
Submitted:
06 November 2024
Posted:
06 November 2024
You are already at the latest version
Abstract
Periprosthetic fractures of the proximal femur are one of the most frequent causes of revision after total hip arthroplasty. Internal fixation may be chosen if the hip implant is stable or if a stable fixation may be obtained. Preservation of bone perfusion and adequate stability are essential for successful fracture healing. As presented in this report, a patient developed both osteonecrosis and atrophy of the cortical bone due to use of a specific plate to treat a periprosthetic fracture of the femur. An 82-year-old female sustained a periprosthetic fracture of the proximal femur two years after cemented hemiarthroplasty. The fracture was treated by plate fixation. Along the proximal femoral diaphysis, cerclages were applied to avoid interference of screws with the femoral stem. Due to postoperative restrictions and finally due to pain, the patient never could be mobilized out of a wheelchair. After 4 years, pain persisted while the fracture had healed without loosening of the joint replacement components. However, pronounced atrophy of the whole femur was present, with devitalized areas of the bone underlying the plate. When not strictly applied as an internal fixator at a distance from the bone, the plate model used in this case may disturb periosteal blood flow, causing osteonecrosis. Furthermore, high bending rigidity of the plate-bone construct may lead to stress shielding and atrophy. The case illustrates that design and mechanical properties of a plate are relevant in bone biology and healing.conclusions. Clinical trial abstracts should include items that the CONSORT group has identified as essential.
Keywords:
Periprosthetic fracture
; femur
; Plate fixation
; internal fixation
; bone biology
; bone necrosis
; plate contact
1. Introduction
The introduction should briefly place the study in a broad context and highlight why it is important. It should define the purpose of the work and its significance. The current state of the research field should be carefully reviewed and key publications cited. Please highlight controversial and diverging hypotheses when necessary. Finally, briefly mention the main aim of the work and highlight the principal conclusions. As far as possible, please keep the introduction comprehensible to scientists outside your particular field of research. References should be numbered in order of appearance and indicated by a numeral or numerals in square brackets—e.g., [1] or [2,3], or [4,5,6]. See the end of the document for further details on references. Periprosthetic fractures (PPF) of the proximal femur are one of the most frequent causes of revision after total hip arthroplasty (THA) as well as after hip hemiarthroplasty (HHA) [1-3]. Revision of the stem is not always necessary in case of PPF, even if the fracture affects the area of anchorage of the implant. Internal fixation with cerclages and plate may be an adequate treatment option if the prosthetic stem is stable, or if a stable construct may be obtained with fixation [2,4-10].
Preservation of bone perfusion and adequate stability are essential for bone healing and thus success of internal fixation [11]. One of the main issues with internal fixation using plates is the potential compromise of bone perfusion by compression of the periosteal blood flow due to contact of the implant [12-15]. Additionally, bone healing may be impaired if stiffness of the construct does not correspond to fracture characteristics, respectively an implant too rigid may cause later stress shielding with consecutive bone atrophy [16]. Despite increasing experience and further development of internal fixation techniques for many decades, classical problems associated with plate fixation may still happen nowadays. As presented in this report, a patient developed necrosis and atrophy of the cortical bone following fixation of a PPF of the femur, despite using a plate specifically designed for this particular indication. Identification of these complications led to further investigations of the mechanical properties of plates commonly used for fixation of PPF of the femur.
2. Patient and Methods
Case Description
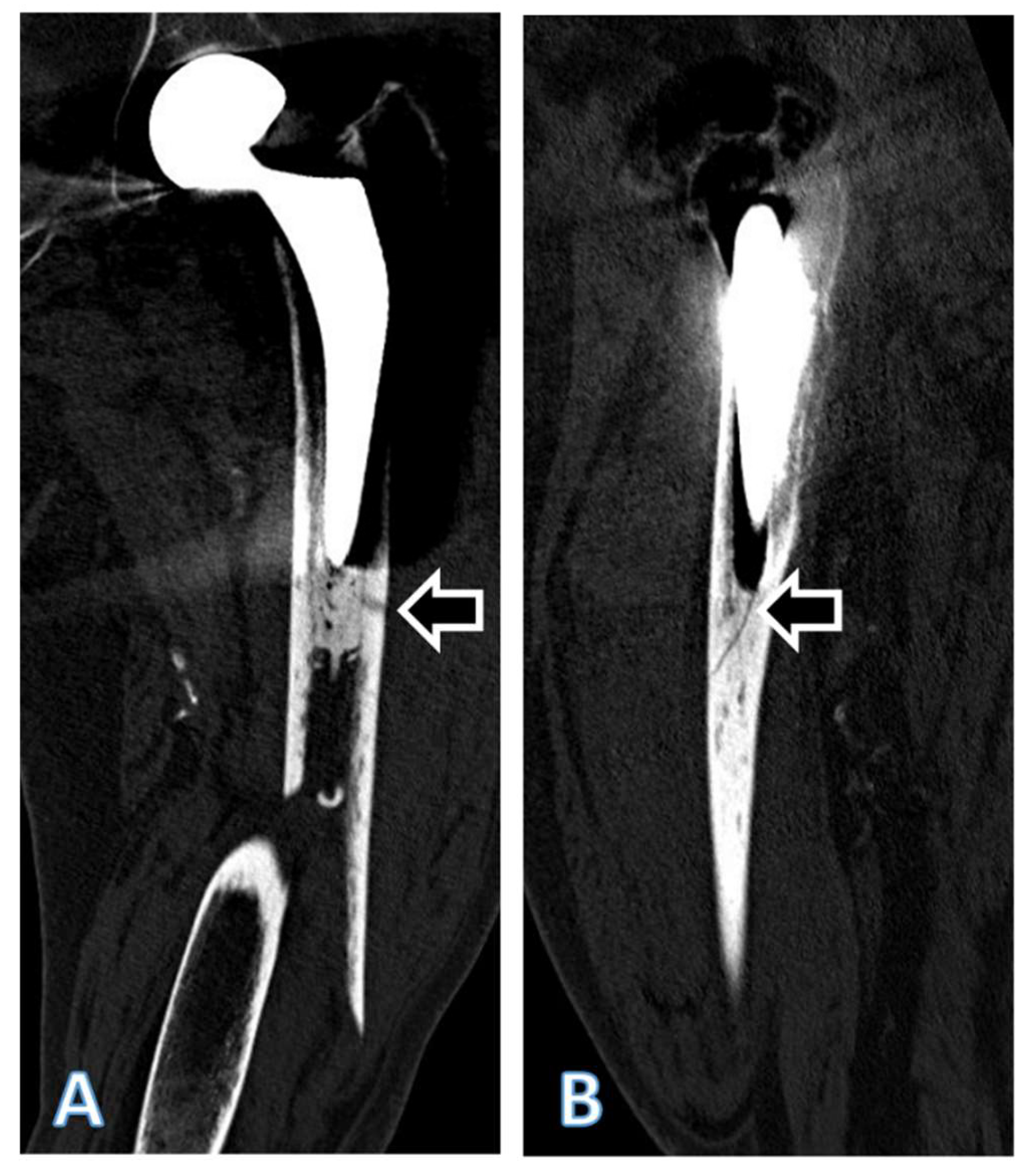
An 80-year-old female had been treated with a cemented HHA (AMIStem-C, Medacta, Castel San Pietro, Switzerland) for a low-energy femoral neck fracture (Figure 1A). Two years later, the now 82-years-old patient tripped and fell again, suffering a PPF of the femur (Figure 1B and 2). As the treating team considered the stem to be stable, with a fracture evaluated as being located distally to the area of fixation (UCS Type C)[17], plate fixation was chosen. Open reduction and internal fixation of the fracture was performed through a subvastus approach, with reduction and fixation by a cable cerclage (Cable System 1.7 mm, DePuy Synthes, Zuchwil, Switzerland) and application of a lateral neutralization plate (Non-Contact Bridging (NCB) Periprosthetic Femur Plate System 18 hole, Zimmer Biomet, Zug, Switzerland), fixated distally with screws and along the level of the stem with further cable cerclages (Cable System 1.7 mm). Postoperatively, the patient was mobilized in a wheelchair, as full weight-bearing was not recommended and as partial weight-bearing was not possible. Wound healing was uneventful.
