
Submitted:
16 December 2024
Posted:
25 December 2024
You are already at the latest version
Abstract
Background: Four research article had been published recently in peer-reviewed scientific journals reviewing and reevaluating the key statistical data of the COVID-19 pandemic in the USA. The first article [1] introduced the “political score” for quantitative characterization of the political orientation of the 50 states and concluded that the most alarming signals regarding the dangerousness of COVID infection had been originating in a few states with predominantly left oriented citizens.The second article [2] critically reviewed the diagnostic and statistical support for COVID epidemic in USA and concluded, that many states largely ignored the importance of a) specific viral tests and b) considerations of the “natural”, age-related deaths when determining and reporting the correct number of COVID mortality and lethality. The third article [3] focused on the effects of restrictions on the COVID lethality and concluded that restrictions had no health benefits at all. The fourth article [4] focused on the “human” contributions to the demages caused by the virus and concluded, that much of the negative effects of the pandemic was actually self-made. Objective: The resent article is aiming to go one step further and concludes that much of the mistakes during the COVID pandemic were a) the result of well-meaning but poorly executed actions by unprofessional actors; b) the excessive involvement of left oriented states in the overestimation of the virus related harm and enforcement of harsh restrictions were the signs of political bias; c) there were strong political and monetary motives behind the interpretation of the COVID events. We can understand and even forgive the ignorance and political blindness behind most of the mistakes, however the economic incentive is not excusable. Profiting on other people’s fear and despair is - in our opinion - a criminal act even if it is not by any means a new phenomenon in the history of mankind. Conclusion: It is suggested that the “new” political and scientific leaders (following the latest presidential election in 2024) seriously consider invoking the Federal False Claim Act for definitively ending the COVID syndemic in the USA and effectively preventing ‘relapse’ in the near future.
Keywords:
Introduction
Critical Review of the Critical Decisions: The Triumvirate of Errors with Consequences
- 1)
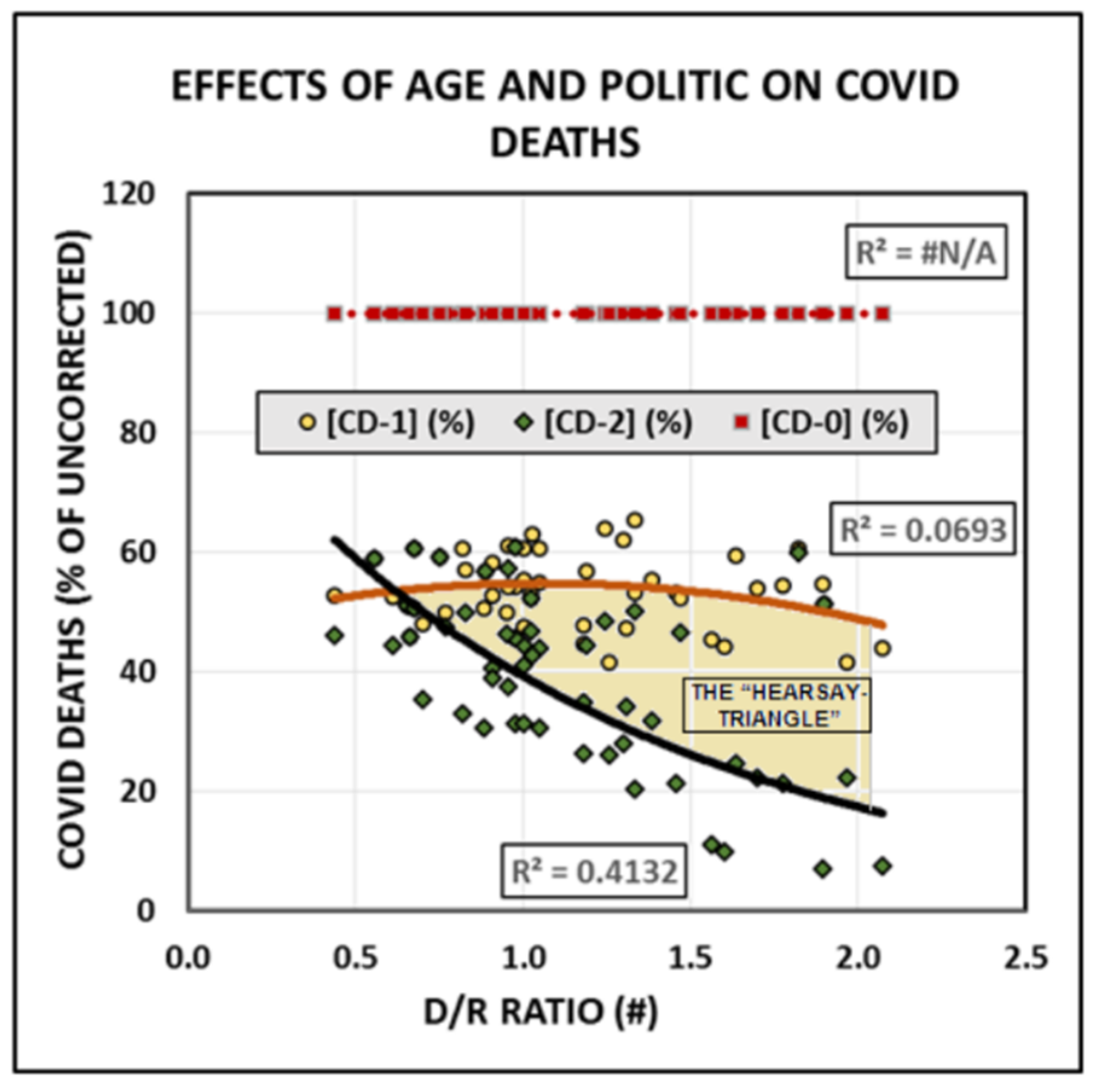
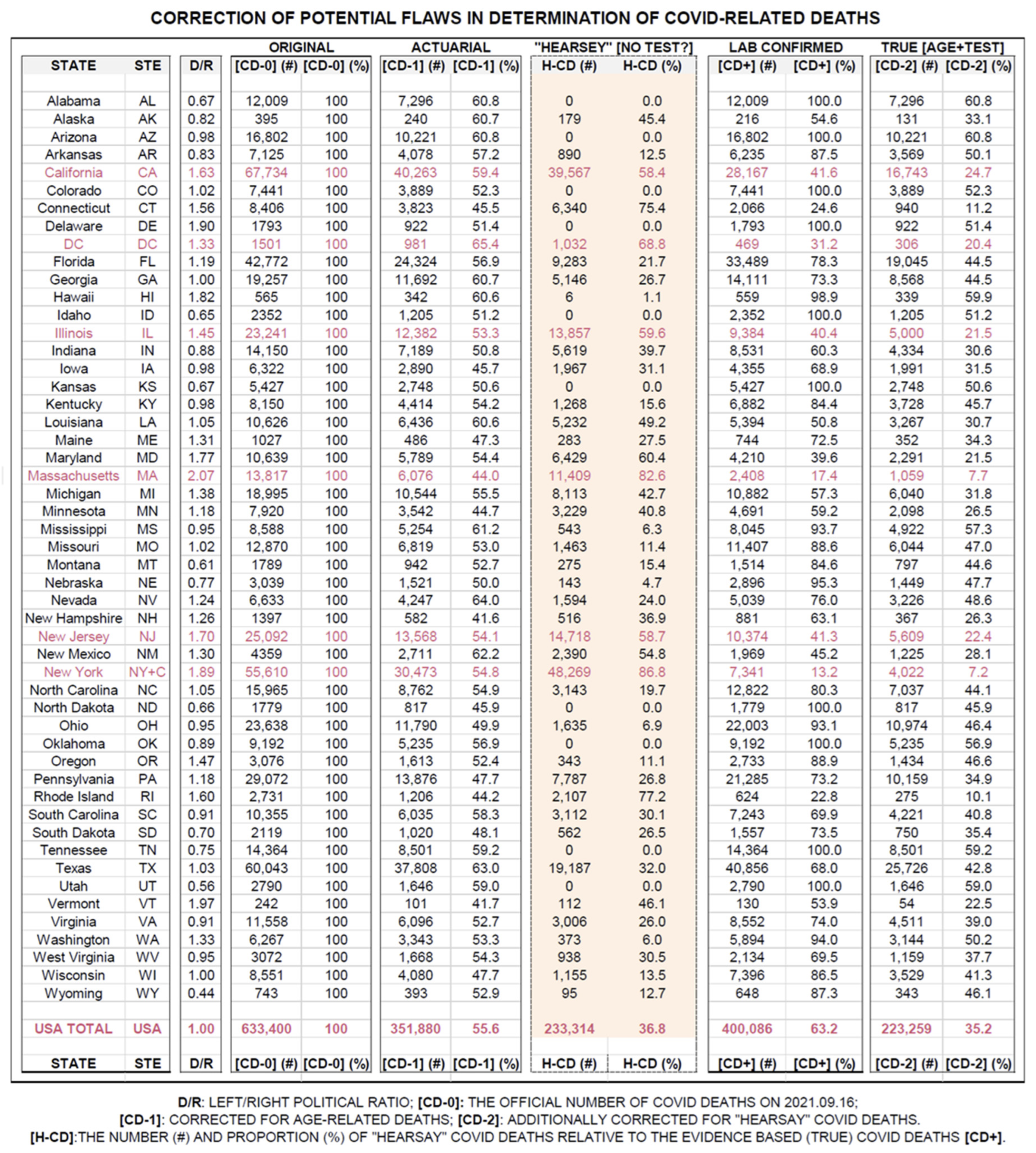
- PSEUDO COVID counting and reporting occurred in every state. It contributed with ca 45-50% to the overestimation of the COVID mortality/lethality by adding cases, there the person died “with COVID” (test positive) but not “due to COVID” disease. Separation of the pathological (abnormal) and physiological (normal, usual, expectable) deaths is not possible at the bedside. It is possible only statistically. Ignoring natural deaths is a shameful error for an epidemiologist who supposed to be expert of all possible aspect of a pandemic. However rationally dealing with the natural deaths is not easy for many Americans, because of their cultural/religious traditions. Therefore the PSEUDO COVID counting remains an unintentional error that we have to live with.
