
Submitted:
01 March 2025
Posted:
03 March 2025
You are already at the latest version
Abstract
Prostatic disorders are commonly observed in older, intact male dogs and have been a primary etiological factor in the development of PH. Most literature recommends per-forming perineal herniorrhaphy concurrently with castration to reduce the recurrence of PH, although some studies remain controversial. Limited literature exists regarding correcting PH with castration in dogs suffering from prostatic disorders, including management and long-term clinical outcomes. This retrospective study aimed to de-scribe the management of prostatic disorders and evaluate outcomes and recurrence following perineal herniorrhaphy with castration. A total of 315 intact male dogs that underwent perineal herniorrhaphy due to prostatic disorders were classified into two groups: a castrated group (PHC; n=184) and a non-castrated group (PHNC; n=131). The clinical signs of the PHC group showed significant improvement in the postoperative, short and long-term follow-up phases (p< 0.001). Prostate gland enlargement, hetero-geneous parenchyma and intraparenchymal cystic lesions were more prevalent in the short-term of the PHNC group and the long-term of the PHNC-2 group (p< 0.001). Nevertheless, the incidence of recurrent PH showed no significant differences between the PHC and PHNC groups (p=0.48). In conclusion, this study indicates that castration does not significantly reduce PH recurrence, addressing prostatic diseases during sur-gery is crucial to improve outcomes.
Keywords:
Canine
; Castration
; Perineal hernia
; Prostatic disorders
; Prostatic cyst
; Prostatic abscess
1. Introduction
The prostate gland, which is the only accessory sex gland in male canines, plays a vital role in producing and secreting prostatic fluid [1,2,3,4,5,6]. Prostatic disorders are associated with androgen-dependent hormones and are commonly observed in older, intact male dogs [1,2,3,4,5,7,8,9]. According to several studies, benign prostatic hyperplasia (BPH) is the most common prostatic disorder, affecting approximately 50%, 80%, and 90% of dogs aged over 4, 6, and 8 years, respectively [3,4,7,9,10,11,12]. Dogs with BPH may be predisposed to the development of prostatitis or the formation of prostatic cysts or abscesses, which may manifest as intraparenchymal or extraparenchymal (paraprostatic) lesions [12,13].
The clinical manifestations of prostatic disorders can vary from asymptomatic to more severe signs including tenesmus, dyschezia, constipation, small or ribbon-like feces, hematuria, dysuria, stranguria, abdominal discomfort, and septicemia [4,7,12,13,14,15]. Perineal hernia (PH) has been reported to be associated with prostatic disorders in older intact male dogs [15,16]. The enlargement or inflammation of the prostate can lead to tenesmus or stranguria, increase intra-abdominal or pelvic diaphragm pressure, and result in instability of the pelvic diaphragm muscles. As a consequence, abdominal organs may protrude into the perineal region [7,15,16,17,18,19,20]. Hormonal influences are likely to assume a principal role in the pathogenesis of PH; however, the underlying etiopathologies remain ambiguous and are multifactorial, involving factors such as constipation, rectal abnormalities, severe cough, neurogenic atrophy of the pelvic diaphragm muscles, and the effects of relaxin [17,19,21,22,23,24]. Surgical correction, also known as perineal herniorrhaphy, is the preferred treatment option for dogs suffering from PH [17,25,26,27]. Most studies in the literature recommend performing perineal herniorrhaphy concurrently with castration to reduce the recurrence rate of PH, although some studies are controversial [17,28,29,30,31]. Conversely, the effective management of severe prostatic disorders, including prostatitis and prostatic abscess, requires appropriate medical treatment to control the infection before considering further castration as a preventive measure against chronic urinary tract infections (UTIs) or recurrent prostatic abscesses [12,14,32,33]. Consequently, the decision regarding castration in cases of severe prostatic disorders that occur concurrently with PH remains a subject of controversy among veterinarians concerning its actual advantages or disadvantages in surgery.
In our clinical practice, numerous dogs that underwent neutering during the correction of PH often experience recurrence. The underlying cause of this recurrence was inappropriate treatment of severe prostatitis or prostatic cystic lesions at the previous surgery. No previous literature has reported on the surgical and medical management of canine PH associated with diagnosed prostatic disorders, as well as the subsequent treatment outcomes. This retrospective study aimed to describe the management of prostatic disorders and the surgical outcomes combined with the castration of intact male dogs suffering from PH associated with prostatic disorders.
2. Materials and Methods
2.1. Study Design and Case Selection
This retrospective study reviewed intact male dogs that underwent perineal herniorrhaphy and were diagnosed with prostatic disorders at the Kasetsart University Veterinary Teaching Hospital (KUVTH) in Thailand from 2018 to 2023.
2.2. Inclusion Criteria
The study included intact male dogs at KUVTH who showed signs of perineal swelling and underwent clinical examination to confirm the symptoms via digital rectal examination. In addition, all of the dogs were diagnosed with PH due to prostatic disorders such as BPH, prostatitis, prostatic cysts and abscesses. Dogs with testicular tumors and cryptorchidism were included in this study. All patients had perineal herniorrhaphy with different surgical techniques used by the surgeons.
2.3. Exclusion Criteria
Patients were excluded from the study if the cause of PH was unrelated to prostatic disorders including severe constipation or enteritis, rectal mass, lumbosacral stenosis, cardiac disease, severe coughing and suspected prostatic tumor.
2.4. Data Collection
The data collection included the following: age, breed, body weight (BW), clinical signs, PH content and previous treatment history. The pre-operative clinical signs were categorized into 4 groups: urogenital systems, gastrointestinal (GI) systems, systemic signs and other signs. The diagnoses of PH and prostatic disorders were performed through physical examination and digital rectal examination to evaluate perineal content and prostatic disorders. Complete blood count (CBC) and serum chemistry analysis were performed before surgery to assess overall health and identify systemic diseases. Radiographic and ultrasonographic examinations of the caudal abdominal and perineal regions were performed to examine the positioning of abdominal organs and identify prostatic disorders. Additionally, diagnoses of prostatic disorders were based on semen or prostatic fluid analysis, urinalysis and/ or urine culture. The actual prostatic volume (cm3) was measured from the prostate ultrasonography and calculated using the following formula [34]:
The prostate gland enlargement in all case studies was compared to the predicted normal prostatic volume (cm3), calculated using the following formula [35]:
Normal prostatic volume (cm3) = (0.33 x BW (kg)) + 3.28
2.5. Medical Treatments
Before surgery, any pre-existing health issues were stabilized. Dogs with azotemia or dehydration required fluid therapy. Cystocentesis was performed in the urinary bladder (UB) retroflexion to release urine and reduce urethral pressure. Urinary catheterization was placed in the UB displacement or retroflexion patients until the day of surgery. Antimicrobials were administered based on the drug of choice for prostatitis/ UTIs or the results of bacterial culture and drug sensitivity tests from semen, prostatic fluid and/ or urine samples. The finasteride, 5α-reductase inhibitors (Proscar®, Merck & Co., Inc., USA or Firide®, Siam Bheasach CO., LTD., Thailand) at the dosage of 0.1-0.5 mg/kg once a day were used for BPH treatment [36].
2.6. Surgical Procedure
The anesthetic protocols were carried out by the anesthesiologist, including sedation and anesthetic induction, following endotracheal intubation and inhalation to maintain anesthesia. The prophylaxis antimicrobial and analgesia drugs were routinely administered before surgery. The surgical procedure for the correct PH was chosen according to the surgeon preference. The aseptic surgical field was prepared at the perineal area and the caudal abdomen, fecal evacuation and a purse-string suture were placed in the anus. Before surgery, urethral catheterization was placed in all patients for identification of the urethra and the prevention of accidental urethral injury during surgery. For castration, a pre-scrotal or caudal scrotal approach [37] was performed before perineal herniorrhaphy. If a testicular tumor was presented, histopathological evaluation was performed. For perineal herniorrhaphy, all dogs were positioned in sternal recumbency with their hindquarters elevated and tails lifted craniodorsally. Surgical procedures were recorded, including rectal diverticulum correction, colopexy, cystopexy, and additional procedures.
2.7. Postoperative Outcome and Follow-Up
Intraoperative and postoperative complications such as wound dehiscence, seroma, rectal prolapse, fecal incontinence, urinary incontinence and sciatic nerve injury were recorded. The follow-up evaluations after surgery from the available medical records were divided into 3 phases: postoperative phase (1-2 weeks), short-term phase (1-2 months) and long-term phase (>6 months-the latest examination). The postoperative clinical signs were compared with pre-operative signs and hernial recurrence and cause of recurrence were evaluated.
2.8. Statistical Analysis
All statistical analyses were performed using R-statistic under RStudio ver. 2023.06.0+421 with package Rcmdr. The bar chart was performed by Microsoft Excel (Microsoft Office Home and Student 2021). Descriptive statistics were calculated with mean±standard deviation (SD) and 95% CI for normally distributed data and the median (range) and 95% CI for non-normally distributed data. Student's T-test was used to compare the continuous variables between groups for normally distributed data and homogeneity of variance, while the Welch T-test was used for the non-normal distribution and/or heterogeneity of variance. Shapiro-Wilk tested the normal distribution, whereas homogeneity of variance tested by Levene's test. The differences in discrete or dichotomous variables between groups were analyzed with the Chi-square test. P values <0.05 were considered statistically significant differences. Survival analysis was performed using the survival package for Cox proportional hazards regression and survival curve fitting, while the survminer package was utilized to visualize the survival curves.
3. Results
3.1. Signalment and Pre-Operative Findings
During 2018-2023, a total of three hundred and thirty-two intact male dogs that underwent perineal herniorrhaphy were evaluated. Of these, 315 cases were in the inclusion criteria associated with prostatic disorderss. Seventeen cases were excluded due to non-prostatic disorders, including constipation (n=6), cardiorespiratory disease (n=6), trauma (n=3), prostatic carcinoma (n=1) and muscle atrophy (n=1). The most common breeds were Crossbreed (n=78), Chihuahua (n=65), Shih Tzu (n=45), Pomeranian (n=40), Poodle (n=29), Spitz (n=9), Siberian Husky (n=9), Schnauzer (n=5), French Bulldog (n=5), Miniature Pinscher (n=5), Yorkshire Terrier (n=5), Bangkaew (n=3), Jack Russell Terrier (n=2), Weimaraner (n=2) and one each of Affenpinscher, American Pit Bull Terrier, American Toy Fox Terrier, Beagle, Boston Terrier, Coton de Tulear, Italian Greyhound, Labrador Retriever, Maltese, Pekingese, Pug, Thai Ridgeback and Welsh Terrier. All dogs involved in this study were classified into 2 groups: a castrated group (PHC), which underwent castration in conjunction with perineal herniorrhaphy, and a non-castrated group (PHNC), which underwent perineal herniorrhaphy only. The PHC and PHNC groups had 184 and 131 cases, respectively. The mean age (±SD; range) was 9 years (±2.7; 3-16 and ±2.5; 4-15), while BW were 9 kg (±6.6; 2-44 kg) and 8 kg (±6.2; 2-34 kg) of the PHC and PHNC group, respectively, with no significant difference (p=0.72). Pre-operative clinical signs are outlined in Table 1. The average duration of clinical signs before diagnosis at KUVTH was 83 days (range: 0 day to 5 years) and 110 days (range: 0 day to 3 years) in the PHC and PHNC groups, respectively (no significant difference between groups; p=0.079) (Figure 1). Before surgery, 13.04% (24/184) of the PHC group and 2.29% (3/131) of the PHNC group were available for semen collection, which was subsequently submitted for semen cytology and culture. Of these, BPH and prostatitis were diagnosed from semen cytology and culture. The incidence of BPH was 66.67% (16/24) in the PHC group and 33.33% (1/3) in the PHNC group, while the incidence of prostatitis was 70.83% (17/24) versus 66.67% (2/3), respectively.
