
Submitted:
21 November 2024
Posted:
25 November 2024
You are already at the latest version
Abstract
Substance use disorders (SUDs) and anxiety disorders are highly comorbid, a co-occurrence linked to worse clinical outcomes than either condition alone. While the neurobiological mechanisms involved in SUDs and anxiety disorders are well understood separately, the mechanisms underlying their comorbidity remain largely unknown. This narrative review explores the neurobiological processes underlying this comorbidity, using the Research Domain Criteria (RDoC) framework to map disruptions in positive valence, negative valence, and cognitive systems across the three stages of the addiction cycle: binge/intoxication, withdrawal/negative affect, and preoccupation/anticipation. Anxiety exacerbates each stage of addiction, marked by significant psychosocial impairment and dysregulation in the brain. A more thorough understanding of the neural underpinnings involved in comorbid SUD and anxiety disorders will contribute to more tailored and effective therapeutic interventions and assessments.
Keywords:
SUDs
; substance use
; addiction
; anxiety
; neuroimaging
; fMRI
; limbic system
; RDoC
1. Introduction
Substance use disorders (SUDs) are highly prevalent and costly. In the United States, drug and alcohol use contributed to nearly 11 million premature deaths in 2019 alone [1]. Effective treatment is particularly challenging due to the significant comorbidity between SUD and other mental health conditions. Among the concomitant mental health diagnoses, mood and anxiety disorders have strong reciprocal relationships with SUD [2,3]. For example, drug withdrawal can result in well-characterized autonomic and somatic symptoms classically accompanied by anxiety symptoms [4,5]. Psychological symptoms accompanying withdrawal, like anxiety, may be mistaken as part of withdrawal rather than an underlying separate mood disorder that requires careful treatment [6]. Aversive affective withdrawal symptoms, such as anxiety, can contribute to the escalation of compulsive drug use, maintenance of use, and relapse after periods of abstinence, i.e. negative reinforcement of drug addiction to alleviate negative emotional states [7,8,9].
Three explanatory models about the potential causal impacts of chronic anxiety on substance use (and vice versa) have been proposed. First, having a psychiatric disorder increases susceptibility to addictive behaviors because certain substances may temporarily reduce symptoms of mental conditions and act as a negative reinforcer [10]. Social anxiety disorder has been identified as an example of such a relationship, but for other anxiety disorders, the temporality with SUD development remains unclear [11]. Second, SUDs may promote vulnerability to anxiety disorders due to the consequences of chronic drug use or related withdrawal symptoms [12]. A study using National Epidemiological Survey on Alcohol and Related Conditions (NESARC) data found a higher likelihood of individuals having alcohol use disorder (AUD) as their primary diagnosis among patients with comorbid panic disorder or generalized anxiety disorder [11]. Third, shared genetic and environmental factors (e.g., traumatic or stressful life experiences) may mediate the relationship between SUDs and anxiety rather than reflecting a direct causal association ([13,14]. Importantly, these three possibilities are not mutually exclusive [15]. Neurobiological study of the pathogenesis and evolution of comorbid SUD and anxiety disorders is crucial to resolve these questions, advance treatment, and improve outcomes.
One approach for this purpose is to use the Research Domain Criteria (RDoC), a multi-system framework that maps domains of neurobehavioral functioning to mental disorders. Prior studies have successfully applied the RDoC framework to produce clinically-relevant insights for depressive, personality, and psychotic disorders [16,17,18]. Here we examine SUD-AD comorbidity through this lens, reviewing studies that highlight limbic system neuroadaptations associated with these disorders. For the purposes of this review, we included anxiety disorder diagnoses from multiple iterations of the DSM (i.e., panic disorder, generalized anxiety disorder, social anxiety disorder) and also included search terms that describe state and trait anxiety symptoms.
2. Dimensional Frameworks for Understanding Comorbidity
RDoC provides a transdiagnostic, systematic framework to characterize shared neurobiological processes underlying SUDs and ADs across domains. The RDoC matrix covers six domains: negative valence, positive valence, cognitive, social processes, arousal/regulatory, and sensorimotor systems. The AARDoC further delineates the major underlying domains of functions relevant to SUD: Negative Emotionality (mapping onto the negative valence system), Incentive Salience (mapping onto the positive valence system), and Executive Function (mapping onto the cognitive system). We note that the social processing, arousal, and sensorimotor systems are also relevant for SUD but here we focus on the three relevant domains suggested by [19].
Current neuroscience-based models conceptualize SUD as a three-stage cyclical process that intensifies with continuing drug use. These stages include 1) binge and intoxication, 2) withdrawal and negative affect, and 3) preoccupation and craving [20]. The three stages in the addiction cycle represent three functional psychobiological constructs: incentive salience or pathological habits, reward deficit or stress surfeit, and executive dysfunction. Anxiety, marked by a state of distress and arousal, is relevant to all three stages of SUD. Given significant overlaps between SUDs and anxiety in various domains, especially negative valence and cognitive systems, this psychobiological framework is of particular relevance to the SUD-AD comorbid condition. Core dysfunctions of SUD and AD and their manifestations were investigated in the context of the RDoC matrices for negative valence, positive valence, and cognitive systems for each disorder.
Below we summarize the basic neurobiology underlying each process, followed by a narrative review of the relevant neuroimaging data.
2.1. Positive Valence Systems–Binge/Intoxication
2.1.1. Neurobiology
Individuals with anxiety often exhibit diminished sensitivity in positive valence systems, including the motivation to obtain rewards [21,22,23]. This is evidenced by decreased activation of the striatum to reward feedback [24]. Blunted reward processing to natural rewards may prime people with anxiety disorders to seek out other experiences that increase reward signaling, such as substance use [25]. During the binge and intoxication phase, consuming drugs increases activity related to positive valence systems, such as reward seeking and habit learning [26]. The mesolimbic and the mesocortical dopamine systems are highly involved in this drug-induced reward processing. The mesolimbic system includes neurons that originate in the ventral tegmental area (VTA) and project upwards to the ventral striatum (VS), including the nucleus accumbens. Drug consumption induces rapid ‘bursts’ of dopamine release in the vs. (also known as phasic dopamine release) [27], which activate dopamine D1 receptors and are associated with the rewarding experience of feeling “high” or euphoric [28,29]. The adjacent nigrostriatal dopamine system has been classically associated with motor control, but it also plays a role in reward processing. This pathway originates in the substantia nigra and projects upward to the dorsal striatum (DS). Like in the VS, drug consumption also increases dopamine release in the DS, though to a lesser extent than in the other dopamine systems [28,29].
With long-term drug use, an individual’s reward processing distorts to disproportionately favor drug consumption over other rewards. This reflects in part long term potentiation (LTP), which is one of the mechanisms driving neuroplasticity in the brain triggered by drug-induced signaling [30]. These neuroplastic changes drive incentive salience i.e. heightened or focused attention toward cues linked to rewarding behaviors [31]. Similar to the mesolimbic system, the mesocortical system also originates in the VTA and includes neuronal projections to the medial prefrontal cortex (mPFC). Release of dopamine into the mPFC cues incentive salience, which increases motivation for further drug consumption [20,29]. This is further evidenced by research that has found that as an individual starts to develop drug-cue associations, phasic dopamine bursts also occur in response to drug cues [32].
2.1.2. Neuroimaging Findings: Anxiety → Binge/Intoxication
Stress, particularly during early life, can sensitize reward circuitry and make someone more prone to engaging in substance use [33]. There is neurobiological evidence for this idea; neuroimaging studies find acute intoxication could potentially counteract anxiety-related neural dysregulation. Anxiety is associated with dampened or dysregulated activity in the vs. [34,35], so during intoxication, the supraphysiological bursts of vs. dopamine and heightened vs. activity may overcome these deficits [20,36,37]. As people consume drugs more frequently, drug cues alone can also prompt increased vs. activity [38]. Further, many anxiety disorders are consistently associated with increased activity in fear-related limbic regions including the amygdala [39], particularly in response to relevant anxiety cues [40]. Similar to how acute intoxication can increase vs. activity to potentially counteract dysregulated reward-related activity in people with anxiety, some studies have found that intoxication, particularly with alcohol, can acutely decrease amygdala reactivity [41,42].
2.1.3. Neuroimaging Findings: Binge/Intoxication → Anxiety
While drugs may temporarily relieve feelings of anxiety, chronic self-medication leads to maladaptive neuroplastic changes that decrease the value of drugs. For example, with long-term substance use, stimulant drugs do not induce an increase in dopamine signaling to the same degree as healthy controls [37]. Simultaneously, changes in the nigrostriatal system may support habit formation [43], which may be why drug cues alone are sufficient to induce dopamine increases in dorsal striatum in SUD [44]). Intriguingly, a case study found that damage to the dorsal striatum completely reversed addictive behavior [45]. Over time, a paradoxical brain response develops; dopamine responses to drug consumption decrease while incentive salience increases [20,46]. This mismatch results in increased “wanting” and decreased “liking” [46].
Impaired reward prediction error (RPE) learning underlies the drive to seek rewards in SUDs [47] and can lead to increased negative emotions and feelings of anxiety, as the experience of drug consumption does not match the anticipated response. Disrupted dopamine RPE signal is associated with neuronal plasticity alterations in the striatum, frontal cortex, and amygdala [48]. Behaviorally, prediction errors are also implicated in anxiety disorders as wrong expectations of danger can trigger excessive fear levels and motivate avoidance behaviors [49]. Clinical studies showed that prediction error signaling is disrupted in patients with generalized anxiety disorder (GAD) completing a passive avoidance task and associated their performance with ventromedial prefrontal cortex (vmPFC) and ventral striatum regions. Individuals with social anxiety disorder (SAD) also show similar trends but with elevated dmPFC activation correlating to prediction errors, and reduced dmPFC-ventral pallidum connectivity [50].
