Submitted:
04 March 2025
Posted:
06 March 2025
You are already at the latest version
Abstract
Background: Subcarinal hemangioma is a rare benign vascular tumor and the presence of such a lesion in a patient with renal cell carcinoma is unusual. Case presentation: A 75-year-old male with a history of renal cell carcinoma was incidentally found to have a lesion in the subcarinal region during computed tomography (CT) imaging studies for screening purposes. Management and outcome: The patient underwent successful lesion resection in the subcarinal region using Uniportal video-assisted thoracic surgery (U-VATS), and histopathological examination confirmed the diagnosis of hemangioma. The patient did not report any symptoms related to the subcarinal hemangioma, and it was only discovered during routine imaging studies. Conclusion: The successful resection of the lesion through Uniportal video-assisted thoracoscopic surgery (U-VATS) indicates that minimally invasive techniques can be effective in treating such rare tumors. This case highlights the importance of thorough evaluation and follow-up in patients with a history of renal cell carcinoma, as unexpected findings like subcarinal hemangiomas can be encountered
Keywords:
subcarinal hemangioma
; renal cell carcinoma
; uniportal-video assisted thoracoscopic surgery
; computed tomography (CT) scan
Introduction
With an incidence rate of less than 0.5% among all mediastinal masses, hemangioma is a rare benign soft tissue tumor that mostly affects the liver, brain parenchyma, and subcutaneous tissue. [1]
The mediastinal hemangioma's nonspecific computed tomography computed tomography (CT) characteristics are frequently characterized as an augmenting mass or linked to calcified phleboliths. [2]
In the past, benign vascular tumors were divided into two categories: (1) lesion types, such as lymphangioma or hemangioma, which contained blood; and (2) capillary and cavernous, which contained large and small diameter vascular channels, based on the size of the vascular channels. [3]
In 2010 90–95% of kidney-related neoplasms and 3.8% of adult malignancies would be due to renal cell carcinoma (RCC), whose prevalence is growing yearly. [4]
This case report describes a patient with renal cell carcinoma who had a subcarinal hemangioma that was effectively removed via Uniportal video-assisted thoracoscopic surgery (U-VATS).
Case Presentation
A 75-year-old male patient with a known case of renal cell carcinoma underwent a chest computed tomography (CT) scan for screening purposes and incidentally found a lesion in the posterior mediastinum. The patient had no signs or symptoms and no other past medical history, his physical examination and laboratory data were normal. A computed tomography (CT) scan revealed that there was a lesion located in the posterior mediastinum in the subcarinal and para-esophageal regions. We suspected that the lesion in the posterior mediastinum was a primary malignancy, or a metastasis, not a hemangioma, due to renal cell carcinoma.
Management and Treatment
For diagnosis and treatment, on March 27, 2024, we performed a minimally invasive thoracoscopic mediastinal tumor resection by Uniportal video-assisted thoracoscopic surgery (U-VATS) and sent the resected tumor for postoperative histopathological examination (HPE). The operative note was supine position under general anesthesia with the patient intubated using double-lumen endotracheal tube for selective lung ventilation, through single port 1.5cm at mid axillary line between 4th and 5th intercostal space via Uniportal video-assisted thoracic surgery (U-VATS) we used wound protecter thoracoscope camera size 10 with 30 degree angle, grasper and sucker, the lesion located at posterior mediastinum at subcarinal and para-esophageal region, posteriorly open the posterior mediastinum by opening posterior mediastinal pleura, size of the lesion was between 5-10cm, it was round inferior to azygos vein, it has high vascularity with intercostal vein and had adhesion with esophagus, thoracic vertebrae (T4-T5) and it had drain via subcostal vein and azygos vein, adhered to subcarinal and descending aorta. We used Ligasure for the removal of adhesion, and all the feeders were secured by Hemo-lock clips. We performed an excisional biopsy. The resected lesion was sent for histopathological examination (HPE). The surgery was successful, and postoperative recovery was uneventful. The histopathological examination result was mediastinal hemangioma, and the patient was discharged home on April 2, 2024, in stable condition after staying 24 hours at the ICU post op and 4 days at the ward. The patient was examined at the first visit 1 week later, the second visit was 1 month later, and the third visit was 3 months later. The patient showed no signs of complications or recurrence during the follow-up visits, and he is doing well and has resumed his normal daily activities without any limitations.
Figures
Figure 1.
CT scan of the patient: shows subcarinal mass.
Figure 2.
U-VATS – subcarinal mass resection.