Figure 1.
Conventional anteroposterior radiographs of the left hip, respectively the left femur of the patient described. In A, after cemented hemiarthroplasty, performed due to a femoral neck fracture, at an age of 80 years. In B, periprosthetic spiral fracture of the femoral diaphysis, two years postoperatively, following a low-energy fall. In C, after internal fixation of the femur. The fracture was first reduced with a cerclage (arrow), then a lateral neutralization plate was applied, fixated proximally with further cerclages and distally with screws. In D, follow-up 4 months after internal fixation. Note that no callus formation is visible, indicative of absolute stability. In E, follow-up 4 years after internal fixation. Note the atrophy of the cortical bone, both medially and laterally, but particularly under the plate (arrows). There were no signs of loosening of the stem, respectively of the cement mantle. The yellow line marks the level of the cross section from Figure 4 and 5.
Figure 1.
Conventional anteroposterior radiographs of the left hip, respectively the left femur of the patient described. In A, after cemented hemiarthroplasty, performed due to a femoral neck fracture, at an age of 80 years. In B, periprosthetic spiral fracture of the femoral diaphysis, two years postoperatively, following a low-energy fall. In C, after internal fixation of the femur. The fracture was first reduced with a cerclage (arrow), then a lateral neutralization plate was applied, fixated proximally with further cerclages and distally with screws. In D, follow-up 4 months after internal fixation. Note that no callus formation is visible, indicative of absolute stability. In E, follow-up 4 years after internal fixation. Note the atrophy of the cortical bone, both medially and laterally, but particularly under the plate (arrows). There were no signs of loosening of the stem, respectively of the cement mantle. The yellow line marks the level of the cross section from Figure 4 and 5.
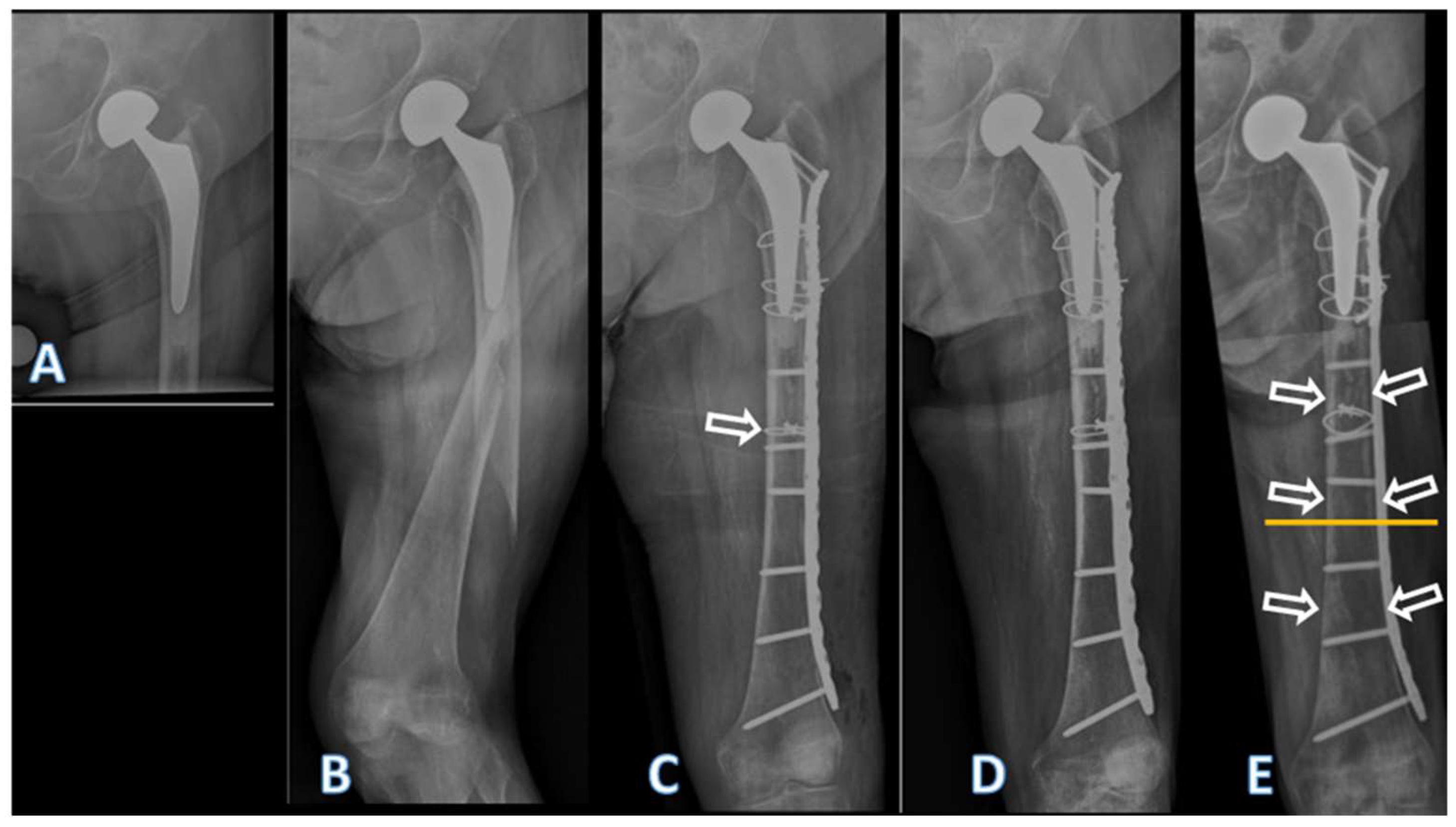
Figure 2.
Coronal (A) and sagital (B) CT scan reconstructions of the left femur of the patient described, showing the periprosthetic fracture. The extension of the fracture into the lateral cortex at the level of the tip of the stem (arrow in A) as well as a fracture of the cement distally to the tip of the stem (arrow in B) are visible. Both fracture extensions had been missed by the treating team. Accordingly, and considering the line-to-line principle of cementation of the affected stem, the fracture should be classified at least as UCS Type B2, if not B3, and not as a type C. The subluxated appearance of the head of the femoral head prosthesis is an artefact due to movement of the patient during the CT examination.
Figure 2.
Coronal (A) and sagital (B) CT scan reconstructions of the left femur of the patient described, showing the periprosthetic fracture. The extension of the fracture into the lateral cortex at the level of the tip of the stem (arrow in A) as well as a fracture of the cement distally to the tip of the stem (arrow in B) are visible. Both fracture extensions had been missed by the treating team. Accordingly, and considering the line-to-line principle of cementation of the affected stem, the fracture should be classified at least as UCS Type B2, if not B3, and not as a type C. The subluxated appearance of the head of the femoral head prosthesis is an artefact due to movement of the patient during the CT examination.
The radiological follow-up after 8 weeks showed intact material without evidence of loosening (Figure 1C). Mobilization under full weight-bearing with support by physical therapy was then attempted. Four months postoperatively, the radiological follow-up showed a general atrophy of the cortical bone, which was accentuated at the lateral cortex, underneath the plate (Figure 1D). Mobilization was hampered due to thigh pain, which had been interpreted to be caused by muscle atrophy. Thus, further physical therapy was recommended. As the impaired mobility caused difficulties attending consultation at the hospital, no further follow-up visit was planned.
