
Submitted:
22 January 2025
Posted:
23 January 2025
You are already at the latest version
Abstract
BACKGROUND: Pneumonia is a significant cause of morbidity and mortality in neonates, particularly when accompanied by respiratory failure. This study aims to compare the effectiveness and outcomes of HHFNC and CPAP in improving respiratory outcomes and reducing adverse effects.
METHODS: The 220 patients were enrolled in the study (110 in each group) from the neonatal unit, after obtaining written informed consent from their parents/guardians. Nasal CPAP was applied to patients in group A through nasal canula with the following settings FiO2: 40-60%, PEEP: 5-8 cm H2O, flow: 4-6L/min. HHFNC was applied to patients in group B through the nasal cannula with the following setting FiO2: 40-60%, flow: 4-6L/min. Study variables were recorded in the proforma and analyzed using SPSS version 23.0.
RESULTS: The comparison of CPAP (Group A) and HHFNC (Group B) showed no significant differences in age, gestational age, or clinical parameters, except for a higher respiratory rate in HHFNC. The HHFNC group had significantly shorter durations of non-invasive ventilatory support and hospital stay. Adverse effects were more common in HHFNC, especially nasal mucosal injury, while sepsis was more frequent in CPAP. Treatment failure occurred more often in the HHFNC group. Neonatal outcomes were similar, with no significant differences in discharge rates, mortality, or intubation rates.
CONCLUSION: The study found that the duration of non-invasive ventilator support, shown by HHFNC, was significantly less when compared to CPAP. This suggests that HHFNC might be preferred for providing extended respiratory support in this patient population. Nonetheless, both HHFNC and CPAP appear safe and effective in supporting neonates through their respiratory challenges.
Keywords:
Continuous Nasal Positive Airway Pressure (CPAP)
; Humidified High Flow Nasal (HHFNC)
; Pneumonia
; Respiratory Failure
Introduction
The major age-related mortality with pneumonia occurs in neonates because of their poor lung defences and nonspecific clinical symptoms [1]. Pneumonia was the third largest cause of mortality among neonates, with 21.7 deaths per 100,000 live births in the first 7 days and 13.3 deaths per 100,000 live births from 7 to 27 days [2]. UNICEF estimates the number of pneumonia-related fatalities among children under the age of five in poor countries each year [3]. Pneumonia, a leading cause of respiratory failure and ICU admissions in paediatrics, is primarily attributed to hypoxemia due to ventilation-perfusion mismatch, increased breathing work, and hypercarbia [4].
Nasal continuous positive airway pressure (nCPAP) is the most popular non-invasive breathing assistance for preterm newborns, but its usage needs competent nursing care because of the bulky interfaces [5]. High-flow nasal cannula treatment (HFNC) is a gentler option that is becoming popular among newborns and children with respiratory diseases [6].
HFNC are tiny, thin binasal prongs that supply oxygen or oxygen/air mixes at flow rates greater than 1 L per minute. They are located inside the nares and can take up to half of the available space without a seal [7]. Patients may tolerate larger flow rates since the gas is appropriately warmed and humidified when given. These high flow rates can equal or surpass patients' inspiratory flow rates, limiting room air intake while ensuring that the percentage of oxygen (FiO2) inspired by patients matches the FiO2 given by the HFNC system. The heated, humidified high-flow delivered via nasal cannulae (HHHFNC) approach is increasingly being employed for noninvasive respiratory support in preterm newborns, critically sick children, and adults [8].
Over the last six years, the usage of HHFNC in neonatal intensive care units (NICUs) in wealthy nations has expanded dramatically [9]. This is owing to its effectiveness, safety, and perceived advantages to nCPAP, such as a simpler, smaller nasal interface and more comfort for babies. However, data is only available from larger randomised controlled studies, with the majority comparing basic respiratory assistance in preterm newborns [10]. Over the previous two years, 6 randomised studies have included 936 preterm newborns[11,12].
Literature supports that HFNC can avoid extubation failure, improve respiratory function, and aid in weaning off CPAP[13]. Another research found that nasal cannulae flows of up to 2.5 L/min are equally effective as nasal CPAP for treating apnoea of prematurity without raising oxygen requirements [14].
Previous studies on the treatment of respiratory failure in pre-term neonates have focused on comparing Humidified High Flow Nasal Cannula (HHFNC) with CPAP [15,16]. This study aims to compare both treatment modalities, focusing on the mean duration of hospital stay and the mean duration of dependency on respiratory support, focusing on the ease of administration, improved compliance, and better patient outcomes compared to traditional ventilation methods.
Materials and Methods
Study Design and Patient Enrolment
The quasi-experimental study was conducted after the ethical approval and consent taken from the parent/guardian. Patients were enrolled from the Neonatal Unit, at the University of Lahore teaching hospital, Lahore, Pakistan. Non-probability, consecutive sampling was used to add 220 (110 in each group) patients to the study. The sample size is calculated by using the power of study equal to 80% and level of significance equal to 5%, taking treatment failure in the HHFNC group as 38.1% and in CPAP as 20.9% was 220(110in each group) patients were enrolled in the study [17].
