
Submitted:
09 January 2025
Posted:
10 January 2025
You are already at the latest version
Abstract
Background/Objectives: Urinary incontinence (UI) is a common condition in women of all ages. Type 2 diabetes (T2D) has been associated with UI, but Gestational diabetes (GD), glucose intolerance first recognized during pregnancy, has received relatively little attention as an independent risk factor for UI. We explored the roles of GD and T2D, independently and in combination, on risk of UI in the Black Women’s Health Study (BWHS) a follow-up of US Black women aged 21-69 at enrolment in 1995. Methods: We analyzed the 28,978 parous women who had information on GD, T2D, and UI in 2011. We estimated odds ratios (OR) and 95% confidence intervals (95% CI) using logistic regression with adjustment for several important variables, including age, parity, body mass index, and diuretic use. We also stratified analyses according to T2D status (T2D, no T2D). Results: The multivariable-adjusted ORs for women with a history of GD, compared to those without, was 1.18 (95% CI: 1.02, 1.37), for UI frequency of ≥1/week; the estimate among women with a history of T2D, compared to those without, was 1.15 (1.06, 1.26) for the same frequency. In stratified analyses, GD was associated with a 24% increased risk of weekly UI among women without a history T2D, while there was no association observed among those with a history of T2D. Conclusions: In the BWHS, GD was positively associated with urinary incontinence, independent of T2D status. Our results suggest that women who experience GD – even without subsequent development of T2D - might be at increased risk of UI and may benefit from early intervention.
Keywords:
Urinary incontinence
; gestational diabetes
; type 2 diabetes
; black women
; urge incontinence
; stress incontinence
1. Introduction
Urinary incontinence (UI), defined as any involuntary leakage of urine, is a common condition in women of all ages [1,2,3]. In the US, the reported prevalence of UI among US adult women is 62%, with nearly a third reporting symptoms at least monthly [4]. Global estimates range from 5% to 70%, and prevalence increases with age[3]. UI is routinely classified into three subtypes: stress (loss of urine upon exertion including coughing, lifting, or laughing), urgency (loss of urine with a strong need to urinate), and mixed (co-existing symptoms of stress and urgency), with stress UI being the most common [4,5]. UI is associated with embarrassment, decreased participation in social/physical activity [6], and disruption of daily life [7]. Direct costs for treatments, extra laundry, absorbent pads, and diapers have been estimated to exceed $12 billion/year [8], while the estimated societal costs (lost wages, quality of life) are estimated to exceed $80 billion annually[9]. Some studies have reported increased frequency of UI among Black women compared with non-Hispanic White (NHW) women and Asian women [5,10,11,12], while others report decreased UI among Black women, including severe UI (wetting of underwear) [13] compared to NHW women [14,15,16].
Type 2 diabetes (T2D) has been associated with UI [13,15,17,18,19,20,21,22], and is estimated to increase the risk of UI more than two-fold [23]. Gestational diabetes (GD) is a state of glucose intolerance first recognized during pregnancy [24,25], and accounts for over 90% of all cases of diabetes in pregnancy [26]. Glucose levels often return to pre-pregnancy levels during the postpartum period, but affected women have an increased risk of developing T2D in the future compared to non-affected women [17,18,27]. In 2019, the overall prevalence of GD in was highest for non-Hispanic Asian women (14.9%), and lowest for Black (7.0%) and White (6.5%) women, but lower than in Asian and Hispanic women [28,29]. Black women with a history of GD, however, are more likely to develop T2D than white women with a history of GD [30,31].
GD has received relatively little attention as an independent risk factor for UI. Both animal and human studies suggest that the hypoglycemic environment may impair the structure, morphology, and function of skeletal muscle tissue including the pelvic floor [32,33]. Studies in the US [34], Taiwan [35], and Brazil [36,37] have reported positive associations between GD and UI during pregnancy [34] and within two years of a term delivery [35,36,37]. Yet other studies have linked pre-diabetes, an intermediate phase of blood glucose dysregulation38, with both stress and urgency UI [13,19]. Studies of both T2D and GD, to date have included few or no Black/African American women [19,20,34,35]. We therefore sought to explore the role of GD and T2D, both independently and in combination, on risk of UI (including UI types) in a cohort of US Black women.
2. Materials and Methods
The Black Women’s Health Study (BWHS). In 1995, 64,500 Black women ages 21-69 years (median 38 years) from the continental U.S. enrolled in the BWHS by completing a 14-page health questionnaire [39,40,41]; the 59,000 women who completed the first (1997) and/or second (1999) follow-up questionnaires in addition to the baseline (1995) questionnaire, comprise the cohort that has been followed. At baseline, participants provided data on demographics, anthropometry (current weight and height, weight at age 18), medical and reproductive history, vigorous physical activity, cigarette smoking, alcohol use, and other variables. Biennial follow-up questionnaires and yearly linkage with the National Death Index provide updated information. Follow-up of the cohort has been successful for >80% of potential person-years. The Institutional Review Board of Boston University Medical Campus approved the study and participants have indicated their consent by filling out and returning study questionnaires.
Potential participants for the current analysis were the 42,803 women who completed the 2011 questionnaire, which included questions about UI. From these women, we excluded those who did not answer the UI questions (n=3,850); remained nulliparous through 2009 (n=9,489); did not complete the 1997, 1999, or 2009 questionnaires (which asked about GD) (n=57); reported prevalent diabetes at baseline in 1995 (n=326); reported incident diabetes prior to GD (n=13); whose age at GD was ≥50 years (n=2); or gave contradictory reports of GD status (n=88), leaving an analytic sample of 28,978 (Figure 1).
Gestational Diabetes (GD). The 1997, 1999, and 2009 questionnaires asked questions about the history of GD. The 1997 questionnaire asked “If a doctor has told you that you had any . . .” of a list of conditions including “diabetes during pregnancy” and whether diagnosis occurred before or after “March 1, 1995”, the start of the BWHS. The 1999 questionnaire asked whether “Between March 1997 and March 1999, you were diagnosed with diabetes during pregnancy”, with space for the participant to provide the year of diagnosis. The 2009 questionnaire asked, “Did you ever develop diabetes during a pregnancy (gestational diabetes)?” Response options included “no”, “yes (if yes, “how old were you?”)”, and “don’t know”.
We assessed the reproducibility of the GD variable in a sample of BWHS participants. During each follow-up cycle, multiple waves of questionnaires are mailed to women who have not yet responded. During the 2009 follow-up cycle, when the GD questions were most recently asked, 1,319 women returned duplicate questionnaires. There was 90% agreement between the first and duplicate questionnaire for those reporting a diagnosis of GD.
Type 2 Diabetes (T2D). The baseline and all follow-up questionnaires ask specifically about the diagnosis of T2D, as well as the date of diagnosis. We defined T2D as a report of diabetes at age 30 or older. In a BWHS validation study among 293 women who reported a diagnosis of incident T2D during follow-up and provided permission to contact their physicians. A completed physician checklist was returned for 229 participants; a diagnosis of diabetes was confirmed for 220 (96%) [42]. The estimated prevalence of undiagnosed T2D in the BWHS was 6.1% based on tests for hemoglobin A1C (HbA1C) (≥6.5%) among 10,249 participants who provided a blood sample to the BWHS, but had never previously reported T2D [43].
