
Submitted:
07 January 2025
Posted:
08 January 2025
You are already at the latest version
Abstract
Objective: To explore recent findings on how nutritional, gastrointestinal, social, and epigenetic factors interact in autism spectrum disorder (ASD), highlighting their implications for clinical management and intervention strategies that could improve development and quality of life of affected children. Sources: Published materials from main scientific databases were included, providing a narrative review of recent or current literature. Scope constraints determined the completeness of the search. Summary of the findings: Children with ASD have restrictive eating habits and often exhibit food selectivity with either hyper- or hypo-sensory characteristics. This review provides an overview of the literature on diagnosis and intervention strategies for selectivity in ASD, including the involvement of family members in meals, sharing a healthy diet and positive relationship with food, and the importance of exploring visual, olfactory, and tactile experiences of food and introducing new foods through play activities to expand the food repertoire. Modifications in the microbiota and gastrointestinal disorders may also be present in ASD and are presented due to their frequent nutritional repercussions. The medium and long-term implications of food preferences and behavior issues for nutritional status are also discussed, given the tendency for children with ASD to consume low-quality and energy-dense foods, leading to nutritional problems. Conclusions: Children with ASD have feeding difficulties, especially selectivity, gastrointestinal problems, changes in the microbiota and can evolve with micronutrient deficiencies, malnutrition and obesity. This review describes the evidence for possible targets for interventions aiming to improve nutritional health for children with ASD.
Keywords:
Autism Spectrum Disorder
; Food Fussiness
; Feeding and Eating Disorders
; Gastrointestinal Diseases
; Microbiota
; Brain-Gut Axis
1. Introduction
Autism Spectrum Disorder (ASD) is characterized by deficits in communication and social interaction, as well as restricted and repetitive patterns of behavior, interests, or activities. [1] Globally, around 1 in 100 children are affected. At the same time, data from the CDC (Centers for Disease Control and Prevention) in 2023 describes that about 1 in 36 children in the United States is diagnosed with ASD. [2] The scientific literature has been expanding robustly, addressing a range of factors associated with ASD and its comorbidities, including nutritional, environmental, and biological influences that impact the development and health of affected children.
One of the most promising and recent areas of research on ASD involves studies on alterations in the nutritional status and gastrointestinal tract of affected children. Children with autism often exhibit food selectivity, with restricted eating patterns, which can lead to nutritional deficiencies, affecting both physical and cognitive development. Additionally, many individuals with ASD experience gastrointestinal disorders, such as constipation, chronic diarrhea, and gut microbiota-related disturbances, which may exacerbate the behavioral symptoms of the disorder, creating a vicious cycle.[3] Obesity and malnutrition are frequently observed comorbidities, further complicating the clinical picture. Recent research has also focused on the relationship between gut microbiota composition and the neurobehavioral aspects of autism, suggesting that microbial balance may influence brain development. [4,5] This scenario underscores the need for a more integrated approach that considers the multiple dimensions of ASD, particularly those related to the digestive system and nutrition.
Recent advancements in understanding epigenetic mechanisms have shown a significant impact on the development of ASD, elucidating how environmental and genetic factors may interact to influence gene expression and the risk of developing the disorder. Epigenetics, which studies modifications in gene expression without altering the DNA sequence, has become a key area in understanding how factors such as diet and stress during critical periods of development can affect the health and behavior of children with ASD. These findings open new perspectives for preventive and therapeutic interventions based on a more detailed understanding of how the environment interacts with the individual's biology. Given this complexity, this article reviews recent discoveries on the interactions between nutritional, gastrointestinal, and epigenetic factors in ASD, highlighting the implications for clinical management and intervention strategies that may improve the development and quality of life of affected children.
2. Eating Behavior
The formation of eating habits begins soon after birth, with breastfeeding, and is perpetuated in the life of the human being. This process, which is dynamic and shapes eating behaviors, is built from the combination of genetic, environmental, cultural, socioeconomic, and psychological factors, which will result in future food preferences and choices, subject to modifications throughout life. [6] The existence of several nutritional problems among children diagnosed with ASD is recognized, derived from atypical eating and not-eating behaviors that are very prevalent in this group.[7,8,9] The age of onset can be early while still breastfeeding, with premature weaning already being a possible symptom.[10] However, selectivity and resistance to trying new foods are the symptoms that stand out throughout development.[6,11]
Eating behavior is connected to impairments in sensory processing, manifested by excessive responsiveness or atypical responsiveness to sensory stimuli.[9,10] The act of eating involves sensory, emotional, cognitive, and neurological aspects in a complex conjunction of factors. The decision to eat or reject a food goes through sensory perception and processing (visual, olfactory, vestibular, tactile, and gustatory) that, at a responsive level, enables the construction of behavioral food decisions. In ASD, this ability to categorize stimuli, hedonically and cognitively, based on sensory apprehension, seems altered, making it difficult to build models that serve as an internal reference for decision-making at the beginning of the action based on previously acquired experiences. The result of this distorted sensory processing capacity results in discrepant eating behaviors, ranging from total rejection or exclusive preference, with a low number of possible responses.[8]
From a social point of view, socialization problems make it difficult to eat in a family or a group and, therefore, to learn by imitation, which is an important aspect related to the increase in the food repertoire in childhood. [7,10] Parents have a significant influence on the development of their children's eating behavior, so children with ASD in families that choose a healthy diet tend to share such habits.[10] In this aspect, it is difficult for parents to perceive their children beyond the disorder,[6] which makes them abandon attempts to stimulate a more regulated food education to give in to their preferences.[10]
Eating behavior can be considered to reflect characteristics of ASD defined in the DSM-V: (1) a) restrictive and repetitive patterns of behavior; b) insistence on routine; c) inflexibility; d) rigid standards; e) restricted and fixed interests; f) hyper or hypoactivity to sensory stimuli. Inflexibility arises at mealtimes, manifesting itself in the form of rituals, such as always eating in the same place, the child's inability to remain seated at the table or difficulty in diversifying the food ingested, making the family environment chaotic and stressful [10] and interfering with adequate nutrient intake.[7] In this scenario, behavioral rigidity is still pointed out as a point of connection between food selectivity and obesity, as it is primarily linked to atypical eating patterns.[12,13] On the other hand, the attempt to ensure adequate intake and sufficient food repertoire for children promotes intense suffering for parents and caregivers of children with ASD,[9,11] increasing the likelihood of depression and anxiety symptoms in this group.[10]
Selectivity is the most frequently observed profile and refers to a behavior characterized by the frequent or permanent refusal of certain foods or entire food groups due to characteristics such as taste, color, smell, consistency, or form of presentation.[14] This condition is very prevalent in patients with ASD, affecting 50 to 90% of them [15] and being 15 times more common in these children than in their healthy peers. [16]
There is a significant variation in the presentation form, that can evolve from a very mild condition, which resembles the common food neophobia of childhood, to extreme situations in which no food is accepted.[17] However, an aspect that may accompany this behavior is the presence of an essential disruptive behavior during the meal, almost always mediated by inflexibility[18], that imposes great suffering on the patient and the family, [15] including crying, screaming, running away from the dining environment, aggression, spitting, lack of chewing, and throwing food and utensils [19] Often, the onset of eating difficulties precedes the diagnosis of ASD [20] and other disorders, in addition to selectivity, may be present due to gastrointestinal problems, deliberate restrictions made by parents due to unfounded beliefs, as well as physical and motor difficulties. [21]
Children with ASD may have food selectivity profiles of hyper- or hypo-sensory characteristics. [16,17,22] The most common aspect is related to hyper-sensoriality, [3] leading to refusal due to low tolerance to environmental stimuli.[14] Almost always, the condition exceeds the limits of food, and intolerant behaviors are observed in relation to multiple aspects of daily life, such as noise, odors, and light, among others. [20] These children do not eat well because they feel the characteristics of food very intensified [16] and may resemble "supertasters."[23] We suggest calling this behavior "hyper-sensory selectivity." However, in some cases, the opposite aspect is observed, and some patients, due to ASD, have great difficulty in performing the central processing of information from the environment. [24] In this way, it is as if they were less likely to perceive flavors, smells, colors, noises, and textures, which configures a hypo-sensoriality profile. [3] These children do not eat well because they do not feel the food. [16] We suggest calling this profile "hypo-sensory selectivity." The differentiation between the two types is relatively simple. When it comes to hyper-sensoriality, refused foods, when offered, generate repulsion, nausea, and intense discomfort for the child.[20] In cases of hypo-sensoriality, there is an evident lack of interest in everyday foods, which are refused due to the fact that they do not cause any interest in being ingested, and there may be better acceptance of foods that are sweet, salty, fatty and highly palatable.[17] In both cases, the severity of symptoms is variable and may be pretty low, with little or no repercussions on nutritional status. On the other hand, relevant consequences are often observed, which can lead to severe malnutrition, evolving to intense thinness, stunting, hidden hunger, or obesity. [3] These different outcomes may be a consequence of energy insufficiency, leading to negative caloric balance in extreme selectivity; of the small variety, leading to vitamin and mineral deficiency; or compulsive and repetitive eating profiles in which few foods are consumed in large quantities, with a frankly positive energy balance. Changes in nutritional status will be detailed later.