Patient Selection and Grouping
Patients were assigned to two groups (group A applied to CPAP and group B applied to HHFNC) using a computerized random table generator to obtain a trial sequence which was hidden in sequentially numbered sealed opaque envelopes prepared by co-investigator.
The research looked at individuals aged 1 to 28 days who had type 1 respiratory failure and needed non-invasive ventilatory assistance, such as a High-Flow Nasal Cannula or nasal Continuous Positive Airway Pressure. Patients with congenital heart disease or neuromuscular abnormalities were excluded, as were newborns suffering from type 2 respiratory failure or requiring invasive mechanical ventilation or intubation. The study intended to maintain the study's integrity. Additionally, participation was limited to those whose parents or guardians consented to take part in the study. This approach helps create a focused and relevant cohort for better understanding and managing type 1 respiratory failure in neonates.
Training Session
The Training session was arranged by the principal researcher for fellow doctors and nurses of the neonatal unit in which they were given detailed training regarding data collection, procedures and interventions used in this study. Term neonates meeting inclusion criteria were inducted into the study. All patients were evaluated to rule out any exclusion criteria.
Data Collection
Written and informed consent was taken from parents/legal guardians for each patient after explaining the procedure and complications. The patient’s history including gestational age was noted. Diagnosis of pneumonia and respiratory failure was established with the help of clinical findings, radiological findings, and arterial blood gas analysis. Baseline variables pH, PaCO2, and PaO2 were noted by arterial blood gases. The respiratory rate was recorded. Nasal CPAP was applied to group 1 through nasal canula with the following settings FiO2: 40-60%, PEEP: 5-8 cm H2O, Flow: 4-6L/min. HHFNC was applied to group 2 through the nasal cannula with the following setting FiO2: 40-60%, Flow: 4-6L/min. Any patient who could not maintain oxygen saturation (Spo2 < 90% on pulse oximetry) with CPAP or HHFNC or ABG suggestive of type 2 respiratory failure, was intubated and shifted to invasive ventilation, which was counted as treatment failure and was excluded from the study. Data was recorded about the duration of hospital stay in days & duration of application of respiratory support i.e. nCPAP or HHFNC at the time of discharge. Arterial Blood Gases were performed daily or as per the requirement to check the PaO2 and PaCO2. Vitals were recorded on an hourly basis, and any change of nCPAP & HHFNC settings were recorded. The same Antibiotics (Cefotaxime150mg/kg/24hr & Ampicillin 200mg/kg/24hr as 1st line) and other treatments including maintenance fluid were given to both groups as per requirement. All the data was recorded on a pre-designed proforma by the staff members and results were subjected to statistical analysis by the principal researcher to determine the significance of observed differences. The data collection continued until the enrolled neonates were discharged from the hospital.
The data collection aimed to analyse the following outcomes; Total. Duration of hospital stay in days, mean duration of application of respiratory support in hours, frequency of adverse events including sepsis, frequency of nasal mucosal injury, abdominal distension, feeding intolerance, outcome (discharged, expired, intubated and treatment failure) and neonatal outcomes (Discharge, Expired, Intubated).
Data Analysis
Collected data was entered and analyzed using Statistical Package for Social Science (SPSS) version 23.0. all the quantitative variables like age, APGAR score, gestational age of mother, duration of hospital, respiratory support, and total days of oxygen use up to the time of discharge for each group were reported by Mean+SD. All the qualitative variables like gender, neonatal outcomes (Discharge, Expired, Intubated), adverse events like sepsis, abdominal distention, feeding intolerance, and nasal mucosal injury) and outcome (discharged, expired, intubated and treatment failure) have been presented by frequency/percentages. Duration of hospital stay in days and mean duration of application of respiratory support in hours have been compared with Man Whitney U test according to normality of data. The comparison of adverse effects among both groups was compared by the Chi-square test. A P-value less than or equal to 0.05 was considered significant.