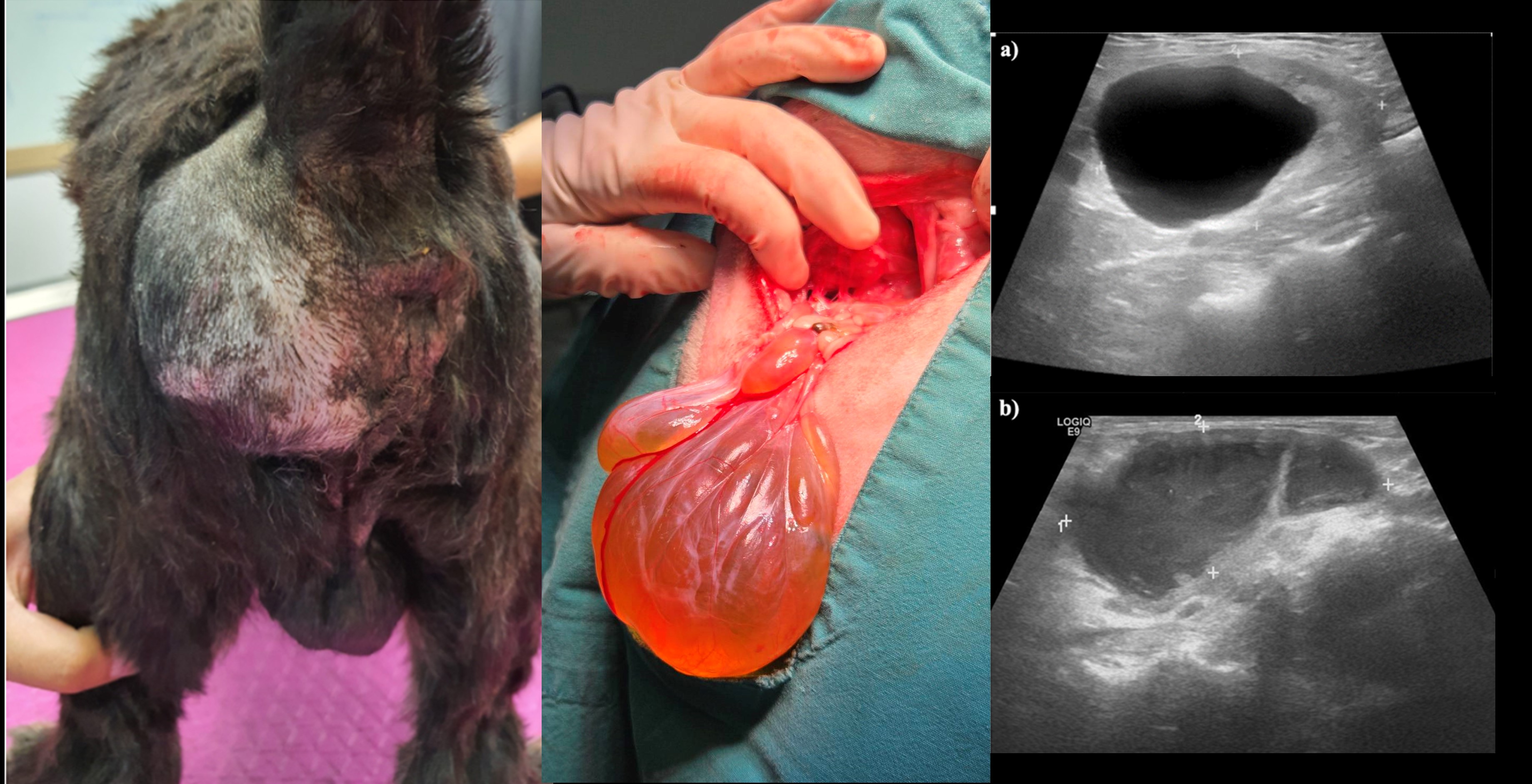
Transabdominal and perineal ultrasonography were performed on 181 dogs in the PHC group and 130 dogs in the PHNC group. The preoperative ultrasonographic findings of the prostate gland are shown in Figure 2. Prostate enlargement was observed in 96% of cases and did not differ significantly between both groups. The most significant ultrasonographic finding of the prostate showed intraparenchymal prostatic cystic lesions in both groups, with no significant differences between groups. In the PHC group, intraparenchymal cystic lesions were observed in the following sizes: less than 1 cm (61.32%, 111/181), 1-5 cm (24.31%, 44/181), and larger than 5 cm (0.55%, 1/181). In the PHNC group, sizes included less than 1 cm (48.46%, 63/130), 1-5 cm (43.08%, 56/130), and larger than 5 cm (0.77%, 1/130). However, extraparenchymal cystic lesions of prostate gland showed a significant difference between the groups (p<0.05). Extraparenchymal cystic lesions were observed in the following sizes: less than 1 cm (2.76%, 5/181), 1-5 cm (1.66%, 3/181), and larger than 5 cm (0.55%, 1/181). Contrast in the PHNC group was found only in 1-5 cm (6.92%, 9/130). Urine sediment was observed in 32.6% (59/181) of the PHC group, while the PHNC group showed a higher rate of 53.08% (69/130). Additionally, cystic calculi were found in 3.31% (6/181) of the PHC group and in 2.31% (3/130) of the PHNC group (significant difference; p<0.05). Urinalysis and urine culture results were available for 97 and 57 dogs in the PHC and PHNC groups, respectively. The results indicated that 47.25% (43/91) of the PHC group and 68.89% (31/45) of the PHNC group had cystitis/UTIs, with no significant difference (χ²=0.58, p=0.81).
At the time of surgery, bilateral herniorrhaphy had 38.04% (70/184) of the PHC and 52.67% (69/131) of the PHNC groups, while unilateral herniorrhaphy was performed in 61.96% (114/184) versus 46.56% (61/131), respectively. The most frequently herniated contents in both groups were prostate gland and UB (Figure 3). UB retroflexion was observed in 33.15% (61/184) and 38.17% (50/131) of the PHC and PHNC groups, respectively. The most commonly used surgical technique in both groups was the sacro-ischial sling method (SS); 34.78% (64/184) in PHC and 33.58% (44/131) in the PHNC group (Figure 4). The additional intraoperative procedure, 5 dogs in the PHC group and 3 dogs in the PHNC group had severe UB necrosis, and 3 of PHC group showed UB rupture. This resulted in a partial cystectomy and UB reconstruction, while one dog required UB marsupialization. Additionally, one dog from the PHNC group had severe prostatic necrosis, resulting in a total prostatectomy with urethral anastomosis. Cyst wall resection and partial prostatectomy with omentalization were performed for one dog in the PHC group and three dogs in the PHNC group. Fine needle aspiration (FNA) of prostatic fluid was performed on 13 dogs in the PHC and 9 dogs in the PHNC groups. The results of the prostatic fluid cytology and culture were as follows: cysts were found in 40% (4/10) of the PHC group and 77.78% (7/9) of the PHNC group, while abscesses were found in 60% (6/10) versus 22.22% (2/9), respectively. Regarding the castration technique, in the PHC group, 98.37% (181/184) of dogs underwent prescrotal castration, and 1.63% (3/184) underwent postscrotal (perineal) castration. Rectal reconstruction was performed on two dogs in the PHC and PHNC groups due to rectal tears. Three dogs in the PHC group received cystopexy and colopexy procedures.
3.3. Postoperative Outcome and Follow-Up
After their surgeries, all dogs required hospitalization to receive IV fluid, analgesia and antimicrobial administration. Both groups of dogs showed signs of surgical wound bruising, inflammation and mild tenesmus a few days after the surgery. A total of 167 dogs from the PHC and 120 dogs from the PHNC groups were included in the follow-up assessment. The study found no significant difference in postoperative complications between the groups (χ²=0.14, p=0.71). The postoperative complications of both groups are shown in Figure 5.
3.3.1. Postoperative Phase (1-2 Weeks)
One hundred sixty-five dogs from the PHC and 115 dogs from the PHNC groups were available for follow-up, and the postoperative outcome showed differentiated significance between the groups (χ²=38.10, p<0.001). In the PHC group, 67.88% (112/165) and in the PHNC group, 30.43% (35/115) had resolved pre-operative clinical signs. Postoperative abnormalities in the PHC and PHNC group are shown in Table 2. The changes observed in prostatic disorders following surgical intervention are shown in Figure 1. Notably, the enlargement of prostate gland was significantly greater in the PHNC group (p<0.05). In this phase, there was no differentiation in the echogenicity of prostate gland and the intraparenchymal and extraparenchymal cystic lesions between the groups. After surgery, 3 dogs in the PHC group died a few days later, while one dog in the PHNC group was euthanized due to severe UB necrosis and UB rupture. The incidence of recurrent PH during this phase was 1.82% (3/165) in the PHC group and 2.61% (3/115) in the PHNC group.
3.3.2. Short-Term Phase (1-2 Months)
During the short-term follow-up phase, there were 104 dogs in the PHC group and 90 dogs in the PHNC group, with significant differences in the post-operative outcomes (χ²=32.63, p<0.001). In the PHC group, 46.15% (48/104) and in the PHNC group, 8.89% (8/90) had resolved pre-operative clinical signs. In both groups, urogenital signs, GI signs, and systemic signs were still presented, as shown in Table 2. Cystitis and UTIs were more incidence in the PHNC group compared to the PHC group, showing a significant difference (p<0.05). The changes observed in prostatic disorders following surgical intervention are shown in Figure 1. Prostate gland enlargement, heterogeneous parenchyma, and intraparenchymal cystic lesions were significantly higher in the PHNC group (p<0.001). At this time, two dogs in the PHC group had recurrent PH, and 6 dogs in the PHNC group had recurrent PH.
