
Submitted:
16 November 2024
Posted:
19 November 2024
You are already at the latest version
Abstract
Background: The development of different phenotypes of coronary artery (CA) lesions is regu-lated by many various factors such as proinflammatory agents, zinc-dependent endopeptidases, growth factors and circulating microRNAs (miRs). Objective: to evaluate the expression levels of miR-34a, miR-145 and miR-222, tumor necrosis factor α (TNF-α), matrix metalloproteinases (MMP-1, -9, -13, -14) and vascular endothelial growth factor (VEGF) in patients with different phenotypes of coronary artery disease (CAD): ischemia/angina with non- obstructive coronary arteries (INOCA/ANOCA) and obstructive CAD (oCAD) compared with the control group. Method: The cross-sectional observational study included 157 subjects with verified CAD diag-nosis (51 patients with INOCA, 76 patients with oCAD and 30 healthy volunteers). The expression of miR-34a, miR-145, miR-222 (RT-PCR) and the levels of VEGF, TNF-α, MMP-1, MMP-9, MMP-13, MMP-14 (ELISA) were estimated in the plasma samples. Results: Higher concentration of MMP-9 was found in oCAD group samples compared to the INOCA/ANOCA group. The INOCA/ANOCA group was characterized by higher levels of TNF-α. Based on multivariate regression analysis, a mathematical model predicting the type of CA lesion was constructed. MiR-145 was the inde-pendent predictor of INOCA/ANOCA (p=0.006). Conclusions: Changes in concentrations of MMP-9 and MMP-14 were found in both investigated CAD groups, with MMP-9 levels were sig-nificantly higher in obstructive CAD samples than in INOCA/ANOCA, which confirms the role of inflammation in the development of atherosclerosis. The multivariate regression analysis allowed us to obtain a model that can predict the phenotype of stable CAD and MiR-145 can be assumed as independent predictor of the INOCA/ANOCA.
Keywords:
microRNA (miR-34a
; miR-145
; miR-222)
; matrix metalloproteinases (MMP-1
; MMP-9
; MMP-13
; MMP-14)
; tumor necrosis factor α (TNF-α)
; vascular endothelial growth factor (VEGF)
; ischemia/angina with non-obstructive coronary arteries (INOCA/ANOCA)
; coronary artery disease (CAD)
; cardiovascular diseases (CVD)
1. Introduction
The prevalence of metabolic risk factors and aging of the population in developed countries lead to persistence of high mortality rates from non-communicable diseases, and from coronary artery disease (CAD) in the world [1]. According to World Health Organization (WHO) in 2021, the mortality rate from CAD reached 17.9 million people [2]. Among patients with CAD there are phenotypes with ischemia/angina and non-obstructive coronary arteries (INOCA/ANOCA), the prevalence of which in the population with CAD, according to some studies, reaches 13% [3]. At the same time, INOCA/ANOCA is significantly more common in women (61%, and, in accordance with other data – 65%) than in men (32%) [4,5,6,7]. The development of different types of CA lesions is regulated by many various factors, among which proinflammatory agents play a significant role. According to a study by Karakayali M. et al., the systemic immuno-inflammatory index (SII, platelet × neutrophil/lymphocyte ratio) is independently associated with the presence of INOCA [8]. It is known that in case of INOCA, an increase in the systemic inflammation response index (SIRI) plays a potentially important role in the diagnosis of the slow coronary flow phenomenon [9]. Additionally, numerous factors—including pro-inflammatory cytokines (IL, TNF-α), reactive oxygen species (ROS), an imbalance between vasodilation (NO) and vasoconstriction mediators, several zinc-dependent endopeptidases (matrix metalloproteinases, MMP), and growth factors (such as VEGF)—influence the progression of CA atherosclerosis. This effect was particularly demonstrated in the study by Beatty et al., which showed that TNF-α induces activation of macrophages, T-helper 1 lymphocytes, and endothelial cells in atherosclerosis. Activated endothelial cells produce receptors and adhesion molecules that promote abnormal leukocyte migration into the vascular wall, leading to dysregulated secretion of pro-inflammatory cytokines. The authors conclude that TNF-α and IL-6 play significant roles as risk factors for the development of CAD [10].
MMP are zinc-dependent endopeptidases, which are multi-domain proteins with a highly conserved signal peptide, a propeptide domain, and a catalytic domain [11]. The expression of MMPs as inactive zymogens is transcriptionally regulated by a variety of proinflammatory signals, and MMPs are involved in the destruction of the extracellular matrix [12].
MMPs can be divided into six groups based on substrate specificity and sequence similarity: collagenases, gelatinases, stromelysins, matrilysins, membrane-type MMP and others [13,14]. It is known that foamy and smooth muscle cells (SMC) synthesize MMPs, which play a key role in the formation and growth of atherosclerotic plaques [15]. At the same time, MMPs produced by macrophages are actively involved in the process of the fibrous cap thinning and plaque destabilization [16]. Thus, increased expression of activated MMP-13 is associated with increased collagenolysis in vivo, mainly in atheromatous plaques, and a decrease in the accumulation of SMC at different stages of atherogenesis, in particular, at the preclinical stage [17]. The investigation by Lehrke M. et al. demonstrated that the level of circulating MMP-1 can be used as a predictive marker of the presence of atherosclerotic plaques [18].
The study of the role of circulating microRNAs (miRs) in the epigenetic regulation of the development and progression of atherosclerosis is also of considerable interest. MiRs are short non-coding RNA molecules that regulate gene expression by inhibiting translation or enhancing mRNA degradation. Recent research highlights the significance of miRNAs as promising diagnostic biomarkers for assessing the degree of CA obstruction. In particular, the expression of miR-34a increases in the heart during myocardial hypertrophy caused by stretch, adrenergic stimulation and hypoxia, that has been shown to contribute to the disruption of angiogenesis by uncoupling hypoxia-inducible factor 1-α – VEGF (HIF-1α-VEGF) signaling [19]. In addition, it is known that miR-34a, miR-92a, miR-181c and miR-210 are involved in the regulation of vascular endothelial function by inducing or reducing the level of oxidative stress markers [20,21].
The expression of miR-145 decreases in acute coronary syndrome (ACS), what makes it possible to consider this miR as a potential diagnostic biomarker. A negative correlation of miR-145 with markers of endothelial damage (von Willebrand factor (vWF), heart-type fatty acid-binding protein (H-FABP)) and proinflammatory cytokines (IL-6 and TNF-α) was also found [22]. In turn, miR-221 and miR222 are involved in the regulation of endothelial inflammation, angiogenesis and apoptosis of endothelial cells [23].
According to the literature data, there are isolated evidence on the expression of miR-34a, miR-145 and miR-222 in patients with CAD, including those with INOCA/ANOCA. It should be noted that in patients with CAD (including non-obstructive phenotype), no investigation was conducted of the possible association of the expression of these miRs with proinflammatory cytokines (TNF-α), MMPs and growth factors (VEGF). The study of miR expression levels in such patients can clarify some aspects of the pathogenesis of atherosclerotic lesions of the CA and, in consequence, may be important for determining their potential as possible diagnostic biomarkers and for the development of new therapies with antagomiRs.
2. Results
2.1. Basic Clinical Characteristics
All plasma samples were obtained from patients hospitalized in the cardiology department with a chest pain and shortness of breath have undergone the physical activity tests (stress Echo-CG, myocardial scintigraphy, and cardiac MRI with stress test) to verify the diagnosis of CAD. Patients with confirmed myocardial ischemia were further undergone imaging of the CA (coronary angiography or MSCT of the CA) to address the need for their revascularization. The study included 127 patients, who were divided into 2 groups depending on the degree of CA obstruction: group 1 – 51 patients with hemodynamically insignificant stenosis (INOCA/ANOCA, stenosis <50%) and group 2 – 76 patients with CA obstruction (obstructive CAD, stenosis >50%). The third group (control) consisted of 30 healthy volunteers without CVD risk factors. The design of the study is presented in Figure 1.
CAD – coronary artery disease; INOCA/ANOCA—ischemia/angina with non-obstructive coronary arteries; qPCR – quantitative polymerase chain reaction; MRI – magnetic resonance imaging; MSCT - multi-detector computed tomography.
The general clinical and demographic characteristics of the groups are summarized in Table 1. The investigated groups were comparable according to the main clinical and demographic indicators (age, body mass index (BMI)). In the group of patients with INOCA/ANOCA, women prevailed (60.8% women vs. 39.2% men) and vice versa in the group of patients with obstructive CAD (the number of men was higher in a ratio 2:1 (67.1% men vs. 32.9% women)).
