
Submitted:
06 March 2025
Posted:
06 March 2025
You are already at the latest version
Abstract
Background and Objectives: Kawasaki Disease (KD) is a childhood vasculitis with potential long-term neurological implications. This study examines the association between KD and subsequent neuropsychiatric and neurodevelopmental disorders using national health data from South Korea. Materials and Methods: Using the National Health Infor-mation Database, we identified KD patients diagnosed between 2002 and 2021 and se-lected those born between 2008 and 2015. A 1:4 propensity score matching was applied to create a control group. The incidence of neuropsychiatric and neurodevelopmental disor-ders from 2017 to 2021 was analyzed using Cox proportional hazards models, adjusting for age, sex, and urbanicity. Results: The study included 41,806 KD subjects and 163,829 matched controls. KD was associated with an increased risk of certain neuropsychiatric disorders: anxiety disorder (HR 1.124, 1.047–1.207), sleep-related disorder (HR 1.257, 1.094–1.444), movement disorder (HR 1.227, 1.030–1.461), and any neuropsychiatric dis-order (HR 1.102, 1.053–1.153). For neurodevelopmental disorders, KD patients showed a lower incidence of intellectual disability (HR 0.747, 0.641–0.871) but an increased risk of tic disorder (HR 1.148, 1.020–1.292). No significant associations were found with other neurodevelopmental disorders. Male gender and urban residency were associated with higher incidence rates for certain conditions. Conclusions: KD patients show increased risks for anxiety, sleep-related, movement disorder and tic disorder, a reduced incidence of intellectual disability, and a higher risk of tic disorder. These findings highlight the need for long-term neurological monitoring in KD patients and provide insights into its poten-tial neurodevelopmental impact.
Keywords:
Kawasaki disease
; neuropsychiatric disorder
; neurodevelopmental disorder
1. Introduction
Kawasaki disease (KD) is an acute systemic vasculitis primarily affecting children, with cardiac complications being the major focus of its long-term prognosis [1]. However, KD is also associated with various neurological manifestations, such as seizures, hearing loss, facial nerve palsy, and paralysis, which suggest the potential involvement of the central nervous system [2]. Previous studies have explored KD-related neurological complications using diverse approaches, such as cerebrospinal fluid (CSF) cytokine analyses and single-photon emission computed tomography (SPECT) imaging that revealed acute-phase hypoperfusion in KD patients [3,4]. These findings suggest that underlying neuroinflammatory mechanisms may contribute to the risk of neurological complications in patients with KD.
In addition to neurological complications, evidence from autoimmune diseases like systemic lupus erythematosus, rheumatoid arthritis, and ankylosing spondylitis suggests a strong association between chronic inflammatory conditions and psychiatric disorders [5-7]. Atopic dermatitis and asthma have also been linked to mental health conditions [8]. Given KD’s inflammatory nature, it is plausible to hypothesize that KD may similarly predispose patients to neuropsychiatric and neurodevelopmental disorders, thereby influencing its long-term prognosis and emphasizing the importance of early intervention and management.
While limited studies, such as national cohort studies from Taiwan and Canada, have attempted to elucidate the relationship between KD and neuropsychiatric disorders, their findings remain inconsistent [9,10]. The multifactorial etiology of neuropsychiatric diseases—encompassing genetic markers of the immune system, environmental exposures, and social determinants—further complicates this relationship [11,12]. Notably, no studies have explored this association in the context of Korean patients. This study aims to address this gap by analyzing data from the National Health Insurance Service (NHIS) to evaluate the incidence and prevalence of neurodevelopmental and neuropsychiatric disorders in children with a history of KD, providing insights into the broader impact of KD on long-term mental health outcomes.
