
Submitted:
30 December 2024
Posted:
31 December 2024
You are already at the latest version
Abstract
The study examines the effects of metformin on brain functions focusing on the variability of results reported in the literature. While some studies suggest that metformin may have neuroprotective effects in diabetic patients, others report an insignificant impact of metformin on cognitive function, or even a negative effect. We propose that this inconsistency may be due to intrinsic cellular-level variability among individuals, which we term “biovariance”. Biovariance persists even in demographically homogeneous samples due to complex and stochastic biological processes. Additionally, the complex metabolic actions of metformin, including AMPK activation and mTOR inhibition, may produce different effects depending on individual metabolic characteristics.
Keywords:
metformin
; diabet
; cognition
; neuroprotection
; biovariance
1. Introduction
Metformin, a drug belonging to the biguanide class, is a widely prescribed medication for managing non-insulin-dependent type 2 diabetes mellitus (T2DM) and has garnered significant scientific attention due to its multifaceted effects on cellular metabolism and its emerging therapeutic potential in diverse areas of medicine. Its well-documented mechanisms, such as enhancing insulin sensitivity, reducing hepatic gluconeogenesis, and improving overall energy metabolism, have paved the way for research into a broad range of possible therapeutic applications [1], spanning from antitumor effects to roles in neuroplasticity and cognitive function. Additionally, metformin’s therapeutic potential has been evaluated in a variety of metabolic and endocrine disorders, such as polycystic ovary syndrome [2].
This growing interest in metformin has spurred numerous studies exploring its effects across various human pathologies, including cardiovascular and metabolic diseases [3,4], inflammatory conditions [5], processes associated with senescence and anti-aging properties [6], and psychiatric conditions [7]. This review examines the intriguing neuropsychiatric effects of metformin, with a focus on its influence on cognitive function and the underlying biocellular mechanisms that contribute to interindividual variation in its effects.
Cognitive decline is a well-recognized complication of diabetes [8], hypothesized to be driven by glycemic fluctuations and disruptions in neuronal metabolism. Similarly, there is documented evidence of a direct link between diabetes and structural changes in white matter integrity [9]. Existing studies, however, present mixed findings on metformin’s effect on cognitive function in both human and non-human subjects, with notable variations across specific population subgroups.
The present review aims to reconcile the conflicting effects of metformin on cognitive function by identifying the studies that report opposing results and proposing a possible biochemical explanation. Documentation of studies was performed through systematic searches of the PubMed and Google Scholar databases. To identify relevant studies, combinations of subject-specific terms were used: “metformin,” “diabetes,” “T2DM,” “white matter,” “cognition,” “dementia,” ”memory,” “inflammation,” “mechanism of action,” “neuro,” “molecular,” “cellular target,” “stroke,” and “endothelium.”
The search focused on articles published in recent years, employing truncation operators to broaden terminological coverage (e.g., “metformin,” “diabet*” “neuro*”, “cognit*”). The selection of studies was based on the following eligibility criteria:
Inclusion criteria: studies published after 2018 and written in English; studies specifically examining the impact of metformin treatment on cognitive function or neurodegenerative disorders; studies analyzing changes in brain structures; clinical trials; relevant preclinical studies; review articles and meta-analyses; studies investigating metformin’s mechanisms of action on inflammation and neurodegeneration.
Exclusion criteria: studies not analyzing the impact of metformin treatment on brain function, studies lacking clear differentiation between the effects of metformin and other oral antidiabetic drugs, studies in languages other than English, small observational studies without adequate control, or studies with notable methodological errors.
Studies investigating metformin’s mechanisms of action on inflammation and neurodegeneration, with emphasis on cellular signaling pathways and neuroprotective processes, were also included. In particular, meta-analyses and review articles were prioritized to provide a comprehensive overview of metformin’s effects.
Relevant articles were selected through a manual screening of search results, facilitating an in-depth evaluation of design characteristics of the identified studies (Figure 1). This approach allowed for a thorough assessment of inclusion and exclusion criteria, while also helping to mitigate the risk of overlooking relevant studies due to database indexing limitations.
In addition to the primary articles identified through the systematic search, additional references cited within the bibliographies of selected studies were reviewed. Preclinical animal studies examining metformin’s effects on neurobiological structures and cellular mechanisms were also included, as these studies offer complementary mechanistic insights to clinical data. Study assessments took into account design characteristics, statistical analysis methods, population sizes, and follow-up durations where applicable, with primary emphasis placed on the authors' conclusions. The Table 1 below provides an overview of the key studies exploring the impact of metformin.
2. Effects of Metformin on Metabolism and the Brain
Metformin is a first-line drug used in the treatment of type 2 diabetes. Its hypoglycemic effect is primarily attributed to a reduction in endogenous glucose production at the hepatic level by inhibiting gluconeogenesis [10]. However, other mechanisms have also been well documented, such as the improvement of insulin sensitivity in peripheral tissues, which promotes glucose utilization by muscles and other tissues. Among the proposed molecular mechanisms are the stimulation of cellular expression of the insulin-sensitive glucose transporter GLUT4 and the inhibition of SHIP2 enzyme activity [11,12,13,14]. The complete basis for the hypoglycemic effect of metformin has yet to be fully elucidated.
The bioavailability of metformin is relatively modest, ranging between 50-60% after oral administration [15]. Its absorption occurs primarily in the small intestine, is influenced by diet [16], and the drug is largely excreted unchanged by the kidneys. An essential characteristic of metformin is that it does not bind to plasma proteins and is not Mmetabolized by the liver. Metformin is widely distributed throughout body tissues. Furthermore, the unabsorbed portion of metformin (approximately 50%) can influence the intestinal microflora, with evidence showing that metformin affects the microbiome [17,18,19]. One study even suggests a possible correlation between an individual’s intestinal microbiome and their response to metformin [20].
Regarding metformin’s action on the brain, it is important to note that animal studies confirm its ability to cross the blood-brain barrier [21,22]. We emphasize that the permeability of the blood-brain barrier varies between species and, additionally, between individuals. Metformin concentrations in cerebrospinal fluid (CSF) are lower than in plasma, and studies measuring CSF concentrations in human subjects following oral administration are limited and address this issue only indirectly.
Metformin can influence cognitive function both directly and indirectly.
Indirectly, it can do so by reducing blood glucose and influencing metabolic functions. Chronic hyperglycemia is a major risk factor for cognitive decline and structural brain damage [23]. Numerous studies correlate diabetes with an increased risk of developing dementia or other cognitive disorders [24,25,26,27]. It should be noted that beyond the impact of glycemic fluctuations, diabetes is associated with other metabolic dysfunctions that negatively affect the brain. Additionally, metformin exhibits significant anti-inflammatory and antioxidant effects [28,29,30,31], which may partially counteract the oxidative stress and inflammation associated with high glycemic variability.
Diabetes is also a significant cardiovascular risk factor [32,33], and metformin has demonstrated a protective role on cardiovascular health as well as on vascular endothelium [34,35,36], which may contribute to its indirect effects on cognition.
Directly, there is evidence that metformin may exert neuroprotective effects by activating the AMPK pathway [37], which regulates cellular energy homeostasis. AMPK activation in brain neurons can promote neurogenesis, reduce inflammation, and improve mitochondrial function, all of which are important for cognitive health.
3. Effects of Metformin on Cognitive Function
Numerous studies have demonstrated the beneficial effects of metformin on cognitive function in patients with type 2 diabetes mellitus (T2DM), suggesting improvements in short-term memory, a reduced risk of developing dementia, and enhanced executive function [38,39,40,41,42,43,44,45,46,47]. One study identified interesting correlations between metformin, the gut microbiome, and the risk of developing dementia [48].
Regarding its multimodal impact on cognitive function, a recent animal study found a positive correlation between metformin and cognitive function (as measured by attention and inhibitory control) in young subjects [49], which shifted to a negative correlation in older subjects, suggesting an age-related effect on cognitive performance. Notably, two human studies reported more pronounced effects of metformin in Western populations [43,46], thereby raising the hypothesis that racial factors may influence the effects of metformin.
Interestingly, positive cognitive effects were also observed in patients with neuropsychiatric conditions. One study reported improvements in cognitive function and psychotic symptoms in patients with schizophrenia [50]. Similarly, studies indicate a possible anti-epileptic effect of metformin, suggesting it may modulate multiple factors implicated in the etiopathogenesis of epilepsy [51,52].
However, some research has suggested that the cognitive benefits of metformin may be time-limited, with a tendency to diminish or even reverse with long-term use. Additionally, some studies have shown no cognitive benefits from metformin treatment, including in the prevention of dementia [53,54], and others have even suggested an increased risk of Alzheimer's dementia associated with metformin use [55]. Furthermore, one study found a dose-related correlation, with lower doses linked to a reduced risk of developing dementia, while higher doses showed no benefit [56]. A similar correlation was observed in another study [57], led by the same primary author, specifically in the context of Parkinson’s disease.
