
Submitted:
05 November 2024
Posted:
07 November 2024
You are already at the latest version
Abstract
Background/Objectives: The present study aimed to identify information from health research that used mixed-method data collection, considering the approach of face-to-face interviews and telephone interviews (MMFT), with a more specific focus on identifying its themes, objectives, designs, populations involved and implementation process. Methods: A scoping review was developed, with systematic searches applied in March 2024, in five databases (Pubmed; Scielo; Scopus and Web of Science), Google Scholar and reference lists. The inclusion criteria were based on the strategy "Participants" (observational epidemiological studies, with no restrictions as to where they were carried out, sampling technique or sample profile); "Concept” (use of MMFT in data collection) and “Context” (studies carried out in the health area, with no restrictions on the theme/subject). The review process was conducted by three researchers who worked independently. Results: from the initial 1,515 potential references, the synthesis of this review was composed of data from seven original studies, highlighting: cross-sectional design, involvement of adults and/or elderly people without specific health conditions, variability between data collection strategies and complementary use of online approaches. Conclusions: based on the evidence generated, it is recommended that future studies assess aspects of the MMFT approach in terms of response rate, cost reduction and increasing the speed with which health surveys are carried out.
Keywords:
Data Collection
; Interviews as Topic
; Telephone
; Health Surveys
; Review
1. Introduction
Data collection is an essential process in a scientific study, as it generates the data that will validate it. Among the biases related to it, we can mention “non-response” [1] and “non-coverage” [2], which, respectively, refer to the non-participation of the people selected in the sampling process (e.g., due to refusal, or even some type of inability to participate in the study) and the non-involvement of certain audiences in the sample, generally due to lack of access and opportunity to participate in the study.
Previous surveys suggest that non-respondents or those with incomplete data have poorer socioeconomic and health conditions compared to respondents [1,3]. Furthermore, excluding people who do not have a telephone line in face-to-face surveys can distort the results, since it does not include profiles that are more vulnerable [4].
Recognizing that data obtained from health surveys can vary depending on the data collection method [5], there is a need to adopt strategies that facilitate the participation of all people selected in the sampling process. Thus, the importance of using different approaches emerges in order to expand the opportunities for participation of people selected in the sampling process. This strategy is called ‘mixed mode data collection’ and one of the potential possibilities involves the use of face-to-face interviews and telephone interviews (MMFT) [6].
Even though the ways in which telephones are used have expanded since mobile telephony and the commercialization of smartphones, the prospect of complementarity of the MMFT approach can, as mentioned above, facilitate the research team's access to people, reduce costs and make it possible to obtain a more realistic (or less biased) estimate of the situation of interest.
Therefore, in order to identify the characteristics, strategies and strengthen decision-making for an original project, the present study was aimed to identify information from health research that used MMFT, with a more specific focus on identifying its themes, objectives, designs, populations involved and implementation process.
2. Materials and Methods
2.1. Design
This study is part of a larger study, entitled “Health Survey of Sao Paulo: Physical Activity and Environment” (“Inquérito de Saúde de São Paulo-ISA: Atividade Física e Ambiente” in Brazilian Portuguese) [7].
In order to identify previous experiences and thus support the strategic options adopted for the original study of the project, a scoping review was developed, based on the references: JBI Manual for Evidence Synthesis [8], PRISMA Extension for Scoping Reviews (PRISMA-ScR) [9], Tricco et al. [10] and Munn et al. [11]. The protocol was previously registered on the Open Science Framework platform (https://doi.org/10.17605/OSF.IO/7TBXD).
2.2. Inclusion Criteria
Based on the “Participants, Concept and Context” framework, the inclusion criteria were drawn up:
- “Participants”: observational epidemiological studies (e.g. cross-sectional, case-control and cohort studies), with no restrictions as to where they were carried out, sampling technique or sample profile. Observing the descriptive nature of the review, it was established that research protocols would also be accepted;
- “Concept”: use of mixed methods for data collection, necessarily involving face-to-face approaches and telephone calls and;
- “Context”: studies carried out in the health area, with no restrictions on the theme/subject.