2. Materials and Methods
2.1. Data Source
The South Korean healthcare system boasts a comprehensive public health database known as the National Health Information Database (NHID), overseen by the NHIS [13]. This extensive repository encompasses data on more than 50 million individuals, dating back to 2002, and includes information on healthcare utilization, health screenings, socio-demographic factors, and mortality rates. The NHID is composed of several interlinked databases, including eligibility, national health screening, healthcare utilization, long-term care insurance, and healthcare provider information. These databases offer detailed insights into insurance contributions, demographic data, health behaviors, medical treatments, prescription records, and healthcare facilities. To ensure privacy, the NHID employs deidentified join keys to connect these databases. This valuable resource has been instrumental for researchers investigating various diseases, health conditions, risk factors, and the impact of health policies. Access to NHID is granted through a formal application process, which necessitates ethical approval and review by the NHIS committee.
2.2. Study Design and Population
The study identified individuals diagnosed with KD using the M303 diagnostic code between 2002 and 2021. The researchers focused on patients admitted with KD as the primary diagnosis who received intravenous immunoglobulin or aspirin treatment. The cohort was further refined to include only those born between 2008 and 2015. To establish a control group, the researchers employed 1:4 propensity score matching, accounting for age, sex, and urbanicity (Figure 1). This method facilitated a balanced comparison between KD cases and controls, reducing potential confounding variables.
2.3. Study Outcomes
In our study, we categorized neurologic disorders into two main groups: neuropsychiatric disorders and neurodevelopmental disorders. The neuropsychiatric disorders category encompassed seven conditions: psychotic disorder, mood disorder, anxiety disorder, sleep-related disorder, cognitive disorder, movement disorder, and personality disorder. The neurodevelopmental disorders category included six conditions: intellectual disability, communication disorder, specific learning disorder, autism spectrum disorder, attention deficit hyperactivity disorder (ADHD), and tic disorder. We identified these disorders using their corresponding ICD-10 diagnostic codes, which are detailed in the Table S1 [14,15]. Our observational period for assessing the incidence and prevalence of these neurologic disorders spanned from 2017 to 2021. We defined incident cases as newly diagnosed neurologic disorders within this observational period. Prevalent cases were considered as the total number of subjects who received treatment for neurologic disorders during the same period.
2.4. Ethics
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Wonju Severance Christian Hospital (CR322347). Given the retrospective nature of the study utilizing anonymized claims data, the requirement for informed consent was waived.
2.5. Statistical Analysis
In our statistical analysis, we compared the baseline characteristics of KD cases and controls using the Mann–Whitney U test for continuous variables and the chi-square test for categorical variables. We employed propensity score matching with a caliper width of 0.3 and the Greedy matching method to identify KD cases and controls. To assess the incidence of neurologic disorders, we utilized a Cox proportional hazard model, expressing results as hazard ratios (HRs) with 95% confidence intervals. For prevalence assessment, we applied a logistic regression model, presenting outcomes as odds ratios (ORs) with 95% confidence intervals. In our multivariate analysis of both HR and OR, we adjusted for all variables including age, sex, and urbanicity. All statistical analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA). We considered a P value less than 0.05 to be statistically significant.
3. Results
3.1. Demographics of Study Participants
In our study of KD in Korea, we initially identified 158,766 subjects with a KD diagnosis from 2002 to 2021, drawn from a population of approximately 50 million (Figure 1). To enhance the accuracy of our cohort, we narrowed our focus to 95,461 patients who were admitted with KD as the primary diagnosis and received KD-specific treatment. Our final KD cohort consisted of 41,806 subjects born between 2008 and 2015. Using a 1:4 ratio, we identified 163,829 matched controls.
Table 1 provides a comprehensive overview of the baseline characteristics for our study participants. The KD patients had a mean age of 2.63 ± 1.84 years, while the control group had a mean age of 2.64 ± 1.85 years (p = 0.119). In terms of gender distribution, females made up 42.20% of the KD group and 42.55% of the control group, showing no significant difference between the two cohorts (p = 0.199). When examining the urban-rural split, we found that 67.11% of the KD group resided in urban areas, compared to 66.53% of the control group (p = 0.025).