Urinary Incontinence (UI). Questions on UI were included for the first time on the 2011 questionnaire. Two questionnaire items asked about frequency of UI in the past year and cause (type) of leakage. The question about the frequency of UI asked, “During the past year, how often have you leaked or lost control of your urine?” Response options were never, less than once per month, once per month, 2-3 times per month, about once per week, and almost every day. The question about the type of UI asked, “When you lose urine, what is the usual cause?” Responses options were a) “coughing, sneezing, laughing or doing physical activity” (stress); b) “a sudden urgent need to go to the bathroom” (urge); “Both a) and b) equally” (mixed); and “In other circumstances” (other). Women reporting “other” were asked to specify: responses included “waiting too long to go to the bathroom”, “taking diuretics”, and “drinking too many fluids”. We assessed self-reported UI among the 1,091 women who completed a duplicate questionnaire during the 2011 follow-up cycle. Eighty-three percent of women reported a frequency of less than monthly, and 77% of women reporting at least weekly leakage answered the second questionnaire within 1 category of their original response.
Covariates. Data on potential confounders were obtained from the same (or prior) questionnaire on which gestational diabetes was reported. Otherwise, the variables were obtained from the 2011 questionnaire when data on UI was reported. These include age (years), current weight (pounds), vigorous physical activity, smoking, parity, and diuretic use. Self-reported adult height (feet and inches) was collected at baseline (1995). Completed education (≤12, 13-15, ≥16 years) was obtained in 1995 and updated in 2003. Body mass index (BMI) (not during pregnancy) is calculated for the 2011 questionnaire cycle as kg/m2. Information was also collected on dietary intake in 2001 using the short-form National Cancer Institute-Block Food Frequency Questionnaire [44]; from these data we calculated Prudent (high in fruits/vegetables) and Western (high in meat/fried foods) dietary patterns [45]. A neighborhood socioeconomic status (NSES) score was derived from socioeconomic data obtained by linking the women’s 2011 residential addresses to U.S. Census block-group data on wealth, income, and education [46,47].
Data Analysis. We estimated odds ratios (OR) and 95% confidence intervals (95%CI) for the association between GD or T2D (separately) and UI using multivariable-adjusted logistic regression models (PROC LOGISTIC, SAS version 9.4, SAS Institute, Inc., Cary, NC). The age-adjusted model included terms for age (years), while the multivariable-adjusted model included age plus BMI (<25, 25-29, 30-34, ≥35 kg/m2), parity (1, 2, ≥3), completed education (12, 13-15, ≥16 years), NSES (quintiles, 1=low, 5=high), Western dietary pattern (quintiles, 1=low, 5=high), Prudent dietary pattern (quintiles, 1=low, 5=high), vigorous physical activity (none, <5 years, ≥5 hours/week), cigarette smoking (current, past, never) and diuretic use (yes, no). We stratified analyses according to T2D status (ever, never) in order to explore the GD/UI association independent from and in combination with T2D.
3. Results
A total of 1,611 and 4,514women, respectively reported a diagnosis of GD and T2D through 2009. UI was common, with more than 50% of women reporting some frequency. Most covariates were associated with UI frequency (Table 1).
BMI, ≥ 3 births, Western diet (Q5), ever smoking, and diuretic use were positively associated with increased UI frequency, while vigorous physical activity was inversely associated. Overall, there were no clear associations between baseline characteristics and UI subtypes. Only diuretic use showed a positive association with both urge and mixed incontinence.
Table 2 provides the odds ratios for the association of GD and T2D, respectively, with UI frequency. The age- and multivariable-adjusted ORs for women with a history of GD, compared to those without, were 1.48 (95% CI: 1.25, 1.75) and 1.36 (1.15, 1.62), respectively for UI frequency of 2-3 times per month, and 1.32 (1.14, 1.52) and 1.18 (1.02, 1.37), respectively, for weekly or greater frequency of UI. For women with a history of T2D, compared to those without, the corresponding age- and multivariable-adjusted ORs for 2-3 monthly UI episodes were 1.44 (1.28, 1.61) and 1.15 (1.02, 1.30), while those for weekly or more UI frequency were 1.68 (1.54, 1.83) and 1.16 (1.06, 1.27).
We assessed the relationship of GD and T2D and UI sub-types (Table 2). For GD, there was little difference between age- and multivariable models across phenotypes. The multivariable-adjusted ORs for stress and mixed UI among women with GD compared to women without, were 1.18 (1.03, 1.36), and 1.31 (1.12, 1.54), respectively. The multivariable-adjusted ORs for the association of T2D with urge and mixed UI were 1.20 (1.10, 1.31) and 1.28 (1.16, 1.42), respectively. There was no clear association between either GD or T2D and “other” UI, although the estimate was stronger for women with GD.
Table 3 presents analyses of GD and UI frequency stratified by history of T2D (no T2D, T2D). Overall, the associations between GD and UI frequency were stronger among women without T2D (GD alone) than among those with T2D. The multivariable-adjusted OR for the GD and UI association among those without T2D reporting 2-3 times/month and weekly or more UI was 1.36 (1.09, 1.69) and 1.23 (1.01, 1.49), respectively. Among those with a history of T2D, the respective ORs were 1.32 (0.98, 1.76) and 0.95 (0.74, 1.21). We found a similar pattern for UI sub-types as stress and urge UI multivariable estimates were stronger among women without T2D. In contrast, the multivariable ORs for mixed and other UI were similar in both strata of T2D.
4. Discussion
Between 2016 and 2021, the overall percentage of GD diagnoses in the US increased from 6.0% to 8.3% in all maternal age groups [48]; previous estimates have placed the prevalence at over 9% [49]. In this study of nearly 29,000 US Black women, GD was positively associated with UI after controlling for several potential confounders. Associations with 2-3 times monthly and ≥ 1/week occurrences of UI were strongest among women free of T2D, suggesting that women who experience GD – even without subsequent development of T2D - may be at increased risk of UI. We also explored the relationship between T2D status and UI frequency and found positive, albeit weaker, associations with UI frequency 2-3 times/month and weekly or more, consistent with previously reported findings [13,15,19,20,22]. The relationships between both GD and T2D with UI subtypes were less clear. Overall, both conditions were modestly associated with increased risk of stress, urge and/or mixed UI, but these associations did not always achieve statistical significance.
T2D has been associated with an increased risk of UI [23,50]. In contrast, GD has received relatively little attention as an independent risk factor for UI. Women with a history of GD have an increased risk of subsequent development of T2D. Results from meta-analyses indicate at least a 7-fold overall risk of subsequent T2D [17,18], a risk that appears to be higher in Black women compared to White [10,20,30,31]. Nevertheless, studies of GD and UI, to date, have involved mostly White, Asian, and non-US populations [19,20,34,35]. Our findings are consistent with several analyses linking states of hyperglycemia (GDM, T2D, and IFG) to UI. For example, in a study of women with GD enrolled in a managed care plan, nearly half of the participants reported stress UI at least weekly during pregnancy and postpartum [34]. A Taiwanese study that compared GD-affected to GD-unaffected women also found an independent association between GD and any type of postpartum UI occurring within two years of a term delivery [35]. In other analyses, the association between GD and UI was observed among women undergoing cesarean births, where the presumed adverse effects of vaginal birth on the pelvic floor had been avoided [36,37]. In a perinatal study of 529 primiparous Brazilian women undergoing c-sections, those with GD diagnosed between 24 and 28 weeks had an increased incidence of UI and decreased vaginal squeeze pressure persisting for two years postpartum [36]. A more recent study involved 93 primiparous Brazilian women (aged 18-38 years) with mild GD. The women, treated only with diet and exercise, underwent cesarean births and showed an 8-fold increased risk of UI within the two-year postpartum period (P=0.034) [37].
