
Submitted:
03 January 2025
Posted:
06 January 2025
You are already at the latest version
Abstract
Background: Hypertension remains a significant public health challenge in Ghana. Understanding the lived experiences of hypertensive patients can inform strategies to improve their management. This study explored the perceived enablers and barriers to hypertension management among patients in the Ashanti region, Ghana, using the Chronic Care Model as a framework. Methods: In-depth interviews were conducted with 20 hypertensive patients receiving care at Komfo Anokye Teaching Hospital. Inductive thematic analysis was employed to identify key themes and subthemes. Results: Several barriers to hypertension management emerged, including economic constraints, environmental and lifestyle factors, knowledge and awareness deficits, medication-related issues, and policy and provider-level barriers. Conversely, enablers such as patient empowerment, education, healthcare access, and policy, and provider support and relationships were identified. Conclusions: Effective hypertension management requires addressing a complex interplay of barriers and enablers. Interventions targeting economic factors, lifestyle modifications, knowledge dissemination, medication adherence, and systemic improvements are crucial. Additionally, empowering patients, enhancing education, improving healthcare access, and fostering strong provider-patient relationships can significantly contribute to better outcomes. Future research should investigate the impact of a multi-level intervention on hypertension management in Ghana.
Keywords:
patients
; hypertension
; management
; enablers
; barriers
; Ghana
1. Introduction
Building national capacity to combat non-communicable diseases (NCDs) is important, particularly in low- and middle-income countries (LMICs) [1]. Globally, the prevalence of hypertension (HPT), a primary risk factor for many NCDs, continues to increase [2]. Epidemiological data reveal that HPT remains a significant health concern, with global prevalence ranging from 13% to 41% [2], 54% across Africa [3,4], 27% in Ghana [5], and 30.7% in Ghana's Ashanti Region [A/R]. These figures indicate that HPT substantially contributes to mortality both locally [6] and globally [7]. The response of health systems to managing NCDs has been inconsistent, resulting in low rates of HPT control both locally [8] and among LMICs [9]. Current control trends threaten to undermine global targets aimed at reducing uncontrolled HPT from 25 to30% by 2030 [10,11], and jeopardise the Sustainable Development Goal [SDG] 3.4, which seeks to decrease premature deaths from NCD by one-third by 2030 [12]. This situation necessitates sustained efforts from a diverse array of stakeholders, including HPT patients, healthcare providers, government and health systems, to effectively tackle the inherent challenges.
Despite the considerable global burden of HPT, awareness and treatment remain inadequate: only 34% of Africans recognise their hypertensive status, 31.3% are receiving medication, and a mere 6.5% believe their HPT is under control [13]. This deficiency raises concerns among stakeholders [10].
Effective health programmes cannot be implemented without the engagement of a broad spectrum of stakeholders [14], including patients, policymakers, and healthcare practitioners, who must collaborate continuously to manage conditions such as HPT [14]. However, productive provider-patient interactions are often hampered by both endogenous and exogenous factors, adversely affecting patient health outcomes. Thus, understanding the perspectives of individuals with HPT is imperative for applying available evidence to disease management [15]. Patients' self-management practices can reveal critical bottlenecks within the care process, thereby enhancing future quality of care.
Numerous studies have identified enablers that facilitate effective HPT management [16,17,18,19,20]. For instance, research conducted in Nepal identified family support, positive illness perceptions, free healthcare services, patient knowledge about HPT, medication reminders, proximity to health facilities, perceived severity of the condition, availability of healthcare services, and physician recommendations as significant enablers of HPT control [16,17]. A study by Nakwafila et al. [19] in Namibia highlighted patient education, drug availability, and support systems as essential facilitators of HPT management. In Ghana, Byiringiro et al. [20] noted that the presence of wellness and HPT clinics at the primary healthcare level, patients owning personal blood pressure (BP) monitors, and nurses' expanded roles in HPT control efforts served as key enablers. While these facilitators present valuable opportunities for HPT management, the context-specific nature of the findings may limit their broader applicability, particularly in relation to context-specific barriers that could undermine these potential gains.
Barriers to effective HPT management are diverse, encompassing provider, healthcare system, and patient-level obstacles that significantly hinder successful control efforts [10,19,20,21,22]. Systematic reviews have elucidated various challenges related to patients’ inadequacies in self-management of HPT [23,24]. For example, research conducted in Nepal identified several key barriers, including a lack of knowledge regarding HPT and its treatment, poor adherence to antihypertensive medication, inconsistent follow-up by patients, the absence of standard treatment protocols within the healthcare system, and inadequate health education provided by healthcare professionals [25,26]. Similarly, a study in Namibia revealed that gaps in knowledge about HPT, insufficient social support, the complexity of multiple drug regimens, side effects of medications, and drug shortages significantly hinder patients' self-management efforts [19]. Furthermore, Galson et al. [27] in Tanzania identified a range of barriers affecting HPT control, including knowledge gaps among patients, disease severity, communication with healthcare providers, follow-up care, family support, medication costs, access to health services, waiting times, transportation costs, and fear.
In Ghana, previous studies have highlighted a variety of barriers impeding effective HPT management [20,28,29]. These include patient-level issues such as negative self-management behaviours, socio-economic factors, medication non-adherence, reliance on traditional treatments, and sociocultural influences. At the healthcare provider level, barriers include perceived low quality of antihypertensive medications, communication gaps, inadequate collaboration among healthcare teams, insufficient training on HPT, and challenges related to patient referrals. Additionally, systemic barriers encompass a lack of investment and funding, inadequate health facilities, shortages of antihypertensive medications and healthcare providers, logistical challenges, and issues related to national health insurance and policy frameworks [20,28,29]. If these barriers are not thoroughly examined and addressed, they may significantly undermine empirical interventions aimed at managing uncontrolled HPT in Ghana.
Several studies in Ghana have explored the perspectives of various stakeholders regarding the enablers [20] and barriers [20,28,29] to effective HPT management. However, many of these investigations have primarily focused on healthcare providers [20,29], while Laar et al. [28] included HPT patients as part of their participant pool, albeit in a peri-urban setting in the Eastern region of Ghana. The current study aims to examine chronic HPT management at the Komfo Anokye Teaching Hospital (KATH), a major tertiary referral facility serving eight administrative regions in Ghana. This study is grounded within the Chronic Care Model [14] to systematically unpack the barriers and enablers impacting HPT management, thereby aligning with national and global objectives of achieving a 25% reduction in HPT prevalence by 2025 [10].
1.1. Conceptual Framework
This study is part of a larger study that utilises Chronic Care Model [14] as its theoretical framework. The primary objective is to assess the perspectives of patients with HPT regarding their perceived enablers and barriers to effective management of their condition in Ghana. The model posits that health outcomes for patients result from the collective actions and inputs of various stakeholders, including governmental health policies and investments, as well as healthcare providers who implement clinical protocols and practices in managing chronic conditions, such as HPT [14]. By integrating the roles of healthcare practitioners and patients, the model seeks to enhance health outcomes [30]. It underscores the critical role of “self-management” by patients [14,31], which encompasses both pharmacological and non-pharmacological strategies essential for effective control of HPT [32]. Consequently, this study explores the lived experiences of HPT patients, focusing on the enablers and barriers that influence their management efforts.
2. Materials and Methods
2.1. Ethics Approval
This study adhered to the ethical principles outlined in the Declaration of Helsinki [37]. Ethical approval was obtained from the James Cook University (JCU) Human Ethics Committee (H9031), the Komfo Anokye Teaching Hospital (KATH) Ethical Review Committee (KATHIRB/AP/029/23), and the Ghana Health Service (GHS) Ethics Review Committee (GHS-ERC: 005/09/22). Additional approval was granted by the Ashanti Regional Health Directorate. Informed consent, both written and verbal, was obtained from participants after a detailed explanation of the study's objectives, procedures, potential risks, and benefits. Participants were assured of confidentiality and the right to withdraw at any time.