3.2. Risk of Neuropsychiatric Disorders
The KD was associated with an increased risk of certain neuropsychiatric disorders, particularly anxiety disorder (HR 1.124, 1.047–1.207, p = 0.001), sleep-related disorder (HR 1.257, 1.094–1.444, p = 0.001), movement disorder (HR 1.227, 1.030–1.461, p = 0.022) and any neuropsychiatric disorder (HR 1.102, 1.053–1.153, p < 0.001) (Figure 2). No statistically significant association was found between KD and the development of psychotic disorder (HR 1.097, 0.859–1.400, p = 0.459), mood disorder (HR 1.074, 0.980–1.176, p = 0.126), cognitive disorder (HR 1.049, 0.988–1.114, p = 0.118), personality disorder (HR 1.215, 0.990–1.492, p = 0.063). Detailed incidence results were presented in Table 2. Gender had a notable impact, indicating that female correlated with lower incidences of all neuropsychiatric disorders. Urban residency was associated with higher incidence rates for mood disorder, anxiety disorder, cognitive disorder, and personality disorder.
Our analysis of prevalence yielded results consistent with those observed in the incidence study. KD patients exhibited a higher prevalence of anxiety disorder (OR 1.112, 1.037–1.192, p = 0.003), sleep-related disorder (OR 1.328, 1.163–1.518, p < 0.001), movement disorder (OR 1.324, 1.120–1.565, p = 0.001) and any neuropsychiatric disorder (OR 1.104, 1.057–1.153, p < 0.001). Detailed prevalence results were presented in Table S2.
3.3. Risk of Neurodevelopment
3.3. Risk of Neurodevelopmental Disorders
We observed the lower incidence of intellectual disability in individuals with KD compared to those without (HR 0.747, 0.641–0.871, p < 0.001). The KD was associated with an increased risk of tic disorder (HR 1.148, 1.020–1.292), p = 0.022) (Figure 3). However, KD was not associated with a risk of communication disorder (HR 0.894, 0.760–1.052, p = 0.179), specific learning disorder (HR 0.641, 0.399–1.030, p = 0.066), autism spectrum disorder (HR 0.872, 0.724–1.051, p = 0.150), ADHD (HR 1.017, 0.943–1.096, p = 0.663), and any neurodevelopmental disorder (HR 1.027, 0.971–1.086, p = 0.361). Detailed incident results were presented in Table 3. Female gender was consistently correlated with lower incidence rates across all neurodevelopmental disorders examined. In contrast, urban residency was associated with higher incidence rates for ADHD, tic disorder, and any neurodevelopmental disorder in general.
The prevalence analysis yielded results that aligned with our incidence findings. KD patients showed a significantly lower prevalence of intellectual disability compared to controls (OR 0.771, 0.674–0.883, p < 0.001). However, KD patients exhibited a higher prevalence of tic disorder (OR 1.172, 1.046–1.312, p = 0.006). Detailed prevalence results were presented in Table S3.
4. Discussion
The findings of our study provide important insights into the association between KD and neurologic disorders in children. Our results demonstrate significant associations between KD and certain neuropsychiatric and neurodevelopmental disorders, highlighting the potential long-term neurological implications of this acute systemic vasculitis.
Our analysis revealed an increased risk of anxiety disorder, sleep-related disorder, movement disorder, and overall neuropsychiatric disorders in children with a history of KD. These findings align with the growing body of evidence suggesting a link between inflammatory conditions and psychiatric disorders [2]. The association between KD and anxiety disorder is particularly noteworthy, as it may indicate a lasting impact of the acute inflammatory process on emotional regulation and stress response systems. The increased risk of sleep-related disorders in KD patients is an important finding that warrants further investigation. Sleep disturbances can significantly impact a child's quality of life, cognitive function, and overall health. The higher incidence of movement disorders in KD patients is intriguing and may suggest subtle neurological sequelae of the disease. This finding underscores the importance of long-term neurological follow-up in KD survivors, even in the absence of overt neurological symptoms during the acute phase. Interestingly, our study did not find significant associations between KD and psychotic disorders, mood disorders, cognitive disorders, or personality disorders. This selective pattern of neuropsychiatric risk suggests that KD may affect specific neural pathways or regions, rather than causing global neuropsychiatric dysfunction.
