
Submitted:
10 February 2025
Posted:
11 February 2025
You are already at the latest version
Abstract
Background/Objectives: To determine the reliability of simple ultrasound (US) markers and CA-125 measurement in diagnosing peri- and postmenopausal ovarian masses. Methods: The study was conducted in a retrospective setting. Preoperative imaging properties of peri- (PEM) and postmenopausal (POM) ovarian cysts were examined. According to US findings, two groups were made: (1) simple cysts: unilocular, anechoic cysts without any solid part, (2) complex cysts: cystic structures with different parameters from the simple cysts. Imaging characteristics, size of the mass, and demographic data were matched with histology and CA125 levels. Results: 379 cystic structures (PEM: N=195, average age: 45.6yrs; range: 40-54yrs, POM: N=184, average age 61.2yrs; range: 41-88yrs) were analyzed. In the PEM group 75 simple (Ø<5cm N=32, Ø≥5cm N=43) and 122 complex cysts (Ø<5cm N=29, Ø≥5cm, N=93), while in the POM group 49 simple (Ø<5cm N=9, Ø≥5cm N=40) and 135 complex cysts (Ø<5cm N=15, Ø≥5cm N=120) were found. In the PEM group, malignancy was detected in complex cysts larger than 5cm (N=16, 17.58%). In the POM group malignancy was present in 40 cases, three of them proved to be smaller than 5cm. Majority of cysts were functional (54.36 %) in the PEM group. In the POM group, serous cysts were the most frequent (38.04%), followed by malignant (21.74%) and mucinous cysts (13.04%). CA125 was elevated in 66 of 217 cases (30.41%); only 23 were malignant (NPV: 0.95, PPV: 0.35). Conclusions: Functional cysts are frequently found among perimenopausal ovarian cysts, but malignancy was detected only in cysts with complex morphology larger than 5 cm. However, complex cysts of any size carry a significant risk of malignancy in menopause, thus, surgery is recommended. Simple cysts can be followed by serial scans in both groups. CA-125 did not give added value to the detection of malignancy.
Keywords:
ovary
; ovarian cancer
; ultrasonography
; complex cyst
; simple cyst
; CA125
; diagnostics
; basic ultrasound scan
1. Introduction
The prevalence of cystic ovarian structures in the peri- and postmenopause is increased. Bimanual examination, serum tumor markers, and transvaginal ultrasound examinations can also help to detect adnexal masses. As the majority of these cystic structures show no malignant potential, it is essential to easily and effectively select the high-risk masses for appropriate care [1]. Functional and malignant cysts can be characterized by their symptoms at the same time. Therefore, more than 60% of ovarian cancers are detected at stage III. or IV.[2]. In case of ovarian malignancies CA-125 was recommended to increase the detection rate, but it can be used effectively together with transvaginal US scans [3,4,5].
Since transvaginal probes have been introduced, several scoring systems have been developed to increase the detection rate of grayscale ultrasonography [6,7,8,9,10]. Papillary projections, thick and irregular walls, and septated or large multilocular cysts proved to carry a higher risk for malignancy as they are called complex cysts [11,12,13].
As a result of international multicentre studies evidence-based scoring systems have been developed by the IOTA (International Ovarian Tumour Analysis) group [10,14,15]. The work of this collaboration group has been dominant in the ultrasound-based diagnosis of adnexal masses in the last two decades and put the diagnostic process on an evidence-based and reliable level. Since ADNEX model has been developed, a mathematical model is on hand for everyone with different experiences to distinguish between benign and malignant lesions with an efficacy reaching the level of expert's opinion, so-called ‘pattern recognition’ [16,17,18].
Risk factors affecting the formation of cystic ovarian structures, such as genetic predisposition, multiparity, and previous gynecological surgeries, were examined in several studies [19,20].
The aim of this study was to determine the efficacy of simple grayscale ultrasound markers and the additive value of CA-125 in the detection and the triage of ovarian cystic structures in the peri- and postmenopause.
2. Materials and Methods
This study was performed in the Department of Obstetrics and Gynecology at the University of Debrecen, Debrecen, Hungary. Imaging properties of peri- (PEM) and postmenopausal (POM) ovarian cysts were examined preoperatively. All patients underwent transvaginal ultrasound examinations preoperatively (ATL HDI-3000, Bothell, Washington, USA, equipped with 5,9MHz transvaginal probe and Medison Accuvix XQ, Medison Co., Ltd. Seoul, South Korea, equipped with a 5-8MHz transvaginal probe Kretztechnik AG, Zipf, Austria). Patients over the age of 40 with cystic adnexal masses were consecutively recruited. Patients without evident clinical signs of menopause reporting no climacteric symptoms were involved in the PEM group, as well as those who previously underwent hysterectomy under the age of 50 (range: 40-54yrs, average: 45.57yrs). Lack of regular periods for more than one year or hysterectomy in the history of patients over 50 years of age were selected for the POM group (range: 41-88yrs, average: 61,24yrs). Overall, 343 patients with 379 cystic structures were involved in the study. US examinations were independent of the menstrual cycle and were repeated within three months in 168 cases (44,32%). When follow-up was performed, only the preoperative US finding was chosen to participate. According to US findings, two groups were made: (1) simple cysts: unilocular, anechoic cysts without any solid structure, (2) complex cysts: cystic structures with different parameters and even containing solid parts. Imaging characteristics, and size were matched with histology and CA125 levels. The cut-off level for CA-125 was 35 kIU/L. According to the size of the cysts, two subgroups were made within each reproductive group, and 5cm was chosen for this purpose. Risk factors affecting the formation of cystic structures in the ovary were also observed in this study, such as parity, previous pelvic surgeries, and family history of ovarian cancer.
