
Submitted:
18 November 2024
Posted:
19 November 2024
You are already at the latest version
Abstract
The first part of this review highlighted the evolving landscape of atherosclerosis, noting emerging cardiometabolic risk factors, the growing impact of exposomes, and social determinants of health. The prominent role of atherosclerosis in the bidirectional relationship between cardiovascular disease and cancer was also discussed. In this second part, we examine the complex interplay between multimorbid cardio-oncologic patients, cardiometabolic risk factors, and the harmful environments that lend a “syndemic” nature to these chronic diseases. We summarize management strategies targeting disordered cardiometabolic factors to mitigate cardiovascular disease and explore molecular mechanisms enabling more tailored therapies. Importantly, we emphasize the early interception of atherosclerosis through multifactorial interventions that detect subclinical signs (via biomarkers and imaging) to treat modifiable risk factors and prevent clinical events. A concerted preventive effort—referred to by some as a “preventome”—is essential to reduce the burden of atherosclerosis-driven chronic diseases, shifting from mere chronic disease management to the proactive promotion of “chronic health.”
Keywords:
atherosclerosis
; cardiovascular disease
; cancer
; exposome
; syndemic
; preventome
1. Introduction
The secular trend in hospital admissions indicates an increasing recognition of cancer among patients hospitalized for cardiovascular disease (CVD) [1]. Population-based studies further demonstrate that optimal control of atherosclerotic cardiovascular disease (ASCVD) risk factors—through appropriate behaviours and treatments as recommended by the American Heart Association (AHA) [2] — reduces the incidence of both cancer and CVD, as well as lowers all-cause, cardiovascular, and cancer-specific mortality [3,4]. These interventions include maintaining healthy sleep patterns, avoiding smoking, achieving normal plasma glucose and cholesterol levels, adopting a healthy diet, preventing obesity, engaging in regular physical activity, and managing blood pressure within the normal range. Importantly, these findings support the hypothesis of a shared pathophysiological "common soil" between cancer and CVD [5]. This notion is further emphasized by contemporary international clinical guidelines, which highlight cancer as a clinical condition warranting special attention in the management and prevention of ASCVD [6,7].
However, ASCVD risk is often underestimated and undertreated in oncological patients [8,9,10,11,12,13], and the interactions between environmental exposures (the exposome) and cardiometabolic risk factors remain dangerously neglected. This situation is no longer acceptable, especially given the progressive improvement in cancer patient survival, the aging of the general population, and the increasing incidence of early-onset cancer (before the age of 50). In the first part of this review, we discussed the evolving landscape of atherosclerosis and the central role of chronic low-grade inflammation in both CVD and cancer [14]. In this second part, we will explore the intricate interconnectedness of environmental exposures and cardiometabolic risk factors through a syndemic approach, which adds complexity to the management of contemporary oncological patients. From this perspective, we aim to define an updated strategy for managing ASCVD in patients with a history of or active cancer, with a particular focus on preventive cardio-oncology.
1. The Complexity of Current Oncologic Patients
Currently, at least 80% of heart disease, stroke, and type 2 diabetes, as well as 40-50% of cancers, are linked to an unhealthy lifestyle [15,16,17,18,19]. Cancer patients often present with a high cardiovascular (CV) risk or a history of heart disease, frequently associated with exposure to multiple risk factors, which often cluster together [20,21,22,23]. This includes both the direct and indirect CV effects of cancer and oncologic treatments, impacting not only physical health but also mental well-being [24,25].
Advancements in oncological diagnosis and therapy, along with the uncertainty surrounding prognosis, have led to the emergence of novel patient profiles, including long-term cancer survivors. A growing proportion of these individuals are living with advanced metastatic cancer, maintained in remission through prolonged and ongoing treatments. This expanding patient group requires vigilant and continuous surveillance to detect disease recurrence, CV complications, or second cancers [26].
From this perspective, patient management must also address socio-economic factors associated with cancer treatment [27,28]. The improved survival rates and "chronicity" of cancer, facilitated by expensive therapies and continuous medical investigations, give rise to the issue of "financial toxicity"—the economic strain linked to long-term care necessary to maintain favourable outcomes and prevent complications particularly when cancer and CVD coexist in the same patient [29], given the fact that chronic CVDs, such as atherosclerosis and heart failure, are inherently associated with a high risk of financial distress [30,31,32]. Financial toxicity, encompassing both the objective financial burden and the subjective distress caused by a cancer diagnosis and its treatment, has significant implications not only for healthcare systems but also for the quality of life of cancer patients and their families. As highlighted by the ESMO expert consensus statements, socio-economic determinants play a critical role in this regard [33]. They include "intrinsic" factors (e.g. gender, age, ethnicity, lower income), "disease-related" factors (e.g. costs of systemic anticancer therapies), and "extrinsic" factors (e.g. travel expenses, out-of-pocket healthcare costs, lost wages, and medical appointments or tests). All of these contribute to financial toxicity, which can influence cancer diagnosis, treatment access, quality of life, and survival [34,35,36,37]. In addition, comorbidities have a relevant impact: in a cohort of long-term survivors of adolescent and young adult (AYA) cancer from the Kaiser Permanente database, 40% of patients had multiple comorbidities 10 years after diagnosis. The most common atherosclerosis-related comorbidities included dyslipidaemia (22 per 1,000 person-years), hypertension (16 per 1,000 person-years), diabetes (10 per 1,000 person-years), and severe depression or anxiety [38]. More recently, in the St. Jude Lifetime Cohort of childhood cancer survivors [39], 45.5% of individuals aged 40-49 had prediabetes, and 14% had diabetes. Over a median follow-up of 5.1 years, 10% of those with prediabetes progressed to diabetes. Survivors with a worse cardio-metabolic profile experienced significantly more CV events, including myocardial infarction (MI) in those with prediabetes and cardiomyopathy or stroke in diabetics. These findings underscore the need for comprehensive management strategies that address both the medical and socio-economic challenges faced by long-term cancer survivors.
Preventing and managing the risk of ASCVD is particularly important in patients with adult-onset cancer. Aging, which is often accompanied by chronic low-grade inflammation (inflammaging), is a major risk factor for non-communicable diseases (NCDs) such as CVD and cancer [40,41]. Many older adults present with comorbidities at the time of cancer diagnosis, and these conditions may worsen during and after cancer treatment [42,43,44]. Currently, more than 50% of elderly cancer patients live with two or more chronic conditions, with CVD, diabetes, lung disease, and chronic kidney disease (CKD) being the most prevalent [45,46,47,48,49,50,51]. The clinical complexity in these cases is often compounded by hazardous environments, further complicating the management of both cancer and comorbidities [52].
1.1. Assessing ASCVD Risk in Individual Cancer Patients
According to harmonized data from 112 cohort studies involving 1,518,028 participants (54.1% women) across 34 countries and 8 geographic regions, with a median age of 54.4 years and a median follow-up of 7.3 years, approximately 57.2% of incident CVD in women and 52.6% in men, as well as 22.2% and 19.1% of deaths from any cause, respectively, were attributable to five modifiable risk factors: body mass index (BMI), systolic blood pressure, non–high-density lipoprotein cholesterol (non-HDL-C), current smoking, and diabetes [19]. The Global Burden of Diseases, Injuries, and Risk Factors Study (GBD) 2019 further emphasizes that a large proportion of cancer deaths are linked to modifiable risk factors, with smoking, alcohol use, and high BMI contributing the most. Additionally, metabolic risk factors saw the largest increase between 2010 and 2019 (34.7%) [17].
The rise in obesity and related conditions, particularly metabolic syndrome (MetS), is unsurprising given the increasing prevalence of energy-dense food consumption, sedentary behaviour, urbanization, and lower socio-economic status [53,54,55]. Obesity, a chronic low-grade inflammatory state, is commonly associated with hypertension, dyslipidaemia, and increased risk of several cancers, including colorectal, gallbladder, pancreatic, kidney, liver, and breast cancers (in post-menopausal women) [56,57]. Obesity also accelerates atherosclerosis progression [53,58]. Alarmingly, the incidence of obesity has risen sharply among children and adolescents. Overweight or obesity in childhood is linked to future cancer, type 2 diabetes, and ASCVD, often before the age of 50 [59,60,61,62,63]. In young patients with "obesity-related" cancer, ASCVD risk should not be underestimated, as cardiometabolic risk factors often emerge during childhood and adolescence [64,65]. For example, the PESA (Progression of Early Subclinical Atherosclerosis) study, which examined the vascular systems of 4,184 asymptomatic individuals aged 40-54, found that over 60% (71% of men and 48% of women) had silent atherosclerosis in one or more vascular regions [66], with progression observed in over 40% after a 3-year follow-up [67].
In recent years, there has been increasing focus on refining traditional CV risk factors using indices derived from common lab tests. One promising parameter is the TyG index, calculated as logarithmized semi-product of fasting levels of triglycerides and glucose: ln [triglycerides (mg/dl) x blood glucose (mg/dl)/2]. The TyG index is highly sensitive and specific for insulin resistance [68], correlates with metabolic syndrome [69,70], and is a predictor of type 2 diabetes and CVD events [71,72], particularly in low- and middle-income countries [73]. Additionally, the TyG index has been associated with cancers of the kidney, liver, pancreas, and colon-rectum, and mediates a significant portion of the effect of BMI on cancer risk [74,75]. Recent metanalyses, finally, indicate that the Tyg index is a proxy for coronary artery disease (CAD) risk prediction, severity assessment and prognosis evaluation [76,77].
Despite its simplicity and affordability, the TyG index has limitations, as most studies are based on single measurements and lack data on confounding factors such as diet, physical activity, and alcohol intake. Furthermore, insights regarding demographic categories such as children, adolescents, and women remain at a preliminary stage [78]. Prognostic accuracy may be enhanced by incorporating inflammatory markers like high-sensitivity C-reactive protein (hsCRP) or cell-derived markers such as neutrophil-lymphocyte ratio (NLR) [79,80,81,82,83,84,85,86,87]. Another important risk factor is non-HDL-C, particularly triglyceride-rich lipoproteins, which have stronger atherogenic potential than low-density lipoprotein cholesterol (LDL-C) [88].
Addressing obesity requires a focus not just on the quantity of adipose tissue but also on its type (brown vs. white adipose tissue) and distribution [89,90]. Advanced body composition methods, such as dual-energy X-ray absorptiometry (DEXA) and computed tomography (CT), have shown the limitations of BMI in predicting CV risk, especially in oncologic patients with normal or reduced BMI [91,92,93,94]. These fat deposits, including intramuscular and pericardial fat, contribute to systemic inflammation and accelerated atherosclerosis. "Sarcopenic obesity," characterized by reduced muscle mass and strength alongside fat accumulation, is common in cancer patients [95] and linked to subclinical atherosclerosis and CVD events [89,90,91,92,93,94,95,96,97,98,99,100]. Chronic inflammation plays a major role in sarcopenia, with hsCRP and NLR serving as useful markers for silent atherosclerosis [101,102,103,104]. This is particularly relevant for patients on immune checkpoint inhibitors (ICIs), preliminary observations identify sarcopenia and high hsCRP as independent risk factors for poor outcomes in cancer patients treated with ICIs [105,106,107].
Inadequate treatment of CV risk factors is common in oncology patients and may worsen cancer prognosis while increasing the likelihood of CV events. In the prospective multicentre RADICAL-PC program, which involved newly diagnosed prostate cancer (PCa) patients scheduled for androgen deprivation therapy (ADT), obesity, hypertension, and hypercholesterolemia were the most common comorbidities, yet they were often inadequately managed [8]. Similar findings were reported by Sun in a retrospective analysis of PCa patients from the US Veterans Database [9]. Additionally, the CARDIOTOX Registry revealed that hypercholesterolemia and elevated blood pressure were frequently overlooked and poorly controlled [10]. A recent study by Lin et al. demonstrated that pretreatment lipid profiles may contribute to resistance to ADT with androgen receptor pathway inhibitors in localized cancer, based on findings from both human cohorts and explant models [108]. Likewise, non-adherence to Life's Simple 7 [109] was associated with increased risk of ASCVD (MI, angina, stroke, and heart failure) in long-term survivors of gastric, colorectal, and breast cancers enrolled in the Japanese National Registry [4]. This challenge is becoming increasingly unsustainable, given the improved survival rates offered by new cancer therapies [110,111,112,113].
Adherence to a healthy lifestyle, as recommended by guidelines, has been shown to reduce the risk of both cancer and ASCVD in the general population, as well as in high-risk groups such as individuals with high polygenic risk [114], diabetes [115], or CKD [116]. Emerging evidence suggests that these benefits may also extend to cardio-oncology patients [3].
Hypertension, the most common risk factor for ASCVD, is a leading comorbidity in cancer patients at all stages—before, during, and after treatment [19]. Many oncologic therapies can induce 'de novo' hypertension or worsen pre-existing high blood pressure [117]. Several mechanisms, including oxidative stress, endothelin-1 activity, prostaglandin imbalance, endothelial dysfunction, increased sympathetic activity, microvascular rarefaction and reduced nitric oxide production, contribute to hypertension, many of which overlap with those involved in atherogenesis [118,119]. Managing hypertension during cancer treatment is challenging, especially as it is often accompanied by a worsening cardiometabolic risk profile, such as during hormonal therapy for breast or prostate cancer [120,121,122]. In a large retrospective cohort of cancer survivors, maintaining blood pressure within normal ranges (<130/90 mmHg) per international guidelines was associated with a reduced incidence of CV complications, particularly in patients with elevated cardiometabolic risk [123].
Although an individual’s absolute CV risk is key to guiding treatment, especially in primary prevention, risk prediction models have evolved in recent years to reflect the growing prevalence of cardiovascular-kidney-metabolic (CKM) conditions, such as obesity, diabetes, and CKD, often clustering with adverse social factors like living in socioeconomically deprived neighbourhoods [124,125,126]. In Europe, the Systematic Coronary Risk Estimation 2 (SCORE2) and SCORE2-Older Persons (SCORE2-OP) are widely used [6]. In the U.S., the AHA's recent PREVENT equations have been validated to predict risk in adults aged 30–79 without known CVD [127], addressing the limitations of older models like the 2013 Pooled Cohort Equations (PCEs) [128]. PREVENT uses traditional risk factors (e.g., smoking, systolic blood pressure, cholesterol, diabetes) and estimated glomerular filtration rate, with models being sex-specific, race-neutral, age-scaled, and adjusted for non-CVD death [127]. However, none of these CV risk scores consider the unique challenges of cancer patients, including the elevated CV risk due to shared risk factors, the CV toxicity of cancer therapies, and cancer itself [129]. As recent research from the UK Biobank shows, established CV risk scores such as QRISK3, SCORE2, Framingham, and others do not perform as well in cancer survivors compared to non-cancer patients [13]. To address these limitations, coronary imaging—such as coronary artery calcium (CAC) scoring and coronary computed tomography angiography (CCTA)—can enhance the prognostic accuracy of clinical scores [130,131]. CCTA has shown promise in detecting coronary inflammation through radiological changes in perivascular adipose tissue (PVAT), measured via the Fat Attenuation Index (FAI) [132]. Inflammation biomarkers, such as hsCRP and interleukin-6 (IL-6), have long been associated with CV risk independent of cholesterol levels. Numerous trials demonstrate improved outcomes with reductions in both LDL-C and CRP [133,134,135,136,137,138,139]. A recent meta-analysis of 53 randomized controlled trials (RCTs) involving 171,668 participants showed significant reductions in CRP levels from treatments like statins, bempedoic acid, ezetimibe, and omega-3 fatty acids, independent of LDL-C reduction [140]. Notably, hsCRP predicted future CV events more effectively than LDL-C in high-risk, statin-intolerant patients [141].
2. How to Manage Atherosclerosis -Driven Chronic Diseases in Cancer Patient
NON pharmacologic treatments
The importance of lifestyle in preventing NCDs is well-established. Risk factors such as tobacco use; unhealthy diets high in saturated and trans fats, salt, and sugar; physical inactivity, and excessive alcohol consumption are responsible for more than two-thirds of all new NCD cases and significantly increase the risk of complications [19].
Diet. The EUROASPIRE V study highlights the importance of dietary guidance in managing patients at high CV risk [142]. Both vegetarian and Mediterranean diets, low in saturated fats and red meat, have been shown to improve blood lipid profiles, blood pressure, fasting glucose, and glycosylated haemoglobin levels. These diets also positively influence inflammation, oxidative stress markers, insulin sensitivity, and endothelial and antithrombotic function [143,144,145,146,147]. Meta-analyses of observational studies and randomized trials confirm the protective effect of Mediterranean diet against all-cause mortality, CVD, CAD, MI, cancer, neurodegenerative diseases, and diabetes [148,149]. In the Women's Health Study, a 25-year cohort of 25,315 women, those with greater adherence to the Mediterranean diet had a 23% reduced risk of all-cause mortality. This effect was largely attributed to improvements in small molecule metabolites, inflammation, triglyceride-rich lipoproteins, insulin resistance, and BMI, with less impact from traditional cholesterol or glycaemic markers [150]. For patients with established CAD, the Mediterranean diet with extra virgin olive oil (EVOO) outperformed low-fat diets in preventing major CV events [151], slowing atherosclerosis progression [152], and preserving kidney function in obese patients with type 2 diabetes [153]. A strong inverse association between Mediterranean diet adherence and cancer risk has also been observed, particularly for breast cancer (BC). In the Women's Health Initiative study, postmenopausal women with BC following a diet rich in vegetables, whole grains, fruits, and reduced fat intake showed a 38% reduction in CV deaths over 10 years [154]. Similarly, the PREDIMED trial found that women at high CV risk who followed a Mediterranean diet enriched with EVOO had a reduced incidence of BC [155]. The MOLI-SANI study further underscored the importance of dietary quality, demonstrating that higher olive oil consumption was linked to lower rates of cancer, CV, and all-cause mortality, independent of overall diet quality [156]. In the Multi-Ethnic Study of Atherosclerosis (MESA), consumption of plant-based foods and beverages high in bioflavonoids was inversely associated with subclinical atherosclerosis in peripheral and carotid arteries [157].
In contrast, there is growing concern about the health impacts of ultra-processed foods (UPFs), which are typically high in energy, sugars, unhealthy fats, salt, and low in fibres, protein, vitamins, and minerals. Greater consumption of UPFs, as classified by the NOVA system [158], has been linked to increased cardiometabolic risk, depression, and mortality [159,160]. A systematic review of eight retrospective and three prospective cohort studies found that a 10% increase in UPF daily consumption was associated with a higher risk of overall cancer (HR = 1.13, 95% CI 1.07–1.18) [161]. Children are also affected by high UPF consumption. In the CORALS (Childhood Obesity Risk Assessment Longitudinal Study) cohort of 1,426 children (mean age 5.8 years), higher UPF intake was significantly associated with increased adiposity and worse cardiometabolic risk. Mothers of children with high UPF consumption tended to be younger, with higher BMIs, lower education levels, and lower employment rates [162]. Given these findings, reducing UPF consumption is crucial. The 2022 ESC Guidelines on Cardio-Oncology recommend dietary patterns rich in vegetables, fruits, and whole grains, which are associated with lower mortality and cancer recurrence compared to diets high in refined grains, processed and red meats, and high-fat dairy products [129]. According to the American Cancer Society Guidelines for Cancer Prevention the “healthy eating pattern includes a variety of vegetables (dark green, red, and orange), fiber-rich legumes (beans and peas), fruits, especially whole fruits with a variety of colors; and does not include red and processed meats, sugar-sweetened beverages and highly processed foods and refined grain products” [163].
Microbiota and microbiome. Diet plays a crucial role in regulating gut microbiota, a complex community of intestinal microorganisms, including bacteria, archaea, viruses, and fungi. The intestinal microbiota is often considered the largest endocrine organ in the human body, supporting immune responses against pathogens, aiding food digestion, and facilitating vitamin production [164]. A healthy gut microbiota stabilizes its host, contributing to CV health (CVH) and cardiovascular-kidney-metabolic health (CVKMH) [165], although the exact mechanisms and the influences of genetic and environmental factors on microbiota composition are not yet fully understood [166,167]. Dysregulated microbiota can exacerbate inflammatory pathways, including IL-6, CRP, lipopolysaccharide (LPS), short-chain fatty acids (SCFAs), mitogen-activated protein kinase (MAPK), nuclear factor-kB (NF-kB), and oncometabolite production [168]. Current research actively investigates the potential link between alterations in faecal microbial community composition and conditions such as obesity, insulin resistance, atherosclerosis, CVD, and cancer [169,170,171,172]. Preliminary pooled analyses suggest that manipulating intestinal flora may improve cardio-metabolic risk [173]. In a recent small randomized clinical trial, obese patients with type 2 diabetes who combined an appropriate lifestyle with "lean-associated" faecal microbiota transplantation showed significant improvements in lipid profiles and liver stiffness—markers of predisposition to atherosclerosis, cirrhosis, and hepatocellular carcinoma [174]. Initial studies exploring the causal relationship between the gut microbiome and CVD focused on trimethylamine N-oxide (TMAO), an intestinal microbiota-dependent metabolite derived from the choline head group of phosphatidylcholines, mainly found in Western dietary nutrients (e.g., lecithin, choline, carnitine). Elevated plasma levels of TMAO, produced by gut microbiota, are significantly predictive of major adverse CV events [175], facilitating atherosclerosis through dysregulated lipid metabolism, adiposity, impaired glucose homeostasis, high blood pressure, platelet reactivity, thrombosis, and vascular inflammation [176]. The relationship between dietary patterns and gut microbiota is evidenced by the correlation between prolonged red meat consumption and increased TMAO levels; conversely, an isocaloric-isoprotein diet without red meat can reduce TMAO levels [175]. Emerging data also suggest a link between microbiota and cancer development, as well as responses to oncological treatments [177,178,179]. Many bacterial species within the microbiome may play oncogenic roles, making the influence of bacterial flora potentially relevant in the context of personalized oncology treatments [180]. Recent observations indicate that intestinal flora may impact the development of early-onset cancer [181,182,183] and the response to immunotherapy [184,185,186].
Alcohol. Traditional population studies have suggested a J- or U-shaped relationship between alcohol consumption and cardiovascular health (CVH), indicating that mild to moderate use may offer cardioprotective effects, while alcohol abuse is cardiotoxic [187]. However, recent findings have called into question the protective effects of moderate or mild alcohol consumption, citing potential confounding factors such as genetic polymorphisms, lifestyle behaviours among light drinkers, and inadequate analyses of social and economic influences [188,189,190,191,192]. In oncology, alcohol consumption has been causally linked to several types of cancer, with no safe level of intake. The risk of alcohol-associated cancer increases with consumption, and this risk is consistent across all ethanol-containing beverages. Regarding CV prevention, the 2021 ESC Guidelines on CVD prevention recommend limiting alcohol consumption to a maximum of 100 g per week (about 5–6 standard UK glasses of wine or pints of beer per week) [6] while the American Cancer Society's Guidelines for Diet and Physical Activity for Cancer Prevention advise against alcohol consumption, stating that individuals who choose to drink should limit their intake to no more than one drink per day for women and two drinks per day for men [163].
Physical activity (PA) In oncology, PA significantly impacts cellular processes and tumour growth [193] by modulating insulin and glucose metabolism, immune function, inflammation, sex hormones, oxidative stress, genomic instability, and myokines [163,194,195]. Furthermore, PA may reduce cancer risk related to obesity. The physical effects of PA, such as increased blood flow, shear stress on the vascular system, pH regulation, heat production, and sympathetic activation, along with endocrine effects like stress hormones, myokines, and circulating exosomes, may help regulate cancer progression and biology by affecting tumour growth, metastatic potential, tumour metabolism, and the immunogenic profile of tumours. Exercise also has beneficial effects on cancer symptoms and treatment-related adverse effects [196].
Smoking cessation is a critical priority for preventing both CVD and cancer. Smoking significantly increases mortality from all causes and is a leading contributor to ASCVD. Cigarette smoke contains over 7,000 chemical compounds, including at least 72 known carcinogens and numerous pro-carcinogens [197,198]. Tobacco use is causally linked to various CVD phenotypes, ranging from early-onset atherosclerosis in adolescents and young adults to increased risks of acute MI, stroke, peripheral artery disease, aortic aneurysm, and sudden death [199]. Both cigarette smoke and second-hand smoke activate, damage, and kill endothelial cells, leading to lipid and inflammatory cell infiltration. Additionally, activated leukocytes release inflammatory cytokines and enhance the expression of adhesion molecules, contributing to the formation of vulnerable plaques, a pro-thrombotic environment, and reduced fibrinolytic capacity [200]. Smoking also contributes to the development of diabetes and dyslipidaemia [201]. In 1964, the Surgeon General's report first established the causal link between smoking and lung cancer [202]. Fifty years later, the 2014 report highlighted the increased risk of smoking exposure for several other cancers. While lung, laryngeal, and pharyngeal cancers have the highest relative risks for current smokers, elevated risks have also been observed for cancers of the upper digestive tract, oral cavity, lower urinary tract, oesophagus, nasopharynx, cervix, pancreas, stomach, kidney, liver, and colorectal regions [199,203]. Meta-analyses have confirmed smoking as a major risk factor for urothelial bladder cancer [204,205] and for an unfavourable course of prostate cancer [206].
Social and psychological determinants of health. Inequalities in wealth, income, and education are key factors in the development and progression of multimorbidity. Low socioeconomic status is a recognized risk factor for many mental and behavioral problems, that eventually lead to lifelong physical diseases [207,208]. Food insecurity (FI), or “the lack of consistent access to enough food for an active and healthy life” [209] has indeed been associated to ASCVD risk through the nutrition/anthropometric, psychological/mental health, and access to care pathways [210].
In 2019, Tawakol et al. documented a link between socioeconomic disparities and CVD through a stress-related neurobiological pathway [211]. In 2022, the American Heart Association (AHA) included sleep as an essential component of CVH and addressed social determinants of health (SDOH) and psychological well-being, recognizing their importance for achieving equitable CVH outcomes [2]. Positive psychological traits, such as optimism, purpose in life, environmental mastery, perceived social role reward, and resilient coping, have been associated with better CVH, while psychosocial stress and depression are linked to worse outcomes [2,212]. Loneliness, a recognized SDOH, is also a risk factor for both CVD and cancer [213,214,215]. In a systematic review of 51 cohort studies involving 2,611,907 participants with an average follow-up period of 10.3 years, depression and anxiety were associated with a significantly higher risk of cancer incidence (adjusted RR: 1.13; 95% CI: 1.06-1.19), specific cancer mortality (1.21; 1.16-1.26) and all-cause mortality in cancer patients (1.24; 1.13-1.35) [216]. Psychological distress is common in cancer [217,218] and may intersect with the cognitive change associated with therapy, or “chemo-brain” [219], an entity that has been identified in people with a variety of cancers who have undergone chemotherapy and/or hormone treatment. These patients may have difficulties in executive functions, multitasking, short-term memory and attention and coping ability. Anxiety and depression are emerging as significant risk factors for subclinical atherosclerosis [220,221,222], in the context of cardio-oncology there is an urgent need to address these novel risk enhancers. An example is offered by the positive impact of spirituality in serious health conditions and its ability to counter loneliness, hopelessness, and depersonalization, often overlooked in patient-centred care [223]. Spirituality can enhance coping abilities [224] and potentially improve outcomes through effects on the autonomic nervous system, and hormonal, immunological, and neurological pathways [225]. Since 2008 The Institute of Medicine (IOM) stated: “Attending psychosocial needs should be an integral part of quality cancer care. All components of the health care system involved in cancer patient management should explicitly incorporate attention to psychosocial needs into their policies, practices, and standards addressing clinical care” [226,227]. Psychotherapeutic interventions useful for mental health in cancer patients are based on emotional support and include education, behavioural training, group interventions and individual psychotherapy.
Pollution is an increasingly significant health issue, acting as a "syndemic" risk factor when combined with traditional risk factors. Air and noise pollution, light disruption at night, climate change, and chemical exposure contribute to the development and progression of cardiometabolic multimorbidity [228]. Studies on populations living near airports, heavy road traffic, and industrial zones highlight the impact of environmental pollution on cardio-metabolic and oncological risks [229,230,231,232,233]. These stressors—through mechanisms such as altered stress responses, circadian rhythm disruption, immune activation, inflammation, oxidative stress, microvascular dysfunction, heart rate variability, and hypercoagulability—heighten CV risk and burden [52]. For example, air pollution amplifies the adverse effects of heat, particularly in vulnerable elderly populations, while exposure to heavy metals like lead and mercury has been linked to hyperlipidaemia [234]. Addressing pollution from an "exposomic" perspective, which considers the total environmental exposure across an individual's life, is a crucial issue. Simply controlling traditional risk factors will not be enough to reverse the rising trend of NCDs. Efforts must focus on improving environmental conditions alongside traditional risk factor management.