2.2. Negative Valence Systems - Withdrawal/Negative Affect
2.2.1. Neurobiology
Withdrawal/negative affect follows the binge/intoxication stage of the addiction cycle and includes core components of anxiety disorders. During withdrawal, dopamine transmission decreases in mesolimbic circuits are associated with motivational deficits and decreased mood [30]. As dependence and withdrawal develops, the brain’s antireward system is activated and negative affective symptoms emerge including anxiety, irritability, and hyperkatifeia [51]. While different drugs can elicit different withdrawal symptoms, negative affect is a universal and motivational element of withdrawal [52]. These negative emotional states spur further drug use to avoid discomfort, i.e. negative reinforcement [53]. Individuals with a history of anxiety experience more intense withdrawal symptoms and withdrawal-related discomfort and relapse from substances like methamphetamine, nicotine, or alcohol [54,55]), and baseline diagnosis of anxiety disorders like SAD and panic disorder significantly predicted early alcohol relapse [56].
These negative emotional states are driven by increased corticotropin-releasing factor (CRF), noradrenaline, and dynorphin signaling [51]. Injection of CRF antagonists into the central amygdala reduces anxiogenic-like states in rats withdrawn from substances including alcohol, nicotine, and cocaine [57,58,59,60]. Further, noradrenergic antagonists administered into the BNST reversed opioid withdrawal-induced place aversion in rodents [61]. Recent evidence suggests changes in endogenous endocannabinoid systems in the extended amygdala are associated with heightened anxiogenic responses in rats with cannabis withdrawal undergoing classical anxiety paradigms like the elevated plus-maze and the light/dark box [62,63,64]. Clinically, classical medications used to treat alcohol and heroin withdrawal include α-adrenergic drugs that inhibit noradrenergic release. Together, these findings highlight the importance of stress signaling in the extended amygdala, a component of the limbic system that is linked with anxiety disorders as demonstrated in human imaging studies.
2.2.2. Neuroimaging Findings: Withdrawal/Negative Affect ⟷ Anxiety
While the directionality between anxiety and SUD specific to the withdrawal stage remains hard to disentangle through neuroimaging research, we present general findings regarding neurobiological overlap between withdrawal and anxiety phenotypes.
The amygdala is heavily implicated in the withdrawal/negative affect stage and increased connectivity in amygdala-related networks is associated with increased emotional reactivity [65,66]. Alterations in connectivity between large-scale brain networks, such as the salience network (SN, including the insula, anterior cingulate, amygdala and hypothalamus) and the default mode network (DMN, including medial prefrontal and parietal cortex) are critically involved in both withdrawal and anxiety. SN-DMN connectivity is elevated during withdrawal from substances such as tobacco and alcohol [67,68]. Elevated SN-DMN connectivity is also commonly observed in adolescents and adults with anxiety disorders compared to healthy controls [69,70,71,72], and positively correlates with anxiety severity among both anxiety patients and healthy controls [69,73,74].
These connectivity changes are thought to direct attention towards withdrawal-induced physiological sensations, heightening internalizing and anxiety symptoms [75]. For example, both nicotine and alcohol withdrawal [76], self-reported anxiety [77], and irritability [78] have all been linked to elevated amygdala-insula functional connectivity. This may explain why individuals with a history of anxiety experience more intense withdrawal symptoms and withdrawal-related discomfort and relapse from substances like methamphetamine, nicotine, or alcohol [55]), as increased amygdala-insula reactivity has been observed in anxiety patients across all ages [79,80,81,82].
As mentioned above, α-adrenergic drugs are effective in treating alcohol withdrawal symptoms, and imaging evidence supports this. Prazosin treatment improves dysregulation in DMN regions including medial prefrontal cortex (mPFC), which has been associated with severity of alcohol withdrawal symptoms [83] and implicated in anxiety psychopathology [84]. While the SN is involved in processing internal or external stimuli, and mediates the switching between DMN and executive control network (ECN), the DMN plays a central role in self-referential processes (evaluating salience or internal and external cues, remembering the past, and planning the future) implicated in affective disorders like anxiety [85] and in SUD [29]. Dysfunctions in within-network and between-network DMN connectivity is heavily implicated across all anxiety disorders [86], and recent studies have suggested DMN aberrations may underlie anxiety symptoms such as perseverative thoughts in generalized anxiety disorder (GAD) [87,88] and possibly predict anxiety disorders such as GAD and social anxiety disorder [88,89]. Therefore, among the existing resting state networks, the DMN may be of particular interest in comorbid SUD-anxiety conditions during the withdrawal stage.
Chronic drug use has opposing effects on DMN engagements, which may contribute to the predominance of anti-reward systems during the withdrawal/negative affect stage [86]. The DMN can be further split into anterior and posterior portions, and reduced anterior-posterior DMN connectivity has been associated with impaired self-awareness [90], and in addicted persons this contribute to uncontrolled drug-taking [91,92]. Increased posterior DMN involvement may underlie ruminatory behaviors, resulting in distress and negative emotional states like anxiety [93,94], and resting-state studies in individuals addicted to substances like alcohol, heroin, or cannabis found that chronic drug use enhances posterior DMN, and exacerbates the imbalance of anterior-posterior DMN [29,95,96]. Decreased connectivity between the posterior and anterior DMN may contribute to the inability to inhibit negative emotional states, interfering with abstinence and flexible decision-making which could further exacerbate the anxiety symptoms experienced during withdrawal [97].
Emerging evidence also highlights the importance of the bed nucleus of the stria terminalis (BNST) in withdrawal related-anxiety and relapse as a critical node in both the stress and reward circuitries [2]. During withdrawal, the amygdala releases CRF on receptors in the bed nucleus stria terminalis (BNST) [98], and heightened amygdala-BNST connectivity was observed in people undergoing alcohol withdrawal [68,99]. The BNST is involved in withdrawal related-anxiety and relapse, serving as a critical node in both stress and addiction circuitry with connections to multiple limbic and brainstem regions including the amygdala and VTA. fMRI studies using shock paradigms described increased BNST engagement mediating sustained fear responses, and activity correlated with physiological skin conductance and self-reported anxiety ratings [100,101,102,103].
2.3. Cognitive Systems - Preoccupation/Anticipation
2.3.1. Neurobiology
Commonly known as “craving”, the preoccupation/anticipation stage of addiction is characterized by a disruption of executive function and involves the prefrontal cortex. Studies have linked poor executive function (i.e., inhibition, working memory) with early initiation of alcohol, tobacco, and other substance use [104,105,106]. In turn, acute craving decreases the ability to control attention away from drug cues [107,108]. Comorbid anxiety disorder exacerbates drug craving [109] and both cue- and stress-induced craving and anxiety are linked to early attrition from alcohol use disorder treatment; these observations are in part driven by dysregulated hypothalamic-pituitary-adrenal (HPA) axis function [110].
Prior studies found working memory, attentional control, inhibitory control to be among the most common cognitive domains impacted by anxiety as well as SUD. Reciprocal glutamatergic connections between the PFC and the dorsal striatum are heavily involved in the flexible control of these behaviors [111]. Preclinical evidence showed that rats withdrawn from substances like cocaine or methamphetamine were unable to develop long-term potentiation and long-term depression in the nucleus accumbens region after stimulating the PFC, suggesting that chronic substance use depresses PFC-accumbens synapses [112,113]. However, N-acetylcysteine (NAC) treatment prevents relapse by activating cystine-glutamate exchange in the cortico-accumbens circuitry [114], a finding that is consistent in human studies that reported decreased desire to use drugs in response to cocaine cue-reactivity [115].
Persistent prefrontal dopamine D1 receptor signaling is crucial for working memory, a foundational cognitive function [116,117,118]. Nonhuman primate studies showed blocking D1Rs in the PFC impaired learning of novel associations and decreased cognitive flexibility during a working memory task [117,119], and human studies reported that systemic administration of mixed D1/D2 agonist facilitated working memory while D2 agonist had no effect [120]. Striatal dopamine D1 versus D2 receptor signaling is also implicated in flexible control of behavior. Animal studies using the probabilistic reversal learning paradigm found that positive feedback learning is modulated by D1R signaling in the ventral striatum while D2R signaling modulates negative feedback learning. Stimulation of D2R in the ventral or dorsolateral striatum promoted explorative choice behavior [121] and reversal learning was impaired by D2R antagonism but not D1R antagonism in the dorsal striatum [122]. Studies have provided evidence that dorsal striatum D1 medium spiny neurons (MSNs) mediate reward/reinforcement and D2-MSNs mediate aversion [123]. Further, rats completing an instrumental task showed that D1R inhibition and D2 activation both promote the expression of flexible responding after development of habitual or compulsive-like behaviors [124].
2.3.2. Neuroimaging Findings: Anxiety → Preoccupation/Anticipation
During the preoccupation and anticipation phase of the addiction cycle, attention to drug cues is heightened [125,126]. Neuroimaging studies of cue reactivity have found increased activation related to craving for alcohol, nicotine, or cannabis in cognitive control regions, such as the anterior cingulate cortex (ACC) and ventromedial prefrontal cortex (vmPFC) and limbic regions like the ventral striatum [126,127,128,129]. Alcohol cue-elicited activation of the ventral striatum correlated with behavioral measures [128] and nicotine craving correlated with left vmPFC and amygdala activation when viewing smoking-related pictures [126] People with anxiety disorders also exhibit problems with cognitive flexibility [130], and high trait anxiety is linked to low PFC activity during attentional control [131] and dysregulated connectivity between PFC and subcortical regions including the amygdala, basolateral amygdala (BLA), insula, and hippocampus [130,132,133,134,135,136]. In task-based fMRI studies with the stop signal task, amygdala activation positively correlated with trait anxiety, and with the vmPFC during risk taking. Using the same SST task in cocaine-dependent patients [137], vmPFC activation correlated negatively with improved inhibitory control during methylphenidate treatment [138]. Together, these findings suggest that anxiety-related dysregulation in cognitive systems, combined with increased amygdala activation and stress symptoms associated with the preoccupation phase [20], may worsen or reinforce altered cognitive control associated with cue reactivity.
2.3.3. Neuroimaging Findings: Preoccupation/Anticipation → Anxiety
Long-term substance use creates a paradoxical effect in which reward responses are blunted while anticipation heightens [20,46]. During this preoccupation and anticipation phase, many factors promote craving. Neural biomarkers like the insula, hippocampus, and prefrontal cortex are implicated in the craving stage [125]. The insula, particularly its anterior regions, are reciprocally connected to several limbic regions and is responsible for an interoceptive function (integrating autonomic/visceral information with emotion, motivation, and conscious awareness) [139].