The differences in total cholesterol and low-density lipoproteins (LDL) levels between the groups are most likely determined by the better results in reducing the level of total cholesterol and LDL in patients with obstructive CAD who were treated with higher doses of statins. The therapy that patients received at the time of hospitalization is summarized in Table 2.
2.2. Concentration of MMPs, TNF-a and VEGF in Plasma
According to the results of the study, significant differences in the concentration of MMPs-9 and -14, and TNF-α were revealed when compared with the control group. The level of VEGF was significantly higher only in INOCA/ANOCA group than in control. Also, we found differences between the variants of CADs (obstructive and non-obstructive) in case of TNF-α and MMP-9.
When analyzing the results between the groups, higher levels of MMP-9 were noted in patients with CAD and obstructive CA lesions. The obstructive CAD group was lower in VEGF and TNF-α concentrations versus the INOCA/ANOCA. The concentration of MMP-1 and MMP-13 in the study groups did not differ significantly (Table 3).
2.3. MiRNA Expression in Plasma of Patients with CAD
The expression levels of miR-34a (p<0.001) and miR-222 (p<0.001) was were significantly higher in all patients with CAD (obstructive and non-obstructive) in comparison with the control group, while the expression of miR-145 was significantly higher in the INOCA/ANOCA group than in the control (p=0.039) (Figure 2).
2.4. Correlations of VEGF, TNF-α and MMPs with Circulating miRNAs
According to the correlation analysis in the INOCA/ANOCA group, notable associations were recorded between VEGF and MMP-1 (p = 0.668; p< 0.001), as well as MMP-14 (p = 0.629; p< 0.001). In the obstructive CAD group, a moderate association was observed between VEGF and MMP-9 (ρ = 0.400; p< 0.001) and a strong association - between MMP-1 (ρ = 0.825; p< 0.001) and MMP-14 (ρ = 0.736; p< 0.001).
In the INOCA/ANOCA group, there were observed moderate correlations of miR-145 with VEGF (ρ = 0.442; p = 0.013) and TNF-a (negative relationship, ρ = - 0.386; p = 0.032) and a strong negative linkage with MMP-13 (ρ = - 0.729; p< 0.001). Moderate positive association of miR-222 with VEGF (ρ = 0.414; p = 0.021), a significant correlation with MMP-1 (ρ = 0.652; p < 0.001) and a strong correlation with MMP-14 (ρ = 0.701; p < 0.001) were also found.
In the obstructive CAD group, a significant correlation of miR-145 with VEGF (ρ = 0.584; p < 0.001) and a strong negative association with MMP-13 (ρ = - 0.380; p = 0.002) were observed. In addition, a moderate association of miRNA-222 with TNF-a (ρ = 0.363; p = 0.004) and a significant correlation with VEGF (ρ = 0.595; p < 0.001), as well as a strong linkage with MMP-1 (ρ = 0.726; p < 0.001) and with MMP-14 (ρ = 0.727; p < 0.001) were demonstrated.
Univariate logistic regression determined expressions of miR-145 as significant predictors of INOCA/ANOCA. The results of univariate logistic regression are presented in Table 4.
Multivariate regression analysis allowed to obtain a mathematical model predicting the type of CA lesion. Table 5 demonstrates that miRNA-145 is significant independent predictor of INOCA/ANOCA.
This ROC curve predicts non-obstructive CA lesions in patients with stable CAD (cut-off = 0.48) with sensitivity 77.8% [50.0; 100.0]%, specificity 78.9% [62.5; 93.3]%, ROC-AUC = 77.8% [60.2; 93.8]%. If the cut-off is >0.48, then we can assume the probability of INOCA/ANOCA (Figure 3).
3. Discussion
The development and progression of CA atherosclerosis in stable CAD is influenced by many independent factors that play a crucial role in the formation of different variants of CA lesion. One of these factors is angiogenesis, in the regulation of which VEGF is actively involved. There are six variants of VEGF, each has structurally similar proteins included in the regulation and differentiation of the vascular system. In the previous studies, it has been demonstrated that VEGF can influence plaque growth and instability through angiogenesis-independent processes [24,25].
It is known that in metabolic syndrome, the activity of angiogenesis processes in CA may be reduced, despite the increased expression of VEGF, which is associated with an altered VEGF signaling pathway – VEGF/VEGFR signaling [26] VEGF is involved not only in angiogenesis, stimulating the proliferation and growth of endothelial cells, but also affects pro-inflammatory cytokines and cells: it increases the levels of TNF-α and IL-1 in monocytes and reduces IL-6. Similar results were obtained in our study in plasma samples with obstructive CAD [27].
TNF-α is mainly produced by activated macrophages and many other types of cells. Recent studies have demonstrated that TNF-α and VEGFA gene expression was significantly lower in patients with INOCA compared to patients with obstructive CAD [28].
In addition, VEGF induces the expression of MMP-1, MMP-3 and MMP-13 [29]. Changes in MMP levels may also be associated with an increased risk of CAD and various severity of the disease. Our study revealed significant differences between levels of MMP-9 and MMP-14 in samples with obstructive CAD and INOCA/ANOCA compared with the control group. Direct correlations of VEGF with MMP-1, MMP-9 and MMP-14 were found in obstructive CA lesions, and only MMP-1 and MMP-14 non–obstructive ones.
According to Buchler A., et al. and Quillard T., et al., increased expression of activated MMP-13 is associated with increased collagenolysis in vivo, which accelerates vascular remodeling processes in atherosclerotic lesions [17,30]. In the study of Gaubatz J. W. et al. a positive relationship between plasma levels of MMP-1 and calcification of the carotid arteries was revealed [31]. At the same time, although in the study Polonskaya Y.V. et al. the levels of MMP-1 and MMP-9 were higher in calcified plaques. According to logistic regression analysis, the relative risk of calcification formation in the CA was associated only with MMP-9 [32].
MMP-9 is a strong predictor of plaque instability, whereas MMP-13 can act in both ways: in the early stages of atherosclerosis, MMP-13 cleaves ICAM-1, thereby preventing the adhesion of circulating monocytes to the lesion site [33], while in the later stages MMP-13 promotes degradation of the extracellular matrix, thus leading to plaque destabilization [30,34].
Currently, the role of MMP-14 in the development of CAD has been proven in many studies. Thus, high levels of MMP-14 were independently associated with CVD [35]. Increased expression of MMP-14 was detected by Johnson J.L. et al. in the foamy cells of unstable atherosclerotic plaques [36].
In our study the absence of significant differences between the groups in MMP-1 and MMP-13 levels may be due to the fact that MMP activity was determined only in stable CAD and inclusion of a group with ACS may help reveal these differences.
It has been established that miRs are involved in the regulation of various processes, among which the most important in atherogenesis are endothelial damage, inflammation development, activation of macrophages, the formation of foam cells in the vascular wall, proliferation, migration and apoptosis of SMCs, and, as a consequence, vascular remodeling [16,37].
In the present study, the level of expression of miR-145 in the groups significantly differed and reached the highest values in patients with INOCA/ANOCA. It should be noted that a negative high-strength correlation was found between miR-145 and MMP-13. According to available scientific data, miR-145-5p can act as a “cardioprotective” molecule in patients with myocardial ischemia and, through negative regulation of CD40, is involved in reducing the activity of the inflammatory response and apoptosis caused by hypoxia [38]. Overexpression of miR-145 can eliminate endothelial damage and reduce the activity of abnormal inflammation, which makes it possible to consider this miR as a potential candidate for targeted therapy of ACS [22].
Non-obstructive and obstructive phenotypes of CAD can be united by the presence of endothelial dysfunction. It can be hypothesized that INOCA/ANOCA represents an initial stage in the progression of classical CAD. The anti-atherogenic miRNA-145 may function as part of a compensatory mechanism protecting vascular walls against stenotic atherosclerosis.
In the study of Wu S. et al., a negative relationship between miR-145 expression and levels of vWF, H-FABP, IL-6 and TNF-α was demonstrated. Thus, the authors concluded that the reduced expression of miR-145 in serum can serve as a potential diagnostic biomarker of ACS [22]. In our study, similar results were obtained in INOCA/ANOCA group: a moderate negative correlation between miR-145 and TNF-a was revealed. According to the work of Zhang X. et al., miR-145-5p expression was reduced in blood samples and arterial walls of patients with stenotic atherosclerosis of the coronary arteries [39]. Kumar A. et al. found that lower levels of miR-145 and miR-155, along with endothelial dysfunction, were associated with the severity of CKD and were associated with a higher risk of CVD development [40]. Thus, our data support the assumption that a lower level of miR-145 expression in obstructive CAD, in contrast to INOCA, may be associated with a more severe atherosclerotic lesion of the CA.