Regarding other neurodegenerative conditions, results remain inconclusive. Some studies did not find any correlation between metformin use and the risk of developing Parkinson's disease [58], while one study suggested a possible association between metformin and an increased risk of Parkinson’s disease [59]. This finding partially contradicts other studies that suggest metformin may reduce the incidence and severity of neurodegenerative diseases [46,60]. The conflicting findings on metformin’s impact on Parkinson’s disease have been investigated in several studies [61], none of which have demonstrated a definitive effect. Interestingly, one study in animal models of Parkinson’s disease demonstrated a positive impact on motor function, potentially mediated by metformin’s effects on astrocytes [62].
Several studies have reported that metformin has a positive impact on cerebral white matter in diabetic individuals, helping to preserve white matter microarchitecture [60]. Long-term metformin use has been associated with increased white matter integrity and reduced diabetes-related brain volume loss in metformin-treated patients [63], particularly in regions such as the parietal lobes and cingulate cortex, which are involved in spatial orientation and memory processes. Moreover, a study based on fractional anisotropy measurements showed increased cerebral parenchymal integrity in diabetic patients treated with metformin [60]
In a murine model, one study hypothesized that metformin stimulates oligodendrocyte progenitor cells (OPCs) under hypoxic conditions [63]. Another animal study demonstrated metformin’s anti-inflammatory and neuroprotective properties against the neurotoxic effects of streptozotocin [64], a compound used to mimic Alzheimer’s dementia in animal experiments. Additionally, metformin administration counteracted neurotoxic effects from repeated alcohol exposure, indicating neuroprotective potential under toxic conditions [65].
The hypothesis that metformin acts as a cardiovascular protective factor has also been explored, and several studies have demonstrated its beneficial effects on endothelial function and its role in reducing oxidative stress at this level [66,67,68]. These findings may be crucial in understanding metformin's role in cognitive protection, particularly through the enhancement of cerebral circulation and the prevention of ischemic strokes. Similarly, several studies have reported a decrease in the incidence and severity of ischemic attacks among patients already undergoing treatment with metformin, as well as a positive association between metformin use and improved clinical outcomes [69,70,71].
Additionally, studies aimed at elucidating metformin’s mechanism of action at the biocellular level were identified. The primary cellular targets of metformin are illustrated in the Table 2. Although other cellular targets are not included due to challenges in defining metformin’s specific effects on them, these targets certainly play a role in explaining and understanding metformin's mechanism of action.
4. Biovariance: A New Frontier in Personalized Medicine
Interindividual variability is a well-documented concept in medical sciences, explaining differences in response to a particular treatment between individuals. In another sense, this reflects the axiom "each individual is unique". This variability accounts for the fact that a drug can exhibit a different action profile from one patient to another and may also cause adverse effects or allergic reactions in certain individuals. Clinical trials primarily assess general effects within a population, allowing conclusions to be drawn about efficacy, optimal dosage, and safety profile. Ultimately, a risk-benefit ratio is calculated, determining if the drug qualifies for therapeutic application
Interindividual variability arises from numerous factors, ranging from age, genetics, environmental influences to the intricate dynamics of chemical reactions within cells. Unlike other factors, cellular factors are challenging to use as population selection filters due to their stochastic and partly unpredictable nature. Biovariance addresses this type of variability, which cannot be eliminated by selection criteria but can be reduced if the criteria are adapted to target metabolic function. This approach enables a personalized therapeutic strategy and maximizes the therapeutic potential of drugs by identifying subgroups with a strong positive response.
Biovariance refers to the heterogeneity of a drug’s effect, characterizing the response to treatment rather than the substance itself. Its biological foundation lies in the complex dynamics of metabolic reactions occurring at the cellular level, which are influenced by the pre-existing biochemical context, competition for receptors, and subtle molecular interactions that generate stochastic behavior. Therefore, biovariance is fundamentally tied to how living organisms process and respond to a range of substances, reflecting the complexity of metabolic interactions that vary among individuals and even within the same individual. While biovariance is directly related to the complexity of a biological system, this relationship is not linear; as complexity increases, biovariance tends to increase exponentially. The brain is a striking example: due to the unique and highly varied organization of neuronal networks, synaptic plasticity, and the dynamic interactions between neurons, the central nervous system introduces an additional layer of variability in response to treatments. This is consistent with the findings of our study, which demonstrate the difficulty in establishing a clear effect of metformin on cognitive function based on the existing literature.
4.1. Role of Biovariance in Shaping Clinical Trial Design
We believe that one of the most significant consequences of accepting and validating the concept of biovariance would be a reorientation of clinical trial design. This would involve adapting selection criteria to include specific markers of cellular metabolism and selecting patients based on the characteristics of their metabolome. Such an approach would enable the development of new, relevant evaluation criteria for metabolic status, providing a more accurate picture of how patients respond to treatments according to their metabolic profiles and bringing us closer to the goal of truly personalized medicine.
Most medical studies aim to identify a correlation between the administration of a substance and the occurrence of a particular effect within a population. While these studies provide valuable clinical insights, their methodology often falls short when investigating effects with high biovariance. Ignoring inherent interindividual variability can lead to misinterpretations of the data and frequently results in the conclusion that further, larger studies are necessary. Acceptance of the biovariance concept could, therefore, help halt the "race" for ever-larger, costlier studies, as the biovariant drug effects of a drug will continue to differ among individuals. Consequently, even studies with substantial sample sizes, numbering in the hundreds of thousands of participants, may still fail to yield conclusive results. In contrast, a single, highly relevant study that identifies distinct or even opposing effects within a homogeneous sample, carefully selected based on well-defined criteria, could effectively reveal the biovariant nature of the effects.
The Figure 2 (reproducible via the functions described above right) illustrates a bimodal distribution model in comparison to a normal distribution, highlighting the limitations of statistical analysis when applied to abnormal distributions in identifying clinically valuable data.
4.2. Metabolic Profiling Drugs. Metabolic Markers
The most accessible methods for studying cellular metabolism involve measuring metabolic products in blood samples or, when feasible, in the pericellular space. In certain contexts, radioisotopes can be employed to trace metabolic pathways and provide detailed insights into cellular biochemical dynamics, although their use is typically restricted to preclinical research or specialized laboratory settings due to safety and regulatory limitations. Additional methods, such as advanced imaging techniques and fluorescence-based assays, can also provide indirect but valuable insights into metabolic activity.
Relatively new concepts, such as fluxomics [80], complement these methods by synthesizing data from multiple -omics fields .(e.g., genomics, proteomics, microbiomics etc.). Together, these methods provide a comprehensive toolkit for understanding the metabolic status of individuals, offering insights into intracellular activity, metabolic abnormalities associated with various pathologies, and the potential for customized treatment approaches. The totality of small molecules resulting from metabolic processes, known as metabolites, constitute the metabolome. Metabolome constitutes a promising resource in medical research [81,82,83], providing information about the metabolic status of a subject and enabling the understanding of the metabolic abnormalities associated with various pathologies, which can be used to customize treatment.
The metabolome also serves as a mirror of intracellular activity, reflecting changes that occur following the administration of a drug and providing an effective means of studying individual metabolic responses. Additionally, prior to drug administration, biologically inert substances that produce no effects in the body but allow for the evaluation of individual metabolic characteristics through the measurement of metabolic by-products could be utilized.
We could refer to these substances as metabolic profiling drugs. By using them, we could identify population subgroups that exhibit common metabolic patterns, subgroups which could later be selected for clinical studies adapted to their metabolic profile. In this way, conclusions could be drawn about the effects of a drug by referring to the metabolic response that the population subgroup presents to the administration of the profiling drug, a process illustrated in Figure 3:
An example of a drug that could be used for metabolic profiling is codeine. Codeine (methylmorphine) is a medication used to treat cough and pain. Its analgesic effect is primarily due to its conversion to morphine in the liver, a process mediated by the enzyme CYP2D6. This enzyme catalyzes the demethylation process, converting the methoxy group at position 3 of the aromatic ring into a hydroxyl group, resulting in morphine. Another metabolic pathway involves the enzyme CYP3A4, which transforms codeine by removing the methyl group from the nitrogen atom in codeine’s structure, producing norcodeine, an inactive metabolite in terms of analgesic effect. If CYP3A4 activity is predominant, less morphine is generated, leading to a weaker analgesic effect. Conversely, if CYP2D6 activity is dominant, more morphine is produced. This variability can result in significant heterogeneity in codeine’s effects, depending on individual metabolic characteristics.
CYP2D6 and CYP3A4 are part of the cytochrome P450 enzyme family, which is widely distributed across living organisms. These two enzymes play a role in the metabolism of a broad range of drugs [84,85,86], and differences in their activity contribute to variability in individual responses to a drug. Codeine’s role as a metabolic profiler is particularly important for drugs that are substrates for both CYP2D6 and CYP3A4, as identifying the predominance of one enzyme’s activity can significantly aid in treatment personalization. Enzyme activity is subject to multiple variations, and this must be interpreted in the context of the specific substrate, as activity depends on affinity, which describes the enzyme-substrate interaction.
It is important to acknowledge the limitations of this approach, as each enzyme has distinct affinities for different chemical structures. Therefore, a patient with predominant CYP2D6 activity for one drug may still experience more intensive metabolism via CYP3A4 for another drug, depending on the chemical structure of the drug. To address this challenge and provide a more comprehensive view of overall metabolism, it may be necessary for a metabolic profiling drug to exhibit enzyme polyspecificity, allowing metabolic variations to be correlated more accurately with changes in metabolite concentrations.
