
Submitted:
04 November 2024
Posted:
05 November 2024
You are already at the latest version
Abstract
Calcium (Ca) and phosphorus (P) are critical nutrients and essential elements for the growth and development of humans. Since proper diagnosis and treatment are indispensable parts of personalized and precision medicine in patients with chronic diseases, in addition to unknown about the role of Ca/P ratios, the main aim of this cross-sectional study was to assess serum and urine Ca and P levels, the Ca/P ratios and their association with health and nutritional biomarkers in children and adolescents with chronic diseases. We carried out anthropometric, body composition, clinical evaluation, biochemical analysis, dietary survey, and bone densitometry methods. In 39 patients (2-19 years, 61.5% women, 56.4% adolescents), results showed that 20% of subjects had hypercalciuria, 23% had high Ca/Cr rate, and 44% exhibited hyperphosphaturia. No one patient was hypocalcemic or hyperphosphatemic. Serum and urinary Ca/P ratios were 2.12 and 0.13, respectively. 36% and 5% of subjects had hypophosphatemia and hypercalcemia, respectively. Serum and urine Ca and P levels were associated with several nutritional parameters studied. This study confirms the need to investigate Ca, P, and their relationship in urine in childhood.
Keywords:
calcium-phosphorus product
; phosphatase alkaline
; physical activity
1. Introduction
Phosphorus or phosphate (P) and calcium (Ca) homeostasis are critical for several physiological processes, such as DNA structure, cell signaling, blood coagulation, muscle contraction, bone mineral density, and neuronal excitation [1,2].
Calcium is an intracellular and extracellular ion necessary for muscle and
heart contraction, rhythm, neurological function, bone and tooth structure,
blood clotting, hormone release, and enzyme function [3].
Abnormal Ca is associated with the risk of osteoporosis, hypertension, colon
cancer, breast cancer, kidney stones and lead harming [4]. Phosphorus plays a substantial role in all cell
and tissue maintenance and repair [5]. It
is an essential element closely related to dietary intake. Recent studies have
found that increased P loading can trigger the activation of inflammatory
signaling in various parts of the body, triggering cardiovascular diseases
(CVD), tumorigenesis, depression and neuronal disorders [6]. Serum Ca and P levels are approximately and
inversely related [7]. The kidneys, intestine
and bones, through the combined effects of phosphotropic and calciumtropic
hormones, parathyroid hormone (PTH), active vitamin D (Vit-D) 3 and fibroblast
growth factor 23 (FGF23) tightly regulated plasma Ca and P levels [8].
It is fundamental to compare urinary excretions of
minerals with their regular reference ranges to detect mineral metabolic
disorders. In adults, these reference standards vary within relatively narrow
limits. In the pediatric population, these ranges vary widely by race, country
and age, making it impossible to have defined references [9]. Renal P reabsorption controls serum P
concentration and is quantified as tubular P reabsorption and expressed as the
renal P threshold, closely reflecting the normal range of serum P [10]. Since endogenous and dermal Ca loss is low,
the relationship between dietary Ca and its loss depends on the efficiency of
its intestinal absorption, skeletal turnover and balance, and Ca urinary
excretion in the kidneys [11]. The kidneys may
under excrete Ca, as in some hypercalcemic disorders, and over excrete Ca, as
in some patients with nephrolithiasis, and under excrete P, as in renal failure
and defects in FGF23 action, and over excrete P as in some renal tubular
disorders and renal P loss due to excess FGF23 and other phosphatonins [12]. Hypocalcemia is frequently due to
dysregulation of PTH production, Vit-D deficiency (VDD), and various
gastrointestinal (GI) disorders that cause malabsorption. Hypophosphatemia is
due to reduced intake, poor GI absorption, increased renal excretion, or
transcellular redistribution from extracellular fluid into cells [13].
The Ca/P ratio in the diet is a factor that
deserves special attention for bone health. Research in animals and humans
indicates that a low Ca/P ratio is detrimental to the skeleton, but a high Ca
intake would not counteract the adverse effect of a high P intake, especially
from food additives [11]. Nevertheless, little
is known about the relationship between serum and urine Ca and P levels and
their ratios in healthy children populations and even less in patients with
non-communicable diseases (NCDs). In cystic fibrosis (CF) patients, there was a
meaningful association between serum and urine Ca/P ratios, suggesting that
both might be useful as Ca and P metabolism indicators [1]. We believe personalized and precision medicine
is helpful and indispensable tools to improve the quality of life in pediatric
ages with chronic conditions. Ensuring an adequate supply of Ca and P in
childhood populations with chronic conditions should be a priority. We
hypothesize that children and adolescents with chronic illnesses could have
abnormal excretion of Ca and P levels. Therefore, the main aim of this study
was to evaluate serum and urine Ca and P levels and their Ca/P ratios and their
association with health and nutritional biomarkers in a group of children and
adolescents with chronic diseases.
2. Materials and Methods
2.1. Study site, Design and Participants
The design of this prospective observational study
(Figure 1) has been previously published
[14,15,16,17]. Patients were successively referred to the Nutrition Unit of the
Pediatric Service of the University Clinical Hospital of Valladolid, Spain, for
18 months. The inclusion criteria were patients under 19 years of age with
chronic illnesses. Chronic diseases include malnutrition (cause unknown),
syndromic diseases, encephalopathies, renal diseases, hyperlipidemia, and
eating disorders. We excluded patients with CF [1],
acute infection, those hospitalized, and those who refused to participate.
2.2. Ethical Consideration
The Ethics Committee of the University Clinical
Hospital of Valladolid (INSALUD-Valladolid, February 14, 2002) approved the
study protocol. We carried out this study following the recommendations of the
Declaration of Helsinki. Family members/guardians of all patients signed the
informed consent before the study.
2.3. Clinical Evaluation
We assess each
patient for symptoms related to their nutritional status and daily physical
activity (PA). We used a questionnaire based on the Global Physical Activity
Questionnaire (GPAQ), adapted to the patient's age [18], the week
before the clinical assessment, recording the total time spent on PA (TTSAF:
sport, school gymnastics, and physiotherapy) in hours/week. We classified them
into three categories: active/very active PA, light PA, and sedentary/very
sedentary PA.
2.4. Assessment of Phenotypic Characteristics
We assessed
anthropometric measurements of weight, height, wrist, hip, waist, and hip, and
mid-upper-arm circumference using standard techniques. We calculated using
Frisancho
[19]
and Orbegozo tables
[20]
, the Z-score of weight-for-age, height-for-age
(HA), height-age or age-for-50°height (A50°H), weight-for-height, BMI-for-age
(BMI), BMI-height-age (BHA), nutritional index,
Waterlow I and II (weight and height)
[21]
, and upper arm area, upper arm
muscle area, upper arm fat area, mid-arm muscle circumference, fat-free
mass (FFM) and fat mass (FM), waist/hip ratio, and waist/height index. Using a
Holtain Skinfold Caliper (Holtain LTD, Crymych, UK), triceps, biceps,
subscapular, and suprailiac skinfolds thickness and the sum of skinfolds were
measured. The BMI Z-score was used to classify patients as underweight (<−2
standard deviations [SD]), eutrophic (−2 to +2 SD), or obese (> +2 SD). Body
composition assessed three compartments, including FM, bone mineral content,
and FFM, using anthropometric measurements and bioelectrical impedance analysis
(BIA) [RJL BIA-101 (RJL System, Detroit, MI, USA)]. We calculated body fat
percentage [(BF%: fat mass/total weight) × 100], and the
excess body adiposity was
≥
25% for boys and
≥
30% for girls. The fraction of body fat was estimated using the fat
mass index [FMI = fat mass/height2 (kg/m2)] and the free
fraction of body fat with the fat-free mass index [FFMI = fat-free mass/height2
(kg/m2)]
[22]
. Bone mineral density (BMD) was assessed by
quantitative ultrasound [DBM Sonic 1200 IGEA (Emsor S.A., Madrid, Spain)] using
bone conduction speed (BCS: absolute value and Z-score) of the last four
fingers of the non-dominant hand, using a population of healthy young Spaniards
matched by age and sex from the Community of Castilla y León as a reference
population
[23,24]
. Basal energy expenditure (BEE) was measured with
Indirect Calorimetry (IC) in fasting, using a canopy system under standardized
conditions [Deltatrac II (Datex-Ohmeda. Helsinki, Finland)].
2.5. Dietary Assessment
In a prospective 72-hour dietary survey (including
one of the weekend days), parents/guardians/patients recorded all foods eaten
and their amounts (using common kitchen measurements) the week before the blood
test. Daily energy intake; fiber; carbohydrates; protein; lipids;
monounsaturated, polyunsaturated, and saturated fats; Vit-A, Vit-B1, Vit-B2,
Vit-B6, Vit-B12, Vit-C, Vit-D, Vit-E, niacin and folic acid; and Ca, Mg, iron
(Fe), zinc (Zn), and iodine, was calculated as the percentage of Dietary
Reference Intake (% DRI, normal range: 80% - 120%) or adequate intake using the
Mataix Food and Health software (FUNIBER, v.1.1.5. 2005), which provided the
percentage of actual nutrient intake relative to the Spanish recommendations [25,26].
The Ca/Mg intake ratio used the cut-off points of 1.70-2.60 [27].
2.6. Laboratory Exploration
Complete blood count, biochemical profile, and
acute-phase protein activity, including C-reactive protein and erythrocyte
sedimentation rate, and serum prealbumin, albumin, transferrin, lymphocytes,
total cholesterol, and low-density-lipoprotein cholesterol, were measured using
standardized methods. We assessed the total immunoglobulin (Ig) G levels,
IgG1-4, IgA, IgM and IgE, complement C3 and C4, CD3, CD4, CD8, CD16+56, CD19
lymphocytes and CD4/CD8 ratio, insulin-like growth factor-1 and insulin-like
growth factor-binding protein 3, folic acid, beta-carotene, Vit-B12, Vit-C,
Vit-D, Vit-E, Ca, P, Fe, Mg [17,28], serum
Ca/Mg ratio is 3.91–4.70 [29], and the serum Mg/Ca ratio of 0.4 is
optimal (0.36–0.28 too low) [30,31], using
methods standardized. Serum Zn [15] and copper
(Cu) [16] were evaluated in the Department of
Chemistry of the University of Valladolid. The Cu/Zn ratio is 0.7 to 1.0 [32], and the Zn/Cu ratio is <4.0 [33].
For serum Vit-D: severe deficiency <5 ng/mL,
deficiency <20 ng/mL, insufficiency 20-30 mg/mL, sufficiency >30 ng/mL [34,35]. Serum Ca was corrected when the serum
albumin level was <4.0 g/dL, using the formula: Corrected Ca (mg/dL) =
measured Ca (mg/dL) + [4 - albumin (g/dL) [36];
normal from 8.8 to 10.8 mg/dL [37], and
hypercalcemia >10.5 mg/dL or ionized Ca > 5.25 mg/dL [32]. Normal serum P is from 4.5 to 6.5 mg/dL, hypophosphatemia
<4.5 mg/dL, and 8yperphosphatemia >6.5 mg/dL [37].
The serum Ca/P ratio <18 years is 1.7-2.7, and >18-34 years is 2.2-3.2 [39]. >3.5 for primary hyperparathyroidism (PHPT)
[7],
and <2.3 (normal range from 2.3 to 3.3 for HypoPT) [40]. The
Ca-P product (Ca-PP) >55-60 mg2/dL2 risk factor for
increasing CV morbidity [41,42], >72 mg2/dL2
increased relative mortality risk [42].
Serum creatinine (Cr) for infants is 0.2-0.4 mg/dL, for children is 0.3-0.7
mg/dL, and for adolescents is 0.5-1.0 mg/dL [37]. Alkaline phosphatase (ALP) from 1 to
<10 years is 156-369 U/L, from 10 to <13 years is 141-160 U/L, from 13 to
<15 years female is 62-280 U/L, male is 57-127 U/L, from 15 to <17 years
female is 54-128 U/L, male is 89-365 U/L, from 17 to <19 years female is
48-95 U/L, male is 59-164 [43].
In 24-hour urine samples, Ca, P, and Cr levels were
assessed by standardized methods. Hypercalciuria >4 mg/kg/d at any age [44] and >200 mg/L (20 mg/dL) [45]. Hypercalciuria by Ca/Cr rate from 2 to 4 years
is >0.28, children ≥4 years is >0.20
(<0.20 is normal while less than 0.18 mg Ca/Cr rate is optimal) [45,46]. Urinary Ca excretion (UCaE): Urine Ca x (serum
Cr/urine Cr) <0.175 in men and < 0.150 in women [47]. Urinary Cr in childhood is 15-25 mg/kg/day for
men and 10-20 mg/kg/day for women [48], and
24-hour urine creatinine from 500 to 2000 mg/d [49,50]. Urine P: 700-900 mg/d [51], for body weight: 7.8-17 mg/kg/d [52]. Fractional excretion of P (FEP): FEPO4 = [PO4
(Urine) * Creatinine (Serum)] / [PO4 (Serum) * Creatinine (Urine)] * 100:
<20% are considered normal [53]. The Fractional Tubular Reabsorption of
Phosphate (TRP) {1 − [(urinary P × serum Cr) / (urinary Cr × serum P)]} x
100 [54] is 78-91% [52]. Tubular maximum P reabsorption per glomerular
filtration rate (TmP/GFR): If TRP ≤0.86,
TmP/GFR = TRP x serum P. If TRP >0.86, TmP/GFR = α x serum P, where α = 0.3
x TRP/{1-(0.8 x TRP)} [55]. TmP/GFR from
1 to 5 years = 3.25 to 5.51 mg/dL, from 6 to 12 years = 3.00 to 5.08 mg/dL;
from 13 to 15 years = 2.82 to 5.20 mg/dL, and ≥16
years is 2.60-3.80 mg/dL [56]. TmP/GFR <2.8
mg/dL indicated the renal tubular P loss [55].
Ca-P product from 40.42 to 89.18 (data no published). The urine Ca/P ratio
range is from 0.89 to 1.62 [1].
2.7. Statistical Analysis
We classified participants by chronological age (CA) group according to Tanner stages in children and adolescents and by nutritional status based on their BMI in obese, eutrophic, and underfed groups. The main variables were Ca, P levels, Ca/P ratio and Ca-PP in serum and urine samples. Secondary variables were clinical and anthropometric assessments, body composition, bone densitometry, diet, complete blood count, blood and urinary biochemistry, and BEE. We show anthropometric (quantitatively and Z-scores) and biochemical results as mean, median, quartiles, SD, and ranges, and the duration of diseases (DD) in months. We studied biomarker status and expressed comorbidities as a percentage. To analyze unpaired or paired variables, we used a two-tailed Student t-test. We performed a one-way analysis of variance (ANOVA test) and Pearson’s bivariate correlation test to analyze normally distributed values. We analyzed the categorical results using Pearson’s Chi-square test (X2) with Yates’ correction and Fisher’s exact test (FET). We used non-parametric tests for variables with non-normal distribution. We calculated odds ratios (OR) to estimate the magnitude of the association between exposure and disease. Only correlations and associations with an r/R2 value > 0.500, p < 0.01** were included in the final analysis. The effects of various factors on Ca and P levels were analyzed using a linear/multilinear regression model (direct method). We used IBM SPSS software version 29.0 (IBM Corp., Armonk, NY, USA) for data management and statistical analysis. We set the significance level at p < 0.05* and <0.01**.
3. Results
The results of these patients have been previously published [14,15,16,17]. Table 1 reports the clinical and biochemical characteristics of 39 participants (61.5%, 24 women) by BMI groups. The mean age was 10.4 ± 3.9 years (2 to 19 years), 43.6% of subjects (17 cases) were children, and 56.4% (22 cases) were teenagers. The mean A50°H was 0.6 ± 3.9 months lower than CA, but there was no significant difference between either. There was a significant correlation between CA and A50°H (r = 0.659, p < 0.001), and both had a noteworthy correlation with HA (r= 0.804, p < 0.001, and r = 0.926, p < 0.001, respectively). Among the four patients with short stature, three teenagers had A50°H <10 years (HA <-2SD). Only one child had A50°H >10 years (HA > +2SD) among children <10 years of CA. The mean DD was 73 ± 45 months (6 to 182 months) with no significant differences between groups. 30.8% (12 cases) of participants had multiple health conditions. Based on BMI, 51.3% (20 cases), 33.3% (13 cases) and 15.4% (6 cases) of patients were obese, malnourished and eutrophic, respectively. BMI had a meaningful correlation (p < 0.001) with BFP (r = 0.894), FMI (r = 0.980) and FFMI (r = 0.960), and females had a higher BFP than males. The BHA had a positive and significant correlation and association with BMI (r = 0.913 and R2 = 0.683, p < 0.001). The mean TTSPA was 3.8 ± 2.2 hours/week. There was no significant difference between groups. 61.5% were active/very active PA, 20.5% had light PA, and 17.9% were sedentary/very sedentary. TTSPA and BCS significantly correlated (r = 0.423, p = 0.014). The mean BCS’s AV (1934 ± 76) and Z-score (-0.5 ± 1.0) were regular in the whole series and by gender, age and BMI groups. BCS was positive associated with age (R2 = 0.496, p < 0.001). Only three cases had low BCS <-2DS.