3.3.3. Long-Term Phase (>6 Months to the Last Examination)
Seventy-five dogs from the PHC group and 47 dogs from the PHNC group were available for long-term evaluation and showed highly significantly improved clinical signs in the PHC group compared with the PHNC groups (χ²=14.47, p<0.001). The PHNC group was divided into two subgroups during this phase: 7 dogs were castrated within 2 months after perineal herniorrhaphy (PHNC-1), while 40 dogs remained intact or had castration (surgical castration or GnRH implantation) after 2 months of follow-up (PHNC-2). In the PHNC-1 group, two dogs continued to exhibit large prostatic cystic lesions and required partial prostatectomy with omentalization during castration at this phase. The changes observed in prostatic disorders following surgical intervention in this phase are shown in Figure 6. In the PHNC-2, the prostate enlargement, heterogeneous parenchyma, and intraparenchymal cystic lesions were significantly greater than in the other group (p<0.001). The recurrent PH in this phase was not significantly different between the groups (χ²=0.45, p=0.48). Recurrent PH or rectal pouch was observed in 13.58% (25/184) of the PHC and 16.79% (22/131; n=4 in the PHNC-1 and n=18 in the PHNC-2) of the PHNC groups. The mean duration of no recurrent perineal swelling after surgery to the last visit at KUVTH was 466 days (range: 1 day to 3.5 years) for the PHC, 499 days (range: 30 days to 4 years) for the PHNC-1 group and 475 days (range: 1 day to 4 years) for the PHNC-2 group (no significant difference between the groups, p=0.34) (Figure 7). The following concurrent diseases were presented at the time of PH recurrence in the PHC group: prostatic disorders 12% (n=3), muscle atrophy 8% (n=2), cardiorespiratory diseases 20% (n=5), neurological diseases 8% (n=2), GI diseases with constipation 28% (n=7), trauma 5% (n=1) and unknown cause or loss follow up 20% (n=5). The causes of recurrence in the PHNC-1 group (n=4) include one case each of prostatitis and muscle atrophy associated with coughing, prostatitis, and a paraprostatic abscess. In the PHNC-2 group (n=18), the potential causes of PH recurrence were identified as follows: prostatic disorders accounted for 88.89%, including BPH with prostatitis in 44.44% (n=8); prostatic cysts in 16.67% (n=3, consisting of 1 intraparenchymal and 2 paraprostatic cysts); prostatic abscesses in 16.67% (n=3); muscle atrophy with prostatitis in 5.56% (n=1); cardiorespiratory diseases associated with prostatic abscess in 5.56% (n=1); trauma in 5.56% (n=1); and excessive barking in 5.56% (n=1).
4. Discussion
The study revealed that prostatic disorders were the primary condition affecting older dogs in both the PHC and PHNC groups, significantly contributing to the development of PH, consistent with previous research findings [20,26,28,38]. In contrast to the literature, the data findings indicate a higher prevalence of dogs with PH among smaller breeds [17,39], which likely reflects the larger population of small-breed dogs in our country. Most intact male dogs with PH have been reported to have an incidence rate of 10% to 80% [20,25,40,41,42]. However, the current study reveals a significantly higher incidence of prostatic disorders, measured at 94.88%, compared to earlier research findings. According to the data presented, intact older male dogs of any breed size that have PH should be regularly monitored for prostatic disorders and undergo routine andrological examinations before making any decisions regarding the correction of PH. The heterogeneous parenchyma and intraparenchymal prostatic cystic lesions less than 1 cm represent the most common pathological changes observed through ultrasonography of prostate in this study. According to previous literature, Haverkamp et al. (2019) reported that 84.8% of prostatic cysts were identified through CT scans in dogs older than four years [43], while Ahlberg et al. (2022) indicated that dogs presented with 97.8% of heterogeneous prostate and 93.5% of intraprostatic cysts in cases diagnosed with PH [40]. In the surgical field of this study, the most common hernial contents in both groups were the prostate gland and UB, which is consistent with previous studies [20,25,40]. These results confirm the earlier theory that prostatic disorders primarily cause PH by increasing abdominal and pelvic diaphragm pressure, which may lead to tenesmus and caudal displacement of organs into a hernia. Nevertheless, the etiology of PH may be multifactorial contributors, including rectal abnormalities, neurological factors, trauma, constipation, and severe cardiorespiratory diseases; consequently, additional causes should be ruled out [17,25,40]. The formation of prostatic cysts can result from the obstruction of prostatic fluid in the canaliculi due to BPH, resulting in cysts that vary in size from small to larger cystic lesions [4]. Furthermore, the abnormal positioning of the UB and prostate gland can contribute to obstructive prostatic fluid drainage into the urethra, resulting in cystic formation within the prostate [4,7,40,44].
According to previous reports, the most common signs of PH in dogs include perineal swelling, dyschezia, tenesmus, cystitis and UB retroflexion [20,24,26,28,38]. From the study results, UB retroflexion has a high incidence (33-38%) in PH dogs, which is a higher prevalence than in previous studies [40]. This condition can lead to urinary tract obstruction, azotemia and bladder necrosis, resulting in a high rate of postoperative complications and potentially causing death. Urinary catheterization should be performed until surgical intervention is deemed necessary as part of pre-operative management to prevent urinary obstruction. Abdominal and perineal ultrasonography serve as effective diagnostic instruments for the evaluation of dogs with PH in conjunction with prostate disorders. These modalities facilitate the evaluation of prostate size, characteristics of the prostate, as well as prostatic lesions, and the localization of abdominal organs [10,20,40,45]. In our report, the PHNC group demonstrated a lower prevalence of prostatic hyperplasia compared to the PHC group, primarily attributable to the limited capability of ultrasonography in fully assessing prostatic characteristics in cases of UB or prostate displacement into the pelvic canal. The CT scan has been reported to assist in evaluating prostatic disorders associated with PH [40,43]; however, this method is not practical in clinical practice due to its high cost and the requirement for anesthesia. The diagnosis of prostatic disorders was based on the cytological examination of semen or prostatic fluid and/or culture [10,13,14]. However, specimen collection was available in some dogs in our study; pain or discomfort is primarily caused by unsuccessful semen collection. Based on the literature, the presence of heterogeneous parenchyma with or without hypoechoic intraparenchymal prostatic cyst lesions from ultrasonography may be assumed as prostatitis [14,40,46]. According to the prior study, prostatitis concurrent with cystitis constituted the most prevalent condition observed in intact male dogs [47]. In our study, UTIs were confirmed through urine cultures in 47% of the PHC group and 69% of the PHNC group, respectively.
For the management of PH associated with prostatic disorders, castration accompanied by the correction of PH is advised for canines exhibiting both conditions simultaneously, as indicated in the majority of the literature [4,15,19]. One month after surgery and during the long-term evaluation, the pre-operative clinical signs showed a more significant resolution in the PHC group compared to the PHNC group. The incidence of prostatic gland enlargement, heterogeneous parenchyma and intraparenchymal cystic lesions of prostate was lower in the PHC group compared to the PHNC and PHNC-2 groups. Furthermore, six months after surgery, the PHC group did not exhibit any prostatic abscesses in contrast to the PHNC group. Conversely, for dogs with large prostatic cavities, castration should not be performed without drainage or surgical treatment of prostatic cystic lesions [7,48]. The prostatic cystic lesions may recur or develop into a prostatic abscess after castration leading to a recurrence of PH [7,14,32]. Consequently, the veterinarian decided against performing castration at the time of the perineal herniorrhaphy when the cavitary lesions of the prostate were unclear. In this study, FNA for drainage, cyst or abscess resection, or partial prostatectomy with omentalization was performed as a treatment for large prostatic cysts or abscesses during perineal herniorrhaphy to prevent recurrence of prostatic cystic lesions after surgery in both groups. During the follow-up period, the PHNC group exhibited a recurrence of a prostatic abscess, necessitating multiple drainage procedures, which was not observed in the PHC group. In the PHNC-1 group, two dogs persisted in displaying significant prostatic cystic lesions, requiring a second surgical intervention for partial prostatectomy with omentalization and castration. Furthermore, no recurrence of PH was observed during long-term follow-up. This was attributed to the effective elimination of hormonal effects on the prostate and cystic formation due to castration [7,14]. Castration provides benefits for prostatic atrophy by reducing prostatic size and bacterial infections, especially when combined with prostatic cyst management, which consequently contributes to the recurrence of PH [15,40]. In this study, caudal scrotal castration can be performed during perineal herniorrhaphy, thereby reducing anesthetic time and eliminating the necessity to change position during surgery [37].
During long-term postoperative follow-up, no significant differences were observed in the prevalence and duration of PH recurrence between groups. The findings of this retrospective study indicated that castration does not influence the recurrence of PH following herniorrhaphy, inconsistent with numerous other studies [17,19,20,24,37,49,50]. Nevertheless, the etiology of recurrent PH in the PHNC group revealed a higher incidence of prostatic disorders when compared to the PHC group. When comparing the outcomes after surgery, mild postoperative complications were observed a few days following surgical herniorrhaphy in all cases, including wound inflammation, wound dehiscence, scrotal inflammation, hematoma/seroma, and hind limb edema. In the PHC group, three dogs died under the following circumstances: one dog had urethral stenosis, disseminated intravascular coagulation (DIC), and abdominal bleeding after surgery; one dog suffered from pancreatitis and a seizure; and one dog developed progressive azotemia after returning home. Outstanding postoperative care in the hospital is recommended, as all patients demonstrated clinical improvement signs. Other than that, one dog in the PHNC group was euthanized after surgery because the owner declined treatment with UB and prostatic necrosis, and the dog developed prostatic necrosis and UB rupture 2 weeks after surgical repair. Additionally, UTIs/cystitis and cystic calculi or sediment were still present in the long-term follow-up of both groups. UTIs or bacterial cystitis are frequently reported in conjunction with prostatitis [14,46,51]. Numerous research studies recommend the administration of antimicrobials for a minimum duration of 4 to 6 weeks for the treatment of cystitis and prostatitis; in certain cases, this duration may extend beyond six months [12,14]. Furthermore, the ongoing evaluation of both prostatitis and cystitis remains essential following surgical procedures [14,46].
The primary limitation of this retrospective study lies in the reliance on medical records, which may lack complete data, including detailed follow-up information and consistent diagnostic methods across cases. Additionally, the decision to perform castration and surgical procedures was influenced by the individual surgeon’s preferences, potentially introducing variability in treatment outcomes. Another limitation is the relatively small sample size for certain subgroups, which restricts the ability to generalize findings to broader populations. Further research should focus on long-term follow-ups with larger sample sizes to evaluate the recurrence rates and explore alternative surgical and medical protocols. Advanced imaging techniques, like CT or MRI, could provide deeper insights into the pathophysiology of prostatic lesions and PH. Additionally, prospective studies assessing the efficacy of various treatment combinations, including targeted antibiotic therapies and innovative surgical techniques, may help refine the current standards of care. Finally, examining the genetic predispositions in specific breeds could aid in preventive strategies.
5. Conclusions
In conclusion, this study indicates that castration does not affect the prevalence and duration of PH recurrence; however, the recurrence of PH associated with prostatic disorders such as BPH, prostatitis, and prostatic cysts/abscesses can be reduced. The recommended treatment for large prostatic cysts or abscesses during perineal herniorrhaphy includes FNA for drainage, cyst or abscess resection, or partial prostatectomy with omentalization, so as to prevent recurrence of prostatic cystic lesions thereafter surgery.
Author Contributions
Conceptualization, P.S. and C.L.; methodology, P.S.; formal analysis, A.K.; investigation, P.S.; data curation, P.S.; writing—original draft preparation, P.S.; writing—review and editing, C.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research was supported by KASETSART VETERINARY DEVELOPMENT FUNDS, Faculty of Veterinary Medicine, Kasetsart University.
