
Submitted:
28 February 2025
Posted:
03 March 2025
You are already at the latest version
Abstract
Urolithiasis is one of the most burdensome urinary tract conditions with a prevalence ranging from 1% to 20%. Approximately half of the patients experience a recurrence, while 10% face multiple stone episodes. Long before the advent of surgical treatment options, herbal therapy, or phytotherapy, had been used for both the prevention and management of urolithiasis. Recently, interest in phytotherapy has been rekindled due to the limitations associated with modern urolithiasis treatment, the limited options for conventional medical therapy and the added cost of interventions for stones. While research on phytotherapy is still limited, it is ongoing and is yielding promising results. In order to capture the current trend in phytotherapy for urolithiasis we performed a narrative review from data collected and synthesized from electronic databases, with a specific focus on randomized human studies. Our analysis revealed that the use of various herbal medicines and phytotherapy, either as mixtures or as sole plant extracts, in urolithiasis is on the rise and is mainly utilized as complementary therapy to conventional treatment. Although most studies demonstrate the effectiveness of phytotherapy in reducing stone size and facilitating stone expulsion, several questions regarding specific dosages, mechanisms of action, drug interactions, treatment duration, and types of stones that respond to phytotherapy remain unanswered. This review aims to summarize the current knowledge surrounding the role of phytotherapy in urolithiasis, as well as to determine its role as a primary or complementary treatment alongside traditional treatment options. Ultimately, further research is essential to clarify the abovementioned unresolved issues, overcome the existing challenges, and optimize the best possible phytotherapy strategies and optimal timing for dissolving specific types of stones with these regimens.
Keywords:
Herbal medicines
; Phytotherapy
; Kidney stones
; Urinary calculi
; Urolithiasis
1. Introduction
Urolithiasis, also known as urinary stone disease, is the presence of stones in the lower (bladder, urethra) or upper (kidneys, ureter) urinary tract. According to extensive epidemiological studies, the prevalence of urolithiasis in the general population in economically developed countries ranges from 1% to 20% [1]. The prevalence of urolithiasis varies according to geographical area and is related to sex, age, diet, and climate factors [2]. One in two stone formers will have at least another stone episode during their lifetime, while 10% of patients will suffer multiple stone episodes [3,4]. Nearly half of the stone-formers will have another episode within ten years [5]. Diet plays an important role in urolithiasis, with those following a plant-based diet presenting with lower risk of stone formation [6]. Modification of diet can help reduce stone recurrence rates, especially for patients who would have undergone a metabolic stone work-up [7].
Urinary stone disease is the third most common pathological condition affecting the urinary tract, after urinary tract infections and prostate conditions [8]. The size, site, and number (single or multiple) of stone(s), distinct urinary system anatomy, comorbidities, age, and individual performance status are essential for treatment planning [9]. Urolithiasis is a disorder with significant socioeconomic implications, influencing the quality of life. Urinary stones are a recurrent disorder of multifactorial origin, all of which need to be assessed, and their understanding should be used to influence management [10]. A schematic presentation of the most common causes and predisposing risk factors of urolithiasis is depicted in Figure 1.
The treatment of urolithiasis is a matter of socioeconomic concern. Medical Expulsive Therapy (MET), Shockwave Lithotripsy (SWL), Ureteroscopy (URS), Retrograde Intrarenal Surgery (RIRS), and Percutaneous Nephrolithotomy (PCNL) are the available options depending on stone size and location, stone burden, comorbidities and patient preferences [11]. Stone factors, anatomy, patient factors, and the surgeon’s preference determine the optimal treatment selection [12]. There has been a shift in the management of urinary stone disease from inpatient to outpatient setting, and hospitalization time has decreased due to minimally invasive treatment modalities; costs, however, continue to rise, likely due to the increasing prevalence of urinary stone disease [13,14]. Treatment of urolithiasis remains a challenge for conventional medicine. Figure 2 shows an overview of the available treatment options for urolithiasis.
Phytotherapy has been used since time immemorial in traditional practices and has gained traction lately, mainly due to the limitations of conventional medical therapy [15]. The mechanisms of action for certain herbal supplements have yet to be fully elucidated [16]. Current evidence suggests multiple ways of actions including but not limited to increasing diuresis, enhancing citraturia, decreasing calcinuria and oxaluria, inhibiting of nucleation and aggregation of crystals, stone dissolution, and elevating the glycosaminoglycan level [17,18,19]. There is evidence supporting the use of phytotherapy in urolithiasis and UTI management as alternative or adjunct therapy [20,21,22,23]. Some studies have shown that there is also evidence that plant flavonoids inhibit stone formation both in vitro and in vivo [24]. There are many phytotherapy/food supplement products that renal lithiasis patients use over the counter. However, there are limited clinical studies on manufacturers’ claims and limited information on side effect profiles despite the high rating by some patients [25,26]. To date, the effects of these food supplements or phytotherapy are still unknown or understudied in humans; the unavailability of evidence must not be taken to imply the absence of potential harm [27].
This review aims to explore the role of phytotherapy in urolithiasis and identify gaps in knowledge relevant to using such compounds to prevent recurrent episodes and diminish stone formation. The ultimate goal is to increase awareness among urologists and better prepare future urologists treating de novo or recurrent stone formers.
