Submitted:
13 November 2024
Posted:
15 November 2024
You are already at the latest version
Abstract
Background: The prognostic significance of achieving an axillary pathologic complete response (AxpCR) following neoadjuvant chemotherapy (NAT) in clinically node-positive (cN+) breast cancer (BC) is well established; however, there is currently no consensus regarding the optimal strategy for axillary management, particularly in patients with HER2-positive BC. This study, which seeks to assess the utility of the maximum standardized uptake value of axillary lymph nodes (N-SUVmax) obtained from baseline 18F-FDG PET/CT scans, in conjunction with the absolute monocyte count (AMC), as predictors of AxpCR to NAT in patients with cN+ HER2-positive BC, promises to bring significant benefits to the field of breast cancer treatment. Methods: The clinical, pathological, and imaging data of HER2-positive BC patients with cN+, who were eligible for NAT at the time of diagnosis, were analyzed retrospectively. Individual receiver operating characteristic curves were employed to establish the optimal cut-off values for both baseline N-SUVmax and AMC. Results: Involving 117 patients diagnosed with HER2+BC, 86 initially presented with cN+ disease. Among this group, 56 patients, representing 66.3%, achieved AxpCR following NAT. Patients with an N-SUVmax of 3.5 or higher exhibited a 4.6-fold increased probability of achieving AxpCR (p=0.039, odds ratio [OR]=4.638 [1.081; 1.904]). Conversely, those with an AMC exceeding 340/mm³ experienced a 90.4% decrease in the likelihood of achieving AxpCR (p<0.001, OR=0.096 [0.028; 0.324]). The interaction between N-SUVmax and AMC was thoroughly investigated, revealing that an increase in AMC mitigated the significance of N-SUVmax on the probability of attaining AxpCR after treatment (p=0.006, OR=0.999 [0.997; 1.000]). Patients were categorized into three groups based on their N-SUVmax and AMC levels: 1. High N-SUVmax – Low AMC group (Group 1, n=38) 2. High N-SUVmax – High AMC group or Low N-SUVmax – Low AMC group (Group 2, n=37) 3. Low N-SUVmax – High AMC group (Group 3, n=11) Individuals in Group 2 (p<0.001; OR=0.047 [0.009; 0.237]) and those in Group 3 (p<0.001, OR=0.017 [0.002; 0.137]) demonstrated a significantly lower probability of achieving AxpCR following NAT compared to patients in Group 1. Conclusions: Evaluating axillary treatment response in the neoadjuvant setting presents a valuable opportunity for HER2-positive breast cancer patients. By combining baseline N-SUVmax and AMC, clinicians can enhance their ability to determine the most appropriate axillary surgical approach for each patient, paving the way for enhanced treatment outcomes.
Keywords:
Axillary treatment
; Neoadjuvant chemotherapy
; HER2 positive
; 18F-FDG
; PET/CT
; SUVmax
; absolute monocyte count
1. Introduction
Breast cancer (BC) is the most frequently diagnosed cancer and the leading cause of cancer-related mortality in women worldwide [1]. Less-invasive surgical procedures for BC are currently a widely discussed and important subject within the medical community and beyond [2]. Neoadjuvant therapy (NAT) is increasingly used for patients with locally advanced BC, regardless of subtype, or with initial BC with unfavorable tumor characteristics and/or axillary lymph node metastases. NAT can reduce the axillary disease burden, allowing for less invasive axillary surgery [3]. The cancer subtype influences the response of the axilla to NAT. Patients with human epidermal growth factor receptor 2 (HER2)-positive and triple-negative BC have a heightened chance of achieving axillary pathologic complete response (AxpCR) compared to those with estrogen receptor (ER)-positive BC [4]. Multiple meta-analyses consistently emphasize the substantial impact of achieving an AxpCR following NAT, influencing outcome and prognosis [5,6,7]. The discussion surrounding the management of axillary lymph nodes in the context of NAT has ignited intense debate in recent years. Achieving an AxpCR potentially eliminates the need for conventional axillary lymph node dissection (ALND) [8]. While sentinel lymph node biopsy (SLNB) is generally accepted as an axillary staging procedure after NAT for patients with no clinical evidence of lymph node involvement (cN0), the optimal surgical approach for patients with histologically confirmed lymph node involvement (pN+) before NAT but with no clinical evidence of lymph node involvement (ycN0) after that, remains a subject of ongoing discussion [9,10].
Positron emission tomography/computed tomography (PET/CT) using 2-[18F] Fluoro-2-deoxy-D-glucose (18F-FDG) is crucial for staging patients with locally advanced or recurrent BC [11]. Several studies have suggested that axillary lymph node metastases with elevated baseline glycolytic activity, thus increased 18F-FDG uptake as indicated by standardized uptake values (SUVs), are less likely to achieve AxpCR [11]. However, the association between baseline glycolytic activity on PET/CT and axillary response seems to be impacted by the subtype of BC [12,13]. While a well-established negative correlation exists between ER expression and 18F-FDG uptake, the connection between 18F-FDG uptake and HER2 status remains a topic of discussion [14,15,16].
Tumor-promoting inflammation represents a well-established biological hallmark of cancer, with the host immune system significantly influencing the clinical response to chemotherapy [17,18]. Increasing evidence indicates a correlation between the absolute monocyte count (AMC) and a poor clinical outcome in patients with BC [19,20,21,22].
The predictive role of SUVmax and AMC in pN+ HER2-positive BC requires further validation.
Combining baseline nodal SUVmax (N-SUVmax) and AMC at diagnosis before NAT may provide valuable insights into axillary response and potentially identify patients in whom AxpCR is most likely, enhancing patient selection for less invasive surgery.
2. Materials and Methods
2.1. Patient Selection
From January 2018 to January 2024, patients with cN+ HER2-positive early BC treated with NAT were included. All patients underwent a comprehensive disease staging process involving breast and axilla examination, mammography, ultrasonography (US) or magnetic resonance imaging, and 18F-FDG PET/CT scan. Patients with distant metastases were excluded from the study. Additional exclusion criteria comprised the absence of axillary surgery post-NAT, inflammatory BC, and incomplete exams. The diagnosis of BC was histologically confirmed via core biopsy. HER2-positive status was determined based on immunohistochemistry (IHC) 3+ or fluorescence in situ hybridization (FISH) by the ASCO-CAP guidelines of 2023 [23]. Central pathologic assessment was conducted to assess HER2 and hormone receptor expression, with negativity defined as less than 1% estrogen and progesterone receptor expression by IHC. Axillary lymph nodes were evaluated using axillary US and 18F-FDG PET/CT scan, with histologic confirmation of suspicious lymph nodes [24]. The decision to clip axillary lymph nodes was left to the physicians' discretion. All patients with clinically detected axillary nodal metastasis before NAT underwent appropriate axillary surgery with or without sentinel lymph node biopsy (SLNB) post-NAT. In the case of bilateral invasive BC, lymph nodes were assessed in both axillae separately.