Considering the therapeutic approach of selectivity in a generic way, supplementation with complete and isocaloric profile supplements has been used with satisfactory results to ensure the adequate supply of macro- and micronutrients. [25,26,27,28,29,30] So far, there is no consensus on how to treat selectivity linked to ASD,[31] but some strategies have been adopted and described in the literature. The recommendation is that, whenever possible, the approach should be multidisciplinary.[31]
In cases of hypo-sensory selectivity, the child may sometimes respond to hyperstimulation. [32] This can be achieved by increasing the sensory properties of food, making it, for example, crunchier, more colorful, sweet, salty, seasoned, spicy, noisy, and fragrant. [26,33] Substances such as curry, peppers, herbs, and colorants can be used to modify foods, making them capable of producing more intense sensations and more likely to be perceived, processed, and interpreted in the central nervous system.[26] One of the problems for treatment in these cases refers to the fact that acceptance may be better for highly palatable foods that, in general, are richer in carbohydrates, lipids, salt, and sugar. This, in association with the other characteristics of ASD, especially tendencies to impulsivity, can increase the risk of progression to obesity, insulin resistance, hypertension, and dyslipidemia.[17] Hyper-sensory selectivity, on the other hand, has a more complex treatment. From the point of view of food, the trend is a greater acceptance of those with a more neutral profile, less colorful, less striking flavor and odor, and liquid or pasty consistency.[26]
Due to the refusal behavior associated with phenomena such as nausea, vomiting, choking, and neurovegetative disorders, the moment of the meal becomes challenging. For this reason, the therapeutic process must involve the whole family.[20] The participation of parents in meals should be encouraged and characterized as fundamental,[6] because they are the ones who will serve as models and will be the promoters of the interventions. The environment has a substantial impact on eating habits; for this reason, it is recommended that the family share a healthy diet, establishing a positive relationship with food at mealtime.[10,34] Changes in the family's lifestyle are necessary, based on adequate nutritional guidance.[9] Adjustments must be made to the food profile and the environment where meals are held, as well as the preparation of a schedule that meets the difficulties and demands in an individualized way, respecting the needs and uniqueness of each case. [9] Guidance for the expansion of sensory aspects, with the offer of new foods and the inclusion of other forms of experiences that involve the purchase and preparation of food, are resources to be used.[6] Exploring visual, olfactory, and tactile experiences of food in the form of actions that increase sensory familiarization allows the development of the hedonic characteristics of sensory stimuli, resulting in the expansion of the food repertoire in children with ASD.[8] Toomey and Ross (2011) advise that children with food selectivity are slowly introduced to food in progressive steps through the use of a "desensitization" hierarchy to encourage them to explore, interact, and eventually eat new foods. This hierarchy involves six main categories: "tolerating", "interacting", "smelling", "touching", "tasting" and "eating" the foods presented and is used to encourage sensory processing and the acquisition of oral motor skills. [35] This hierarchical scale was called the Sequential Oral Sensory Approach to Feeding (SOS Approach) [35] and appears to be beneficial for children with neurological impairment, including autism. [36] In general, initially, the professional must understand which sensory changes (tactile, olfactory, visual, auditory, and/or gustatory sensitivity) impact the child's diet. Then, familiarization with new foods will begin through playful activities involving sight, smell, and touch. Then, the gradual advancement of taste and contact with food will be achieved through a series of small steps. [27]By respecting the child's sensory processing, there is a greater probability of approaching the food. Professionals to be involved in the interdisciplinary management of food selectivity include occupational therapists, nutritionists, psychologists, speech therapists, and physicians. [37]
An additional relevant point is that Avoidant/Restrictive Food Intake Disorder (ARFID) and autism are conditions that often co-occur. [38] In a large Swedish cohort, 12.1% of children with ARFID also had autism, highlighting a strong association between the two conditions. [39,40] Therefore, when evaluating feeding difficulties in children with autism, clinicians should consider the possibility of ARFID, mainly if the child exhibits extreme selectivity or avoidance of foods based on sensory characteristics. In fact, the presence of comorbid neurodevelopmental or psychiatric conditions, such as ASD, ADHD, or anxiety disorders, can increase the likelihood of ARFID. [41] Research highlights cognitive behavioral therapy (CBT) as a possible intervention for children with ARFID. [42,43] CBT can be performed in conjunction with sensory integration or "desensitization" methods. [27] This means that the introduction of new foods can be done in stages or phases, setting sensory goals to "desensitize" the child and subsequently ensure familiarity with the taste and texture of the food. [44,45]
3. Macro and Micronutrients
The food preferences of children with ASD [64] contribute to increasing the difficulty in composing meals and introducing new foods, resulting in preferences for refined, processed, soft, and sweet foods [65,66,67] and rejection of vegetables, fruits, and grains, along with sour and bitter flavors. [65,68,69] Limitations in food categories are observed, [68,70] associating altered and inflexible rituals and behaviors [65,67,71] with compromised quality and quantity of nutrients in the diet, leading to medium- and long-term repercussions on nutritional status. [65,72,73]
Increased consumption of energy-dense foods with high amounts of carbohydrates [66,68] and fats [74] can lead to excessive weight gain. Studies conducted on all continents have found a high prevalence of obesity. [37,65,67,74,75,76,77,78] On the other hand, protein intake falls short of requirements since the primary sources of this nutrient are scarce in these children’s diets. [79,80,81,82]
The association of frequently observed characteristics, sometimes in an extreme form, [83] such as oral defensiveness, food selectivity, neophobia, and gastrointestinal disorders, [71,73] contributes to an increased risk of deficiency of several micronutrients. [64,84,85,86,87] Regarding minerals, low ferritin concentrations have been observed in children with ASD, mainly due to the low intake of meat, whose appearance and texture are usually rejected. [76,81,88] This leads to an increased risk of anemia, contributing to reduced cognitive performance and accentuating some characteristics of ASD itself. [52,86,89] Zinc deficiency is also common among children with ASD and may contribute to impaired neurodevelopment and immunity. [38,68,80,89,90,91,92] Changes in appetite and taste associated with low zinc concentrations contribute to increased eating difficulties.[93] Calcium has also been found in low concentrations among children with ASD. [68,69,79,80,87,94] Chronic calcium deficiency can result in long-term problems, especially osteopenia and osteoporosis. [76,81]
Patients with ASD are also at higher risk of vitamin deficiencies. [11,69] Vitamin D deficiency (VDD) has been frequently reported, [95,96,97,98] and lower serum concentrations of 25-OH-vitamin D are observed in this group. [96,98] Low intake, [69,79,99] genetic factors,[100] and reduced sun exposure (due to difficulties with social interaction and subsequent isolation) contribute to this condition. [101] Obesity, often associated with ASD, [102] is another risk factor. [103] At the same time, VDD may exacerbate symptoms associated with ASD, which are alleviated after the correction of the deficiency, [104] as observed in studies in China and Turkey. [105,106] An “inflammatory state” in specific brain areas could help explain these findings, [107,108] as there is a negative correlation between serum concentrations of 25-OH-vitamin D3 and peripheral inflammation markers. [109] Regarding vitamin A, although some studies have reported serum retinol concentrations within the normal range in children with ASD, [110,111] Cases of vitamin A deficiency (VAD), sometimes severe, with ocular symptoms of deficiency (night blindness, xerophthalmia and loss of vision) have been reported.[112, 113] Godfrey et al. reported the cases of six individuals with VAD, impaired visual acuity, and imp[105,106] rovement following vitamin A supplementation. [114] The ocular manifestations of severe VAD may be aggravated by hyperostosis of the optic canal, with consequent compression of the optic nerve. [115] A Chinese study with children aged two to seven observed, among boys, a negative correlation between serum retinol concentrations and scores on the Social Responsiveness Scale and the communication warning behavior subscale of the Children Neuropsychological and Behavior Scale (2016 Revision). [111] Regarding vitamin C, the development of scurvy in children with ASD was reported by Sharp et al. [116] and Kinlin & Weinstein. [117] Some studies have also found a lower intake of B-complex vitamins among individuals with ASD [118,119] , and several authors have highlighted vitamin B12 (cyanocobalamin) as frequently deficient in these cases. [118,120,121,122] Additionally, some studies have reported deficient serum concentrations of vitamin B9 (folate) [105,118,122] Deficiencies in vitamin B6 (pyridoxine) and vitamin B1 (thiamine) have also been reported. [105,123]
Given the dietary profile that includes imbalance or deficiency in the intake of macro and/or micronutrients, the initial treatment should be readjusting the diet. However, given the characteristics of these children, this measure presents varying degrees of difficulty and takes time to produce the desired effects. Broader nutritional supplementation, through complete supplements, has been adopted as an alternative. [25,26,27,28,29,30] Supplementation should be initiated gradually, using products that provide general benefits with minimal side effects, always under the supervision of a healthcare professional. [72,124] However, there is no consensus regarding dosages and duration of use. [125] Amino acid supplements may help regulate neurotransmitters in the central nervous system. [126] Several authors have demonstrated that DHA supplementation contributes to improvements in social communication, behavior, and cognition. Minerals such as iron, zinc, and magnesium have also been used successfully and have contributed to improvements in sleep conditions, [88] cognitive performance, and motor skills.[127,128] The treatment of vitamin and mineral deficiencies is outlined in Table 1. [46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63]
4. Underweight and Obesity
Individuals with ASD face unique challenges in relation to their nutritional status and are at greater risk of being underweight, although the prevalence of overweight and obesity is also significant. This dual risk, which can also be associated with micronutrient deficiencies, highlights the complexity of nutritional problems in ASD, requiring careful monitoring and personalized interventions. [129] Children with ASD have a 6.5% prevalence of being underweight and a 28.5% higher risk of being underweight compared to neurotypical controls. [130] Malhi et al. observed lower levels of certain micronutrients and lower growth parameters in children with severe ASD, who were smaller and lighter compared to those with less severe symptoms. [131] The relationship between ASD and body weight is complicated by the presence of other health conditions in which present and past comorbidities can influence nutritional status. [132] The association with psychiatric conditions such as anorexia nervosa suggests that underweight may be exacerbated by restrictive eating behaviors, although this relationship is complex and not fully understood. [133] Nutritional deficit is a pattern in children with greater severity of the spectrum, and the greater the inflexibility and food restriction, the more significant the low weight. A study by Bölte et al. showed that 28% of males with ASD had a body mass index (BMI) in the fifth percentile or below, suggesting a significant presence of low body weight in this population. Still, this association was inconsistent and partially mediated by hyperactivity. [134] According to Bölte et al., maladaptive social and communicative behaviors, as well as stereotypical characteristics, do not show a significant association with BMI, except for hyperactive behavior, which was partially responsible for low body weight in some cases. [134] ARFID, on the other hand, when associated with ASD, can often lead to low weight. [39,40]
A population-based study in Israel showed that low birth weight and premature birth were associated with a higher risk of ASD, potentially affecting growth trajectories. [135] A Chinese study has shown that overall body growth may not be so significantly affected in early childhood. [136]
Although the relationship between ASD and low weight or height is clear, it is important to consider the variability within the affected population. Factors such as symptom severity, eating behaviors, and developmental problems play crucial roles in influencing growth. More research is needed to understand these dynamics better and develop targeted interventions that meet the specific needs of individuals with ASD. Treatment will depend on food intake capacity, the degree of selectivity, and the severity of the condition. Children with a higher degree of involvement have greater inflexibility and difficulty in accepting foods with nutrients that are in deficit. More significant dietary restrictions lead to greater risks of malnutrition and an association with ARFID. Nutritional planning should consider hypercaloric supplements (up to 1.5 Cal/mL) if there is milk acceptance. The possibility of using powdered supplements with food will be considered if there is minimal acceptance of staple foods. In cases of extremely low weight, intense selectivity for a prolonged period, unsuccessful oral acceptance, and lack of response to conventional interventions, preferential gastric feeding should be considered, with gastrostomy and a gastric inlet button for the shortest possible time. [72,137,138,139]
Childhood obesity is a growing public health problem with a negative impact on physical and mental health. It is associated with comorbidities such as type 2 diabetes, dyslipidemia, non-alcoholic fatty liver disease, and cardiovascular diseases, as well as social and emotional consequences such as bullying and depression. [140] Children and adolescents with ASD have a higher prevalence of obesity compared to healthy controls. [141,142] Systematic reviews with meta-analysis estimate that this prevalence varies between 7.9% and 31.8%. [78,143] The relative risk of obesity in children with ASD ranges from 1.41 (95% CI: 1.062–1.876) to 1.58 (95% CI: 1.34–1.86).[78,143] The reasons for the development of obesity in children with ASD are multifactorial [144] , and many of them are similar or additional to the causes already defined for the general population. [142] Maternal metabolic disorders during pregnancy, such as diabetes, hypertension, and obesity, [144] and shorter duration of exclusive breastfeeding are also associated with a higher risk. [145,146] Food selectivity contributes to a preference for energy-rich foods, sweetened beverages and snacks [147] and a low intake of vegetables.[147,148]. The use of medications, such as second-generation antipsychotics, to reduce disruptive behaviors also contributes to substantial weight gain. [149,150] Children with ASD spend less time engaged in physical activities [151] due to social and behavioral challenges, [152] motor deficits [153] and increased screen time. [154,155] Poor sleep quality is also associated with weight gain. [156,157] Other risk factors involve changes in specific appetite hormones, such as leptin, adiponectin, and ghrelin, as well as changes in the intestinal microbiota, which are more prevalent in ASD and individuals with obesity. [144] Finally, genetic vulnerabilities, such as deletions in 16p11.2, have been associated with obesity and ASD. [158,159]