Pharmacologic therapies: cardiometabolic and anti-inflammatory agent
- 2.2.1.
- Cardiometabolic Therapies and Their Impact on Atherosclerotic Plaque
- (i)
- Lipid-lowering therapies (LLTs), including statins, ezetimibe, polyunsaturated fatty acids (PUFAs), and proprotein convertase subtilisin/kexin type 9 (PCSK9) inhibitors, have been extensively studied for their beneficial effects on atherosclerotic plaque regression, both as monotherapies and in combination [235,236,237,238,239,240,241,242,243,244,245,246,247,248,249,250,251,252,253,254,255,256]. LLTs also influence platelets and interact with various atherosclerosis mediators, including the endothelium, monocytes, and smooth muscle cells [257]. Table 1 summarizes key studies on LLTs and their effects on atherosclerotic plaques.
- (ii)
- Metformin, first introduced in the late 1950s and still widely used today, targets three key molecular pathways: complex 1 of the mitochondrial electron transport chain (ETC), adenosine monophosphate (AMP)-activated protein kinase (AMPK), and mechanistic target of rapamycin complex 1 (mTORC1). Inhibition of hepatic gluconeogenesis is linked to its effect on mitochondrial complex 1, which reduces ATP levels and increases the AMP/ATP ratio, activating AMPK and further inhibiting gluconeogenesis [258,259]. Metformin also stimulates the release of glucagon-like peptide 1 (GLP-1) from the intestine [260]. Additionally, AMPK can be activated via the serine-threonine liver kinase B1 (LKB1) and mitochondrial glycerol-3-phosphate dehydrogenase (mGPD), which increases the cytosolic redox state [261,262]. Activation of AMPK by metformin results in reduced blood sugar, improved inflammatory control, enhanced oxidative status, and activation of endothelial nitric oxide synthase, which may explain metformin's protective effect on endothelial function. Preclinical studies suggest that metformin stabilizes atherosclerotic plaques by inhibiting matrix metalloproteinase 9 (MMP-9), an enzyme responsible for degrading the extracellular matrix (ECM) of blood vessels [263,264]. A retrospective clinical study of 313 patients with type 2 diabetes and CAD found that metformin, particularly when not combined with insulin, reduced the prevalence of vulnerable plaque features based on optical coherence tomography (OCT) analysis of 409 non-culprit plaques [265].
- (iii)
- Preclinical studies in animal models have demonstrated that sodium-glucose co-transporter-2 inhibitors (SGLT-2 inhibitors) have favourable effects on plaque size, composition, and inflammatory pathways [266,267]. However, there are limited data on these effects in humans [268,269,270], they are summarized in Table 2.
- 2.2.2.
- Cardiometabolic Therapies and Their Potential Effect in Cardioncology
The shared mechanisms between CVD and cancer explain the unexpected anticancer effects of
many cardiometabolic drugs. These effects are largely due to metabolic remodelling in cancer cells.
- (i)
- Statins. Statins reduce low-density lipoprotein cholesterol (LDL-C) in a dose-dependent manner, lower triglycerides (TG) by 10-20% (with greater reductions from high-intensity statins), and have a minimal effect on lipoprotein(a) [Lp(a)] [271]. Their beneficial impact on CV morbidity and mortality is well-documented [272,273,274,275]. Statins can be safely and effectively used in elderly patients, including those over 75 years of age [276]. The ESC Guidelines on CVD prevention (Class I A) recommend high-intensity statins at the highest tolerated dose to achieve LDL-C targets based on specific risk groups [6]. Statins may have anticancer properties due to their cholesterol-lowering effects [277,278] and ability to enhance efficacy of ICIs [279,280]. Preclinical studies have shown statins' direct antiproliferative and immunomodulatory effects, promoting immunogenic cell death in KRAS (Kirsten rat sarcoma viral oncogene homolog) -mutated cancer cells. This occurs through increased expression of "eat me" signals and damage-associated molecular patterns, while reducing proteins that suppress T cell antitumor responses [281].
- (ii)
- Ezetimibe. In a meta-analysis of eight randomized, double-blind, placebo-controlled trials (12-week duration), Ezetimibe showed a significant reduction in LDL-C compared to placebo [282]. When combined with statins, it provided an additional 21-27% reduction in LDL-C [283]. The IMPROVE-IT trial, involving over 18,000 patients with acute coronary syndrome (ACS), demonstrated a modest but significant CV benefit from adding ezetimibe to simvastatin, with encouraging safety data [284]. These findings support the use of ezetimibe as second-line therapy alongside statins when LDL-C targets are unmet, or statins are not viable options.
- (iii)
- Bempedoic acid inhibits ATP citrate lyase, a cytosolic enzyme upstream of 3-hydroxy-3-methylglutaryl-CoA (HMG-CoA) reductase, and reduces LDL-C levels. It has a low incidence of muscle-related side effects, making it suitable for patients who are statin-intolerant. The CLEAR OUTCOMES trial, a double-blind, placebo-controlled study that included high-risk CVD patients who could not tolerate statins, has documented a significantly lower risk of major adverse CV events (MACE), including CV death, nonfatal MI, stroke, or coronary revascularization in patients treated with bempedoic acid [285]. The 2024 ESC Guidelines on chronic coronary disease (CCD) recommend bempedoic acid in combination therapy for statin-intolerant patients or those not reaching LDL-C goals on maximum tolerated statin and ezetimibe therapy [286].
- (iv)
- PCSK9 inhibitors (PCSK9Is). PCSK9Is target the PCSK9 protein, which regulates LDL receptors (LDLRs). These inhibitors work through monoclonal antibodies (mAbs) that lower plasma PCSK9 levels by reducing its binding to LDLRs, and through a small interfering RNA (siRNA), Inclisiran, that inhibits PCSK9 synthesis. The result is a significant reduction in plasma LDL-C levels. Alirocumab and evolocumab effectively lower LDL-C in high or very high CV risk patients, including those with T2DM, and reduce CVD events [287,288]. Statins increase circulating PCSK9 levels, enhancing the benefits of the mAbs. These drugs are recommended for secondary prevention in patients who do not achieve LDL-C targets with statins and ezetimibe [6,286]. The long-term benefits of PCSK9 inhibitors (PCSK9Is) were evaluated in the FOURIER-Open Label Extension (FOURIER-OLE) study, which followed individuals originally randomized to evolocumab in the FOURIER trial [288]. The study confirmed both the efficacy and safety of extended PCSK9I use [289], which Shapiro described as "the gift that keeps giving" [290]. The efficacy in lowering LDL-C of Inclisiran was demonstrated in the ORION trials in patients with familial hypercholesterolemia, atherosclerosis, and high CV risk [291,292]. Beyond LDL-C lowering, PCSK9Is have pleiotropic effects, such as reducing platelet reactivity, decreasing smooth muscle cell proliferation, limiting macrophage accumulation, and promoting plaque regression and stabilization [293]. Emerging data suggest a link between PCSK9 and cancer: PCSK9 gain-of-function variants are associated with higher LDL-C and an increased risk of BC, while loss-of-function variants show the opposite effect [294]. PCSK9Is may also enhance the anticancer efficacy of immune checkpoint inhibitors (ICIs), as seen in colorectal cancer, where PCSK9 inhibition boosts the effectiveness of PD-1 blockade by reducing LDL-R and transforming growth factor-β (TGF-β) levels [295].
- (v)
- Fibrates (bezafibrate and fenofibrate) are used to lower triglyceride levels, but their limited impact on CV outcomes has led to a Class IIb recommendation in the 2021 ESC Guidelines on CVD prevention. They are suggested for patients on statins who have reached LDL-C targets but still have triglyceride levels >2.3 mmol/L (200 mg/dL) [6]. A recent meta-analysis of 12 trials involving over 50,000 patients found that fibrate therapy was associated with a reduced risk of major adverse CV events (MACE); however, this benefit was attributed to LDL-C reduction rather than changes in triglyceride levels [296].
- (vi)
- Metformin. Untreated patients with type 2 diabetes (T2DM) have an increased risk of cancer, likely due to the growth-promoting effects of chronically elevated glucose and insulin levels. This heightened risk is most pronounced for cancers of the liver, pancreas, endometrium, colon, breast, and bladder [297]. The anticancer potential of metformin has been widely studied, but its preventive role remains debated. A review and meta-analysis of 27 trials involving over 10,000 patients found no significant reduction in cancer incidence with metformin use [298]. However, another meta-analysis of 166 studies indicated a decreased risk of T2DM-associated cancers (gastrointestinal, urologic, and hematologic), suggesting metformin may reduce cancer risk indirectly by improving diabetes control [299]. A recent review by Galal et al. [300] highlights metformin influence on cancer cell biology through its effects on energy metabolism, cellular growth, angiogenesis, and programmed cell death. Metformin exerts both direct (insulin-independent) and indirect (insulin-dependent) effects on cancer cells, which may interact with each other. However, in recent clinical trials, metformin failed to improve the clinical course of prostate cancer [301,302] and BC [303]. Metformin has also been proposed as an immuno-metabolic adjuvant for cancer therapy. Preclinical studies suggest it can alter the tumor immune microenvironment [304,305] and reduce programmed death ligand 1 (PD-L1) expression, enhancing its degradation [306,307]. However, the "boosting" effect of metformin on cancer immunotherapy has been questioned due to confounding factors [308]. A meta-analysis of 22 studies involving over 9,000 patients revealed a significant association between metformin use and poorer overall survival, suggesting an adverse prognosis when combined with immune checkpoint inhibitors (ICIs) [309]. Further research is needed to fully assess metformin’s clinical and immunomodulatory potential in cancer treatment.
- (vii)
- Glucagon-like peptide 1 Receptor Agonists Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) are incretin-based therapies that enhance insulin secretion in response to meals [310]. In addition to their role in glucose regulation, they promote weight loss, reduce chylomicron secretion, and lower blood pressure [311,312]. GLP-1 RAs, such as Liraglutide, Semaglutide, Exenatide, Albiglutide, and Dulaglutide, are approved for treating type 2 diabetes mellitus (T2DM) and have shown CV benefits in several trials [313,314,315,316,317,318,319]. A meta-analysis of 40 randomized controlled trials demonstrated that GLP-1 RAs significantly reduce inflammatory markers such as CRP, tumor necrosis factor-alpha (TNF-α), and malondialdehyde (MDA) [320]. Notably, the effects of Liraglutide and Semaglutide on CV outcomes are independent of baseline blood pressure [321], BMI [322], glycated hemoglobin A1c (HbA1c) levels [323], and triglycerides [324]. The 2023 ESC Guidelines for the management of CVD inpatients with diabetes recommend GLP-1 RAs with proven CV benefits (Liraglutide, Semaglutide, Dulaglutide, Efpeglenatide) for patients with T2DM and ASCVD to reduce CV events, irrespective of baseline HbA1c or other glucose-lowering treatments [325]. Liraglutide and Semaglutide have also been approved for obesity treatment. Liraglutide approval for weight loss followed the SCALE program [326], while Semaglutide approval was based on the STEP program, which included four key trials [327,328,329,330]. A recent trial demonstrated a significant reduction in death from CV causes, nonfatal MI, and nonfatal stroke with weekly Semaglutide (2.4 mg) in overweight or obese patients with preexisting CV disease but without diabetes, over a 39.8-month follow-up [331]. The 2024 ESC Guidelines for CCD recommend Semaglutide for patients without diabetes but with overweight or obesity (BMI >27 kg/m²) to reduce CV mortality, MI, or stroke (class IIa, B) [286]. GLP-1 receptor agonists (GLP-1 RAs) may have a potential role in reducing obesity-related cancer risk [332]. A recent study involving over 1.6 million patients with type 2 diabetes (T2DM) compared the incidence of 13 obesity-associated cancers among those treated with GLP-1 RAs, insulin, or metformin. GLP-1 RA treatment was associated with a significant reduction in the risk of 10 cancers, including esophageal, colorectal, endometrial, gallbladder, kidney, liver, ovarian, and pancreatic cancers, as well as meningioma and multiple myeloma, compared to insulin-treated patients. When compared to metformin, GLP-1 RAs showed a beneficial effect in reducing the risk of colorectal and gallbladder cancer [333]. In preclinical studies liraglutide has shown potential to enhance the anti-tumor efficacy of immune checkpoint inhibitors (ICIs) in lung and liver cancers [334]. However, conflicting data exist regarding the effects of GLP-1 RAs on cancer initiation and progression. The expression of the GLP-1 receptor (GLP-1R) varies across different tumor types, as well as between healthy and diseased tissues [335]. GLP-1R is highly expressed in endocrine tumors and has also been detected in embryonic cancers, nervous system tumors, and certain carcinomas. It is also expressed in various healthy tissues, including the pancreas, digestive tract, heart, skeletal muscle, liver, central nervous system, and immune cells, where it can be activated [336]. The effects of GLP-1 RAs appear to be tumor-specific. Notably, Semaglutide carries a boxed warning from the Food and Drug Administration (FDA) regarding the potential risk of thyroid C-cell cancer, specifically medullary thyroid carcinoma; [337]; this increased risk has not been observed with liraglutide A recent French multicenter registry reported an association between GLP-1 RA use for 1-3 years and an increased risk of thyroid cancers (adjusted hazard ratio [HR] 1.58, 95% CI 1.27-1.95) [338], a finding supported by a systematic review of 64 randomized controlled trials [339].
- (viii)
- SGLT2 Inhibitors Numerous trials have evaluated the effects of SGLT2 Inhibitors (Empagliflozin, Canagliflozin, Dapagliflozin, Ertugliflozin) on CV morbidity and mortality, as well as the effects of Canagliflozin and Sotagliflozin on reducing the risk of kidney failure and CV events [340,341,342,343,344,345,346,347,348,349]. According to the 2023 ESC Guidelines for managing CVD in patients with diabetes, empagliflozin, canagliflozin, dapagliflozin, and sotagliflozin are recommended for patients with T2DM and ASCVD to reduce CV events, regardless of baseline or target HbA1c levels and independent of other glucose-lowering treatments [325]. In T2DM patients without ASCVD or severe target organ damage (TOD), but with a 10-year CV risk of ≥10% according to the SCORE2-Diabetes algorithm, SGLT2 inhibitors may also be considered to lower CV risk, a benefit that appears to be independent of their glucose-lowering effects [350,351]. Empagliflozin and dapagliflozin have shown impressive results in improving outcomes for patients with symptomatic heart failure (HF), regardless of ejection fraction [352]. SGLT2 inhibitors have demonstrated antiproliferative effects against certain tumor types. Cancer cells often exhibit high glucose uptake and glycolysis, and the antineoplastic activity of SGLT2 Inhibitors is partially attributed to their ability to block glucose uptake in metabolically reprogrammed cancer cells expressing SGLT2 receptors. However, preclinical studies suggest that the anticancer effects of SGLT2 Inhibitors are multifactorial, involving several metabolic pathways [353]. Beyond their potential direct anticancer effects, SGLT2 Inhibitors may offer protective benefits against cancer therapy-induced CV toxicity. Preclinical studies have shown significant cardioprotective effects against anthracycline exposure [354,355] and ponatinib-induced cardiac toxicity [356]. Clinical studies have also reported favorable outcomes in patients with cancer and T2DM treated with anthracyclines [357], as well as improved outcomes in patients with cancer therapy-related cardiac dysfunction or heart failure [358].
- 2.2.4.
- Anti-Inflammatory Agents in CVD and Cancer
In atherosclerosis, the NLRP3 inflammasome (nucleotide oligomerization domain-like receptor protein 3) detects environmental danger signals—such as cholesterol, disturbed blood flow, and dead cells—and activates caspase-mediated processing of pro-IL-1β into its active form, IL-1β. This promotes an inflammatory response in endothelial cells, triggering the activation of adhesion
molecules such as intercellular cell adhesion molecule-1 (ICAM-1) and vascular cell adhesion
molecule-1 (VCAM-1); and chemokines like monocyte chemoattractant protein-1 (MCP-1), which
recruit leukocytes to the site [359]. Cells in atherosclerotic plaques can also produce IL-1 in response
to inflammatory stimuli [360]. The association of inflammatory biomarkers, such as hsCRP and
interleukin-6 (IL-6), with CV risk—independent of cholesterol levels—has been well established [361,362,363]. Numerous studies have shown improved outcomes with reductions in both LDL-C and CRP
[364,365,366,367,368]. A recent meta-analysis of 53 randomized controlled trials involving 171,668 subjects found
that statins, bempedoic acid, ezetimibe, and omega-3 fatty acids significantly reduced CRP levels,
independent of LDL-C reduction [369]. Notably, in high-risk, statin-intolerant patients, inflammation
(assessed by hsCRP) was a stronger predictor of future CV events than hyperlipidaemia (assessed by
LDL-C) [370]. The critical role of inflammation in atherosclerosis has sparked interest in clinical trials
investigating anti-inflammatory therapies, such as the Canakinumab Anti-inflammatory Thrombosis
Outcome Study (CANTOS) with the IL-1 inhibitor canakinumab [371], and colchicine studies [372,373,374] with potential interest in cardioncology.
- (i)
- Interleukin inhibitors - The CANTOS trial was the first to test the inflammatory hypothesis of atherosclerosis by selectively inhibiting interleukin-1β with canakinumab in 10,061 patients with a history of MI and hsCRP levels of 2 mg/L or higher. Treatment with canakinumab (150 mg every 3 months) significantly reduced the incidence of the primary endpoint (nonfatal MI, nonfatal stroke, or CV death) and the secondary endpoint (including urgent revascularization), independent of lipid lowering [371]. Interestingly, CANTOS also observed a reduced incidence of lung cancer in the canakinumab group [375]. However, later trials failed to demonstrate a survival benefit in patients with resected or advanced non–small-cell lung cancer (NSCLC) [376,377,378]. These contradictory findings highlight the complex, pleiotropic role of IL-1 signalling [379]. Elevated IL-1 levels are associated with poor prognosis in various cancers [380] and promotes carcinogenesis by driving chronic inflammation and establishing a protumor cytokine network [381]. Furthermore, IL-1 exert paradoxical effects on antitumor immunity. While it enhances the activation of natural killer- and T- cells, promoting antitumor activity [382], it also contributes to immunosuppression by facilitating the expansion and mobilization of immune cells such as myeloid-derived suppressor cells (MDSCs) [383]. As a result, therapeutic strategies targeting IL-1 require further clinical studies to determine the efficacy and optimal use of anti-IL-1 therapies in specific clinical contexts. The phase II RESCUE trial showed that Ziltivekimab, a monoclonal antibody targeting the IL-6 ligand, significantly reduced inflammation and thrombosis biomarkers linked to atherosclerosis [384]. The results of this small study with Ziltivekimab are particularly intriguing from a cardio-oncology perspective. IL-6 plays a key role in tumorigenesis, cancer progression, and treatment resistance [385]. In preclinical studies, IL-6 inhibition combined with immune checkpoint blockade (ICB) enhanced antitumor immunity and slowed tumor progression across various cancer models [386,387,388]. IL-6 is also implicated in the development of immune-related adverse events (irAEs) associated with ICB, as shown by the effectiveness of tocilizumab, an IL-6 receptor inhibitor in managing these events in clinical practice. Thus, combining IL-6 inhibitors with ICB holds promise for improving cancer immunotherapy while reducing the risk of adverse events [389,390], including atherosclerosis [391]. More definitive data are expected from the ongoing ZEUS trial, which is investigating the effects of Ziltivekimab on CV outcomes (CV death, nonfatal MI, and nonfatal stroke) in 6,000 patients with CVD, CKD and systemic inflammation [392].
- (ii)
- Colchicine is a potent anti-inflammatory agent that works by inhibiting microtubule polymerization, neutrophil extracellular trap (NET) release, platelet activation, and the NLRP3 inflammasome [393,394]. Its effects on the NLRP3 inflammasome limit the activation of inflammatory cytokines, such as interleukin-1 and interleukin-18, in response to danger signals. Preclinical studies have shown that low-dose colchicine exerts anti-atherosclerotic and plaque-stabilizing effects, strongly inhibiting foam cell formation and cholesterol crystal-induced inflammation [395]. In 2013, Nidorf et al. reported a significant reduction in the primary outcome (a composite of ACS, out-of-hospital cardiac arrest, or non-cardioembolic ischemic stroke) after a 3-year follow-up in patients with stable coronary disease treated with colchicine in addition to aspirin (and/or clopidogrel) and statins, compared to those who did not receive colchicine [372]. These findings were confirmed in 2019 by a larger study on patients within 30 days of AMI [373]. Low-dose colchicine also showed benefits in chronic coronary disease, as demonstrated in the LoDoCo2 RCT, where colchicine-treated patients had a significantly lower incidence of CV events (CV death, non-procedural MI, ischemic stroke, or ischemia-driven coronary revascularization) after a 28.6-month follow-up compared to placebo [374]. Colchicine reduces hsCRP levels and may decrease coronary artery plaque volume [396]. A low-dose regimen (0.5 mg daily) has been approved by the FDA for secondary prevention in patients with CAD [397]. The drug's role in oncogenicity remains unclear. In the LoDoCo2 trial, non-cardiovascular deaths were more frequent in colchicine-treated patients than in the placebo group (hazard ratio, 1.51), although cancer diagnosis rates were similar [374]. However, a study of 85,374 Israeli patients with Familial Mediterranean Fever (FMF) showed a significantly lower incidence of cancer compared to the general population, potentially due to colchicine treatment [398]. Shared risk factors between gout and cancer (e.g. obesity and alcohol) have suggested a potential cancer susceptibility in gout patients, as demonstrated in a study of 8,408 male gout patients [399]. A further analysis of 24,050 gout patients found that those diagnosed with cancer were older and had a lower rate of colchicine prescriptions than those without cancer [400]. Interestingly, preclinical studies have shown a cardioprotective effect of low-dose colchicine in doxorubicin-induced cardiotoxicity, likely through the restoration of autophagy [401]. A recent study has documented, in mice and humans carrying CHIP (clonal hematopoiesis of indeterminated potential)-mutations, that colchicine can blunt the higher risk of ASCVD associated with somatic TET2 mutation-driven CHIP by suppressing IL-1β overproduction [402].
Conclusions
The evolving landscape of atherosclerosis—shaped by emerging exposomes, cardiometabolic, socioeconomic and psychological factors, and the complex role of immunity with a growing interest in complement (the so-called immuno-atherosclerosis) [403,404]—has heightened the complexity of cardiac patient management. The exposome concept, which contextualizes patients within their environment and lifestyle, encompasses biochemical and metabolic changes resulting from various lifelong exposures; these components, as identified by Münzel [229], play crucial roles in the development of both CVD and cancer. Moreover, the interaction between exposomes and metabolic disorders is not merely additive but represents a "syndemic," a term introduced in 1996 to describe an "interrelated complex of health and social crises” [405]. In this scenario, cardio-oncology patients present unique challenges due to the overlap of CVD and cancer, compounded by the cardiotoxic effects of cancer treatments. Prevention is therefore essential and it has to start at baseline, with a comprehensive evaluation of all the complexities: the modifiable risk factors (the essential 8), the unmodifiable risk factors (e.g. age), the psychological determinants of health and the socioeconomic background. As illustrated in Figure 1 all the risk factors in the inner circle (the CVH components) may interact with the components of the other circles and all the interactions have a syndemic nuance. The patient may be the target of all these syndemic effects and only a proactive multidisciplinary intervention can prevent the dangerous “swiss cheese effect”[406].
At baseline, cardiovascular health (CVH) should be optimized, risk factors must be actively searched for and managed earlier, more intensively, and with greater precision adopting the principles widely used in cardiology: “the earlier, the better” and “strike early, strike strong”[407]. Machine learning-based recalibration of CV risk models, as proposed by Zinzuwadia et al. [408], may further improve risk stratification within local healthcare systems. An oncology-like screening approach for CVD may be particularly effective, aiming to detect preclinical signs of atherosclerosis, or “the lump in our artery,” [131] and this can be done with meticulous evaluation of routine tests used in cancer patients such as computed tomography (CT) and blood testing to detect indicators of CAD, such as vascular calcification or inflammatory and cardiometabolic markers. Emerging technologies, especially if artificial intelligence-assisted, enhance the potential of this preventive approach: advanced vascular imaging offers near-histologic evaluation of plaque composition and progression; Positron emission tomography (PET) imaging can reveal molecular and cellular events before structural changes arise; cardiac CT provides a complete assessment of fractional flow reserve, perfusion, peri-coronary adipose tissue, plaque characterization, and cardiac abnormalities; and hybrid PET-CT imaging allows simultaneous evaluation of cardiac perfusion and coronary anatomy in a single scan. This vigilant approach should be sustained during and after cancer treatment to detect early signs of cardiotoxicity, allowing for timely interventions to prevent clinical events. Effective management of cardio-oncology patients requires a multidisciplinary team—cardiologists, oncologists, haematologists, radiotherapists, and specialized nurses—collaborating to address cancer and cardiac issues. Allied professionals, including primary care physicians, cancer surgeons, pathologists, palliative care providers, pharmacists, psychologists, social workers, and data managers, contribute critical support. Fostering effective and productive communication among members of the multidisciplinary team is essential; moreover, equitable and accessible cardio-oncology services, tailored to regional needs, must be prioritized. Addressing the current complexity of NCDs requires a paradigm shift towards promoting “chronic health” instead of merely managing “chronic disease.” This preventive shift is embodied in the concept of the “Preventome”—an integrated, multifactorial approach that identifies individual and environmental factors influencing health from before birth and throughout life [52,409]. Achieving this goal demands commitment from communities, researchers, healthcare providers, and public health workers to quantify and monitor cumulative exposures as illustrated in Table 3. Tackling the root social and environmental causes of metabolic disorders should be a priority. Seen from this perspective, cardio-oncology serves as a valuable tool for identifying novel disease mechanisms, following a unique pathway from clinical observations through preclinical functional studies to clinical validation and drug development, as highlighted by Moslehi [410]. Addressing inequity in preventive measures is also urgent; policymakers and communities must support cardio-oncology teams in expanding equitable access to essential healthcare resources.
Author Contributions
Conceptualization, L.T., G.G., M.L., F.M.T. ; methodology, L.T., G.G., F.M.T.;validation, L.T., G.G., A.I., M.L.C., S.O., N.S. and L.T.; writing—original draft preparation, G.G., L.T., A.I., and F.M.T; writing—review and editing, A.N., M.L.C., S.O., G.B., A.T., D.A., A.R., S.G. N.S., and C.P.; supervision, L.T.; funding acquisition, L.T. All authors have read and agreed to the published version of the manuscript.