The diet for the entire series was normocaloric (94% DRI), hyperproteic (283% DRI), with regular cholesterol intake (100% DRI), carbs consumption (81% DRI) and total lipids (112% DRI). The diet was deficient in Vit-D (76.9%, 30 cases), Zn (71.8%, 28 cases) and iodine (69.2%, 27 cases). The mean iodine intake was significantly lower in undernutrition patients than in eutrophic and obese ones. 12.8% (5 cases) had high Vit-D consumption. The mean dietary Ca intake (94% DRI) was regular and there were no significant differences by groups. 46.2% (18 cases) and 17.9% (7 cases) of patients had deficient and high dietary Ca intake, respectively. 38.5% of patients (15 cases) had simultaneously deficient Ca and Vit-D eating. The mean of serum Ca, Cr, P, the Ca/P ratio and Ca-PP were regular, and there was no significant difference between groups. No patients had hypocalcemia, but two subjects had hypercalcemia >10.5 mg/dL. The mean serum Vit-D levels in the entire series were in insufficient range. 17.9% of subjects had Vit-D levels ≥30 mg/dL. 82% of patients (32 cases) had a Vit-D level <30 mg/dL: 48.7% (19 cases) had VDD, and 33.3% (13 cases) had insufficient Vit-D levels. No patients had hyperphosphatemia, but 35.9% (14 cases) of participants had hypophosphatemia. 7.7% (3 cases) of patients had simultaneous hypophosphatemia and VDD. Two patients had higher serum Ca/P ratio. 7.7% (3 cases) of subjects had higher Ca-PP (from 55.1 to 62.6 mg2/dL2). The mean ALP level was high in the whole series and all groups, with no significant differences. 56.4% of participants had higher ALP levels.
The mean urine Ca, Cr and P (mg/kg/d and 24-h), Ca/Cr rate, UCaE, FEP, TRP and TmP/GFR were regular. 41% (16 cases) of the patients presented hypercalciuria. 28.2% (11 cases) and 20.5% (8 cases) of participants had high and low urine Cr excretion (mg/kg/d), respectively. No patients had Cr loss >2000 mg/d. 23.1% of participants (9 cases) had a high Ca/Cr rate. 12.8% of patients had abnormal UCaE (5 cases). 20.5% (8 cases) of subjects had a urine Ca loss >4 mg/kg/day. 15.4% (6 cases) had a urine Ca loss >200 mg/L. Only three cases had simultaneously high urine Ca >4 mg/kg/d and >200 mg/L. The mean urine P (mg/kg/d and 24-hour) was high. 51.3% of subjects (20 cases) exhibited hyperphosphaturia (mg/kg/d), 20.5% of patients (eight cases) had 24-urine P >900 mg/d, and 7.7% (3 cases) patients had FEP >20%. 23.1% (9 cases) of patients had coincident VDD and hyperphosphaturia. The mean urine Ca/P ratio was 0.14 ± 0.11, and the Ca-PP was 50.2 ± 57.5. Only 15.4% (6 cases) of subjects had TRP <85% and 12.8% of participants (5 cases) had a high TmP/GFR. No one patient had TmP/GFR < 2.8 mg/dL. 17.9% (7 cases) of patients had simultaneously hypercalciuria (>4 mg/kg/d) and hyperphosphaturia (>17 mg/kg/d, X2 = 0.022).
Table 2 shows the differences among subjects with chronic conditions in the entire series and Table 3 displays the OR in the whole series.
Figure 2 shows the meaningful relationship between 24-hour urine Ca (p = 0.001), P and Cr (p < 0.001) excretion by age in this series. There was no significant association between urine and serum Ca/P ratio. Serum and urine Ca-PP had a direct and meaningful association when they were adjusted to the age (R2 = 0.106, p = 0.043). Table 4 shows the features of hypercalciuria and hyperphosphaturia patients.
Table 5 summarizes the regression analysis with R2 > 0.500. We display significant (r > 0.500, p < 0.01) correlations (Tables S1–S3) between dietary Ca, serum and urinary levels of Ca, P, Ca/P ratio, and Ca-PP with the nutritional and health biomarkers studied.
4. Discussion
Interestingly, little is known about the serum and urinary Ca and P relationship in pediatric populations. This study assessed serum and urine Ca and P levels, their Ca/P ratios and their association with health and nutritional indicators in a series of children and adolescents with chronic diseases. The results pointed out that the mean dietary Ca intake was regular. 46.2% and 17.9% of individuals had high and deficient Ca intake, respectively. The mean serum Ca, P, Cr, Ca/Cr, the Ca/P ratio and Ca-PP were regular. No patients had hypocalcemia or hyperphosphatemia. Two patients had hypercalcemia, and 35.9% had hypophosphatemia. Two individuals had a higher serum Ca/P ratio. 7.7% of subjects had a higher Ca-PP. 38.5% (15 cases) of patients had simultaneously deficient Ca and Vit-D eating. 7.7% (3 cases) of patients had simultaneous hypophosphatemia and VDD. Although 20.5% of patients had urine Ca loss >4 mg/kg/d, 15.4% had urine Ca loss >200 mg/d. 23% had a high Ca/Cr rate. 51.3% of subjects had hyperphosphaturia (mg/kg/d), 15.4% had 24-urine P >900 mg/d, and 7.7% (three cases) had FEP >20%. 23.1% (9 cases) of patients had coincident VDD and hyperphosphaturia. Only 10.3% of individuals had TRP <85% and 17.9% had high TmP/GFR. No one patient had TmP/GFR < 2.8 mg/dL. The mean urine Ca/P ratio was 0.14, and the Ca-PP was 50.2.
4.1. Clinical Status
First, we characterized this series of pediatric patients with chronic conditions. The average age was 10.4 ± 3.9 (2 to 19 years), and the mean A50°H was 9.9 ± 5.1 years. A50°H was 0.6 ± 3.9 months lower than CA, without significant difference. There was a meaningful correlation between CA and A50°H (r = 0.659, p < 0.001), and both had a noteworthy correlation with HA (r= 0.804, p < 0.001, and r = 0.926, p < 0.001, respectively). Only 5.1% (2 cases) of subjects were simultaneously short stature and underweight. Among the four patients with short stature, three teenagers had A50°H <10 years (HA <-2SD), indicating growth retardation. Only one child had A50°H >10 years (HA > +2SD) among children <10 years of CA, showing an increased growth rate. The A50°H would be a reasonable indicator of maturity in most children, as it is the age at which a child would have a height in the 50th percentile and would likely be close to the age at which most healthy children would have a similar level of sexual and physical development [57]. Besides, the population-average A50°H provides an empirical measure of the average stage of skeletal growth compared to the reference population [58]. In our series, 30.8% (12 cases) of patients had polymorbidity. According to the World Health Organization (WHO), the double burden of malnutrition refers to the coexistence of undernutrition (stunting) with overweight, obesity, or diet-related NCDs in individuals, households, and populations, occurring throughout life, posing a real and growing challenge to global health, with long-term, as in our series.
Additionally, in this series, BMI had a meaningful correlation (p < 0.001) with BFP (r = 0.894), FMI (r = 0.980) and FFMI (r = 0.960), and females had a higher BFP than males. These results are consistent with the fact that for the same BMI, women tend to have a BFP approximately 10% higher than men. These sex-specific differences in body composition depend on sex-based differences in patterns of energy substrate utilization. The unique actions of sex hormones and adipokines in each sex and their nutritional status and physical fitness influence these patterns [59]. It is crucial to consider that chronic diseases such as chronic kidney disease (CKD), Turner syndrome, and Marfan syndrome, among other chronic conditions, can affect linear growth and maturation, influencing the relationship between age, BP, and sexual maturation, leading to an underestimation (in short children) or an overestimation (in tall children) of BMI compared to their peers of the same CA [60]. Therefore, we assessed the BHA that had a positive and significant association with BMI (r = 0.913 and R2 = 0.683, p < 0.001). While only one child with a higher BMI was eutrophic by BHA, eight patients (five children and three adolescents) with lower BMI were considered eutrophic by BHA. Since in children with CKD from 5 years to adolescence, BHA reflects physical development in the same way as BMI in healthy children, BHA is the preferred method in children with CKD [61]. In 84.6% of our patients, the BMI and BHA gave the same nutritional status. Thus, this indicator could evaluate body composition in other pediatric chronic diseases.
Concerning PA, the mean TTSPA was 3.8 ± 2.2 hours/week. There was no significant difference between groups. Prior studies have noted the importance of PA in the health status of humans, especially in the growth and development of children and adolescents [62]. Children with chronic conditions have specific pathophysiologies that uniquely contribute to exercise tolerance. Regular exercise appears to be beneficial for children with CF, asthma, congenital heart disease, obesity, type 2 diabetes, juvenile idiopathic arthritis, and cancer [62,63]. Despite their health conditions, in our series, 61.5% of subjects were between active and very active, 20.5% had light PA, and 17.9% were very sedentary and sedentary. TTSPA and BCS significantly correlated (r = 0.423, p = 0.014), suggesting the importance of PA in the bone development in the pediatric population with chronic conditions. The WHO has suggested that PA confers benefits for bone health in the pediatric population [64]. Both PA and exercise may influence chronic disease by preventing the development of new chronic diseases (such as metabolic syndrome), by directly modifying the disease (disease reversal in type 2 diabetes), and or by helping to manage symptoms associated with the chronic disease (e.g., arthritis or cancer) [65].
Chronic health conditions in children can affect their growth potential, body composition, bone tissue, physiological stress, physical function, activity levels, and underlying causes that could alter energy balance. This heterogeneous set of factors has the potential to modify BEE, total energy expenditure (TEE), and, or the energy cost of growth [66]. In our study, the mean BEE of 1095 ± 409 kcal/d was lower than theoretical (1865 kcal/d, p < 0.001) and WHO’s formula (1342 kcal/d, p< 0.001). Moreover, IC had a positive correlation with 24-hour urine P (r = 0.709) and Cr (r = 0.733, p <0.001). In contrast, although in CF patients the mean basal EE (1077 ± 303 kcal) was lower than theoretical (p = 0.001), it was acceptable based on the WHO’s recommendation (p = 0.074), and as in our series, IC had a positive association with urine P [1]. There is little data on EE in sick children with different degrees of malnutrition. In hospitalized malnourished predictive equations underestimated EE in 92% of participants and recommended feeding goals, during the acute phase of illness, exceeded their EE [67]. Chronic diseases have a significant impact on energy homeostasis and growth. It is essential to understand EE in children to prevent malnutrition (undernutrition or obesity) through personalized dietary advice. EE is also important in those diseases where better clinical results occur with an optimal nutritional status, such as CF [68].
It is essential to note that the pediatric population with chronic diseases is a heterogeneous group, with substantial variation in their nutritional needs that differ from those of their healthy population peers [66]. The diet for the entire series was normocaloric (94% DRI), hyperproteic (283% DRI), with regular cholesterol intake (100% DRI), carbs consumption (81% DRI), and total lipids (112% DRI). The diet was deficient in Vit-D (76.9%, 30 cases), Zn (71.8%, 28 cases), and iodine (69.2%, 27 cases). Several studies show that iodine intake in Spain is inadequate. In 2015, the ANIVA study detected deficient iodine consumption in schoolchildren. The National Survey of Nutrition in the Child and Adolescent Population (ENALIA study, 2017) reported that iodine-rich foods were inadequate in children from 14 years old [69]. Moreover, although the diet was Zn deficient (71.8%, 28 cases), only three patients with hypozincemia had simultaneous deficient Zn intake. One 3-year-old eutrophic boy with hypercupremia (160 µg/dL), high Cu/Zn ratio (2.35) and hyperphosphaturia. There was a significant association between the Cu/Zn ratio and 24-hour urine P and Cr. In patients with chronic diseases, a Cu/Zn ratio > 1.00 is associated with inflammatory diseases, malnutrition, increased oxidative stress, and altered immune status [70].
Even though 12.8% (5 cases) had high Vit-D consumption, 76.9% of patients had deficient Vit-D (76.9%, 30 cases) intake. What is more, the mean serum Vit-D levels (23.6 ng/mL) in the entire series were in insufficient range. 17.9% of subjects had Vit-D levels ≥30 mg/dL, and 82% of patients (32 cases) had a Vit-D level <30mg/dL as follows: 48.7% (19 cases had <20 ng/mL) had hypovitaminosis D, and 33.3% (13 cases between 20-30 ng/mL) had insufficient Vit-D levels. In contrast, in La Rioja, in 21490 Spanish patients (14-105 years, 74% women), the mean serum Vit-D of 18.3 ng/mL was at insufficient levels, and 30.9% of the population had VDD (<12 ng/mL) and 32.8% (12–20 ng/mL) were in deficient range [71]. 45%, 30.8%, and 33% of obese, underfed, and eutrophic patients had simultaneously deficient Vit-D intake and VDD, respectively. Obese children and adolescents are at risk for Vit-D insufficiency or deficiency [14]. The prevalence of Vit-D deficiency in obese children and adolescents is high: 96.0% in Germany, 78.4% in the USA, and 92.0% in the Russian Federation [72]. The accumulation of adipose tissue, the development of adipocyte hypertrophy, impaired adipocyte function, and altered secretion profile of adipocytes lead to migration and transformation of macrophages and the development of inflammation in adipose tissue. This inflammation increases the synthesis of proinflammatory cytokines, and insulin resistance develops. In addition, it plays a crucial role in the hormonal regulation of glucose metabolism [72,73,74].
In childhood and adolescence, VDD is more prevalent in chronic illnesses, such as long-term systemic diseases that compromise renal, hepatic, gastrointestinal, skin, neurological, and musculoskeletal systems [75]. In our series, 38.5% of patients (15 cases) had simultaneous deficient Ca and Vit-D eating. Under normal conditions, Vit-D increases intestinal absorption of Ca and P while inhibiting PTH and stimulating FGF23 synthesis. PTH, Ca levels by the Ca-sensing receptor regulation, increase Ca levels but inhibit TPR, thus inducing hypophosphatemia. PTH stimulates both FGF23 and Vit-D synthesis. FGF23, synthesized by osteocytes in bone, inhibits both PTH and Vit-D while inhibiting TPR, also inducing hypophosphatemia. FGF23 increases distal tubular reabsorption of Ca, with a mild effect on Ca levels under physiological conditions [76]. Children with chronic diseases are deficient in Vit-D due to dietary restrictions, parental beliefs, common in inflammatory diseases, or decreased intestinal Ca absorption during corticosteroid treatment [77], enhance catabolism due to anticonvulsants or by enzymes induction with nifedipine, clotrimazole, etcetera [76]. Because children with chronic health conditions have Vit-D and Ca deficiency, the target threshold for Vit-D level should be >30 ng/mL. Also, in children, the risk of hypercalciuria and subsequent nephrolithiasis and or nephrocalcinosis is probably increased with persistently elevated Vit-D levels [75,76].
4.2. Calcium and Creatinine
Calcium status is the level of Ca intake that meets dietary recommendations for age, sex, and life stage [78], and Ca deficiency may happen due to prolonged lower Ca intake. In this study, the mean dietary Ca consumption (94% DRI) and serum Ca (9.3 mg/dL) were regular. While 46% (18 cases) of participants had deficient Ca eating, no patients had hypocalcemia [38]. This percentage is lower than 25.8% of inadequate Ca intake reported in 1176 Spanish schoolchildren [79]. It is essential to consider that although Ca deficiency in nutrition may not manifest clinically for a long time, it often causes insufficient bone mass in critical periods of life (first year, 1-2 years, 5-7 years, 12-14 years) and at an advanced age, contributing to osteoporosis [80]. In addition, some studies performed in various regions of the world show that the healthy pediatric population is deficient in Ca and Vit-D, which is why the incidence of rickets and osteomalacia is increasing [81]. As mentioned above, this is a risk factor in our series, where 38.5% of patients (15 cases) had simultaneous deficiencies in Ca and Vit-D intake. Also, in this series, 20.5% of the patients (8 instances) presented simultaneous deficiencies in kilocalories and Ca intake, with this deficient Ca consumption being 7.6 times higher in subjects with deficient kilocalories intake. It is crucial to know that although the increased growth rate, dietary characteristics, and Ca-deficient diet can improve the efficiency of Ca absorption, its bioavailability will depend on the net Ca retention in bones and organs, Ca absorption, and its urinary losses [76].