SUDs impair interoception [140] and damaged interoceptive awareness is likely one of the contributing factors to why people with SUD continue substance use [141]. Chronic drug use can lead an individual to associate interoceptive cues with the rewards of drugs to trigger cravings, as the body is reminded of the positive effects of drugs and primes the urge to seek drugs. The imbalance between interoception/exteroception causes an increased focus on external stimuli (i.e. drug cues) and a decreased ability to perceive internal bodily states [78,142]. Neuroimaging studies demonstrated insula activity in response to drug cues in patients addicted to cigarettes, cocaine, and alcohol, and correlated insula activity with self-reported cravings [139,143,144,145,146]. SUD patients with lesions to the insula (or even other regions functionally connected to the insula) can remarkably have a complete remission of their addiction and no longer experience drug cravings or relapse [147,148]. The anterior insula is reciprocally connected to several limbic regions, and cue-reactivity fMRI studies on alcohol-related craving found increased connectivity between the left insula-left dorsomedial PFC but decreased connectivity in a network including the ACC, insula, and hippocampus [149].
The insula, particularly the anterior insula, is also heavily implicated in the pathophysiology of anxiety and anxiety disorders [150,151,152]. Alvarez et al. found that individuals with greater anxiety proneness and less perceived control showed greater activity in the anterior insula during anticipation of unpredictable threat [153]. Individuals who are prone to anxiety experience augmented signaling between observed and expected body state, and may use worrying about possible aversive outcomes as a cognitive avoidance response to stressful, unpredictable life events [151,154]. Similarly, addicted individuals with diminished interoceptive abilities may have difficulties regulating internal/external states in response to stressful situations, and turn to further substance use like alcohol as a coping mechanism [155,156,157]. Given the overlap in dysregulated insular activity and interoceptive abilities underlying both SUDs and anxiety disorders, it is likely that anxiety symptoms are amplified or anxiety disorders emerge during the preoccupation/anticipation stage.
3. Conclusions and Future Directions
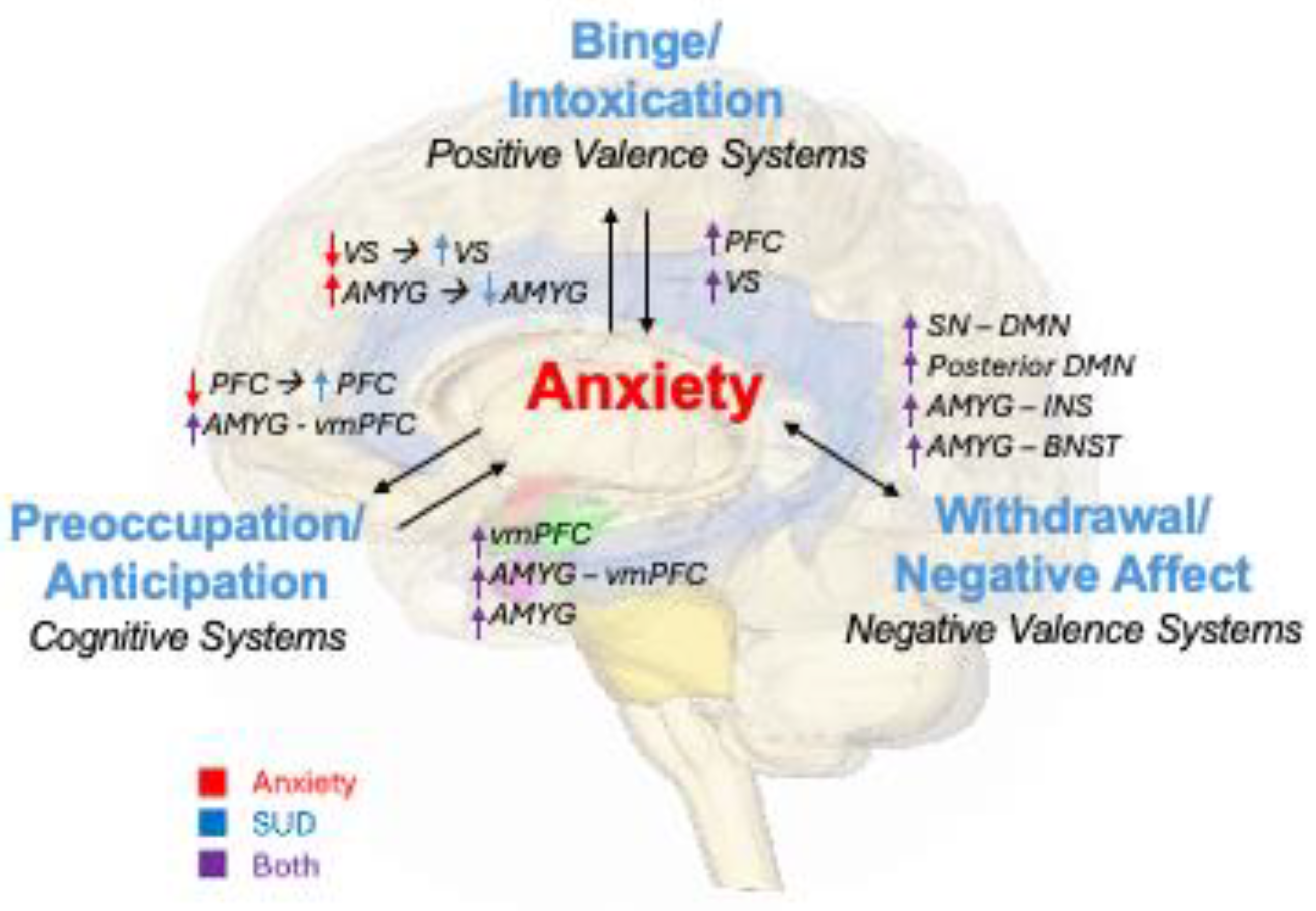
The neurobiological circuits underlying SUDs and anxiety disorders interact to exacerbate symptoms as individuals cycle through the three stages of addiction. Anxiety can prompt people to consume drugs, which temporarily recruits positive valence systems and increases incentive salience over time. During withdrawal, activity in negative valence systems heightens, and anxiety symptoms increase rapidly. As people enter into the preoccupation and anticipation phase, changes to cue reactivity and interoception are reflected in cognitive systems. The cycle repeats as people become intoxicated again due to lack of cognitive control and increased incentive salience and cue reactivity. As tolerance increases, people binge with increasing drug quantities and neuroplastic changes are reinforced. Each stage of the cycle can worsen preexisting or SUD-induced anxiety. Common findings from task and resting state fMRI are related to these processes as summarized in Figure 1.
Encouragingly, longitudinal studies of people with SUDs in recovery have found that drug-related functional deficits can be at least partially reversed with abstinence. For example, an investigation of people in OUD recovery found improvements in nucleus accumbens function in response to reward [159]. Increased DA transporters after abstinence was observed in methamphetamine users [160], and DA transporter binding in alcohols matched healthy controls after a 4-week period of abstinence [161]. There is also some promising research that anxiety treatment can cause positive functional changes; studies have found decreases in overactivation of regions of the limbic system, such as the ACC [162], amygdala [163], and hippocampus [164]. Decreased activity in these regions correlated with improvement in PTSD [165] and social anxiety [163] symptom severity.
Further research is needed on treatments for comorbid anxiety and SUDs, including studies with a focus on assessing functional changes in the brain. Longitudinal investigations may prove especially useful, as they would provide information about acute versus long-term changes in these disorders. The direction of causality between anxiety and SUDs could also be better understood; it is important to explore whether "self-medication" of anxiety using substances is more prevalent than SUD-inducing anxiety disorders and whether the order of onset reflects differences in underlying neurobiology. Furthermore, future research should focus on sex differences to investigate how sex influences comorbid anxiety and SUD, and to what extent differences are genetically determined or influenced by environmental factors. Variables such as the duration of drug use, abstinence periods, relapse rates, and overdose rates should also be included to better understand the progression and outcomes of SUD. These research aims would help develop more effective treatment and prevention strategies for SUDs and anxiety disorders.
Author Contributions
P.M. and E.R.L. conceived the paper topic. E.R.L. and F.N.V. wrote the first draft of the manuscript, and all authors edited and approved of the final draft.
