
Submitted:
04 December 2024
Posted:
05 December 2024
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Recent studies indicate that nurses experienced higher levels of occupational burnout and insomnia during the pandemic compared to other healthcare professionals. The aim of this study was to assess occupational burnout, insomnia, and psychological resilience and to explore their interrelations among nurses in Greece in the post-pandemic era. The study was conducted online in July 2024 and included 380 nurses currently working in Greek hospitals, who completed the Copenhagen Burnout Inventory (CBI), the Athens Insomnia Scale (AIS), and the Brief Resilience Scale (BRS). Overall, 56.1% of the nurses exhibited insomnia symptoms and 46.8% displayed signs of occupational burnout. Low resilience scores were observed in 26.3%. Female nurses had a higher mean burnout score compared to their male counterparts. Multiple regression analysis indicated that CBI Total explained 34.4% of the variance in the AIS scores, with an additional 3% explained by BRS. Mediation analysis further revealed that resilience operates protectively as a negative mediator in the relationship between burnout and insomnia. In conclusion, the levels of occupational burnout and insomnia among nurses remain high one year after the end of the pandemic and consequently there is an urgent need to enhance the support for nurses to protect them from adverse physical and psychological effects.
Keywords:
occupational burnout
; insomnia
; psychological resilience
; post-COVID era
; nurses
1. Introduction
A multitude of recent studies have highlighted that the COVID-19 pandemic led to unprecedented stress among healthcare professionals [1,2,3,4,5,6], exacerbating their already burdened mental health [7]. The long-term psychological impacts remain uncertain [3]. Specifically, contemporary research evidenced that nursing staff were particularly vulnerable to developing physical and psychological issues, experiencing higher levels of occupational burnout and insomnia compared to other healthcare professionals [8,9]. This vulnerability might be largely attributed to the unique working conditions of nurses, whose profession involves high and complex physical and psychological demands [10], such as excessive workload, frequent shift work, and exposure to actual death [10].
Occupational burnout is described as a workplace phenomenon, which manifests itself as a syndrome linked to emotional and cognitive changes, including emotional exhaustion, depersonalization or cynicism, and reduced personal efficacy due to chronic work-related stress [11]. According to Maslach and Jackson, burnout is defined as a response to chronic and long-term workplace stress, characterized by three dimensions: emotional exhaustion, depersonalization, and diminished personal accomplishment [12]. Schaufeli and Greenglass further defined it as a state of physical, emotional, and mental exhaustion resulting from prolonged involvement in emotionally demanding work situations [13]. Burnout can adversely affect the sleep quality of nursing staff and has been recognized as a cause of insomnia [14]. Nursing work involves certain characteristics that may increase sleep problems and trigger excessive adrenaline release [15]. Nurses often work rotating shifts, which can disrupt circadian rhythms [16,17] and affect sleep quality [18]. These factors can increase sleep onset latency, prolong the persistence of insomnia, and decrease overall sleep quality and duration [19,20].
Sleep is essential for life and significantly contributes to health maintenance and well-being. According to the literature, 7–9 hours of sleep are recommended to support optimal adult health [21]. Therefore, it is crucial to examine the relationship between occupational burnout and sleep problems in nurses [15]. From a different perspective, psychological resilience may serve as a protective mechanism against the adverse effects of nursing work [22]. Due to the nature of their work, nurses encounter challenges that can undermine their resilience [23]. Resilience is defined as the ability to recover from adversity and overcome difficult life circumstances or, alternatively, as a process of adapting to adversity [24,25]. Studies have evidenced that psychological resilience effectively shields healthcare professionals against stress, depression, psychological distress, and burnout [23,26,27]. Furthermore, recent studies have observed an inverse relationship between resilience and insomnia [28,29]. Research conducted during the pandemic demonstrated that healthcare professionals with high resilience levels were better adjusted to recover and withstand psychological strain compared to their less resilient counterparts [26,30,31]. However, since psychological resilience is a dynamic process, certain factors may weaken it and influence coping strategies [26,30,31].
This study was conducted 14 months after the end of the pandemic crisis, which the World Health Organization declared on 5 May 2023 [28]. We considered this period sufficient for the extreme negative emotions and adverse professional experiences faced by nurses during the pandemic, to subside. A literature review did not find any studies that described the psychological state of nurses one year after the official ending of the pandemic. Therefore, this study aimed to assess the levels and investigate the interrelations among occupational burnout, insomnia, and psychological resilience in nurses working in Greek hospitals under regular conditions. Also, based on the theoretical framework that enhanced psychological resilience may counteract the harmful effects of burnout on insomnia, we sought to confirm the following research hypotheses:
Hypothesis 1: burnout is positively associated with and predicts insomnia.
Hypothesis 2: resilience is negatively related to and predicts insomnia.
Hypothesis 3: resilience serves as a negative mediator in the association between burnout and insomnia.
2. Materials and Methods
2.1. Research Design
This was a cross-sectional study involving nurses working in Greek hospitals. Inclusion criteria for the study population were set as a minimum of one year of professional experience. Data collection was performed via self-report questionnaires distributed through email addresses retrieved from scientific and professional registries of Greek nurses. The email invitation contained an anonymous link granting access to the GoogleTM Forms online research platform. Acceptance of participation, as stated on the first page of the online questionnaire, was considered informed consent. The study sample comprised nurses who agreed to participate and responded to the email (convenience sampling).
2.2. Study Participants
The study was conducted in July 2024. To calculate the sample size, with a target population of 27,103 individuals, a confidence level of 95%, a confidence interval of 5%, and an assumption of a 50% response rate, a minimum sample size of 379 participants was required [32,33,34,35]. A total of 500 invitations were emailed, with 380 responses received (response rate: 76%).
2.3. Ethical Considerations
The study was conducted following ethical principles outlined in the General Data Protection Regulation (GDPR - 2016/679) of the European Union, the World Medical Association Declaration of Helsinki (1975, revised 2008), and the guidelines of the International Committee of Medical Journal Editors. The study protocol was approved by the Ethics Committee of Clinical Research of the General Hospital for Thoracic Diseases of Athens “SOTIRIA” (Approval Number: 20649/23).
2.4. Measurement Tools
Before completing the questionnaires, participants provided demographic and professional information, including gender, age, education level, and years of work experience.
2.4.1. Copenhagen Burnout Inventory (CBI)
The Copenhagen Burnout Inventory (CBI) is a tool designed to measure personal and work-related burnout, consisting of 19 items. Responses include options like “always,” “often,” “sometimes,” “rarely,” and “never/almost never,” or “to a very high degree,” “to a high degree,” “somewhat,” “to a low degree,” and “to a very low degree.” Response options are coded into scores of 100, 75, 50, 0. The possible scoring range for burnout scales is 0-100, with higher scores indicating higher levels of occupational burnout [36,37,38]. The scale comprises three subscales:
[i]. Personal burnout: Assesses the degree of physical and psychological burnout experienced by the individual (questions 1–6). It refers to both physical and psychological burnout accumulated during the day (e.g., “How often do you feel weak and/or vulnerable to illness?”).