- 2)
- HEARSAY COVID counting and reporting is when the virus is regarded to be the case of disease or the UCOD without access to specific laboratory viral test. This situation can occur at the beginning of an epidemic - when test is not developed yet - or when the viral test is too expansive for routine clinical diagnoses. This was certainly not the case after Marsh 2020 in USA. Accepting test-free diagnosis of the UCOD is difficult even if we consider that there are doctors who don’t like to spend valuable time lamenting over the correct death-diagnoses, insisting that “death is death”.
- 3)
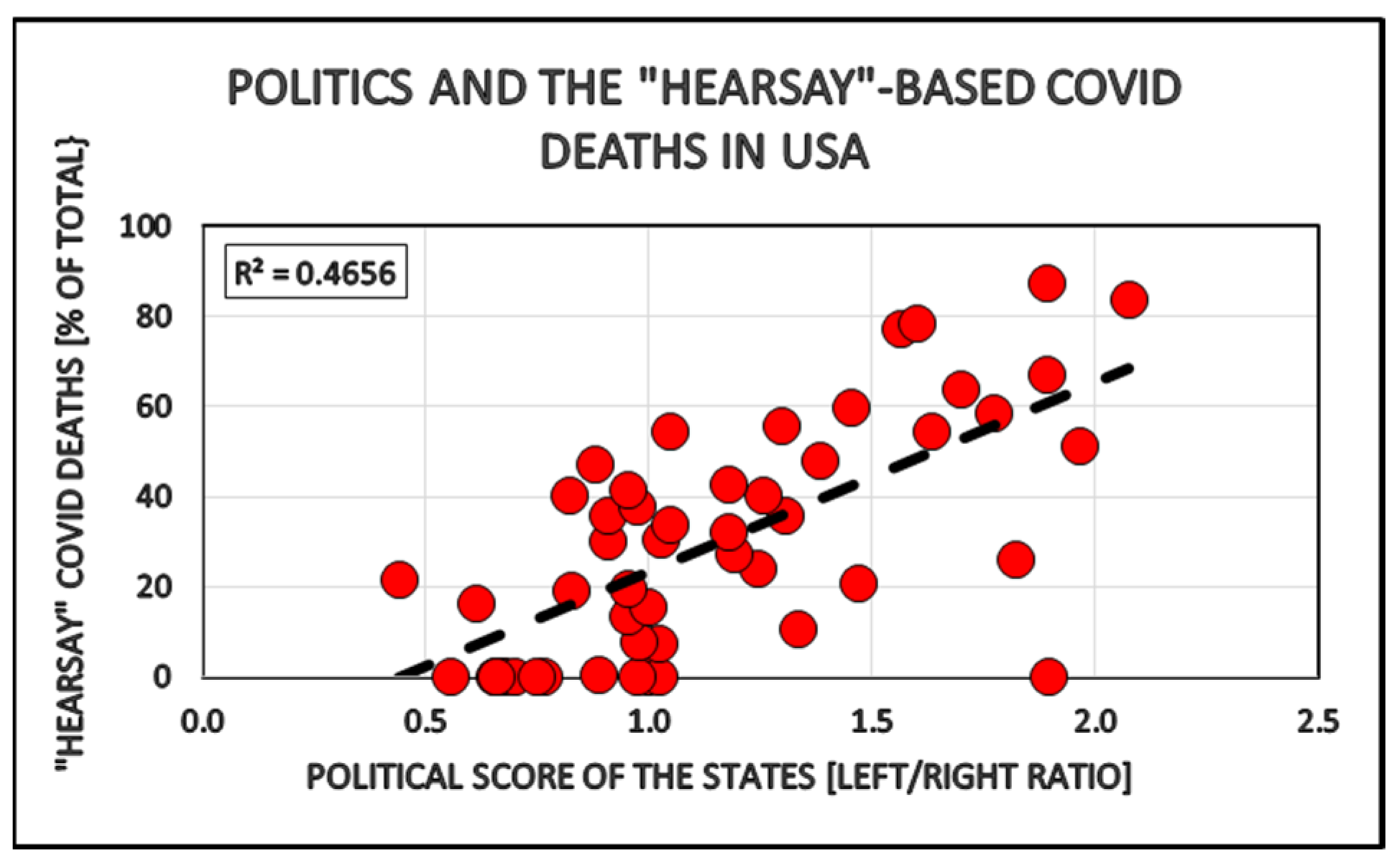
- POLITICAL BIAS in counting and reporting COVID deaths is certainly the most disturbing form of statistical error under the pandemic. It is caused by the excessive HEARSAY COVID diagnostic by the states with large left-oriented population. Political leaning is obviously not caused or recognized by any virus, therefore this bias is man-made.
- 1)
- COVID was almost exclusively targeted elderly and chronically sick persons, those who provided the largest income for the medical-pharmaceutical industry. The epidemic threatened the largest and most profitable market of the healthcare- and related industries.
- 2)