2.2. Study Setting, Design and Population
The study was conducted at KATH in the Ashanti Region (A/R) of Ghana as part of a broader research project. KATH is a major referral hospital serving a significant portion of the Ghanaian population. The A/R was selected due to its high prevalence of HPT [38]. Evidence shows that 15.3% of women aged 15-49 years and 18.1% of men aged 15-49 years in the A/R report high rates of HPT, with the region showing the highest prevalence in Ghana. Furthermore, epidemiological data reveals that 25.9% of men and women aged 15-49 years in the A/R have severe levels of HPT, making it the highest quintile statewide [38].
Data was collected from both inpatients and outpatients receiving care for HPT at KATH. KATH is also famous for its pool of skilled healthcare professionals specialising in HPT management [39]. This site provided an opportunity to access HPT patients with varying degrees of severity, allowing for a comprehensive assessment of the enablers and barriers affecting HPT management in Ghana.
This study employed a descriptive qualitative design [40] and utilised an inductive thematic analysis framework [41] to explore perceived enablers and barriers to HPT management in the A/R [36]. Participants included HPT patients registered with the KATH HPT clinic who had attended follow-up appointments for at least one year and had previously participated in a quantitative data collection process. Additionally, HPT patients who were hospitalised for their condition, alert, and who provided consent were included in the study. The research adhered to the Consolidated Criteria for Reporting Qualitative Studies (COREQ) guidelines [42]. Further details are available in the supplementary material.
2.3. Target Population and Sample
The participant cohort comprised a diverse group of adults diagnosed with HPT, varying in age, gender, socioeconomic status, and educational background. This diversity ensured a comprehensive understanding of the factors influencing HPT management. A total of twenty (20) HPT patients were recruited, selected conveniently during a pre-interview survey [36]. The determination of sample size was guided by the principle of data saturation [43].
2.4. Data Collection
The first author (FS) and the research assistant (RA) piloted the interview guide with five HPT patients who were excluded from the main study. No amendments were deemed necessary for the instrument. All in-depth interviews were conducted face-to-face in English and Twi by the trained RA and FS at various locations, including participants' homes, the KATH HPT clinic, hospital wards, and other convenient sites for both participants and researchers. With participant consent, each interview was digitally recorded. Probes were employed as needed to clarify concepts and obtain detailed information. Field notes documented non-verbal cues and researcher reflections. The average duration of the interviews was approximately 40 minutes.
2.5. Data Analysis
Following the interview process, the Twi-language interviews were translated and transcribed into English by the RA, who is a native Twi speaker and has conducted similar cross-language qualitative research at both undergraduate and Master of Philosophy levels [44]. The first author (F.S) cross-referenced these transcripts with the original audio recordings to ensure accuracy. Data analysis was conducted using NVivo version 12 (QSR International, Ltd., Daresbury Cheshire, UK) through an inductive thematic framework [41,45,46]. The transcripts were meticulously examined to identify key themes and points, with significant elements highlighted by the first author (F.S).
Collaborative discussions with co-authors K.M.-R, A.S, and T.I.E facilitated the refinement of the analysis framework and thematic categorisation. The first author initiated the grouping of codes into overarching themes, which were subsequently categorised into thematic networks by the research team. This process involved further analysis to explore relationships among the themes, leading to the identification of pertinent quotes that exemplified the themes and supported the findings. The team collectively agreed upon the selection of quotes, ensuring they accurately represented the themes derived from the data. Ultimately, the final themes were substantiated with verbatim statements, augmented by relevant demographic details of participants, including sex, age, and HPT status. In summary, the methodological rigor of this study was upheld through a systematic approach to ethics approval, participant recruitment, data collection, and analysis, enabling a nuanced exploration of the enablers and barriers to HPT management in the A/R of Ghana.
3. Results
3.1. Demographic Characteristics of Participants
The study included 20 participants, with 11 females and 9 males. Participants’ ages ranged from 48 to 89 years. The majority identified as Christian (n=18) and Akans (n=16). Twelve participants were married, and 12 had no formal education. The average duration of HPT was 8.5 years.
3.2. Themes Generated from the Data
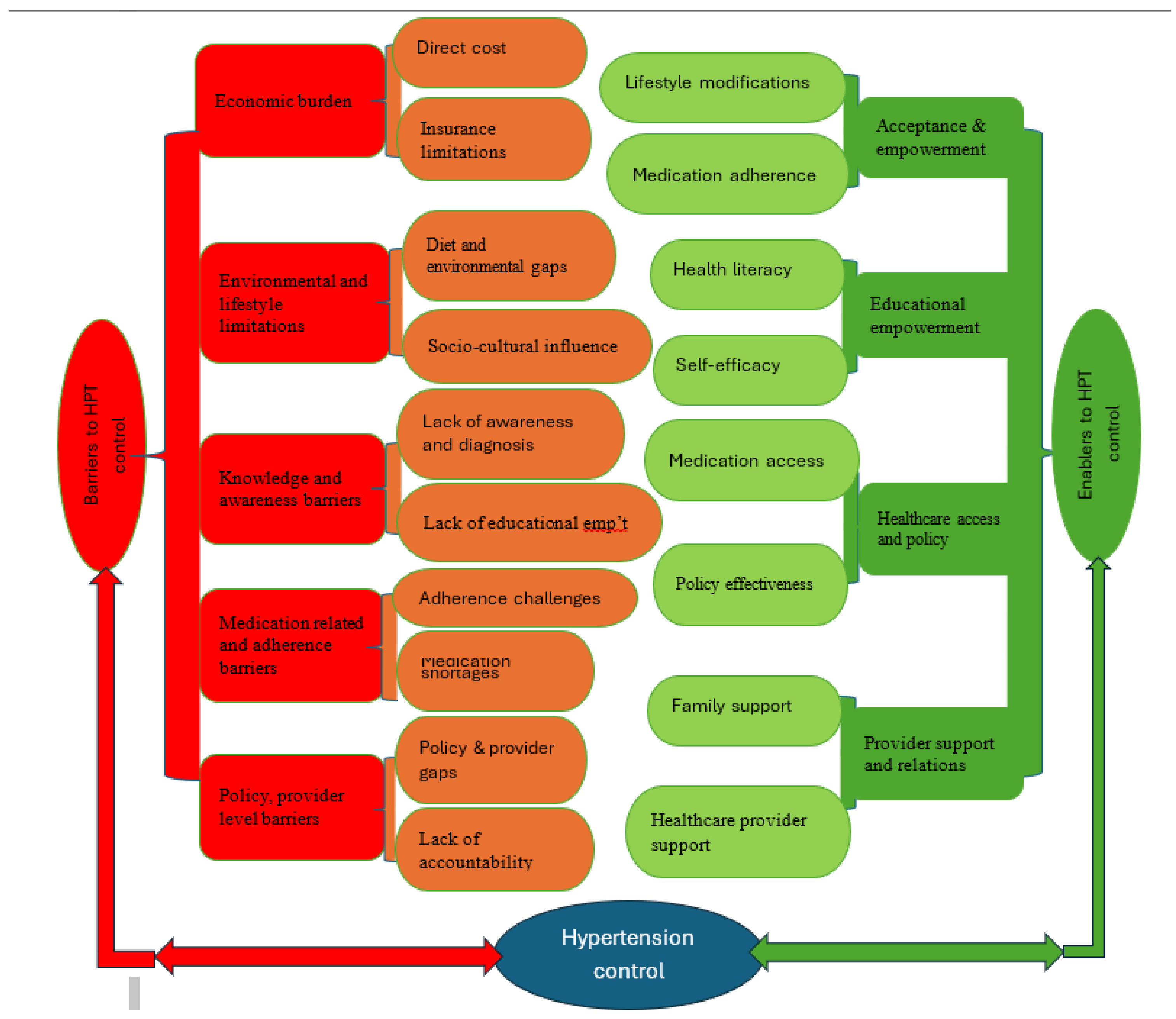
An inductive thematic analysis revealed five major themes regarding barriers to patients' HPT management: (a) Economic burden, (b) Environmental and lifestyle influences, (c) Knowledge and awareness barriers, (d) Medication-related and adherence barriers, and (e) Policy and provider-level barriers. In contrast, four themes emerged as enablers for effective hypertension management: (a) Acceptance and empowerment, (b) Educational empowerment, (c) Healthcare access and policy, and (d) Provider support and relations. Figure A1 summarises the themes and subthemes of the study. Each theme is discussed in detail, supplemented with illustrative quotes from the participants.