2. Materials and Methods
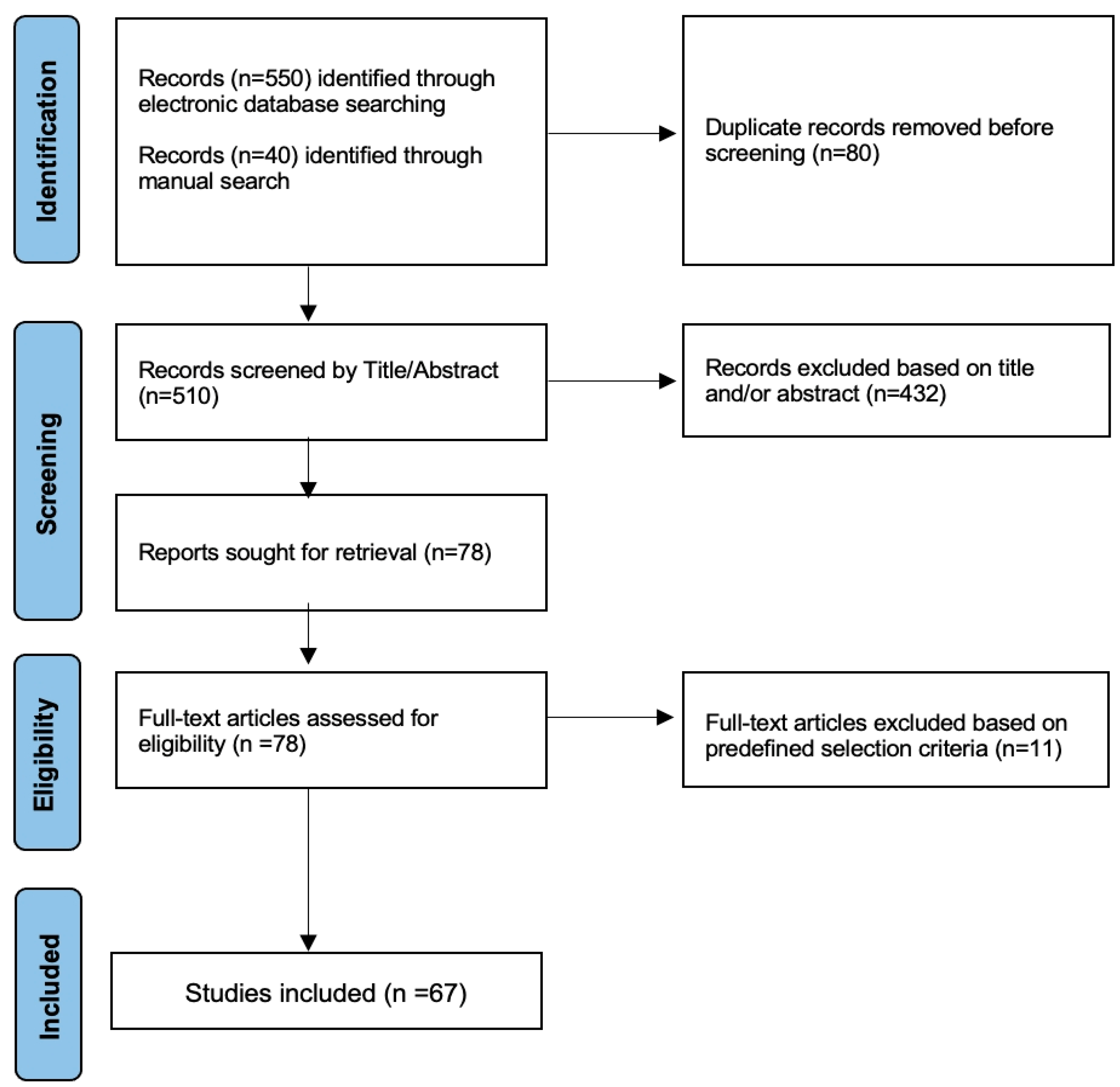
The electronic databases of PubMed and Scopus were searched for English-written articles on phytotherapy and herbal remedies in urolithiasis published from inception through November 2024. The keywords used were “urolithiasis,” “stone disease,” “herbal,” and “phytotherapy.” These search terms were combined with Boolean operators (AND, OR) to refine the search better. One author (WFM) performed the initial search, which resulted in the retrieval of 550 articles. Subsequently, the references of the studies were screened to identify additional articles, thereby expanding the collected data by 40 articles. Following duplicate removal, 510 articles were scrutinized based on their title and abstracts. The search was performed iteratively throughout the review process to capture up-to-date information. Articles of any design, except for case reports, questionnaires, comments, and editorials, were evaluated, and those eligible underwent full-text screening. Special emphasis was placed on research that reports findings from randomized controlled trials, particularly those published within the last two decades. In addition, studies reporting on animals, irrelevant topics or outdated content, outside the treatment scope, or not reporting the use of phytotherapy for urolithiasis were unanimously excluded. In cases of ambiguity, a second author (ENS) followed the same search strategy and reviewed the relevance of the selected manuscripts. Ultimately, a total of 67 articles were included in the final analysis. The search strategy is highlighted through a flow diagram in Figure 3.
3. Phytotherapy: Current evidence from clinical trials
A randomized, controlled, open-label pilot study comparing the efficacy of Celosia argentea (Cock’s Comb) seeds (titled Sitivaraka) with potassium citrate was done. An ultrasound scan was used to determine Sitivaraka’s effects on 44 participants with an average stone size of 8mm. Twenty-one participants received Sitivaraka thrice daily, while the 23 participants in the control group received potassium citrate for six months. The Sitivaraka group showed a decrease in Parathyroid Hormone (PTH) and a reduction in stone size at 3 and 6 months, while the potassium citrate group did not have significant reductions. The results, despite being on a small sample, showed the effectiveness of Cock’s Comb seeds on urinary stones compared to potassium citrate after a six months treatment [28].
Phyllanthus niruri (Chanca Piedra), or “stone breaker,” is a tropical herb growing in tropical and subtropical areas like the rainforests of South America. Its tea has been used to treat many ailments, including urinary stone disease, in countries like Brazil [29]. A study was done investigating the effect of P. niruri on the urinary metabolic parameters of 56 patients with kidney stones <10mm. No significant anthropometric and serum measurements were noticed in the results. Still, there was an increase in urinary potassium, magnesium/creatinine ratio, and potassium/creatinine ratio accompanied by a decrease in stone size. Urinary oxalate was reduced in a group of patients with hyperoxaluria, while uric acid decreased in patients with hyperuricosuria. These results demonstrate the safety and effectiveness of “stone breaker” in the elimination of urinary stones and reduction in stone size [30]. A review suggested the need for RCTs to determine the therapeutic properties of P. niruri, but the preventive effect in stone formation or elimination was elucidated [31]. In a comprehensive review of the literature, Phyllanthus niruri was shown to interfere with calcium oxalate crystallization while at the same time reducing hyperoxaluria and hyperuricosuria [32].
In another single-arm study, 48 participants were recruited to take 225mg capsules of P. niruri dried leaf extract mixed with 152 mg magnesium stearate and 2 mg pyridoxine hydrochloride (vitamin B6) for three months. A non-contrast CT scan was used to determine stone parameters before and after intervention, and recruited participants had a maximum stone diameter of 15mm before intervention in this study. Less than 3mm of upper and mid-calyx stones were expelled, and 3-4mm stones reduced in size, but the bigger stones were not affected. The study recommended a prolonged treatment duration to increase the intervention's effectiveness [33]. A systematic review and meta-analysis on P. niruri showed limited clinical evidence supporting its efficacy in stone size reduction [34].
Black seed (Nigella sativa) has been a Middle Eastern medicinal herb since time immemorial and has been considered effective in treating kidney stones when mixed with honey and water. Black seed’s effects on stones were investigated in a randomized, double-blind, placebo-controlled clinical trial involving 60 participants, 30 in each group. The participants had at least a 5mm stone, and they took two tablets of 500mg encapsulated black seed powder daily for ten weeks in the interventional group and two tablets of placebo in the control group. The results, assessed by a pre- and post-intervention ultrasound scan, showed a 44.4% stone expulsion and 51.8% stone reduction compared to a 15.3 % expulsion and 11.5% size reduction in the control group. Of note in the results is a 15.3 % increase in stone size in the control group, signifying Black seed's effectiveness on urinary stone treatment. [35]
Jalal et al. investigated the antiurolithic effects of Phaseolus vulgaris, the common beans grown and eaten worldwide in their RCT, placebo-controlled, involving 60 patients with stones less than or equal to 10mm. Urinary volume and potassium significantly increased after 6 weeks of treatment in the intervention group, and urinary calcium, oxalate, and uric acid significantly decreased compared to the placebo group, while there was a slight increase in urine pH and magnesium. A significant decrease in the number of stones and reduction in stone sizes on ultrasound scan in the treatment group was seen compared to the placebo arm, indicating the effectiveness of common beans on stone treatment [36].