Health professionals must work on preventing obesity in ASD to minimize the risk of associated comorbidities, which can considerably worsen the child's quality of life. Once the diagnosis of obesity is confirmed, the initial (and first-line) treatment is similar to that for neurotypical children and involves behavioral and dietary modifications. However, these first therapeutic steps can be problematic for children who have difficulties with social and behavioral communication, difficulties with changes in routine, sensory processing, and decision-making. [160,161] Despite this, efforts must be concentrated on improving the consumption of fruits, vegetables, and legumes, which are capable of reducing the energy density of the diet, being sources of dietary fiber and impacting the development of the microbiota; reducing the consumption of sugary drinks and high-calorie foods; encourage physical activity; [162] involve the whole family in changing eating habits and physical activity; [163] refer to physiotherapy sessions in case of motor difficulties; [164] in addition to reducing screen time and improving sleep quality, establishing bedtime routines. [44] Replacing obesogenic drugs, frequently prescribed in ASD, with others without this effect can be discussed with a neurologist or psychiatrist. [165] GLP1 agonists have not yet been sufficiently studied in ASD. Still, their use is authorized for typical children from 12 years of age, configuring a therapeutic option to be considered, especially when binge eating is present. [166]
5. Gastrointestinal Issues
ASD is associated with a variety of gastrointestinal (GI) disorders that can be generated or influenced by aspects related to social interactions, communication difficulties, repetitive movements, behavioral changes (irritability and aggression), and psychiatric disorders.[167] Food preferences and selectivity exacerbate gastrointestinal symptoms. [15] The prevalence of GI problems in individuals with ASD is considerably high and more prevalent in these individuals than in those with other causes of developmental delays [168] , ranging from 46% to 84%, depending on the assessment method and population studied. [73,169] GI issues in individuals with ASD significantly impact the quality of life of children and their families, affecting well-being, school attendance, and participation in social activities. [170] The main clinical manifestations are constipation, chronic diarrhea, abdominal pain, nausea, abdominal distension, and gastroesophageal reflux, [171] which contribute to the worsening of the behavioral and sensorimotor manifestations in affected children. [172] This interference suggests complex interactions involving the brain-gut axis. [173] Factors related to genetic mutations and variations, [173] altered gut microbiota, [167] as well as food intolerances and allergies, particularly to gluten and casein, [174] are implicated in gastrointestinal manifestations. Immune system dysfunction is observed in some children with ASD. [173] Chronic intestinal inflammation, altered gut motility, and increased intestinal permeability are considered relevant mechanisms in the manifestations of GI issues. [175]
Ferguson et al. (2019) investigated GI issues in 340 children and adolescents with ASD and found constipation to be the most prevalent symptom (65% of cases), followed by stomach pain (47.9%), nausea (23.2%), and diarrhea (29.7%). In this study, the presence of aggressive behavior was associated with nausea in children aged 2 to 5 years, and among those aged 6 to 18 years, anxiety behavior increased by 11% in the presence of constipation symptoms. The association of differences in sensory processing and integration may exacerbate the response to gastrointestinal symptoms and discomforts. [176]
The treatment for GI disorders varies and is related to individualized approaches tailored to each specific manifestation, considering the complexity of each patient. The modulation of gut microbiota through prebiotics and probiotics is discussed in this article. Studies investigating dietary interventions, such as the elimination of gluten and casein, reduction of complex carbohydrate, lactose, and sucrose intake, and ketogenic diets, among others, have shown inconsistent and potentially harmful results due to the lack of scientific evidence on its effectiveness, to the strict adherence required for these diets and to the risks of nutritional deficiencies. [125,177] An individualized dietary approach is essential to meet the specific needs of everyone with ASD and assist in the treatment of their symptoms. For constipation, treatment generally includes the use of laxatives (such as polyethylene glycol) to facilitate bowel movements and relieve discomfort. Dietary adjustments are recommended, such as paying attention to food preferences, including or adjusting fiber intake, encouraging fluid intake, establishing a bathroom routine after meals, and promoting regular physical exercise. [73,178] It is important to remember that constipation can also be associated with sensory issues related to contact with feces or odors, as well as vestibular limitations that can make sitting on the toilet complex. These aspects should be considered for an appropriate intervention.
Chronic diarrhea’s higher occurrence may be related to sensory behavior (preferences/aversions), food sensitivities/intolerances, side effects of medications used to improve ASD-related symptoms, anxiety, and stress. Treatment aims to address the cause of diarrhea. It should be individualized, enable hydration, and re-establish a balanced diet adjusted to the child's nutritional needs. Recognizing the cause and having strategies that facilitate adherence to the treatment are vital for controlling the diarrheal process. [73,172]
Abdominal pain impacts the quality of life of children with ASD, and the difficulties in understanding painful events and communicating discomfort lead to problems in proper diagnosis and treatment. [168,179] Painful sensations can intensify aggressive behaviors, abnormal vocalizations, motor signs, hyperactivity, anxiety, and alter sleep patterns.[176] The treatment should focus on the cause of abdominal pain (constipation, GER, irritable bowel syndrome, food intolerances) and sensory, emotional, medicinal, musculoskeletal, and urinary factors. The approach must be comprehensive, collaborative, and individualized, with dietary modifications, behavioral therapies, and prescription medications for symptom relief. A multidisciplinary approach involving pediatricians, gastroenterologists, and behavioral therapists is desirable. The appropriate treatment, tailored to specific needs, will improve the quality of life and overall well-being of patients with GI disorders and ASD.
6. Microbiota
The gut microbiota regulates hormonal and inflammatory functions, which directly impact digestive function and the nervous system through the brain-gut axis.[180] Thus, an unsatisfactory microbiota composition can compromise the intestinal epithelial barrier, increase intestinal permeability, and alter the synthesis and release of neurotransmitters (serotonin, gamma-aminobutyric acid, and oxytocin). [180]
The influence of the gut microbiota in patients with ASD has been studied since the 1990s when it was observed that the use of antibiotics, initially vancomycin, resulted in behavioral improvements and gastrointestinal symptoms in these patients. [167] Recent studies have shown that people with ASD have significant changes in their gut microbiota. [181] Concomitantly, chronic gastrointestinal alterations are found in up to 70% of children with ASD and can manifest in the forms of diarrhea, constipation, gastroesophageal reflux, alteration of the permeability of the intestinal barrier, immune dysregulation, and inflammation of the gastrointestinal tract. [181,182]
Several factors seem to contribute to these changes, such as type of delivery, gestational age, genetic factors, and diet, in addition to the use of antibiotics, which are more frequently prescribed to ASD patients. [181,182,183] Studies suggest that the microbiota of these individuals has a lower diversity of microorganisms, high levels of Clostridium, Bacteroides, and Desulfovibrio, and lower levels of Actinomyces and Firmicutes, which correlates with the severity of gastrointestinal manifestations, with higher production of short-chain fatty acids, especially propionic acid, which has been related to the development and severity of the ASD symptoms. [180,181,182] When food selectivity is present, high values of Prevotella, Anaerophilum, Clostridium, and Salmonella are observed, in addition to a higher Escherichia/Shigella ratio. [82]
There is a large discrepancy between microbiota profiles, which is attributed to the variables gender, age, previous comorbidities, use of medications, use of antibiotics, diet, cultural differences, and environment. [182,184] Thus, it is not possible to establish a pattern of varieties and concentrations of microorganisms in the microbiota of the population with ASD, so a generalized treatment cannot be determined. Studies suggest that the use of probiotics can improve gut dysbiosis, which would result in modulation of the immune system, attenuation of gastrointestinal symptoms, reinforcement of intestinal barrier function, and regulation of the production of neuroactive components. [172] Gut microbiota is involved in modulating neurotransmitters like dopamine, GABA, and glutamate, which have implications for neuropsychological disorders and gastrointestinal diseases. [185] In a recent review, Mhanna et al. state that targeting the gut microbiome represents a promising intervention for patients with ASD.[185] The strains that seem to show the best results are Lactobacillus and Bifidobacterium. Still, studies present controversial and uncertain results about the treatment protocols and actual benefits of this supplementation. [172,182] Researchers attribute these limitations to the significant variability in the samples and the interference of environmental factors [182].
Prebiotics, in turn, promote an increase in populations of beneficial microorganisms, which can impact intestinal health, improve stool consistency, and reduce inflammation of the tract. In animal models, it is suggested that the modulation of the immune system resulting from supplementation with prebiotics culminates in positive effects on the behavior and cognition of individuals with ASD. [172] However, studies in humans are scarce, and standardized doses of supplementation have not yet been established, although it is recommended to include foods that are sources of prebiotics [onions, garlic, bananas, asparagus, among others) in the diet of these patients, adding to a healthy and balanced dietary context. [172,182]
Another treatment that has been studied is fecal microbiota transplantation, which appears to result in more prolonged effects on chronic intestinal disorders and has actions to reduce symptoms of anxiety and depression. [182] On the other hand, there is a greater risk of adverse effects, in addition to being an experimental, invasive, and discouraging procedure, especially in this population. [182]
7. Limitations
Due to the lack of standardization of the scientific literature regarding the diagnostic criteria for ASD and its comorbidities, it would not be possible to seek conclusions based on meta-analysis. For this reason, it was decided to carry out a narrative review, through articles originating only in journals indexed in the main databases. Thus, an important limitation of the present study refers to the fact that it is not possible to generalize the information obtained, which cannot be taken as absolute truths, but rather as paths for intervention opportunities and future investigations.
The paper highlights the lack of consensus regarding dosages and duration of nutritional supplementation for children with Autism Spectrum Disorder (ASD), which complicates treatment approaches. It notes the difficulty in adjusting diets due to the restrictive eating habits of children with ASD, leading to challenges in introducing new foods. The variability in individual responses to dietary interventions and the influence of environmental factors on gut microbiota complicate the establishment of generalized treatment protocols. Additionally, the paper mentions that many signs and symptoms associated with ASD can also be found in the general population, complicating diagnosis.
8. Conclusion
Many children with ASD have restrictive eating habits, leading to nutritional deficiencies that affect physical and cognitive development. They also often experience gastrointestinal problems such as constipation, diarrhea, and gut microbiota imbalances, which can exacerbate behavioral symptoms. This review explored recent evidence on how nutritional, gastrointestinal, and epigenetic factors interact in ASD, highlighting their implications for clinical management and intervention strategies that could improve the development and quality of life of affected children. The diversity of eating habits, defining different profiles of food selectivity, highlights that strategy to provide adequate nutrition for children with ASD cannot be based on a single approach but must consider their personal preferences and different ways of dealing with sensory aspects. It also emphasizes that the therapeutic process must include the participation of the child's whole family in promoting healthy eating habits and that interventions for the practical approach to food is a challenge that requires the involvement of a multidisciplinary professional team. It is important to note that many of the signs and symptoms described in the present review are not exclusive to ASD and can be found in the general population and may even be present in children with ASD without a cause-and-consequence relationship. Figure 2 seeks to summarize the nutritional-related aspects most frequently found in children with ASD.
References
- APA. Diagnostic and Statistical Manual of Mental Disorders. 5th ed: American Psychiatric Publishing (2014).
- CDC. Prevalence of Autism Spectrum Disorder among Children Aged 8 Years — United States, 2020. Centers for Disease Control and Prevention, (2020).
- Esposito M, Mirizzi P, Fadda R, Pirollo C, Ricciardi O, Mazza M, et al. Food Selectivity in Children with Autism: Guidelines for Assessment and Clinical Interventions. Int J Environ Res Public Health (2023) 20(6). Epub 20230314. [CrossRef]
- Iglesias-Vázquez L, Van Ginkel Riba G, Arija V, Canals J. Composition of Gut Microbiota in Children with Autism Spectrum Disorder: A Systematic Review and Meta-Analysis. Nutrients (2020) 12(3). [CrossRef]
- Yap CX, Henders AK, Alvares GA, Wood DLA, Krause L, Tyson GW, et al. Autism-Related Dietary Preferences Mediate Autism-Gut Microbiome Associations. Cell (2021) 184(24):5916-31.e17. Epub 20211111. [CrossRef]
- Carneiro ACdS, Moreira ES, Lisboa CS. Eating Habits and Behaviors of Children with Autism Spectrum Disorder: An Integrative Review. Research, Society and Development (2022) 11(8):e37211830976. [CrossRef]
- da Silva RV, Gomes DL. Eating Behavior and Nutritional Profile of Children with Autism Spectrum Disorder in a Reference Center in the Amazon. Nutrients (2024) 16(3):452.