As for the analysis of miR-34a, the minimal level of expression of this miR was observed in the control group, represented by healthy volunteers without CVD risk factors, while in obstructive and non-obstructive CA lesions the expression was significantly higher. Similar results were obtained by Gatsiou, A. et al.: high miR-34a levels were independently associated with the presence of CAD, while simultaneous high expression of miR-34-a/c or all three miR-34a/b/c was associated with increased stiffness of aorta [41].
MiR-34a promotes downregulation of SIRT1 and VEGF protein expression, causing disruption of angiogenesis processes and inducing cell death [19]. A study of the role of miR-21, -34a, -146a, -146b-5p and -210 demonstrated a significant increase in their expression in atherosclerotic plaques compared to intact arteries [42]. All these data confirm a significant upregulation in miR-34a expression levels in the plasma of patients with CAD compared with the control group [43].
Similar results were obtained when studying miR-222, the expression of which was significantly higher in both study groups when compared with the control. According to available scientific data, miR-222 also takes part in atherogenesis, being involved in the regulation of many processes. MiR-221/222 and miR-155 suppress the inflammatory response induced by angiotensin II in endothelial cells, affecting the transcription factor Ets-1 and the genes vascular cell adhesion molecule 1 (VCAM-1) and monocyte chemoattractant protein-1 (MCP1) [44]. Overexpression of miR-19b-3p, miR-221-3p, and miR-222-3p induced by inflammatory cytokines TNF-α and IFNγ resulted in intracellular ROS accumulation, leading to cell apoptosis [45]. In obstructive CAD a moderate association between miR-222 and TNF-α expression was found, as well as a high-strength correlation with MMP-1 and MMP-14 [46]. Karere G.M. et al. identified vascular miRs expressed in baboons and humans and potential novel miRs associated with atherosclerosis. The expression of miR-144-3p, miR-146a-5p, miR-21, miR-221/222-3p was increased in fibrous plaques, while miR-195-5p was decreased. These results indicate that some miRs are not only lesion type specific but also exhibit differential expression at different stages of the disease, indicating their importance in the initiation and progression of atherosclerosis [47].
In our study potential non-invasive diagnostic marker of stable CAD were found among investigated miRs. Based on the results of the multivariate regression analysis, we can assume miR-145 as independent predictors of the non-obstructive phenotype of stable CAD.
In accordance with the results of the ROC analysis, it was concluded that various miRs can be considered as potential diagnostic noninvasive markers of CAD. Multivariate logistic regression analysis revealed that levels of circulating miR-145 and miR-155 were associated with CAD and may be powerful markers for detecting CAD [48]. O'Sullivan et. al. concluded that four miRNAs (miR-15a-5p, miR-146a-5p, miR-16-5p, and miR-93-5p) were predictors of the stable CAD development [49]. Zhang et. al. suggested another miRs (miR-29a-3p, miR-574-3p, and miR-574-5p with AUCs 0.83, 0.792, and 0.789, respectively) as potential markers for noninvasive diagnosis of CAD [50]. Recent data suggest that plasma levels of miR-23b and miR-143 could be useful as noninvasive biomarkers of in-stent restenosis [51]. Gholipour, A. et al. established potential suitability of miR-6721-5p as a biomarker for CAD [52].
Our results can be useful in comprehension of potential roles of miRs and we are planning to continue further studies on the mechanisms of epigenetic regulation of the pathogenesis of different phenotypes of CAD. Investigation of the pathogenesis of atherosclerotic CA lesions may be important for determining the potential role of miRs as possible diagnostic biomarkers and in development of new treatment methods using antagomiRs. It is necessary to continue careful study and fundamental research to solve this complicated problem.
4. Materials and Methods
4.1. Patient Population
A cross-sectional observational study included 127 subjects, who were eligible according to the inclusion criteria and signed informed consent from 2020 to 2024. The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethic Committee of the Sechenov University (Number: 01–21, 22 January 2021). The study included men and women aged 45–75 years with a verified CAD diagnosis.
The myocardial ischemia in hospitalized patients with stable angina or its analogs was confirmed by using instrumental diagnostic methods, namely stress echocardiography (echo-CG) or single-photon emission computed tomography (myocardial scintigraphy), against the background of the exercise testing. Depending on the results of coronary angiogram (CAG) or multispiral computed tomography (CT), the patients were divided into two groups: 51 patients with non-obstructive CA lesions (stenosis <50% or unchanged CA); 76 patients with obstructive CAD (presence of hemodynamically significant CA stenosis). The control group (n = 30) included healthy volunteers without CVD and risk factors. Exclusion criteria were the following: diabetes mellitus, acute coronary syndrome, myocardial infarction, and stroke in the previous 3 months, chronic heart failure III-IV functional class (NYHA), autoimmune and oncological diseases, signs and symptoms of liver disease in the decompensation stage, portal hypertension, uncontrolled bronchial asthma and chronic obstructive pulmonary disease, gastric or duodenal ulcer in the exacerbation stage, chronic pancreatitis in the exacerbation stage, malignant neoplasms, thyroid diseases, Cushing’s syndrome, acute renal failure, terminal renal failure (GFR < 15 mm/min/1.73 m2 ), mental illness, alcoholism, drug addiction, substance abuse, pregnancy, and breastfeeding.
4.2. Collection of Blood Samples and ELISA
Blood plasma samples were collected in tubes with EDTA K3 as an anticoagulant, centrifuged for 20 min at 1000 × g (1000 RCF), and further frozen in cryotubes at −80 ◦ C. To estimate the MMPs levels, VEGF and TNF-α enzyme immunoassay (ELISA) was performed on the ELISA analyzer Adaltis Personal Lab (Rome, Italy) using Wuhan Fine Biotech Co., Ltd. kits (Wuhan, Hubei, China) (catalogue numbers: Cat. No.: EH0232, EH0238, EH0234, EH0369, EH0302, EH0327). The coefficient of variation (CV) for the sets was 10% and 12%, respectively. All patients have undergone standard biochemical tests, including indicators of the lipid spectrum, glucose, and uric acid.
4.3. RNA Extraction and Reverse Transcription-Polymerase Chain Reaction (RT-PCR) Assay
Blood total RNA, including miRNA, was extracted from samples using Qiazol (Qiagen, Germany) following the manufacturers’ protocols. The concentration and purity of the obtained RNA were estimated on the NanoDrop 2000 microvolume spectrophotometer (Thermo Fisher Scientific, Waltham, MA, USA). The process of extraction was repeated for each sample until a sufficient amount of RNA was obtained for the next steps.
cDNA was synthesized using MiScript II RT Kit (Qiagen, Hilden, Germany) according to the recommended protocol. To obtain cDNA, 300 ng of total RNA isolated from each sample was used.
The expression level for each analyzed miRNA and the control was quantified in three repetitions on the CFX96 Real-Time PCR Detection System (Bio-Rad, Hercules, CA, USA) by using the MiScript SYBR Green PCR Kit (Qiagen, Hilden, Germany; Catalogue number: 218073) according to the manufacturer’s recommended program (15 min at 95 ◦ C, followed by 40 cycles of 94 ◦ C for 15 s, 55 ◦ C for 30 s, and 70 ◦ C for 30 s). Primers for miRNAs were designed according to the instructions [53] and their sequences are listed in Table 6. The presynthesized MiScript Primer Assay (Ce_miR-39_1, identification code MS00019789, Qiagen, Germany) was used for the control. The obtained Ct values were normalized to the exogenous control cel-miR-39-3p and analyzed using the 2−∆Ct method. The results are presented as REU (relative units of expression).
4.4. Statistical Analysis
Statistical analysis of the results was performed using the program StatTech v.v. 3.1.10 (StatTech, Russia) and the free Python computing software environment (v.3.11). The normality of sample distribution was evaluated using the Shapiro–Wilk (n < 50) or Kolmogorov-Smirnov (n > 50) tests. Quantitative variables with normal distribution were described using arithmetic averages (M) and standard deviations (SD) with a 95% confidence interval (95% CI). When the distribution of variables differed from the normal, quantitative data were described using the median (Me) and the lower and upper quartiles (Q1; Q3). The two groups were compared quantitatively with an abnormal distribution using the Mann-Whitney U-test. Three or more groups were compared quantitatively with an abnormal distribution using the Kruskal–Wallis test; the post-hoc testing was performed using the Dunn test with Bonferroni adjustment. To estimate the diagnostic significance of quantitative variables in predicting a certain outcome, the ROC curve analysis method was used. The cut-off value of the quantitative variable was determined to correspond to the maximum Youden index.