Erickson et al. investigated the effects of Cystone® tablets on urinary composition and stone formation in a year-long study. Cystone® tablets are one of the traditional Indian Ayurvedic treatments for stones. It was investigated in a first-phase randomized double-blinded 12-week cross-over study for its alterations in urinary supersaturation (6 weeks), and there was no statistically significant effect of Cystone® on urinary composition. The open-label, one-year’s duration second phase aimed to determine the effectiveness on stone burden using a CT scan. Again, no statistically significant effect was recorded, leading to the study deduction not supporting the efficacy of Cystone® on renal stones [37]. The study was limited by its very small sample size, as it included ten patients, all of which were also recurrent stone formers [38].
Differently, an open-label study on 65 patients with stones between 5 - 12mm taking Cystone forte two tablets twice a day for three months showed significant stone expulsion, reduction in stone size, and general amelioration of clinical symptoms. This study concluded that Cystone is safe and effective in managing renal stones [39]. Another prospective randomized placebo-controlled study by Patki et al concluded that Cystone® effectively managed ureteric stones by reducing stone size, improving passage rate, and reducing pain [40]. A systemic review that cited 2 RCTs [41,42] deducted that Cystone® was effective compared to placebo in lowering renal stone size and stone clearance rates [43].
Wu-Ling-San (WLS) formula is a traditional Chinese medicine for pain and urinary stone disease [44]. WLS formula is a mixture made up of the following five herbs: Rhizoma alismatis, Poria cocos Wolf, Polyporus umbellatus Fries, Rhizoma Atractylodis Macrocephalae, and Ramulus Cinnamomi Cassiae mixed in a weight ratio of 4:3:3:3:2 respectively. In a 1-month’s duration RCT of 28 recurrent stone formers with proven calcium oxalate urinary stones, half taking 2g WLS three times a day and the other half taking placebo three times a day, the 24-hr urine output, which was used as a measure, increased in the treatment group compared to placebo. WLS was proven to be safe and to increase urine output [45]. On the contrary, in a study investigating the clinical efficacy of WLS for the prevention of recurrent nephrolithiasis, its long-term use did not have a preventive effect on the need for urolithiasis surgical treatment [44]. These two studies did not confirm the effectiveness of WLS.
Mujumdar et al. investigated the safety and efficacy of Subap in a 28-week, randomized, double-blind, placebo-controlled study. Subap is an herbal formulation by mixing the dried stem bark of C. nurvala Buch-ham, the stem and roots of Musa x paradisiaca Linn, the whole plant of A. aspera Linn, and the seeds of H. vulgare Linn. Asymptomatic patients with stone size between 4 to 9mm were enrolled, and the treatment group received Subap, which was compared to placebo. Results showed statistically significant increased stone expulsion rate, reduced stone density, and reduced stone surface area for the treatment group compared to placebo [46].
The antiurolithiasic effects of another mixture of five plant extracts, Tribulus Terrestris, Urtica dioica, Adiantum capillus-veneris, Stigma maydis (corn silk), and Cucumis melo were investigated in a randomized, single-blinded, placebo-controlled clinical trial. It involved 54 participants (with renal stones less than or equal to 10mm), 27 in the intervention and 27 in the placebo arms, respectively. The intervention group took standard treatment and 60 drops thrice daily for one month, and the control group took standard treatment plus placebo. An ultrasound scan was used to evaluated stone parameters in this study. The result showed significant stone expulsion and stone size reduction in the intervention group, and on the other parameters, only urine volume significantly differed [47]. The study concluded that the five-herb mixture is more effective in managing urinary lithiasis than the placebo.
Brardi et al. in a prospective randomized comparison study investigated the effects of the combination of potassium citrate and Agropyron repens in renal stone treatment comparing it with potassium citrate alone. In an unblinded study, 50 participants were divided into two arms, the first 25 taking potassium citrate plus Agropyron repens combination and the other arm of 25 participants taking only potassium citrate. Both arms were advised to take the same diet and increased fluid intake in a 5-month follow-up period. There was a significant reduction in the total number of stones, stone diameter, and reduction of excreted uric acid in the combination arm compared to the potassium citrate-only group without a significant difference in citraturia, oxaluria, urinary calcium, and urinary pH. This study concluded that using the combination of couch grass and potassium citrate is safe and effective compared to potassium citrate alone to treat urinary stones [48].
Kristyantoro et al. investigated the effectiveness of Renalof® supplement, comparing it to Kalkurenal and placebo. Thirty patients with renal stones up to 2cm measured by plain X-ray and Ultrasound Scans were recruited and divided into three arms; 9 took a placebo, 8 took kalkurenal, and 13 were on Renalof®. After a month of intervention, the result showed a statistically insignificant decrease in all patients' 24-hour urine excretion of calcium and uric acid. Still, there was also a significant decrease in stone parameters in the Renalof® arm. The study concluded that Renalof® can be safely used as an adjunct treatment in urolithiasis [49].
Extracts from Agropyron repens (Elymnus repens, Elytrigia repens, quack grass, couch grass), a worldwide infesting rhizomatous plant native to Europe and Central Asia [50], are the main constituents of Renalof® supplement along with mannitol, and magnesium [51]. A double-blind, randomized, placebo-controlled, parallel-group phase III clinical trial was conducted to evaluate the safety and effectiveness of Renalof® in the dissolution and expulsion of calcium-containing renal stones less than 10mm in diameter. Renalof® was taken as one tablet three times daily for three months in the treatment group with 52 patients, and the control arm had 58 patients taking a placebo 3 times daily. After three months, there was a 7.7% stone reduction and 86.5% stone expulsion in the Renalof® group compared to a 0% stone reduction in the placebo arm. This study concluded that Renalof® is safe and effective in stone size reduction and expulsion [52]. Likewise, a phase II randomized, prospective, observational, single-blind study of 155 patients with urinary stones less than 10 mm that enrolled 120 patients in the treatment arm taking Renalof® 325mg twice daily for three months and 35 patients on placebo showed the safety and effectiveness of Renalof®. There was a 65% expulsion in the Renalof® group compared to 11.4% in the placebo arm, a result in favour of Renalof® [51].
Notably, a recent study pointed toward the safety, efficacy, and tolerability of a 3-component herbal compound in a paediatric population with small stone fragments after endourological treatment. Patients were randomly divided into two groups and were followed up for 3 months. The drug proved an efficient ancillary treatment to prevent new stone growth and reduce residual fragments [53].
Renalof® was evaluated in a recent placebo-controlled RCT that included 82 patients with predominantly calcium oxalate stones (Hounsfield units>500) randomized to Renalof and placebo. Stone volume, surface and location were evaluated by CT and analyzed using a dedicated computer software (Invesalius) both before and after the 3-month intervention period. From the 73 patients that were available for analysis (9 patients had passed their stones during the study period) patients in the Renalof group had a statistically significant (approximately 25%) reduction is stone surface and stone volume at 3 months [54]. The study’s strong point was the use of a software to accurately measure stone surface and volume instead of maximum stone diameter.

Table 1.