- The well-meaning emergency Provider Relieve COVID Fund (PRF) provided extra profit for everybody who became involved into the care of COVID patients. Diagnosing and treating COVID disease became much more profitable than, say, a very similar seasonal flu. It was an effect that was certainly not intended by the fund providers – the US Government – but it became the result and nobody wanted to know about it and prevent it.
- 3)
- The strongly promoted need of vaccination provided the “ones in the lifetime opportunity” for the pharmaceutical industry to generate the largest possible market for their vaccine products and access to a flood of Federal ‘easy money’. The US Government (taxpayers) marketed, sold and payed for the COVID vaccines. No other industry was ever in this dream situation, with the only exception of the wapen manufacturers and related industries under WWII.
An Example of Misleading COVID Information

The possible curative and preventive use of the Federal False Claim Act [31 U.S.C. §3730(B)(2).] - (FCA, Quo Tam).
The Provider Relief Fund, PRF - Terms and Conditions
“To address potential Medicare program integrity risks, effective with admissions occurring on or after September 1, 2020, claims eligible for the 20 percent increase in the MS-DRG weighting factor will also be required to have a positive COVID-19 laboratory test documented in the patient’s medical record. Positive tests must be demonstrated using only the results of viral testing (i.e., molecular or antigen), consistent with CDC guidelines. The test may be performed either during the hospital admission or prior to the hospital admission”.