3.3. Barriers to Hypertension Management
3.3.1. Theme One: Economic Burden
The first theme identified from the data concerning barriers to HPT management was the economic burden. This theme encompasses two sub-themes: direct costs and insurance limitations. Participants shared their experiences with the healthcare system and their personal management of HPT, highlighting significant challenges related to the cost of antihypertensive medication and gaps in the health insurance system. Most participants indicated that the economic burden severely hampers efforts to manage HPT effectively
Sub-theme: Direct cost
Many participants expressed concerns about the out-of-pocket payments required at each visit to the HPT clinic, noting these costs continue to rise and act as a barrier to care. Some patients reported being referred to private pharmacies to purchase antihypertensive medications at exorbitant prices. Additionally, the unpredictable costs of health services often compel some patients to seek financial assistance from others, and those unable to obtain help sometimes leave without refilling their prescriptions.
“We are in difficult times, but our health should matter most to government and the health system actors. Like the charges they unilaterally impose on us is in bad taste to our hypertension management progress. For my last two visits, they have consistently increased the charges which is a great disservice to the poor patients. So many patients who are not able to borrow from others had to go home without medication. I feel so bad that patients with chronic conditions like hypertension and on health insurance should be subjected to such pathetic treatment”.[Female HPT patient, 70years].
Sub-theme: Insurance limitations
Participants also discussed challenges related to the national health insurance system. While some acknowledged that health insurance has been beneficial in reducing health care costs, the majority lamented that the current state of the health insurance system does not meet their expectations. Many decried the persistent out-of-pocket payments despite having insurance and the continuous increase in charges at HPT clinics, which act as a disincentive to effective HPT management. Some patients now perceive the health insurance system as ineffective and a departure from its initial promise to alleviate healthcare costs for subscribers.
“At first it was good, now we pay money (GHS40.00) for every review which is not good. Some people leave without taking the drugs because they don’t have money to pay. I will say the policies are not effective. Why because the health insurance is basically losing it relevance. You subscribe for health insurance yet when you are sick and come to the hospital, if you don’t have money, you cannot still attend for health service. What is the essence of a policy you subscribe to yet cannot benefit from when the need arises. It’s a hoax insurance”.[Female HPT patient, 58years]
3.3.2. Theme Two: Environmental and Lifestyle Influences
Participants highlighted the pervasive influence of environmental factors, including the use of chemical fertilisers and herbicides by farmers, and how these contribute to NCDs such as HPT. They expressed concern that these factors severely hinder patients’ ability to manage their HPT effectively.
Sub-theme: Diet and environmental factors
Many participants reported that their dietary habits negatively impacted their ability to manage HPT. Some attributed their challenges in achieving successful HPT management to their diet, while others blamed illegal mining activities (locally referred to as galamsey), which introduce harmful chemical residues into the soil and subsequently into food crops. Additionally, some participants admitted to neglecting lifestyle modifications, such as engaging in regular physical activity, which is a non-pharmacological measure essential for HPT management.
“The food we eat now has brought about all this illness. At first there was nothing like chemicals but now is coming and even farmers apply right from planting, so it has affected our foods which has brought all these sicknesses to the world. Worst is the rampant galamsey activities in our farming areas with hazardous chemicals that seep into water bodies use for vegetables growing, irrigation and a whole lot. Those are part of our challenge and the reason for the increasing noncommunicable diseases in Ghana….Duty bearers are failing to implement and enforce our public health laws in the agricultural sector, the mining sector and the health sector as well on ineffective low-quality drugs, the rampant sugary and fast foods in our schools, it is just bad”.[Male HPT patient, 66years].
Sub-theme: Socio cultural influence
Some participants indicated that their struggles with managing HPT were influenced by cultural beliefs that favour herbal medicine as a treatment alternative. They expressed that resorting to herbal remedies is a deeply ingrained practice within their culture. However, it was evident from their accounts that even those who rely on herbal medicine often revert to conventional antihypertensive treatments when blood pressure levels rise.
“If I fail to take it, then is deliberate because I take my herbal drugs and don’t drink both together. For me, herbal medicine is part of my family heritage and our people tradition. Before orthodox medicine our herbal medicines were our medications, and we can’t ditch them like that. I can even tell you most of these orthodox drugs are extracts from herbal so why should we give away our herbs. I can attest that the herbal medicines I take is contributing hugely to the effective control of my condition. I usually give myself sometime to take the herbal drugs and later revert to the orthodox drugs when … I see my BP level rising before I take the orthodox drugs. These herbal drugs I use are not prescribed by any physician but sometimes I listen to specialist in herbal medicine and apply their directives together with the knowledge I gain from our family herbalist. I prepare the drug myself using the herbs the herbal experts teach, and it is giving me positive outcome”.[Male HPT patient, 66 years]
3.3.3. Theme Three: Knowledge and Awareness Barriers
Another theme that emerged from the data is the lack of knowledge and awareness among patients regarding the determinants of HPT, which leads to delayed diagnosis and refusal to accept their diagnosis. This theme generated two sub-themes: lack of awareness regarding diagnosis and lack of educational empowerment. Patients displayed a deficiency in knowledge about HPT-related risk factors, signs, and symptoms that ultimately affect their ability to control the condition. Furthermore, the lack of educational opportunities to help them understand how to prevent or manage HPT results in delayed diagnoses and subsequent complications.
Subtheme: Lack of awareness and diagnosis
Patients reported a significant lack of knowledge and awareness of the precursors to HPT, which has contributed to detrimental health behaviours and delayed diagnosis. Many expressed frustrations over the late diagnosis of their condition, which adversely affects their management efforts.
“I didn’t know from the onset it was hypertension. I was experiencing throat dryness so after further consultation with the Doctor that I realized it was also a symptom of the condition. Because they couldn’t detect the condition from the previous clinics, I was taking anti-anaemic drugs which has high sugar content so after the diagnosis I was restricted from those drugs then the BP level started coming down”[Female HPT patient, 70years]
Subtheme: Lack of educational empowerment
Participants discussed how a lack of formal education or literacy hampers their ability to monitor their health and engage effectively with healthcare services.
“Education is good because you can learn more on the disease on your own. If they give you wrong medication you can easily detect but we those who lack the formal education, I sometimes have to ask people to check my hospital card for me to know my follow-up date. It is only God we depend upon. There was a time a pharmacy gave someone medicine that was not for him. It took an educated person to read before informing him the drug is not for his sickness so I will say education helps a lot. So, to answer your question, my lack of education is indeed affecting my adequate management of my condition, but it is what it is.”[Male HPT patient, 71years]
Another participant acknowledged the impact of educational deficits on health literacy and how it could hinder effective HPT management.
“I can’t read but I know the alphabet so if I have the monitoring apparatus, I will engage someone to assist me. I don’t know if is affecting my treatment of this condition. Only the doctors can tell. However, I think I would have better handled my hypertension situation if I could read and search for information concerning the disease myself. To an extent I can say my educational background is affecting my ability to self-manage my condition”.[Female HPT patient, 67years]
3.3.4. Theme Four: Medication Related and Adherence Barriers
This theme elucidates the medication-related and adherence challenges faced by participants in managing their hypertensive condition. Two subthemes emerged: adherence challenges and medication shortages. This theme highlights the pharmacological deficiencies in the management of patients' conditions. Participants frequently reported difficulties in obtaining adequate antihypertensive refills from government hospital pharmacies during routine follow-ups, primarily due to medication shortages. Consequently, many patients are directed to procure medications from private pharmacies, a process not covered by their health insurance. The additional financial burden often hampers their ability to adhere to prescribed regimens. Furthermore, some participants cited adverse effects associated with the antihypertensive medications provided by their health insurance as a contributing factor to their nonadherence.
Subtheme: Adherence challenges
Participants expressed concerns regarding the side effects of antihypertensive medications, particularly those dispensed through their health insurance, which hindered their adherence to treatment protocols. Reported side effects included decreased libido and frequent urination, which disrupted sleep patterns and limited participation in sociocultural activities. One participant remarked:
“I only buy the orthodox one the doctor prescribes for me. Because of the excessive urination that comes after taking the drugs so anytime I am traveling or going to any public gathering like going to the mosque, I don’t usually take it. This distort the fixed time I apply in the taking of the drug. So, I don’t have an exact time like 8am or 9am that I take my medication but the convenient time I am able to eat or available at home. I know it is a problem in the management of my condition, but my choices are limited”.[Female HPT patient, 67years]
Other participants noted forgetfulness as a significant barrier, while some felt that their stable blood pressure levels justified skipping doses.