2.2. Treatment
Patients were offered an anthracycline-free regimen NAT by the prevailing BC guidelines [25,26]. The neoadjuvant therapy regimen was the TCbHP with docetaxel (75 mg/m2), carboplatin [area under the concentration-time curve (AUC): 6 mg/mL/min] intravenously, once every three weeks in association with trastuzumab and pertuzumab. The trastuzumab loading dose was 8 mg/kg, followed by 6 mg/kg intravenously, once every three weeks. The pertuzumab loading dose was 840 mg, followed by 420 mg intravenously, once every three weeks. Patients who experienced drug reactions during chemotherapy had their doses modified accordingly or were switched to paclitaxel weekly in association with trastuzumab and pertuzumab.
All patients underwent surgery after six cycles of neoadjuvant therapy.
2.3. 18 F-FDG PET/CT Imaging Acquisition
Whole body PET/CT image acquisition was performed at 60±5 min after intravenous injection of 18F-FDG with a mean activity of 3 MBq/Kg. Before radiotracer injection, fasting for at least 6 hours and a blood glucose value <160 mg/dL were ensured in all patients. PET/CT scans were obtained with Bio-graph® mCT40 (Siemens Medical Solutions, Germany), applying standard protocols in accordance with the European Association of Nuclear Medicine guidelines [27]. The PET/CT scan was acquired in flow-motion using the same axial field as the CT scan from the mid-thigh toward the base of the skull. PET images (CT corrected for attenuation) were reconstructed with standard iterative 3D algorithms, including Time-of-Flight (TOF) and Point-Spread Function (PFS) corrections. A contrast-enhanced CT (ceCT) of the head-neck, thorax, abdomen and pelvis was performed following PET protocol when requested. The scanning parameters were as follows: section thickness, 3 mm; voltage, 100 kV; tube current, 150 mA; and matrix 500×500. An intravenous bolus dose of 90 mL of nonionic iodinated contrast agent (Accupaque, GE Healthcare) was administered at a rate of 2 mL/s.
2.4. Imaging Assessment
Two highly experienced nuclear medicine physicians (M.C. and G.P.), blinded to the patients' clinical and pathological information, carefully examined all images, using simultaneous displays of PET, CT, and fused PET/CT images.
Quantitative standardized uptake value (SUV) derived parameters on 18F-FDG PET/CT images were obtained using dedicated software (MM Oncology, VOI isocenter, SyngoVia®, Siemens Medical Solutions, Germany). For each patient, the volume of interest (VOI) encompassing the most FDG-avid axillary lymph node (N) was derived by manual segmentation, and metabolic SUV-derived parameters such as the maximum value of SUV (N-SUVmax) were obtained. The SUVmax value was calculated for each volume of interest by adjusting the measured activity for radioactive decay, total administered activity, and body weight.
2.5. Response Assessment of Axillary Nodes
Following NAT, all patients proceeded with standard surgery. The approach to the axillary lymph nodes was based on the surgeons' discretion and patient preference. AxpCR was defined as the absence of invasive residuals in the lymph nodes (ypN0) post-NAT. Post-NAT, axillary lymph nodes were clinically evaluated as ycN0, ycN+, or ycNx (missing data). Hematoxylin-eosin staining was utilized to examine all removed axillary lymph nodes and micrometastases (ypN1mi), which were carefully considered as ypN1. All histopathological reports underwent central review for pCR assessment.
2.6. Blood Tests
5 mL of venous blood was drawn from each patient on an empty stomach and placed in an anticoagulation tube at baseline before treatment at the time of diagnosis. The blood was then centrifuged at a centrifugal rate of 1500 r/min. Absolute monocyte count (AMC) was determined automatically with a hematology analyzer. Subsequently, the lymphocyte and monocyte counts were collected, and the lymphocyte-to-monocyte ratio (LMr) was calculated for each patient, defined as the ratio of lymphocyte to monocyte count.
2.7. Statistical Analysis
Statistical analyses were performed using SPSS software (version 28, IBM Corporation, Armonk, New York, USA). For continuous variables, univariate distribution may be described utilizing descriptive statistics such as median, interquartile range (IQR), or mean and standard deviation (SD). Categorical variables were compared using the Pearson chi-square test or Fisher's exact test. Univariate descriptive analysis of the variables under study was carried out by calculating the centrality and variability indices for the quantitative variables and frequency tables for the qualitative variables. Multiple logistic regression models have been used to investigate the effect of AMC, N-SUVmax, LMr, ER, and HER2 on the probability of AxpCR after NAT or whether certain combinations of parameters are associated with it. Results are expressed as hazard ratios (HR) with 95% confidence intervals (95% CI). Receiver operating characteristic (ROC) curves and relative areas under the curves (AUC) were used to select the best potential cutoff value for the AMC and metabolic markers, including N-SUVmax, to predict AxpCR to NAT. The corresponding sensitivity and specificity were calculated.
An alpha significance level of 0.05 was used in all analyses mentioned.
3. Results
3.1. Patient Characteristics
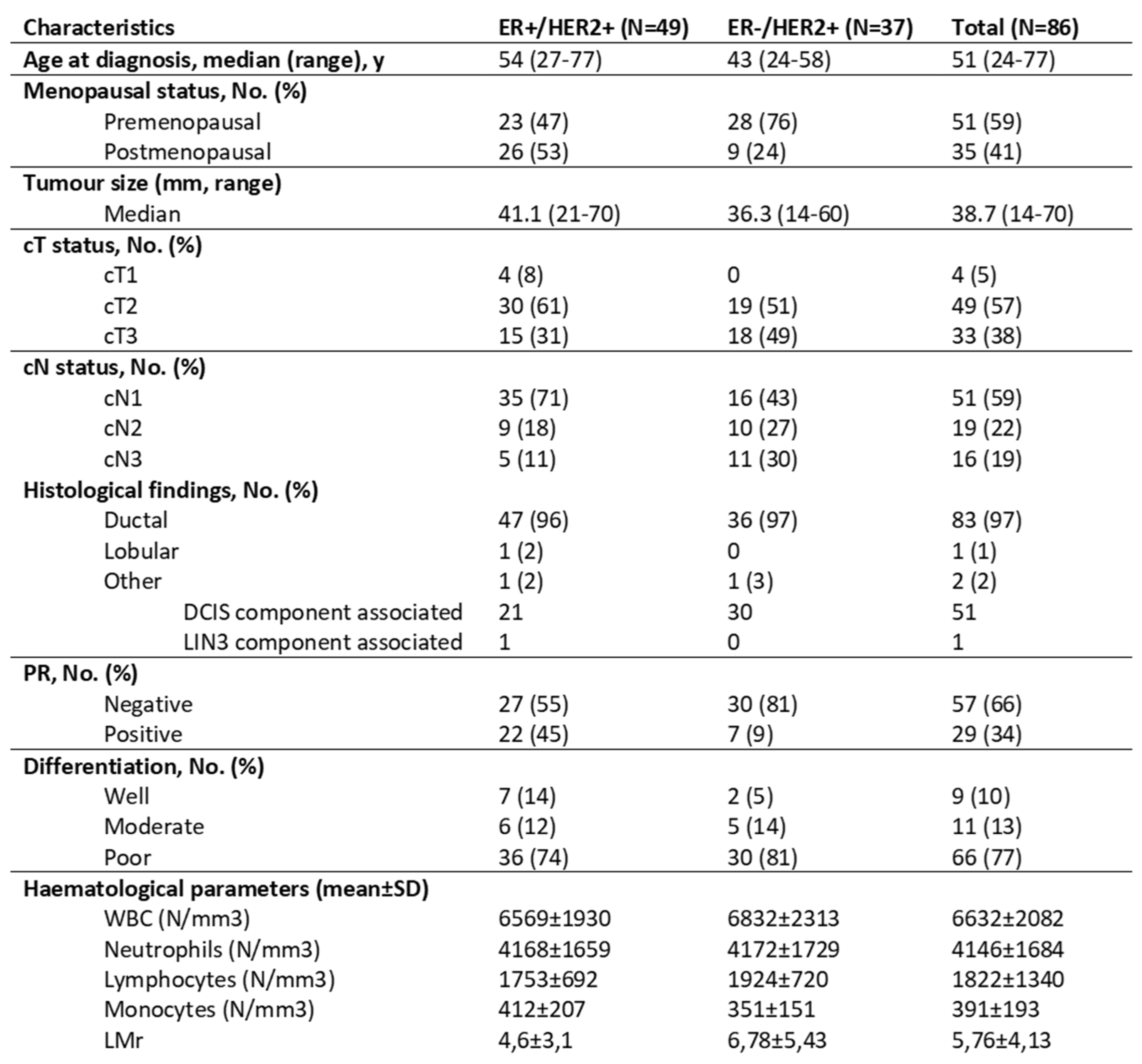
One hundred and seven consecutive patients with HER2-positive BC underwent 18F-FDG PET/CT before NAT at the Oncology Institute of Southern Switzerland. All patients had their suspicious nodal status confirmed pathologically through fine needle aspiration. After excluding twenty-one cases with pathologically confirmed clinically node-negative HER2-positive invasive BC, the study included 86 patients. The clinicopathologic and operative characteristics of the included patients are detailed in Table 1.