Approximately 43 million adults are estimated to have “pre-diabetes,” or impaired fasting glucose (IFG) [51,52]. Studies have found correlations between pre-diabetes, for which GD may be a surrogate measure, and UI [13,19,34,35]. A cross-sectional analysis by Brown et al [19], estimated the prevalence of UI among 1,461 nonpregnant adult women in the 2001–2002 National Health and Nutrition Examination Survey (NHANES) to be 35.4% among those with T2D. Similarly. the prevalence among those with IFG was 33.4%. The prevalence of UI among those with normal fasting glucose levels was 16.8%, approximately half of that observed in the two hyperglycemic groups [19]. In a more recent study of over 10,000 women included in the 2007-2016 NHANES dataset, investigators found a positive association between pre-diabetic HbA1c levels and prevalence and frequency of SUI [53]. Forty percent of the study sample reported SUI (n=4,305) of which 32% had pre-diabetic HbA1c levels ranging from 5.7- 6.5, compared to 25.9% among those without SUI. Furthermore, approximately 9% of the study sample reported experiencing SUI weekly, of which 38.5% were classified as pre-diabetic [53]. These findings lend further support for the association between hyperglycemia and UI.
The exact pathophysiology linking GD with UI is not clear. Both animal and human studies suggest that the hypoglycemic environment impacts the structure and morphology of skeletal muscle tissue leading to atrophy, and impairment of muscle function [32]. It has also been suggested that such changes may similarly impair pelvic floor muscle function [33]. Hyperglycemia, however, has been associated with an increased urine volume and over-activity of bladder smooth muscle [54], both key factors in UI, urgency UI, in particular [20,55,56]. For example, hyperglycemia can cause osmotic diuresis, increasing urinary frequency and amplifying the risk of incontinence [20]. Patients with diabetes are also at increased risk of urinary tract infections, which may exacerbate existing lower urinary tract symptoms, including increased urinary frequency and incontinence [57]. Further, microvascular damage associated with hyperglycemia includes alteration of the detrusor smooth muscle and the nerves of the bladder or sphincter muscles, resulting in urethral dysfunction and involuntary bladder contractions [13,54,58]. Such changes have been observed in the bladders of diabetic rats [59,60], and support the hypothesis of diabetes-related damage to the lower urinary tract [61]. Sartorao Filho and colleagues, utilizing pelvic floor muscle electromyography to compare motor control in pregnant women, with and without GDM, identified markers of hyperglycemic myopathy in those with GDM [35]. Future applications of this technique may predict UI in late pregnancy and postpartum [62].
Hyperglycemia may also impact muscles beyond the pelvis, such as abdominal muscles, which are implicated in the function of pelvic floor muscles [63] and urethral closure [64]. Results from a study by Catinelli et al, using rat models with mild hyperglycemia during pregnancy suggests that atrophy of both the rectus abdominis and pelvic floor muscles results from a shift in maternal fiber type composition and increased collagen deposition [65]. A separate study, however, compared the impact of diabetic pregnancy on the rectus abdominis muscle and found an increase in the number of slow fibers, possibly indicating a change in the functionality of skeletal muscles exposed to excess glucose [32]. Finally, a cross-sectional study evaluating pregnant women from 28 weeks gestation found that GDM, lower levels of pelvic floor muscle strength, and UI, were associated with significantly lower levels of relaxin, a reproductive hormone thought to play a role in maintaining urinary continence by degrading collagen in pelvic floor connective tissue, loosening the muscle to facilitate delivery [33]. Thus, lower levels of relaxin may be associated with higher levels of fibrosis and subsequent urinary tract dysfunction [33]. Previous studies also show that diabetes is characterized by an increase in muscle collagen [66,67]. Despite these observations, the link, if any between GDM and myopathy remains largely unexplored and without an effective treatment [65].
Overall, we found associations between both T2D and GD, and all UI subtypes, although we did not observe significant difference across phenotypes. We found increased associations between T2D and both urge and mixed UI. In a study of the predominantly white Nurses’ Health Study I and II cohorts, Danforth and colleagues found that T2D was associated with an increased odds of at least weekly episodes of urge incontinence: 1.4 (1.0,1.9) [20]. A study of Turkish women (aged 20-87 years) by Izci and colleagues, found a 2.5-fold higher risk of UI among (type 2) diabetic women compared to nondiabetic women. They also observed the highest prevalence of both stress and mixed incontinence among diabetic women [23]. Studies have also reported UI phenotypes according to race. Data from the Study of Women’s Health Across the Nation (SWAN) showed an increased prevalence of urgency UI in Black women (n=719; 85 cases) compared to other racial groups [12]. Similar results were reported by Townsend et al, where urgency incontinence was the most common subtype reported among Black women in the Nurses’ Health Study cohorts (n=1,138; 19 cases) [11]. We found a statistically significant association between T2D and urge UI: 1.16 (1.06, 1.28) (n=916 cases). In contrast, our stratified analyses involving over 22,000 Black women showed a statistically significant 23% increased odds of stress UI (n=194 cases), and a borderline significant 23% increased odds of mixed UI (n=109 cases), among those with GD alone (no subsequent development of T2D) compared to those without GD.
Our analysis also has several limitations. Because we asked about any history of UI in 2011, after we collected data on GD, we were unable to establish the temporal sequence between GD and UI. We relied on self-reported GD without medical record confirmation; but found high agreement in duplicate questionnaires. Because GD is diagnosed by the end of the second trimester and intensively managed during the remainder of pregnancy, affected women are likely to remember having been diagnosed [68]. Validation of maternal self-report of GD against perinatal records in the CHARGE (CHildhood Autism Risks from Genetics and the Environment) study reported 70% to 85% for sensitivity and ≥98% for specificity [68]. The New York State Pregnancy Risk Assessment Monitoring System (PRAMS) survey, estimated a prevalence- and bias-adjusted kappa of 0.88 for 258 births, indicating very good agreement between self-report and birth records for GD [69]. Our data suggested acceptable reliability of self-reported UI. Several studies have evaluated self-reported UI versus a detailed physical exam and found high validity of the self-report. Diokno et al [70], reported 86.5% agreement between self-reported and clinically diagnosed UI among 169 women aged 60 and older. In a larger group of 456 women from the MESA study, Herzog and Fultz [71], collected UI information both through a self-reported questionnaire and a clinical exam finding 83% agreement between the two methods. The results of our validation are consistent with these findings. Furthermore, we used instruments applied to other studies. Finally, the BWHS is not a probability sample of U.S. black women. Participants have higher educational status, underrepresenting the 15% of US black women nationally who have not completed high school [72]. Conversely, participants reside in all regions of the United States. Thus, the present results might apply to a large population of U.S. Black women. The current study also has several strengths including the large sample size and the successful follow-up of the cohort. To our knowledge, this is the largest study to date to explore the role of GD in relation to UI risk in US Black women. We controlled for many factors of relevance to UI occurrence in multivariable analyses, including parity and BMI which are established risk factors for UI and are also associated with GD. In addition, our validation of T2D showed high accuracy of self-report. Thus, the estimated prevalence of undiagnosed T2D in the cohort would likely have had a small effect on the risk estimation [73].