Funding
This work was accomplished with support from the National Institute on Alcohol Abuse and Alcoholism (ZIAAA000550).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Volkow, N.D.; Blanco, C. Substance Use Disorders: A Comprehensive Update of Classification, Epidemiology, Neurobiology, Clinical Aspects, Treatment and Prevention. World Psychiatry, 2023, 22, 203–229. [Google Scholar] [CrossRef]
- Avery, S.N.; Clauss, J.A.; Blackford, J.U. The Human BNST: Functional Role in Anxiety and Addiction. Neuropsychopharmacol, 2016, 41, 126–141. [Google Scholar] [CrossRef]
- Lüthi, A.; Lüscher, C. Pathological Circuit Function Underlying Addiction and Anxiety Disorders. Nat Neurosci, 2014, 17, 1635–1643. [Google Scholar] [CrossRef]
- Colasanti, A.; Rabiner, E.; Lingford-Hughes, A.; Nutt, D. Opioids and Anxiety. J Psychopharmacol, 2011, 25, 1415–1433. [Google Scholar] [CrossRef]
- Vorspan, F.; Mehtelli, W.; Dupuy, G.; Bloch, V.; Lépine, J.-P. Anxiety and Substance Use Disorders: Co-Occurrence and Clinical Issues. Curr Psychiatry Rep, 2015, 17, 4. [Google Scholar] [CrossRef]
- Quello, S.B.; Brady, K.T.; Sonne, S.C. Mood Disorders and Substance Use Disorder: A Complex Comorbidity. Science & Practice Perspectives, 2005, 3, 13. [Google Scholar] [CrossRef]
- Aston-Jones, G.; Harris, G.C. Brain Substrates for Increased Drug Seeking during Protracted Withdrawal. Neuropharmacology, 2004, 47, 167–179. [Google Scholar] [CrossRef]
- Schulteis, G.; Koob, G.F. Reinforcement Processes in Opiate Addiction: A Homeostatic Model. Neurochem Res, 1996, 21, 1437–1454. [Google Scholar] [CrossRef]
- Self, D.W.; Nestler, E.J. Relapse to Drug-Seeking: Neural and Molecular Mechanisms. Drug Alcohol Depend, 1998, 51, 49–60. [Google Scholar] [CrossRef]
- Robinson, J. Role of Self-Medication in the Development of Comorbid Anxiety and Substance Use Disorders: A Longitudinal Investigation. Arch Gen Psychiatry, 2011, 68, 800. [Google Scholar] [CrossRef]
- Pacek, L.R.; Storr, C.L.; Mojtabai, R.; Green, K.M.; La Flair, L.N.; Alvanzo, A.A.H.; Cullen, B.A.; Crum, R.M. Comorbid Alcohol Dependence and Anxiety Disorders: A National Survey. Journal of Dual Diagnosis, 2013, 9, 271–280. [Google Scholar] [CrossRef]
- Blaney, D.; Jackson, A.K.; Toy, O.; Fitzgerald, A.; Piechniczek-Buczek, J. Substance-Induced Anxiety and Co-Occurring Anxiety Disorders. In Substance Use and the Acute Psychiatric Patient: Emergency Management; Donovan, A.L., Bird, S.A., Eds.; Springer International Publishing: Cham, 2019; pp. 125–144. [Google Scholar] [CrossRef]
- María-Ríos, C.E.; Morrow, J.D. Mechanisms of Shared Vulnerability to Post-Traumatic Stress Disorder and Substance Use Disorders. Front. Behav. Neurosci., 2020, 14. [Google Scholar] [CrossRef]
- Marquenie, L.A.; Schadé, A.; van Balkom, A.J.L.M.; Comijs, H.C.; de Graaf, R.; Vollebergh, W.; van Dyck, R.; van den Brink, W. Origin of the Comorbidity of Anxiety Disorders and Alcohol Dependence: Findings of a General Population Study. European Addiction Research, 2006, 13, 39–49. [Google Scholar] [CrossRef]
- Bartoli, F.; Carretta, D.; Clerici, M.; Carrà, G. Comorbid Anxiety and Alcohol or Substance Use Disorders: An Overview. In Textbook of Addiction Treatment: International Perspectives; el-Guebaly, N., Carrà, G., Galanter, M., Eds.; Springer Milan: Milano, 2015; pp. 1971–1983. [Google Scholar] [CrossRef]
- Koudys, J.W.; Traynor, J.M.; Rodrigo, A.H.; Carcone, D.; Ruocco, A.C. The NIMH Research Domain Criteria (RDoC) Initiative and Its Implications for Research on Personality Disorder. Curr Psychiatry Rep, 2019, 21, 37. [Google Scholar] [CrossRef]
- Morris, S.E.; Pacheco, J.; Sanislow, C.A. Applying Research Domain Criteria (RDoC) Dimensions to Psychosis. In Psychotic disorders: Comprehensive conceptualization and treatments; Oxford University Press: New York, NY, US, 2021; pp. 29–37. [Google Scholar] [CrossRef]
- Woody, M.L.; Gibb, B.E. Integrating NIMH Research Domain Criteria (RDoC) into Depression Research. Curr Opin Psychol, 2015, 4, 6–12. [Google Scholar] [CrossRef]
- Litten, R.Z.; Ryan, M.L.; Falk, D.E.; Reilly, M.; Fertig, J.B.; Koob, G.F. Heterogeneity of Alcohol Use Disorder: Understanding Mechanisms to Advance Personalized Treatment. Alcohol Clin Exp Res, 2015, 39, 579–584. [Google Scholar] [CrossRef]
- Koob, G.F.; Volkow, N.D. Neurobiology of Addiction: A Neurocircuitry Analysis. The Lancet Psychiatry, 2016, 3, 760–773. [Google Scholar] [CrossRef]
- Craske, M.G.; Meuret, A.E.; Ritz, T.; Treanor, M.; Dour, H.J. Treatment for Anhedonia: A Neuroscience Driven Approach: 2015 ADAA Scientific Research Symposium: Treatment for Anhedonia. Depress Anxiety, 2016, 33, 927–938. [Google Scholar] [CrossRef]
- Dillon, D.G.; Rosso, I.M.; Pechtel, P.; Killgore, W.D.S.; Rauch, S.L.; Pizzagalli, D.A. PERIL AND PLEASURE: AN RDOC-INSPIRED EXAMINATION OF THREAT RESPONSES AND REWARD PROCESSING IN ANXIETY AND DEPRESSION: Neighborhood Characteristics and Mental Health. Depress Anxiety, 2014, 31, 233–249. [Google Scholar] [CrossRef]
- Taylor, C.T.; Hoffman, S.N.; Khan, A.J. Anhedonia in Anxiety Disorders. In Anhedonia: Preclinical, Translational, and Clinical Integration; Pizzagalli, D.A., Ed.; Current Topics in Behavioral Neurosciences; Springer International Publishing: Cham, 2022; Volume 58, pp. 201–218. [Google Scholar] [CrossRef]
- McDermott, T.J.; Berg, H.; Touthang, J.; Akeman, E.; Cannon, M.J.; Santiago, J.; Cosgrove, K.T.; Clausen, A.N.; Kirlic, N.; Smith, R.; Craske, M.G.; Abelson, J.L.; Paulus, M.P.; Aupperle, R.L. Striatal Reactivity during Emotion and Reward Relates to Approach-Avoidance Conflict Behaviour and Is Altered in Adults with Anxiety or Depression. J Psychiatry Neurosci, 2022, 47, E311–E322. [Google Scholar] [CrossRef]
- Smith, J.P.; Book, S.W. Anxiety and Substance Use Disorders: A Review. Psychiatr Times, 2008, 25, 19–23. [Google Scholar] [PubMed]
- Kwako, L.E.; Momenan, R.; Litten, R.Z.; Koob, G.F.; Goldman, D. Addictions Neuroclinical Assessment: A Neuroscience-Based Framework for Addictive Disorders. Biol Psychiatry, 2016, 80, 179–189. [Google Scholar] [CrossRef] [PubMed]
- Grace, A.A. The Tonic/Phasic Model of Dopamine System Regulation and Its Implications for Understanding Alcohol and Psychostimulant Craving. Addiction, 2000, 95, 119–128. [Google Scholar] [CrossRef]
- Wise, R.A. Roles for Nigrostriatal—Not Just Mesocorticolimbic—Dopamine in Reward and Addiction. Trends in Neurosciences, 2009, 32, 517–524. [Google Scholar] [CrossRef]
- Zhang, R.; Volkow, N.D. Brain Default-Mode Network Dysfunction in Addiction. Neuroimage, 2019, 200, 313–331. [Google Scholar] [CrossRef]
- Koob, G.F.; Volkow, N.D. Neurocircuitry of Addiction. Neuropsychopharmacol, 2010, 35, 217–238. [Google Scholar] [CrossRef]
- Robinson, M.J.F.; Robinson, T.E.; Berridge, K.C. Incentive Salience and the Transition to Addiction. In Biological Research on Addiction; Elsevier, 2013; pp 391–399. [CrossRef]
- Volkow, N.D.; Michaelides, M.; Baler, R. The Neuroscience of Drug Reward and Addiction. Physiological Reviews, 2019, 99, 2115–2140. [Google Scholar] [CrossRef]
- Hellberg, S.N.; Russell, T.I.; Robinson, M.J.F. Cued for Risk: Evidence for an Incentive Sensitization Framework to Explain the Interplay between Stress and Anxiety, Substance Abuse, and Reward Uncertainty in Disordered Gambling Behavior. Cogn Affect Behav Neurosci, 2019, 19, 737–758. [Google Scholar] [CrossRef]
- Boehme, S.; Ritter, V.; Tefikow, S.; Stangier, U.; Strauss, B.; Miltner, W.H.R.; Straube, T. Brain Activation during Anticipatory Anxiety in Social Anxiety Disorder. Soc Cogn Affect Neurosci, 2014, 9, 1413–1418. [Google Scholar] [CrossRef]
- Sripada, C.; Angstadt, M.; Liberzon, I.; McCabe, K.; Phan, K.L. Aberrant Reward Center Response to Partner Reputation during a Social Exchange Game in Generalized Social Phobia. Depress Anxiety, 2013, 30, 353–361. [Google Scholar] [CrossRef]
- Gilman, J.M.; Ramchandani, V.A.; Davis, M.B.; Bjork, J.M.; Hommer, D.W. Why We like to Drink: A Functional Magnetic Resonance Imaging Study of the Rewarding and Anxiolytic Effects of Alcohol. J Neurosci, 2008, 28, 4583–4591. [Google Scholar] [CrossRef] [PubMed]