The median age at diagnosis was 51 years (range: 24-77), with the majority (59%) being in a premenopausal status.
The mean ± SD primary tumor size was 38.7±16 mm (range: 14-70 mm). Histopathological evaluation showed that 97% of the patients (83 individuals) had invasive ductal BC (IDC), while 1% presented with invasive lobular carcinoma (ILC) in the breast. Immunohistochemical profiling of the 86 patients indicated that 57% had luminal and 43% had non-luminal HER2-positive BC.
3.2. Axillary Response to NAT
Of the 86 node-positive HER2-positive patients who underwent NAT, 57 individuals (66.3%) achieved AxpCR. A notable discrepancy in AxpCR rates was observed across subtypes, with an overall AxpCR rate of 82.4% in the ER-HER2+ group, surpassing 55.8% in the luminal HER2-positive group (p=0.0116).
3.3. Relationship Between AMC and AxpCR
The median AMC for all patients was 360 cells/mm3 (25th-75th percentile, 230-500 cells/mm3). A ROC curve was constructed, and Youden’s Index was utilized to ascertain the optimal cut-off value for AMC, maximizing sensitivity and specificity. The optimal cut-off level from the ROC curve analysis was 340 cells/mm3, and the AUC was 0.86 (95% CI, 0.71-0.91).
Overall, sensitivity and specificity were 93% and 48%.
Using a cutoff value of 340 cells/mm³, patients were categorized into two groups: AMC-low (≤340 cell/mm3, n=40) and AMC-high (≥340 cell/mm3, n=46). Patients in the AMC-low group exhibited a higher AxpCR rate (n=36; 90%) than those in the AMC-high group (n=21; 46%) (p< 0.0001).
3.4. Relationship Between N-SUVmax and AxpCR
The median SUVmax for all patients was 9.63±8.2 (range: 0-51).
A ROC curve was constructed, and Youden’s Index was utilized to ascertain the optimal cut-off value for N-SUVmax. The identified best N-SUVmax cut-off of 3.5 yielded a sensitivity of 93% and specificity of 67%.
Using a cut-off value of 3.5, patients were categorized into two groups: N-SUVmax-low (<3.5, n=13) and N-SUVmax-high (≥3.5, n=73). Patients in the N-SUVmax-high group exhibited a higher AxpCR rate (n=53, 73%) than those in the N-SUVmax-low group (n=4, 31%) (p= 0.005).
AxpCR and the Combination of AMC and N-SUVmax
The logistic regression analysis included N-SUVmax and AMC as independent variables. These two variables significantly influenced the likelihood of AxpCR occurrence. Specifically, N-SUVmax value of 3.5 or higher resulted in a nearly 4.6-fold increase in the probability of AxpCR (p-value=0.039, OR=4.638 [1.081; 1.904]), while an AMC exceeding 340/mm3 correlated with a 90.4% reduction in the likelihood of AxpCR (p-value<0.001, OR=0.096 [0.028; 0.324]) (Table 2).
Another logistic regression analysis involving N-SUVmax, AMC, LMr, and the interaction between N-SUVmax and AMC as independent variables was conducted. An increase in LMr corresponded to an increased likelihood of AxpCR (p-value=0.038, OR=1.474 [1.021; 2.126]).
Moreover, an increase in N-SUVmax demonstrated a direct correlation with an increased likelihood of AxpCR (p-value=0.006, OR=2.158 [1.250; 3.726]). The interaction between N-SUVmax and AMC yielded a statistically significant odds ratio of 0.999, signifying that the effect of N-SUVmax on the likelihood of AxpCR was diminished with an increase in AMC (p-value=0.006, OR=0.999 [0.997; 1.000]) (Table 3).
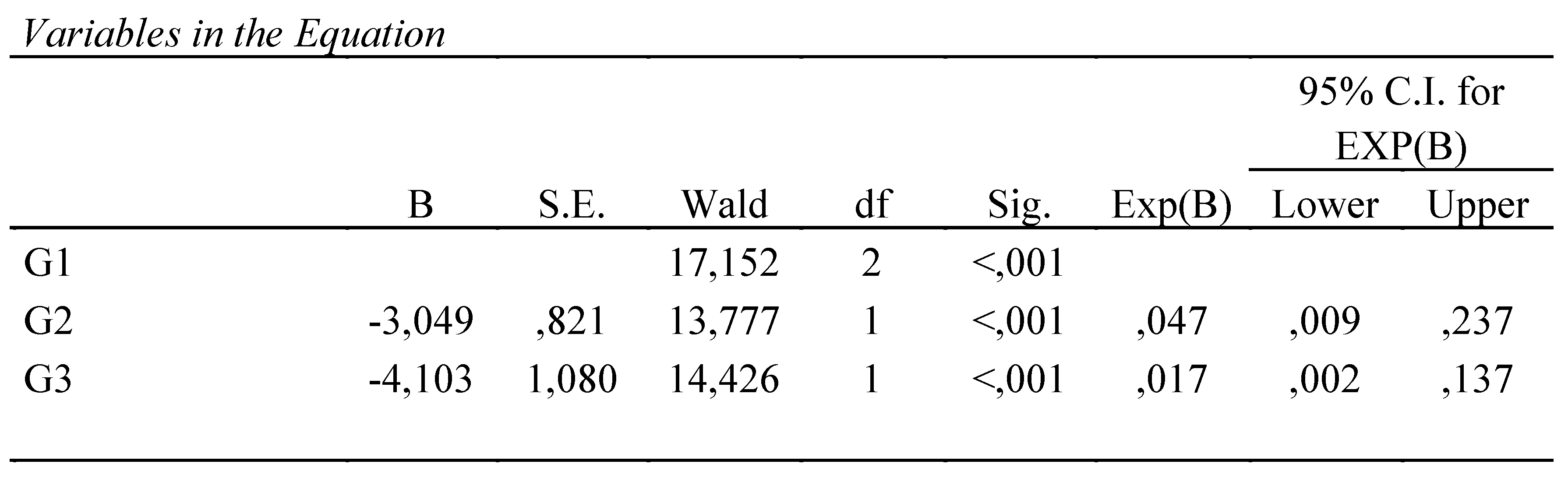
Given the substantial predictive value of both N-SUVmax and AMC, patients were stratified based on their N-SUVmax values, categorized as either ≥3.5 or <3.5, and AMC levels, classified as >340/mm3 or ≤340/mm3, resulting in the classification of three distinct risk groups. These groups include the low-risk level (N-SUVmax-high and AMC-low group, Group 1, G1; n=38, 44%), the intermediate level (N-SUVmax-high and AMC-high group or N-SUVmax-low and AMC-low group, Group 2, G2; n=37, 43%), and the high-risk level (N-SUVmax-low and AMC-high group, Group 3, G3; n=11, 13%).