- Petitpierre G, Luisier A-C, Bensafi M. Eating Behavior in Autism: Senses as a Window Towards Food Acceptance. Current Opinion in Food Science (2021) 41:210-6. [CrossRef]
- Trinh NB, Phan NDT, Bui AT, Phan HT, Nguyen LTT, Nguyen LHT, et al. Nutritional Status and Eating Behavior of Children with Autism Spectrum Disorders in Vietnam: A Case-Control Study. Nutrition and Health (2023):02601060231152278. [CrossRef]
- Lázaro CP, Pondé MP. Narratives of Mothers of Children with Autism Spectrum Disorders: Focus on Eating Behavior. Trends in Psychiatry and Psychotherapy (2017) 39. [CrossRef]
- Plaza-Diaz J, Flores-Rojas K, Torre-Aguilar MJ, Gomez-Fernandez AR, Martin-Borreguero P, Perez-Navero JL, et al. Dietary Patterns, Eating Behavior, and Nutrient Intakes of Spanish Preschool Children with Autism Spectrum Disorders. Nutrients (2021) 13(10):3551. Epub 20211010. [CrossRef]
- Lemes MA, Garcia GP, Carmo BLd, Santiago BA, Teixeira DDB, Agostinho Junior F, et al. Comportamento Alimentar De Crianças Com Transtorno Do Espectro Autista. Jornal Brasileiro de Psiquiatria (2023) 72. [CrossRef]
- Nadeau MV, Richard E, Wallace GL. The Combination of Food Approach and Food Avoidant Behaviors in Children with Autism Spectrum Disorder: "Selective Overeating". Journal of Autism and Developmental Disorders (2022) 52:987+. [CrossRef]
- Nogueira-de-Almeida CA, Del Ciampo LA, Ued FdV, Ferraz IS, Contini AA, Epifanio M, et al. Feeding Difficulties among Brazilian Children: Prevalence and Associated Factors. Research, Society and Development (2022) 11(13). [CrossRef]
- Wenzell ML, Pulver SL, McMahon MXH, Rubio EK, Gillespie S, Berry RC, et al. Clinical Correlates and Prevalence of Food Selectivity in Children with Autism Spectrum Disorder. The Journal of Pediatrics (2024) 269:114004. [CrossRef]
- Kozak A, Czepczor-Bernat K, Modrzejewska J, Modrzejewska A, Matusik E, Matusik P. Avoidant/Restrictive Food Disorder (Arfid), Food Neophobia, Other Eating-Related Behaviours and Feeding Practices among Children with Autism Spectrum Disorder and in Non-Clinical Sample: A Preliminary Study. Int J Environ Res Public Health (2023) 20(10). Epub 20230514. [CrossRef]
- Rodrigues JVS, Poli MCF, Petrilli PH, Dornelles RCM, Turcio KH, Theodoro LH. Food Selectivity and Neophobia in Children with Autism Spectrum Disorder and Neurotypical Development: A Systematic Review. Nutr Rev (2023) 81(8):1034-50. [CrossRef]
- Hodges A, Davis T, Crandall M, Phipps L, Weston R. Using Shaping to Increase Foods Consumed by Children with Autism. J Autism Dev Disord (2017) 47(8):2471-9. [CrossRef]
- Alibrandi A, Zirilli A, Loschiavo F, Gangemi MC, Sindoni A, Tribulato G, et al. Food Selectivity in Children with Autism Spectrum Disorder: A Statistical Analysis in Southern Italy. Children (Basel) (2023) 10(9). Epub 20230914. [CrossRef]
- St John BM, Ausderau KK. The Characterization of Feeding Challenges in Autistic Children. Autism (2024) 28(9):2381-93. Epub 20240202. [CrossRef]
- Kinnaird E, Norton C, Pimblett C, Stewart C, Tchanturia K. Eating as an Autistic Adult: An Exploratory Qualitative Study. PLoS One (2019) 14(8):e0221937. Epub 20190829. [CrossRef]
- Silva ÁGS, Chaves SPL, Almeida LNA, Nascismento RLd, Macêdo MLM, Sarmento AQ. Aspectos Sensoriais E a Seletividade Alimentar Da Criança Com Transtorno Do Espectro Autista: Um Estudo De Revisão Integrativa. Research, Society and Development (2021) 10(10). [CrossRef]
- Sarnat H, Samuel E, Ashkenazi-Alfasi N, Peretz B. Oral Health Characteristics of Preschool Children with Autistic Syndrome Disorder. Journal of Clinical Pediatric Dentistry (2016) 40(1):21-5. [CrossRef]
- Byrska A, Błażejczyk I, Faruga A, Potaczek M, Wilczyński KM, Janas-Kozik M. Patterns of Food Selectivity among Children with Autism Spectrum Disorder. Journal of Clinical Medicine [Internet]. (2023; 12(17). Available from: https://mdpi-res.com/d_attachment/jcm/jcm-12-05469/article_deploy/jcm-12-05469-v2.pdf?version=1693203876.
- Huynh DT, Estorninos E, Capeding RZ, Oliver JS, Low YL, Rosales FJ. Longitudinal Growth and Health Outcomes in Nutritionally at-Risk Children Who Received Long-Term Nutritional Intervention. J Hum Nutr Diet (2015) 28(6):623-35. Epub 20150325. [CrossRef]
- Kerzner B, Milano K, MacLean WC, Berall G, Stuart S, Chatoor I. A Practical Approach to Classifying and Managing Feeding Difficulties. Pediatrics (2015) 135(2):344-53. [CrossRef]
- Milano K, Chatoor I, Kerzner B. A Functional Approach to Feeding Difficulties in Children. Current Gastroenterology Reports (2019) 21(10). [CrossRef]
- Nogueira-de-Almeida C, de Mello E, Filho D, Maximino P, Fisberg M. Consenso Da Associação Brasileira De Nutrologia Sobre O Uso De Suplementos Alimentares Para Crianças Com Dificuldades Alimentares. International Journal of Nutrology (2018) 11(S 01):S4-S15. [CrossRef]
- Nogueira-de-Almeida CA, Del Ciampo LA, Martinez EZ, Contini AA, Nogueira-de-Almeida ME, Ferraz IS, et al. Clinical Evolution of Preschool Picky Eater Children Receiving Oral Nutritional Supplementation during Six Months: A Prospective Controlled Clinical Trial. Children (2023) 10(3). [CrossRef]
- Susilowati E, Umayah A, Diniayuningrum A. Interventions for Managing Picky Eating in Preschool Children: Literature Review. Media Publikasi Promosi Kesehatan Indonesia (MPPKI) (2024) 7(11):2584-91. [CrossRef]
- Breda C, Santero S, Conti MV, Cena H. Programmes to Manage Food Selectivity in Individuals with Autism Spectrum Disorder. Nutr Res Rev (2024):1-14. Epub 20240222. [CrossRef]
- Ahearn WH. Using Simultaneous Presentation to Increase Vegetable Consumption in a Mildly Selective Child with Autism. J Appl Behav Anal (2003) 36(3):361-5. [CrossRef]
- Sarnat H, Samuel E, Ashkenazi-Alfasi N, Peretz B. Oral Health Characteristics of Preschool Children with Autistic Syndrome Disorder. J Clin Pediatr Dent (2016) 40(1):21-5. [CrossRef]
- Soares RCS, Candido FG, Filgueiras MS, Rosa COB, de Novaes JF, Araujo RMA. Problematic Behaviors at Mealtimes and the Nutritional Status of Brazilian Children with Autism Spectrum Disorder. Front Public Health (2024) 12:1392478. Epub 20241014. [CrossRef]
- Toomey KA, Ross ES. Sos Approach to Feeding. Perspectives on Swallowing and Swallowing Disorders (Dysphagia) (2011) 20(3):82-7. [CrossRef]
- Benson JD, Parke CS, Gannon C, Muñoz D. A Retrospective Analysis of the Sequential Oral Sensory Feeding Approach in Children with Feeding Difficulties. Journal of Occupational Therapy, Schools, & Early Intervention (2013) 6(4):289-300. [CrossRef]
- Maitin-Shepard M, O'Tierney-Ginn P, Kraneveld AD, Lyall K, Fallin D, Arora M, et al. Food, Nutrition, and Autism: From Soil to Fork. Am J Clin Nutr (2024) 120(1):240-56. Epub 20240425. [CrossRef]
- Keski-Rahkonen A, Ruusunen A. Avoidant-Restrictive Food Intake Disorder and Autism: Epidemiology, Etiology, Complications, Treatment, and Outcome. Curr Opin Psychiatry (2023) 36(6):438-42. Epub 20230829. [CrossRef]
- Nyholmer M, Wronski M-L, Hog L, Kuja-Halkola R, Lichtenstein P, Lundström S, et al. (2024). [CrossRef]
- Wronski M-L, Kuja-Halkola R, Hedlund E, Martini MI, Lichtenstein P, Lundström S, et al. (2024). [CrossRef]
- James RM, O’Shea J, Micali N, Russell SJ, Hudson LD. Physical Health Complications in Children and Young People with Avoidant Restrictive Food Intake Disorder (Arfid): A Systematic Review and Meta-Analysis. BMJ Paediatrics Open (2024) 8(1). [CrossRef]
- Thomas JJ, Lawson EA, Micali N, Misra M, Deckersbach T, Eddy KT. Avoidant/Restrictive Food Intake Disorder: A Three-Dimensional Model of Neurobiology with Implications for Etiology and Treatment. Current Psychiatry Reports (2017) 19(8). [CrossRef]
- Thomas JJ, Wons OB, Eddy KT. Cognitive–Behavioral Treatment of Avoidant/Restrictive Food Intake Disorder. Current Opinion in Psychiatry (2018) 31(6):425-30. [CrossRef]
- Hyman SL, Levy SE, Myers SM, Council On Children With Disabilities SOD, Behavioral P. Identification, Evaluation, and Management of Children with Autism Spectrum Disorder. Pediatrics (2020) 145(1). Epub 20191216. [CrossRef]
- Nadon G, Feldman DE, Dunn W, Gisel E. Association of Sensory Processing and Eating Problems in Children with Autism Spectrum Disorders. Autism Research and Treatment (2011) 2011:1-8. [CrossRef]
- Bahadir A, Reis PG, Erduran E. Oral Vitamin B12 Treatment Is Effective for Children with Nutritional Vitamin B12 Deficiency. Journal of Paediatrics and Child Health (2014) 50(9):721-5. [CrossRef]
- Bastos Maia S, Rolland Souza AS, Costa Caminha MdF, Lins da Silva S, Callou Cruz RdSBL, Carvalho dos Santos C, et al. Vitamin a and Pregnancy: A Narrative Review. Nutrients (2019) 11(3). [CrossRef]
- Chandra J, Dewan P, Kumar P, Mahajan A, Singh P, Dhingra B, et al. Diagnosis, Treatment and Prevention of Nutritional Anemia in Children: Recommendations of the Joint Committee of Pediatric Hematology-Oncology Chapter and Pediatric and Adolescent Nutrition Society of the Indian Academy of Pediatrics. Indian Pediatr (2022) 59(10):782-801.