- Volkow, N.D.; Tomasi, D.; Wang, G.-J.; Logan, J.; Alexoff, D.L.; Jayne, M.; Fowler, J.S.; Wong, C.; Yin, P.; Du, C. Stimulant-Induced Dopamine Increases Are Markedly Blunted in Active Cocaine Abusers. Mol Psychiatry, 2014, 19, 1037–1043. [Google Scholar] [CrossRef] [PubMed]
- Volkow, N.D.; Wang, G.-J.; Telang, F.; Fowler, J.S.; Logan, J.; Childress, A.-R.; Jayne, M.; Ma, Y.; Wong, C. Dopamine Increases in Striatum Do Not Elicit Craving in Cocaine Abusers Unless They Are Coupled with Cocaine Cues. NeuroImage, 2008, 39, 1266–1273. [Google Scholar] [CrossRef] [PubMed]
- Liberzon, I.; Duval, E.; Javanbakht, A. Neural Circuits in Anxiety and Stress Disorders: A Focused Review. TCRM, 2015, 115. [CrossRef]
- Shin, L.M.; Liberzon, I. The Neurocircuitry of Fear, Stress, and Anxiety Disorders. Neuropsychopharmacol, 2010, 35, 169–191. [Google Scholar] [CrossRef]
- Hur, J.; Kaplan, C.M.; Smith, J.F.; Bradford, D.E.; Fox, A.S.; Curtin, J.J.; Shackman, A.J. Acute Alcohol Administration Dampens Central Extended Amygdala Reactivity. Sci Rep, 2018, 8, 16702. [Google Scholar] [CrossRef]
- Sripada, C.S.; Angstadt, M.; McNamara, P.; King, A.C.; Phan, K.L. Effects of Alcohol on Brain Responses to Social Signals of Threat in Humans. NeuroImage, 2011, 55, 371–380. [Google Scholar] [CrossRef]
- Lipton, D.M.; Gonzales, B.J.; Citri, A. Dorsal Striatal Circuits for Habits, Compulsions and Addictions. Front. Syst. Neurosci., 2019, 13, 28. [Google Scholar] [CrossRef]
- Volkow, N.D.; Wang, G.-J.; Telang, F.; Fowler, J.S.; Logan, J.; Childress, A.-R.; Jayne, M.; Ma, Y.; Wong, C. Cocaine Cues and Dopamine in Dorsal Striatum: Mechanism of Craving in Cocaine Addiction. Journal of Neuroscience, 2006, 26, 6583–6588. [Google Scholar] [CrossRef]
- Muskens, J.B.; Schellekens, A.F.A.; De Leeuw, F.E.; Tendolkar, I.; Hepark, S. Damage in the Dorsal Striatum Alleviates Addictive Behavior. General Hospital Psychiatry, 2012, 34, 702.e9–702.e11. [Google Scholar] [CrossRef]
- Olney, J.J.; Warlow, S.M.; Naffziger, E.E.; Berridge, K.C. Current Perspectives on Incentive Salience and Applications to Clinical Disorders. Curr Opin Behav Sci, 2018, 22, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Tolomeo, S.; Yaple, Z.A.; Yu, R. Neural Representation of Prediction Error Signals in Substance Users. Addiction Biology, 2021, 26, e12976. [Google Scholar] [CrossRef] [PubMed]
- Schultz, W. Dopamine Reward Prediction Error Coding. Dialogues in Clinical Neuroscience, 2016, 18, 23. [Google Scholar] [CrossRef] [PubMed]
- Papalini, S.; Beckers, T.; Vervliet, B. Dopamine: From Prediction Error to Psychotherapy. Transl Psychiatry, 2020, 10, 1–13. [Google Scholar] [CrossRef]
- Becker, M.P.I.; Voegler, R.; Peterburs, J.; Hofmann, D.; Bellebaum, C.; Straube, T. Reward Prediction Error Signaling during Reinforcement Learning in Social Anxiety Disorder Is Altered by Social Observation. bioRxiv October 30, 2019, p 821512. [CrossRef]
- Koob, G.F. Negative Reinforcement in Drug Addiction: The Darkness Within. Current Opinion in Neurobiology, 2013, 23, 559–563. [Google Scholar] [CrossRef]
- Piper, M.E. Withdrawal: Expanding a Key Addiction Construct. Nicotine & Tobacco Research, 2015, 17, 1405. [Google Scholar] [CrossRef]
- Koob, G.F. Drug Addiction: Hyperkatifeia/Negative Reinforcement as a Framework for Medications Development. Pharmacol Rev, 2021, 73, 163–201. [Google Scholar] [CrossRef]
- Weinberger, A.H.; Desai, R.A.; McKee, S.A. Nicotine Withdrawal in U.S. Smokers with Current Mood, Anxiety, Alcohol Use, and Substance Use Disorders. Drug and Alcohol Dependence, 2010, 108, 7–12. [Google Scholar] [CrossRef]
- Zweben, J.E.; Cohen, J.B.; Christian, D.; Galloway, G.P.; Salinardi, M.; Parent, D.; Iguchi, M.; Project, M.T. Psychiatric Symptoms in Methamphetamine Users. The American Journal on Addictions, 2004, 13, 181–190. [Google Scholar] [CrossRef]
- Schellekens, A.F.A.; Jong, C.A.J. de; Buitelaar, J.K.; Verkes, R.J. Co-Morbid Anxiety Disorders Predict Early Relapse after Inpatient Alcohol Treatment. European Psychiatry, 2015, 30, 128–136. [Google Scholar] [CrossRef]
- George, O.; Ghozland, S.; Azar, M.R.; Cottone, P.; Zorrilla, E.P.; Parsons, L.H.; O’Dell, L.E.; Richardson, H.N.; Koob, G.F. CRF–CRF1 System Activation Mediates Withdrawal-Induced Increases in Nicotine Self-Administration in Nicotine-Dependent Rats. Proceedings of the National Academy of Sciences, 2007, 104, 17198–17203. [Google Scholar] [CrossRef] [PubMed]
- Mantsch, J.R. Corticotropin Releasing Factor and Drug Seeking in Substance Use Disorders: Preclinical Evidence and Translational Limitations. Addiction Neuroscience, 2022, 4, 100038. [Google Scholar] [CrossRef] [PubMed]
- Marcinkiewcz, C.A.; Prado, M.M.; Isaac, S.K.; Marshall, A.; Rylkova, D.; Bruijnzeel, A.W. Corticotropin-Releasing Factor Within the Central Nucleus of the Amygdala and the Nucleus Accumbens Shell Mediates the Negative Affective State of Nicotine Withdrawal in Rats. Neuropsychopharmacol, 2009, 34, 1743–1752. [Google Scholar] [CrossRef] [PubMed]
- Zorrilla, E.P.; Logrip, M.L.; Koob, G.F. Corticotropin Releasing Factor: A Key Role in the Neurobiology of Addiction. Frontiers in Neuroendocrinology, 2014, 35, 234–244. [Google Scholar] [CrossRef] [PubMed]
- Delfs, J.M.; Zhu, Y.; Druhan, J.P.; Aston-Jones, G. Noradrenaline in the Ventral Forebrain Is Critical for Opiate Withdrawal-Induced Aversion. Nature, 2000, 403, 430–434. [Google Scholar] [CrossRef] [PubMed]
- Haller, J. Anxiety Modulation by Cannabinoids—The Role of Stress Responses and Coping. International Journal of Molecular Sciences, 2023, 24, 15777. [Google Scholar] [CrossRef]
- Parsons, L.H.; Hurd, Y.L. Endocannabinoid Signaling in Reward and Addiction. Nature reviews. Neuroscience, 2015, 16, 579. [Google Scholar] [CrossRef]
- Ruehle, S.; Rey, A.A.; Remmers, F.; Lutz, B. The Endocannabinoid System in Anxiety, Fear Memory and Habituation. Journal of Psychopharmacology (Oxford, England), 2012, 26, 23. [Google Scholar] [CrossRef]
- Davis, M.; Whalen, P.J. The Amygdala: Vigilance and Emotion. Mol Psychiatry, 2001, 6, 13–34. [Google Scholar] [CrossRef]
- Upadhyay, J.; Verrico, C.D.; Cay, M.; Kodele, S.; Yammine, L.; Koob, G.F.; Schreiber, R. Neurocircuitry Basis of the Opioid Use Disorder–Post-Traumatic Stress Disorder Comorbid State: Conceptual Analyses Using a Dimensional Framework. The Lancet Psychiatry, 2022, 9, 84–96. [Google Scholar] [CrossRef]
- Lerman, C.; Gu, H.; Loughead, J.; Ruparel, K.; Yang, Y.; Stein, E.A. Large-Scale Brain Network Coupling Predicts Acute Nicotine Abstinence Effects on Craving and Cognitive Function. JAMA Psychiatry, 2014, 71, 523–530. [Google Scholar] [CrossRef] [PubMed]
- O’Daly, O.G.; Trick, L.; Scaife, J.; Marshall, J.; Ball, D.; Phillips, M.L.; Williams, S.S.C.; Stephens, D.N.; Duka, T. Withdrawal-Associated Increases and Decreases in Functional Neural Connectivity Associated with Altered Emotional Regulation in Alcoholism. Neuropsychopharmacology, 2012, 37, 2267–2276. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Shen, F.; Sun, X.; Zou, T.; Li, L.; Wang, X.; Deng, C.; Duan, X.; He, Z.; Yang, M.; Li, Z.; Chen, H. Dissociable Salience and Default Mode Network Modulation in Generalized Anxiety Disorder: A Connectome-Wide Association Study. Cerebral Cortex, 2023, 33, 6354–6365. [Google Scholar] [CrossRef]
- Maresh, E.L.; Allen, J.P.; Coan, J.A. Increased Default Mode Network Activity in Socially Anxious Individuals during Reward Processing. Biol Mood Anxiety Disord, 2014, 4, 7. [Google Scholar] [CrossRef]
- Viard, A.; Mutlu, J.; Chanraud, S.; Guenolé, F.; Egler, P.-J.; Gérardin, P.; Baleyte, J.-M.; Dayan, J.; Eustache, F.; Guillery-Girard, B. Altered Default Mode Network Connectivity in Adolescents with Post-Traumatic Stress Disorder. NeuroImage : Clinical, 2019, 22, 101731. [Google Scholar] [CrossRef]
- Xiong, H.; Guo, R.-J.; Shi, H.-W. Altered Default Mode Network and Salience Network Functional Connectivity in Patients with Generalized Anxiety Disorders: An ICA-Based Resting-State fMRI Study. Evidence-Based Complementary and Alternative Medicine, 2020, 2020, 4048916. [Google Scholar] [CrossRef]
