
Submitted:
04 March 2025
Posted:
04 March 2025
You are already at the latest version
Abstract
: This systematic review explores the neurophysiological principles underlying bilateral movement training (BMT) and interlimb coupling in post-stroke rehabilitation. A 10-year literature search yielded 199 studies, of which 28 met inclusion criteria for detailed analysis. These studies examined the effectiveness of BMT in enhancing motor recovery, promoting neuroplasticity, and improving functional outcomes. Interventions such as task-specific and rhythmic exercises, robotic assistance, sensory enhancement, and virtual reality were highlighted for their ability to address the complexities of motor recovery. The review underscores the role of neurophysiological mechanisms, including central pattern generators (CPGs), interhemispheric coupling, and cortical disinhibition, in facilitating functional improvements. Evidence shows that high-intensity BMT provides significant gains for individuals with moderate to severe impairments, while low-intensity training benefits early recovery stages or those with limited capacity. Despite short-term successes, these improvements’ sustainability and impact on long-term functional independence remain underexplored. Key gaps include a limited understanding of individualized responses to BMT, insufficient research on combined upper and lower limb training, and minimal integration of advanced technologies like robotics and virtual reality. Additionally, the psychosocial dimensions of rehabilitation, such as emotional well-being and patient engagement, are often overlooked despite their critical influence on recovery outcomes. This review advocates a paradigm shift towards personalized, evidence-based rehabilitation strategies that address these gaps. Stroke rehabilitation can achieve improved outcomes by leveraging the neurophysiological mechanisms of BMT and interlimb coupling and incorporating advanced tools and patient-centered approaches. Future research should prioritize longitudinal studies, technology integration, and stratified interventions tailored to individual needs to optimize neuroplasticity and enhance the quality of life for stroke survivors.
Keywords:
stroke rehabilitation
; post-stroke rehabilitation
; bilateral movement training
; cross-education
; interlimb coupling
; interlimb transfer
1. Introduction
Over the past two decades, a substantial body of research has significantly advanced our understanding of bilateral movement training, cross-education, and stroke rehabilitation, placing us at the forefront of this rapidly evolving field. This research is of paramount importance, as it underpins the effectiveness of these approaches in post-stroke motor recovery.
Bilateral movement training is a stroke rehabilitation approach involving using both limbs to perform symmetrical movements. This method leverages neural coupling between the brain hemispheres, promoting interhemispheric communication and synchronization to facilitate motor recovery in the affected limb [1,2]. Studies show that bilateral movement training can improve strength, dexterity, and functional use of the paretic limb, increasing neural network efficiency [3]. Bilateral movement training maximizes recovery outcomes, often integrated with task-specific training and technology-assisted interventions [4]. Cross-education in stroke rehabilitation refers to improvements in motor performance of the untrained limb when training the contralateral limb.
This concept is grounded in neural plasticity and interhemispheric transfer. It occurs due to bilateral motor cortices and transcallosal communication activation during unilateral exercise [5]. Cross-education is advantageous for patients with significant impairments in one limb, using the unaffected limb to drive recovery in the affected limb. Mechanisms include increased cortical excitability, enhanced motor unit recruitment, and improved coordination and strength in the untrained limb [6].
Harjpal et al. [7] and Stewart [2] underscore the increasing utilization and effectiveness of bilateral movement training in post-stroke motor recovery. Cauraugh [8] further supports this view, identifying that coupled protocols, such as combining bilateral training with EMG-triggered neuromuscular stimulation, demonstrated particularly significant effects. Liu et al. [9] cautions that not all rehabilitation methods, including bilateral arm training, have shown superiority over other methods and that combinations of methods can result in better outcomes. Timmermans et al. [10] emphasizes the exciting potential of integrating technology-assisted training with basic and clinical science research in stroke recovery and rehabilitation for improved outcomes.
Evidence suggests that bilateral movement therapy is an effective alternative for training affected limbs post-stroke, mainly when minimal or no active movement is possible. It is important to note that most studies on bilateral training have focused on the arms and hands.
Several authors have indicated that interlimb connections can yield positive training effects in stroke rehabilitation [11]. Other papers emphasizing the importance of interlimb coupling in stroke rehabilitation include Zehr et al. [12], who highlighted the significant impact of treatment studies, particularly for stroke. Li et al. [13] proposed a protocol for analyzing the clinical benefits of interlimb-coordinated intervention in gait recovery and rehabilitation. Maceira-Elvira et al. [14] and Arya et al. [15] explored advanced technologies in stroke rehabilitation, such as brain-computer interfaces and interlimb coupling protocols.
Although humans have adopted a hindlimb strategy for locomotion, the central nervous system retains a capacity for quadrupedal movement, utilizing all limbs synchronously. Numerous studies have examined the effectiveness of combined upper and lower limb movement training in stroke rehabilitation. Khan et al. [16] found that combining task-oriented approaches, occupational therapy, and physical therapy can be effective, while Keeling et al. [17] highlighted the potential benefits of integrating robotic rehabilitation with other therapeutic approaches. Hesse et al. [18] discussed the promise of robot-assisted rehabilitation, with Hesse noting its potential for both upper and lower limb rehabilitation. Cauraugh and Kang [19] and Hatem et al. [20] emphasized the importance of combined interventions, with Cauraugh and Kang specifically noting the benefits of coupled bilateral training. French et al. [21] and Yoon et al. [22] provided comprehensive overviews of various rehabilitation strategies, with French focusing on task-oriented repetitive training and Yoon highlighting the effectiveness of constraint-induced movement therapy and mirror therapy. However, research exploring the efficacy of interlimb coupling [15], including quadrupedal or crawling movements [23], as part of stroke rehabilitation strategy is sparse.
There is a need for a more precise description of interlimb coupling and bilateral movement training strategies and, more importantly, their underpinning neurophysiological concepts. Although several authors have shown that bilateral and interlimb strategies can produce favorable outcomes in stroke rehabilitation, most studies focus on bilateral movement training for the upper limbs [24]. Few have identified specific movement strategies or protocols that enhance existing bilateral and interlimb movement strategies [23,25]. For clinicians involved in stroke rehabilitation, it is not always clear which interlimb strategies and protocols are most effective and have the most potential to work alongside other therapeutic interventions based on the current collection of research. This gap in knowledge presents an exciting challenge and opportunity for further exploration and innovation in the field.
Therefore, the primary objective of this review is to highlight the neuro-physiological underlying principles of some of the most promising bilateral and interlimb movement strategies that led to positive clinical post-stroke rehabilitation outcomes.
2. Method
Search Strategy and Selection Criteria
A literature search was conducted per PRISMA guidelines to include papers published between 2014 and May 2024, using three databases: PubMed, Cochrane, and Google Scholar. This ten-year time frame was retained as an update of the previous ten-year period. The concepts of bilateral movement training, cross-education, interlimb coupling, and interlimb transfer started to appear in the literature in the early 2000s through the groundbreaking work of Whitall et al. [26], Cauraugh and Summers [27], and Stewart [2].
The three databases were chosen for several reasons, including that they are free and would enable readers to access the abstracts, at least, if not the full articles. They cover multidisciplinary, peer-reviewed journal articles in science, life, and biomedical sciences, medicine, robotics, and rehabilitation-related literature.
The databases were screened using the keywords stroke rehabilitation, post-stroke rehabilitation, bilateral movement training, cross-education, interlimb coupling, and interlimb transfer. The entire review protocol is shown in Figure 1 (PRISMA flow diagram for the search and selection process). A first screening process resulted in 134 articles on stroke rehabilitation, bilateral movement therapy, and cross-education and 65 studies on stroke rehabilitation, interlimb coupling, and interlimb transfer. and interlimb transfer.
Further inclusion criteria were applied to the 134 studies on stroke rehabilitation, bilateral movement training, and cross-education: humans, clinical trials, and stroke survivors. Exclusion criteria were reviews, meta-analyses, animal studies, unilateral training, and no training method or protocol described. These criteria narrowed the number of papers to 43 based on their abstracts. Twenty-six papers were further excluded after reading the full papers, which led to the retention of 17 post-stroke rehabilitation, bilateral movement training, and cross-education-related full papers.
The inclusion criteria applied to the 65 post-stroke rehabilitation, interlimb coupling, and interlimb transfer studies were as follows: humans, stroke survivors, clinical trials, and bilateral training protocols. Studies were excluded if no exercise protocol was described and unilateral training methods were used. These criteria reduced the number of papers to 21 based on their abstracts. Further exclusion of articles after reading the full papers brought the total down to 11 post-stroke rehabilitation, interlimb coupling, and interlimb transfer-related full papers being retained.
3. Results and Discussions
3.1. Bilateral Movement Training
Bilateral movement training (BMT) has gained prominence as a beneficial rehabilitation technique for stroke patients experiencing upper extremity hemiparesis. This approach involves the simultaneous movement of both arms, showing efficacy in enhancing motor function and facilitating recovery [2,28,29]. The definition of bilateral movement training was popularized by Cauraugh and Summers [27], who discuss the concept of bilateral movement training in their paper. They delve into the importance of this type of training, which involves coordinated movements of both sides of the body simultaneously or alternatingly. Although bilateral movement training is mainly used to describe bilateral upper limb training, recent research has also explored the efficacy of bilateral lower limb training for improving balance and walking in stroke survivors [7,30]. This paper will use bilateral movement training to describe bilateral upper and lower limb training protocols. Table 1 summarizes the specific definitions used throughout the paper.
The mechanisms underlying BMT include interlimb cross-transfer effects of upper and lower limbs and interlimb coupling between the upper and lower limbs, cortical disinhibition, increased recruitment of ipsilateral pathways, and the upregulation of descending commands [24,25,27].
Of particular interest are the significant positive outcomes of the various BMT protocols, such as rhythmic alternating movements used during bilateral arm training with rhythmic auditory cueing (BATRAC) and coupled bilateral training with EMG-triggered neuromuscular stimulation [8]. These protocols involve training methods that engage both limbs simultaneously, aiming to enhance motor function and coordination. Studies have shown that training with BATRAC and coupled bilateral and active stimulation protocols can substantially improve motor capabilities, particularly in individuals with stroke [8]. Functional multichannel neuromuscular electrostimulation has been highlighted as a practical approach to induce specific movements and improve upper extremity function in stroke patients [34].
Moreover, research by Cauraugh and Kim [32] indicated that coupled motor recovery protocols incorporating EMG-triggered neuromuscular stimulation and bilateral movement training resulted in superior motor improvement compared to unilateral training methods. This suggests that combining these techniques can lead to better outcomes in stroke rehabilitation. Additionally, a meta-analysis reported that combining EMG-triggered neuromuscular stimulation and bilateral training significantly enhanced upper limb function in chronic stroke patients [35].
Furthermore, the involvement of the reticulospinal system in neural coupling during bilateral hand movements has been investigated, indicating the importance of brainstem motor centers in coordinating such movements [36]. This neural coordination is crucial for optimizing motor recovery and functional outcomes in individuals post-stroke. Additionally, studies have shown that early initiation of FES-assisted gait training in stroke survivors can lead to improved functional outcomes and reduced therapy duration [37].
In summary, the integration of various BMT protocols, including BATRAC and coupled bilateral training with EMG-triggered neuromuscular stimulation, has shown promise in promoting motor recovery and functional improvements in individuals with stroke. These protocols target bilateral coordination, muscle activation, and neural coupling, all essential for enhancing motor function post-stroke.
Other research indicates that BMT can improve upper limb function in chronic stroke patients [29,38]. While both bilateral and unilateral training offer benefits, bilateral training may be superior for enhancing shoulder motion and upper limb strength [29,39]. Conversely, unilateral training may improve unilateral jumping performance and activities of daily living [39,40]. Both methods appear equally effective for lower limb function and horizontal movement performance [41]. Bilateral arm training has significantly improved motor impairment, as assessed by the Fugl-Meyer Assessment [42]. The choice between bilateral and unilateral training should align with specific rehabilitation goals, with a combined approach potentially offering the most comprehensive benefits and providing reassurance about the adaptability of BMT in stroke rehabilitation [2,7].
Bilateral movement training simultaneously engages the affected and unaffected limbs, promoting motor function and recovery post-stroke. Over the past decade, studies have highlighted the effectiveness of BMT in stroke rehabilitation, demonstrating significant upper limb recovery [43,44]. BMT is associated with increased activation of the non-affected motor cortex during movements, reflecting its impact on neural processes [45]. Robotic systems have also gained attention for their potential to enhance post-stroke motor rehabilitation [46].
The benefits of BMT extend to various aspects of stroke recovery, facilitating functional motor recovery of the upper extremities [47], promoting rapid motor performance improvements, and enhancing movement quality after an ischemic infarct in the motor cortex [48]. Bilateral priming has been shown to enhance the efficacy of movement therapy, especially for patients with low motor function post-stroke [49]. The significant improvements in motor performance, especially when combined with general occupational therapy, should encourage and motivate healthcare professionals and stroke patients about the potential of BMT in stroke rehabilitation [48].
Additionally, sequencing bilateral and unilateral task-oriented training has been suggested to enhance arm and hand function gains in individuals with moderate to severe paresis post-stroke [50]. This sequential combination significantly increases motor cortex activation during hand movement, highlighting its potential to improve functional outcomes [50].
While some studies have shown promising results in using bilateral movement training to expedite progress in upper limb recovery post-stroke [51], there is also critical research that questions the efficacy of this approach. One study by Syed et al. [52] found that while bilateral extremity training improved the amount of arm usage, the quality of movement did not significantly improve. This suggests that while bilateral training may increase the overall use of the arms, it may not necessarily enhance the quality of movement, which is crucial for functional recovery.
Moreover, Shih et al. [53] highlighted inconsistent results in longitudinal studies regarding bilateral movement rehabilitation approaches such as BATRAC and Bilateral Arm training (BBT). This inconsistency in outcomes raises concerns about the reliability and effectiveness of bilateral training methods. Additionally, Dembele et al. [43] conducted a meta-analysis comparing the effects of bilateral and unilateral training in (sub)acute stroke and found that integrating high-dosage bilateral movements may not significantly improve the quality of upper limb recovery after stroke.
Furthermore, while some research has suggested that bilateral training can improve motor recovery and functional laterality [2], other studies have raised doubts about the extent of these benefits. For instance, Wang et al. [54] indicated that the effect of bilateral training on subsequent unilateral performance is robust but may not be sensitive to the context of bilateral training. This suggests that while bilateral training may have some transfer effects on unilateral performance, the specificity and magnitude of these effects may vary. Moreover, Wu et al. [55] found that distributed constraint-induced therapy, which focuses exclusively on unilateral training, resulted in similar improvements in movement smoothness compared to bilateral arm training. This challenges the notion that bilateral training is superior to unilateral training in all motor control and recovery aspects. Additionally, Langan et al. [56] suggested that the influence of the task itself plays a significant role in interlimb coordination, indicating that the type of movement involved in bilateral training protocols may impact their effectiveness.
3.1.1. Neurophysiological Processes Underpinning Bilateral Movement Training
The research cited in this systematic review emphasizes the positive outcomes of various BMT protocols, such as BATRAC and coupled bilateral training with EMG-triggered neuromuscular stimulation [57]. To comprehend the underlying neurophysiological mechanisms of these interventions, it is crucial to explore sensorimotor coupling in humans, the effects of bilateral movement training, and interlimb coupling in post-stroke rehabilitation. Table 2 summarizes the effects of BMT and interlimb coupling in post-stroke rehabilitation and summarizes neuro-physiological mechanisms underpinning training effectiveness. Studies have demonstrated that rhythmic attentional sampling is a critical neurophysiological mechanism that can resolve conflicts in decision-making processes [58]. Additionally, electroencephalography experiments have unveiled the connection between action planning and perceptually relevant neuronal oscillations, shedding light on the neurophysiological basis of this coupling [59].
The ability to synchronize movements with external rhythms, such as music, is a fundamental aspect of human experience and has been extensively studied across various disciplines, including neuroscience, psychology, and movement sciences. This synchronization, often called sensorimotor synchronization, is crucial for understanding motor timing and reward processes, particularly in clinical populations affected by conditions like Parkinson’s disease and stroke [60,61]. Research has shown that the capacity to align movements with rhythmic stimuli is a fundamental human ability and a complex interplay of neural mechanisms that can be disrupted in certain neurological conditions [60].
Central Pattern Generators (CPGs) are neural mechanisms that play a significant role in controlling rhythmic movements in both animals and humans. These networks can produce rhythmic outputs without sensory feedback, which is essential for various motor activities such as walking and breathing [62,63,64]. Studies have highlighted the importance of CPGs in understanding how the brain regulates rhythmic movements, emphasizing their role in generating motor patterns that can be modulated by external cues [65-67]. Furthermore, interhemispheric interactions between cortical motor areas have been shown to mediate the modulation of excitability in motor pathways during rhythmic movements, indicating a sophisticated level of neural coordination [68,69].
The research surrounding sensorimotor synchronization and CPGs has implications for understanding not only essential motor control but also the underlying neural mechanisms that can be affected by neurological disorders. For instance, the ability to synchronize movements can be impaired in individuals with Parkinson’s disease, where the disruption of the basal ganglia and associated neural circuits can lead to difficulties in movement initiation and coordination [60,61,67]. Understanding these mechanisms is crucial for developing therapeutic interventions to improve motor function in affected populations [70].

Table 2.
Effects of Bilateral Movement Training, Interlimb Coupling in Post-Stroke Rehabilitation, and Potential Neurophysiological Mechanisms Underpinning Intervention Effect.
Table 2.
Effects of Bilateral Movement Training, Interlimb Coupling in Post-Stroke Rehabilitation, and Potential Neurophysiological Mechanisms Underpinning Intervention Effect.