Study findings regarding neurodevelopmental disorders present a complex picture. Surprisingly, we observed a lower incidence of intellectual disability in individuals with KD compared to controls. This unexpected finding requires careful interpretation and further investigation. It is possible that children with KD receive more intensive medical care and follow-up, potentially leading to earlier detection and intervention for developmental issues, which could mitigate the risk of intellectual disability. The increased risk of tic disorder in KD patients is an important finding that adds to the growing evidence of neurological involvement in KD. Tic disorders have been associated with other inflammatory conditions, and this link with KD further supports the potential role of inflammation in the pathogenesis of tic disorders [16]. Notably, we did not find significant associations between KD and other neurodevelopmental disorders such as autism spectrum disorder, ADHD, or specific learning disorders. This selective pattern of risk suggests that the neurological impact of KD may be more nuanced than previously thought, affecting specific neurodevelopmental pathways while sparing others.
Demographic factor analyses revealed that the risk of developing neuropsychiatric and neurodevelopmental disorders varied depending on specific disease characteristics, age at KD onset, sex, and residential area. Notably, patients diagnosed with KD at age ≥5 years exhibited a lower risk of these disorders compared to those diagnosed at ≤1 year of age. This finding is consistent with a previous Taiwanese study reporting an increased cerebrovascular risk and neurological disorder in children diagnosed with KD before the age of 5 [2,17]. One possible explanation is that younger children, particularly infants, experience a more intense inflammatory response, which may have long-term effects on neurodevelopment. Given that refractory KD and coronary aneurysm complications are more common in younger patients, heightened systemic inflammation during a critical period of neuroplasticity may disrupt neurocircuitry development [18-21]. Additionally, male sex and urban residency were associated with a higher incidence of neuropsychiatric and neurodevelopmental disorders. Male patients exhibited a higher incidence of neuropsychiatric and neurodevelopmental disorders, which may be related to the increased prevalence of KD complications in males [22]. Potential biological explanations include sex-based differences in immune regulation, as suggested in prior research [23]. Furthermore, urban residency was associated with a greater risk of neuropsychiatric disorders. Previous studies also reported that urban environment is associated with an increased risk for mental illness [24,25]. However, this association may be confounded by disparities in healthcare access and diagnostic awareness, as rural populations might experience underdiagnosis of neuropsychiatric conditions due to limited healthcare resources and lower recognition of mental health issues.
The mechanisms underlying the association between KD and neuropsychiatric or neurodevelopmental disorders remain incompletely understood. KD-induced systemic inflammation may extend to cerebral vasculature, potentially leading to persistent neuroinflammatory processes that increase the risk of neuropsychiatric disorders [26-28]. This hypothesis is supported by findings of elevated cytokine levels in the CSF of KD patients compared to serum [3,29]. Chronic inflammation and vascular remodeling, which are well-documented in KD-affected coronary arteries, may similarly affect cerebral vasculature, contributing to long-term neuroinflammatory sequelae [17]. Additionally, studies linking mental health disorders with inflammatory pathways, as well as microbiome dysbiosis, provide further support for a shared pathological basis between KD and neuropsychiatric conditions [30-32]. Matrix metalloproteinases (MMPs), implicated in KD pathogenesis and psychiatric disorders, suggest potential molecular-level intersections [33-36]. Earlier studies documenting hypoperfusion in acute KD through SPECT imaging further reinforce the possibility of transient but significant cerebrovascular involvement during the disease’s acute phase [4].
While our findings highlight a potential link between KD and anxiety disorders, it is essential to note that our study did not classify neuropsychiatric outcomes based on specific complications or subgroups of KD, such as coronary artery involvement or systemic manifestations. Importantly, the observed anxiety disorders may not solely result from molecular or inflammatory mechanisms. Unlike healthy individuals, KD patients may develop anxiety related to their condition, such as concerns about potential complications, long-term health risks, or the need for ongoing medical follow-up. This raises the possibility that some anxiety disorders in KD patients may be influenced, at least in part, by psychological stress or health-related worries. Nonetheless, this psychological component does not diminish the importance of underlying biological mechanisms but rather emphasizes the multifactorial nature of the association. Future studies should address this distinction by exploring the psychological and biological factors contributing to anxiety disorders in KD patients, ideally through longitudinal or stratified analyses.