- Devalia V, Hamilton MS, Molloy AM. Guidelines for the Diagnosis and Treatment of Cobalamin and Folate Disorders. British Journal of Haematology (2014) 166(4):496-513. [CrossRef]
- Hemamy M, Pahlavani N, Amanollahi A, Islam SMS, McVicar J, Askari G, et al. The Effect of Vitamin D and Magnesium Supplementation on the Mental Health Status of Attention-Deficit Hyperactive Children: A Randomized Controlled Trial. BMC Pediatrics (2021) 21(1). [CrossRef]
- Imdad A, Rogner J, Sherwani RN, Sidhu J, Regan A, Haykal MR, et al. Zinc Supplementation for Preventing Mortality, Morbidity, and Growth Failure in Children Aged 6 Months to 12 Years. Cochrane Database of Systematic Reviews (2023) 2023(3). [CrossRef]
- Kaczmarek KA, Dobrzyńska M, Drzymała-Czyż S. Iron, Magnesium, Zinc and Selenium - the Most Common Elemental Deficiencies in Children with Autism Spectrum Disorder. Research in Autism Spectrum Disorders (2024) 110. [CrossRef]
- Khan KM, Jialal I. Folic Acid Deficiency. Statpearls. Treasure Island (FL)(2024).
- McGuire S. Who Guideline: Vitamin a Supplementation in Pregnant Women. Geneva: Who, 2011; Who Guideline: Vitamin a Supplementation in Postpartum Women. Geneva: Who, 2011. Advances in Nutrition (2012) 3(2):215-6. [CrossRef]
- Mousain-Bosc M, Siatka C, Bali JP. Magnesium, Hyperactivity and Autism in Children. In: Vink R, Nechifor M, editors. Magnesium in the Central Nervous System. Adelaide (AU): University of Adelaide Press. © 2011 The Authors. (2011).
- Munns CF, Shaw N, Kiely M, Specker BL, Thacher TD, Ozono K, et al. Global Consensus Recommendations on Prevention and Management of Nutritional Rickets. The Journal of Clinical Endocrinology & Metabolism (2016) 101(2):394-415. [CrossRef]
- Nogueira-de-Almeida CA, Fernandes SL, Soriano EdA, Lourenço DM, Zotarelli Filho IJ, Iucif Junior N, et al. Consensus of the Brazilian Association of Nutrology on Diagnosis, Prophylaxis, and Treatment of Vitamin B12 Deficiency. International Journal of Nutrology (2023) 16(1). [CrossRef]
- Rasmussen SA, Fernhoff PM, Scanlon KS. Vitamin B12 Deficiency in Children and Adolescents. The Journal of Pediatrics (2001) 138(1):10-7. [CrossRef]
- Ross DA. Recommendations for Vitamin a Supplementation. The Journal of Nutrition (2002) 132(9):2902S-6S. [CrossRef]
- Sezer RG, Bozaykut A, Akoğlu HA, Özdemir GN. The Efficacy of Oral Vitamin B12 Replacement for Nutritional Vitamin B12 Deficiency. Journal of Pediatric Hematology/Oncology (2018) 40(2):e69-e72. [CrossRef]
- Srinivasan S, O'Rourke J, Bersche Golas S, Neumeyer A, Misra M. Calcium and Vitamin D Supplement Prescribing Practices among Providers Caring for Children with Autism Spectrum Disorders: Are We Addressing Bone Health? Autism Res Treat (2016) 2016:6763205. Epub 2016/04/05. [CrossRef]
- Valavi E, Hakimzadeh M, Shamsizadeh A, Aminzadeh M, Alghasi A. The Efficacy of Zinc Supplementation on Outcome of Children with Severe Pneumonia. A Randomized Double-Blind Placebo-Controlled Clinical Trial. Indian J Pediatr (2011) 78(9):1079-84. Epub 2011/06/11. [CrossRef]
- Weinstein M, Babyn P, Zlotkin S. An Orange a Day Keeps the Doctor Away: Scurvy in the Year 2000. Pediatrics (2001) 108(3):e55-e. [CrossRef]
- Peretti S, Mariano M, Mazzocchetti C, Mazza M, Pino MC, Verrotti Di Pianella A, et al. Diet: The Keystone of Autism Spectrum Disorder? Nutritional Neuroscience (2018) 22(12):825-39. [CrossRef]
- Molina-López J, Leiva-García B, Planells E, Planells P. Food Selectivity, Nutritional Inadequacies, and Mealtime Behavioral Problems in Children with Autism Spectrum Disorder Compared to Neurotypical Children. International Journal of Eating Disorders (2021) 54(12):2155-66. [CrossRef]
- Omaña Covarrubias A, Hernández Fernández IG, Conde Vega J, Rodríguez Ávila J, Díaz Martínez G, Moya Escalera A, et al. Nutritional Status and Food Intake Frequency in Children with Autism Spectrum Disorder. Nutrición Hospitalaria (2023). [CrossRef]
- Trinh NB, Phan NDT, Bui AT, Phan HT, Nguyen LTT, Nguyen LHT, et al. Nutritional Status and Eating Behavior of Children with Autism Spectrum Disorders in Vietnam: A Case-Control Study. Nutr Health (2023):2601060231152278. Epub 20230127. [CrossRef]
- Narzisi A, Masi G, Grossi E. Nutrition and Autism Spectrum Disorder: Between False Myths and Real Research-Based Opportunities. Nutrients (2021) 13(6). [CrossRef]
- Sharp WG, Postorino V, McCracken CE, Berry RC, Criado KK, Burrell TL, et al. Dietary Intake, Nutrient Status, and Growth Parameters in Children with Autism Spectrum Disorder and Severe Food Selectivity: An electronic Medical Record Review. Journal of the Academy of Nutrition and Dietetics (2018) 118(10):1943-50. [CrossRef]
- Ali F, Mouzaki M. Nutritional Deficiencies in Children. Curr Opin Gastroenterol (2024) 40(2):106-11. Epub 20240102. [CrossRef]
- G. Santiago F, D. S. Lyra E, Da Silva Pantoja P. A Systematic Review: Nutritional Status and the Effect in Autism Spectrum Disorder. Brazilian Journal of Health and Biomedical Sciences (2024) 23(1). [CrossRef]
- Adams JB, Kirby J, Audhya T, Whiteley P, Bain J. Vitamin/Mineral/Micronutrient Supplement for Autism Spectrum Disorders: A Research Survey. BMC Pediatr (2022) 22(1):590. Epub 20221013. [CrossRef]
- Al-Beltagi M, Saeed NK, Bediwy AS, Elbeltagi R, Alhawamdeh R. Role of Gastrointestinal Health in Managing Children with Autism Spectrum Disorder. World J Clin Pediatr (2023) 12(4):171-96. Epub 20230909. [CrossRef]
- Arija V, Esteban-Figuerola P, Morales-Hidalgo P, Jardi C, Canals-Sans J. Nutrient Intake and Adequacy in Children with Autism Spectrum Disorder: Epined Epidemiological Study. Autism (2023) 27(2):371-88. Epub 20220620. [CrossRef]
- De Moraes LS, Bubolz VK, Marques AyC, Borges LR, Muniz LC, Bertacco RTA. Seletividade Alimentar Em Crianças E Adolescente Com Transtorno Do Espectro Autista. Revista da Associação Brasileira de Nutrição - RASBRAN (2021) 12(2):42-58. [CrossRef]
- Kittana M, Ahmadani A, Williams KE, Attlee A. Nutritional Status and Feeding Behavior of Children with Autism Spectrum Disorder in the Middle East and North Africa Region: A Systematic Review. Nutrients (2023) 15(3). Epub 20230130. [CrossRef]
- Li YJ, Xie XN, Lei X, Li YM, Lei X. Global Prevalence of Obesity, Overweight and Underweight in Children, Adolescents and Adults with Autism Spectrum Disorder, Attention-Deficit Hyperactivity Disorder: A Systematic Review and Meta-Analysis. Obesity Reviews (2020) 21(12). [CrossRef]
- Sammels O, Karjalainen L, Dahlgren J, Wentz E. Autism Spectrum Disorder and Obesity in Children: A Systematic Review and Meta-Analysis. Obes Facts (2022) 15(3):305-20. Epub 20220309. [CrossRef]
- Esteban-Figuerola P, Canals J, Fernández-Cao JC, Arija Val V. Differences in Food Consumption and Nutritional Intake between Children with Autism Spectrum Disorders and Typically Developing Children: A Meta-Analysis. Autism (2018) 23(5):1079-95. [CrossRef]
- Neumeyer AM, Cano Sokoloff N, McDonnell EI, Macklin EA, McDougle CJ, Holmes TM, et al. Nutrition and Bone Density in Boys with Autism Spectrum Disorder. J Acad Nutr Diet (2018) 118(5):865-77. Epub 20180302. [CrossRef]
- Sharp WG, Berry RC, McCracken C, Nuhu NN, Marvel E, Saulnier CA, et al. Feeding Problems and Nutrient Intake in Children with Autism Spectrum Disorders: A Meta-Analysis and Comprehensive Review of the Literature. J Autism Dev Disord (2013) 43(9):2159-73. [CrossRef]
- Tomova A, Soltys K, Kemenyova P, Karhanek M, Babinska K. The Influence of Food Intake Specificity in Children with Autism on Gut Microbiota. Int J Mol Sci (2020) 21(8). Epub 20200417. [CrossRef]
- Yule S, Wanik J, Holm EM, Bruder MB, Shanley E, Sherman CQ, et al. Nutritional Deficiency Disease Secondary to Arfid Symptoms Associated with Autism and the Broad Autism Phenotype: A Qualitative Systematic Review of Case Reports and Case Series. Journal of the Academy of Nutrition and Dietetics (2021) 121(3):467-92. [CrossRef]
- da Silva RV, Gomes DL. Eating Behavior and Nutritional Profile of Children with Autism Spectrum Disorder in a Reference Center in the Amazon. Nutrients (2024) 16(3). [CrossRef]
- Magagnin T, Silva MAd, Nunes RZdS, Ferraz F, Soratto J. Aspectos Alimentares E Nutricionais De Crianças E Adolescentes Com Transtorno Do Espectro Autista. Physis: Revista de Saúde Coletiva (2021) 31(1). [CrossRef]
- Marinov D, Chamova R, Pancheva R. Micronutrient Deficiencies in Children with Autism Spectrum Disorders Compared to Typically Developing Children – a Scoping Review. Research in Autism Spectrum Disorders (2024) 114. [CrossRef]
- Meguid NA, Anwar M, Bjorklund G, Hashish A, Chirumbolo S, Hemimi M, et al. Dietary Adequacy of Egyptian Children with Autism Spectrum Disorder Compared to Healthy Developing Children. Metab Brain Dis (2017) 32(2):607-15. Epub 20170110. [CrossRef]
- Dosman CF, Brian JA, Drmic IE, Senthilselvan A, Harford MM, Smith RW, et al. Children with Autism: Effect of Iron Supplementation on Sleep and Ferritin. Pediatr Neurol (2007) 36(3):152-8. [CrossRef]
- Sidrak S, Yoong T, Woolfenden S. Iron Deficiency in Children with Global Developmental Delay and Autism Spectrum Disorder. J Paediatr Child Health (2014) 50(5):356-61. Epub 20131223. [CrossRef]
- Conti MV, Santero S, Luzzi A, Cena H. Exploring Potential Mechanisms for Zinc Deficiency to Impact in Autism Spectrum Disorder: A Narrative Review. Nutr Res Rev (2023):1-9. Epub 20230920. [CrossRef]
- Ross MM, Hernandez-Espinosa DR, Aizenman E. Neurodevelopmental Consequences of Dietary Zinc Deficiency: A Status Report. Biol Trace Elem Res (2023) 201(12):5616-39. Epub 20230325. [CrossRef]
- Siddiqi UR, Begum S, Shahjadi S, Afroz S, Mahruba SN, Parvin J, et al. Plasma Zinc, Copper and Serum Ceruloplasmin Levels of Autism Spectrum Disorder Children in Bangladesh. Heliyon (2023) 9(8):e18624. Epub 20230809. [CrossRef]