| Intervention Type & Authors | Participants(Sex/Number/Age) | Measurement(s) | Effect on Stroke Condition | Neurophysiological, Interlimb Coupling, and Transfer Effects * | No. of Potential Facilitating Neurophysiological Mech. |
|---|---|---|---|---|---|
| I. BILATERAL ARM TRAINING | |||||
| Bruyneel, et al. [71] | n/a-15 poststroke 17 healthy volunteers-n/a | CMSA/Levin Scale/Ashworth/Semmes-Weinstein/Box and Blocks | Bilateral pushing with gradual efforts induces impaired postural strategies and coordination between limbs in individuals after a stroke. | 1, 2, 3, 4, 5, 7 and 8 | 7 |
| Dhakate, D., & Bhattad, R. [72] | n/a-40 post-stroke subjects-45–65 | FIM (Functional Independence Measure) and FMA UE (Fugl-Meyer et al.) | Bilateral Arm Training proved more effective than the Conventional Training program in improving affected upper extremity motor function. | 1, 2, 3, 4, 5, 6 and 8 | 7 |
| Duff, et al. [73] | M/F, 20 post-stroke/20 healthy controls | Adult Assisting Hand Assessment (Ad-AHA Stroke) and UE Fugl-Meyer (UEFM) | Algorithm and sensor data analyses distinguished task types within and between groups and predicted clinical scores. | 1, 2, 3, 4, 5, 6, 7 and 8 | 8 |
| Han, K. J., & Kim, J. Y. [29] | n/a, 30 post-stroke subjects, n/a | FMA UE/ Box and Blocks/ MBI (Modified Barthel Index | In both the experimental and control groups, the FMA, BBT, and MBI scores were significantly higher after the intervention than before the intervention (p < 0.05). The changes in the FMA, BBT, and MBI scores were more significant in the experimental group than in the control group (p < 0.05). | 1, 2, 3, 4, 5, 6 and 8 | 7 |
| Itkonen, M., et al. [74] | M/F, 11 post-stroke subjects, 52–90 |
Surface EMG measurements | The paretic arms of the patients were more strongly affected by the task conditions compared with the non-paretic arms. These results suggest that in-phase motion may activate neural circuits that trigger recovery. | 1, 2, 3, 4, 5, 7 and 8 | 7 |
| Kim, N., et al. [75] | n/a, 13 hemiparetic stroke patients and 12 healthy participants), n/a | EMG data | The upper extremity muscle activities of stroke patients during bimanual tasks varied between the paretic and non-paretic sides. Interestingly, the non-paretic side muscle activities also differed from regular participants. | 1, 2, 3, 4, 5, 6 and 8 | 7 |
| Kumagai, M., et al. [76] | M/F, 24 subjects, n/a | NHPT, Purdue Pegboard task, Box and Blocks test, FMA UE | Alternating bilateral training may augment training effects and improve upper-limb motor function in patients with left hemiparesis. | 1, 2, 3, 4, 5, 6 and 8 | 7 |
| Lee, M. J., et al. [38] | M/F, 15 pos stroke, 15 healthy, n/a | FMA UE, Box and Blocks test, MBI | Bilateral arm training and general occupational therapy might be more effective than alone for improving upper limb function and ADL performance. | 1, 2, 3, 4, 5, 6 and 8 | 7 |
| Meng, G., et al. [77] | M/F, 128 subjects | FMA UE and Action research Reach Test Secondary: Neurophysiological improvement TMS | Hand-arm intensive bilateral training significantly improved motor functional and neuro-physiological outcomes in patients with acute stroke. | 1, 2, 3, 4, 5, 6 and 8 | 7 |
| Kaupp, C., et al. [24] | M/F, 19 subjects, 57–87 y/o | MAS, Chedoke, Monofilaments sensory discrimination, Berg Balance Test | Results show significant changes in function and neurophysiological integrity. | 1, 2, 3, 4, 5, 8, 13, 14 and 15 | 9 |
| II. BILATERAL ARM TRAINING AND SENSORY ENHANCEMENT | |||||
| Lin, C.H, et al. [78] | M/F, 33 subjects, mean age = 55.1 ± 10.5, | BI, FMA UE, WMFT, MAS | Computer-aided interlimb force coupling training improves the motor recovery of a paretic hand. It facilitates motor control and enhances functional performance in the paretic upper extremity of people with chronic stroke. | 1, 2, 3, 4, 5, 6, 7, 8, 9 and 11 | 9 |
| Rodrigues, L. C., et al. [79] | M/F, 26 subjects, n/a | The primary outcome measure was unilateral and bilateral UL activity according to the Test d’Évaluation des Membres Supérieurs de Personnes Âgées (TEMPA). | The total TEMPA score showed the main effect of time. Significant improvement was found for bilateral but not unilateral tasks. Both groups showed gains after training, with no differences between them. | 1, 2, 3, 4, 5, 7 and 8 | 7 |
| Song, G. B. [80]. | M/F, 40 subjects, mean age 51.15 ± 14.81 years, | Box and Block test (BBT), Jebsen Taylor test (JBT), and Modified Barthel Index (MBI) | Upper limb function and the ability to perform activities of daily living improved significantly in both groups. Although there were significant differences between the groups, the task-oriented group showed more remarkable improvement in upper limb function and activities of daily living. | 1, 2, 3, 4, 5, 6, 7, 8, 9 and 17 | 10 |
| Van Delden, A. L. E. Q, et al. [81] | M/F, 60 subjects, n/a | Potentiometer, smoothness, and harmony mean amplitude and bimanual coordination measurements. | The coupling between both hands was not significantly higher after bilateral than unilateral training and control treatment. BATRAC group showed greater movement harmonicity and larger amplitudes. | 1, 2, 3, 4, 5, 7, 8, 9 and 17 | 9 |
| III. BILATERAL ARM TRAINING AND ROBOTICS | |||||
| Abdollahi, F., et al. [82] | M/F, 26 subjects, 26–77 y/o | FMA/ Wolf Motor Functional Ability Scale (WMFAS)/Motor activity log | Subjects’ 2-week gains in Fugl-Meyer score averaged 2.92, and we also observed improvements in Wolf Motor Functional Ability Scale average of 0.21 and Motor Activity Log of 0.58 for quantity and 0.63 for quality of life scores. | 1, 2, 3, 4, 5, 8, 9, 10, 11 and 16 | 10 |
| Huang, J. J., et al. [83] | n/a, 40 subjects, n/a | EEG measurements | The results showed that stroke duration might influence the effects of hand rehabilitation in bilateral cortical corticocortical communication with significant main effects under different alpha and beta band conditions. | 1, 2, 3, 4, 5, 6, 8, 9 and 10 | 9 |
| Li, Y. C., et al. [13] | F/M, 72 subjects, 20 to 80 y/o |
FMA UE/MAS/ABIL hand stroke impact scale/lateral pinch/accelerometer | Only between-group differences were detected for the primary outcome, FMA-UE. R-mirr enhanced upper limb motor improvement more effectively, and the effect could be maintained at 3 months of follow-up. | 1, 2, 3, 4, 5, 6, 8, 9 and 16 | 9 |
| IV. BAT. AND VIRTUAL REALITY/VIDEO GUIDANCE | |||||
| Jayasinghe, S. A., et al. [84] | M/F, 15 stroke survivors and seven age-matched neurologically intact adults, 45–79 y/o | Fugl-Meyer, Jebsen Taylor | Chronic stroke survivors with mild hemiparesis show significant deficits in reaching aspects of bilateral coordination, However, there are no deficits in stabilizing against a movement-dependent spring load. |
1, 2, 3, 4, 5, 8 | 6 |
| V. BILATERAL LEG TRAINING | |||||
| Ardestani, et al. [85] | M/F, 50 subjects, 18–85 y/o | FMA UE, Changes in spatiotemporal, joint kinematics, and kinetics plus heart physiology variables were measured | High-intensity LT results in greater changes in kinematics and kinetics than lower-intensity interventions. The results may suggest greater paretic-limb contributions. | 1, 2, 3, 4, 5, 6, 8, 12, 13 and 15 | 10 |
| Jo, P. Y. [86] | M/F, 20 subjects, n/a | The primary clinical measure was a 10-m walk time. Additional measures were the Timed and test and the Stroke Impact Scale 3.0 | Interlimb symmetry and knee-ankle Variability post-stroke relate to walking performance. Interlimb angle-angle asymmetry does not relate to walking performance post-stroke. | 1, 2, 3, 4, 5, 6, 8, 12, 13 and 15 | 10 |
| VI. BILATERAL LEG TRAINING PLUS SENSORY ENHANCEMENT | |||||
| Kwong, P.W.H., et al. [87] | M/F, 72 subjects, 55–85 y/0 | The muscle strength of paretic ankle dorsiflexors (pDF) and plantarflexors (pPF) and paretic knee extensors (pKE) and flexors (pKF) were selected as the primary outcome measures of this study. | The application of bilateral TENS over the common peroneal nerve combined with TOT was superior to that of unilateral TENS combined with TOT in improving paretic ankle dorsiflexion strength. | 1, 2, 3, 4, 5, 6, 7, 8, 9 and 12 | 10 |
| VII. COMBINED BILATERAL ARM AND LEG TRAINING | |||||
| Arya et al. [15] | M/F, 50 subjects, n/a | The outcome measures were feasibility of activities, Fugl-Meyer assessment (FMA), Rivermead visual gait assessment (RVGA), Functional ambulation category (FAC), and modified Rankin scale (mRS). | The interlimb coupling training, a feasible program, may enhance stroke recovery of the upper and lower limbs and gait. | 1, 2, 3, 4, 5, 6, 7, 8, 12, 13, 14, 15 and 16 | 13 |
| VIII. BILATERAL RHYTHMIC LEG AND ARM TRAINING | |||||
| Klarner, T., et al. [25] | M/F, 19 subjects, 45–86 y/o | Test for muscle tone (modified Ashworth), functional ambulation (FAC), physical impairment (Chedoke–McMaster scale), touch discrimination (monofilament test), and reflex function for stroke participants. | Arm and leg cycling training induces plasticity and modifies reflex excitability after stroke. | 1, 2, 3, 4, 5, 8, 12, 13, 14 and 15 | 10 |
| IX. BILATERAL MOVEMENT PRIMING | |||||
| Stoykov, M. E., et al. [88] | F/M, 76 subjects, | The primary outcome measure is the Fugl-Meyer Test of Upper Extremity Function. The secondary outcome is the Chedoke Arm and Hand Activity Index-Nine, an assessment of bimanual functional tasks. | The first large-scale clinical trial of bilateral priming plus task-specific training. The authors have previously completed a feasibility intervention study of bilateral motor priming plus task-specific training and have considerable experience using this protocol. Outcome follows. | 1, 2, 3, 4, 5, 8, 9, 13, 15 and 16 | 10 |
* 1. Engaging both hemispheres and reducing inhibition in the affected cerebral cortex, leveraging interhemispheric coupling and neural cross-talk [89]. 2. Bilateral arm training induces more trunk muscle contractions, leading to better control of the proximal upper extremity and facilitating the expression of brain-derived neurotrophic factors and brain function remodeling [89]. 3. Facilitating neuroplasticity [89]. 4. Intact neural circuits within the spinal cord remain relatively unimpaired and accessible [89]. 5. The maintenance of spatial and temporal coupling after stroke is often (partially) intact and can be used in stroke rehabilitation [90]. 6. Applying meaningful, motivated tasks [90]. 7. In-phase motion of bilateral training causes more muscle synergy, especially in the affected arm [74]. 8. Transferability of skills acquired through bilateral training to unilateral tasks [54]. 9. Sensory enhancement can amplify interlimb reflexes and enhance motor learning and coordination. Sensory enhancement can modulate functional connectivity in sensory-motor networks and improve sensorimotor adaptation [91]. 10. Passive robot-controlled arm movements and proprioceptive decision-making and feedback have been shown to modulate functional connectivity in sensory-motor networks and enhance sensorimotor adaptation [91]. 11. Adding virtual reality and video guidance targets motor function and stimulates cognitive and perceptual processes, providing a more comprehensive approach to rehabilitation [92,93]. 12. Bilateral leg movement training has been associated with increased activation of the non-affected motor cortex during paretic leg movements, indicating neuroplastic changes [45]. 13. Antiphase oscillatory effects on central pattern generators (CPGs) [15]. Central pattern-generating networks (CPGs) are believed to be central to spinal circuits, assisting in producing rhythmic coordinated movements of all four limbs [23]. 14. Quadrupedic interlimb transfer with arm training: Rhythmic movements of the arms impact reflexes in the lower limbs, resulting in both inhibitory [94,95] and facilitative effects [96]. 15. Interlimb coupling effects can facilitate bilateral motor output during rhythmic leg cycling after stroke [12]. Active rhythmic arm movements have been found to modulate the corticospinal drive to the legs, suggesting a potential mechanism for enhancing bilateral motor function [97]. 16. Bilateral movement priming increases corticomotor excitability in the primary motor cortex [98] and improves motor learning and recovery [99]. 17. Rhythmic auditory cues can significantly improve gait parameters and motor performance in individuals with neurological conditions like stroke and Parkinson’s disease [100].
3.1.2. Bilateral Arm Training
Bilateral upper extremity movement training, primarily focusing on arm and hand exercises, has been extensively studied for its effectiveness in enhancing motor activity and function in individuals with hemiplegia or stroke. This training emphasizes synchronizing and coordinating movements in both limbs simultaneously (Syed et al., 2015). It typically involves repetitive practice of identical bilateral arm movements in symmetrical or alternating patterns, as well as bimanual training where both limbs perform different tasks [43].
Over the last two decades, bilateral upper extremity movement training has emerged as an effective intervention for stroke rehabilitation. Numerous studies have demonstrated its efficacy in improving motor function and recovery [2,8,19,28,29,50,72,101,102]. Various bilateral upper extremity training protocols, including alternating hand movements, movements preceded by bilateral robotic motor priming, meaningful daily task training, and error-augmented task training, have been investigated, further validating the approach [29,72,76,82,103].
Recent research on bilateral arm training (BAT) has expanded our understanding of effective interventions for post-stroke rehabilitation [103]. Studies have incorporated bilateral hand movement training [77,78,82,83] and have focused on the effects of bilateral arm interventions on shoulder function [29], coordination, and trajectory control [71,84]. Combining bilateral upper extremity training with other therapies, such as occupational therapy [103] or bilateral robotic movement priming, has shown additional benefits.
Research by Bruyneel [71] emphasizes that bilateral training may surpass traditional unilateral methods, as it closely mirrors real-life tasks. Thus, it reinforces movement patterns and strengthens ecological validity within rehabilitation programs [104].
The inclusion of sensory feedback within BAT has also emerged as an influential factor in optimizing recovery outcomes. Han and Kim [29] highlight how sensory feedback mechanisms—like visual and auditory cues—can improve patients’ engagement and comprehension of their movements, thereby enhancing motor learning. Their findings align with emerging practices that leverage technology to enrich sensory feedback, presenting a promising avenue for rehabilitation protocols. Such approaches could allow patients to understand better and adjust their movements, facilitating a deeper integration of motor skills [105].
Kim et al. [75] explore the neurophysiological processes underlying BAT, presenting evidence that bilateral training may influence neuroplasticity, an essential aspect of motor recovery following neurological injury. BAT appears to induce changes in brain activity and connectivity in regions responsible for motor control, suggesting that it may profoundly affect the brain’s ability to rewire and adapt post-injury. Kim et al.’s study emphasizes the importance of examining how distinct rehabilitation modalities can impact neural networks, thereby guiding targeted and effective interventions in motor recovery.
BAT’s adaptability extends to younger populations, as shown by Kumagai [76], who investigates its application in pediatric patients with hemiparesis. Kumagai et al.’s findings reveal that BAT can facilitate significant improvements in motor function and coordination in children, with benefits that parallel those seen in adult populations. Early intervention appears particularly advantageous in neurodevelopment, as BAT’s repetitive, bilateral movements may help solidify motor pathways during a critical period of growth and learning [20].
Research has highlighted the significance of task-specific versus non-task-specific BAT. Some experimental studies have found that autonomy in task control during bilateral upper extremity movement training significantly impacts outcomes for the better [82]. Bilateral upper arm movement training can be categorized into task-oriented training, focusing on goal-directed movements, and movement-oriented training, enhancing sensorimotor abilities like speed, accuracy, and endurance [75,77].
In exploring the efficacy of bilateral arm training (BAT) in stroke rehabilitation, Lee [103] demonstrates how BAT can facilitate substantial improvements in motor function, particularly in the functional use of the affected arm. This study underscores that engaging both arms simultaneously during rehabilitation strengthens the affected limb and promotes crucial interlimb coordination, enhancing the patient’s ability to perform everyday tasks. Lee’s findings align with theories of bilateral training by suggesting that engaging both arms capitalizes on the neural connections between the brain’s hemispheres, thereby supporting the functional recovery of the impaired limb [54].
Meng et al.’s [77] research adds depth to the understanding of BAT by highlighting the critical role of sensory feedback in enhancing training outcomes. By incorporating visual or auditory cues into BAT, Meng et al. reveal that patients experience better movement comprehension, which promotes motor learning and improves overall rehabilitation effectiveness. This approach suggests that integrating sensory feedback into BAT protocols could optimize functional recovery, as patients receive real-time feedback that helps them refine motor control and achieve more coordinated movements. The findings indicate that combining BAT with sensory feedback offers superior outcomes compared to BAT alone, supporting the integration of technology in rehabilitation to enhance sensory-motor interactions [54].
Extending the scope of BAT applications, Kaupp et al. [24] investigate the impact of bilateral arm training in pediatric populations, particularly in children with hemiparesis. The research indicates that BAT yields significant improvements in motor function and coordination in children, mirroring the positive results observed in adults. Kaupp et al.’s study advocates for early intervention, proposing that BAT may positively influence developmental outcomes in children with motor impairments. This perspective highlights the importance of tailoring BAT protocols to be age-appropriate, recognizing the distinct neurodevelopmental needs of younger patients to maximize their rehabilitative potential [101].
Task-specific training involves intensive practice of actions or functional tasks relevant and significant to the individual’s daily life, promoting neuroplasticity, motor learning, and improved functional reorganization. Studies suggest that engaging in task-specific actions leads to better rehabilitation outcomes than non-task-specific approaches, highlighting the critical role of tailored and meaningful task training in optimizing recovery and promoting neural reorganization in stroke survivors. Repetition alone without functional meaning is insufficient to produce meaningful improvements in rehabilitation [106].
Task-specific training is recommended internationally in stroke rehabilitation guidelines and involves intensive practice of actions or functional tasks [20]. Rehabilitation therapies involving task-specific actions often have better effects than traditional non-task-specific rehabilitation therapies [20]. This is supported by a systematic review highlighting the benefits of task-oriented training for improving functional outcomes in stroke patients, indicating that such training is more effective than conventional therapies [20].
Moreover, the integration of task-specific training into rehabilitation protocols has been shown to enhance motor function recovery, particularly in the upper limbs, by promoting neuroplasticity and facilitating the relearning of motor skills [107]. The evidence suggests that engaging patients in meaningful and functional tasks improves their motor abilities and enhances their overall quality of life [108]. This aligns with findings that emphasize the importance of personalized and intensive practice in rehabilitation settings, which can significantly improve daily activities and independence for stroke survivors [107,108].
Studies have demonstrated the feasibility of delivering hundreds of repetitions of task-specific training in one-hour therapy sessions, leading to improvements in secondary measures of activity and participation [109]. Activity-Based Restorative Therapies (ABRT) involve repetitive task-specific training using weight-bearing and external facilitation of neuromuscular activation [110]. Technology, such as virtual reality-based therapy, offers advantages in rehabilitation by maximizing variables aligning with neuroplastic processes needed in stroke rehabilitation, including massed practice, repetition, task specificity, and meaningful tasks [90].
Task-specific training within bilateral upper extremity movement training is crucial for optimizing recovery and promoting neural reorganization in stroke survivors. Task-specific training involves intensive practice of actions or functional tasks relevant to daily life, leading to better rehabilitation outcomes than non-task-specific approaches. For instance, Cunningham et al. emphasize that task-specific training is recommended in stroke rehabilitation guidelines and has been shown to improve upper limb function significantly through repetitive task training [111]. This aligns with findings from Khallaf, who noted that task-specific training enhances trunk control and balance, which are essential for daily activities post-stroke [112].
Moreover, task-specific actions promote neuroplasticity, motor learning, and improved functional reorganization. Research indicates that meaningful and tailored task training is vital for effective stroke rehabilitation. For example, Grefkes and Fink discuss how training-based interventions enhance functional recovery and neural plasticity, underscoring the importance of targeted rehabilitation strategies [113]. Similarly, the work of Demers et al. highlights the neural plastic changes associated with task-specific training, suggesting that such interventions can lead to significant cortical reorganization in chronic stroke patients [114].
Furthermore, the delivery of hundreds of repetitions of task-specific training in therapy sessions has improved secondary measures of activity and participation. This is supported by findings from Iqbal et al., which demonstrate that task-oriented training significantly enhances balance and activities of daily living performance in stroke patients [115]. Additionally, the systematic review by Chiaramonte et al. reinforces the notion that task-specific training is essential for improving balance control and reducing fall risk, particularly during dual-tasking scenarios [116]. These studies collectively emphasize the significance of task specificity in rehabilitation, highlighting its role in fostering recovery and enhancing the quality of life for stroke survivors.
Integrating bilateral upper extremity training with other therapies, such as occupational therapy or bilateral robotic movement priming, has shown additional benefits in stroke rehabilitation [117].
- Neurophysiological processes underpinning bilateral upper extremity (arms) training
The mechanism suggested by many of the authors in this paper is that the activation of neural circuits in both hemispheres during bilateral tasks enhances brain plasticity, improving motor control and coordination [27,118]. The timing and nature of interventions during rehabilitation significantly impact recovery outcomes.
To understand the intricate mechanisms that drive the efficacy of interventions in stroke rehabilitation, it is essential to explore the role of bilateral training involving symmetrical, reciprocal, and alternating movements. Research indicates that such training significantly enhances unilateral performance in stroke patients by activating neural circuits across both hemispheres during bilateral tasks. This activation is linked to improved brain plasticity, motor control, and coordination, as evidenced by studies highlighting the importance of these neural adaptations in recovery processes [119,120].
During bilateral upper extremity training, synchronizing movements in both limbs is crucial for promoting neuroplasticity and motor learning. This is particularly evident in the context of repetitive practice of symmetrical or alternating patterns and bimanual tasks, which have been shown to facilitate functional reorganization in stroke survivors [121,122]. For instance, coupling movements during bimanual training enhances motor performance and fosters a cooperative strategy between the limbs, vital for effective rehabilitation [122,123]. Furthermore, the role of specific neural pathways and the modulation of motor variability during bimanual coordination have been highlighted as significant factors influencing recovery outcomes [42].
In addition, use-dependent plasticity is critical in understanding how motor skills are acquired and refined through practice. Studies have demonstrated that repetitive voluntary movements can lead to reorganizational changes in the motor cortex, essential for learning and recovery [124,125]. The integration of somatosensory stimulation during rehabilitation has also been shown to enhance excitability in the motor cortex, further supporting the notion that targeted interventions can lead to meaningful improvements in motor function following stroke [119,125]. These findings underscore the importance of bilateral training and the underlying neural mechanisms that facilitate recovery in stroke patients.
The effectiveness of bilateral training is rooted in its capacity to engage neural processes that facilitate bilateral and unilateral movements. This engagement is critical for promoting motor recovery and enhancing functional outcomes in stroke patients. Research indicates that bilateral arm training significantly improves activities of daily living (ADL) performance compared to conventional occupational therapy, highlighting the functional advantages of such interventions [36,126]. The neural coupling associated with bilateral movements is essential for effective rehabilitation, as it allows for integrating motor commands across both hemispheres, which is particularly beneficial for stroke patients who often experience unilateral deficits [36,126].
Studies have demonstrated that the neural coordination involved in bilateral hand movements is not merely a summation of two unilateral movements but reflects a complex interplay of neural circuits that operate bilaterally [127]. This is supported by findings that show increased phase coherence in the subthalamic nucleus during unimanual movements, suggesting that even unilateral actions can invoke bilateral neural responses, which may enhance motor function in both limbs [127]. Furthermore, the involvement of brainstem motor centers in coordinating bilateral movements underscores the importance of these neural pathways in rehabilitation strategies aimed at improving motor function post-stroke [36,126].
In addition, Cauraugh et al. [8] highlight that practicing bilateral arm training activates both central and peripheral input, leading to improvements in motor functions related to activities of daily living [8]. This activation of sensorineural pathways through bilateral movements enhances motor control and contributes to functional recovery in stroke survivors.
Furthermore recent studies have emphasized the importance of task-oriented training over repetitive bilateral arm training, indicating that the former can lead to more favorable functional outcomes in stroke rehabilitation [128]. This is supported by evidence suggesting that specific training protocols can enhance motor recovery by targeting the unique needs of stroke patients [129]. In addition, the integration of advanced technologies, such as robotic-assisted rehabilitation, has been shown to facilitate motor learning and improve upper extremity function through structured and repetitive task engagement [130,131].
In exploring the neural mechanisms underlying bilateral training, research has demonstrated that simultaneous movement of both upper extremities can stabilize the affected limb and promote symmetric interaction in the cerebral cortex, which is crucial for effective rehabilitation [131]. This aligns with findings that highlight the role of the cerebellum in motor learning and recovery, particularly in the context of constraint-induced movement therapy [132]. Moreover, studies have shown that enhancing trunk control through bilateral upper extremity exercises not only improves balance but also significantly reduces the risk of falls among chronic stroke patients, thereby underscoring the necessity of a holistic approach in stroke rehabilitation [133].