Funding
This study was partially funded by Italian Ministry of Health—Ricerca Corrente Annual Program 2025.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| ACE-Is | Angiotensin converting enzyme-Inhibitors; |
| ACS | acute coronary syndrome |
| ADT | androgen deprivation therapy |
| AHA | American Heart Association |
| AMI | acute myocardial infarction |
| AMP | adenosine monophosphate |
| AMPK | adenosine monophosphate (AMP)-activated protein kinase |
| ARBs | angiotensin receptor blockers |
| ASCVD | atherosclerotic cardiovascular disease |
| ATP | adenosine triphosphate |
| AYA | adolescent young adult |
| BMI | body mass index |
| CAC | coronary artery calcium |
| CAD | coronary artery disease |
| CANTOS | Canakinumab Anti-inflammatory Thrombosis Outcome Study |
| CCB | calcium channel blockers |
| CCD | chronic coronary disease |
| CCTA | coronary computed tomography angiography |
| CHIP | clonal hematopoiesis of indeterminate potential |
| CKD | chronic kidney disease |
| CKM | cardiovascular-kidney-metabolic |
| CKMH | cardiovascular-kidney-metabolic health |
| CORALS | Childhood Obesity Risk Assessment Longitudinal Study |
| CRP | C reactive protein |
| CT | computed tomography |
| CV | cardiovascular; |
| CVD | cardiovascular disease |
| CVH | cardiovascular health; |
| DASH | dietary approaches to Stop Hypertension |
| DEXA | dual-energy X-ray absorptiometry |
| ECM | extracellular matrix |
| ESMO | European society of medical oncology |
| EVOO | extra virgin olive oil |
| ETC | electron transport chain; |
| FAI | Fat Attenuation Index |
| FDA | Food and Drug Administration |
| FI | Food insecurity |
| FMF | Familial Mediterranean Fever |
| GLP-1 | glucagon-like peptide 1 |
| GLP-1 RAs | Glucagon-like peptide-1 receptor agonists; |
| HbA1c | hemoglobin A1c |
| HF | heart failure |
| HMG-CoA | 3-hydroxy-3-methylglutaryl-CoA |
| hs | high-sensitivity |
| ICAM-1 | intercellular cell adhesion molecule-1 |
| ICB | immune checkpoint blockade |
| ICIs | immune checkpoint inhibitors |
| IGFR | |
| IL | interleukin |
| IOM | Institute of Medicine |
| irAEs | immune-related adverse events |
| LDL-C | low-density lipoprotein cholesterol |
| LDLRs | LDL receptors |
| LLT | lipid lowering therapy |
| LKB1 | liver kinase B1 |
| Lp(a) | lipoprotein(a) |
| LPS | lipopolysaccharide |
| MACE | major adverse cardiovascular events |
| MAPK | mitogen-activated protein kinase |
| MCP-1 | monocyte chemoattractant protein-1 |
| MDA | malondialdehyde |
| MDSCs | myeloid-derived suppressor cells |
| MESA | Multi-Ethnic Study of Atherosclerosis |
| MetS | metabolic syndrome |
| mGPD | mitochondrial glycerol-3-phosphate dehydrogenase |
| MI | myocardial infarction |
| MMP-9 | matrix metalloproteinase 9 |
| mTORC1 | mechanistic target of rapamycin complex 1; |
| NCDs | non-communicable diseases |
| NET | neutrophil extracellular trap |
| NF-Kb | nuclear factor-kB |
| NLRP3 | nucleotide oligomerization domain-like receptor protein 3 |
| NLR | neutrophil-lymphocyte ratio |
| NO | nitric oxide |
| Non-HDL-C | non–high-density lipoprotein cholesterol |
| NRT | Nicotine Replacement Therapy |
| NSCLC | non–small-cell lung cancer |
| OCT | optical coherence tomography |
| PA | Physical activity |
| PCa | prostate cancer |
| PCEs | Pooled Cohort Equations |
| PCSK9-Is | proprotein convertase subtilisin/kexin type 9 Inhibitors |
| PD-L1 | programmed death ligand 1 |
| PESA | Progression of Early Subclinical Atherosclerosis |
| PET | Positron emission tomography |
| PUFA | polyunsaturated fatty acids |
| PVAT | perivascular adipose tissue |
| RCT | randomized controlled trial |
| SCFAs | short-chain fatty acids |
| SCORE2 | Systematic Coronary Risk Estimation 2 |
| SCORE2-OP | SCORE2-Older Persons |
| SDOH | social determinants of health |
| SGLT2-Is | sodium-glucose co-transporter-2 inhibitors |
| T2DM | type 2 diabetes mellitus |
| TMAO | trimethylamine N-oxide |
| TNF-α | tumor necrosis factor-alpha |
| TG | triglycerides |
| TGF-β | transforming growth factor-β |
| TyG index | logarithmized semi-product of fasting levels of triglycerides and glucose {ln [triglycerides (mg/dl) x blood glucose (mg/dl)/2]} |
| UPF | ultra-processed foods |
| VCAM-1 | vascular cell adhesion molecule-1 |
References
- Kobo, O.; Raisi-Estabragh, Z.; Gevaert, S.; Rana, J.S.; Van Spall, H.G.C.; Roguin, A.; Petersen, S.E.; Ky, B.; Mamas, M.A. Impact of cancer diagnosis on distribution and trends of cardiovascular hospitalizations in the USA between 2004 and 2017. Eur Heart J Qual Care Clin Outcomes. 2022, 8, 787–797. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lloyd-Jones, D.M.; Ning, H.; Labarthe, D.; Brewer, L.; Sharma, G.; Rosamond, W.; Foraker, R.E.; Black, T.; Grandner, M.A.; Allen, N.B. Status of cardiovascular health in US adults and children using the American Heart Association’s new “Life’s essential 8” metrics: prevalence estimates from the National Health and Nutrition Examination Survey (NHANES), 2013 through 2018. Circulation. 2022, 146, 822–835. [Google Scholar] [CrossRef]
- Abramov, D.; Kobo, O.; Mamas, M.A. Association of Cardiovascular Health Metrics and Mortality Among Individuals With and Without Cancer. J Am Heart Assoc. 2024, 13, e032683. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kaneko, H.; Suzuki, Y.; Ueno, K.; Okada, A.; Fujiu, K.; Matsuoka, S.; Michihata, N.; Jo, T.; Takeda, N.; Morita, H.; et al. Association of Life's Simple 7 with incident cardiovascular disease in 53 974 patients with cancer. Eur J Prev Cardiol. 2022, 29, 2324–2332. [Google Scholar] [CrossRef] [PubMed]
- Rasmussen-Torvik, L.J.; Shay, C.M.; Abramson, J.G.; Friedrich, C.A.; Nettleton, J.A.; Prizment, A.E.; Folsom, A.R. Ideal cardiovascular health is inversely associated with incident cancer: the Atherosclerosis Risk In Communities study. Circulation. 2013, 127, 1270–5. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno,D. ; et al. ESC National Cardiac Societies; ESC Scientific Document Group. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice. Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Virani, S.S.; Newby, L.K.; Arnold, S.V.; Bittner, V.; Brewer, L.C.; Demeter, S.H.; Dixon, D.L.; Fearon, W.F.; Hess, B.; Johnson, H.M.; et al. Peer Review Committee Members. 2023 AHA/ACC/ACCP/ASPC/NLA/PCNA Guideline for the Management of Patients With Chronic Coronary Disease: A Report of the American Heart Association/American College of Cardiology Joint Committee on Clinical Practice Guidelines. Circulation. 2023, 148, e9–e119. [Google Scholar] [CrossRef] [PubMed]
- Klimis, H.; Pinthus, J.H.; Aghel, N.; Duceppe, E.; Fradet, V.; Brown, I.; Siemens, D.R.; Shayegan, B.; Klotz, L.; Luke, P.P.; et al. The Burden of Uncontrolled Cardiovascular Risk Factors in Men With Prostate Cancer: A RADICAL-PC Analysis. JACC CardioOncol. 2023, 5, 70–81. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sun, L.; Parikh, R.B.; Hubbard, R.A.; Cashy,J. ; Takvorian, S.U.; Vaughn, D.J.; Robinson, K.W.; Narayan, V.; Ky, B. Assessment and Management of Cardiovascular Risk Factors Among US Veterans With Prostate Cancer. JAMA Netw Open. 2021, 4, e210070. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Caro-Codón, J.; López-Fernández, T.; Álvarez-Ortega, C.; Zamora Auñón, P.; Rodríguez, I.R.; Gómez Prieto, P.; Buño Soto, A.; Canales Albendea, M.; Albaladejo, A.; Mediavilla, G.; et al. CARDIOTOX registry investigators. Cardiovascular risk factors during cancer treatment. Prevalence and prognostic relevance: insights from the CARDIOTOX registry. Eur J Prev Cardiol. [CrossRef] [PubMed]
- Weaver, K.E.; Dressler, E.V.; Smith, S.; Nightingale, C.L.; Klepin, H.D.; Lee, S.C.; Wells, B.J.; Hundley, W.G.; DeMari, J.A.; Price, S.N.; et al. Cardiovascular health assessment in routine cancer follow-up in community settings: survivor risk awareness and perspectives. BMC Cancer. 2024, 24, 158. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sayed, A.; Munir, M.; Addison, D.; Abushouk, A.I.; Dent, S.F.; Neilan, T.G.; Blaes, A.; Fradley, M.G.; Nohria, A.; Moustafa, K.; et al. The underutilization of preventive cardiovascular measures in patients with cancer: an analysis of the Behavioural Risk Factor Surveillance System, 2011-22. Eur J Prev Cardiol. 2023, 30, 1325–1332. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- McCracken, C.; Condurache, D.G.; Szabo, L.; Elghazaly, H.; Walter F.M.; Mead A.J.; Chakraverty R.; Harvey N.C.; Charlotte, H.; Petersen, S.E.; et al. Predictive Performance of Cardiovascular Risk Scores in Cancer Survivors From the UK Biobank. JACC: CardioOncology Volume 6, Issue 4, August 2024, Pages 575-588. [CrossRef]
- Gallucci, G.; Turazza, F.M.; Inno, A.; Canale, M.L.; Silvestris, N.; Farì, R.; Navazio, A.; Pinto, C.; Tarantini,L. Atherosclerosis and the Bidirectional Relationship between Cancer and Cardiovascular Disease: From Bench to Bedside-Part 1. Int J Mol Sci. 2024, 25, 4232. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wagner, K.H.; Brath, H. A global view on the development of non communicable diseases. Prev Med. 2012, 54, S38–41. [Google Scholar] [CrossRef] [PubMed]
- Uddin, R.; Lee, E.Y.; Khan, S.R.; Tremblay, M.S.; Khan, A. Clustering of lifestyle risk factors for non-communicable diseases in 304,779 adolescents from 89 countries: A global perspective. Prev Med. 2020, 131, 105955. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Cancer Risk Factors Collaborators. The global burden of cancer attributable to risk factors, 2010–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2022, 400, 563–591. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Fan, X.; Wei, L.; Yang, K.; Jiao, M. The impact of high-risk lifestyle factors on all-cause mortality in the US non-communicable disease population. BMC Public Health. 2023, 23, 422. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Global Cardiovascular Risk Consortium; Magnussen, C.; Ojeda, F.M.; Leong, D.P.; Alegre-Diaz, J.; Amouyel, P.; Aviles-Santa, L.; De Bacquer, D.; Ballantyne, C.M.; Bernabé-Ortiz, A.; Bobak, M; et al. Global Effect of Modifiable Risk Factors on Cardiovascular Disease and Mortality. N. Engl. J. Med. 2023, 389, 1273–1285. [CrossRef] [PubMed]
- Freisling, H.; Viallon, V.; Lennon, H.; Bagnardi, V.; Ricci, C.; Butterworth, A.S.; Sweeting, M.; Muller, D.; Romieu, I.; Bazelle, P.; et al. Lifestyle factors and risk of multimorbidity of cancer and cardiometabolic diseases: a multinational cohort study. BMC Med. 2020, 18, 5. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ortiz, C.; López-Cuadrado, T.; Rodríguez-Blázquez, C.; Pastor-Barriuso, R.; Galán, I. Clustering of unhealthy lifestyle behaviors, self-rated health and disability. Prev Med. 2022, 155, 106911. [Google Scholar] [CrossRef] [PubMed]
- Shi, S.; Huang, H.; Huang, Y.; Zhong, V.W.; Feng, N. Lifestyle Behaviors and Cardiometabolic Diseases by Race and Ethnicity and Social Risk Factors Among US Young Adults, 2011 to 2018. J Am Heart Assoc. 2023, 12, e028926. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chen, X.; Ding, J.; Li, H.; Carr, P.R.; Hoffmeister, M.; Brenner, H. The power of a healthy lifestyle for cancer prevention: the example of colorectal cancer. Cancer Biol Med. 2022, 19, 1586–97. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stein, K.D.; Syrjala, K.L.; Andrykowski, M.A. Physical and psychological long-term and late effects of cancer. Cancer. 2008, 112, 2577–92. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Emery, J.; Butow, P.; Lai-Kwon, J.; Nekhlyudov, L.; Rynderman, M.; Jefford, M. Management of common clinical problems experienced by survivors of cancer. Lancet. 2022, 399, 1537–1550. [Google Scholar] [CrossRef] [PubMed]
- Mollica, M.A.; Smith, A.W.; Tonorezos, E.; Castro, K.; Filipski, K.K.; Guida, J.; Perna, F.; Green, P.; Jacobsen, P.B.; Mariotto, A.; et al. Survivorship for Individuals Living With Advanced and Metastatic Cancers: National Cancer Institute Meeting Report. J Natl Cancer Inst. 2022, 114, 489–495. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mollica, M.A.; Zaleta, A.K.; Gallicchio, L.; Brick, R.; Jacobsen, P.B.; Tonorezos, E.; Castro, K.M.; Miller, M.F. Financial toxicity among people with metastatic cancer: findings from the Cancer Experience Registry. Support Care Cancer. 2024, 32, 137. [Google Scholar] [CrossRef] [PubMed]
- Ngan, T.T.; Tien, T.H.; Donnelly, M.; O'Neill, C. Financial toxicity among cancer patients, survivors and their families in the United Kingdom: a scoping review. J Public Health (Oxf). 2023, 45, e702–e713. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Valero-Elizondo, J.; Chouairi, F.; Khera, R.; Grandhi, G.R.; Saxena, A.; Warraich, H. J.; Virani, S.S.; Desai, N.R.; Sasangohar, F.; Krumholz, H.M.; et al. Atherosclerotic cardiovascular disease, cancer, and financial toxicity among adults in the United States. Cardio Oncology 2021; 3: 236-246.
- Osibogun, O.; Ogunmoroti, O.; Turkson-Ocran, R.A.; Okunrintemi, V.; Kershaw, K.N.; Allen, N.B.; & Michos, E.D. Financial strain is associated with poorer cardiovascular health: The multi-ethnic study of atherosclerosis. American Journal of Preventive Cardiology, 2024;17:100640.
- Shah, C. H.; Fonarow, G.C.; Echouffo-Tcheugui, J. B. Trends in direct health care costs among US adults with atherosclerotic cardiovascular disease with and without diabetes. Cardiovascular Diabetology, 2024;23: 238.
- Sukumar, S.; Wasfy, J.H.; Januzzi, J.L.; Peppercorn, J.; Chino, F.; Warraich, H. J. Financial toxicity of medical management of heart failure: JACC review topic of the week. Journal of the American College of Cardiology, 2023;81, 2043-2055.
- Carrera, P.M.; Curigliano, G.; Santini, D.; Sharp, L.; Chan, R.J.; Pisu, M.; Perrone, F.; Karjalainen, S.; Numico, G.; Cherny, N.; et al. ESMO expert consensus statements on the screening and management of financial toxicity in patients with cancer. ESMO Open. 2024, 9, 102992. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Orsini, M.; Trétarre, B.; Daurès, J.P.; Bessaoud, F. Individual socioeconomic status and breast cancer diagnostic stages: a French case-control study. Eur J Public Health. 2016, 26, 445–50. [Google Scholar] [CrossRef] [PubMed]
- Lyratzopoulos, G.; Abel, G.A.; Brown, C.H.; Rous, B.A.; Vernon, S.A.; Roland, M.; Greenberg, D.C. Socio-demographic inequalities in stage of cancer diagnosis: evidence from patients with female breast, lung, colon, rectal, prostate, renal, bladder, melanoma, ovarian and endometrial cancer. Ann Oncol. 2013, 24, 843–50. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yanez, B.; Perry, L.M.; Peipert, J.D.; Kuharic, M.; Taub, C.; Garcia, S.F.; Diaz, A.; Buitrago, D.; Mai, Q.; Gharzai, L.A.; et al. Exploring the Relationship Among Financial Hardship, Anxiety, and Depression in Patients With Cancer: A Longitudinal Study. JCO Oncol Pract. 2024, OP2400025. [Google Scholar] [CrossRef] [PubMed]
- Sandoval, J.L.; Franzoi, M.A.; di Meglio, A.; Ferreira, A.R.; Viansone, A.; André, F.; Martin, A.L.; Everhard, S.; Jouannaud, C.; Fournier, M.; et al. Magnitude and Temporal Variations of Socioeconomic Inequalities in the Quality of Life After Early Breast Cancer: Results From the Multicentric French CANTO Cohort. J Clin Oncol. 2024, 42, 2908–2917. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chao, C.; Bhatia, S.; Xu, L.; Cannavale, K.L.; Wong, F.L.; Huang, P.S.; Cooper, R.; Armenian, S.H. Chronic Comorbidities Among Survivors of Adolescent and Young Adult Cancer. J Clin Oncol. 2020, 38, 3161–3174. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dixon, S.B.; Wang, F.; Lu, L.; Wilson, C.L.; Green, D.M.; Merchant, T.E.; Srivastava, D.K.; Delaney, A.; Howell, R.M.; Jefferies, J.L.; et al. Prediabetes and Associated Risk of Cardiovascular Events and Chronic Kidney Disease Among Adult Survivors of Childhood Cancer in the St Jude Lifetime Cohort. J Clin Oncol. 2024, 42, 1031–1043. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, B.K.; Berger, S.L.; Brunet, A.; Campisi, J.; Cuervo, A.M.; Epel, E.S.; Franceschi, C.; Lithgow, G.J.; Morimoto,R. I.; Pessin, J.E.; et al. Geroscience: linking aging to chronic disease. Cell. 2014, 159, 709–13. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Furman, D.; Campisi, J.; Verdin, E.; Carrera-Bastos, P.; Targ, S.; Franceschi, C.; Ferrucci, L.; Gilroy, D.W.; Fasano, A.; Miller, G.W.; et al. Chronic inflammation in the etiology of disease across the life span. Nat Med. 2019, 25, 1822–1832. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rowland, J.H.; Bellizzi, K.M. Cancer survivorship issues: life after treatment and implications for an aging population. J Clin Oncol. 2014, 32, 2662–8. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jiang, C.; Deng, L.; Karr, M.A.; Wen, Y.; Wang, Q.; Perimbeti, S.; Shapiro, C.L.; Han, X. Chronic comorbid conditions among adult cancer survivors in the United States: Results from the National Health Interview Survey, 2002-2018. Cancer. 2022, 128, 828–838. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Whyne, E.Z.; Shults, E.M.; Choi, S-H. ; Dowell, J.E.; Conzen, S.; Jeon-Slaughter, H. Abstract 13066: Ten-Year Atherosclerotic Cardiovascular Risk Trajectory Among Women Veterans Diagnosed With Breast, Colorectal, Lung and Thyroid Cancer. Circulation. 2023, 148, A13066. [Google Scholar] [CrossRef]
- Sarfati, D.; Gurney, J.; Lim, B.T.; Bagheri, N.; Simpson, A.; Koea, J.; Dennett, E. Identifying important comorbidity among cancer populations using administrative data: Prevalence and impact on survival. Asia Pac J Clin Oncol. 2016, 12, e47–56. [Google Scholar] [CrossRef] [PubMed]
- Garg, T.; Young, A.J.; Kost, K.A.; Danella, J.F.; Larson, S.; Nielsen, M.E.; Kirchner, H.L. Burden of Multiple Chronic Conditions among Patients with Urological Cancer. J Urol. 2018, 199, 543–550. [Google Scholar] [CrossRef] [PubMed]
- Strongman, H.; Gadd, S.; Matthews, A.; Mansfield, K.E.; Stanway, S.; Lyon, A.R.; Dos-Santos-Silva, I.; Smeeth, L.; Bhaskaran, K. Medium and long-term risks of specific cardiovascular diseases in survivors of 20 adult cancers: a population-based cohort study using multiple linked UK electronic health records databases. Lancet. 2019, 394, 1041–1054. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fowler, H.; Belot, A.; Ellis, L.; Maringe, C.; Luque-Fernandez, M.A.; Njagi, E.N.; Navani, N. Sarfati, D. ; Rachet, B. Comorbidity prevalence among cancer patients: a population-based cohort study of four cancers. BMC Cancer. 2020, 20, 2. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Loeppenthin, K.; Dalton, S.O.; Johansen, C.; Andersen, E.; Christensen, M.B.; Pappot, H.; Petersen, L.N.; Thisted, L.B.; Frølich, A.; Mortensen, C.E.; et al. Total burden of disease in cancer patients at diagnosis-a Danish nationwide study of multimorbidity and redeemed medication. Br J Cancer. 2020, 123, 1033–1040. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Keats, M.R.; Cui, Y.; DeClercq, V.; Grandy, S.A.; Sweeney, E.; Dummer, T.J.B. Burden of multimorbidity and polypharmacy among cancer survivors: a population-based nested case-control study. Support Care Cancer. 2021, 29, 713–723. [Google Scholar] [CrossRef] [PubMed]
- Plasencia, G.; Gray, S.C.; Hall, I.J.; Smith, J.L. Multimorbidity clusters in adults 50 years or older with and without a history of cancer: National Health Interview Survey, 2018. BMC Geriatr. 2024, 24, 50. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Blaustein, J.R.; Quisel, M.J.; Hamburg, N.M.; Wittkopp, S. Environmental Impacts on Cardiovascular Health and Biology: An Overview. Circ Res. 2024, 134, 1048–1060. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Powell-Wiley, T.M.; Poirier, P.; Burke, L.E.; Després, J.P.; Gordon-Larsen, P.; Lavie, C.J.; Lear, S.A.; Ndumele, C.E.; Neeland, I.J.; Sanders, P.; et al. American Heart Association Council on Lifestyle and Cardiometabolic Health; Council on Cardiovascular and Stroke Nursing; Council on Clinical Cardiology; Council on Epidemiology and Prevention; and Stroke Council. Obesity and Cardiovascular Disease: A Scientific Statement From the American Heart Association. Circulation. 2021, 143, e984–e1010. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Swinburn, B.A.; Kraak, V.I.; Allender, S.; Atkins, V.J.; Baker, P.I.; Bogard, J.R.; Brinsden, H.; Calvillo, A.; De Schutter, O.; Devarajan, R.; et al. The Global Syndemic of Obesity, Undernutrition, and Climate Change: The Lancet Commission report. Lancet. 2019, 393, 791–846. [Google Scholar] [CrossRef] [PubMed]
- AHIMA, Rexford, S. Overview of metabolic syndrome. In: Metabolic syndrome: a comprehensive textbook. Cham: Springer International Publishing, 2024. p. 3-14.