There were no restrictions on the date of publication or the use of other data collection methods (e.g. online forms), as long as the study included face-to-face approaches and telephone calls. On the other hand, the eligibility criteria included only studies published in English, Portuguese and Spanish, and disseminated in peer-reviewed journals.
2.3. Identification of Potential Studies
Potential studies were searched for using three strategies: (I) systematic searches in four databases (Pubmed; Scielo; Scopus and Web of Science), (II) searches in Google Scholar, considering the records of the first 10 pages and (III) manual searches in the reference lists of the articles selected for full-text assessment. More specifically regarding the work on the databases, the searches were conducted on 26/03/2024, using as a reference the strategy developed for Pubmed: (((mixed mode[Text Word]) OR (multi mode[Text Word])) OR (mixing modes[Text Word])) AND (((telephone[Text Word]) OR (phone[Text Word])) OR (call*[Text Word])).
2.4. Study Selection Process
The review was conducted by three researchers (AF, LS and PG), who worked independently throughout the process. PG designed and applied the systematic searches in the electronic databases and Google Scholar. LS and PG were responsible for identifying and removing duplicates, assessing titles, abstracts and full texts and extracting data. AF participated as a third reviewer in the titles, abstracts and full texts assessment and data extraction, in order to resolve any doubts and establish consensus.
Data extraction was conducted based on other experiences of the working group members, in an electronic spreadsheet involving descriptive data (e.g. study name/acronym, objective, subject, country and year of collection) and methodological data from the included studies (e.g. sample size; gender; age group; sample characteristics; design; study context; implementation and other strategies used in data collection).
Given the more descriptive focus on MMFT populations, methods and approaches, from the very beginning of the research there was no intention to present and/or discuss results. AF, LS and PG worked together to refine the data in the extraction spreadsheet and draw up the descriptive summary. The refinement and visualization of the descriptive synthesis was done by all the authors of this manuscript (AF, DU, LS and PG).
3. Results
After removing 384 duplicates, 1,131 potential articles were assessed by their titles and abstracts. Of these, 28 remained in the selection process and, with the addition of five articles from the complementary searches, 33 were assessed for their full texts. With the exclusion of 25, the most frequent reasons being “design” (n = 5) and “not having a face-to-face approach” (n = 5), eight articles, containing data from seven original studies, were forwarded to the descriptive synthesis (Figure 1) [12,13,14,15,16,17,18,19].
More specifically, the synthesis contains data from five complete studies [12,13,14,15,16,17] and two protocols [18,19] (Table 1). There was great variation among the topics covered, with the “health of immigrants” line standing out (n = 2) [14,18]; the countries where the research was carried out and, also, in relation to the years in which the collections were carried out, between 1986-1992 [13] and 2021-2022 [17].
Regarding the profile of the samples, there was a higher frequency of studies aimed at the general population (n = 6; 85.7%) [12,13,14,15,16,18,19]. However, in the ethnic-racial aspect, in addition to the concern for the health of migrants, it is also worth mentioning the inclusion of two studies involving African Americans [12,13]. By design, there was a predominance of cross-sectional studies (n = 6; 85.7%) [12,14,15,16,17,18,19], conducted in community contexts (n = 5; 71.4%) [12,13,15,16,18,19] (Table 2).
Also in Table 2, in relation to the implementation of the MMFT, the strategies indicated different paths, from the use of the telephone as an initial screening, to later face-to-face interviews (n = 1; 14.3%) [12]; the use of face-to-face interviews and telephone calls, according to the geographical accessibility of the districts (n = 1; 14.3%) [15,16]; the choice of one of the techniques according to the availability of people (n = 1; 14.3%) [17] and the feasibility of face-to-face or telephone calls in cases for people who did not answer the self-completion questionnaire [18]. In three studies (42.9%), the implementation of online strategies for data collection (interview or self-completion questionnaire) was also observed [17,18,19].
4. Discussion
In order to map the information from health surveys that used the MMFT approach in their data collection, the synthesis of this review was composed of data from seven original studies, highlighting: cross-sectional design, involvement of adults and/or elderly people without specific health conditions, variability between data collection strategies and complementary use of online approaches.
Given the more specific interest in health surveys, since the planning of the review it was expected that the descriptive synthesis would be composed mostly – or even entirely – of cross-sectional studies. It was also expected that a greater number of studies conducted in community settings than in clinical or hospital settings.