The number of patients achieving AxpCR was 36 in G1, 18 in G2, and 3 in G3, with corresponding objective response rates (ORRs) of 95%, 47%, and 27%, respectively. These discrepancies were found to be statistically significant (p-value < 0.001). Group 1 demonstrated the highest AxpCR rate (95%), while Group 3 exhibited the lowest rate (27%). Group 1 was individually compared to the other two groups to further investigate the potential differences between the groups (Table 4). The statistical analysis indicated that being in the low-N-SUVmax – high AMC group (p-value < 0.001, OR= 0.017 [0.002; 0.137]) or being in Group 2 (p-value < 0.001; OR= 0.047 [0.009; 0.237]) rather than being in the high-N-SUVmax with low AMC group decreased the likelihood of achieving AxpCR. Furthermore, the p-values were < 0.001 when Group 1 was compared with Group 2 and Group 3.
4. Discussion
Accurate detection of nodal-positive disease is crucial in BC for treatment decisions and prognostic assessment, making developing precise diagnostic methods essential [28,29].
The current BC guidelines recommend a clinical examination in combination with imaging, which should include bilateral diagnostic mammography and US of both breasts and regional lymph nodes. A chest and abdomen CT scan is warranted when clinically positive axillary nodes are identified [30].
Recent research findings have suggested that both US and CT imaging modalities may have limitations in terms of sensitivity. Alvarez et al. have proposed that the effectiveness of the US in excluding nodal involvement may be somewhat restricted by its moderate sensitivity, and negative US results may not definitively rule out the presence of axillary lymph node metastases [31].
The findings from Ogasawara's study demonstrated that CT's sensitivity in detecting axillary nodal involvement in BC patients was 76.9% if a short-axis diameter of 5 mm was utilized as the cut-off value for suspicious lymph nodes [32].
To address these limitations, implementing 18F-FDG PET/CT in clinical practice has been considered to enhance the detection of nodal involvement with a reduced false negative rate [33].
Riegger et al. found that 18F-FDG PET/CT outperformed US in detecting axillary lymph node metastasis (p=0.019) [34]. According to their study, PET/CT demonstrated a sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), and accuracy of 54%, 89%, 77%, 75%, and 75%, respectively, for detecting axillary lymph node metastasis. US yielded values of 38%, 78%, 54%, and 62%, respectively. However, it is essential to note that 18F-FDG PET/CT exhibits low sensitivity in detecting micrometastases in axillary lymph nodes [35], reasonably due to the spatial resolution limit of 4-5 mm. As in our study, Keam et al. did not find a difference in baseline SUVmax between clinically node-positive patients with AxpCR and residual axillary disease [36].
The AxpCR rates significantly vary for different BC subtypes, occurring more frequently in HER2-positive BC [4].
In a comprehensive meta-analysis that included nodal-positive BC, Houssami et al. found that the non-luminal HER2-positive subtypes exhibited the highest probability of achieving AxpCR [37].
Several studies have elucidated a probable rationale for the association between HER2 and SUVmax. Ueda et al. have documented a correlation between the overexpression of the cerbB2 oncogene and SUVmax, potentially attributable to the involvement of the HER2 gene in the glycolytic pathway [38,39].
The glycolytic pathway activates and regulates the immune system, particularly in macrophage polarization [40,41]. Monocytes, which are recruited to the tumor microenvironment (TME) by inflammatory cytokines released by cancer cells, differentiate into macrophages and tumor-associated macrophages (TAMs) under the influence of colony-stimulating factor 1 [42]. Following this, TAMs undergo further polarization into immunosuppressive M2-like macrophages due to the presence of specific cytokines [43]. These M2-like macrophages promote cancer progression and mediate immunosuppression by expressing high levels of T-cell immune checkpoint ligands that directly inhibit T cells or by releasing cytokines that contribute to maintaining an immunosuppressive TME [44]. The accumulation of lactate, a product of glycolysis, further contributes to the polarization of M2-type macrophages, thereby promoting tumor development and leading to worse outcomes in BC patients [45].
It is increasingly clear how tumor glycolytic activity and AMC could be used as indicators to predict tumor response and achieve AxpCR in HER2-positive BC patients.
Pursuing surgical de-escalation strategies in lymph node surgery following NAT is currently sparking intense and invigorating debate.
There is a discernible shift in favor of utilizing sentinel lymph node biopsy over ALND in patients lacking clinical evidence of lymph node involvement.
An analysis of the National Cancer Data Base (NCDB) has demonstrated that among cN0 patients with HER2-positive disease who achieved a complete response in the breast post-treatment, the rate of nodal involvement was below 2% [46]. This observation has prompted inquiries into the potential omission of lymph node surgery in this specific patient subgroup, leading to the initiation of new prospective trials.
The 2019 St. Gallen International Consensus Guidelines for the Primary Therapy of Early BC proposed that patients with BC presenting with clinical N2 disease should undergo ALND and regional lymph node irradiation, irrespective of their response to the NAT [47].
It is well-established that patients diagnosed with clinically node-positive BC frequently undergo NAT and this treatment approach has been shown to successfully eradicate nodal disease in 40% to 75% of cases [48,49,50].
The findings from the GeparOcto study revealed that over 50% of patients showed a negative lymph node status after treatment, indicating that subjecting them to complete ALND could be excessive [51]. Moreover, ALND is correlated with the development of lymphedema in around 20% of BC patients, and this risk increases to 25% when radiotherapy is added due to the high initial axillary burden. This significantly impacts the patient's quality of life [52].
Consequently, there is an increasing emphasis on employing minimally invasive axillary surgery to assess the lymph node status following NAT accurately.
Identifying patients who may not need ALND has presented a formidable yet rewarding challenge. BC molecular subtypes respond differently to NAT.
Rouzier et al. demonstrated that HER2-positive tumors exhibited the highest pathologic complete response rate [53].
In their study, Garcia-Tejedor et al. documented 221 cases of patients presenting a high axillary burden (N2) or with a diagnosis of at least three suspicious metastatic axillary lymph nodes as determined by US. Following NAT, the rate of AxpCR was observed to be 67.9% for the HER2-positive subtype [54].