5. Conclusions
Based on our findings, we recommend reorienting the selection criteria in clinical trials for metformin and other medications that display a wide range of observed effects to include specific markers of cellular metabolism. Additionally, we call for the development of metabolic profiling drugs designed to tailor treatments to individual metabolic profiles.
Given that sufficient large-scale studies have confirmed variable effects of metformin on cognition, instead of undertaking more extensive research with large sample sizes, a focused strategy may more effectively elucidate underlying mechanism of the distinct effects of metformin across different subgroups. This approach could optimize resources by reducing the need for large, inconclusive studies, redirecting them towards investigations of individual responses.
By integrating biovariance into study design and developing metabolic profiling drugs to assess cellular metabolism, research can advance towards personalized medicine, maximizing both treatment effectiveness and the predictability of therapeutic outcomes. This approach could pave the way for more precise patient stratification in future metformin research and, more broadly, contribute to a deeper understanding of variability in drug response.
6. Limitations
This review has several limitations that may affect the interpretation of findings. First, the selection of studies in this review is limited due to our selection criteria, database limitations, or the exclusion of publications in languages other than English. Second, the heterogeneity of cognitive tests used in the analyzed studies complicates direct comparisons, as varied assessments may differ in sensitivity to metformin’s cognitive effects. Additionally, linguistic and cultural differences in test adaptations may introduce biases, affecting cross-study consistency.
The new concepts proposed to explain the effects of metformin, like biovariance, have not been validated through experimental or clinical studies, highlighting the need for further research to confirm and apply these ideas in practice. The interpretation of data and development of these concepts may be influenced by our own perspectives, introducing a potential subjective bias on the part of the authors.
Author Contributions
Conceptualization, D.C., MT, C.A.S. and AEM; methodology, D.C., M.T., M.M., and A.M.S.; software, D.C. and M.T.; validation, O.V., F.J.A., and D.M.; investigation, C.A.S., M.M., and D.M.; data curation, D.C., M.T., C.A.S., and A.E.M.; writing—original draft preparation, D.C., M.T., C.A.S., M.M., and A.E.M; writing—review and editing, O.V., A.M.S., and F.J.A.; su-pervision, M.M. and A.E.M.; project administration, D.C., M.T., and C.A.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding. The APC was funded by Carol Davila University of Medicine and Pharmacy, Bucharest, Romania through the institutional program Publish, not Perish.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data are reported in the text.
Conflicts of Interest
All authors declare that they have no conflicts of interest.
References
- Wu, H., Huang, D., Zhou, H., Sima, X., Wu, Z., Sun, Y., Wang, L., Ruan, Y., Wu, Q., Wu, F., She, T., Chu, Y., Huang, Q., Ning, Z., & Zhang, H. (2022). Metformin: A promising drug for human cancers. Oncology letters, 24(1), 204. [CrossRef]
- Attia, G. M., Almouteri, M. M., & Alnakhli, F. T. (2023). Role of Metformin in Polycystic Ovary Syndrome (PCOS)-Related Infertility. Cureus, 15(8), e44493. [CrossRef]
- Li, J. Z., & Li, Y. R. (2023). Cardiovascular Protection by Metformin: Latest Advances in Basic and Clinical Research. Cardiology, 148(4), 374–384. [CrossRef]
- Ziqubu, K., Mazibuko-Mbeje, S. E., Mthembu, S. X. H., Mabhida, S. E., Jack, B. U., Nyambuya, T. M., Nkambule, B. B., Basson, A. K., Tiano, L., & Dludla, P. V. (2023). Anti-Obesity Effects of Metformin: A Scoping Review Evaluating the Feasibility of Brown Adipose Tissue as a Therapeutic Target. International journal of molecular sciences, 24(3), 2227. [CrossRef]
- Feng, Y. Y., Wang, Z., & Pang, H. (2023). Role of metformin in inflammation. Molecular biology reports, 50(1), 789–798. [CrossRef]
- Mohammed, I., Hollenberg, M. D., Ding, H., & Triggle, C. R. (2021). A Critical Review of the Evidence That Metformin Is a Putative Anti-Aging Drug That Enhances Healthspan and Extends Lifespan. Frontiers in endocrinology, 12, 718942. [CrossRef]
- Battini, V., Cirnigliaro, G., Leuzzi, R., Rissotto, E., Mosini, G., Benatti, B., Pozzi, M., Nobile, M., Radice, S., Carnovale, C., Dell'Osso, B., & Clementi, E. (2023). The potential effect of metformin on cognitive and other symptom dimensions in patients with schizophrenia and antipsychotic-induced weight gain: a systematic review, meta-analysis, and meta-regression. Frontiers in psychiatry, 14, 1215807. [CrossRef]
- Xue, M., Xu, W., Ou, Y. N., Cao, X. P., Tan, M. S., Tan, L., & Yu, J. T. (2019). Diabetes mellitus and risks of cognitive impairment and dementia: A systematic review and meta-analysis of 144 prospective studies. Ageing research reviews, 55, 100944. [CrossRef]
- Wang, D. Q., Wang, L., Wei, M. M., Xia, X. S., Tian, X. L., Cui, X. H., & Li, X. (2020). Relationship Between Type 2 Diabetes and White Matter Hyperintensity: A Systematic Review. Frontiers in endocrinology, 11, 595962. [CrossRef]
- LaMoia, T. E., & Shulman, G. I. (2021). Cellular and Molecular Mechanisms of Metformin Action. Endocrine reviews, 42(1), 77–96. [CrossRef]
- Herman, R., Kravos, N. A., Jensterle, M., Janež, A., & Dolžan, V. (2022). Metformin and Insulin Resistance: A Review of the Underlying Mechanisms behind Changes in GLUT4-Mediated Glucose Transport. International journal of molecular sciences, 23(3), 1264. [CrossRef]
- Kaneto, H., Kimura, T., Obata, A., Shimoda, M., & Kaku, K. (2021). Multifaceted Mechanisms of Action of Metformin Which Have Been Unraveled One after Another in the Long History. International journal of molecular sciences, 22(5), 2596. [CrossRef]
- Polianskyte-Prause, Z., Tolvanen, T. A., Lindfors, S., Dumont, V., Van, M., Wang, H., Dash, S. N., Berg, M., Naams, J. B., Hautala, L. C., Nisen, H., Mirtti, T., Groop, P. H., Wähälä, K., Tienari, J., & Lehtonen, S. (2019). Metformin increases glucose uptake and acts renoprotectively by reducing SHIP2 activity. FASEB journal : official publication of the Federation of American Societies for Experimental Biology, 33(2), 2858–2869. [CrossRef]
- Lehtonen S. (2020). SHIPping out diabetes-Metformin, an old friend among new SHIP2 inhibitors. Acta physiologica (Oxford, England), 228(1), e13349. [CrossRef]
- Graham, G. G., Punt, J., Arora, M., Day, R. O., Doogue, M. P., Duong, J. K., Furlong, T. J., Greenfield, J. R., Greenup, L. C., Kirkpatrick, C. M., Ray, J. E., Timmins, P., & Williams, K. M. (2011). Clinical pharmacokinetics of metformin. Clinical pharmacokinetics, 50(2), 81–98. [CrossRef]
- Sun, M. L., Liu, F., Yan, P., Chen, W., & Wang, X. H. (2023). Effects of food on pharmacokinetics and safety of metformin hydrochloride tablets: A meta-analysis of pharmacokinetic, bioavailability, or bioequivalence studies. Heliyon, 9(7), e17906. [CrossRef]