As mentioned, this review was designed on the assumption that the MMFT approach is more potential than implementing them separately, in different aspects, justifying the non-inclusion of studies that compare different techniques. It is worth noting that the literature suggests differences between the approaches in terms of motivating interviewees to provide an accurate answer, reducing the difficulty of the task [20] and, among the elderly, in terms of memory performance [21].
In addition to these issues, the indication of the MMFT approach can also be justified by the increased feasibility of data collection, in the sense of facilitating access, or even avoiding losses / dropouts in situations where there is difficulty in dialogue, as in the study by Garrett et al, which mostly involved people with no English proficiency. Perhaps these issues also justify the use of the MMFT approach in studies focused on the health of immigrants [14,18] and the health of the black population [12,13], considering that these groups are generally situated in greater contexts of vulnerability [22] and inequality of access to health services [23].
However, it is worth noting that the MMFT is not restricted to research conducted among people in vulnerable situations. In the study by Rada et al., for example, telephone collection was carried out to reach people who lived in a higher-income district, characterized by gated and guarded housing, which differentiated it from the characteristics of the other three districts chosen for the research, made up of blocks of houses and buildings, more easily accessible, where data collection took place face-to-face.
With regard to the operationalization of data collection, the results showed great variability, with examples being the periodic alternation between approaches [13], the choice of approach according to people's availability [17], and the adoption of the telephone approach as initial screening, for later operationalization of the face-to-face approach [12,14]. Given that each option was chosen on the basis of particularities such as identity, geographical or territorial aspects, or the resources and infrastructure available to the research teams, it can be assumed that contextual factors led to this heterogeneity.
The additional use of online strategies was one of the points that caught our attention among the studies included [17,18,19]. With the consolidation of digital technologies, the application of online questionnaires has become a possibility for reaching more people, reducing costs [24], highlighting the existence of large-scale health surveys conducted using online data collection [25,26,27].
However, recognizing that each form of data collection administration has its own particularities, it is important to be cautious about the impossibility of describing the sample and the bias of the answers [28], since respondents can pass the instrument on to people with similar conditions to prepare other answers. When designing data collection based on a probabilistic sample, it is necessary to ensure that the online instruments are sent to and answered by people who have actually been selected for the survey.
Recognizing the state of the art among studies that have used the MMFT approach for data collection allows us to share suggestions for future studies. One of the points to be taken forward is a more detailed analysis of the success rates between the face-to-face and telephone approaches, since, among the completed studies, little has been discussed about the prerogatives and the extent to which the MMFT approach managed to reach the total number of people initially drawn for the study, in order to control non-response and non-coverage biases. This is a debate that seems important to us, given the indication that the effects of non-response bias are intensified when response rates are lower than 70% [29].
Even so, it is worth recommending the MMFT approach for data collection in future health surveys, not just for more specific populations. The complementarity between the approaches allows for faster, cheaper and more comprehensive data collection, as long as the implementation of data collection is based on recognizing the contextual conditions that permeate the study (e.g. territories, infrastructures and access to the target population). In addition, we hypothesize that longitudinal studies can also use the MMFT approach to collect data over the course of follow-up, avoiding losses and dropouts.
The main limitation is the small number of studies in the synthesis, particularly complete studies, which, if there were more of them, would allow for a more in-depth discussion of the aspects mentioned and greater exploration of the data. On the other hand, the study's potential lies in its focus on the complexity of the MMFT approach, in order to present the themes, contexts, populations and the ways in which they can be operationalized in health surveys.