Due to increasing thigh pain, the patient was readdressed for evaluation by her general practitioner 4 years after the operative treatment of the PPF. Not having been mobilized outside a wheelchair in the meantime, the patient showed bilateral hip and knee flexion contractures. Consequently, she was unable to stand, disregarding the issue of thigh pain. Radiologically, there was now pronounced atrophy of the cortical bone of the femur, particularly of the lateral cortex under the plate (Figure 1E). An infection was considered unlikely, as there was no pain at rest, as the soft tissues were inconspicuous, as the fracture had healed, and as there were no general symptoms. A SPECT-CT showed areas of necrotic cortical bone underneath the plate (Figure 3). The CT better illustrated a general atrophy of the femur with thinning of the bone cortex in comparison to the contralateral femur (Figure 4 and 5). There was however no sign of loosening of the stem. Considering comorbidities, very limited potential for recovery and the patients' desire for no more surgery, the option of a revision was rejected, accepting the present situation. The patient died 7 months later.
Mechanical properties of the plates
The following plates were chosen for further investigation: a NCB plate, made of titanium-aluminum-vanadium alloy, corresponding to the one used in this case, a broad curved 4.5/5.0 mm LCP made of stainless steel (DePuy Synthes, Oberdorf, Switzerland), a broad curved 4.5/5.0 mm LCP made of forged titanium (DePuy Synthes) and a narrow 4.5/5.0 mm LCP made of stainless steel (DePuy Synthes). Differing from the LCP design, the NCB plate has a varying cross-section along the length of the plate. The plates were photo-documented and dimensions measured before destructive testing.
A 4-point bending test according to ASTM (American Society for Testing and Materials) F382-17 was performed to determine the bending behavior of the plates [18]. The NCB plate, considering the non-uniform cross-section in the longitudinal axis, was positioned according to the in vivo situation, the compression area corresponding approximately to the tip of the stem (Figure 1).
3. Results
The undersurface of the NCB has a design markedly different from the LCP, as it has a longitudinal groove adapting to the curvature of the femoral diaphysis and it has no undercuts (Figure 6). While having nearly the same thickness (NCB: 6.2 mm, 4.5/5.0 mm LCP: 5.8 mm), the NCB is wider (20.8 mm at the approximate level of the tip of the stem in this case) than the broad 4.5/5.0 mm LCP plate (17.5 mm; Figure 6). Considering the cross-section being rectangular and disregarding screw holes, the cross-sectional area of the NCB at the level of interest is 129 mm2, and 101.5 mm2 for the broad 4.5/5.0 mm LCP, thus 27% larger for the NCB. The axial area moment of inertia of the plate (Iz=1/12 x (height3 x width)), representing the resistance of the cross-section against bending, would be approximately 413 mm4 for the NCB plate and thus approximately 45% greater than for the broad 4.5/5.0 mm LCP, which has approximately 285 mm4. Considering the modulus of elasticity of pure and alloyed titanium equal, the bending stiffness of the NBC being 45% greater than the broad LCP
There were marked differences between the four plates regarding bending behavior (Table 1, Figure 6). The narrow 4.5/5.0 mm LCP had the lowest resistance to bending. The titanium alloy NCB plate had the highest stiffness and resistance to bending due to its greater cross-section. The NCB was about twice as rigid as the broad LCP made of pure titanium. The broad 4.5/5.0 mm LCP made of stainless steel was more rigid than the narrow 4.5/5.0 mm LCP of the same material.
4. Discussion
The treatment of a PPF with internal fixation is an established surgical treatment option [8,19]. Whether internal fixation is adequate for treatment of PPF of the femur depends on the stability of the stem, respectively the fracture pattern and localization, as well as potential stability after fixation [2]. The general condition of the patient may also be part of the decision-making process, internal fixation being potentially less invasive than stem revision. Thus internal fixation may be an acceptable option in case of severe comorbidities and limited functional requirements, even if otherwise stem revision would be the treatment of choice from a mechanical point of view [9,19-24].
In the presented case, the fracture had been classified by the treating team as a type C fracture, according to the UCS classification [17]. However, a more detailed analysis of the CT scan showed an extension of the fracture into the lateral cortex at the level of the tip of the stem, as well as a fracture of the cement at the same level (Figure 2). Cement fixation of the stem design used in this case was based on the line-to-line concept [25-27]. An interruption of the connection between the stem and the cement leads to an unstable situation with this kind of cementation principle [2,27]. Therefore, the fracture should have been classified correctly as a type B2, possibly even B3, considering the poor bone quality. Low functional demands were probably decisive regarding the outcome of the stem, as the patient never became ambulatory again. Thorough radiologic work-up of PPF, including evaluation of the zone of fixation of the affected implant, is recommended before decision-making [20].
When opting for internal fixation, it is recommended to apply a plate spanning the entire length of the femur (Froberg, Troelsen et al. 2012). Various implants are available for the treatment of PPF. Universal plates such as the standard large fragment LCP (DePuy Synthes) can be used. Alternatively, anatomically pre-shaped plates are available from different manufacturers, such as the NCB plate (Zimmer Biomet), which had been applied in this case. The latter plate possesses some specific design features that need consideration when employing it for internal fixation of PPF.
A relevant proportion of the blood supply to the bone of the diaphysis originates from the periosteum [12,28]. Implants used for internal fixation, such as conventional plate-screw-constructs, can impede blood supply by exerting direct pressure on the bone, consecutively increasing the risk of local bone necrosis and nonunion [11-13,15,29]. Undercuts have been incorporated into plate designs to reduce contact with the underlying bone and preserve blood supply [11-13,15,29,30]. In contrast, the undersurface of the NCB plate lacks such indentations (Figure 7). When applied directly to the bone, the longitudinal groove of the NCB may potentially compromise blood perfusion on a relatively large surface, especially if the edges of the groove compress the periosteum. In the present case, the plate had been in applied in direct contact with the bone and with considerable pressure, exerted by the cerclages and conventional non-locking screws. Cortical bone necrosis due to compression of the periosteal vessels may be avoided if the NCB plate is used as an internal fixator, applied at a distance from the bone. However, this may not be possible if cerclages have to be used to avoid interference of screws with the prosthesis stem and/or cement. While the NCB system offers the possibility to use stub screws as distance holders, this may prove inadequate in such situations., Cerclages are usually necessary in the segment of the underlying stem to achieve and maintain adequate reduction of the bone fragments and stabilize the plate. In osteoporotic bone, stub screws would be prone to being crushed into the bone cortex, failing the distance holding function or creating additional fractures lines. Additionally, cortical screws are often required in the distal plate segment for reduction or to reduce the risk of later peri-implant fracture [31]. This would lead to loss of the non-contact concept of the NCB plate and compression of the periosteum by the plate. Beside the biological advantages of plate undercuts, they also serve homogenizing stiffness along the plate despite the presence of screw holes [32]. This is obtained on the NCB plate with various outcuts, that do not offer any protection for the periosteal vessels.
In the presented case, the fracture healed despite application of the plate, and there was no mechanical failure of the plate itself. However, marked atrophy of the cortical bone developed (Figure 1, 3, 4 and 5), additionally to the necrosis of the bone directly under the plate (Figure 4). The stiffness of the plate-bone composite beam leads to unloading of the underlying bone (stress shielding). Mechanical unloading of the bone cortex is probably triggering bone remodeling and localized bone atrophy as a long-term effect [33]. Avoidance of postoperative weight-bearing certainly was contributive, but as the contralateral femur did not develop particular atrophy, rigidity of the fixation may be considered as the main cause in this case. The hip replacement implant may not be incriminated, as the atrophy appeared far more distally along the femur. Even if the bending stiffness of the various plates differ only moderately, the bending rigidity of the plate-bone-composite beam may however be increased by a much higher proportion and end up being excessive and problematic [34].