[ii]. Work-related burnout: Evaluates the perceived physical and psychological burnout related to work (questions 7–13). It describes burnout associated with the job (e.g., “Do you feel every hour at work is exhausting?”).
[iii]. Patient-related burnout: Assesses perceived physical and psychological burnout from interaction with patients (questions 14–19). It reflects burnout resulting from interpersonal relationships with patients (e.g., “Do you feel frustrated working with patients?”) [36,37,38].
In this study, the Greek version of the CBI, which is a valid scale with good psychometric properties, was used. In the reliability analysis, Cronbach’s alpha exceeded 0.7 for all subscales, indicating a high level of internal consistency [39]. The Cronbach’s alpha coefficient for the entire scale in this study was α = 0.933. A total score of ≥50 [37,38,40,41,42,43,44,45,46] indicates professional burnout.
2.4.2. Athens Insomnia Scale (AIS)
The Athens Insomnia Scale (AIS) is a self-assessment psychometric tool designed to measure sleep difficulty based on the 10th Revision of the International Classification of Diseases and Related Health Problems (ICD-10). The AIS comprises eight items, with the first five assessing sleep induction (time needed to fall asleep), awakenings during the night, final awakening, total sleep duration, and overall sleep quality. The final three items assess well-being, functioning, and sleepiness during the day. Each item is scored from 0 to 3. A total score of 0 to 24 is possible, with higher scores indicating greater severity of insomnia. A score of 6 or above indicates insomnia [47]. The AIS is a widely used tool for assessing insomnia. The Greek version of the AIS has demonstrated good psychometric properties [48,49]. Cronbach's alpha in this study was measured at α = 0.878.
2.4.3. Brief Resilience Scale (BRS)
The Brief Resilience Scale (BRS) is a tool designed to measure resilience. It comprises six items (three positive and three negative), with responses on a 5-point Likert scale (ranging from “strongly disagree” to “strongly agree”). The positive questions assess the ability to recover from adverse situations (e.g., “I tend to bounce back quickly after hard times”), while the negative questions assess difficulties in overcoming adverse events (e.g., “It is hard for me to snap back when something bad happens”). The total BRS score is calculated by summing the scores of the six items and dividing by the number of responses. Possible scores range from 1 to 5, with higher scores indicating greater resilience [50,51]. Low scores range from 1.00 to 2.99, medium scores from 3.00 to 4.30, and high scores from 4.31 to 5.00 [51]. The BRS has shown high reliability and validity and is frequently used in studies with healthcare professionals [52]. The Greek version of the BRS has been validated, demonstrating high reliability and validity in measuring resilience [51]. Cronbach’s alpha in this study was measured at α = 0.875.
2.5. Statistical Analysis
Descriptive statistical methods were employed to estimate means and standard deviations for continuous variables. Subsequently, we examined the representativeness of the sample using t-tests and χ2 tests, comparing the sample with the general population of nurses in Greece in terms of years of professional experience, age, and gender. We assessed the presence of gender differences as to the study variables using t-tests. Correlations were investigated using Pearson's correlation test. Linear regression analysis was utilized to determine if the correlated variables were significant predictors of insomnia. Before proceeding with the regression, linearity was confirmed through visual inspection of scatter plot pairs, normality was checked using P-P plots, and homoscedasticity was verified through a residual scatterplot. The Durbin-Watson test was employed to assess the independence of residuals, while the absence of multicollinearity in the data was examined using Variance Inflation Factor (VIF) analysis. Mediation analysis was conducted using Hayes' SPSS Process Macro Model 4. In the mediation analysis, the outcome variable was AIS, the mediator variable was BRS, and the predictor variable was CBI (total). For all statistical analyses, statistical significance was set at p < 0.05 (two-tailed).
3. Results
The study included 74 male and 306 female nurses. No statistically significant differences were observed between the study sample and the overall population of nurses working in Greece regarding gender, age, and years of professional experience [32]. In the sample, 56.1% showed symptoms of insomnia (AIS ≥ 6), while 46.8% exhibited signs of burnout (CBI Total ≥ 50). Low resilience scores were seen in 26.3% of the sample (BRS ≤ 2.99), while high scores were observed in 16.6% (BRS ≥ 4.31). Table 1 presents the mean values and standard deviations of the study variables.
The study sample showed a higher mean insomnia score compared to a study of the same population conducted in May 2020 (t-test p < 0.001, 7.12 ± 4.24 vs. 5.98 ± 4.24, Hedges' g: 0.27) [52]. Although burnout showed some increase, it did not differ statistically (t-test p > 0.05, 48.72 ± 18.89 vs. 46.95 ± 18.75) compared to a study conducted among Greek nurses in February 2021 using the same method [37]. Resilience showed a statistically significant decrease (t-test p < 0.01, 3.43 ± 0.83 vs. 3.61 ± 0.8, Hedges' g: 0.22) compared to a study conducted in June 2020 [26].
Regarding gender, female nurses had a higher mean burnout score compared to male nurses (t-test p < 0.05, 49.64 ± 19.03 vs. 44.91 ± 17.39, Table 1). Additionally, female nurses showed higher scores in both personal burnout and work-related burnout (Table 1).
AIS negatively correlated with BRS and positively correlated with CBI total, as well as with its three subscales. BRS showed a negative correlation with both the CBI total and its subscales. As expected, the three CBI subscales positively correlated with each other (Pearson Correlations p < 0.01, Table 2).
Before proceeding to regression analysis, we checked if the necessary assumptions for regression analysis were met. Independence of residuals was tested using the Durbin-Watson test, with a value of 1.92 (Table 3), supporting the absence of autocorrelation. The VIF value of 1.264, less than 4, indicated a lack of multicollinearity (Table 3). Normality was verified by visual inspection of the predicted probability plots. Homoscedasticity was examined through visual inspection of the scatter plot of standardized and predicted residual values. Linearity was confirmed by visually inspecting scatter plots of variable pairs.
We conducted a multiple regression analysis using the Stepwise method to explore which factors best explain the scores of the Athens Insomnia Scale (AIS). In the multiple regression, AIS was set as the dependent variable, while age, gender, years of work experience, the Copenhagen Burnout Inventory (CBI Total), and the Brief Resilience Scale (BRS) were set as independent variables. The analysis showed that CBI Total explained 34.4% of the variance in AIS, while an additional 3% was explained by BRS (Table 3). The remaining variables did not play a statistically significant role in explaining AIS.