5. Conclusions
In conclusion, the main characteristics of the studies that used the MMFT approach for data collection are: cross-sectional design, involvement of adults and/or elderly people without specific health conditions, variability between data collection strategies and complementary use of online approaches. It is recommended that future studies assess aspects of the MMFT approach in terms of response rate, cost reduction and increasing the speed with which health surveys are carried out
Author Contributions
Conceptualization (AF and PG); Methodology (AF, DU, LS and PG); Validation (AF, DU, LS and PG); Formal analysis (AF, DU, LS and PG); Investigation (AF, LS and PG); Resources (AF, DU, LS and PG); Data curation (AF, DU, LS and PG); Writing—original draft preparation (PG); writing—review and editing (AF, DU and LS) Visualization (AF, DU, LS and PG); Supervision (AF, and PG); Project administration (AF and PG). All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Data Availability Statement
Not applicable
Acknowledgments
Not applicable
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Cheung, K.L.; Ten Klooster, P.M.; Smit, C.; de Vries, H.; Pieterse, M.E. The impact of non-response bias due to sampling in public health studies: A comparison of voluntary versus mandatory recruitment in a Dutch national survey on adolescent health. BMC Public Health. 2017, 17, 276. [Google Scholar] [CrossRef] [PubMed]
- Eckman, S.; Kreuter, F. ; Undercoverage Rates and Undercoverage Bias in Traditional Housing Unit Listing. Sociol. Methods Res. 2013, 42, 264–293. [Google Scholar] [CrossRef]
- Tolonen, H.; Dobson, A.; Kulathinal, S.; WHO MONICA Project. Effect on trend estimates of the difference between survey respondents and non-respondents: results from 27 populations in the WHO MONICA Project. Eur. J. Epidemiol. 2005, 20, 887–98. [Google Scholar] [CrossRef] [PubMed]
- Segri, N.J.; Cesar, C.L.; Barros, M.B.; Alves, M.C.; Carandina, L.; Goldbaum, M. Health survey: comparison of interviewees according to ownership of a residential telephone line. Rev. Saude. Publica. 2010, 44, 503–512. [Google Scholar] [CrossRef]
- Hoebel, J.; von der Lippe, E.; Lange, C.; Ziese, T. Mode differences in a mixed-mode health interview survey among adults. Arch. Public Health. 2014, 72, 46. [Google Scholar] [CrossRef]
- Herman, J.B. Mixed-mode data collection: Telephone and personal interviewing. J. Appl. Psychol. 1977, 62, 399–404. [Google Scholar] [CrossRef]
- Florindo, A.A.; Teixeira, I.P.; Barrozo, L.V.; Sarti, F.M.; Fisberg, R.M.; Andrade, D.R.; Garcia, L.M.T. Study protocol: health survey of Sao Paulo: ISA-Physical Activity and Environment. BMC Public Health. 2021, 21, 283. [Google Scholar] [CrossRef]
- Aromataris, E.; Lockwood, C.; Porritt, K.; Pilla, B.; Jordan, Z. editors. JBI Manual for Evidence Synthesis. JBI; Available from: https://synthesismanual.jbi.global. https://doi.org/10.46658/JBIMES-24-01. [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O'Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O'Brien, K.; Colquhoun, H.; Kastner, M.; Levac, D.; Ng, C.; Sharpe, J.P.; Wilson, K.; et al. A scoping review on the conduct and reporting of scoping reviews. BMC Med. Res. Methodol. 2016, 16, 15. [Google Scholar] [CrossRef]
- Munn, Z.; Peters, M.D.J.; Stern, C.; Tufanaru, C.; McArthur, A.; Aromataris, E. Systematic review or scoping review? Guidance for authors when choosing between a systematic or scoping review approach. BMC Med. Res. Methodol. 2018, 18, 143. [Google Scholar] [CrossRef]
- Chadiha, L.A.; Morrow-Howell, N.; Proctor, E.K.; Picot, S.J.; Gillespie, D.C.; Pandey, P.; Dey, A. Involving rural, older African Americans and their female informal caregivers in research. J. Aging Health. 2004, 16 (5 Suppl), 18S–38S. [Google Scholar] [CrossRef]