5. Conclusions
Urinary incontinence is a condition that can greatly impact the quality of life and finances of those affected. Our findings suggest that gestational diabetes may be an independent risk factor for UI in US Black women, challenging the narrative that the effects of GDM resolve soon after delivery. Our study is an important first step and will contribute to the identification of younger, high-risk women who may benefit from earlier intervention, management, treatment of UI.
Author Contributions
Conceptualization, Y.C.C., B.L.H, P.K.; methodology, Y.C.C., N.C.W., K.A.B., P.K, S.S., and L.R.; validation, Y.C.C. and L.R..; formal analysis, Y.C.C. and N.C.W.; data curation, Y.C.C., N.C.W., and L.R.; writing—original draft preparation, Y.C.C., N.C.W., K.A.B., M.N, T.C, B.L.H., and P.K..; writing—review and editing, Y.C.C., N.C.W., K.A.B., N.M., P.K., B.L.H., T.C., S.S., and L.R.; supervision, Y.C.C.; project administration, Y.C.C.; funding acquisition, Y.C.C. and L.R. All authors have read and agreed to the published version of the manuscript.
Funding
This work was supported by the National Institute of Cancer (Grant No. U01CA164974) and the National Institute of Diabetes and Digestive and Kidney Diseases (Grant No. U01DK106786).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and the study protocol was approved by the Institutional Review Board {IRB) of The Boston University Medical Center (IRB protocol number: H-36793, date of approval: 01/26/2018).
Informed Consent Statement
BWHS participants indicate consent by completing and returning questionnaires. All participants entered the BWHS voluntarily. They fill out follow-up and supplemental questionnaires voluntarily and may chose not to do so or to withdraw from the study. The reason for collecting questionnaire information, and the use to which the information will be put, are described in explanatory letters that accompany each questionnaire. Requests for biological samples or access to medical records involve written informed consent forms. All procedures and consent forms have been approved by the Boston University Medical Center IRB.
Data Availability Statement
Data underlying the study cannot be made publicly available due to ethical concerns about patient confidentiality. Data will be made available to qualified researchers on request to BWHS@bu.edu.
Acknowledgments
We thank the staff and participants of the BWHS.
Conflicts of Interest
The authors have no conflicts to declare. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results”.
Abbreviations
The following abbreviations are used in this manuscript:
| BMI | Body Mass Index |
| BWHS | Black Women’s Health Study |
| GD | Gestational diabetes |
| HbA1c | Hemoglobin A1c |
| IFG | Impaired fasting glucose |
| NHW | Non-Hispanic White |
| NSES | Neighborhood socioeconomic status |
| SUI | Stress urinary incontinence |
| T2D | Type 2 diabetes |
| UI | Urinary incontinence |
| US | United States |
References
- Grodstein, F.; Fretts, R.; Lifford, K.; Resnick, N.; Curhan, G. Association of age, race, and obstetric history with urinary symptoms among women in the Nurses' Health Study. Am. J. Obstet. Gynecol. 2003, 189, 428–434. [CrossRef]
- Minassian VA, Stewart WF, Wood GC. Urinary incontinence in women: variation in prevalence estimates and risk factors. Obstet Gynecol 2008;111:324-31.
- Milsom, I.; Gyhagen, M. Breaking news in the prediction of pelvic floor disorders. Best Pr. Res. Clin. Obstet. Gynaecol. 2019, 54, 41–48. [CrossRef]
- Patel, U.J.; Godecker, A.L.; Giles, D.L.M.; Brown, H.W.M. Updated Prevalence of Urinary Incontinence in Women: 2015–2018 National Population-Based Survey Data. Urogynecology 2022, 28, 181–187. [CrossRef]
- Abufaraj, M.; Xu, T.; Cao, C.; Siyam, A.; Isleem, U.; Massad, A.; Soria, F.; Shariat, S.F.; Sutcliffe, S.; Yang, L. Prevalence and trends in urinary incontinence among women in the United States, 2005–2018. 2021, 225, 166.e1–166.e12. [CrossRef]
- Landefeld, C.S.; Bowers, B.J.; Feld, A.D.; Hartmann, K.E.; Hoffman, E.; Ingber, M.J.; King, J.T.; McDougal, W.S.; Nelson, H.; Orav, E.J.; et al. National Institutes of Health State-of-the-Science Conference Statement: Prevention of Fecal and Urinary Incontinence in Adults. Ann. Intern. Med. 2008, 148, 449–458. [CrossRef]
- Bani-Issa, W.; Almomani, F.; Eldeirawi, K. Urinary incontinence among adult women with diabetes in Jordan: epidemiology, correlates and perceived impact on emotional and social well-being. J. Clin. Nurs. 2013, 23, 2451–2460. [CrossRef]
- Chong, E.C.; Khan, A.A.; Anger, J.T. The Financial Burden of Stress Urinary Incontinence Among Women in the United States. Curr. Urol. Rep. 2011, 12, 358–362. [CrossRef]
- Coyne, K.S.; Wein, A.; Nicholson, S.; Kvasz, M.; Chen, C.-I.; Milsom, I. Economic Burden of Urgency Urinary Incontinence in the United States: A Systematic Review. J. Manag. Care Pharm. 2014, 20, 130–140. [CrossRef]
- Coyne, K.S.; Sexton, C.C.; Clemens, J.; Thompson, C.L.; Chen, C.-I.; Bavendam, T.; Dmochowski, R. The Impact of OAB on Physical Activity in the United States: Results from OAB-POLL. Urology 2013, 82, 799–806. [CrossRef]
- Townsend, M.K.; Curhan, G.C.; Resnick, N.M.; Grodstein, F. The incidence of urinary incontinence across Asian, black, and white women in the United States. Am. J. Obstet. Gynecol. 2010, 202, 378.e1–378.e7. [CrossRef]
- Waetjen LE, Liao S, Johnson WO, et al. Factors associated with prevalent and incident urinary incontinence in a cohort of midlife women: a longitudinal analysis of data: study of women's health across the nation. Am J Epidemiol 2007;165:309-18.
- Danforth, K.N.; Townsend, M.K.; Lifford, K.; Curhan, G.C.; Resnick, N.M.; Grodstein, F. Risk factors for urinary incontinence among middle-aged women. Am. J. Obstet. Gynecol. 2006, 194, 339–345. [CrossRef]
- Phelan S, Kanaya AM, Subak LL, et al. Prevalence and risk factors for urinary incontinence in overweight and obese diabetic women: action for health in diabetes (look ahead) study. Diabetes Care 2009;32:1391-7.
- Matthews CA, Whitehead WE, Townsend MK, Grodstein F. Risk factors for urinary, fecal, or dual incontinence in the Nurses' Health Study. Obstet Gynecol 2013;122:539-45.
- Komesu, Y.M.; Schrader, R.M.; Ketai, L.H.; Rogers, R.G.; Dunivan, G.C. Epidemiology of mixed, stress, and urgency urinary incontinence in middle-aged/older women: the importance of incontinence history. Int. Urogynecology J. 2015, 27, 763–772. [CrossRef]
- Kim C, Newton KM, Knopp RH. Gestational diabetes and the incidence of type 2 diabetes: a systematic review. Diabetes Care 2002;25:1862-8.