Statistical analysis was performed using SPSS 10.0. Significance was checked using Mann-Whitney, Chi-square, and Kruskal-Wallis tests.
3. Results
In the PEM group 75 simple (Ø<5cm N=32, Ø≥5cm N=43) and 122 complex cysts (Ø<5cm N=29, Ø≥5cm, N=93), while in the POM group 49 simple (Ø<5cm N=9, Ø≥5cm N=40) and 135 complex cysts (Ø<5cm N=15, Ø≥5cm N=120) were found. In the PEM group malignancy was detected only in complex cysts larger than 5cm (N=16, 17.58%). In the POM group, malignancy was present in 40 cases, three of which proved to be smaller than 5cm. The majority of the masses were functional (54.36 %) in the PEM group. In the POM group, serous cysts were the most frequent (38.04%), followed by malignant (21.74%) and mucinous cysts (13.04%). It should be noticed that in the POM group, functional cysts can also be found in 5.43% of the cases (N=10). Details are shown in Table 1.
CA 125 determination was performed in 194 cases (51.19%). In case of masses larger than 5cm the distribution of CA125 values is different between simple and complex structures (p=0.003). Postmenopausal status is responsible for this significance, as dividing the patients into PEM and POM groups (PEM: p=0.112, NS while POM: p=0.009). There is no significant difference in the CA125 values between PEM and POM groups in case of masses smaller than 5cms (p=0.51). On the other hand, a significant correlation was also detected between histological findings and abnormal biomarker values in the POM group (p‹0.05), while the same could not be seen in the PEM group (p=0.159). Naturally, higher serum biomarker levels were detected in borderline and malignant tumors (p‹0.001). Moreover, the distribution of CA125 values is different in complex morphology-associated histological results (p‹0.001) but not in the simple morphological group (p=0.171).
The occurrence of malignant or borderline lesions was significantly higher in the POM group (p=0.001) and also among the complex masses (p‹0.001). Complex morphology carries a significant risk for malignancy both in perimenopausal and postmenopausal adnexal masses (p=0.005). The same tendency cannot be noticed in lesions with simple ultrasonographic features (p=0.402). The largest diameter of the mass affects the histological findings. In the whole study population, borderline and malignant masses were significantly larger (p‹0.001). This difference is supported by perimenopausal cases (p‹0.001), while the same cannot be noticed in case of postmenopausal patients (p=0.147). Details are shown in Figure 1.
The importance of the cut-off size is supported by the fact that a significant difference (p‹0.001) is present in complex structures between different histological findings regarding the largest diameter of the tumor, which correlation is not present in case of simple cysts (p=0.109). Regardless of the cut-off size, a difference still exists between histological types of complex morphology (p‹0.001), which is present in simple morphology as well (p=0.017).
Factors affecting the formation of cystic structures in the ovary can be seen in Table 2. At least one delivery was present in 84.96% of the cases. 210 cysts caused some kind of complaint for the patient (55.41%), of which the most common was pelvic pain in 160 cases (42.22%). A positive correlation was found between the number of deliveries and symptoms: women having at least two deliveries are more likely to suffer from pelvic pain (p=0.046). A negative correlation was detected between tumor size and presence of any complaint (p=0.842) (Figure 3.). In 336 cases, laparotomy was performed (88.65%). Previous interventions affecting the pelvis were found overall in 114 cases (30.08%), majority of these were hysterectomies (N=71, 18.73%). Family history of ovarian cancer was found only in 4 cases (1.06%).
4. Discussion
Cystic structures of the ovaries can be found in 11-16% of the cases in postmenopause and more frequently in the perimenopause [21]. The risk of malignant transformation of benign cysts is still an open question [22]. It was proven in several studies that the risk of malignant transformation is directly proportional to the number of EGF receptors in the cystic fluid [23,24,25]. In our study, we did not observe this connection.
According to the fact that ovarian pathologies depend on the functional state of the ovaries, the division of the population into peri-and postmenopausal groups is necessary. Koonings et al. found 13% risk for malignant transformation in the perimenopause, which increases to 45% in the postmenopausal group [26]. This transformation is more likely to develop in larger cysts. Modesitt et al. advised 10 cm for cut off level while Osmers et al. found 3 cms of diameter for the border between low-risk and high-risk groups [27,28]. 5 cms was recommended by Auslender et al. and Reimer et al., and so it was used in this study as well [23,29]. The IOTA group advises several diagnostic algorithms for the detection of adnexal masses. In these algorithms, most ultrasound characteristics, such as tumor size, are independent of the menopausal status. On the other hand, tumor size affects the performance of subjective assessment, mathematical models (LR1 and LR2), the IOTA simple rules, and also the risk of malignancy index (RMI) in discriminating correctly between benign and malignant adnexal masses [30]. Using the IOTA simple rules to determine reproductive status is not a basic step. Subjective assessment, called as “pattern recognition” is superior to any scoring system especially if it was carried out by experienced hands [15]. On the other hand, the most developed mathematical model, the so-called ADNEX-model uses not just the largest diameter of the lesion but also the largest diameter of the presenting solid component, if there is any [16]. Based on a recent paper by Landolfo et al. the suggested method for routine management of adnexal masses is the ‘Two step strategy’ using the Benign descriptors (BD) and the ADNEX model as a second step in unclassifiable cases. According to their data 37% of the adnexal lesions can be treated as benign just using the benign descriptors, which use 10 cm as a threshold for discrimination. The unclassifiable masses were analyzed using the ADNEX model. Excellent diagnostic performance has been reported providing an AUC of 0.94 for the use of this strategy. The discrimination between benign and malignant was better calibrated in postmenopausal patients, but the diagnostic efficiency was nearly the same in both groups [31].