- Lee, Y.J.; Guell, X.; Hubbard, N.A.; Siless, V.; Frosch, I.R.; Goncalves, M.; Lo, N.; Nair, A.; Ghosh, S.S.; Hofmann, S.G.; Auerbach, R.P.; Pizzagalli, D.A.; Yendiki, A.; Gabrieli, J.D.E.; Whitfield-Gabrieli, S.; Anteraper, S.A. Functional Alterations in Cerebellar Functional Connectivity in Anxiety Disorders. Cerebellum, 2021, 20, 392–401. [Google Scholar] [CrossRef]
- Zhang, Y.; Duan, M.; He, H. Deficient Salience and Default Mode Functional Integration in High Worry-Proneness Subject: A Connectome-Wide Association Study. Brain Imaging and Behavior, 2024. [CrossRef]
- Sutherland, M.T.; McHugh, M.; Pariyadath, V.; Stein, E.A. Resting State Functional Connectivity in Addiction: Lessons Learned and a Road Ahead. NeuroImage, 2012, 62, 2281. [Google Scholar] [CrossRef]
- Sutherland, M.T.; Stein, E.A. Functional Neurocircuits and Neuroimaging Biomarkers of Tobacco Use Disorder. Trends in Molecular Medicine, 2018, 24, 129–143. [Google Scholar] [CrossRef]
- Baur, V.; Hänggi, J.; Langer, N.; Jäncke, L. Resting-State Functional and Structural Connectivity Within an Insula–Amygdala Route Specifically Index State and Trait Anxiety. Biological Psychiatry, 2013, 73, 85–92. [Google Scholar] [CrossRef]
- Naqvi, N.H.; Bechara, A. The Insula and Drug Addiction: An Interoceptive View of Pleasure, Urges, and Decision-Making. Brain Struct Funct, 2010, 214, 435–450. [Google Scholar] [CrossRef]
- Etkin, A.; Wager, T.D. Functional Neuroimaging of Anxiety: A Meta-Analysis of Emotional Processing in PTSD, Social Anxiety Disorder, and Specific Phobia. The American Journal of Psychiatry, 2007, 164, 1476. [Google Scholar] [CrossRef]
- Rabinak, C.A.; Angstadt, M.; Welsh, R.C.; Kenndy, A.E.; Lyubkin, M.; Martis, B.; Phan, K.L. Altered Amygdala Resting-State Functional Connectivity in Post-Traumatic Stress Disorder. Front Psychiatry, 2011, 2, 62. [Google Scholar] [CrossRef]
- Roy, A.K.; Fudge, J.L.; Kelly, C.; Perry, J.S.A.; Daniele, T.; Carlisi, C.; Benson, B.; Castellanos, F.X.; Milham, M.P.; Pine, D.S.; Ernst, M. Intrinsic Functional Connectivity of Amygdala-Based Networks in Adolescent Generalized Anxiety Disorder. Journal of the American Academy of Child & Adolescent Psychiatry, 2013, 52, 290–299.e2. [Google Scholar] [CrossRef]
- Stein, M.B.; Simmons, A.N.; Feinstein, J.S.; Paulus, M.P. Increased Amygdala and Insula Activation during Emotion Processing in Anxiety-Prone Subjects. Am J Psychiatry, 2007, 164, 318–327. [Google Scholar] [CrossRef]
- Sinha, R.; Fogelman, N.; Wemm, S.; Angarita, G.; Seo, D.; Hermes, G. Alcohol Withdrawal Symptoms Predict Corticostriatal Dysfunction That Is Reversed by Prazosin Treatment in Alcohol Use Disorder. Addiction Biology, 2022, 27, e13116. [Google Scholar] [CrossRef]
- Zhao, X.-H.; Wang, P.-J.; Li, C.-B.; Hu, Z.-H.; Xi, Q.; Wu, W.-Y.; Tang, X.-W. Altered Default Mode Network Activity in Patient with Anxiety Disorders: An fMRI Study. European Journal of Radiology, 2007, 63, 373–378. [Google Scholar] [CrossRef]
- Coutinho, J.F.; Fernandesl, S.V.; Soares, J.M.; Maia, L.; Gonçalves, Ó.F.; Sampaio, A. Default Mode Network Dissociation in Depressive and Anxiety States. Brain Imaging and Behavior, 2016, 10, 147–157. [Google Scholar] [CrossRef]
- Koob, G.F.; Moal, M.L. Addiction and the Brain Antireward System. Annual Review of Psychology 2008, 59, 29–53. [Google Scholar] [CrossRef]
- Thomas, E.; Juliano, A.; Owens, M.; Cupertino, R.B.; Mackey, S.; Hermosillo, R.; Miranda-Dominguez, O.; Conan, G.; Ahmed, M.; Fair, D.A.; Graham, A.M.; Goode, N.J.; Kandjoze, U.P.; Potter, A.; Garavan, H.; Albaugh, M.D. Amygdala Connectivity Is Associated with Withdrawn/Depressed Behavior in a Large Sample of Children from the Adolescent Brain Cognitive Development (ABCD) Study®. Psychiatry Research: Neuroimaging, 2024, 344, 111877. [Google Scholar] [CrossRef]
- Yuan, M.; Liu, B.; Yang, B.; Dang, W.; Xie, H.; Lui, S.; Qiu, C.; Zhu, H.; Zhang, W. Dysfunction of Default Mode Network Characterizes Generalized Anxiety Disorder Relative to Social Anxiety Disorder and Post-Traumatic Stress Disorder. J Affect Disord, 2023, 334, 35–42. [Google Scholar] [CrossRef]
- Tao, Y.; Liu, B.; Zhang, X.; Li, J.; Qin, W.; Yu, C.; Jiang, T. The Structural Connectivity Pattern of the Default Mode Network and Its Association with Memory and Anxiety. Front. Neuroanat., 2015, 9. [Google Scholar] [CrossRef]
- Carhart-Harris, R.L.; Erritzoe, D.; Williams, T.; Stone, J.M.; Reed, L.J.; Colasanti, A.; Tyacke, R.J.; Leech, R.; Malizia, A.L.; Murphy, K.; Hobden, P.; Evans, J.; Feilding, A.; Wise, R.G.; Nutt, D.J. Neural Correlates of the Psychedelic State as Determined by fMRI Studies with Psilocybin. Proceedings of the National Academy of Sciences, 2012, 109, 2138–2143. [Google Scholar] [CrossRef]
- Moeller, S.J.; Goldstein, R.Z. Impaired Self-Awareness in Human Addiction: Deficient Attribution of Personal Relevance. Trends in Cognitive Sciences, 2014, 18, 635–641. [Google Scholar] [CrossRef]
- Volkow, N.D.; Morales, M. The Brain on Drugs: From Reward to Addiction. Cell, 2015, 162, 712–725. [Google Scholar] [CrossRef]
- Killingsworth, M.A.; Gilbert, D.T. A Wandering Mind Is an Unhappy Mind. Science, 2010, 330, 932–932. [Google Scholar] [CrossRef]
- Xu, X.; Yuan, H.; Lei, X. Activation and Connectivity within the Default Mode Network Contribute Independently to Future-Oriented Thought. Sci Rep, 2016, 6, 21001. [Google Scholar] [CrossRef]
- Li, Q.; Li, Z.; Li, W.; Zhang, Y.; Wang, Y.; Zhu, J.; Chen, J.; Li, Y.; Yan, X.; Ye, J.; Li, L.; Wang, W.; Liu, Y. Disrupted Default Mode Network and Basal Craving in Male Heroin-Dependent Individuals: A Resting-State fMRI Study. J Clin Psychiatry, 2016, 77, 4560. [Google Scholar] [CrossRef]
- Zhu, X.; Cortes, C.R.; Mathur, K.; Tomasi, D.; Momenan, R. Model-Free Functional Connectivity and Impulsivity Correlates of Alcohol Dependence: A Resting-State Study. Addiction Biology, 2017, 22, 206–217. [Google Scholar] [CrossRef]
- Koob, G.F.; Volkow, N.D. Neurobiology of Addiction: A Neurocircuitry Analysis. The Lancet Psychiatry, 2016, 3, 760–773. [Google Scholar] [CrossRef]
- Davis, M.; Walker, D.L.; Miles, L.; Grillon, C. Phasic vs. Sustained Fear in Rats and Humans: Role of the Extended Amygdala in Fear vs. Anxiety. Neuropsychopharmacol, 2010, 35, 105–135. [Google Scholar] [CrossRef]
- Flook, E.A.; Feola, B.; Benningfield, M.M.; Silveri, M.M.; Winder, D.G.; Blackford, J.U. Alterations in BNST Intrinsic Functional Connectivity in Early Abstinence from Alcohol Use Disorder. Alcohol Alcohol, 2023, 58, 298–307. [Google Scholar] [CrossRef]
- Alvarez, R.P.; Chen, G.; Bodurka, J.; Kaplan, R.; Grillon, C. Phasic and Sustained Fear in Humans Elicits Distinct Patterns of Brain Activity. Neuroimage, 2011, 55, 389–400. [Google Scholar] [CrossRef]
- Choi, J.M.; Padmala, S.; Pessoa, L. Impact of State Anxiety on the Interaction between Threat Monitoring and Cognition. NeuroImage, 2012, 59, 1912–1923. [Google Scholar] [CrossRef]
- Klumpers, F.; Kroes, M.C.; Heitland, I.; Everaerd, D.; Akkermans, S.E.A.; Oosting, R.S.; van Wingen, G.; Franke, B.; Kenemans, J.L.; Fernández, G.; Baas, J.M.P. Dorsomedial Prefrontal Cortex Mediates the Impact of Serotonin Transporter Linked Polymorphic Region Genotype on Anticipatory Threat Reactions. Biological Psychiatry, 2015, 78, 582–589. [Google Scholar] [CrossRef]
- McMenamin, B.W.; Langeslag, S.J.E.; Sirbu, M.; Padmala, S.; Pessoa, L. Network Organization Unfolds over Time during Periods of Anxious Anticipation. J Neurosci, 2014, 34, 11261–11273. [Google Scholar] [CrossRef]
- Giancola, P.R.; Tarter, R.E. Executive Cognitive Functioning and Risk for Substance Abuse. Psychol Sci, 1999, 10, 203–205. [Google Scholar] [CrossRef]
- Kim-Spoon, J.; Kahn, R.E.; Lauharatanahirun, N.; Deater-Deckard, K.; Bickel, W.K.; Chiu, P.H.; King-Casas, B. Executive Functioning and Substance Use in Adolescence: Neurobiological and Behavioral Perspectives. Neuropsychologia, 2017, 100, 79. [Google Scholar] [CrossRef]
- Young, S.E.; Friedman, N.P.; Miyake, A.; Willcutt, E.G.; Corley, R.P.; Haberstick, B.C.; Hewitt, J.K. Behavioral Disinhibition: Liability for Externalizing Spectrum Disorders and Its Genetic and Environmental Relation to Response Inhibition across Adolescence. Journal of Abnormal Psychology, 2009, 118, 117–130. [Google Scholar] [CrossRef]