- Bellamy, L.; Casas, J.-P.; Hingorani, A.D.; Williams, D. Type 2 diabetes mellitus after gestational diabetes: A systematic review and meta-analysis. Lancet 2009, 373, 1773–1779. [CrossRef]
- Brown JS, Vittinghoff E, Lin F, Nyberg LM, Kusek JW, Kanaya AM. Prevalence and risk factors for urinary incontinence in women with type 2 diabetes and impaired fasting glucose: findings from the National Health and Nutrition Examination Survey (NHANES) 2001-2002. Diabetes Care 2006;29:1307-12.
- Danforth KN, Townsend MK, Curhan GC, Resnick NM, Grodstein F. Type 2 diabetes mellitus and risk of stress, urge and mixed urinary incontinence. J Urol 2009;181:193-7.
- Devore, E.E.; Minassian, V.A.; Grodstein, F. Factors associated with persistent urinary incontinence. Am. J. Obstet. Gynecol. 2013, 209, 145.e1–145.e6. [CrossRef]
- Bani-Issa, W.A.; Halabi, J.O.; Abdullah, A.R.; Hasan, H.A.; Raigangar, V.L. Prevalence and Risk Factors for Incontinence Among Emirati Women With Diabetes. J. Transcult. Nurs. 2013, 25, 42–50. [CrossRef]
- Izci, Y.; Topsever, P.; Filiz, T.M.; Çınar, N.D.; Uludağ, C.; Lagro-Janssen, T. The association between diabetes mellitus and urinary incontinence in adult women. Int. Urogynecology J. 2009, 20, 947–952. [CrossRef]
- Metzger, B.E.; Buchanan, T.A.; Coustan, D.R.; de Leiva, A.; Dunger, D.B.; Hadden, D.R.; Hod, M.; Kitzmiller, J.L.; Kjos, S.L.; Oats, J.N.; et al. Summary and Recommendations of the Fifth International Workshop-Conference on Gestational Diabetes Mellitus. Diabetes Care 2007, 30, S251–S260. [CrossRef]
- Ashwal E, Hod M. Gestational diabetes mellitus: Where are we now? Clin Chim Acta 2015;451:14-20.
- American College of Obstetrics and Gynecologists. Practice Bulletin No. 137: Gestational diabetes mellitus. Obstet Gynecol 2013;122:406-16.
- Varner, M.W.; Rice, M.M.; Landon, M.B.; Casey, B.M.; Reddy, U.M.; Wapner, R.J.; Rouse, D.J.; Tita, A.T.N.; Thorp, J.M.; Chien, E.K.M.; et al. Pregnancies After the Diagnosis of Mild Gestational Diabetes Mellitus and Risk of Cardiometabolic Disorders. Obstet. Gynecol. 2017, 129, 273–280. [CrossRef]
- Shah, N.S.; Wang, M.C.; Freaney, P.M.; Perak, A.M.; Carnethon, M.R.; Kandula, N.R.; Gunderson, E.P.; Bullard, K.M.; Grobman, W.A.; O’brien, M.J.; et al. Trends in Gestational Diabetes at First Live Birth by Race and Ethnicity in the US, 2011-2019. JAMA 2021, 326, 660–669. [CrossRef]
- Gregory, E.C.; Ely, D.M. Trends and Characteristics in Gestational Diabetes: United States, 2016-2020.. 2022, 71, 1–15.
- Wang, Y.; Chen, L.; Horswell, R.; Xiao, K.; Besse, J.; Johnson, J.; Ryan, D.H.; Hu, G. Racial Differences in the Association Between Gestational Diabetes Mellitus and Risk of Type 2 Diabetes. J. Women's Heal. 2012, 21, 628–633. [CrossRef]
- Xiang, A.H.; Li, B.H.; Black, M.H.; Sacks, D.A.; Buchanan, T.A.; Jacobsen, S.J.; Lawrence, J.M. Racial and ethnic disparities in diabetes risk after gestational diabetes mellitus. Diabetologia 2011, 54, 3016–3021. [CrossRef]
- Vesentini, G.; Barbosa, A.M.P.; Damasceno, D.C.; Marini, G.; Piculo, F.; Matheus, S.M.M.; Hallur, R.L.S.; Nunes, S.K.; Catinelli, B.B.; Magalhães, C.G.; et al. Alterations in the structural characteristics of rectus abdominis muscles caused by diabetes and pregnancy: A comparative study of the rat model and women. PLOS ONE 2020, 15, e0231096. [CrossRef]
- Prudencio, C.B.; Nunes, S.K.; Pinheiro, F.A.; Filho, C.I.S.; Antônio, F.I.; Nava, G.T.d.A.; Rudge, M.V.C.; Barbosa, A.M.P.; Calderon, I.M.P.; Souza, F.P.; et al. Relaxin-2 during pregnancy according to glycemia, continence status, and pelvic floor muscle function. Int. Urogynecology J. 2022, 33, 3203–3211. [CrossRef]
- Kim, C.; McEwen, L.N.; Sarma, A.V.; Piette, J.D.; Herman, W.H. Stress Urinary Incontinence in Women with a History of Gestational Diabetes Mellitus. J. Women's Heal. 2008, 17, 783–792. [CrossRef]
- Chuang, C.; Lin, I.; Horng, H.; Hsiao, Y.; Shyu, I.; Chou, P. The impact of gestational diabetes mellitus on postpartum urinary incontinence: a longitudinal cohort study on singleton pregnancies. BJOG: Int. J. Obstet. Gynaecol. 2012, 119, 1334–1343. [CrossRef]
- Barbosa, A.M.P.; Dias, A.; Marini, G.; Calderon, I.M.P.; Witkin, S.; Rudge, M.V.C. Urinary incontinence and vaginal squeeze pressure two years post-cesarean delivery in primiparous women with previous gestational diabetes mellitus. 2011, 66, 1341–1345. [CrossRef]
- Sartorao Filho CI, Nunes SK, Magyori ABM, Calderon IMP, Barbosa AMP, Rudge MVC. The role of Gestational Diabetes Mellitus and pelvic floor 3D-ultrasound assessment during pregnancy predicting urinary incontinence: a prospective cohort study. BMC Pregnancy Childbirth 2023;23:637.
- American Diabetes A. 2. Classification and Diagnosis of Diabetes: Standards of Medical Care in Diabetes-2020. Diabetes Care 2020;43:S14-S31.
- Rosenberg L, Adams-Campbell L, Palmer JR. The Black Women's Health Study: a follow-up study for causes and preventions of illness. J Am Med Womens Assoc (1972) 1995;50:56-8.
- Russell C, Palmer JR, Adams-Campbell LL, Rosenberg L. Follow-up of a large cohort of Black women. Am J Epidemiol 2001;154:845-53.
- Russell CW, Boggs DA, Palmer JR, Rosenberg L. Use of a web-based questionnaire in the Black Women's Health Study. Am J Epidemiol 2010;172:1286-91.
- Wise, L.A.; Rosenberg, L.; Radin, R.G.; Mattox, C.; Yang, E.B.; Palmer, J.R.; Seddon, J.M. A Prospective Study of Diabetes, Lifestyle Factors, and Glaucoma Among African-American Women. Ann. Epidemiology 2011, 21, 430–439. [CrossRef]
- Palmer JR, Castro-Webb N, Bertrand K, Bethea TN, Denis GV. Type II Diabetes and Incidence of Estrogen Receptor Negative Breast Cancer in African American Women. Cancer Res 2017;77:6462-9.