Additionally, in our series, although there were no sex differences in dietary Ca and Vit-D consumption, Ca intake was 20 times higher in adolescents than in children. In contrast, the prevalence of deficient Ca intake in 1176 Spanish schoolchildren was significantly higher in girls (p = 0.006) [79]. While, in this study, 17.9% (7 cases) had a high dietary Ca intake, only two obese patients (5%, a 2-year-old girl with VDD and a 12-year-old boy with insufficient Vit-D and short stature) with regular Ca and deficient Vit-D consumption had hypercalcemia (Ca >10.5 mg/dL) [38], high Ca-PP (>55 mg2/dL2) [42] and hypercalciuria (Ca/Cr rate >0.2). Only the boy had hyperphosphaturia (mg/kg/d >17 and mg/d >900). Although serum Ca concentration is not a marker of Ca deficiency, low Ca/Cr <0.2, as happened in our series, might be associated with low Ca intake [77]. In our series, no patients had hypercalcemic symptoms such as hypotonia, vomiting, constipation, abdominal pain, lethargy, polyuria, dehydration, and seizures [82]. Hypercalcemia may result from increased bone resorption, intestinal absorption, or decreased renal excretion of Ca [83]. In children, causes of hypercalcemia can be classified as PTH-dependent or PTH-independent and may be congenital or acquired. Acquired causes of PTH-independent hypercalcemia in children include hypervitaminosis, granulomatous disorders, and endocrinopathies [38].
Other interesting results showed that the mean urine Ca (mg/kg/d and 24-hour), UCaE, and Ca/Cr rates were regular, but depending on the urine biomarker used, the percentage of hypercalciuric patients varied (Table 4). 41% (16 cases) of the patients presented high urine Ca loss. While 23.1% (9 cases) had elevated Ca/Cr ratio, 12.8% (5 cases) had abnormal UCaE, and 20.5% (8 cases) and 15.4% (6 cases) had Ca loss >4 mg/kg/day and >200 mg/L, respectively. Only three normocalcemic female adolescents with deficient Ca intake, elevated Ca/Cr ratio, and UCaE had hypercalciuria with simultaneously high urinary Ca >4 mg/kg/day and >200 mg/L. Physiological hypercalciuria is a problem associated with many ailments and excessive sodium, Ca, or protein content in the diet [84]. It is essential to consider in this series of pediatric chronic patients, the diagnosis of idiopathic hypercalciuria because 75% (6/8 cases) of individuals had urine Ca loss >4 mg/kg/d, other two subjects with hypercalciuria >4mg/kg/d had hypercalcemia. Idiopathic hypercalciuria is the increased urinary Ca excretion without other causes of hypercalcemia and other causes of hypercalciuria [44,85]. It is one of the most common metabolic disorders and is the most frequent cause of kidney stones, both in adults (60%) and children (40%). The prevalence varies in healthy populations, depending on the country, between 0.6 and 12.5%. In Spain, the prevalence rate is between 3.8 and 7.8% [44]. In 1375 schoolchildren (6-18 years) in Tokat province, the prevalence of hypercalciuria was 4.7% [86].
Interestingly, in our series, 24-hour urine Ca loss was positively associated with age (R2 = 0.254, p = 0.000) (Figure 2), and this value was higher in adolescents than in children. Among subjects with hypercalciuria (mg/kg/d), the likelihood of finding patients with abnormal UCaE was 26 times higher, and among patients with high Ca/Cr rate, the probability of seeing patients with Ca loss >4 mg/kg/d and >200 mg/L was 28 and 11.2 times higher, respectively. Remarkably, one undernourished 4-year-old male with deficient Vit-D intake had severe hypercalciuria, with a Ca/Cr rate of 0.94 and urine Ca of 11.04 mg/kg/d. Even though Ca is the most relevant element in the formation of kidney stones and hypercalciuria is associated with frequency, dysuria, enuresis, abdominal pain, hematuria, and urinary lithiasis [84], in our series, no patients had this symptomatology. Hypercalciuria is the main metabolic risk factor for pediatric urolithiasis. This condition presents high morbidity, with or without lithiasis, such as hematuria and deterioration of bone mass [87]. Even though there is a connection between stone formation and BMI in adults, there are no definitive conclusions in the pediatric population [88]. Besides, it is critical to consider the increasing incidence of pediatric nephrolithiasis and its association with obesity. In 110 patients from the US Centers for Disease Control and Prevention with stone formation, overweight and obese patients with lower levels of urinary citrate, P, and Mg had a higher incidence of hypercalciuria compared with those with low or normal BMI [89]. In our series, 20% (4 cases) of obese teenagers had high 24-hour urine Ca >200 mg/d and two of them had high Ca/Cr rate and UCaE.
According to several reports, 24-hour urine Ca >250 mg/d is the reference to determine hypercalciuria [46]. In our study, three normocalcemic patients had 24-hour urine Ca loss >250 mg/d and had simultaneous urine Ca loss >4 mg/kg/d, high Ca/Cr ratio, UCaE, and deficient Ca intake. In another group of CF patients, 12% had a Ca/Cr ratio > 0.2. Although only four subjects (23%) had a urine Ca loss > 4 mg/kg/day, all these patients had a urine Ca loss >200 mg/L [1]. Another method to diagnose hypercalciuria is the Ca/Cr ratios according to age [45,46,89]. In this study, the mean Ca/Cr rate of 0.15 was regular, and 23.1% (9 cases) had a high Ca/Cr rate. Two subjects had hypercalcemia, six patients had high urine Ca loss >4mg/kg/d, five had high 24-hour urine Ca, and three had high UCaE. Nonetheless, in other children’s populations, the prevalence of hypercalciuria can vary greatly. In 593 healthy Dubai children, the mean Ca/Cr was 0.08 ± 0.07 mg/mg. The mean Ca/Cr was significantly higher in boys than girls and decreased with age [90]. Only 3 of 529 healthy Japanese schoolchildren (0.6%) had hypercalciuria (Ca/Cr >0.17) [91]. Of 205 children from the Aral Sea region, a severely polluted natural area, 38.6% had extremely high Ca/Cr levels (0.75 ± 0.74) [92]. In 1375 schoolchildren (6 to 18 years), the Ca/Cr rate was 0.08. Since the 95th percentile was 0.28, 4.7% had hypercalcemia [86]. It is interesting to know that in a follow-up study of 230 adult patients, 33% had hypercalciuria. UCaE predicted the development of kidney stones and BMD loss. A lower level of UCaE independently predicted the development of major adverse cardiac events and CVD [93], which can be a risk in children with hypercalciuria as our study.
Creatinine excretion in urine occurs at a constant rate throughout the day. Since Cr excretion reflects the body's muscle mass, its measurement could assess lean body mass or body composition [94,95]. In our series, the mean serum (0.53 mg/dL) and urine Cr (18.6 mg/kg/d and 819.8 mg/d) were regular. Patients with deficient Ca intake had a higher urine Cr loss (mg/kg/d and 24-hour) than regular ones. The mean urine Cr between 3 to 14 years in our patients (34 cases) was 18.3 ± 7.5 mg/kg/d, and there was no significant difference with the value of 19.49 ± 2.87 mg/kg/d in 401 healthy Spaniard children (3-14 years, 46.6% males) [96]. Although women (19.2 ± 7.5) had higher urine Cr (17.0 ± 6.8) than males, there was no significant difference. However, they were significantly higher than the results in 710 healthy Chinese children, whose mean urine Cr for boys was 15.3 ± 3.6 mg/kg/d (p = 0.030) and for girls was14.3 ± 3.2 mg/kg/d (p = 0.009) [95], and both were significant lower compare with their peers in age group and sex. In Dubai children, urinary Cr excretion was 17.9 ± 3.12 mg/kg/d. Boys had a marginally higher Cr excretion than girls [90]. Between 8 and 13 years, in our series, boys had a higher 24-hour urine Cr than girls without significant difference. Nonetheless, they were significantly higher than the results in Chinese children, whose mean 24-hour urine Cr for boys was 565.0 ± 171.5 mg/d (p = 0.006) and for girls 502.0 ± 141.5 mg/day (p = 0.002) [95].
Interestingly, in our series, while 28.2% (11 cases) and 20.5% (8 cases) of subjects had high and low urine Cr levels (mg/kg/d), respectively, 35.9% (14 cases) of participants had low 24-hour urine Cr <500 mg/d. In addition, although there were no patients with high 24-hour urine Cr >2000 mg/d, 28.2% (11 cases) and 10.3% (4 cases) had simultaneous regular (mg/kg/d) and low urine Cr (24-hour). Patients with hypophosphatemia had a higher BCS AV and urine Cr. Also, 24-hour urine Cr levels had a meaningful association with age (R2 = 0.509) (Figure 2), and adolescents had higher levels than children. This is consistent with urinary Cr excretion in Chinese children, which increased significantly with age [95]. In our series, 24-hour urine Cr had a significant association with age and showed more significant correlations with anthropometric, body composition, dietary, and biochemical parameters than urinary Cr in mg/kg/d. Similarly, in Chinese children, the mean 24-h Cr excretion was significantly correlated with age, body height, and body weight. In our series, anthropometric and body composition assessments had a significant association with urine Cr excretion. The urinary Cr reference range varies considerably because of anthropometric factors such as weight, height, and ethnicity. Age- and sex-specific reference values for urinary Cr are necessary because age affects body composition in growing children. In addition, there was a close correlation between body height and weight with corporal mass reference values [97].
It is imperative to consider that bone mass acquisition during childhood and adolescence should occur without interference. Lifelong abnormal Ca loss could be a risk factor for changing bone structure and determining low bone mass [85,87,98]. In children, it is preferable to speak of bone fragility rather than osteoporosis [99]. Recent studies in pediatric populations with chronic conditions focus on adjusting body composition and BMD for height due to short stature and delayed maturation of bone size [100]. In our series, the mean BCS AV (1934 ± 76) and Z-score (-0.5 ± 1.0) were regular in the whole series and by gender, age, A50°H, and BMI groups. BCS had a positive and significant association with age (R2 =0.496, p < 0.001), and females had higher BCS AV than males. In 6143 US adolescents aged 8 to 19 years, BMI had a significant association with BMD [101]. Three cases had low BCS <-2DS. While BCS-AV had a significant correlation with Ca intake, serum P, the Ca/P ratio, and Ca-PP, 24-hour urine Ca and Cr (mg/kg/d and 24-hour), BCS Z-score had a meaningful correlation with Cr (mg/kg/d). Patients with deficient Ca intake and hypophosphatemia had higher BCS AV than those with regular Ca intake and serum P, respectively.
Serum concentrations of Ca, P and ALP vary considerably with age, sex, and pubertal stage, even in healthy children. In our series, the mean ALP level was high in the whole series and all groups, with no significant differences. 56.4% of participants had higher ALP levels. Serum ALP was significantly higher in males than females. It has been reported that use of serum P levels in combination with ALP, increases the sensitivity of screening and contributes to specifying preterm babies who carry a risk for osteopenia. Serum ALP value above 900 U/L (sensitivity 88% and specificity 71%), and serum P level of <5.5 mg/dL (sensitivity 96% and specificity 50%) were associated with low BMD [102]. Based on these results, this series of children and adolescents with chronic health diseases were at high risk of hypercalcemia and hypercalciuria.
4.3. Phosphorus
A complex network of factors, including PTH, 1,25-dihydroxyvitamin D (1,25(OH)2D), fibroblast growth factor 23 (FGF23), and calcitonin, regulate the P homeostasis. The phosphatonins, secreted frizzled-related protein 4, and IGF-1 modulate P concentration by affecting the activity of 25-hydroxyvitamin D3-1α-hydroxylase [103]. Childhood and adolescence require an adequate supply of P for the proper mineralization of cartilage and osteoid tissue [104]. In this series, the mean serum P (4.7 mg/mL), serum Ca/P ratio (2.1), and serum Ca-PP (46.8 mg2/dl2) were regular without significant differences by groups. No patients had hyperphosphatemia, but 35.9% (14 cases) of participants had hypophosphatemia (<4.5 mg/dL) [37]. In contrast, 18% of CF patients had hypophosphatemia [1]. In addition, hypophosphatemia may be due to internal redistribution, and increased urine P losses [105]. In pediatrics, it is essential to interpret P levels according to age. Under normal conditions, the lower regular value of serum P at birth is higher than the upper regular value in adults [106], decreasing at puberty and with a decrease in phosphatemia at puberty [55]. Nonetheless, in our series, serum P levels had an inverse and significant association with age (R2 = 0.259, p = 0.001), and children had higher serum P levels than adolescents. The likelihood of children with higher serum P levels was 1.7 times higher than adolescents. Males had higher serum P levels than females, and patients with regular Ca intake had higher serum P levels than patients with deficient Ca eating.
Phosphatemia presents inter- and intra-individual variations during the day that can be explained by dietary P intake, P exchanges between bone and the extracellular space, TRP, which depends on phosphoremia, and phosphate intake, and finally GFR [55]. Hypophosphatemia is a relatively common laboratory abnormality and is often an incidental finding. Even though hypophosphatemia has been associated with organ dysfunction and mortality it remains poorly characterized in terms of real prevalence and timing of onset. Severe hypophosphatemia can lead to significant clinical consequences and a possible increased mortality risk [107]. The most common causes of hypophosphatemia are inadequate absorption of P, increased excretion, and extracellular movement into the intracellular space [108]. In our series, patients with regular Ca intake had higher serum P levels than patients with deficient Ca eating. Almost all types of diet contain a sufficient surplus of P to meet needs. Secondary hypophosphatemia occurs due to inadequate P intake in the context of P-poor dietary sources over a prolonged period, intestinal malabsorption, and intestinal binding by exogenous agents [107]. Although most patients have mild to moderate hypophosphatemia and recover without complications, the presence of severe hypophosphatemia is associated with a significantly higher mortality rate in critically ill patients with sepsis or septic shock [109].
Phosphorus is an essential element associated with dietary intake. Nevertheless, Western diets contain high levels of inorganic P, which can overwhelm established regulatory mechanisms to maintain its homeostasis. Furthermore, individuals with impaired renal function may experience exacerbated symptoms of P overload due to decreased filtration and elimination. Phosphorus overload can produce inflammatory signaling and many diseases can arise from P overload and its subsequent inflammatory signaling, including CVD, tumorigenesis, depression, and neuronal disorders. In acute patients, both malnutrition and sepsis are considered risk factors for hypophosphatemia [6,110]. Even though in adulthood, the classification <0.65 mmol/L as “moderate” and <0.32 mmol/L as “severe” comes from non-ICU populations; there is no universal definition of cut-off points for the severity of hypophosphatemia, even in children [111]. In critically ill children admitted to the pediatric intensive care unit (PICU), the prevalence of hypophosphatemia was 71.6% and was associated with prolonged PICU length of stay > 6 days. One of its causes was the increased urinary loss of P and the inability to provide P during this phase of its urinary [110]. In adult patients in ICU, hypophosphatemia may occur in approximately 35% of admissions, especially in patients requiring renal replacement therapy, diabetic ketoacidosis, respiratory alkalosis, or patients admitted with malnutrition. Severe hypophosphatemia is associated with organ dysfunction, rhabdomyolysis, muscle weakness, and increased mortality [111].
Even though the mean urinary P (17.6 mg/kg/d) was high [52], the mean 24-hour urine P of 690.8 mg/d was regular [51]. Urine P had a meaningful positive association with age (R2 = 0.347, p < 0.001) (Figure 2). 51.3% of subjects (20 cases) exhibited hypephosphaturia >17 mg/kg/d, 20.5% of patients (8 instances) had 24-urine P loss >900 mg/d, and 7.7% (3 cases) of individuals had FEP >20%. The FEP is the relationship between P and Cr clearance, and values <20% are considered regular. In individuals with normal renal function, FEP could assess nephron stress [53]. In our study, 12.8% (4 cases) of patients had simultaneous high urine P in mg/kg/d and 24-hour. Only one patient had simultaneous high urine P levels (mg/kg/d and 24-hour) and FEP. In CF patients, urine P excretion was normal for values under 25 mg/kg/day [1,112]. In contrast, in our study, the values were under 17 mg/kg/d [52]. In 3913 healthy children and adolescents (2 to 18 years), boys had significantly higher daily urinary P excretion than girls. Gender differences in urinary P were negatively higher when adjusted for Cr since boys had meaningful higher Cr excretion. Urinary P measurement is crucial in childhood since its excretion is associated with the prevalence of metabolic risk factors such as lithiasis and presents a significant risk of recurrence in this population [113].