In our study, it was shown that perimenopausal cystic structures carry malignancy in 4.22% of the cases which correlates with the results of Ekerhovd et al (0.7%) and Osmers et al. (0.8%) [2,32]. Echogenicity, wall structure, septation, and presence of papillarization or solid part should be noticed when considering the complexity of a cyst because this is compulsory for a correct diagnostic decision. Timmerman et al. and Ueland et al. designed scoring systems based on the volume of cysts and wall structures to help these decisions [8,10]. Neither these systems nor any of the IOTA’s mathematical models were not used in this study.
In the postmenopausal group the risk of malignancy is not irrelevant which fact was supported by our result: 40 cysts found out to be malignant (10.55%) of the cases, 39 of them proved to have complex morphological findings (97.5%). Our data correlates with the results of Osmers et al. (9.6%) and Ekerhovd et al. (10%) [2,28]. According to these facts, surgical removal of these structures is necessary. According to this study, simple postmenopausal cysts can carry malignancy in only 0.26% of the cases, their regular follow-up is recommended with or without determination of CA-125. In a recent review by Ya-Na Liu et al. 1 in 10000 malignancy rate was reported in postmenopausal simple cysts which supports our finding [33].
CA-125 alone has a very low screening sensitivity for stage I. ovarian cancer (60%) and a specificity of 99% [34,35]. In combination with TVS, sensitivity increases up to 85% [36]. In this study, the detection rate was only 30.41%. It can be elevated in benign diseases such as endometriosis, PID, fibroids, and Meigs-syndrome [37,38]. Several studies support that it has to be used together with ultrasound scans to improve its diagnostic benefit and should not be used alone for the decision of the dignity of ovarian cysts, especially in perimenopause [17,39,40,41]. It has been proven that elevated CA125 values do not improve the discrimination between benign and malignant lesions, especially in experienced examiners [42]. On the other hand it is used also in the most sophisticated mathematical model, the ADNEX where it facilitates the discrimination of malignant subtypes [16].
5. Conclusions
A simple diagnostic algorithm based on simple or complex morphology of ovarian masses during ultrasonography can easily decrease the number of surgeries and high hospital costs. Categorizing cystic structures into these two groups can be a reliable alternative to mathematical models in the case of simple cysts both peri- and postmenopause.
Author Contributions
Conceptualization, B.E., Z.T. and A.J.; methodology, B.E..; formal analysis, B.E.; investigation, B.E.; writing—original draft preparation, B.E.; writing—review and editing, B.E., A.J.; visualization, G.J.Sz..; supervision, J.A. and Z.K..; project administration, B.E. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of University of Debrecen (DE RKEB 4606-2016).
Informed Consent Statement
Patient consent was waived due to the retrospective nature of the study.
Data Availability Statement
In accordance with the journal’s guidelines, the data presented in this study are available upon request from the corresponding author for the reproducibility of this study if such is requested.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Menon, U.; Gentry-Maharaj, A.; Hallett, R.; Ryan, A.; Burnell, M.; Sharma, A.; Lewis, S.; Davies, S.; Philpott, S.; Lopes, A.; et al. Sensitivity and specificity of multimodal and ultrasound screening for ovarian cancer, and stage distribution of detected cancers: results of the prevalence screen of the UK Collaborative Trial of Ovarian Cancer Screening (UKCTOCS). Lancet Oncol 2009, 10, 327–340. [Google Scholar] [CrossRef] [PubMed]
- Ekerhovd, E.; Wienerroith, H.; Staudach, A.; Granberg, S. Preoperative assessment of unilocular adnexal cysts by transvaginal ultrasonography: a comparison between ultrasonographic morphologic imaging and histopathologic diagnosis. Am J Obstet Gynecol 2001, 184, 48–54. [Google Scholar] [CrossRef] [PubMed]
- Einhorn, N.; Sjovall, K.; Knapp, R.C.; Hall, P.; Scully, R.E.; Bast, R.C., Jr.; Zurawski, V.R., Jr. Prospective evaluation of serum CA 125 levels for early detection of ovarian cancer. Obstet Gynecol 1992, 80, 14–18. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, I.J.; Skates, S.J.; MacDonald, N.; Menon, U.; Rosenthal, A.N.; Davies, A.P.; Woolas, R.; Jeyarajah, A.R.; Sibley, K.; Lowe, D.G.; et al. Screening for ovarian cancer: a pilot randomised controlled trial. Lancet 1999, 353, 1207–1210. [Google Scholar] [CrossRef]
- Collins, W.P.; Bourne, T.H.; Campbell, S. Screening strategies for ovarian cancer. Curr Opin Obstet Gynecol 1998, 10, 33–39. [Google Scholar] [CrossRef]
- Goldstein, S.R.; Subramanyam, B.; Snyder, J.R.; Beller, U.; Raghavendra, B.N.; Beckman, E.M. The postmenopausal cystic adnexal mass: the potential role of ultrasound in conservative management. Obstet Gynecol 1989, 73, 8–10. [Google Scholar] [CrossRef]