- Block, G.; Hartman, A.M.; Naughton, D. A Reduced Dietary Questionnaire: Development and Validation. Epidemiology 1990, 1, 58–64. [CrossRef]
- Boggs DA, Palmer JR, Spiegelman D, Stampfer MJ, Adams-Campbell LL, Rosenberg L. Dietary patterns and 14-y weight gain in African American women. Am J Clin Nutr 2011;94:86-94.
- Coogan PF, Cozier YC, Krishnan S, et al. Neighborhood socioeconomic status in relation to 10-year weight gain in the Black Women's Health Study. Obesity (Silver Spring) 2010;18:2064-5.
- US Census Bureau. Census 2000 basics. Washington, DC: US Government Printing Office; 2002.
- Villarroel, M.A.; Lucas, J.W. QuickStats: Percentage of Mothers with Gestational Diabetes,* by Maternal Age — National Vital Statistics System, United States, 2016 and 2021. Mmwr-Morbidity Mortal. Wkly. Rep. 2023, 72, 16–132. [CrossRef]
- Bloomgarden, Z.T. Gestational Diabetes Mellitus and Obesity. Diabetes Care 2010, 33, e60–e65. [CrossRef]
- Alvaro, R.; Araco, F.; Gravante, G.; Sorge, R.; Overton, J.; Vellone, E.; Venturini, G.; Piccione, E. Epidemiological aspects of urinary incontinence in a female population of an Italian region. Int. Urogynecology J. 2010, 21, 873–883. [CrossRef]
- Davidson, M.B.; Landsman, P.B.; Alexander, C.M. Lowering the Criterion for Impaired Fasting Glucose Will Not Provide Clinical Benefit. Diabetes Care 2003, 26, 3329–3330. [CrossRef]
- Benjamin SM, Valdez R, Geiss LS, Rolka DB, Narayan KM. Estimated number of adults with prediabetes in the US in 2000: opportunities for prevention. Diabetes Care 2003;26:645-9.
- Ying, Y.; Xu, L.; Huang, R.; Chen, T.; Wang, X.; Li, K.; Tang, L. Relationship Between Blood Glucose Level and Prevalence and Frequency of Stress Urinary Incontinence in Women. Urogynecology 2021, 28, 304–310. [CrossRef]
- Brown, J.S.; Nyberg, L.M.; Kusek, J.W.; Burgio, K.L.; Diokno, A.C.; Foldspang, A.; Fultz, N.H.; Herzog, A.; Hunskaar, S.; Milsom, I.; et al. Proceedings of the national institute of diabetes and digestive and kidney diseases international symposium on epidemiologic issues in urinary incontinence in women. Am. J. Obstet. Gynecol. 2003, 188, S77–S88. [CrossRef]
- Brown, J.S. Urinary Incontinence: An Important and Underrecognized Complication of Type 2 Diabetes Mellitus. J. Am. Geriatr. Soc. 2005, 53, 2028–2029. [CrossRef]
- Brown JS, Luft J. Women & diabetes. Urinary incontinence. Diabetes Self Manag 2005;22:48-50.
- Smith DB. Urinary incontinence and diabetes: a review. J Wound Ostomy Continence Nurs 2006;33:619-23.
- Brown, J.S.; Wessells, H.; Chancellor, M.B.; Howards, S.S.; Stamm, W.E.; Stapleton, A.E.; Steers, W.D.; Eeden, S.K.V.D.; McVary, K.T. Urologic Complications of Diabetes. Diabetes Care 2005, 28, 177–185. [CrossRef]
- Rizk, D.E.E.; Padmanabhan, R.K.; Tariq, S.; Shafiullah, M.; Ahmed, I. Ultra-structural morphological abnormalities of the urinary bladder in streptozotocin-induced diabetic female rats. Int. Urogynecology J. 2005, 17, 143–154. [CrossRef]
- Stevens LA, Sellers DJ, McKay NG, Chapple CR, Chess-Williams R. Muscarinic receptor function, density and G-protein coupling in the overactive diabetic rat bladder. Auton Autacoid Pharmacol 2006;26:303-9.
- Marini, G.; Piculo, F.; Vesentini, G.; Damasceno, D.C.; Delella, F.K.; Calderon, I.M.; Daneshgari, F.; Felisbino, S.L.; Barbosa, A.M.; Rudge, M.V. The influence of hyperglycemia on the remodeling of urethral connective tissue in pregnant rats. Eur. J. Obstet. Gynecol. Reprod. Biol. 2018, 221, 81–88. [CrossRef]
- Rudge, M.V.C.; The Diamater Study Group; Souza, F.P.; Abbade, J.F.; Hallur, R.L.S.; Marcondes, J.P.C.; Piculo, F.; Marini, G.; Vesentini, G.; Thabane, L.; et al. Study protocol to investigate biomolecular muscle profile as predictors of long-term urinary incontinence in women with gestational diabetes mellitus. BMC Pregnancy Childbirth 2020, 20, 1–14. [CrossRef]
- Vesentini, G.; El Dib, R.; Righesso, L.A.R.; Piculo, F.; Marini, G.; Ferraz, G.A.R.; Calderon, I.d.M.P.; Barbosa, A.M.P.; Rudge, M.V.C. Pelvic floor and abdominal muscle cocontraction in women with and without pelvic floor dysfunction: a systematic review and meta-analysis. Clinics 2019, 74, e1319. [CrossRef]
- Sapsford, R.R.; Hodges, P.W. Contraction of the pelvic floor muscles during abdominal maneuvers. Arch. Phys. Med. Rehabilitation 2001, 82, 1081–1088. [CrossRef]
- Catinelli, B.B.; Rossignoli, P.S.; Floriano, J.F.; Carr, A.M.; de Oliveira, R.G.; dos Santos, N.J.; Úbeda, L.C.C.; Spadella, M.A.; Hallur, R.L.S.; Sobrevia, L.; et al. Reversal of diabetic-induced myopathy by swimming exercise in pregnant rats: a translational intervention study. Sci. Rep. 2022, 12, 1–12. [CrossRef]
- Richardson, D.K.; Kashyap, S.; Bajaj, M.; Cusi, K.; Mandarino, S.J.; Finlayson, J.; DeFronzo, R.A.; Jenkinson, C.P.; Mandarino, L.J. Lipid Infusion Decreases the Expression of Nuclear Encoded Mitochondrial Genes and Increases the Expression of Extracellular Matrix Genes in Human Skeletal Muscle. J. Biol. Chem. 2005, 280, 10290–10297. [CrossRef]
- Berria, R.; Wang, L.; Richardson, D.K.; Finlayson, J.; Belfort, R.; Pratipanawatr, T.; De Filippis, E.A.; Kashyap, S.; Mandarino, L.J. Increased collagen content in insulin-resistant skeletal muscle. Am. J. Physiol. Metab. 2006, 290, E560–E565. [CrossRef]
- Krakowiak, P.; Walker, C.K.; Tancredi, D.J.; Hertz-Picciotto, I. Maternal Recall Versus Medical Records of Metabolic Conditions from the Prenatal Period: A Validation Study. Matern. Child Heal. J. 2015, 19, 1925–1935. [CrossRef]
- Hosler, A.S.; Nayak, S.G.; Radigan, A.M. Agreement Between Self-Report and Birth Certificate for Gestational Diabetes Mellitus: New York State PRAMS. Matern. Child Heal. J. 2009, 14, 786–789. [CrossRef]
- Diokno AC, Normolle DP, Brown MB, Herzog AR. Urodynamic tests for female geriatric urinary incontinence. Urology 1990;36:431-9.