Results
Baseline Characteristics of Study Sample
The comparison of characteristics between Group A and Group B reveals no significant differences in several variables. The mean age (14.72 ± 8.45 days for Group A vs. 15.07 ± 8.02 days for Group B) and gestational age (32.71 ± 2.52 weeks for Group A vs. 32.45 ± 2.94 weeks for Group B) were similar between the two groups, with p-values of 0.796 and 0.472, respectively, indicating no significant differences. The gender distribution also showed no notable difference (p = 0.495), with a slightly higher percentage of females in both groups. Regarding clinical parameters, the APGAR score, SpO₂, heart rate (HR), arterial pH, pO₂, and pCO₂ values were similar between the groups, with p-values of 0.971, 0.735, 0.765, 0.363, 0.941, and 0.344, respectively, suggesting no significant differences. However, the respiratory rate was significantly higher in Group B (55.75 ± 11.66) compared to Group A (52.29 ± 11.23), with a p-value of 0.028, indicating a statistically significant difference between the two groups. (Table 1)
Comparison of Duration of Application of Non-Invasive Ventilatory Support (Hours) and Hospital Stay Between the Groups
The comparison of the duration of application of non-invasive ventilatory support and hospital stay between the two groups shows significant differences. The mean duration of non-invasive ventilatory support was significantly shorter in Group B (HHFNC) at 65.20 hours (±15.9) compared to Group A (CPAP), which had a mean of 72.29 hours (±20.7), with a p-value of 0.013, indicating statistical significance. Similarly, the mean duration of hospital stay was significantly shorter in Group B (HHFNC) at 20.14 days (±3.50) compared to Group A (CPAP), which had a mean of 24.25 days (±6.07), with a p-value of 0.000, confirming a significant difference. These finding suggest support that the HFNC may be associated with a shorter duration of both non-invasive ventilatory support and hospital stay compared to CPAP (Table 2). The most prevalent adverse impact in the CPAP group was sepsis, which was documented in eight instances, followed by nasal mucosal damage in seven. Feeding intolerance and stomach distention were reported in five and four patients, respectively. In contrast, the HHFNC group exhibited a greater rate of nasal mucosal damage (18 instances) compared to CPAP. Feeding intolerance and abdominal distention were recorded in 9 and 6 instances, respectively, whereas sepsis was diagnosed in 10 cases. These findings show that, while both groups suffered similar adverse effects, HHFNC was linked with a greater frequency of nasal mucosal damage, whereas sepsis was more common in the CPAP group (Figure 1).
Comparison of Treatment Failure in Both Groups
The incidence of treatment failure in the CPAP and HFNC groups. The 12 patients experienced treatment failure in the CPAP group, whereas 18 patients had treatment failure in HFNC. This suggests that a higher proportion of patients in the HFNC group experienced treatment failure compared to those in the CPAP group (Figure 2).
Comparison of Duration of Neonatal Outcome Between the Groups
The neonatal outcomes for both CPAP and HHFNC groups were compared. Among the total of 220 neonates, 194 (88.2%) were discharged, with 100 (90.9%) in the CPAP group and 94 (85.5%) in the HHFNC group. The difference in discharge rates between the two groups was not statistically significant, with a p-value of 0.224. In terms of mortality, 9 neonates (4.1%) expired, with 5 (4.5%) from the CPAP group and 4 (3.6%) from the HHFNC group, indicating a similar low incidence of mortality across both groups. Regarding intubation, 17 neonates (7.7%) required intubation, with a higher incidence in the HHFNC group (12 cases, 10.9%) compared to the CPAP group (5 cases, 4.5%). However, the p-value suggests that these differences were not statistically significant (Table 3).
Discussion
CPAP serves as the primary respiratory support modality for the majority of neonates experiencing respiratory distress. Regardless of the underlying etiology, this effective therapeutic approach confers benefits to most newborns [18]. Prompt initiation of nCPAP, either in the delivery room or within the initial hour of respiratory distress onset, has been shown to reduce the reliance on mechanical ventilation and surfactant administration, particularly in very preterm infants [19]. Nevertheless, the application of nCPAP is associated with potential drawbacks, including nasal injury, frequent displacement of nasal prongs, increased nursing time, and a requirement for skilled nursing personnel. Additionally, nCPAP failure rates reach approximately 15-25% among neonates receiving this mode of support [20]. In recent times, HFNC has growing acceptance as an alternative respiratory support modality for preterm infants. HFNC presents certain advantages over nCPAP, such as a reduced incidence of nasal trauma, utilization of patient and parent-friendly nasal prongs, and ease of use [21].
Owing to controversy in existing literature, the present study was aimed to compare two widely used respiratory support methods, HFNC and CPAP, in term neonates suffering from pneumonia with respiratory failure. The study involved term neonates with pneumonia and type 1 respiratory failure, with a mean age of 14.72 ± 8.45 days for Group A and 15.07 ± 8.02 days for Group B. Previous studies reported lower mean ages of 1-2 days respectively, for neonates with pneumonia and type 1 respiratory failure [22,23]. This considerable variation in mean age could potentially be attributed to differences in the age criteria used to include patients in the respective studies [24].