Both the material properties and the design of the plate, particularly the cross-sectional area, are essential determinants of the bending stiffness and behavior of the implant [34]. The NCB plate is made of titanium-aluminum-vanadium alloy, which shares a similar elasticity modulus with the pure titanium used for AO/ASIF-standard implants [35,36]. Among the metals and alloys employed for orthopaedic implants, pure and alloyed titanium come closest to the elasticity of bone, albeit their modulus of elasticity remains up to 7 fold higher than that of cortical bone, whose modulus of elasticity is generally between 17 and 28 GPa [37-39]. In the static bending test carried out, the NCB plate demonstrated the highest bending stiffness among the four implants tested. Calculation of cross-sectional properties and measurement of the bending behavior of the plate both confirm the highest stiffness for the NCB plate. The broad 4.5/5.0 mm LCP made of pure titanium has a significantly lower stiffness than the NCB plate, despite being made of a metals with a similar elasticity modulus. Even though the modulus of elasticity of stainless steel (approximatively 190-200 GPa) is higher than for pure and alloyed titanium (approximatively 110 GPa), the test shows that the NCB plate is stiffer than a broad 4.5/5.0 mm LCP made of stainless steel. This difference can be attributed to the much larger cross-section of the NCB plate (Figure 7). It is worth noting that plates and constructs with higher rigidity have been identified as a risk factor for non-union of distal femur fractures, suggesting that excessive rigidity may be detrimental in fracture fixation [40].
Regaining walking ability following a PPF of the femur is challenging, with only half of the patients able to return to their initial functional level [41]. Elderly people are usually not able to maintain partial weight-bearing cannot be maintained by [42,43]. Therefore, postoperative mobilization of the patients commonly is limited to a wheelchair, for fear full weight-bearing may overload the recently performed fracture fixation. However, such immobilization can have dire consequences for these predominantly elderly and frail patients, as demonstrated in the case presented. Immobilization leads to loss of bone and muscle mass, and accelerates mental deterioration as well [44-46]. Consequently, the treatment of PPF of the femur should aim at early mobilization of the patient to ensure functionally good result. Internal fixation of PPF of the femur in the elderly should ideally provide enough stability to allow unrestricted weight-bearing and early mobilization. In case of a simple periprosthetic fracture and low energy traumatism, optimal stability is achieved best with a tension-band plating (load sharing concept). Unfortunately, this possibility is often overlooked, particularly with the rising popularity of new anatomically pre-shaped plating systems designed as internal fixators. Nevertheless, even internal fixators can be utilized as effective tension band stabilization systems when applied appropriately.
Author Contributions
Conceptualization, Hanna Wellauer and Peter Wahl, investigation, Hanna Wellauer, Niklaus Meyer, writing original draft, Hanna Wellauer, visualization, Hanna Wellauer, Bernd Klaeser, validation, Emanuel Gautier, Christoph Meier, resources, Emanuel Gautier, Supervision, Peter Wahl, writing-review & editing, Emanuel Gautier, Bernd Klaeser, Niklaus Meyer, Christoph Meier.
Funding
This research received no external funding.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Dataset available on request from the authors
Acknowledgments
Special thanks to Stefan Röthlisberger and Stefan Jakobs from RMS Foundation, Bettlach, Switzerland, for the mechanical tests.
Conflicts of Interest
The authors declare no conflicts of interest
References
- Abdel, M.; Watts, C.; Houdek, M.; Lewallen, D.; Berry, D. Epidemiology of periprosthetic fracture of the femur in 32 644 primary total hip arthroplasties: a 40-year experience. The bone & joint journal 2016, 98, 461-467.
- Stoffel, K.; Horn, T.; Zagra, L.; Mueller, M.; Perka, C.; Eckardt, H. Periprosthetic fractures of the proximal femur: beyond the Vancouver classification. EFORT open reviews 2020, 5, 449-456.
- SIRIS. Swiss National Hip&Knee Joint Registry Annual Report 2023; 2023.
- Moloney, G.B.; Westrick, E.R.; Siska, P.A.; Tarkin, I.S. Treatment of periprosthetic femur fractures around a well-fixed hip arthroplasty implant: span the whole bone. Archives of orthopaedic and trauma surgery 2014, 134, 9-14.
- Xue, H.; Tu, Y.; Cai, M.; Yang, A. Locking compression plate and cerclage band for type B1 periprosthetic femoral fractures: preliminary results at average 30-month follow-up. The Journal of Arthroplasty 2011, 26, 467-471. e461.
- Buttaro, M.; Farfalli, G.; Núñez, M.P.; Comba, F.; Piccaluga, F. Locking compression plate fixation of Vancouver type-B1 periprosthetic femoral fractures. JBJS 2007, 89, 1964-1969.
- Ehlinger, M.; Adam, P.; Moser, T.; Delpin, D.; Bonnomet, F. Type C periprosthetic fractures treated with locking plate fixation with a mean follow up of 2.5 years. Orthopaedics & Traumatology: Surgery & Research 2010, 96, 44-48.
- Froberg, L.; Troelsen, A.; Brix, M. Periprosthetic Vancouver type B1 and C fractures treated by locking-plate osteosynthesis: fracture union and reoperations in 60 consecutive fractures. Acta orthopaedica 2012, 83, 648-652.
- González-Martín, D.; Pais-Brito, J.L.; González-Casamayor, S.; Guerra-Ferraz, A.; Ojeda-Jiménez, J.; Herrera-Pérez, M. Treatment algorithm in Vancouver B2 periprosthetic hip fractures: osteosynthesis vs revision arthroplasty. EFORT Open Reviews 2022, 7, 533.
- Graham, S.M.; Moazen, M.; Leonidou, A.; Tsiridis, E. Locking plate fixation for Vancouver B1 periprosthetic femoral fractures: a critical analysis of 135 cases. Journal of Orthopaedic Science 2013, 18, 426-436.
- Perren, S.M. Evolution of the internal fixation of long bone fractures: the scientific basis of biological internal fixation: choosing a new balance between stability and biology. The Journal of bone and joint surgery. British volume 2002, 84, 1093-1110.
- Jacobs, R.; Rahn, B.; Perren, S. Effects of plates on cortical bone perfusion. The Journal of trauma 1981, 21, 91-95.
- Field, J.R.; Hearn, T.C.; Caldwell, C.B. Bone plate fixation: an evaluation of interface contact area and force of the dynamic compression plate (DCP) and the limited contact-dynamic compression plate (LC-DCP) applied to cadaveric bone. Journal of orthopaedic trauma 1997, 11, 368-373.
- Gautier, E.; Rahn, B.; Perren, S. Vascular remodelling. Injury 1995, 26, B11-B19.
- Perren, S.M.; Cordey, J.; Rahn, B.A.; Gautier, E.; Schneider, E. Early temporary porosis of bone induced by internal fixation implants. A reaction to necrosis, not to stress protection? Clin Orthop Relat Res 1988, 139-151.
- Bottlang, M.; Doornink, J.; Lujan, T.J.; Fitzpatrick, D.C.; Marsh, J.L.; Augat, P.; von Rechenberg, B.; Lesser, M.; Madey, S.M. Effects of construct stiffness on healing of fractures stabilized with locking plates. JBJS 2010, 92, 12-22.
- Duncan, C.; Haddad, F. The Unified Classification System (UCS): improving our understanding of periprosthetic fractures. The bone & joint journal 2014, 96, 713-716.
- ASTM. ASTM Volume 13.01: Medical And Surgical Materials And Devices (I): E667–F2477 2023.
- Gonzalez-Martin, D.; Hernández-Castillejo, L.E.; Herrera-Pérez, M.; Pais-Brito, J.L.; Gonzalez-Casamayor, S.; Garrido-Miguel, M. Osteosynthesis versus revision arthroplasty in Vancouver B2 periprosthetic hip fractures: a systematic review and meta-analysis. European Journal of Trauma and Emergency Surgery 2022, 1-20.
- Patsiogiannis, N.; Kanakaris, N.K.; Giannoudis, P.V. Periprosthetic hip fractures: an update into their management and clinical outcomes. EFORT Open Reviews 2021, 6, 75.