- Kelley-Moore, J.A. Assessing racial health inequality in older adulthood: comparisons from mixed-mode panel interviews. J. Gerontol. B. Psychol. Sci. Soc. Sci. 2006, 61, S212–S220. [Google Scholar] [CrossRef] [PubMed]
- Garrett, P.W.; Forero, R.; Dickson, H.G.; Klinken Whelan, A. How are language barriers bridged in acute hospital care? The tale of two methods of data collection. Aust. Health Rev. 2008, 32, 755–764. [Google Scholar] [CrossRef] [PubMed]
- Rada, V.D.; Gomez, J.L.P. Comparación de las tasas de respuesta en el uso combinado de modalidades de encuesta. Rev. Esp. Investig. Sociol. 2013, 141, 159–170. [Google Scholar] [CrossRef]
- Rada, V.D. Complementación entre encuestas presenciales y telefónicas. Pol. Soc. 2014, 51, 201–226. [Google Scholar] [CrossRef]
- Wang, Y.; Huang, Y.; Ma, X.; Wusiman, D.; Zhang, X.; Bi, N. The impact of the COVID-19 pandemic on palliative care practice: A survey of clinical oncologists. Front. Public Health. 2022, 10, 1020937. [Google Scholar] [CrossRef]
- Koschollek, C.; Zeisler, M.L.; Houben, R.A.; Geerlings, J.; Kajikhina, K.; Bug, M.; Blume, M.; Hoffmann, R.; Hintze, M.; Kuhnert, R.; et al. German Health Update Fokus (GEDA Fokus) among Residents with Croatian, Italian, Polish, Syrian, or Turkish Citizenship in Germany: Protocol for a Multilingual Mixed-Mode Interview Survey. JMIR Res. Protoc. 2023, 12, e43503. [Google Scholar] [CrossRef]
- Lewis, T.P.; Kapoor, N.R.; Aryal, A.; Bazua-Lobato, R.; Carai, S.; Clarke-Deelder, E.; Croke, K.; Dayalu, R.; Espinoza-Pajuelo, L.; Fink, G. Measuring people's views on health system performance: Design and development of the People's Voice Survey. PLoS Med. 2023, 20, e1004294. [Google Scholar] [CrossRef]
- Hope, S.; Campanelli, P.; Nicolaas, G.; Lynn, P.; Jäckle, A. The role of the interviewer in producing mode effects: results from a mixed modes experiment comparing face-to-face, telephone and web administration. Survey Research Methods. 2022, 16, 207–226. [Google Scholar] [CrossRef]
- Smith, J.R.; Gibbons, L.E.; Crane, P.K.; Mungas, D.M.; Glymour, M.M.; Manly, J.J.; Zahodne, L.B.; Rose Mayeda, E.; Jones, R.N.; Gross, A.L. Shifting of Cognitive Assessments Between Face-to-Face and Telephone Administration: Measurement Considerations. J. Gerontol. B. Psychol. Sci. Soc. Sci. 2023, 78, 191–200. [Google Scholar] [CrossRef]
- Castañeda, H.; Holmes, S.M.; Madrigal, D.S.; Young, M.E; Beyeler, N.; Quesada, J. Immigration as a social determinant of health. Annu. Rev. Public Health. 2015, 36, 375–392. [Google Scholar] [CrossRef] [PubMed]
- Lebano, A.; Hamed, S.; Bradby, H.; Gil-Salmerón, A.; Durá-Ferrandis, E.; Garcés-Ferrer, J.; Azzedine, F.; Riza, E.; Karnaki, P.; Zota, D.; Linos, A. Migrants' and refugees' health status and healthcare in Europe: a scoping literature review. BMC Public Health. 2020, 20, 1039. [Google Scholar] [CrossRef] [PubMed]
- Van Selm, M.; Jankowski, N.W. Conducting Online Surveys. Qual. Quant. 2006, 40, 435–456. [Google Scholar] [CrossRef]
- Hall, R.; Taylor, J.; Heathcote, C.; Langton, T.; Hewitt, C.E.; Fraser, L. Gender services for children and adolescents across the EU-15+ countries: an online survey. Arch. Dis. Child. 2024, Apr 9, archdischild-2023-326348. [CrossRef]
- Lee, S.W.; Clement, N.; Tang, N.; Atiomo, W. The current provision of community-based teaching in UK medical schools: an online survey and systematic review. BMJ Open. 2014, 4, e005696. [Google Scholar] [CrossRef]
- Armour, M.; Lawson, K.; Wood, A.; Smith, C.A.; Abbott, J. The cost of illness and economic burden of endometriosis and chronic pelvic pain in Australia: A national online survey. PLoS One. 2019, 14, e0223316. [Google Scholar] [CrossRef]
- Andrade, C. The Limitations of Online Surveys. Indian J. Psychol. Med. 2020, 42, 575–576. [Google Scholar] [CrossRef]
- Prince, M. 9 – Epidemiology. Editor(s): Pádraig Wright, Julian Stern, Michael Phelan, Core Psychiatry (Third Edition), W.B. Saunders, 2012, Pages 115-129, ISBN 9780702033971. [CrossRef]
Figure 1.