- DiGirolamo, G.J.; Smelson, D.; Guevremont, N. Cue-Induced Craving in Patients with Cocaine Use Disorder Predicts Cognitive Control Deficits toward Cocaine Cues. Addictive Behaviors, 2015, 47, 86–90. [Google Scholar] [CrossRef]
- Su, B.; Li, S.; Yang, L.; Zheng, M. Reduced Response Inhibition after Exposure to Drug-Related Cues in Male Heroin Abstainers. Psychopharmacology, 2020, 237, 1055–1062. [Google Scholar] [CrossRef]
- Fatseas, M.; Serre, F.; Swendsen, J.; Auriacombe, M. Effects of Anxiety and Mood Disorders on Craving and Substance Use among Patients with Substance Use Disorder: An Ecological Momentary Assessment Study. Drug and Alcohol Dependence, 2018, 187, 242–248. [Google Scholar] [CrossRef]
- Sinha, R.; Fox, H.C.; Hong, K.A.; Hansen, J.; Tuit, K.; Kreek, M.J. Effects of Adrenal Sensitivity, Stress- and Cue-Induced Craving, and Anxiety on Subsequent Alcohol Relapse and Treatment Outcomes. Archives of General Psychiatry, 2011, 68, 942–952. [Google Scholar] [CrossRef]
- Haber, S.N. Corticostriatal Circuitry. Dialogues in Clinical Neuroscience, 2016, 18, 7. [Google Scholar] [CrossRef]
- Bamford, N.S.; Zhang, H.; Joyce, J.A.; Scarlis, C.A.; Hanan, W.; Wu, N.-P.; André, V.M.; Cohen, R.; Cepeda, C.; Levine, M.S.; Harleton, E.; Sulzer, D. Repeated Exposure to Methamphetamine Causes Long-Lasting Presynaptic Corticostriatal Depression That Is Renormalized with Drug Readministration. Neuron, 2008, 58, 89–103. [Google Scholar] [CrossRef]
- Martin, M.; Chen, B.T.; Hopf, F.W.; Bowers, M.S.; Bonci, A. Cocaine Self-Administration Selectively Abolishes LTD in the Core of the Nucleus Accumbens. Nat Neurosci, 2006, 9, 868–869. [Google Scholar] [CrossRef]
- Moussawi, K.; Pacchioni, A.; Moran, M.; Olive, M.F.; Gass, J.T.; Lavin, A.; Kalivas, P.W. N-Acetylcysteine Reverses Cocaine-Induced Metaplasticity. Nat Neurosci, 2009, 12, 182–189. [Google Scholar] [CrossRef]
- LaRowe, S.D.; Myrick, H.; Hedden, S.; Mardikian, P.; Saladin, M.; McRae, A.; Brady, K.; Kalivas, P.W.; Malcolm, R. Is Cocaine Desire Reduced by N -Acetylcysteine? AJP, 2007, 164, 1115–1117. [Google Scholar] [CrossRef]
- Sawaguchi, T.; Goldman-Rakic, P.S. D1 Dopamine Receptors in Prefrontal Cortex: Involvement in Working Memory. Science, 1991, 251, 947–950. [Google Scholar] [CrossRef]
- Sawaguchi, T.; Goldman-Rakic, P.S. The Role of D1-Dopamine Receptor in Working Memory: Local Injections of Dopamine Antagonists into the Prefrontal Cortex of Rhesus Monkeys Performing an Oculomotor Delayed-Response Task. J Neurophysiol, 1994, 71, 515–528. [Google Scholar] [CrossRef]
- Williams, G.V.; Goldman-Rakic, P.S. Modulation of Memory Fields by Dopamine D1 Receptors in Prefrontal Cortex. Nature, 1995, 376, 572–575. [Google Scholar] [CrossRef]
- Puig, M.V.; Miller, E.K. The Role of Prefrontal Dopamine D1 Receptors in the Neural Mechanisms of Associative Learning. Neuron, 2012, 74, 10.1016/j.neuron.2012.04.018. [Google Scholar] [CrossRef]
- Müller, U.; Cramon, D.Y. von; Pollmann, S. D1- Versus D2-Receptor Modulation of Visuospatial Working Memory in Humans. The Journal of Neuroscience, 1998, 18, 2720. [Google Scholar] [CrossRef]
- Verharen, J.P.H.; Adan, R.A.H.; Vanderschuren, L.J.M.J. Differential Contributions of Striatal Dopamine D1 and D2 Receptors to Component Processes of Value-Based Decision Making. Neuropsychopharmacology, 2019, 44, 2195. [Google Scholar] [CrossRef]
- Sala-Bayo, J.; Fiddian, L.; Nilsson, S.R.O.; Hervig, M.E.; McKenzie, C.; Mareschi, A.; Boulos, M.; Zhukovsky, P.; Nicholson, J.; Dalley, J.W.; Alsiö, J.; Robbins, T.W. Dorsal and Ventral Striatal Dopamine D1 and D2 Receptors Differentially Modulate Distinct Phases of Serial Visual Reversal Learning. Neuropsychopharmacol., 2020, 45, 736–744. [Google Scholar] [CrossRef]
- Soares-Cunha, C.; Coimbra, B.; Sousa, N.; Rodrigues, A.J. Reappraising Striatal D1- and D2-Neurons in Reward and Aversion. Neuroscience & Biobehavioral Reviews, 2016, 68, 370–386. [Google Scholar] [CrossRef]
- Barker, J.M.; Torregrossa, M.M.; Taylor, J.R. Bidirectional Modulation of Infralimbic Dopamine D1 and D2 Receptor Activity Regulates Flexible Reward Seeking. Frontiers in Neuroscience, 2013, 7, 126. [Google Scholar] [CrossRef]
- Koob, G.F.; Volkow, N.D. Neurocircuitry of Addiction. Neuropsychopharmacol, 2010, 35, 217–238. [Google Scholar] [CrossRef]
- Goudriaan, A.E.; De Ruiter, M.B.; Van Den Brink, W.; Oosterlaan, J.; Veltman, D.J. Brain Activation Patterns Associated with Cue Reactivity and Craving in Abstinent Problem Gamblers, Heavy Smokers and Healthy Controls: An fMRI Study. Addiction Biology, 2010, 15, 491–503. [Google Scholar] [CrossRef]
- Liu, J.; Shi, Z.; Fabbricatore, J.L.; McMains, J.T.; Worsdale, A.; Jones, E.C.; Wang, Y.; Sweet, L.H. Vaping and Smoking Cue Reactivity in Young Adult Non-Smoking Electronic Cigarette Users: A Functional Neuroimaging Study. Nicotine and Tobacco Research, 2024, ntae257. [CrossRef]
- Schacht, J.P.; Anton, R.F.; Myrick, H. Functional Neuroimaging Studies of Alcohol Cue Reactivity: A Quantitative Meta-analysis and Systematic Review. Addiction Biology, 2013, 18, 121–133. [Google Scholar] [CrossRef]
- Sehl, H.; Terrett, G.; Greenwood, L.-M.; Kowalczyk, M.; Thomson, H.; Poudel, G.; Manning, V.; Lorenzetti, V. Patterns of Brain Function Associated with Cannabis Cue-Reactivity in Regular Cannabis Users: A Systematic Review of fMRI Studies. Psychopharmacology, 2021, 238, 2709–2728. [Google Scholar] [CrossRef]
- Park, J.; Moghaddam, B. Impact of Anxiety on Prefrontal Cortex Encoding of Cognitive Flexibility. Neuroscience, 2017, 345, 193–202. [Google Scholar] [CrossRef]
- Bishop, S.J. Trait Anxiety and Impoverished Prefrontal Control of Attention. Nat Neurosci, 2009, 12, 92–98. [Google Scholar] [CrossRef]
- Bijsterbosch, J.; Smith, S.; Bishop, S.J. Functional Connectivity under Anticipation of Shock: Correlates of Trait Anxious Affect versus Induced Anxiety. Journal of Cognitive Neuroscience, 2015, 27, 1840–1853. [Google Scholar] [CrossRef]
- Makovac, E.; Mancini, M.; Fagioli, S.; Watson, D.R.; Meeten, F.; Rae, C.L.; Critchley, H.D.; Ottaviani, C. Network Abnormalities in Generalized Anxiety Pervade beyond the Amygdala-Pre-Frontal Cortex Circuit: Insights from Graph Theory. Psychiatry Research: Neuroimaging, 2018, 281, 107–116. [Google Scholar] [CrossRef]
- Vytal, K.E.; Overstreet, C.; Charney, D.R.; Robinson, O.J.; Grillon, C. Sustained Anxiety Increases Amygdala–Dorsomedial Prefrontal Coupling: A Mechanism for Maintaining an Anxious State in Healthy Adults. jpn, 2014, 39, 321–329. [Google Scholar] [CrossRef]
- Wang, M.; Cao, L.; Li, H.; Xiao, H.; Ma, Y.; Liu, S.; Zhu, H.; Yuan, M.; Qiu, C.; Huang, X. Dysfunction of Resting-State Functional Connectivity of Amygdala Subregions in Drug-Naïve Patients With Generalized Anxiety Disorder. Front. Psychiatry, 2021, 12. [Google Scholar] [CrossRef]
- Zhang, R.; Chen, Z.; Hu, B.; Zhou, F.; Feng, T. The Anxiety-Specific Hippocampus-Prefrontal Cortex Pathways Links to Procrastination through Self-Control. Hum Brain Mapp, 2022, 43, 1738–1748. [Google Scholar] [CrossRef]
- Li, C.R.; Chao, H.H.-A.; Lee, T.-W. Neural Correlates of Speeded as Compared with Delayed Responses in a Stop Signal Task: An Indirect Analog of Risk Taking and Association with an Anxiety Trait. Cerebral Cortex, 2009, 19, 839–848. [Google Scholar] [CrossRef]
- Li, C.R.; Morgan, P.T.; Matuskey, D.; Abdelghany, O.; Luo, X.; Chang, J.L.K.; Rounsaville, B.J.; Ding, Y.; Malison, R.T. Biological Markers of the Effects of Intravenous Methylphenidate on Improving Inhibitory Control in Cocaine-Dependent Patients. Proceedings of the National Academy of Sciences, 2010, 107, 14455–14459. [Google Scholar] [CrossRef]
- Naqvi, N.H.; Bechara, A. The Hidden Island of Addiction: The Insula. Trends in Neurosciences, 2009, 32, 56–67. [Google Scholar] [CrossRef]
- Verdejo-Garcia, A.; Clark, L.; Dunn, B.D. The Role of Interoception in Addiction: A Critical Review. Neuroscience & Biobehavioral Reviews, 2012, 36, 1857–1869. [Google Scholar] [CrossRef]
- Schmidt, A.F.; Eulenbruch, T.; Langer, C.; Banger, M. Interoceptive Awareness, Tension Reduction Expectancies and Self-Reported Drinking Behavior. Alcohol and Alcoholism, 2013, 48, 472–477. [Google Scholar] [CrossRef]