- Mondanelli, N.; Troiano, E.; Facchini, A.; Ghezzi, R.; Di Meglio, M.; Nuvoli, N.; Peri, G.; Aiuto, P.; Colasanti, G.B.; Giannotti, S. Treatment algorithm of periprosthetic femoral fracturens. Geriatric Orthopaedic Surgery & Rehabilitation 2022, 13, 21514593221097608.
- Niikura, T.; Lee, S.Y.; Sakai, Y.; Nishida, K.; Kuroda, R.; Kurosaka, M. Treatment results of a periprosthetic femoral fracture case series: treatment method for Vancouver type b2 fractures can be customized. Clinics in Orthopedic Surgery 2014, 6, 138-145.
- Spina, M.; Scalvi, A. Vancouver B2 periprosthetic femoral fractures: a comparative study of stem revision versus internal fixation with plate. European Journal of Orthopaedic Surgery & Traumatology 2018, 28, 1133-1142.
- Stoffel, K.; Blauth, M.; Joeris, A.; Blumenthal, A.; Rometsch, E. Fracture fixation versus revision arthroplasty in Vancouver type B2 and B3 periprosthetic femoral fractures: a systematic review. Archives of Orthopaedic and Trauma Surgery 2020, 140, 1381-1394.
- Verdonschot, N. Philosophies of stem designs in cemented total hip replacement. Orthopedics 2005, 28, S833-S840.
- Scheerlinck, T.; Casteleyn, P.-P. The design features of cemented femoral hip implants. The Journal of Bone and Joint Surgery. British volume 2006, 88, 1409-1418.
- Beel, W.; Klaeser, B.; Kalberer, F.; Meier, C.; Wahl, P. The Effect of a Distal Centralizer on Cemented Femoral Stems in Arthroplasty Shown on Radiographs and SPECT/CT: A Case Report. JBJS Case Connector 2021, 11, e20.
- Rhinelander, F.W. The normal microcirculation of diaphyseal cortex and its response to fracture. JBJS 1968, 50, 784-800.
- Gautier, E.; Perren, S. Limited Contact Dynamic Compression Plate (LC-DCP)--biomechanical research as basis to new plate design. Der Orthopade 1992, 21, 11-23.
- Gautier, E.; Sommer, C. Guidelines for the clinical application of the LCP. Injury 2003, 34, 63-76.
- Bottlang, M.; Doornink, J.; Byrd, G.D.; Fitzpatrick, D.C.; Madey, S.M. A nonlocking end screw can decrease fracture risk caused by locked plating in the osteoporotic diaphysis. JBJS 2009, 91, 620-627.
- Perren, S.; Mane, K.; Pohler, O.; Predieri, M.; Steinemann, S.; Gautier, E. The limited contact dynamic compression plate (LC-DCP). Archives of orthopaedic and trauma surgery 1990, 109, 304-310.
- Gautier, E.; Perren, S.; Cordey, J. Strain distribution in plated and unplated sheep tibia an in vivo experiment. Injury 2000, 31, 37-93.
- Gautier, E.; Perren, S.; Cordey, J. Effect of plate position relative to bending direction on the rigidity of a plate osteosynthesis. A theoretical analysis. Injury 2000, 31, 14-92.
- Disegi, J. Implant Materials. Titanium - 6% Aluminum - 7% Niobium. 2008, Second Edition.
- Zimmer. Periprosthetic Bone Plate. 7 juni 2010 2011.
- Niinomi, M. Mechanical properties of biomedical titanium alloys. Materials Science and Engineering: A 1998, 243, 231-236.
- Geetha, M.; Singh, A.K.; Asokamani, R.; Gogia, A.K. Ti based biomaterials, the ultimate choice for orthopaedic implants–a review. Progress in materials science 2009, 54, 397-425.
- Dickenson, R.; Hutton, W. The mechanical properties of bone in osteoporosis. The Journal of Bone & Joint Surgery British Volume 1981, 63, 233-238.
- Rodriguez, E.K.; Zurakowski, D.; Herder, L.; Hall, A.; Walley, K.C.; Weaver, M.J.; Appleton, P.T.; Vrahas, M. Mechanical construct characteristics predisposing to non-union after locked lateral plating of distal femur fractures. Journal of Orthopaedic Trauma 2016, 30, 403-408.
- Moreta, J.; Aguirre, U.; de Ugarte, O.S.; Jáuregui, I.; Martínez-De Los Mozos, J.L. Functional and radiological outcome of periprosthetic femoral fractures after hip arthroplasty. Injury 2015, 46, 292-298.
- Eickhoff, A.M.; Cintean, R.; Fiedler, C.; Gebhard, F.; Schütze, K.; Richter, P.H. Analysis of partial weight bearing after surgical treatment in patients with injuries of the lower extremity. Archives of orthopaedic and trauma surgery 2022, 142, 77-81.
- Vasarhelyi, A.; Baumert, T.; Fritsch, C.; Hopfenmüller, W.; Gradl, G.; Mittlmeier, T. Partial weight bearing after surgery for fractures of the lower extremity–is it achievable? Gait & posture 2006, 23, 99-105.
- Bentler, S.E.; Liu, L.; Obrizan, M.; Cook, E.A.; Wright, K.B.; Geweke, J.F.; Chrischilles, E.A.; Pavlik, C.E.; Wallace, R.B.; Ohsfeldt, R.L. The aftermath of hip fracture: discharge placement, functional status change, and mortality. American journal of epidemiology 2009, 170, 1290-1299.
- Mobily, P.R.; Kelley, L.S. Iatrogenesis in the elderly: factors of immobility. 1991, 17, 5-9.
- Osnes, E.; Lofthus, C.; Meyer, H.; Falch, J.; Nordsletten, L.; Cappelen, I.; Kristiansen, I.S. Consequences of hip fracture on activities of daily life and residential needs. Osteoporosis international 2004, 15, 567-574.
Figure 3.
In A, overview image for orientation. In B, paracoronal view of the SPECT of the left femur 4 years after plate fixation of a periprosthetic fracture of the proximal femur after cemented hemiarthroplasty of the hip. In C, paracoronal reconstruction of the SPECT/CT fusion image of the left femur, also illustrating the implant. The bone directly under the plate showed no detectable metabolic activity in various areas (arrows). In the area of the medial cortex, however, there was compensatory increased activity, which is to be explained by the atrophy of the bone.
Figure 3.
In A, overview image for orientation. In B, paracoronal view of the SPECT of the left femur 4 years after plate fixation of a periprosthetic fracture of the proximal femur after cemented hemiarthroplasty of the hip. In C, paracoronal reconstruction of the SPECT/CT fusion image of the left femur, also illustrating the implant. The bone directly under the plate showed no detectable metabolic activity in various areas (arrows). In the area of the medial cortex, however, there was compensatory increased activity, which is to be explained by the atrophy of the bone.