Multiple logistic regression (MLR) was used to build a model for predicting the presence/absence of a characteristic. The choice of the method was based on the dichotomy of the dependent variable and the fact that independent variables characterize both categorical and quantitative characteristics. The independent variables were selected by step-by-step reverse selection using Wald statistics as an exclusion criterion. The statistical significance of the obtained model was determined using the criterion χ 2. To balance the training dataset for a more stable predictive model, the SMOTE (Synthetic Minority Over-sampling Technique) method was employed. To estimate the quality of the constructed model, the following criteria were used: ROC-AUC, accuracy, sensitivity, specificity, and DCA analysis (decision curve analysis). Metrics were calculated together with 95% CI. The 95% CI was calculated using the bootstrap method with a sample of 1000 instances. The threshold value was chosen in accordance with the maximization of sensitivity and specificity.
5. Conclusions
The aim of this study was to evaluate the expression levels of miR-34a, miR-145, and miR-222, TNF-α, MMP-1, -9, -13, -14, and VEGF to search for possible diagnostic markers of different phenotypes of CAD. Changes in MMP levels may be associated with an increased risk of the development of CAD and varying severity of the disease. In our study, significant differences in MMP-9 and MMP-14 levels were found compared to the control group, with MMP-9 levels significantly different between the groups with obstructive CAD and INOCA/ANOCA. Direct correlations of VEGF with MMP-1, MMP-9 and MMP-14 were found in obstructive CAD, and only MMP-1 and MMP-14 in INOCA/ANOCA.
MiRs can be considered as potential diagnostic markers of stable CAD. The expression level of miR-34a and miR-222 was significantly higher in all patients with CAD (obstructive and INOCA/ANOCA) in comparison with the control group, while the expression of miR-145 was significantly higher in the INOCA group than in the control. The multivariate regression analysis allowed us to obtain a model that can predicting the phenotype of stable CAD with high sensitivity and specificity. MiR-145 can be used as predictor of INOCA/ANOCA.
Author Contributions
Conceptualization, Y.N.B. and A.O.I.; methodology, I.V.B.; software, N.N.P.; validation, M.V.N. and I.V.B.; formal analysis, N.N.P.; investigation, N.N.P., O.A.S., I.V.B.; resources, M.V.N., I.V.B.; data curation, N.N.P.; writing—original draft preparation, A.O.I., N.N.P., O.A.S., N.V.K.; writing—review and editing, M.V.N. and E.V.P.; visualization, N.N.P.; supervision, A.O.I.; project administration, Y.N.B.; funding acquisition, Y.N.B. All authors have read and agreed to the published version of the manuscript.
Funding
The study was financially supported by the Russian Science Foundation in the form of scientific project No. 22-15-00424, a scientific grant «The role of activation of the WNT signaling cascade, the processes of its epigenetic regulation and immune-mediated inflammation in the progression of atherosclerosis and the possibility of influencing it by therapeutic neoangiogenesis in patients with stable coronary heart disease».
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Sechenov University (Number: 01–21, 22 January 2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available because some data sets will be used for further research.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Ralapanawa, U.; Sivakanesan, R. Epidemiology and the Magnitude of Coronary Artery Disease and Acute Coronary Syndrome: A Narrative Review. J Epidemiol Glob Health 2021, 11, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Silva, S.; Fatumo, S.; Nitsch, D. Mendelian Randomization Studies on Coronary Artery Disease: A Systematic Review and Meta-Analysis. Syst Rev 2024, 13, 29. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, H.R.; Diaz, A.; Cyr, D.D.; Shaw, L.J.; Mancini, G.B.J.; Leipsic, J.; Budoff, M.J.; Min, J.K.; Hague, C.J.; Berman, D.S.; et al. Ischemia With Nonobstructive Coronary Arteries: Insights From the ISCHEMIA Trial. JACC Cardiovasc Imaging 2023, 16, 63–74. [Google Scholar] [CrossRef] [PubMed]
- Pepine, C.J.; Ferdinand, K.C.; Shaw, L.J.; Light-McGroary, K.A.; Shah, R.U.; Gulati, M.; Duvernoy, C.; Walsh, M.N.; Bairey Merz, C.N. Emergence of Nonobstructive Coronary Artery Disease: A Woman’s Problem and Need for Change in Definition on Angiography. J Am Coll Cardiol 2015, 66, 1918–1933. [Google Scholar] [CrossRef]
- Mileva, N.; Nagumo, S.; Mizukami, T.; Sonck, J.; Berry, C.; Gallinoro, E.; Monizzi, G.; Candreva, A.; Munhoz, D.; Vassilev, D.; et al. Prevalence of Coronary Microvascular Disease and Coronary Vasospasm in Patients With Nonobstructive Coronary Artery Disease: Systematic Review and Meta-Analysis. J Am Heart Assoc 2022, 11, e023207. [Google Scholar] [CrossRef]
- Chang, A.; Kang, N.; Chung, J.; Gupta, A.R.; Parwani, P. Evaluation of Ischemia with No Obstructive Coronary Arteries (INOCA) and Contemporary Applications of Cardiac Magnetic Resonance (CMR). Medicina (Kaunas) 2023, 59. [Google Scholar] [CrossRef]
- Jespersen, L.; Hvelplund, A.; Abildstrøm, S.Z.; Pedersen, F.; Galatius, S.; Madsen, J.K.; Jørgensen, E.; Kelbæk, H.; Prescott, E. Stable Angina Pectoris with No Obstructive Coronary Artery Disease Is Associated with Increased Risks of Major Adverse Cardiovascular Events. Eur Heart J 2012, 33, 734–744. [Google Scholar] [CrossRef]
- Karakayali, M.; Altunova, M.; Yakisan, T.; Aslan, S.; Omar, T.; Artac, I.; Ilis, D.; Arslan, A.; Cagin, Z.; Karabag, Y.; et al. The Relationship between the Systemic Immune-Inflammation Index and Ischemia with Non-Obstructive Coronary Arteries in Patients Undergoing Coronary Angiography. Arq Bras Cardiol 2024, 121, e20230540. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.-D.; Wen, Z.-G.; Long, J.-J.; Wang, Y. Association Between Systemic Inflammation Response Index and Slow Coronary Flow Phenomenon in Patients with Ischemia and No Obstructive Coronary Arteries. Int J Gen Med 2024, 17, 4045–4053. [Google Scholar] [CrossRef]