Additionally, in our series, among subjects with hyperphosphaturia, the likelihood of finding hypercalciuria was 9.7 times greater, and the probability of finding hyperphosphaturia in patients with hypercalciuria was 2.1 times greater than among patients with normal urinary P level. Also, 17.9% (7 cases) of patients simultaneously had hypercalciuria (>4 mg/kg/d) and hyperphosphaturia (>17 mg/kg/d, X2 = 0.022). The likelihood of finding normal urine P (mg/d) was 1.4 times higher in active patients than sedentary ones. The most crucial P excretion occurs primarily in the renal system, where of the filtered P, the proximal renal tubule typically reabsorbs about 70% to 80%, and the distal tubule reabsorbs about 15%. Low serum P levels stimulated P reabsorption [8,107]. Hypophosphatemia produced by increased urinary P excretion is generally due to either excess PTH or an inherited disorder of renal P handling in the proximal tubule. Increased renal reabsorption of P can compensate for all but the most severe dietary deficiency. As most dietary P comes from protein, children in parts of the world where protein malnutrition is common are particularly susceptible to this [8,107]. In our series, 7.7% (3 instances) of patients had simultaneous hypophosphatemia and VDD and 23.1% (9 cases) had coincident VDD and hyperphosphaturia. Deficiency of vitamin D leads to decreased intestinal absorption of phosphorus. In addition, vitamin D deficiency leads to hypocalcemia, HPT, and a consequent PTH-mediated increase in renal phosphorus excretion [114].
The mean urine TRP (88.6%) [115] and TmP/GFR (3.9) [56] were normal. The normal range of TRP is 85-95% and a value above 95% is a significant marker showing insufficient P supplement [116]. Only 15.4% (6 cases) of subjects had TRP <85% and 12.8% of participants (5 cases) had a high TmP/GFR. No one patient had TmP/GFR < 2.8 mg/dL. That is, no patients had the renal tubular P loss [55]. In critically ill children, renal P loss was evaluated by TmP/GFR <2.8 mg/dL. Renal P threshold was meaningful lower on all the days in the hypophosphatemic group compared to that of non-hypophosphatemic one [110]. The TmP/GFR ratio depends on the TRP, the proportion of P in primary urine that is tubularly reabsorbed. Up to a TRP of 86%, there is a linear relationship between TRP and the TmP/GFR ratio and can be calculated as the product of TRP and serum P. With a TRP above 86% (low P excretion), there is no longer a linear relationship. TmP/GFR is decreased in hyperphosphatemia due to increased P flux from the gut and increased in hypophosphatemia due to decreased P flux [55]. The normal range for both TmP/GFR and serum P is generally numerically similar at each age. Both are highest in childhood and decline with age. This higher range is necessary for the proper mineralization of the growing skeleton [117]. To assess tubular reabsorption, we used the GFR. Since 85-95% of P is reabsorbed in the proximal tubule, a TRP rate below 85% indicates tubular P leakage [54]. When TmP/GFR, which is also age-dependent [55], decreases in the presence of hypophosphatemia, it informs a renal P leak [118].
4.5. Calcium and Phosphorus relationships
Calcium is directly interconnected with P in their homeostasis since serum Ca interacts with serum P by modulating various hormones, so their serum concentration is inversely related [1,7]. Optimal homeostasis between Ca and P is crucial for bone matrix formation. Microcrystalline apatite in bone contains 99% Ca and 85% P. Calcium and P homeostasis depend on intestinal absorption, bone accretion and resorption, urinary excretion, Vit-D status, and dietary intake [119]. This means that as P levels in the blood rise, Ca levels in the blood fall because P binds to Ca reducing the available free Ca in the blood [12]. On the other hand, Ca has a similar relationship to Vit-D, which means that when Vit-D rises, Ca also rises. It should be noted that the levels are those of free Ca in the blood and not the Ca stored in the bones. Calcium is regulated by the parathyroid, which releases PTH, as well as the kidneys. When Ca levels are low, PTH is released to break down bones and allow the Ca stored in the bones to be available in the bloodstream. PTH also activates Vit-D, which encourages additional Ca to be absorbed from the digestive tract and encourages the kidneys to retain more Ca while excreting P [12,1120].
Even though the authors suggest that adequate Ca and P intake should be in the appropriate ratio of 1:2 to reduce the risk of Ca malabsorption, little is known about the serum and urine Ca/P ratio [119,121]. Results of this study showed that the mean serum Ca/P ratio (2.1) [39] and serum Ca-PP (46.8 mg2/dl2) were regular [41,42]. In adults, in PHPT, the Ca/P ratios can be used in its diagnosis, especially in those patients with normocalcemic HPT, being their higher value compared to the serum Ca/corrected Ca. When the Ca/P ratio is >3.5 mg/dl (3.35 mg/dL), it acts as an accurate, oversensitive (90.5%), and specific (93.2%) indicator for the diagnosis of HPT [7,122]. On the other hand, a serum Ca/P ratio <2.32 mg/dl can be used to diagnose hypoparathyroidism [40,123]. Considering these ratios, in our study, no patients had a serum Ca/P ratio over 3.5, but 79.5% (31 cases) had a serum Ca/P <2.32. These lower values are pathological and suggest a possible diagnosis of HypoPT. In the adult population, serum Ca/P ratios range from 2.3 to 3.3 in patients with normal parathyroid function. The altered Ca/P ratios indicate abnormalities of Ca–P metabolism, including disorders of parathyroid function [40].
In our series, while serum Ca/P ratios were meaningfully higher in females (2.2 ± 0.3) than males (2.0 ± 0.2), and adolescents had higher serum Ca/P ratios (2.2 ± 0.3) than children (1.9 ± 0.2), there were no significant differences in urine Ca/P ratios by gender and age. In contrast, in 593 Dubai children, the mean Ca/P was lower (0.15 ± 0.15), it was significantly higher in boys (0.17 ± 0.16) than girls (0.14 ± 0.14) and did not change with age [90]. Likewise, in 590 healthy school-age children (7-11 years, 50.5% girls), the mean and 95th percentile urine Ca/P was 0.155 ± 0.095 and 0.36 respectively. There was no significant difference by age. This ratio decreased with aging and had a significant negative correlation with age. Girls had higher urine Ca/P (0.16 ± 0.1) levels than boys (0.15 ± 0.09) [84]. In adults, the urinary Ca/P ratio of 0.17 (sensitivity 100% and specificity 96%) because of its discriminatory power between thyrotoxic periodic paralysis (TPP) and non-TPP hypokalemic paralysis can act as a biomarker [124]. While in this study there was no significant association between urine and serum Ca/P ratio, in a series of CF patients the serum and urine Ca/P ratio had a negative correlation between each other [1]. In this study, serum Ca/P ratio had a positive and significant association with serum P, and serum Ca-PP individually and together, and urine Ca/P ratio with 24-hour urine Ca and Ca/Cr rate. Patients with hypophosphatemia had a higher serum Ca/P ratio than those with normal serum P. Serum Ca-PP had a positive and significant association with TmP/GFR and serum P, and serum P and Ca, and urine Ca/P ratio had a meaningful positive association with urine Ca and urine Ca and urine Ca/P ratio and HDL-C and serum Vit-C.
Additionally, in our study, the mean urine Ca/P ratio was 0.14 ± 0.11 and the Ca-PP was 50.2 ± 57.5. Urinary Ca and P excretion is a good indicator of their status. Collecting a 24-hour urine sample or a spot urine test can assess those nutrients. 24-hour urine collection is the gold standard [90]. There are few studies on urine Ca/P ratio in adults and even fewer in the pediatric population. In an animal study performed in pregnant and lactating sows, the best cut-off point for urinary Ca/P ratio was 1.5 (sensitivity 94% and specificity 68%) to identify diets fed with P deficiency and 0.5 for diets with excess P (sensitivity 82% and specificity 82%) [125]. If we were to rely on these values, in our study, all patients would have diets with excess P. Since the Ca-PP in our series is < 55-60 mg2/dL2 and <72 mg2/dL2, there was no risk factor for increasing CV morbidity [41,42] and no increased relative mortality risk [42]. Urinary and serum Ca-PP had a direct and meaningful association when they were adjusted to the age (R2 = 0.106, p = 0.043). Underfed patients had a significantly higher urine Ca-PP than eutrophic and obese ones. Two adolescent females (12 and 16 years) had a high serum Ca/P ratio. One was underfed (2.9), and another was an obese (2.8) child. 7.7% (3 cases) of subjects who were obese had a higher Ca-PP between 55.1 to 62.6 mg2/dl2. Two of them were hypercalcemic. Serum Ca-PP was significantly higher in males than females. Participants with deficient Ca intake had a higher serum Ca/P ratio and lower serum P and Ca-PP than patients with regular Ca consumption. Although serum P and Ca-PP were substantially higher in children than adolescents, serum Ca/P ratio, urine P, and Ca/P ratio were higher in adolescents than children.
The Ca-PP should be kept within the normal range, at least below 60 mg2/dL2, since an elevated Ca-PP is a risk factor for CV morbidity, and P and or Ca levels should be reduced [41]. For example, in end-stage renal disease (ESRD), in the absence of dietary P restriction or P-chelating supplements, hyperphosphatemia includes the development and progression of secondary hyperparathyroidism (HPT) and a predisposition to metastatic calcification in high Ca-PP. There is a relative risk (RR: 1.27) of death for those with serum P >6.5 mg/dl, with younger patients at ESRD onset, female sex, white race, diabetes, active smoking, and higher serum Cr (significant predictors). Ca-PP in this population showed a trend for mortality risk than serum P alone. Patients with the highest quintile of Ca-PP (>72 mg2/dL2) had a RR (1.34) of mortality compared with those with products of 42 to 52 mg2/dL2. These facts support the need for strict control of hyperphosphatemia to improve patient survival [42].
Calcium and P metabolism disorders occur when their levels in the body deviate from their basal state, leading, as we have seen, to pathological states of hypercalcemia, hypocalcemia, hyperphosphatemia, and hypophosphatemia. They may produce changes in the levels of ALP and PTH, Vit-D, and FGF23, which could affect the quality of life and even shorten the life expectancy of patients by inducing growth retardation, osteomalacia, skeletal and dental abnormalities, muscle spasms, nephrolithiasis, seizures due to hypocalcemia, etc. Both nutrients play essential roles in the human body. While calcium is involved in hormonal secretion, blood coagulation, and nervous excitation, P is necessary for energy metabolism, cell signaling, and stabilization of phospholipid content in the cell membrane. Therefore, it is essential to understand the metabolism of Ca and P for an adequate early diagnosis that leads to the corresponding therapeutic strategies [120].
At this point, it is crucial to consider several aspects to highlight. First and foremost, most of these children and adolescents patients with chronic health conditions had an increased risk of persistent hypovitaminosis D. This deficiency state can lead to secondary hyperparathyroidism and changes in the immune system. Secondly, there was an imbalance in the metabolism of Ca and P due to increasing urinary losses despite their dietary intake. Elevated ALP levels were related to urinary Ca and P losses. We should consider the possibility of an imbalance in body composition and the risk of an inadequate immune system response. Thirdly, the urinary Ca/P ratio showed associations primarily with anthropometric and body composition assessments. Finally, PA in most of these patients may have contributed to their health and nutritional status.
A limitation of this study is the small number of participants. In addition, one aspect we could not address to complete the assessment of these nutrients was the assessment of dietary P intake and urinary Vit-D levels. Nevertheless, this study provides valuable and detailed information on Ca, P, and their relationship in serum and urine in a series of children and adolescents with chronic diseases. The strengths of this study lie in the determination of Ca; P; Vit-D; Ca/P ratios; Ca-PP levels and their relationship with anthropometric, body composition, bone densitometry, biochemical and dietary indicators, in addition to the assessment of health and nutritional status in these patients.
The findings of this study have many practical implications in clinical practice and support the need to assess dietary, serum, and urinary Ca and P levels at least annually. Relevant data on these nutrients in healthy children are scarce, especially for different age subgroups. It is crucial to detect children at higher risk and for clinicians to be able to rely on reference values that identify the normal range of their urinary composition. Research is critical to confirm that the levels of these nutrients are adequate, which will allow appropriate dietary changes or the addition of supplements. Further studies that take these variables into account will be necessary. A natural progression of this work is to implement multicenter trials to improve knowledge of Ca, P, and Vi-D to determine the necessary and appropriate amount of supplementation for effective prevention with personalized nutritional recommendations.
5. Conclusions
In this series of children and adolescents with chronic diseases, 20% of subjects had hypercalciuria, 23% had high Ca/Cr rate, and 44% exhibited hyperphosphaturia. No one patient was hypocalcemic or hyperphosphatemic. Serum and urinary Ca/P ratios were 2.12 and 0.13, respectively. 36% and 5% of subjects had hypophosphatemia and hypercalcemia, respectively. Our results support that there was an imbalance in Ca and P in these patients with high vitamin D impairment. In addition, there were significant associations between calcium, phosphorus, and vitamin D with several health and nutritional biomarkers.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, Table S1: Correlations between serum calcium (Ca) and phosphorus (P), Ca/P ratio, Ca-P product, vitamin D and alkaline phosphatase with the studied biomarkers (n = 39); Table S2: Correlations between urine calcium (Ca) and phosphorus (P), Ca/P ratio, Ca-P product, urine Ca excretion and creatinine with the studied nutritional biomarkers (n = 39); Table S3: Correlations between urine calcium/phosphorus ratio, calcium-phosphorus product, phosphorus excretion, tubular reabsorption of phosphorus, tubular maximum phosphorus reabsorption/glomerular filtration rate with the studied nutritional biomarkers (n = 39).
Author Contributions
M.F.E.-M. designed the study, oversaw data collection and study implementation, managed the samples, performed micronutrients status assays, oversaw all laboratory aspects of the study, assisted with statistical analysis, analyzed the data, and wrote the manuscript. J.M.M.-M. supervised data collection, assisted with results interpretation, and provided inputs to the manuscript. J.P.-R., M.P.B.-C., and D.J.-A. provided inputs to the manuscript. M.A.E.-M. and G.S. collaborated in the review of the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Ethical Committee of the University Clinical Hospital management board (INSALUD-Valladolid, 14 February 2002).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data is contained within the article and supplementary materials. Data supporting the reported results can also be found in references 1, 14, 15, 16 and 17.
Acknowledgments
We are grateful to the staff of Pediatric service of University Clinical Hospital and the Laboratory of Instrumental Techniques of the Chemistry Department of the Valladolid University. I would like to especially thank Carmen Escobedo Monge and José Escobedo Monje for their technical support in the preparation and presentation of this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| BMI | Body mass index |
| FFM | Fat free mass |
| FM | Fat mass |
| BIA | Bioelectrical impedance analysis |
| Ca | Calcium |
| P | Phosphorus or phosphate |
| Cr | Creatinine |
| Vit | Vitamin |
| PA | Physical Activity |
| %DRI | % Dietary Reference Intake |
| ALP | Alkaline phosphatase |
| TRP | Fractional tubular reabsorption of phosphate |
| TmP/GFR | Tubular maximum phosphate reabsorption per glomerular filtration rate |
| EE | Energy expenditure |
| WHO | World Health Organization |
| ANIVA | Anthropometry and Child Nutrition in Valencia |
| ENALIA | The National Survey of Nutrition in the Child and Adolescent Population |
References
- Escobedo-Monge, M.F.; Marcos-Temprano, M.; Parodi-Román, J.; Escobedo-Monge, M.A.; Alonso-Vicente, C.; Torres-Hinojal, M.C.; Marugán-Miguelsanz, J.M. Calcium, Phosphorus, and Vitamin D Levels in a Series of Cystic Fibrosis Patients: A Cross-Sectional Study. Int. J. Mol. Sci. 2024, 25, 1900. [CrossRef]
- Civitelli, R.; Ziambaras, K. Calcium and phosphate homeostasis: Concerted interplay of new regulators. J. Endocrinol. Investig. 2011, 34 (Suppl. S7), 3–7.
- Hanna, R.M.; Ahdoot, R.S.; Kalantar-Zadeh, K.; Ghobry, L.; Kurtz, I. Calcium Transport in the Kidney and Disease Processes. Front Endocrinol (Lausanne). 2022, 12, 762130. [CrossRef]
- Peterlik, M.; Cross, H.S. Vitamin D and calcium deficits predispose for multiple chronic diseases. Eur J Clin Invest. 2005, 35(5), 290-304. [CrossRef]
- Kiela, P.R.; Radhakrishnan, V.M.; Ghishan, F.K. Phosphorus: Basic Nutritional Aspects. In Molecular, Genetic, and Nutritional Aspects of Major and Trace Minerals; Collins, J.F., Ed.; Academic Press: Cambridge, MA, USA, 2017; Chapter 34; pp. 413–427.
- Erem, A.S.; Osuka, S.; Razzaque, M.S. Phosphate Burden and Inflammation. Adv Exp Med Biol. 2022, 1362, 7-13.