- Sassone, A.M.; Timor-Tritsch, I.E.; Artner, A.; Westhoff, C.; Warren, W.B. Transvaginal sonographic characterization of ovarian disease: evaluation of a new scoring system to predict ovarian malignancy. Obstet Gynecol 1991, 78, 70–76. [Google Scholar]
- Ueland, F.R.; DePriest, P.D.; Pavlik, E.J.; Kryscio, R.J.; van Nagell, J.R., Jr. Preoperative differentiation of malignant from benign ovarian tumors: the efficacy of morphology indexing and Doppler flow sonography. Gynecol Oncol 2003, 91, 46–50. [Google Scholar] [CrossRef]
- Granberg, S.; Wikland, M.; Jansson, I. Macroscopic characterization of ovarian tumors and the relation to the histological diagnosis: criteria to be used for ultrasound evaluation. Gynecol Oncol 1989, 35, 139–144. [Google Scholar] [CrossRef]
- Timmerman, D.; Ameye, L.; Fischerova, D.; Epstein, E.; Melis, G.B.; Guerriero, S.; Van Holsbeke, C.; Savelli, L.; Fruscio, R.; Lissoni, A.A.; et al. Simple ultrasound rules to distinguish between benign and malignant adnexal masses before surgery: prospective validation by IOTA group. BMJ 2010, 341, c6839. [Google Scholar] [CrossRef]
- Tan, P.L.; Willatt, J.M.; Lindsell, D. The ability of ultrasound to detect gynaecological neoplasms and their ultrasound morphological features. Australas Radiol 2007, 51, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Kurjak, A.; Prka, M.; Arenas, J.M.; Sparac, V.; Merce, L.T.; Corusic, A.; Ivancic-Kosuta, M. Three-dimensional ultrasonography and power Doppler in ovarian cancer screening of asymptomatic peri- and postmenopausal women. Croat Med J 2005, 46, 757–764. [Google Scholar] [PubMed]
- Timor-Tritsch, I.E.; Goldstein, S.R. The complexity of a "complex mass" and the simplicity of a "simple cyst". J Ultrasound Med 2005, 24, 255–258. [Google Scholar] [CrossRef] [PubMed]
- Van Calster, B.; Timmerman, D.; Valentin, L.; McIndoe, A.; Ghaem-Maghami, S.; Testa, A.C.; Vergote, I.; Bourne, T. Triaging women with ovarian masses for surgery: observational diagnostic study to compare RCOG guidelines with an International Ovarian Tumour Analysis (IOTA) group protocol. BJOG 2012, 119, 662–671. [Google Scholar] [CrossRef]
- Kaijser, J.; Bourne, T.; Valentin, L.; Sayasneh, A.; Van Holsbeke, C.; Vergote, I.; Testa, A.C.; Franchi, D.; Van Calster, B.; Timmerman, D. Improving strategies for diagnosing ovarian cancer: a summary of the International Ovarian Tumor Analysis (IOTA) studies. Ultrasound Obstet Gynecol 2013, 41, 9–20. [Google Scholar] [CrossRef]
- Van Calster, B.; Van Hoorde, K.; Valentin, L.; Testa, A.C.; Fischerova, D.; Van Holsbeke, C.; Savelli, L.; Franchi, D.; Epstein, E.; Kaijser, J.; et al. Evaluating the risk of ovarian cancer before surgery using the ADNEX model to differentiate between benign, borderline, early and advanced stage invasive, and secondary metastatic tumours: prospective multicentre diagnostic study. BMJ 2014, 349, g5920. [Google Scholar] [CrossRef]
- Sayasneh, A.; Ferrara, L.; De Cock, B.; Saso, S.; Al-Memar, M.; Johnson, S.; Kaijser, J.; Carvalho, J.; Husicka, R.; Smith, A.; et al. Evaluating the risk of ovarian cancer before surgery using the ADNEX model: a multicentre external validation study. Br J Cancer 2016, 115, 542–548. [Google Scholar] [CrossRef]
- Meys, E.M.J.; Jeelof, L.S.; Achten, N.M.J.; Slangen, B.F.M.; Lambrechts, S.; Kruitwagen, R.; Van Gorp, T. Estimating risk of malignancy in adnexal masses: external validation of the ADNEX model and comparison with other frequently used ultrasound methods. Ultrasound Obstet Gynecol 2017, 49, 784–792. [Google Scholar] [CrossRef]
- Padilla, L.A.; Radosevich, D.M.; Milad, M.P. Accuracy of the pelvic examination in detecting adnexal masses. Obstet Gynecol 2000, 96, 593–598. [Google Scholar] [CrossRef]
- Hartge, P.; Hayes, R.; Reding, D.; Sherman, M.E.; Prorok, P.; Schiffman, M.; Buys, S. Complex ovarian cysts in postmenopausal women are not associated with ovarian cancer risk factors: preliminary data from the prostate, lung, colon, and ovarian cancer screening trial. Am J Obstet Gynecol 2000, 183, 1232–1237. [Google Scholar] [CrossRef]
- Bailey, C.L.; Ueland, F.R.; Land, G.L.; DePriest, P.D.; Gallion, H.H.; Kryscio, R.J.; van Nagell, J.R., Jr. The malignant potential of small cystic ovarian tumors in women over 50 years of age. Gynecol Oncol 1998, 69, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Curtin, J.P. Management of the adnexal mass. Gynecol Oncol 1994, 55, S42–46. [Google Scholar] [CrossRef] [PubMed]
- Reimer, T.; Gerber, B.; Muller, H.; Jeschke, U.; Krause, A.; Friese, K. Differential diagnosis of peri- and postmenopausal ovarian cysts. Maturitas 1999, 31, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Owens, O.J.; Stewart, C.; Leake, R.E.; McNicol, A.M. A comparison of biochemical and immunohistochemical assessment of EGFR expression in ovarian cancer. Anticancer Res 1992, 12, 1455–1458. [Google Scholar]
- Scambia, G.; Benedetti-Panici, P.; Ferrandina, G.; Distefano, M.; Salerno, G.; Romanini, M.E.; Fagotti, A.; Mancuso, S. Epidermal growth factor, oestrogen and progesterone receptor expression in primary ovarian cancer: correlation with clinical outcome and response to chemotherapy. Br J Cancer 1995, 72, 361–366. [Google Scholar] [CrossRef]