- Ezzamouri, B., Rosario, D., Bidkhori, G., Lee, S., Uhlen, M., & Shoaie, S. (2023). Metabolic modelling of the human gut microbiome in type 2 diabetes patients in response to metformin treatment. NPJ systems biology and applications, 9(1), 2. [CrossRef]
- Induri, S. N. R., Kansara, P., Thomas, S. C., Xu, F., Saxena, D., & Li, X. (2022). The Gut Microbiome, Metformin, and Aging. Annual review of pharmacology and toxicology, 62, 85–108. [CrossRef]
- Zhang, Q., & Hu, N. (2020). Effects of Metformin on the Gut Microbiota in Obesity and Type 2 Diabetes Mellitus. Diabetes, metabolic syndrome and obesity : targets and therapy, 13, 5003–5014. [CrossRef]
- Elbere, I., Silamikelis, I., Dindune, I. I., Kalnina, I., Ustinova, M., Zaharenko, L., Silamikele, L., Rovite, V., Gudra, D., Konrade, I., Sokolovska, J., Pirags, V., & Klovins, J. (2020). Baseline gut microbiome composition predicts metformin therapy short-term efficacy in newly diagnosed type 2 diabetes patients. PloS one, 15(10), e0241338. [CrossRef]
- Thinnes, A., Westenberger, M., Piechotta, C., Lehto, A., Wirth, F., Lau, H., & Klein, J. (2021). Cholinergic and metabolic effects of metformin in mouse brain. Brain research bulletin, 170, 211–217. [CrossRef]
- Łabuzek, K., Suchy, D., Gabryel, B., Bielecka, A., Liber, S., & Okopień, B. (2010). Quantification of metformin by the HPLC method in brain regions, cerebrospinal fluid and plasma of rats treated with lipopolysaccharide. Pharmacological reports : PR, 62(5), 956–965. [CrossRef]
- Mortby, M. E., Janke, A. L., Anstey, K. J., Sachdev, P. S., & Cherbuin, N. (2013). High "normal" blood glucose is associated with decreased brain volume and cognitive performance in the 60s: the PATH through life study. PloS one, 8(9), e73697. [CrossRef]
- Xue, M., Xu, W., Ou, Y. N., Cao, X. P., Tan, M. S., Tan, L., & Yu, J. T. (2019). Diabetes mellitus and risks of cognitive impairment and dementia: A systematic review and meta-analysis of 144 prospective studies. Ageing research reviews, 55, 100944. [CrossRef]
- Sebastian, M. J., Khan, S. K., Pappachan, J. M., & Jeeyavudeen, M. S. (2023). Diabetes and cognitive function: An evidence-based current perspective. World journal of diabetes, 14(2), 92–109. [CrossRef]
- Dao, L., Choi, S., & Freeby, M. (2023). Type 2 diabetes mellitus and cognitive function: understanding the connections. Current opinion in endocrinology, diabetes, and obesity, 30(1), 7–13. [CrossRef]
- Cao, F., Yang, F., Li, J., Guo, W., Zhang, C., Gao, F., Sun, X., Zhou, Y., & Zhang, W. (2024). The relationship between diabetes and the dementia risk: a meta-analysis. Diabetology & metabolic syndrome, 16(1), 101. [CrossRef]
- Feng, Y. Y., Wang, Z., & Pang, H. (2023). Role of metformin in inflammation. Molecular biology reports, 50(1), 789–798. [CrossRef]
- Petrasca, A., Hambly, R., Kearney, N., Smith, C. M., Pender, E. K., Mac Mahon, J., O'Rourke, A. M., Ismaiel, M., Boland, P. A., Almeida, J. P., Kennedy, C., Zaborowski, A., Murphy, S., Winter, D., Kirby, B., & Fletcher, J. M. (2023). Metformin has anti-inflammatory effects and induces immunometabolic reprogramming via multiple mechanisms in hidradenitis suppurativa. The British journal of dermatology, 189(6), 730–740. [CrossRef]
- Buczyńska, A., Sidorkiewicz, I., Krętowski, A. J., & Adamska, A. (2024). Examining the clinical relevance of metformin as an antioxidant intervention. Frontiers in pharmacology, 15, 1330797. [CrossRef]
- Manica, D., Sandri, G., da Silva, G. B., Manica, A., da Silva Rosa Bonadiman, B., Dos Santos, D., Flores, É. M. M., Bolzan, R. C., Barcelos, R. C. S., Tomazoni, F., Suthovski, G., Bagatini, M. D., & Benvegnú, D. M. (2023). Evaluation of the effects of metformin on antioxidant biomarkers and mineral levels in patients with type II diabetes mellitus: A cross-sectional study. Journal of diabetes and its complications, 37(7), 108497. [CrossRef]
- Joseph, J. J., Deedwania, P., Acharya, T., Aguilar, D., Bhatt, D. L., Chyun, D. A., Di Palo, K. E., Golden, S. H., Sperling, L. S., & American Heart Association Diabetes Committee of the Council on Lifestyle and Cardiometabolic Health; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Clinical Cardiology; and Council on Hypertension (2022). Comprehensive Management of Cardiovascular Risk Factors for Adults With Type 2 Diabetes: A Scientific Statement From the American Heart Association. Circulation, 145(9), e722–e759. [CrossRef]
- Dal Canto, E., Ceriello, A., Rydén, L., Ferrini, M., Hansen, T. B., Schnell, O., Standl, E., & Beulens, J. W. (2019). Diabetes as a cardiovascular risk factor: An overview of global trends of macro and micro vascular complications. European journal of preventive cardiology, 26(2_suppl), 25–32. [CrossRef]
- Li, T., Providencia, R., Jiang, W., Liu, M., Yu, L., Gu, C., Chang, A. C. Y., & Ma, H. (2022). Association of Metformin with the Mortality and Incidence of Cardiovascular Events in Patients with Pre-existing Cardiovascular Diseases. Drugs, 82(3), 311–322. [CrossRef]
- Han, Y., Xie, H., Liu, Y., Gao, P., Yang, X., & Shen, Z. (2019). Effect of metformin on all-cause and cardiovascular mortality in patients with coronary artery diseases: a systematic review and an updated meta-analysis. Cardiovascular diabetology, 18(1), 96. [CrossRef]
- Salvatore, T., Pafundi, P. C., Galiero, R., Rinaldi, L., Caturano, A., Vetrano, E., Aprea, C., Albanese, G., Di Martino, A., Ricozzi, C., Imbriani, S., & Sasso, F. C. (2020). Can Metformin Exert as an Active Drug on Endothelial Dysfunction in Diabetic Subjects?. Biomedicines, 9(1), 3. [CrossRef]
- Ameen, O., Samaka, R. M., & Abo-Elsoud, R. A. A. (2022). Metformin alleviates neurocognitive impairment in aging via activation of AMPK/BDNF/PI3K pathway. Scientific reports, 12(1), 17084. [CrossRef]
- Li, X., Yuan, J., Han, J., Hu, W., Li, L., Zhang, L., ... & Wang, Y. (2021). Long-Term Use of Metformin Is Associated With Reduced Risk of Cognitive Impairment With Alleviation of Cerebral Small Vessel Disease Burden in Patients With Type 2 Diabetes. Frontiers in Aging Neuroscience, 13, 773797. [CrossRef]
- Samaras, K., Makkar, S., Crawford, J. D., Kochan, N. A., Wen, W., Draper, B., ... & Sachdev, P. S. (2020). Metformin Use Is Associated With Slowed Cognitive Decline and Reduced Incident Dementia in Older Adults With Type 2 Diabetes: The Sydney Memory and Ageing Study. Diabetes Care, 43(11), 2691–2701. [CrossRef]
- Tang, X., Brinton, R. D., Chen, Z., Farland, L. V., Klimentidis, Y., Migrino, R., ... & Zhou, J. J. (2022). Use of oral diabetes medications and the risk of incident dementia in U.S. veterans aged ≥60 years with type 2 diabetes. BMJ Open Diabetes Research & Care, 10(5), e002894. [CrossRef]
- Hui, S. C., Chan, J. C., Ma, R. C., Chow, E. Y., Tang, C., & Lam, V. C. (2024). Metformin use is associated with lower risks of dementia, anxiety, and depression: The Hong Kong Diabetes Study. Journal of Diabetes Research, 2024, 377322485.