- Madeo, B.; Kara, E.; Cioni, K.; Vezzani, S.; Trenti, T.; Santi, D.; Simoni, M.; Rochira, V. Serum Calcium to Phosphorous (Ca/P) Ratio Is a Simple, Inexpensive, and Accurate Tool in the Diagnosis of Primary Hyperparathyroidism. JBMR Plus. 2017, 2, 2, 109-117. [CrossRef]
- Lee, J.J.; Plain, A.; Beggs, M.R.; Dimke, H.; Alexander, R.T. Effects of phospho- and calciotropic hormones on electrolyte transport in the proximal tubule. F1000Res. 2017, 6, 1797. [CrossRef]
- El Mallah, C.; Ghattas, H.; Shatila, D.; Francis, S.; Merhi, K.; Hlais, S.; Toufeili, I.; Obeid, O. Urinary Magnesium, Calcium, and Phosphorus to Creatinine Ratios of Healthy Elementary School Lebanese Children. Biol Trace Elem Res. 2016, 170(2), 264-270. [CrossRef]
- Emmens, J.E.; de Borst, M.H.; Boorsma, E.M.; Damman, K.; Navis, G.; van Veldhuisen, D.J.; Dickstein, K.; Anker, S.D.; Lang, C.C.; Filippatos, G.; Metra, M.; Samani, N.J.; Ponikowski, P.; Ng, L.L.; Voors, A.A.; Ter Maaten, J.M. Assessment of Proximal Tubular Function by Tubular Maximum Phosphate Reabsorption Capacity in Heart Failure. Clin J Am Soc Nephrol. 2022, 17(2), 228-239. [CrossRef]
- Lamberg-Allardt, C.; Kemi, V. Interaction Between Calcium and Phosphorus and the Relationship to Bone Health. In: Gutiérrez, O.; Kalantar-Zadeh, K.; Mehrotra, R. (eds) Clinical Aspects of Natural and Added Phosphorus in Foods. Nutrition and Health. Springer, New York, NY. 2017, 145-157.
- Shaker, J.L.; Deftos, L. Calcium and Phosphate Homeostasis. [Updated 2023 May 17]. In: Feingold, K.R.; Anawalt, B.; Blackman, M.R.; et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; 2000-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK279023/.
- Dowhan Hoag, L.; Dharmarajan, T.S. Calcium and Phosphorus. In: Pitchumoni, C.S.; Dharmarajan, T. (eds) Geriatric Gastroenterology. Springer, Cham. 2021, 735-763.
- Escobedo-Monge, M.F.; Bahillo-Curieses, P.; Parodi-Román, J.; Escobedo-Monge, M.A.; Alonso-López, P.; Marugán-Miguelsanz, J.M. Calcium, Phosphate, and Vitamin D in Children and Adolescents with Chronic Diseases: A Cross-Sectional Study. Nutrients 2024, 16, 1349. [CrossRef]
- Escobedo-Monge, M.F.; Torres-Hinojal, M.C.; Barrado, E.; Escobedo-Monge, M.A.; Marugán-Miguelsanz, J.M. Zinc Nutritional Status in a Series of Children with Chronic Diseases: A Cross-Sectional Study. Nutrients 2021, 13, 1121. [CrossRef]
- Escobedo-Monge, M.F.; Barrado, E.; Parodi-Román, J.; Escobedo-Monge, M.A.; Torres-Hinojal, M.C.; Marugán-Miguelsanz, J.M. Copper and Copper/Zn Ratio in a Series of Children with Chronic Diseases: A Cross-Sectional Study. Nutrients 2021, 13, 3578. [CrossRef]
- Escobedo-Monge, M.F.; Barrado, E.; Parodi-Román, J.; Escobedo-Monge, M.A.; Torres-Hinojal, M.C.; Marugán-Miguelsanz, J.M. Magnesium Status and Ca/Mg Ratios in a Series of Children and Adolescents with Chronic Diseases. Nutrients 2022, 14, 2941. [CrossRef]
- World Health Organization. Physical activity surveillance. Noncommunicable Disease Surveillance, Monitoring and Reporting. www.who.int/teams/noncommunicable-diseases/surveillance/systems-tools/physical-activity-surveillance. (Accessed May 11, 2023).
- Frisancho, A.R. New norms of upper limb fat and muscle areas for assessment of nutritional status. Am. J. Clin. Nutr. 1981, 34, 2540–2545. [CrossRef]
- Hernández, M.; Sobradillo, B.; Aguirre, A.; Aresti, U.; Bilbao, A.; Fernández-Ramos, C.; Lizárraga, A.; Lorenzo, H.; Madariaga, L.; Rica, I. Curvas y Tablas de Crecimiento (Estudios Longitudinal y Transversal); Fundación Faustino Orbegozo: Bilbao, Spain, 1985.
- Waterlow, J.C. Classification and definition of protein-calorie malnutrition. Br. Med. J. 1972, 3, 566–569. [CrossRef]
- Moraes, A.B.V.; Veiga, G.V.; Azeredo, V.B.; Sichieri, R.; Pereira, R.A. High dietary calcium intake and low adiposity: Findings from a longitudinal study in Brazilian adolescents. Cad. Saude Publica. 2022, 38, e00144521. [CrossRef]
- Martínez, M.J.; Redondo, D.; Conde, F.; Redondo, P.; Franch, M.A. Gráficas Longitudinales de Velocidad de Conducción Media de Ultrasonidos en Falanges. In Estudio Nutricional de Castilla y León; de CyL, J., Ed.; Junta Castilla y León: Valladolid, Spain, 2009.
- Alonso Franch M, Redondo Del Río MP, Suárez Cortina L, Jan, En Nombre del Comité de Nutrición de la Asociación Española de Pediatría. Nutrición infantil y salud ósea [Nutrition and bone health in children]. An Pediatr (Barc). 2010 y 72, 1, 80.e1-11.
- Mataix Verdú, J.; García Diaz, J. NUTRIBER. V. 1.0.; Fundación Universitaria Iberoamericana: Barcelona, Spain, 2005.
- Cuervo, M.; Corbalán, M.; Baladía, E.; Cabrerizo, L.; Formiguera, X.; Iglesias, C.; Lorenzo, H.; Polanco, I.; Quiles, J.; De Avila, M.D.R.; et al. Comparison of dietary reference intakes (DRI) between different countries of the European Union, The United States and the World Health Organization. Nutr. Hosp. 2009, 24, 384–414.
- Costello, R.B.; Rosanoff, A.; Dai, Q., Saldanha, L.G.; Potischman N.A. Perspective: Characterization of Dietary Supplements Containing Calcium and Magnesium and Their Respective Ratio-Is a Rising Ratio a Cause for Concern? Adv. Nutr. 2021 y 10., 12:291–297.
- Costello, R.B.; Elin, R.J.; Rosanoff, A.; Wallace, T.C.; Guerrero-Romero, F.; Hruby, A.; Lutsey, P.L.; Nielsen, F.H.; Rodriguez-Moran, M.; Song, Y.; et al. Perspective: The Case for an Evidence-Based Reference Interval for Serum Magnesium: The Time Has Come12345. Adv. Nutr. 2016, 7, 977–993. [CrossRef]
- Li, Q.; Chen, Q.; Zhang, H.; Xu, Z.; Wang, X.; Pang, J.; Ma, J.; Ling, W.; Li, D. Associations of serum magnesium levels and calcium-magnesium ratios with mortality in patients with coronary artery disease. Diabetes Metab. 2020, 46, 384–391. [CrossRef]
- Mathew, A.A.; Panonnummal, R. ‘Mg’-the master cation-as a drug-possibilities and evidences. Biometals 2021, 34, 955–986.
- Rosanoff, A.; Wolf, F.I. A guided tour of presentations at the xiv international magnesium symposium. Magnes. Res. 2016, 29, 55–59.
- Kaslow, J.E. Copper/Zinc Imbalance. Medical Board of California. Available online: http://www.mbc.ca.gov (accessed on 15 August 2021). Nutrients 2022, 14, 2941 26 of 31.
- Eck, P.; Wilson, L. Toxic Metals in Human Health and Disease Eck; Institute of Applied Nutrition and Bioenergetics, Ltd.: Phoenix, AZ, USA, 1989.
- Shroff, R., Wan, M., Nagler, E. V., Bakkaloglu, S., Fischer, D. C., Bishop, N., Cozzolino, M., Bacchetta, J., Edefonti, A., Stefanidis, C. J., Vande Walle, J., Haffner, D., Klaus, G., Schmitt, C. P., & European Society for Paediatric Nephrology Chronic Kidney Disease Mineral and Bone Disorders and Dialysis Working GroupsClinical practice recommendations for native vitamin D therapy in children with chronic kidney disease Stages 2-5 and on dialysis. Nephrol Dial Transplant Off Publ Eur Dial Transpl Assoc- Eur Ren Assoc. 1 de julio de 2017;32(7):1098-113.
- Bordelon, P.; Ghetu, M.V.; Langan, R.C. Recognition and management of vitamin D deficiency. Am. Fam. Physician 2009, 80, 841–846.
- Goltzman, D. Approach to Hypercalcemia. In Endotext [Internet]; Feingold, K.R., Anawalt, B., Boyce, A., Chrousos, G., de Herder, W.W.; Dhatariya, K.; Dungan, K.; Hershman, J.M.; Hofland, J.; Kalra, S.; et al., Eds.; MDText.com, Inc.: South Dartmouth, MA, USA, 2019.
- Pagana, K.D.; Pagana, T.J.; Pagana, T.N. Mosby’s Diagnostic & Laboratory Test Reference, 14th ed.; Elsevier: St. Louis, MO, USA, 2019.
- Stokes, V.J.; Nielsen, M.F.; Hannan, F.M.; Thakker, R.V. Hypercalcemic Disorders in Children. J. Bone Miner. Res. 2017, 32, 2157–2170. [CrossRef]
- Díaz Romero, C.; Henríquez Sánchec, P.; López Blanco, F.; Rodríguez Rodríguez, E.; Serra Majem, L. Concentrations of Na, K, Ca, and P in serum from a representative sample of the Canary Islands population]. Nutr Hosp. 2002, 17, 4, 204-12.
- Madeo, B.; De Vincentis, S.; Repaci, A.; Altieri, P.; Vicennati, V.; Kara, E.; Vescini, F.; Amadori, P.; Balestrieri, A.; Pagotto, U.; Simoni, M.; Rochira, V. The calcium-to-phosphorous (Ca/P) ratio in the diagnosis of primary hyperparathyroidism and hypoparathyroidism: a multicentric study. Endocrine. 2020, 68, 3, 679-687. [CrossRef]
- Klaus, G.; Watson, A.; Edefonti, A.; Fischbach, M.; Rönnholm, K.; Schaefer, F.; Simkova, E.; Stefanidis, C.J.; Strazdins, V.; Vande Walle, J.; Schröder, C.; Zurowska, A.; Ekim, M.; European Pediatric Dialysis Working Group (EPDWG). Prevention and treatment of renal osteodystrophy in children on chronic renal failure: European guidelines. Pediatr Nephrol. 2006, 21(2), 151-159. [CrossRef]
- Block, G.A.; Hulbert-Shearon, T.E.; Levin, N.W.; Port, F.K. Association of serum phosphorus and calcium x phosphate product with mortality risk in chronic hemodialysis patients: a national study. Am J Kidney Dis. 1998, 31(4), 607-617. [CrossRef]
- Adeli, K.; Higgins, V.; Trajcevski, K.; White-Al Habeeb, N. The Canadian laboratory initiative on pediatric reference intervals: a CALIPER white paper. Crit Rev Clin Lab Sci 2017, 54, 358–413. [CrossRef]
- García Nieto, V.M.; Luis Yanes, M.I., Tejera Carreño, P., Perez Suarez, G., Moraleda Mesa, T. The idiopathic hypercalciuria reviewed. Metabolic abnormality or disease? La hipercalciuria idiopática revisada. ¿Anomalía metabólica o enfermedad? Nefrologia (Engl Ed). 2019, 39, 6, 592-602.
- Leslie, S.W.; Taneja, A. Treasure Island (FL): Stat Pearls Publishing; Hypercalciuria. Stat Pearls [Internet] 2017 Dec 14 [updated 2018 Dec 6]. Available from: https://www.ncbi.nlm.nih.gov/books/NBK448183/ (Accessed February 10, 2023).
- Marwaha, R.K.; Garg, M.K.; Dang, N.; Mithal, A.; Narang, A.; Chadha, A.; Gupta, N.; Kumar, M.R. Reference range of random urinary calcium creatinine ratio in North Indian children and adolescents. Ann. Pediatr. Endocrinol. Metab. 2019, 24, 34–40. [CrossRef]
- Nephrology Calculator and Formulas. https://www.senefro.org/modules.php?name=webstructure&idwebstructure=26. Access on 27 July 2023.
- Seigle, R.L.; Nash, M.A. Chapter 13 – Nephrology. Editor(s): Polin, R.A.; Ditmar, M.F. In: Pediatric Secrets (Fifth Edition), Mosby, 2011, 480-523.
- Landry, D.W.; Gharavi, A.G. Approach to the patient with renal disease. In: Goldman, L.; Cooney, K.A.; eds. Goldman-Cecil Medicine. 27th ed. Philadelphia, PA: Elsevier, 2024, 100.
- Oh M.S.; Briefel, G.; Pincus, M.R. Evaluation of renal function, water, electrolytes, and acid-base balance. In: McPherson, R.A.; Pincus, M.R, eds. Henry's Clinical Diagnosis and Management by Laboratory Methods. 24th ed. Philadelphia, PA: Elsevier, 2022, chap 15.
- Prasad, N.; Bhadauria, D. Renal phosphate handling: Physiology. Indian J Endocrinol Metab. 2013, 17(4), 620-627. [CrossRef]
- Gil Gómez, R.; Milano Manso, G. Electrolitos urinarios. An. Pediatría Contin. 2014, 12, 133–136. [CrossRef]
- Bellasi, A.; Di Micco, L.; Russo, D.; De Simone, E.; Di Iorio, M.; Vigilante, R.; Di Lullo, L.; Di Iorio, B.R. Fractional Excretion of Phosphate (FeP) Is Associated with End-Stage Renal Disease Patients with CKD 3b and 5. J Clin Med. 2019, 8(7), 1026.
- Alon, U.; Hellerstein, S. Assessment and interpretation of the tubular threshold for phosphate in infants and children. Pediatr Nephrol. 1994, 8, 250–251. [CrossRef]
- Payne, R.B. Renal tubular reabsorption of phosphate (TmP/GFR): indications and interpretation. Ann Clin Biochem. 1998, 35, 201–206. [CrossRef]
- Brodehl, J. Assessment and interpretation of the tubular threshold for phosphate in infants and children. Pediatr Nephrol. 1994, 8, 645. [CrossRef]
- KDOQI Work Group. KDOQI Clinical Practice Guideline for Nutrition in Children with CKD: 2008 update. Executive summary. Am J Kidney Dis. 2009, 53(3 Suppl 2), S11-S104.
- Mansukoski, L.; Qamar, H.; Perumal, N.; Aimone, A.; Bassani, D.G.; Roth, D.E. Growth delay: an alternative measure of population health based on child height distributions. Ann Hum Biol. 2022, 49(2), 100-108. [CrossRef]
- Ethun, Kelly. Chapter 9. Sex and gender differences in body composition, lipid metabolism, and glucose regulation. In Sex differences in physiology. Editor(s): Neigh, G.N.; Mitzelfelt, M.M. Academic Press, 2016. 145-165. [CrossRef]
- Gao, T.; Leonard, M.B.; Zemel, B.; Kalkwarf, H.J., Foster, B.J. Interpretation of Body Mass Index in Children with CKD. Clin J Am Soc Nephrol 2012, 7, 558-564.
- Bonthuis, M.; Jager, K.J.; Abu-Hanna, A.; Verrina, E.; Schaefer, F.; van Stralen, K.J. Application of body mass index according to height-age in short and tall children. PLoS One. 2013, 8(8), e72068. [CrossRef]
- Stöcker, N.; Gaser, D.; Oberhoffer-Fritz, R.; Sitzberger, C. KidsTUMove—A Holistic Program for Children with Chronic Diseases, Increasing Physical Activity and Mental Health. J. Clin. Med. 2024, 13, 3791.
- West, S.L.; Banks, L.; Schneiderman, JE.; Caterini, J.E.; Stephens, S.; White, G.; Dogra, S.; Wells, G.D. Physical activity for children with chronic disease; a narrative review and practical applications. BMC Pediatr. 2019, 19(1), 12. [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.P.; et al.World Health Organization 2020 Guidelines on Physical Activity and Sedentary Behaviour. . Br J Sports Med. 2020, 54(24), 1451-1462.
- Thornton, J.S.; Frémont, P.; Khan, K.; Poirier, P.; Fowles, J.; Wells, G.D.; Frankovich, R.J. Physical activity prescription: a critical opportunity to address a modifiable risk factor for the prevention and management of chronic disease: a position statement by the Canadian academy of sport and exercise medicine. Br J Sports Med. 2016, 50(18), 1109–1114. [CrossRef]
- Butte, N.F. 1.3.2 Energy Requirements of Infants, Children, and Adolescents. World Rev Nutr Diet. 2022, 124, 47-54.