- Koonings, P.P.; Campbell, K.; Mishell, D.R., Jr.; Grimes, D.A. Relative frequency of primary ovarian neoplasms: a 10-year review. Obstet Gynecol 1989, 74, 921–926. [Google Scholar] [CrossRef]
- Modesitt, S.C.; Pavlik, E.J.; Ueland, F.R.; DePriest, P.D.; Kryscio, R.J.; van Nagell, J.R., Jr. Risk of malignancy in unilocular ovarian cystic tumors less than 10 centimeters in diameter. Obstet Gynecol 2003, 102, 594–599. [Google Scholar] [CrossRef]
- Osmers, R.G.; Osmers, M.; von Maydell, B.; Wagner, B.; Kuhn, W. Evaluation of ovarian tumors in postmenopausal women by transvaginal sonography. Eur J Obstet Gynecol Reprod Biol 1998, 77, 81–88. [Google Scholar] [CrossRef]
- Auslender, R.; Atlas, I.; Lissak, A.; Bornstein, J.; Atad, J.; Abramovici, H. Follow-up of small, postmenopausal ovarian cysts using vaginal ultrasound and CA-125 antigen. J Clin Ultrasound 1996, 24, 175–178. [Google Scholar] [CrossRef]
- Di Legge, A.; Testa, A.C.; Ameye, L.; Van Calster, B.; Lissoni, A.A.; Leone, F.P.; Savelli, L.; Franchi, D.; Czekierdowski, A.; Trio, D.; et al. Lesion size affects diagnostic performance of IOTA logistic regression models, IOTA simple rules and risk of malignancy index in discriminating between benign and malignant adnexal masses. Ultrasound Obstet Gynecol 2012, 40, 345–354. [Google Scholar] [CrossRef]
- Landolfo, C.; Bourne, T.; Froyman, W.; Van Calster, B.; Ceusters, J.; Testa, A.C.; Wynants, L.; Sladkevicius, P.; Van Holsbeke, C.; Domali, E.; et al. Benign descriptors and ADNEX in two-step strategy to estimate risk of malignancy in ovarian tumors: retrospective validation in IOTA5 multicenter cohort. Ultrasound Obstet Gynecol 2023, 61, 231–242. [Google Scholar] [CrossRef] [PubMed]
- Osmers, R.G.; Osmers, M.; von Maydell, B.; Wagner, B.; Kuhn, W. Preoperative evaluation of ovarian tumors in the premenopause by transvaginosonography. Am J Obstet Gynecol 1996, 175, 428–434. [Google Scholar] [CrossRef] [PubMed]
- Liu, Y.N.; Tan, X.; Xiong, W.; Dong, X.; Liu, J.; Wang, Z.L.; Chen, H.X. Natural history and malignant potential of simple ovarian cysts in postmenopausal women: a systematic review and meta-analysis. Menopause 2023. [Google Scholar] [CrossRef] [PubMed]
- Bast, R.C., Jr.; Klug, T.L.; St John, E.; Jenison, E.; Niloff, J.M.; Lazarus, H.; Berkowitz, R.S.; Leavitt, T.; Griffiths, C.T.; Parker, L.; et al. A radioimmunoassay using a monoclonal antibody to monitor the course of epithelial ovarian cancer. N Engl J Med 1983, 309, 883–887. [Google Scholar] [CrossRef]
- Jacobs, I.; Bast, R.C., Jr. The CA 125 tumour-associated antigen: a review of the literature. Hum Reprod 1989, 4, 1–12. [Google Scholar] [CrossRef]
- Jacobs, I.; Oram, D.; Fairbanks, J.; Turner, J.; Frost, C.; Grudzinskas, J.G. A risk of malignancy index incorporating CA 125, ultrasound and menopausal status for the accurate preoperative diagnosis of ovarian cancer. Br J Obstet Gynaecol 1990, 97, 922–929. [Google Scholar] [CrossRef]
- Conway, C.; Zalud, I.; Dilena, M.; Maulik, D.; Schulman, H.; Haley, J.; Simonelli, K. Simple cyst in the postmenopausal patient: detection and management. J Ultrasound Med 1998, 17, 369–372. [Google Scholar] [CrossRef]
- Timmerman, D.; Moerman, P.; Vergote, I. Meigs' syndrome with elevated serum CA 125 levels: two case reports and review of the literature. Gynecol Oncol 1995, 59, 405–408. [Google Scholar] [CrossRef]
- Kaijser, J.; Van Gorp, T.; Smet, M.E.; Van Holsbeke, C.; Sayasneh, A.; Epstein, E.; Bourne, T.; Vergote, I.; Van Calster, B.; Timmerman, D. Are serum HE4 or ROMA scores useful to experienced examiners for improving characterization of adnexal masses after transvaginal ultrasonography? Ultrasound Obstet Gynecol 2014, 43, 89–97. [Google Scholar] [CrossRef]
- Montagnana, M.; Danese, E.; Ruzzenente, O.; Bresciani, V.; Nuzzo, T.; Gelati, M.; Salvagno, G.L.; Franchi, M.; Lippi, G.; Guidi, G.C. The ROMA (Risk of Ovarian Malignancy Algorithm) for estimating the risk of epithelial ovarian cancer in women presenting with pelvic mass: is it really useful? Clin Chem Lab Med 2011, 49, 521–525. [Google Scholar] [CrossRef]
- Kaijser, J.; Van Gorp, T.; Van Hoorde, K.; Van Holsbeke, C.; Sayasneh, A.; Vergote, I.; Bourne, T.; Timmerman, D.; Van Calster, B. A comparison between an ultrasound based prediction model (LR2) and the risk of ovarian malignancy algorithm (ROMA) to assess the risk of malignancy in women with an adnexal mass. Gynecol Oncol 2013, 129, 377–383. [Google Scholar] [CrossRef] [PubMed]
- Valentin, L.; Jurkovic, D.; Van Calster, B.; Testa, A.; Van Holsbeke, C.; Bourne, T.; Vergote, I.; Van Huffel, S.; Timmerman, D. Adding a single CA 125 measurement to ultrasound imaging performed by an experienced examiner does not improve preoperative discrimination between benign and malignant adnexal masses. Ultrasound Obstet Gynecol 2009, 34, 345–354. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Correlation between tumor size and histological finding: (a) Perimenopausal (PEM) patients, (b) Postmenopausal (POM) patients.