Brief summary of studies reporting on the use of phytotherapeutic regimens for urolithiasis. RCT: Randomized-controlled trial, US: Ultrasound, CT: Computed Tomography, NCCT: Non-contrast Computed Tomography, vs: versus, NS: not stated *: weeks, †: recurrent stone formers.
Table 1.
Brief summary of studies reporting on the use of phytotherapeutic regimens for urolithiasis. RCT: Randomized-controlled trial, US: Ultrasound, CT: Computed Tomography, NCCT: Non-contrast Computed Tomography, vs: versus, NS: not stated *: weeks, †: recurrent stone formers.
| Authors, year | Study Type | Regimen | Stone size (mm) | Imaging modality | Recruited/Randomised | Maximum period (months) |
Findings |
|---|---|---|---|---|---|---|---|
| Singh et al., 2011 [28] | RCT | Sitivaraka Vs Potassium Citrare | ≥8mm | US | 21/ 23 | 6 | -Stone size reduction |
| Pucci et al., 2018 [30] | RCT |
Phyllanthus Niruri (Stone breaker) |
<10mm | USCT | 56 | 26 * | -Increased urinary excretion of magnesium and potassium |
| Cealan et al., 2019 [33] | RCT | P. niruri + Mg + VitB6 | <15mm | NCCT | 48 | 3 | -No change |
| Movaghati et al., 2019 [35] | RCT |
Nigella Sativa (Black Seed) |
≥5mm | US | 30/30 | 10* | -Stone size reduction -Stone expulsion |
| Jalal et al., 2020 [36] |
RCT | Phaseolus vulgaris | ≤10mm | US | 60 | 6* | -Stone size reduction -Stone expulsion |
| Erickson et al., 2011 [37] | RCT and Crossover |
Cystone® | NS | CT | 10 † | 12 | Not effective |
| Palaniyamma and Jeyaraman 2017 [39] | RCT | Cystone® | 5-12mm | US | 65 | 3 | -Stone size reduction -Stone expulsion |
| Patki et al., 2010 [40] | RCT | Cystone® | 5-10mm | X ray US |
26/26 | 6 | -Stone size reduction -Stone expulsion |
| Patankar et al., 2020 [46] | RCT | Subap Plus | 4-9mm | NCCT | 34/31 | 6 | -Stone size reduction -Stone expulsion |
| Samandarian et al., 2023 [47] | RCT | 5 herbal extracts | ≤10mm | US | 27/27 | 4 | -Stone size reduction -Stone expulsion |
| Brardi et al., 2012 [48] | RCT | Potassium citrate + Agropyron repens | NS | US | 25/25 | 5 | -Stone size reduction -Stone expulsion |
| Kristyantoro et al., 2012 [49] | RCT | Renalof vs Kalkurenal vs Placebo | <20mm | X ray US |
13/8/9 | 1 | -Stone size reduction -Stone expulsion |
| Chamorro et al., 2021 [51] | RCT | Renalof vs Placebo | <10mm | US CT |
120/35 | 3 | Increased stone expulsion |
| Sánchez et al., 2012 [52] | RCT | Renalof vs Placebo | <10mm | X ray US CT |
52/58 | 3 | -Stone size reduction -Stone expulsion |
| Caione et al., 2022[53] | RCT | Herniaria hirsuta and Peumus boldus | Small stone fragments | NS | 15/19 | 3 | Stone expulsion post endourology |
| Sountoulides et al, 2024 [54] | RCT | Renalof vs placebo | <2 cm | CT | 82/82 | 3 | -stone surface and stone volume reduction |
4. Phythotherapy: Something to Worry About or Much ado About Nothing?
The increased use of herbal treatments has influenced the scientific community to get interested in their toxicity. Risk assessment tests have been developed for traditional herbal medicines [55]. “Safe” and “natural” are not synonyms; therefore, herbal medicines have to be treated as orthodox medicines to determine their mode of action, potential adverse reactions, contraindications, and interactions with other medicines [56]. Environmental pollutants and phytochemicals can affect the final product, and strides have been made in the authentication of herbal species, detection of harmful chemicals, toxicity mechanisms, pathway elucidation, and quantification of environmental pollutants in plants [57]. In a nutshell, despite the generalised use of phytotherapy in urolithiasis, there is a significant lack of high-level evidence published on these commonly utilised treatments [58]. Its conscious administration warrants attention to limit side effects, toxicity, and ineffective treatment [59]. The RCTs included in this narrative review also checked on the interventions' adverse effect profile and were recorded. Drug interaction, though, was not determined.
5. Evidence from Systematic Reviews
A systematic review by Monti E et al. concluded that a herbal mixture induced stone clearance, size reduction, and stone clearance significantly better than a placebo. However, citrate was better than phytotherapy in decreasing stone size [60]. A recent systematic review found that phytotherapy can be used as an alternative treatment, but more research is still necessary to attain maximum treatment benefits [61]. Another systematic review of the anti-urolithic effects of medicinal plants on calcium oxalate stones in rats found favourable changes in the lithogenic factors and also a reduction in calcium oxalate crystal deposition in the kidneys despite having only a small percentage assessing the antioxidation and diuretic activities of these treatments [62].
6. Strengths, Limitations, and Future Directions
Our review provides a comprehensive overview of studies reporting on phytotherapy and herbal remedies in urolithiasis. It included various studies and provided an overall summary, interpreting and critiquing the results in a non-systematic manner [63,64]. This allowed the inclusion of varying studies to offer a readable, thoughtful, and practical synthesis of urolithiasis and its management through herbal medicine or phytotherapy in a broad-spectrum [64,65]. This review is limited by its narrative nature. There is sometimes potential selection bias, selectiveness, and lack of exhaustiveness [64,65]. In this narrative review, extra care was taken to improve the thought process, stick to the purpose, and increase transparency in selecting the involved studies [64]. Selected RCTs, though, had heterogeneity in the herbs used, their chemical compositions, treatment period, radiology type used to determine lithiasis size and density, and dosages.
Urolithiasis has been high in developed countries and is also increasing in developing countries [66,67]. The use of herbal supplements for urolithiasis is on an upward trajectory. However, further studies are still required to determine doses, effective mixtures, mechanisms of action, drug interactions, and the efficacy of phytotherapy. This will assist in developing a predetermined concoction with doses and a treatment period, as is the case with current orthodox treatments for urolithiasis.
7. Conclusions
The prevalence of urolithiasis is high, and its management has significant economic implications in both developed and developing economies. Ancient treatment of urolithiasis was centered on herbal medicines, but conventional treatment modalities have overtaken phytotherapy along the way. Phytotherapy is bouncing back, and its use in urolithiasis is gradually increasing, albeit with limited clinical evidence to support its use. Thus, phytotherapy is increasingly involved in the management of urolithiasis, both in prevention and treatment. Different plant extracts have undergone trials, some being mixtures and others being sole plant extracts, with varying results. Most studies show the effectiveness of phytotherapy in urolithiasis, but no exact mode(s) of action have been established. Further studies are required to determine doses, modes of action, drug interactions, and duration of treatment depending on the phytotherapy used and stone type.