In our study, the combination of N-SUVmax and AMC yielded 95% of patients achieving AxpCR. Precisely, a SUVmax higher than 3.5 measured on most FDG-avid axillary lymph nodes, along with an AMC lower than 340 cells/mm3 in BC patients with the HER2-positive subtype, is predictive of having no residual axillary disease following NAT.
The number of affected lymph nodes before NAT was not associated with the final axillary response, and HER2-positive patients with cN1, cN2, and cN3 could achieve AxpCR through NAT. This suggests that the axillary response may not directly correlate with the number of suspicious lymph nodes at diagnosis. We acknowledge the limitations of our study, such as its retrospective nature and the small number of patients. More data are needed from a more significant number of patients from multiple centers studies.
5. Conclusions
Our results suggest improving the already high predictive value of 18F-FDG PET/CT by combining it with easily detectable AMC in peripheral blood. Efforts to reduce the extent of axillary surgery after NAT have been consistently in progress.
Our study suggests that combining hematological and easily computed 18F-FDG PET/CT quantitative parameters could help predict axillary response in HER2-positive BC patients after NAT, enhancing the ability of 18F-FDG PET/CT alone to identify HER2-positive patients with AxpCR.
Author Contributions
Conceptualization, R.L., C.M. and R.L.; methodology, C.M. and P.G..; software, C.M. and P.G..; formal analysis, R.L., C.M., P.N. and H.Y.; investigation, S.D. and V.B..; resources, R.L. and G.G.R.; data curation, R.L.,C-M., G.G.R, R.M and R.L.; writing—original draft preparation, R.L., C.M. and R.L.; writing—review and editing, R.L., V.B. and G.M.L.; visualization, S.D.; supervision, C.M., R.M. and R.L.; project administration, R.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study and written informed consent has been obtained from the patients to publish this paper.
Data Availability Statement
We encourage all authors of articles published in MDPI journals to share their research data. In this section, please provide details regarding where data supporting reported results can be found, including links to publicly archived datasets analyzed or generated during the study. Where no new data were created, or where data is unavailable due to privacy or ethical restrictions, a statement is still required. Suggested Data Availability Statements are available in section “MDPI Research Data Policies” at https://www.mdpi.com/ethics.
Acknowledgments
We wish to thank all the patients, family members and staff from all the units that participated in the study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- The Lancet Oncology (2024). Curbing the climb in cancer incidence. The Lancet. Oncology, 25(5), 529. [CrossRef]
- Shubeck, S.P. , Morrow, M. & Dossett, L.A. De-escalation in BC surgery. npj BC 8, 25 (2022). [CrossRef]
- Simons JM, van Nijnatten TJA, van der Pol CC, Luiten EJT, Koppert LB, Smidt ML. Diagnostic accuracy of different surgical procedures for axillary staging after neoadjuvant systemic therapy in node-positive BC: a systematic review and meta-analysis. Ann Surg. 2019;269(3):432–42. [CrossRef]
- Samiei S, Simons JM, Engelen SME, Beets-Tan RGH, Classe JM, Smidt ML, et al. Axillary pathologic complete response after neoadjuvant systemic therapy by BC subtype in patients with initially clinically node-positive disease: a systematic review and meta-analysis. JAMA Surg. 2021;156(6): e210891. [CrossRef]
- Early BC Trialists’ Collaborative Group (EBCTCG). Long-term outcomes for neoadjuvant versus adjuvant chemotherapy in early BC: Meta-analysis of individual patient data from ten randomised trials. Lancet Oncol. 2018, 19, 27–39.
- Gustavo Werutsky, G.; Untch, M.; Hanusch, C.; Fasching, P.A.; Blohmer, J.U.; Seiler, S.; Denkert, C.; Tesch, H.; Jackisch, C.; Gerber, B.; et al. Locoregional recurrence risk after neoadjuvant chemotherapy: A pooled analysis of nine prospective neoadjuvant BC trials. Eur. J. Cancer 2020, 130, 92–101. [Google Scholar] [CrossRef]
- Ivanovic N, Bjelica D, Loboda B, Bogdanovski M, Colakovic N, Petricevic S, Gojgic M, Zecic O, Zecic K, Zdravkovic D. Changing the role of pCR in BC treatment - an unjustifiable interpretation of a good prognostic factor as a "factor for a good prognosis". Front Oncol. 2023 Jul 18; 13:1207948. PMCID: PMC10391828. [CrossRef] [PubMed]
- Lim GH, Leong LCH. Oncologic outcomes in BC patients with metastatic nodes and pathological nodal response following neoadjuvant chemotherapy without axillary dissection: a literature review. Ann Transl Med. 2023 Mar 15;11(5):218. Epub 2023 Mar 9. PMCID: PMC10061475. [CrossRef] [PubMed]
- Carter, S.; Neuman, H.; Mamounas, E.P.; Bedrosian, I.; Moulder, S.; Montero, A.J.; Jagsi, R. Debating the optimal approach to nodal management after pathologic complete response to neoadjuvant chemotherapy in patients with BC. Am. Soc.Clin. Oncol. Educ. Book 2019, 39, 42–48. [Google Scholar] [CrossRef] [PubMed]
- Tausch C, Däster K, Hayoz S, et al. Trends in use of neoadjuvant systemic therapy in patients with clinically node-positive BC in Europe: prospective TAXIS study (OPBC-03, SAKK 23/16, IBCSG 57-18, ABCSG-53, GBG 101). BC Res Treat. 2023;201(2):215-225. [CrossRef]
- Vaz SC, Woll JPP, Cardoso F, et al. Joint EANM-SNMMI guideline on the role of 2-[18F]FDG PET/CT in no special type BC : (endorsed by the ACR, ESSO, ESTRO, EUSOBI/ESR, and EUSOMA). Eur J Nucl Med Mol Imaging. Published online May 14, 2024. [CrossRef]
- Koolen BB, Valdés Olmos RA, Wesseling J, et al. Early assessment of axillary response with ¹⁸F-FDG PET/CT during neoadjuvant chemotherapy in stage II-III BC: implications for surgical management of the axilla. Ann Surg Oncol. 2013;20(7):2227-2235. [CrossRef]
- Cheng J, Wang Y, Mo M, et al. 18F-fluorodeoxyglucose (FDG) PET/CT after two cycles of neoadjuvant therapy may predict response in HER2-negative, but not in HER2-positive BC. Oncotarget. 2015;6(30):29388-29395. [CrossRef]
- Koolen BB, Pengel KE, Wesseling J, et al. FDG PET/CT during neoadjuvant chemotherapy may predict response in ER-positive/HER2-negative and triple negative, but not in HER2-positive BC. Breast. 2013;22(5):691-697. [CrossRef]
- van Ramshorst MS, Teixeira SC, Koolen BB, et al. Additional value of 18F-FDG PET/CT response evaluation in axillary nodes during neoadjuvant therapy for triple-negative and HER2-positive BC. Cancer Imaging. 2017;17(1):15. Published 2017 May 25. [CrossRef]
- Groheux D, Mankoff D, Espié M, Hindié E. ¹⁸F-FDG PET/CT in the early prediction of pathological response in aggressive subtypes of BC: review of the literature and recommendations for use in clinical trials. Eur J Nucl Med Mol Imaging. 2016;43(5):983-993. [CrossRef]
- Hernandez CM, Madrona AP, Vazquez PJG, Fernandez PJG, Merino GR, Romero JLA, et al.. Usefulness of Lymphocyte-to-Monocyte, Neutrophil-to-Monocyte and Neutrophil-to-Lymphocyte Ratios as Prognostic Markers in BC Patients Treated With Neoadjuvant Chemotherapy. Clin Trans Oncol (2018) 20(4):476–83. [CrossRef]
- Kzhyshkowska J, Gudima A, Moganti K, Gratchev A, Orekhov A. Perspectives for Monocyte/Macrophage-Based Diagnostics of Chronic Inflammation. Transfus Med Hemother (2016) 43(2):66–77. [CrossRef]
- Michaud DE, Guerriero JL. Myeloid Cells Pave the Metastatic Road in BC. Cancer Res. 2024;84(2):181-183. [CrossRef]
- Ueno T, Toi M, Saji H, Muta M, Bando H, Kuroi K, et al.. Significance of Macrophage Chemoattractant Protein-1 in Macrophage Recruitment, Angiogenesis, and Survival in Human BC. Clin Cancer Res (2000) 6(8):3282–3289.