Figure 1.
Correlation between tumor size and histological finding: (a) Perimenopausal (PEM) patients, (b) Postmenopausal (POM) patients.
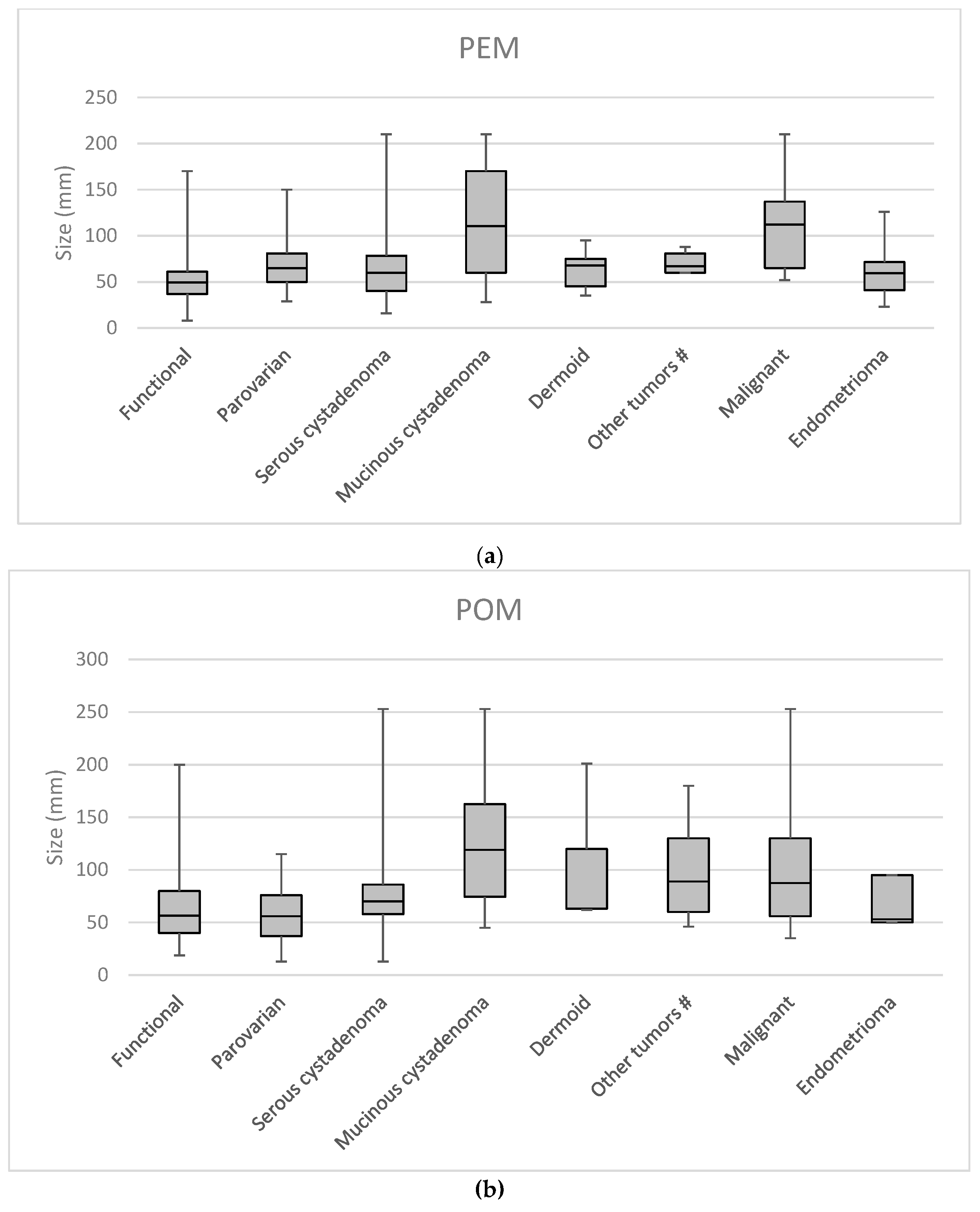
Figure 2.
Link between dignity and the largest diameter of adnexal masses according to menopausal status: Perimenopausal (PEM) malignant tumors are significantly larger than benign masses; No significant difference can be observed in the size of postmenopausal (POM) benign and malignant lesions.
Figure 2.
Link between dignity and the largest diameter of adnexal masses according to menopausal status: Perimenopausal (PEM) malignant tumors are significantly larger than benign masses; No significant difference can be observed in the size of postmenopausal (POM) benign and malignant lesions.