“Well, forgetfulness is one of my biggest barriers as I have been skipping the time of my medication and a number of times, not able to take it at all. This has made me take my medication at different times against the advice of the doctors and pharmacies. This may be part of my struggle to manage my hypertension”.[Male HPT patient, 71years]
Subtheme: Medication shortages
Most participants reported frequent shortages of antihypertensive medications at hospital pharmacies during their visits to the hypertension clinic for refills. Consequently, patients are often issued prescriptions to obtain medications from private pharmacies, which imposes additional financial costs that many cannot afford, exacerbating their adherence challenges.
“There is another issue of antihypertension medication shortage at the hospital. How can that be when government is aware of a chronic condition like hypertension requires patients to live on drugs. This situation leads to extra healthcare expenditure on the patient since we have to purchase the drugs from private pharmacies at exorbitant prices”.[Male HPT patient, 59years]
3.3.5. Theme Five: Policy, Provider Level Barriers
Another significant barrier identified in the data pertains to healthcare policy and provider-related gaps. Two subthemes emerged: policy and provider gaps, and governmental lack of accountability, both of which impact patients’ management of HPT. Several participants expressed dissatisfaction with the current health policies, particularly the national health insurance policy, which they believe fails to adequately address the needs of hypertensive patients. Many noted that the existing health insurance framework does not cover approximately 20% or more of the services required for effective HPT management, compelling patients to purchase essential medications at inflated prices from private pharmacies, thus undermining the fundamental objective of universal health coverage.
Subtheme: Policy and provider gaps
Participants voiced concerns regarding the limitations of healthcare providers that adversely affect the quality of care in the management of their condition. A common complaint was the inconsistency of healthcare teams at the HPT clinic, which impedes the development of an in-depth understanding of individual patient histories. This inconsistency hampers effective management, as highlighted by one participant:
“The other barrier to hypertension care is the different doctors we meet at every follow up visit. It is a serious challenge to us as it doesn’t offer that symbiotic patient doctor relationship aim at enhancing medical care for the patient”.[Male HPT patient, 49years]
Additionally, some participants raised concerns about the competence of healthcare providers and the reliability of blood pressure monitoring equipment, which undermined their confidence in their HPT diagnosis and adherence to treatment.
“Well, I'm not a hypertension patient, permit me to say that, because sometime when you do a stressful work, your BP is bound to increase. This has been my contest with the results since I was diagnosed hypertensive. I know an error occurred somewhere or their machines are faulty. So, I have never accepted this condition called hypertension that the hospital claimed I have. You see the day I went, I did not relax enough before the examination was done...sometimes their faulty machines declare people with conditions that might not be, and I have protested to the doctor in the consulting room and the nurses are aware of my protest, but they keep given me medication and you think I will take it, no”.[Male HPT patient, 49years]
Subtheme: Lack of accountability
Participants expressed frustration regarding the perceived lack of transparency and accountability from the government concerning the financial resources generated through health insurance subscriptions. Many questioned the use of their health insurance contributions when they still faced charges for basic outpatient services, laboratory tests, and medications.
“The hospital is partly compounding our plight by continuously introducing charges on services which is affecting some of us. It is unfair and wickedness. So, there is no progress regarding the management of hypertension in this country except that the monies the hospital collect from patients on basic services that we pay for through our subscription to the health insurance have been misapplied to the detriment of the subscriber”.[Female HPT patient, 71years]
3.4. Enablers to Hypertension Management
Four key themes emerged as enablers that enhance effective management of HPT among patients: acceptance and empowerment, educational empowerment, healthcare access and policy and provider support.
3.4.1. Theme One: Acceptance and Empowerment
The successful control of HPT is contingent upon both pharmacological and non-pharmacological adherence, which relies on the patient’s capacity for self-management, rooted in acceptance and compliance with recommended medication and lifestyle modifications. Two subthemes were identified: lifestyle modifications and medication adherence.
Subtheme: Lifestyle modifications
Effective management of HPT necessitates adjustments to certain lifestyle behaviours that adversely affect the condition, complementing the use of antihypertensive medications. Many participants reported actively accepting their diagnosis and engaging in recommended practices such as regular physical exercise, reducing or eliminating salt and oily foods, ensuring adequate rest, and avoiding stress. These modifications are vital for enhancing health outcomes.
“My diet pattern and choices has changed greatly compared to when I was not diagnosed with hypertension. I don’t drink alcohol anymore; I don’t take salty foods and even sugary foods because I have diabetes too. I have also decreased the rate at which I eat fufu. So, I eat fufu” (i.e. a local food from yam) …” on monthly basis and even that I always eat small quantity.”[Female HPT patient, 70years]
Subtheme: Medication adherence
Participants indicated a strong commitment to adhering to their antihypertensive medication regimens. Many reported not only taking their medications regularly but also adhering to a strict schedule for doses and attending follow-up appointments consistently. Trust in orthodox medicine further supported their adherence behaviours.
“I follow the medication instructions. I attend reviews anytime they ask me to come and also take drugs every day. I don’t wait for a day to past. For the drugs I take it regularly and timely. I take it twice daily, morning and evening”.[Female HPT patient, 58years].
3.4.2. Theme Two: Educational Empowerment
This theme highlights the opportunities that empower patients to take control over their health decisions. Two subthemes emerged: health literacy and self-efficacy.
Subtheme: Health literacy
Participants emphasised the role of their educational background in effectively managing HPT. Increased health literacy enabled them to seek information about their condition and make informed health decisions. Many noted a positive correlation between literacy levels and health outcomes.
“Education is critical as one literacy level helps improve one health literacy level. So, my education has helped me to know my review date and time to attend my reviews, without waiting for someone to remind me. A woman came for review today but was not attended to because her appointment date was not today. If she was educated, she could have seen her actual date for the review that is usually written on the card. So, I think education really help”.[Male HPT patient, 57years]
Subtheme: Self-efficacy
Participants expressed a strong sense of self-efficacy in managing their HPT, attributing their commitment to lifestyle adjustments and self-management efforts to their educational backgrounds and a desire to maintain health. This commitment is reflected in their willingness to invest both financial and personal resources to achieve control over their condition.
“I will say my personal abilities/self-efficacy to managing my condition is great. And this is made possible due to my education level, my desire to live so I am committed to every literature and directives the healthcare providers give me.”[Male HPT patient. 40years]
3.4.3. Theme Three: Healthcare Access and Policy
Access to healthcare and supportive policy frameworks were identified as positive factors in managing HPT. Two subthemes emerged: medication access and policy effectiveness. While some participants noted inefficiencies in the National Health Insurance Scheme (NHIS), others found it beneficial for achieving their healthcare objectives related to HPT management.
Subtheme: Medication access
This subtheme explored participants’ access to antihypertensive medications. Some reported never experiencing shortages of their medications, which positively impacts adherence and control. Instances of running out of medication were often attributed to poor handling rather than supply issues.
“I haven’t experience drug shortage before coming for next checkup. They usually give us more than the days for next review. Right now, I have old ones here that I want to ask the Doctor if I should continue taking it or discard once I will get new refill”.[Female HPT patient, 74years]
Subtheme: Policy effectiveness
Participants evaluated the effectiveness of healthcare policies in managing HPT, noting the positive impact of having dedicated clinics for hypertension patients, which reduced waiting times and facilitated easier access to care. Some patients highlighted how policies like the NHIS help subsidise healthcare costs, allowing them to access free antihypertensive medications.
“I will say to an extent the health policies towards the management of hypertension are somewhat effective, because you can get some drugs and care for free at the public health facilities and some accredited private facilities on the NHIS. I got free drugs the last time and even forgot to find out if I am to continue taking it because I still have leftover of the previous visit. But government is really doing well and is helpful because not everyone can afford the drugs if not given freely”.[Male HPT patient, 54years]
3.4.4. Theme Four: Provider Support and Relations
The final theme identified comprises two subthemes: family and social support, and healthcare provider support. Participants emphasised the crucial role both family support and healthcare provider relationships play in the effective management of hypertension.