- Lubowicka E, Przylipiak A, Zajkowska M, Piskor BM, Malinowski P, Fiedorowicz W, et al.. Plasma Chemokine CCL2 and Its Receptor CCR2 Concentrations as Diagnostic Biomarkers for BC Patients. BioMed Res Int (2018) 2018:2124390. [CrossRef]
- Patysheva M, Larionova I, Stakheyeva M, et al. Effect of Early-Stage Human Breast Carcinoma on Monocyte Programming. Front Oncol. 2022;11:800235. Published 2022 Feb 14. [CrossRef]
- Wolff AC, Somerfield MR, Dowsett M, Hammond MEH, Hayes DF, McShane LM, Saphner TJ, Spears PA, Allison KH. Human Epidermal Growth Factor Receptor 2 Testing in BC: ASCO-College of American Pathologists Guideline Update. J Clin Oncol. 2023 Aug 1;41(22):3867-3872. Epub 2023 Jun 7. [CrossRef] [PubMed]
- Chang JM, Leung JWT, Moy L, Ha SM, Moon WK. Axillary Nodal Evaluation in BC: State of the Art. Radiology. 2020 Jun;295(3):500-515. Epub 2020 Apr 21. [CrossRef] [PubMed]
- Schneeweiss A, Chia S, Hickish T, et al. Long-term efficacy analysis of the randomised, phase II TRYPHAENA cardiac safety study: evaluating pertuzumab and trastuzumab plus standard neoadjuvant anthracycline-containing and anthracycline-free chemotherapy regimens in patients with HER2-positive early BC. Eur J Cancer 2018; 89:27-35. [CrossRef]
- van Ramshorst MS, van der Voort A, van Werkhoven ED, et al. Neoadjuvant chemotherapy with or without anthracyclines in the presence of dual HER2 blockade for HER2-positive BC (TRAIN-2): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol 2018; 19:1630-40. [CrossRef]
- Boellaard, R.; et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: Version 2.0. Eur. J. Nucl. Med. Mol. Imaging 42(2), 328–354 (2015). [CrossRef]
- Fisher B, Bauer M, Wickerham DL, Redmond CK, Fisher ER, Cruz AB, et al. Relation of number of positive axillary nodes to the prognosis of patients with primary BC. An NSABP update. Cancer 1983. ;52(9):1551–1557. 01 November. [CrossRef]
- Holmström O, Linder N, Moilanen H, Suutala A, Nordling S, Ståhls A, Lundin M, Diwan V, Lundin J. Detection of BC lymph node metastases in frozen sections with a point-of-care low-cost microscope scanner. PLoS One. 2019 Mar 19;14(3):e0208366. PMCID: PMC6424449. [CrossRef] [PubMed]
- Loibl S, André F, Bachelot T, Barrios CH, Bergh J, Burstein HJ, Cardoso MJ, Carey LA, Dawood S, Del Mastro L, Denkert C, Fallenberg EM, Francis PA, Gamal-Eldin H, Gelmon K, Geyer CE, Gnant M, Guarneri V, Gupta S, Kim SB, Krug D, Martin M, Meattini I, Morrow M, Janni W, Paluch-Shimon S, Partridge A, Poortmans P, Pusztai L, Regan MM, Sparano J, Spanic T, Swain S, Tjulandin S, Toi M, Trapani D, Tutt A, Xu B, Curigliano G, Harbeck N; ESMO Guidelines Committee. Electronic address: clinicalguidelines@esmo.org. Early BC: ESMO Clinical Practice Guideline for diagnosis, treatment and follow-up. Ann Oncol. 2024 Feb;35(2):159-182. Epub 2023 Dec 13. [CrossRef] [PubMed]
- Alvarez S, Anorbe E, Alcorta P, Lopez F, Alonso I, Cortes J. Role of sonography in the diagnosis of axillary lymph node metastases in BC: a systematic review. AJR Am J Roentgenol. 2006;186:1342–8. [CrossRef]
- Ogasawara Y, Doihara H, Shiraiwa M, Ishihara S. Multidetectorrow computed tomography for the preoperative evaluation of axillary nodal status in patients with BC. Surg Today. 2008;38:104–8. [CrossRef]
- Wahl RL, Siegel BA, Coleman RE, Gatsonis CG, Group PETS. Prospective multicenter study of axillary nodal staging by positron emission tomography in BC: a report of the staging BC with PET Study Group. J Clin Oncol. 2004;22:277– 85. [CrossRef]
- Riegger C, Koeninger A, Hartung V, Otterbach F, Kimmig R, Forsting M, Bockisch A, Antoch G, Heusner TA. Comparison of the diagnostic value of FDG-PET/CT and axillary ultrasound for the detection of lymph node metastases in BC patients. Acta Radiol. 2012 Dec 1;53(10):1092-8. Epub 2012 Sep 22. [CrossRef] [PubMed]
- Hwang SO, Lee SW, Kim HJ, Kim WW, Park HY, Jung JH. The Comparative Study of Ultrasonography, Contrast-Enhanced MRI, and (18)F-FDG PET/CT for Detecting Axillary Lymph Node Metastasis in T1 BC. J BC. 2013 Sep;16(3):315-21. Epub 2013 Sep 30. PMCID: PMC3800728. [CrossRef] [PubMed]
- Keam B, Im SA, Koh Y, Han SW, Oh DY, Cho N, et al. Predictive value of FDG PET/CT for pathologic axillary node involvement after neoadjuvant chemotherapy. BC. 2013;20(2):167–73. [CrossRef]
- Houssami N, Macaskill P, von Minckwitz G, Marinovich ML, Mamounas E. Meta-analysis of the association of BC subtype and pathologic complete response to neoadjuvant chemotherapy. Eur J Cancer. 2012;48(18):3342-3354. [CrossRef]
- Ueda S, Tsuda H, Asakawa H, et al. Clinicopathological and prognostic relevance of uptake level using 18F-fluorodeoxyglucose positron emission tomography/computed tomography fusion imaging (18F-FDG PET/CT) in primary BC. Jpn J Clin Oncol 2008; 38: 250-8. [CrossRef]
- Groheux D, Giacchetti S, Moretti JL, et al. Correlation of high 18F-FDG uptake to clinical, pathological and biological prognostic factors in BC. Eur J Nucl Med Mol Imaging 2011; 38: 426-35. [CrossRef]
- Li, W. , Xu M., Li Y., Huang Z., Zhou J., Zhao Q., et al. (2020). Comprehensive analysis of the association between tumor glycolysis and immune/inflammation function in BC. J. Transl. Med. 18 (1), 92. [CrossRef]