- Kambe T, Fukue K, Ishida R, Miyazaki S. Overview of Inherited Zinc Deficiency in Infants and Children. J Nutr Sci Vitaminol (Tokyo) (2015) 61 Suppl:S44-6. [CrossRef]
- Hartman JS, Silver AH. Nutritional Rickets Due to Severe Food Selectivity in Autism Spectrum Disorder. Journal of Developmental & Behavioral Pediatrics (2021) 42(1):66-72. [CrossRef]
- Jacob M, Censani M, Faridi MMA. 13-Year-Old Boy Presenting with Bilateral Femur Fractures in the Setting of Severe Vitamin D Deficiency. Case Reports in Pediatrics (2021) 2021:1-4. [CrossRef]
- Pia Riccio M, Catone G, Siracusano R, Occhiati L, Bernardo P, Sarnataro E, et al. Vitamin D Deficiency Is Not Related to Eating Habits in Children with Autistic Spectrum Disorder. AIMS Public Health (2020) 7(4):792-803. [CrossRef]
- Şengenç E, Kıykım E, Saltik S. Vitamin D Levels in Children and Adolescents with Autism. Journal of International Medical Research (2020) 48(7). [CrossRef]
- Wang T, Shan L, Du L, Feng J, Xu Z, Staal WG, et al. Serum Concentration of 25-Hydroxyvitamin D in Autism Spectrum Disorder: A Systematic Review and Meta-Analysis. European Child & Adolescent Psychiatry (2015) 25(4):341-50. [CrossRef]
- Çıtar Dazıroğlu ME, Sağdıçoğlu Celep AG. Determination of Nutrient Intake and Dietary Antioxidant Capacity in Autism Spectrum Disorder: A Case–Control Study. Journal of Autism and Developmental Disorders (2023) 54(6):2322-32. [CrossRef]
- Shom S, Saha S, Chatterjee M, Sinha S, Mukhopadhyay K. Indian Asd Probands with 25(Oh)D and Vitamin D Binding Protein Deficiency Exhibited Higher Severity. Scientific Reports (2024) 14(1). [CrossRef]
- Bener A, Khattab A, Al-Dabbagh M. Is High Prevalence of Vitamin D Deficiency Evidence for Autism Disorder?: In a Highly Endogamous Population. Journal of Pediatric Neurosciences (2014) 9(3). [CrossRef]
- van der Lubbe A, Swaab H, Vermeiren R, van den Akker E, Ester W. Novel Insights into Obesity in Preschool Children with Autism Spectrum Disorder. Child Psychiatry & Human Development (2024). [CrossRef]
- Fiamenghi VI, Mello EDd. Vitamin D Deficiency in Children and Adolescents with Obesity: A Meta-Analysis. Jornal de Pediatria (2021) 97(3):273-9. [CrossRef]
- Feng J, Shan L, Du L, Wang B, Li H, Wang W, et al. Clinical Improvement Following Vitamin D3 Supplementation in Autism Spectrum Disorder. Nutritional Neuroscience (2016) 20(5):284-90. [CrossRef]
- Altun H, Kurutaş EB, Şahin N, Güngör O, Fındıklı E. The Levels of Vitamin D, Vitamin D Receptor, Homocysteine and Complex B Vitamin in Children with Autism Spectrum Disorders. Clinical Psychopharmacology and Neuroscience (2018) 16(4):383-90. [CrossRef]
- Qi X, Yang T, Chen J, Dai Y, Chen L, Wu L, et al. Vitamin D Status Is Primarily Associated with Core Symptoms in Children with Autism Spectrum Disorder: A Multicenter Study in China. Psychiatry Research (2022) 317. [CrossRef]
- Vargas DL, Nascimbene C, Krishnan C, Zimmerman AW, Pardo CA. Neuroglial Activation and Neuroinflammation in the Brain of Patients with Autism. Annals of Neurology (2004) 57(1):67-81. [CrossRef]
- Noriega DB, Savelkoul HFJ. Immune Dysregulation in Autism Spectrum Disorder. European Journal of Pediatrics (2013) 173(1):33-43. [CrossRef]
- Esnafoglu E, Subaşı B. Association of Low 25-Oh-Vitamin D Levels and Peripheral Inflammatory Markers in Patients with Autism Spectrum Disorder. Psychiatry Research (2022) 316. [CrossRef]
- Sweetman DU, O'Donnell SM, Lalor A, Grant T, Greaney H. Zinc and Vitamin a Deficiency in a Cohort of Children with Autism Spectrum Disorder. Child: Care, Health and Development (2019) 45(3):380-6. [CrossRef]
- Yang T, Chen L, Dai Y, Jia F, Hao Y, Li L, et al. Vitamin a Status Is More Commonly Associated with Symptoms and Neurodevelopment in Boys with Autism Spectrum Disorders—a Multicenter Study in China. Frontiers in Nutrition (2022) 9. [CrossRef]
- Chiu M, Watson S. Xerophthalmia and Vitamin a Deficiency in an Autistic Child with a Restricted Diet. BMJ Case Rep (2015) 2015. Epub 20151005. [CrossRef]
- Moreno N, Lynch FC, Zalazar MA, Miranda CF, Vidal SH, Armeno ML. [Decreased Vision Due to Hypovitaminosis a in Children with Food Selectivity]. Medicina (B Aires) (2024) 84(5):860-7.
- Godfrey D, Stone RT, Lee M, Chitnis T, Santoro JD. Triad of Hypovitaminosis a, Hyperostosis, and Optic Neuropathy in Males with Autism Spectrum Disorders. Nutritional Neuroscience (2021) 25(8):1697-703. [CrossRef]
- Togari A, Kondo M, Arai M, Matsumoto S. Effects of Retinoic Acid on Bone Formation and Resorption in Cultured Mouse Calvaria. General Pharmacology: The Vascular System (1991) 22(2):287-92. [CrossRef]
- Sharp WG, Berry RC, Burrell L, Scahill L, McElhanon BO. Scurvy as a Sequela of Avoidant-Restrictive Food Intake Disorder in Autism: A Systematic Review. Journal of Developmental & Behavioral Pediatrics (2020) 41(5):397-405. [CrossRef]
- Kinlin LM, Weinstein M. Scurvy: Old Disease, New Lessons. Paediatrics and International Child Health (2023) 43(4):83-94. [CrossRef]
- Al-Farsi YM, Waly MI, Deth RC, Al-Sharbati MM, Al-Shafaee M, Al-Farsi O, et al. Low Folate and Vitamin B12 Nourishment Is Common in Omani Children with Newly Diagnosed Autism. Nutrition (2013) 29(3):537-41. Epub 20130101. [CrossRef]
- Tsujiguchi H, Miyagi S, Nguyen TTT, Hara A, Ono Y, Kambayashi Y, et al. Relationship between Autistic Traits and Nutrient Intake among Japanese Children and Adolescents. Nutrients (2020) 12(8). [CrossRef]
- Yektaş Ç, Alpay M, Tufan AE. <P>Comparison of Serum B12, Folate and Homocysteine Concentrations in Children with Autism Spectrum Disorder or Attention Deficit Hyperactivity Disorder and Healthy Controls</P>. Neuropsychiatric Disease and Treatment (2019) Volume 15:2213-9. [CrossRef]
- Erden S, Akbaş İleri B, Sadıç Çelikkol Ç, Nalbant K, Kılınç İ, Yazar A. Serum B12, Homocysteine, and Anti-Parietal Cell Antibody Levels in Children with Autism. International Journal of Psychiatry in Clinical Practice (2021) 26(1):8-13. [CrossRef]
- Zou M, Zhang Y, Li D, Li S, Hu J, Gao Y, et al. Correlation of Co-Morbidities with Symptom Severity of Children with Autism Spectrum Disorder: A Cross-Sectional Survey. Nutrients (2024) 16(17). [CrossRef]
- Baird JS, Ravindranath TM. Vitamin B Deficiencies in a Critically Ill Autistic Child with a Restricted Diet. Nutrition in Clinical Practice (2014) 30(1):100-3. [CrossRef]
- Ângelo KHdA, Silva Filho PFd, Araújo NDd, Guedes TAL, Almeida LHAd. Suplementação Nutricional Como Abordagem Terapêutica No Transtorno Do Espectro Autista: Uma Revisão De Literatura. Research, Society and Development (2021) 10(9). [CrossRef]
- Monteiro MA, Santos AAAd, Gomes LMM, Rito RVVF. Autism Spectrum Disorder: A Systematic Review About Nutritional Interventions. Revista Paulista de Pediatria (2020) 38. [CrossRef]
- Jayashree R, Gayathri G, Udayakumar N. Nutritional Supplements in Autism Spectrum Disorder: A Scoping Review. International Journal of Nutrition, Pharmacology, Neurological Diseases (2024) 14(2):153-6. [CrossRef]
- Leonario Rodríguez M, Díaz Vargas D. Effectiveness of Nutritional Interventions on Behavioral Symptomatology of Autism Spectrum Disorder: A Systematic Review. Nutrición Hospitalaria (2022). [CrossRef]
- Meguid NA, Bjørklund G, Gebril OH, Doşa MD, Anwar M, Elsaeid A, et al. The Role of Zinc Supplementation on the Metallothionein System in Children with Autism Spectrum Disorder. Acta Neurologica Belgica (2019) 119(4):577-83. [CrossRef]
- Maximino P, Fisberg M. A Alimentação Da Criança Com Transtorno Do Espectro Autista. São Paulo: Centro de Excelência em Nutrição e Dificuldades Alimentares (CENDA) do Instituto PENSI (2024). Available from: https://autismoerealidade.org.br/convivendo-com-o-tea/cartilhas/cartilha-a-alimentacao-da-crianca-com-tea/.
- Kahathuduwa CN, Dhanasekara CS, Wakefield S, Moustaid-Moussa N, Mastergeorge A. Autism Spectrum Disorder Is Associated with an Increased Risk of Development of Underweight in Children and Adolescents: A Systematic Review and Meta-Analysis. Research in Autism Spectrum Disorders (2022) 94:101969. [CrossRef]
- Malhi P, Saini S, Bharti B, Attri S, Sankhyan N. Sensory Processing Dysfunction and Mealtime Behavior Problems in Children with Autism. Indian Pediatr (2021) 58(9):842-5. Epub 20210520.
- Ward JH, Weir E, Allison C, Baron-Cohen S. Increased Rates of Chronic Physical Health Conditions across All Organ Systems in Autistic Adolescents and Adults. Molecular Autism (2023) 14(1):35. [CrossRef]
- Nuyttens L, De Vlieger L, Diels M, Schrijvers R, Bullens DMA. The Clinical and Immunological Basis of Early Food Introduction in Food Allergy Prevention. Frontiers in Allergy (2023) 4. [CrossRef]
- Bölte S, Özkara N, Poustka F. Autism Spectrum Disorders and Low Body Weight: Is There Really a Systematic Association? International Journal of Eating Disorders (2002) 31(3):349-51. [CrossRef]
- Talmi Z, Mankuta D, Raz R. Birth Weight and Autism Spectrum Disorder: A Population-Based Nested Case–Control Study. Autism Research (2020) 13(4):655-65. [CrossRef]
- Wei L, Zhong S, Nie S, Gong G. Aberrant Development of the Asymmetry between Hemispheric Brain White Matter Networks in Autism Spectrum Disorder. Eur Neuropsychopharmacol (2018) 28(1):48-62. Epub 20171207. [CrossRef]
- Adams JB, Audhya T, Geis E, Gehn E, Fimbres V, Pollard EL, et al. Comprehensive Nutritional and Dietary Intervention for Autism Spectrum Disorder-a Randomized, Controlled 12-Month Trial. Nutrients (2018) 10(3). Epub 20180317. [CrossRef]
- Lordan R, Storni C, De Benedictis CA. Autism Spectrum Disorders: Diagnosis and Treatment. In: Grabrucker AM, editor. Autism Spectrum Disorders. Brisbane (AU): Exon Publications. Copyright: The Authors. (2021).