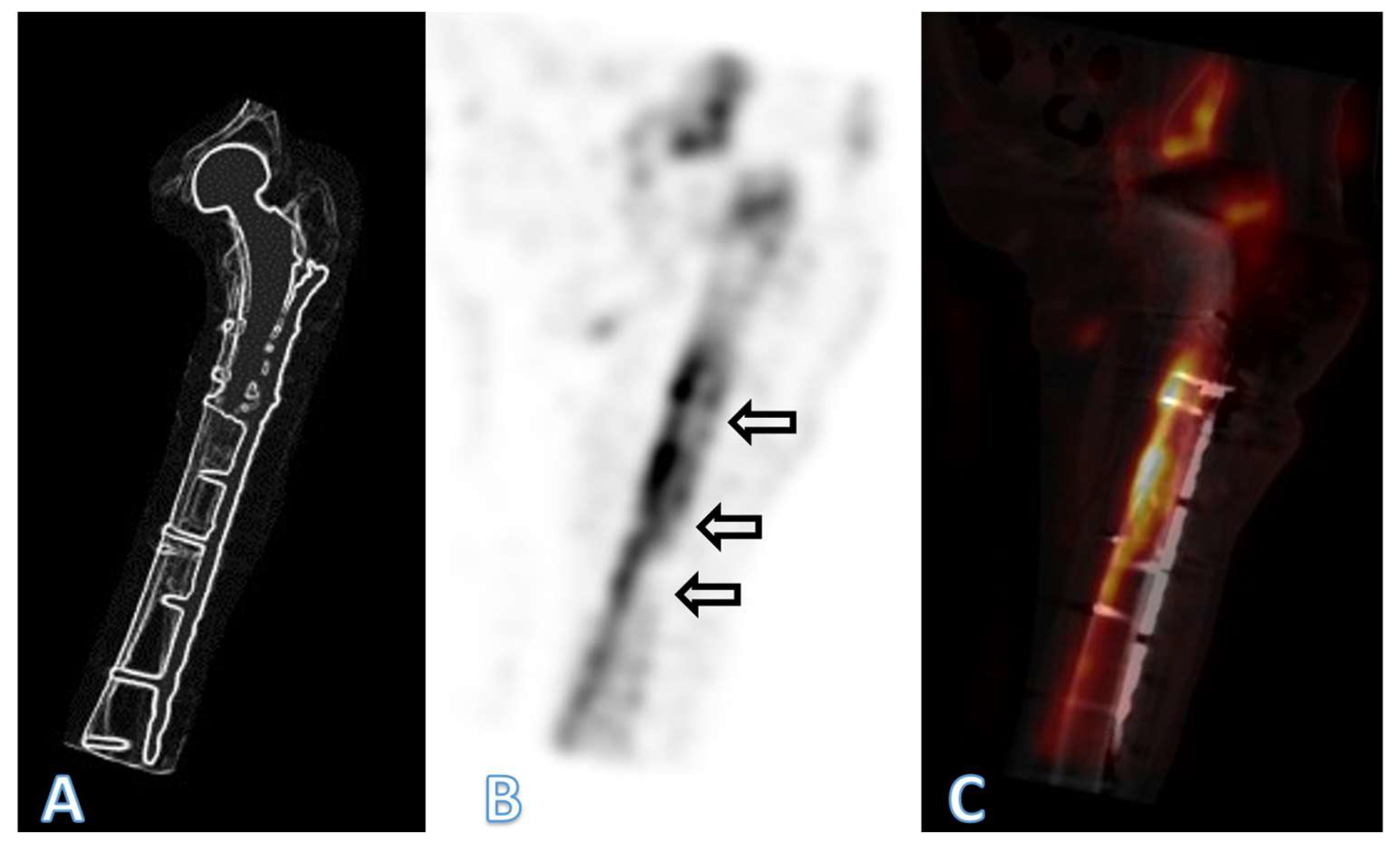
Figure 4.
Axial CT-scan images illustrating the cross-section of the femoral diaphysis of the patient described, at the level of the yellow line in Figure 1. In A, at the time of the periprosthetic fracture. In B, 4 years after internal fixation with a lateral plate. Note general atrophy with thinning out of the cortex. In the area under the plate (arrow), there were areas of necrosis, with no detectable bone metabolism in a SPECT. The quality of the image in B is reduced due to artefacts caused by the implants and due to movement of the patient during the procedure. Only the geometry of the bone may be compared. The apparent density of the bone is affected by differing acquisition protocols as well as due to artefacts induced by the implants, limiting comparison of the density.
Figure 4.
Axial CT-scan images illustrating the cross-section of the femoral diaphysis of the patient described, at the level of the yellow line in Figure 1. In A, at the time of the periprosthetic fracture. In B, 4 years after internal fixation with a lateral plate. Note general atrophy with thinning out of the cortex. In the area under the plate (arrow), there were areas of necrosis, with no detectable bone metabolism in a SPECT. The quality of the image in B is reduced due to artefacts caused by the implants and due to movement of the patient during the procedure. Only the geometry of the bone may be compared. The apparent density of the bone is affected by differing acquisition protocols as well as due to artefacts induced by the implants, limiting comparison of the density.
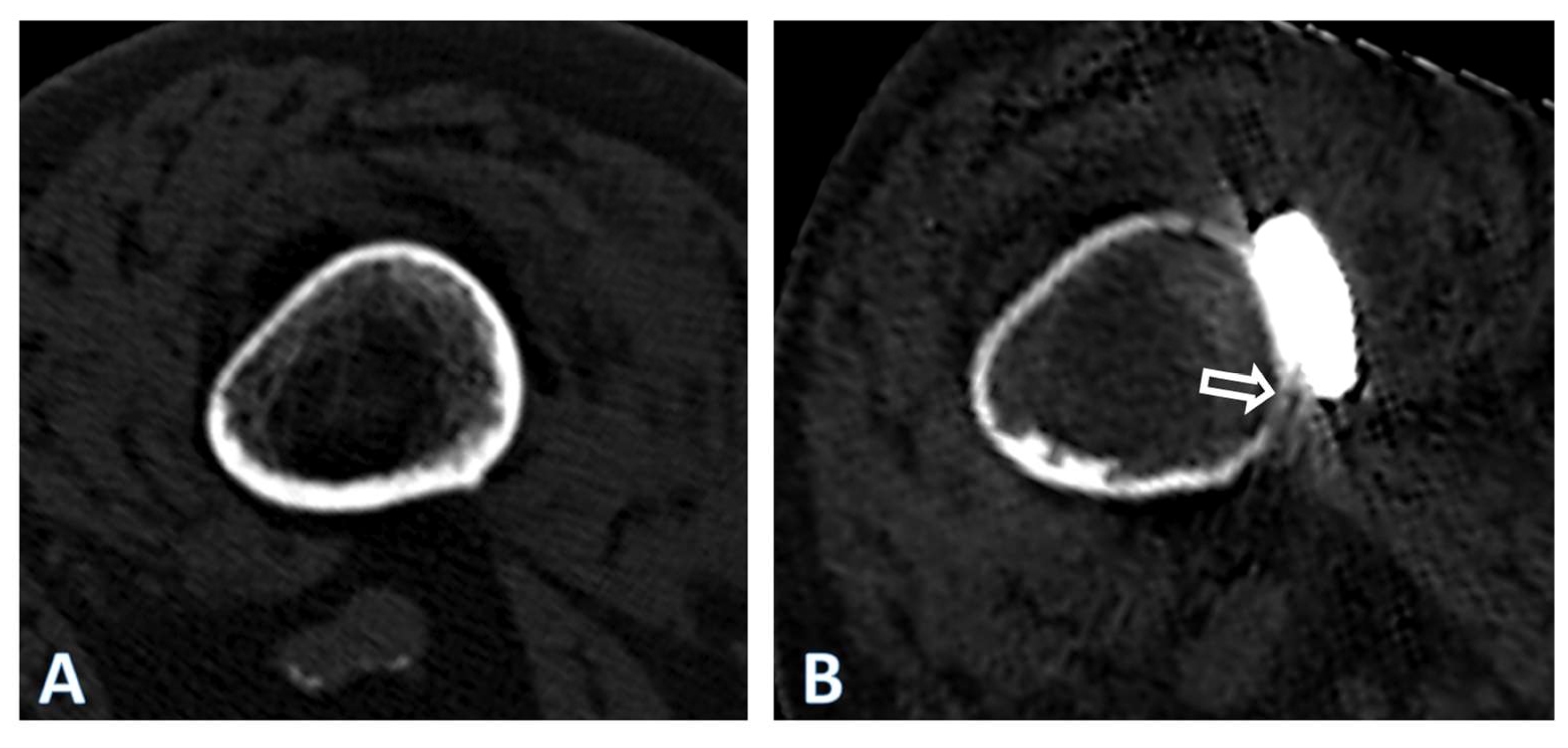
Figure 5.