- Larsson, S.C.; Spyrou, N.; Mantzoros, C.S. Body fatness associations with cancer: evidence from recent epidemiological studies and future directions. Metabolism. 2022, 137, 155326. [Google Scholar] [CrossRef] [PubMed]
- Liu, E.E.; Suthahar, N.; Paniagua, S.M.; Wang, D.; Lau, E.S.; Li, S.X.; Jovani, M.; Takvorian, K.S.; Kreger, B.E.; Benjamin, E.J.; et al. Association of Cardiometabolic Disease With Cancer in the Community. JACC CardioOncol. 2022, 4, 69–81. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- McGill, H.C. Jr; McMahan, C.A.; Herderick, E.E.; Zieske, A.W.; Malcom, G.T.; Tracy, R.E.; Strong, J.P. Pathobiological Determinants of Atherosclerosis in Youth (PDAY) Research Group. Obesity accelerates the progression of coronary atherosclerosis in young men. Circulation. 2002, 105, 2712–8. [Google Scholar] [CrossRef] [PubMed]
- Tan, D.J.H.; Ng, C.H.; Muthiah, M.; Yong, J.N.; Chee, D.; Teng, M.; Wong, Z.Y.; Zeng, R.W.; Chin, Y.H.; Wang, J.W.; et al. Rising global burden of cancer attributable to high BMI from 2010 to 2019. Metabolism. 2023, 152, 155744. [Google Scholar] [CrossRef] [PubMed]
- Jensen, B.W.; Aarestrup, J.; Blond, K.; Jørgensen, M.E.; Renehan, A.G.; Vistisen, D.; Baker, J.L. ; Childhood body mass index trajectories, adult-onset type 2 diabetes, and obesity-related cancers. J Natl Cancer Inst. 2023, 115, 43–51. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Meyer, J.F.; Larsen, S.B.; Blond, K.; Damsgaard, C.T.; Bjerregaard, L.G.; Baker, J.L. Associations between body mass index and height during childhood and adolescence and the risk of coronary heart disease in adulthood: A systematic review and meta-analysis. Obes Rev. 2021, 22, e13276. [Google Scholar] [CrossRef] [PubMed]
- Falaschetti, E.; Hingorani, A.D.; Jones, A.; Charakida, M.; Finer, N.; Whincup, P.; Lawlor, D.A.; Davey Smith, G.; Sattar, N.; Deanfield, J.E. Adiposity and cardiovascular risk factors in a large contemporary population of pre-pubertal children. Eur Heart J. 2010, 31, 3063–72. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cardel, M.I.; Atkinson, M.A.; Taveras, E.M.; Holm, J.C.; Kelly, A.S. Obesity Treatment Among Adolescents: A Review of Current Evidence and Future Directions. JAMA Pediatr. 2020, 174, 609–617. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Jacobs, D.R.Jr; Woo, J.G.; Sinaiko, A.R.; Daniels, S.R.; Ikonen, J.; Juonala, M.; Kartiosuo, N.; Lehtimäki, T.; Magnussen, C.G.; Viikari, J.S.A.; et al. Childhood Cardiovascular Risk Factors and Adult Cardiovascular Events. N Engl J Med. 2022, 386, 1877–1888. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wu, F.; Juonala, M.; Jacobs, D.R. Jr; Daniels, S.R.; Kähönen, M.; Woo, J.G.; Sinaiko, A.R.; Viikari, J.S.A.; Bazzano, L.A.; Burns, T.L.; et al. Childhood Non-HDL Cholesterol and LDL Cholesterol and Adult Atherosclerotic Cardiovascular Events. Circulation. 2024, 149, 217–226. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Friera, L.; Peñalvo, J.L.; Fernández-Ortiz, A.; Ibañez, B.; López-Melgar, B.; Laclaustra, M.; Oliva, B.; Mocoroa, A.; Mendiguren, J.; Martínez de Vega, V.; et al. Prevalence, Vascular Distribution, and Multiterritorial Extent of Subclinical Atherosclerosis in a Middle-Aged Cohort: The PESA (Progression of Early Subclinical Atherosclerosis) Study. Circulation 2015, 131, 2104–2113. [Google Scholar] [CrossRef] [PubMed]
- López-Melgar, B.; Fernández-Friera, L.; Oliva, B.; García-Ruiz, J.M.; Sánchez-Cabo, F.; Bueno, H.; Mendiguren, J.M.; Lara-Pezzi, E.; Andrés, V.; Ibáñez, B.; et al. Short-Term Progression of Multiterritorial Subclinical Atherosclerosis. J Am Coll Cardiol. 2020, 75, 1617–1627. [Google Scholar] [CrossRef] [PubMed]
- Simental-Mendía, L.E.; Rodríguez-Morán, M.; Guerrero-Romero, F. The product of fasting glucose and triglycerides as surrogate for identifying insulin resistance in apparently healthy subjects. Metab Syndr Relat Disord. 2008, 6, 299–304. [Google Scholar] [CrossRef] [PubMed]
- Guerrero-Romero, F.; Simental-Mendía, L.E.; González-Ortiz, M.; Martínez-Abundis, E.; Ramos-Zavala, M.G.; Hernández-González, S.O.; Jacques-Camarena, O.; Rodríguez-Morán, M. The product of triglycerides and glucose, a simple measure of insulin sensitivity. Comparison with the euglycemic-hyperinsulinemic clamp. J Clin Endocrinol Metab. 2010, 95, 3347–51. [Google Scholar] [CrossRef] [PubMed]
- Nabipoorashrafi, S.A.; Seyedi, S.A.; Rabizadeh, S.; Ebrahimi, M.; Ranjbar, S.A.; Reyhan, S.K.; Meysamie, A.; Nakhjavani, M.; Esteghamati, A. The accuracy of triglyceride-glucose (TyG) index for the screening of metabolic syndrome in adults: A systematic review and meta-analysis. Nutr Metab Cardiovasc Dis. 2022, 32, 2677–2688. [Google Scholar] [CrossRef] [PubMed]
- D'Elia, L.; Masulli, M.; Virdis, A.; Casiglia, E.; Tikhonoff, V.; Angeli, F.; Barbagallo, C.M.; Bombelli, M.; Cappelli, F.; Cianci, R.; et al. Triglyceride-glucose Index and Mortality in a Large Regional-based Italian Database (Urrah Project). J Clin Endocrinol Metab. 2024, 14, dgae170. [Google Scholar] [CrossRef] [PubMed]
- Che, B.; Zhong, C.; Zhang, R.; Pu, L.; Zhao, T.; Zhang, Y.; Han, L. Triglyceride-glucose index and triglyceride to high-density lipoprotein cholesterol ratio as potential cardiovascular disease risk factors: an analysis of UK biobank data. Cardiovasc Diabetol. 2023, 22, 34. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lopez-Jaramillo, P.; Gomez-Arbelaez, D.; Martinez-Bello, D.; Abat, M.E.M.; Alhabib, K.F.; Avezum, Á.; Barbarash, O.; Chifamba, J.; Diaz, M.L.; Gulec, S.; et al. Association of the triglyceride glucose index as a measure of insulin resistance with mortality and cardiovascular disease in populations from five continents (PURE study): a prospective cohort study. Lancet Healthy Longev. 2023, 4, e23–e33. [Google Scholar] [CrossRef] [PubMed]
- Fritz, J.; Bjørge, T.; Nagel, G.; Manjer, J.; Engeland, A.; Häggström, C.; Concin, H.; Teleka, S. , Tretli, S.; Gylling, B, et al. The triglyceride-glucose index as a measure of insulin resistance and risk of obesity-related cancers. Int J Epidemiol. 2020, 49, 193–204. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Zhou, L.; Yang, S.; Zhou, H. The relationship between Triglyceride and glycose (TyG) index and the risk of gynaecologic and breast cancers. Clin Nutr ESPEN. 2022, 51, 345–352. [Google Scholar] [CrossRef] [PubMed]
- Liang, S.; Wang, C.; Zhang, J.; Liu, Z.; Bai, Y.; Chen, Z.; Huang, H.; He, Y. Triglyceride-glucose index and coronary artery disease: a systematic review and meta-analysis of risk, severity, and prognosis. Cardiovasc Diabetol. 2023, 22, 170. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ding, X.; Wang, X.; Wu, J.; Zhang, M.; Cui, M. Triglyceride-glucose index and the incidence of atherosclerotic cardiovascular diseases: a meta-analysis of cohort studies. Cardiovasc Diabetol. 2021, 20, 76. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tao, L.C.; Xu, J.N.; Wang, T.T.; Hua, F.; Li, J.J. Triglyceride-glucose index as a marker in cardiovascular diseases: landscape and limitations. Cardiovasc Diabetol. 2022, 21, 68. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bertero, E.; Carmisciano, L.; Jonasson, C.; Butler, J.; Maack, C.; Ameri, P. Association of inflammatory markers with incident heart failure or cancer in the HUNT3 and Health ABC population studies. European Journal of Preventive Cardiology 2024, 31, 1400–1407. [Google Scholar] [CrossRef] [PubMed]
- Van't Klooster, C.C.; Ridker, P.M.; Hjortnaes, J.; van der Graaf, Y. ; Asselbergs,F. W.; Westerink, J.; Aerts, J.G.J.V.; Visseren, F.L.J. The relation between systemic inflammation and incident cancer in patients with stable cardiovascular disease: a cohort study. Eur Heart J. 2019, 40, 3901–3909. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Oikawa, T.; Sakata, Y.; Nochioka, K.; Miura, M.; Abe, R.; Kasahara, S.; Sato, M.; Aoyanagi, H.; Shiroto, T.; Sugimura, K.; et al.; CHART-2 Investigators Increased risk of cancer death in patients with chronic heart failure with a special reference to inflammation-A report from the CHART-2 Study. Int J Cardiol. 2019, 290, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Mazhar, F.; Faucon, A.L.; Fu, E.L.; Szummer, K.E.; Mathisen, J.; Gerward, S.; Reuter, S.B.; Marx, N.; Mehran, R.; Carrero, J.J. Systemic inflammation and health outcomes in patients receiving treatment for atherosclerotic cardiovascular disease. Eur Heart J. 2024, ehae557. [Google Scholar] [CrossRef] [PubMed]
- Fest, J.; Ruiter, R.; Mulder, M.; Groot Koerkamp, B.; Ikram, M.A.; Stricker, B.H.; van Eijck, C.H.J. The systemic immune-inflammation index is associated with an increased risk of incident cancer-A population-based cohort study. Int J Cancer. 2020, 146, 692–698. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Deng, X.; Liu, D.; Li, M.; He, J.; Fu, Y. Association between systemic immune-inflammation index and insulin resistance and mortality. Sci Rep. 2024, 14, 2013. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yang, R.; Chang, Q.; Meng, X.; Gao, N.; Wang, W. Prognostic value of Systemic immune-inflammation index in cancer: A meta-analysis. J Cancer. 2018, 9, 3295–3302. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yang, Y.L.; Wu, C.H.; Hsu, P.F.; Chen, S.C.; Huang, S.S.; Chan WL, Lin SJ, Chou CY, Chen JW, Pan JP, et al. Systemic immune-inflammation index (SII) predicted clinical outcome in patients with coronary artery disease. Eur J Clin Invest. 2020, 50, e13230. [Google Scholar] [CrossRef] [PubMed]
- Xu, B.; Wu, Q.; La, R.; Lu, L.; Abdu, F.A.; Yin, G.; Zhang, W.; Ding, W.; Ling, Y.; He, Z.; et al. Is systemic inflammation a missing link between cardiometabolic index with mortality? Evidence from a large population-based study. Cardiovasc Diabetol. 2024, 23, 212. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Björnson, E.; Adiels, M.; Gummesson, A.; Taskinen, M.R.; Burgess, S.; Packard, C.J.; Borén, J. Quantifying Triglyceride-Rich Lipoprotein Atherogenicity, Associations With Inflammation, and Implications for Risk Assessment Using Non-HDL Cholesterol. J Am Coll Cardiol. 2024, 84, 1328–1338. [Google Scholar] [CrossRef] [PubMed]
- Perdomo, C.M.; Avilés-Olmos, I.; Dicker, D.; Frühbeck, G. Towards an adiposity-related disease framework for the diagnosis and management of obesities. Rev Endocr Metab Disord. 2023, 24, 795–807. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Cypess, A.M. Reassessing Human Adipose Tissue. N Engl J Med. 2022, 386, 768–779. [Google Scholar] [CrossRef] [PubMed]
- Cespedes Feliciano, E.M.; Chen, W.Y.; Bradshaw, P.T.; Prado, C.M.; Alexeeff, S.; Albers, K.B.; Castillo, A.L.; Caan, B.J. Adipose Tissue Distribution and Cardiovascular Disease Risk Among Breast Cancer Survivors. J Clin Oncol. 2019, 37, 2528–2536. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wibmer, A.G.; Dinh, P.C.; Travis, L.B.; Chen, C.; Bromberg, M.; Zheng, J.; Capanu, M.; Sesso, H.D.; Feldman, D.R.; Vargas, H.A. Associations of Body Fat Distribution and Cardiometabolic Risk of Testicular Cancer Survivors After Cisplatin-Based Chemotherapy. JNCI Cancer Spectr. 2022, 6, pkac030. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Barbi, J.; Patnaik, S.K.; Pabla, S.; Zollo, R.; Smith, R.J.Jr; Sass, S.N.; Srinivasan, A.; Petrucci, C.; Seager, R.; Conroy, J.; et al. Visceral Obesity Promotes Lung Cancer Progression-Toward Resolution of the Obesity Paradox in Lung Cancer. J Thorac Oncol. 2021, 16, 1333–1348. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chaplin, A.; Rodriguez, R.M.; Segura-Sampedro, J.J.; Ochogavía-Seguí, A.; Romaguera, D.; Barceló-Coblijn, G. Insights behind the Relationship between Colorectal Cancer and Obesity: Is Visceral Adipose Tissue the Missing Link? Int J Mol Sci. 2022, 23, 13128. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Williams, G.R.; Dunne, R.F.; Giri, S.; Shachar, S.S.; Caan, B.J. Sarcopenia in the Older Adult With Cancer. J Clin Oncol. 2021, 39, 2068–2078. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Atkins, J.L.; Wannamathee, S.G. Sarcopenic obesity in ageing: cardiovascular outcomes and mortality. Br J Nutr. 2020, 124, 1102–1113. [Google Scholar] [CrossRef] [PubMed]
- Batsis, J.A.; Mackenzie, T.A.; Jones, J.D.; Lopez-Jimenez, F.; Bartels, S.J. Sarcopenia, sarcopenic obesity and inflammation: Results from the 1999-2004 National Health and Nutrition Examination Survey. Clin Nutr. 2016, 35, 1472–1483. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bilski, J.; Pierzchalski, P.; Szczepanik, M.; Bonior, J.; Zoladz, J.A. Multifactorial Mechanism of Sarcopenia and Sarcopenic Obesity. Role of Physical Exercise, Microbiota and Myokines. Cells. 2022, 11, 160. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ko, B.J.; Chang, Y.; Jung, H.S.; Yun, K.E.; Kim, C.W.; Park, H.S.; Chung, E.C.; Shin, H.; Ryu, S. Relationship Between Low Relative Muscle Mass and Coronary Artery Calcification in Healthy Adults. Arterioscler Thromb Vasc Biol. 2016, 36, 1016–21. [Google Scholar] [CrossRef] [PubMed]
- Jun, J.E.; Choi, M.S.; Park, S.W.; Kim, G.; Jin, S.M.; Kim, K.; Hwang, Y.C.; Ahn, K.J.; Chung, H.Y.; Jeong, I.K.; et al. Low Skeletal Muscle Mass Is Associated With the Presence, Incidence, and Progression of Coronary Artery Calcification. Can J Cardiol. 2021, 37, 1480–1488. [Google Scholar] [CrossRef] [PubMed]
- Bano, G.; Trevisan, C.; Carraro, S.; Solmi, M.; Luchini, C.; Stubbs, B.; Manzato, E.; Sergi, G.; Veronese, N. Inflammation and sarcopenia: A systematic review and meta-analysis. Maturitas. 2017, 96, 10–15. [Google Scholar] [CrossRef] [PubMed]
- Öztürk, Z.A.; Kul, S.; Türkbeyler, İ.H.; Sayıner, Z.A.; Abiyev, A. Is increased neutrophil lymphocyte ratio remarking the inflammation in sarcopenia? Exp Gerontol. 2018, 110, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Açar, G.; Fidan, S.; Uslu, Z.A.; Turkday, S.; Avci, A.; Alizade, E.; Kalkan, M.E.; Tabakci, O.N.; Tanboğa, I.H.; Esen, A.M. Relationship of neutrophil-lymphocyte ratio with the presence, severity, and extent of coronary atherosclerosis detected by coronary computed tomography angiography. Angiology. 2015, 66, 174–9. [Google Scholar] [CrossRef] [PubMed]
- Adamstein, N.H.; MacFadyen, J.G.; Rose, L.M.; Glynn, R.J.; Dey, A.K.; Libby, P.; Tabas, I.A.; Mehta, N.N.; Ridker, P.M. The neutrophil-lymphocyte ratio and incident atherosclerotic events: analyses from five contemporary randomized trials. Eur Heart J. 2021, 42, 896–903. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Takenaka, Y.; Oya, R.; Takemoto, N.; Inohara, H. Predictive impact of sarcopenia in solid cancers treated with immune checkpoint inhibitors: a meta-analysis. J Cachexia Sarcopenia Muscle. 2021, 12, 1122–1135. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Abolhassani, A.R.; Schuler, G.; Kirchberger, M.C.; Heinzerling, L. C-reactive protein as an early marker of immune-related adverse events. J Cancer Res Clin Oncol. 2019, 145, 2625–2631. [Google Scholar] [CrossRef] [PubMed]
- Husain, B.; Kirchberger, M.C.; Erdmann, M.; Schüpferling, S.; Abolhassani, A.R.; Fröhlich, W.; Berking, C.; Heinzerling, L. Inflammatory markers in autoimmunity induced by checkpoint inhibitors. J Cancer Res Clin Oncol. 2021, 147, 1623–1630. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lin, H.M.; Yang, X.; Centenera, M.M.; Huynh, K.; Giles, C.; Dehairs, J.; Swinnen, J.V.; Hoy, A.J.; Meikle, P.J.; Butler, L.M.; et al. Circulating Lipid Profiles Associated With Resistance to Androgen Deprivation Therapy in Localized Prostate Cancer. JCO Precis Oncol. 2024, 8, e2400260. [Google Scholar] [CrossRef] [PubMed]
- Lloyd-Jones, D.M.; Hong, Y.; Labarthe, D.; Mozaffarian, D.; Appel, L.J.; Van Horn, L.; Greenlund, K.; Daniels, S.; Nichol, G.; Tomaselli, G.F.; et al. American Heart Association Strategic Planning Task Force and Statistics Committee. Defining and setting national goals for cardiovascular health promotion and disease reduction: The American Heart Association’s strategic Impact Goal through 2020 and beyond. Circulation 2010, 121, 586–613.
- Miglietta, F.; Bottosso, M.; Griguolo, G.; Dieci, M.V.; Guarneri, V. Major advancements in metastatic breast cancer treatment: when expanding options means prolonging survival. ESMO Open. 2022 Apr;7(2):100409. [CrossRef] [PubMed]
- Howlader, N.; Forjaz, G.; Mooradian, M.J.; Meza, R.; Kong, C.Y.; Cronin, K.A.; Mariotto, A.B.; Lowy, D.R.; Feuer, E.J. The Effect of Advances in Lung-Cancer Treatment on Population Mortality. N Engl J Med. 2020, 383, 640–649. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guida, J.L.; Ahles, T.A.; Belsky, D.; Campisi, J.; Cohen HJ, DeGregori, J. ; Fuldner, R.; Ferrucci, L.; Gallicchio, L.; Gavrilov, L.; et al. Measuring Aging and Identifying Aging Phenotypes in Cancer Survivors. J Natl Cancer Inst. 2019, 111, 1245–1254. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guida, J.L.; Agurs-Collins, T.; Ahles, T.A.; Campisi, J.; Dale, W.; Demark-Wahnefried, W.; Dietrich, J.; Fuldner, R.; Gallicchio, L.; Green, P.A.; et al. Strategies to Prevent or Remediate Cancer and Treatment-Related Aging. J Natl Cancer Inst. 2021, 113, 112–122. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hasbani, N.R.; Ligthart, S.; Brown, M.R.; Heath, A.S.; Bebo, A.; Ashley, K.E.; Boerwinkle, E.; Morrison, A.C.; Folsom, A.R.; Aguilar, D.; et al. American Heart Association's Life's Simple 7: Lifestyle Recommendations, Polygenic Risk, and Lifetime Risk of Coronary Heart Disease. Circulation. 2022, 145, 808–818. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, G.; Li, Y.; Hu, Y.; Zong, G.; Li, S.; Rimm, E.B.; Hu, F.B.; Manson, J.E.; Rexrode, K.M.; Shin, H.J.; et al. Influence of Lifestyle on Incident Cardiovascular Disease and Mortality in Patients With Diabetes Mellitus. J Am Coll Cardiol. 2018, 71, 2867–2876. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ricardo, A.C.; Anderson, C.A.; Yang, W.; Zhang, X.; Fischer, M.J.; Dember, L.M.; Fink, J.C. Frydrych, A.; Jensvold, N.G.; Lustigova, E.; et al. CRIC Study Investigators. Healthy lifestyle and risk of kidney disease progression, atherosclerotic events, and death in CKD: findings from the Chronic Renal Insufficiency Cohort (CRIC) Study. Am J Kidney Dis. 2015, 65, 412–24. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chang, H.M.; Moudgil, R.; Scarabelli, T.; Okwuosa, T.M.; Yeh, E.T.H. Cardiovascular complications of cancer therapy: best practices in diagnosis, prevention, and management: Part 1. J Am Coll Cardiol. 2017, 70, 2536–51.
- Cohen, J.B.; Brown, N.J.; Brown, S.A.; Dent, S.; van Dorst, D.C.H.; Herrmann, S.M.; Lang, N.N.; Oudit, G.Y.; Touyz, R.M. American Heart Association Council on Hypertension; Council on Arteriosclerosis, Thrombosis and Vascular Biology; and Council on the Kidney in Cardiovascular Disease. Cancer Therapy-Related Hypertension: A Scientific Statement From the American Heart Association. Hypertension. 2023, 80, e46–e57. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Butel-Simoes, L.E.; Haw, T.J.; Williams, T.; Sritharan, S.; Gadre, P.; Herrmann, S.M.; Herrmann, J.; Ngo, D.T. M, Sverdlov, A.L. Established and Emerging Cancer Therapies and Cardiovascular System: Focus on Hypertension-Mechanisms and Mitigation. Hypertension 2023, 80, 685–710. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Okwuosa, T.M.; Morgans, A.; Rhee, J.W.; Reding, K.W.; Maliski, S.; Plana, J.C.; Volgman, A.S.; Moseley, K.F.; Porter, C.B.; Ismail-Khan, R. American Heart Association Cardio-Oncology Subcommittee of the Council on Clinical Cardiology and the Council on Genomic and Precision Medicine; Council on Arteriosclerosis, Thrombosis and Vascular Biology; and Council on Cardiovascular Radiology and Intervention. Impact of Hormonal Therapies for Treatment of Hormone-Dependent Cancers (Breast and Prostate) on the Cardiovascular System: Effects and Modifications: A Scientific Statement From the American Heart Association. Circ Genom Precis Med. 2021, 14, e000082. [Google Scholar] [CrossRef] [PubMed]
- Rillamas-Sun, E.; Kwan, M.L.; Iribarren, C.; Cheng, R.; Neugebauer, R.; Rana, J.S.; Nguyen-Huynh, M.; Shi, Z.; Laurent, C.A.; Lee, V.S.; et al. Development of cardiometabolic risk factors following endocrine therapy in women with breast cancer. Breast Cancer Res Treat. 2023, 201, 117–126. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chan, J.S.K.; Satti, D.I.; Lee, Y.H.A.; Hui, J.M.H.; Dee, E.C.; Ng, K.; Liu, K.; Tse, G.; Ng, C.F. ; Temporal trends in cardiovascular burden among patients with prostate cancer receiving androgen deprivation therapy: a population-based cohort study. Br J Cancer. 2023, 128, 2253–2260. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kaneko, H.; Yano, Y.; Lee, H.; Lee, H.H.; Okada, A.; Suzuki, Y.; Itoh, H.; Matsuoka, S.; Fujiu, K.; Michihata, N.; et al. Blood Pressure Classification Using the 2017 ACC/AHA Guideline and Heart Failure in Patients With Cancer. J Clin Oncol. 2023, 41, 980–990. [Google Scholar] [CrossRef] [PubMed]
- Ndumele, C.E.; Neeland, I.J.; Tuttle, K.R.; Chow, S.L.; Mathew, R.O.; Khan, S.S.; Coresh, J.; Baker-Smith, C.M.; Carnethon, M.R.; Després, J-P. ; et al. A synopsis of the evidence for the science and clinical management of cardiovascular-kidney-metabolic (CKM) syndrome: a scientific statement from the American Heart Association. Circulation. 2023, 148, 1636–1664. [Google Scholar] [CrossRef]
- Ndumele, C.E.; Rangaswami, J.; Chow, S.L.; Neeland, I.J.; Tuttle, K.R.; Khan, S.S.; Coresh, J.; Mathew, R.O.; Baker-Smith, C.M.; Carnethon, M.R.; et al. Cardiovascular-kidney-metabolic health: a presidential advisory from the American Heart Association. Circulation. 2023, 148, 1606–1635. [Google Scholar] [CrossRef]
- Shah, N.S.; Huang, X.; Petito, L.C. , Bancks, M.P.; Ning, H.; Cameron, N.A.; Kershaw, K.N.; Kandula, N.R.; Carnethon, M.R.; Lloyd-Jones, D.M.; et al. Social and psychosocial determinants of racial and ethnic differences in cardiovascular health in the United States population. Circulation. 2023, 147, 190–200. [Google Scholar] [CrossRef]
- Khan, S.S.; Matsushita, K.; Sang, Y.; Ballew, S.H.; Grams, M.E.; Surapaneni, A.; Blaha, M.J.; Carson, A.P.; Chang, A.R.; Ciemins, E.; et al. Chronic Kidney Disease Prognosis Consortium and the American Heart Association Cardiovascular-Kidney-Metabolic Science Advisory Group. Development and Validation of the American Heart Association's PREVENT Equations. Circulation. 2024, 149, 430–449. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stone, N.J.; Robinson, J.G.; Lichtenstein, A.H.; Bairey Merz, C.N.; Blum, C.B.; Eckel, R.H.; Goldberg, A.C.; Gordon, D.; Levy, D.; Lloyd-Jones, D.M.; et al. American College of Cardiology/American Heart Association Task Force on Practice Guidelines. 2013 ACC/AHA guideline on the treatment of blood cholesterol to reduce atherosclerotic cardiovascular risk in adults: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014, 63, 2889–934, Epub 2013 Nov 12. Erratum in: J Am Coll Cardiol. 2014 Jul 1;63(25 Pt B):3024-3025. Erratum in: J Am Coll Cardiol. 2015 Dec 22;66(24):2812. [Google Scholar] [CrossRef] [PubMed]
- Lyon, A.R.; López-Fernández, T.; Couch, L.S.; Asteggiano, R.; Aznar, M.C.; Bergler-Klein, J.; Boriani, G.; Cardinale, D.; Cordoba, R.; Cosyns, B.; et al. ESC Scientific Document Group. 2022 ESC Guidelines on cardio-oncology developed in collaboration with the European Hematology Association (EHA), the European Society for Therapeutic Radiology and Oncology (ESTRO) and the International Cardio-Oncology Society (IC-OS). Eur Heart J. 2022, 43, 4229–4361, Erratum in: Eur Heart J. 2023, 44, 1621. 10.1093/eurheartj/ehad196. [Google Scholar] [CrossRef] [PubMed]
- Razavi, A.C.; Agatston, A.S.; Shaw, L.J.; De Cecco, C.N.; van Assen, M.; Sperling, L.S.; Bittencourt, M.S.; Daubert, M.A.; Nasir, K.; Blumenthal, R.S.; et al. Evolving Role of Calcium Density in Coronary Artery Calcium Scoring and Atherosclerotic Cardiovascular Disease Risk. JACC Cardiovasc. Imaging 2022, 15, 1648–1662. [Google Scholar] [CrossRef]
- Williams, K.J. Eradicating Atherosclerotic Events by Targeting Early Subclinical Disease: It Is Time to Retire the Therapeutic Paradigm of Too Much, Too Late. Arterioscler Thromb Vasc Biol. 2024, 44, 48–64. [Google Scholar] [CrossRef] [PubMed]
- Chan, K.; Wahome, E.; Tsiachristas, A.; Antonopoulos, A.S.; Patel, P.; Lyasheva, M.; Kingham, L.; West, H.; Oikonomou, E.K.; Volpe, L.; et al. ORFAN Consortium. Inflammatory risk and cardiovascular events in patients without obstructive coronary artery disease: the ORFAN multicentre, longitudinal cohort study. Lancet. 2024, 403, 2606–2618. [Google Scholar] [CrossRef] [PubMed]
- Koenig, W.; Sund, M.; Fröhlich, M.; Fischer, H.G.; Löwel, H.; Döring, A.; Hutchinson, W.L.; Pepys, M.B. C-Reactive protein, a sensitive marker of inflammation, predicts future risk of coronary heart disease in initially healthy middle-aged men: results from the MONICA (Monitoring Trends and Determinants in Cardiovascular Disease) Augsburg Cohort Study, 1984, 99, 237-42. [CrossRef] [PubMed]
- Libby, P.; Ridker, P.M. Hansson GK. Inflammation in atherosclerosis: from pathophysiology to practice. J Am Coll Cardiol 2009; 54: 2129-8.
- Braunwald, E. Creating controversy where none exists: the important role of C-reactive protein in the CARE, AFCAPS/TexCAPS, PROVE IT, REVERSAL, A to Z, JUPITER, HEART PROTECTION, and ASCOT trials. Eur Heart J. 2012, 33, 430–2. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M. , Cannon, C.P.; Morrow, D.; Rifai, N.; Rose, L.M.; McCabe, C.H.; Pfeffer, M.A.; Braunwald, E. Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis in Myocardial Infarction 22 (PROVE IT-TIMI 22) Investigators. C-reactive protein levels and outcomes after statin therapy. N Engl J Med. 2005, 352, 20–8. [Google Scholar] [CrossRef] [PubMed]
- Morrow, D.A.; de Lemos, J.A.; Sabatine, M.S.; Wiviott, S.D.; Blazing, M.A.; Shui, A.; Rifai, N.; Califf, R.M.; Braunwald, E. Clinical relevance of C-reactive protein during follow-upof patients with acute coronary syndromes in the Aggrastat-to-Zocor Trial. Circulation 2006;114:281–288.
- Ridker, P.M.; Danielson, E.; Fonseca, F.A.; Genest, J.; Gotto, A.M.Jr; Kastelein, J.J.; Koenig, W.; Libby, P.; Lorenzatti, A.J.; MacFadyen, J.G.; Nordestgaard, B.G.; Shepherd, J.; Willerson, J.T.; Glynn, R.J. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med 2008;359:2195–2207.
- Ridker, P.M.; Danielson, E.; Fonseca, F.A.; Genest, J.; Gotto, A.M.Jr.; Kastelein, J.J.; Koenig, W.; Libby, P.; Lorenzatti, A.J.; Macfadyen, J.G.; et al. Reduction in C-reactive protein and LDL cholesterol and cardiovascular event rates after initiation of rosuvastatin: a prospective study of the JUPITER trial. Lancet 2009;373:1175–1182.
- Xie, S.; Galimberti, F.; Olmastroni, E.; Luscher, T.F.; Carugo, S.; Catapano, A.L.; Casula, M.; META-LIPID Group. Effect of lipid-lowering therapies on C-reactive protein levels: a comprehensive meta-analysis of randomized controlled trials. Cardiovasc Res. 2024, 120, 333–344. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ridker, P.M.; Lei, L.; Louie, M.J.; Haddad, T.; Nicholls, S.J.; Lincoff, A.M.; Libby, P.; Nissen, S.E.; CLEAR Outcomes Investigators. Inflammation and Cholesterol as Predictors of Cardiovascular Events Among 13 970 Contemporary High-Risk Patients With Statin Intolerance. Circulation. 2024, 149, 28–35. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Marques-Vidal, P.; Jankowski, P.; Reiner, Ž.; De Bacquer, D. Kotseva, K. EUROASPIRE EUROASPIRE V collaborators. Dietary management of patients at high risk for cardiovascular disease; EUROASPIRE V. Clin Nutr ESPEN 2023, 55, 144–150.
- Sofi, F.; Dinu, M.; Pagliai, G.; Cesari, F.; Gori, A.M.; Sereni, A.; Becatti, M.; Fiorillo, C.; Marcucci, R.; Casini, A. Low-Calorie Vegetarian Versus Mediterranean Diets for Reducing Body Weight and Improving Cardiovascular Risk Profile: CARDIVEG Study (Cardiovascular Prevention With Vegetarian Diet). Circulation. 2018, 137, 1103–1113. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Kroeger, C.M.; Cassidy, S.; Mitra, S.; Ribeiro, R.V.; Jose, S.; Masedunskas, A.; Senior, A.M.; Fontana, L. Vegetarian Dietary Patterns and Cardiometabolic Risk in People With or at High Risk of Cardiovascular Disease: A Systematic Review and Meta-analysis. JAMA Netw Open. 2023, 6, e2325658. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Filippou, C.D.; Tsioufis, C.P.; Thomopoulos, C.G.; Mihas, C.C.; Dimitriadis, K.S.; Sotiropoulou, L.I.; Chrysochoou, C.A.; Nihoyannopoulos, P.I.; Tousoulis, D.M. Dietary Approaches to Stop Hypertension (DASH) Diet and Blood Pressure Reduction in Adults with and without Hypertension: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Adv Nutr. 2020, 11, 1150–1160. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lari, A.; Sohouli, M.H.; Fatahi, S.; Cerqueira, H.S.; Santos, H.O.; Pourrajab, B.; Rezaei, M.; Saneie, S.; Rahideh, S.T. The effects of the Dietary Approaches to Stop Hypertension (DASH) diet on metabolic risk factors in patients with chronic disease: A systematic review and meta-analysis of randomized controlled trials. Nutr Metab Cardiovasc Dis. 2021, 31, 2766–2778. [Google Scholar] [CrossRef] [PubMed]
- Dinu, M.; Pagliai, G.; Casini, A.; Sofi, F. Mediterranean diet and multiple health outcomes: an umbrella review of metaanalyses of observational studies and randomized trials. Eur J Clin Nutr 2018, 72, 30–43. [Google Scholar] [CrossRef]
- Yannakoulia, M.; Scarmeas, N. Diets. N Engl J Med. 2024, 390, 2098–2106. [Google Scholar] [CrossRef] [PubMed]
- Schwingshackl, L.; Morze, J.; Hoffmann, G. Mediterranean diet and health status: active ingredients and pharmacological mechanisms. Br J Pharmacol 2020; 177: 1241-57.