The gender distribution also showed no notable difference (p = 0.495), with a slightly higher percentage of females in both groups. Other studies reported the higher male-to-female ratios of 1.66:1 reported by Sarkar et al. (2018) [25] and Sharma (2018) reported an even higher proportion of male neonates (78.6%) in their study conducted in India [26]. The gestational age were similar between the two groups, indicating no significant differences. It is noteworthy that no previous study has been conducted specifically on term neonates in this particular comparison. However, studies conducted on preterm neonates have reported gestational ages of 32.5±1.5 weeks by Shin et al. (2017) in Korea [27]
The mean SPO2 at admission suggests that the patients in this study presented with lower oxygen saturation levels, indicating potential respiratory compromise or respiratory failure. The higher mean SPO2 observed in the literature suggests better oxygenation levels in their study population, possibly reflecting more favourable respiratory status or different patient characteristics [28]. In contrast, the lower mean SPO2 reported in the prior study implies that their sample population had insufficient oxygenation levels at admission, perhaps indicating more serious respiratory distress [29]. Maintaining proper oxygen levels is critical for controlling hypoxia which can cause organ malfunction and consequences. Differences in mean SPO2 levels between studies might be attributed to patient characteristics, illness severity, or treatment procedures. Consistency in respiratory rate with previous research improves outcomes dependability and generalizability. However, increased respiratory rates may suggest changes in illness severity, patient characteristics, or clinical care strategies [30]. Similarly, the heart rate data from this investigation and the current literature add to the results' consistency and dependability, as well as their generalizability to comparable patient groups. Previous reports of increased heart rates may imply variations in illness severity, patient characteristics, or clinical care techniques in their individual research cohorts. [31].
The arterial pH findings reported in this study and other studies highlights consistency in the acid-base status of patients with similar respiratory conditions in different research settings. Acid-base disturbances are crucial indicators of the patient's overall physiological status and can help identify the underlying cause and guide appropriate management. The similarity in PO2 values suggests comparable oxygenation levels in patients from both cohorts [32].
In this study, the mean duration of non-invasive ventilatory support and duration of hospital stay was significantly shorter in Group B compared to Group A. These results suggest that HHFNC may be associated with a shorter duration of both non-invasive ventilatory support and hospital stay compared to CPAP. These findings align with results reported previously where the mean duration of application was also higher in the CPAP group than the HHFNC group (69±94.8 vs. 65±99.9 hours), but the difference was not statistically significant [12]. However, it is important to note that other studies have reported different findings. Some studies showed an inverse relation, where the mean duration of application was less in the CPAP group than in the HHFNC group, but again the difference was not significant [33].
The longer mean duration of application in the CPAP group in this study suggests that CPAP may be utilized for a more extended period compared to HHFNC for providing non-invasive ventilatory support in this particular patient population. The variations in the duration of application between different studies may be influenced by differences in patient selection criteria, disease severity, and clinical management approaches. The lack of statistical significance in some studies could be due to the relatively small sample sizes or other factors that contribute to the variability in results.
The higher incidence of treatment failure in the HFNC group (compared to CPAP) is noteworthy. As reported in the literature indicates that HFNC may be less effective in cases of severe respiratory distress, necessitating intubation or escalation of care [34,35]. This underscores the importance of patient selection when deciding between HHFNC and CPAP as initial interventions. Studies advocate for clear clinical criteria to minimize the risk of treatment failure in vulnerable neonates [36].
This study adds to the expanding body of evidence comparing HFNC and CPAP for treating respiratory insufficiency in preterm babies. While HHFNC has benefits such as shorter hospital stays and shorter ventilatory support duration, it may also be linked with increased rates of treatment failure and particular side effects such as nasal mucosal damage. These findings highlight the necessity of individualised therapy strategies based on clinical severity and patient-specific characteristics in optimising outcomes. The study's applicability to other healthcare settings may be restricted, and it may not address long-term effects such as chronic respiratory diseases. Future multicenter research including bigger, varied populations and standardised techniques are required.
Conclusions
The duration of non-invasive ventilator support, shown by HFNC, was significantly less while compared to CPAP. Moreover, length of hospital stay was also significantly short in HHFNC group than CPAP. This suggests that HHFNC might be preferred for providing extended respiratory support in this patient population. Nonetheless, both HHFNC and CPAP appear safe and effective in supporting neonates through their respiratory challenges. Ultimately, individual patient needs and clinical considerations should guide the selection of the most suitable respiratory support method. Further research is needed to confirm these findings and explore potential strategies for mitigating adverse effects associated with HHFNC.
Conflicts of Interest statement
All authors declare no conflict of Interest
Author’s contribution
All Authors contributed equally to the work
Acknowledgments
N.A.
Funding
There is no funding source.
Informed consent
Informed consent was obtained from the Parents and the attendees of all participants included in the study.
Data Availability
The datasets generated for this study are available in the attachment
Ethics Statement
The studies involving human participants were reviewed and approved by the Human Research Ethics Committee at The University of Lahore, Pakistan. Written informed consent to participate in this study was provided by the participants.
References
- Long, M.E.; Mallampalli, R.K.; Horowitz, J.C.J.C.S. Pathogenesis of pneumonia and acute lung injury. 2022, 136, 747–769. [Google Scholar] [CrossRef] [PubMed]
- Kumar, C.S.; Subramanian, S.; Murki, S.; Rao, J.; Bai, M.; Penagaram, S. , et al. Predictors of mortality in neonatal pneumonia: an INCLEN childhood pneumonia study. 2021, 58, 1040–1045. [Google Scholar]
- Chisti, M.J.; Kawser, C.A.; Rahman, A.S.M.M.H.; Shahid, A.S.M.S.B.; Afroze, F.; Shahunja, K. , et al. Prevalence and outcome of anemia among children hospitalized for pneumonia and their risk of mortality in a developing country. 2022, 12, 10741. [Google Scholar] [PubMed]
- Nascimento-Carvalho CMJJdp. Community-acquired pneumonia among children: the latest evidence for an updated management. 2020, 96, 29–38.