The timing and nature of interventions are critical in determining recovery outcomes in stroke rehabilitation. Research indicates that transfer effects in motor learning are more pronounced in proximal compared to distal effectors, which emphasizes the need for specificity in training approaches [134]. Additionally, symmetrical movements of the upper extremities have been found to activate neural networks across both hemispheres, enhancing inter-limb coordination and improving functional outcomes in patients with varying degrees of hemiplegia [135]. This is further corroborated by evidence suggesting that cognitive deficits can significantly impact arm motor recovery, highlighting the intricate relationship between cognitive and motor rehabilitation strategies [135,136].
The review by Waller and Whitall [137] calls for more randomized controlled trials and studies on neurophysiological mechanisms to further elucidate the benefits of bilateral training in stroke rehabilitation. They stress the need to tailor specific training approaches to individual patient characteristics and recognize the importance of bilateral and unilateral functioning in daily activities. Moreover, the study by Stoykov and Corcos [101] highlights that stroke survivors, even at the chronic stage, can experience improvements in upper extremity motor skills through targeted rehabilitation interventions, emphasizing the potential for ongoing recovery and functional gains post-stroke.
3.1.3. Bilateral Arm Training Plus Sensory Enhancement
Recent research underscores the growing potential of bilateral arm training (BAT) combined with sensory enhancement as a powerful approach in stroke rehabilitation. Integrating sensory enhancement modalities, such as visual, auditory, or tactile feedback, refines BAT by providing real-time information that aids in movement accuracy and motor learning. Studies indicate that this sensory feedback amplifies the engagement of motor and sensory pathways, facilitating adaptive changes in the brain that improve coordination and function in the affected arm. For instance, Wang et al. highlight that the neural mechanisms underlying motor learning significantly overlap between bilateral and unilateral training, suggesting that BAT can facilitate functional recovery of the paretic arm in stroke patients with hemiparesis [54]. Furthermore, Chuang et al. demonstrate that bilateral arm training, when combined with neuromuscular electrical stimulation, can lead to improved arm function and reduced shoulder pain in hemiplegic patients, indicating the efficacy of this approach in enhancing rehabilitation outcomes [138].
The role of sensory feedback in motor learning is further supported by the findings of Huang et al., who report that both bilateral and unilateral training can induce changes in cortical sensorimotor maps, thereby improving motor function post-stroke [83]. Additionally, the systematic review by Pérez-Marcos et al. emphasizes that various rehabilitation strategies, including BAT, are essential for addressing upper extremity impairments following stroke, as they promote neural plasticity and functional recovery [139].
Emerging methods in rehabilitation, such as robotic priming paired with body-oriented therapy (BAT), mirror therapy, and impairment-oriented training, are being actively explored to enhance the effectiveness of therapeutic approaches for patients with motor impairments. Robotic priming, in particular, provides precise control over movements, facilitating consistent practice that reinforces neural pathways and supports interhemispheric communication. This is crucial as effective rehabilitation can leverage the brain’s functional plasticity to establish new neural pathways, allowing other brain regions to compensate for diminished functions in damaged areas [83,140].
Robotic-assisted therapy has been shown to offer intensive and repetitive training, which is essential for the formation of new neural pathways in the brain [141]. This method is complemented by mirror therapy, which utilizes visual illusions to promote movement in the affected limb by reflecting the movements of the unaffected limb. This technique has been demonstrated to enhance motor recovery by engaging the brain’s visual and motor systems, thereby facilitating interhemispheric communication [83,142]. Furthermore, the integration of these advanced rehabilitation techniques can lead to significant improvements in motor function and neural plasticity, as they encourage the brain to reorganize and adapt following injury [140,143].
Sun and Zehr [91] demonstrated that sensory enhancement can amplify interlimb cutaneous reflexes in wrist extensor muscles. This finding aligns with the impact of sensory enhancement on Bilateral Arm Training (BAT) success. Sensory enhancement can amplify interlimb cutaneous reflexes in wrist extensor muscles, as demonstrated by Sun and Zehr [91]. This finding aligns with the impact of sensory enhancement on Bilateral Arm Training (BAT) success. The amplification of interlimb reflexes is particularly relevant in the context of cooperative bimanual tasks, where stronger reflexes are observed when both arms are dynamically coupled, compared to performing independent static tasks. This suggests that shared cutaneous input during bilateral movements can enhance motor control and coordination, which is crucial for effective rehabilitation strategies [91]. Furthermore, bilateral arm training can induce concurrent activation of neural pathways, leading to improved motor control in the affected limb through mechanisms such as cortical disinhibition and enhanced interhemispheric communication, as noted by Chuang et al. [138]. These findings support the notion that sensory enhancement facilitates reflexive responses and contributes to the overall efficacy of bilateral training interventions in rehabilitation settings.
Song et al. [80] focused on the role of sensory enhancement in facilitating motor performance, examining the influence of sensory feedback—particularly visual and tactile—on motor task accuracy and speed. Their findings indicated that sensory feedback substantially improved both aspects of performance, likely by providing additional sensory information to aid motor planning and execution. This supports the notion that sensory input is fundamental to motor control, as it allows for real-time adjustments and fine-tuning of movements, making it a critical component in motor rehabilitation [144].
Building on these findings, Rodrigues et al. [79] investigated the integration of sensory feedback into motor training protocols, finding that enhanced sensory modalities during training contributed to improved motor learning and performance. Participants receiving augmented sensory feedback exhibited more significant gains than those training without this added feedback, suggesting that sensory enhancement could be a valuable tool for rehabilitation and skill acquisition. These results underscore the importance of sensory input in optimizing motor function, reinforcing the value of sensory-integrated strategies in clinical settings [145].
Unfortunately, one of the primary methodological challenges across these studies is the inconsistency in BAT protocols, which complicates direct comparisons and limits generalizability. Van Delden et al. [81] demonstrated the efficacy of BAT for individuals with hemiparesis. However, the specific training regimens varied considerably across studies, making it difficult to understand the exact impact of BAT consistently. Similarly, Song et al. [80] examined the effects of task-oriented versus repetitive BAT but did not achieve a clear consensus regarding optimal training duration or intensity. The absence of standardized protocols in BAT research underscores the need for future studies to develop uniform guidelines to enhance comparability and reliability across findings.
In addition to methodological challenges, the studies primarily address stroke patients but often lack diversity in stroke-related conditions and population characteristics. For instance, Rodrigues et al. [79] emphasized sensory feedback’s role in enhancing motor learning; however, the findings were mainly limited to specific stroke subpopulations.
- Neurophysiological processes underpinning bilateral upper extremity plus sensory enhancement training
The mechanism behind bilateral arm training’s effectiveness lies in its ability to facilitate neuroplasticity, optimize interhemispheric coupling, and enhance motor coordination [91]. Bilateral arm training promotes improved motor activity in individuals with hemiplegia by engaging both hemispheres and reducing inhibition in the cerebral cortex [146].
Moreover, when sensory enhancement is added to bilateral arm training, such as stimulation to evoke cutaneous reflexes, it can amplify interlimb reflexes and further enhance motor learning and coordination [91]. This sensory enhancement can modulate functional connectivity in sensory-motor networks and improve sensorimotor adaptation, contributing to better motor outcomes in stroke patients [147].
When sensory enhancement is integrated into bilateral arm training, such as stimulation to evoke cutaneous reflexes, it can have profound implications for motor learning and coordination, particularly in stroke patients. This sensory enhancement has been shown to amplify interlimb reflexes, indicating that spinal interlimb neural connections can be strengthened through sensory augmentation, even during independent bimanual tasks [91]. Sensory enhancement to bilateral arm training can be seen as optimizing rehabilitation by leveraging the brain’s neuroplasticity. Passive robot-controlled arm movements, combined with proprioceptive decision-making and feedback, have modulated functional connectivity in sensory-motor networks and enhanced sensorimotor adaptation in stroke patients [147].
Moreover, the generalization of sensorimotor learning from bilateral to unilateral movement conditions has been observed, indicating the transferability of skills acquired through bilateral training to unilateral tasks [54].
In a systematic review, van Delden et al. analyzed various bilateral upper limb training devices and their effectiveness in post-stroke rehabilitation. They found that BAT, particularly when combined with rhythmic auditory cueing, can significantly improve motor function and coordination. Their findings support the notion that bilateral training can lead to better functional outcomes compared to unilateral training, as it engages both hemispheres of the brain, thereby optimizing neural pathways involved in motor control [26,137,148]. The review also emphasizes the importance of task-oriented approaches in rehabilitation, which aligns with the findings of Lin et al. [78].
3.1.4. Bilateral Arm Training and Robotics
Robotic solutions offer benefits such as providing repetitive movements, objective measurements of functional improvements, and adapting training tasks based on patient needs [149]. Robotic systems can also assist in re-educating balance, walking, and improving lower limb function in post-stroke survivors [30]. Additionally, robotic devices can be crucial in functional hand rehabilitation after stroke, providing training and assistance for daily activities [136].
Robotic devices in bilateral training, such as the Mirror Image Movement Enabler (MIME), have shown promise in providing shoulder and elbow neurorehabilitation in subacute stroke patients [150]. These robotic devices offer bilateral training modes that can enhance the effectiveness of rehabilitation by providing repetitive and consistent training movements [151].
The control systems integrated into these devices enable precise movements and can provide electrical stimulation to specific muscle groups, facilitating plasticity and recovery in post-stroke patients [151]. The design of robotic exoskeletons is crucial in delivering intensive, personalized, and cost-effective physiotherapy, which is essential for optimizing rehabilitation outcomes, especially in stroke survivors [152].
Moreover, comparing active and active-assistive robotic rehabilitation groups in stroke survivors highlights the importance of robotic interventions in delivering consistent and structured training sessions, which are essential for promoting recovery [153].
Robotic devices have diverse benefits. Their ability to increase motivation, adapt training tasks based on individual needs, collect data for monitoring progress, ensure patient safety, and enable intensive repetitive practice underscores their significance in enhancing rehabilitation effectiveness [154]. The development of wearable robotic devices for in-bed acute stroke rehabilitation underscores the potential of robotics in delivering targeted and accessible rehabilitation interventions [155].
Integrating bilateral arm training (BAT) and robotic assistance in stroke rehabilitation has gained considerable traction, as evidenced by the research contributions of AbdollahI et al. [82], Huang et al. [83], and Li et al. [156]. Together, their studies underscore the promising role of robotic-assisted therapies in enhancing motor function, coordination, and overall recovery in stroke patients.
Compared to traditional therapist-led rehabilitation, Huang et al. [83] demonstrated that robotic assistance can significantly improve motor control and functional performance in stroke patients, particularly in tasks requiring bilateral coordination. This led to additional increases in independence in daily activities. The consistency and intensity of training provided by robotics emerge as a key advantage over conventional therapy, which may vary in quality and intensity due to human limitations [157].
Li et al.’s research takes a novel approach by examining the impact of robotic priming techniques combined with BAT [156]. His findings suggest that integrating robotic priming with task-oriented therapies effectively reduces motor impairments and encourages the functional use of the affected arm in everyday tasks [158]. Li’s studies also delve into the neural mechanisms underlying these improvements, proposing that robotic-assisted training can enhance brain plasticity and connectivity within sensory-motor networks, thus facilitating recovery [147]. These insights advocate for a holistic approach to stroke rehabilitation that combines robotic technology with established therapeutic techniques to optimize patient outcomes [157].
Further exploration of the neural mechanisms underlying the effectiveness of BAT and robotic training remains essential. While Li’s [156] research suggests that robotic interventions may enhance brain plasticity, the specific neural pathways are not well-defined. Studies have indicated that bilateral training can engage both hemispheres, yet the exact nature of these bilateral interactions and their potential to inform targeted rehabilitation strategies require more detailed investigation [159]. Understanding these neural processes could lead to more optimized rehabilitation protocols to enhance neuroplasticity and functional recovery.
- Neurophysiological processes underpinning bilateral arm plus robotics training
Brain interfacing technology, such as electroencephalography (EEG)-based brain-computer interfaces (BCI), offers new strategies for robotic gait re-education after a stroke by enabling active engagement in movement intent and providing neurophysiological feedback, thus enhancing the effectiveness of robotic interventions [52].
Simultaneous movement of the same muscle groups on both sides during bilateral training can activate similar neural networks in bilateral hemispheres, reducing inter-hemispheric inhibition and improving functional performance in the affected limb [137]. Bilateral robot-assisted training has led to greater neural stimulation in the contralateral side of the motor cortex, which is crucial for promoting neural adaptations and improving motor function in stroke patients [42]. Moreover, bilateral sensorimotor cortical communication, modulated by multiple-hand training, is essential for coordinating movements and enhancing motor control in robotic rehabilitation individuals [83].
3.1.5. Bilateral Arm Training and Virtual Reality/Computer Guidance
When combined with modified constraint-induced movement therapy, virtual reality training has been found effective for upper extremity function recovery in acute stroke patients [160]. Furthermore, virtual reality technology has been utilized in various fields, such as dance movement analysis, sports music integration training, and balance training for the elderly, showcasing its versatility and effectiveness in movement training [156,161,162].
Jayasinghe et al.’s [84] paper on bilateral arm training (BAT) integrated with virtual reality (VR) and video guidance found a significant increase patient motivation and engagement in rehabilitation. The immersive nature of VR creates an interactive environment that encourages active participation, which is crucial given the established link between patient motivation and positive rehabilitation outcomes [93]. Furthermore, VR’s interactive and enjoyable aspects are suggested to enhance the retention of motor skills practiced during therapy, facilitating repeated movement practice essential for neuroplasticity and motor recovery [26]. By fostering a stimulating atmosphere, VR-based BAT could thus play a critical role in improving patient adherence and maximizing the therapeutic benefits of rehabilitation.
Jayasinghe et al. also highlights the advantages of video guidance (VG) with BAT, providing real-time feedback for motor learning. Immediate visual feedback enables patients to observe and correct their movement patterns, thereby supporting motor learning through improved accuracy and coordination over time [163]. This feedback mechanism is particularly relevant in stroke rehabilitation, where patients frequently encounter challenges with coordination and movement execution due to motor impairments. VG also aids in monitoring and adjusting training protocols based on individual needs and progress.
- Neurophysiological processes underpinning bilateral arm training and virtual reality—computer guidance
Research indicates that combining bilateral arm training with VR can impact brain activity in post-stroke patients, suggesting that this approach can modulate neural networks and potentially optimize motor recovery [92]. By involving individuals in bilateral upper-extremity exercises within a VR environment, this approach targets motor function and stimulates cognitive and perceptual processes, providing a comprehensive approach to rehabilitation [92]. Owing to its immersive and interactive nature, individuals utilizing BAT + VR can engage in a more stimulating and motivating rehabilitation process, potentially leading to improved motor function and coordination [93]. Further, studies have demonstrated that VR-based interventions can be as effective as real-world experiences. They may even offer superior learning effects in some cases (“Examining the User Experience of a Digital Camera Virtual Reality Lab with Attention Guidance”, 2022).
3.2. Bilateral Leg Training
Walking therapy is one of the most widely used forms of post-stroke rehabilitation; however, it is often one of the only bilateral leg therapies used during the initial rehabilitation period [164]. Research shows early and intensive walking training can significantly enhance stroke survivors’ motor function and mobility recovery [165].
Over the last decade, walking therapy has been recognized as crucial in post-stroke rehabilitation. Studies have highlighted the importance of whole-body activities like walking in enhancing recovery after a stroke [166]. Research has shown that interventions focusing on walking can significantly improve walking speed, balance ability, and overall functional recovery in stroke patients [167]. Moreover, varying doses of higher-intensity, task-specific walking-related interventions have been investigated to improve walking recovery, physical function, cognition, and overall well-being post-stroke [168]. The findings from Wonsetler and Bowden emphasize that walking endurance is vital for home and community walking activities after a stroke, which aligns with the notion that walking therapy is integral to rehabilitation [166]. Furthermore, Khan et al. demonstrate that task-oriented walking interventions can significantly aid in the early recovery of stroke patients, reinforcing the effectiveness of walking-focused rehabilitation strategies [16]. These studies collectively underscore the importance of structured walking interventions in enhancing recovery outcomes for stroke survivors.
Recent findings indicate that specific interventions can improve lower limb motor function and address early ankle dorsiflexion dysfunction, which is critical for mobility and balance [169]. Furthermore, the efficacy of bilateral therapy, mainly through lower limb strengthening exercises, has been demonstrated to promote balance in hemiparetic stroke patients effectively. This approach underscores the advantages of bilateral training in optimizing rehabilitation outcomes for individuals recovering from stroke [30,169]. The benefits of bilateral training are further corroborated by studies highlighting its role in enhancing functional reach and balance scores among stroke survivors. Jeon and Hwang’s randomized controlled trial illustrated that patients engaging in bilateral lower limb strengthening exercises exhibited significantly improved balance and walking capabilities compared to those undergoing unilateral training [169]. This finding aligns with the broader literature suggesting that bilateral training not only aids in restoring motor function but also plays a crucial role in improving overall balance and mobility in post-stroke rehabilitation [30]. Moreover, the neurophysiological underpinnings of these rehabilitation strategies are supported by evidence indicating that intensive training correlates with increased activity in brain regions associated with motor control, such as the cerebellum and primary motor cortex [170]. This neuroplasticity is essential for recovery, as it facilitates the reorganization of motor pathways, thereby enhancing functional outcomes in stroke patients [170,171]. Overall, the integration of bilateral exercises and targeted rehabilitation techniques presents a promising avenue for improving motor function and balance in individuals affected by hemiparetic stroke
Walking therapy is a fundamental aspect of post-stroke recovery; however, there are scenarios where alternative or supplementary interventions may be more appropriate based on individual needs. For instance, in cases where individuals with stroke have significant balance impairments, incorporating backward walking training alongside conventional therapy has been shown to enhance balance and functional outcomes [172].
Moreover, for stroke survivors with cognitive deficits that impact their ability to engage effectively in walking therapy, virtual reality training with cognitive load has been proposed as a beneficial approach to improving walking function [133].
Studies have explored the efficacy of exoskeleton-based physical therapy programs and functional electrical stimulation gait training in improving gait performance, walking speed, balance, and overall activity post-stroke [173]. Functional electrical stimulation therapy has been shown to significantly improve walking ability and motor recovery in chronic stroke patients when combined with conventional therapy [174]. Robotic exoskeletons for overground walking have shown promise in enhancing functional outcomes like increased walking speed, which strongly predicts independent community ambulation [175]. For non-ambulatory stroke patients or those with severe mobility limitations, early rehabilitation programs utilizing exoskeleton-based physical therapy have been recommended to be goal-oriented, repetitive, and task-specific to optimize gains in mobility and walking [173]. Furthermore, in instances where stroke survivors have reached a plateau in their recovery despite ongoing rehabilitation efforts, gait training with wearable robotic devices has led to further improvements in walking ability [176].
Ardestani et al. [85] and Jo [86] found that BLT leads to notable improvements in muscle strength and functional performance compared to unilateral training. Participants engaging in BLT demonstrated significantly more significant strength gains attributed to the simultaneous activation of both legs during exercises, which enhances neuromuscular adaptations, benefiting overall lower limb functionality [177]. This bilateral approach supports a more balanced strength development across both legs, reducing the risk of compensatory movement patterns that could result in further injury—a critical consideration for individuals recovering from injuries or surgeries [178].
Furthermore, Ardestani and Jo emphasize incorporating functional tasks into BLT. Their findings suggest that combining BLT with task-oriented activities, such as squats or step exercises, enhances performance in daily living tasks. This is particularly relevant in rehabilitation, as improved functional performance translates to better mobility and independence in daily life [179]. The researchers argue that integrating functional movements builds strength and improves coordination and balance, which are vital for maintaining overall mobility and independence.
The studies highlight Bilateral Leg Training (BLT)’s role in promoting neural adaptations that enhance motor control. In Ardestani and Jo’s studies, participants exhibited better coordination and timing between their legs, which is fundamental for tasks requiring bilateral leg use, such as walking or running [180]. These improvements in neuromuscular timing suggest enhanced interhemispheric communication and coordination, which may be particularly beneficial for individuals with neurological impairments [179]. This aligns with previous literature supporting the concept of cross-education, where training one limb can produce strength gains in the untrained limb through neural adaptations [181,182]. The evidence indicates that such adaptations benefit athletic performance and play a crucial role in rehabilitation settings, where restoring balance and coordination is essential for recovery [183].
The effectiveness of rhythmic auditory stimulation (RAS) in motor rehabilitation has been well-documented. RAS involves providing auditory cues, such as metronomic beats or music with a precise rhythm, to support and enhance motor tasks like gait and cyclic training [91]. RAS can significantly improve gait parameters and motor performance in individuals with neurological conditions like stroke and Parkinson’s disease [138,177]. These cues act as external forcing functions, simplifying motor tasks and enhancing motor control, leading to improvements in step length, accuracy, gait speed, cadence, and stride length [178,179]. Incorporating bilateral lower-limb training with simultaneous auditory cues is more effective than unilateral training in re-educating balance and walking in post-stroke survivors [184].
Incorporating bilateral lower-limb training with simultaneous auditory cues is more effective than unilateral training in re-educating balance and walking in post-stroke survivors [30,185]. This approach enhances the functioning and motor performance of the affected extremity, promoting improvements in lower limb motor function and early ankle dorsiflexion dysfunction [186]. Additionally, bilateral therapy involving lower limb strengthening exercises has effectively promoted balance in hemiparetic stroke patients, further supporting the benefits of bilateral training in stroke rehabilitation [7,169].