- Ahmad, S.; Moorthy, M.V.; Lee, I.M.; Ridker, P.M.; Manson, J.E.; Buring, J.E.; Demler, O.V.; Mora, S. Mediterranean Diet Adherence and Risk of All-Cause Mortality in Women. JAMA Netw Open. 2024, 7, e2414322. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Delgado-Lista, J.; Alcala-Diaz, J.F.; Torres-Peña, J.D.; Quintana-Navarro, G.M.; Fuentes, F.; Garcia-Rios, A.; Ortiz-Morales, A.M.; Gonzalez-Requero, A.I.; Perez-Caballero, A.I.; Yubero-Serrano, E.M.; et al. CORDIOPREV Investigators. Long-term secondary prevention of cardiovascular disease with a Mediterranean diet and a low-fat diet (CORDIOPREV): a randomised controlled trial. Lancet. 2022, 399, 1876–1885. [Google Scholar] [CrossRef] [PubMed]
- Jimenez-Torres, J.; Alcalá-Diaz, J.F.; Torres-Peña, J.D.; Gutierrez-Mariscal, F.M.; Leon-Acuña, A.; Gómez-Luna, P.; Fernández-Gandara, C.; Quintana-Navarro, G.M.; Fernandez-Garcia, J.C.; Perez-Martinez, P.; et al. Mediterranean Diet Reduces Atherosclerosis Progression in Coronary Heart Disease: An Analysis of the CORDIOPREV Randomized Controlled Trial. Stroke. 2021, 52, 3440–3449. [Google Scholar] [CrossRef] [PubMed]
- Podadera-Herreros, A.; Arenas-de Larriva, A.P.; Gutierrez-Mariscal, F.M.; Alcala-Diaz, J.F.; Ojeda-Rodriguez, A.; Rodriguez-Cantalejo, F.; Cardelo, M.P.; Rodriguez-Cano, D.; Torres-Peña, J.D.; Luque, R.M.; et al. Mediterranean diet as a strategy for preserving kidney function in patients with coronary heart disease with type 2 diabetes and obesity: a secondary analysis of CORDIOPREV randomized controlled trial. Nutr Diabetes. 2024, 14, 27. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chlebowski, R.T.; Aragaki, A.K.; Anderson, G.L.; Simon, M.S.; Manson, J.E.; Neuhouser, M.L.; Pan, K.; Stefanic, M.L.; Rohan, T.E.; Lane, D.; et al. Association of Low-Fat Dietary Pattern With Breast Cancer Overall Survival: A Secondary Analysis of the Women's Health Initiative Randomized Clinical Trial. JAMA Oncol. 2018, 4, e181212. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Toledo, E.; Salas-Salvadó, J.; Donat-Vargas, C.; Buil-Cosiales, P.; Estruch, R.; Ros, E.; Corella, D.; Fitó, M.; Hu, F.B.; Arós, F.; et al. Mediterranean Diet and Invasive Breast Cancer Risk Among Women at High Cardiovascular Risk in the PREDIMED Trial: A Randomized Clinical Trial. JAMA Intern Med. 2015, 175, 1752–1760. [Google Scholar] [CrossRef] [PubMed]
- Ruggiero, E.; Di Castelnuovo, A.; Costanzo, S.; Esposito, S.; De Curtis, A.; Persichillo, M.; Cerletti, C.; Donati, M.B.; de Gaetano, G.; Iacoviello, L.; et al. Moli-sani Study Investigators. Olive oil consumption is associated with lower cancer, cardiovascular and all-cause mortality among Italian adults: prospective results from the Moli-sani Study and analysis of potential biological mechanisms. Eur J Clin Nutr. 2024, 78, 684–693. [Google Scholar] [CrossRef] [PubMed]
- Bondonno, N.P.; Parmenter, B.H.; Murray, K.; Bondonno, C.P.; Blekkenhorst, L.C.; Wood, A.C.; Post, W.S.; Allison, M.; Criqui, M.H.; Lewis, J.R.; et al. Associations Between Flavonoid Intake and Subclinical Atherosclerosis: The MESA. Arterioscler Thromb Vasc Biol. 2024, Epub ahead of print. [CrossRef] [PubMed]
- Monteiro, C.A.; Cannon, G.; Levy, R.B.; Moubarac, J.C.; Louzada, M.L.; Rauber, F.; Khandpur, N.; Cediel, G.; Neri, D.; Martinez-Steele, E.; et al. Ultra-processed foods: what they are and how to identify them. Public Health Nutr. 2019, 22, 936–941. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lane, M.M.; Gamage, E.; Du, S.; Ashtree, D.N.; McGuinness, A.J.; Gauci, S.; Baker, P.; Lawrence, M.; Rebholz, C.M.; Srour, B.; et al. Ultra-processed food exposure and adverse health outcomes: umbrella review of epidemiological meta-analyses. BMJ. 2024, 384, e077310. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Samuthpongtorn, C.; Nguyen, L.H.; Okereke, O.I.; Wang, D.D.; Song, M.; Chan, A.T.; Mehta, R.S. Consumption of Ultraprocessed Food and Risk of Depression. JAMA Netw Open. 2023, 6, e2334770. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Isaksen, I.M.; Dankel, S.N. Ultra-processed food consumption and cancer risk: A systematic review and meta-analysis. Clin Nutr. 2023, 42, 919–928. [Google Scholar] [CrossRef] [PubMed]
- Khoury, N.; Martínez, M.Á.; Garcidueñas-Fimbres, T.E.; Pastor-Villaescusa, B.; Leis, R.; de Las Heras-Delgado, S.; Miguel-Berges, M.L.; Navas-Carretero, S.; Portoles, O.; Pérez-Vega, K.A.; et al. Ultraprocessed Food Consumption and Cardiometabolic Risk Factors in Children. JAMA Netw Open. 2024, 7, e2411852. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rock, C.L.; Thomson, C.; Gansler, T.; Gapstur, S.M.; McCullough, M.L.; Patel, A.V.; Andrews, K.S.; Bandera, E.V.; Spees, C.K.; Robien, K.; et al. American Cancer Society guideline for diet and physical activity for cancer prevention. CA Cancer J Clin. 2020, 70, 245–271. [Google Scholar] [CrossRef] [PubMed]
- Hillman, E.T.; Lu, H.; Yao, T.; Nakatsu, C.H. . Microbial Ecology along the Gastrointestinal Tract. Microbes Environ. 2017, 32, 300–313. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Martins, D.; Silva, C.; Ferreira, A.C.; Dourado, S.; Albuquerque, A.; Saraiva, F.; Batista, A.B.; Castro, P.; Leite-Moreira, A.; Barros, A.S.; et al. Unravelling the Gut Microbiome Role in Cardiovascular Disease: A Systematic Review and a Meta-Analysis. Biomolecules. 2024, 14, 731. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tang, W.H.W.; Hazen, S.L. Unraveling the Complex Relationship Between Gut Microbiome and Cardiovascular Diseases. Circulation. 2024, 149, 1543–1545. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Shreiner, A.B.; Kao, J.Y.; Young, V.B. The gut microbiome in health and in disease. Curr. Opin. Gastroenterol. 2015, 31, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Hou, K.; Wu, Z.X.; Chen, X.Y.; Wang, J.Q.; Zhang, D.; Xiao, C.; Zhu, D.; Koya, J.B.; Wei, L.; Li, J.; et al. Microbiota in health and diseases. Signal Transduct Target Ther. 2022, 7, 135. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- de Wit, D.F.; Hanssen, N.M.; Wortelboer, K.; Herrema, H.; Rampanelli, E.; Nieuwdorp, M. (2023). Evidence for the contribution of the gut microbiome to obesity and its reversal. Science Translational Medicine, 2023, 15, eadg2773. [Google Scholar] [CrossRef] [PubMed]
- Byndloss, M.; Devkota, S.; Duca, F.; Niess, J.H.; Nieuwdorp, M.; Orho-Melander, M.; Sanz, Y.; Tremaroli, V.; Zhao, L. The gut microbiota and diabetes: research, translation, and clinical applications 2023 Diabetes, Diabetes Care, and Diabetologia Expert Forum. Diabetologia. 2024, Epub ahead of print. [CrossRef] [PubMed]
- Jie, Z.; Xia, H.; Zhong, S.L.; Feng, Q.; Li, S.; Liang, S.; Zhong, H.; Liu, Z.; Gao, Y.; Zhao, H.; et al. The gut microbiome in atherosclerotic cardiovascular disease. Nat Commun. 2017, 8, 845. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lee, K.A.; Luong, M.K.; Shaw, H.; Nathan, P.; Bataille, V.; Spector, T.D. The gut microbiome: what the oncologist ought to know. Br J Cancer. 2021, 125, 1197–1209. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zecheng, L.; Donghai, L.; Runchuan, G.; Yuan, Q.; Qi, J.; Yijia, Z.; Shuaman, R.; Xiaoqi, L.; Yi, W.; Ni, M.; et al. Fecal microbiota transplantation in obesity metabolism: A meta analysis and systematic review. Diabetes Res Clin Pract. 2023, 202, 110803. [Google Scholar] [CrossRef] [PubMed]
- Ng, S.C.; Xu, Z.; Mak, J.W.Y.; Yang, K.; Liu, Q.; Zuo, T.; Tang, W.; Lau, L.; Lui, R.N.; Wong, S.H.; et al. Microbiota engraftment after faecal microbiota transplantation in obese subjects with type 2 diabetes: a 24-week, double-blind, randomised controlled trial. Gut. 2022, 71, 716–723. [Google Scholar] [CrossRef] [PubMed]
- Tang, W.H.W.; Wang, Z.; Levison, B.S.; Koeth, R.A.; Britt, E.B.; Fu, X.; Wu, Y.; Hazen, S.L. Intestinal microbial metabolism of phosphatidylcholine and cardiovascular risk. N Engl J Med. 2013, 368, 1575–1584. [Google Scholar]
- Witkowski, M.; Weeks, T.L.; Hazen, S.L. ; Gut Microbiota and Cardiovascular Disease. Circ Res. 2020, 127, 553–570. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Liu, L.; Shah, K. The Potential of the Gut Microbiome to Reshape the Cancer Therapy Paradigm: A Review. JAMA Oncol. 2022, 8, 1059–1067. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.L.; Larkinson, M.L.Y.; Clarke, T.B. Immunological design of commensal communities to treat intestinal infection and inflammation. PLoS Pathog. 2021, 17, e1009191. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Coyte, K.Z.; Schluter, J.; Foster, K.R. The ecology of the microbiome: networks, competition, and stability. Science. 2015;350(6261):663-666. [CrossRef]
- Sun, J.; Chen, F.; & Wu, G. Potential effects of gut microbiota on host cancers: focus on immunity, DNA damage, cellular pathways, and anticancer therapy. The ISME Journal, 2023, 17, 1535-1551. [CrossRef] [PubMed]
- Molly (Menglin) Luo.
- Qin, Y.; Tong, X.; Mei, W.J.; Cheng, Y.; Zou, Y.; Han, K. , Yu J; Jie Z; Zhang T, Zhu S. Consistent signatures in the human gut microbiome of old-and young-onset colorectal cancer. Nature Communications, 2024, 15, 3396. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Dai, Z.; Coker, O.O.; Nakatsu, G.; Wu, W. K K.; Zhao, L.; Chen, Z.; Chan FKL, Kristiansen K, Sung JJY, Wong SH, et al.. Multi-cohort analysis of colorectal cancer metagenome identified altered bacteria across populations and universal bacterial markers. Microbiome. 2018, 6, 70. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fujii, T.; Kuzuya, T.; Kondo, N.; Funasaka, K.; Ohno, E.; Hirooka, Y.; Tochio, T. Altered intestinal Streptococcus anginosus and 5α-reductase gene levels in patients with hepatocellular carcinoma and elevated Bacteroides stercoris in atezolizumab/bevacizumab non-responders. J Med Microbiol. 2024, 73. [Google Scholar] [CrossRef] [PubMed]
- Peng, Z.; Cheng, S.; Kou, Y.; Wang, Z.; Jin, R.; Hu, H.; Zhang, X.; Gong, J.F.; Li, J.; Lu, M.; et al. The Gut Microbiome Is Associated with Clinical Response to Anti-PD-1/PD-L1 Immunotherapy in Gastrointestinal Cancer. Cancer Immunol Res. 2020, 8, 1251–1261. [Google Scholar] [CrossRef] [PubMed]
- Chau, J.; Yadav, M.; Liu, B.; Furqan, M.; Dai, Q.; Shahi, S.; Gupta, A.; Mercer, K.N.; Eastman, E.; Hejleh, T.A.; et al. Prospective correlation between the patient microbiome with response to and development of immune-mediated adverse effects to immunotherapy in lung cancer. BMC Cancer. 2021, 21, 808. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Whitman, I.R.; Agarwal, V.; Nah, G.; Dukes, J.W.; Vittinghoff, E.; Dewland, T.A.; Marcus, G.M. Alcohol Abuse and Cardiac Disease. J Am Coll Cardiol. 2017, 69, 13–24. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Biddinger, K.J.; Emdin, C.A.; Haas, M.E.; Wang, M.; Hindy, G.; Ellinor, P.T.; Kathiresan, S.; Khera, A.V.; Aragam, K.G. Association of Habitual Alcohol Intake With Risk of Cardiovascular Disease. JAMA Netw Open. 2022, 5, e223849. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhao, J.; Stockwell, T.; Naimi, T.; Churchill, S.; Clay, J.; Sherk, A. Association between daily alcohol intake and risk of all-cause mortality: a systematic review and meta-analyses. JAMA Network Open, 2023;6(3), e236185-e236185.
- Thelle, D.S.; Grønbæk, M. Alcohol - a scoping review for Nordic Nutrition Recommendations 2023. Food Nutr Res. 2024 Apr 1;68. [CrossRef] [PubMed]
- Krittanawong, C.; Isath, A.; Rosenson, R.S.; Khawaja, M.; Wang, Z.; Fogg, S.E.; Virani, S.S.; Qi, L.; Cao, Y.; Long, M.T.; et al. Alcohol Consumption and Cardiovascular Health. Am J Med. 2022, 135, 1213–1230e3. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Schutte, R.; Smith, L.; Wannamethee, G. Alcohol–The myth of cardiovascular protection. Clinical Nutrition, 2022, 41, 348–355. [Google Scholar] [CrossRef]
- Koelwyn, G.J.; Quail, D.F.; Zhang, X.; White, R.M.; Jones, L.W. Exercise dependent regulation of the tumour microenvironment. Nat Rev Cancer. 2017, 17, 620. [Google Scholar] [CrossRef] [PubMed]
- Kerr, J.; Anderson, C.; Lippman, S.M. Physical activity, sedentary behaviour, diet, and cancer: an update and emerging new evidence. Lancet Oncol. 2017, 18, e457–71. [Google Scholar] [CrossRef] [PubMed]
- Sanchis-Gomar F, Lavie CJ, Marín J, Perez-Quilis C, Eijsvogels TMH, O'Keefe JH, Perez MV, Blair SN. Exercise effects on cardiovascular disease: from basic aspects to clinical evidence. Cardiovasc Res. 2022, 118, 2253–2266. [Google Scholar] [CrossRef] [PubMed]
- Hawley, J.A.; Hargreaves, M.; Joyner, M.J.; and Zierath, J.R. Integrative biology of exercise. Cell 2014;159, 738–749.
- Rodgman, A.; Smith, C.J.; Perfetti, T.A. The composition of cigarette smoke: a retrospective, with emphasis on polycyclic components. Hum Exp Toxicol 2000;19:573-95.
- Hecht, S.S. Lung carcinogenesis by tobacco smoke. Int. J. Cancer 2012, 131, 2724–2732 . [Google Scholar] [CrossRef]
- U.S. Department of Health and Human Services. The Health Consequences of Smoking—50 Years of Progress: A Report of the Surgeon General. Atlanta, GA: U.S. Department of Health and Human Services, Centers for Disease Control and Prevention, National Center for Chronic Disease Prevention and Health Promotion, Office on Smoking and Health, 2014.
- Morris, P.B.; Ference, B.A.; Jahangir, E.; Feldman, D.N.; Ryan, J.J.; Bahrami, H.; El-Chami, M.F.; Bhakta, S.; Winchester, D.E.; Al-Mallah, M.H.; et al. Cardiovascular Effects of Exposure to Cigarette Smoke and Electronic Cigarettes: Clinical Perspectives From the Prevention of Cardiovascular Disease Section Leadership Council and Early Career Councils of the American College of Cardiology. J Am Coll Cardiol. 2015, 66, 1378–91. [Google Scholar] [CrossRef] [PubMed]
- Campagna, D.; Alamo, A.; Di Pino, A.; Russo, C.; Calogero, A.E.; Purrello, F.; Polosa, R. Smoking and diabetes: dangerous liaisons and confusing relationships. Diabetol Metab Syndr. 2019, 15, 117. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- U.S. Department of Health, Education, and Welfare. Smoking and Health: Report of the Advisory Committee to the Surgeon General of the Public Health Service. Washington: U.S. Department of Health, Education, and Welfare, Public Health Service, Center for Disease Control; 1964. PHS Publication No. 1103.
- Gandini, S.; Botteri, E.; Iodice, S.; Boniol, M.; Lowenfels, A.B.; Maisonneuve, P.; Boyle, P. Tobacco smoking and cancer: a meta-analysis. Int J Cancer. 2008;122:155–164. [CrossRef]
- Cumberbatch, M.G.; Rota, M.; Catto, J.W.; La Vecchia, C. The Role of Tobacco Smoke in Bladder and Kidney Carcinogenesis: A Comparison of Exposures and Meta-analysis of Incidence and Mortality Risks. Eur. Urol. 2016, 70, 458–466. [Google Scholar] [CrossRef]
- Alouini, S. Risk Factors Associated with Urothelial Bladder Cancer. Int J Environ Res Public Health. 2024, 21, 954. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Islami, F.; Moreira, D.M.; Boffetta, P.; Freedland, S.J. A systematic review and meta-analysis of tobacco use and prostate cancer mortality and incidence in prospective cohort studies. Eur Urol. 2014, 66, 1054–1064. [Google Scholar] [CrossRef]
- Dalstra, J.A.; Kunst, A.E.; Borrell, C.; Breeze, E.; Cambois, E.; Costa, G.; Geurts, J.J. ;, Lahelma E, Van Oyen H, Rasmussen NK, et al. . Socioeconomic differences in the prevalence of common chronic diseases: an overview of eight European countries. Int J Epidemiol. 2005, 34, 316–26. [Google Scholar] [CrossRef] [PubMed]
- Kivimäki, M.; Batty, G.D.; Pentti, J.; Shipley, M.J.; Sipilä, P.N.; Nyberg, S.T.; Suominen, S.B.; Oksanen, T.; Stenholm, S.; Virtanen, M.; et al. Association between socioeconomic status and the development of mental and physical health conditions in adulthood: a multi-cohort study. Lancet Public Health. 2020, 5, e140–e149. [Google Scholar] [CrossRef] [PubMed]
- Coleman-Jensen, A. ; Rabbit. M.P.; Gregory, C.A.; Singh, A.; Household Food Insecurity in the United States in 2019, ERR-275.U.S. Department of Agriculture Economic Research Service.
- Palakshappa, D.; Ip, E.H.; Berkowitz, S.A.; Bertoni, A.G.; Foley, K.L.; Miller, D.P. Jr; Vitolins, M.Z.; Rosenthal, G.E. Pathways by Which Food Insecurity Is Associated With Atherosclerotic Cardiovascular Disease Risk. J Am Heart Assoc. 2021, 10, e021901. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Tawakol, A.; Osborne, M.T.; Wang, Y.; Hammed, B.; Tung, B.; Patrich, T.; Oberfeld, B.; Ishai, A.; Shin, L.M.; Nahrendorf, M.; et al. Stress-Associated Neurobiological Pathway Linking Socioeconomic Disparities to Cardiovascular Disease. J Am Coll Cardiol. 2019, 73, 3243–3255. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Civieri G, Abohashem S, Grewal SS, Aldosoky W, Qamar I, Hanlon E, Choi KW, Shin LM, Rosovsky RP, Bollepalli SC, et al. Anxiety and Depression Associated With Increased Cardiovascular Disease Risk Through Accelerated Development of Risk Factors. JACC Adv. 2024, 3, 101208. [CrossRef] [PubMed] [PubMed Central]
- Rico-Uribe, L. A.; Caballero, F. F.; Martín-María, N.; Cabello, M.; Ayuso-Mateos, J.L.; Miret, M. Association of loneliness with all-cause mortality: A meta-analysis. PloS one, 2018, 13, e0190033. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lim, M. H.; Eres, R.; Vasan, S. Understanding loneliness in the twenty-first century: An update on correlates, risk factors, and potential solutions. Soc. Psychiatry. Psychiatr. Epidemiol 2020, 55, 793–810. [Google Scholar] [CrossRef] [PubMed]
- Vasan S, Lim MH, Eikelis N, Lambert E. Investigating the relationship between early cardiovascular disease markers and loneliness in young adults. Sci Rep. 2024, 14, 14221. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wang, Y.H.; Li, J.Q.; Shi, J.F.; Que, J.Y.; Liu, J.J.; Lappin, J.M.; Leung, J.; Ravindran, A.V.; Chen, W.Q.; Qiao, YL.; et al. Depression and anxiety in relation to cancer incidence and mortality: a systematic review and meta-analysis of cohort studies. Mol Psychiatry. 2020, 25, 1487–1499. [Google Scholar] [CrossRef] [PubMed]
- Carlson, L.E.; Zelinski, E.L.; Toivonen, K.I.; Sundstrom, L.; Jobin, C.T.; Damaskos, P.; Zebrack, B. Prevalence of psychosocial distress in cancer patients across 55 North American cancer centers. J Psychosoc Oncol. 2019, 37, 5–21. [Google Scholar] [CrossRef] [PubMed]
- Mehnert, A.; Hartung, T.J.; Friedrich, M.; Vehling, S.; Brähler, E.; Härter. M.; Keller, M.; Schulz, H.; Wegscheider, K.; Weis, J.; et al. One in two cancer patients is significantly distressed: Prevalence and indicators of distress. Psychooncology. 2018, 27, 75–82. [Google Scholar] [CrossRef] [PubMed]
- Hurria, A.; Somlo, G.; Ahles, T. Renaming "chemobrain". Cancer Invest. 2007, 25, 373–7. [Google Scholar] [CrossRef] [PubMed]
- Boehm, J.K.; Soo, J.; Chen, Y.; Zevon, E.S.; Hernandez, R.; Lloyd-Jones, D.; Kubzansky, L.D. Psychological well-being’s link with cardiovascular health in older adults. Am J Prev Med. 2017;53:791–798. [CrossRef]
- Ogunmoroti, O.; Osibogun, O.; Spatz, E.S.; Okunrintemi, V.; Mathews, L.; Ndumele, C.E.; Michos, E.D. A systematic review of the bidirectional relationship between depressive symptoms and cardiovascular health. Prev Med.2022;154:106891.
- Khan, S.A.; Shahzad, U.; Zarak, M. S.; Channa, J.; Khan, I.; & Ghani, M.O. A. Association of depression with subclinical coronary atherosclerosis: a systematic review. Journal of cardiovascular translational research, 2021;14: 685-705.
- Balboni, T.A.; VanderWeele, T.J.; Doan-Soares, S.D.; Long, K.N.G.; Ferrell, B.R.; Fitchett, G.; Koenig, H.G.; Bain, P.A.; Puchalski, C.; Steinhauser, K.E.; et al. Spirituality in Serious Illness and Health. JAMA. 2022, 328, 184–197. [Google Scholar] [CrossRef] [PubMed]
- Chinnaiyan, K.M.; Revankar, R.; Shapiro, M.D.; Kalra, A. Heart, mind, and soul: spirituality in cardiovascular medicine. Eur Heart J. 2021, 42, 2965–2968. [Google Scholar] [CrossRef] [PubMed]
- Seeman, T. E.; Dubin, L. F.; Seeman, M. Religiosity/spirituality and health: A critical review of the evidence for biological pathways. American psychologist, 2003;58(1), 53.
- Adler, N.E.; Page AEK (eds) Cancer Care for the Whole Patient: Meeting Psychosocial Health Needs. Washington DC: National Academies Press, 2008.
- Mira, R.; Newton, T.; Sabbah, W. Socioeconomic and ethnic inequalities in the progress of multimorbidity and the role of health behaviors. Journal of the American Medical Directors Association, 2023;24(6), 811-815.
