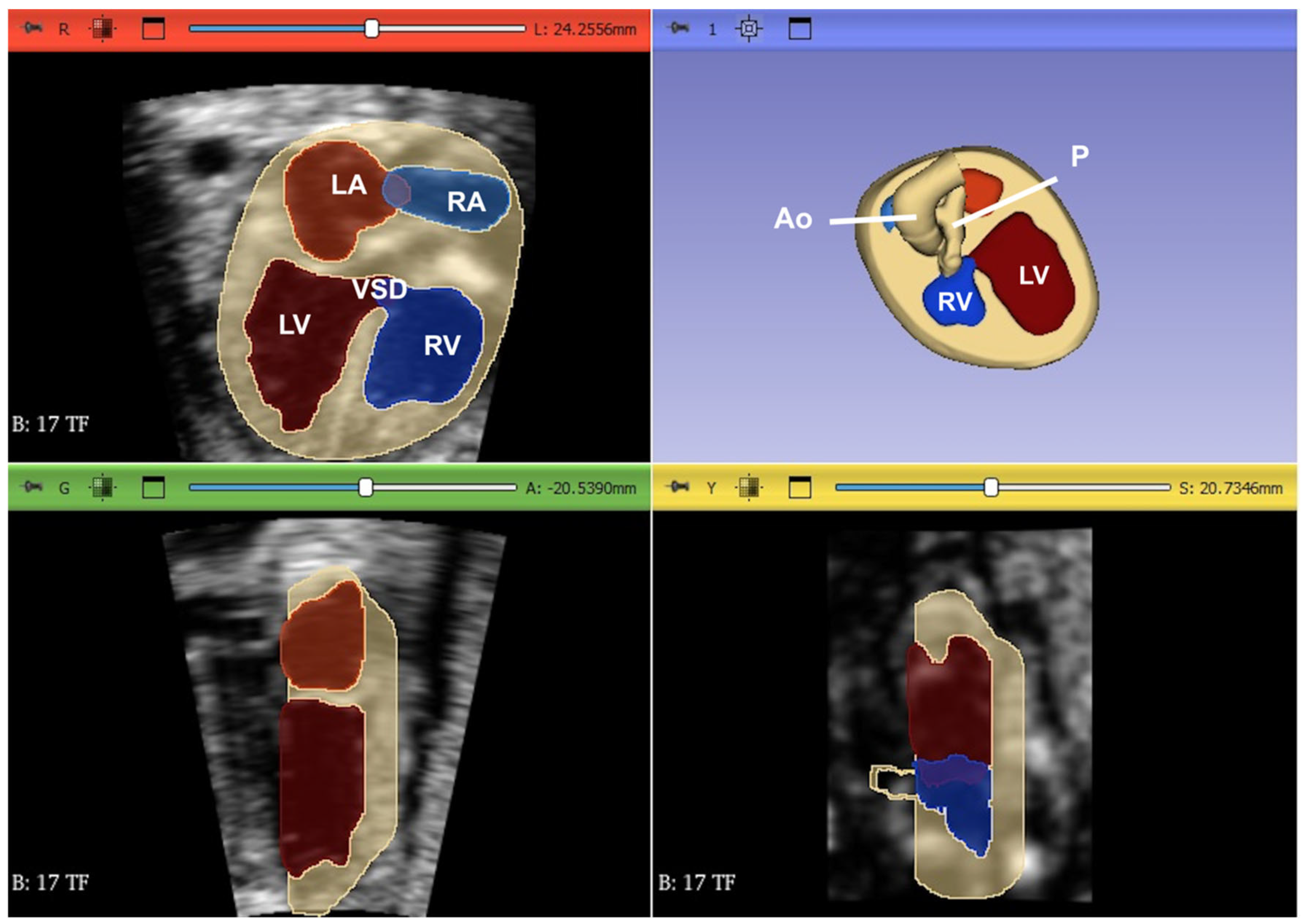
Figure 24.
A. Fetal cardiac MRI (fCMR) performed at 32 weeks and 5 days. Images were obtained at 1.5 T using a balanced turbo field echo (BTFE) sequence, gated with an MRI compatible Doppler ultrasound (DUS) device (North Medical, Hamburg, Germany). 4-chamber view in systole (A) and diastole (B). LA: left atrium; LV: left ventricle; RA: right atrium; LA: left atrium.
Figure 24.