Author Contributions
Conceptualization, W.F.M and P.S.; methodology E.N.S., P.S; validation, W.F.M., and E.N.S.; formal analysis, W.F.M., and E.N.S.; investigation, W.F.M., and E.N.S.; data curation, W.F.M., and E.N.S.; writing—original draft preparation, W.F.M., and E.N.S.; writing—review and editing, W.F.M, E.N.S.; visualization, P.S.; supervision, P.S; All authors have read and agreed to the published version of the manuscript.
Funding
Not applicable
Institutional Review Board Statement
Not applicable
Informed Consent Statement
Not applicable
Data Availability Statement
Not applicable
Acknowledgments
Not applicable
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| PCNL | Percutaneous Nephrolithotomy |
| RIRS | Retrograde Intrarenal Surgery |
| URS | Ureteroscopy |
| SWL | Shockwave Lithotripsy |
| MET | Medical Expulsive Therapy |
| UTI | Urinary Tract Infections |
| RCTs | Randomized-controlled trials |
References
- Tiselius, H.-G. Epidemiology and medical management of stone disease: EPIDEMIOLOGY and MEDICAL MANAGEMENT OF STONE DISEASE. BJU Int. 2003, 91, 758–767. [Google Scholar] [CrossRef] [PubMed]
- López, M.; Hoppe, B. History, epidemiology and regional diversities of urolithiasis. Pediatr. Nephrol. Berl. Ger. 2010, 25, 49–59. [Google Scholar] [CrossRef]
- Fink, H.A.; Wilt, T.J.; Eidman, K.E.; Garimella, P.S.; MacDonald, R.; Rutks, I.R.; Brasure, M.; Kane, R.L.; Ouellette, J.; Monga, M. Medical Management to Prevent Recurrent Nephrolithiasis in Adults: A Systematic Review for an American College of Physicians Clinical Guideline. Ann. Intern. Med. 2013, 158, 535. [Google Scholar] [CrossRef] [PubMed]
- Türk, C.; Petřík, A.; Sarica, K.; Seitz, C.; Skolarikos, A.; Straub, M.; Knoll, T. EAU Guidelines on Interventional Treatment for Urolithiasis. Eur. Urol. 2016, 69, 475–482. [Google Scholar] [CrossRef] [PubMed]
- Uribarri, J.; Oh, M.S.; Carroll, H.J. The first kidney stone. Ann. Intern. Med. 1989, 111, 1006–1009. [Google Scholar] [CrossRef]
- Oswal, M.; Varghese, R.; Zagade, T.; Dhatrak, C.; Sharma, R.; Kumar, D. Dietary supplements and medicinal plants in urolithiasis: diet, prevention, and cure. J. Pharm. Pharmacol. 2023, 75, 719–745. [Google Scholar] [CrossRef]
- Kotsiris, D.; Adamou, K.; Kallidonis, P. Diet and stone formation: a brief review of the literature. Curr. Opin. Urol. 2018, 28, 408–413. [Google Scholar] [CrossRef]
- McDonald, M.W.; Stoller, M.L. Urinary stone disease: a practical guide to metabolic evaluation. Geriatrics 1997, 52, 38–40. [Google Scholar]
- Karakoç, O.; Karakeçi, A.; Ozan, T.; Fırdolaş, F.; Tektaş, C.; Özkarataş, Ş.E.; Orhan, İ. Comparison of retrograde intrarenal surgery and percutaneous nephrolithotomy for the treatment of renal stones greater than 2 cm. Turk. J. Urol. 2015, 41, 73–77. [Google Scholar] [CrossRef]
- Alelign, T.; Petros, B. Kidney Stone Disease: An Update on Current Concepts. Adv. Urol. 2018, 2018, 3068365. [Google Scholar] [CrossRef]
- Hughes, T.; Ho, H.C.; Pietropaolo, A.; Somani, B.K. Guideline of guidelines for kidney and bladder stones. Turk. J. Urol. 2020, 46, S104–S112. [Google Scholar] [CrossRef] [PubMed]
- Dokubo, I.I.; Wiseman, O. Management of urolithiasis. Surg. Oxf. 2022, 40, 531–539. [Google Scholar] [CrossRef]
- Pearle, M.S.; Calhoun, E.A.; Curhan, G.C. ; the UROLOGIC DISEASES OF AMERICA PROJECT UROLOGIC DISEASES IN AMERICA PROJECT: UROLITHIASIS. J. Urol. 2005, 173, 848–857. [Google Scholar] [CrossRef] [PubMed]
- Scales, C.D.; Smith, A.C.; Hanley, J.M.; Saigal, C.S. Prevalence of Kidney Stones in the United States. Eur. Urol. 2012, 62, 160–165. [Google Scholar] [CrossRef]
- Patle, A.; Hatware, K.V.; Patil, K.; Sharma, S.; Gupta, G. Role of Herbal Medicine in the Management of Urolithiasis— A Review for Future Perspectives. J. Environ. Pathol. Toxicol. Oncol. 2019, 38, 97–118. [Google Scholar] [CrossRef] [PubMed]
- Gürocak, S.; Küpeli, B. Consumption of historical and current phytotherapeutic agents for urolithiasis: a critical review. J. Urol. 2006, 176, 450–455. [Google Scholar] [CrossRef]
- Nirumand, M.; Hajialyani, M.; Rahimi, R.; Farzaei, M.; Zingue, S.; Nabavi, S.; Bishayee, A. Dietary Plants for the Prevention and Management of Kidney Stones: Preclinical and Clinical Evidence and Molecular Mechanisms. Int. J. Mol. Sci. 2018, 19, 765. [Google Scholar] [CrossRef]
- Jiang, C.; Wang, L.; Wang, Y.; Xu, R.; Yang, H.; Peng, J. Therapeutic effects of Chinese herbal medicines for treatment of urolithiasis: A review. Chin. Herb. Med. 2023, 15, 526–532. [Google Scholar] [CrossRef]
- Miyaoka, R.; Monga, M. Use of traditional Chinese medicine in the management of urinary stone disease. Int. Braz J Urol Off. J. Braz. Soc. Urol. 2009, 35, 396–405. [Google Scholar] [CrossRef]
- Akram, M.; Idrees, M. Progress and prospects in the management of kidney stones and developments in phyto-therapeutic modalities. Int. J. Immunopathol. Pharmacol. 2019, 33, 205873841984822. [Google Scholar] [CrossRef]
- Shaheen, G.; Akram, M.; Jabeen, F.; Ali Shah, S.M.; Munir, N.; Daniyal, M.; Riaz, M.; Tahir, I.M.; Ghauri, A.O.; Sultana, S.; et al. Therapeutic potential of medicinal plants for the management of urinary tract infection: A systematic review. Clin. Exp. Pharmacol. Physiol. 2019, 46, 613–624. [Google Scholar] [CrossRef] [PubMed]