- Beatty, C.; Richardson, K.P.; Tran, P.M.H.; Satter, K.B.; Hopkins, D.; Gardiner, M.; Sharma, A.; Purohit, S. Multiplex Analysis of Inflammatory Proteins Associated with Risk of Coronary Artery Disease in Type-1 Diabetes Patients. Clin Cardiol 2024, 47, e24143. [Google Scholar] [CrossRef]
- Hu, Q.; Ecker, M. Overview of MMP-13 as a Promising Target for the Treatment of Osteoarthritis. Int J Mol Sci 2021, 22. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Carracedo, R.; Hernández, I.; Moreno-Gómez-Toledano, R.; Díez-Mata, J.; Tesoro, L.; González-Cucharero, C.; Jiménez-Guirado, B.; Alcharani, N.; Botana, L.; Saura, M.; et al. NOS3 Prevents MMP-9, and MMP-13 Induced Extracellular Matrix Proteolytic Degradation through Specific MicroRNA-Targeted Expression of Extracellular Matrix Metalloproteinase Inducer in Hypertension-Related Atherosclerosis. J Hypertens 2024, 42, 685–693. [Google Scholar] [CrossRef] [PubMed]
- Parks, W.C.; Shapiro, S.D. Matrix Metalloproteinases in Lung Biology. Respir Res 2001, 2, 10–19. [Google Scholar] [CrossRef]
- Hey, S.; Linder, S. Matrix Metalloproteinases at a Glance. J Cell Sci 2024, 137. [Google Scholar] [CrossRef]
- Ramirez-Carracedo, R.; Tesoro, L.; Hernandez, I.; Diez-Mata, J.; Filice, M.; Toro, R.; Rodriguez-Piñero, M.; Zamorano, J.L.; Saura, M.; Zaragoza, C. Non-Invasive Detection of Extracellular Matrix Metalloproteinase Inducer EMMPRIN, a New Therapeutic Target against Atherosclerosis, Inhibited by Endothelial Nitric Oxide. Int J Mol Sci 2018, 19. [Google Scholar] [CrossRef]
- Maitrias, P.; Metzinger-Le Meuth, V.; Nader, J.; Reix, T.; Caus, T.; Metzinger, L. The Involvement of MiRNA in Carotid-Related Stroke. Arterioscler Thromb Vasc Biol 2017, 37, 1608–1617. [Google Scholar] [CrossRef]
- Buchler, A.; Munch, M.; Farber, G.; Zhao, X.; Al-Haddad, R.; Farber, E.; Rotstein, B.H. Selective Imaging of Matrix Metalloproteinase-13 to Detect Extracellular Matrix Remodeling in Atherosclerotic Lesions. Mol Imaging Biol 2022, 24, 93–103. [Google Scholar] [CrossRef]
- Lehrke, M.; Greif, M.; Broedl, U.C.; Lebherz, C.; Laubender, R.P.; Becker, A.; von Ziegler, F.; Tittus, J.; Reiser, M.; Becker, C.; et al. MMP-1 Serum Levels Predict Coronary Atherosclerosis in Humans. Cardiovasc Diabetol 2009, 8, 50. [Google Scholar] [CrossRef] [PubMed]
- Reddy, S.; Hu, D.-Q.; Zhao, M.; Ichimura, S.; Barnes, E.A.; Cornfield, D.N.; Alejandre Alcázar, M.A.; Spiekerkoetter, E.; Fajardo, G.; Bernstein, D. MicroRNA-34a-Dependent Attenuation of Angiogenesis in Right Ventricular Failure. J Am Heart Assoc 2024, 13, e029427. [Google Scholar] [CrossRef]
- Li, Q.; Kim, Y.-R.; Vikram, A.; Kumar, S.; Kassan, M.; Gabani, M.; Lee, S.K.; Jacobs, J.S.; Irani, K. P66Shc-Induced MicroRNA-34a Causes Diabetic Endothelial Dysfunction by Downregulating Sirtuin1. Arterioscler Thromb Vasc Biol 2016, 36, 2394–2403. [Google Scholar] [CrossRef]
- Wu, J.; Liang, W.; Tian, Y.; Ma, F.; Huang, W.; Jia, Y.; Jiang, Z.; Wu, H. Inhibition of P53/MiR-34a Improves Diabetic Endothelial Dysfunction via Activation of SIRT1. J Cell Mol Med 2019, 23, 3538–3548. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Sun, H.; Sun, B. MicroRNA-145 Is Involved in Endothelial Cell Dysfunction and Acts as a Promising Biomarker of Acute Coronary Syndrome. Eur J Med Res 2020, 25, 2. [Google Scholar] [CrossRef] [PubMed]
- Qin, B.; Cao, Y.; Yang, H.; Xiao, B.; Lu, Z. MicroRNA-221/222 Regulate Ox-LDL-Induced Endothelial Apoptosis via Ets-1/P21 Inhibition. Mol Cell Biochem 2015, 405, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Couffinhal, T.; Kearney, M.; Witzenbichler, B.; Chen, D.; Murohara, T.; Losordo, D.W.; Symes, J.; Isner, J.M. Vascular Endothelial Growth Factor/Vascular Permeability Factor (VEGF/VPF) in Normal and Atherosclerotic Human Arteries. Am J Pathol 1997, 150, 1673–1685. [Google Scholar] [PubMed]
- Mao, Y.; Liu, X.Q.; Song, Y.; Zhai, C.G.; Xu, X.L.; Zhang, L.; Zhang, Y. Fibroblast Growth Factor-2/Platelet-Derived Growth Factor Enhances Atherosclerotic Plaque Stability. J Cell Mol Med 2020, 24, 1128–1140. [Google Scholar] [CrossRef]
- Bartkowiak, K.; Bartkowiak, M.; Jankowska-Steifer, E.; Ratajska, A.; Kujawa, M.; Aniołek, O.; Niderla-Bielińska, J. Metabolic Syndrome and Cardiac Vessel Remodeling Associated with Vessel Rarefaction: A Possible Underlying Mechanism May Result from a Poor Angiogenic Response to Altered VEGF Signaling Pathways. J Vasc Res 2024, 61, 151–159. [Google Scholar] [CrossRef]
- Zhao, Q.; Egashira, K.; Inoue, S.; Usui, M.; Kitamoto, S.; Ni, W.; Ishibashi, M.; Hiasa Ki, K.; Ichiki, T.; Shibuya, M.; et al. Vascular Endothelial Growth Factor Is Necessary in the Development of Arteriosclerosis by Recruiting/Activating Monocytes in a Rat Model of Long-Term Inhibition of Nitric Oxide Synthesis. Circulation 2002, 105, 1110–1115. [Google Scholar] [CrossRef]
- Bonanni, A.; d’Aiello, A.; Pedicino, D.; Di Sario, M.; Vinci, R.; Ponzo, M.; Ciampi, P.; Lo Curto, D.; Conte, C.; Cribari, F.; et al. Molecular Hallmarks of Ischemia with Non-Obstructive Coronary Arteries: The “INOCA versus Obstructive CCS” Challenge. J Clin Med 2022, 11. [Google Scholar] [CrossRef]
- Pufe, T.; Harde, V.; Petersen, W.; Goldring, M.B.; Tillmann, B.; Mentlein, R. Vascular Endothelial Growth Factor (VEGF) Induces Matrix Metalloproteinase Expression in Immortalized Chondrocytes. J Pathol 2004, 202, 367–374. [Google Scholar] [CrossRef]
- Quillard, T.; Tesmenitsky, Y.; Croce, K.; Travers, R.; Shvartz, E.; Koskinas, K.C.; Sukhova, G.K.; Aikawa, E.; Aikawa, M.; Libby, P. Selective Inhibition of Matrix Metalloproteinase-13 Increases Collagen Content of Established Mouse Atherosclerosis. Arterioscler Thromb Vasc Biol 2011, 31, 2464–2472. [Google Scholar] [CrossRef]