Institutional Review Board Statement
The animal study protocol was submitted and approved by the Kasetsart University Institutional Animal Care and Use Committee, Faculty of Veterinary Medicine, Kasetsart University (protocol no. ACKU66-VET-088, 13 November 2023).
Informed Consent Statement
Not applicable
Data Availability Statement
All data are contained in the manuscript.
Acknowledgments
The authors are grateful to the Theriogenology Center, the Operation and Laparoscopic Center, and the Kasetsart Veterinary Imaging and Radiotherapy Center of KUVTH, Kasetsart University, for their support and data contribution to this study. Financial support by the Faculty of Veterinary Medicine, Kasetsart University.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| BPH | Benign prostatic hyperplasia |
| PH | Perineal hernia |
| UTIs | Urinary tract infections |
| BW | Body weight |
| GI | Gastrointestinal tract |
| CBC | Complete blood count |
| cm3 | Cubic centimeter |
| UB | Urinary bladder |
| SD | Standard deviation |
| PHC | Castrated group which underwent castration in conjunction with perineal herniorrhaphy |
| PHNC | Non-castrated group which underwent perineal herniorrhaphy only |
| kg | Kilogram |
| cm | Centimeter |
| P/O | Postoperative |
| SS | The sacro-ischial sling method |
| IOMT | The Internal obturator muscle transposition technique |
| FNA | Fine needle aspiration |
| PHNC-1 | PHNC group which castrated within 2 months after perineal herniorrhaphy |
| PHNC-2 | PHNC group which remained intact or castrated 2 months after perineal herniorrhaphy |
| GnRH | Gonadotropin-releasing hormone |
| DIC | Disseminated intravascular coagulation |
| CT scan | Computerized Tomography Scan |
| MRI | Magnetic Resonance Imaging |
References
- Fernando Leis-Filho, A., & E. Fonseca-Alves, C.. Anatomy, histology, and physiology of the canine prostate gland. In Veterinary Anatomy and Physiology; IntechOpen: 2018.
- Verma, A.; Singh, R.; Jawre, S.; Khan, A.; Namdev, N.; Vishvakarma, S.; Sinha, A. Prostate disorders in dogs, with a focus on benign prostatic hyperplasia (BPH): An overview. Int. J. Vet. Sci. Anim. Husb. 2024, 9, 868–875. [Google Scholar]
- Palmieri, C.; Fonseca-Alves, C.E.; Laufer-Amorim, R. A review on canine and feline prostate pathology. Front Vet Sci 2022, 9, 881232. [Google Scholar] [CrossRef] [PubMed]
- Smith, J. Canine prostatic disease: A review of anatomy, pathology, diagnosis, and treatment. Theriogenology 2008, 70, 375–383. [Google Scholar] [CrossRef] [PubMed]
- Johnston, S.D.; Kamolpatana, K.; Root-Kustritz, M.V.; Johnston, G.R. Prostatic disorders in the dog. Anim Reprod Sci 2000, 60-61, 405–415. [Google Scholar] [CrossRef]
- Ryman-Tubb, T.; Lothion-Roy, J.H.; Metzler, V.M.; Harris, A.E.; Robinson, B.D.; Rizvanov, A.A.; Jeyapalan, J.N.; James, V.H.; England, G.; Rutland, C.S.; et al. Comparative pathology of dog and human prostate cancer. J Vet Med Sci 2022, 8, 110–120. [Google Scholar] [CrossRef]
- Del Magno, S.; Pisani, G.; Dondi, F.; Cinti, F.; Morello, E.; Martano, M.; Foglia, A.; Giacobino, D.; Buracco, P. Surgical treatment and outcome of sterile prostatic cysts in dogs. Vet Surg 2021, 50, 1009–1016. [Google Scholar] [CrossRef]
- Ruetten, H.; Wehber, M.; Murphy, M.; Cole, C.; Sandhu, S.; Oakes, S.; Bjorling, D.; Waller, K., 3rd; Viviano, K.; Vezina, C. A retrospective review of canine benign prostatic hyperplasia with and without prostatitis. Clin Theriogenology 2021, 13, 360–366. [Google Scholar]
- Polisca, A.; Troisi, A.; Fontaine, E.; Menchetti, L.; Fontbonne, A. A retrospective study of canine prostatic diseases from 2002 to 2009 at the Alfort Veterinary College in France. Theriogenology 2016, 85, 835–840. [Google Scholar] [CrossRef]
- Levy, X.; Nizanski, W.; von Heimendahl, A.; Mimouni, P. Diagnosis of common prostatic conditions in dogs: an update. Reprod Domest Anim 2014, 49, 50–57. [Google Scholar] [CrossRef]
- Palmieri, C.; Foster, R.A.; Grieco, V.; Fonseca-Alves, C.E.; Wood, G.A.; Culp, W.T.N.; Murua Escobar, H.; De Marzo, A.M.; Laufer-Amorim, R. Histopathological terminology standards for the reporting of prostatic epithelial lesions in dogs. J Comp Pathol 2019, 171, 30–37. [Google Scholar] [CrossRef]
- Christensen, B.W. Canine Prostate Disease. Vet Clin North Am Small Anim Pract 2018, 48, 701–719. [Google Scholar] [CrossRef] [PubMed]
- Cunto, M.; Ballotta, G.; Zambelli, D. Benign prostatic hyperplasia in the dog. Anim Reprod Sci 2022, 247, 107096. [Google Scholar] [CrossRef]
- Lea, C.; Walker, D.; Blazquez, C.A.; Zaghloul, O.; Tappin, S.; Kelly, D. Prostatitis and prostatic abscessation in dogs: retrospective study of 82 cases. Aust Vet J 2022, 100, 223–229. [Google Scholar] [CrossRef]
- Moses, W.B.; Tipler, A.E. Surgical excision and omentalisation of mineralised paraprostatic cysts with concurrent ureteroneocystostomy and perineal herniorrhaphy in a 9-year-old male entire Bearded Collie. Aust Vet J 2024. [Google Scholar] [CrossRef]
- Welsh, E.M.; Kirby, B.M.; Simpson, J.W.; Munro, E. Surgical management of perineal paraprostatic cysts in three dogs. J Small Anim Pract 2000, 41, 358–361. [Google Scholar] [CrossRef]
- Gill, S.S.; Barstad, R.D. A review of the surgical management of perineal hernias in dogs. J Am Anim Hosp Assoc 2018, 54, 179–187. [Google Scholar] [CrossRef] [PubMed]
- Sjollema, B.E.; Venker-van Haagen, A.J.; van Sluijs, F.J.; Hartman, F.; Goedegebuure, S.A. Electromyography of the pelvic diaphragm and anal sphincter in dogs with perineal hernia. Am J Vet Res 1993, 54, 185–190. [Google Scholar]
- Hosgood, G.; Hedlund, C.S.; Pechman, R.D.; Dean, P.W. Perineal herniorrhaphy: perioperative data from 100 dogs. J Am Anim Hosp Assoc 1995, 31, 331–342. [Google Scholar] [CrossRef]
- Brissot, H.N.; Dupré, G.P.; Bouvy, B.M. Use of laparotomy in a staged approach for resolution of bilateral or complicated perineal hernia in 41 dogs. Vet Surg 2004, 33, 412–421. [Google Scholar] [CrossRef]
- Ahlberg, T.M.; Jokinen, T.S.; Salonen, H.M.; Laitinen-Vapaavuori, O.M.; Molsa, S.H. Exploring the association between canine perineal hernia and neurological, orthopedic, and gastrointestinal diseases. Acta Vet Scand 2022, 64, 39. [Google Scholar] [CrossRef]
- Baines, S.; Aronson, L.; Johnston, S.; Tobias, K. Rectum, anus and perineum. In Veterinary Surgery: Small Animal, 2nd ed.; Johnston SJ, T.K., Ed.; Elsevier: St. Louis, Missouri, 2017; pp. 1783–1827. [Google Scholar]
- Burrows, C.F.; Harvey, C.E. Perineal hernia in the dog. J Small Anim Pract 1973, 14, 315–332. [Google Scholar] [CrossRef] [PubMed]
- Shaughnessy, M.; Monnet, E. Internal obturator muscle transposition for treatment of perineal hernia in dogs: 34 cases (1998-2012). J Am Vet Med Assoc 2015, 246, 321–326. [Google Scholar] [CrossRef]
- Zambelli, D.; Ballotta, G.; Valentini, S.; Cunto, M. Total Perineal Prostatectomy: A Retrospective Study in Six Dogs. Animals (Basel) 2022, 12. [Google Scholar] [CrossRef]
- Tobias, K.M.; Crombie, K. Perineal hernia repair in dorsal recumbency in 23 dogs: Description of technique, complications, and outcome. Vet Surg 2022, 51, 772–780. [Google Scholar] [CrossRef] [PubMed]