- Malakian, A.; Aramesh, M.R.; Agahin, M.; Dehdashtian, M.J.B.p. Non-invasive duo positive airway pressure ventilation versus nasal continuous positive airway pressure in preterm infants with respiratory distress syndrome: a randomized controlled trial. 2021, 21, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Kenner, C.; Boykova, M.V. Neonatal nursing care handbook: an evidence-based approach to conditions and procedures; Springer Publishing Company, 2021. [Google Scholar]
- Campbell, D.E. Continuing Care of the Infant After Transfer From Neonatal Intensive Care; Neonatology for Primary Care: American Academy of Pediatrics Itasca: IL, 2020. [Google Scholar]
- Sjöblom, A. Clinical and Physiological Consequences of Preoxygenation Using High-Flow Nasal Oxygen in Emergency Anaesthesia; Karolinska Institutet: Sweden, 2023. [Google Scholar]
- Çetinkaya, M.; Atasay, B.; Perk, Y.J.T.A.o.P.T.P.A. Turkish Neonatal Society guideline on the transfusion principles in newborns. 2018, 53 (Suppl 1), S101. [Google Scholar] [CrossRef]
- Owen, L.S.; Manley, B.J.; Davis, P.G.; Doyle, L.W.J.T.L. The evolution of modern respiratory care for preterm infants. 2017, 389, 1649–1659. [Google Scholar] [CrossRef] [PubMed]
- Dunn, M.S.; Kaempf, J.; de Klerk, A.; de Klerk, R.; Reilly, M.; Howard, D. , et al. Randomized trial comparing 3 approaches to the initial respiratory management of preterm neonates. 2011, 128, e1069–e1076. [Google Scholar]
- Murki, S.; Singh, J.; Khant, C.; Kumar Dash, S.; Oleti, T.P.; Joy, P. , et al. High-flow nasal cannula versus nasal continuous positive airway pressure for primary respiratory support in preterm infants with respiratory distress: a randomized controlled trial. 2018, 113, 235–241. [Google Scholar] [PubMed]
- Chang, C.-J.; Chiang, L.-L.; Chen, K.-Y.; Feng, P.-H.; Su, C.-L.; Hsu, H.-S.J.C.r.j. High-Flow Nasal Cannula versus Noninvasive Positive Pressure Ventilation in Patients with Heart Failure after Extubation: An Observational Cohort Study. 2020, 2020, 6736475. [Google Scholar] [CrossRef]
- Sreenan, C.; Lemke, R.P.; Hudson-Mason, A.; Osiovich, H.J.P. High-flow nasal cannulae in the management of apnea of prematurity: a comparison with conventional nasal continuous positive airway pressure. 2001, 107, 1081–1083. [Google Scholar] [CrossRef]
- Frat, J.-P.; Coudroy, R.; Marjanovic, N.; Thille, A.W.J. High-flow nasal oxygen therapy and noninvasive ventilation in the management of acute hypoxemic respiratory failure. 2017, 5((14)). [Google Scholar] [CrossRef]
- Dumpa, V.; Avulakunta, I.; Bhandari, V.J.E.R.o.R.M. Respiratory management in the premature neonate. 2023, 17, 155–170. [Google Scholar] [CrossRef]
- Lavizzari, A.; Colnaghi, M.; Ciuffini, F.; Veneroni, C.; Musumeci, S.; Cortinovis, I. , et al. Heated, humidified high-flow nasal cannula vs nasal continuous positive airway pressure for respiratory distress syndrome of prematurity: a randomized clinical noninferiority trial. 2016. [Google Scholar]
- Madar, J.; Roehr, C.C.; Ainsworth, S.; Ersdal, H.; Morley, C.; Ruediger, M. , et al. European Resuscitation Council Guidelines 2021: Newborn resuscitation and support of transition of infants at birth. 2021, 161, 291–326. [Google Scholar] [PubMed]
- De Paoli, A.; Morley, C.; Davis, P.J.A.o.D.i.C.-F.; Edition, N. Nasal CPAP for neonates: what do we know in 2003? 2003, 88, F168–F172. [Google Scholar] [CrossRef]
- Chan, S.Y. Development, Implementation, and Evaluation of a Clinical Practice Guideline for Care of Preterm Infants Receiving Non-Invasive Ventilation: A Before and After Study. The Chinese University of Hong Kong: Hong Kong, 2021. [Google Scholar]
- Shi, Y.; Muniraman, H.; Biniwale, M.; Ramanathan, R.J. A review on non-invasive respiratory support for management of respiratory distress in extremely preterm infants. 2020, 8, 270. [Google Scholar] [CrossRef]