- Afroze, F.; Khoshnevisan, F.; Harawa, P.P.; Islam, Z.; Bourdon, C.; Khoswe, S.; Islam, M.; Sarker, S.A.; Islam, F.; Sayeem Bin Shahid, A.S.M.; Joosten, K.; Hulst, J.M.; Eneya, C; Walson, J.L.; Berkley, J.A.; Potani, I.; Voskuijl, W.; Ahmed, T.; Chisti, M.J.; Bandsma, R.H.J. Trajectories of resting energy expenditure and performance of predictive equations in children hospitalized with an acute illness and malnutrition: a longitudinal study. Sci Rep. 2024, 14(1), 3613. [CrossRef]
- Luo, B.; Davidson, Z.E.; O'Brien, K.; Volders, E.; Lu, J.; Dunlea, K.; Lazzari, M.: Billich, N.; Nguo, K. Describing Energy Expenditure in Children with a Chronic Disease: A Systematic Review. Adv Nutr. 2024, 15(4), 100198. [CrossRef]
- García-Ascaso, M.T.; Ares-Segura, S.; Ros-Pérez, P. Is iodine nutrition in the Spanish pediatric population adequate? Historical review and current situation. Endocrinol Diabetes Nutr (Engl Ed). 2018, 65(8), 458-467. [CrossRef]
- Escobedo-Monge, M.F.; Barrado, E.; Parodi-Román, J.; Escobedo-Monge, M.A.; Torres-Hinojal, M.C.; Marugán-Miguelsanz, J.M. Copper/Zinc Ratio in Childhood and Adolescence: A Review. Metabolites 2023, 13, 82. [CrossRef]
- Díaz-López, A.; Paz-Graniel, I.; Alonso-Sanz, R.; Marqués Baldero, C.; Mateos Gil, C.; Arija Val, V. Vitamin D deficiency in primary health care users at risk in Spain. Nutr. Hosp. 2021, 38, 1058–1067. [CrossRef]
- Zakharova, I.; Klimov, L.; Kuryaninova, V.; Nikitina, I.; Malyavskaya, S.; Dolbnya, S.; Kasyanova, A.; Atanesyan, R.; Stoyan, M.; Todieva, A.; Kostrova, G.; Lebedev, A. Vitamin D Insufficiency in Overweight and Obese Children and Adolescents. Front Endocrinol (Lausanne). 2019, 10, 103. [CrossRef]
- Szymczak-Pajor, I.; Drzewoski, J.; Śliwińska, A. The Molecular Mechanisms by Which Vitamin D Prevents Insulin Resistance and Associated Disorders. Int. J. Mol. Sci. 2020, 21, 6644. [CrossRef]
- Ghaseminejad-Raeini, A.; Ghaderi, A.; Sharafi, A.; Nematollahi-Sani, B.; Moossavi, M.; Derakhshani, A.; Sarab, G.A. Immunomodulatory actions of vitamin D in various immune-related disorders: A comprehensive review. Front. Immunol. 2023, 14, 950465. [CrossRef]
- Joshi, M.; Uday, S. Vitamin D Deficiency in Chronic Childhood Disorders: Importance of Screening and Prevention. Nutrients 2023, 15, 2805. [CrossRef]
- Bacchetta, J.; Edouard, T.; Laverny, G.; Bernardor, J.; Bertholet-Thomas, A.; Castanet, M.; Garnier, C.; Gennero, I.; Harambat, J.; Lapillonne, A.; Molin, A.; Naud, C.; Salles, J.P.; Laborie, S.; Tounian, P.; Linglart, A. Vitamin D and calcium intakes in general pediatric populations: A French expert consensus paper. Arch Pediatr. 2022, 29(4), 312-325. [CrossRef]
- Edouard, T.; Guillaume-Czitrom, S., Bacchetta, J.; Sermet-Gaudelus, I.; Dugelay, E.; Martinez-Vinson, C.; Salles, J.P.; Linglart, A. Guidelines for the management of children at risk of secondary bone fragility: Expert opinion of a French working group. Arch Pediatr. 2020, 27(7), 393-398. [CrossRef]
- Rana, Z.H.; Bourassa, M.W.; Gomes, F.; Khadilkar, A.; Mandlik, R.; Owino, V.; Pettifor, J.M.; Roth, D.E.; Shlisky, J.; Thankachan, P.; Weaver, C.M. Calcium status assessment at the population level: Candidate approaches and challenges. Ann N Y Acad Sci. 2022, 1517(1), 93-106. [CrossRef]
- Rubio-López, N.; Llopis-González, A.; Picó, Y.; Morales-Suárez-Varela, M. Dietary Calcium Intake and Adherence to the Mediterranean Diet in Spanish Children: The ANIVA Study. Int. J. Environ. Res. Public Health 2017, 14, 637. [CrossRef]
- Tytusa, A.; Wyszyńska, J.; Yatsula, M.; Nyankovskyy, S.; Mazur, A.; Dereń, K. Deficiency of Daily Calcium and Vitamin D in Primary School Children in Lviv, Ukraine. Int J Environ Res Public Health. 2022, 19(9), 5429. [CrossRef]
- Bae, Y.J.; Kratzsch, J. Vitamin D and calcium in the human breast milk. Best Pract. Res. Clin. Endocrinol. Metab. 2018, 32, 39–45. [CrossRef]
- Çullas İlarslan, N.E.; Şıklar, Z.; Berberoğlu, M. Childhood Sustained Hypercalcemia: A Diagnostic Challenge. J. Clin. Res. Pediatr. Endocrinol. 2017, 9, 315–322. [CrossRef]
- Tinawi ,M. Disorders of Calcium Metabolism: Hypocalcemia and Hypercalcemia. Cureus. 2021, 13(1), e12420. [CrossRef]
- Sorkhi, H.; Haji Aahmadi, M. Urinary calcium to creatinine ratio in children. Indian J Pediatr. 2005, 72(12), 1055-1056. [CrossRef]
- Penido, M.G.M.G.; Tavares, M.S. Should pediatric idiopathic hypercalciuria be treated with hypocalciuric agents? World J Nephrol. 2021, 10(4), 47-58.
- Gül, A.; Özer, S.; Yılmaz, R.; Sönmezgöz, E.; Kasap, T.; Takçı, Ş.; Karaaslan, E.; Önder, Y.; Çıtıl, R.; Bütün, İ.; Demir, O. Prevalence of hypercalciuria and urinary calcium excretion in school-aged children in the province of Tokat. Turk Pediatri Ars. 2016, 51(4), 193-197. [CrossRef]
- Penido, M.G M.G.; Tavares, M.S. Beyond kidney stones: Why pediatricians should worry about hypercalciuria. World J Clin Pediatr. 2021, 10(6), 137-150. [CrossRef]
- Cambareri, G.M.; Giel, D.W.; Bayne, A.P.; Corbett, S.; Schurtz, E.; Kovacevic, L.; Sukhu, T.; Yap, M.; Chiang, G. Overweight and Obese Pediatric Stone Formers Have Differences in Metabolic Abnormalities Compared With Normal-weight Stone Formers?. Urology. 2017, 101, 26-30. [CrossRef]
- Bandari, J.; Dangle, P.P.; Lyon, T.D.; Lee, A.; Schneck, F.X.; Cannon, G.M.; Stephany, H.A.; Ost, M.C. 24-Hour Urinary Parameters in Overweight and Obese Children with Urolithiasis. J Urol. 2016, 196(2), 526-530. [CrossRef]
- Al Ghali, R.; El-Mallah, C.; Obeid, O.; El-Saleh, O.; Smail, L.; Haroun, D. Urinary minerals excretion among primary schoolchildren in Dubai-United Arab Emirates. PLoS One. 2021, 16(8), e0255195. [CrossRef]
- Kaneko, K.; Tsuchiya, K.; Kawamura, R.; Ohtomo, Y.; Shimizu, T.; Yamashiro, Y.; Yamada, T.; Yamauchi, K.; Kitagawa, T. Low prevalence of hypercalciuria in Japanese children. Nephron. 2002, 91(3), 439-443. [CrossRef]
- Kaneko, K.; Chiba, M.; Hashizume, M., Kunii, O.; Sasaki, S.; Shimoda, T.; Yamashiro, Y.; Dauletbaev, D.; Caypil, W.; Mazhitova, Z. Extremely high prevalence of hypercalciuria in children living in the Aral Sea region. Acta Paediatrica. 2007, 91(10), 1116-20.
- Abdalbary, M.; Chishti, E.; Shakhashiro, M.; Mohamed, R.; Parikh, T.; Nassar, M.K.; Sayed-Ahmed, N.; Faugere, M.C.; Sawaya, B.P.; El-Husseini, A. Impact of urinary calcium excretion on kidney, bone, and cardiovascular systems in patients with bone biopsy proven osteoporosis: a longitudinal long-term follow-up study. Osteoporos Int. 2023, 34(4), 763-774. [CrossRef]
- Stam, S.P.; Eisenga, M.F.; Gomes-Neto, A.W.; van Londen, M.; de Meijer, V.E.; van Beek, A.P.; Gansevoort, R.T.: Bakker, S.J.L. Muscle mass determined from urinary creatinine excretion rate, and muscle performance in renal transplant recipients. J Cachexia Sarcopenia Muscle. 2019; (3), 621-629. [CrossRef]
- Stam, S.P.; Eisenga, M.F.; Gomes-Neto, A.W.; van Londen, M.; de Meijer, V.E.; van Beek, A.P.; Gansevoort, R.T.: Bakker, S.J.L. Muscle mass determined from urinary creatinine excretion rate, and muscle performance in renal transplant recipients. J Cachexia Sarcopenia Muscle. 2019, 10(3), 621-629. [CrossRef]
- Ubetagoyena Arrieta, M.; Areses Trapote, R.; Mendia Ubetagoyena, J.; Perez Revuelta, M.; García Albizua, I. Basal renal function in paediatric patients: correlation of methods that depend on a 24h urine collection with simpler methods that do not require a timed urine. An Pediatr. 2020, 92(2), 65-70. [CrossRef]
- Remer, T.; Neubert, A.; Maser-Gluth, C. Anthropometry-based reference values for 24-h urinary creatinine excretion during growth and their use in endocrine and nutritional research. Am J Clin Nutr. 2002, 75(3), 561-569. [CrossRef]
- Ullal, J.; Kutney, K.; Williams, K. M.; Weber, D. R. Treatment of cystic fibrosis related bone disease. J Clin Transl Endocrinol. 2021, 27, 100291. [CrossRef]
- Gordon, R.J.; Misra, M.; Mitchell, D.M. Osteoporosis and Bone Fragility in Children. [Updated 2023 Jul 20]. In: Feingold, K.R.; Anawalt, B.; Blackman, M.R; et al., editors. Endotext [Internet]. South Dartmouth (MA): MDText.com, Inc.; from, 2000.
- Williams, K.M.; Darukhanavala, A.; Hicks, R.; Kelly, A. An update on methods for as-sessing bone quality and health in Cystic fibrosis. J Clin Transl Endocrinol. 2021, 27, 100281.
- Ouyang, Y.; Quan, Y.; Guo, C.; Xie, S.; Liu, C.; Huang, X.; Huang, X.; Chen, Y.; Xiao, X.; Ma, N.; Xie, R. Saturation Effect of Body Mass Index on Bone Mineral Density in Adolescents of Different Ages: A Population-Based Study. Front Endocrinol (Lausanne). 2022, 13, 922903. [CrossRef]
- Acar, D.B.; Kavuncuoğlu, S.; Çetinkaya, M.; Petmezci, E.; Dursun, M.; Korkmaz, O.; Altuncu, E. K. Assessment of the place of tubular reabsorption of phosphorus in the diagnosis of osteopenia of prematurity. Turk Pediatri Ars. 2015, 50(1), 45-50. [CrossRef]
- Koljonen, L.; Enlund-Cerullo, M.; Hauta-Alus, H.; Holmlund-Suila, E.; Valkama, S.; Rosendahl, J.; Andersson, S.; Pekkinen, M.; Mäkitie, O. Phosphate Concentrations and Modifying Factors in Healthy Children From 12 to 24 Months of Age. J Clin Endocrinol Metab. 2021, 106(10), 2865-2875. [CrossRef]
- Arnold, A.; Dennison, E.; Kovacs, C.S.; Mannstadt, M.; Rizzoli, R.; Brandi, M.L.; Clarke, B.; Thakker, R.V. Hormonal regulation of biomineralization. Nat Rev Endocrinol. 2021; 17(5):261-275. [CrossRef]
- Akimbekov, N.S.; Digel, I.; Sherelkhan, D.K.; Razzaque, M.S. Vitamin D and Phosphate Interactions in Health and Disease. Adv. Exp. Med. Biol. 2022, 1362, 37–46.
- Bacchetta, J.; Bernardor, J.; Garnier, C.; Naud, C.; Ranchin, B. Hyperphosphatemia and Chronic Kidney Disease: A Major Daily Concern Both in Adults and in Children. Calcif Tissue Int. 2021, 108(1), 116-127. [CrossRef]
- Sharma, S.; Hashmi, M.F.; Kaur, J.; Castro, D. Hypophosphatemia. [Updated 2024 Feb 12]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2024 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK493172/.
- Uday, S.; Sakka, S.; Davies, J.H.; Randell, T.; Arya, V.; Brain, C.; Tighe, M.; Allgrove, J.; Arundel, P.; Pryce, R.; Högler, W.; Shaw, N.J. Elemental formula associated hypophosphataemic rickets. Clin Nutr. 2019, 38(5), 2246-2250. [CrossRef]
- Al Harbi, S.A.; Al-Dorzi, H.M.; Al Meshari, A.M.; Tamim, H.; Abdukahil, S.A.I.; Sadat, M.; Arabi, Y. Association between phosphate disturbances and mortality among critically ill patients with sepsis or septic shock. BMC Pharmacol Toxicol. 2021, 28, 22(1), 30. [CrossRef]
- Shah, S.K.; Irshad, M.; Gupta, N.; Kabra, S.K.; Lodha, R. Hypophosphatemia in Critically Ill Children: Risk Factors, Outcome and Mechanism. Indian J Pediatr. 2016, 83(12-13), 1379-1385. [CrossRef]
- Berger, M.M.; Appelberg, O.; Reintam-Blaser, A.; Ichai, C.; Joannes-Boyau, O.; Casaer, M.; Schaller, S.J.; Gunst, J.; Starkopf, J.; ESICM-MEN section. Prevalence of hy-pophosphatemia in the ICU - Results of an international one-day point prevalence survey. Clin Nutr. 2021, 40(5), 3615-3621.
- Sands D.; Mielus M.; Umławska W.; Lipowicz A.; Oralewska B.; Walkowiak J. Evaluation of factors related to bone disease in Polish children and adolescents with cystic fibrosis. Adv Med Sci. 2015, 60(2), 315–320. [CrossRef]
- Taranta-Janusz, K.; Łabieniec, Ł.; Porowski, T.; Szymański, K.; Porowska, H.; Wasilewska, A. Determining normal values of urinary phosphorus excretion in 3913 healthy children aged 2-18 to aid early diagnosis and treatment for urolithiasis. Acta Paediatr. 2017, 106(7), 1170-1175. [CrossRef]
- Jacquillet, G.; Unwin, R.J. Physiological regulation of phosphate by vitamin D, parathyroid hormone (PTH) and phosphate (Pi). Pflugers Arch. 2019, 471(1), 83-98. [CrossRef]
- Gil Gómez, R.; Milano Manso, G. Electrolitos urinarios. Anales de Pediatría Continuada. 2014, 12, 3, 133-136.
- Harrison, C.M, Johnson, K., McKechnie, E. Osteopenia of prematurity: a national survey and review of practice. Acta Pediatr. 2008, 97, 407–13. [CrossRef]
- Verploegen, M.F.A.; Vargas-Poussou, R.; Walsh, S.B.; Alpay, H.; Amouzegar, A.; Ariceta, G.; et.al. Parathyroid hormone and phosphate homeostasis in patients with Bartter and Gitelman syndrome: an international cross-sectional study. Nephrol Dial Transplant. 2022, 37(12), 2474-2486. [CrossRef]
- Mosca, M.; Bernardor, J.; Lemoine, S.; Bertholet-Thomas, A.; Bacchetta, J. Rare diseases of phosphate and calcium metabolism: Crossing glances between nephrology and endocrinology. Ann Endocrinol (Paris). 2021, 82(1), 30-35. [CrossRef]
- Loughrill, E.; Wray, D.; Christides, T.; Zand, N. Calcium to phosphorus ratio, essential elements and vitamin D content of infant foods in the UK: Possible implications for bone health. Matern. Child. Nutr. 2017, 13, e12368. [CrossRef]
- Sun, M.; Wu, X.; Yu, Y.; Wang, L.; Xie, D.; Zhang, Z.; Chen, L.; Lu, A.; Zhang, G.; Li, F. Disorders of Calcium and Phosphorus Metabolism and the Proteomics/Metabolomics-Based Research. Front Cell Dev Biol. 2020, 8, 576110.). [CrossRef]
- Cuadrado-Soto, E.; López-Sobaler, A.M.; Jiménez-Ortega, A.I.; Aparicio, A.; Bermejo, L.M., Hernández-Ruiz, Á.; et. al. Usual Dietary Intake, Nutritional Adequacy and Food Sources of Calcium, Phosphorus, Magnesium and Vitamin D of Spanish Children Aged One to <10 Years. Findings from the EsNuPI Study. Nutrients. 2020, 12(6), 1787.