- Butterweck, V.; Khan, S.R. Herbal medicines in the management of urolithiasis: alternative or complementary? Planta Med. 2009, 75, 1095–1103. [Google Scholar] [CrossRef] [PubMed]
- Singh, R.P.; Mishra, A.; Chandel, S.S.; Agarwal, M.; Chawra, H.S.; Singh, M.; Dubey, G. Unlocking New Approaches to Urolithiasis Management ViaNutraceuticals. Curr. Pharm. Biotechnol. 2024, 25, 1124–1131. [Google Scholar] [CrossRef] [PubMed]
- Zeng, X.; Xi, Y.; Jiang, W. Protective roles of flavonoids and flavonoid-rich plant extracts against urolithiasis: A review. Crit. Rev. Food Sci. Nutr. 2019, 59, 2125–2135. [Google Scholar] [CrossRef]
- Koo, K.; Aro, T.; Matlaga, B.R. Buyer Beware: Evidence-Based Evaluation of Dietary Supplements for Nephrolithiasis. J. Endourol. 2020, 34, 702–707. [Google Scholar] [CrossRef]
- Kasote, D.M.; Jagtap, S.D.; Thapa, D.; Khyade, M.S.; Russell, W.R. Herbal remedies for urinary stones used in India and China: A review. J. Ethnopharmacol. 2017, 203, 55–68. [Google Scholar] [CrossRef]
- Cupisti, A.; Giannese, D.; D’Alessandro, C.; Benedetti, A.; Panichi, V.; Alfieri, C.; Castellano, G.; Messa, P. Kidney Stone Prevention: Is There a Role for Complementary and Alternative Medicine? Nutrients 2023, 15, 877. [Google Scholar] [CrossRef]
- Singh, I.; Bishnoi, I.; Agarwal, V.; Bhatt, S. Prospective randomized clinical trial comparing phytotherapy with potassium citrate in management of minimal burden (≤8 mm) nephrolithiasis. Urol. Ann. 2011, 3, 75. [Google Scholar] [CrossRef]
- Calixto, J.B.; Santos, A.R.; Cechinel Filho, V.; Yunes, R.A. A review of the plants of the genus Phyllanthus: their chemistry, pharmacology, and therapeutic potential. Med. Res. Rev. 1998, 18, 225–258. [Google Scholar] [CrossRef]
- Pucci, N.D.; Marchini, G.S.; Mazzucchi, E.; Reis, S.T.; Srougi, M.; Evazian, D.; Nahas, W.C. Effect of phyllanthus niruri on metabolic parameters of patients with kidney stone: a perspective for disease prevention. Int. Braz J Urol Off. J. Braz. Soc. Urol. 2018, 44, 758–764. [Google Scholar] [CrossRef]
- Boim, M.A.; Heilberg, I.P.; Schor, N. Phyllanthus niruri as a promising alternative treatment for nephrolithiasis. Int. Braz J Urol Off. J. Braz. Soc. Urol. 2010, 36, 657–664. [Google Scholar] [CrossRef]
- Emiliani, E.; Jara, A.; Kanashiro, A.K. Phytotherapy and Herbal Medicines for Kidney Stones. Curr. Drug Targets 2021, 22, 22–30. [Google Scholar] [CrossRef] [PubMed]
- Cealan, A.; Coman, R.-T.; Simon, V.; Andras, I.; Telecan, T.; Coman, I.; Crisan, N. Evaluation of the efficacy of Phyllanthus niruri standardized extract combined with magnesium and vitamin B6 for the treatment of patients with uncomplicated nephrolithiasis. Med. Pharm. Rep. 2019, 92, 153–157. [Google Scholar] [CrossRef]
- Dhawan, S.; Olweny, E.O. Phyllanthus niruri (stone breaker) herbal therapy for kidney stones; a systematic review and meta-analysis of clinical efficacy, and Google Trends analysis of public interest. Can. J. Urol. 2020, 27, 10162–10166. [Google Scholar]
- Ardakani Movaghati, M.R.; Yousefi, M.; Saghebi, S.A.; Sadeghi Vazin, M.; Iraji, A.; Mosavat, S.H. Efficacy of black seed (Nigella sativa L.) on kidney stone dissolution: A randomized, double-blind, placebo-controlled, clinical trial. Phytother. Res. PTR 2019, 33, 1404–1412. [Google Scholar] [CrossRef] [PubMed]
- Jalal, S.M.; Alsultan, A.A.; Alotaibi, H.H.; Mary, E.; Alabdullatif, A.A.I. Effect of Phaseolus Vulgaris on Urinary Biochemical Parameters among Patients with Kidney Stones in Saudi Arabia. Nutrients 2020, 12, 3346. [Google Scholar] [CrossRef]
- Erickson, S.B.; Vrtiska, T.J.; Lieske, J.C. Effect of Cystone® on Urinary Composition and Stone Formation Over a One Year Period. Phytomedicine Int. J. Phytother. Phytopharm. 2011, 18, 863–867. [Google Scholar] [CrossRef]
- Patki, P.S. Cystone in cystine stone formers. Urol. Res. 2011, 39, 323–323. [Google Scholar] [CrossRef]
- Palaniyamma, D.; Jeyaraman, R. Evaluation of Efficacy and Safety of a Herbal Formulation Cystone Forte in the Management of Urolithiasis. 2017.
- Patki, P. Safety and Efficacy of an Ayurvedic Formulation Cystone in Management of Ureteric Calculi: A Prospective Randomized Placebo Controlled Study. Am. J. Pharmacol. Toxicol. 2010. [Google Scholar]
- Mohanty, N.K.; Nayak, R.L.; Patki, P.S. Safety and Efficacy of an Ayurvedic Formulation Cystone in Management of Ureteric Calculi: A Prospective Randomized Placebo Controlled Study. Am. J. Pharmacol. Toxicol. 2010, 5, 58–64. [Google Scholar] [CrossRef]
- Shekar Kumaran, M.G.; Patki, P.S. Evaluation of an Ayurvedic formulation (Cystone), in urolithiasis: A double blind, placebo-controlled study. Eur. J. Integr. Med. 2011, 3, 23–28. [Google Scholar] [CrossRef]
- Azarfar, A.; Rafiee, Z.; Ravanshad, Y.; Saber Moghadam, N.; Bakhtiari, E. Effect of Herbal Formulation “Cystone®” on Urolithiasis. Jundishapur J. Nat. Pharm. Prod. 2020, 15. [Google Scholar] [CrossRef]
- Wu, S.-Y.; Chen, H.-Y.; Tsai, K.-S.; Chiang, J.-H.; Muo, C.-H.; Sung, F.-C.; Chen, Y.-H.; Chen, W.-C. Long-Term Therapy With Wu-Ling-San, a Popular Antilithic Chinese Herbal Formula, Did Not Prevent Subsequent Stone Surgery. Inq. J. Med. Care Organ. Provis. Financ. 2016, 53, 0046958016681148. [Google Scholar] [CrossRef]