3.2.1. Bilateral Leg Training and Sensory Enhancement
Transcutaneous electrical nerve stimulation (TENS) has emerged as a significant adjunctive intervention for enhancing various aspects of rehabilitation in individuals who have suffered strokes, including improvements in paretic lower-limb muscle strength, walking speed, balance performance, and overall functional mobility. The therapeutic effects of TENS are mediated through both peripheral and central mechanisms [198]. From a peripheral perspective, TENS applied to paretic limbs has been shown to influence spinal reflex pathways, which may enhance motor control. However, the specific effects on H-reflex amplitude and latency in chronic stroke patients are not adequately supported by the cited reference [199], focusing on analgesic mechanisms rather than motor control. Therefore, this claim should be revised to reflect the general understanding of TENS effects without specific unsupported details. Centrally, TENS has been demonstrated to affect cortical processes. For instance, a study found that a single session of electrical stimulation on a paretic hand resulted in changes in cortical excitability and connectivity during thumb contractions on the affected side [147]. This finding highlights the potential of TENS to enhance cortical excitability and connectivity, which are essential for motor recovery following a stroke. Moreover, a regimen of TENS combined with task-oriented training (TOT) has been shown to yield improvements in lower-limb muscle strength and walking performance compared to placebo-TENS combined with TOT in chronic stroke subjects [198]. This suggests that the integration of TENS with structured rehabilitation protocols can significantly enhance recovery outcomes in stroke patients. Additionally, the research by Lim and Madhavan [198] on non-paretic leg movements facilitating cortical drive to the paretic leg provides further insights into the efficacy of combined sensory and motor interventions for improving motor function in stroke patients [198]. This approach aligns with the understanding that enhancing sensory feedback can facilitate motor recovery, as sensory inputs play a critical role in motor learning and rehabilitation.
The research by Kwong et al. [87] on bilateral leg training (BLT) combined with sensory enhancement training offers valuable insights into its efficacy for improving motor function and sensory integration, among other things, in individuals with lower limb impairments. However, several notable research gaps remain, highlighting areas where further investigation is essential.
A primary limitation of Kwong et al.’s study is the lack of investigation into the long-term effects of BLT combined with sensory enhancement on functional independence and quality of life. While the findings indicate immediate gains in motor function and sensory integration, little is known about the sustainability of these improvements. Longitudinal studies that follow participants over extended periods are needed to determine the durability of these benefits and their influence on overall functional capabilities in daily life.
Additionally, there is a need for a more detailed exploration of the neurophysiological mechanisms driving the benefits of this combined training approach. While Kwong et al. report improvements in motor and sensory functions, their study does not examine the neural adaptations that may underlie these effects. Employing neuroimaging techniques could help clarify how BLT with sensory enhancement influences brain plasticity and interhemispheric communication. This is especially relevant for individuals with neurological impairments who may benefit from targeted rehabilitation strategies.
Lastly, Kwong et al.’s study, like many studies covering bilateral arm and/or leg training, does not fully consider the psychosocial aspects of rehabilitation, which can be critical in influencing recovery trajectories.
Psychosocial factors are essential in rehabilitation because they significantly impact motivation, adherence to therapy, and overall recovery outcomes, and they are well-established in influential studies on rehabilitation psychology. For instance, Bandura’s [200] work on self-efficacy highlights that a patient’s belief in their ability to succeed in a task can directly influence their engagement and persistence in rehabilitation exercises. In stroke and motor rehabilitation, self-efficacy improves compliance with therapy and actual physical recovery outcomes [201]. Furthermore, Deci and Ryan’s [202] Self-Determination Theory emphasizes the importance of intrinsic motivation, often boosted by supportive and autonomy-promoting environments. This motivation plays a critical role in rehabilitation, as it can enhance engagement and the willingness to perform challenging tasks necessary for recovery [203]. Similarly, the work by Sheldon et al. [204] underlines that patients who receive psychological support and participate in interventions that promote a positive outlook and coping skills demonstrate faster recovery and higher quality of life. These foundational theories and studies illustrate that integrating psychological support within rehabilitation protocols—through encouragement, goal-setting, and feedback—can foster a patient’s psychological resilience, improving mental and physical health outcomes in a more comprehensive, patient-centered approach to rehabilitation.
- Neurophysiological mechanisms underpinning Bilateral leg training and sensory enhancement
The neurophysiological effects of bilateral post-stroke leg training and the application of Transcutaneous Electrical Nerve Stimulation (TENS) or other sensory enhancement methods have garnered significant attention in stroke rehabilitation research. Wang et al. [205] highlighted the importance of sensory stimulation tools in restoring motor function during stroke recovery. Lim and Madhavan [198] also demonstrated increased ipsilateral drive to the paretic muscle post-stroke with severe leg motor impairment after skill training, indicating the potential benefits of motor priming.
Regarding TENS, Tan et al. [206] showed that TENS can alleviate brain ischemic injury by regulating neuronal oxidative stress, pyroptosis, and mitophagy, indicating its potential neuroprotective effects. Moreover, Tan et al. [206] demonstrated that bilateral TENS combined with task-oriented training can effectively improve motor recovery of the upper limb following a stroke. Additionally, Kwong et al. [87] found that combining TENS with bilateral leg training significantly enhances muscle strength and motor function in post-stroke patients, further supporting the integration of TENS in rehabilitation protocols for optimizing outcomes [87,198,205,206].
Clinical studies consistently highlight the advantages of bilateral motor training over unilateral or conventional training for recovering motor control, muscle strength, upper limb kinematics, hand dexterity, and overall upper-limb function after a stroke. For instance, a systematic review by Dembele et al. [43] demonstrates that bilateral upper limb training significantly enhances motor function compared to unilateral training, promoting activity-dependent neuronal plasticity in stroke patients [43]. Furthermore, Hirayama et al. [207] reported that employing somatosensory stimulation on the wrist can enhance subsequent hand choice, indicating that peripheral stimulation can influence sensorimotor regions of the brain, which is crucial for motor recovery [207]. This aligns with findings from Noble et al. [208], who showed that bilateral motor tasks activate more brain regions and elicit higher neural activation than unilateral tasks, suggesting a broader engagement of neural networks during bilateral training [208]. Additionally, the mechanisms underlying the efficacy of bilateral interventions in stroke patients involve rebalancing interhemispheric inhibition and activating similar neural networks in both brain hemispheres. Grefkes and Fink [209] provide insights into how stroke affects the interaction between motor areas and how therapeutic interventions, such as transcranial magnetic stimulation, can correct pathological connectivity among motor regions, thereby facilitating recovery [209]. This is supported by the work of Taud et al. [210], which indicates that transcranial direct current stimulation can improve motor training outcomes in stroke rehabilitation, further emphasizing the role of neuromodulation in enhancing motor function [210]. In summary, integrating bilateral motor training and neuromodulatory techniques such as transcranial magnetic stimulation and direct current stimulation presents a promising approach to enhancing motor recovery in stroke patients.
The effectiveness of utilizing transcranial magnetic stimulation (TMS) in stroke patients by coordinating maximal voluntary contraction of the unaffected extremity and less forceful contraction of the affected side leads to an elevation in cortical excitability of the motor representation zone for the affected hand in the affected hemisphere, compared to contracting the affected hand alone [29].
Grefkes and Fink [113] further support this by demonstrating positive neural connectivity between the affected primary motor cortex (M1) and unaffected motor-related regions during synchronized bilateral hand movements in stroke patients [113]. Safdar et al. [211] discuss using noninvasive brain stimulation, such as repetitive TMS, to facilitate motor function recovery in stroke patients by modulating intracortical neuronal circuits [211].
The diagnostic potential of transcranial magnetic stimulation (TMS) in predicting motor recovery after a stroke is significant, as highlighted by various studies. For instance, Kumar et al. [212] discuss the utility of TMS in conjunction with diffusion tensor imaging to predict upper-limb motor recovery in acute ischemic stroke patients, emphasizing its role in assessing cortical excitation-inhibition balance and cortical reorganization [212]. This aligns with the findings of Rolle et al. [213], who identified that TMS-EEG data can effectively predict motor recovery over time, thus supporting the notion that TMS can serve as a valuable diagnostic tool in stroke rehabilitation [213].
3.3. Bilateral Arm and Leg Training
Recent studies have increasingly focused on using bilateral arm and bilateral leg training in stroke rehabilitation to enhance motor recovery and functional outcomes in individuals post-stroke. Bilateral arm training has been recognized as a valuable approach in upper extremity rehabilitation after stroke, facilitating neuroplasticity and improving motor function [42]. Similarly, bilateral leg training has shown promise in improving stroke survivors’ lower limb function and gait [24]. By integrating bilateral arm and leg training, researchers aim to target comprehensive motor recovery and functional improvements in individuals with stroke.
Studies have highlighted the effectiveness of bilateral arm training in improving upper extremity function post-stroke, emphasizing its role in facilitating motor recovery and enhancing daily activities [214]. Additionally, incorporating bilateral leg training has improved walking ability and enhanced neurophysiological integrity in chronic stroke patients, indicating the potential benefits of combining bilateral arm and leg interventions [24]. This integrated approach aims to address both upper and lower limb impairments commonly observed in stroke survivors, providing a holistic rehabilitation strategy.
Arya et al. [15] provide significant evidence on the effectiveness of combined bilateral arm and leg training in enhancing motor function and rehabilitation outcomes for individuals with mobility impairments. Their study highlights the benefits of integrating upper and lower limb training, which promotes a more holistic approach to functional recovery.
One of Arya et al.’s findings is that combined bilateral arm and leg training yields more substantial improvements in overall motor function than unilateral training. Participants who engaged in this combined training regimen demonstrated increased strength and coordination across both arms and legs—an essential factor for performing activities of daily living. This outcome supports existing research suggesting that bilateral training facilitates cross-education effects, whereby training one limb induces strength gains in the untrained limb due to neural adaptations [42,88]. Arya et al. argue that this approach enhances strength and builds the inter-limb coordination needed for complex, simultaneous movements involving both arms and legs.
Further, Arya et al. [15] emphasize the role of combined training in fostering neuroplasticity. The study demonstrates that simultaneous activation of upper and lower limbs in rehabilitation can stimulate the brain’s capacity for reorganization and adaptation, which is especially valuable for individuals with neurological impairments such as stroke. The authors propose that engaging multiple muscle groups together may expand the cortical representation of the trained limbs, leading to improved motor control and functional recovery [15]. This neuroplastic response is critical for refining movement quality and mitigating fall risks, a common challenge for individuals with mobility impairments.
The research also highlights the value of incorporating task-oriented training within the combined regimen. Arya et al. found that including functional tasks, such as reaching and stepping, during sessions significantly enhanced skill transfer to real-world activities. This approach strengthened and coordinated the limbs and promoted greater independence in daily life, a key goal of rehabilitation [15]. Arya et al. advocate for functional movement integration in rehabilitation programs to ensure that gains in strength and coordination translate into meaningful improvements in quality of life for individuals facing mobility challenges.
In the paper by Arya et al. on combined rhythmic arm and leg training, several significant research gaps can be identified that could inform future studies and enhance the understanding of this rehabilitation approach. These gaps highlight areas where further investigation could improve outcomes for individuals undergoing rehabilitation.
One significant research gap is the need for a more comprehensive understanding of the long-term effects of combined rhythmic arm and leg training on functional outcomes. While Arya et al. demonstrate immediate improvements in motor performance, the sustainability of these benefits, particularly regarding functional independence in daily activities, remains underexplored. Longitudinal studies that track patients over extended periods could provide insights into how these training effects persist and influence overall quality of life [24].
3.3.1. Combined Bilateral Rhythmic Arm and Leg Training
Studies have highlighted the effectiveness of bilateral arm training in improving upper extremity function post-stroke, emphasizing its role in facilitating motor recovery and enhancing daily activities [214]. Additionally, incorporating bilateral leg training has improved walking ability and enhanced neurophysiological integrity in chronic stroke patients, indicating the potential benefits of combining bilateral arm and leg interventions [24]. This integrated approach aims to address both upper and lower limb impairments commonly observed in stroke survivors, providing a more holistic rehabilitation strategy.
Klarner et al. [25] provide compelling evidence on the effectiveness of combined rhythmic arm and leg training in enhancing motor function and rehabilitation outcomes, particularly for individuals recovering from stroke. The study underscores the importance of incorporating rhythmic, coordinated movements of both upper and lower limbs to facilitate functional recovery and improve interlimb coordination, which is essential for daily activities requiring integrated limb use.
A significant outcome of Klarner et al.’s research is that rhythmic, bilateral training significantly enhances motor performance in stroke patients. Participants who engaged in this combined training displayed marked improvements in gait parameters, such as walking speed and stride length, compared to those receiving unilateral training. The authors attribute these advancements to enhanced interlimb coordination, which is crucial for efficient locomotion [25]. The study proposes that the rhythmic coupling of arm and leg movements may activate shared neural pathways, thereby improving motor control and coordination efficiency [25].
The study further delves into the neurophysiological mechanisms supporting combined rhythmic training. Klarner et al. [25] observed that rhythmic arm and leg movements increase the excitability of spinal reflex pathways, which play a vital role in coordinating movements between the limbs. This aligns with prior research suggesting that rhythmic, simultaneous movements can modulate reflex pathways, improving sensorimotor integration [100]. These neural adaptations may enhance communication between the brain and spinal cord, crucial for practical motor function in individuals recovering from neurological impairments such as stroke [97].
Task-oriented training emerged as an essential component within Klarner et al.’s [25] rhythmic training regimen. The rhythmic sessions notably improved skill transfer to real-world applications by incorporating functional tasks, such as stepping and reaching. This task-oriented approach strengthened and coordinated muscle groups and promoted greater independence in daily activities—a central goal of rehabilitation [218]. The authors advocate for integrating functional movements into rehabilitation programs to ensure that gains in motor performance translate into meaningful, real-world improvements for individuals with mobility challenges.
Additionally, the study calls for deeper investigation into the neurophysiological mechanisms that underpin the observed benefits of combined rhythmic training. Although the authors discuss the benefits of interlimb coordination and neural adaptation, research using neuroimaging techniques could further illuminate how combined rhythmic training influences brain plasticity and connectivity, which is especially relevant for stroke rehabilitation [219,220].
Individual variability in response to combined rhythmic training is another area that requires attention. Age, baseline motor function, and comorbid conditions can significantly impact rehabilitation outcomes. Future research should identify and accommodate these individual differences, tailoring training protocols to optimize results based on specific patient profiles. This approach could involve participant stratification and examining how these factors interact with training intensity and duration [221,222].
Klarner et al.’s study also underexplored technology’s potential to enhance combined rhythmic training. Given recent advances in rehabilitation technology, examining how tools like virtual reality or robotic assistance can support combined training could yield important insights. Such technology could improve patient engagement, provide real-time feedback, and facilitate adherence to training regimens, ultimately enhancing rehabilitation outcomes [16,223].
- Neurophysiological mechanisms underpinning combined bilateral rhythmic arm and leg training
Recent research by Klarner et al. has illuminated the neurological processes underlying the benefits of rhythmic training involving arm and leg cycling for individuals with chronic stroke [25]. This training has induced muscle activation and reflex modulation alterations across all four limbs, improving gait quality [24,97,224]. The findings suggest the existence of a common neural element that is active during rhythmic arm and leg movement, receiving input from both contralateral arms and legs [224]. Training locomotor central pattern-generating networks through arm and leg cycling has enhanced walking ability in individuals with chronic stroke [24]. Additionally, the importance of arm movements in modulating the corticospinal drive to the legs has been highlighted, indicating that active engagement of the arms in lower limb rehabilitation may result in better neural regulation and functional restoration [97].
Moreover, studies have demonstrated bidirectional reflex modulation induced by arm cycling, leading to facilitation or suppression in participants after stroke. This aligns with the findings of Thant et al. [225], who explored the effects of task-oriented training on upper extremity functional performance in patients with sub-acute stroke. Their randomized controlled trial indicated that task-oriented training significantly improved motor performance and facilitated neural adaptations, enhancing reflex pathways and sensorimotor integration in stroke patients. The interaction of rhythmic arm and leg movement during human locomotion has been experimentally supported, emphasizing the neural coupling between the arms and legs [226]. Furthermore, the conservation of neural control mechanisms between the arms and legs during locomotor behaviors in humans has been suggested, indicating a coordinated neural network operation during rhythmic limb movement [218].
Bilateral rhythmic leg training has been shown to improve motor function through various neurophysiological mechanisms. Studies have indicated that rhythmic arm and leg movements share common neural control elements [25]. This neural coupling between the arms and legs allows for coordinated rhythmic movement during locomotion [226]. Applying high-frequency stimuli to thoracolumbar segments can also neuromodulate locomotor-related neuronal networks, generating bilateral rhythmic step-like movements [227].
Furthermore, the interlimb coupling effects can facilitate bilateral motor output during rhythmic leg cycling after stroke [12]. Active rhythmic arm movements have been found to modulate the corticospinal drive to the legs, suggesting a potential mechanism for enhancing bilateral motor function [97]. Moreover, studies have shown that rhythmic leg cycling can suppress certain reflexes, likely through the involvement of central pattern-generating networks [97].
Although more complex rehab strategies such as quadruped crawling, Nordic walking, and swimming appear to be logical choices once stroke survivors are more mobile, not many authors have undertaken to study the effect of these combined upper and lower limb strategies. One of the few relevant studies in the last decade showed that Nordic walking has promise in enhancing cardiovascular health and overall well-being in post-stroke survivors [228]. Supported or unsupported swimming as therapy appears too complex to have been considered a topic of study post-stroke.
Quadrupedal movements may be crucial in coupling upper and lower extremity movements in rehabilitation, particularly post-stroke recovery. The coordination of quadrupedal locomotion involves a task-dependent neuronal coupling of upper and lower limbs, allowing for the integration of arm movements during gait while maintaining the ability to uncouple this connection during voluntary arm and hand movements [229]. This coupling mechanism is essential in rehabilitation as it synchronizes upper and lower limb movements, promoting overall motor coordination and functional recovery.
Quadrupedal movement training has been identified as an effective method to enhance whole-body stabilization and flexibility, emphasizing the importance of integrating such movements to improve functional movement patterns and range of motion [230]. By altering the base of support and center of mass through stationary and traveling variations, quadrupedal movement training provides opportunities to enhance total body joint stability patterns, facilitating the coordination of upper and lower extremity movements [231].
Additionally, developing wearable robotic devices for in-bed rehabilitation post-stroke highlights the importance of intensive sensorimotor therapy to promote motor recovery in severely impaired lower limbs, underscoring the need for comprehensive rehabilitation strategies that address both upper and lower extremities [232].
Furthermore, the concept of postural synergy-based exoskeletons for upper limb rehabilitation emphasizes the importance of replicating natural movements and activities of daily living to enhance motor recovery. By focusing on postural synergies and natural movement patterns, these devices facilitate the coupling of upper and lower extremity movements, promoting functional recovery and rehabilitation progress. A study by Hatem et al. [20] highlights the effectiveness of various rehabilitation techniques, including those that emphasize natural movement patterns, in improving upper extremity recovery after stroke [20].
3.4. Bilateral Movement Priming
Bilateral motor priming (BMP) is a form of neuromodulation methodology rather than an independent therapeutic intervention. This approach can involve mirror-image bilateral wrist movements facilitated by a device with mechanical components that ensure the synchronized movement of the less affected and affected hands [88,118]. Unlike bilateral training, where the focus is on the bilateral movements, the bilateral symmetrical actions in BMP are classified as a neuromodulation technique. Through a case-control investigation, it was observed that BMP conducted prior to Wii-based therapy yielded enhanced therapeutic outcomes for post-stroke patients, including those with severe impairments [47].
Additionally, studies have explored the use of bilateral upper extremity motor priming (BUMP) combined with task-specific training for severe, chronic upper limb hemiparesis, highlighting the potential benefits of this approach [88]. Furthermore, the effectiveness of bilateral motor priming has been linked to its ability to increase corticomotor excitability in the primary motor cortex [98]. This increase in corticomotor excitability may improve motor learning and recovery in individuals undergoing motor rehabilitation after conditions like stroke [99].
Moreover, combining high-dose therapy, bilateral motor priming, and vagus nerve stimulation has been proposed as a comprehensive approach to treating the hemiparetic upper limb in chronic stroke survivors, emphasizing the potential of integrating different rehabilitation techniques for enhanced recovery [233]. In neurorehabilitation, understanding various motor priming paradigms and their underlying neural mechanisms is crucial for optimizing therapeutic interventions [1]. Studies have also highlighted the importance of movement-based priming, such as continuous wrist flexion and extension through low-tech devices, in post-stroke rehabilitation, showcasing the practical applications of neuromodulation techniques in clinical settings [234]. Additionally, research has explored the effects of robotic priming combined with mirror therapy and bilateral upper limb training in stroke survivors, indicating the potential benefits of hybrid therapies in rehabilitation [158].
3.5. Interlimb Coupling and Quadrupedal Transfer
After a cerebrovascular event, the communication of descending motor instructions and supraspinal regulation is interrupted and impaired [12]. Nevertheless, intact neural circuits within the spinal cord remain relatively unimpaired and accessible [25]. These spinal circuits are thought to control rhythmic movements of the limbs, such as walking, cycling, or swimming [12]. Central pattern-generating networks (CPGs) are believed to be central to these spinal circuits, assisting in producing rhythmic coordinated movements of all four limbs [23].
In the context of humans, the evidence for CPG networks and connections between the upper and lower limbs is indirectly deduced due to methodological constraints [12,95,238]. The adjustment of reflexes observed during human movement displays numerous crucial features of modulation influenced by CPG regulation, including task and phase reliance [23,95]. Therefore, an intervention that triggers a consistent change in reflex modulation can provide insights into the mechanisms at work within the spinal cord.