Next, we explored the hypothesis that BRS might act as a mediator in the relationship between CBI Total and AIS. In this analysis, CBI Total was set as the predictor variable, BRS as the mediator variable, and AIS as the outcome variable. Covariates included work experience and age. Hayes' SPSS Process Macro Model 4 was used, with the analysis based on 5000 bootstrap samples. Unstandardized coefficients for the variables with standard errors are illustrated in Figure 1.
The mediation analysis revealed that BRS acts as a mediator in the relationship between CBI Total and AIS. In this context, the covariates, age, and work experience, did not exhibit statistically significant relationships (Figure 1 and Table 4). The indirect effect of BRS was statistically significant [b = 0.0012, 95% CI (0.0006, 0.0019), p ≤ 0.01]. Furthermore, even in the presence of the BRS mediator, the direct effect of CBI total on AIS remained significant [b = 0.0067, 95% CI (0.1521, 0.2288) p ≤ 0.001)]. This model explains 15% of the variance in the AIS outcome variable.
4. Discussion
This study was conducted 14 months after the World Health Organization officially declared the end of the COVID-19 pandemic. This period was considered sufficient to assess, under regular conditions, the levels of occupational burnout, insomnia, and psychological resilience among nurses working in Greek hospitals. However, the findings of the present study indicate that both burnout and insomnia levels among nurses remain high. Regarding occupational burnout, our results are similar to those of a study conducted one year after the onset of the pandemic (February 2021) involving nurses in Greek hospitals [37], as well as to another study conducted around the same period (the second half of March 2021) in Greek hospitals [38]. In terms of insomnia, this study recorded significantly higher levels compared to a study conducted two months after the onset of the pandemic (May 2020) among nurses in Greek hospitals [52]. These findings are also comparable to those of a study conducted in approximately two years after the onset of the pandemic among Greek hospital nurses [34], and another study conducted two months after the pandemic ended [28].
Concerning psychological resilience, this study evidenced significantly lower levels compared to a study conducted during the first wave of the pandemic (June 2020) involving nurses and doctors in Greece [26]. According to another study carried out two months after the end of the pandemic among Greek hospital nurses [28], resilience levels were similar to those in the present study (mean ± SD = 3.39 ± 0.78). Comparable results (mean ± SD = 3.50 ± 0.7) were also found in the study by Moisoglou et al., conducted two and a half years after the onset of the pandemic among Greek hospital nurses [53].
The persistence of high burnout and insomnia may be attributed, among other factors, to the reduced perceived organizational support for nurses, while the impact of the pandemic still seems to linger [53,54]. Moreover, the severe shortage of nursing staff in the Greek National Health System [55], coupled with challenging working conditions, and the low wages of Greek nurses compared to their counterparts in other OECD countries [56], are significant contributors to the situation. Additionally, we assume that the reduced perceived family support experienced by the Greek nurses after the first year of the pandemic when they were celebrated as "heroes", may have undermined the protective role of family support on nurses' mental health [34,57,58]. Furthermore, a recent study indicated that Greek nurses exhibited higher levels of burnout compared to other healthcare professionals even in the post-pandemic era [59]. Also, as stated by another study conducted after the pandemic in Greece, increased workplace bullying was positively associated with burnout [60].
Therefore, nurse managers and health policymakers should be aware of these findings to implement timely and preventive interventions to improve working conditions [60]. It is crucial that organizations recognize the magnitude of the issue, as addressing burnout caused by organizational factors will likely be more effective than isolated individual interventions [61]. Likewise, the moderate levels of resilience observed in this study may be due to the perceived lack of organizational support [53,54], the severe shortage of nursing staff and challenging working conditions [55], the low salaries of nurses in Greece [56], and the perceived reduced family support experienced during the pandemic [34,58]. According to a review article by Baskin and Bartlett, the psychological resilience of healthcare professionals worldwide during the pandemic was found to be at moderate levels [6]. Data analysis revealed a decline in resilience among U.S. nurses during the pandemic, while Chinese nurses showed increased resilience compared to pre-pandemic levels [6]. As indicated by Jo et al., in a cross-sectional study based on international data, organizational support and nurse participation in policy development during the pandemic enhanced their resilience [62]. The same study found that U.S. nurses exhibited higher resilience compared to their counterparts in Japan, Turkey, and Korea [62].
Regarding gender, no statistically significant differences were found in insomnia and psychological resilience. However, female nurses displayed higher levels of occupational burnout overall and specifically in the dimensions related to personal and work-related burnout, consistent with findings from previous studies [37,38]. This study also showed significant positive correlations between occupational burnout (particularly the subscales related to personal and work-related burnout) and insomnia. These findings align with the literature that supports this relationship [63,64,65,66]. Sleep and burnout have a bidirectional relationship, similar to other mental health conditions. Reduced sleep duration and/or poor sleep quality can affect burnout, while burnout can also impact on sleep duration and quality [63,64,65,66]. Sufficient and good-quality sleep can help address occupational burnout [67]. As stated, chronic depletion of individual energy reserves, influenced by the continuous activation of the hypothalamic-pituitary-adrenal axis and increased stress levels, can lead to both sleep disturbances and burnout [68].
Furthermore, multiple regression analysis in this study indicated that occupational burnout could explain 34.4% of the variance in insomnia. This finding is consistent with research suggesting that burnout can affect the quality of sleep and is recognized as a cause of insomnia [20,69]. Possible ways that burnout may contribute to insomnia include heightened pre-sleep arousal, intrusive thoughts and worries that prevent relaxation, and psychosomatic symptoms such as headaches and digestive symptoms that can interfere with sleep [70,71,72,73]. In contrast, sleep deprivation alone cannot cause burnout but can precipitate and/or exacerbate it [72,74].
Regarding psychological resilience, this study found that it was negatively associated with both occupational burnout and insomnia, highlighting its positive influence. Additionally, multiple regression analysis showed that resilience could explain 3% of the variance in insomnia. Furthermore, mediation analysis evidenced that resilience operates as a negative mediator in the relationship between burnout and insomnia. These findings align with results from other studies supporting the protective role of resilience against burnout and insomnia in nurses [28,53], as well as in the general population’s mental health [75,76]. A recent study highlighted the significant beneficial effect of resilience in patients with post-COVID-19 syndrome, who were found to experience better mental health and quality of life [77].
The above findings underscore the urgent need to address occupational burnout and insomnia among nurses and simultaneously strengthen their psychological resilience. In addition to the organizational support for nurses [53,54], stress management programs based on psychoeducation could improve sleep and mitigate burnout [78], as could self-care programs [79]. Enhancing resilience has a multifaceted positive influence on nurses, protecting them not only from burnout but also from other negative aspects of their profession [80]. During the pandemic, the shielding effect of resilience against burnout, especially when nurses did not receive adequate support from their supervisors, was significant [81]. Strengthening resilience is a necessary and important intervention effectuating improvements on nurses' well-being and can be cultivated [82,83]. Resilience is a dynamic process that evolves over time and involves an adaptive functioning style that allows individuals to cope with difficulties. It may start with recognizing that negative emotions such as sadness, anger, or anxiety are natural consequences of being human in the midst of a crisis and not necessarily problems that simply need to be resolved [84,85]. Finally, nursing authorities and leaders should propose and introduce programs for the regular assessment and enhancement of nurses' resilience to protect them from burnout and sleep disorders [86].