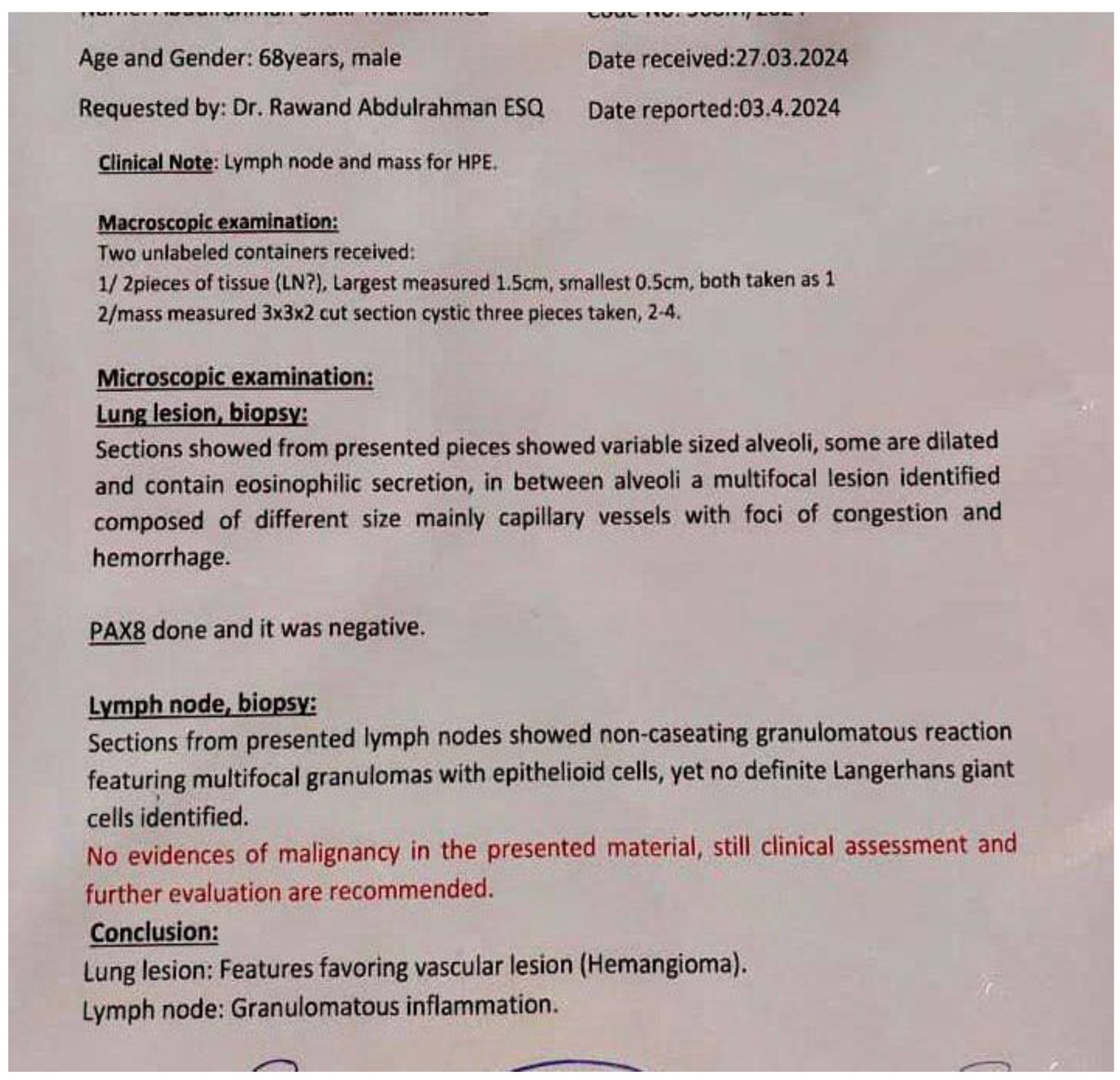
Figure 3.
HPE report.
Discussion
Of all mediastinal masses, fewer than 0.5% are mediastinal hemangiomas, an uncommon benign vascular tumor. [5]
In 1914, Shannon documented one of the earliest instances of a vascular tumor of the mediastinum. Hemangioma of the mediastinum was described by Pettersson and Romanus in 1932. [6]
As to Taori et al, there were just 125 cases of mediastinal hemangioma that were thoroughly recorded in the literature till the year 2000. [7]
The majority of mediastinal hemangiomas are benign and are categorized as cavernous or capillary hemangiomas. Less common benign varieties include venous hemangiomas, angiolymphangiomas, fibroangiomas, angiolipomas, and angioleiomyomas. [7,8]
The anterior mediastinum is where they happen most commonly, followed by the posterior compartment. Additionally, before the age of 35 year, their occurrence is greater. [1,2,9]
These lesions can be incidentally found on a chest radiograph or chest computed tomography (CT) scan. They can cause symptoms if they are infectious or if they put pressure on nearby tissues after growing larger. [10]
The clinical manifestations of mediastinal hemangioma are typically non-specific and include dyspnea, cough, wheezing, chest pain, hoarseness, superior vena cava obstruction, Horner syndrome, or dysphagia brought on by esophageal compression, and tumor invasion of the spinal canal, which may cause neurological symptoms associated with compression of the spinal cord. [1,6,11]
While focal phleboliths are observed in around 10% of instances, they are a diagnostic marker of hemangioma. The lesion typically appears as a nonspecific mass, making the preoperative identification of a mediastinal hemangioma using conventional radiography challenging. [9] Our case doesn’t have any clinical manifestations, even we sent the patient to do an endoscopy for the esophagus by an endoscopist; but there was no any esophageal relation.