- Lin, E.; Ho, L.; Lin, M.-S.; Huang, M.-H.; Chen, W.-C. Wu-Ling-San Formula Prophylaxis Against Recurrent Calcium Oxalate Nephrolithiasis - A Prospective Randomized Controlled Trial. Afr. J. Tradit. Complement. Altern. Med. 2013, 10, 199–209. [Google Scholar]
- Patankar, S.B.; Mujumdar, A.M.; Bernard, F.; Supriya, P. Safety and efficacy of an herbal formulation in patients with renal calculi - A 28 week, randomized, double-blind, placebo-controlled, parallel group study. J. Ayurveda Integr. Med. 2020, 11, 62–67. [Google Scholar] [CrossRef] [PubMed]
- Samandarian, S.; Soltani, R.; Hajhashemi, V.; Dehghani, M.; Matinfar, M.; Mahboubi, M.; Mohsenzadeh, A. Efficacy of an Oral Solution Containing Five Herbal Extracts in the Treatment of Urolithiasis: A Randomized, Single-blind, Placebo-controlled Clinical Trial. J. Res. Pharm. Pract. 2023, 12, 96–103. [Google Scholar] [CrossRef]
- Brardi, S.; Imperiali, P.; Cevenini, G.; Verdacchi, T.; Ponchietti, R. Effects of the association of potassium citrate and agropyrum repens in renal stone treatment: results of a prospective randomized comparison with potassium citrate. Arch. Ital. Urol. Androl. Organo Uff. Soc. Ital. Ecogr. Urol. E Nefrol. 2012, 84, 61–67. [Google Scholar]
- Kristyantoro, B.; Alif, S.; Djojodimedjo, T.; Budiono, B. THE EFFECTIVENESS OF RENALOF® COMPARED TO KALKURENAL® AND PLACEBO. Indones. J. Urol. 2012, 19. [Google Scholar] [CrossRef]
- Bortolami, M.; Di Matteo, P.; Rocco, D.; Feroci, M.; Petrucci, R. Metabolic Profile of Agropyron repens (L.) P. Beauv. Rhizome Herbal Tea by HPLC-PDA-ESI-MS/MS Analysis. Molecules 2022, 27, 4962. [Google Scholar] [CrossRef]
- Chamorro, M.M.A.; Collado, S.A.V.; Márquez, D. Effectiveness of Using Renalof® in the Elimination of Kidney Stones under 10 mm Located in the Renal-Ureteral Tract. Open J. Nephrol. 2021, 11, 78–92. [Google Scholar] [CrossRef]
- Sánchez, M.C.A.; Villanueva, V.E.; Vázquez, R.A. Randomized double-blind study with Renalof in patients with calcium oxalate renal lithiasis. Rev. Cuba. Investig. Biomed. 2012, 31, 87–100. [Google Scholar]
- Caione, P.; Salerno, A.; Collura, G.; De Dominicis, M.; Innocenzi, M.; Martucci, C.; Capozza, N. Phytotherapy as ancillary treatment after urinary stone lithotripsy in pediatric age. Ann. Ital. Chir. 2022, 92, 313–318. [Google Scholar]
- Petros, S. A Randomized, Double-blind, Placebo-controlled Study of Agropyron Repens, Mannitol and Magnesium Supplement for the Treatment of Calcium Oxalate Upper Urinary Tract Stones: The AMMOS Study; clinicaltrials.gov, 2023.
- Aydιn, A.; Aktay, G.; Yesilada, E. A Guidance Manual for the Toxicity Assessment of Traditional Herbal Medicines. Nat. Prod. Commun. 2016, 11, 1763–1773. [Google Scholar] [CrossRef]
- Ekor, M. The growing use of herbal medicines: issues relating to adverse reactions and challenges in monitoring safety. Front. Pharmacol. 2014, 4, 177. [Google Scholar] [CrossRef] [PubMed]
- Jităreanu, A.; Trifan, A.; Vieriu, M.; Caba, I.-C.; Mârțu, I.; Agoroaei, L. Current Trends in Toxicity Assessment of Herbal Medicines: A Narrative Review. Processes 2023, 11, 83. [Google Scholar] [CrossRef]
- Garbens, A.; Pearle, M.S. Causes and prevention of kidney stones: separating myth from fact. BJU Int. 2021, 128, 661–666. [Google Scholar] [CrossRef]
- Allegra, S.; De Francia, S.; Turco, F.; Bertaggia, I.; Chiara, F.; Armando, T.; Storto, S.; Mussa, M.V. Phytotherapy and Drugs: Can Their Interactions Increase Side Effects in Cancer Patients? J. Xenobiotics 2023, 13, 75–89. [Google Scholar] [CrossRef] [PubMed]
- Monti, E.; Trinchieri, A.; Magri, V.; Cleves, A.; Perletti, G. Herbal medicines for urinary stone treatment. A systematic review. Arch. Ital. Urol. Androl. Organo Uff. Soc. Ital. Ecogr. Urol. E Nefrol. 2016, 88, 38–46. [Google Scholar] [CrossRef]
- Allam, E.A.H.; Sabra, M.S. Plant-based therapies for urolithiasis: a systematic review of clinical and preclinical studies. Int. Urol. Nephrol. 2024, 56, 3687–3718. [Google Scholar] [CrossRef]
- Khan, A.; Bashir, S.; Khan, S.R. Antiurolithic effects of medicinal plants: results of in vivo studies in rat models of calcium oxalate nephrolithiasis-a systematic review. Urolithiasis 2021, 49, 95–122. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Thorne, S.; Malterud, K. Time to challenge the spurious hierarchy of systematic over narrative reviews? Eur. J. Clin. Invest. 2018, 48, e12931. [Google Scholar] [CrossRef] [PubMed]
- Sukhera, J. Narrative Reviews: Flexible, Rigorous, and Practical. J. Grad. Med. Educ. 2022, 14, 414. [Google Scholar] [CrossRef] [PubMed]
- Sarkar, S.; Bhatia, G. Writing and appraising narrative reviews. J. Clin. Sci. Res. 2021, 10, 169–172. [Google Scholar] [CrossRef]
- Borumandnia, N.; Fattahi, P.; Talebi, A.; Taheri, M.; Alvani, M.S.; Balani, M.M.; Ashrafi, S.; Alavimajd, H. Longitudinal trend of urolithiasis incidence rates among world countries during past decades. BMC Urol. 2023, 23, 166. [Google Scholar] [CrossRef]
- Zhang, L.; Zhang, X.; Pu, Y.; Zhang, Y.; Fan, J. Global, Regional, and National Burden of Urolithiasis from 1990 to 2019: A Systematic Analysis for the Global Burden of Disease Study 2019. Clin. Epidemiol. 2022, 14, 971–983. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Schematic presentation of the most common causes and predisposing risk factors of urolithiasis.
Figure 1.
Schematic presentation of the most common causes and predisposing risk factors of urolithiasis.