Flowchart of Scoping Review.
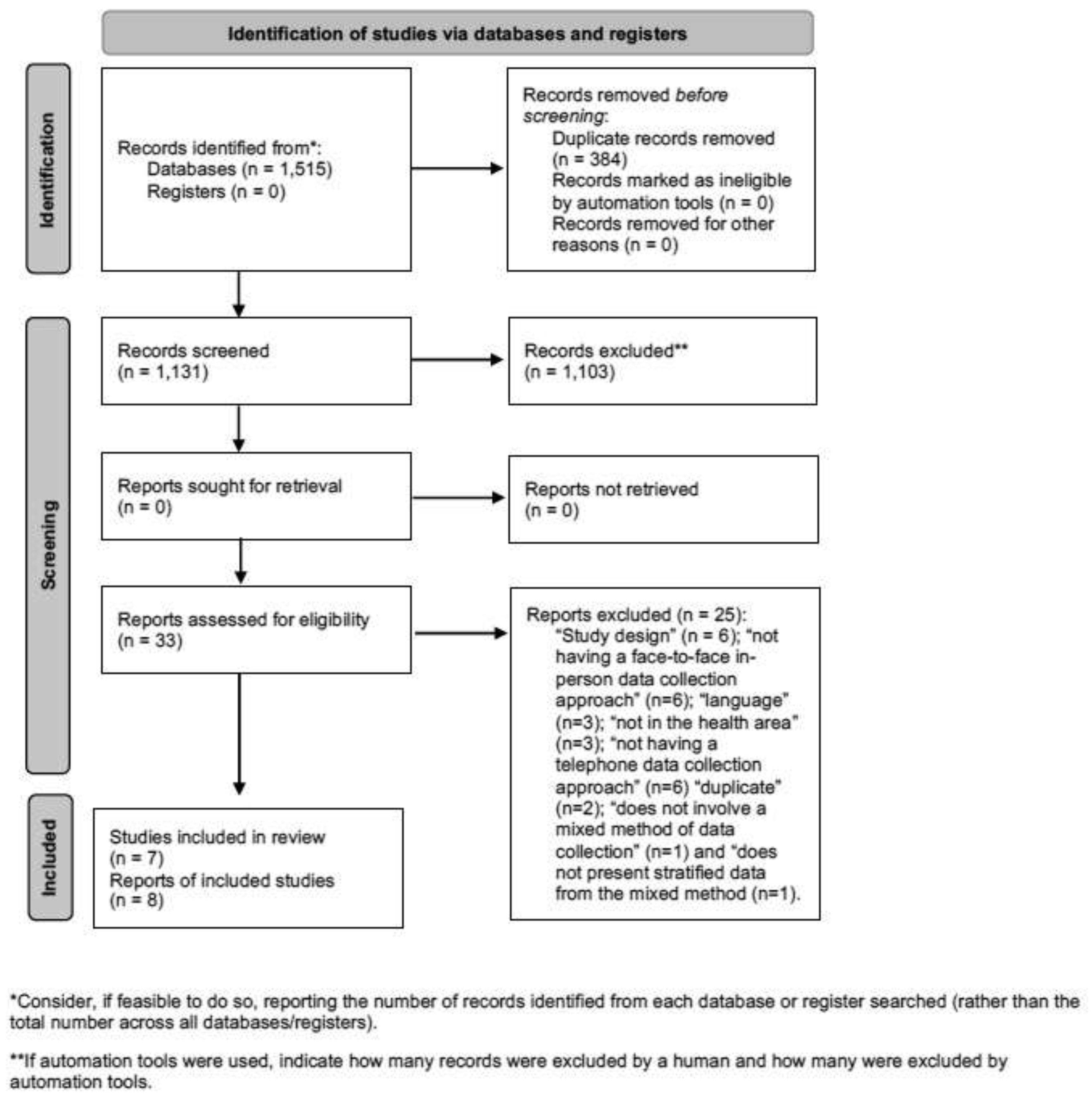

Table 1.