- Tobias, K.M.; Johnston, S.A. Veterinary Surgery: Small Animal - E-BOOK: 2-Volume Set; Elsevier Health Sciences, 2013. [Google Scholar]
- Bernarde, A.; Rochereau, P.; Matres-Lorenzo, L.; Brissot, H. Surgical findings and clinical outcome after bilateral repair of apparently unilateral perineal hernias in dogs. J Small Anim Pract 2018, 59, 734–741. [Google Scholar] [CrossRef]
- Hayashi, A.M.; Rosner, S.A.; de Assumpcao, T.C.; Stopiglia, A.J.; Matera, J.M. Retrospective study (2009-2014): perineal hernias and related comorbidities in bitches. Top Companion Anim Med 2016, 31, 130–133. [Google Scholar] [CrossRef]
- Heishima, T.; Asano, K.; Ishigaki, K.; Yoshida, O.; Sakurai, N.; Terai, K.; Seki, M.; Teshima, K.; Tanaka, S. Perineal herniorrhaphy with pedunculated tunica vaginalis communis in dogs: Description of the technique and clinical case series. Front Vet Sci 2022, 9, 931088. [Google Scholar] [CrossRef] [PubMed]
- Hatch, A.L.; Wallace, M.L.; Carroll, K.A.; Grimes, J.A.; Sutherland, B.J.; Schmiedt, C.W. Dogs neutered prior to perineal herniorrhaphy or that develop postoperative fecal incontinence are at an increased risk for perineal hernia recurrence. J Am Vet Med Assoc 2025, 1–6. [Google Scholar] [CrossRef]
- Freitag, T.; Jerram, R.M.; Walker, A.M.; Warman, C.G. Surgical management of common canine prostatic conditions. Compend Contin Educ Vet. 2007, 29, 656–658. [Google Scholar]
- Cunto, M.; Mariani, E.; Anicito Guido, E.; Ballotta, G.; Zambelli, D. Clinical approach to prostatic diseases in the dog. Reprod Domest Anim 2019, 54, 815–822. [Google Scholar] [CrossRef]
- Kamolpatana, K.; Johnston, G.R.; Johnston, S.D. Determination of canine prostatic volume using transabdominal ultrasonography. Vet Radiol Ultrasound 2000, 41, 73–77. [Google Scholar] [CrossRef] [PubMed]
- Sannamwong, N.; Saengklub, N.; Sriphuttathachot, P.; Ponglowhapan, S. Formula derived prostate volume determination of normal healthy intact dogs in comparison to dogs with clinical BPH. Proceeding of the 7th International Symposium on Canine and Feline Reproduction 2012, 226. [Google Scholar]
- Sirinarumitr, K.; Johnston, S.D.; Kustritz, M.V.; Johnston, G.R.; Sarkar, D.K.; Memon, M.A. Effects of finasteride on size of the prostate gland and semen quality in dogs with benign prostatic hypertrophy. J Am Vet Med Assoc 2001, 218, 1275–1280. [Google Scholar] [CrossRef]
- Snell, W.L.; Orsher, R.J.; Larenza-Menzies, M.P.; Popovitch, C.A. Comparison of caudal and pre-scrotal castration for management of perineal hernia in dogs between 2004 and 2014. N Z Vet J 2015, 63, 272–275. [Google Scholar] [CrossRef]
- Swieton, N.; Singh, A.; Lopez, D.; Oblak, M.; Hoddinott, K. Retrospective evaluation on the outcome of perineal herniorrhaphy augmented with porcine small intestinal submucosa in dogs and cats. Can Vet J 2020, 61, 629–637. [Google Scholar]
- Fossum, T.W. Small Animal Surgery Textbook - E-Book; Elsevier Health Sciences, 2012. [Google Scholar]
- Ahlberg, T.M.; Salonen, H.M.; Laitinen-Vapaavuori, O.M.; Molsa, S.H. CT imaging of dogs with perineal hernia reveals large prostates with morphological and spatial abnormalities. Vet Radiol Ultrasound 2022, 63, 530–538. [Google Scholar] [CrossRef]
- Grand JG, B.S., Monnet E. Effects of urinary bladder retroflexion and surgical technique on postoperative complication rates and long-term outcome in dogs with perineal hernia. J Am Vet Med Assoc. 2013, 243, 1442-1447. [CrossRef] [PubMed]
- Merchav, R.; Feuermann, Y.; Shamay, A.; Ranen, E.; Stein, U.; Johnston, D.E.; Shahar, R. Expression of relaxin receptor LRG7, canine relaxin, and relaxin-like factor in the pelvic diaphragm musculature of dogs with and without perineal hernia. Vet Surg 2005, 34, 476–481. [Google Scholar] [CrossRef]
- Haverkamp, K.; Harder, L.K.; Kuhnt, N.S.M.; Lupke, M.; Nolte, I.; Wefstaedt, P. Validation of canine prostate volumetric measurements in computed tomography determined by the slice addition technique using the Amira program. BMC Vet Res 2019, 15, 49. [Google Scholar] [CrossRef]
- McGill, J.; Thieman Mankin, K.M.; Parambeth, J.C.; Edwards, J.; Cook, A. Urine-Filled Large Prostatic Cystic Structure in Two Unrelated Male Miniature Dachshunds. J Am Anim Hosp Assoc 2018, 54, e54606. [Google Scholar] [CrossRef]
- Mantziaras, G. Imaging of the male reproductive tract: Not so easy as it looks like. Theriogenology 2020, 150, 490–497. [Google Scholar] [CrossRef] [PubMed]
- Phongphaew, W.; Kongtia, M.; Kim, K.; Sirinarumitr, K.; Sirinarumitr, T. Association of bacterial isolates and antimicrobial susceptibility between prostatic fluid and urine samples in canine prostatitis with concurrent cystitis. Theriogenology 2021, 173, 202–210. [Google Scholar] [CrossRef] [PubMed]
- Lee, A.J.; Chung, W.H.; Kim, D.H.; Lee, K.P.; Suh, H.J.; Do, S.H.; Eom, K.D.; Kim, H.Y. Use of canine small intestinal submucosa allograft for treating perineal hernias in two dogs. J Vet Sci 2012, 13, 327–330. [Google Scholar] [CrossRef] [PubMed]
- Zedda, M.T.; Bogliolo, L.; Antuofermo, E.; Falchi, L.; Ariu, F.; Burrai, G.P.; Pau, S. Hypoluteoidism in a dog associated with recurrent mammary fibroadenoma stimulated by progestin therapy. Acta Vet. Scand. 2017, 59, 55. [Google Scholar] [CrossRef]
- Szabo, S.; Wilkens, B.; Radasch, R.M. Use of polypropylene mesh in addition to internal obturator transposition: a review of 59 cases (2000-2004). J Am Anim Hosp Assoc 2007, 43, 136–142. [Google Scholar] [CrossRef]
- Grand, J.G.; Bureau, S.; Monnet, E. Effects of urinary bladder retroflexion and surgical technique on postoperative complication rates and long-term outcome in dogs with perineal hernia: 41 cases (2002-2009). J Am Vet Med Assoc 2013, 243, 1442–1447. [Google Scholar] [CrossRef]
- Weese, J.S.; Blondeau, J.; Boothe, D.; Guardabassi, L.G.; Gumley, N.; Papich, M.; Jessen, L.R.; Lappin, M.; Rankin, S.; Westropp, J.L.; et al. International Society for Companion Animal Infectious Diseases (ISCAID) guidelines for the diagnosis and management of bacterial urinary tract infections in dogs and cats. Vet J 2019, 247, 8–25. [Google Scholar] [CrossRef]
Figure 1.
The survival analysis of overall survival time from the duration of clinical signs before presented to diagnosis in the castrated (PHC) and non-castrated (PHNC) groups with no significant difference between the groups (p=0.079).
Figure 1.
The survival analysis of overall survival time from the duration of clinical signs before presented to diagnosis in the castrated (PHC) and non-castrated (PHNC) groups with no significant difference between the groups (p=0.079).
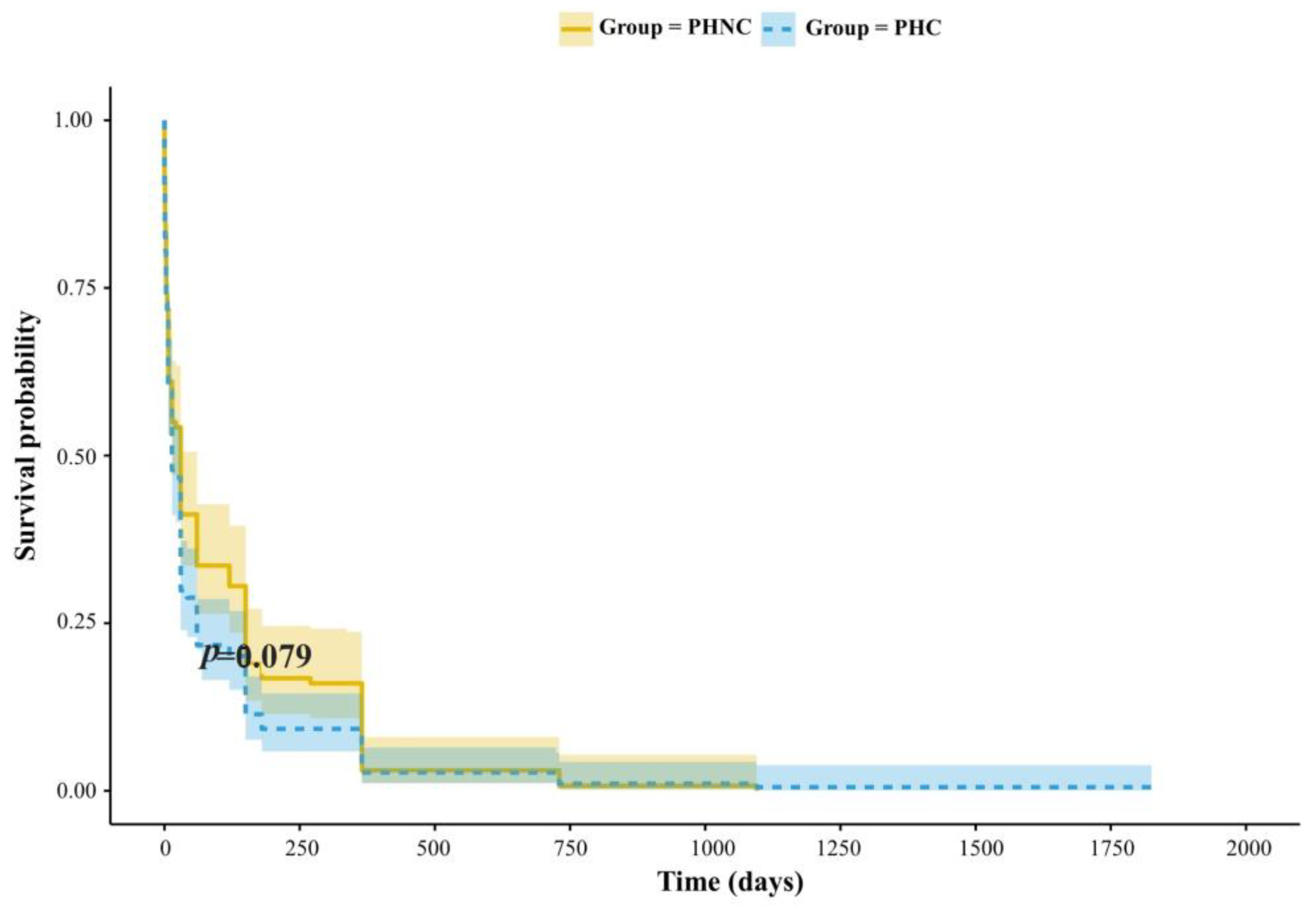
Figure 2.
The percentage of preoperative and postoperative (P/O) ultrasonographic results for prostate gland in perineal hernia (PH) dogs associated with prostatic disorders between the castrated (PHC) and non-castrated (PHNC) groups.3.2. Surgery.
Figure 2.
The percentage of preoperative and postoperative (P/O) ultrasonographic results for prostate gland in perineal hernia (PH) dogs associated with prostatic disorders between the castrated (PHC) and non-castrated (PHNC) groups.3.2. Surgery.