- Gaubatz, J.W.; Ballantyne, C.M.; Wasserman, B.A.; He, M.; Chambless, L.E.; Boerwinkle, E.; Hoogeveen, R.C. Association of Circulating Matrix Metalloproteinases with Carotid Artery Characteristics: The Atherosclerosis Risk in Communities Carotid MRI Study. Arterioscler Thromb Vasc Biol 2010, 30, 1034–1042. [Google Scholar] [CrossRef]
- Polonskaya, Y. V; Kashtanova, E. V; Murashov, I.S.; Striukova, E. V; Kurguzov, A. V; Stakhneva, E.M.; Shramko, V.S.; Maslatsov, N.A.; Chernyavsky, A.M.; Ragino, Y.I. Association of Matrix Metalloproteinases with Coronary Artery Calcification in Patients with CHD. J Pers Med 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Tarín, C.; Gomez, M.; Calvo, E.; López, J.A.; Zaragoza, C. Endothelial Nitric Oxide Deficiency Reduces MMP-13-Mediated Cleavage of ICAM-1 in Vascular Endothelium: A Role in Atherosclerosis. Arterioscler Thromb Vasc Biol 2009, 29, 27–32. [Google Scholar] [CrossRef] [PubMed]
- Deguchi, J.-O.; Aikawa, E.; Libby, P.; Vachon, J.R.; Inada, M.; Krane, S.M.; Whittaker, P.; Aikawa, M. Matrix Metalloproteinase-13/Collagenase-3 Deletion Promotes Collagen Accumulation and Organization in Mouse Atherosclerotic Plaques. Circulation 2005, 112, 2708–2715. [Google Scholar] [CrossRef]
- Melin, E.O.; Dereke, J.; Hillman, M. Galectin-3, Metalloproteinase-2 and Cardiovascular Disease Were Independently Associated with Metalloproteinase-14 in Patients with Type 1 Diabetes: A Cross Sectional Study. Diabetol Metab Syndr 2021, 13, 118. [Google Scholar] [CrossRef] [PubMed]
- Johnson, J.L.; Jenkins, N.P.; Huang, W.-C.; Di Gregoli, K.; Sala-Newby, G.B.; Scholtes, V.P.W.; Moll, F.L.; Pasterkamp, G.; Newby, A.C. Relationship of MMP-14 and TIMP-3 Expression with Macrophage Activation and Human Atherosclerotic Plaque Vulnerability. Mediators Inflamm 2014, 2014, 276457. [Google Scholar] [CrossRef]
- Lu, Y.; Thavarajah, T.; Gu, W.; Cai, J.; Xu, Q. Impact of MiRNA in Atherosclerosis. Arterioscler Thromb Vasc Biol 2018, 38, e159–e170. [Google Scholar] [CrossRef] [PubMed]
- Yuan, M.; Zhang, L.; You, F.; Zhou, J.; Ma, Y.; Yang, F.; Tao, L. MiR-145-5p Regulates Hypoxia-Induced Inflammatory Response and Apoptosis in Cardiomyocytes by Targeting CD40. Mol Cell Biochem 2017, 431, 123–131. [Google Scholar] [CrossRef]
- Zhang, X.; Zai, L.; Tao, Z.; Wu, D.; Lin, M.; Wan, J. MiR-145-5p Affects Autophagy by Targeting CaMKIIδ in Atherosclerosis. Int J Cardiol 2022, 360, 68–75. [Google Scholar] [CrossRef]
- Kumar, A.; Priyadarshini, G.; Parameswaran, S.; Ramesh, A.; Rajappa, M. Evaluation of MicroRNA 145 and MicroRNA 155 as Markers of Cardiovascular Risk in Chronic Kidney Disease. Cureus 2024, 16, e66494. [Google Scholar] [CrossRef]
- Gatsiou, A.; Georgiopoulos, G.; Vlachogiannis, N.I.; Pfisterer, L.; Fischer, A.; Sachse, M.; Laina, A.; Bonini, F.; Delialis, D.; Tual-Chalot, S.; et al. Additive Contribution of MicroRNA-34a/b/c to Human Arterial Ageing and Atherosclerosis. Atherosclerosis 2021, 327, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Raitoharju, E.; Lyytikäinen, L.-P.; Levula, M.; Oksala, N.; Mennander, A.; Tarkka, M.; Klopp, N.; Illig, T.; Kähönen, M.; Karhunen, P.J.; et al. MiR-21, MiR-210, MiR-34a, and MiR-146a/b Are up-Regulated in Human Atherosclerotic Plaques in the Tampere Vascular Study. Atherosclerosis 2011, 219, 211–217. [Google Scholar] [CrossRef]
- Han, H.; Qu, G.; Han, C.; Wang, Y.; Sun, T.; Li, F.; Wang, J.; Luo, S. MiR-34a, MiR-21 and MiR-23a as Potential Biomarkers for Coronary Artery Disease: A Pilot Microarray Study and Confirmation in a 32 Patient Cohort. Exp Mol Med 2015, 47, e138. [Google Scholar] [CrossRef] [PubMed]
- Zhu, N.; Zhang, D.; Chen, S.; Liu, X.; Lin, L.; Huang, X.; Guo, Z.; Liu, J.; Wang, Y.; Yuan, W.; et al. Endothelial Enriched MicroRNAs Regulate Angiotensin II-Induced Endothelial Inflammation and Migration. Atherosclerosis 2011, 215, 286–293. [Google Scholar] [CrossRef] [PubMed]
- Xue, Y.; Wei, Z.; Ding, H.; Wang, Q.; Zhou, Z.; Zheng, S.; Zhang, Y.; Hou, D.; Liu, Y.; Zen, K.; et al. MicroRNA-19b/221/222 Induces Endothelial Cell Dysfunction via Suppression of PGC-1α in the Progression of Atherosclerosis. Atherosclerosis 2015, 241, 671–681. [Google Scholar] [CrossRef]
- Laffont, B.; Rayner, K.J. MicroRNAs in the Pathobiology and Therapy of Atherosclerosis. Can J Cardiol 2017, 33, 313–324. [Google Scholar] [CrossRef]
- Karere, G.M.; Glenn, J.P.; Li, G.; Konar, A.; VandeBerg, J.L.; Cox, L.A. Potential MiRNA Biomarkers and Therapeutic Targets for Early Atherosclerotic Lesions. Sci Rep 2023, 13, 3467. [Google Scholar] [CrossRef]
- Faccini, J.; Ruidavets, J.-B.; Cordelier, P.; Martins, F.; Maoret, J.-J.; Bongard, V.; Ferrières, J.; Roncalli, J.; Elbaz, M.; Vindis, C. Circulating MiR-155, MiR-145 and Let-7c as Diagnostic Biomarkers of the Coronary Artery Disease. Sci Rep 2017, 7, 42916. [Google Scholar] [CrossRef]
- O Sullivan, J.F.; Neylon, A.; McGorrian, C.; Blake, G.J. MiRNA-93-5p and Other MiRNAs as Predictors of Coronary Artery Disease and STEMI. Int J Cardiol 2016, 224, 310–316. [Google Scholar] [CrossRef]
- Zhang, L.; Zhang, Y.; Xue, S.; Ding, H.; Wang, Y.; Qi, H.; Wang, Y.; Zhu, W.; Li, P. Clinical Significance of Circulating MicroRNAs as Diagnostic Biomarkers for Coronary Artery Disease. J Cell Mol Med 2020, 24, 1146–1150. [Google Scholar] [CrossRef]
- Saavedra, N.; Rojas, G.; Herrera, J.; Rebolledo, C.; Ruedlinger, J.; Bustos, L.; Bobadilla, B.; Pérez, L.; Saavedra, K.; Zambrano, T.; et al. Circulating MiRNA-23b and MiRNA-143 Are Potential Biomarkers for In-Stent Restenosis. Biomed Res Int 2020, 2020, 2509039. [Google Scholar] [CrossRef] [PubMed]
- Gholipour, A.; Zahedmehr, A.; Arabian, M.; Shakerian, F.; Maleki, M.; Oveisee, M.; Malakootian, M. MiR-6721-5p as a Natural Regulator of Meta-VCL Is Upregulated in the Serum of Patients with Coronary Artery Disease. Noncoding RNA Res 2025, 10, 25–34. [Google Scholar] [CrossRef] [PubMed]
- Busk, P.K. A Tool for Design of Primers for MicroRNA-Specific Quantitative RT-QPCR. BMC Bioinformatics 2014, 15, 29. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The design of the study.
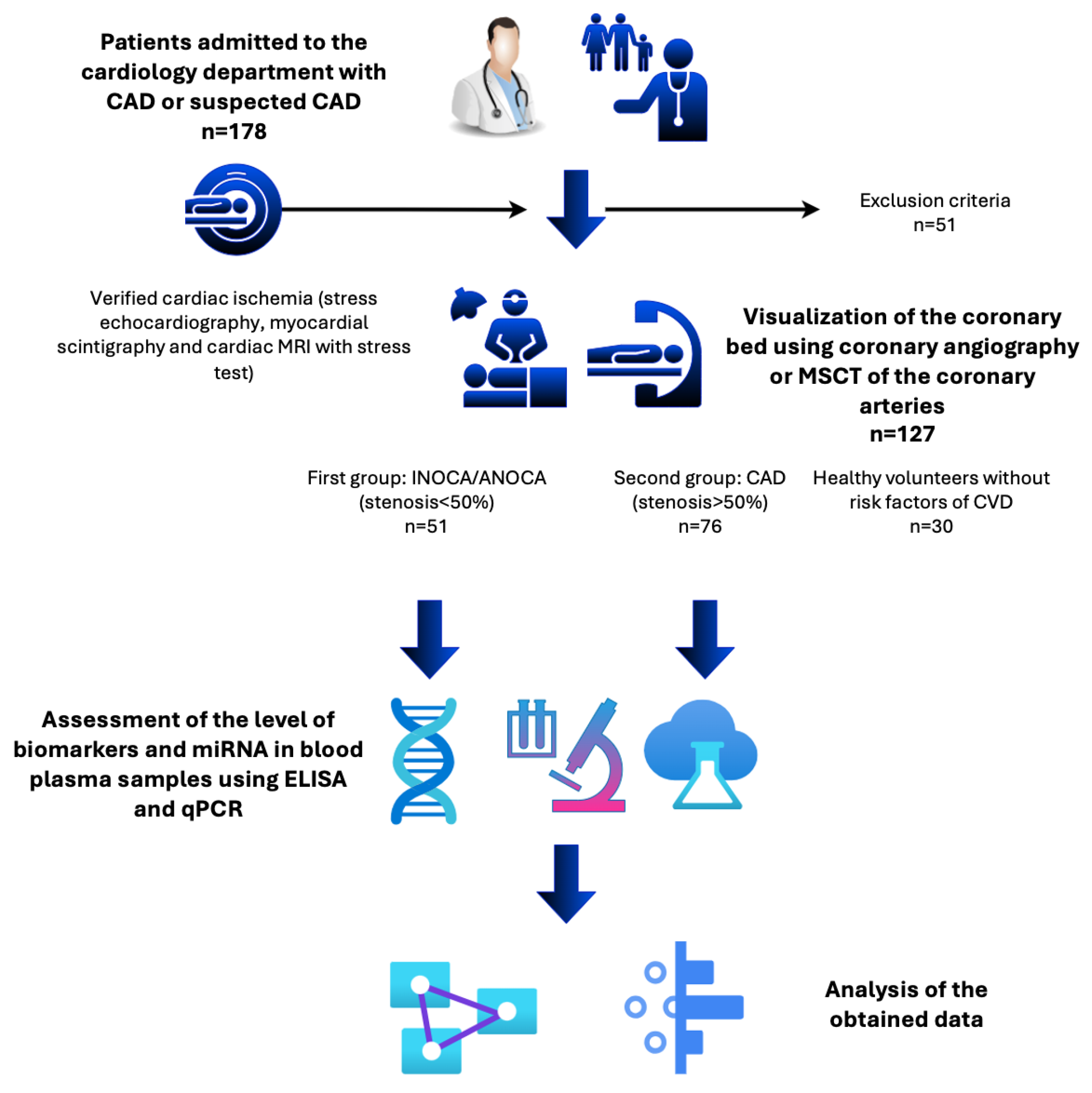
Figure 2.