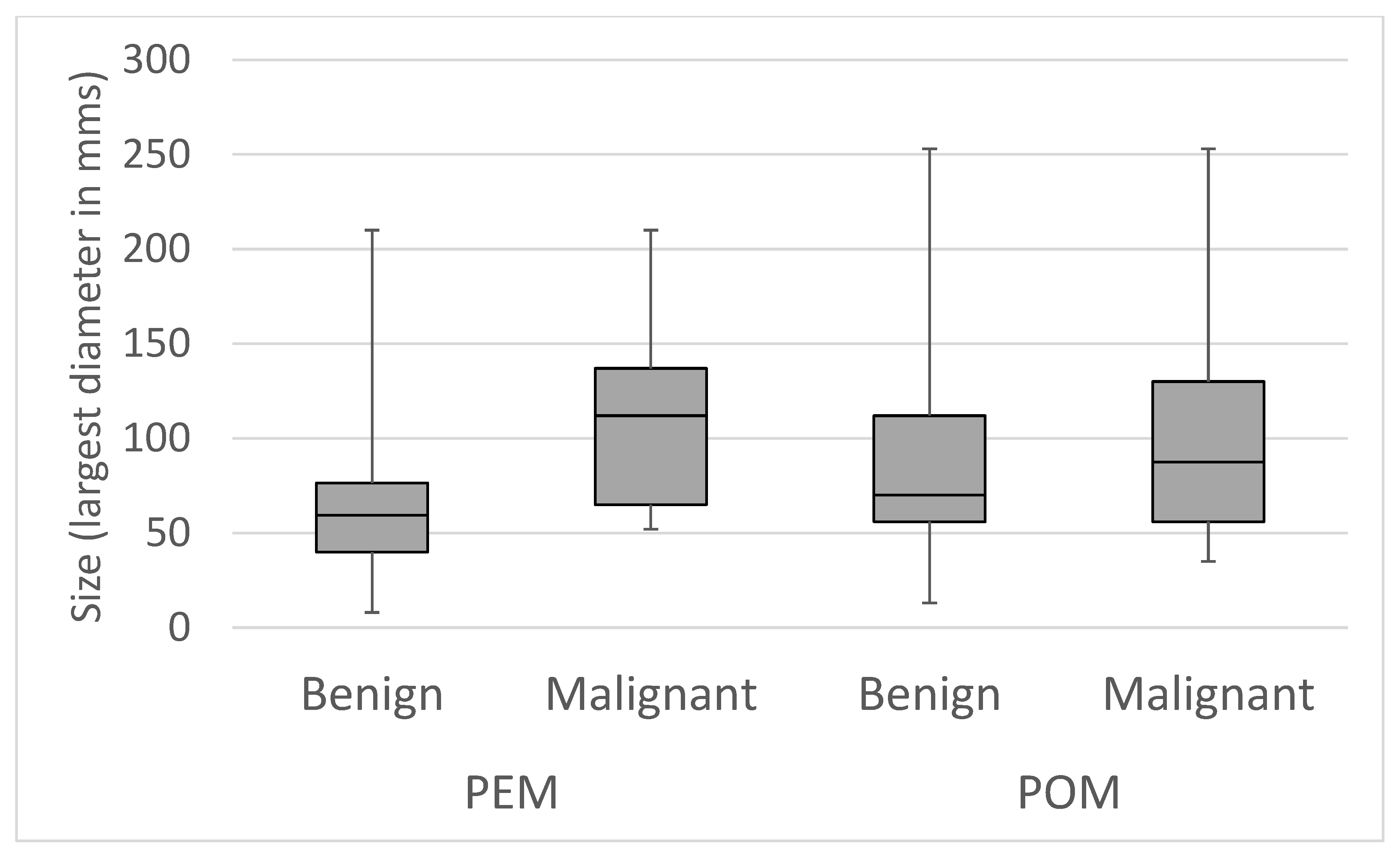
Figure 3.
Correlation between tumor size and patients complaints. (a) Perimenopausal (PEM) patients complaints and their correlation to tumor size (b) Postmenopausal (POM) patients complaints and its correlation to tumor size.
Figure 3.
Correlation between tumor size and patients complaints. (a) Perimenopausal (PEM) patients complaints and their correlation to tumor size (b) Postmenopausal (POM) patients complaints and its correlation to tumor size.
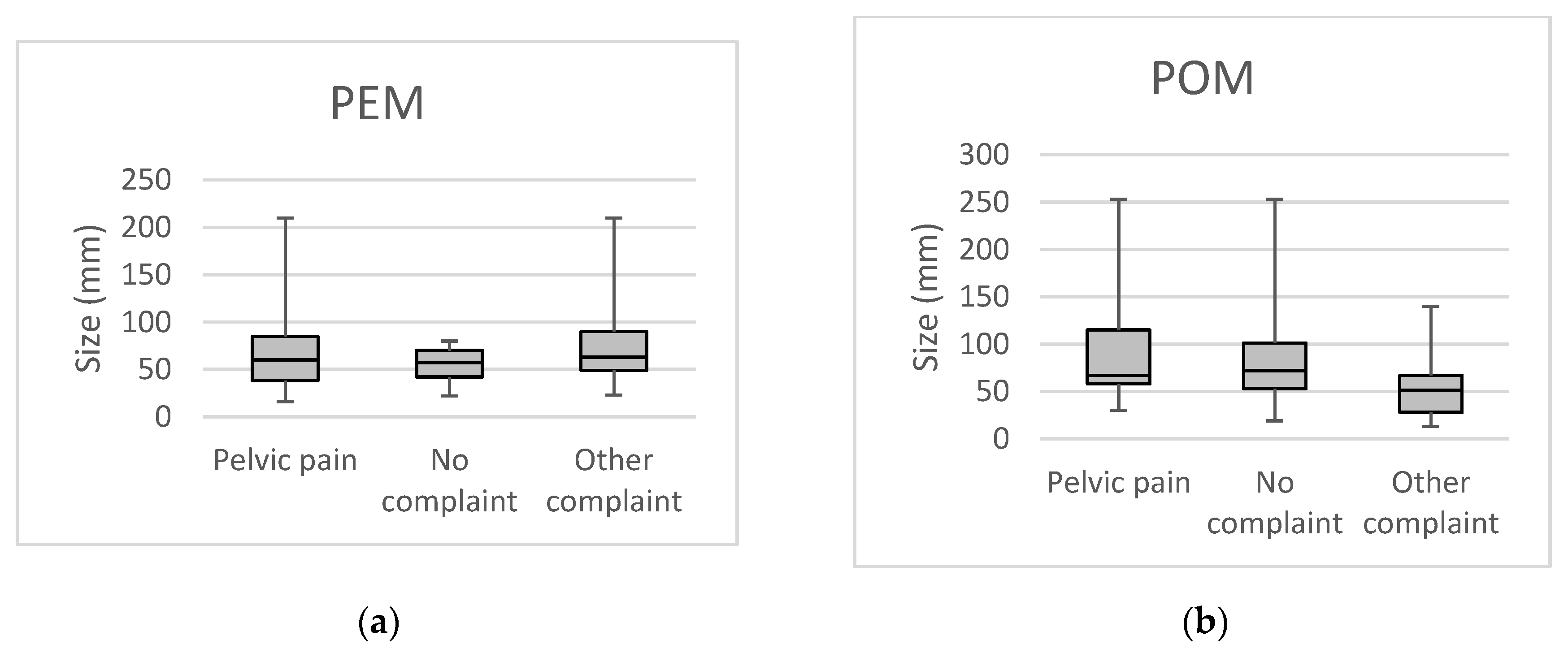

Table 1.