- Xiao, Y.; Yu, D. Tumor microenvironment as a therapeutic target in cancer. Pharmacol. Ther. 2021, 221, 107753. [Google Scholar] [CrossRef] [PubMed]
- Martinez FO, Gordon S, Locati M, Mantovani A. Transcriptional profiling of the human monocyte-to-macrophage differentiation and polarization: new molecules and patterns of gene expression. J Immunol. 2006;177:7303–11. [CrossRef]
- Qiu SQ, Waaijer SJH, Zwager MC, de Vries EGE, van der Vegt B, Schroder CP. Tumor-associated macrophages in BC: innocent bystander or important player? Cancer Treat Rev. 2018;70:178–89. [CrossRef]
- Alderton, GK. Tumour immunology: turning macrophages on, off and on again. Nat Rev Immunol. 2014;14:136–7. [CrossRef]
- Jiang, H. , Wei H., Wang H., Wang Z., Li J., Ou Y., et al. (2022). Zeb1-induced metabolic reprogramming of glycolysis is essential for macrophage polarization in BC. Cell Death Dis. 13 (3), 206. [CrossRef]
- Barron, A.U. , Hoskin T.L., Day C.N., Hwang E.S., Kuerer H.M., Boughey J.C. Association of low nodal positivity rate among patients with erbb2-positive or triple-negative BC and breast pathologic complete response to neoadjuvant chemotherapy. JAMA Surg. 2018;153:1120–1126. [CrossRef]
- Burstein HJ, Curigliano G, Loibl S, Dubsky P, Gnant M, Poortmans P, Colleoni M, Denkert C, Piccart-Gebhart M, Regan M, Senn HJ, Winer EP, Thurlimann B; Members of the St. Gallen International Consensus Panel on the Primary Therapy of Early BC 2019. Estimating the benefits of therapy for early-stage BC: the St. Gallen International Consensus Guidelines for the primary therapy of early BC 2019. Ann Oncol. 2019 Oct 1;30(10):1541-1557. [CrossRef] [PubMed]
- Kim JY, Park HS, Kim S, Ryu J, Park S, Kim SIL (2015) Prognostic nomogram for prediction of axillary pathologic complete response after neoadjuvant chemotherapy in cytologically proven node-positive BC. Medicine 94(43):1–9. [CrossRef]
- Mamtani A, Barrio AV, King TA, Van Zee KJ, Plitas G, Pilewskie M et al (2016) How often does neoadjuvant chemotherapy avoid axillary dissection in patients with histologically confrmed nodal metastases? Results of a prospective study. Ann Surg Oncol 23(11):3467–3474. [CrossRef]
- Diego EJ, McAulife PF, Soran A, McGuire KP, Johnson RR, Bonaventura M et al (2016) Axillary staging after neoadjuvant chemotherapy for BC: a pilot study combining sentinel lymph node biopsy with radioactive seed localization of pre-treatment positive axillary lymph nodes. Ann Surg Oncol 23(5):1549–1553. [CrossRef]
- Schneeweiss A, Michel LL, Möbus V, Tesch H, Klare P, Hahnen E, Denkert C, Kast K, Pohl-Rescigno E, Hanusch C, Link T, Untch M, Jackisch C, Blohmer JU, Fasching PA, Solbach C, Schmutzler RK, Huober J, Rhiem K, Nekljudova V, Lübbe K, Loibl S; GBG and AGO-B. Survival analysis of the randomised phase III GeparOcto trial comparing neoadjuvant chemotherapy of intense dose-dense epirubicin, paclitaxel, cyclophosphamide versus weekly paclitaxel, liposomal doxorubicin (plus carboplatin in triple-negative BC) for patients with high-risk early BC. Eur J Cancer. 2022 Jan; 160:100-111. Epub 2021 Nov 17. [CrossRef] [PubMed]
- Gillespie TC, Sayegh HE, Brunelle CL, Daniell KM, Taghian AG (2018) BC-related lymphedema: risk factors, precautionary measures, and treatments. Gland Surg 7(4):379–403. [CrossRef]
- Rouzier R, Perou CM, Symmans WF, Ibrahim N, Cristofanilli M, Anderson K et al (2005) BC molecular subtypes respond diferently to preoperative chemotherapy. Clin Cancer Res 11(16):5678–5685. [CrossRef]
- Garcia-Tejedor A, Fernandez-Gonzalez S, Ortega R, Gil-Gil M, Perez-Montero H, Fernandez-Montolí E, Stradella A, Recalde S, Soler T, Petit A, Bajen MT, Benitez A, Guma A, Campos M, Pla MJ, Martinez E, Laplana M, Pernas S, Perez-Sildekova D, Catala I, Ponce J, Falo C. Can we avoid axillary lymph node dissection in N2 BC patients with chemo-sensitive tumours such as HER2 and TNBC? BC Res Treat. 2021 Feb;185(3):657-666. Epub 2020 Oct 17. [CrossRef] [PubMed]
Figure 1.
Comparison between patients with AxpCR and those with residual disease. (A) Baseline AMC, (B) baseline N-SUVmax. Fifty-seven (66.3%) patients achieved AxpCR, while 29 (33.7%) had residual tumors after NAT. Patients with residual tumors had a higher mean baseline AMC than those with AxpCR (480/mm3 vs. 300/mm3, p<0.001; see Figure 1A). There was no association observed between baseline mean N-SUVmax and AxpCR (7.928 vs 10.52, p = 0.1665; see Figure 1B). Abbreviation: AxpCR, axillary pathologic complete response; AxRD, axillary residual disease.
Figure 1.
Comparison between patients with AxpCR and those with residual disease. (A) Baseline AMC, (B) baseline N-SUVmax. Fifty-seven (66.3%) patients achieved AxpCR, while 29 (33.7%) had residual tumors after NAT. Patients with residual tumors had a higher mean baseline AMC than those with AxpCR (480/mm3 vs. 300/mm3, p<0.001; see Figure 1A). There was no association observed between baseline mean N-SUVmax and AxpCR (7.928 vs 10.52, p = 0.1665; see Figure 1B). Abbreviation: AxpCR, axillary pathologic complete response; AxRD, axillary residual disease.