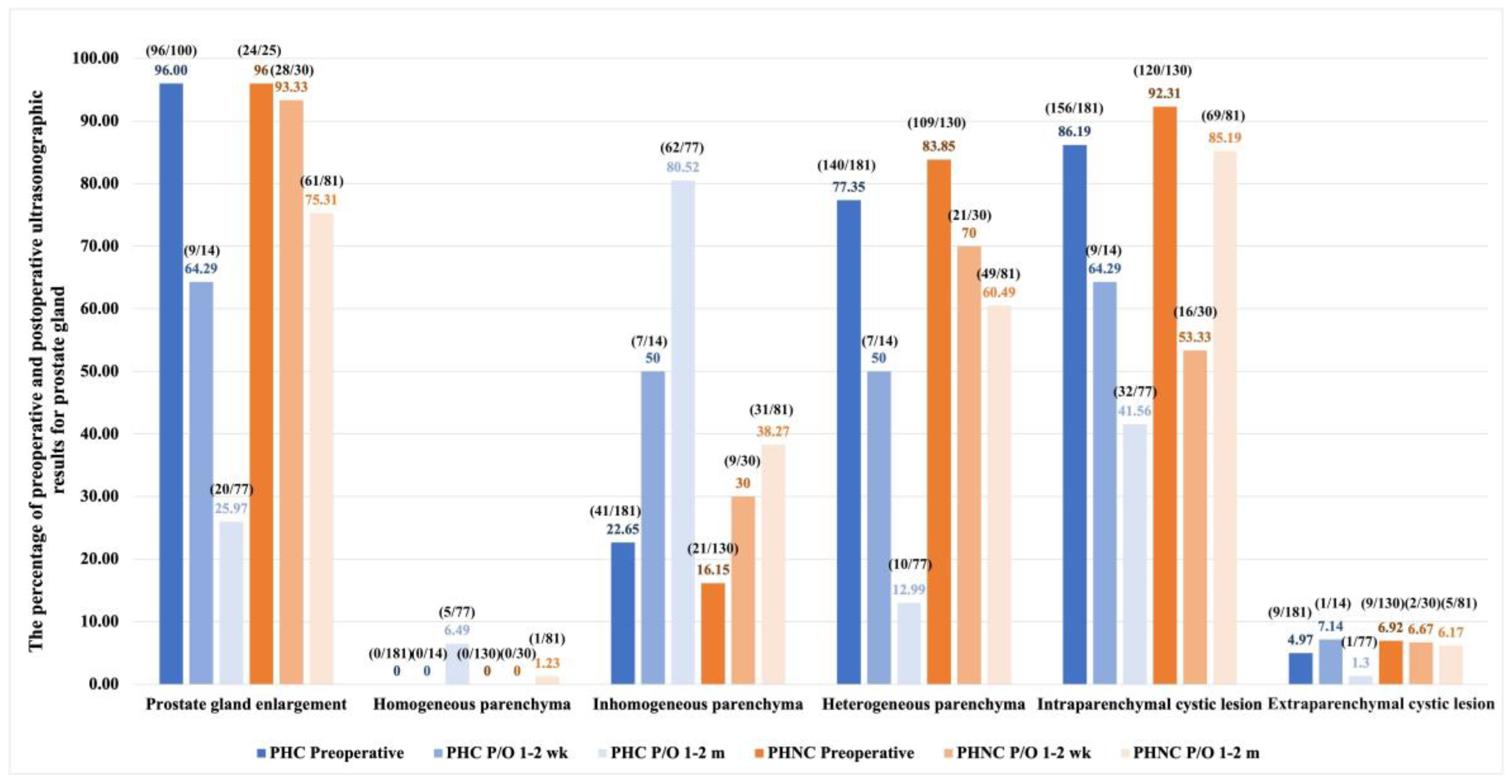
Figure 3.
The percentage of perineal hernia content at the time of surgery between the castrated (PHC) and the non-castrated (PHNC) groups.
Figure 3.
The percentage of perineal hernia content at the time of surgery between the castrated (PHC) and the non-castrated (PHNC) groups.
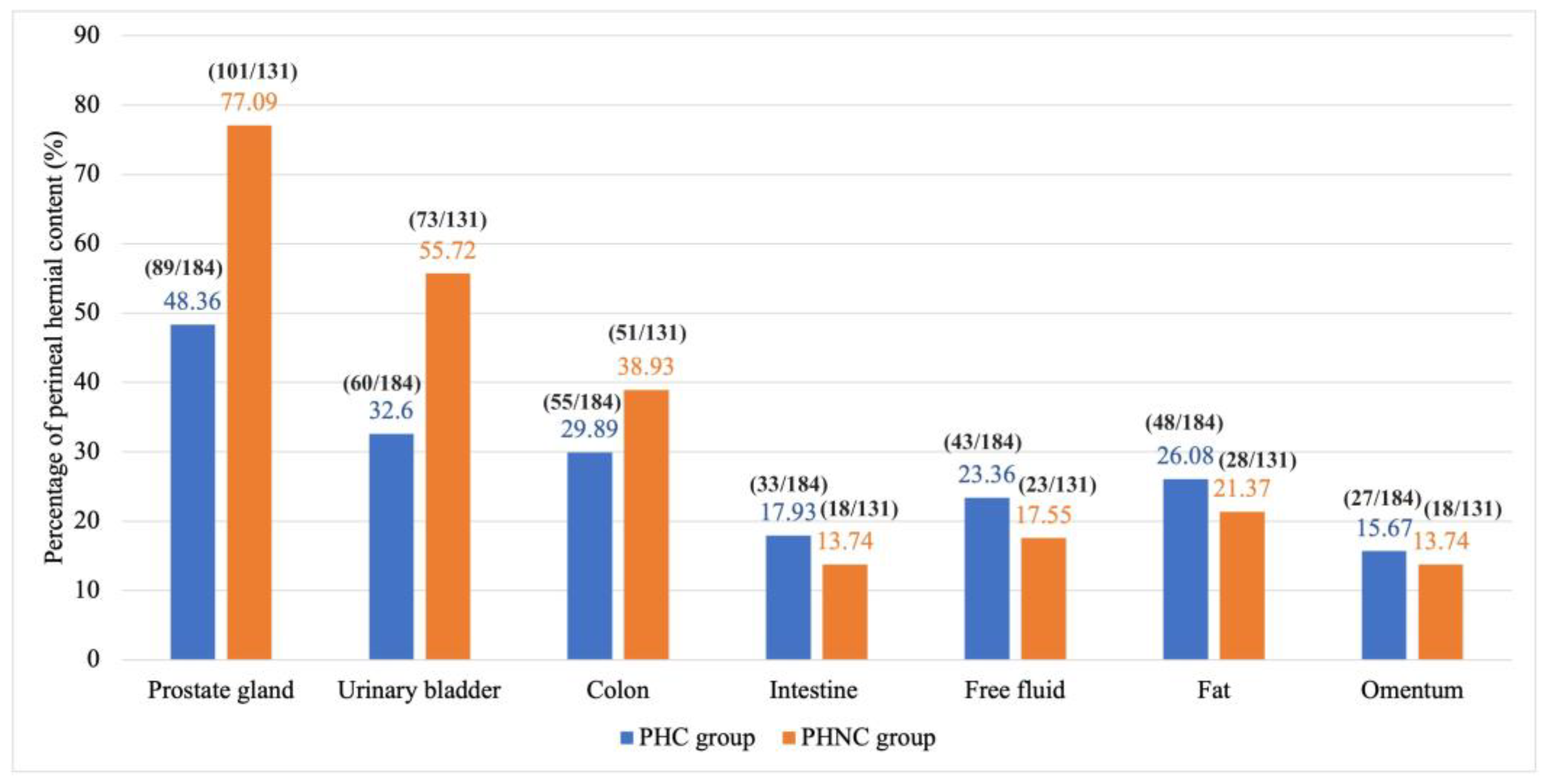
Figure 4.
The percentage of surgical techniques for perineal herniorrhaphy between the castrated (PHC) and the non-castrated (PHNC) groups.
Figure 4.
The percentage of surgical techniques for perineal herniorrhaphy between the castrated (PHC) and the non-castrated (PHNC) groups.
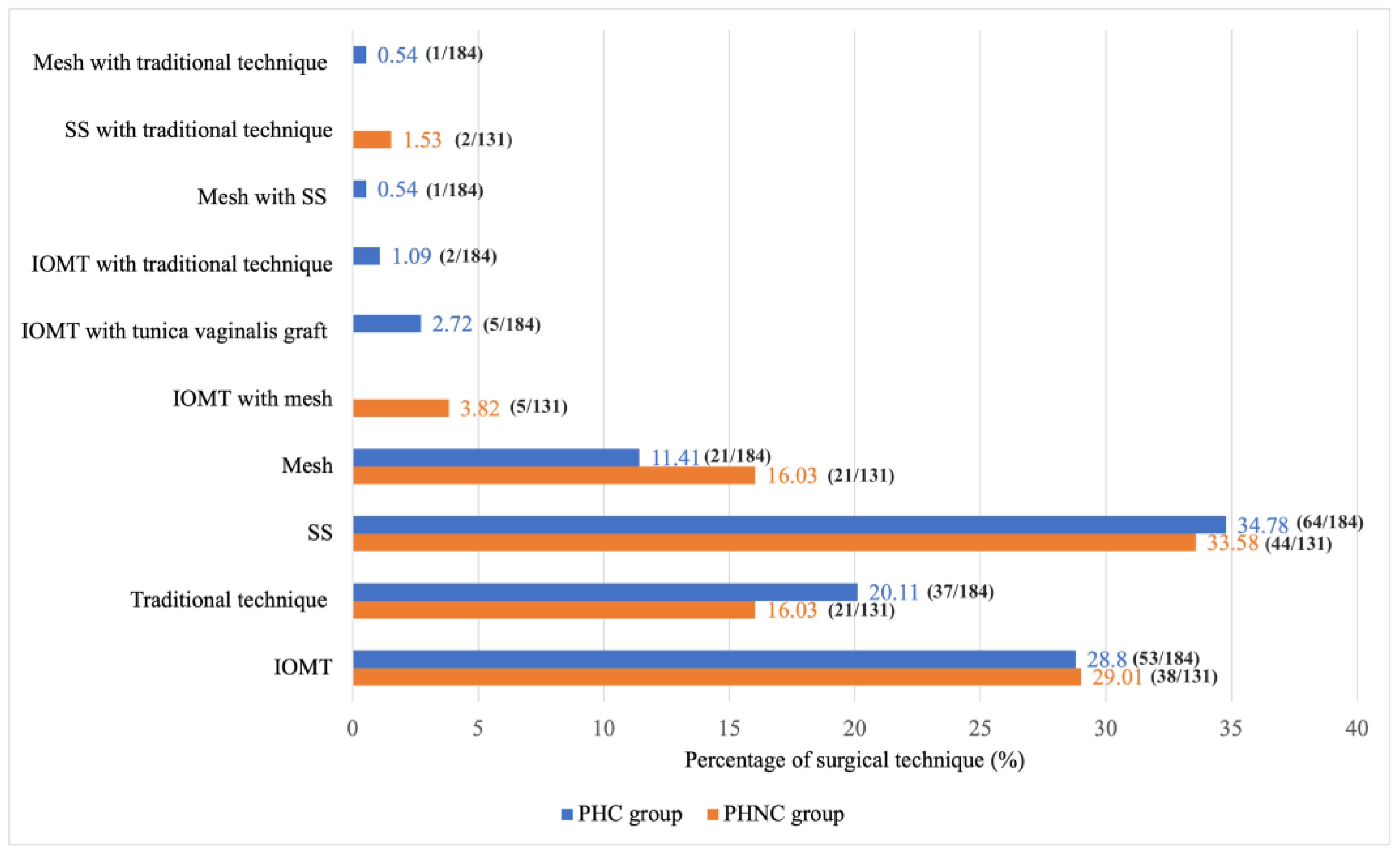
Figure 5.
The percentage of postoperative complications between the castrated (PHC) and the non-castrated (PHNC) groups.
Figure 5.
The percentage of postoperative complications between the castrated (PHC) and the non-castrated (PHNC) groups.