CT scan images 4 years after fixation of the periprosthetic fracture of the left femur after cemented hemiarthroplasty of the hip in the patient described, illustrating the cross-section at the level of the yellow line in Figure 1, for both the right (A) and the left (B) femur. Note the general atrophy of the bone of the left femur, compare to the thickness of the cortex of the right femur, which may be considered as normal at such age in females, despite immobilization. There nevertheless is a cancellous transformation at the inner cortex of the right femur, typical for endostal resorption, as expected after prolonged unloading, the patient having never regained walking ability.
Figure 5.
CT scan images 4 years after fixation of the periprosthetic fracture of the left femur after cemented hemiarthroplasty of the hip in the patient described, illustrating the cross-section at the level of the yellow line in Figure 1, for both the right (A) and the left (B) femur. Note the general atrophy of the bone of the left femur, compare to the thickness of the cortex of the right femur, which may be considered as normal at such age in females, despite immobilization. There nevertheless is a cancellous transformation at the inner cortex of the right femur, typical for endostal resorption, as expected after prolonged unloading, the patient having never regained walking ability.
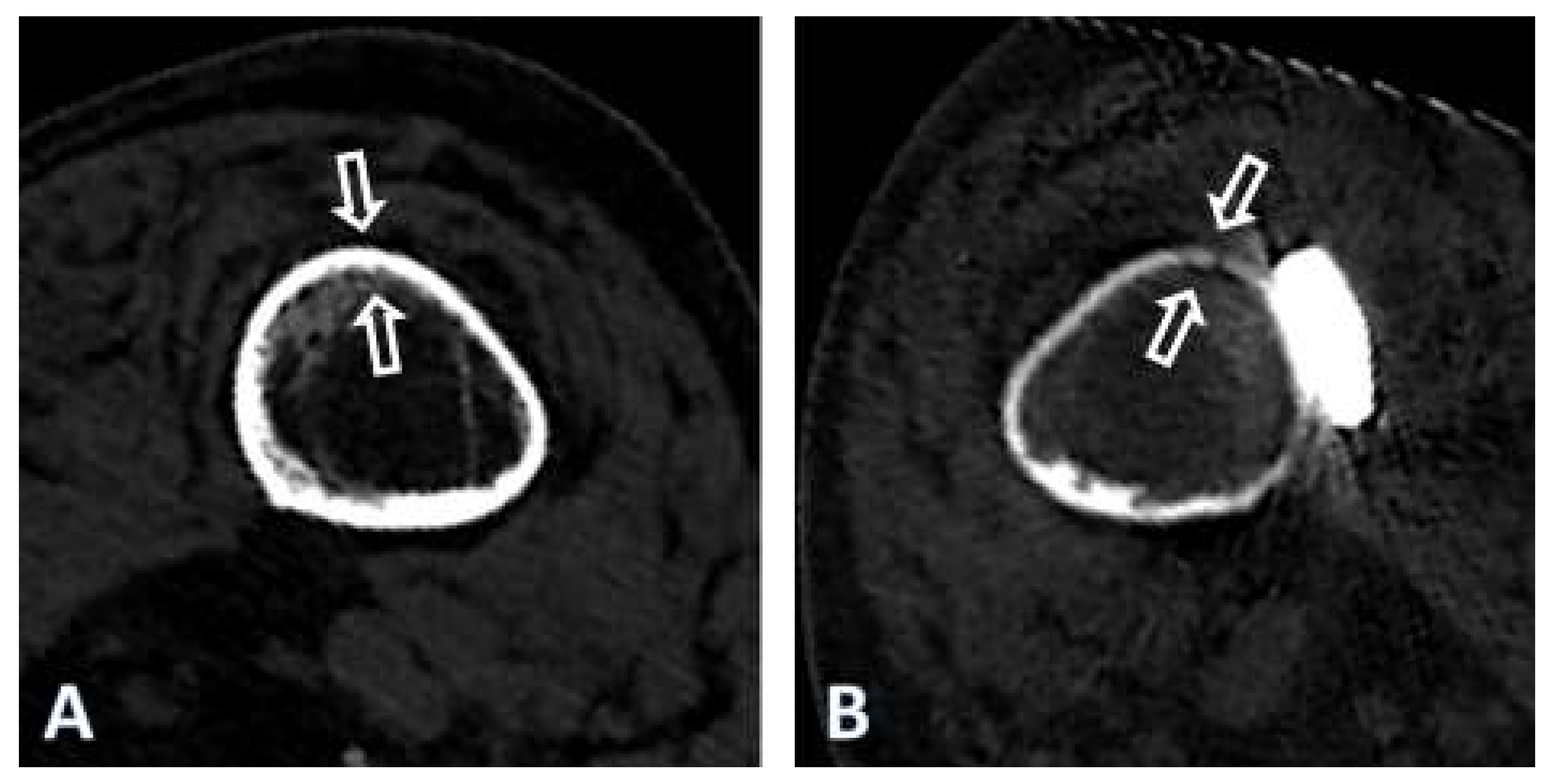
Figure 6.
Results of the 4-point bending test according to ASTM F382-17 of the 4 plates tested. The NCB plate was tested at the approximative level of the tip of the stem of the total hip replacement in the patient described, as this plate is asymmetric with a varying cross-section. As a comparison, a narrow 4.5/5.0 mm LCP made of stainless steel, a broad curved 4.5/5.0 mm LCP made of stainless steel and a broad curved 4.5/5.0 mm LCP made of pure titanium were tested.
Figure 6.
Results of the 4-point bending test according to ASTM F382-17 of the 4 plates tested. The NCB plate was tested at the approximative level of the tip of the stem of the total hip replacement in the patient described, as this plate is asymmetric with a varying cross-section. As a comparison, a narrow 4.5/5.0 mm LCP made of stainless steel, a broad curved 4.5/5.0 mm LCP made of stainless steel and a broad curved 4.5/5.0 mm LCP made of pure titanium were tested.