“…payments for discharges that report the ICD-10-CM diagnosis code U07.1 (COVID-19). CMS may conduct post-payment medical review to confirm the presence of a positive COVID-19 laboratory test and, if no such test is contained in the medical record, the additional payment resulting from the 20 percent increase in the MS-DRG relative weight will be recouped.” [13,19]
CDC INSTRUCTION FOR DETERMINATION COVID RELATED DEATHS AND REPORTING USING THE U07.1 CODE
“Code only a conformed diagnoses of the 2019 novel coronavirus disease (COVID-19) as documented by the provider or documentation of a positive COVID-19 test result. For confirmed diagnoses, assign code U07.1, COVID-19.” [20]
“If the provider documents "suspected," "possible," "probable," or “inconclusive” COVID-19, do not assign code U07.1. Instead, code the signs and symptoms reported.” [21]
“Monitoring the emergence of COVID–19 in the United States and guiding public health response will also require accurate and timely death reporting. The purpose of this report is to provide guidance to death certifiers on proper cause-of-death certification for cases where confirmed or suspected COVID–19 infection resulted in death. As clinical guidance on COVID–19 evolves, this guidance may be updated, if necessary. When COVID–19 is determined to be a cause of death, it is important that it be reported on the death certificate to assess accurately the effects of this pandemic and appropriately direct public health response.”
- reliable COVID diagnostic is only possible by positive laboratory viral test;
- Report only test positive (confirmed) cases of death under code U07.1;
- Claim elevated reimbursement from the insurance or emergency fund only for procedures on confirmed (test positive) cases.
IS IT POSSIBLE TO RECOVER FALSELY CLAIMED (PREMIUM)-PAYMENTS FOR “HEARSAY COVID CASES”?
“A False Claims Act violation includes four elements: falsity, causation, knowledge, and materiality.” [26]
References
- Biro JC. (2024). The “Politi-COVID (USA)” Epidemic in the “Pre-Election” America, 2020 and 2024. Bio Med. 16:731. Published: 17-Oct-2024. https://doi.org/10.35248/2375-446X.24.12.286. - https://www.walshmedicalmedia.com/open-access/the-ldquopoliticovid-usardquo-epidemic-in-the-ldquopreelectionrdquo-america-2020-and-2024-131327.html. [CrossRef]
- Jan Charles Biro* - Critical Review of the Diagnostic and Statistical Support for COVID Epidemic in USA - Journal of Environmental and Occupational Health, 2024 VOL 14, NO. 06, PAGE 01-08 - Published: 25-Oct-2024 – DOI: https://www.jenvoh.com/jenvoh-articles/critical-review-of-the-diagnostic-and-statistical-support- for-covid-epidemic-in-usa.pdf.
- Jan Charles Biro* Covidalism©®: COVID Restrictions in USA have no Health Benefits at all - J Community Med Health Educ. 2024; 14(5): - DOI: 10.4172/2161-0711.1000897 - https://www.omicsonline.org/open-access/covidalism-covid-restrictions-in-usa-have-no-health-benefits-at-all.pdf. [CrossRef]
- Biro JC (2024) Face Off: The Socio-Political Background of the COVID-19 Syndemic in USA. Health Sci J Vol.18 No.S12:001. : 22-Oct-2024. https://doi.org/10.36648/1791- 809X.18.S12.001- https://www.itmedicalteam.pl/articles/face-off-the-sociopolitical-background-of-the-covid19-syndemic-in-usa.pdf COVID-19 vs. flu: Similarities and differences - Mayo Clinic Staff - July 22, 2023 - https://www.mayoclinic.org/diseases-conditions/coronavirus/in-depth/coronavirus-vs-flu/art-20490339. [CrossRef]
- COVID waves: Europe and US compared – Pandemic - January 28, 2024 - https://pandem-ic.com/covid-waves- europe-and-us-compared/.
- Gates, B. Responding to COVID-19-a once in a century pandemic? N Engl J Med 2020, 382, 1677–1679. [Google Scholar] [CrossRef] [PubMed]
- John Ioannidis Warned COVID-19 Could Be a “Once-In-A-Century” Data Fiasco. – FEE - JULY 23, 2020 - https://fee.org/articles/john-ioannidis-warned-covid-19-could-be-a-once-in-a-century-data-fiasco-he-was-right/.
- USA Facts – How many people get the fly? (2023) https://usafacts.org/articles/how-many-people-die-flu/.