Previous studies have shown that rhythmic movements of the arms impact reflexes in the lower limbs, resulting in both inhibitory [94] and facilitative effects [96]. It is suggested that rhythmic arm movements produce a substantial, enduring descending input that adjusts presynaptic inhibition levels, thereby altering the communication between muscle group Ia afferents and alpha motor neurons that innervate the lower limb muscles [94].
Recently, there has been a resurgence of interest in the role of arms in human movement. While walking on two legs differs from walking on four, they share many fundamental characteristics. It is proposed that during movement, the coordination between the arms and legs in two-legged individuals resembles that of four-legged creatures, with this coordination only being separated during complex upper limb tasks [23]. Contrary to earlier beliefs of their passive function during walking, the arms have been shown to actively aid in maintaining a smooth, rhythmic gait by counteracting the rotational force generated by the lower limbs [239]. Arm swing has been proven to boost the activation of lower limb muscles, indicating their active participation in movement [240]. It is theorized that the arms impact the legs through the same interlimb networks present in other animal species [12].
A neurological injury caused by a stroke leads to lasting impairments, such as weakness on one side of the body, foot drop, unequal gait, and difficulties in daily tasks [95]. Despite the continued benefits of rehabilitation long after a stroke [241], treatment is usually restricted to the initial six months post-injury.
Recent research has illustrated that rhythmic training involving arm and leg cycling among individuals with chronic stroke can induce alterations in muscle activation and reflex modulation across all four limbs, consequently leading to improved gait quality [25]. These results expand on earlier studies suggesting that arm movements in chronic stroke patients can induce temporary changes in reflex excitability in the lower limbs [242]. Established interlimb connections, evident in animal studies and neurologically healthy subjects, persist to some extent following a stroke [25]. Additionally, rhythmic movements beyond walking can engage these spinal networks [25,95], particularly beneficial for chronic stroke survivors who cannot fulfill the walking criteria for treadmill-based interventions.
3.6. High-Intensity Versus Low-Intensity Bilateral Movement Post-Stroke Rehabilitation Training
High-intensity versus low-intensity bilateral movement training in post-stroke rehabilitation is critical in optimizing outcomes for stroke survivors. High-intensity training involves a more rigorous and demanding approach, often characterized by more repetitions or movements per session. In contrast, low-intensity training typically involves fewer repetitions or movements, resulting in a less demanding regimen [243].
Studies have shown that high-intensity bilateral movement training can lead to significant improvements in motor function, arm activity, self-perceived bilateral arm ability, daily activity, upper limb function, cardiovascular fitness, physical activity, cognition, endothelial response, quality of life, balance, gait speed, and upper extremity function in stroke patients [165]. Training intensity promotes rapid motor recovery and enhances movement quality post-stroke [244]. Additionally, high-intensity training has been associated with improved task and motor performance in the upper extremities of chronic stroke patients [245].
High-intensity stepping training significantly enhances spatial and temporal parameters, movement pattern consistency, and power generation compared to lower-intensity activities. Analysis using principal components indicates improved coordination in the weaker limb and increased joint powers after high-intensity training in various settings. Specifically, high-intensity training focused on forward walking shows substantial bilateral improvements [85]. These findings support that high-intensity, diverse stepping exercises targeting the weaker limb can enhance movement patterns and force production, indicating recovery rather than mere compensation [246].
Moreover, Cauraugh and Summers [27] emphasized the importance of intensive training methods, including bilateral symmetrical arm movements, in maximizing gains post-stroke. These gains encompass improvements in motor function, arm activity, self-perceived bilateral arm ability, daily activity, upper limb function, cardiovascular fitness, physical activity, cognition, endothelial response, quality of life, balance, gait speed, and upper extremity function. This underscores the significance of incorporating both arms in rehabilitation strategies to improve outcomes for stroke patients. Furthermore, Cauraugh and Kang [19] indicated that bimanual training can enhance post-stroke rehabilitation outcomes by improving interlimb coordination between both limbs. Moreover, implementing high-intensity interval training, including bilateral arm movements, early after a stroke can improve cardiovascular fitness, physical activity, cognition, endothelial response, and quality of life [247].
In contrast, low-intensity bilateral movement training may still offer benefits in stroke rehabilitation but to a lesser extent than high-intensity training. Low-intensity training may be suitable for individuals with lower physical capabilities or those in the early stages of recovery. However, it is essential to note that the gains achieved through low-intensity training may be more gradual and potentially less pronounced than those achieved through high-intensity interventions [248].
4. Limitations
The central part of research studying the effects of bilateral movement training has focused on interventions involving bilateral arm training in its various forms. There is an apparent lack of studies incorporated into this literature research involving bilateral leg, combined bilateral leg and arm (quadrupedal), bilateral rhythmic leg, and or combined leg and arm interventions to come to a balanced conclusion on the diversity efficiency and effects between the different bilateral training methods.
5. Conclusions
The objective of this review was to shed light on the neuro-physiological underlying principles of the bilateral and interlimb movement strategies that led to positive clinical post-stroke rehabilitation outcomes. The results show the critical role of *bilateral movement training (BMT) and interlimb coupling in post-stroke rehabilitation, demonstrating their efficacy in enhancing motor function, promoting neuroplasticity, and improving overall recovery. BMT, particularly when integrated with robotic assistance, sensory enhancement, and virtual reality, offers a robust framework for maximizing rehabilitation outcomes.
A key strength of BMT lies in its ability to engage neurophysiological mechanisms such as central pattern generators, interhemispheric coupling, and cortical disinhibition, facilitating neural plasticity and interlimb coordination. High-intensity BMT is particularly beneficial for patients with moderate to severe motor impairments, while low-intensity training remains valuable for early-stage recovery.
Despite its promise, research gaps persist, particularly in long-term functional outcomes, patient stratification, and individualized rehabilitation protocols. The review underscores the need for longitudinal studies to assess the durability of motor improvements and the impact of advanced rehabilitation technologies. Additionally, psychosocial factors, including emotional well-being and motivation, must be integrated into rehabilitation strategies to enhance patient engagement.
To optimize recovery, future research should focus on personalized rehabilitation approaches, combined upper and lower limb training, and the neurophysiological mechanisms underlying BMT’s benefits. Integrating robotic assistance, virtual reality, and quadrupedal training holds promise for advancing stroke rehabilitation. By addressing these gaps, rehabilitation programs can become more patient-centered, evidence-based, and practical, ultimately improving stroke survivors’ functional independence and quality of life.
6. Recommendations and Future Directions
The findings in this paper advocate for a multidisciplinary approach incorporating advanced technologies and innovative methods to optimize recovery outcomes. Future research should focus on refining these strategies, particularly in understanding the specific protocols, for example, interlimb coupling mechanisms and the translation into de novo, quadrupedal training protocols, as well as conditions that yield the most effective results, to further enhance the quality of care for stroke survivors.
Author Contributions
J.A.K.: Conceptualization, methodology, analysis, writing, original draft preparation, review and editing, project administration. N.H.: Analysis, writing, review, and editing. F.R.C.: Analysis, writing, review, and editing. M.J.: Conceptualization, methodology, analysis, writing, original draft preparation, review and editing, project administration, and supervision.
All authors have read and agreed to the published version of the manuscript.
Funding
This research did not receive a specific grant from funding agencies in either public, commercial, or not-for-profit sectors.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data are included in the publication.
Acknowledgments
The authors thank the Carrick Institute Admin staff members for their continued support.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Stoykov, M.E.; Madhavan, S. Motor priming in neurorehabilitation. J. Neurol. Phys. Ther. 2015, 39, 33–42. [Google Scholar] [CrossRef] [PubMed]
- Stewart, K.C.; Cauraugh, J.H.; Summers, J.J. Bilateral movement training and stroke rehabilitation: A systematic review and meta-analysis. J. Neurol. Sci. 2006, 244, 89–95. [Google Scholar] [CrossRef] [PubMed]
- Stinear, C.M.; Byblow, W.D.; Ward, S.H. An update on predicting motor recovery after stroke. Ann. Phys. Rehabil. Med. 2014, 57, 489–498. [Google Scholar] [CrossRef]
- Kwakkel, G.; Veerbeek, J.M.; Van Wegen, E.E.H.; Wolf, S.L. Constraint-induced movement therapy after stroke. The Lancet Neurology 2015, 14, 224–234. [Google Scholar] [CrossRef]
- Farthing, J.P.; Zehr, E.P. Restoring symmetry: Clinical applications of cross-education. Exerc. Sport Sci. Rev. 2014, 42, 70–75. [Google Scholar] [CrossRef]
- Lee, M.; Carroll, T.J. Cross education: Possible mechanisms for the contralateral effects of unilateral resistance training. Sports Med. 2007, 37, 1–14. [Google Scholar] [CrossRef]
- Harjpal, P.; Qureshi, M.d.I.; Kovela, R.K.; Jain, M. Bilateral lower limb training for post-stroke survivors: A bibliometric analysis. Cureus 2022. [Google Scholar] [CrossRef]
- Cauraugh, J.H.; Lodha, N.; Naik, S.K.; Summers, J.J. Bilateral movement training and stroke motor recovery progress: A structured review and meta-analysis. Human Movement Science 2010, 29, 853–870. [Google Scholar] [CrossRef]
- Liu, Y.; Tang, Y.; Wang, L.; Yu, P.; Wang, C.; Zeng, L.; Yuan, J.; Zhao, L. Optimal acupuncture methods for lower limb motor dysfunction after stroke: A systematic review and network meta-analysis. Front. Neurol. 2024, 15, 1415792. [Google Scholar] [CrossRef]
- Timmermans, A.A.; Seelen, H.A.; Willmann, R.D.; Kingma, H. Technology-assisted training of arm-hand skills in stroke: Concepts on reacquisition of motor control and therapist guidelines for rehabilitation technology design. J. Neuroeng. Rehabil. 2009, 6, 1. [Google Scholar] [CrossRef]
- Vasudevan, E.V.; Kirk, E.M. Jensen, W., Andersen, O.K., Akay, M., Eds.; Improving interlimb coordination following stroke: How can we change how people walk (and why should we). In Replace, repair, restore, relieve – bridging clinical and engineering solutions in neurorehabilitation; Springer International Publishing: Cham, Switzerland, 2014; Volume 7, pp. 195–202. [Google Scholar]
- Zehr, E.P.; Barss, T.S.; Kaupp, C.; Klarner, T.; Mezzarane, R.A.; Nakajima, T.; Sun, Y.; Komiyama, T. Neuromechanical interlimb interactions and rehabilitation of walking after stroke. In Replace, repair, restore, relieve – bridging clinical and engineering solutions in neurorehabilitation; Jensen, W., Andersen, O.K., Akay, M., Eds.; Springer International Publishing: Cham, Switzerland, 2014; Volume 7, pp. 219–225. [Google Scholar]
- Li, K.-P.; Wu, J.-J.; Zhou, Z.-L.; Xu, D.-S.; Zheng, M.-X.; Hua, X.-Y.; Xu, J.-G. Noninvasive brain stimulation for neurorehabilitation in post-stroke patients. Brain Sciences 2023, 13, 451. [Google Scholar] [CrossRef] [PubMed]
- Maceira-Elvira, P.; Popa, T.; Schmid, A.-C.; Hummel, F.C. Wearable technology in stroke rehabilitation: Towards improved diagnosis and treatment of upper-limb motor impairment. J. Neuroeng. Rehabil. 2019, 16, 142. [Google Scholar] [CrossRef] [PubMed]
- Arya, K.N.; Pandian, S.; Sharma, A.; Kumar, V.; Kashyap, V.K. Interlimb coupling in poststroke rehabilitation: A pilot randomized controlled trial. Top. Stroke Rehabil. 2020, 27, 272–289. [Google Scholar] [CrossRef]
- Khan, A.; Malik, A.; Yaseen, A.; Mahmood, T.; Nazir, M.; Khan, S. Mobility related confidence level in chronic stroke patients through task oriented walking intervention. The Superior Journal of Physical Therapy and Rehabilitation 2023, 3. [Google Scholar] [CrossRef]
- Keeling, A.B.; Piitz, M.; Semrau, J.A.; Hill, M.D.; Scott, S.H.; Dukelow, S.P. Robot enhanced stroke therapy optimizes rehabilitation (restore): A pilot study. J. Neuroeng. Rehabil. 2021, 18, 10. [Google Scholar] [CrossRef]
- Hesse, S.; Mehrholz, J.; Werner, C. Robot-assisted upper and lower limb rehabilitation after stroke: Walking and arm/hand function. Deutsches Arzteblatt international 2008, 105, 330–336. [Google Scholar] [CrossRef]
- Cauraugh, J.H.; Kang, N. Bimanual movements and chronic stroke rehabilitation: Looking back and looking forward. Applied Sciences 2021, 11, 10858. [Google Scholar] [CrossRef]
- Hatem, S.M.; Saussez, G.; Della Faille, M.; Prist, V.; Zhang, X.; Dispa, D.; Bleyenheuft, Y. Rehabilitation of motor function after stroke: A multiple systematic review focused on techniques to stimulate upper extremity recovery. Front. Hum. Neurosci. 2016, 10. [Google Scholar] [CrossRef]
- French, B.; Thomas, L.H.; Coupe, J.; McMahon, N.E.; Connell, L.; Harrison, J.; Sutton, C.J.; Tishkovskaya, S.; Watkins, C.L. Repetitive task training for improving functional ability after stroke. Cochrane Database Syst. Rev. 2016, 2016. [Google Scholar] [CrossRef]
- Yoon, J.A.; Koo, B.I.; Shin, M.J.; Shin, Y.B.; Ko, H.-Y.; Shin, Y.-I. Effect of constraint-induced movement therapy and mirror therapy for patients with subacute stroke. Annals of Rehabilitation Medicine 2014, 38, 458. [Google Scholar] [CrossRef]
- Dietz, V. Spinal cord pattern generators for locomotion. Clin. Neurophysiol. 2003, 114, 1379–1389. [Google Scholar] [CrossRef] [PubMed]
- Kaupp, C.; Pearcey, G.E.P.; Klarner, T.; Sun, Y.; Cullen, H.; Barss, T.S.; Zehr, E.P. Rhythmic arm cycling training improves walking and neurophysiological integrity in chronic stroke: The arms can give legs a helping hand in rehabilitation. J. Neurophysiol. 2018, 119, 1095–1112. [Google Scholar] [CrossRef] [PubMed]
- Klarner, T.; Barss, T.; Sun, Y.; Kaupp, C.; Loadman, P.; Zehr, E. Long-term plasticity in reflex excitability induced by five weeks of arm and leg cycling training after stroke. Brain Sciences 2016, 6, 54. [Google Scholar] [CrossRef] [PubMed]
- Whitall, J.; Waller, S.M.; Silver, K.H.C.; Macko, R.F. Repetitive bilateral arm training with rhythmic auditory cueing improves motor function in chronic hemiparetic stroke. Stroke 2000, 31, 2390–2395. [Google Scholar] [CrossRef]
- Cauraugh, J.H.; Summers, J.J. Neural plasticity and bilateral movements: A rehabilitation approach for chronic stroke. Prog. Neurobiol. 2005, 75, 309–320. [Google Scholar] [CrossRef]
- Summers, J.J.; Kagerer, F.A.; Garry, M.I.; Hiraga, C.Y.; Loftus, A.; Cauraugh, J.H. Bilateral and unilateral movement training on upper limb function in chronic stroke patients: A tms study. J. Neurol. Sci. 2007, 252, 76–82. [Google Scholar] [CrossRef]
- Han, K.J.; Kim, J.Y. The effects of bilateral movement training on upper limb function in chronic stroke patients. Journal of Physical Therapy Science 2016, 28, 2299–2302. [Google Scholar] [CrossRef]
- Harjpal, P.; Qureshi, M.d.I.; Kovela, R.K.; Jain, M. Efficacy of bilateral lower limb training over unilateral to re-educate balance and walking in post-stroke survivors: A protocol for randomized clinical trial. Journal of Pharmaceutical Research International 2021, 281–287. [Google Scholar] [CrossRef]
- Schaefer, S.Y.; Lang, C.E. Using dual tasks to test immediate transfer of training between naturalistic movements: A proof-of-principle study. Journal of Motor Behavior 2012, 44, 313–327. [Google Scholar] [CrossRef]
- Cauraugh, J.H.; Kim, S. Two coupled motor recovery protocols are better than one: Electromyogram-triggered neuromuscular stimulation and bilateral movements. Stroke 2002, 33, 1589–1594. [Google Scholar] [CrossRef]
- Lewis, G.N.; Perreault, E.J. Side of lesion influences bilateral activation in chronic, post-stroke hemiparesis. Clin. Neurophysiol. 2007, 118, 2050–2062. [Google Scholar] [CrossRef] [PubMed]
- Schick, T.; Kolm, D.; Leitner, A.; Schober, S.; Steinmetz, M.; Fheodoroff, K. Efficacy of four-channel functional electrical stimulation on moderate arm paresis in subacute stroke patients—results from a randomized controlled trial. Healthcare 2022, 10, 704. [Google Scholar] [CrossRef] [PubMed]
- Bolton, D.A.E.; Cauraugh, J.H.; Hausenblas, H.A. Electromyogram-triggered neuromuscular stimulation and stroke motor recovery of arm/hand functions: A meta-analysis. J. Neurol. Sci. 2004, 223, 121–127. [Google Scholar] [CrossRef]
- Dietz, V.; Holliger, N.S.; Christen, A.; Geissmann, M.; Filli, L. Neural coordination of bilateral hand movements: Evidence for an involvement of brainstem motor centres. The Journal of Physiology 2024, 602, 397–412. [Google Scholar] [CrossRef]
- Allen, J.L.; Ting, L.H.; Kesar, T.M. Gait rehabilitation using functional electrical stimulation induces changes in ankle muscle coordination in stroke survivors: A preliminary study. Front. Neurol. 2018, 9, 1127. [Google Scholar] [CrossRef]
- Lee, D.H.; Park, S.H.; Han, J.W. Effect of bilateral upper extremity exercise on trunk performance in patients with stroke. Journal of Physical Therapy Science 2017, 29, 625–628. [Google Scholar] [CrossRef]
- Richardson, M.C.; Tears, C.; Morris, A.; Alexanders, J. The effects of unilateral versus bilateral motor training on upper limb function in adults with chronic stroke: A systematic review. J. Stroke Cerebrovasc. Dis. 2021, 30, 105617. [Google Scholar] [CrossRef]
- Chen, Y.-W.; Lin, K.-c.; Li, Y.-c.; Lin, C.-J. Predicting patient-reported outcome of activities of daily living in stroke rehabilitation: A machine learning study. J. Neuroeng. Rehabil. 2023, 20, 25. [Google Scholar] [CrossRef]
- Renner, C.I.E.; Brendel, C.; Hummelsheim, H. Bilateral arm training vs unilateral arm training for severely affected patients with stroke: Exploratory single-blinded randomized controlled trial. Arch. Phys. Med. Rehabil. 2020, 101, 1120–1130. [Google Scholar] [CrossRef]
- Chen, S.; Qiu, Y.; Bassile, C.C.; Lee, A.; Chen, R.; Xu, D. Effectiveness and success factors of bilateral arm training after stroke: A systematic review and meta-analysis. Front. Aging Neurosci. 2022, 14, 875794. [Google Scholar] [CrossRef]
- Dembele, J.; Triccas, L.T.; Amanzonwé, L.E.R.; Kossi, O.; Spooren, A. Bilateral versus unilateral upper limb training in (sub)acute stroke: A systematic and meta-analysis. South African Journal of Physiotherapy 2024, 80. [Google Scholar] [CrossRef]
- Sethy, D.; Bajpai, P.; Kujur, E.S.; Mohakud, K.; Sahoo, S. Effectiveness of modified constraint induced movement therapy and bilateral arm training on upper extremity function after chronic stroke: A comparative study. Open Journal of Therapy and Rehabilitation 2016, 04, 1–9. [Google Scholar] [CrossRef]
- Crosby, L.D.; Marrocco, S.; Brown, J.; Patterson, K.K. A novel bilateral lower extremity mirror therapy intervention for individuals with stroke. Heliyon 2016, 2, e00208. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.H.; Kim, Y.-H. Robot-assisted therapy in stroke rehabilitation. Journal of Stroke 2013, 15, 174. [Google Scholar] [CrossRef]
- Shiner, C.T.; Byblow, W.D.; McNulty, P.A. Bilateral priming before wii-based movement therapy enhances upper limb rehabilitation and its retention after stroke: A case-controlled study. Neurorehabil. Neural Repair 2014, 28, 828–838. [Google Scholar] [CrossRef]
- Chen, P.-m.; Kwong, P.W.H.; Lai, C.K.Y.; Ng, S.S.M. Comparison of bilateral and unilateral upper limb training in people with stroke: A systematic review and meta-analysis. PLoS One 2019, 14, e0216357. [Google Scholar] [CrossRef]
- Stinear, C.M.; Petoe, M.A.; Anwar, S.; Barber, P.A.; Byblow, W.D. Bilateral priming accelerates recovery of upper limb function after stroke: A randomized controlled trial. Stroke 2014, 45, 205–210. [Google Scholar] [CrossRef]
- Waller, M.S.; Whitall, J.; Jenkins, T.; Magder, L.S.; Hanley, D.F.; Goldberg, A.; Luft, A.R. Sequencing bilateral and unilateral task-oriented training versus task oriented training alone to improve arm function in individuals with chronic stroke. BMC Neurol. 2014, 14, 236. [Google Scholar] [CrossRef]
- Van Delden, A.L.E.Q.; Peper, C.L.E.; Kwakkel, G.; Beek, P.J. A systematic review of bilateral upper limb training devices for poststroke rehabilitation. Stroke Research and Treatment 2012, 2012, 1–17. [Google Scholar] [CrossRef]
- Syed, N.; Biswas, A.; Hanifa, N.; Rv, P.; Sundaram, P. Bilateral versus unilateral upper extremity training on upper limb motor activity in hemiplegia. International journal of neurorehabilitation 2015, 02. [Google Scholar] [CrossRef]
- Shih, P.-C.; Steele, C.J.; Hoepfel, D.; Muffel, T.; Villringer, A.; Sehm, B. The impact of lesion side on bilateral upper limb coordination after stroke. J. Neuroeng. Rehabil. 2023, 20, 166. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Lei, Y.; Xiong, K.; Marek, K. Substantial generalization of sensorimotor learning from bilateral to unilateral movement conditions. PLoS One 2013, 8, e58495. [Google Scholar] [CrossRef]
- Wu, C.-y.; Chuang, L.-l.; Lin, K.-c.; Chen, H.-c.; Tsay, P.-k. Randomized trial of distributed constraint-induced therapy versus bilateral arm training for the rehabilitation of upper-limb motor control and function after stroke. Neurorehabil. Neural Repair 2011, 25, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Langan, J.; Doyle, S.T.; Hurvitz, E.A.; Brown, S.H. Influence of task on interlimb coordination in adults with cerebral palsy. Arch. Phys. Med. Rehabil. 2010, 91, 1571–1576. [Google Scholar] [CrossRef]
- Gerardin, E.; Bontemps, D.; Babuin, N.-T.; Herman, B.; Denis, A.; Bihin, B.; Regnier, M.; Leeuwerck, M.; Deltombe, T.; Riga, A.; et al. Bimanual motor skill learning with robotics in chronic stroke: Comparison between minimally impaired and moderately impaired patients, and healthy individuals. J. Neuroeng. Rehabil. 2022, 19, 28. [Google Scholar] [CrossRef]
- O’Connell, R.G.; Kelly, S.P. Neurophysiology of human perceptual decision-making. Annu. Rev. Neurosci. 2021, 44, 495–516. [Google Scholar] [CrossRef]
- Wilken, S.; Böttcher, A.; Adelhöfer, N.; Raab, M.; Beste, C.; Hoffmann, S. Neural oscillations guiding action during effects imagery. Behav. Brain Res. 2024, 469, 115063. [Google Scholar] [CrossRef]
- Repp, B.H.; Su, Y.-H. Sensorimotor synchronization: A review of recent research (2006–2012). Psychonomic Bulletin & Review 2013, 20, 403–452. [Google Scholar] [CrossRef]
- Mu, Y.; Huang, Y.; Ji, C.; Gu, L.; Wu, X. Auditory over visual advantage of sensorimotor synchronization in 6- to 7-year-old children but not in 12- to 15-year-old children and adults. JExPH 2018, 44, 818–826. [Google Scholar] [CrossRef]
- Nakada, K.; Asai, T.; Amemiya, Y. An analog cmos central pattern generator for interlimb coordination in quadruped locomotion. IEEE Trans. Neural Networks 2003, 14, 1356–1365. [Google Scholar] [CrossRef]
- Grillner, S. Biological pattern generation: The cellular and computational logic of networks in motion. Neuron 2006, 52, 751–766. [Google Scholar] [CrossRef] [PubMed]
- MacKay-Lyons, M. Central pattern generation of locomotion: A review of the evidence. Phys. Ther. 2002, 82, 69–83. [Google Scholar] [CrossRef] [PubMed]
- Morquette, P.; Verdier, D.; Kadala, A.; Féthière, J.; Philippe, A.G.; Robitaille, R.; Kolta, A. An astrocyte-dependent mechanism for neuronal rhythmogenesis. Nat. Neurosci. 2015, 18, 844–854. [Google Scholar] [CrossRef] [PubMed]
- Williams, C.A.; DeWeerth, S.P. A comparison of resonance tuning with positive versus negative sensory feedback. Biol. Cybern. 2007, 96, 603–614. [Google Scholar] [CrossRef]
- Guertin, P.A. Central pattern generator for locomotion: Anatomical, physiological, and pathophysiological considerations. Front. Neurol. 2013, 3. [Google Scholar] [CrossRef]
- Lakens, D.; Stel, M. If they move in sync, they must feel in sync: Movement synchrony leads to attributions of rapport and entitativity. Soc. Cogn. 2011, 29, 1–14. [Google Scholar] [CrossRef]
- Aschersleben, G. Temporal control of movements in sensorimotor synchronization. Brain Cogn. 2002, 48, 66–79. [Google Scholar] [CrossRef]
- Shachykov, A.; Henaff, P.; Shachykov, A.; Popov, A.; Shulyak, A. Neuro-musculoskeletal simulator of human rhythmic movements. In Proceedings of the 2017 IEEE First Ukraine Conference on Electrical and Computer Engineering (UKRCON), 5/2017, 2017; pp. 278–283.