- Bestepe, N.; Cuhaci, F.N.; Polat, B.; Ogmen, B.E.; Ozdemir, D.; Ersoy, R.; Cakir, B. Serum Calcium/Phosphorus Ratio in Biochemical Screening of Primary Hyperparathyroidism. Rev. Assoc. Med. Bras. (1992) 2022, 68, 1668–1674. [CrossRef]
- De Vincentis, S.; Del Sindaco, G.; Pagnano, A.; Brigante, G.; Moretti, A.; Zirilli, L.; Rochira, V.; Simoni, M.; Mantovani, G.; Madeo, B. Application of calcium-to-phosphorus (Ca/P) ratio in the diagnosis of pseudohypoparathyroidism: Another piece in the puzzle of diagnosis of Ca-P metabolism disorders. Front. Endocrinol. 2023, 14, 1268704. [CrossRef]
- Lin, S.H.; Chu, P.; Cheng, C.J.; Chu, S.J.; Hung, Y.J.; Lin, Y.F. Early diagnosis of thyrotoxic periodic paralysis: spot urine calcium to phosphate ratio. Crit Care Med. 2006, 34(12), 2984-2989. [CrossRef]
- Grez-Capdeville, M.; Crenshaw, T.D. Evaluation of calcium to phosphorus ratio in spot urine samples as a practical method to monitor phosphorus intake adequacy in sows. J. Anim. Sci. 2021, 99, skab335. [CrossRef]
Figure 1.
Flow diagram assignment of children with chronic disease (n = 39).
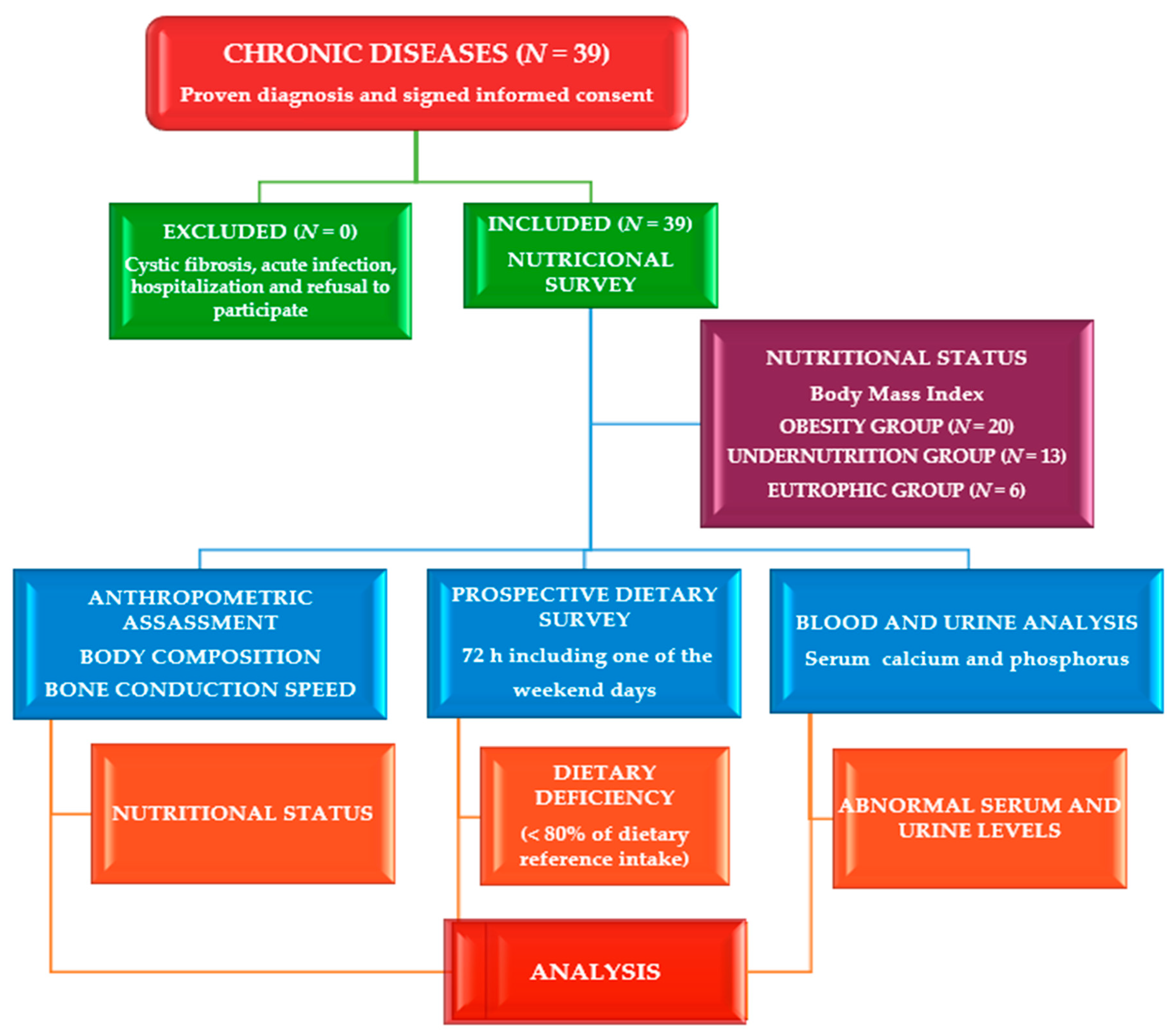
Figure 2.
Calcium (mg/L) and Phosphorus (mg/d) levels in urine 24-hours by age (years) (n = 39).
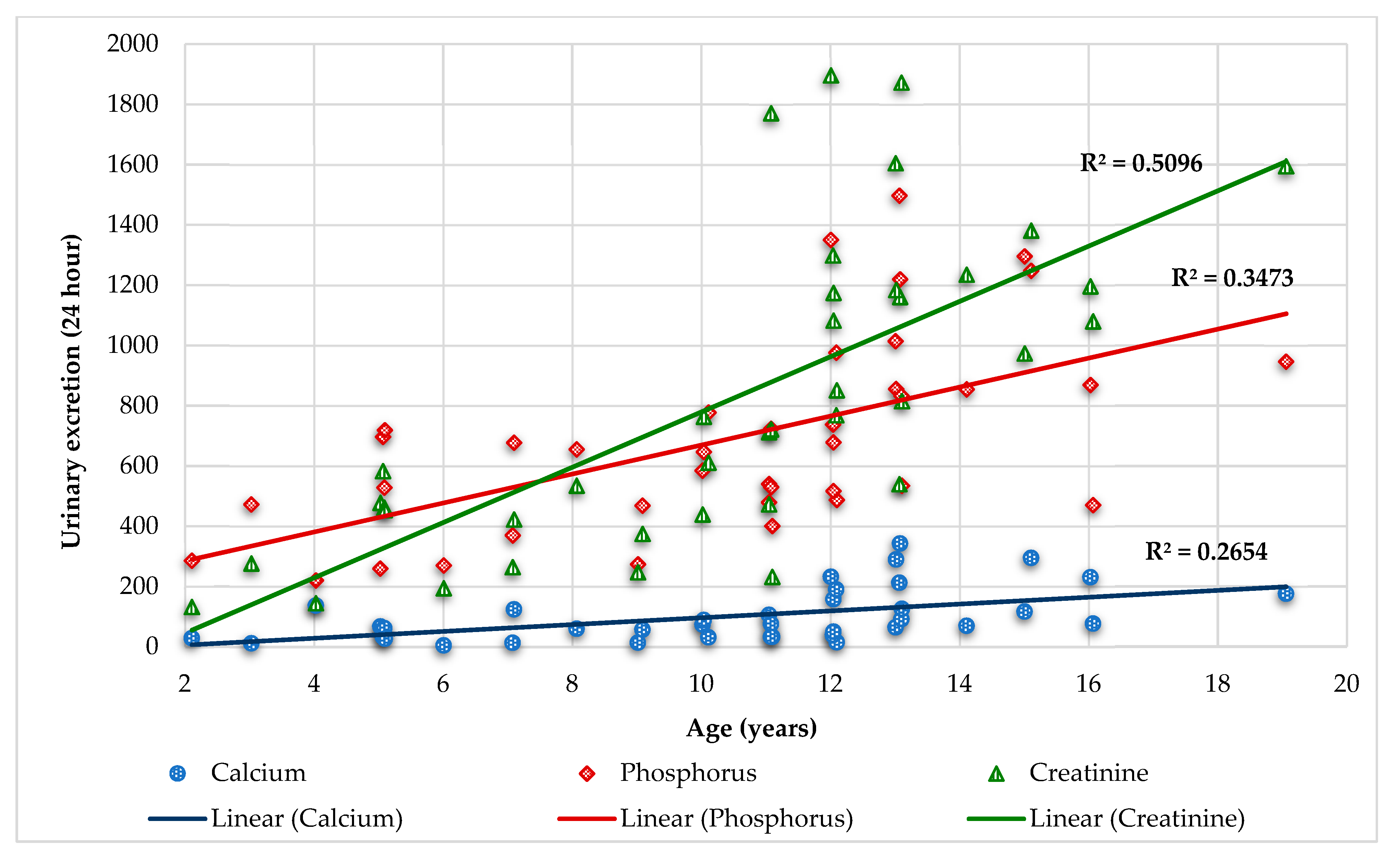

Table 1.
Baseline features of children with chronic diseases by body mass index groups (n = 39).
| Characteristics | Total (n = 39) |
Obesity (n = 20) |
Undernutrition (n = 13) |
Eutrophic (n = 6) |
p-Value |
|---|---|---|---|---|---|
| Mean ± SD | Mean ± SD | Mean ± SD | Mean ± SD | ||
| Dietary | |||||
| Calcium (%DRI) | 94 ± 28 | 93 ± 28 | 93 ± 27 | 100 ± 36 | 0.865 |
| Vitamin D (%DRI) | 75 ± 145 | 93 ± 194 | 61 ± 59 | 47 ± 74 | 0.734 |
| Serum | |||||
| Vitamin D (ng/mL) | 23.6 ± 15.9 | 18.2 ± 8.2 | 28.0 ± 21.6 | 32.3 ± 17.2 | 0.075 |
| Calcium (mg/dL) | 9.8 ± 0.3 | 9.9 ± 0.4 | 9.8 ± 0.2 | 9.9 ± 0.4 | 0.779 |
| Creatinine (mg/dL) | 0.53 ± 0.21 | 0.51 ± 0.16 | 0.47 ± 0.14 | 0.72 ± 0.39 | 0.059 |
| Phosphorus (mg/dL) | 4.7 ± 0.6 | 4.7 ± 0.6 | 4.7 ± 0.5 | 4.8 ± 0.4 | 0.894 |
| Calcium/phosphorus ratio | 2.12 ± 0.27 | 2.12 ± 0.28 | 2.13 ± 0.29 | 2.07 ± 0.16 | 0.919 |
| Calcium - phosphorus product | 46.8 ± 6.5 | 47.1 ± 7.6 | 45.9 ± 5.3 | 48.1 ± 5.2 | 0.818 |
| Alkaline phosphatase (U/L) | 353 ± 235 | 329 ± 252 | 435 ± 243 | 254 ± 91 | 0.244 |
| Urine | |||||
| Urine calcium (mg/kg/d) | 2.5 ± 2.3 | 1.7 ± 1.1 | 3.5 ± 3.0 | 2.9 ± 3.2 | 0.078 |
| 24-urine calcium (mg/L) | 101.2 ± 86.5 | 108.7 ± 82.6 | 79.1 ± 51.1 | 123.6 ± 150.5 | 0.509 |
| Creatinine (mg/kg/d) | 18.6 ± 7.3 | 15.6 ± 5.4 | 23.5 ± 8.1 | 18.2 ± 6.2 | 0.007* |
| 24-urine creatinine (mg/d) | 819.8 ± 504.5 | 999.5 ± 545.9 | 624.4 ± 383.9 | 644.5 ± 427.3 | 0.070 |
| Calcium/creatinine rate | 0.15 ± 0.16 | 0.14 ± 0.09 | 0.18 ± 0.25 | 0.14 ± 0.11 | 0.723 |
| Urine calcium excretion | 0.08 ± 0.07 | 0.06 ± 0.06 | 0.08 ± 0.09 | 0.09 ± 0.07 | 0.597 |
| Urine phosphorus (mg/kg/d) | 17.6 ± 7.4 | 13.8 ± 4.9 | 21.6 ± 7.6 | 21.7 ± 7.8 | 0.002* |
| 24-urine phosphorus (mg/d) | 690.8 ± 320.2 | 794.1 ± 305.5 | 530.8 ± 297.6 | 693.3 ± 320.7 | 0.066 |
| Fractional excretion of phosphorus | 11.4 ± 7.3 | 10.5 ± 7.0 | 9.6 ± 2.7 | 18.1 ± 11.6 | 0.043* |
| Calcium/phosphorus ratio | 0.14 ± 0.11 | 0.13 ± 0.07 | 0.17 ± 0.16 | 0.14 ± 0.14 | 0.571 |
| Calcium x phosphorus product | 50.2 ± 57.5 | 26.1 ± 21.8 | 78.9 ± 64.5 | 68.5 ± 92.0 | 0.021* |
| Tubular Reabsorption of Phosphate | 88.6 ± 7.3 | 89.5 ± 7.0 | 90.4 ± 2.7 | 81.9 ± 11.6 | 0.043* |
| TmP/GFR (mg/dL) | 4.6 ± 0.9 | 4.8 ± 1.1 | 4.6 ± 0.8 | 4.0 ± 0.7 | 0.261 |
Legend: TmP/GFR: Tubular maximum phosphate reabsorption per glomerular filtration rate.
Table 2.
Differences between participants with chronic diseases (n = 39).
| Gender | Female (n = 15) | Male (n = 24) | p-value |
|---|---|---|---|
| Body Fat Percentage | 28.9 ± 12.2 | 20.4 ± 11.2 | 0.036 |
| Bone Conduction Speed (Absolute value) | 1961 ± 79 | 1894 ± 50 | 0.006 |
| Serum phosphorus (mg/dL) | 4.6 ± 0.6 | 4.9 ± 0.5 | 0.029 |
| Serum calcium/phosphorus ratio | 2.2 ± 0.3 | 2.0 ± 0.2 | 0.049 |
| Serum calcium-phosphorus product | 45.0 ± 6.5 | 49.5 ± 5.6 | 0.035 |
| Alkaline phosphatase (mg/dL) | 286 ± 167 | 461 ± 291 | 0.022 |
| Urine phosphorus (mg/kg/d) | 15.2 ± 5.6 | 21.5 ± 8.4 | 0.008 |
| Age group | Children (n = 17) | Adolescents (n = 22) | |
| Calcium intake (%DRI) | 115 ± 26 | 78 ± 19 | <0.001 |
| Serum phosphorus (mg/dL) | 5.0 ± 0.4 | 4.5 ± 0.6 | 0.003 |
| Serum calcium/phosphorus ratio | 1.9 ± 0.2 | 2.2 ± 0.3 | 0.003 |
| Serum calcium-phosphorus product | 49.7 ± 4.7 | 44.5 ± 6.8 | 0.011 |
| 24-hour urine calcium | 50.2 ± 38.5 | 140.5 ± 93.2 | <0.001 |
| Urine creatinine (mg/kg/d) | 15.5 ± 5.9 | 21.0 ± 7.5 | 0.018 |
| 24-hour urine creatinine | 388.2 ± 177.9 | 1153.4 ± 411.1 | <0.001 |
| 24-hour urine phosphorus | 487.9 ± 187.3 | 847.6 ± 315.9 | <0.001 |
| Calcium intake (%DRI) | Deficient (n = 18) | Normal (n = 21) | |
| Bone conduction speed AV | 1966 ± 68 | 1906 ± 72 | 0.013 |
| Kilocalories (%DRI) | 85 ± 19 | 104 ± 26 | 0.013 |
| Serum phosphorus (mg/dL) | 4.5 ± 0.5 | 4.9 ± 0.5 | 0.016 |
| Serum calcium/phosphorus ratio | 2.2 ± 0.3 | 2.0 ± 0.2 | 0.016 |
| Serum Ca-P product (mg2/dL2) | 44.3 ± 5.8 | 48.9 ± 6.4 | 0.029 |
| Urine creatinine (mg/kg/d) | 21.1 ± 7.0 | 16.5± 7.3 | 0.049 |
| 24-hour urine creatinine | 1091.9 ± 509.3 | 586.6 ± 373.2 | 0.001 |
| Serum phosphorus | Deficiency (n = 14) | Normal (n = 25) | |
| Bone conduction speed AV | 1974 ± 61 | 1909 ± 73 | 0.011 |
| Serum calcium/phosphorus ratio | 2.4 ± 0.2 | 1.9 ± 0.1 | <0.001 |
| Serum calcium-phosphorus product | 40.4 ± 4.1 | 50.6 ± 4.4 | <0.001 |
| 24-hour urine creatinine | 1078.6 ± 558.9 | 674.9 ± 415.7 | 0.014 |
| TmP/GFR | 3.9 ± 0.6 | 5.0 ± 0.9 | <0.001 |
Legend: TmP/GFR: Tubular maximum phosphate reabsorption per glomerular filtration rate.