- Abadesso, C.; Nunes, P.; Silvestre, C.; Matias, E.; Loureiro, H.; Almeida, H.J.P.R. Non-invasive ventilation in acute respiratory failure in children. 2012, 4, e16. [Google Scholar] [CrossRef]
- De Luca, D.; Tingay, D.G.; Van Kaam, A.H.; Courtney, S.E.; Kneyber, M.C.; Tissieres, P. , et al. Epidemiology of neonatal acute respiratory distress syndrome: prospective, multicenter, international cohort study. 2022, 23, 524–534. [Google Scholar]
- Silveyra, P.; Fuentes, N.; Rodriguez Bauza, D.E. Sex and gender differences in lung disease. Lung Inflammation in Health and Disease; Springer, 2021; Volume II, pp. 227–258. [Google Scholar]
- Sarkar, M.; Sinha, R.; Roychowdhoury, S.; Mukhopadhyay, S.; Ghosh, P.; Dutta, K. , et al. Comparative study between noninvasive continuous positive airway pressure and hot humidified high-flow nasal cannulae as a mode of respiratory support in infants with acute bronchiolitis in pediatric intensive care unit of a tertiary care hospital. 2018, 22, 85. [Google Scholar]
- Sharma, D.; Kaur, A.; Farahbakhsh, N.; Agarwal, S.J.T.J.o.M.-F.; Medicine, N. To compare nasal mask with binasal prongs in delivering continuous positive airway pressure for reducing need of invasive ventilation: randomized controlled trial. 2021, 34, 1896. [Google Scholar] [CrossRef]
- Shin, J.; Park, K.; Lee, E.H.; Choi, B.M. Humidified high flow nasal cannula versus nasal continuous positive airway pressure as an initial respiratory support in preterm infants with respiratory distress: a randomized, controlled non-inferiority trial. 2017, 32, 650. [Google Scholar] [CrossRef] [PubMed]
- Foglia, E.E.; Carper, B.; Gantz, M.; DeMauro, S.B.; Lakshminrusimha, S.; Walsh, M. , et al. Association between policy changes for oxygen saturation alarm settings and neonatal morbidity and mortality in infants born very preterm. 2019, 209, 17–22.e2. [Google Scholar]
- Sarker, S.K.; Choudhury, U.K.; Mohsin, M.; Mondal, S.K.; Begum, M.J.J.o.C.; Research, A.M. Diagnostic validity of ratio between differences of central venous to arterial CO2 and arterial to central venous O2 content in diagnosis of anaerobic metabolism among septic patients. 2021, 8, 34–38. [Google Scholar] [CrossRef]
- Cristea, A.I.; Ren, C.L.; Amin, R.; Eldredge, L.C.; Levin, J.C.; Majmudar, P.P. , et al. Outpatient respiratory management of infants, children, and adolescents with post-prematurity respiratory disease: an official American Thoracic Society clinical practice guideline. 2021, 204, e115–e133. [Google Scholar]
- Wu, C.; Chen, X.; Cai, Y.; Zhou, X.; Xu, S.; Huang, H. , et al. Risk factors associated with acute respiratory distress syndrome and death in patients with coronavirus disease 2019 pneumonia in Wuhan, China. 2020, 180, 934–943. [Google Scholar]
- Friedman, M.L.; Nitu, M.E. Acute respiratory failure in children. 2018, 47, e268–e273. [Google Scholar] [CrossRef]
- Luo, J.; Duke, T.; Chisti, M.J.; Kepreotes, E.; Kalinowski, V.; Li, J.J. Efficacy of high-flow nasal cannula vs standard oxygen therapy or nasal continuous positive airway pressure in children with respiratory distress: a meta-analysis. 2019, 215, 199–208.e8. [Google Scholar] [CrossRef]
- Thota, U.R.; Palle, S.; Pandala, P.; Gangadhari, S.; Cherukuri, N.J.I. Outcome of High-flow Nasal Cannula Therapy in Children with Acute Respiratory Distress in A Tertiary Care Centre: A Prospective Cohort Study. 6 (S1), 13360–13367. [CrossRef]
- Jeengar, B. To compare the effectiveness of Heated Humidified High-Flow Nasal Cannula (HHHFNC) and Continuous Positive Airway Pressure (CPAP) in neonates with respiratory distress syndrome (RDS). 2024. [Google Scholar]
- Jose, D.; Parameswaran, N.J.I.J.o.P. Advances in management of respiratory failure in children. 2023, 90, 470–480. [Google Scholar] [CrossRef]
Figure 1.
Comparison of adverse effects in both groups. b Chi Square test. Taking p-value≤0.05 as significant.
Figure 1.
Comparison of adverse effects in both groups. b Chi Square test. Taking p-value≤0.05 as significant.