Subtheme: Family and social support
Several participants articulated the critical role of support received from significant others and relatives in managing their hypertension. This support often manifests as financial assistance for purchasing medication and accessing healthcare services, which participants identified as vital enablers in their condition management. Additionally, family members provide essential prompts that aid in medication adherence and the utilisation of follow-up services. One participant noted,
“My children have been supporting me morally and financially. They prompt me on my medication intake and the food I should avoid. It is not only me, but my husband too is also hypertensive, so we have been complementing each other in the management of our condition”.[Female HPT patient, 50years]
Subtheme: Healthcare provider support
This subtheme explored the support that healthcare providers offer to patients with HPT, which is crucial for effective condition management. Participants expressed appreciation for the cooperation and assistance received from healthcare providers, highlighting the enhancement of trust and confidence in their care. This support encompasses various services, including health education on nutrition and lifestyle modifications necessary for effective hypertension management. One male participant remarked,
“The health staff at KATH are helping… Some of the health workers are so nice and compassionate….”[Male HPT patient, 54years]
3.2. Figure 1. Shows the diagrammatic representation of the themes and their interrelationships.
4. Discussion
This study highlights the multifaceted barriers and enablers affecting HPT management among patients in Ghana. The qualitative nature of this research captures the personal experiences and perceptions of patients, providing a rich understanding of the dynamics involved in HPT management. Our finding identifies five primary barriers: economic burden, environmental and lifestyle influences, knowledge and awareness barrier, medication related and adherence barrier and policy, provider level obstacles. Also, four enablers enhancing HPT control were uncovered: access to healthcare and policy support, acceptance and empowerment, provider support and relationship, and educational empowerment. This suggests the complexity of HPT management, indicating that effective strategies must address both systemic and individual challenges.
The economic burden associated with HPT management emerged as a significant barrier, with participants reporting that the costs of medications, healthcare services, and regular healthcare visits were prohibitive, leading to non-adherence to treatment. This finding is consistent with existing literature highlighting the financial strain of chronic conditions, particularly in LMICs with limited healthcare resources ([47]. Out-of-pocket payments negatively impacted HPT management, as document in Eriteria [48], India [49], China [50], Tanzania [27], Uganda [21], and Ghana [20,28,51]. Participants attributed the cost burden to the NHIS not covering all aspects of HPT care, underscoring the NHIS's critical role in mitigating healthcare expenses associated with HPT management [52,53]. Policymakers must consider strategies to subsidise medication costs and enhance access to affordable healthcare services, including negotiating lower drug prices or establishing community health initiatives focused on delivering affordable care.
The study further highlighted environmental and lifestyle-related limitations as critical barriers to effective HPT management, aligning with previous research that links environmental toxins and unhealthy lifestyle choices to poor HPT control [54,55]. For example, small-scale artisanal mining in Ghana has contaminated water and food supplies, worsening health outcomes [56] in a context marked by rising incidences of non-communicable diseases (NCDs) and lifestyle changes associated with urbanisation [57]. Limited access to exercise facilities exacerbates these challenges. Public health campaigns promoting healthy eating and physical activity, alongside community-level initiatives that improve access to healthy foods and safe exercise environments, could mitigate these issues. We recommend that the Ghanaian government address the detrimental effects of galamsey activities and implement effective land reclamation measures. Conversely, the study identified provider support and positive familial relationships as enablers, which can help mitigate the environmental and socio-cultural pressures affecting lifestyle-related limitations. Our findings confirm the literature that suggests family and social support can serve as effective measures against lifestyle and other environmental challenges in HPT management [18,27,48]. Family support is vital in facilitating access to balanced, low-sodium diets and addressing dietary limitations, especially in areas with limited healthy food options. Family members also promote consistent physical activity through encouragement and accountability, thereby making exercise more sustainable even in resource-constrained settings. Furthermore, emotional and practical support from family members reduces stress—an essential factor in HPT control—by alleviating daily burdens such as transportation to medical appointments. The combined involvement of healthcare providers and family members enhances medication adherence and improves health literacy and consistency in medication use. This social support network facilitates adaptive responses to environmental limitations, emphasising the importance of family-centred approaches for effective HPT management.
The study identified a significant lack of knowledge and awareness regarding HPT and its management among participants. Similar findings have been observed in studies conducted in Namibia [19], Nepal [18], and China [50], where participants expressed uncertainty and poor knowledge regarding HPT management practices. This lack of awareness is concerning as it can inhibit patients from taking proactive measures for early diagnosis and management of their conditions. For example, Bhattarai et al. [18] found that inadequate knowledge of hypertension among patients often led to medication non-adherence. Similarly, research in Malaysia indicated that knowledge deficits regarding hypertension resulted in poor blood pressure monitoring opportunities [58]. These findings highlight the pervasive misconceptions and lack of awareness surrounding HPT and its management across cultures. We infer that the absence of formal education may exacerbate barriers to HPT control in Ghana, as many participants reported minimal or no formal education. However, our findings also suggest a pathway to address these barriers. Participants indicated that educational empowerment through increased health literacy and self-efficacy could enable better management of their HPT. Many participants noted that their formal education had equipped them with essential health literacy skills and boosted their self-efficacy, thereby enhancing their ability to control their HPT conditions. This aligns with previous research conducted in LMICs [48,59,60,61] and Asia [16,18,25], which emphasised the importance of knowledge empowerment in facilitating effective self-management practices for HPT. We advocate for intensified health education campaigns aimed at empowering patients to take an active role in managing their hypertension. Implementing educational programmes within healthcare settings and community platforms can enhance patient understanding, ultimately leading to improved adherence and better health outcomes [62,63]. It may also be beneficial to tailor educational materials to accommodate cultural and linguistic contexts, ensuring they are accessible and relevant to diverse populations [62,63]. Additionally, adopting a personalised health education strategy that involves a multidisciplinary team—comprising pharmacists, nurses, doctors, and community health practitioners—can enhance patients’ health literacy and empowerment, yielding positive outcomes in hypertension management [64,65].
Our findings indicate that medication-related barriers significantly challenge patients’ self-management and their ability to achieve hypertension control goals. Additional sub-themes, including medication non-adherence and medication shortages, underscore patients' concerns regarding the challenges of antihypertensive medications impacting their management of hypertension. This finding points to significant factors hindering effective HPT control, including medication side effects (e.g., frequent urination, reduced libido in men, sleep disturbances, and headaches), forgetfulness, and shortages of medications at government hospital pharmacies affecting patients' refills. This medication-related adherence barrier has been well-documented in literature as a significant obstacle to pharmacological management of hypertension [16,19,20,28,54]. For example, medication side effects have been reported as obstacles to adherence across studies conducted in Iran [54], Nepal [16], Namibia [19], and Ghana [20,28]. Furthermore, medication shortages [19,20,28] and forgetfulness [19,54] further complicate adherence to medication regimens. These findings highlight the need for healthcare providers to engage patients not only in prescribing medications but also in discussing their treatment plans, including potential side effects and the importance of adherence. Strategies such as simplifying treatment regimens, developing reminders for medication dosing, and conducting regular follow-ups can significantly improve adherence. Furthermore, involving patients in shared decision-making regarding their treatment can enhance adherence by fostering a sense of ownership over their health management. Regarding medication shortages, we recommend that the Ministry of Health and the authorities at KATH explore better supply chain solutions to ensure consistent availability of essential antihypertensive medications at government health facilities.
Participants in the present study identified opportunities to address medication-related adherence barriers by highlighting that effective medication access and policy can significantly enhance adherence to treatment regimens and overall hypertension (HPT) management. Patients who consistently reported adequate medication refills noted a corresponding adherence to their medication schedules, suggesting that access to medicines is crucial for facilitating HPT control. This observation is consistent with findings from previous studies [16,18,19], which indicate that improved availability of services and free healthcare provisions enhance the utilisation of services among HPT patients, thereby yielding positive management outcomes. Participants noted that the NHIS has been instrumental in enabling access to subsidised healthcare services and free antihypertensive medications, which contribute to adherence and effective HPT management. To achieve the goal of a 25% reduction in HPT burden by 2025, it is essential to improve the NHIS by expanding coverage to encompass more health services and allowing medical practitioners greater flexibility in prescribing a wider range of medications [10].