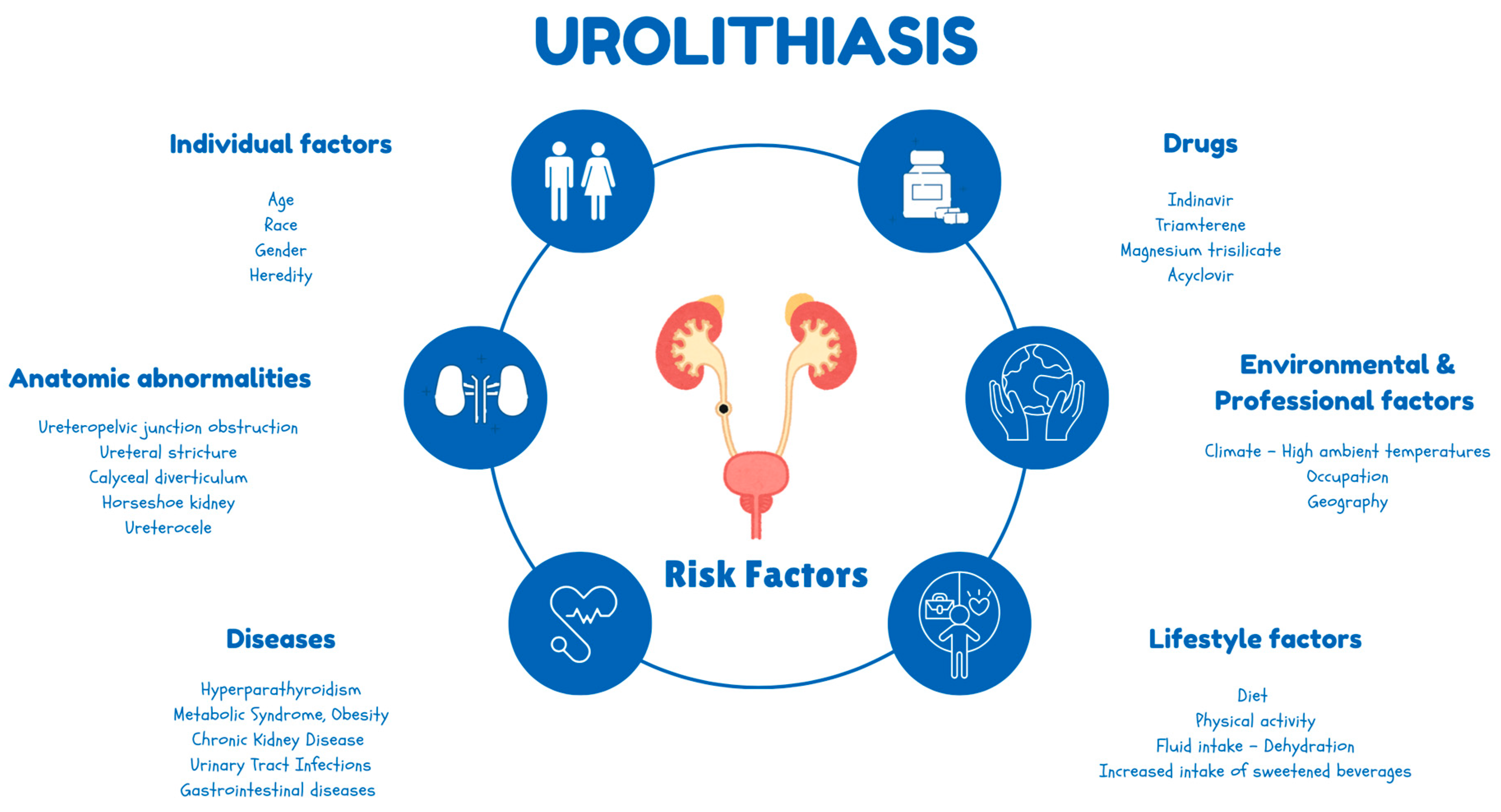
Figure 2.
Overview of the available treatment options for urolithiasis.
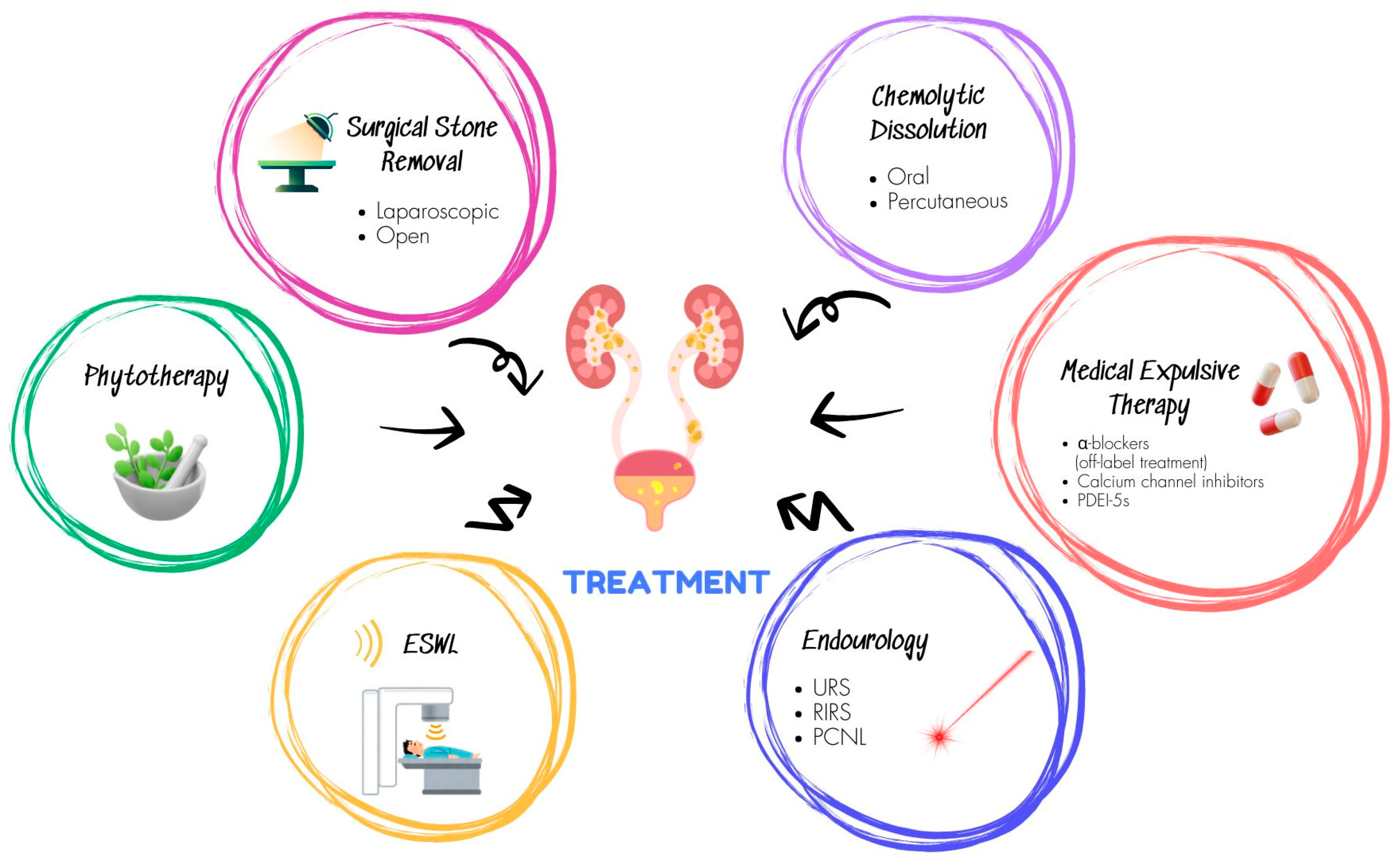
Figure 3.
Flow chart of the included studies in the narrative synthesis.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