- Siafis S, Çıray O, Wu H, Schneider-Thoma J, Bighelli I, Krause M, et al. Pharmacological and Dietary-Supplement Treatments for Autism Spectrum Disorder: A Systematic Review and Network Meta-Analysis. Mol Autism (2022) 13(1):10. Epub 20220304. [CrossRef]
- SBP. Obesidade Na Infância E Adolescência – Manual De Orientação. 3 ed. Weffort VRS, editor. São Paulo: Departamento de Nutrologia da Sociedade Brasileira de Pediatria (2019).
- Micai M, Fatta LM, Gila L, Caruso A, Salvitti T, Fulceri F, et al. Prevalence of Co-Occurring Conditions in Children and Adults with Autism Spectrum Disorder: A Systematic Review and Meta-Analysis. Neurosci Biobehav Rev (2023) 155:105436. Epub 20231031. [CrossRef]
- Nogueira-de-Almeida CA, Weffort VRS, Ued FdV, Ferraz IS, Contini AA, Martinez EZ, et al. What Causes Obesity in Children and Adolescents? Jornal de Pediatria (2024) 100:S48-S56. [CrossRef]
- Kahathuduwa CN, West BD, Blume J, Dharavath N, Moustaid-Moussa N, Mastergeorge A. The Risk of Overweight and Obesity in Children with Autism Spectrum Disorders: A Systematic Review and Meta-Analysis. Obes Rev (2019) 20(12):1667-79. Epub 20191008. [CrossRef]
- Dhaliwal KK, Orsso CE, Richard C, Haqq AM, Zwaigenbaum L. Risk Factors for Unhealthy Weight Gain and Obesity among Children with Autism Spectrum Disorder. Int J Mol Sci (2019) 20(13). Epub 20190704. [CrossRef]
- Ortega-García JA, Kloosterman N, Alvarez L, Tobarra-Sánchez E, Cárceles-Álvarez A, Pastor-Valero R, et al. Full Breastfeeding and Obesity in Children: A Prospective Study from Birth to 6 Years. Childhood Obesity (2018) 14(5):327-37. [CrossRef]
- Tseng PT, Chen YW, Stubbs B, Carvalho AF, Whiteley P, Tang CH, et al. Maternal Breastfeeding and Autism Spectrum Disorder in Children: A Systematic Review and Meta-Analysis. Nutr Neurosci (2019) 22(5):354-62. Epub 20171018. [CrossRef]
- Evans EW, Must A, Anderson SE, Curtin C, Scampini R, Maslin M, et al. Dietary Patterns and Body Mass Index in Children with Autism and Typically Developing Children. Res Autism Spectr Disord (2012) 6(1):399-405. [CrossRef]
- Bandini LG, Anderson SE, Curtin C, Cermak S, Evans EW, Scampini R, et al. Food Selectivity in Children with Autism Spectrum Disorders and Typically Developing Children. J Pediatr (2010) 157(2):259-64. Epub 20100401. [CrossRef]
- Correll CU, Manu P, Olshanskiy V, Napolitano B, Kane JM, Malhotra AK. Cardiometabolic Risk of Second-Generation Antipsychotic Medications during First-Time Use in Children and Adolescents. JAMA (2009) 302(16):1765-73. [CrossRef]
- Lai M-C, Lombardo MV, Baron-Cohen S. Autism. The Lancet (2014) 383(9920):896-910. [CrossRef]
- Jones RA, Downing K, Rinehart NJ, Barnett LM, May T, McGillivray JA, et al. Physical Activity, Sedentary Behavior and Their Correlates in Children with Autism Spectrum Disorder: A Systematic Review. PLoS One (2017) 12(2):e0172482. Epub 20170228. [CrossRef]
- Bishop SL, Havdahl KA, Huerta M, Lord C. Subdimensions of Social-Communication Impairment in Autism Spectrum Disorder. J Child Psychol Psychiatry (2016) 57(8):909-16. Epub 20160108. [CrossRef]
- McPhillips M, Finlay J, Bejerot S, Hanley M. Motor Deficits in Children with Autism Spectrum Disorder: A Cross-Syndrome Study. Autism Research (2014) 7(6):664-76. [CrossRef]
- Healy S, Haegele JA, Grenier M, Garcia JM. Physical Activity, Screen-Time Behavior, and Obesity among 13-Year Olds in Ireland with and without Autism Spectrum Disorder. J Autism Dev Disord (2017) 47(1):49-57. [CrossRef]
- Mazurek MO, Wenstrup C. Television, Video Game and Social Media Use among Children with Asd and Typically Developing Siblings. J Autism Dev Disord (2013) 43(6):1258-71. [CrossRef]
- Maxwell-Horn A, Malow BA. Sleep in Autism. Semin Neurol (2017) 37(4):413-8. Epub 20170824. [CrossRef]
- Zuckerman KE, Hill AP, Guion K, Voltolina L, Fombonne E. Overweight and Obesity: Prevalence and Correlates in a Large Clinical Sample of Children with Autism Spectrum Disorder. J Autism Dev Disord (2014) 44(7):1708-19. [CrossRef]
- Bachmann-Gagescu R, Mefford HC, Cowan C, Glew GM, Hing AV, Wallace S, et al. Recurrent 200-Kb Deletions of 16p11.2 That Include the Sh2b1 Gene Are Associated with Developmental Delay and Obesity. Genet Med (2010) 12(10):641-7. [CrossRef]
- Walters RG, Jacquemont S, Valsesia A, de Smith AJ, Martinet D, Andersson J, et al. A New Highly Penetrant Form of Obesity Due to Deletions on Chromosome 16p11.2. Nature (2010) 463(7281):671-5. [CrossRef]
- Bennett EA, Kolko RP, Chia L, Elliott JP, Kalarchian MA. Treatment of Obesity among Youth with Intellectual and Developmental Disabilities: An Emerging Role for Telenursing. West J Nurs Res (2017) 39(8):1008-27. Epub 20170328. [CrossRef]
- Leekam SR, Nieto C, Libby SJ, Wing L, Gould J. Describing the Sensory Abnormalities of Children and Adults with Autism. Journal of Autism and Developmental Disorders (2006) 37(5):894-910. [CrossRef]
- Hinckson EA, Dickinson A, Water T, Sands M, Penman L. Physical Activity, Dietary Habits and Overall Health in Overweight and Obese Children and Youth with Intellectual Disability or Autism. Res Dev Disabil (2013) 34(4):1170-8. Epub 20130209. [CrossRef]
- Helsel BC, Foster RNS, Sherman J, Steele R, Ptomey LT, Montgomery R, et al. The Family Nutrition and Physical Activity Survey: Comparisons with Obesity and Physical Activity in Adolescents with Autism Spectrum Disorder. J Autism Dev Disord (2023) 53(1):89-95. Epub 20220104. [CrossRef]
- Draudviliene L, Draudvila J, Stankeviciute S, Daniuseviciute-Brazaite L. Two Physiotherapy Methods to Improve the Physical Condition of Children with Autism Spectrum Disorder. Children (Basel) (2024) 11(7). Epub 20240628. [CrossRef]
- Mano-Sousa BJ, Pedrosa AM, Alves BC, Galduróz JCF, Belo VS, Chaves VE, et al. Effects of Risperidone in Autistic Children and Young Adults: A Systematic Review and Meta-Analysis. Current Neuropharmacology (2021) 19(4):538-52. [CrossRef]
- Järvinen A, Laine MK, Tikkanen R, Castrén ML. Beneficial Effects of Glp-1 Agonist in a Male with Compulsive Food-Related Behavior Associated with Autism. Frontiers in Psychiatry (2019) 10. [CrossRef]
- Hung LY, Margolis KG. Autism Spectrum Disorders and the Gastrointestinal Tract: Insights into Mechanisms and Clinical Relevance. Nature Reviews Gastroenterology & Hepatology (2023) 21(3):142-63. [CrossRef]
- Madra M, Ringel R, Margolis KG. Gastrointestinal Issues and Autism Spectrum Disorder. Psychiatric Clinics of North America (2021) 44(1):69-81. [CrossRef]
- Holingue C, Pfeiffer D, Ludwig NN, Reetzke R, Hong JS, Kalb LG, et al. Prevalence of Gastrointestinal Symptoms among Autistic Individuals, with and without Co-Occurring Intellectual Disability. Autism Research (2023) 16(8):1609-18. [CrossRef]
- Holingue C, Poku O, Pfeiffer D, Murray S, Fallin MD. Gastrointestinal Concerns in Children with Autism Spectrum Disorder: A Qualitative Study of Family Experiences. Autism (2021) 26(7):1698-711. [CrossRef]
- McElhanon BO, McCracken C, Karpen S, Sharp WG. Gastrointestinal Symptoms in Autism Spectrum Disorder: A Meta-Analysis. Pediatrics (2014) 133(5):872-83. [CrossRef]
- Al-Beltagi M. Nutritional Management and Autism Spectrum Disorder: A Systematic Review. World Journal of Clinical Pediatrics (2024) 13(4). [CrossRef]
- Wang X, Tang R, Wei Z, Zhan Y, Lu J, Li Z. The Enteric Nervous System Deficits in Autism Spectrum Disorder. Frontiers in Neuroscience (2023) 17. [CrossRef]
- Xu G, Snetselaar LG, Jing J, Liu B, Strathearn L, Bao W. Association of Food Allergy and Other Allergic Conditions with Autism Spectrum Disorder in Children. JAMA Network Open (2018) 1(2). [CrossRef]
- Yu Y, Zhao F. Microbiota-Gut-Brain Axis in Autism Spectrum Disorder. Journal of Genetics and Genomics (2021) 48(9):755-62. [CrossRef]
- Ferguson BJ, Dovgan K, Takahashi N, Beversdorf DQ. The Relationship among Gastrointestinal Symptoms, Problem Behaviors, and Internalizing Symptoms in Children and Adolescents with Autism Spectrum Disorder. Frontiers in Psychiatry (2019) 10. [CrossRef]
- Nogay NH, Nahikian-Nelms M. Effects of Nutritional Interventions in Children and Adolescents with Autism Spectrum Disorder: An Overview Based on a Literature Review. International Journal of Developmental Disabilities (2022) 69(6):811-24. [CrossRef]
- Buie T, Campbell DB, Fuchs GJ, Furuta GT, Levy J, VandeWater J, et al. Evaluation, Diagnosis, and Treatment of Gastrointestinal Disorders in Individuals with Asds: A Consensus Report. Pediatrics (2010) 125(Supplement_1):S1-S18. [CrossRef]
- Whitney DG, Shapiro DN. National Prevalence of Pain among Children and Adolescents with Autism Spectrum Disorders. JAMA Pediatrics (2019) 173(12). [CrossRef]
- Yu R, Hafeez R, Ibrahim M, Alonazi WB, Li B. The Complex Interplay between Autism Spectrum Disorder and Gut Microbiota in Children: A Comprehensive Review. Behavioural Brain Research (2024) 473:115177. [CrossRef]
- Lagod PP, Naser SA. The Role of Short-Chain Fatty Acids and Altered Microbiota Composition in Autism Spectrum Disorder: A Comprehensive Literature Review. Int J Mol Sci (2023) 24(24). Epub 20231213. [CrossRef]
- Lewandowska-Pietruszka Z, Figlerowicz M, Mazur-Melewska K. Microbiota in Autism Spectrum Disorder: A Systematic Review. Int J Mol Sci (2023) 24(23):16660. Epub 20231123. [CrossRef]
- Niehus R, Lord C. Early Medical History of Children with Autism Spectrum Disorders. J Dev Behav Pediatr (2006) 27(2 Suppl):S120-7. [CrossRef]
- Wang H, Liu S, Xie L, Wang J. Gut Microbiota Signature in Children with Autism Spectrum Disorder Who Suffered from Chronic Gastrointestinal Symptoms. BMC Pediatr (2023) 23(1):476. Epub 20230920. [CrossRef]
- Mhanna A, Martini N, Hmaydoosh G, Hamwi G, Jarjanazi M, Zaifah G, et al. The Correlation between Gut Microbiota and Both Neurotransmitters and Mental Disorders: A Narrative Review. Medicine (Baltimore) (2024) 103(5):e37114. [CrossRef]
Figure 1.