- Tang, H., Guo, J., Shaaban, C. E., Feng, Z., Wu, Y., ... & Bian, J. (2024). Heterogeneous treatment effects of metformin on risk of dementia in patients with type 2 diabetes: A longitudinal observational study. Alzheimer's & Dementia, 20(2), 975–985. [CrossRef]
- Defo, A. K., Bakula, V., Pisaturo, A., Labos, C., Wing, S. S., & Daskalopoulou, S. S. (2024). Diabetes, antidiabetic medications and risk of dementia: A systematic umbrella review and meta-analysis. Diabetes, Obesity and Metabolism, 26(2), 441-462. [CrossRef]
- Doran, W., Tunnicliffe, L., Muzambi, R., Rentsch, C. T., Bhaskaran, K., & Warren-Gash, C. (2024). Incident dementia risk among patients with type 2 diabetes receiving metformin versus alternative oral glucose-lowering therapy: An observational cohort study using UK primary healthcare records. BMJ Open Diabetes Research & Care, 12(1), e003548. [CrossRef]
- Teng, Z., Feng, J., Qi, Q., Dong, Y., Xiao, Y., Xie, X., Meng, N., Chen, H., Zhang, W., & Lv, P. (2021). Long-term use of metformin is associated with reduced risk of cognitive impairment with alleviation of cerebral small vessel disease burden in patients with type 2 diabetes. Frontiers in Aging Neuroscience, 13, 773797. [CrossRef]
- Zhang, Q.-Q., Li, W.-S., Liu, Z., Zhang, H.-L., Ba, Y.-G., & Zhang, R.-X. (2020). Metformin therapy and cognitive dysfunction in patients with type 2 diabetes: A meta-analysis and systematic review. Medicine (Baltimore), 99(10), e19378. [CrossRef]
- Zheng, B., Su, B., Ahmadi-Abhari, S., Kapogiannis, D., Tzoulaki, I., Riboli, E., & Middleton, L. (2023). Dementia risk in patients with type 2 diabetes: Comparing metformin with no pharmacological treatment. Alzheimer's & Dementia, 19(12), 5681-5689. [CrossRef]
- Rosell-Díaz, M., & Fernández-Real, J. M. (2024). Metformin, cognitive function, and changes in the gut microbiome. Endocrine Reviews, 45(2), 210–226. [CrossRef]
- Cho, S. Y., Kim, E. W., Park, S. J., Phillips, B. U., Jeong, J., Kim, H., ... & Kim, E. (2024). Reconsidering repurposing: long-term metformin treatment impairs cognition in Alzheimer's model mice. Translational Psychiatry, 14(1), 34. [CrossRef]
- Shao, T., Huang, J., Zhao, Y., Wang, W., Tian, X., Hei, G., ... & Wu, R. (2023). Metformin improves cognitive impairment in patients with schizophrenia: associated with enhanced functional connectivity of dorsolateral prefrontal cortex. Translational Psychiatry, 13, 315. [CrossRef]
- Alnaaim, S. A., Al-Kuraishy, H. M., Al-Gareeb, A. I., Ali, N. H., Alexiou, A., Papadakis, M., ... & Batiha, G. E. (2023). New insights on the potential anti-epileptic effect of metformin: Mechanistic pathway. Journal of Cellular and Molecular Medicine, 27(24), 3953-3965. [CrossRef]
- Singh, R., Sarangi, S. C., & Tripathi, M. (2022). A review on role of metformin as a potential drug for epilepsy treatment and modulation of epileptogenesis. Seizure, 101, 253-261. [CrossRef]
- Malazy, O. T., Bandarian, F., Qorbani, M., Mohseni, S., Mirsadeghi, S., Peimani, M., & Larijani, B. (2022). The effect of metformin on cognitive function: A systematic review and meta-analysis. Journal of Psychopharmacology, 36(6), 666-679. [CrossRef]
- Xue, Y., & Xie, X. (2023). The association between metformin use and risk of developing severe dementia among AD patients with type 2 diabetes. Biomedicines, 11(11), 2935. [CrossRef]
- Ha, J., Choi, D.-W., Kim, K. J., Cho, S. Y., Kim, H., Kim, K. Y., Koh, Y., Nam, C. M., & Kim, E. (2021). Association of metformin use with Alzheimer's disease in patients with newly diagnosed type 2 diabetes: a population-based nested case-control study. Scientific Reports, 11(1), 24069. [CrossRef]
- Huang, K.-H., Tsai, Y.-F., Lee, C. B., Gau, S.-Y., Tsai, T.-H., Chung, N.-J., & Lee, C.-Y. (2023). The correlation between metformin use and incident dementia in patients with new-onset diabetes mellitus: A population-based study. Journal of Personalized Medicine, 13(5), 738. [CrossRef]
- Huang, K. H., Chang, Y. L., Gau, S. Y., Tsai, T. H., & Lee, C. Y. (2022). Dose-Response Association of Metformin with Parkinson's Disease Odds in Type 2 Diabetes Mellitus. Pharmaceutics, 14(5), 946. [CrossRef]
- Newby, D., Linden, A. B., Fernandes, M., Molero, Y., Winchester, L., Sproviero, W., ... & Nevado-Holgado, A. J. (2022). Comparative effect of metformin versus sulfonylureas with dementia and Parkinson's disease risk in U.S. patients over 50 with type 2 diabetes mellitus. BMJ Open Diabetes Research & Care, 10(5), e003036. [CrossRef]
- Ping, F., Jiang, N., & Li, Y. (2020). Association between metformin and neurodegenerative diseases: A systematic review and meta-analysis. BMJ Open Diabetes Research & Care, 8(1), e001370. [CrossRef]
- Abbaszadeh, S., Raei Dehaghi, G., Ghahri Lalaklou, Z., Beig Verdi, H., Emami, D., & Dalvandi, B. (2023). Metformin attenuates white matter microstructural changes in Alzheimer’s disease. Neurology Letters, 3(2), 39. [CrossRef]
- Agostini, F., Masato, A., Bubacco, L., & Bisaglia, M. (2021). Metformin Repurposing for Parkinson Disease Therapy: Opportunities and Challenges. International journal of molecular sciences, 23(1), 398. [CrossRef]
- Ryu, Y. K., Go, J., Park, H. Y., Choi, Y. K., Seo, Y. J., Choi, J. H., Rhee, M., Lee, T. G., Lee, C. H., & Kim, K. S. (2020). Metformin regulates astrocyte reactivity in Parkinson's disease and normal aging. Neuropharmacology, 175, 108173. [CrossRef]
- He, Y., Li, Z., Shi, X., Ding, J., & Wang, X. (2023). Metformin attenuates white matter injury and cognitive impairment induced by chronic cerebral hypoperfusion. Journal of Cerebral Blood Flow & Metabolism, 43(2 Suppl), 78–94. [CrossRef]
- Rabieipoor, S., Zare, M., Ettcheto, M., Camins, A., & Javan, M. (2023). Metformin restores cognitive dysfunction and histopathological deficits in an animal model of sporadic Alzheimer's disease. Heliyon, 9(7), e17873. [CrossRef]
- Baradaran, Z., Vakilian, A., Zare, M., Hashemzehi, M., Hosseini, M., Dinpanah, H., & Beheshti, F. (2021). Metformin improved memory impairment caused by chronic ethanol consumption: Role of oxidative stress and neuroinflammation. Behavioral Brain Research, 411, 113399. [CrossRef]
- Ding, Y., Zhou, Y., Ling, P., Feng, X., Luo, S., Zheng, X., Little, P. J., Xu, S., & Weng, J. (2021). Metformin in cardiovascular diabetology: a focused review of its impact on endothelial function. Theranostics, 11(19), 9376–9396. [CrossRef]
- Salvatore, T., Pafundi, P. C., Galiero, R., Rinaldi, L., Caturano, A., Vetrano, E., & Sasso, F. C. (2021). Can metformin exert as an active drug on endothelial dysfunction in diabetic subjects? Biomedicines, 9(1), 3. [CrossRef]
- Liu, J., Aylor, K. W., Chai, W., Barrett, E. J., & Liu, Z. (2022). Metformin prevents endothelial oxidative stress and microvascular insulin resistance during obesity development in male rats. American Journal of Physiology-Endocrinology and Metabolism, 322(3), E293-E306. [CrossRef]
- Paridari, P., Jabermoradi, S., Gholamzadeh, R., Vazifekhah, S., Vazirizadeh-Mahabadi, M., Roshdi Dizaji, S., & Yousefifard, M. (2023). Can metformin use reduce the risk of stroke in diabetic patients? A systematic review and meta-analysis. Diabetes & Metabolic Syndrome, 17(2), 102721. [CrossRef]
- Akhtar, N., Singh, R., Kamran, S., Babu, B., Sivasankaran, S., Joseph, S., & Shuaib, A. (2022). Chronic metformin treatment and outcome following acute stroke. Frontiers in Neurology, 13, 849607. [CrossRef]
- Tu, W.-J., Liu, Z., Chao, B.-H., Yan, F., Ma, L., Cao, L., & Ji, X.-M. (2022). Metformin use is associated with low risk of case fatality and disability rates in first-ever stroke patients with type 2 diabetes. Therapeutic Advances in Chronic Disease, 13, 20406223221076894. [CrossRef]
- Zhang, Y. M., Zong, H. C., Qi, Y. B., Chang, L. L., Gao, Y. N., Zhou, T., Yin, T., Liu, M., Pan, K. J., Chen, W. G., Guo, H. R., Guo, F., Peng, Y. M., Wang, M., Feng, L. Y., Zang, Y., Li, Y., & Li, J. (2023). Anxiolytic effect of antidiabetic metformin is mediated by AMPK activation in mPFC inhibitory neurons. Molecular psychiatry, 28(9), 3955–3965. [CrossRef]
- Li, J., Zhang, B., Liu, W. X., Lu, K., Pan, H., Wang, T., Oh, C. D., Yi, D., Huang, J., Zhao, L., Ning, G., Xing, C., Xiao, G., Liu-Bryan, R., Feng, S., & Chen, D. (2020). Metformin limits osteoarthritis development and progression through activation of AMPK signalling. Annals of the rheumatic diseases, 79(5), 635–645. [CrossRef]
- Apostolova, N., Iannantuoni, F., Gruevska, A., Muntane, J., Rocha, M., & Victor, V. M. (2020). Mechanisms of action of metformin in type 2 diabetes: Effects on mitochondria and leukocyte-endothelium interactions. Redox biology, 34, 101517. [CrossRef]
- Martín-Rodríguez, S., de Pablos-Velasco, P., & Calbet, J. A. L. (2020). Mitochondrial Complex I Inhibition by Metformin: Drug-Exercise Interactions. Trends in endocrinology and metabolism: TEM, 31(4), 269–271. [CrossRef]
- Feng, J., Wang, X., Ye, X., Ares, I., Lopez-Torres, B., Martínez, M., Martínez-Larrañaga, M. R., Wang, X., Anadón, A., & Martínez, M. A. (2022). Mitochondria as an important target of metformin: The mechanism of action, toxic and side effects, and new therapeutic applications. Pharmacological research, 177, 106114. [CrossRef]
- Guo, X., Li, X., Yang, W., Liao, W., Shen, J. Z., Ai, W., Pan, Q., Sun, Y., Zhang, K., Zhang, R., Qiu, Y., Dai, Q., Zheng, H., & Guo, S. (2021). Metformin Targets Foxo1 to Control Glucose Homeostasis. Biomolecules, 11(6), 873. [CrossRef]
- Cao, G., Gong, T., Du, Y., Wang, Y., Ge, T., & Liu, J. (2022). Mechanism of metformin regulation in central nervous system: Progression and future perspectives. Biomedicine & pharmacotherapy = Biomedecine & pharmacotherapie, 156, 113686. [CrossRef]
- Van Nostrand, J. L., Hellberg, K., Luo, E. C., Van Nostrand, E. L., Dayn, A., Yu, J., Shokhirev, M. N., Dayn, Y., Yeo, G. W., & Shaw, R. J. (2020). AMPK regulation of Raptor and TSC2 mediate metformin effects on transcriptional control of anabolism and inflammation. Genes & development, 34(19-20), 1330–1344. [CrossRef]
- Emwas, A. H., Szczepski, K., Al-Younis, I., Lachowicz, J. I., & Jaremko, M. (2022). Fluxomics - New Metabolomics Approaches to Monitor Metabolic Pathways. Frontiers in pharmacology, 13, 805782. [CrossRef]
- Schmidt, D. R., Patel, R., Kirsch, D. G., Lewis, C. A., Vander Heiden, M. G., & Locasale, J. W. (2021). Metabolomics in cancer research and emerging applications in clinical oncology. CA: a cancer journal for clinicians, 71(4), 333–358. [CrossRef]
- Alarcon-Barrera, J. C., Kostidis, S., Ondo-Mendez, A., & Giera, M. (2022). Recent advances in metabolomics analysis for early drug development. Drug discovery today, 27(6), 1763–1773. [CrossRef]
- Gonzalez-Covarrubias, V., Martínez-Martínez, E., & Del Bosque-Plata, L. (2022). The Potential of Metabolomics in Biomedical Applications. Metabolites, 12(2), 194. [CrossRef]
- Wang, D., Guo, Y., Wrighton, S. A., Cooke, G. E., & Sadee, W. (2011). Intronic polymorphism in CYP3A4 affects hepatic expression and response to statin drugs. The pharmacogenomics journal, 11(4), 274–286. [CrossRef]
- Zhou, S. F., Xue, C. C., Yu, X. Q., Li, C., & Wang, G. (2007). Clinically important drug interactions potentially involving mechanism-based inhibition of cytochrome P450 3A4 and the role of therapeutic drug monitoring. Therapeutic drug monitoring, 29(6), 687–710. [CrossRef]
- Zhou S. F. (2009). Polymorphism of human cytochrome P450 2D6 and its clinical significance: Part I. Clinical pharmacokinetics, 48(11), 689–723. [CrossRef]
Figure 1.