A. Fetal cardiac MRI (fCMR) performed at 32 weeks and 5 days. Images were obtained at 1.5 T using a balanced turbo field echo (BTFE) sequence, gated with an MRI compatible Doppler ultrasound (DUS) device (North Medical, Hamburg, Germany). 4-chamber view in systole (A) and diastole (B). LA: left atrium; LV: left ventricle; RA: right atrium; LA: left atrium.
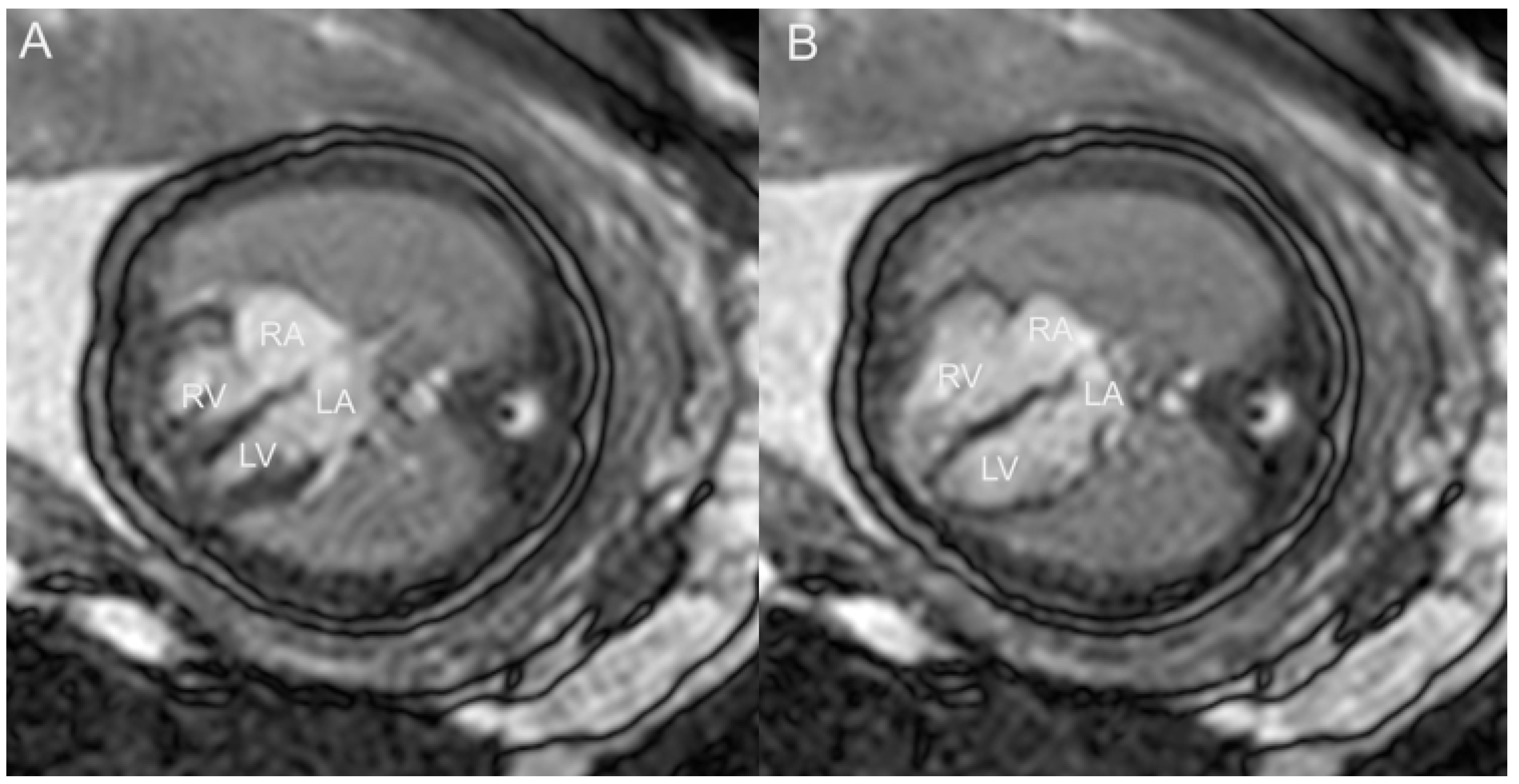
Figure 25.