Correlation between cyst size, ultrasound morphology and histology. N=379 (100%).
| PEM simplex | PEM complex | POM simplex | POM complex | |||||
|---|---|---|---|---|---|---|---|---|
| <5cm | ≥5cm | <5cm | ≥5cm | <5cm | ≥5cm | <5cm | ≥5cm | |
| Functional cysts | ||||||||
| Corp. lut. cyst. hem.* | 8 (25.00%) |
5 (12.20%) |
6 (20.69%) |
12 (12.90%) |
2 (13.33%) |
5 (4.17%) |
||
| Follicular cyst | 5 (15.63%) |
6 (14.63%) |
6 (20.69%) |
2 (2.15%) | 1 (11.11%) |
2 (1.67%) |
||
| Parovarian cysts | 1 (3.13%) |
11 (26.83%) |
3 (10.34%) |
3 (3.23%) |
2 (22.22%) |
5 (12.50%) |
3 (20.00%) |
5 (4.17%) |
| Benign | ||||||||
| Cystadenoma serosum | 16 (50.00%) |
16 (39.02%) |
3 (10.34%) |
21 (22.58%) |
5 (55.56%) |
27 (67.50%) |
4 (26.67%) |
34 (28.33%) |
| Cystadenoma mucinosum | 1 (3.13%) |
2 (4.88%) |
1 (3.45%) |
10 (10.75%) |
4 (10.00%) |
2 (13.33%) |
18 (15.00%) |
|
| Dermoid | 4 (13.79%) |
10 (10.75%) |
5 (4.17%) |
|||||
| Endometriosis | 1 (3.13%) |
1 (2.44%) |
6 (20.69%) |
12 (12.90%) |
3 (2.50%) |
|||
| Fibroid | 3 (3.23%) |
2 (5.00%) |
1 (6.67%) |
7 (5.83%) |
||||
| Hydrosalpinx | 1 (11.11%) |
1 (2.50%) |
2 (1.67%) |
|||||
| Struma ovarii | 1 (1.08%) |
1 (0.83%) |
||||||
| Brenner tu. | 3 (3.23%) |
2 (1.67%) |
||||||
| Malignant | 16 (17.20%) |
1 (2.50%) |
3 (20.00%) |
36 (30.00%) |
||||
Table 2.
Risk factors affecting the formation of ovarian cysts.
| Risk factors | PEM simplex | PEM complex | POM simplex | POM complex | Total (% of total cases) |
||||
|---|---|---|---|---|---|---|---|---|---|
| <5cm | ≥5cm | <5cm | ≥5cm | <5cm | ≥5cm | <5cm | ≥5cm | ||
| Parity | |||||||||
| Nulliparous | 2 (6%) |
10 (24%) |
6 (21%) |
14 (15%) |
1 (11%) |
1 (3%) |
3 (20%) |
20 (17%) |
57 (15.04%) |
| 1-2 children | 20 (63%) |
23 (56%) |
19 (66%) |
65 (70%) |
6 (67%) |
31 (78%) |
8 (53%) |
78 (65%) |
250 (65.96%) |
| 3-4 children | 10 (31%) |
8 (20%) |
3 (10%) |
13 (14%) |
2 (22%) |
7 (18%) |
4 (27%) |
20 (17%) |
67 (17.68%) |
| ≥5 children | 1 (3%) |
1 (1%) |
1 (3%) |
2 (2%) |
5 (1.32%) |
||||
| Family history of ovarian cancer | 2 (6%) |
1 (3%) |
1 (1%) |
4 (1.06%) |
|||||
| Previous pelvic surgery | |||||||||
| Hysterectomy | 5 (16%) |
4 (10%) |
3 (10%) |
17 (18%) |
3 (33%) |
2 (5%) |
4 (27%) |
33 (28%) |
71 (18.73%) |
| Adnexectomy | 1 (3%) |
1 (2%) |
1 (3%) |
8 (9%) |
1 (7%) |
2 (2%) |
14 (3.69%) |
||
| Laparotomy | 1 (3%) |
4 (10%) |
1 (3%) |
10 (11%) |
1 (3%) |
5 (4%) |
22 (5.80%) |
||
| Punction | 3 (7%) |
1 (3%) |
1 (1%) |
1 (3%) |
1 (7%) |
7 (1.85%) |
|||
| No previous surgery | 25 (78%) |
29 (71%) |
23 (79%) |
57 (61%) |
6 (67%) |
36 (90%) |
9 (60%) |
80 (67%) |
265 (69.92%) |
| Total (n) | 32 | 41 | 29 | 93 | 9 | 40 | 15 | 120 | 379 (100%) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