This diagram illustrates the selection and analysis process of the studies.
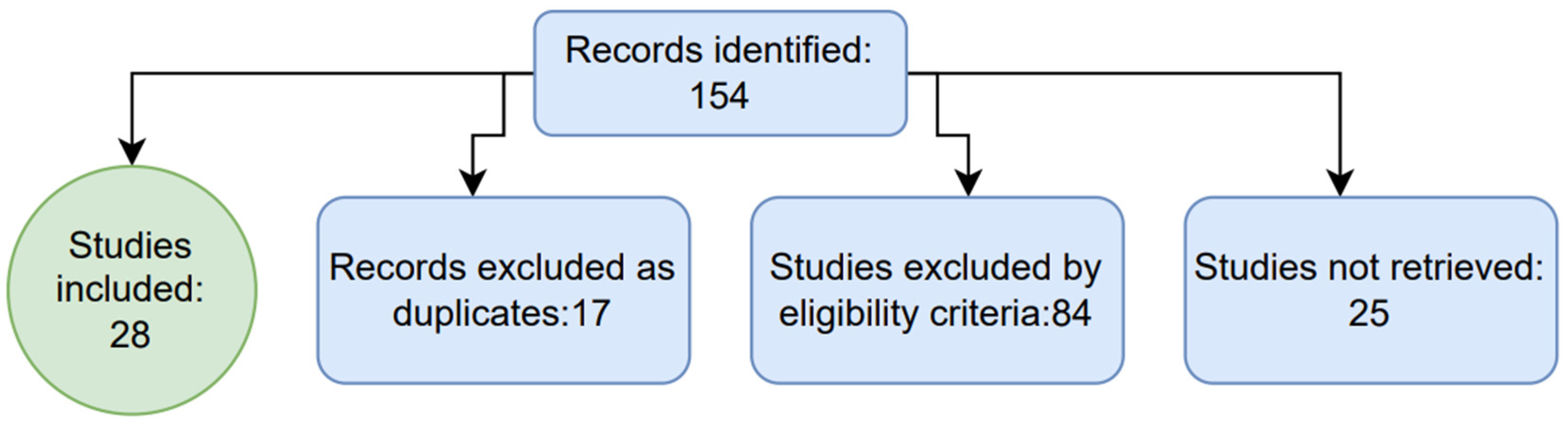
Figure 2.
The red line (corresponding to the function f(x)) represents a bimodal distribution, suggesting two subgroups within the population, each with a different response profile or characteristic. In contrast, the black line, denoted as f1(x), illustrates a unimodal, normal (Gaussian) distribution. This distribution reflects a homogeneous response pattern with values clustering symmetrically around the mean. The blue vertical line marks the shared mean of the two functions, underscoring a key limitation: while mean is common to both distributions, it fails to capture the unique characteristics of each distribution.
Figure 2.
The red line (corresponding to the function f(x)) represents a bimodal distribution, suggesting two subgroups within the population, each with a different response profile or characteristic. In contrast, the black line, denoted as f1(x), illustrates a unimodal, normal (Gaussian) distribution. This distribution reflects a homogeneous response pattern with values clustering symmetrically around the mean. The blue vertical line marks the shared mean of the two functions, underscoring a key limitation: while mean is common to both distributions, it fails to capture the unique characteristics of each distribution.
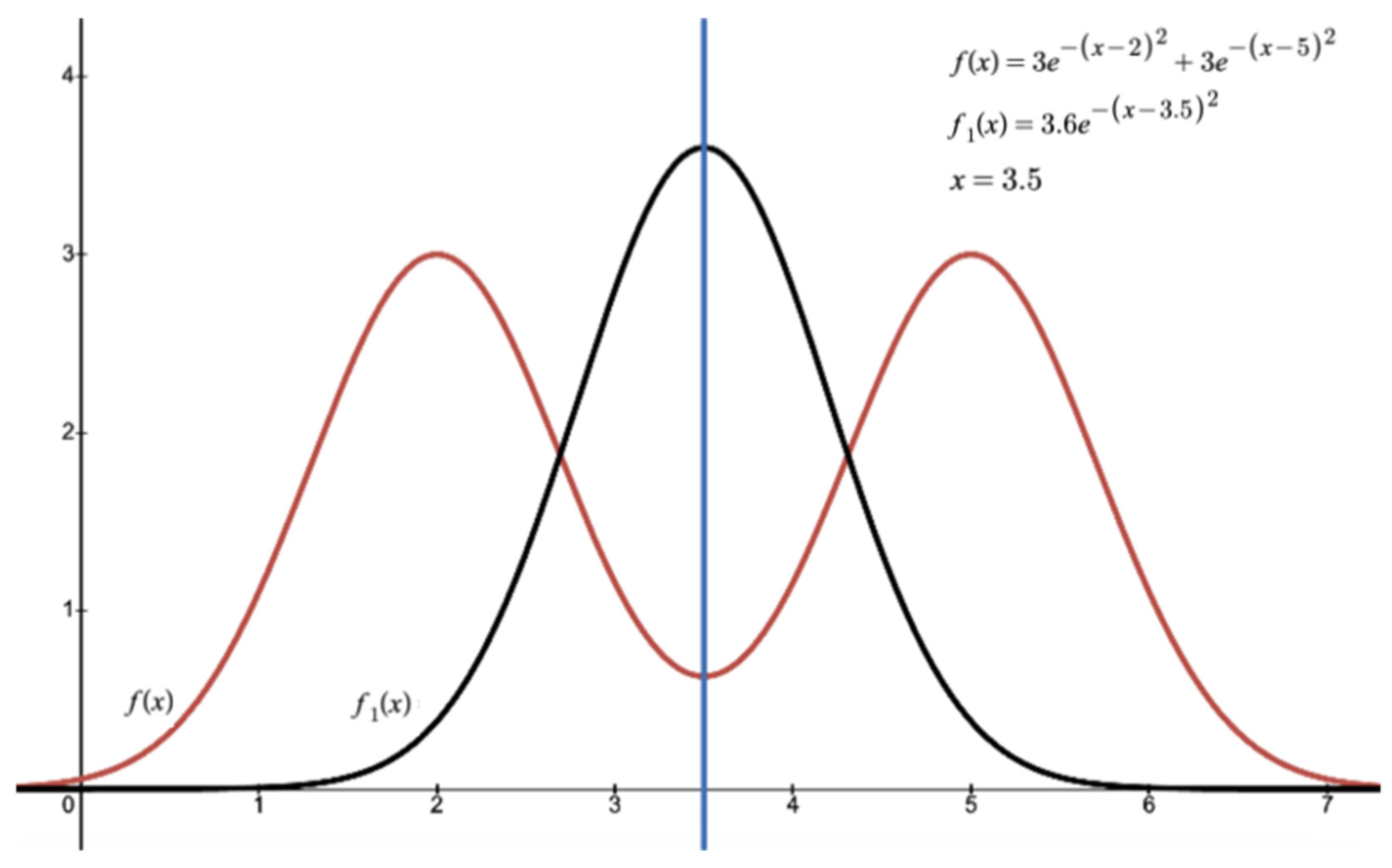
Figure 3.