- Herzog, A.R.; Fultz, N.H. Prevalence and Incidence of Urinary Incontinence in Community-Dwelling Populations. J. Am. Geriatr. Soc. 1990, 38, 273–281. [CrossRef]
- Newburger EC, Curry A. Educational Attainment in the United States, March 1999. Current Population Reports: Washington, DC: U.S. Department of Commerce; 2000.
- Vimalananda VG, Palmer JR, Gerlovin H, et al. Night-shift work and incident diabetes among African-American women. Diabetologia 2015;58:699-706.
Figure 1.
BWHS Flow Chart of Gestational Diabetes (GD) and Urinary Incontinence (UI), 2011.
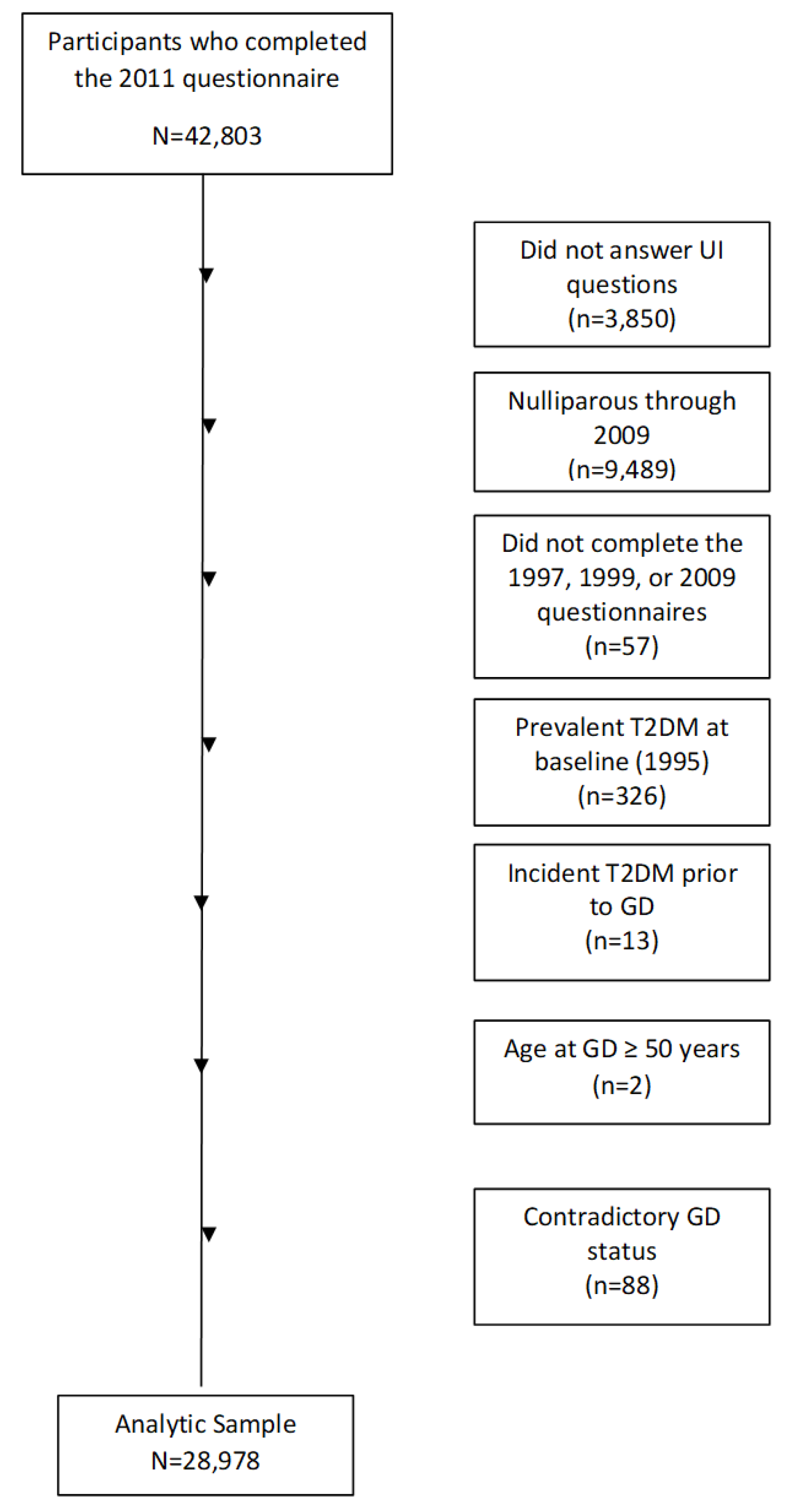

Table 1.
Age-Standardized Characteristics by Urinary Incontinence frequency and type among parous women, BWHS (N=28,978).
Table 1.
Age-Standardized Characteristics by Urinary Incontinence frequency and type among parous women, BWHS (N=28,978).
| Frequency of Urinary Incontinence | Type of Urinary Incontinence (any frequency)a | ||||||||
| Never (n=14045) | ≤ 1/month (n=8087) | 2-3 month (n=2523) | ≥ 1 week (n=4323) | Stress (n=4946) | Urgency (n=4886) | Mixed (n=3123) | Other (n=1680) | ||
| Age, years, mean (SD) | 24.2 (6.2) | 24.1 (6.2) | 23.8 (6.2) | 23.2 (6.0) | 24.3 (6.2) | 24.4 (6.3) | 23.8 (6.1) | 23.0 (6.0) | |
| Body Mass Index, kg/m2, mean (SD) | 27.3 (5.9) | 28.1 (6.2) | 29.2 (6.8) | 30.2 (7.0) | 27.3 (5.9) | 28.1 (6.0) | 29.0 (6.7) | 30.0 (7.0) | |
| Parity (%) | |||||||||
| 1 birth | 47 | 44 | 43 | 40 | 44 | 41 | 42 | 43 | |
| 2 birth | 30 | 32 | 32 | 31 | 33 | 32 | 31 | 29 | |
| 3+ birth | 23 | 24 | 25 | 29 | 23 | 27 | 27 | 27 | |
| Years of education (%) | |||||||||
| ≤12 | 19 | 17 | 19 | 20 | 17 | 18 | 20 | 16 | |
| 13-15 | 36 | 36 | 37 | 36 | 37 | 35 | 37 | 37 | |
| ≥16 | 44 | 47 | 44 | 44 | 46 | 47 | 43 | 47 | |
| Neighborhood Socioeconomic Status, quintiles (%) | |||||||||
| Q1 (low) | 18 | 18 | 19 | 18 | 17 | 18 | 20 | 19 | |
| Q5 (high) | 19 | 19 | 18 | 18 | 20 | 19 | 16 | 18 | |
| Western Diet, quintiles (%) | |||||||||
| Q1 (low) | 20 | 19 | 17 | 17 | 17 | 18 | 16 | 21 | |
| Q5 (high) | 17 | 19 | 18 | 21 | 19 | 20 | 21 | 17 | |
| Prudent diet, quintiles (%) | |||||||||
| Q1 (low) | 19 | 18 | 19 | 18 | 19 | 17 | 19 | 18 | |
| Q5 (high) | 19 | 18 | 18 | 18 | 17 | 20 | 16 | 19 | |
| Vigorous activity, hours/week (%) | |||||||||
| None | 35 | 34 | 36 | 42 | 34 | 38 | 38 | 35 | |
| < 5 | 49 | 52 | 49 | 45 | 52 | 48 | 47 | 51 | |
| ≥ 5 | 11 | 10 | 10 | 9 | 10 | 9 | 10 | 10 | |
| Cigarette smoking status, (%) | |||||||||
| Current | 13 | 13 | 15 | 17 | 13 | 15 | 16 | 13 | |
| past | 21 | 22 | 23 | 25 | 21 | 23 | 24 | 25 | |
| never | 66 | 65 | 62 | 58 | 65 | 62 | 60 | 62 | |
| Recent diuretic use (2011), (%) | |||||||||
| Yes | 10 | 11 | 13 | 15 | 9 | 14 | 14 | 12 | |
a A total of 298 women who reported a frequency of urinary incontinence did not report a type of urinary incontinence. Values are means (SD) or percentages and are standardized to the age distribution of the study population.Unless otherwise indicated, variables were obtained from the same (or prior) questionnaire on which gestational diabetes was reported. Otherwise, the variables were obtained from the 2011 questionnaire when data on UI was reported. Some frequencies may not sum to 100% due to missing values.