Descriptive information of included studies (n = 7).
| Reference | Study Name | Objective | Topic | Country | Year of data collection |
|---|---|---|---|---|---|
| Complete studies (n = 5) | |||||
| Chadiha et al., 2004 [12] | Health Care Financing Administration – HCFA | Presents the methodology, procedures, and results for involving rural, older African Americans and recruiting their female informal caregivers for a well-being and service use study | Healthcare | United States of America | 2000–2001 |
| Kelley-Moore, 2006 [13] | Established Populations for Epidemiologic Studies of the Elderly | To systematically compare responses from Black and White older adults in telephone and face-to-face interviews in order to determine whether estimates of racial health inequality vary by survey interview mode. | Health inequities | United States of America | 1986–1992 |
| Garrett et al., 2008 [14] | nd | To explore language service provision in a pilot hospital study with two methods of data collection | Immigrant health | Australia | 2004 |
| Rada, 2014; Rada et al., 2024 [15,16] | nd | To present the results of a research that uses face-to-face and telephone surveys together | Physical activity and Sports | Spain | nd |
| Wang et al., 2022 [17] | nd | To explore the current status of palliative care practice for cancer and the influence of COVID-19, from the perspective of oncologists | Palliative care | China | 2021–2022 |
| Study protocols (n = 2) | |||||
| Koschollek et al., 2023 [18] | German Health Update Fokus – GEDA Fokus | To collect comprehensive data on the health status and social, migration-related, and structural factors among people with selected citizenships to enable differentiated explanations of the associations between migration-related aspects and their impact on migrant health. | Immigrant health | Germany | – |
| Lewis et al., 2023 [19] | People’s Voice Survey – PVS | The PVS is a rapid population-representative survey that aims to inform action toward more effective and people-centered health systems and promote health system accountability to populations | Health systems assessment | Low and middle income countries | – |
| Legends: nd: not described | |||||
Table 2.
Methodological information of the included studies (n = 7).
| Reference | Sample size | Gender | Age Range | Sample characteristics | Study design | Study setting | Implementation | Other strategies | |
|---|---|---|---|---|---|---|---|---|---|
| Complete studies (n = 5) | |||||||||
| Chadiha et al., 2004 [12] | 1,547 | Both | Older adults | Rural African Americans and their informal caregivers (women) | Cross-sectional | Community | Telephone interview for initial screening (to see if you meet eligibility criteria) and, subsequently, face-to-face interview | – | |
| Kelley-Moore, 2006 [13] | 2,387 | Both | Older adults | Higher frequency of African Americans | Cohort | Community | Seven annual interviews (1986–1992): Interviews 1, 4, and 7 were face-to-face residential interviews and the remainder were by telephone | – | |
| Garrett et al., 2008 [14] | 258 | Both | Older adults | Most were not proficient in the English language | Cross-sectional | Hospital | Telephone interview (7–14 days after hospital discharge) and review of medical records | – | |
| Rada, 2014; Rada et al., 2024 [15,16] | 600 | Both | Adolescents, Adults and Older adults | Majority of men, aged 35 or under | Cross-sectional | Community | Face-to-face interview in three districts and by telephone in one district, considering social and geographical characteristics. | – | |
| Wang et al., 2022 [17] | 37 | Both | Adults | Professionals involved in palliative cancer treatment (mostly men, doctors, who work in urban contexts) | Cross-sectional | Hospital | Interviews could be in person, online or by telephone, depending on people's availability. | Online interview | |
| Study protocols (n = 2) | |||||||||
| Koschollek et al., 2023 [18] | 33,436 | Both | Adults and Older adults | Immigrants residing in Germany (e.g., Croatian, Italian, Polish, Syrian, or Turkish) | Cross-sectional | Community | Face-to-face and/or telephone interviews as an alternative for people who did not respond to the self-completion questionnaire (online or on paper) | Self-completion questionnaire online and on paper | |
| Lewis et al., 2023 [19] | ND | Both | Adults and Older adults | People from low and middle income countries, preferably | Cross-sectional | Community | Interviews preferably conducted by telephone. Implementation can be supplemented by face-to-face interviews, or by online interviews. | Online interview | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