This diagram illustrates how individual metabolic variations, represented by their metabolic products (the primary metabolites Y and Z) resulting from the administration of Drug X, could predict a patient’s response to the subsequent administration of another drug. Consequently, the administration of Drug A may lead to different effects, either favorable or unfavorable, depending on the predominant metabolite.
Figure 3.
This diagram illustrates how individual metabolic variations, represented by their metabolic products (the primary metabolites Y and Z) resulting from the administration of Drug X, could predict a patient’s response to the subsequent administration of another drug. Consequently, the administration of Drug A may lead to different effects, either favorable or unfavorable, depending on the predominant metabolite.
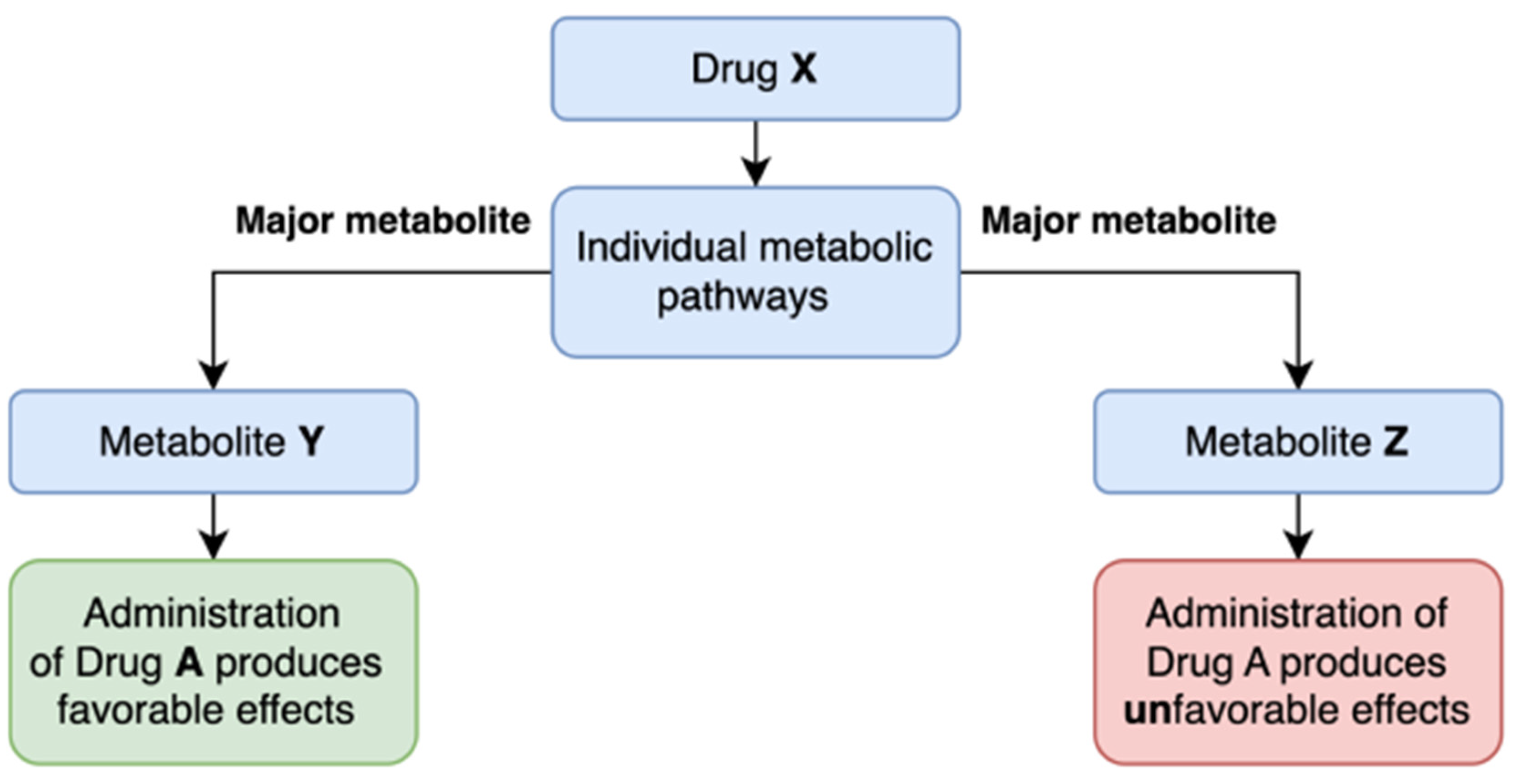

Table 1.
Summary of key studies addressing metformin's effects.
| Ref. No. | Study Title | Objective | Methodoly | Conclusion |
| [38] | Long-Term Use of Metformin Is Associated With Reduced Risk of Cognitive Impairment With Alleviation of Cerebral Small Vessel Disease Burden in Patients With Type 2 Diabetes | Evaluate the relationship between metformin use, cognitive impairment, and cerebral small vessel disease (CSVD) in type 2 diabetes patients | Cross-sectional study of patients with type 2 diabetes; | Long-term metformin use was associated with reduced cognitive decline |
| [39] | Metformin Use Is Associated With Slowed Cognitive Decline and Reduced Incident Dementia in Older Adults With Type 2 Diabetes: The Sydney Memory and Ageing Study | Evaluate if metformin use in older adults with type 2 diabetes is linked to a slower cognitive decline and lower incidence of dementia. | Prospective study comparing metformin users to non-users and non-diabetics over 6 years | Metformin users showed significantly slower decline in global cognition and executive function compared to non-users. Metformin also reduced dementia risk compared to non-users |
| [46] | Metformin Therapy and Cognitive Dysfunction in Patients With Type 2 Diabetes: A Meta-Analysis and Systematic Review | Assessing the association between metformin therapy and cognitive dysfunction in type 2 diabetes patients | Meta-analysis of observational studies | Metformin therapy is linked to a reduced risk of neurodegenerative diseases, although effects vary based on treatment duration |
| [60] | Metformin Attenuates White Matter Microstructural Changes in Alzheimer’s Disease | Examine metformin’s effect on white matter microstructural integrity in non-demented diabetic individuals | Study of non-demented diabetic subjects, divided into metformin users and non-users | Metformin users showed higher fractional anisotropy (FA) in the left hippocampal cingulum and right internal capsule, suggesting reduced neurodegeneration compared to non-users. |
| [48] | Metformin, Cognitive Function, and Changes in the Gut Microbiome | To explore the impact of metformin on cognitive function and gut microbiome in T2DM | Review of human studies, focusing on microbiome changes, cognitive function, and metabolic implications related to metformin | Metformin was shown to partially restore gut dysbiosis related to diabetes and may reduce dementia risk, although study results were not entirely consistent. |
| [40] | Use of Oral Diabetes Medications and the Risk of Incident Dementia in U.S. Veterans Aged ≥60 Years With Type 2 Diabetes | Assess dementia risk among veterans with type 2 diabetes using different drugs, including metformin | Observational study. Dementia risk comparison among those on metformin, sulfonylurea (SU), or thiazolidinedione (TZD) | Metformin alone had a moderate protective effect against dementia |
| [63] | Metformin Attenuates White Matter Injury and Cognitive Impairment Induced by Chronic Cerebral Hypoperfusion | Examine metformin's impact on white matter integrity and cognitive impairment under chronic hypoperfusion conditions | Mouse model of chronic cerebral hypoperfusion | Metformin reduced white matter damage and improved cognitive function by preserving oligodendrocyte function |
| [58] | Comparative Effect of Metformin Versus Sulfonylureas With Dementia and Parkinson's Disease Risk in U.S. Patients Over 50 With Type 2 Diabetes Mellitus | To assess the dementia and Parkinson's disease risks in older adults with type 2 diabetes (metformin compared to sulfonylureas) | Study on metformin users and sulfonylurea users over a 5-year follow-up | MET users had a lower risk of all-cause dementia, Alzheimer's disease, and vascular dementia compared to SU users.No significant difference for Parkinson's disease. |
| [53] | The Effect of Metformin on Cognitive Function: A Systematic Review and Meta-Analysis | Assess the relationship between metformin therapy and cognitive performance | Systematic review and meta-analysis of 19 studies | Metformin therapy showed no significant improvement in cognitive function or protection against dementia |
| [56] | The Correlation Between Metformin Use and Incident Dementia in Patients with New-Onset Diabetes Mellitus: A Population-Based Study | Examine the association between metformin use and dementia risk in patients with T2DM | Population-based study with 3- and 5-year follow-ups, categorizing patients by cumulative defined daily dose of metformin | Low-intensity metformin use was associated with a reduced dementia risk, while higher doses showed no protective effect. |
| [41] | Metformin Use Is Associated With Lower Risks of Dementia, Anxiety, and Depression: The Hong Kong Diabetes Study | Evaluate the effects of metformin on dementia, anxiety, and depression risks in diabetic patients | Retrospective cohort study | Metformin use was linked to significantly reduced risks of dementia, anxiety, and depression |
| [42] | Heterogeneous Treatment Effects of Metformin on Risk of Dementia in Patients with Type 2 Diabetes: A Longitudinal Observational Study | To evaluate varied effects of metformin on dementia risk in T2DM patients | Longitudinal study on participants aged ≥50 with normal cognition at baseline | Metformin was linked to a reduced overall dementia risk, with varied effects across subgroups |
| [43] | Diabetes, Antidiabetic Medications and Risk of Dementia: A Systematic Umbrella Review and Meta-Analysis | Study the impact of diabetes and antidiabetic drugs on dementia risk | Systematic review and meta-analysis of 100 reviews and 27 cohort/case-control studies | MET, TZD, pioglitazone, GLP1 receptor agonists, and SGLT2 inhibitors significantly reduced dementia risk, particularly in Western populations. |
| [44] | Incident Dementia Risk Among Patients with Type 2 Diabetes Receiving Metformin Versus Alternative Oral Glucose-Lowering Therapy | To assess the dementia and mild cognitive impairment risks in T2DM patients using metformin versus other oral hypoglycemic drugs | Observational cohort study using UK primary healthcare records | Metformin use was associated with a 14% lower risk of dementia, with a more pronounced effect in patients under 80 |
| [45] | Long-Term Use of Metformin Is Associated With Reduced Risk of Cognitive Impairment With Alleviation of Cerebral Small Vessel Disease Burden in Patients With Type 2 Diabetes | Investigate metformin’s effects on cognitive impairment and cerebral small vessel disease (CSVD) in patients with type 2 diabetes | Case-control study | Metformin was associated with reduced cognitive impairment risk |
| [54] | The Association Between Metformin Use and Risk of Developing Severe Dementia Among AD Patients with Type 2 Diabetes | Study the link between metformin use and severe dementia risk in Alzheimer’s patients with T2DM | Cohort study. Compared metformin users and non-users over 3.6 years | No significant association between metformin use and reduced severe dementia risk |