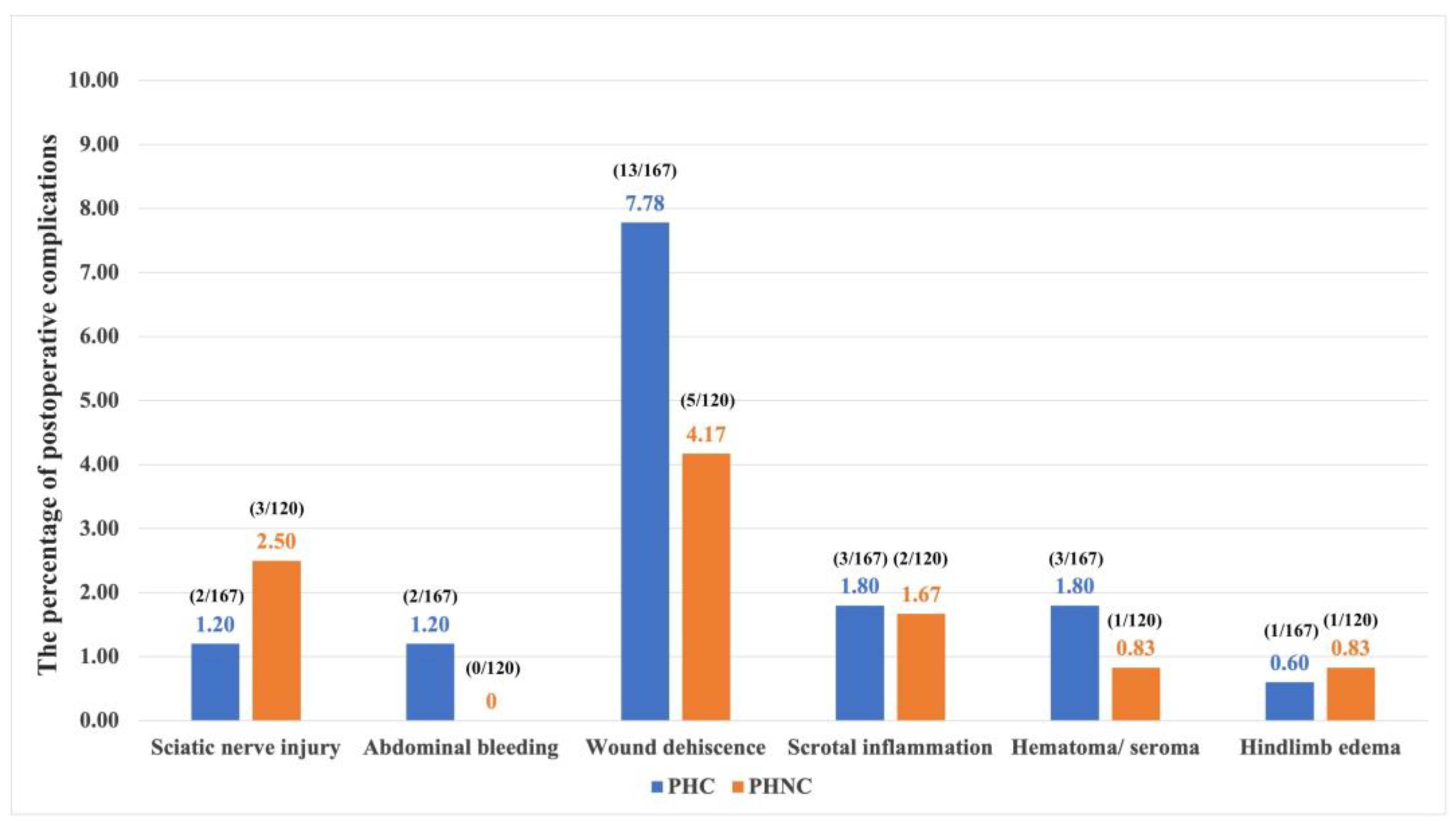
Figure 6.
The percentage of postoperative ultrasonographic outcomes for prostate gland in dogs with perineal hernia (PH) associated with prostatic disorders during the long-term phase between the castrated (PHC) and non-castrated (PHNC) groups, which are categorized into two subgroups: castrated within 2 months after perineal herniorrhaphy (PHNC-1) and castration after 2 months of follow-up (PHNC-2).
Figure 6.
The percentage of postoperative ultrasonographic outcomes for prostate gland in dogs with perineal hernia (PH) associated with prostatic disorders during the long-term phase between the castrated (PHC) and non-castrated (PHNC) groups, which are categorized into two subgroups: castrated within 2 months after perineal herniorrhaphy (PHNC-1) and castration after 2 months of follow-up (PHNC-2).
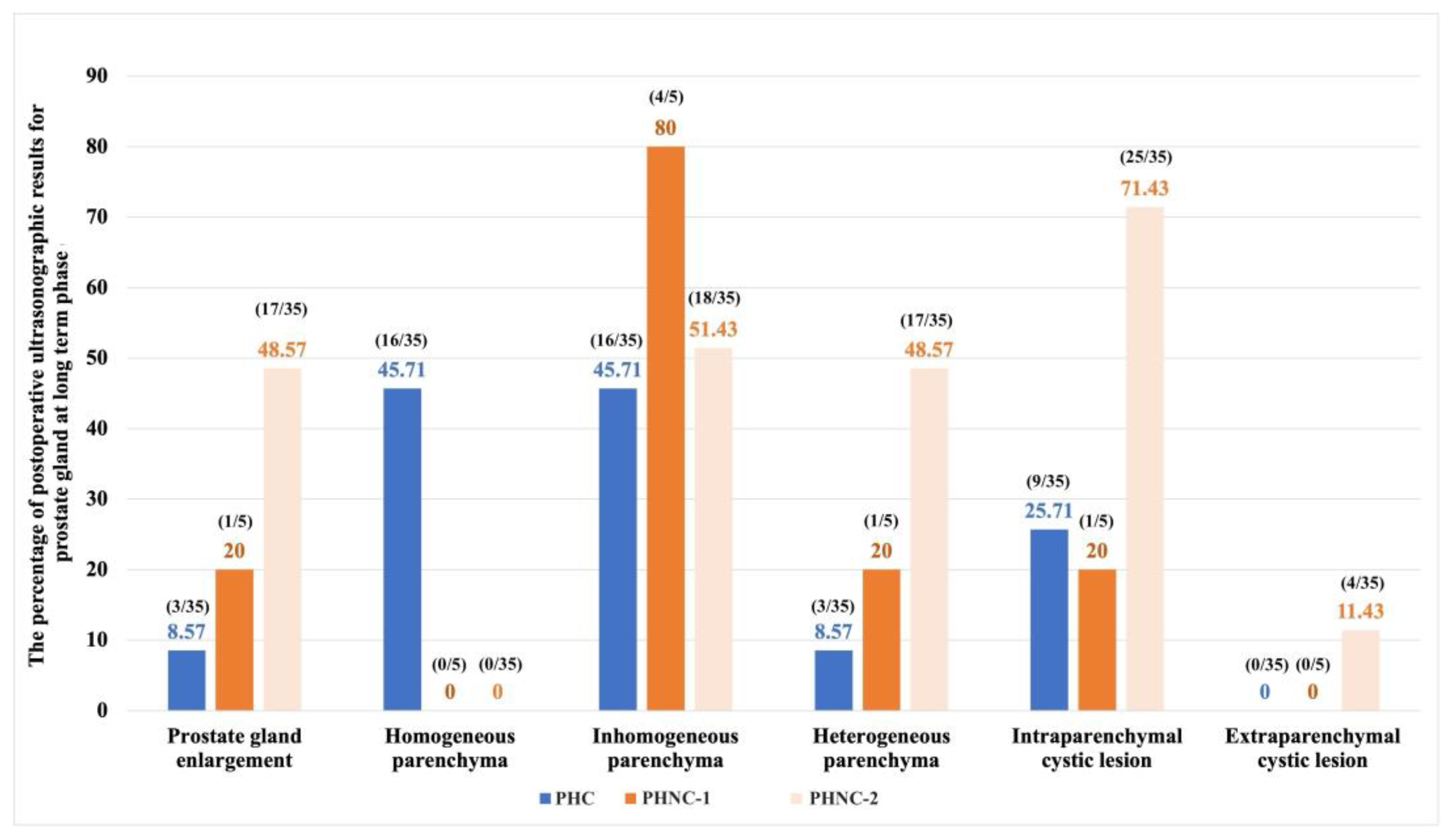
Figure 7.
The survival analysis of overall survival time from the duration of no recurrent perineal swelling post-surgery to the last follow-up between the castrated (PHC) and non-castrated (PHNC) groups, which are categorized into two subgroups: castrated within 2 months after perineal herniorrhaphy (PHNC-1) and intact or castration after 2 months of follow-up (PHNC-2) (no significant difference; p=0.34).
Figure 7.
The survival analysis of overall survival time from the duration of no recurrent perineal swelling post-surgery to the last follow-up between the castrated (PHC) and non-castrated (PHNC) groups, which are categorized into two subgroups: castrated within 2 months after perineal herniorrhaphy (PHNC-1) and intact or castration after 2 months of follow-up (PHNC-2) (no significant difference; p=0.34).
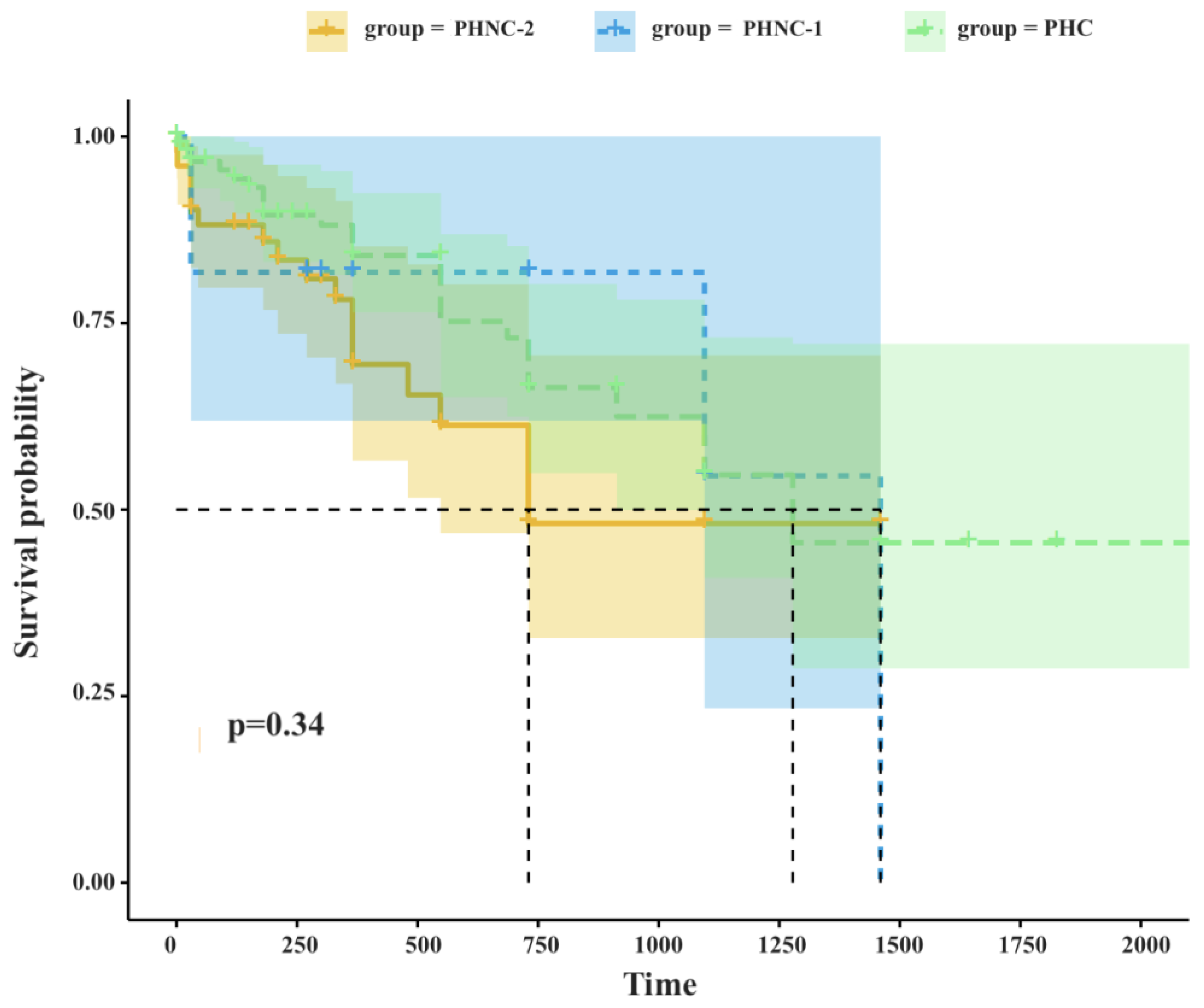

Table 1.