- Bruyneel, A.-V.; Higgins, J.; Akremi, H.; Aissaoui, R.; Nadeau, S. Postural organization and inter-limb coordination are altered after stroke when an isometric maximum bilateral pushing effort of the upper limbs is performed. Clin. Biomech. 2021, 86, 105388. [Google Scholar] [CrossRef]
- Dhakate, D.; Bhattad, R. Study the effectiveness of bilateral arm training on upper extremity motor function and activity level in patients with sub-acute stroke. International Journal of Current Research and Review 2020, 12. [Google Scholar] [CrossRef]
- Duff, S.V.; Miller, A.; Quinn, L.; Youdan, G.; Bishop, L.; Ruthrauff, H.; Wade, E. Quantifying intra- and interlimb use during unimanual and bimanual tasks in persons with hemiparesis post-stroke. J. Neuroeng. Rehabil. 2022, 19, 44. [Google Scholar] [CrossRef]
- Itkonen, M.; Costa, Á.; Yamasaki, H.; Okajima, S.; Alnajjar, F.; Kumada, T.; Shimoda, S. Influence of bimanual exercise on muscle activation in post-stroke patients. ROBOMECH Journal 2019, 6, 14. [Google Scholar] [CrossRef]
- Kim, N.; Jo, S.; Bae, K.; Song, C. Comparison of upper extremity muscle activity between stroke patients and healthy participants while performing bimanual tasks. Physical Therapy Rehabilitation Science 2022, 11, 526–534. [Google Scholar] [CrossRef]
- Kumagai, M.; Uehara, S.; Kurayama, T.; Kitamura, S.; Sakata, S.; Kondo, K.; Shimizu, E.; Yoshinaga, N.; Otaka, Y. Effects of alternating bilateral training between non-paretic and paretic upper limbs in patients with hemiparetic stroke: A pilot randomized controlled trial. J. Rehabil. Med. 2022, 54, jrm00336. [Google Scholar] [CrossRef] [PubMed]
- Meng, G.; Meng, X.; Tan, Y.; Yu, J.; Jin, A.; Zhao, Y.; Liu, X. Short-term efficacy of hand-arm bimanual intensive training on upper arm function in acute stroke patients: A randomized controlled trial. Front. Neurol. 2018, 8, 726. [Google Scholar] [CrossRef]
- Lin, C.-H.; Chou, L.-W.; Luo, H.-J.; Tsai, P.-Y.; Lieu, F.-K.; Chiang, S.-L.; Sung, W.-H. Effects of computer-aided interlimb force coupling training on paretic hand and arm motor control following chronic stroke: A randomized controlled trial. PLoS One 2015, 10, e0131048. [Google Scholar] [CrossRef]
- Rodrigues, L.C.; Farias, N.C.; Gomes, R.P.; Michaelsen, S.M. Feasibility and effectiveness of adding object-related bilateral symmetrical training to mirror therapy in chronic stroke: A randomized controlled pilot study. Physiother. Theory Pract. 2016, 32, 83–91. [Google Scholar] [CrossRef]
- Song, G.B. The effects of task-oriented versus repetitive bilateral arm training on upper limb function and activities of daily living in stroke patients. Journal of Physical Therapy Science 2015, 27, 1353–1355. [Google Scholar] [CrossRef]
- Van Delden, A.L.E.Q.; Beek, P.J.; Roerdink, M.; Kwakkel, G.; Peper, C.L.E. Unilateral and bilateral upper-limb training interventions after stroke have similar effects on bimanual coupling strength. Neurorehabil. Neural Repair 2015, 29, 255–267. [Google Scholar] [CrossRef]
- Abdollahi, F.; Corrigan, M.; Lazzaro, E.D.C.; Kenyon, R.V.; Patton, J.L. Error-augmented bimanual therapy for stroke survivors. NeuroRehabilitation 2018, 43, 51–61. [Google Scholar] [CrossRef]
- Huang, J.-J.; Pei, Y.-C.; Chen, Y.-Y.; Tseng, S.-S.; Hung, J.-W. Bilateral sensorimotor cortical communication modulated by multiple hand training in stroke participants: A single training session pilot study. Bioengineering 2022, 9, 727. [Google Scholar] [CrossRef]
- Jayasinghe, S.A.L.; Maenza, C.; Good, D.C.; Sainburg, R.L. Deficits in performance on a mechanically coupled asymmetrical bilateral task in chronic stroke survivors with mild unilateral paresis. Symmetry 2021, 13, 1366. [Google Scholar] [CrossRef] [PubMed]
- Ardestani, M.M.; Henderson, C.E.; Mahtani, G.; Connolly, M.; Hornby, T.G. Locomotor kinematics and kinetics following high-intensity stepping training in variable contexts poststroke. Neurorehabil. Neural Repair 2020, 34, 652–660. [Google Scholar] [CrossRef] [PubMed]
- Jo, P.Y. Intralimb coordination and intermuscular coherence in walking after stroke. Dissertation, George Mason University, Fairfax, VA, 2019.
- Kwong, P.W.H.; Ng, G.Y.F.; Chung, R.C.K.; Ng, S.S.M. Bilateral transcutaneous electrical nerve stimulation improves lower-limb motor function in subjects with chronic stroke: A randomized controlled trial. Journal of the American Heart Association 2018, 7, e007341. [Google Scholar] [CrossRef] [PubMed]
- Stoykov, M.E.; King, E.; David, F.J.; Vatinno, A.; Fogg, L.; Corcos, D.M. Bilateral motor priming for post stroke upper extremity hemiparesis: A randomized pilot study. Restor. Neurol. Neurosci. 2020, 38, 11–22. [Google Scholar] [CrossRef]
- Kiper, P.; Godart, N.; Cavalier, M.; Berard, C.; Cieślik, B.; Federico, S.; Kiper, A.; Pellicciari, L.; Meroni, R. Effects of immersive virtual reality on upper-extremity stroke rehabilitation: A systematic review with meta-analysis. Journal of Clinical Medicine 2023, 13, 146. [Google Scholar] [CrossRef]
- Cazac, G.I. Virtual reality based-therapy: Targeting balance impairments to improve gait in stroke. Știința și arta mișcării 2022, 15, 4. [Google Scholar] [CrossRef]
- Sun, Y.; Zehr, E.P. Sensory enhancement amplifies interlimb cutaneous reflexes in wrist extensor muscles. J. Neurophysiol. 2019, 122, 2085–2094. [Google Scholar] [CrossRef]
- Lee, S.-H.; Kim, Y.-M.; Lee, B.-H. Effects of virtual reality-based bilateral upper-extremity training on brain activity in post-stroke patients. Journal of Physical Therapy Science 2015, 27, 2285–2287. [Google Scholar] [CrossRef]
- Song, Y.-H.; Lee, H.-M. Effect of immersive virtual reality-based bilateral arm training in patients with chronic stroke. Brain Sciences 2021, 11, 1032. [Google Scholar] [CrossRef]
- Frigon, A.; Collins, D.F.; Zehr, E.P. Effect of rhythmic arm movement on reflexes in the legs: Modulation of soleus h-reflexes and somatosensory conditioning. J. Neurophysiol. 2004, 91, 1516–1523. [Google Scholar] [CrossRef]
- Zehr, E.P.; Balter, J.E.; Ferris, D.P.; Hundza, S.R.; Loadman, P.M.; Stoloff, R.H. Neural regulation of rhythmic arm and leg movement is conserved across human locomotor tasks. The Journal of Physiology 2007, 582, 209–227. [Google Scholar] [CrossRef] [PubMed]
- Dragert, K.; Zehr, E.P. Rhythmic arm cycling modulates hoffmann reflex excitability differentially in the ankle flexor and extensor muscles. Neurosci. Lett. 2009, 450, 235–238. [Google Scholar] [CrossRef] [PubMed]
- Zhou, R.; Alvarado, L.; Kim, S.; Chong, S.L.; Mushahwar, V.K. Modulation of corticospinal input to the legs by arm and leg cycling in people with incomplete spinal cord injury. J. Neurophysiol. 2017, 118, 2507–2519. [Google Scholar] [CrossRef] [PubMed]
- Jordan, H.T.; Stinear, C.M. Effects of bilateral priming on motor cortex function in healthy adults. J. Neurophysiol. 2018, 120, 2858–2867. [Google Scholar] [CrossRef]
- Madhavan, S.; Stinear, J.W.; Kanekar, N. Effects of a single session of high intensity interval treadmill training on corticomotor excitability following stroke: Implications for therapy. Neural Plast. 2016, 2016, 1–8. [Google Scholar] [CrossRef]
- Ghai, S.; Ghai, I. Effects of rhythmic auditory cueing in gait rehabilitation for multiple sclerosis: A mini systematic review and meta-analysis. Front. Neurol. 2018, 9, 386. [Google Scholar] [CrossRef]
- Stoykov, M.E.; Corcos, D.M. A review of bilateral training for upper extremity hemiparesis. Occup. Ther. Int. 2009, 16, 190–203. [Google Scholar] [CrossRef]
- Stoykov, M.E.; Lewis, G.N.; Corcos, D.M. Comparison of bilateral and unilateral training for upper extremity hemiparesis in stroke. Neurorehabil. Neural Repair 2009, 23, 945–953. [Google Scholar] [CrossRef]
- Lee, M.-J.; Lee, J.-H.; Koo, H.-M.; Lee, S.-M. Effectiveness of bilateral arm training for improving extremity function and activities of daily living performance in hemiplegic patients. J. Stroke Cerebrovasc. Dis. 2017, 26, 1020–1025. [Google Scholar] [CrossRef]
- Moran, J.; Ramirez-Campillo, R.; Liew, B.; Chaabene, H.; Behm, D.G.; García-Hermoso, A.; Izquierdo, M.; Granacher, U. Effects of bilateral and unilateral resistance training on horizontally orientated movement performance: A systematic review and meta-analysis. Sports Med. 2021, 51, 225–242. [Google Scholar] [CrossRef]
- Lin, J.; He, J.; Shu, B.; Jia, J. Multi-sensory feedback therapy combined with task-oriented training on the hemiparetic upper limb in chronic stroke: Study protocol for a pilot randomized controlled trial. 2020. [CrossRef]
- Bayona, N.A.; Bitensky, J.; Salter, K.; Teasell, R. The role of task-specific training in rehabilitation therapies. Top. Stroke Rehabil. 2005, 12, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Carlsson, H.; Rosén, B.; Björkman, A.; Pessah-Rasmussen, H.; Brogårdh, C. Sensory re-learning of the upper limb (sensupp) after stroke: Development and description of a novel intervention using the tidier checklist. Trials 2021, 22, 430. [Google Scholar] [CrossRef] [PubMed]
- Amki, M.; Baumgartner, P.; Bracko, O.; Luft, A.R.; Wegener, S. Task-specific motor rehabilitation therapy after stroke improves performance in a different motor task: Translational evidence. Translational Stroke Research 2017, 8, 347–350. [Google Scholar] [CrossRef]
- Birkenmeier, R.L.; Prager, E.M.; Lang, C.E. Translating animal doses of task-specific training to people with chronic stroke in 1-hour therapy sessions: A proof-of-concept study. Neurorehabil. Neural Repair 2010, 24, 620–635. [Google Scholar] [CrossRef]
- Dolbow, D.R.; Gorgey, A.S.; Recio, A.C.; Stiens, S.A.; Curry, A.C.; Sadowsky, C.L.; Gater, D.R.; Martin, R.; McDonald, J.W. Activity-based restorative therapies after spinal cord injury: Inter-institutional conceptions and perceptions. Aging Dis. 2015, 6, 254. [Google Scholar] [CrossRef]
- Cunningham, P.; Turton, A.J.; Van Wijck, F.; Van Vliet, P. Task-specific reach-to-grasp training after stroke: Development and description of a home-based intervention. Clin. Rehabil. 2016, 30, 731–740. [Google Scholar] [CrossRef]
- Khallaf, M.E. Effect of task-specific training on trunk control and balance in patients with subacute stroke. Neurol. Res. Int. 2020, 2020, 1–8. [Google Scholar] [CrossRef]
- Grefkes, C.; Fink, G.R. Recovery from stroke: Current concepts and future perspectives. Neurological Research and Practice 2020, 2, 17. [Google Scholar] [CrossRef]
- Demers, M.; Varghese, R.; Winstein, C.J. Retrospective exploratory analysis of task-specific effects on brain activity after stroke. 2021. [CrossRef]
- Iqbal, S.; Saeed, A.; Batool, S.; Waqqar, S.; Khattak, H.G.; Jabeen, H. Effects of task-oriented balance training with sensory integration in post stroke patients. The Rehabilitation Journal 2023, 07, 18–23. [Google Scholar] [CrossRef]
- Chiaramonte, R.; Bonfiglio, M.; Leonforte, P.; Coltraro, G.; Guerrera, C.; Vecchio, M. Proprioceptive and dual-task training: The key of stroke rehabilitation, a systematic review. Journal of Functional Morphology and Kinesiology 2022, 7, 53. [Google Scholar] [CrossRef]
- Hermann, D.M.; Bassetti, C.L. Role of sleep-disordered breathing and sleep-wake disturbances for stroke and stroke recovery. Neurology 2016, 87, 1407–1416. [Google Scholar] [CrossRef] [PubMed]
- Stinear, C.M.; Byblow, W.D.; Steyvers, M.; Levin, O.; Swinnen, S.P. Kinesthetic, but not visual, motor imagery modulates corticomotor excitability. Exp. Brain Res. 2006, 168, 157–164. [Google Scholar] [CrossRef] [PubMed]
- Hosp, J.A.; Luft, A.R. Cortical plasticity during motor learning and recovery after ischemic stroke. Neural Plast. 2011, 2011, 1–9. [Google Scholar] [CrossRef]
- McDonnell, M.N.; Koblar, S.; Ward, N.S.; Rothwell, J.C.; Hordacre, B.; Ridding, M.C. An investigation of cortical neuroplasticity following stroke in adults: Is there evidence for a critical window for rehabilitation? BMC Neurol. 2015, 15, 109. [Google Scholar] [CrossRef]
- Sleimen-Malkoun, R.; Temprado, J.-J.; Thefenne, L.; Berton, E. Bimanual training in stroke: How do coupling and symmetry-breaking matter? BMC Neurol. 2011, 11, 11. [Google Scholar] [CrossRef]
- Ranganathan, R.; Gebara, R.; Andary, M.; Sylvain, J. Chronic stroke survivors show task-dependent modulation of motor variability during bimanual coordination. J. Neurophysiol. 2019, 121, 756–763. [Google Scholar] [CrossRef]
- Metrot, J.; Mottet, D.; Hauret, I.; Van Dokkum, L.; Bonnin-Koang, H.-Y.; Torre, K.; Laffont, I. Changes in bimanual coordination during the first 6 weeks after moderate hemiparetic stroke. Neurorehabil. Neural Repair 2013, 27, 251–259. [Google Scholar] [CrossRef]
- Sawaki, L.; Boroojerdi, B.; Kaelin-Lang, A.; Burstein, A.H.; Bütefisch, C.M.; Kopylev, L.; Davis, B.; Cohen, L.G. Cholinergic influences on use-dependent plasticity. J. Neurophysiol. 2002, 87, 166–171. [Google Scholar] [CrossRef]
- Sawaki, L.; Wu, C.W.-H.; Kaelin-Lang, A.; Cohen, L.G. Effects of somatosensory stimulation on use-dependent plasticity in chronic stroke. Stroke 2006, 37, 246–247. [Google Scholar] [CrossRef]
- Caldelari, P.; Lemon, R.; Dietz, V. Differential neural coordination of bilateral hand and finger movements. Physiological Reports 2020, 8. [Google Scholar] [CrossRef]
- Merrick, C.M.; Doyle, O.N.; Gallegos, N.E.; Irwin, Z.T.; Olson, J.W.; Gonzalez, C.L.; Knight, R.T.; Ivry, R.B.; Walker, H.C. Differential contribution of sensorimotor cortex and subthalamic nucleus to unimanual and bimanual hand movements. Cereb. Cortex 2024, 34, bhad492. [Google Scholar] [CrossRef] [PubMed]
- Winstein, C.J.; Wolf, S.L.; Dromerick, A.W.; Lane, C.J.; Nelsen, M.A.; Lewthwaite, R.; Cen, S.Y.; Azen, S.P.; Team, f.t.I.C.A.R.E.I.I. Effect of a task-oriented rehabilitation program on upper extremity recovery following motor stroke: The icare randomized clinical trial. JAMA 2016, 315, 571. [Google Scholar] [CrossRef] [PubMed]
- Van De Winckel, A.; Ehrlich-Jones, L. Measurement characteristics and clinical utility of the motor evaluation scale for upper extremity in stroke patients. Arch. Phys. Med. Rehabil. 2018, 99, 2657–2658. [Google Scholar] [CrossRef]
- Frisoli, A.; Procopio, C.; Chisari, C.; Creatini, I.; Bonfiglio, L.; Bergamasco, M.; Rossi, B.; Carboncini, M. Positive effects of robotic exoskeleton training of upper limb reaching movements after stroke. J. Neuroeng. Rehabil. 2012, 9, 36. [Google Scholar] [CrossRef]
- Bertani, R.; Melegari, C.; De Cola, M.C.; Bramanti, A.; Bramanti, P.; Calabrò, R.S. Effects of robot-assisted upper limb rehabilitation in stroke patients: A systematic review with meta-analysis. Neurol. Sci. 2017, 38, 1561–1569. [Google Scholar] [CrossRef]
- Xie, Z.; Cui, F.; Zou, Y.; Bai, L. Acupuncture enhances effective connectivity between cerebellum and primary sensorimotor cortex in patients with stable recovery stroke. Evid. Based Complement. Alternat. Med. 2014, 2014, 603909. [Google Scholar] [CrossRef]
- Cho, K.H.; Song, W.-K. Robot-assisted reach training for improving upper extremity function of chronic stroke. The Tohoku Journal of Experimental Medicine 2015, 237, 149–155. [Google Scholar] [CrossRef]
- Wadden, K.P.; Asis, K.D.; Mang, C.S.; Neva, J.L.; Peters, S.; Lakhani, B.; Boyd, L.A. Predicting motor sequence learning in individuals with chronic stroke. Neurorehabil. Neural Repair 2017, 31, 95–104. [Google Scholar] [CrossRef]
- Mullick, A.A.; Subramanian, S.K.; Levin, M.F. Emerging evidence of the association between cognitive deficits and arm motor recovery after stroke: A meta-analysis. Restor. Neurol. Neurosci. 2015, 33, 389–403. [Google Scholar] [CrossRef]
- Liu, G.; Cai, H.; Leelayuwat, N. Intervention effect of rehabilitation robotic bed under machine learning combined with intensive motor training on stroke patients with hemiplegia. Front. Neurorobot. 2022, 16, 865403. [Google Scholar] [CrossRef]
- Waller, S.M.; Whitall, J. Bilateral arm training: Why and who benefits? NeuroRehabilitation 2008, 23, 29–41. [Google Scholar] [CrossRef]
- Chuang, L.-L.; Chen, Y.-L.; Chen, C.-C.; Li, Y.-C.; Wong, A.M.-K.; Hsu, A.-L.; Chang, Y.-J. Effect of emg-triggered neuromuscular electrical stimulation with bilateral arm training on hemiplegic shoulder pain and arm function after stroke: A randomized controlled trial. J. Neuroeng. Rehabil. 2017, 14, 122. [Google Scholar] [CrossRef] [PubMed]
- Perez, C.; Morales-Quezada, L.; Fregni, F. A combined therapeutic approach in stroke rehabilitation: A review on non-invasive brain stimulation plus pharmacotherapy. International journal of neurorehabilitation 2014, 1. [Google Scholar] [CrossRef]