MiRNAs expression in plasma of CAD patients and healthy volunteers (control). All values are presented as the median and CI. Statistically significant p < 0.05; CAD—coronary artery disease, INOCA/ANOCA—ischemia/angina with non-obstructive coronary arteries.
Figure 2.
MiRNAs expression in plasma of CAD patients and healthy volunteers (control). All values are presented as the median and CI. Statistically significant p < 0.05; CAD—coronary artery disease, INOCA/ANOCA—ischemia/angina with non-obstructive coronary arteries.
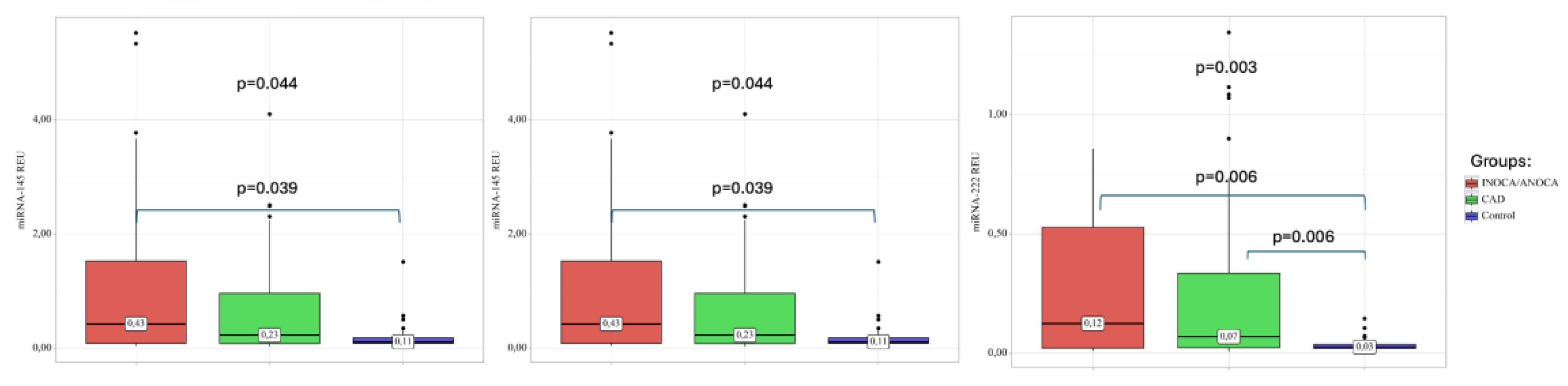
Figure 3.
ROC analysis of the model defining the risk of occurrence of INOCA/ANOCA.
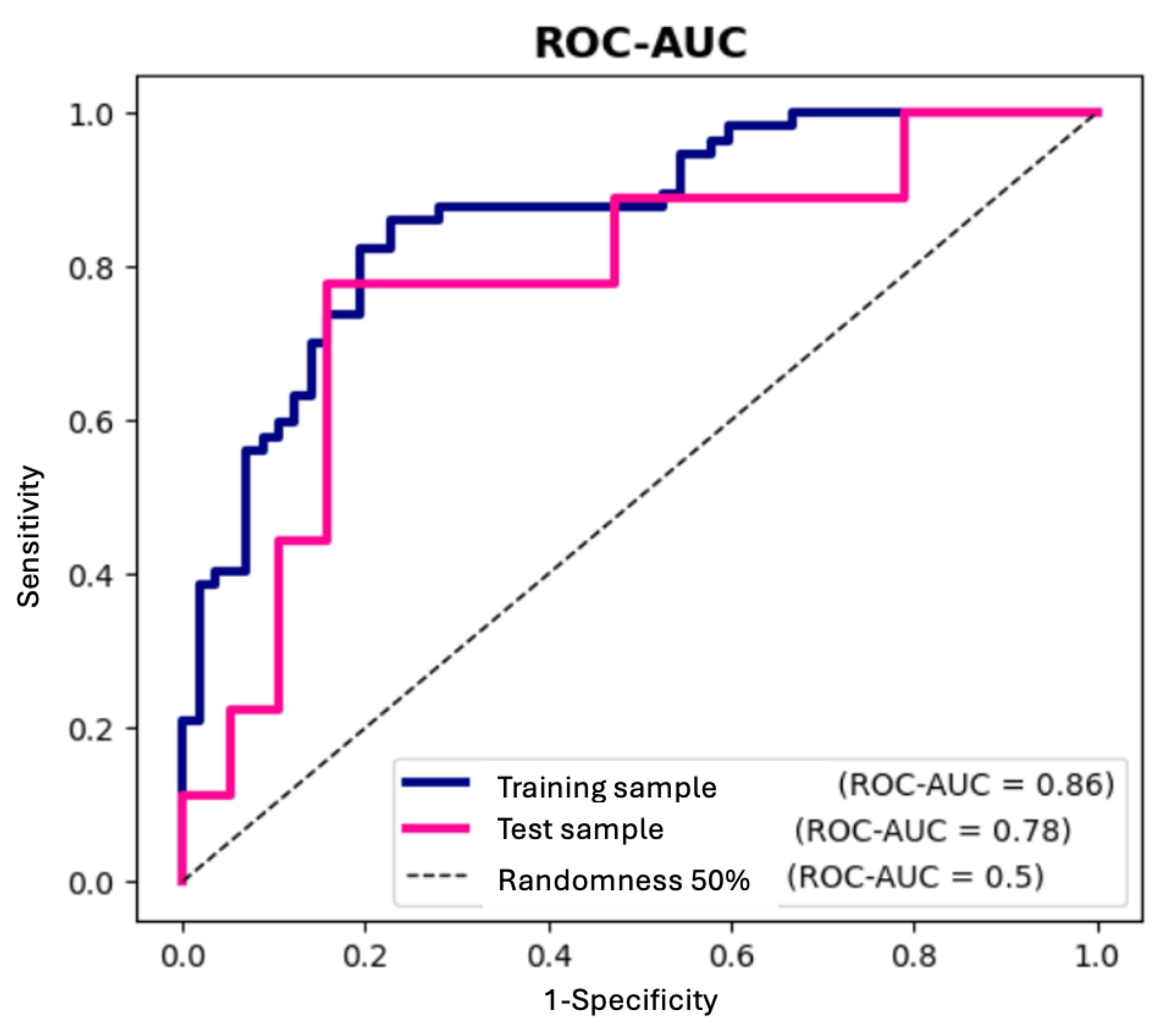

Table 1.
Basic clinical characteristics.
| All CAD (n=127) |
INOCA/ANOCA (n=51) |
Obstructive CAD (n=76) |
Control (n=30) |
p-value | |
|---|---|---|---|---|---|
| Men (%) | 71(57.4) | 20 (39.2) | 51 (67.1) | 10 (33.3) | 0.001* p INOCA/ANOCA – obstructive CAD = 0.004 p obstructive CAD – Control = 0.003 |
| Women (%) | 56(42.6) | 31 (60.8) | 25 (32.9) | 20 (66.7) | |
| Age (year) | 64 [59; 71] | 64 [59; 70.5] |
63 [56; 71] |
28.5 [26; 39.2] |
< 0.001* p control – INOCA/ANOCA < 0.001 p control – obstructive CAD < 0.001 |
| BMI (kg/m2) | 26.9 [24.9; 29.8] | 26.20 [25.67; 30.40] | 27.4 [24.77; 29.75] | 21.95 [20.75; 25.23] | < 0.001* p control – INOCA/ANOCA < 0.001 p control – obstructive CAD < 0.001 |
| Smoking (%) | 9 (7.8) | 3 (7.7) | 6 (7.9) | - | 0.953 |
| Hemoglobin (g/L) | 142 [133;152] | 142 [134;151] | 144 [133;152] | 136 [129;152] | 0.459 |
| Glucose (mmol/L) | 5.5 [5.17;5.8] | 5.53 [5.25; 5.81] | 5.43 [5.31; 5.54] | 4.9 [4.67; 5.35] | 0.005* pINOCA/ANOCA – Control = 0.011 pobstructive CAD – Control = 0.007 |
| Creatinine (µmol/L) | 89 [78.2;99.2] | 80.45 [72.08; 91.67] | 91.5 [81; 101.32] | 82 [77.7; 87] | 0.009* p INOCA/ANOCA – obstructive CAD = 0.023 |
| Total cholesterol (mmol/L) | 4.39[3.34; 4.77] | 4.45 [3.49; 5.36] | 3.79 [3.25; 4.36] | 4.94 [4.39; 5.52] | <0.001* p INOCA/ANOCA – obstructive CAD = 0.015 p obstructive CAD – Control < 0.001 |
| LDL (mmol/L) | 2.36 [1.85; 2.97] | 2.72 [2.03; 3.2] | 2.16 [1.58; 2.55] | 2.54 [2.28; 3.21] | 0.006* p obstructive CAD – INOCA/ANOCA = 0.016 p control – obstructive CAD = 0.044 |
| HDL (mmol/L) | 1.17 [1.04; 1.35] | 1.31 [1.03; 1.46] | 1.08 [1.08; 1.32] | 1.62 [1.35; 1.9] | <0.001* p control – INOCA/ANOCA = 0.021 p control – obstructive CAD < 0.001 |
*Statistically significant p < 0.05; n—number of patients in the group; CAD—coronary artery disease; INOCA/ANOCA—ischemia/angina with non-obstructive coronary arteries; BMI—body mass index; LDL—low density lipoproteins; HDL—high density lipoproteins.