- Luo, H.; Zhang, Q.; Yu, K.; Meng, X.; Kan, H.; Chen, R. Long-term exposure to ambient air pollution is a risk factor for trajectory of cardiometabolic multimorbidity: a prospective study in the UK Biobank. EBioMedicine, 2022;84:104282. [CrossRef] [PubMed]
- Münzel, T.; Sørensen, M.; Daiber, A. Transportation noise pollution and cardiovascular disease. Nat Rev Cardiol. 2021, 18, 619–636. [Google Scholar] [CrossRef] [PubMed]
- Cai, Y.; Zijlema, W.L.; Sørgjerd, E.P.; Doiron, D.; de Hoogh, K.; Hodgson, S.; Wolffenbuttel, B.; Gulliver, J.; Hansell, A.L.; Nieuwenhuijsen, M.; et al. Impact of road traffic noise on obesity measures: Observational study of three European cohorts. Environ Res. 2020 Dec;191:110013. [CrossRef] [PubMed]
- Letellier, N.; Yang, J.A.; Cavaillès, C.; Casey, J.A.; Carrasco-Escobar, G.; Zamora, S.; Jankowska, M.M.; Benmarhnia, T. Aircraft and road traffic noise, insulin resistance, and diabetes: The role of neighborhood socioeconomic status in San Diego County. Environ Pollut. 2023 Oct 15;335:122277. [CrossRef] [PubMed]
- Abbasi, M.; Yazdanirad, S.; Dehdarirad, H.; Hughes, D. Noise exposure and the risk of cancer: a comprehensive systematic review. Rev Environ Health. 2022, 38, 713–726. [Google Scholar] [CrossRef] [PubMed]
- Turner, M.C.; Andersen, Z.J.; Baccarelli, A.; Diver, W.R.; Gapstur, S.M.; Pope, C.A. 3rd; Prada, D.; Samet, J.; Thurston, G.; Cohen, A. 3rd; Prada, D.; Samet, J.; Thurston, G.; Cohen, A. Outdoor air pollution and cancer: An overview of the current evidence and public health recommendations. CA Cancer J Clin. 2020, 25, 103322/caac21632, Epub ahead of print. [Google Scholar] [PubMed] [PubMed Central]
- Kim, D.W.; Ock, J.; Moon, K.W.; Park, C.H. Association between heavy metal exposure and dyslipidemia among Korean Adults: from the Korean National Environmental Health Survey, 2015-2017. Int J Environ Res Public Health. 2022, 19, 3181. [Google Scholar] [CrossRef] [PubMed]
- Nissen, S.E.; Tuzcu EM, Schoenhagen P, Brown BG, Ganz P, Vogel RA, Crowe T, Howard G, Cooper CJ, Brodie B, et al. REVERSAL Investigators. Effect of intensive compared with moderate lipid-lowering therapy on progression of coronary atherosclerosis: a randomized controlled trial. JAMA 2004, 291, 1071–80. [Google Scholar] [CrossRef] [PubMed]
- Nissen, S.E.; Nicholls, S.J.; Sipahi, I.; Libby, P.; Raichlen, J.S.; Ballantyne, C.M.; Davignon, J.; Erbel, R.; Fruchart, J.C.; Tardif, J.C.; et al. ASTEROID Investigators. Effect of very high-intensity statin therapy on regression of coronary atherosclerosis: the ASTEROID trial. JAMA. 2006, 295, 1556–65. [Google Scholar] [CrossRef] [PubMed]
- Takayama, T.; Hiro, T.; Yamagishi, M.; Daida, H.; Hirayama, A.; Saito, S.; Yamaguchi, T.; Matsuzaki, M.; COSMOS Investigators. Effect of rosuvastatin on coronary atheroma in stable coronary artery disease: multicenter coronary atherosclerosis study measuring effects of rosuvastatin using intravascular ultrasound in Japanese subjects (COSMOS). Circ J. 2009, 73, 2110–7. [Google Scholar] [CrossRef] [PubMed]
- Hiro, T.; Kimura, T.; Morimoto, T.; Miyauchi, K.; Nakagawa, Y.; Yamagishi, M.; Ozaki, Y.; Kimura, K.; Saito, S.; Yamaguchi, T.; et al. JAPAN-ACS Investigators. Effect of intensive statin therapy on regression of coronary atherosclerosis in patients with acute coronary syndrome: a multicenter randomized trial evaluated by volumetric intravascular ultrasound using pitavastatin versus atorvastatin (JAPAN-ACS [Japan assessment of pitavastatin and atorvastatin in acute coronary syndrome] study). J Am Coll Cardiol. 2009, 54, 293–302. [Google Scholar] [CrossRef] [PubMed]
- Nicholls, S.J.; Ballantyne, C.M.; Barter, P.J.; Chapman, M.J.; Erbel, R.M.; Libby, P.; Raichlen, J.S.; Uno, K.; Borgma, M.; Wolski, K.; et al. Effect of two intensive statin regimens on progression of coronary disease. N Engl J Med. 2011, 365, 2078–87. [Google Scholar] [CrossRef] [PubMed]
- Guo, S.; Wang, R.; Yang, Z.; Li, K.; Wang, Q. Effects of atorvastatin on serum lipids, serum inflammation and plaque morphology in patients with stable atherosclerotic plaques. Exp Ther Med. 2012, 4, 1069–1074. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kini, AS, Baber, U. ; Kovacic, J.C.; Limaye,A.; Ali, Z.A.; Sweeny,J.; Maehara. A.; Mehran, R.; Dangas, G.; Mintz, G.S.; et al. Changes in plaque lipid content after short-term int.ensive versus standard statin therapy: the YELLOW trial (reduction in yellow plaque by aggressi.;e lipid-lowering therapy). J Am Coll Cardiol. 2013, 62, 21–9. [CrossRef] [PubMed]
- Räber, L.; Taniwaki, M.; Zaugg, S.; Kelbæk, H.; Roffi, M.; Holmvang, L.; Noble. S.; Pedrazzini, G.; Moschovitis.A.; Lüscher, T.F.; et al. IBIS 4 (Integrated Biomarkers and Imaging Study-4) Trial Investigators (NCT00962416). Effect of high-intensity statin therapy on atherosclerosis in non-infarct-related coronary arteries (IBIS-4): a serial intravascular ultrasonography study. Eur Heart J. 2015, 36, 490–500. [Google Scholar] [CrossRef] [PubMed]
- Räber, L.; Koskinas, K.C.; Yamaji, K.; Taniwaki, M.; Roffi, M; Holmvan,g. ; Garcia, Garcia. H.M.; Zanchin, T.; Maldonado, R.; Moschovitis, A, Pedrazzini, G.; et al. Changes in Coronary Plaque Composition in Patients With Acute Myocardial Infarction Treated With High-Intensity Statin Therapy (IBIS-4): A Serial Optical Coherence Tomography Study. JACC Cardiovasc Imaging. 2019, 12, 1518–1528. [Google Scholar] [CrossRef] [PubMed]
- Tsujita, K.; Sugiyama, S.; Sumida, H.; Shimomura, H.; Yamashita, T.; Yamanaga, K, Komura, N. ; Sakamoto, K,. Oka, H.; Nakao, K.; et al. PRECISE–IVUS Investigators. Impact of Dual Lipid-Lowering Strategy With Ezetimibe and Atorvastatin on Coronary Plaque Regression in Patients With Percutaneous Coronary Intervention: The Multicenter Randomized Controlled PRECISE-IVUS Trial. J Am Coll Cardiol. 2015, 66, 495–507. [Google Scholar] [CrossRef] [PubMed]
- Park, S.J.; Kang, S.J.; Ahn, J.M.; Chang, M.; Yun, S.C.; Roh, J.H.; Lee, P.H.; Park, H.W.; Yoon, S.H.; Park, D.W.; et al. Effect of Statin Treatment on Modifying Plaque Composition: A Double-Blind, Randomized Study. J Am Coll Cardiol. 2016, 67, 1772–1783. [Google Scholar] [CrossRef] [PubMed]
- Ahn, J.; Park, S.K.; Park, T.S.; Kim, J.H.; Yun, E.; Kim, S.P.; Lee, H.W.; Oh, J.H.; Choi, J.H.; Cha, K.S.; et al. Effect of n-3 Polyunsaturated Fatty Acids on Regression of Coronary Atherosclerosis in Statin Treated Patients Undergoing Percutaneous Coronary Intervention. Korean Circ J. 2016, 46, 481–9. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nicholls, S.J.; Puri, R.; Anderson, T.; Ballantyne, C.M.; Cho, L.; Kastelein, J.J.; Koenig, W.; Somaratne, R.; Kassahun, H.; Yang, J.; et al. Effect of Evolocumab on Progression of Coronary Disease in Statin-Treated Patients: The GLAGOV Randomized Clinical Trial. JAMA. 2016, 316, 2373–2384. [Google Scholar] [CrossRef] [PubMed]
- Alfaddagh, A.; Elajami, T.K.; Ashfaque, H.; Saleh, M.; Bistrian, B.R.; Welty, FK. Effect of Eicosapentaenoic and Docosahexaenoic Acids Added to Statin Therapy on Coronary Artery Plaque in Patients With Coronary Artery Disease: A Randomized Clinical Trial. J Am Heart Assoc. 2017, 6, e006981. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nishiguchi, T.; Kubo, T.; Tanimoto, T.; Ino, Y.; Matsuo, Y.; Yamano, T.; Terada, K.; Emori, H.; Katayama, Y.; Taruya, A.; et al. Effect of Early Pitavastatin Therapy on Coronary Fibrous-Cap Thickness Assessed by Optical Coherence Tomography in Patients With Acute Coronary Syndrome: The ESCORT Study. JACC Cardiovasc Imaging. 2018, 11, 829–838. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.E.; Chang, H.J.; Sung, J.M.; Park, H.B.; Heo, R.; Rizvi, A.; Lin, F.Y.; Kumar, A.; Hadamitzky, M.; Kim, Y.J.; et al. Effects of Statins on Coronary Atherosclerotic Plaques: The PARADIGM Study. JACC Cardiovasc Imaging. 2018, 11, 1475–1484. [Google Scholar] [CrossRef] [PubMed]
- Ako, J.; Hibi, K.; Tsujita, K.; Hiro, T.; Morino, Y.; Kozuma, K.; Shinke, T.; Otake, H.; Uno, K.; Louie, M.J.; et al. Effect of Alirocumab on Coronary Atheroma Volume in Japanese Patients With Acute Coronary Syndrome - The ODYSSEY J-IVUS Trial. Circ J. 2019, 83, 2025–2033. [Google Scholar] [CrossRef] [PubMed]
- Budoff, M.J.; Bhatt, D.L.; Kinninger, A.; Lakshmanan, S.; Muhlestein, J.B.; Le, V.T.; May, H.T.; Shaikh, K.; Shekar, C.; Roy, S.K.; et al. Effect of icosapent ethyl on progression of coronary atherosclerosis in patients with elevated triglycerides on statin therapy: final results of the EVAPORATE trial. Eur Heart J. 2020, 41, 3925–3932. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nicholls, S.J.; Kataoka, Y.; Nissen, S.E.; Prati, F.; Windecker, S.; Puri, R.; Hucko, T.; Aradi, D.; Herrman, J.R.; Hermanides, R.S.; et al. Effect of Evolocumab on Coronary Plaque Phenotype and Burden in Statin-Treated Patients Following Myocardial Infarction. JACC Cardiovasc Imaging. 2022, 15, 1308–1321. [Google Scholar] [CrossRef] [PubMed]
- Räber, L.; Ueki, Y.; Otsuka, T.; Losdat, S.; Häner, J.D.; Lonborg, J.; Fahrni, G.; Iglesias, J.F.; van Geuns, R.J.; Ondracek, A.S.; et al. PACMAN-AMI collaborators. Effect of Alirocumab Added to High-Intensity Statin Therapy on Coronary Atherosclerosis in Patients With Acute Myocardial Infarction: The PACMAN-AMI Randomized Clinical Trial. JAMA. 2022, 327, 1771–1781. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nakano, Y.; Yamamoto, M.; Matoba, T.; Katsuki, S.; Nakashiro, S.; Takase, S.; Akiyama, Y.; Nagata, T.; Mukai, Y.; Inoue, S.; et al. Association between Serum Oxysterols and Coronary Plaque Regression during Lipid-Lowering Therapy with Statin and Ezetimibe: Insights from the CuVIC Trial. J Atheroscler Thromb. 2023, 30, 907–918. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rivera, F.B.; Cha, S.W.; Varona, M.C.; Fernandez, Co. E.M.; Magalong, J.V.; Aparece, J.P.; De Oliveira-Gomes, D.; Kaur, G.; Gulati, M. Atherosclerotic coronary plaque regression from lipid-lowering therapies: A meta-analysis and meta-regression. Am J Prev Cardiol. 2024, 18, 100645. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Di Costanzo, A.; Indolfi, C.; Sorrentino, S.; Esposito, G.; Spaccarotella, C.A.M. The Effects of Statins, Ezetimibe, PCSK9-Inhibitors, Inclisiran, and Icosapent Ethyl on Platelet Function. Int. J. Mol. Sci. 2023, 24, 11739. [Google Scholar] [CrossRef] [PubMed]
- Hardie, D.G.; Hawley, S.A.; Scott, J.W. AMP-activated protein kinase–development of the energy sensor concept. J Physiol 2006;574(1):7–15.
- Triggle, C.R.; Mohammed, I.; Bshesh, K.; Marei, I.; Ye, K.; Ding, H.; MacDonald, R.; Hollenberg, M.D.; Hill, M.A. . Metformin: Is it a drug for all reasons and diseases? Metabolism. 2022, 133, 155223. [Google Scholar] [CrossRef] [PubMed]
- Owen, M.R.; Doran, E.; Halestrap, A.P. Evidence that metformin exerts its anti-diabetic eff8cts through inhibition of complex 1 of the mitochondrial respiratory chain. Biochem J 2000, 348, 607–14. [Google Scholar] [CrossRef] [PubMed]
- Madiraju, A.K.; Qiu, Y.; Perry, R.J.; Rahimi, Y.; Zhang, X.M.; Zhang, D.; Camporez, J.G.; Cline, G.W.; Butrico, G.M.; Kemp, B.E.; et al. Metformin inhibits gluconeogenesis via a redox-dependent mechanism in vivo. Nat Med. 2018, 24, 1384–1394. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- LaMoia, T.E.; Shulman, G.I. Cellular and molecular mechanisms of metformin action. Endocr Rev 2021, 42, 77–96. [Google Scholar] [CrossRef]
- Holm Nielsen, S.; Jonasson, L.; Kalogeropoulos, K.; Karsdal, M.A.; Reese-Petersen, A.L.; Auf dem Keller, U.; Genovese, F.; Nilsson, J.; Goncalves, I. Exploring the role of extracellular matrix proteins to develop biomarkers of plaque vulnerability and outcome. J. Intern. Med. 2020, 287, 493–513. [Google Scholar] [CrossRef]
- Chen, X.; Wang, S.; Xu, W.; Zhao, M.; Zhang, Y.; Xiao, H. Metformin Directly Binds to MMP-9 to Improve Plaque Stability. J Cardiovasc Dev Dis. 2023, 10, 54. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kataoka, Y.; Nicholls, S.J.; Andrews, J.; Uno, K.; Kapadia, S.R.; Tuzcu, E.M.; Nissen, S.E.; Puri, R. Plaque microstructures during metformin therapy in type 2 diabetic subjects with coronary artery disease: optical coherence tomography analysis. Cardiovasc Diagn Ther. 2022, 12, 77–87. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fu, J.; Xu, H.; Wu, F.; Tu, Q.; Dong, X.; Xie, H.; Cao, Z. Empagliflozin inhibits macrophage inflammation through AMPK signaling pathway and plays an anti-atherosclerosis role. Int J Cardiol. 2022, 367, 56–62. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.C.; Jandeleit-Dahm, K.; Peter, K. Sodium-Glucose Co-Transporter 2 (SGLT2) Inhibitor Dapagliflozin Stabilizes Diabetes-Induced Atherosclerotic Plaque Instability. J Am Heart Assoc. 2022, 11, e022761. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sardu, C.; Trotta, M.C.; Sasso, F.C.; Sacra, C.; Carpinella, G.; Mauro, C.; Minicucci, F.; Calabrò, P, D' Amico, M. ; D' Ascenzo, F.; et al. SGLT2-inhibitors effects on the coronary fibrous cap thickness and MACEs in diabetic patients with inducible myocardial ischemia and multi vessels non-obstructive coronary artery stenosis. Cardiovasc Diabetol. 2023, 22, 80. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kurozumi, A.; Shishido, K.; Yamashita, T.; Sato, D.; Uchida, S.; Koyama, E.; Tamaki, Y.; Hayashi, T.; Miyashita, H.; Yokoyama, H.; et al. Sodium-Glucose Cotransporter-2 Inhibitors Stabilize Coronary Plaques in Acute Coronary Syndrome With Diabetes Mellitus. Am J Cardiol. 2024, 214, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Katakami, N.; Mita, T.; Maeda, N.; Sato, Y.; Watada, H.; Shimomura, I. UTOPIA Study Investigators. Evaluation of the effect of tofogliflozin on the tissue characteristics of the carotid wall-a sub-analysis of the UTOPIA trial. Cardiovasc Diabetol. 2022, 21, 19. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Reiner, Z. Managing the residual cardiovascular disease risk associated with LDL-cholesterol and triglycerides in statin-treated patients: a clinical update. Nutr Metab Cardiovasc Dis 2013;23:799-807.
- Scandinavian Simvastatin Survival Study Group. Randomised trial of cholesterol lowering in 4444 patients with coronary heart disease: the Scandinavian Simvastatin Survival Study (4S). Lancet 1994; 344: 1383–89.
- Baigent, C.; Keech, A.; Kearney, P.M.; Blackwell, L.; Buck, G.; Pollicino, C.; Kirby, A.; Sourjina, T.; Peto, R.; Collins, R.; et al. Cholesterol Treatment Trialists' (CTT) Collaborators. Efficacy and safety of cholesterol-lowering treatment: prospective meta-analysis of data from 90,056 participants in 14 randomised trials of statins. Lancet. 2005, 366, 1267–78, Erratum in: Lancet. 2005 Oct 15-21;366(9494):1358. Erratum in: Lancet. 2008 Jun 21;371(9630):2084. [Google Scholar] [CrossRef] [PubMed]
- Cholesterol Treatment Trialists Collaboration, Baigent, C. ; Blackwell, L.; Emberson, J., Holland, L.E., Reith, C., Bhala, N., Peto, R., Barnes, E.H., Keech, A., Simes, J., Eds.; et al. Efficacy and safety of more intensive lowering of LDL cholesterol: a metaanalysis of data from 170, 000 participants in 26 randomised trials. Lancet 2010. [Google Scholar]
- Ford, I.; Murray, H.; McCowan, C.; Packard, C.J.; Long-term safety and efficacy of lowering low-density lipoprotein cholesterol with statin therapy: 20-year follow-up of West of Scotland Coronary Prevention Study. Circulation 2016;133:1073-1080.
- Cholesterol Treatment Trialists C. Efficacy and safety of statin therapy in older people: a meta-analysis of individual participant data from 28 randomised controlled trials. Lancet 2019;393:407-415.
- Jiang, W.; Hu, J.W.; He, X.R.; Jin, W.L.; He, X.Y. . Statins: a repurposed drug to fight cancer. J Exp Clin Cancer Res. 2021, 40, 241. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Buccioli, G.; Testa, C.; Jacchetti, E.; Pinoli, P.; Carelli, S.; Ceri, S.; Raimondi, M.T. The molecular basis of the anticancer effect of statins. Sci Rep. 2024, 14, 20298. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kansal, V.; Burnham, A.J.; Kinney, B.L.C.; Saba, N.F.; Paulos, C.; Lesinski, G.B.; Buchwald, Z.S.; Schmitt, N.C. . Statin drugs enhance responses to immune checkpoint blockade in head and neck cancer models. J Immunother Cancer. 2023, 11, e005940. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Vos, W.G.; Lutgens, E.; Seijkens, T.T.P. Statins and immune checkpoint inhibitors: a strategy to improve the efficacy of immunotherapy for cancer? Journal for ImmunoTherapy of Cancer 2022, 10, e005611. [Google Scholar] [CrossRef]
- Nam, G.H.; Kwon, M.; Jung, H.; Ko, E.; Kim, S.A.; Choi, Y.; Song, S.J.; Kim, S.; Lee, Y.; Kim, G.B.; et al. Statin-mediated inhibition of RAS prenylation activates ER stress to enhance the immunogenicity of KRAS mutant cancer. J Immunother Cancer. 2021, 9, e002474. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Pandor, A.; Ara, R.M.; Tumur, I.; Wilkinson, A.J. , Paisley, S.; Duenas, A.; Durrington, P.N.; Chilcott, J. Ezetimibe monotherapy for cholesterol lowering in 2,722 people:systematic review and meta-analysis of randomized controlled trials. J Intern Med 2009, 265, 568–580. [Google Scholar] [CrossRef] [PubMed]
- Morrone, D.; Weintraub, W.S.; Toth, P.P.; Hanson, M.E.; Lowe, R.S.; Lin, J.; Shah, A.K.; Tershakovec, A.M. Lipid-altering efficacy of ezetimibe plus statin and statin monotherapy and identification of factors associated with treatment response: a pooled analysis of over 21,000 subjects from 27 clinical trials. Atherosclerosis 2012, 223, 251–261. [Google Scholar] [CrossRef] [PubMed]
- Cannon, C.P.; Blazing, M.A.; Giugliano, R.P.; McCagg, A.; White, J.A.; Theroux, P.; Darius, H.; Lewis, B.S.; Ophuis, T.O.; Jukema, J.W.; et al.; IMPROVE-IT Investigators Ezetimibe added to statin therapy after acute coronary syndromes. N Engl J Med 2015, 372, 2387–2397. [Google Scholar] [CrossRef]
- Nissen, S.E.; Lincoff, A.M.; Brennan, D.; Ray, K.K.; Mason, D.; Kastelein, J.J.P.; Thompson, P.D.; Libby, P.; Cho, L.; Plutzky, J.; et al. CLEAR Outcomes Investigators. Bempedoic Acid and Cardiovascular Outcomes in Statin-Intolerant Patients. N Engl J Med. 2023, 388, 1353–1364. [Google Scholar] [CrossRef] [PubMed]
- Vrints, C.; Andreotti, F.; Koskinas, K.C.; Rossello, X.; Adamo, M.; Ainslie, J.; Banning, A.P.; Budaj, A.; Buechel, R.R.; Chiariello, G.A.; et al.; ESC Scientific Document Group 2024 ESC Guidelines for the management of chronic coronary syndromes. Eur Heart J. 2024, 45, 3415–3537. [Google Scholar] [CrossRef] [PubMed]
- Schwartz, G.G.; Steg, P.G.; Szarek, M.; Bhatt, D.L.; Bittner, V.A.; Diaz, R.; Edelberg, J.M.; Goodman, S.G.; Hanotin, C.; Harrington, R.A.; et al. ODYSSEY OUTCOMES Committees and Investigators. Alirocumab and Cardiovascular Outcomes after Acute Coronary Syndrome. N Engl J Med. 2018, 379, 2097–2107. [Google Scholar] [CrossRef] [PubMed]
- Sabatine, M.S.; Giugliano, R.P.; Keech, A.C.; Honarpour, N.; Wiviott, S.D.; Murphy, S.A.; Kuder, J.F.; Wang, H.; Liu, T.; Wasserman, S.M.; et al. Steering Committee and Investigators. Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease. N Engl J Med. 2017, 376, 1713–1722. [Google Scholar] [CrossRef] [PubMed]
- O'Donoghue, M.L.; Giugliano, R.P.; Wiviott, S.D.; Atar, D.; Keech, A.; Kuder, J.F.; Im, K.; Murphy, S.A.; Flores-Arredondo, J.H.; López, J.A.G.; et al. Long-Term Evolocumab in Patients With Established Atherosclerotic Cardiovascular Disease. Circulation. 2022, 146, 1109–1119. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, M.D. Prolonged and Pronounced Low-Density Lipoprotein Cholesterol Lowering: The Gift That Keeps Giving. Circulation. 2022, 146, 1120–1122. [Google Scholar] [CrossRef] [PubMed]
- Wright, R.S.; Ray, K.K.; Raal, F.J.; Kallend, D.G.; Jaros, M.; Koenig, W.; Leiter, L.A.; Landmesser, U.; Schwartz, G.G.; Friedman, A.; et al. ORION Phase III Investigators. Pooled Patient-Level Analysis of Inclisiran Trials in Patients With Familial Hypercholesterolemia or Atherosclerosis. J Am Coll Cardiol. 2021, 77, 1182–1193. [Google Scholar] [CrossRef] [PubMed]
- Ray, K.K.; Troquay, R.P.T.; Visseren, F.L.J.; Leiter, L.A.; Scott Wright, R.; Vikarunnessa, S.; Talloczy, Z.; Zang, X.; Maheux, P.; Lesogor, A.; et al. Long-term efficacy and safety of inclisiran in patients with high cardiovascular risk and elevated LDL cholesterol (ORION-3): results from the 4-year open-label extension of the ORION-1 trial. Lancet Diabetes Endocrinol. 2023, 11, 109–119. [Google Scholar] [CrossRef] [PubMed]
- Karagiannis, A.D.; Liu, M.; Toth, P.P.; Zhao, S.; Agrawal, D.K.; Libby, P.; Chatzizisis, Y.S. Pleiotropic Anti-atherosclerotic Effects of PCSK9 InhibitorsFrom Molecular Biology to Clinical Translation. Curr Atheroscler Rep. 2018, 20, 20. [Google Scholar] [CrossRef] [PubMed]
- Nowak, C.; Ärnlöv, J. A Mendelian randomization study of the effects of blood lipids on breast cancer risk. Nat Commun. 2018, 9, 3957. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wang, R.; Liu, H.; He, P.; An, D.; Guo, X.; Zhang, X.; Feng, M. Inhibition of PCSK9 enhances the antitumor effect of PD-1 inhibitor in colorectal cancer by promoting the infiltration of CD8+ T cells and the exclusion of Treg cells. Front Immunol. 2022, 13, 947756. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Kim, K.A.; Kim, N.J.; Choo, EH. The effect of fibrates on lowering low-density lipoprotein cholesterol and cardiovascular risk reduction: a systemic review and meta-analysis. Eur J Prev Cardiol. 2024, 31, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Ling, S.; Brown, K.; Miksza, J.K.; Howells, L.; Morrison, A.; Issa, E.; Yates, T.; Khunti, K.; Davies, M.J.; Zaccardi, F. Association of Type 2 Diabetes with Cancer: A Meta-analysis With Bias Analysis for Unmeasured Confounding in 151 Cohorts Comprising 32 Million People. Diabetes Care 2020, 43, 2313–2322. [Google Scholar] [CrossRef] [PubMed]
- Mesquita, L.A.; Spiazzi, B.F.; Piccoli, G.F.; Nogara, D.A.; da Natividade, G.R.; Garbin, H.I.; Wayerbacher, L.F.; Wiercinski, V.M.; Baggio, V.A.; Zingano, C.P.; et al. Does metformin reduce the risk of cancer in obesity and diabetes? A systematic review and meta-analysis. Diabetes Obes Metab. 2024, 26, 1929–1940. [Google Scholar] [CrossRef] [PubMed]
- O'Connor, L.; Bailey-Whyte, M.; Bhattacharya, M.; Butera, G.; Hardell, K.N.L. Seidenberg, A.B.; Castle, P.E.; Loomans-Kropp, H.A. Association of metformin use and cancer incidence: a systematic review and meta-analysis. J Natl Cancer Inst. 2024, 116, 518–529. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Galal, M.A.; Al-Rimawi, M.; Hajeer, A.; Dahman, H.; Alouch, S.; Aljada, A. ; Metformin: A Dual-Role Player in Cancer Treatment and Prevention. Int J Mol Sci. 2024, 25, 4083. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Fleshner, N.E.; Bernardino, RM.; Lajkosz, K.; Saad, F.; Izawa, J.; Drachenberg, D.; Saranchuk, J.W.; Tanguay, S.; Rendon, RA.; Leveridge, M.; et al. A randomized, double-blind, placebo-controlled trial of metformin in reducing progression among men on expectant management for low-risk prostate cancer: The MAST (Metformin Active Surveillance Trial) study. JCO 2024 42, LBA5002–LBA5002. [CrossRef]
- Gillessen, S.; Murphy, L.R.; James, N.D.; Sachdeva, A.; Attard, G.; Jones, R.J.; Adler, A.; El-Taji, O.; Varughese, M.; Gale, J.; et al. LBA70 - Adding metformin to androgen deprivation therapy (ADT) for patients (pts) with metastatic hormone sensitive prostate cancer (mHSPC): Overall survival (OS) results from the multi-arm, multi-stage randomized platform trial STAMPEDE. Annals of Oncology 2024, 35, 1–72 101016/annonc/annonc1623. [Google Scholar] [CrossRef]
- Goodwin, P.J.; Chen, B.E.; Gelmon, K.A.; Whelan, T.J.; Ennis, M.; Lemieux, J.; Ligibel, J.A.; Hershman, D.L.; Mayer, I.A.; Hobday, T.J.; et al. Effect of Metformin vs Placebo on Invasive Disease-Free Survival in Patients With Breast Cancer: The MA.32 Randomized Clinical Trial. JAMA. 2022, 327, 1963–1973. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Crist, M.; Yaniv, B.; Palackdharry, S.; Lehn, M.A.; Medvedovic, M.; Stone, T.; Gulati, S.; Karivedu, V.; Borchers, M.; Fuhrman, B.; et al. Metformin increases natural killer cell functions in head and neck squamous cell carcinoma through CXCL1 inhibition. J Immunother Cancer. 2022, 10, e005632. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wang, S.; Lin, Y.; Xiong, X.; Wang, L.; Guo Y, Chen Y, Chen S, Wang G, Lin P, Chen H, Yeung SJ, Bremer E, Zhang H. Low-Dose Metformin Reprograms the Tumor Immune Microenvironment in Human Esophageal Cancer: Results of a Phase II Clinical Trial. Clin Cancer Res. 2020, 26, 4921–4932. [Google Scholar] [CrossRef] [PubMed]
- Cha, J.H.; Yang, W.H.; Xia, W.; Wei, Y.; Chan, L.C.; Lim, S.O.; Li, C.W.; Kim, T.; Chang, S.S.; Lee, H.H.; et al. Metformin Promotes Antitumor Immunity via Endoplasmic-Reticulum-Associated Degradation of PD-L1. Mol Cell. 2018, 71, 606–620e7. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wen, M.; Cao, Y.; Wu, B.; Xiao, T.; Cao, R.; Wang, Q.; Liu, X.; Xue, H.; Yu, Y.; Lin, J.; et al. PD-L1 degradation is regulated by electrostatic membrane association of its cytoplasmic domain. Nat Commun. 2021, 12, 5106. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Panaampon, J.; Zhou, Y.; Saengboonmee, C. Metformin as a booster of cancer immunotherapy. Int Immunopharmacol. 2023 Aug;121:110528. [CrossRef] [PubMed]
- Shen, J.; Ye, X.; Hou, H.; Wang, Y. Clinical evidence for the prognostic impact of metformin in cancer patients treated with immune checkpoint inhibitors. Int Immunopharmacol. 2024, 134, 112243. [Google Scholar] [CrossRef] [PubMed]
- Baggio, L. L. & Drucker, D. J. Biology of incretins: GLP-1 and GIP. Gastroenterology 2007, 132, 2131–2157. [Google Scholar]
- Hammoud, R. Drucker, D. J. Beyond the pancreas: contrasting cardiometabolic actions of GIP and GLP1. Nat. Rev. Endocrinol.2023, 19, 201–216.