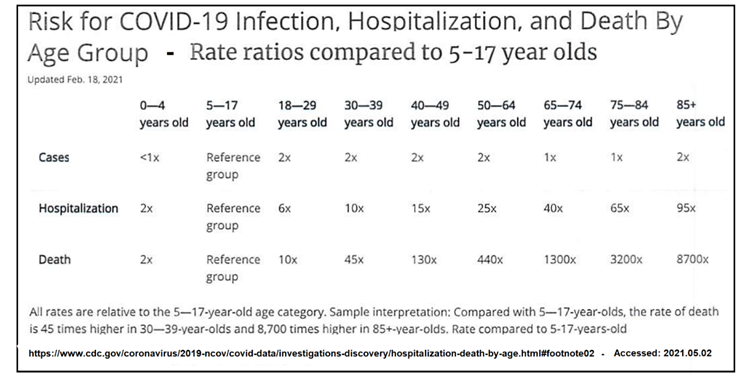
- Risk for COVID-19 Infection, Hospitalization, and Death By Age Group Source: CDC – https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-age.html#footnote02 - Accessed: 2021.05.02.
- Tracking Accountability in Government Grants System (TAGGS). Annual Reports - May 18, 2021 - https://taggs.hhs.gov/.
- Reporting and Audit Requirements for Provider Relief Fund Recipients – NONPROFIT STANDARD - March 16, 2021 - https://www.bdo.com/blogs/nonprofit-standard/march-2021/reporting-and-auditrequirements-for- provider-reli.
- U.S. Department of Health and Human Services - Reporting Requirements Policy Update - October 22, 2020 - https://www.hhs.gov/sites/default/files/reporting-requirements-policy-update.pdf.
- CARES Act Provider Relief Fund Frequently Asked Questions - Last updated: 4/1/2021 - https://www.hhs.gov/sites/default/files/provider-relief-fund-general-distribution-faqs.pdf.
- Acceptance of Terms and Conditions - https://www.hhs.gov/sites/default/files/terms-and-Conditions-phase-3-general-distribution-relief-fund.pdf - Accessed: 2021.05.30.
- New Waivers for Inpatient Prospective Payment System (IPPS) Hospitals, Long-Term Care Hospitals (LTCHs), and Inpatient Rehabilitation Facilities (IRFs) due to Provisions of the CARES Act – MLN Matters Number: SE20015, https://www.cms.gov/files/document/se20015.pdf.
- ICD-10-CM Official Coding and Reporting Guidelines -https://www.cdc.gov/nchs/data/icd/COVID-19-guidelines-final.pdf - ACCESSED: 2021.05.30.
- ICD-10-CM Official Coding Guideline – Supplement – https://www.cdc.gov/nchs/data/icd/ICD-10-CM-Official-odingGudance-Interim-Advice-coronavirus-feb-20-2020.pdf.
- New Waivers for Inpatient Prospective Payment System (IPPS) Hospitals, Long-Term Care Hospitals (LTCHs), and Inpatient Rehabilitation Facilities (IRFs) due to Provisions of the CARES Act - https://www.cms.gov/files/document/se20015.pdf - ACCESSED: 2021.05.30.
- ICD-10-CM Official Guidelines for Coding and Reporting FY - https://www.cdc.gov/nchs/data/icd/10cmguidelines-FY2021.pdf.
- IDEM, p. 29.
- National Center for Health Statistics. Guidance for certifying deaths due to COVID–19. Hyattsville, MD. 2020. Vital Statistics Reporting Guidance Rapport No. 3 April 2020.- https://www.cdc.gov/nchs/data/nvss/vsrg/vsrg03-508.Pdf.
- ICD-10-CM Official Guidelines for Coding and Reporting FY 2021 (October 1, 2020 - September 30, 2021) CHAPTER 1(g) (1) – CORONAVIRUS INFECTIONS - https://www.cdc.gov/nchs/data/icd/10cmguidelines-FY2021.pdf - Accessed: 2021.05.31.
- National Center for Health Statistics. Guidance for certifying deaths due to COVID–19. Hyattsville, MD. 2020.- https://stacks.cdc.gov/view/cdc/86344.
- Tyson Foods v. Bouaphakeo, 136 S. Ct. 1036, 1046 (2016).
- United States ex rel. Petratos v. Genentech Inc., 855 F.3d 481, 487 (3d Cir. 2017).
- Marshall, 812 F.3d at 561.
- See 31 U.S.C. § 3729.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