Despite its strong theoretical and methodological basis, this study has certain limitations. The cross-sectional nature did not allow us to establish causal relationships between occupational burnout, insomnia, and psychological resilience, requiring caution in interpreting the results. Longitudinal studies are needed to more accurately determine the relationships among the aforementioned variables. Data collection was conducted through self-reported questionnaires, which, while valid, may still carry the potential for response bias. The absence of clinical interviews or objective data to confirm subjective differences, and the use of convenience sampling, necessitate caution in interpreting or generalizing the results. Finally, an important drawback was the absence of information on the nurses' work department, work shifts, rotation and staff shortages.
5. Conclusions
As we move on to the second year after the end of the pandemic, with its impact on health systems diminished, the same does not apply to nurses. Both burnout and insomnia levels among nurses remain high and tend to persist. Psychological resilience among nurses also appears to remain at moderate levels. There is an urgent need to improve support for nurses from their leaders and employers, including recognition of their work, moral and financial support, ensuring adequate staffing to reduce workload and shift work, and applying meritocracy and justice in their management. Additionally, it is crucial for nursing authorities and leaders to propose and introduce programs for the regular assessment and enhancement of nurses' resilience to protect them from adverse physical and psychological effects.
Author Contributions
Conceptualization, Ar.P., C.S. and A.T.; methodology, As.P., E-P.S. and A.T.; software, S.A, I.I., and C.S.; validation, Ar.P., As.P., and C.S.; formal analysis, Ar.P., I.I. and A.T.; investigation, As.P, C.S. and A.T.; resources, Ar.P. and I.I.; data curation, E-P.S., C.S. and A.T.; writing—original draft preparation, Ar.P., S.A, and A.T.; writing—review and editing, Ar.P., As.P., I.I. and C.S.; supervision, Ar.P. and A.T.; project administration, As.P. and A.T. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was conducted in accordance with the Declaration of Helsinki and approved by the Clinical Research Ethics Committee of “Sotiria” General Hospital (Number 20649/16-05-2023).
Informed Consent Statement
Informed consent was obtained from all subjects involved in this study.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author, [A.T.], upon reasonable request.
Acknowledgments
We would like to thank all participants in our study.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Štěpánek, L.; Nakládalová, M.; Janošíková, M.; et al. Prevalence of Burnout in Healthcare Workers of Tertiary-Care Hospitals during the COVID-19 Pandemic: A Cross-Sectional Survey from Two Central European Countries. International Journal of Environmental Research and Public Health 2023, 20, 3720. [Google Scholar] [CrossRef]
- Tselebis, A.; Pachi, A. Primary Mental Health Care in a New Era. Healthcare 2022, 10, 2025. [Google Scholar] [CrossRef]
- Sikaras, C.; Zyga, S.; Tsironi, M.; et al. Assessment of insomnia and fatigue in nursing staff during the COVID-19 pandemic. Nosileftiki 2023, 62, 75–86. [Google Scholar]
- Hovland, I.S.; Skogstad, L.; Diep, L.M.; et al. Burnout among intensive care nurses, physicians and leaders during the COVID-19 pandemic: A national longitudinal study. Acta Anaesthesiologica Scandinavica 2024. [Google Scholar] [CrossRef]
- Burkhart Sasangohar, F.; Jones, S.L.; Masud, F.N.; et al. Provider burnout and fatigue during the COVID-19 pandemic: lessons learned from a high-volume intensive care unit. AnesthAnalg 2020, 131, 106–111. [Google Scholar] [CrossRef]
- Baskin, R.G.; Bartlett, R. Healthcare worker resilience during the COVID-19 pandemic: An integrative review. Journal of Nursing Management 2021, 29, 2329–2342. [Google Scholar] [CrossRef] [PubMed]
- Firew, T.; Sano, E.D.; Lee, J.W.; et al. Protecting the front line: a cross-sectional survey analysis of the occupational factors contributing to healthcare workers' infection and psychological distress during the COVID-19 pandemic in the USA. BMJ Open 2020, 10, e042752. [Google Scholar] [CrossRef] [PubMed]
- Preti, E.; Di Mattei, V.; Perego, G.; et al. The Psychological Impact of Epidemic and Pandemic Outbreaks on Healthcare Workers: Rapid Review of the Evidence. Current Psychiatry Reports 2020, 22, 43. [Google Scholar] [CrossRef] [PubMed]
- Jahrami, H.A.; Alhaj, O.A.; Humood, A.M.; et al. Sleep disturbances during the COVID-19 pandemic: A systematic review, meta-analysis, and meta-regression. Sleep Medicine Reviews 2022, 62, 101591. [Google Scholar] [CrossRef]
- Sarafis, P.; Rousaki, E.; Tsounis, A.; et al. The impact of occupational stress on nurses' caring behaviors and their health related quality of life. BMC Nursing 2016, 15, 56. [Google Scholar] [CrossRef]
- Arnsten, A.F.T.; Shanafelt, T. Physician Distress and Burnout: The Neurobiological Perspective. Mayo Clinic Proceedings 2021, 96, 763–769. [Google Scholar] [CrossRef] [PubMed]
- Maslach, C.; Jackson, S.E. The measurement of experienced burnout. J Organ Behav 1981, 2, 99–113. [Google Scholar] [CrossRef]
- Schaufeli, W.B.; Greenglass, E.R. Introduction to special issue on burnout and health. Psychology & Health 2001, 16, 501–510. [Google Scholar] [CrossRef]
- Parada, M.E.; Moreno, R.; Mejías, M.Z.; et al. Job satisfaction and burnout syndrome in the nursing staff of the Instituto Autónomo Hospital Universitario Los Andes, Mérida, Venezuela. Rev. Fac. Nac 2005, 23, 33–45. [Google Scholar]