Table 2.
CAD patients’ therapy characteristics.
| INOCA/ANOCA | obstructive CAD | p-value | |
|---|---|---|---|
| ACE inhibitors | 18 (35.3) | 47 (61.8) | 0.027* |
| ARB II | 17(33.3) | 20 (26.7) | 0.123 |
| Beta-blocker | 26 (86.7) | 53 (81.5) | 0.535 |
| Calcium channel blockers | 16 (53.3) | 24 (36.9) | 0.33 |
| Antiaggregants | 26 (66.7) | 62 (81.5) | 0.202 |
| Anticoagulants | 4 (10.2) | 7 (9.2) | 0.738 |
| Antiarrhythmic drugs | 3 (7.7) | 8 (10.5) | 1.000 |
| HMG-CoA reductase inhibitors | 29 (74.4) | 63 (82.9) | 0.539 |
INOCA/ANOCA—ischemia/angina with non-obstructive coronary arteries; ACE inhibitors—angiotensin-converting enzyme inhibitors; ARB II—angiotensin II receptor blockers.
Table 3.
The concentration of VEGF, TNF-α, and MMPs in plasma.
| Proteins | Groups | Concentration (Me [Q1 – Q3]) |
p-value |
|---|---|---|---|
| VEGF, ng/ml | INOCA/ANOCA | 41.66 [36.23 – 47.58] | 0.043* p INOCA/ANOCA – control = 0.036 |
| Obstructive CAD | 36.4 [13.12 – 66.05] | ||
| Control | 35.03 [10.50 – 41.62] | ||
| TNF-α, ng/ml | INOCA/ANOCA | 28.33 [13.97 – 29.74] | < 0.004* p control – obstructive CAD = 0.037 p INOCA/ANOCA– obstructive CAD = 0.03 |
| Obstructive CAD | 13.85 [10.76 – 25.30] | ||
| Control | 28.23 [14.17 – 28.73] | ||
| MMP-1, ng/ml | INOCA/ANOCA | 0.21 [0.17 – 0.29] | 0.161 |
| Obstructive CAD | 0.23 [0.21 – 0.23] | ||
| Control | 0.24 [0.22 – 0.32] | ||
| MMP-9 ng/ml | INOCA/ANOCA | 3.58 [1.98 – 6.18] | < 0.001* p obstructive CAD – INOCA/ANOCA < 0.001 |
| Obstructive CAD | 7.2 [4.25 – 10.68] | ||
| Control | 5.45 [4.02 – 6.81] | ||
| MMP-13, ng/ml | INOCA/ANOCA | 123.95 [68.85 – 285.43] | 0.055 |
| Obstructive CAD | 91.57 [49.77 – 339.51] | ||
| Control | 67.5 [47.79 – 111.30] | ||
| MMP-14, ng/ml | INOCA/ANOCA | 0.71 [0.29 – 1.04] | < 0.001* p obstructive CAD – control < 0.001 p control – INOCA = 0.02 |
| Obstructive CAD | 0.45 [0.26 – 0.78] | ||
| Control | 1.00 [0.75 – 1.31] |
*Statistically significant p < 0.05; CAD—coronary artery disease; INOCA/ANOCA—ischemia/angina with non-obstructive coronary arteries; VEGF – vascular endothelial growth factor; TNFα – tumor necrosis factor-α; MMP – matrix metalloproteinase.
Table 4.
Univariate logistic regression analysis for obstructive CAD and INOCA/ANOCA groups.
| Factor/Predictor | B | Exp (B) [95%CI] | p | Pseudo R-squ |
|---|---|---|---|---|
| Gender (male/female) | -1,409 | 0.244 [0.094, 0.636] | p=0.004* | 0.080 |
| Smoking (n) | 0,063 | 1.064 [0.244, 4.641] | p=0.933 | 0.000 |
| Hypertension (n) | 0,138 | 1.147 [0.210, 6.28] | p=0.874 | 0.000 |
| Dyslipidemia (n) | 0,323 | 1.381 [0.138, 13.85] | p=0.784 | 0.001 |
| Angina pain (n) | 0,642 | 1.899 [0.629, 5.736] | p=0.255 | 0.012 |
| Fasting glucose (mmol/L) | 0,018 | 1.018 [1.004, 1.033] | p=0.014* | 0.053 |
| Myocardial infarction (n) | -1,488 | 0.226 [0.077, 0.662] | p=0.007* | 0.073 |
| ACE inhibitors | -1,082 | 0.339 [0.138, 0.831] | p=0.018* | 0.049 |
| ARB II | 0,799 | 2.222 [0.876, 5.637] | p=0.093 | 0.024 |
| Beta blockers | 0,386 | 1.471 [0.432, 5.01] | p=0.536 | 0.003 |
| Calcium channel blocker | 0,669 | 1.952 [0.813, 4.691] | p=0.135 | 0.019 |
| Antiaggregant | -1,157 | 0.314 [0.066, 1.505] | p=0.148 | 0.018 |
| Statin | -0,776 | 0.460 [0.028, 7.619] | p=0.588 | 0.002 |
| Age (years) | 0,004 | 1.004 [0.953, 1.058] | p=0.871 | 0.000 |
| BMI (kg/m2) | 0,007 | 1.006 [0.903, 1.122] | p=0.905 | 0.000 |
| VEGF (ng/ml) | 0,000 | 1.000 [0.998, 1.001] | p=0.691 | 0.001 |
| TNF-a (ng/ml) | -0,002 | 0.998 [0.992, 1.004] | p=0.433 | 0.006 |
| MMP-1 (ng/ml) | -0,046 | 0.955 [0.587, 1.553] | p=0.853 | 0.000 |
| MMP-9 (ng/ml) | -0,044 | 0.957 [0.906, 1.011] | p=0.118 | 0.029 |
| MMP-13 (ng/ml) | 0,000 | 1.000 [1.000, 1.0] | p=0.972 | 0.000 |
| MMP-14 (ng/ml) | -0,025 | 0.975 [0.890, 1.07] | p=0.600 | 0.003 |
| miR-34a REU | -0,050 | 0.951 [0.869, 1.041] | p=0.274 | 0.010 |
| miR-145 REU | 0,444 | 1.558 [1.066, 2.277] | p=0.022* | 0.042 |
| miR-222 REU | 0,458 | 1.581 [0.422, 5.93] | p=0.497 | 0.003 |
Statistically significant p < 0.05; CAD—coronary artery disease, INOCA/ANOCA—ischemia/angina with non-obstructive coronary arteries; BMI—body mass index; ACE inhibitors—angiotensin-converting enzyme inhibitors; ARB II—angiotensin II receptor blockers; VEGF – vascular endothelial growth factor; TNFα – tumor necrosis factor-α; MMP – matrix metalloproteinase.
Table 5.
Multivariate logistic regression analysis for CAD and INOCA/ANOCA groups.
| Variables | coef (B) | Exp (B) | p |
|---|---|---|---|
| miR-145 REU | 0,921 | 2.512 [1.294, 4.875] | p=0.006* |
| Gender (male/female) | -1,116 | 0.328 [0.121, 0.889] | p=0.029* |
* Statistically significant p < 0.05.
Table 6.
Primer sequences for RT-PCR.
| Primer | Sequence |
|---|---|
| miR-34а | 5’- TGGCAGTGTCTTAGCTGGTTGT-3’ |
| miR-145 | 5’ - TCCAGTTTTCCCAGGAATCCCT - 3’ |
| miR-222 | 5’ - CTCAGTAGCCAGTGTAGATCCT - 3’ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