- Drucker, D. J. The cardiovascular biology of glucagon-like peptide-1. Cell Metab. 2016, 24, 15–30. [Google Scholar] [CrossRef]
- Marso, S.P.; Daniels, G.H.; Brown-Frandsen, K.; Kristensen, P.; Mann, J.F.; Nauck, M.A.; Nissen, S.E.; Pocock, S.; Poulter, N.R.; Ravn, L.S.; et al. LEADER Steering Committee; LEADER Trial Investigators. Liraglutide and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med. 2016, 375, 311–22. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Marso, S.P.; Bain, S.C.; Consoli, A.; Eliaschewitz, F.G.; Jódar, E.; Leiter, L.A.; Lingvay, I.; Rosenstock, J.; Seufert, J.; Warren, M.L.; et al. SUSTAIN-6 Investigators. Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med. 2016, 375, 1834–1844. [Google Scholar] [CrossRef] [PubMed]
- Husain, M.; Birkenfeld, A.; Donsmark, M.; Dungan, K.; Eliaschewitz, F.G.; Franco, D.; Jeppesen, O.K.; Lingvay, I.; Mosenzon, O.; Pedersen, S.D.; et al. PIONEER 6 Investigators. Oral Semaglutide and Cardiovascular Outcomes in Patients with Type 2 Diabetes. N Engl J Med. 2019, 381, 841–851. [Google Scholar] [CrossRef] [PubMed]
- Holman, R.R.; Bethel, M.A.; Mentz, R.J.; Thompson, V.P.; Lokhnygina, Y.; Buse, J.B.; Chan, J.C.; Choi, J.; Gustavson, S.M.; Iqbal, N.; et al. EXSCEL Study Group. Effects of Once-Weekly Exenatide on Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med. 2017, 377, 1228–1239. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hernandez, A.F.; Green, J.B.; Janmohamed, S.; D'Agostino, R.B. Sr; Granger, C.B.; Jones, N.P.; Leiter, L.A.; Rosenberg, A.E.; Sigmon, K.N.; Somerville, M.C.; et al. Harmony Outcomes committees and investigators. Albiglutide and cardiovascular outcomes in patients with type 2 diabetes and cardiovascular disease (Harmony Outcomes): a double-blind, randomised placebo-controlled trial. Lancet. 2018, 392, 1519–1529. [Google Scholar] [CrossRef] [PubMed]
- Gerstein, H.C.; Colhoun, H.M.; Dagenais, G.R.; Diaz, R.; Lakshmanan, M.; Pais, P.; Probstfield, J.; Riesmeyer, J.S.; Riddle, M.C.; Rydén, L.; et al. REWIND Investigators. Dulaglutide and cardiovascular outcomes in type 2 diabetes (REWIND): a double-blind, randomised placebo-controlled trial. Lancet. 2019, 394, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Piccini, S.; Favacchio, G.; Panico, C.; Morenghi, E.; Folli, F.; Mazziotti, G.; Lania, A.G.; Mirani, M. Time-dependent effect of GLP-1 receptor agonists on cardiovascular benefits: a real-world study. Cardiovasc Diabetol. 2023, 22, 69. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bray, J.J.H.; Foster-Davies, H.; Salem, A.; Hoole, A.L.; Obaid, D.R.; Halcox, J.P.J.; Stephens, J.W. Glucagon-like peptide-1 receptor agonists improve biomarkers of inflammation and oxidative stress: A systematic review and meta-analysis of randomised controlled trials. Diabetes Obes Metab. 2021, 23, 1806–1822. [Google Scholar] [CrossRef] [PubMed]
- Leiter, L.A.; Bain, S.C.; Bhatt, D.L.; Buse, J.B.; Mazer, C.D.; Pratley, R.E.; Rasmussen, S.; Ripa, M.S.; Vrazic, H.; Verma, S. The effect of glucagon-like peptide-1 receptor agonists liraglutide and semaglutide on cardiovascular and renal outcomes across baseline blood pressure categories: Analysis of the LEADER and SUSTAIN 6 trials. Diabetes Obes Metab. 2020, 22, 1690–1695. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Verma, S.; McGuire, D.K.; Bain, S.C.; Bhatt, D.L.; Leiter, L.A.; Mazer, C.D.; Monk Fries, T.; Pratley, R.E.; Rasmussen, S.; Vrazic, H; et al. Effects of glucagon-like peptide-1 receptor agonists liraglutide and semaglutide on cardiovascular and renal outcomes across body mass index categories in type 2 diabetes: Results of the LEADER and SUSTAIN 6 trials. Diabetes Obes Metab. 2020, 22, 2487–2492. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mellbin LG, Bhatt DL, David JP, Ekström K, Petrie MC, Rasmussen S, Vilsbøll T. Semaglutide and cardiovascular outcomes by baseline HbA1c in diabetes: the SUSTAIN 6 and PIONEER 6 trials. Eur Heart J. 2024, 45, 1371–1374. [CrossRef] [PubMed] [PubMed Central]
- Verma, S.; David, J.P.; Leiter, L.A.; Michelsen, M.M.; Rasmussen, S.; Bhatt, D.L. Semaglutide reduces the risk of major adverse cardiovascular events consistently across baseline triglyceride levels in patients with type 2 diabetes: Post hoc analyses of the SUSTAIN 6 and PIONEER 6 trials. Diabetes Obes Metab. 2023, 25, 2388–2392. [Google Scholar] [CrossRef] [PubMed]
- Marx, N.; Federici, M.; Schütt, K.; Müller-Wieland, D.; Ajjan, R.A.; Antunes, M.J.; Christodorescu, R.M.; Crawford, C.; Di Angelantonio, E.; Eliasson, B.; et al. ESC Scientific Document Group. 2023 ESC Guidelines for the management of cardiovascular disease in patients with diabetes. Eur Heart J. 2023, 44, 4043–4140. [Google Scholar] [CrossRef] [PubMed]
- Pi-Sunyer, X.; Astrup, A.; Fujioka, K.; Greenway, F.; Halpern, A.; Krempf, M.; Lau, D.C.; le Roux, C.W.; Violante Ortiz, R.; Jensen, C.B.; et al. SCALE Obesity and Prediabetes NN8022-1839 Study Group. A Randomized, Controlled Trial of 3.0 mg of Liraglutide in Weight Management. N Engl J Med. 2015, 373, 11–22. [Google Scholar] [CrossRef] [PubMed]
- Wilding, J.P.H.; Batterham, R.L.; Calanna, S.; Davies, M.; Van Gaal, L.F.; Lingvay, I.; McGowan, B.M.; Rosenstock, J.; Tran, M.T.D.; Wadden, T.A.; et al. STEP 1 Study Group. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021, 384, 989–1002. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.; Færch, L.; Jeppesen, O.K.; Pakseresht, A.; Pedersen, S.D.; Perreault, L.; Rosenstock, J.; Shimomura, I.; Viljoen, A.; Wadden, T.A.; et al. STEP 2 Study Group. Semaglutide 2·4 mg once a week in adults with overweight or obesity, and type 2 diabetes (STEP 2): a randomised, double-blind, double-dummy, placebo-controlled, phase 3 trial. Lancet. 2021, 397, 971–984. [Google Scholar] [CrossRef] [PubMed]
- Wadden, T.A.; Bailey, T.S.; Billings, L.K.; Davies, M.; Frias, J.P.; Koroleva, A.; Lingvay, I.; O'Neil, P.M.; Rubino, D.M.; Skovgaard, D.; et al. STEP 3 Investigators. Effect of Subcutaneous Semaglutide vs Placebo as an Adjunct to Intensive Behavioral Therapy on Body Weight in Adults With Overweight or Obesity: The STEP 3 Randomized Clinical Trial. JAMA. 2021, 325, 1403–1413. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Rubino, D.; Abrahamsson, N.; Davies, M.; Hesse, D.; Greenway, F.L.; Jensen, C.; Lingvay, I.; Mosenzon, O.; Rosenstock, J.; Rubio, M.A.; et al. STEP 4 Investigators. Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity: The STEP 4 Randomized Clinical Trial. JAMA. 2021, 325, 1414–1425. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lincoff, A.M.; Brown-Frandsen, K.; Colhoun, H.M.; Deanfield, J.; Emerson, S.S.; Esbjerg, S.; Hardt-Lindberg, S.; Hovingh, G.K.; Kahn, S.E.; Kushner, R.F.; et al. SELECT Trial Investigators. Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes. N Engl J Med. 2023, 389, 2221–2232. [Google Scholar] [CrossRef] [PubMed]
- Carbonell, C.; Mathew Stephen, M.; Ruan, Y.; Warkentin, M.T.; Brenner, D.R. Next Generation Weight Loss Drugs for the Prevention of Cancer? Cancer Control. 2024, 31, 10732748241241158. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wang, L.; Xu, R.; Kaelber, D.C.; Berger, N.A. Glucagon-Like Peptide 1 Receptor Agonists and 13 Obesity-Associated Cancers in Patients With Type 2 Diabetes. JAMA Netw Open. 2024, 7, e2421305. [CrossRef] [PubMed] [PubMed Central]
- Chen, D.; Liang, H.; Huangm, L.; Zhou, H.; Wang, Z. Liraglutide enhances the effect of checkpoint blockade through the inhibition of neutrophil extracellular traps in murine lung and liver cancers. FEBS Open Bio. 2024, 14, 1365–1377. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Korner, M.; Stockli, M.; Waser, B.; Reubi, J.C. GLP-1 receptor expression in human tumors and human normal tissues: Potential for in vivo targeting. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2007, 48, 736–743. [Google Scholar] [CrossRef]
- Hammoud, R.; Drucker, D.J. ; Beyond the pancreas: contrasting cardiometabolic actions of GIP and GLP1. Nat Rev Endocrinol. 2023, 19, 201–216. [Google Scholar] [CrossRef] [PubMed]
- Nordisk, N.; Ozempic (Semaglutide) Injection, for Subcutaneous Use. Available online: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/209637s009lbl.pdf (accessed on 19 April 2024).
- Bezin, J.; Gouverneur, A.; Pénichon, M.; Mathieu, C.; Garrel, R.; Hillaire-Buys, D.; Pariente, A.; Faillie, J.L. GLP-1 Receptor Agonists and the Risk of Thyroid Cancer. Diabetes Care. 2023, 46, 384–390. [Google Scholar] [CrossRef] [PubMed]
- Silverii, G.A.; Monami, M.; Gallo, M. , Ragni, A.; Prattichizzo, F.; Renzelli, V.; Ceriello, A.; Mannucci, E. Glucagon-like peptide-1 receptor agonists and risk of thyroid cancer: A systematic review and meta-analysis of randomized controlled trials. Diabetes Obes Metab. 2024, 26, 891–900. [Google Scholar] [CrossRef] [PubMed]
- Zinman, B. , Wanner, C.; Lachin, J.M.; Fitchett, D.; Bluhmki, E.; Hantel, S.; Mattheus, M.; Devins, T.; Johansen, O.E.; Woerle, H.J.; et al. EMPA-REG OUTCOME Investigators. Empagliflozin, Cardiovascular Outcomes, and Mortality in Type 2 Diabetes. N Engl J Med. 2015, 373, 2117–28. [Google Scholar] [CrossRef] [PubMed]
- Abdul-Ghani, M.; Stefano Del Prato, S.; Chilton, R.; DeFronzo, R.A. SGLT2 Inhibitors and Cardiovascular Risk: Lessons Learned From the EMPA-REG OUTCOME Study. Diabetes Care 2016, 39, 717–725. [Google Scholar] [CrossRef] [PubMed]
- Neal, B.; Perkovic, V.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Law, G.; Desai. M.; Matthews, D.R. CANVAS Program Collaborative Group. Canagliflozin and Cardiovascular and Renal Events in Type 2 Diabetes. N Engl J Med. 2017, 377, 644–657. [Google Scholar] [CrossRef] [PubMed]
- Mahaffey, K.W.; Neal, B.; Perkovic, V.; de Zeeuw, D.; Fulcher, G.; Erondu, N.; Shaw, W.; Fabbrini, E.; Sun, T.; Li, Q.; et al. Canagliflozin for Primary and Secondary Prevention of Cardiovascular Events Results from the CANVAS Program (Canagliflozin Cardiovascular Assessment Study). Circulation 2018, 137, 323–334. [Google Scholar] [CrossRef] [PubMed]
- Rådholm, K.; Figtree, G.; Perkovic, V.; Solomon, S.D.; Mahaffey, K.W.; de Zeeuw, D.; Fulcher, G.; Barrett, T.D.; Shaw,W. ; Desai,M.; et al. Canagliflozin and Heart Failure in Type 2 Diabetes Mellitus Results from the CANVAS Program. Circulation 2018, 138, 458–468. [Google Scholar] [CrossRef]
- Shah, S.R.; Najim, N.I.; Abbasi, Z.; Fatima, M.; Jangda, A.A.; Shahnawaz, W.; Shahid, M.; Shah, S.A. Canagliflozin and Cardiovascular disease—results of the CANVAS trial. J. Community Hosp. Intern. Med. Perspect. 2018, 8, 267–268. [Google Scholar]
- Wiviott, S.D.; Raz, I.; Bonaca, M.P.; Mosenzon, O.; Kato, E.T.; Cahn, A.; Silverman, M.G.; Zelniker, T.A.; Kuder, J.F.; Murphy, S.A.; et al. DECLARE–TIMI 58 Investigators. Dapagliflozin and Cardiovascular Outcomes in Type 2 Diabetes. N Engl J Med. 2019, 380, 347–357. [Google Scholar] [CrossRef] [PubMed]
- Furtado, R.H.M.; Bonaca, M.P.; Raz, I.; Zelniker, T.A. , Mosenzon, O.; Cahn, A.; Kuder, J.; Murphy, S.A.; Bhatt, D.L.; Leiter, L.A. et al. Dapagliflozin and Cardiovascular Outcomes in Patients With Type 2 Diabetes Mellitus and Previous Myocardial Infarction. Circulation. 2019, 139, 2516–2527. [Google Scholar] [CrossRef] [PubMed]
- Cannon, C.P.; Pratley, R.; Dagogo-Jack, S.; Mancuso, J.; Huyck, S.; Masiukiewicz, U.; Charbonnel, B.; Frederich, R.; Gallo, S.; Cosentino, F.; et al. VERTIS CV Investigators. Cardiovascular Outcomes with Ertugliflozin in Type 2 Diabetes. N Engl J Med. 2020, 383, 1425–1435. [Google Scholar] [CrossRef] [PubMed]
- Perkovic, V.; Jardine, M.J.; Neal, B.; Bompoint, S.; Heerspink, H.J.L.; Charytan, D.M.; Edwards, R.; Agarwal, R.; Bakris, G.; Bull, S.; et al. CREDENCE Trial Investigators. Canagliflozin and Renal Outcomes in Type 2 Diabetes and Nephropathy. N Engl J Med. 2019, 380, 2295–2306. [Google Scholar] [CrossRef] [PubMed]
- Das, S.R.; Everett, B.M.; Birtcher, K.K.; Brown, J.M.; Cefalu, W.T.; Januzzi JL, Kalyani, R.R.; Kosiborod, M.; Magwire, M.L.; Morris, P.B.; et al. 2018 ACC Expert Consensus Decision Pathway on Novel Therapies for Cardiovascular Risk Reduction in Patients With Type 2 Diabetes and Atherosclerotic Cardiovascular Disease: A Report of the American College of Cardiology Task Force on Expert Consensus Decision Pathways. J Am Coll Cardiol. 2018, 72, 3200-3223. [CrossRef] [PubMed]
- American Diabetes Association Professional Practice Committee. 10. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes-2022. Diabetes Care 2022;45(Suppl 1):S144–S174. [CrossRef]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. ESC Scientific Document Group. 2023 Focused Update of the 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur Heart J. 2023, 44, 3627–3639. [Google Scholar] [CrossRef] [PubMed]
- Dutka, M.; Bobiński, R.; Francuz, T.; Garczorz, W.; Zimmer, K.; Ilczak T, Ćwiertnia M, Hajduga MB. SGLT-2 Inhibitors in Cancer Treatment-Mechanisms of Action and Emerging New Perspectives. Cancers (Basel). 2022, 14, 5811. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Quagliariello, V.; De Laurentiis, M.; Rea, D.; Barbieri, A.; Monti, M.G.; Carbone, A.; Paccone, A.; Altucci, L.; Conte, M.; Canale,M. L.; et al. The SGLT-2 inhibitor empagliflozin improves myocardial strain, reduces cardiac fibrosis and pro-inflammatory cytokines in non-diabetic mice treated with doxorubicin. Cardiovasc. Diabetol. 2021, 20, 150. [Google Scholar] [CrossRef]
- Quagliariello, V.; Canale, M.L.; Bisceglia, I.; Iovine, M.; Paccone, A.; Maurea, C.; Scherillo, M.; Merola, A.; Giordano, V.; Palma, G.; et al. (2024) Sodium-glucose cotransporter 2 inhibitor dapagliflozin prevents ejection fraction reduction, reduces myocardial and renal NF-κB expression and systemic pro-inflammatory biomarkers in models of short-term doxorubicin cardiotoxicity. Front. Cardiovasc. Med. 2024;11:1289663. [CrossRef]
- Biondi, F.; Ghelardoni, S.; Moscato, S.; Mattii, L.; Barachini, S.; Novo, G.; Zucchi, R.; De Caterina, R.; Madonna, R. Empagliflozin restores autophagy and attenuates ponatinib-induced cardiomyocyte senescence and death. Vascular Pharmacology Volume 155, June 2024, 107300. [CrossRef]
- Gongora, C.A.; Drobni, Z.D.; Quinaglia Araujo Costa Silva, T.; Zafar, A.; Gong, J.; Zlotoff, D.A.; Gilman, H.K.; Hartmann, S.E.; Sama, S.; Nikolaidou, S.; et al. Sodium-Glucose Co-Transporter-2 Inhibitors and Cardiac Outcomes Among Patients Treated With Anthracyclines. JACC Heart Fail. 2022, 10, 559–567. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Avula, V.; Sharma, G.; Kosiborod, M.N.; Vaduganathan, M.; Neilan, T.G.; Lopez, T.; Dent, S.; Baldassarre, L.; Scherrer-Crosbie, M.; Barac, A.; et al. SGLT2 Inhibitor Use and Risk of Clinical Events in Patients With Cancer Therapy-Related Cardiac Dysfunction. JACC Heart Fail. 2024, 12, 67–78. [Google Scholar] [CrossRef] [PubMed]
- Dinarello, C.A. Interleukin-1 in the pathogenesis and treatment of inflammatory diseases. Blood. 2011, 117, 3720–32 [PubMed: 21304099. [Google Scholar] [CrossRef]
- Libby, P. Interleukin-1 Beta as a Target for Atherosclerosis Therapy: Biological Basis of CANTOS and Beyond. J Am Coll Cardiol. 2017, 70, 2278–2289. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Koenig, W.; Sund, M.; Fröhlich, M.; Fischer, H.G.; Löwel, H.; Döring, A.; Hutchinson, W.L.; Pepys, M.B. C-Reactive protein, a sensitive marker of inflammation, predicts future risk of coronary heart disease in initially healthy middle-aged men: results from the MONICA (Monitoring Trends and Determinants in Cardiovascular Disease) Augsburg Cohort Study, 1984 to 1992. Circulation. 1999, 99, 237–42. [Google Scholar] [CrossRef] [PubMed]
- Libby, P.; Ridker, P.M.; Hansson, G.K. Inflammation in atherosclerosis: from pathophysiology to practice. J Am Coll Cardiol 2009; 54: 2129-8.
- Braunwald, E. Creating controversy where none exists: the important role of C-reactive protein in the CARE, AFCAPS/TexCAPS, PROVE IT, REVERSAL, A to Z, JUPITER, HEART PROTECTION, and ASCOT trials. Eur Heart J. 2012, 33, 430–2. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Cannon, C.P.; Morrow, D.; Rifai, N.; Rose, L.M.; McCabe, C.H.; Pfeffer, M.A.; Braunwald, E. Pravastatin or Atorvastatin Evaluation and Infection Therapy-Thrombolysis in Myocardial Infarction 22 (PROVE IT-TIMI 22) Investigators. C-reactive protein levels and outcomes after statin therapy. N Engl J Med. 2005, 352, 20–8. [Google Scholar] [CrossRef] [PubMed]
- Nissen, S.E.; Tuzcu, E.M.; Schoenhagen, P.; Crowe, T.; Sasiela, W.J.; Tsai, J.; Orazem, J.; Magorien, R.D.; O’Shaughnessy, C.; Ganz, P. Statin therapy, LDL cholesterol, C reactive protein, and coronary artery disease. N Engl J Med 2005, 352, 29–38. [Google Scholar] [CrossRef] [PubMed]
- Morrow, D.A.; de Lemos, J.A.; Sabatine, M.S.; Wiviott, S.D.; Blazing, M.A.; Shui, A.; Rifai, N.; Califf, R.M.; Braunwald, E. Clinical relevance of C-reactive protein during follow-up of patients with acute coronary syndromes in the Aggrastat-to-Zocor Trial. Circulation 2006, 114, 281–288. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Danielson, E.; Fonseca, F.A.; Genest, J.; Gotto, A.M., Jr.; Kastelein, J.J.; Koenig, W.; Libby, P.; Lorenzatti, A.J.; MacFadyen, J.G; et al. Rosuvastatin to prevent vascular events in men and women with elevated C-reactive protein. N Engl J Med 2008, 359, 2195–2207. [Google Scholar] [CrossRef]
- Ridker, P.M.; Danielson, E.; Fonseca, F.A.; Genest, J.; Gotto, A.M.Jr.; Kastelein, J.J.; Koenig, W.; Libby, P.; Lorenzatti, A.J.; Macfadyen, J.G.; et al. Reduction in C-reactive protein and LDL cholesterol and cardiovascular event rates after initiation of rosuvastatin: a prospective study of the JUPITER trial. Lancet 2009, 373, 1175–1182. [Google Scholar] [CrossRef] [PubMed]
- Xie, S.; Galimberti, F.; Olmastroni, E.; Luscher, T.F.; Carugo, S.; Catapano, A.L.; Casula, M.; META-LIPID Group. Effect of lipid-lowering therapies on C-reactive protein levels: a comprehensive meta-analysis of randomized controlled trials. Cardiovasc Res. 2024, 120, 333–344. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ridker, P.M.; Lei, L.; Louie, M.J.; Haddad, T.; Nicholls, S.J.; Lincoff, A.M.; Libby, P.; Nissen, S.E.; CLEAR Outcomes Investigators. Inflammation and Cholesterol as Predictors of Cardiovascular Events Among 13 970 Contemporary High-Risk Patients With Statin Intolerance. Circulation. 2024, 149, 28–35. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ridker, P.M.; Everett, B.M.; Thuren, T.; MacFadyen, J.G. ; Chang,W. H.; Ballantyne, C.; Fonseca, F.; Nicolau, J.; Koenig,W.; Anker, S.D.; et al. Antiinflammatory Therapy with Canakinumab for Atherosclerotic Disease. N. Engl. J. Med. 2017, 377, 1119–1131. [Google Scholar] [PubMed]
- Nidorf, S.M.; Eikelboom, J.W.; Budgeon, C.A.; Thompson, P.L. Low-dose colchicine for secondary prevention of cardiovascular disease. J Am Coll Cardiol. 2013, 61, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Tardif, J.C.; Kouz, S.; Waters, D.D.; Bertrand, O.F.; Diaz, R.; Maggioni, A.P.; Pinto, F.J.; Ibrahim, R.; Gamra, H.; Kiwan, G.S.; et al. Efficacy and Safety of Low-Dose Colchicine after Myocardial Infarction. N Engl J Med. 2019, 381, 2497–2505. [Google Scholar] [CrossRef] [PubMed]
- Nidorf, S.M.; Fiolet, A.T.L.; Mosterd, A.; Eikelboom, J.W.; Schut, A.; Opstal, T.S.J.; The, S.H.K.; Xu, X.F.; Ireland, M.A.; Lenderink, T.; et al. LoDoCo2 Trial Investigators. Colchicine in Patients with Chronic Coronary Disease. N Engl J Med. 2020, 383, 1838–1847. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; MacFadyen, J.G.; Thuren,T. ; Everett, B.M.; Libby, P.; Glynn, R.J. CANTOS Trial Group. Effect of interleukin-1β inhibition with canakinumab on incident lung cancer in patients with atherosclerosis: exploratory results from a randomised, double-blind, placebo-controlled trial. Lancet 2017, 390, 1833–1 842. [Google Scholar] [CrossRef]
- Garon, E.B.; Lu, S.; Goto, Y.; De Marchi, P.; Paz-Ares, L.; Spigel, D.R.; Thomas, M.; Yang, J.C.; Ardizzoni, A.; Barlesi, F. Canakinumab as Adjuvant Therapy in Patients With Completely Resected Non-Small-Cell Lung Cancer: Results From the CANOPY-A Double-Blind, Randomized Clinical Trial. J Clin Oncol. 2024, 42, 180–191. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.; Goto, Y.; Wan-Teck Lim, D.; Halmos, B.; Chul Cho, B.; Cobo, M.; Luis González Larriba, J.; Zhou, C.; Demedts, I.; Atmaca, A.; et al. Canakinumab in combination with docetaxel compared with docetaxel alone for the treatment of advanced non-small cell lung cancer following platinum-based doublet chemotherapy and immunotherapy (CANOPY-2): A multicenter, randomized, double-blind, phase 3 trial. Lung Cancer. 2024, 189, 107451, Epub ahead of print. [Google Scholar] [PubMed]
- Tan, D.S.W.; Felip, E.; de Castro, G.; Solomon, B.J.; Greystoke, A.; Cho, B.C.; Cobo, M.; Kim, T.M.; Ganguly, S.; Carcereny, E.; et al. Canakinumab Versus Placebo in Combination With First-Line Pembrolizumab Plus Chemotherapy for Advanced Non-Small-Cell Lung Cancer: Results From the CANOPY-1 Trial. J Clin Oncol. 2024;42(2):192-204. [CrossRef] [PubMed]
- Bent, R. , Moll, L., Grabbe, S.; Bros, M. Interleukin-1 beta-A friend or foe in malignancies? Int. J. Mol. Sci. 2018, 19, 2155. [Google Scholar] [CrossRef] [PubMed]
- Elaraj, D. M. , Weinreich, D. M., Varghese, S., Puhlmann, M., Hewitt, S. M., Carroll, N. M.,... & Alexander, H. R. (2006). The role of interleukin 1 in growth and metastasis of human cancer xenografts. Clinical cancer research: an official journal of the American Association for Cancer Research 2006, 12, 1088–1096. [Google Scholar]
- Lau, L.; Porciuncula, A.; Yu, A.; Iwakura, Y.; David, G. Uncoupling the Senescence-Associated Secretory Phenotype from Cell Cycle Exit via Interleukin-1 Inactivation Unveils Its Protumorigenic Role. Mol Cell Biol. 2019, 39, e00586–18. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lin, D.; Lei, L.; Liu,Y. ; Zhang, Y.; Hu, B.; Bao, G.; Song, Y.; Jin, Z.; Liu, C.; Mei, Y.; et al. Membrane IL1α Inhibits the Development of Hepatocellular Carcinoma via Promoting T- and NK-cell Activation. Cancer Res. 2016, 76, 3179–88. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Gebhardt, C.; Umansky, L.; Beckhove, P.; Schulze, T.J.; Utikal, J.; Umansky, V. Elevated chronic inflammatory factors and myeloid-derived suppressor cells indicate poor prognosis in advanced melanoma patients. Int J Cancer. 2015, 136, 2352–60. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Devalaraja, M.; Baeres, F.M.M.; Engelmann, M.D.M.; Hovingh, G.K.; Ivkovic, M.; Lo, L.; Kling, D.; Pergola, P.; Raj, D.; et al.; RESCUE Investigators IL-6 inhibition with ziltivekimab in patients at high atherosclerotic risk (RESCUE): a double-blind, randomised, placebo-controlled, phase 2 trial. Lancet. 2021, 397, 2060–2069. [Google Scholar] [CrossRef] [PubMed]
- Rašková, M.; Lacina, L.; Kejík, Z.; Venhauerová, A.; Skaličková, M.; Kolář, M.; Jakubek, M.; Rosel, D.; Smetana, K. Jr.; Brábek, J. The Role of IL-6 in Cancer Cell Invasiveness and Metastasis-Overview and Therapeutic Opportunities. Cells. 2022, 11, 3698. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, W.; Wu, Z.; Meng, W.; Zhang, C.; Cheng, M.; Chen, Y.; Zou, Y.; Li, K.; Lin, S.; Xiong, W.; et al. Blockade of IL-6 inhibits tumor immune evasion and improves anti-PD-1 immunotherapy. Cytokine. 2022, 158, 155976. [Google Scholar] [CrossRef] [PubMed]
- Toyoshima, Y.; Kitamura, H.; Xiang, H.; Ohno, Y.; Homma, S.; Kawamura, H.; Takahashi, N.; Kamiyama, T.; Tanino, M.; Taketomi, A. IL6 Modulates the Immune Status of the Tumor Microenvironment to Facilitate Metastatic Colonization of Colorectal Cancer Cells. Cancer Immunol Res. 2019, 7, 1944–1957. [Google Scholar] [CrossRef] [PubMed]
- Yang, Q.; Yu, B.; Kang, J.; Li, A.; Sun, J. Obesity Promotes Tumor Immune Evasion in Ovarian Cancer Through Increased Production of Myeloid-Derived Suppressor Cells via IL-6. Cancer Manag Res. 2021, 13, 7355–7363. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Soler, M.F.; Abaurrea, A.; Azcoaga, P.; Araujo, A.M.; Caffarel, M.M. New perspectives in cancer immunotherapy: targeting IL-6 cytokine family. J Immunother Cancer. 2023, 11, e007530. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hailemichael, Y.; Johnson, D.H.; Abdel-Wahab, N.; Foo, W.C.; Bentebibel, S.E.; Daher, M.; Haymaker, C.; Wani, K.; Saberian, C.; Ogata, D.; et al. Interleukin-6 blockade abrogates immunotherapy toxicity and promotes tumor immunity. Cancer Cell. 2022, 40, 509–523e6. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Okazaki, S.; Sakaguchi, M.; Miwa, K.; Furukado, S.; Yamagami, H.; Yagita, Y.; Mochizuki, H.; Kitagawa, K. Association of interleukin-6 with the progression of carotid atherosclerosis: a 9-year follow-up study. Stroke, 2014, 45, 2924–2929. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M. From RESCUE to ZEUS: will interleukin-6 inhibition with ziltivekimab prove effective for cardiovascular event reduction? Cardiovasc Res. 2021, 117, e138–e140. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Martínez, G.J.; Celermajer, D.S.; Patel, S. The NLRP3 inflammasome and the emerging role of colchicine to inhibit atherosclerosis-associated inflammation. Atherosclerosis. 2018, 269, 262–271. [Google Scholar] [CrossRef] [PubMed]
- Leung, Y.Y.; Hui, L.L.Y.; Kraus, V.B. Colchicine — update on mechanisms of action and therapeutic uses. Semin Arthritis Rheum 2015, 45, 341–50. [Google Scholar] [CrossRef] [PubMed]
- Schwarz, N.; Fernando, S.; Chen, Y.C.; Salagaras, T.; Rao, S.R.; Liyanage, S.; Williamson, A.E.; Toledo-Flores, D.; Dimasi, C.; Sargeant, T.J.; et al. Colchicine exerts anti-atherosclerotic and -plaque-stabilizing effects targeting foam cell formation. FASEB J. 2023, 37, e22846. [Google Scholar] [CrossRef] [PubMed]
- Nidorf, S.M.; Ben-Chetrit, E.; Ridker, P.M. Low-dose colchicine for atherosclerosis: long-term safety. Eur Heart J. 2024, 45, 1596–1601. [Google Scholar] [CrossRef] [PubMed]
- Nelson, K.; Fuster, V.; Ridker, P.M. Low-Dose Colchicine for Secondary Prevention of Coronary Artery Disease: JACC Review Topic of the Week. J Am Coll Cardiol. 2023, 82, 648–660. [Google Scholar] [CrossRef] [PubMed]
- Brenner, R.; Ben-Zvi, I.; Shinar, Y.; Liphshitz, I.; Silverman, B.; Peled, N.; Levy, C.; Ben-Chetrit, E.; Livneh, A.; Kivity, S. Familial Mediterranean Fever and Incidence of Cancer: An Analysis of 8,534 Israeli Patients With 258,803 Person-Years. Arthritis Rheumatol. 2018, 70, 127–133. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.J.; Yen, J.H.; Chang, S.J. Gout patients have an increased risk of developing most cancers, especially urological cancers. Scand J Rheumatol. 2014, 43, 385–90. [Google Scholar] [CrossRef] [PubMed]
- Kuo, M.C.; Chang, S.J.; Hsieh, M.C. Colchicine Significantly Reduces Incident Cancer in Gout Male Patients: A 12-Year Cohort Study. Medicine (Baltimore). 2015, 94, e1570. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Peng, Y.; Li, Z.; Zhang, J.; Dong, Y.; Zhang, C.; Dong, Y.; Zhai, Y.; Zheng, H.; Liu, M.; Zhao, J.; et al. Low-Dose Colchicine Ameliorates Doxorubicin Cardiotoxicity Via Promoting Autolysosome Degradation. J Am Heart Assoc. 2024, 3, e033700. [Google Scholar] [CrossRef] [PubMed]
- Zuriaga, M.A.; Yu, Z.; Matesanz, N.; Truong, B.; Ramos-Neble, B.L.; Asensio-López, M.C.; Uddin, M.M.; Nakao T, Niroula A, Zorita V, Amorós-Pérez M, et al. Colchicine prevents accelerated atherosclerosis in TET2-mutant clonal haematopoiesis. Eur Heart J. 2024, ehae546. Epub ahead of print. [CrossRef] [PubMed]
- Maffia, P.; Mauro, C.; Case, A.; Kemper, C. Canonical and non-canonical roles of complement in atherosclerosis. Nat Rev Cardiol. 2024, 21, 743–761. [Google Scholar] [CrossRef] [PubMed]
- Monaco, C.; Dib, L. Atheroimmunology: keeping the immune system in atherosclerosis in check. Nat Rev Cardiol. 2024, 21, 737–738. [Google Scholar] [CrossRef] [PubMed]
- Singer, M. A dose of drugs, a touch of violence, a case of AIDS: conceptualizing the SAVA syndemic. Free Inquiry in Creative Sociology, 1996, 24, 99–110. [Google Scholar]
- Reason J: Human error: models and management. BMJ 2000, 320, 768–70. [CrossRef] [PubMed]
- Krychtiuk, K.A.; Ahrens, I.; Drexel, H.; Halvorsen, S.; Hassager, C.; Huber, K.; Kurpas, D.; Niessner, A.; Schiele, F.; Semb, A.G.; et al. Acute LDL-C reduction post ACS: strike early and strike strong: from evidence to clinical practice. A clinical consensus statement of the Association for Acute CardioVascular Care (ACVC), in collaboration with the European Association of Preventive Cardiology (EAPC) and the European Society of Cardiology Working Group on Cardiovascular Pharmacotherapy. Eur Heart J Acute Cardiovasc Care. 2022, 11, 939-949. [CrossRef] [PubMed]
- Zinzuwadia, A.N.; Mineeva, O.; Li, C.; Farukhi, Z.; Giulianini, F.; Cade, B.; Chen, L.; Karlson, E.; Paynter, N.; Mora, S.; et al. Tailoring Risk Prediction Models to Local Populations. JAMA Cardiol. 2024, 18, e242912. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Davis, M.M.; Shanley, T.P. The Missing -Omes: Proposing Social and Environmental Nomenclature in Precision Medicine. Clin Transl Sci. 2017, 10, 64–66. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Moslehi, J.J. Cardio-Oncology: A New Clinical Frontier and Novel Platform for Cardiovascular Investigation. Circulation. 2024, 150, 513–515. [Google Scholar] [CrossRef] [PubMed]
- Levine, G.N.; Cohen, B.E.; Commodore-Mensah, Y.; Fleury, J.; Huffman, J.C.; Khalid, U.; Labarthe, D.R.; Lavretsky, H.; Michos, E.D.; Spatz, E.S.; et al. Psychological Health, Well-Being, and the Mind-Heart-Body Connection: A Scientific Statement From the American Heart Association. Circulation. 2021, 143, e763–e783. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The figure illustrates the cardio-oncology patient as a target of many syndemics: in the inner circle the clustering of cardiovascular risk factors and the effects of the oncologic treatments, in the first outer circle the psychological determinant of health, and in the external circle the social determinants of health including environmental exposomes. The arrows illustrate how the various health conditions cluster and interact and how harmful alignments can lead to dangerous conditions mimicking the “Swiss Cheese” effect (Ref. [406]).