Table 3.
Odds Ratio in the whole series (n = 39).
| Fisher’s Exact Test | Odds Ratio | 95% Confidence Interval |
Cochran’s | Mantel–Haenszel | ||
|---|---|---|---|---|---|---|
| Lower | Upper | |||||
| Deficient calcium intake | ||||||
| Deficit kilocalories intake | 0.016 | 7.600 | 1.350 | 42.799 | 0.013 | 0.036 |
| Adolescents | <0.001 | 20.000 | 3.4807 | 114.9202 | <0.001 | <0.001 |
| High calcium/creatinine rate | ||||||
| High urine calcium (mg/kg/d) | 0.001 | 28.000 | 3.810 | 205.791 | <0.001 | <0.001 |
| High urine calcium (24-hour) | 0.018 | 11.200 | 1.600 | 78.400 | 0.006 | 0.028 |
| Hypercalciuria (mg/kg/d) | ||||||
| High urine calcium excretion | 0.006 | 26.000 | 2.287 | 295.637 | 0.001 | 0.008 |
| Hyperphosphaturia (mg/kg/d) | ||||||
| Hypercalciuria (mg/kg/d) | 0.026 | 9.692 | 1.060 | 88.653 | 0.022 | 0.060 |
| Low serum phosphorus | ||||||
| Adolescents | 0.029 | 1.786 | 1.062 | 3004 | 0.037 | 0.084 |
| Normal urine phosphorus (24-hour) | ||||||
| Very active/active | 0.035 | 1.429 | 0.986 | 2.069 | 0.023 | 0.074 |
Table 4.
Clinical and dietary evaluation of calcium and vitamin D intake, and levels of calcium, phosphorus, creatinine, calcium/phosphorus ratio and calcium-phosphorus products in blood and urine in patients with hypercalciuria and hyperphosphaturia (n = 39).
Table 4.
Clinical and dietary evaluation of calcium and vitamin D intake, and levels of calcium, phosphorus, creatinine, calcium/phosphorus ratio and calcium-phosphorus products in blood and urine in patients with hypercalciuria and hyperphosphaturia (n = 39).
| Age (years) |
Sex | BMI | Dietary | Serum | Urinary | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Ca | Vit-D | Ca | P | Vit-D | Ca/P ratio |
Ca-PP | Cr | ALP | Calcium | Creatinine | Ca/Cr rate |
UCaE | Phosphorus | FEP | TmP/ GFR |
Ca/P ratio |
Ca-PP | ||||||
| mg/kg/d | 24hU | mg/kg/d | 24hU | mg/kg/d | 24hU | ||||||||||||||||||
| 2 | F | 1.24 | 107 | 5# | 10.6* | 5.2 | 13# | 2.04 | 55.12* | 0.4 | 256 | 1.40 | 28 | 6.66# | 131 | 0.21* | 0.08 | 14.47 | 285 | 16.71 | 4.33 | 0.10 | 20.26 |
| 4 | M | -2.00# | 103 | 15# | 9.7 | 5.2 | 85 | 1.87 | 50.44 | 0.4 | 437* | 11.04* | 136 | 11.71# | 144 | 0.94* | 0.38* | 17.85* | 220 | 4.69 | 11.73 | 0.62 | 197 |
| 5 | M | -1.68 | 130 | 14# | 9.9 | 5.4 | 33 | 1.83 | 53.46 | 0.4 | 382* | 4.57* | 66 | 32.91* | 477 | 0.14 | 0.06 | 17.86* | 259 | 4.02 | 6.70* | 0.26 | 81.62 |
| 7 | M | -1.72 | 151 | 206 | 9.6 | 5.4 | 59 | 1.78 | 51.84 | 0.4 | 636* | 5.90* | 123 | 20.17 | 421 | 0.29* | 0.12 | 32.39* | 677 | 11.9 | 4.84 | 0.18 | 191.1 |
| 11 | F | -2.31# | 72# | 25 | 9.9 | 4.5 | 15# | 2.20 | 44.55 | 0.4 | 156 | 4.33* | 105 | 19.41 | 472 | 0.22* | 0.09 | 19.71* | 479 | 9.0 | 4.51 | 0.22 | 85.34 |
| 12 | F | -1.79 | 53# | 78# | 9.9 | 4.2# | 21 | 2.36 | 41.58 | 0.5 | 467* | 5.12* | 157 | 35.26* | 1082 | 0.15 | 0.07 | 22.08* | 678 | 7.45 | 4.49 | 0.23 | 113.0 |
| 12 | M | 1.95 | 112 | 32# | 10.8* | 5.8 | 20 | 1.86 | 62.40* | 0.2 | 223* | 3.90 | 189 | 15.80 | 768 | 0.24* | 0.05 | 20.08* | 976* | 4.38 | 7.08* | 0.19 | 78.31 |
| 12 | M | 3.53* | 76# | 33# | 9.7 | 4.5 | 10# | 2.16 | 43.65 | 0.6 | 349* | 2.57 | 232* | 21.04 | 1896 | 0.12 | 0.07 | 14.98 | 1350* | 9.49 | 4.43 | 0.17 | 38.50 |
| 13 | F | 1.52 | 67# | 20# | 9.8 | 4.7 | 58 | 2.09 | 46.06 | 0.7 | 167 | 5.20* | 289* | 21.29* | 1184 | 0.24* | 0.17* | 15.38 | 855 | 10.76 | 4.40 | 0.34 | 79.98 |
| 13 | F | -0.08 | 73# | 13# | 9.9 | 5.2 | 15# | 1.90 | 51.48 | 0.6 | 216 | 8.36* | 342* | 28.37* | 1160 | 0.29* | 0.18* | 29.80* | 1219* | 12.1 | 4.62 | 0.28 | 249.1 |
| 13 | F | 3.65* | 115 | 705 | 9.6 | 4.6 | 25 | 2.09 | 44.16 | 0.6 | 312* | 2.50 | 212* | 6.36# | 539 | 0.39* | 0.24* | 17.65* | 1497* | 36.20* | 2.93 | 0.14 | 44.13 |
| 15 | F | 3.39* | 55# | 103 | 10.1 | 4.5 | 12# | 2.24 | 45.45 | 0.8 | 254* | 4.08* | 294* | 19.15 | 1381 | 0.21* | 0.17* | 17.30* | 1247* | 16.06 | 3.78 | 0.24 | 70.58 |
| 16 | F | 3.44* | 64# | 18# | 10.0 | 3.6# | 23 | 2.78* | 36.00 | 0.7 | 87 | 3.01 | 230* | 15.67 | 1196 | 0.19 | 0.13 | 11.38 | 868 | 14.12 | 3.09 | 0.26 | 34.25 |
| 3 | M | -1.46 | 113 | 46# | 10.0 | 4.3# | 16# | 2.33 | 43.00 | 0.3 | 537* | 2.89 | 32.4 | 2.89# | 21 | 0.14 | 0.04 | 35.71* | 400 | 12.08 | 3.82 | 0.08 | 103.2 |
| 3 | M | -0.08 | 74# | 3# | 10.2 | 5.2 | 47 | 1.96 | 53.04 | 0.4 | 176 | 0.78 | 11.0 | 19.52 | 275 | 0.04 | 0.02 | 33.48* | 472 | 13.19 | 4.43 | 0.02 | 26.11 |
| 5 | M | 4.14* | 95 | 595 | 9.5 | 5.5 | 19# | 1.73 | 52.25 | 0.4 | 190 | 0.90 | 32.6 | 16.09 | 582 | 0.06 | 0.02 | 19.23* | 696 | 8.69 | 5.59* | 0.05 | 17.31 |
| 5 | M | 2.27* | 105 | 35# | 9.8 | 5.4 | 11# | 1.81 | 52.92 | 0.2 | 203 | 2.62 | 61.0 | 19.08 | 461 | 0.13 | 0.03 | 22.66* | 528 | 4.24 | 6.63 | 0.12 | 59.37 |
| 5 | F | 1.75 | 127 | 19# | 10.0 | 5.1 | 12# | 1.96 | 51.00 | 0.4 | 204 | 0.81 | 26.2 | 14.02 | 453 | 0.06 | 0.02 | 22.23* | 718 | 12.44 | 4.47 | 0.04 | 18.01 |
| 6 | F | -3.31# | 75* | 11# | 9.5 | 4.9 | 28 | 1.94 | 46.55 | 0.3 | 530* | 0.27 | 3.8 | 13.83 | 194 | 0.02 | 0.01 | 19.21* | 269 | 8.50 | 5.02 | 0.01 | 5.19 |
| 9 | M | -0.33 | 145 | 195 | 10.4 | 4.9 | 33 | 2.12 | 50.96 | 0.9 | 308 | 1.96 | 56.45 | 12.98# | 374 | 0.15 | 0.14 | 16.25 | 468 | 22.99* | 3.77 | 0.12 | 31.85 |
| 12 | F | -3.31# | 72# | 23# | 9.8 | 3.4# | 8# | 2.88* | 33.32 | 0.7 | 442* | 0.60 | 14.4 | 35.44* | 851 | 0.02 | 0.01 | 20.29* | 487 | 11.79 | 3.06 | 0.03 | 12.17 |
| 13 | M | 1.60 | 80 | 9# | 10.3 | 4.1# | 43 | 2.51 | 42.23 | 0.6 | 1056* | 0.89 | 63.64 | 22.44 | 1604 | 0.04 | 0.02 | 14.18 | 1014* | 9.25 | 4.07 | 0.06 | 12.62 |
| 14 | F | -1.82# | 92 | 59# | 9.9 | 4.4# | 29 | 2.25 | 43.56 | 0.7 | 201 | 1.40 | 69.0 | 25.03* | 1234 | 0.06 | 0.04 | 17.32* | 854 | 11.01 | 4.08 | 0.08 | 24.25 |
| 11 | F | -2.28# | 70# | 150 | 10.2 | 4.8 | 22 | 2.13 | 48.96 | 0.6 | 656* | 3.93 | 116 | 24.13* | 712 | 0.16 | 0.09 | 18.30* | 540 | 9.48 | 4.73 | 0.21 | 70.92 |
| 15 | M | -2.00# | 107 | 32# | 10.0 | 5.1 | 24 | 1.96 | 51.00 | 0.5 | 956* | 3.10 | 116 | 26.02* | 972 | 0.12 | 0.06 | 34.63* | 1295* | 13.05 | 4.37 | 0.09 | 107.3 |
| 10 | M | -0.62 | 97 | 12# | 9.3 | 4.5 | 17# | 2.07 | 41.85 | 1.4 | 408* | 0.74 | 30.7 | 14.71# | 610 | 0.05 | 0.07 | 18.72* | 777 | 39.59* | 2.72 | 0.04 | 13.85 |
| 19 | F | 3.21* | 119 | 17# | 9.4 | 3.7# | 10# | 2.54 | 34.78 | 0.7 | 165* | 1.58 | 175 | 14.36 | 1594 | 0.11 | 0.08 | 8.52 | 945* | 11.22 | 3.40 | 0.19 | 13.46 |
Legend: *: high values. #: low values. BMI: body mass index. F: female. M: male. Ca: calcium. Vit-: vitamin. P: phosphorus. Ca-PP: calcium-phosphorus product. Cr: creatinine, ALP: alkaline phosphatase. UCaE: urinary calcium excretion. FEP: fractional excretion of P. TmP/GFR: Tubular maximum phosphate reabsorption per glomerular filtration rate.
Table 5.
Linear and multilinear regression analysis between studied parameters with nutritional biomarkers in the whole series (n = 39).
Table 5.
Linear and multilinear regression analysis between studied parameters with nutritional biomarkers in the whole series (n = 39).
| Serum P | Serum Ca/P ratio | Serum Ca-PP |
Urine Ca mg/kg/d |
Urine Ca 24-hours |
Ca/Cr rate | Urine Ca excretion |
Urine P mg/kg/d |
Urine P 24-hour |
Urine P excretion | Urine Ca/P ratio |
Urine Ca-PP |
TRP | TmP/GFR |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Linear | regression | analysis | |||||||||||
| IgG3 R2 = 0.867 p = <0.001 |
WA R2 = 0.425 p = <0.001 |
||||||||||||
| TmP/GFR R2 = 0.474 p = <0.001 |
TmP/GFR R2 = 0.510 p = <0.001 |
Urine Ca excretion R2 = 0.847 p = <0.001 |
Ca/Cr rate R2 = 0.847 p = <0.001 |
Hit perimeter R2 = 0.466 p = <0.001 |
TRP R2 = 0.924 p = <0.001 |
Urine Ca (mg/kg/d) R2 = 0.867 p = <0.001 |
Urine P excretion R2 = 0.924 p = <0.001 |
||||||
| Serum Ca/P ratio R2 = 0.900 p = <0.001 |
Serum P R2 = 0.900 p = <0.001 |
Serum Ca-PP R2 = 0.723 p = <0.001 |
Urine Ca-PP R2 = 0.867 p = <0.001 |
Urine P 24-hour R2 = 0.459 p = <0.001 |
Urine Ca R2 = 0.700 p = <0.001 |
FM (kg) A R2 = 0.545 p = <0.001 |
GFR R2 = 0.454 p = <0.001 |
GFR R2 = 0.431 p = <0.001 |
|||||
| Serum Ca-PP R2 = 0.938 p = <0.001 |
Serum Ca-PP R2 = 0.723 p = <0.001 |
Serum P R2 = 0.938 p = <0.001 |
Urine Ca/P ratio R2 = 0.657 p = <0.001 |
Urine Ca/P ratio R2 = 0.714 p = <0.001 |
Urine Ca excretion R2 = 0.847 p = <0.001 |
FM index R2 = 0.432 p = <0.001 |
Excreted nitrogen R2 = 0.969 p = <0.001 |
Serum P R2 = 0.537 p = <0.001 |
|||||
| Multilinear | regression | analysis | Ca intake | ||||||||||
| TmP/GFR UCr 24-h R2 = 0.670 p = <0.001 |
Serum P, Serum Ca-PP R2 = 0.977 p = <0.001 |
Serum P, Serum Ca R2 = 0.999 p = <0.001 |
Urine Ca, Urine Ca/P ratio R2 = 0.988 p = <0.001 |
U. Ca/P ratio, U. P 24-hour R2 = 0.918 p = <0.001 |
Urine Ca*, Urine Ca excretion R2 = 0.878 p = <0.001 |
Ca/Cr rate Urine Ca 24-hour R2 = 0.902 p = <0.001 |
Triceps skinfold and Zs R2 = 0.544 p = <0.001 |
FFM (kg) A and FFM BIA R2 = 0.420 p = 0.003 |
BUN, Cr R2 = 0.754 p = <0.001 |
Urine Ca 24-hour, Ca/Cr rate R2 = 0.776 p = <0.001 |
Urine Ca*, Urine Ca/P ratio R2 = 0.976 p = <0.001 |
BUN, Cr R2 = 0.718 p = <0.001 |
Mg, Vit-E and A R2 = 0.538 p = <0.001 |
| Serum Ca/P ratio S. Ca-PP R2 = 0.995 p = <0.001 |
Urine Ca-PP, Urine Ca R2 = 0.650 p = <0.001 |
Urine Cr, urine Ca 24-hour R2 = 0.637 p = <0.001 |
HDL-C, Serum Vit-C R2 = 0.456 p = <0.001 |
Legend: Ca: calcium. P: phosphorus. Cr: creatinine. TRP: Tubular Reabsorption of Phosphate. TmP/GFR: Tubular maximum P reabsorption per glomerular filtration rate. Ig: immunoglobulin. WA: weight-for-age. FM: fat mas. FFM: fat free mass. A: anthropometry. BIA: bioelectric impedance analysis. GFR: glomerular filtration rate. Ca-PP: Ca-P product. *: mg/kg/d. Z-s: Z-score. %DRI: % Dietary Reference Intake. S: serum. BUN: blood urea nitrogen. Mg: magnesium. Vit: vitamin. HDL-C: high-density lipoprotein cholesterol.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