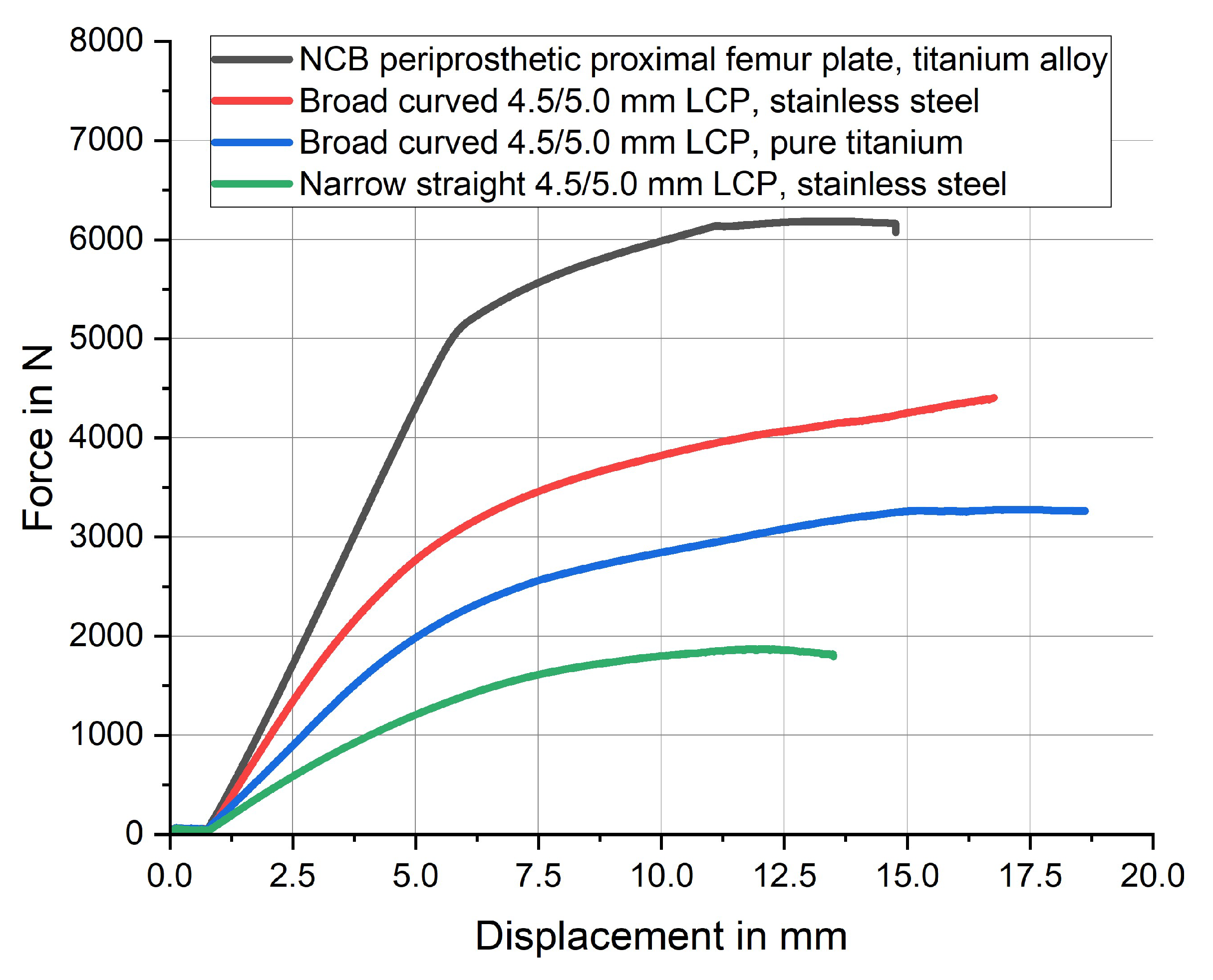
Figure 7.
Undersurface of the NCB periprosthetic proximal femur plate (Zimmer Biomet, Zug, Switzerland) on the left and of a broad curved 4.5/5.0 mm LCP (DePuy Synthes, Oberdorf, Switzerland) on the right. Note that the NCB has no undercuts and has a longitudinal groove, increasing contact with the tubular diaphyseal bone, whereas the LCP has several undercuts to reduce contact of the plate with the underlying bone.
Figure 7.
Undersurface of the NCB periprosthetic proximal femur plate (Zimmer Biomet, Zug, Switzerland) on the left and of a broad curved 4.5/5.0 mm LCP (DePuy Synthes, Oberdorf, Switzerland) on the right. Note that the NCB has no undercuts and has a longitudinal groove, increasing contact with the tubular diaphyseal bone, whereas the LCP has several undercuts to reduce contact of the plate with the underlying bone.
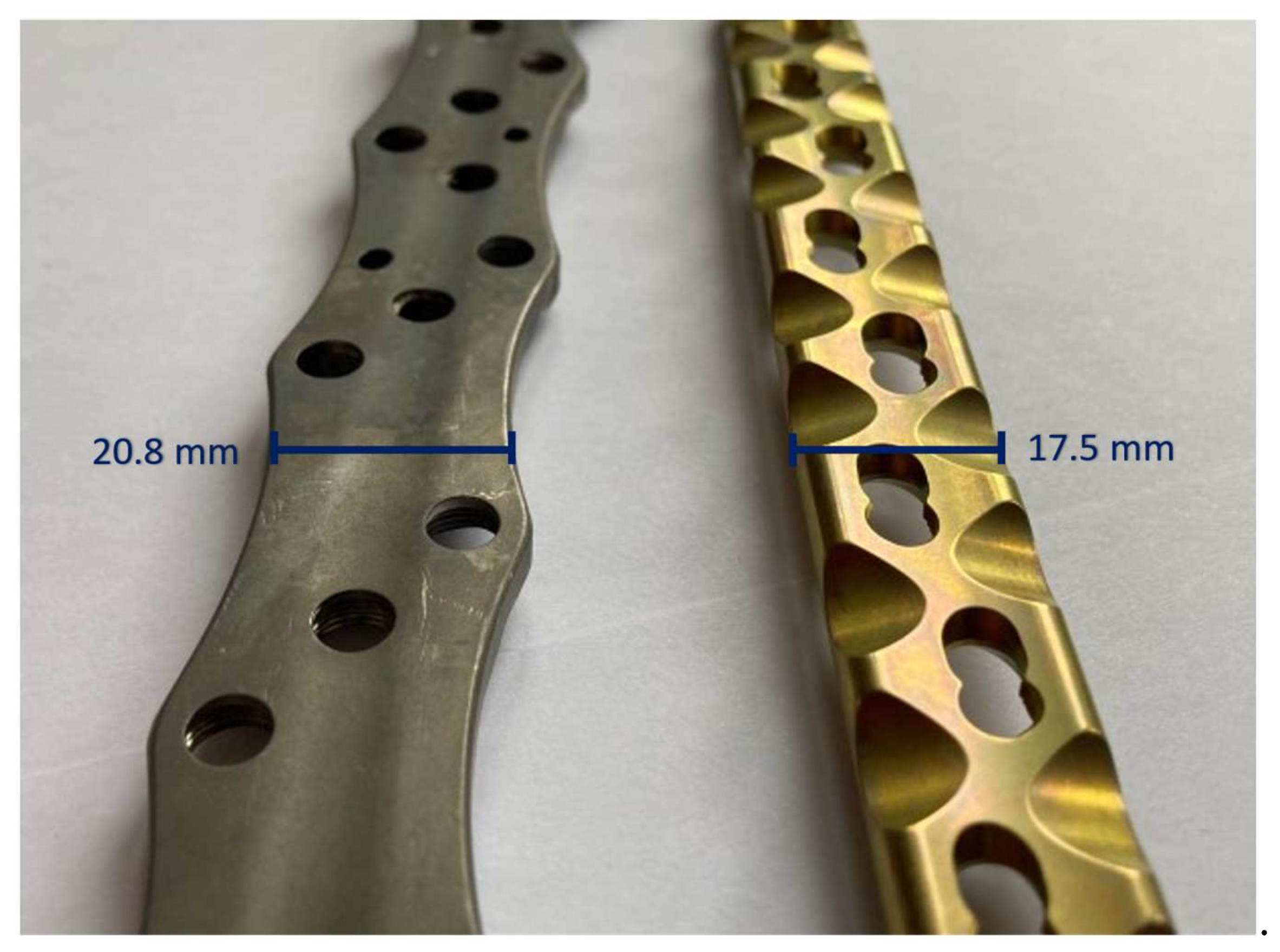

Table 1.
Results of the 4-point bending test according to ASTM F382-17 of the 4 plates tested. The NCB plate was tested at the approximative level of the tip of the stem of the total hip replacement in the patient described, as this plate is asymmetric with a varying cross-section.
Table 1.
Results of the 4-point bending test according to ASTM F382-17 of the 4 plates tested. The NCB plate was tested at the approximative level of the tip of the stem of the total hip replacement in the patient described, as this plate is asymmetric with a varying cross-section.
| Plate type | Material | Bending stiffness | Fmax |
|---|---|---|---|
| NCB periprosthetic proximal femur plate | titanium-aluminum-vanadium alloy | 903.1 [N/mm2] | 6185 [N] |
| 4.5/5.0 mm broad curved LCP | stainless steel | 786.7 [N/mm2] | 4407 [N] |
| 4.5/5.0 mm broad curved LCP | pure titanium | 481.5 [N/mm2] | 3279 [N] |
| 4.5/5.0 mm narrow straight LCP | stainless steel | 327.8 [N/mm2] | 1871 [N] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