Table 2.
Odds Ratios (ORs) of Gestational Diabetes (GD), Type 2 Diabetes (T2D) and Urinary Incontinence Frequency and Type in parous women, BWHS (N=28,978).
Table 2.
Odds Ratios (ORs) of Gestational Diabetes (GD), Type 2 Diabetes (T2D) and Urinary Incontinence Frequency and Type in parous women, BWHS (N=28,978).
| Urinary Incontinence Frequency | Urinary Incontinence Type | |||||||||
| OR 95% CIa | OR (95% CI) a | |||||||||
| Ever Gestational Diabetesb,c | Never | ≤ 1/month | 2-3/ month | ≥ 1 week | Stress | Urge | Mixed | Otherd | ||
| n | Yes | 707 | 457 | 179 | 268 | 304 | 262 | 212 | 103 | |
| Total | 14,045 | 8,087 | 2,523 | 4,323 | 4,946 | 4,886 | 3,123 | 1,680 | ||
| Age-Adjusted | REF | 1.14 (1.01, 1.29) |
1.48 (1.25, 1.75) |
1.32 (1.14, 1.52) |
1.24 (1.08, 1.43) |
1.10 (0.95, 1.27) |
1.48 (1.25, 1.72) |
1.24 (1.00, 1.54) |
||
| Multivariable- Adjustede |
REF | 1.09 (0.97, 1.23) |
1.36 (1.15, 1.62) |
1.18 (1.02, 1.37) |
1.18 (1.03, 1.36) |
1.03 (0.88, 1.19) |
1.31 (1.12, 1.54) |
1.16 (0.94, 1.44) |
||
| Ever Type 2 Diabetesb,f | ||||||||||
| n | Yes | 1,883 | 1,244 | 466 | 921 | 717 | 916 | 669 | 265 | |
| Total | 14,045 | 8,087 | 2,523 | 4,323 | 4,946 | 4,886 | 3,123 | 1,680 | ||
| Age-Adjusted | REF | 1.17 (1.08, 1.26) |
1.44 (1.28, 1.61) |
1.68 (1.54, 1.83) |
1.09 (1.00, 1.20) |
1.46 (1.34, 1.60) |
1.68 (1.52, 1.85) |
1.20 (1.05, 1.38) |
||
| Multivariable- Adjustede |
REF | 1.07 (0.99, 1.16) |
1.15 (1.02, 1.30) |
1.16 (1.06, 1.27) |
1.02 (0.92, 1.12) |
1.16 (1.06, 1.28) |
1.23 (1.11, 1.36) |
0.99 (0.85, 1.14) |
||
a REF=Reference = Never Urinary Incontinence, b Parous women, c Reference = Never Gestational Diabetes, d Includes situations such as “waiting too long to go to the bathroom”, “taking diuretics”, and “drinking too many fluids”. e Adjusted for age, BMI, parity, education, NSES, prudent and western diet, use of diuretics, vigorous physical activity, and smoking status. f Reference = Never TD2
Table 3.
Odds Ratios (ORs) of Gestational Diabetes (GD) and Urinary Incontinence Frequency and Type stratified by Type 2 Diabetes (T2D) status in parous women with and without GD.
Table 3.
Odds Ratios (ORs) of Gestational Diabetes (GD) and Urinary Incontinence Frequency and Type stratified by Type 2 Diabetes (T2D) status in parous women with and without GD.
| Urinary Incontinence Frequencya | Urinary Incontinence Typea | |||||||||
| OR 95% CI | OR (95% CI) | |||||||||
| No T2Db | Never | ≤ 1/month | 2-3 month | ≥ 1 week | Stress | Urge | Mixed | Otherc | ||
| Ever GDd | Yes | 447 | 281 | 103 | 151 | 194 | 160 | 109 | 63 | |
| Total | 12,162 | 6,843 | 2,057 | 3,402 | 4,229 | 3,970 | 2,454 | 1,415 | ||
| Age-Adjusted | REF | 1.13 (0.97, 1.32) |
1.41 (1.13, 1.75) |
1.27 (1.05, 1.54) |
1.26 (1.06, 1.50) |
1.12 (0.93, 1.35) |
1.28 (1.04, 1.59) |
1.23 (0.94, 1.61) |
||
| Multivariable-Adjustede | REF | 1.11 (0.95, 1.29) |
1.36 (1.09, 1.69) |
1.23 (1.01, 1.49) |
1.23 (1.03, 1.46) |
1.10 (0.91, 1.32) |
1.23 (0.99, 1.53) |
1.19 (0.91, 1.56) |
||
| T2Db | ||||||||||
| Ever GDd | Yes | 260 | 176 | 76 | 117 | 110 | 102 | 103 | 110 | |
| Total | 1,883 | 1,244 | 466 | 921 | 717 | 916 | 669 | 265 | ||
| Age-Adjusted | REF | 1.01 (0.82, 1.25) |
1.27 (0.96, 1.70) |
0.93 (0.73, 1.18) |
1.12 (0.87, 1.43) |
0.76 (0.59, 0.98) |
1.21 (0.94, 1.56) |
1.10 (0.76, 1.60) |
||
| Multivariable- Adjustede |
REF | 1.00 (0.80, 1.24) |
1.32 (0.98, 1.76) |
0.95 (0.74, 1.21) |
1.11 (0.86, 1.43) |
0.78 (0.61, 1.01) |
1.19 (0.92, 1.55) |
1.13 (0.77, 1.66) |
||
a REF=Reference = Never Urinary Incontinence, b Parous women, c Includes situations such as “waiting too long to go to the bathroom”, “taking diuretics”, and “drinking too many fluids”. d Reference = Never Gestational Diabetes, e Adjusted for age, BMI, parity, education, NSES, prudent and western diet, use of diuretics, vigorous physical activity, and smoking status.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