Additionally, the study found that patient acceptance and empowerment are critical enablers that can help address medication-related adherence issues. Those who accepted their HPT diagnosis expressed greater self-confidence in adopting lifestyle modifications and committing to medication adherence. Many individuals reported that understanding their diagnosis motivated them to make healthier lifestyle choices and seek necessary medical care. Empowerment initiatives, such as self-management training programmes, can further facilitate this process by equipping patients with the skills and knowledge necessary for effective HPT control.
The study also identified provider-level policy barriers reflected in participants’ experiences within the Ghanaian healthcare system. Patients highlighted gaps in policy and provider accountability regarding the resources mobilised through the NHIS. Some participants expressed concerns that the frequent changes in medical personnel during follow-up visits adversely affect the effective management of their conditions. Moreover, patients reported instances of inadequate training among some healthcare staff, particularly nurses, in accurately capturing vital signs, compounded by issues with faulty or poor-quality blood pressure monitoring devices, which engendered mistrust in their diagnostic results. Although literature contrasting these findings is limited, HPT patients in Nepal have reported similar experiences, citing unsupportive provider behaviours that undermine trust in the care received [16,18]. Other research within the Ghanaian context corroborates our findings [28,29]. For example, lapses in the NHIS coverage for certain HPT-related care and medications, as well as delays in reimbursing healthcare providers for services rendered, have been identified as significant barriers to achieving HPT control in Ghana. This observation has been echoed in the analyses conducted by ISSER [53], which outlined deficiencies within the NHIS in meeting patients’ healthcare financing needs. Furthermore, a scoping review assessing Ghana’s healthcare policy regarding HPT found it to be suboptimal and counterproductive to achieving the target of 25% HPT control by 2025 [66]. Participants also expressed concerns about the reliability of the blood pressure equipment used for monitoring and decision-making at hospitals, a sentiment echoed by Nyaaba et al. [29]. The similarities in these findings underscore broader geo-economic challenges and inequities within the healthcare system and their consequent impact on HPT management.
We recommend that the Ghanaian government shift its focus from merely meeting spending targets to evaluating how resources can be effectively allocated to improve population health and achieve universal health coverage. This involves assessing whether funds are being utilised efficiently to advance community health and identifying ways to improve resource allocation and reduce waste [67]. These issues underscore the need for healthcare systems to foster patient-centred environments that enhance communication and trust between healthcare providers and patients. Training healthcare providers in effective communication skills and patient engagement strategies can cultivate a supportive atmosphere that improves patient satisfaction and adherence.
Additionally, medication access and policy effectiveness emerged as vital enablers in the present study. Participants indicated that existing healthcare policies are effective in managing HPT, crediting the NHIS for providing free medications and healthcare services, which they viewed as essential for successful HPT management. We encourage the Ghanaian government and healthcare providers to continue expanding such support to encompass all HPT-related services, including branded antihypertensive medications, which some patients reported as having fewer side effects and thus improving adherence.
4.1. Strengths and Limitations
This study provides a nuanced understanding of the barriers and enablers in HPT management in Ghana by capturing patients' experiences via a qualitative approach. Key strengths include the identification of specific, intersecting barriers such as economic burdens, lifestyle and environmental factors, limited awareness, medication adherence issues, and healthcare policy constraints. By elucidating these challenges alongside enablers such as healthcare access, social support, educational empowerment, and policy interventions, the study highlights the need for a comprehensive, patient-centred approach. The findings enhance our understanding of chronic disease management in low- and middle-income countries like Ghana and offer insights that could inform targeted interventions and policies in similar contexts.
However, the study has limitations due to its qualitative nature and reliance on self-reported data, which may introduce biases such as recall or social desirability bias. Additionally, the sample may not fully represent the diversity of the Ghanaian HPT patient population, limiting the generalisability of the findings. Moreover, the focus on patient perspectives may omit critical provider-side challenges in HPT management. Future research could address these limitations by employing mixed method approaches that include healthcare providers' perspectives, thereby providing a more comprehensive view of the systemic factors affecting HPT management in Ghana.
4.2. Implications for Policy and Practice
This research highlights important considerations for policymakers and healthcare providers in Ghana concerning the management of hypertension. It outlines the necessity for policymakers to enhance the NHIS to alleviate the economic burden on patients by providing comprehensive coverage for HPT-related medications and medical services. Additionally, robust public health campaigns are essential to foster health literacy and awareness about hypertension, encouraging patients to take proactive roles in their self-management efforts. Furthermore, our findings advocate for the integration of family, social, and provider support into clinical practices, recognising their significant role in promoting adherence and facilitating lifestyle modifications for effective HPT management. The study underscores the importance of community initiatives aimed at increasing access to safe spaces for physical activity and promoting healthy food options to address lifestyle and environmental limitations. Moreover, training healthcare providers in effective communication and engagement strategies can enhance provider-patient relationships, ultimately leading to improved patient satisfaction and adherence to treatment. Lastly, ongoing evaluation of healthcare services is critical to ensuring that HPT patients achieve their self-management goals and realise better health outcomes.
5. Conclusions
This research highlights the various obstacles and facilitators that influence the management of hypertension among patients in Ghana. Our study explores the complex interplay between economic conditions, healthcare policies, environmental factors, and patient knowledge levels, all of which significantly affect treatment adherence and disease control outcomes. We specifically highlighted the detrimental impact of financial constraints, particularly high out-of-pocket costs and limitations within the National Health Insurance Scheme (NHIS), on patients' health aspirations. Furthermore, lifestyle factors and a lack of information exacerbate the challenges faced by individuals striving to manage their hypertension effectively.
Conversely, the research identifies several critical facilitators, including access to healthcare, empowerment through education, support from healthcare providers, and social connections, which can substantially enhance patient outcomes when employed effectively. These findings underscore the necessity for a patient-centred approach that addresses both systemic issues and individual barriers in the management of hypertension. Consequently, it is imperative for policymakers to reform existing healthcare policies, strengthen public health initiatives, and foster collaborative relationships between patients and healthcare providers. Such measures would create a comprehensive framework for effective management of hypertension. Ultimately, the study's findings advocate for holistic strategies that empower individuals to improve their health literacy and ensure equitable access to essential resources, thereby advancing hypertension control and enhancing public health across Ghana.
Future research should consider investigating the effects of multi-level interventions on improving hypertension management outcomes within the Ghanaian context.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org, A1. Consolidated Criteria for Reporting Qualitative Studies (COREQ) guidelines.
Author Contributions
Conceptualization, F.S and T.I.E.; methodology, F.S.; software, F.S., and A-A.S.; validation, F.S and T.I.E.; formal analysis, , F.S., and A-A.S.; investigation, F.S.; resources, F.S. and T.I.E.; data curation, F.S.; writing—original draft preparation, F.S.; writing—review and editing, F.S., K.M-R., A.-A.S., and T.I.E.; visualization, F.S.; supervision, K. M-R and T.I.E.; project administration, F.S.; funding acquisition, T.I.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
This study was guided by the ethical principles outlined in the Declaration of Helsinki (General Assembly of the World Medical Association, 2013). Three institutional review committees: the James Cook University (JCU) Human Ethics Committee (H9031), the Komfo Anokye Teaching Hospital (KATH) Ethical Review Committee (KATHIRB/AP/029/23), and the Ghana Health Service (GHS) Ethics Review Committee (GHS-ERC: 005/09/22) approved the study. Additional approval was obtained from the Ashanti Regional Health Directorate.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the participants that, their identities would not be connected to the output for publication.
Data Availability Statement
The datasets used and/or analysed during the current study are available from the corresponding authors on reasonable request.