- Huang, C.L.; Wu, M.P.; Ho, C.H.; Wang, J.J. Risks of treated anxiety, depression, and insomnia among nurses: A nationwide longitudinal cohort study. PloS ONE 2018, 13, e0204224. [Google Scholar] [CrossRef]
- Hsieh, M.L.; Li, Y.M.; Chang, E.T.; Lai, H.L.; Wang, W.H.; Wang, S.C. Sleep disorder in Taiwanese nurses: a random sample survey. Nursing & Health Sciences 2011, 13, 468–474. [Google Scholar] [CrossRef]
- Yazdanshenas Ghazwin, M.; Kavian, M.; Ahmadloo, M.; et al. The Association between Life Satisfaction and the Extent of Depression, Anxiety and Stress among Iranian Nurses: A Multicenter Survey. Iranian Journal of Psychiatry 2016, 11, 120–127. [Google Scholar] [PubMed]
- Chang, W.P.; Peng, Y.X. Influence of rotating shifts and fixed night shifts on sleep quality of nurses of different ages: a systematic literature review and meta-analysis. Chronobiology International 2021, 38, 1384–1396. [Google Scholar] [CrossRef] [PubMed]
- Geiger-Brown, J.; Rogers, V.E.; Trinkoff, A.M.; et al. Sleep, sleepiness, fatigue, and performance of 12-hour-shift nurses. Chronobiology International 2012, 29, 211–219. [Google Scholar] [CrossRef]
- Membrive-Jiménez, M.J.; Gómez-Urquiza, J.L.; Suleiman-Martos, N.; et al. Relation between Burnout and Sleep Problems in Nurses: A Systematic Review with Meta-Analysis. Healthcare 2022, 10, 954. [Google Scholar] [CrossRef]
- Consensus Conference Panel; Watson, N.F.; Badr, M.S.; et al. Joint Consensus Statement of the American Academy of Sleep Medicine and Sleep Research Society on the Recommended Amount of Sleep for a Healthy Adult: Methodology and Discussion. Sleep 2015, 38, 1161–1183. [Google Scholar] [CrossRef] [PubMed]
- Delgado, C.; Upton, D.; Ranse, K.; et al. Nurses' resilience and the emotional labour of nursing work: An integrative review of empirical literature. International Journal of Nursing Studies 2017, 70, 71–88. [Google Scholar] [CrossRef]
- Hart, P.L.; Brannan, J.D.; De Chesnay, M. Resilience in nurses: an integrative review. Journal of Nursing Management 2014, 22, 720–734. [Google Scholar] [CrossRef] [PubMed]
- McAllister, M.; McKinnon, J. The importance of teaching and learning resilience in the health disciplines: a critical review of the literature. Nurse Education Today 2009, 29, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Thomas, L.J.; Revell, S.H. Resilience in nursing students: An integrative review. Nurse Education Today 2016, 36, 457–462. [Google Scholar] [CrossRef] [PubMed]
- Pachi, A.; Kavourgia, E.; Bratis, D.; et al. Anger and Aggression in Relation to Psychological Resilience and Alcohol Abuse among Health Professionals during the First Pandemic Wave. Healthcare 2023, 11, 2031. [Google Scholar] [CrossRef]
- Lara-Cabrera, M.L.; Betancort, M.; Muñoz-Rubilar, C.A.; et al. The Mediating Role of Resilience in the Relationship between Perceived Stress and Mental Health. International Journal of Environmental Research and Public Health 2021, 18, 9762. [Google Scholar] [CrossRef]
- Pachi, A.; Tselebis, A.; Sikaras, C.; et al. Nightmare distress, insomnia and resilience of nursing staff in the post-pandemic era. AIMS Public Health 2023, 11, 36–57. [Google Scholar] [CrossRef]
- Palagini, L.; Moretto, U.; Novi, M.; et al. Lack of resilience is related to stress-related sleep reactivity, hyperarousal, and emotion dysregulation in insomnia disorder. J Clin Sleep Med 2018, 14, 759–766. [Google Scholar] [CrossRef] [PubMed]
- Lisi, L.; Ciaffi, J.; Bruni, A.; et al. Levels and Factors Associated with Resilience in Italian Healthcare Professionals during the COVID-19 Pandemic: A Web-Based Survey. Behavioral Sciences 2020, 10, 183. [Google Scholar] [CrossRef] [PubMed]
- Labrague, L.J. Psychological resilience, coping behaviours and social support among health care workers during the COVID-19 pandemic: A systematic review of quantitative studies. Journal of Nursing Management 2021, 29, 1893–1905. [Google Scholar] [CrossRef] [PubMed]
- Tziallas, D.; Goutzias, E.; Konstantinidou, E.; et al. Quantitative and qualitative assessment of nurse staffing indicators across NHS public hospitals in Greece. Hell J Nurs 2018, 57, 420–449. [Google Scholar]
- Tselebis, A.; Sikaras, C.; Milionis, C.; et al. A Moderated Mediation Model of the Influence of Cynical Distrust, Medical Mistrust, and Anger on Vaccination Hesitancy in Nursing Staff. European Journal of Investigation in Health, Psychology and Education 2023, 13, 2373–2387. [Google Scholar] [CrossRef]
- Sikaras, C.; Tsironi, M.; Zyga, S.; et al. Anxiety, insomnia and family support in nurses, two years after the onset of the pandemic crisis. AIMS Public Health 2023, 10, 252–267. [Google Scholar] [CrossRef]
- Sikaras, C.; Zyga, S.; Tsironi, M.; et al. The Mediating Role of Depression and of State Anxiety οn the Relationship between Trait Anxiety and Fatigue in Nurses during the Pandemic Crisis. Healthcare 2023, 11, 367. [Google Scholar] [CrossRef] [PubMed]
- Kristensen, T.S.; Borritz, M.; Villadsen, E.; et al. The Copenhagen Burnout Inventory: a new tool for the assessment of burnout. Work Stress 2005, 19, 192–207. [Google Scholar] [CrossRef]
- Sikaras, C.; Ilias, I.; Tselebis, A.; et al. Nursing staff fatigue and burnout during the COVID-19 pandemic in Greece. AIMS Public Health 2021, 9, 94–105. [Google Scholar] [CrossRef]
- Pachi, A.; Sikaras, C.; Ilias, I.; et al. Burnout, Depression and Sense of Coherence in Nurses during the Pandemic Crisis. Healthcare 2022, 10, 134. [Google Scholar] [CrossRef]