| [49] | Reconsidering Repurposing: Long-Term Metformin Treatment Impairs Cognition in Alzheimer's Model Mice | Evaluate effects of long-term metformin treatment on cognitive function in Alzheimer’s model mice | The study examines the cognitive domains in transgenic and non-transgenic mice after 1 and 2 years of metformin treatment. | Metformin enhanced cognition in younger mice but impaired learning and memory in older AD model mice, increasing amyloid pathology and tau protein phosphorylation |
| [64] | Metformin Restores Cognitive Dysfunction and Histopathological Deficits in an Animal Model of Sporadic Alzheimer's Disease | Evaluate the therapeutic effects of metformin in a Alzheimer’s mice model | Alzheimer’s disease induced in mice using streptozotocin; treated with metformin, assessed with memory/cognitive tests and histopathological analysis | Metformin reduced neuroinflammation, preserved neuron integrity, and improved memory in Alzheimer's model mice |
| [59] | Association Between Metformin and Neurodegenerative Diseases: A Systematic Review and Meta-Analysis | Evaluate the effect of metformin on the incidence of neurodegenerative diseases (NDs), including dementia and Parkinson disease | Systematic review and meta-analysis of 19 observational studies with 285,966 participants | Metformin showed no significant protective effect on overall NDs. However, metformin monotherapy was linked to an increased Parkinson’s risk compared to non-metformin |
| [65] | Metformin Improved Memory Impairment Caused by Chronic Ethanol Consumption | Investigate the protective effects of metformin on memory impairment and oxidative stress caused by chronic ethanol exposure in adolescent rats | Adolescent rats were given ethanol with varying doses of metformin; memory and biochemical markers were assessed | Metformin reduced oxidative stress and neuroinflammation, preserving memory function in ethanol-exposed rats |
| [47] | Dementia Risk in Patients With Type 2 Diabetes: Comparing Metformin With No Pharmacological Treatment | Compare dementia risk in T2DM patients treated with metformin versus those untreated | Observational cohort study | MET users showed a 12% lower dementia risk compared to untreated patients, with long-term users experiencing the greatest reduction |
| [50] | Metformin Improves Cognitive Impairment in Patients With Schizophrenia: Enhanced Functional Connectivity of the Dorsolateral Prefrontal Cortex | Investigate metformin’s effects on cognitive impairment and brain connectivity in patients with schizophrenia | Open-label, evaluator-blinded study on 72 schizophrenia patients randomized to metformin plus antipsychotics or antipsychotics alone | Metformin combined with antipsychotics improved cognitive scores significantly |
| [51] | New Insights on the Potential Anti-Epileptic Effect of Metformin: Mechanistic Pathway | Investigate metformin’s anti-seizure effects and underlying mechanisms | Review study analyzing metformin's influence on pathways like AMPK and mTOR | Metformin exerts anti-seizure effects by activating AMPK and inhibiting mTOR, promoting neuroprotection via BDNF expression and reducing inflammation |
| [52] | A Review on Role of Metformin as a Potential Drug for Epilepsy Treatment and Modulation of Epileptogenesis | Evaluate metformin’s potential in epilepsy treatment | Systematic review of preclinical and clinical evidence | Metformin shows anticonvulsant effects by activating AMPK, inhibiting mTOR, protecting the blood-brain barrier, and reducing oxidative stress |
| [55] | Association of Metformin Use With Alzheimer's Disease in Patients With Newly Diagnosed Type 2 Diabetes: A Population-Based Nested Case-Control Study | Investigate the relationship between metformin use and Alzheimer’s disease risk in newly diagnosed T2DM patiens | Retrospective, case-control study of dementia-free type 2 diabetes patients from Korea’s National Health Insurance database | Metformin use was associated with an increased risk of AD, particularly in patients with longer diabetes duration and concurrent depression |
| [69] | Can Metformin Use Reduce the Risk of Stroke in Diabetic Patients? A Systematic Review and Meta-Analysis | To evaluate the impact of metformin on stroke risk in T2DM patients | Systematic review and meta-analysis of 21 studies, comparing stroke risk in metformin users versus other treatments | Metformin monotherapy was associated with a 34% reduction in stroke risk in randomized and cohort studies; |
| [70] | Chronic Metformin Treatment and Outcome Following Acute Stroke | Evaluate the impact of chronic metformin use on stroke severity, outcome, and mortality in diabetic stroke patients | Analysis of acute stroke patients from Qatar; outcomes were compared between diabetic metformin users and non-users | Diabetic patients on metformin had significantly improved 90-day functional outcomes and lower mortality compared to those on other hypoglycemics |
| [71] | Metformin Use Is Associated With Low Risk of Case Fatality and Disability Rates in First-Ever Stroke Patients With Type 2 Diabetes | Assess the impact of metformin on fatality and disability rates post-stroke in T2DM patients | Cohort study of 7,587 first-ever stroke patients in China, comparing metformin users vs. non-users over a 1-year follow-up | Metformin users had significantly lower in-hospital fatality rates and 12 month disability rates |
Table 2.
Intracellular targets of metformin.
| Ref. No. | Hypothesized cellular target | Biological function | Metformin action |
| [72,73] | AMPK | AMPK is a crucial kinase for cellular energy homeostasis, acting as a sensor of cellular energy status. Under low-energy conditions, AMPK activates pathways that promote ATP production and suppresses anabolic processes to conserve energy. | Metformin activates AMPK in neuronal tissues, potentially providing neuroprotective effects by promoting autophagy, reducing oxidative stress, and supporting mitochondrial function. |
| [74] | GPD2 | GPD2 (Glycerol-3-phosphate dehydrogenase 2) is a mitochondrial enzyme involved in redox transfer between the cytoplasm and mitochondria, particularly within the glycerophosphate shuttle. | Metformin modulates GPD2 activity indirectly through mitochondrial effects, promoting efficient glucose use. |
| [75,76] | Complex I | Complex I, also known as NADH oxidoreductase, is a key component of the mitochondrial electron transport chain (ETC). | Metformin inhibits Complex I, leading to controlled reductions in ATP, which activates AMPK. In neurons, this may promote protective autophagy, reduce oxidative damage, and improve mitochondrial efficiency |
| [77] | FOXO1 | FOXO1 is a transcription factor that regulates the expression of genes in many types of tissues, playing a central role in glucose homeostasis. | Metformin reduces FOXO1 activity by activating AMPK, which may limit neuronal apoptosis and enhance neurogenesis |
| [78] | BDNF | Brain-Derived Neurotrophic Factor (BDNF) is a key neurotrophin essential for brain health, known for its role in promoting the growth, survival, and differentiation of neurons. | Metformin has been found to increase BDNF levels, supporting neurogenesis, synaptic plasticity, and potentially offering cognitive protection against neurodegenerative diseases. |
| [79] | mTORC1 | mTORC1 (mammalian target of rapamycin complex 1) is a protein complex that regulates cell growth, protein synthesis, and nutrient sensing. It integrates signals related to nutrient availability, energy levels, and growth factors | Metformin inhibits mTORC1 activity, which may enhance autophagy in neurons and reduce pathological protein accumulation |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