Main therapeutic strategies for selectivity in ASD.
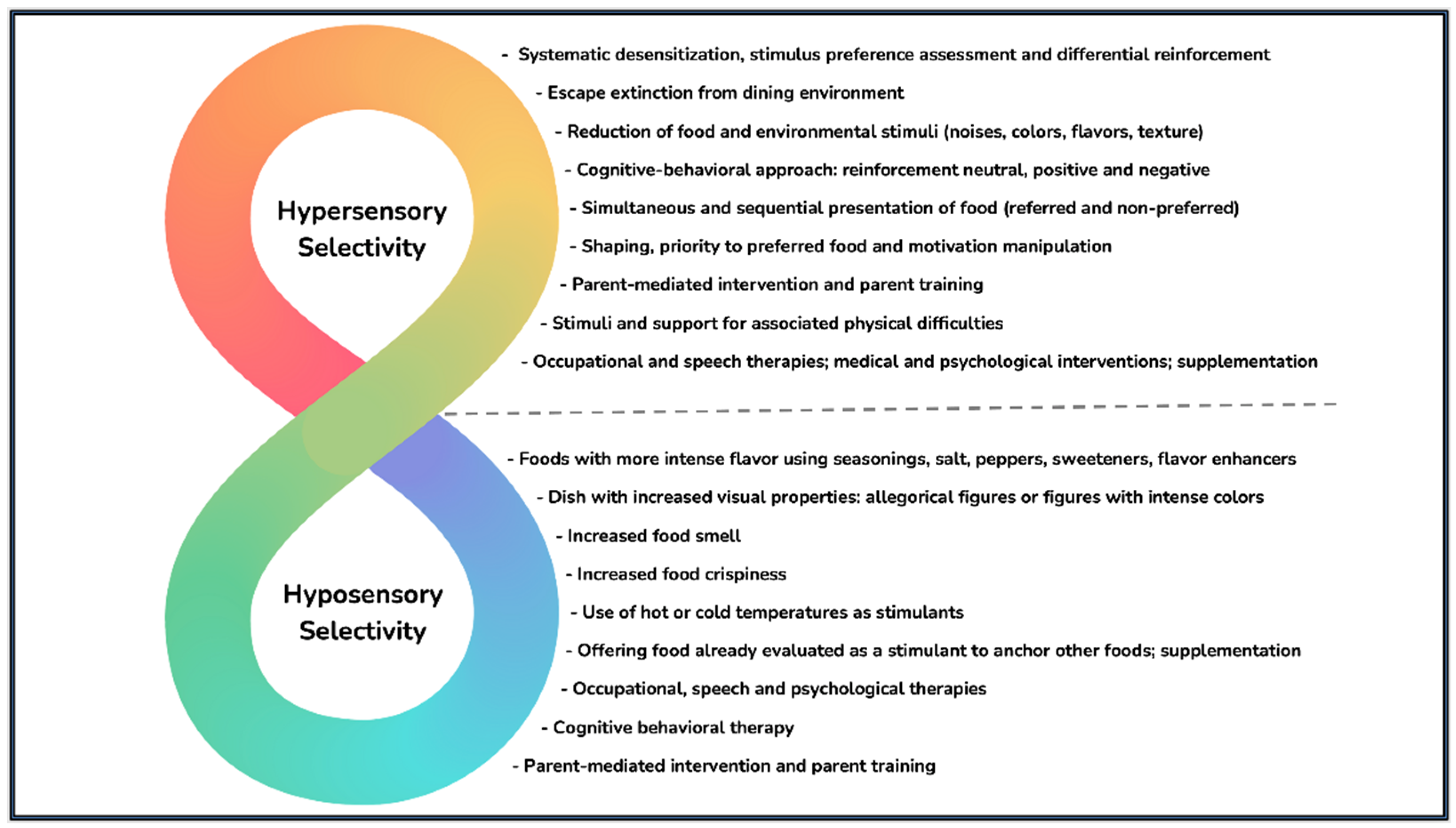
Figure 2.
Nutritional-related aspects most frequently found in children with ASD.
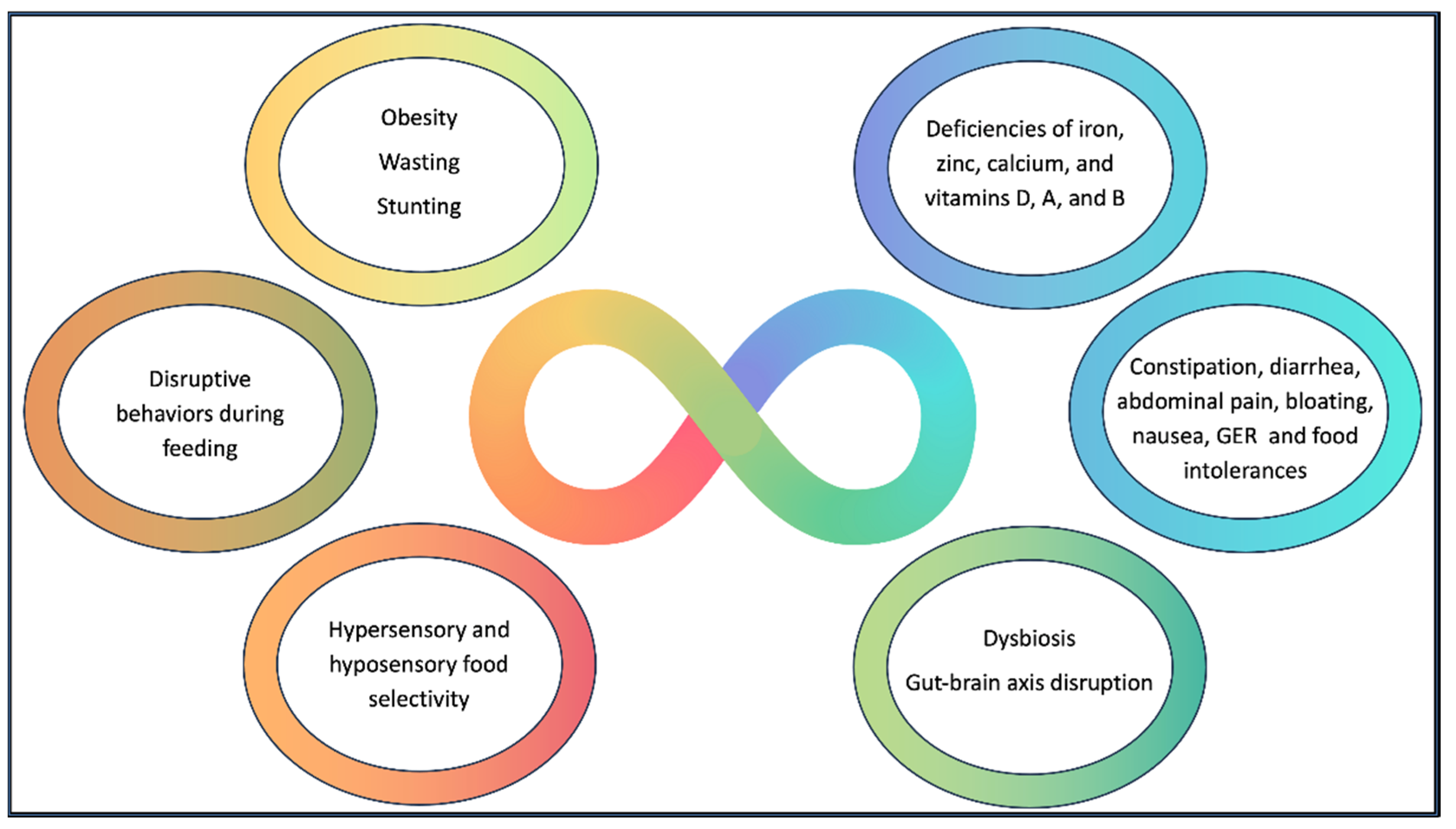

Table 1.
Treatment of vitamin and mineral deficiencies.
| Micronutrient | Therapeutic scheme |
|---|---|
| Iron | Oral dose of 2 mg/kg/day of elemental iron, for a period sufficient to recovery of ferritin and hemoglobin |
| Magnesium | Oral dose of 6 mg/kg/day when serum values are below 1.7 mg/dL or when the dietary survey shows evident deficiency in consumption |
| Zinc | Oral dose of 2 mg/kg/day of elemental zinc, respecting the maximum dose of 20 g/day, until serum zinc concentration reaches 70 mg/dL |
| Calcium | Oral dose of 100 mg per day of elemental calcium while the nutritional risk situation persists |
| Vitamin D | Oral dose for 90 days: - Under 1 year of age: 2,000 IU/day - Between 1 and 12 years of age: 3,000 and 6,000 IU/day - Over 12 years of age: 6,000 IU/day |
| Vitamin A | Oral dose of retinol palmitate: - Under 6 months of age: 50,000 IU/day - Between 6 months and 1 year: 100,000 IU/day - Over 1 year (male): 200,000 IU/day - Between 1 and 12 years (female): 200,000 IU/day - Over 12 years (female): 10,000 IU/day or 25,000 IU/week for three months in cases of night blindness and/or Bitot's spots - Note 1: Treatment should only be administered to individuals with clinical manifestations of VAD (xerophthalmia) or severe malnutrition (regardless of the presence of vitamin deficiency) - Note 2: Treatment will be in a single dose for cases of severe malnutrition and in three doses (D1, D2 and D14) in cases of xerophthalmia and/or active lesions (ulcers) in the cornea - Note 3: In cases of pregnant adolescents or those suspected of being pregnant, the initiation of treatment for active corneal lesions (considered an emergency due to the risk of vision loss within 24 to 48 hours) should be carefully weighed against the risk of maternal blindness and the potential undesirable effects of vitamin A on the fetus. Administration of vitamin A to women of childbearing age should be done with extreme caution due to the risk of teratogenicity to the fetus |
| Vitamin C | Oral dose of 100-300 mg/day of vitamin C for infants and children for one month or until full recovery occur |
| Vitamin B12 | - Initial dose: 0.2 μg/kg, subcutaneously for two days (attention to the possible hypokalemia during this phase in children with severe anemia) - After the initial dose: 1,000 μg/day, subcutaneously for 2 to 7 days; subsequently, a dose of 100 μg/week, subcutaneously, for one month |
| Folate | Oral dose of 1 to 5 mg/day of folic acid for up to four months; in infants, doses of 50 µg/day may be sufficient |
| Vitamin B6 | Except for cases of children with pyridoxine-dependent syndromes who present with seizures, the doses for vitamin B6 supplementation in the pediatric population in cases of nutritional deficiency are not well defined |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