Acknowledgments
The authors are appreciative of the participants. We would like to also thank the Research assistants who helped with the data collection. We would also like to acknowledge James Cook University for the PhD research scholarship for the first author, F.S.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
| NCDs | Non-communicable Diseases |
| LMICs | Low-Middle-Income-Countries |
| AR | Ashanti Region |
| SDGs | Sustainable Development Goals |
| HPT | Hypertension |
| BP | Blood Pressure |
| KATH | Komfo Anokye Teaching Hospital |
| CCM | Chronic Care Model |
| JCU | James Cook University |
| GHS | Ghana Health Service |
| COREQ | Consolidated Criteria for Reporting Qualitative Studies |
| RA | Research Assistant |
| NHIS | National Health Insurance Scheme |
References
- Nations U, Nations U. Political declaration of the high-level meeting of the general assembly on the prevention and control of noncommunicable diseases. In High-level Plenary Meeting of the General Assembly 2011. Geneva, Switzerland: World Health Organization.
- Zeng Z, Chen J, Xiao C, Chen W. A global view on prevalence of hypertension and human develop index. Annals of global health. 2020;86(1).
- Akpa OM, Made F, Ojo A. Regional patterns and association between obesity and hypertension in Africa: evidence from the H3Africa CHAIR study. Hypertension. 2020, 75, 1167–78. [Google Scholar] [CrossRef] [PubMed]
- Sharma JR, Mabhida SE, Myers B. Prevalence of hypertension and its associated risk factors in a rural black population of Mthatha Town, South Africa. International Journal of Environmental Research and Public Health. 2021, 18, 1215. [Google Scholar] [CrossRef] [PubMed]
- Amponsem-Boateng C, Oppong TB, Zhang W. Screening of hypertension, risks, knowledge/awareness in second-cycle schools in Ghana. A national cross-sectional study among students aged 12–22. Journal of Human Hypertension. 2022, 36, 405–15. [Google Scholar] [CrossRef] [PubMed]
- World Health Organisation. Hypertension Ghana 2023 profile. 2023a. Accessed 6th March 2024 from: https://www.who.int/publications/m/item/hypertension-gha-2023-country-profile.
- World Health Organisation. First WHO report details devastating impact of hypertension and ways to stop it. 2023b. Accessed on 29th February 2024 from: https://www.who.int/news/item/19-09-2023-first-who-report-details-devastating-impact-of-hypertension-and-ways-to-stop-it.
- Tannor EK, Nyarko OO, Adu-Boakye Y, Owusu Konadu S, Opoku G, Ankobea-Kokroe F, Opare Addo M, Amuzu EX, Ansah GJ, Appiah-Boateng K, Ansong D. Burden of hypertension in Ghana–Analysis of awareness and screening campaign in the Ashanti Region of Ghana. JRSM Cardiovascular Disease. 2022 Jan;11:20480040221075521.
- Wozniak G, Khan T, Gillespie C. Hypertension control cascade: a framework to improve hypertension awareness, treatment, and control. The Journal of Clinical Hypertension. 2016, 18, 232–9. [Google Scholar] [CrossRef] [PubMed]
- Dzudie A, Twagirumukiza M, Cornick R. Roadmap to achieve 25% hypertension control in Africa by 2025. Cardiovascular journal of Africa. 2017, 28, 262–73. [Google Scholar] [CrossRef] [PubMed]
- Jeemon P, Séverin T, Amodeo C, Balabanova D, Campbell NR, Gaita D, Kario K, Khan T, Melifonwu R, Moran A, Ogola E. World heart federation roadmap for hypertension–A 2021 update. Global Heart. 2021;16(1).
- Thakur JS, Nangia R, Singh S. Progress and challenges in achieving noncommunicable diseases targets for the sustainable development goals. FASEB BioAdvances. 2021, 3, 563. [Google Scholar]
- Chow CK, Teo KK, Rangarajan S. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. Jama. 2013, 310, 959–68. [Google Scholar] [CrossRef] [PubMed]
- Wagner, EH. Chronic disease management: what will it take to improve care for chronic illness?. Effective clinical practice. 1998 Aug;1(1).
- Ghosh N, Karthikeyan V, Das S, Boro P, Chakraborty SN. Stakeholder Analysis for Hypertension Management in the Context of the Indian Public Health System. Indian Journal of Public Health. 2023 Jan 1;67(Suppl 1):S27-34.
- Bhandari B, Narasimhan P, Vaidya A, Subedi M, Jayasuriya R. Barriers and facilitators for treatment and control of high blood pressure among hypertensive patients in Kathmandu, Nepal: a qualitative study informed by COM-B model of behavior change. BMC Public Health. 2021 Dec;21:1-4.
- Dhungana RR, Pedisic Z, Pandey AR, Shrestha N, de Courten M. Barriers, enablers and strategies for the treatment and control of hypertension in Nepal: a mixed-methods systematic review.
- Bhattarai S, Bajracharya S, Shrestha A. Facilitators and barriers to hypertension management in urban Nepal: findings from a qualitative study. Open Heart. 2023, 10, e002394. [Google Scholar] [CrossRef] [PubMed]
- Nakwafila O, Sartorius B, Shumba TW, Dzinamarira T, Mashamba-Thompson TP. Stakeholder’s perspectives on acceptable interventions for promoting hypertension medication adherence in Namibia: nominal group technique. BMJ open. 2023 May 1;13(5):e068238.
- Byiringiro S, Hinneh T, Chepkorir J, Tomiwa T, Commodore-Mensah Y, Marsteller J, Sarfo FS, Saylor MA, Assibey S, Himmelfarb CR. Healthcare system barriers and facilitators to hypertension management in Ghana. Annals of global health. 2024 Jul 4;90(1):38.
- Green AS, Lynch HM, Nanyonga RC, Squires AP, Gadikota-Klumpers DD, Schwartz JI, Heller DJ. Assessing providers’ approach to hypertension management at a large, private hospital in Kampala, Uganda. Annals of global health. 2020;86(1).
- Al-Rousan T, Awad M, Pesantes MA, Kandula NR, Huffman MD, Miranda JJ, Vidal-Perez R, Dzudie A, Anderson CA, BP MONITOR Study Group. Healthcare providers perspectives on home blood pressure management in Peru and Cameroon: Findings from the BPMONITOR study. Preventive Medicine Reports. 2023 Jun 1;33:102179.
- Maimaris W, Paty J, Perel P, Legido-Quigley H, Balabanova D, Nieuwlaat R, Mckee M. The influence of health systems on hypertension awareness, treatment, and control: a systematic literature review. PLoS medicine. 2013 Jul 30;10(7):e1001490.
- Khatib R, Schwalm JD, Yusuf S, Haynes RB, McKee M, Khan M, Nieuwlaat R. Patient and healthcare provider barriers to hypertension awareness, treatment and follow up: a systematic review and meta-analysis of qualitative and quantitative studies. PloS one. 2014 Jan 15;9(1):e84238.
- Devkota S, Dhungana RR, Pandey AR, Bista B, Panthi S, Thakur KK, et al. Barriers to treatment and control of hypertension among hypertensive participants: a community-based cross-sectional mixed method study in municipalities of Kathmandu, Nepal. Fron Cardiovasc Med. 2016;3.
- Shrestha S, Shrestha A, Koju RP, LoGerfo JP, Karmacharya BM, Sotoodehnia N, Fitzpatrick AL. Barriers and facilitators to treatment among patients with newly diagnosed hypertension in Nepal. Heart Asia. 2018 Aug 1;10(2).
- Galson SW, Pesambili M, Vissoci JR. Hypertension in an Emergency Department Population in Moshi, Tanzania; A Qualitative Study of Barriers to Hypertension Control. Plos one. 2023, 18, e0279377. [Google Scholar] [CrossRef]
- Laar AK, Adler AJ, Kotoh AM, Legido-Quigley H, Lange IL, Perel P, Lamptey P. Health system challenges to hypertension and related non-communicable diseases prevention and treatment: perspectives from Ghanaian stakeholders. BMC Health Services Research. 2019 Dec;19:1-3.
- Nyaaba GN, Stronks K, Masana L, Larrea-Killinger C, Agyemang C. Implementing a national non-communicable disease policy in sub-Saharan Africa: Experiences of key stakeholders in Ghana. Health Policy Open. 2020 Dec 1;1:100009.
- Marcelli S, Gatti C, Rocchi R, Troiani S, Di Tuccio S, Giuli C, Postacchini D, Santarelli A. Chronic care model and cost reduction in initial health: a new approach for satisfaction and improvement of chronicity. Geriatric Care. 2017 Oct 16;3(3).