- Papaefstathiou, E.; Tsounis, A.; Malliarou, M.; et al. Translation and validation of the Copenhagen Burnout Inventory amongst Greek doctors. Health Psychology Research 2019, 7, 7678. [Google Scholar] [CrossRef]
- Henriksen, L.; Lukasse, M. Burnout among Norwegian midwives and the contribution of personal and work-related factors: A cross-sectional study. Sexual & Reproductive Healthcare: Official Journal of the Swedish Association of Midwives 2016, 9, 42–47. [Google Scholar] [CrossRef]
- Madsen, I.E.; Lange, T.; Borritz, M.; et al. Burnout as a risk factor for antidepressant treatment - a repeated measures time-to-event analysis of 2936 Danish human service workers. Journal of Psychiatric Research 2015, 65, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Hovland, I.S.; Skogstad, L.; Diep, L.M.; et al. Burnout among intensive care nurses, physicians and leaders during the COVID-19 pandemic: A national longitudinal study. Acta Anaesthesiologica Scandinavica 2024. advance online publication. [Google Scholar] [CrossRef] [PubMed]
- Benson, S.; Sammour, T.; Neuhaus, S.J.; et al. Burnout in Australasian Younger Fellows. ANZ Journal of Surgery 2009, 79, 590–597. [Google Scholar] [CrossRef] [PubMed]
- Chou, L.P.; Li, C.Y.; Hu, S.C. Job stress and burnout in hospital employees: comparisons of different medical professions in a regional hospital in Taiwan. BMJ Open 2014, 4, e004185. [Google Scholar] [CrossRef] [PubMed]
- Kwan, K.Y.; Chan, L.W.; Cheng, P.; Leung, G.K.; Lau, C. Burnout and well-being in young doctors in Hong Kong: a territory-wide cross-sectional survey. Hong Kong Medical Journal = Xianggang Yi Xue Za Zhi 2021, 27, 330–337. [Google Scholar] [CrossRef]
- Creedy, D.K.; Sidebotham, M.; Gamble, J.; et al. Prevalence of burnout, depression, anxiety and stress in Australian midwives: a cross-sectional survey. BMC Pregnancy and Childbirth 2017, 17, 13. [Google Scholar] [CrossRef] [PubMed]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. The diagnostic validity of the Athens Insomnia Scale. Journal of Psychosomatic Research 2003, 55, 263–267. [Google Scholar] [CrossRef] [PubMed]
- Soldatos, C.R.; Dikeos, D.G.; Paparrigopoulos, T.J. Athens Insomnia Scale: validation of an instrument based on ICD-10 criteria. Journal of Psychosomatic Research 2000, 48, 555–560. [Google Scholar] [CrossRef] [PubMed]
- Tselebis, A.; Lekka, D.; Sikaras, C.; et al. Sleep Disorders, Perceived Stress and Family Support Among Nursing Staff During the Pandemic Crisis. 2020; 1–13. [Google Scholar] [CrossRef]
- Smith, B.W.; Dalen, J.; Wiggins, K.; et al. The brief resilience scale: assessing the ability to bounce back. International Journal of Behavioral Medicine 2008, 15, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Kyriazos, T.A.; Stalikas, A.; Prassa, K.; et al. Psychometric evidence of the Brief Resilience Scale (BRS) and modeling distinctiveness of resilience from depression and stress. Psychology 2018, 9, 1828–1857. [Google Scholar] [CrossRef]
- Tselebis, A.; Lekka, D.; Sikaras, C.; et al. Insomnia, Perceived Stress, and Family Support among Nursing Staff during the Pandemic Crisis. Healthcare 2020, 8, 434. [Google Scholar] [CrossRef]
- Moisoglou, I.; Katsiroumpa, A.; Malliarou, M.; et al. Social Support and Resilience Are Protective Factors against COVID-19 Pandemic Burnout and Job Burnout among Nurses in the Post-COVID-19 Era. Healthcare 2024, 12, 710. [Google Scholar] [CrossRef]
- Abdulmohdi, N. The relationships between nurses' resilience, burnout, perceived organisational support and social support during the second wave of the COVID-19 pandemic: A quantitative cross-sectional survey. Nursing Open 2024, 11, e2036. [Google Scholar] [CrossRef] [PubMed]
- Health at a Glance: Europe 2020 STATE OF HEALTH IN THE EU CYCLE. Available online: https://ec.europa.eu/health/system/files/2020-12/2020_healthatglance_rep_en_0.pdf (accessed on 19 August 2024).
- Health at a Glance 2023: OECD Indicators. Available online: https://www.oecd.org/en/publications/health-at-a-glance-2023_7a7afb35-en.html (accessed on 19 August 2024).
- Bratis, D.; Tselebis, A.; Sikaras, C.; et al. Alexithymia and its association with burnout, depression and family support among Greek nursing staff. Human Resources for Health 2009, 7, 72. [Google Scholar] [CrossRef] [PubMed]
- Pachi, A.; Anagnostopoulou, M.; Antoniou, A.; et al. Family support, anger and aggression in health workers during the first wave of the pandemic. AIMS Public Health 2023, 10, 524–537. [Google Scholar] [CrossRef] [PubMed]
- Galanis, P.; Moisoglou, I.; Katsiroumpa, A.; et al. Increased Job Burnout and Reduced Job Satisfaction for Nurses Compared to Other Healthcare Workers after the COVID-19 Pandemic. Nursing Reports 2023, 13, 1090–1100. [Google Scholar] [CrossRef]
- Galanis, P.; Moisoglou, I.; Katsiroumpa, A.; et al. Impact of workplace bullying on job burnout and turnover intention among nursing staff in Greece: Evidence after the COVID-19 pandemic. AIMS Public Health 2024, 11, 614–627. [Google Scholar] [CrossRef]
- De Simone, S.; Vargas, M.; Servillo, G. Organizational strategies to reduce physician burnout: a systematic review and meta-analysis. Aging Clinical and Experimental Research 2021, 33, 883–894. [Google Scholar] [CrossRef] [PubMed]
- Jo, S.; Kurt, S.; Bennett, J.A.; et al. Nurses' resilience in the face of coronavirus (COVID-19): An international view. Nursing & Health Sciences 2021, 23, 646–657. [Google Scholar] [CrossRef]