Figure 1.
The figure illustrates the cardio-oncology patient as a target of many syndemics: in the inner circle the clustering of cardiovascular risk factors and the effects of the oncologic treatments, in the first outer circle the psychological determinant of health, and in the external circle the social determinants of health including environmental exposomes. The arrows illustrate how the various health conditions cluster and interact and how harmful alignments can lead to dangerous conditions mimicking the “Swiss Cheese” effect (Ref. [406]).
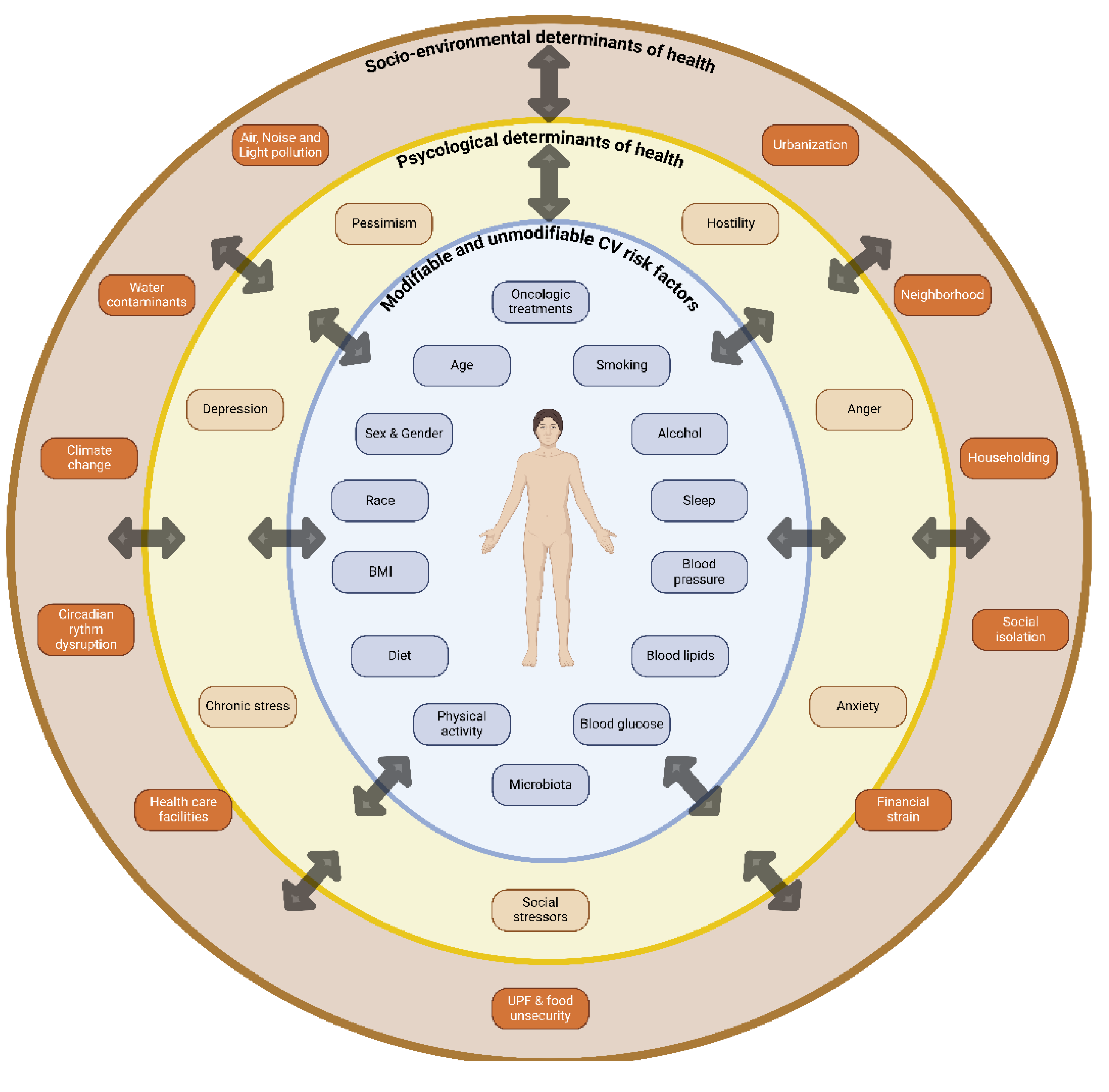

Table 1.
The impact of Lipid Lowering therapies on the atherosclerotic plaque: some studies.
| Study/year/Reference | Type of study | Lipid –lowering therapy | Population | Imaging modality | Endpoints | Results |
|---|---|---|---|---|---|---|
| REVERSAL Nissen SE et al./2004/Ref. [235] | double-blind, randomized active control multicenter | Pravastatin 40 mg versus Atorvastatin 80 mg (for 18 months) | 600 US patients | IVUS | Δ PAV | The progression of the atheroma volume was significantly slowed by Atorvastatin 80 mg |
| ASTEROID Nissen SE et al. /2006/Ref. [236] | Prospective, open-label blinded end-points | Rosuvastatin 40 mg/day | 349/507 pts had evaluable serial IVUS examinations. |
IVUS | Δ PAV, Δ atheroma volume, Δ TAV |
significant reduction of mean change in PAV for the entire vessel, mean change in atheroma volume in the most diseased 10-mm subsegment and change in TAV |
| COSMOS Takayama T et al./2009/Ref. [237] | open-label | Rosuvastatin (2.5-20 mg/day) | 126 pts 92 (72.2%) received the maximum dosage (20 mg/day) |
IVUS | Δ TAV | Rosuvastatin induced significant regression of TAV |
| JAPAN-ACS Hiro T et al. /2009 Ref. [238] | prospective, randomized, open-label, parallel group study with blind end point evaluation | Pitavastin 4 mg/day vs Atorvastatin 20 mg/day |
Among 307 patients with ACS undergoing IVUS-guided PCI, 252 patients had evaluable IVUS examinations at baseline and 8 to 12 months’ follow-up | IVUS | Δ PV in NTL | Pitavastatin and atorvastatin induced an equivalent significant regression of coronary PV |
| SATURN Nicholls SJ/2011/ Ref. [239] | prospective, randomized, multicenter, double-blind clinical |
Atorvastatin 80 mg vs Rosuvastatin 40 mg (for 104 weeks) |
1039 CAD pts | IVUS | Δ PAV Δ TAV |
The regression of PAV was similar in the two groups. A greater reduction in TAV occurred with rosuvastatin |
| Guo et al./2012 Ref. [240] | randomized, controlled |
Placebo (54 pts) vs atorvastatin 10 mg (47 pts) vs atorvastatin 20 mg (45 pts) vs atorvastatin 50 mg (43 pts) vs atorvastatin 80 mg (39 pts) |
228 stable CAD pts with CAG and IVUS | IVUS | Δ PAV Δ Plaque necrosis |
The percentages of plaque necrosis increased in the placebo and atorvastatin 10 mg groups; remained stable in the atorvastatin 20, 40 and 80 mg groups. Plaque volumes did not change in the placebo, atorvastatin 10 and 20 mg groups; decreased in atorvastatin 40 and 80 mg groups, |
| YELLOW Kini AS et al./2013/Ref. [241] | prospective, randomized, single center, single-blinded |
Rosuvastatin 40 mg daily vs standard-of-care lipid-lowering therapy | 87 patients with at least 2-vessel obstructive CAD (angiographic diameter stenosis >70%). TLs were treated with PCI, NTLs with>70% diameter stenosis and FFR ≤0.8 were evaluated for plaque composition |
IVUS NIRS |
change in lipid-core burden index at the 4-mm maximal segment (LCBI4mm max), |
median reduction in LCBI4mm max was significantly greater in the intensive vs standard group |
|
IBIS-4 Raber L et al/2015/ Ref. [242] IBIS-4 Raber L et al./2019/Ref. [243] |
prospective cohort study nested in the COMFORTABLE-AMI trial |
Rosuvastatin 40 mg daily |
82 patients with 146 non-infarct-related arteries (non-IRA) |
IVUS RF-IVUS OCT |
Δ PAV in the proximal segment of non-IRA after 13 months of therapy (IVUS) and reduction of necrotic core (RF-IVUS); changes in coronary plaque composition |
Rosuvastatin induced an atherosclerosis regression (measured by a change in PAV) in the non-IRA, but did not change RF-IVUS defined proportion of necrotic core; significant increase in minimum fibrous cap thickness and reduction in macrophage accumulation |
| PRECISE IVUS Tsujita K et al./2015 Ref. [244] | prospective, randomized, controlled, multicenter | Atorvastatin+ezetimibe vs Atorvastatin |
246 CAD patients scheduled for PCI were enrolled; 202 patients available for IVUS after 9-12 months of treatment (100 in the atorvastatin-ezetimibe group and 102 in the atorvastatin group | IVUS | Δ PAV Δ TAV |
The atorvastatin/ezetimibe group was noninferior to the atorvastatin group for the absolute change in percent atheroma volume (Δ PAV) |
| STABLE Park S et al./2016/Ref. [245] | prospective, single-center, double-blind, randomized | Rosuvastatin 40 mg vs Rosuvastatin 10 mg | 225 patients with an IVUS-defined fibroatheroma-containing index lesion. | IVUS | Δ PAV | Rosuvastatin reduced necrotic core and plaque volume and decreased thin-cap fibroatheroma rate with no significant differences between the two dosages |
| Ahn J et al./2016/ Ref. [246] | prospective randomized placebo-controlled | ώ-3 PUFA vs placebo, All patients were taking statins |
74 patients scheduled for PCI | IVUS | Δ PAV in a target lesion located more than 10 mm away from the stent | No differences |
| GLAGOV Nicholls SJ et al./2016/Ref. [247] | Multicenter, double-blind, placebo-controlled | Patients with angiographic CAD treated with statins | Subcutaneous Evolocumab 420 mg monthly for 76 weeks (484 patients) vs placebo (484 patients) in addition to statins | IVUS | Δ PAV(from baseline to week 76) Δ TAV Plaque regression |
Evolocumab added to statin induced a significant reduction of PAV and TAV and plaque regression in a greater percentage of patients compared to placebo |
| Alfaddagh et al. /2017/Ref. [248] | Randomized controlled | ώ-3 PUFA (1.86 g of EPA and 1.5 g of DHA daily) vs placebo for 30 months | 285 subjects with stable CAD and on statin therapy | CCTA at baseline and after 30 months | Δ indexed volume of non-calcified coronary plaque | High-dose EPA and DHA+statin provided more benefit in preventing progression of fibrous coronary plaque compared to statins only. Omega-3 ethyl-ester supplementation prevented progression of fibrous plaque in those on LIS therapy, but not in those on HIS therapy |
| ESCORT/2018/Ref. [249] | prospective, randomized, active-controlled, single-center | Pitavastatin 4 mg/day from baseline (early statin group) vs pitavastatin 4 mg/day from 3 weeks after the baseline (late statin group) |
53 patients with 1) successful PCI for ACS; 2) de novo, intermediate, NCL suitable for OCT examination; 3) scheduled coronary catheterization at 3 and 36 weeks after the index procedure and 4) untreated dyslipidemia (LDL-C level >100 mg/dl). |
OCT in 53 patients (performed at baseline, 3-week and 36-week follow up) |
Δ FCT | Early therapy with pitavastatin 4 mg/day for patients with ACS provided an increase in FCT in coronary plaques during the first 3 weeks of follow-up and a further increase during 36 weeks of follow-up. T |
| PARADIGM/2018 Ref. [250] | prospective, multinational | Statin naïve patients vs patients on statins (94% of patients on statins were taking moderate to high-intensity statins: atorvastatin or rosuvastatin) |
consecutive patients without history of CAD who underwent serial coronary CTA at an interscan interval of ≥2 years. 1,079 coronary artery lesions were evaluated in statin naïve patients (n 474), and 2,496 coronary artery lesions were evaluated in statin-taking patients (n 781). | CCTA | Δ %DS, Δ PAV, plaque composition, and presence of high-risk plaque (presence of ≥2 features of low-attenuation plaque, positive arterial remodeling, or spotty calcifications). |
Lesions in patients on statin therapy showed a slower rate of overall PAV progression but more rapid progression of calcified PAV Progression of noncalcified PAV and annual incidence of new HRP features were lower in lesions of patients on statin treatment. |
| ODYSSEY J-IVUS/2019 Ref. [251] | Randomized controlled | Alirocumab 75 -150 mg every 2 weeks vs Atorvastatin ≥10 mg/day OR Rosuvastatin ≥5 mg/day) for 36 weeks | 206 patients with ACS and hypercholesterolemia (LDL-C not at target) | IVUS | Δ TAV :Normalized TAV (Week 36)− Normalized TAV (baseline)/Normalized TAV (baseline)×100 Δ PAV from baseline to week 36 |
36 weeks of alirocumab treatment resulted in a numerically greater but not statistically significant percentage reduction in normalized TAV |
| Budoff MJ et al. (EVAPORATE )/2020 Ref. [252] | Randomized, double-blind, placebo-controlled | Statin+icosapent ethyl vs Statin+mineral oil placebo (18 month treatment) |
80 patients with documented CAD and with persistent hypertriglyceridemia | MDCT | Δ low-attenuation plaque (LAP) volume | Significant reduction of LAP volume at 18 months |
| Nicholls SJ et al. (HUYGENS) /2022/Ref. [253] | Randomized, multicenter, double-blind, placebo controlled clinical |
Evolocumab 420 mg /month for 52 weeks + statin vs placebo+statin |
161 patients with a non–ST-segment MI and at least 1 NTL with coronary stenosis>20% 135 had evaluable imaging |
OCT IVUS |
Δ FCT Δ LA Δ TAV Δ PAV |
Evolocumab added to the maximally tolerated statin induced greater increase in minimum FCT, larger decrease in maximum LA, greater regression of TAV and PAV |
| Raber L et al. (PACMAN-AMI)/2022 Ref. [254] | Double-blind,randomized placebo controlled | Biweekly subcutaneous Alirocumab 150 mg +Rosuvastatin 20 mg vs Placebo+Rosuvastatin 20 mg for 52 weeks |
300 patients with AMI treated with PCI: 148 pts Alirocumab+rosuvastatin vs 152 pts Placebo+Rosuvastatin | IVUS, NIRS and OCT of NTLs |
Δ PAV of NTLs (from baseline to week 52) Δ maximum lipid core burden index (MLCBI) Δ minimal FCT |
Significant greater change in PAV with alirocumab (-2.13 vs -0.92%) Greater change in MLCBI Increase in minimal FCT |
| Nakano Y et al. (substudy of the CuVic trial)/2023/ Ref. [255] | Randomized controlled | Statin+ezetimibe (S+E) vs Statin monotherapy (S) (6-8 month- treatment) |
79 CAD patients treated with PCI: S+E 39 pts; S 40 pts | IVUS of NTLs | Δ plaque burden Δ percent change in plaque burden |
Greater plaque regression in the S+E group Lower values of Campesterol (a marker of cholesterol absorption), and oxysterols in the S+E group with a positive correlation with plaque regression |
Abbreviations bid: twice a day; tid: three times a day; qid: four times a day; ASTEROID: A Study to Evaluate the Effect of Rosuvastatin on Intravascular Ultrasound-Derived Coronary Atheroma Burden; BECAIT: Bezafibrate Coronary Intervention Trial; CABG: CAD: coronary artery disease; CCTA: coronary computed tomography angiography; CCT: coronary computed tomography; COMFORTABLE-AMI: Comparison of Biolimus Eluted From an Erodible Stent Coating With Bare Metal Stents in Acute ST-Elevation Myocardial Infarction; %DS: percent diameter stenosis; ESCORT: Effect of PitavaStatin on Coronary Fibrous-cap Thickness–Assessment by Fourier-Domain Optical CoheRence Tomography; FCT: fibrous cap thickness; FFR: fractional flow reserve, HUYGENS (High-Resolution Assessment of Coronary Plaques in a Global Evolocumab Randomized Study); IBIS-4: Integrated biomarker imaging study; IVUS: intravascular ultrasound; MARS: Monitored Atherosclerosis Regression Study; LDL-C serum low density lipoprotein cholesterol; MDCT multidetector computed tomography; MV: multivessel; NIRS = near-infrared spectroscopy; NOCS: non-obstructive coronary stenosis; NTL: non target lesion; OCT: optical coherence tomography; PARADIGM: Progression of AtheRosclerotic PlAque DetermIned by Computed TomoGraphic Angiography Imaging; PAV: percentage change in the atheroma volume; PCI: percutaneous coronary intervention; PRECISE-IVUS: Plaque Regression With Cholesterol Absorption Inhibitor or Synthesis Inhibitor Evaluated by Intravascular Ultrasound; QCA: Quantitative Coronary angiography; REVERSAL: Reversal of Atherosclerosis with Aggressive Lipid Lowering; STABLE: Statin and Atheroma Vulnerability Evaluation; SATURN: Study of CoronaryAtheroma by InTravascular Ultrasound: effect of Rosuvastatin versus AtorvastatiN; STABLE: Statin and Atheroma Vulnerability Evaluation; TAV: total atheroma volume; TC: Total cholesterol; vs: versus; YELLOW: Reduction in Yellow Plaque by Intensive Lipid Lowering Therapy.
Table 2.
SGLT2-Inhibitors and their effects on the atherosclerotic plaque.
| Study/year/Reference | Type of study | Lipid –lowering therapy | Population | Imaging | Endpoints | Results |
|---|---|---|---|---|---|---|
| SGLT2-Is and FCT. Ref. [268] | observational, randomized, multicenter study | SGLT2-Is vs Non-SGLT2-Is |
369 T2DM Patients with MV NO-CS: 111 SGLT2-I users vs 258 non-SLGT2-I users | OCT | Δ FCT (from baseline to a 12 month follow up control) | SGLT2-Is increased FCT and reduced the values of lipid arc degree |
| SGLT2-Is Stabilize Coronary Plaques in Acute Coronary Syndrome With Diabetes Mellitus. Ref. [269] | Retrospective study | SGLT2-Is vs Non-SGLT2-Is |
109 patients in the total cohort: 69 non-SGLT2-I users and 40 SGLT2-I users; 29 patients in the OCT cohort: 15 non-SGLT2-I users and 14 SGLT2-I users | OCT images of unstable plaques in nonstented lesions during ACS catheterization and at the 6-month follow-up. | Δ FCT | SGLT2-Is improved plaque stability through a significantly thicker fibrous cap and a reduced lipid arc |
| Evaluation of the effect of tofogliflozin on the tissue characteristics of the carotid wall—a sub-analysis of the UTOPIA trial. Ref. [270] |
Sub-analysis of the UTOPIA trial | Tofogliflozin |
168 and 169 patients in the tofogliflozin and conventional treatment groups were included in the full analysis set, respectively |
B-mode US carotid arteries | longitudinal change in the ultrasonic tissue characteristics of the carotid wall using gray-scale median (GSM), |
Reduction of IMT, but no change in plaque composition |
Abbreviations ACS: acute coronary syndrome; FCT: fibrous cap thickness; IMT: intima-media-thickness; OCT: optical coherence tomography; SGLT2-Is: sodium-glucose co-transporter-2 inhibitors.
Table 3.
The PREVENTOME: How to manage CV and cancer risk factors, who is in charge, the pathways, the desirable targets.
Table 3.
The PREVENTOME: How to manage CV and cancer risk factors, who is in charge, the pathways, the desirable targets.
| Life style | Risk factors | Committed subjects |
Non-pharmacological management |
Pharmacological Management |
Involved Pathways |
Targets |
| Obesity | Patient, GP, caregiver | Healthy diet, exercise | GLP1-Ras | CRP, TNF-α, MDA (Ref. [320]) | Optimal BMI (Ref. [2]) | |
| Hypertension | Patient, GP, caregiver | Diet (Restriction of sodium to ~ 2 g per day, MD, DASH, moderate or no alcohol), exercise | ACE-Is, ARBs, CCBs, | Impaired NO production, Oxidative stress. Endothelial dysfunction |
Tailored to CV risk, comorbidities and risk modifiers (Ref. [6]) |
|
| Diabetes | Patient, GP, caregiver | Diet, exercise | Metformin, GLP1-RAs, SGLT2-I | AMPK, IGFR, Mtor, ETC, β-Catenin Action, EGFR (Ref. [353]) |
Tailored to CV risk, comorbidities and risk modifiers (Ref. [6]) |
|
| Smoking | Patient, GP, caregiver | QUIT smoking | Drug support for smoking cessation (e.g. NRT) | ED, thrombosis, insulin resistance and dyslipidemia (Ref. [201]) |
No smoking | |
| Dyslipidemia | Patient, GP, caregiver | Diet, exercise | LLT: statins, bempedoic acid, ezetimibe, PCSK9-Is, fibrates | Cholesterol pathway, PCSK9 iperexpression in cancer |
LLT tailored to CV risk (Ref. [6]) and cancer prevention (Ref. [164]) |
|
| sedentary behaviour | Patient, GP, policymakers (for population-based interventions and the promotion of healthy environments) | exercise | n/a | Regulation of cardiometabolic and immune function. Oxidative stress, genomic instability and myokines (Ref. [6]); reduction of obesity-related cancer (Ref. [163]) |
Recommended for adults of all ages at least 150-300 min/week of moderate intensity or 75-150min/w of vigorous intensity aerobic PA. Adults who cannot perform 150 min of moderate-intensity PA/week should stay as active as their abilities and health condition allow (Ref. [6]) |
|
| unhealthy diet alcohol abuse | Patient, GP, caregiver, institutions (e.g. schools, workplaces etc), policymakers | Healthy diet (e.g.mediterranean diet, DASH). Moderate (<100 g/week) or No alcohol (Ref. [6], Ref. [163]) |
n/a. | Oxidative stress | Optimal BMI (Ref. [2]) No alcohol (Refs. [6,163]) |
|
| Psycho | Risk enhancers | Committed subjects |
Non-pharmacological management |
pharmacological management |
Pathways | Targets |
| Anxiety | Patient, Psychological support, caregiver | Healthy lifestyle; Psychotherapy; Care management approach , group-based cognitive behavioral therapy (Ref. [2,411] |
Antidepressants (SSRI) |
Accelerated development of CV risk factors (Ref. [212]) |
Improvement of symptoms, some beneficial effects on CVH | |
| Anger & hostility | Patient, Psychological support, caregiver | Healthy lifestyle | Accelerated development of CV Risk factors (Ref. [212]) |
Improvement of symptoms, some beneficial effects on CVH | ||
| Pessimism | Patient, Psychological support, caregiver | Healthy lifestyle | Psychopharmaco-therapy |
Accelerated development of CV Risk factors (Ref. [212]) | Optimistic behaviour, beneficial effects on CVH | |
| Exposome | Social determinants of health | Committed subjects |
Non-pharmacological management |
Pharmacological management |
Involved pathways | Targets |
| Environmental conditions: Air, Noise and Light pollution | Policymaker, health-care practice | Interventions to improve air quality | n/a | Syndemic effect with CV risk factors | Mitigation strategies for air pollution (e.g. transition from fossil fuels to renewable energy sources and transportation reforms); for noise pollution (e.g. implementation of noise reduction protocols, promotion of green spaces as natural sound buffers) and for light pollution (energy conservation and light pollution regulations (Ref. [229]) |
|
| Socio-economic status | Policymakers, Health professionals |
Improvement of social conditions | n/a | Stress-associated neural activity), bone marrow activity, and arterial inflammation (Ref. [211]) |
Reduction of stressors-induced inflammation, increase of resilience |
|
| Social isolation | Policymakers, health professionals | Tailored interventions | n/a | Increased arterial stiffness (Ref. [216]) | Reduction of loneliness feeling |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