- Du, Q.; Luo, J.; Cheng, Q.; Wang, Y.; Guo, S. Vibrotactile enhancement in hand rehabilitation has a reinforcing effect on sensorimotor brain activities. Front. Neurosci. 2022, 16, 935827. [Google Scholar] [CrossRef]
- Alotaibi, N.D.; Jahanshahi, H.; Yao, Q.; Mou, J.; Bekiros, S. Identification and control of rehabilitation robots with unknown dynamics: A new probabilistic algorithm based on a finite-time estimator. Mathematics 2023, 11, 3699. [Google Scholar] [CrossRef]
- Shin, S.S.; Pelled, G. Novel neuromodulation techniques to assess interhemispheric communication in neural injury and neurodegenerative diseases. Frontiers in Neural Circuits 2017, 11. [Google Scholar] [CrossRef]
- Jia, J. Exploration on neurobiological mechanisms of the central–peripheral–central closed-loop rehabilitation. Front. Cell. Neurosci. 2022, 16, 982881. [Google Scholar] [CrossRef]
- Chen, X.; Liu, F.; Yan, Z.; Cheng, S.; Liu, X.; Li, H.; Li, Z. Therapeutic effects of sensory input training on motor function rehabilitation after stroke. Medicine 2018, 97, e13387. [Google Scholar] [CrossRef]
- Bolognini, N.; Russo, C.; Edwards, D.J. The sensory side of post-stroke motor rehabilitation. Restor. Neurol. Neurosci. 2016, 34, 571–586. [Google Scholar] [CrossRef]
- Tang, C.; Zhou, T.; Zhang, Y.; Yuan, R.; Zhao, X.; Yin, R.; Song, P.; Liu, B.; Song, R.; Chen, W.; et al. Bilateral upper limb robot-assisted rehabilitation improves upper limb motor function in stroke patients: A study based on quantitative eeg. Eur. J. Med. Res. 2023, 28, 603. [Google Scholar] [CrossRef]
- Vahdat, S.; Darainy, M.; Thiel, A.; Ostry, D.J. A single session of robot-controlled proprioceptive training modulates functional connectivity of sensory motor networks and improves reaching accuracy in chronic stroke. Neurorehabil. Neural Repair 2019, 33, 70–81. [Google Scholar] [CrossRef] [PubMed]
- Van Delden, A.; Peper, C.; Beek, P.; Kwakkel, G. Unilateral versus bilateral upper limb exercise therapy after stroke: A systematic review. J. Rehabil. Med. 2012, 44, 106–117. [Google Scholar] [CrossRef] [PubMed]
- Xu, G.; Gao, X.; Pan, L.; Chen, S.; Wang, Q.; Zhu, B.; Li, J. Anxiety detection and training task adaptation in robot-assisted active stroke rehabilitation. International Journal of Advanced Robotic Systems 2018, 15, 1729881418806433. [Google Scholar] [CrossRef]
- Fiore, S.; Battaglino, A.; Sinatti, P.; Sánchez-Romero, E.A.; Ruiz-Rodriguez, I.; Manca, M.; Gargano, S.; Villafañe, J.H. The effectiveness of robotic rehabilitation for the functional recovery of the upper limb in post-stroke patients: A systematic review. Retos 2023, 50, 91–101. [Google Scholar] [CrossRef]
- Khor, K.X.; Chin, P.J.H.; Hisyam, A.R.; Yeong, C.F.; Narayanan, A.L.T.; Su, E.L.M. Development of cr2-haptic: A compact and portable rehabilitation robot for wrist and forearm training. In Proceedings of the 2014 IEEE Conference on Biomedical Engineering and Sciences (IECBES), 12/2014, 2014; pp. 424–429.
- Su, D.; Hu, Z.; Wu, J.; Shang, P.; Luo, Z. Review of adaptive control for stroke lower limb exoskeleton rehabilitation robot based on motion intention recognition. Front. Neurorobot. 2023, 17, 1186175. [Google Scholar] [CrossRef]
- Park, J.H.; Park, G.; Kim, H.Y.; Lee, J.-Y.; Ham, Y.; Hwang, D.; Kwon, S.; Shin, J.-H. A comparison of the effects and usability of two exoskeletal robots with and without robotic actuation for upper extremity rehabilitation among patients with stroke: A single-blinded randomised controlled pilot study. 2020. [CrossRef]
- Park, J.H.; Chung, Y. The effects of providing visual feedback and auditory stimulation using a robotic device on balance and gait abilities in persons with stroke: A pilot study. Physical Therapy Rehabilitation Science 2016, 5, 125–131. [Google Scholar] [CrossRef]
- Ren, Y.; Wu, Y.-N.; Yang, C.-Y.; Xu, T.; Harvey, R.L.; Zhang, L.-Q. Developing a wearable ankle rehabilitation robotic device for in-bed acute stroke rehabilitation. IEEE Trans. Neural Syst. Rehabil. Eng. 2017, 25, 589–596. [Google Scholar] [CrossRef]
- Li, Y.-c.; Lin, K.-c.; Chen, C.-l.; Yao, G.; Chang, Y.-j.; Lee, Y.-y.; Liu, C.-t.; Chen, W.-S. Three ways to improve arm function in the chronic phase after stroke by robotic priming combined with mirror therapy, arm training, and movement-oriented therapy. Arch. Phys. Med. Rehabil. 2023, 104, 1195–1202. [Google Scholar] [CrossRef]
- Lee, Y.-c.; Li, Y.-c.; Lin, K.-c.; Yao, G.; Chang, Y.-j.; Lee, Y.-y.; Liu, C.-t.; Hsu, W.-l.; Wu, Y.-h.; Chu, H.-t.; et al. Effects of robotic priming of bilateral arm training, mirror therapy, and impairment-oriented training on sensorimotor and daily functions in patients with chronic stroke: Study protocol of a single-blind, randomized controlled trial. Trials 2022, 23, 566. [Google Scholar] [CrossRef]
- Li, Y.; Fan, T.; Qi, Q.; Wang, J.; Qiu, H.; Zhang, L.; Wu, X.; Ye, J.; Chen, G.; Long, J.; et al. Efficacy of a novel exoskeletal robot for locomotor rehabilitation in stroke patients: A multi-center, non-inferiority, randomized controlled trial. Front. Aging Neurosci. 2021, 13, 706569. [Google Scholar] [CrossRef]
- Jung, N.-H.; Kim, K.-M.; Oh, J.-S.; Chang, M. The effects of bilateral arm training on reaching performance and activities of daily living of stroke patients. Journal of Physical Therapy Science 2013, 25, 449–452. [Google Scholar] [CrossRef]
- Ji, E.-K.; Lee, S.-H. Effects of virtual reality training with modified constraint-induced movement therapy on upper extremity function in acute stage stroke: A preliminary study. Journal of Physical Therapy Science 2016, 28, 3168–3172. [Google Scholar] [CrossRef] [PubMed]
- Yang, D. Construction of sports music integration training and performance practice system based on virtual reality technology. Journal of Electrical Systems 2024, 20, 493–500. [Google Scholar] [CrossRef]
- Cho, G.H.; Hwangbo, G.; Shin, H.S. The effects of virtual reality-based balance training on balance of the elderly. Journal of Physical Therapy Science 2014, 26, 615–617. [Google Scholar] [CrossRef]
- Hassan, M. Impact of instant visual guidance via video technology on the correction of some offensive skills performance errors in basketball أثر التوجيه البصري الفوري عبر تقنية الفيديو في تصحيح بعض أخطاء أداء المهارات الهجومية في كرة السلة. Asian J. Sports Med. 2023, 14, 1–7. [Google Scholar] [CrossRef]
- Langhorne, P.; Coupar, F.; Pollock, A. Motor recovery after stroke: A systematic review. The Lancet Neurology 2009, 8, 741–754. [Google Scholar] [CrossRef]
- Mehrholz, J.; Pohl, M.; Platz, T.; Kugler, J.; Elsner, B. Electromechanical and robot-assisted arm training for improving activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst. Rev. 2018, 2018. [Google Scholar] [CrossRef]
- Wonsetler, E.C.; Bowden, M.G. A systematic review of mechanisms of gait speed change post-stroke. Part 2: Exercise capacity, muscle activation, kinetics, and kinematics. Top. Stroke Rehabil. 2017, 24, 394–403. [Google Scholar] [CrossRef]
- Wang, C.-Y.; Miyoshi, S.; Chen, C.-H.; Lee, K.-C.; Chang, L.-C.; Chung, J.-H.; Shi, H.-Y. Walking ability and functional status after post-acute care for stroke rehabilitation in different age groups: A prospective study based on propensity score matching. Aging 2020, 12, 10704–10714. [Google Scholar] [CrossRef]
- French, M.A.; Moore, M.F.; Pohlig, R.; Reisman, D. Self-efficacy mediates the relationship between balance/walking performance, activity, and participation after stroke. Top. Stroke Rehabil. 2015, 23, 77–83. [Google Scholar] [CrossRef]
- Jeon, H.J.; Hwang, B.Y. Effect of bilateral lower limb strengthening exercise on balance and walking in hemiparetic patients after stroke: A randomized controlled trial. Journal of Physical Therapy Science 2018, 30, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Bellaiche, S.; Ibarolla, D.; Redouté, J.; Comte, J.-C.; Medée, B.; Arsenault, L.; Mayel, A.; Revol, P.; Delporte, L.; Cotton, F.; et al. Upper limb rehabilitation after stroke: Constraint versus intensive training. A longitudinal case-control study correlating motor performance with fmri data. 2022. [CrossRef]
- Kim, H.; Park, G.; Shin, J.-H.; You, J.H. Neuroplastic effects of end-effector robotic gait training for hemiparetic stroke: A randomised controlled trial. Sci. Rep. 2020, 10, 12461. [Google Scholar] [CrossRef]
- Kalyana, S.; Lohar, D.; Khan, J.; Rao, L.S. Effectiveness of supplemented backward walking training along with conventional therapy on balance and functional outcome in patients with stroke. International Journal of Current Pharmaceutical Research 2023, 108–110. [Google Scholar] [CrossRef]
- Louie, D.R.; Mortenson, W.B.; Durocher, M.; Schneeberg, A.; Teasell, R.; Yao, J.; Eng, J.J. Efficacy of an exoskeleton-based physical therapy program for non-ambulatory patients during subacute stroke rehabilitation: A randomized controlled trial. J. Neuroeng. Rehabil. 2021, 18, 149. [Google Scholar] [CrossRef]
- Kim, C.; Kim, H.-J. Effect of robot-assisted wearable exoskeleton on gait speed of post-stroke patients: A systematic review and meta-analysis of a randomized controlled trials. Physical Therapy Rehabilitation Science 2022, 11, 471–477. [Google Scholar] [CrossRef]
- Nolan, K.J.; Karunakaran, K.K.; Roberts, P.; Tefertiller, C.; Walter, A.M.; Zhang, J.; Leslie, D.; Jayaraman, A.; Francisco, G.E. Utilization of robotic exoskeleton for overground walking in acute and chronic stroke. Front. Neurorobot. 2021, 15, 689363. [Google Scholar] [CrossRef]
- Buesing, C.; Fisch, G.; O’Donnell, M.; Shahidi, I.; Thomas, L.; Mummidisetty, C.K.; Williams, K.J.; Takahashi, H.; Rymer, W.Z.; Jayaraman, A. Effects of a wearable exoskeleton stride management assist system (sma®) on spatiotemporal gait characteristics in individuals after stroke: A randomized controlled trial. J. Neuroeng. Rehabil. 2015, 12, 69. [Google Scholar] [CrossRef]
- Jacksteit, R.; Stöckel, T.; Behrens, M.; Feldhege, F.; Bergschmidt, P.; Bader, R.; Mittelmeier, W.; Skripitz, R.; Mau-Moeller, A. Low-load unilateral and bilateral resistance training to restore lower limb function in the early rehabilitation after total knee arthroplasty: A randomized active-controlled clinical trial. Frontiers in Medicine 2021, 8, 628021. [Google Scholar] [CrossRef]
- Paterno, M.V.; Rauh, M.J.; Schmitt, L.C.; Ford, K.R.; Hewett, T.E. Incidence of contralateral and ipsilateral anterior cruciate ligament (acl) injury after primary acl reconstruction and return to sport. Clin. J. Sport Med. 2012, 22, 116–121. [Google Scholar] [CrossRef]
- Green, L.A.; Gabriel, D.A. The effect of unilateral training on contralateral limb strength in young, older, and patient populations: A meta-analysis of cross education. Phys. Ther. Rev. 2018, 23, 238–249. [Google Scholar] [CrossRef]
- Othman, A.B.; Behm, D.G.; Chaouachi, A. Evidence of homologous and heterologous effects after unilateral leg training in youth. Appl. Physiol. Nutr. Metab. 2018, 43, 282–291. [Google Scholar] [CrossRef] [PubMed]
- Tilp, M.; Ringler, S.; Mariacher, H.; Rafolt, D. Unilateral strength training after total knee arthroplasty leads to similar or better effects on strength and flexibility than bilateral strength training – a randomized controlled pilot study. J. Rehabil. Med. 2023, 55, jrm00381. [Google Scholar] [CrossRef] [PubMed]
- Song, J.S.; Yamada, Y.; Kataoka, R.; Hammert, W.B.; Kang, A.; Spitz, R.W.; Wong, V.; Seffrin, A.; Kassiano, W.; Loenneke, J.P. Does unilateral high-load resistance training influence strength change in the contralateral arm also undergoing high-load training? Scand. J. Med. Sci. Sports 2024, 34, e14772. [Google Scholar] [CrossRef] [PubMed]
- Coratella, G.; Galas, A.; Campa, F.; Pedrinolla, A.; Schena, F.; Venturelli, M. The eccentric phase in unilateral resistance training enhances and preserves the contralateral knee extensors strength gains after detraining in women: A randomized controlled trial. Front. Physiol. 2022, 13, 788473. [Google Scholar] [CrossRef]
- Shimada, K.; Onishi, T.; Ogawa, Y.; Yamauchi, J.; Kawada, S. Effects of motor imagery combined with action observation training on the lateral specificity of muscle strength in healthy subjects. Biomedical Research 2019, 40, 107–113. [Google Scholar] [CrossRef]
- Lee, J.; Song, B.-W.; Yang, W. Design of exoskeleton-type wrist human–machine interface based on over-actuated coaxial spherical parallel mechanism. Advances in Mechanical Engineering 2018, 10, 1687814017753896. [Google Scholar] [CrossRef]
- Peurala, S.H.; Kantanen, M.P.; Sjögren, T.; Paltamaa, J.; Karhula, M.; Heinonen, A. Effectiveness of constraint-induced movement therapy on activity and participation after stroke: A systematic review and meta-analysis of randomized controlled trials. Clin. Rehabil. 2012, 26, 209–223. [Google Scholar] [CrossRef]
- Cai, J.; Ji, Q.; Xin, R.; Zhang, D.; Na, X.; Peng, R.; Li, K. Contralesional cortical structural reorganization contributes to motor recovery after sub-cortical stroke: A longitudinal voxel-based morphometry study. Front. Hum. Neurosci. 2016, 10. [Google Scholar] [CrossRef]
- Goodwill, A.M.; Teo, W.-P.; Morgan, P.; Daly, R.M.; Kidgell, D.J. Bihemispheric-tdcs and upper limb rehabilitation improves retention of motor function in chronic stroke: A pilot study. Front. Hum. Neurosci. 2016, 10. [Google Scholar] [CrossRef]
- Starosta, M.; Cichoń, N.; Saluk-Bijak, J.; Miller, E. Benefits from repetitive transcranial magnetic stimulation in post-stroke rehabilitation. Journal of Clinical Medicine 2022, 11, 2149. [Google Scholar] [CrossRef]
- Mustin, M.; Hensel, L.; Fink, G.R.; Grefkes, C.; Tscherpel, C. Individual contralesional recruitment in the context of structural reserve in early motor reorganization after stroke. 2024. [CrossRef]
- Grefkes, C.; Nowak, D.A.; Eickhoff, S.B.; Dafotakis, M.; Küst, J.; Karbe, H.; Fink, G.R. Cortical connectivity after subcortical stroke assessed with functional magnetic resonance imaging. Ann. Neurol. 2008, 63, 236–246. [Google Scholar] [CrossRef] [PubMed]
- Baker, A.; Schranz, C.; Seo, N.J. Associating functional neural connectivity and specific aspects of sensorimotor control in chronic stroke. Sensors 2023, 23, 5398. [Google Scholar] [CrossRef] [PubMed]
- Gopalakrishnan, R.; Cunningham, D.A.; Hogue, O.; Schroedel, M.; Campbell, B.A.; Plow, E.B.; Baker, K.B.; Machado, A.G. Cortico-cerebellar connectivity underlying motor control in chronic poststroke individuals. The Journal of Neuroscience 2022, 42, 5186–5197. [Google Scholar] [CrossRef] [PubMed]
- Marek, S.; Siegel, J.S.; Gordon, E.M.; Raut, R.V.; Gratton, C.; Newbold, D.J.; Ortega, M.; Laumann, T.O.; Adeyemo, B.; Miller, D.B.; et al. Spatial and temporal organization of the individual human cerebellum. Neuron 2018, 100, 977–993.e977. [Google Scholar] [CrossRef]
- Turkeltaub, P.E.; Swears, M.K.; D’Mello, A.M.; Stoodley, C.J. Cerebellar tdcs as a novel treatment for aphasia? Evidence from behavioral and resting-state functional connectivity data in healthy adults. Restor. Neurol. Neurosci. 2016, 34, 491–505. [Google Scholar] [CrossRef]
- Li, W.; Han, T.; Qin, W.; Zhang, J.; Liu, H.; Li, Y.; Meng, L.; Ji, X.; Yu, C. Altered functional connectivity of cognitive-related cerebellar subregions in well-recovered stroke patients. Neural Plast. 2013, 2013, 1–10. [Google Scholar] [CrossRef]
- Bernard, J.A.; Peltier, S.J.; Wiggins, J.L.; Jaeggi, S.M.; Buschkuehl, M.; Fling, B.W.; Kwak, Y.; Jonides, J.; Monk, C.S.; Seidler, R.D. Disrupted cortico-cerebellar connectivity in older adults. Neuroimage 2013, 83, 103–119. [Google Scholar] [CrossRef]
- Lim, H.; Madhavan, S. Non-paretic leg movements can facilitate cortical drive to the paretic leg in individuals post stroke with severe motor impairment: Implications for motor priming. Eur. J. Neurosci. 2023, 58, 2853–2867. [Google Scholar] [CrossRef]
- Peng, W.W.; Tang, Z.Y.; Zhang, F.R.; Li, H.; Kong, Y.Z.; Iannetti, G.D.; Hu, L. Neurobiological mechanisms of tens-induced analgesia. Neuroimage 2019, 195, 396–408. [Google Scholar] [CrossRef]
- Bandura, A. Self-efficacy: Toward a unifying theory of behavioral change. PsychologR 1977, 84, 191–215. [Google Scholar] [CrossRef]
- Zimmerman, B.J.; Cleary, T.J. Adolescents ’ development of personal agency the role of self-efficacy beliefs and self-regulatory skill. In Adolescence and education: Self-efficacy beliefs of adolescents, Pajares, F., Urdan, T., Eds.; Information Age Publishing: Greenwich, CT, 2006; Volume 5, pp. 45–69.