In our case the hemangioma showed no calcified phlebolith and there were no any expectations regarding hemangioma because he had renal cell carcinoma. The mediastinal hemangioma displayed heterogeneous enhancement on early images and persistently increasing enhancement on delayed images. [2]
There is currently no case report describing a mediastinal hemangioma in a renal cell cancer patient.
According to a review of previously published cases in the literature, the primary treatment of choice for mediastinal hemangiomas is complete surgical resection, as was done in this case. In order to prevent serious complications, mainly bleeding, we should also protect major airways, nearby large vessels, and other vital structures. [1]
We used Uniportal video-assisted thoracoscopic surgery (U-VATS) to remove the subcarinal hemangioma completely in our patient. This procedure was safe, practicable, and resulted in reduced patient stress, a quicker recovery after surgery, and a lower risk of complications like bleeding.
Conclusions
In conclusion, hemangiomas are uncommon benign tumors of the mediastinum, and lacks specific symptoms and relevant imaging features, this study highlights the importance of doing screening in patients with history of renal cell carcinoma, as unexpected findings like subcarinal hemangiomas can be encountered, also resection using Uniportal video-assisted thoracoscopic surgery (U-VATS) would be better option due to its minimally invasive nature and quicker recovery time compared to traditional open surgery.
Author Contributions
Conception and design RAE, DSS acquisition of data RAE, DSS, analysis and interpretation of data RAE, DS, drafting of the manuscript RAE, DS, KKA. all authors critical revision of the manuscript for important intellectual content and approving final draft.
Funding
This research received no external funding.
Informed Consent Statement
Written informed consent was obtained from the patient for publication of this case report and accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Conflicts of Interest
There is no conflict to be declared.
Ethical Approval: Approval is not necessary for case report in our locality.
Abbreviations
The following abbreviations are used in this manuscript:
| U-VATS | Uniportal video-assisted thoracoscopic surgery. |
| HPE | Histopathological Examination. |
| ICU | Intensive Care Unit. |
| RCC | Renal Cell Carcinoma. |
| CT | Computed Tomography |
References
- Li, X., Li, Y., Kang, H., Mao, Y., Ma, Q., & Chen, R. (2019b). Mediastinal Cavernous Hemangioma Presenting as a Cardiophrenic Angle Mass: A Case Report and Literature Review. Iranian Red Crescent Medical Journal, 21(6). [CrossRef]
- Li, S. M., Hsu, H. H., Lee, S. C., Gao, H. W., & Ko, K. H. (2017b). Mediastinal hemangioma presenting with a characteristic feature on dynamic computed tomography images. Journal of Thoracic Disease, 9(5), E412–E415. [CrossRef]
- George, A., Mani, V., & Noufal, A. (2014b). Update on the classification of hemangioma. Journal of Oral and Maxillofacial Pathology/Journal of Oral and Maxillofacial Pathology, 18(4), 117. [CrossRef]
- Koul, H., Huh, J. S., Rove, K. O., Crompton, L., Koul, S., Meacham, R. B., & Kim, F. J. (2011b). Molecular aspects of renal cell carcinoma: a review. PubMed Central (PMC). https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3180049/.
- Kim, J. H., Lee, S. J., Kim, S. J., & Cho, B. S. (2017b). Cavernous Hemangioma Concurrently Involving the Anterior and Middle Mediastinum and the Lung Parenchyma: A Case Report. Daehan Yeongsang Uihak Hoeji/Daehan Yeongsang Ui Haghoeji, 76(4), 273. [CrossRef]
- Cohen, A. J., Sbaschnig, R. J., Hochholzer, L., Lough, F. C., & Albus, R. A. (1987b). Mediastinal Hemangiomas. the Annals of Thoracic Surgery, 43(6), 656–659. [CrossRef]
- Yoshino, N., Okada, D., Ujiie, H., Akiyama, H., Nishimura, Y., Koizumi, K., & Shimizu, K. (2012b). Venous Hemangioma of the Posterior Mediastinum. Annals of Thoracic and Cardiovascular Surgery, 18(3), 247–250. [CrossRef]
- Essa, R. A., Ahmed, S. K., Bapir, D. H., Rasul, S. A., Abubakr, C. P., & Khdir, A. A. (2021b). Surgical management of oropharynx hemangioma: A comprehensive review literature. Advances in Oral and Maxillofacial Surgery, 4, 100183. [CrossRef]
- Lim, K. E., Hsio, J. K., Hsu, Y. Y., Yue, C. T., Chang, H. C., & Huan, C. Y. (2014b). Mediastinal cavernous hemangioma. Tzu-chi Medical Journal/Cí-jì Yīxué, 26(2), 91–93. [CrossRef]
- Hirai, K., Takeuchi, S., Bessho, R., Ohaki, Y., Koizumi, K., & Shimizu, K. (2010b). Venous Hemangioma of the Anterior Mediastinum. Journal of Nippon Medical School, 77(2), 115–118. [CrossRef]
- Das, A., Das, S. K., Basuthakur, S., & Das, S. (2014b). Hemangioma in the posterior mediastinum. Lung India, 31(2), 186. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