- Barr V, Robinson S, Marin-Link B, Underhill L, Dotts A, Ravensdale D, Salivaras S. The expanded chronic care model. Hosp Q. 2003;7(1):73-82.
- Carey, R. M. , Muntner, P., Bosworth, H. B., & Whelton, P. K. (2018). Prevention and control of hypertension: JACC health promotion series. Journal of the American College of Cardiology, 72(11), 1278-1293.
- Wagner EH, Austin BT, Davis C. Improving chronic illness care: translating evidence into action. Health affairs. 2001, 20, 64–78. [Google Scholar] [CrossRef] [PubMed]
- Aekplakorn W, Suriyawongpaisal P, Srithamrongsawadi S, Kaewkamjonchai P. Assessing a national policy on strengthening chronic care in primary care settings of a middle-income country using patients’ perspectives. BMC health services research. 2021 Dec;21:1-2.
- Amu H, Darteh EK, Tarkang EE, Kumi-Kyereme A. Management of chronic non-communicable diseases in Ghana: a qualitative study using the chronic care model. BMC public health. 2021 Jun 11;21(1):1120.
- Sambah F, McBain-Rigg K, Abdul-Aziz Seidu AA, Emeto TI. (forthcoming). Role of interpersonal factors in achieving hypertension control: A focus on chronic hypertension patients in the Ashanti region of Ghana. (Under Review). The Journal of Health Services Report.
- General Assembly of the World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. The Journal of the American College of Dentists. 2014;81(3):14-8.
- Ghana Statistical Service. Ghana Demographic and Health Survey 2014. Rockville: GSS, GHS, and ICF International. 2015.
- Lartey AH, Wang J, Lartey P, Agyei J, Agyei A, Aboagye JS. Modeling and prediction of hypertension in Komfo Anokye Teaching Hospital (KATH), Ghana.2020.
- Bradshaw C, Atkinson S, Doody O. Employing a qualitative description approach in health care research. Global qualitative nursing research. 2017 Nov 21;4:2333393617742282.
- Braun V, Clarke V. Using thematic analysis in psychology. Qualitative research in psychology. 2006 Jan 1;3(2):77-101.
- Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. International journal for quality in health care. 2007 Dec 1;19(6):349-57.
- Saunders B, Sim J, Kingstone T, Baker S, Waterfield J, Bartlam B, Burroughs H, Jinks C. Saturation in qualitative research: exploring its conceptualization and operationalization. Quality & quantity. 2018 Jul;52:1893-907.
- Squires, A. Methodological challenges in cross-language qualitative research: A research review. International journal of nursing studies. 2009, 46, 277–87. [Google Scholar] [CrossRef] [PubMed]
- Attride-Stirling, J. Thematic networks: an analytic tool for qualitative research. Qualitative research. 2001 Dec;1(3):385-405.
- Braun V, Clarke V. One size fits all? What counts as quality practice in (reflexive) thematic analysis? Qualitative research in psychology. 2021, 18, 328–52. [Google Scholar] [CrossRef]
- Essue B, Laba TL, Knaul F, Chu A, Minh H, Nguyen TK, Jan S. Economic Burden of Chronic Ill-Health and Injuries for Households in Low-and Middle-Income Countries. Disease control priorities: improving health and reducing poverty. 2018.
- Gebrezgi MT, Trepka MJ, Kidane EA. Barriers to and facilitators of hypertension management in Asmara, Eritrea: patients’ perspectives. Journal of Health, Population and Nutrition. 2017 Dec;36:1-7.
- Gupta S, Dhamija JP, Mohan I, Gupta R. Qualitative study of barriers to adherence to antihypertensive medication among rural women in India. International journal of hypertension. 2019;2019(1):5749648.
- Xu J, Zhao M, Vrosgou A, Yu NC, Liu C, Zhang H, Ding C, Roth NW, Pan Y, Liu L, Wang Y. Barriers to medication adherence in a rural-urban dual economy: a multi-stakeholder qualitative study. BMC Health Services Research. 2021 Dec;21:1-9.
- Atibila F, Donkoh ET, Ruiter R, Kok G, Hoor GT. Predictors of Nonadherence to Medications among Hypertensive Patients in Ghana: An Application of the Health Belief Model. International Journal of Hypertension. 2022 Aug 24;2022.
- Kusi A, Hansen KS, Asante FA, Enemark U. Does the National Health Insurance Scheme provide financial protection to households in Ghana?. BMC health services research. 2015 Dec;15:1-2.
- Institute of Statistical, Social and Economic Research (ISSER). Ghana’s national health Insurance scheme: Considerations for a more effective scheme (pp. 1-4). Accra: 2020.
- Mostafavi F, Najimi A, Sharifirad G, Golshiri P. Beliefs about medicines in patients with hypertension: The instrument validity and reliability in Iran. Materia socio-medica. 2016 Jul 7;28(4):298.
- Habeeb E, Aldosari S, Saghir SA, Cheema M, Momenah T, Husain K, Omidi Y, Rizvi SA, Akram M, Ansari RA. Role of environmental toxicants in the development of hypertensive and cardiovascular diseases. Toxicology Reports. 2022 Jan 1;9:521-33.
- Opoku RB, Dankyi E, Christian A, Aryeetey R. Environmental exposure and potential health impact of heavy metals in previous mining communities in Ghana. Health Sciences Investigations Journal. 2024 Jun 18;5(2):702-9.
- Kushitor SB, Alangea DO, Aryeetey R. Dietary patterns among adults in three low-income urban communities in Accra, Ghana. Plos one. 2023, 18, e0293726. [Google Scholar] [CrossRef] [PubMed]
- Tan CS, Hassali MA, Neoh CF, Saleem F. A qualitative exploration of hypertensive patients’ perception towards quality use of medication and hypertension management at the community level. Pharmacy Practice (Granada). 2017 Dec;15(4).
- Legido-Quigley H, Camacho Lopez PA, Balabanova D, Perel P, Lopez-Jaramillo P, Nieuwlaat R, Schwalm JD, McCready T, Yusuf S, McKee M. Patients’ knowledge, attitudes, behaviour and health care experiences on the prevention, detection, management and control of hypertension in Colombia: a qualitative study. PloS one. 2015 Apr 24;10(4):e0122112.
- Abaynew Y, Hussien M. A qualitative study on barriers to treatment and control of hypertension among patients at Dessie referral hospital, northeast Ethiopia, Ethiopia: healthcare workers’ perspective. Integrated Blood Pressure Control. 2021 Dec 3:173-8.
- Ukoha-Kalu B., O. , Adibe, M. O., & Ukwe, C. V. (2023). A qualitative study of patients’ and Carers’ perspectives on factors influencing access to hypertension care and compliance with treatment in Nigeria. Journal of Hypertension, 41:845–51.
- O'Brien, E. The Lancet Commission on hypertension: Addressing the global burden of raised blood pressure on current and future generations. The Journal of Clinical Hypertension. 2017, 19, 564. [Google Scholar] [CrossRef]
- Ogungbe O, Byiringiro S, Adedokun-Afolayan A, Seal SM, Dennison Himmelfarb CR, Davidson PM, Commodore-Mensah Y. Medication adherence interventions for cardiovascular disease in low-and middle-income countries: a systematic review. Patient preference and adherence. 2021 Apr 29:885-97.
- Jolles EP, Padwal RS, Clark AM, Braam B. A qualitative study of patient perspectives about hypertension. International Scholarly Research Notices. 2013;2013(1):671691.
- Lu CH, Tang ST, Lei YX, Zhang MQ, Lin WQ, Ding SH, Wang PX. Community-based interventions in hypertensive patients: a comparison of three health education strategies. BMC public health. 2015 Dec;15:1-9.
- Sambah F, Malau-Aduli BS, Seidu AA. Ghana’s Adherence to PASCAR’s 10-Point Action Plan towards Hypertension Control: A Scoping Review. International Journal of Environmental Research and Public Health. 2023, 20, 1425. [Google Scholar] [CrossRef] [PubMed]
- Olalere N, Gatome-Munyua A. Public financing for health in Africa: 15% of an elephant is not 15% of a chicken. Africa Renewal. 2020, 12, 2021. [Google Scholar]
Figure 1.
Diagrammatic representation of themes and subthemes.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