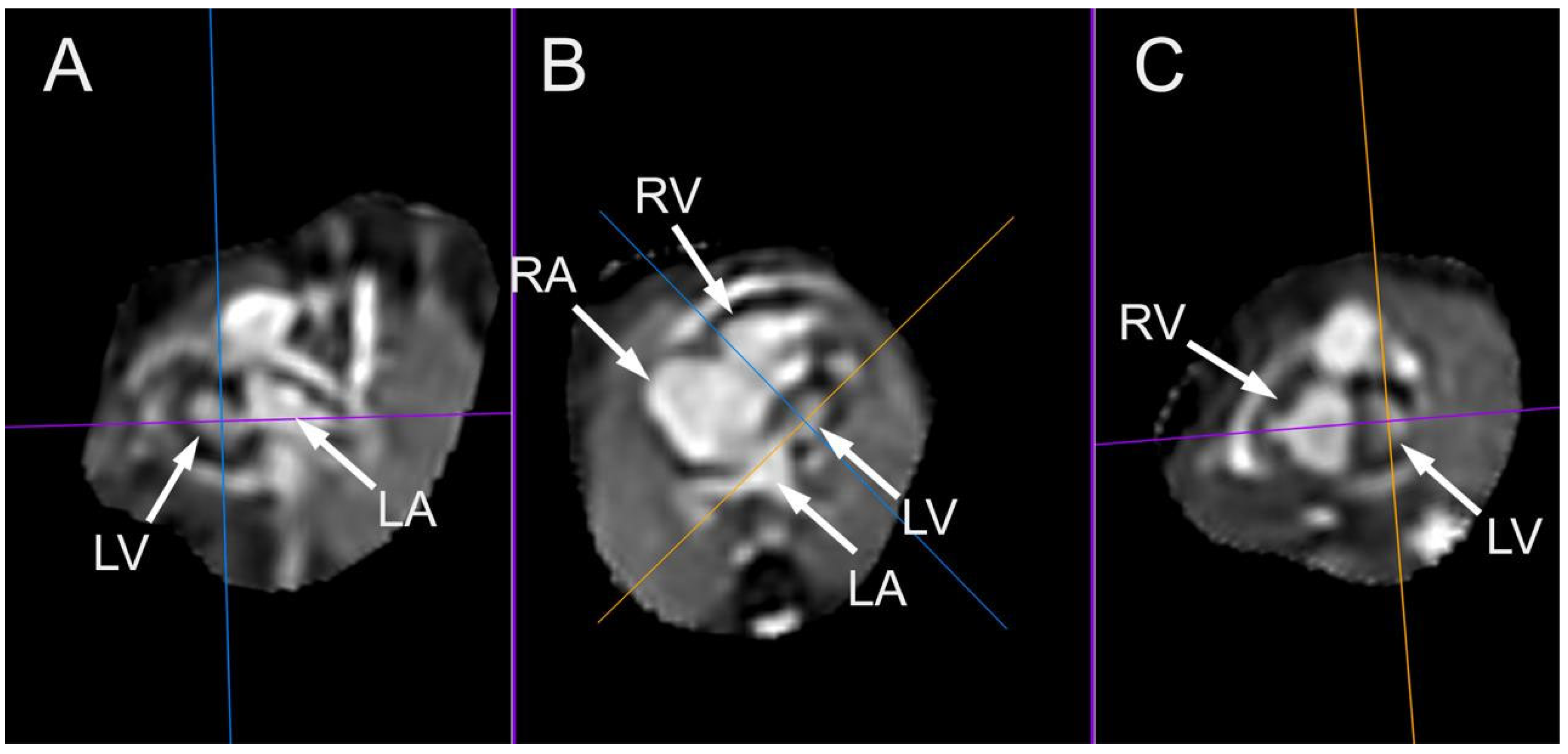
Multiplanar display image of a case of hypoplastic left ventricle examined at 32 weeks and 3 days. Images were acquired using balanced turbo field echo (BTFE) sequence at 1.5T. kt-sense acceleration was used during acquisition. Images were postprocessed using a super-resolution pipeline, resulting in an isovoxel 3D volume dataset. Panel A: sagittal 2-chamber view. Panel B: 4-chamber view. Panel C: coronal short axis view through the ventricles. LA: left atrium; LV: left ventricle; RA: right atrium; RV: right ventricle.
Figure 25.
Multiplanar display image of a case of hypoplastic left ventricle examined at 32 weeks and 3 days. Images were acquired using balanced turbo field echo (BTFE) sequence at 1.5T. kt-sense acceleration was used during acquisition. Images were postprocessed using a super-resolution pipeline, resulting in an isovoxel 3D volume dataset. Panel A: sagittal 2-chamber view. Panel B: 4-chamber view. Panel C: coronal short axis view through the ventricles. LA: left atrium; LV: left ventricle; RA: right atrium; RV: right ventricle.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