- Deci, E.L.; Ryan, R.M. Self-determination theory: A macrotheory of human motivation, development, and health. Canadian Psychology / Psychologie canadienne 2008, 49, 182–185. [Google Scholar] [CrossRef]
- Ryan, R.M.; Deci, E.L. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. AmP 2000, 55, 68–78. [Google Scholar] [CrossRef] [PubMed]
- Sheldon, K.M.; Elliot, A.J.; Kim, Y.; Kasser, T. What is satisfying about satisfying events? Testing 10 candidate psychological needs. JPSP 2001, 80, 325–339. [Google Scholar] [CrossRef]
- Wang, Y.; Xie, H.; Sun, H.; Ren, L.; Jiang, H.; Chen, M.; Dong, C. Influencing factors of psychological resilience in stroke patients: A systematic review and meta-analysis. Arch. Clin. Neuropsychol. 2024, 39, 644–654. [Google Scholar] [CrossRef]
- Tan, Z.; Dong, F.; Wu, L.; Feng, Y.; Zhang, M.; Zhang, F. Transcutaneous electrical nerve stimulation (tens) alleviates brain ischemic injury by regulating neuronal oxidative stress, pyroptosis, and mitophagy. Mediators Inflamm. 2023, 2023, 1–13. [Google Scholar] [CrossRef]
- Hirayama, K.; Takahashi, T.; Koga, T.; Osu, R. Somatosensory stimulation on the wrist enhances the subsequent hand-choice by biasing toward the stimulated hand. 2023. [CrossRef]
- Noble, J.W.; Eng, J.J.; Boyd, L.A. Bilateral motor tasks involve more brain regions and higher neural activation than unilateral tasks: An fmri study. Exp. Brain Res. 2014, 232, 2785–2795. [Google Scholar] [CrossRef]
- Grefkes, C.; Fink, G.R. Reorganization of cerebral networks after stroke: New insights from neuroimaging with connectivity approaches. Brain 2011, 134, 1264–1276. [Google Scholar] [CrossRef]
- Taud, B.; Lindenberg, R.; Darkow, R.; Wevers, J.; Höfflin, D.; Grittner, U.; Meinzer, M.; Flöel, A. No add-on effects of unilateral and bilateral transcranial direct current stimulation on fine motor skill training outcome in chronic stroke. A randomized controlled trial. 2021. [CrossRef]
- Safdar, A.; Smith, M.-C.; Byblow, W.D.; Stinear, C.M. Applications of repetitive transcranial magnetic stimulation to improve upper limb motor performance after stroke: A systematic review. Neurorehabil. Neural Repair 2023, 37, 837–849. [Google Scholar] [CrossRef]
- Kumar, P.; Prasad, M.; Das, A.; Vibha, D.; Garg, A.; Goyal, V.; Srivastava, A.K. Utility of transcranial magnetic stimulation and diffusion tensor imaging for prediction of upper-limb motor recovery in acute ischemic stroke patients. Annals of Indian Academy of Neurology 2022, 25, 54–59. [Google Scholar] [CrossRef]
- Rolle, C.E.; Baumer, F.M.; Jordan, J.T.; Berry, K.; Garcia, M.; Monusko, K.; Trivedi, H.; Wu, W.; Toll, R.; Buckwalter, M.S.; et al. Mapping causal circuit dynamics in stroke using simultaneous electroencephalography and transcranial magnetic stimulation. BMC Neurol. 2021, 21, 280. [Google Scholar] [CrossRef]
- Ambreen, H.; Tariq, H.; Amjad, I. Effects of bilateral arm training on upper extremity function in right and left hemispheric stroke. J. Pak. Med. Assoc. 2020, 1–9. [Google Scholar] [CrossRef]
- Aprile, I.; Guardati, G.; Cipollini, V.; Papadopoulou, D.; Monteleone, S.; Redolfi, A.; Garattini, R.; Sacella, G.; Noro, F.; Galeri, S.; et al. Influence of cognitive impairment on the recovery of subjects with subacute stroke undergoing upper limb robotic rehabilitation. Brain Sciences 2021, 11, 587. [Google Scholar] [CrossRef] [PubMed]
- Krabben, T.; Prange, G.B.; Molier, B.I.; Stienen, A.H.; Jannink, M.J.; Buurke, J.H.; Rietman, J.S. Influence of gravity compensation training on synergistic movement patterns of the upper extremity after stroke, a pilot study. J. Neuroeng. Rehabil. 2012, 9, 44. [Google Scholar] [CrossRef] [PubMed]
- Chu, X.; Liu, S.; Zhao, X.; Liu, T.; Xing, Z.; Li, Q.; Li, Q. Case report: Virtual reality-based arm and leg cycling combined with transcutaneous electrical spinal cord stimulation for early treatment of a cervical spinal cord injured patient. Front. Neurosci. 2024, 18, 1380467. [Google Scholar] [CrossRef]
- Mutai, H.; Furukawa, T.; Araki, K.; Misawa, K.; Hanihara, T. Factors associated with functional recovery and home discharge in stroke patients admitted to a convalescent rehabilitation ward. Geriatrics & Gerontology International 2012, 12, 215–222. [Google Scholar] [CrossRef]
- Page, S.J.; Szaflarski, J.P.; Eliassen, J.C.; Pan, H.; Cramer, S.C. Cortical plasticity following motor skill learning during mental practice in stroke. Neurorehabil. Neural Repair 2009, 23, 382–388. [Google Scholar] [CrossRef]
- Calautti, C.; Baron, J.-C. Functional neuroimaging studies of motor recovery after stroke in adults: A review. Stroke 2003, 34, 1553–1566. [Google Scholar] [CrossRef]
- Dresser, L.P.; Kohn, M.A. Artificial intelligence and the evaluation and treatment of stroke. Delaware Journal of Public Health 2023, 9, 82–84. [Google Scholar] [CrossRef]
- Altaf, S. Technological advancements in neurorehabilitation. The Rehabilitation Journal 2019, 3, 105–106. [Google Scholar] [CrossRef]
- Banyai, A.D.; Brișan, C. Robotics in physical rehabilitation: Systematic review. Healthcare 2024, 12, 1720. [Google Scholar] [CrossRef]
- Sasada, S.; Tazoe, T.; Nakajima, T.; Futatsubashi, G.; Ohtsuka, H.; Suzuki, S.; Zehr, E.P.; Komiyama, T. A common neural element receiving rhythmic arm and leg activity as assessed by reflex modulation in arm muscles. J. Neurophysiol. 2016, 115, 2065–2075. [Google Scholar] [CrossRef] [PubMed]
- Thant, A.A.; Wanpen, S.; Nualnetr, N.; Puntumetakul, R.; Chatchawan, U.; Hla, K.M.; Khin, M.T. Effects of task-oriented training on upper extremity functional performance in patients with sub-acute stroke: A randomized controlled trial. Journal of Physical Therapy Science 2019, 31, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Balter, J.E.; Zehr, E.P. Neural coupling between the arms and legs during rhythmic locomotor-like cycling movement. J. Neurophysiol. 2007, 97, 1809–1818. [Google Scholar] [CrossRef] [PubMed]
- Kumru, H.; Flores, Á.; Rodríguez-Cañón, M.; Edgerton, V.R.; García, L.; Benito-Penalva, J.; Navarro, X.; Gerasimenko, Y.; García-Alías, G.; Vidal, J. Cervical electrical neuromodulation effectively enhances hand motor output in healthy subjects by engaging a use-dependent intervention. Journal of Clinical Medicine 2021, 10, 195. [Google Scholar] [CrossRef]
- Salse-Batán, J.; Sanchez-Lastra, M.A.; Suarez-Iglesias, D.; Varela, S.; Ayán, C. Effects of nordic walking in people with parkinson’s disease: A systematic review and meta-analysis. Health & Social Care in the Community 2022, 30. [Google Scholar] [CrossRef]
- Dietz, V. Quadrupedal coordination of bipedal gait: Implications for movement disorders. J. Neurol. 2011, 258, 1406–1412. [Google Scholar] [CrossRef]
- Buxton, J.D.; Prins, P.J.; Miller, M.G.; Moreno, A.; Welton, G.L.; Atwell, A.D.; Talampas, T.R.; Elsey, G.E. The effects of a novel quadrupedal movement training program on functional movement, range of motion, muscular strength, and endurance. J. Strength Cond. Res. 2022, 36, 2186–2193. [Google Scholar] [CrossRef]
- Eckart, A.C. Quadrupedal movement training: A brief review and practical guide. ACSM’S Health & Fitness Journal 2023, 27, 19–33. [Google Scholar] [CrossRef]
- Boukhennoufa, I.; Zhai, X.; Utti, V.; Jackson, J.; McDonald-Maier, K.D. Wearable sensors and machine learning in post-stroke rehabilitation assessment: A systematic review. Biomed. Signal Process. Control 2022, 71, 103197. [Google Scholar] [CrossRef]
- Jarrassé, N.; Proietti, T.; Crocher, V.; Robertson, J.; Sahbani, A.; Morel, G.; Roby-Brami, A. Robotic exoskeletons: A perspective for the rehabilitation of arm coordination in stroke patients. Front. Hum. Neurosci. 2014, 8. [Google Scholar] [CrossRef]
- Stoykov, M.E.; Corcos, D.M.; Madhavan, S. Movement-based priming: Clinical applications and neural mechanisms. Journal of Motor Behavior 2017, 49, 88–97. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, Y.-w.; Wu, C.-y.; Wang, W.-e.; Lin, K.-c.; Chang, K.-c.; Chen, C.-c.; Liu, C.-t. Bilateral robotic priming before task-oriented approach in subacute stroke rehabilitation: A pilot randomized controlled trial. Clin. Rehabil. 2017, 31, 225–233. [Google Scholar] [CrossRef] [PubMed]
- He, C.; Xiong, C.-H.; Chen, Z.-J.; Fan, W.; Huang, X.-L. Postural synergy-based exoskeleton reproducing natural human movements to improve upper limb motor control after stroke. 2020. [CrossRef]
- Lerner, Z.F.; Damiano, D.L.; Bulea, T.C. A lower-extremity exoskeleton improves knee extension in children with crouch gait from cerebral palsy. Sci. Transl. Med. 2017, 9, eaam9145. [Google Scholar] [CrossRef] [PubMed]
- Zehr, E.P.; Duysens, J. Regulation of arm and leg movement during human locomotion. Neuroscientist 2004, 10, 347–361. [Google Scholar] [CrossRef]
- Elftman, H.O. The function of the arms in walking. Hum. Biol. 1939, 11, 529–535. [Google Scholar]
- Kawashima, N.; Nozaki, D.; Abe, M.O.; Nakazawa, K. Shaping appropriate locomotive motor output through interlimb neural pathway within spinal cord in humans. J. Neurophysiol. 2008, 99, 2946–2955. [Google Scholar] [CrossRef]
- Park, D.; Son, K.J.; Kim, J.H.; Kim, H.S. Effect of the frequency of rehabilitation treatments on the long-term mortality of stroke survivors with mild-to-moderate disabilities under the korean national health insurance service system. Healthcare 2023, 11, 1587. [Google Scholar] [CrossRef]
- Barzi, Y.; Zehr, E.P. Rhythmic arm cycling suppresses hyperactive soleus h-reflex amplitude after stroke. Clin. Neurophysiol. 2008, 119, 1443–1452. [Google Scholar] [CrossRef]
- Veerbeek, J.M.; Langbroek-Amersfoort, A.C.; Van Wegen, E.E.H.; Meskers, C.G.M.; Kwakkel, G. Effects of robot-assisted therapy for the upper limb after stroke: A systematic review and meta-analysis. Neurorehabil. Neural Repair 2017, 31, 107–121. [Google Scholar] [CrossRef]
- Nudo, R.J.; Wise, B.M.; SiFuentes, F.; Milliken, G.W. Neural substrates for the effects of rehabilitative training on motor recovery after ischemic infarct. Science 1996, 272, 1791–1794. [Google Scholar] [CrossRef]
- Boyne, P.; Billinger, S.A.; Reisman, D.S.; Awosika, O.O.; Buckley, S.; Burson, J.; Carl, D.; DeLange, M.; Doren, S.; Earnest, M.; et al. Optimal intensity and duration of walking rehabilitation in patients with chronic stroke: A randomized clinical trial. JAMA Neurology 2023, 80, 342. [Google Scholar] [CrossRef] [PubMed]
- Formaggio, E.; Storti, S.F.; Boscolo Galazzo, I.; Gandolfi, M.; Geroin, C.; Smania, N.; Spezia, L.; Waldner, A.; Fiaschi, A.; Manganotti, P. Modulation of event-related desynchronization in robot-assisted hand performance: Brain oscillatory changes in active, passive and imagined movements. J. Neuroeng. Rehabil. 2013, 10, 24. [Google Scholar] [CrossRef] [PubMed]
- Gjellesvik, T.I.; Becker, F.; Tjønna, A.E.; Indredavik, B.; Lundgaard, E.; Solbakken, H.; Brurok, B.; Tørhaug, T.; Lydersen, S.; Askim, T. Effects of high-intensity interval training after stroke (the hiit stroke study) on physical and cognitive function: A multicenter randomized controlled trial. Arch. Phys. Med. Rehabil. 2021, 102, 1683–1691. [Google Scholar] [CrossRef] [PubMed]
- Bohannon, R. Muscle strength and muscle training after stroke. J. Rehabil. Med. 2007, 39, 14–20. [Google Scholar] [CrossRef]
Figure 1.
PRISMA flow diagram for research and selection process. 28 articles were retained and the review considered all of them.
Figure 1.
PRISMA flow diagram for research and selection process. 28 articles were retained and the review considered all of them.
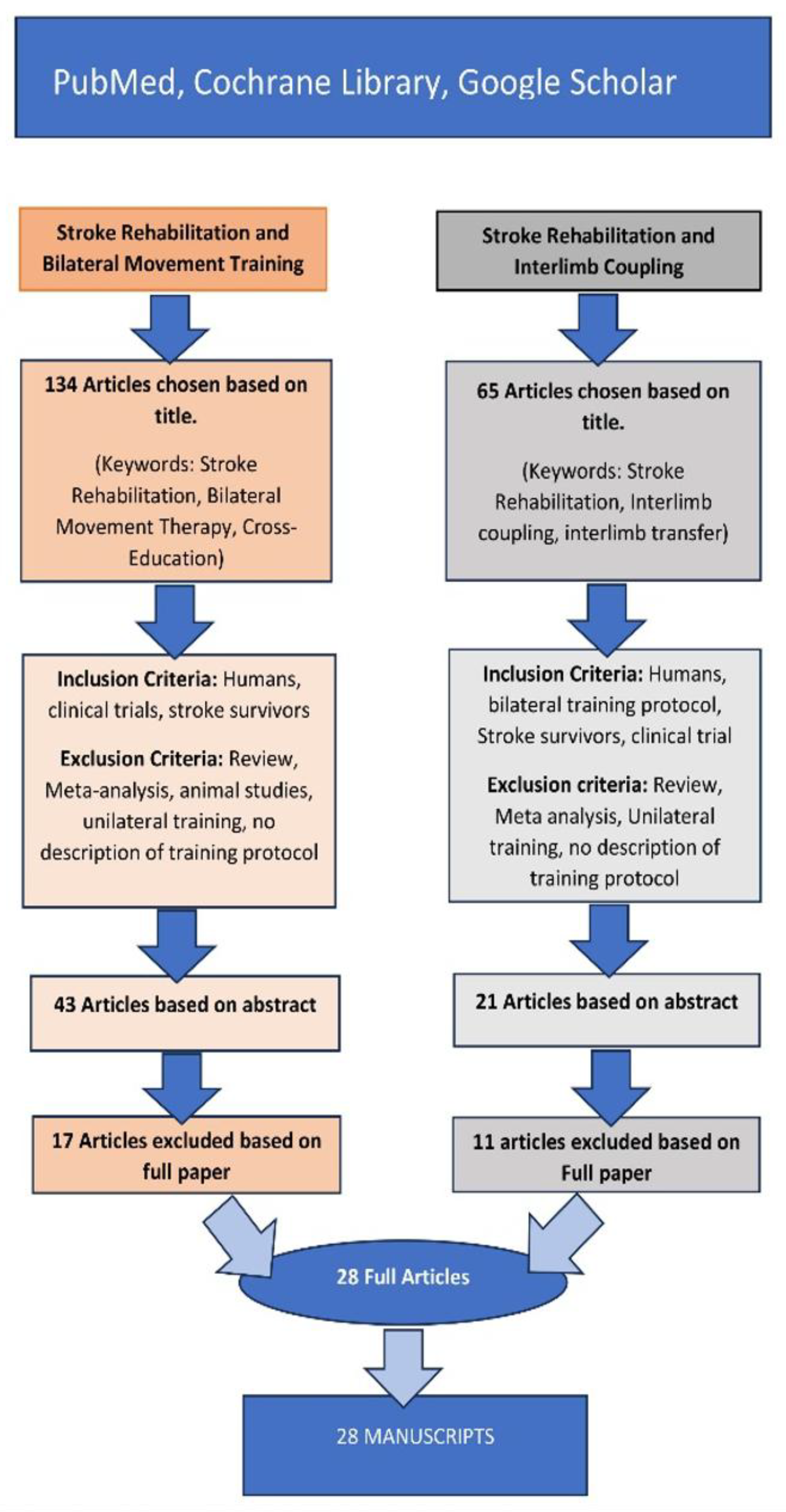
Table 1.
Specific definitions of terms used throughout the paper.
| Definition | Relevance | Authors/Source | |
|---|---|---|---|
| Bilateral Movement Training (BMT) | Bilateral movement training in post-stroke rehabilitation involves the simultaneous use of both limbs to perform tasks, promoting coordination and functional recovery. | This method leverages the concept of neural plasticity, facilitating the reorganization of the brain’s neural networks to improve motor function in the affected limb. | Cauraugh, J. H., & Summers, J. J. Neural plasticity and bilateral movements: A rehabilitation approach for chronic stroke. Progress in Neurobiology, 75(5), 309–320. [27] |
| Interlimb Coupling | Interlimb coupling in stroke rehabilitation refers to the coordination between the movements of both limbs, which can influence motor recovery and functional performance. | Interlimb coupling exercises aim to exploit neural mechanisms that link the movements of the limbs, thereby facilitating the recovery of motor function in the affected limb through synchronized bilateral activities. | Schaefer, S. Y., & Lang, C. E. Using dual tasks to test immediate transfer of training between naturalistic movements: a proof-of-principle study. Journal of Motor Behavior, 44(5), 313–318. [31] |
| Interlimb Transfer | Interlimb transfer in stroke rehabilitation refers to the phenomenon where training or practicing a motor skill with one limb improves the performance of the same skill with the untrained contralateral limb. | This allows therapists to leverage the unaffected limb to enhance motor recovery in the affected limb(s). | Cauraugh, J. H., Kim, S. Two coupled motor recovery protocols are better than one: Electromyogram-triggered neuromuscular stimulation and bilateral movements. Stroke, 33(6). [32] |
| Cross Education | Cross-education in post-stroke rehabilitation refers to the phenomenon where strength training of one limb can lead to strength gains in the contralateral, untrained limb. | This effect is particularly beneficial in stroke rehabilitation, as exercising the unaffected limb can help improve strength and function in the affected limb, aiding overall recovery. | Farthing, J. P., & Zehr, E. P. Restoring symmetry: Clinical applications of cross-education. Exercise and Sport Sciences Reviews, 42(2), 70–75. [5] |
| Bilateral Synergy | Bilateral synergy in post-stroke rehabilitation refers to the coordinated and simultaneous use of both limbs to enhance motor recovery and functional performance. | This concept leverages the interconnectedness of the hemispheres in the brain, encouraging the non-affected limb to assist in rehabilitating the affected limb, thereby improving overall motor function and reducing asymmetry in movement patterns. | Lewis, G. N., & Perreault, E. J. The side of stroke affects interlimb coordination during passive movement. Neurorehabilitation and Neural Repair, 21(4), 280–285. [33] |
| Interlimb Connections | Interlimb connections in post-stroke rehabilitation refer to the neural pathways and mechanisms that facilitate communication and coordination between the limbs. Function. | Interlimb connections are crucial for motor recovery. They enable the unaffected limb to support the rehabilitation of the affected limb by promoting symmetrical movement patterns and improving overall motor function and recovery. | Cauraugh, J. H., & Summers, J. J. Neural plasticity and bilateral movements: A rehabilitation approach for chronic stroke. Progress in Neurobiology, 75(5), 309–320. [27] |
| Central Pattern Generators (CPG) | Central pattern generators (CPGs) in stroke rehabilitation refer to neural networks in the spinal cord that can produce rhythmic patterned outputs, such as walking or other repetitive movements, without sensory feedback. | These neural circuits facilitate motor recovery by enabling rhythmic and coordinated movement patterns. Therapeutic interventions can harness and retrain these patterns to improve functional mobility in stroke patients. | Dietz, V. Spinal cord pattern generators for locomotion. Clinical Neurophysiology, 114(8), 1379–1389. [23] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