- Herman, A.M. Interoception Within the Context of Impulsivity and Addiction. Current Addiction Reports, 2023, 10, 97. [Google Scholar] [CrossRef]
- Brody, A.L.; Mandelkern, M.A.; London, E.D.; Childress, A.R.; Lee, G.S.; Bota, R.G.; Ho, M.L.; Saxena, S.; Baxter, L.R., Jr; Madsen, D.; Jarvik, M.E. Brain Metabolic Changes During Cigarette Craving. Archives of General Psychiatry, 2002, 59, 1162–1172. [Google Scholar] [CrossRef]
- Kilts, C.D.; Schweitzer, J.B.; Quinn, C.K.; Gross, R.E.; Faber, T.L.; Muhammad, F.; Ely, T.D.; Hoffman, J.M.; Drexler, K.P.G. Neural Activity Related to Drug Craving in Cocaine Addiction. Archives of General Psychiatry, 2001, 58, 334–341. [Google Scholar] [CrossRef]
- Myrick, H.; Anton, R.F.; Li, X.; Henderson, S.; Drobes, D.; Voronin, K.; George, M.S. Differential Brain Activity in Alcoholics and Social Drinkers to Alcohol Cues: Relationship to Craving. Neuropsychopharmacology, 2004, 29, 393–402. [Google Scholar] [CrossRef]
- Wang, Z.; Faith, M.; Patterson, F.; Tang, K.; Kerrin, K.; Wileyto, E.P.; Detre, J.A.; Lerman, C. Neural Substrates of Abstinence-Induced Cigarette Cravings in Chronic Smokers. Journal of Neuroscience, 2007, 27, 14035–14040. [Google Scholar] [CrossRef]
- Joutsa, J.; Moussawi, K.; Siddiqi, S.H.; Abdolahi, A.; Drew, W.; Cohen, A.L.; Ross, T.J.; Deshpande, H.U.; Wang, H.Z.; Bruss, J.; Stein, E.A.; Volkow, N.D.; Grafman, J.H.; van Wijngaarden, E.; Boes, A.D.; Fox, M.D. Brain Lesions Disrupting Addiction Map to a Common Human Brain Circuit. Nat Med, 2022, 28, 1249–1255. [Google Scholar] [CrossRef]
- Naqvi, N.H.; Rudrauf, D.; Damasio, H.; Bechara, A. Damage to the Insula Disrupts Addiction to Cigarette Smoking. Science, 2007, 315, 531–534. [Google Scholar] [CrossRef]
- Huang, Y.; Mohan, A.; De Ridder, D.; Sunaert, S.; Vanneste, S. The Neural Correlates of the Unified Percept of Alcohol-Related Craving: A fMRI and EEG Study. Sci Rep, 2018, 8, 923. [Google Scholar] [CrossRef]
- Harrison, O.K.; Köchli, L.; Marino, S.; Luechinger, R.; Hennel, F.; Brand, K.; Hess, A.J.; Frässle, S.; Iglesias, S.; Vinckier, F.; Petzschner, F.H.; Harrison, S.J.; Stephan, K.E. Interoception of Breathing and Its Relationship with Anxiety. Neuron, 2021, 109, 4080–4093.e8. [Google Scholar] [CrossRef]
- Paulus, M.P.; Stein, M.B. An Insular View of Anxiety. Biological Psychiatry, 2006, 60, 383–387. [Google Scholar] [CrossRef]
- Tan, Y.; Wei, D.; Zhang, M.; Yang, J.; Jelinčić, V.; Qiu, J. The Role of Mid-Insula in the Relationship between Cardiac Interoceptive Attention and Anxiety: Evidence from an fMRI Study. Sci Rep, 2018, 8, 17280. [Google Scholar] [CrossRef]
- Alvarez, R.P.; Kirlic, N.; Misaki, M.; Bodurka, J.; Rhudy, J.L.; Paulus, M.P.; Drevets, W.C. Increased Anterior Insula Activity in Anxious Individuals Is Linked to Diminished Perceived Control. Transl Psychiatry, 2015, 5, e591–e591. [Google Scholar] [CrossRef]
- Pang, J.; Tang, X.; Li, H.; Hu, Q.; Cui, H.; Zhang, L.; Li, W.; Zhu, Z.; Wang, J.; Li, C. Altered Interoceptive Processing in Generalized Anxiety Disorder—A Heartbeat-Evoked Potential Research. Frontiers in Psychiatry, 2019, 10, 616. [Google Scholar] [CrossRef]
- Herman, A.M.; Duka, T. Facets of Impulsivity and Alcohol Use: What Role Do Emotions Play? Neuroscience & Biobehavioral Reviews, 2019, 106, 202–216. [Google Scholar] [CrossRef]
- Herman, A.M.; Duka, T. The Role of Impulsivity Facets on the Incidence and Development of Alcohol Use Disorders. In Recent Advances in Research on Impulsivity and Impulsive Behaviors; de Wit, H., Jentsch, J.D., Eds.; Springer International Publishing: Cham, 2020; pp. 197–221. [Google Scholar] [CrossRef]
- Seth, A.K.; Friston, K.J. Active Interoceptive Inference and the Emotional Brain. Philosophical Transactions of the Royal Society B: Biological Sciences, 2016, 371, 20160007. [Google Scholar] [CrossRef]
- lifesciencedb. Human Brain (Hypothalamus=red, Amygdala=green, Hippocampus/Fornix=blue, Pons=gold, Pituitary Gland=pink; 2011.
- Tolomeo, S.; Baldacchino, A.; Volkow, N.D.; Steele, J.D. Protracted Abstinence in Males with an Opioid Use Disorder: Partial Recovery of Nucleus Accumbens Function. Transl Psychiatry, 2022, 12, 81. [Google Scholar] [CrossRef]
- Volkow, N.D.; Chang, L.; Wang, G.-J.; Fowler, J.S.; Franceschi, D.; Sedler, M.; Gatley, S.J.; Miller, E.; Hitzemann, R.; Ding, Y.-S.; Logan, J. Loss of Dopamine Transporters in Methamphetamine Abusers Recovers with Protracted Abstinence. J. Neurosci., 2001, 21, 9414–9418. [Google Scholar] [CrossRef]
- Laine, T.P.J.; Ahonen, A.; Torniainen, P.; Heikkilä, J.; Pyhtinen, J.; Räsänen, P.; Niemelä, O.; Hillbom, M. Dopamine Transporters Increase in Human Brain after Alcohol Withdrawal. Mol Psychiatry, 1999, 4, 189–191. [Google Scholar] [CrossRef] [PubMed]
- Schrammen, E.; Roesmann, K.; Rosenbaum, D.; Redlich, R.; Harenbrock, J.; Dannlowski, U.; Leehr, E.J. Functional Neural Changes Associated with Psychotherapy in Anxiety Disorders – A Meta-Analysis of Longitudinal fMRI Studies. Neuroscience & Biobehavioral Reviews, 2022, 142, 104895. [Google Scholar] [CrossRef]
- Månsson, K.N.T.; Salami, A.; Frick, A.; Carlbring, P.; Andersson, G.; Furmark, T.; Boraxbekk, C.-J. Neuroplasticity in Response to Cognitive Behavior Therapy for Social Anxiety Disorder. Transl Psychiatry, 2016, 6, e727–e727. [Google Scholar] [CrossRef] [PubMed]
- Holzschneider, K.; Mulert, C. Neuroimaging in Anxiety Disorders. Dialogues in Clinical Neuroscience, 2011, 13, 453. [Google Scholar] [CrossRef] [PubMed]
- Dickie, E.W.; Brunet, A.; Akerib, V.; Armony, J.L. An fMRI Investigation of Memory Encoding in PTSD: Influence of Symptom Severity. Neuropsychologia, 2008, 46, 1522–1531. [Google Scholar] [CrossRef]
Figure 1.
Conceptualizing the comorbidity between addiction neurocircuitry domains and anxiety using task-based and resting state fMRI neuroimaging findings. Anxiety leading to binge/intoxication (positive valence) is associated with increased vs. activity and decreased AMYG activity while binge/intoxication leading to anxiety is associated with increased PFC and vs. activity. Bidirectional anxiety and withdrawal/negative affect is associated with increased SN-DMN, AMYG-INS, and AMYG-BNST connectivity, and increased posterior DMN activity. Anxiety leading to preoccupation/anticipation (cognitive) is associated with increased PFC activity and increased AMYG-vmPFC connectivity while preoccupation/anticipation (cognitive) leading to anxiety is associated with increased vmPFC and AMYG activity, and increased AMYG-vmPFC connectivity. Colored arrows depict the associated mental health condition (red = anxiety, blue = SUD, and purple = both). vs. = ventral striatum. AMYG = amygdala. PFC = prefrontal cortex. vmPFC = ventromedial prefrontal cortex. INS = insula. BNST = bed nucleus of the stria terminalis. SN = salience network. DMN = default mode network. Limbic brain image is open access, modified from lifesciencedb [158].
Figure 1.
Conceptualizing the comorbidity between addiction neurocircuitry domains and anxiety using task-based and resting state fMRI neuroimaging findings. Anxiety leading to binge/intoxication (positive valence) is associated with increased vs. activity and decreased AMYG activity while binge/intoxication leading to anxiety is associated with increased PFC and vs. activity. Bidirectional anxiety and withdrawal/negative affect is associated with increased SN-DMN, AMYG-INS, and AMYG-BNST connectivity, and increased posterior DMN activity. Anxiety leading to preoccupation/anticipation (cognitive) is associated with increased PFC activity and increased AMYG-vmPFC connectivity while preoccupation/anticipation (cognitive) leading to anxiety is associated with increased vmPFC and AMYG activity, and increased AMYG-vmPFC connectivity. Colored arrows depict the associated mental health condition (red = anxiety, blue = SUD, and purple = both). vs. = ventral striatum. AMYG = amygdala. PFC = prefrontal cortex. vmPFC = ventromedial prefrontal cortex. INS = insula. BNST = bed nucleus of the stria terminalis. SN = salience network. DMN = default mode network. Limbic brain image is open access, modified from lifesciencedb [158].
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