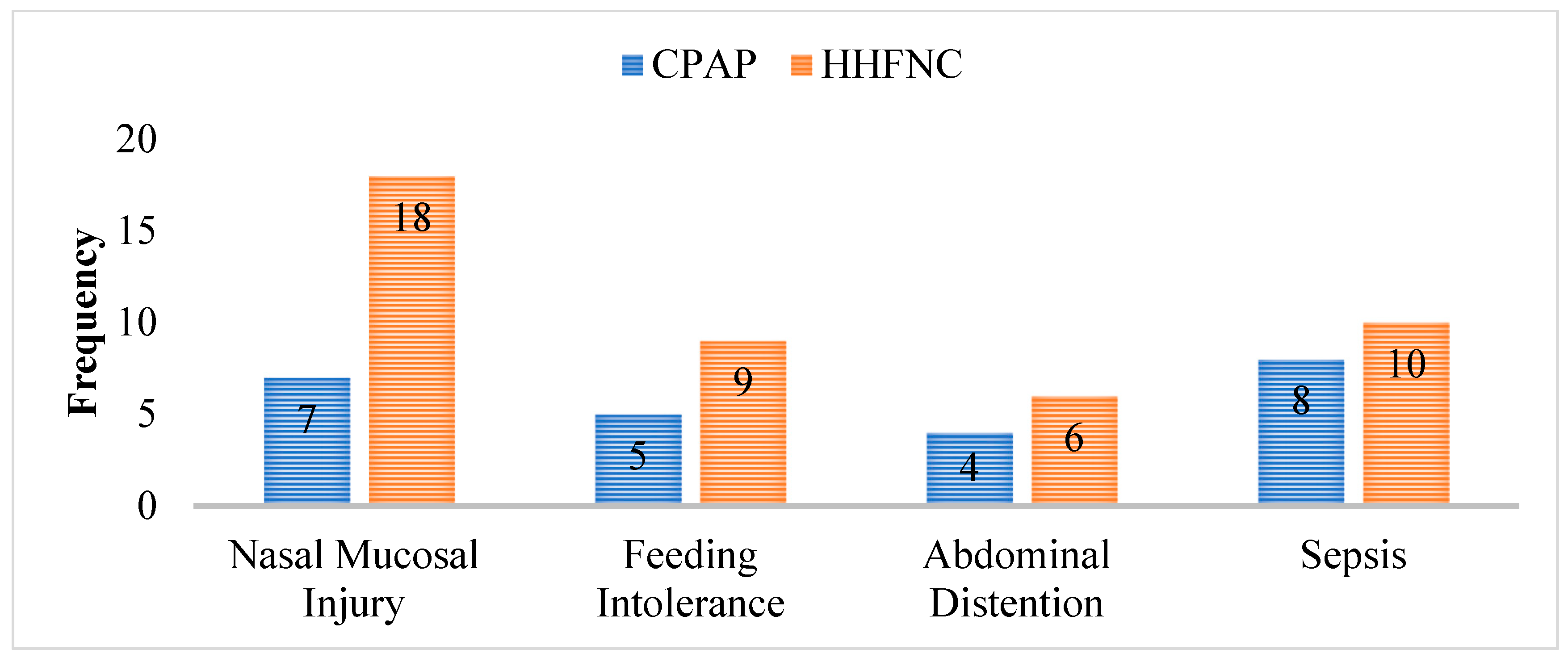
Figure 2.
Comparison of Treatment failure in both groups. b Chi Square test. Taking p-value≤0.05 as significant.
Figure 2.
Comparison of Treatment failure in both groups. b Chi Square test. Taking p-value≤0.05 as significant.
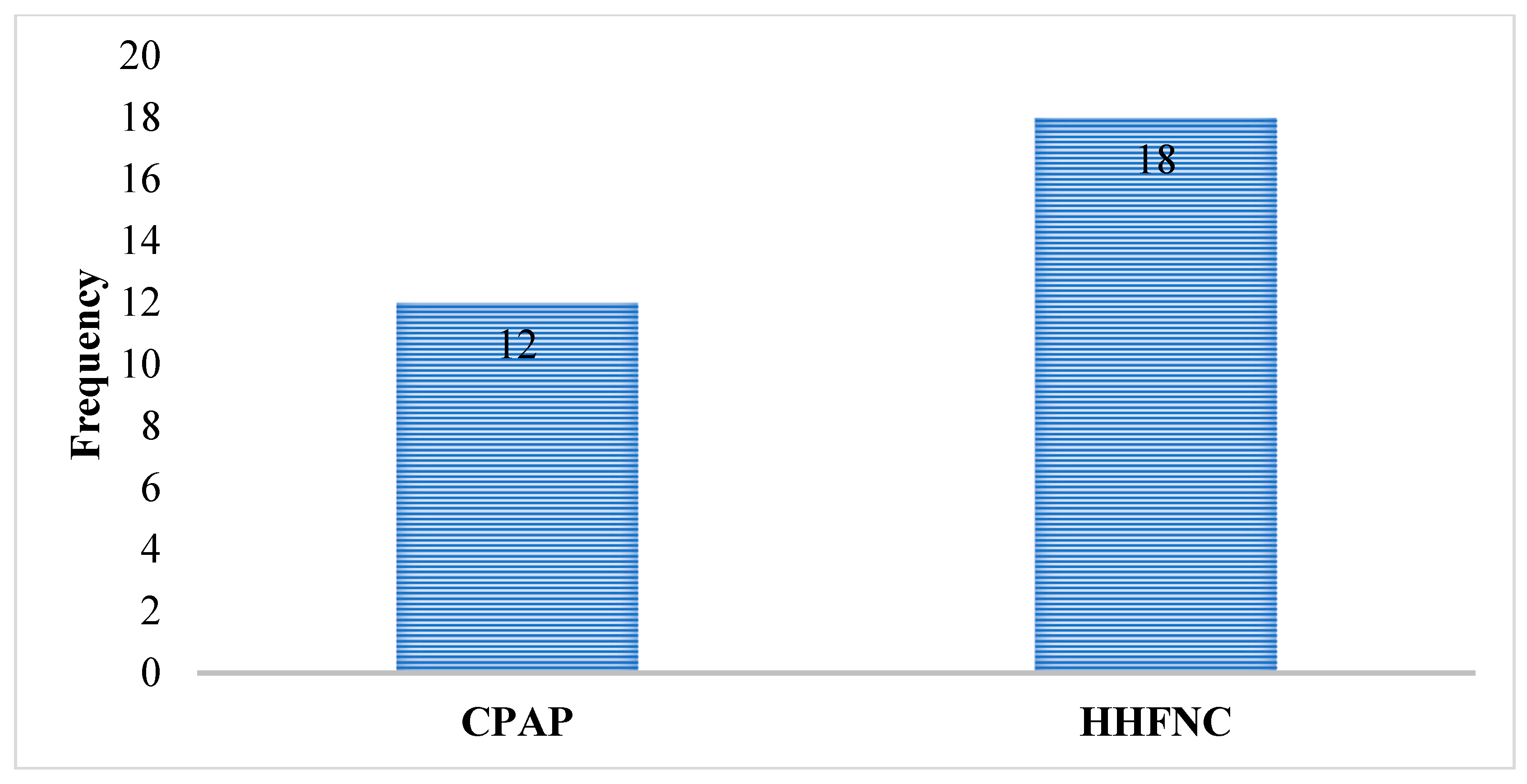

Table 1.
Comparison between the Groups at Baseline.
| Characteristics | Group A (n=128) | Group B (n=128) | p-value |
|---|---|---|---|
| Age (1-28 days) | 14.72±8.45 | 15.07±8.02 | 0.796 a |
| Gender | |||
| Male | 44 (40.0%) | 49 (44.5%) | 0.495 b |
| Female | 66 (60.0%) | 61 (55.5%) | |
| Gestational Age | 32.71±2.52 | 32.45±2.94 | 0.472 a |
| APGAR Score | 5.98+0.88 | 5.46+0.81 | 0.971 a |
| SPO2 | 69.69±18.2 | 70.43±17.38 | 0.735 a |
| Respiratory Rate | 52.29±11.23 | 55.75±11.66 | 0.028 a |
| HR Rate | 134.28±18.69 | 133.46±17/83 | 0.765 a |
| Arterial Ph | 6.26±1.37 | 6.09±1.41 | 0.363 a |
| PO2 | 63.31±12.1 | 63.02±11.5 | 0.941 a |
| PCO2 | 40.56±5.42 | 39.87±5.23 | 0.344 a |
a Mann Whitney U test. b Chi Square test. Taking p-value≤0.05 as significant.
Table 2.