The percentage of pre-operative clinical signs from 315 perineal hernia (PH) dogs associated with prostatic disorders between the castrated (PHC) and the non-castrated (PHNC) groups.
Table 1.
The percentage of pre-operative clinical signs from 315 perineal hernia (PH) dogs associated with prostatic disorders between the castrated (PHC) and the non-castrated (PHNC) groups.
| Pre-operative clinical signs | PHC % (n=184) | PHNC% (n=131) |
|---|---|---|
|
Urogenital signs - Pollakiuria - Stranguria/ dysuria - Hematuria - Urinary incontinence - Bloody preputial discharge - Testis/ scrotal swelling |
2.71% (n=5) 14.13% (n=26) 4.89% (n=9) 7.60% (n=14) 1.08% (n=2) 1.63% (n=3) |
3.81% (n=5) 32.82% (n=43) 4.58% (n=6) 7.63% (n=10) 0.76% (n=1) 0% (n=0) |
|
Gastrointestinal signs - Anorexia - Vomiting - Diarrhea - Dyschezia - Tenesmus - Constipation - Small or ribbon-like-shaped feces - Hematochezia - Fecal incontinence - Rectal prolapse - Rectal tear |
13.58% (n=25) 14.13% (n=26) 14.67% (n=27) 64.67% (n=119) 52.71% (n=97) 9.23% (n=17) 14.67% (n=27) 10.32% (n=19) 0% (n=0) 1.63% (n=3) 1.08% (n=2) |
17.55% (n=23) 9.16% (n=12) 5.34% (n=7) 72.51% (n=95) 50.38% (n=66) 5.34% (n=7) 6.10% (n=8) 9.92% (n=13) 0.76% (n=1) 0% (n=0) 0.76% (n=1) |
|
Systemic signs - Sepsis - DIC - Azotemia |
0.54% (n=1) 0% (n=0) 18.47% (n=34) |
0% (n=0) 0% (n=0) 21.37% (n=28) |
|
Other - Perineal swelling - Perineal necrosis, severe inflammation - Perineal rupture - Hindlimb lameness |
100% (n=184) 9.23% (n=17) 2.17% (n=4) 1.08% (n=2) |
100 % (n=131) 8.39% (n=11) 0.76% (n=1) 0.76% (n=1) |
Table 2.
The postoperative outcome, complications, and follow-up between the castrated (PHC) and non-castrated (PHNC) groups are categorized into two subgroups: castrated within 2 months after perineal herniorrhaphy (PHNC-1) and intact or castration after 2 months of follow-up (PHNC-2).
Table 2.
The postoperative outcome, complications, and follow-up between the castrated (PHC) and non-castrated (PHNC) groups are categorized into two subgroups: castrated within 2 months after perineal herniorrhaphy (PHNC-1) and intact or castration after 2 months of follow-up (PHNC-2).
| Post-operative outcome | 1-2 weeks | 1-2 months | >6 months | ||||||||
|
PHC % (n/ total) |
PHNC % (n/total) |
PHC % (n/ total) |
PHNC % (n/total) |
PHC % (n/ total) |
PHNC-1 % (n/total) |
PHNC-2 % (n/total) |
|||||
| Urogenital system | |||||||||||
| - Pollakiuria | 0 (0/165) |
0 (0/115) |
0 (0/103) |
0 (0/90) |
0 (0/75) |
0 (0/7) |
0 (0/40) |
||||
| - Stranguria/ dysuria | 0.60 (1/165) |
0.86 (1/115) |
0 (0/103) |
1.11 (1/90) |
1.33 (1/75) |
14.29 (1/7) |
2.50 (1/40) |
||||
| - Hematuria | 0.60 (1/165) |
0.86 (1/115) |
0 (0/103) |
1.11 (1/90) |
1.33 (1/75) |
0 (0/7) |
2.50 (1/40) |
||||
| - Urinary incontinence | 4.24 (7/165) |
7.82 (9/115) |
1.94 (2/103) |
6.66 (6/90) |
6.66 (5/75) |
14.29 (1/7) |
7.50 (3/40) |
||||
| - Bloody preputial discharge | 0 (0/165) |
0 (0/115) |
0 (0/103) |
0 (0/90) |
0 (0/75) |
0 (0/7) |
0 (0/40) |
||||
| - Testis / scrotal swelling | 1.21 (2/165) |
1.74 (2/115) |
0.97 (1/103) |
0 (0/90) |
0 (0/75) |
0 (0/7) |
0 (0/40) |
||||
| - UTIs/ cystitis | 64.29 (9/14) |
80 (28/35) |
19.48 (15/77) |
41.98 (34/81) |
31.43 (11/35) |
20 (1/5) |
28.57 (10/35) |
||||
| - Cystic calculi/ sediment | 28.57 (4/14) |
26.67 (8/30) |
12.99 (10/77) |
29.63 (24/81) |
22.86 (8/35) |
40 (2/5) |
34.29 (12/35) |
||||
| - Ureter dilate | 0 (0/14) |
6.67 (2/30) |
0 (0/77) |
1.23 (1/81) |
0 (0/35) |
0 (0/5) |
0 (0/35) |
||||
| - Prostatic urethral dilate | 0 (0/14) |
0 (0/30) |
3.90 (3/77) |
0 (0/81) |
0 (0/35) |
0 (0/5) |
0 (0/35) |
||||
| - Hydronephrosis | 0.60 (1/14) |
0 (0/30) |
1.30 (1/77) |
0 (0/81) |
2.86 (1/35) |
0 (0/5) |
0 (0/35) |
||||
| - Urethral rupture | 0 (0/165) |
0 (0/115) |
0 (0/103) |
1.11 (1/90) |
0 (0/75) |
0 (0/7) |
0 (0/40) |
||||
| - UB rupture | 0 (0/165) |
0.86 (1/115) |
0 (0/103) |
0 (0/90) |
0 (0/75) |
0 (0/7) |
0 (0/40) |
||||
| Post-operative outcome | 1-2 weeks | 1-2 months | >6 months | ||||||||
|
PHC % (n/ total) |
PHNC % (n/total) |
PHC % (n/ total) |
PHNC % (n/total) |
PHC % (n/ total) |
PHNC-1 % (n/total) |
PHNC-2 % (n/total) |
|||||
| Gastrointestinal system | |||||||||||
| - Anorexia | 2.42 (4/165) |
2.60 (3/115) |
0.97 (1/103) |
2.22 (2/90) |
4 (3/75) |
0 (0/7) |
0 (0/40) |
||||
| - Vomiting | 3.03 (5/165) |
2.60 (3/115) |
0.97 (1/103) |
0 (0/90) |
0 (0/75) |
0 (0/7) |
0 (0/40) |
||||
| - Diarrhea | 3.63 (6/165) |
3.47 (4/115) |
0 (0/103) |
2.22 (2/90) |
0 (0/75) |
0 (0/7) |
2.12 (1/40) |
||||
| - Dyschezia | 0.60 (1/165) |
4.35 (5/115) |
0.97 (1/103) |
1.11 (1/90) |
5.33 (4/75) |
0 (0/7) |
6.38 (3/40) |
||||
| - Tenesmus | 3.03 (5/165) |
6.96 (8/115) |
1.94 (2/103) |
5.56 (5/90) |
4 (3/75) |
0 (0/7) |
6.38 (3/40) |
||||
| - Constipation | 0 (0/165) |
0 (0/115) |
0.97 (1/103) |
0 (0/90) |
2.67 (2/75) |
0 (0/7) |
0 (0/40) |
||||
| - Small or ribbon-like-shaped feces | 0 (0/165) |
0.86 (1/115) |
0.97 (1/103) |
0 (0/90) |
0 (0/75) |
0 (0/7) |
2.12 (1/40) |
||||
| - Hematochezia | 1.81 (3/165) |
0.86 (1/115) |
0 (0/103) |
1.11 (1/90) |
0 (0/75) |
0 (0/7) |
0 (0/40) |
||||
| - Fecal incontinence | 3.63 (6/165) |
2.60 (3/115) |
0.97 (1/103) |
4.44 (4/90) |
1.33 (1/75) |
0 (0/7) |
2.12 (1/40) |
||||
| - Rectal prolapse | 1.81 (3/165) |
5.21 (6/115) |
0.97 (1/103) |
0 (0/90) |
1.33 (1/75) |
0 (0/7) |
0 (0/40) |
||||
| - Rectal tear | 0 (0/165) |
0 (0/115) |
0 (0/103) |
0 (0/90) |
0 (0/75) |
0 (0/7) |
0 (0/40) |
||||
| Systemic signs | |||||||||||
| - Sepsis | 0.60 (1/165) |
0.86 (1/115) |
0 (0/103) |
0 (0/90) |
0 (0/75) |
0 (0/7) |
0 (0/40) |
||||
| - DIC | 0.60 (1/165) |
0 (0/115) |
0 (0/103) |
0 (0/90) |
0 (0/75) |
0 (0/7) |
0 (0/40) |
||||
| - Azotemia | 1.81 (3/165) |
2.60 (3/115) |
4.85 (5/103) |
2.22 (2/90) |
5.33 (4/75) |
0 (0/7) |
4.25 (2/40) |
||||
| - Pancreatitis | 0.60 (1/165) |
1.73 (2/115) |
0 (0/103) |
0 (0/90) |
0 (0/75) |
0 (0/7) |
0 (0/40) |
||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