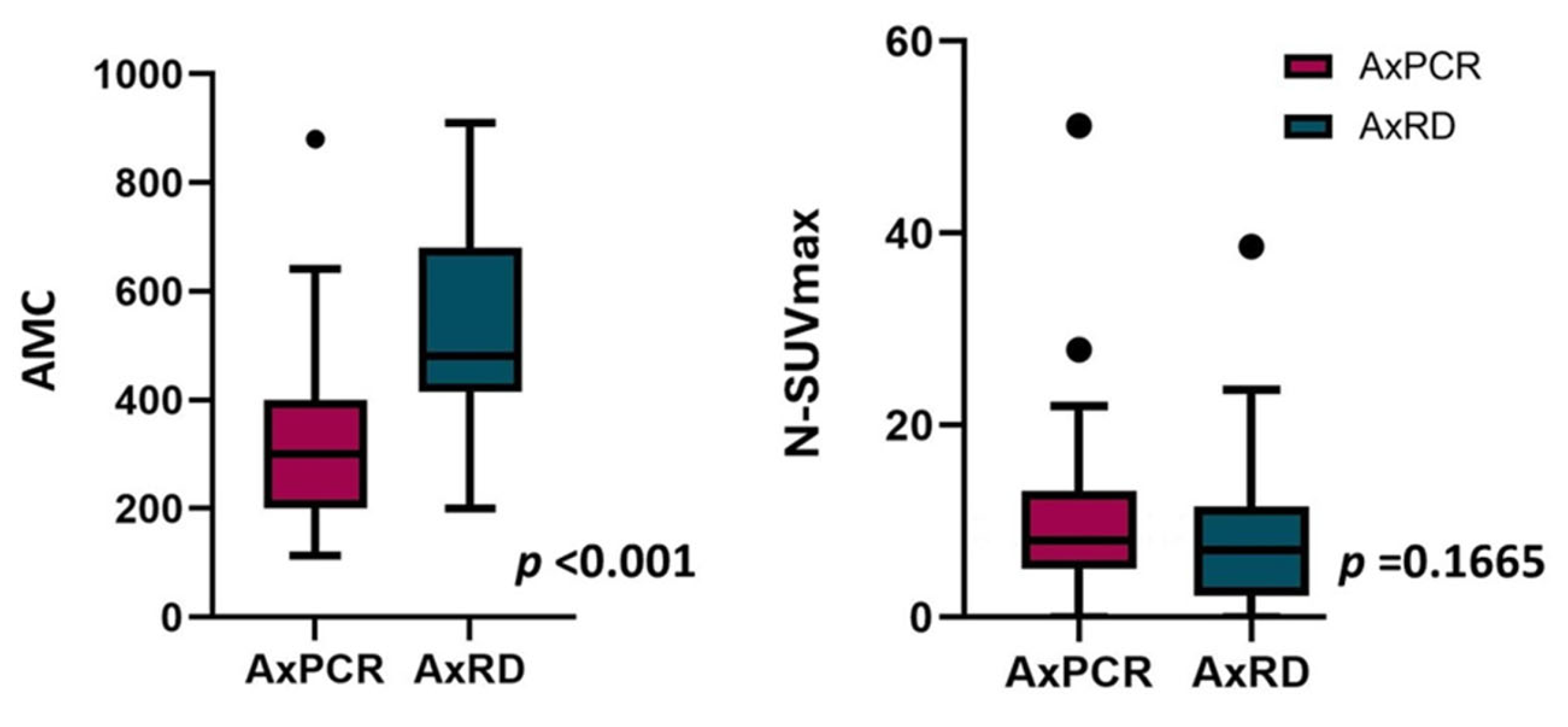

Table 1.
Clinicopathologic characteristics of all BC patients and subdivided by BC subtype.
Abbreviations: cN, clinical node; cT, clinical tumor; ER,estrogen receptor; PR, progesterone receptor; HER2, human epidermal growth factor receptor 2; DCIS ductal carcinoma in situ; LIN, Lobular intraepithelial neoplasia; SD, standard deviation; WBC, white blood count; LMr, lymphocyte-to-monocyte ratio.
Table 2.
AxpCR and the combination of AMC and N-SUVmax.
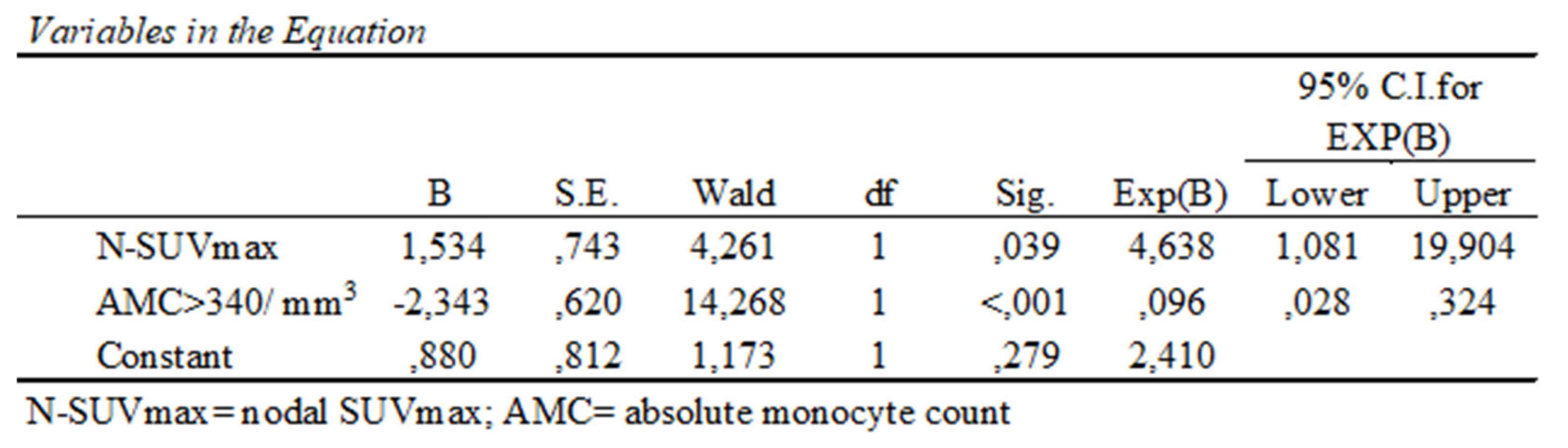
Table 3.
Logistic regression analysis.
| Variables in the Equation | ||||||||
| 95% C.I. for EXP(B) | ||||||||
| B | S.E. | Wald | df | Sig. | Exp(B) | Lower | Upper | |
| AMC | ,004 | ,003 | 1,733 | 1 | ,188 | 1,004 | ,998 | 1,011 |
| LMr | ,388 | ,187 | 4,298 | 1 | ,038 | 1,474 | 1,021 | 2,126 |
| N-SUVmax | ,769 | ,279 | 7,624 | 1 | ,006 | 2,158 | 1,250 | 3,726 |
| AMC by N-SUVmax | -,001 | ,001 | 7,476 | 1 | ,006 | ,999 | ,997 | 1,000 |
| Constant | -4,178 | 2,206 | 3,589 | 1 | ,058 | ,015 | ||
Abbreviation. AMC= absolute monocyte count; N-SUVmax= nodal SUVmax; LMr= lymphocyte-to-monocyte ratio. The logistic regression analysis found that a higher N-SUVmax value significantly increased the likelihood of AxpCR, while an AMC exceeding 340/mm3 reduced the likelihood of AxpCR. Moreover, an increase in LMr and N-SUVmax was linked to a higher likelihood of AxpCR.
Table 4.
Risk groups by N-SUVmax and AMC.
Patients were categorized based on their N-SUVmax values as ≥3.5 or <3.5 and AMC levels as >340/mm3 or ≤340/mm3.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