Comparison of Duration of Application of Non-invasive Ventilatory Support (hours) and hospital stay between the Groups.
Table 2.
Comparison of Duration of Application of Non-invasive Ventilatory Support (hours) and hospital stay between the Groups.
| Duration of Application of Non-invasive Ventilatory Support (hours) | |||
|---|---|---|---|
| Study Group | Mean | Std. Deviation | p-value |
| CPAP (A) | 72.29 | 20.7 | 0.013a |
| HHFNC (B) | 65.20 | 15.9 | |
| Hospital stay in days | |||
| CPAP (A) | 24.25 | 6.07 | 0.000 a |
| HHFNC (B) | 20.14 | 3.50 | |
a Mann Whitney U test, Taking p-value≤0.05 as significant.
Table 3.
Comparison of Duration of Neonatal outcome between the Groups.
| Neonatal Outcome | Groups | Total | P-value | |
|---|---|---|---|---|
| CPAP | HHFNC | |||
| Discharged | 100(90.9%) | 94(85.5%) | 194(88.2%) | b 0.224 |
| Expired | 5(4.5%) | 4(3.6%) | 9(4.1%) | |
| Intubated | 5(4.5%) | 12(10.9%) | 17(7.7%) | |
| Total | 110 | 110 | 220 | |
b Chi Square test. Taking p-value≤0.05 as significant.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