- Wolkow, A.P.; Barger, L.K.; O'Brien, C.S.; et al. Associations between sleep disturbances, mental health outcomes and burnout in firefighters, and the mediating role of sleep during overnight work: A cross-sectional study. Journal of Sleep Research 2019, 28, e12869. [Google Scholar] [CrossRef] [PubMed]
- Söderström, M.; Jeding, K.; Ekstedt, M.; et al. Insufficient sleep predicts clinical burnout. Journal of Occupational Health Psychology 2012, 17, 175–183. [Google Scholar] [CrossRef] [PubMed]
- Armon, G.; Shirom, A.; Shapira, I.; et al. On the nature of burnout-insomnia relationships: a prospective study of employed adults. Journal of Psychosomatic Research 2008, 65, 5–12. [Google Scholar] [CrossRef]
- Weaver, M.D.; Robbins, R.; Quan, S.F.; et al. Association of Sleep Disorders With Physician Burnout. JAMA Network Open 2020, 3, e2023256. [Google Scholar] [CrossRef] [PubMed]
- Assefa, S.Z.; Diaz-Abad, M.; Wickwire, E.M.; Scharf, S.M. The Functions of Sleep. AIMS Neuroscience 2015, 2, 155–171. [Google Scholar] [CrossRef]
- Stewart, N.H.; Arora, V.M. The Impact of Sleep and Circadian Disorders on Physician Burnout. Chest 2019, 156, 1022–1030. [Google Scholar] [CrossRef]
- Salvagioni, D.A.J.; Melanda, F.N.; Mesas, A.E.; et al. Physical, psychological and occupational consequences of job burnout: a systematic review of prospective studies. PLoS One 2017, 12, e0185781. [Google Scholar] [CrossRef]
- Kuriyama, K. The association between work burnout and insomnia: how to prevent workers' insomnia. Sleep Biol Rhythms 2023, 21, 3–4. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sørengaard, T.A.; Saksvik-Lehouillier, I. Associations between burnout symptoms and sleep among workers during the COVID-19 pandemic. Sleep Med 2022, 90, 199–203. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zarei, S.; Fooladvand, K. Mediating effect of sleep disturbance and rumination on work-related burnout of nurses treating patients with coronavirus disease. BMC Psychol 2022, 10, 197. [Google Scholar] [CrossRef] [PubMed]
- Khammissa, R.A.G.; Nemutandani, S.; Feller, G.; et al. Burnout phenomenon: neurophysiological factors, clinical features, and aspects of management. J Int Med Res 2022, 50, 3000605221106428. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Metlaine, A.; Sauvet, F.; Gomez-Merino, D.; et al. Association between insomnia symptoms, job strain and burnout syndrome: a cross-sectional survey of 1300 financial workers. BMJ Open 2017, 7, e012816. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ye, Z.; Yang, X.; Zeng, C.; et al. Resilience, Social Support, and Coping as Mediators between COVID-19-related Stressful Experiences and Acute Stress Disorder among College Students in China. Applied Psychology. Health and Well-Being 2020, 12, 1074–1094. [Google Scholar] [CrossRef] [PubMed]
- Li, F.; Luo, S.; Mu, W.; et al. Effects of sources of social support and resilience on the mental health of different age groups during the COVID-19 pandemic. BMCpsychiatry 2021, 21, 16. [Google Scholar] [CrossRef]
- Moisoglou, I.; Katsiroumpa, A.; Kolisiati, A.; et al. Resilience and Social Support Improve Mental Health and Quality of Life in Patients with Post-COVID-19 Syndrome. European Journal of Investigation in Health, Psychology and Education 2024, 14, 230–242. [Google Scholar] [CrossRef] [PubMed]
- Ekstedt, M.; Söderström, M.; Akerstedt, T. Sleep physiology in recovery from burnout. Biological psychology 2009, 82, 267–273. [Google Scholar] [CrossRef] [PubMed]
- Morimoto, H.; Tanaka, H.; Ohkubo, R.; et al. Self-help therapy for sleep problems in hospital nurses in Japan: a controlled pilot study. Sleep and Biological Rhythms 2016, 14, 177–185. [Google Scholar] [CrossRef]
- Kılınç, T.; Sis Çelik, A. Relationship between the social support and psychological resilience levels perceived by nurses during the COVID-19 pandemic: A study from Turkey. Perspectives in Psychiatric Care 2021, 57, 1000–1008. [Google Scholar] [CrossRef]
- Phillips, K.; Knowlton, M.; Riseden, J. Emergency Department Nursing Burnout and Resilience. Advanced Emergency Nursing Journal 2022, 44, 54–62. [Google Scholar] [CrossRef]
- Foster, K.; Cuzzillo, C.; Furness, T. Strengthening mental health nurses' resilience through a workplace resilience programme: A qualitative inquiry. Journal of Psychiatric and Mental Health Nursing 2018, 25, 338–348. [Google Scholar] [CrossRef]
- Foureur, M.; Besley, K.; Burton, G.; et al. Enhancing the resilience of nurses and midwives: pilot of a mindfulness-based program for increased health, sense of coherence and decreased depression, anxiety and stress. Contemporary Nurse 2013, 45, 114–125. [Google Scholar] [CrossRef] [PubMed]
- Sisto, A.; Vicinanza, F.; Campanozzi, L.L.; et al. Towards a Transversal Definition of Psychological Resilience: A Literature Review. Medicina 2019, 55, 745. [Google Scholar] [CrossRef] [PubMed]
- Barthélemy, E.J.; Thango, N.S.; Höhne, J.; et al. Resilience in the Face of the COVID-19 Pandemic: How to Bend and not Break. World Neurosurgery 2021, 146, 280–284. [Google Scholar] [CrossRef]
- Alameddine, M.; Clinton, M.; Bou-Karroum, K.; et al. Factors Associated With the Resilience of Nurses During the COVID-19 Pandemic. Worldviews on Evidence-Based Nursing 2021, 18, 320–331. [Google Scholar] [CrossRef]
Figure 1.
Mediation analysis of the Brief Resilience Scale (BRS) on the Copenhagen burnout inventory (CBI Total) and the Athens Insomnia Scale (AIS) relationship.
Figure 1.
Mediation analysis of the Brief Resilience Scale (BRS) on the Copenhagen burnout inventory (CBI Total) and the Athens Insomnia Scale (AIS) relationship.
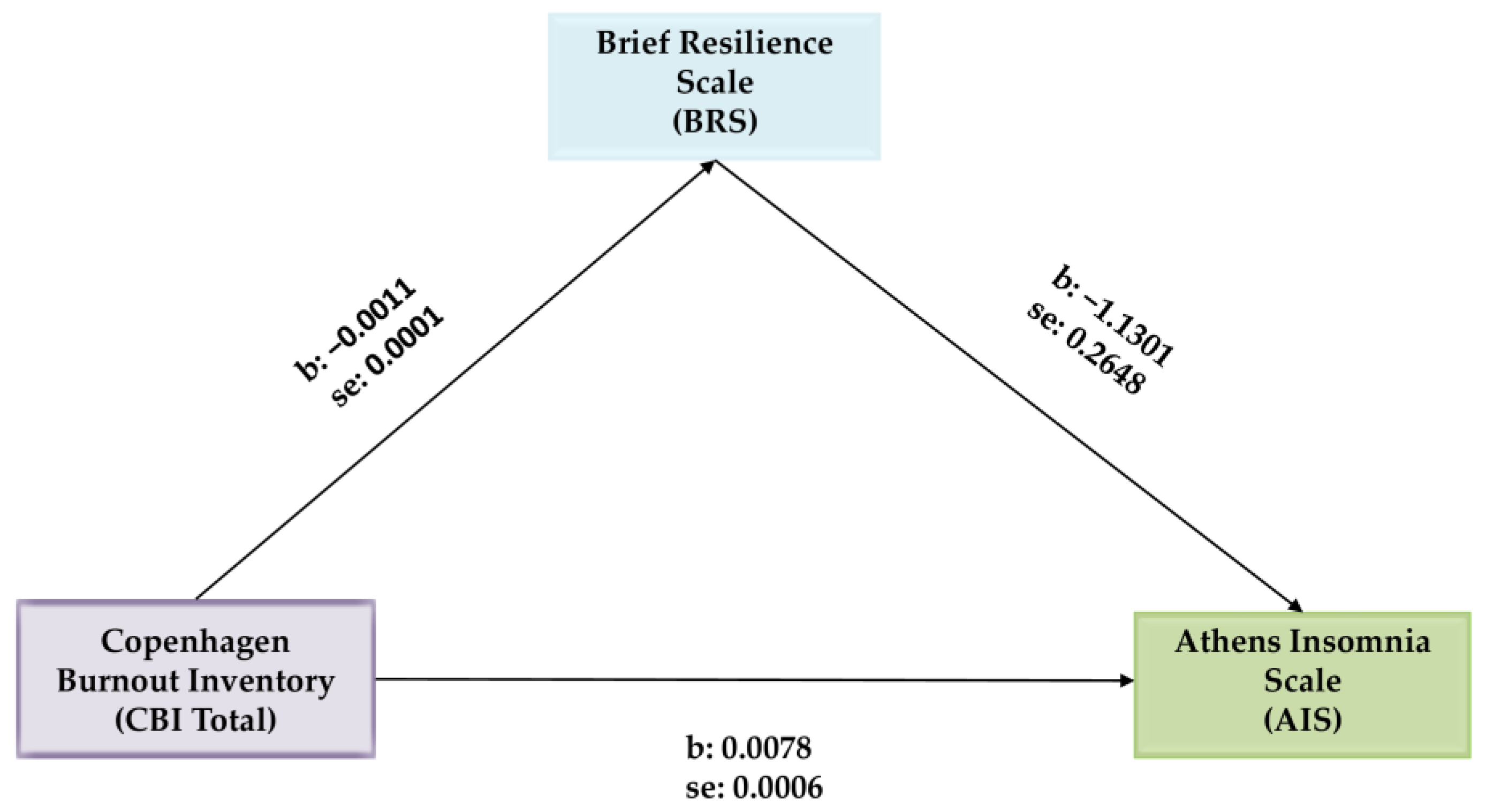

Table 1.
Descriptive statistics of participants.
| Gender | Age | Work experience (in years) | Athens Insomnia Scale | Brief Resilience Scale | Copenhagen Burnout Inventory | ||||
| Total | Personal Burnout | Work Related Burnout | Patient Related Burnout | ||||||
| Male | Mean | 47.57 * | 21.89 | 6.35 | 3.58 | 44.91 * | 44.76 ** | 47.83 ** | 41.67 |
| N | 74 | 74 | 74 | 74 | 74 | 74 | 74 | 74 | |
| S.D. | 10.85 | 11.92 | 4.23 | 0.89 | 17.93 | 18.71 | 20.89 | 21.26 | |
| Female | Mean | 44.58 * | 19.92 | 7.31 | 3.40 | 49.64 * | 52.67 ** | 55.45 ** | 39.84 |
| N | 306 | 306 | 306 | 306 | 306 | 306 | 306 | 306 | |
| S.D. | 10.41 | 11.47 | 4.92 | 0.81 | 19.03 | 19.86 | 22.74 | 23.68 | |
| Total | Mean | 45.16 | 20.30 | 7.12 | 3.43 | 48.72 | 51.13 | 53.97 | 40.20 |
| N | 380 | 380 | 380 | 380 | 380 | 380 | 380 | 380 | |
| S.D. | 10.55 | 11.57 | 4.80 | 0.83 | 18.89 | 19.87 | 22.56 | 23.21 | |
| * t test p < 0.05, ** t test p < 0.01 | |||||||||
Table 2.
Correlations among age, work experience, AIS, BRS and CBI.
| Pearson Correlation N: 380 | Age | Work experience (in years) | AIS | BRS | CBI Total | CPB | CWB | |
| Work experience (in years) | r | 0.894 ** | ||||||
| p | 0.001 | |||||||
| Athens Insomnia Scale (AIS) | r | -0.064 | -0.126 * | |||||
| p | 0.214 | 0.014 | ||||||
| Brief Resilience Scale (BRS) | r | 0.080 | 0.111 * | -0.423 ** | ||||
| p | 0.120 | 0.030 | 0.001 | |||||
| Copenhagen Burnout Inventory (CBI Total) | r | -0.031 | -0.058 | 0.587 ** | -0.457 ** | |||
| p | 0.552 | 0.257 | 0.001 | 0.001 | ||||
| Copenhagen Personal Burnout (CPB) | r | -0.024 | -0.068 | 0.634 ** | -0.449 ** | 0.866 ** | ||
| p | 0.642 | 0.183 | 0.001 | 0.001 | 0.001 | |||
| Copenhagen Work-related Burnout (CWB) | r | -0.029 | -0.047 | 0.567 ** | -0.397 ** | 0.919 ** | 0.789 ** | |
| p | 0.578 | 0.362 | 0.001 | 0.001 | 0.001 | 0.001 | ||
| Copenhagen Patient-related Burnout | r | -0.026 | -0.039 | 0.327 ** | -0.343 ** | 0.794 ** | 0.482 ** | 0.559 ** |
| p | 0.615 | 0.454 | 0.001 | 0.001 | 0.001 | 0.001 | 0.001 | |
* Pearson Correlations p < 0.05, ** Pearson Correlations p < 0.01.
Table 3.
Stepwise multiple regression.
| Dependent Variable: Athens Insomnia Scale | R Square | R Square Change | Beta | t | p | VIF | Durbin-Watson |
| Copenhagen Burnout Inventory (CBI Total) | 0.344 | 0.344 | 0.497 | 10.863 | 0.001 * | 1.264 | 1.918 |
| Brief Resilience Scale | 0.375 | 0.030 | -0.195 | -4.267 | 0.001 * | 1.264 | |
| Notes: Beta = standardized regression coefficient; * Correlations are statistically significant at the p < 0.001 level (only statistically significant variables are included). | |||||||
Table 4.
Mediation analysis of the Brief Resilience Scale (BRS) on the Copenhagen Burnout Inventory (CBI Total) and the Athens Insomnia Scale (AIS) relationship *.
Table 4.
Mediation analysis of the Brief Resilience Scale (BRS) on the Copenhagen Burnout Inventory (CBI Total) and the Athens Insomnia Scale (AIS) relationship *.
| Variables | b | SE | t | p | 95% Confidence Interval | |
| LLCI | ULCI | |||||
| CBI Total → BRS | −0.0011 | 0.0001 | −9.9928 | 0.001 | −0.0013 | −0.0008 |
| CBI Total → AIS | 0.0078 | 0.0006 | 14.0899 | 0.001 | 0.0068 | 0.0089 |
| CBI Total → BRS → AIS | −1.1301 | 0.2648 | −4.2673 | 0.001 | −1.6509 | −0.6094 |
| Effects | ||||||
| Direct | 0.0066 | 0.0006 | 10.8629 | 0.001 | 0.0054 | 0.0079 |
| Indirect * | 0.0012 | 0.0003 | 0.0006 | 0.0019 | ||
| Total | 0.0078 | 0.0006 | 14.0899 | 0.001 | 0.0068 | 0.089 |
Notes: * based on 5000 bootstrap samples.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