Despite these findings, our study has several limitations. First, the analysis was based solely on ICD-10 codes from administrative data, which may be prone to misclassification or underdiagnosis. Second, we were unable to account for key confounding factors such as socioeconomic status, environmental exposures, or healthcare accessibility, all of which could have influenced the observed associations. Third, we did not include clinical parameters such as inflammatory markers, fever duration, or the severity of KD complications, which may provide additional insights into the mechanisms linking KD to neuropsychiatric disorders. These limitations highlight the need for future studies that incorporate more granular clinical data, adjust for potential confounders, and explore the interplay between KD and mental health outcomes in greater detail.
Given the chronic nature of inflammatory processes in KD and its potential impact on neuropsychiatric health, it is crucial to monitor KD patients for mental health outcomes as part of their long-term prognosis. Our findings suggest that mental health surveillance should be integrated into the long-term care of KD patients. Interdisciplinary research, combining clinical, molecular, and psychological approaches, is essential to uncover the complex interplay between KD and neuropsychiatric disorders. Future studies should aim to identify high-risk subgroups and establish preventive strategies, potentially improving long-term outcomes for KD patients.
5. Conclusions
This national cohort study demonstrates that KD is associated with an increased risk of specific neuropsychiatric disorders, including anxiety, sleep-related, movement, and tic disorders, while showing a lower incidence of intellectual disability. These findings suggest potential long-term neurological impacts of KD, possibly driven by systemic inflammation and immune dysregulation. Given these results, long-term neurological monitoring and mental health surveillance should be considered for KD patients. Future research should explore underlying mechanisms and identify high-risk subgroups to improve long-term care strategies.
Supplementary Materials
The following supporting information can be downloaded at: Preprints.org, Table S1: Diagnostic code of neuropsychiatric and neurodevelopmental disorders; Table S2: Comparison of the number of prevalent cases in neuropsychiatric disorder.; Table S3: Comparison of the number of prevalent cases in neurodevelopmental disorder.
Author Contributions
Conceptualization, J.H.S.; methodology, J.H.L.; validation, J.H.S.; formal analysis, T.W.S. and J.H.L.; investigation, J.H.L.; data curation, J.H.L.; writing—original draft preparation, T.W.S. and J.H.L.; writing—review and editing, J.M.P. and J.H.S.; visualization, J.H.L.; supervision, J.H.S. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of Wonju Severance Christian Hospital (CR322347).
Informed Consent Statement
Given the retrospective nature of the study utilizing anonymized claims data, the requirement for informed consent was waived.
Data Availability Statement
The data that support the findings of this study were obtained from the National Health Insurance Service (NHIS) of Korea under strict confidentiality agreements. Due to privacy regulations and data sharing policies of the NHIS, these data cannot be shared publicly. Researchers interested in accessing the data can request access directly from the NHIS (https://nhiss.nhis.or.kr).
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| KD | Kawasaki Disease |
| ADHD | Attention Deficit Hyperactivity Disorder |
| HR OR SPECT NHIS |
Hazard Ratio Odds Ratio Single-Photon Emission Computed Tomography National Health Insurance Service |
References
- Kawasaki, T.; Kosaki, F.; Okawa, S.; Shigematsu, I.; Yanagawa, H. A new infantile acute febrile mucocutaneous lymph node syndrome (MLNS) prevailing in Japan. Pediatrics 1974, 54, 271-276.
- Mauro, A.; Di Mari, C.; Casini, F.; Giani, T.; Sandini, M.; Biondi, L.; Calcaterra, V.; Zuccotti, G.V.; Bernardo, L. Neurological manifestations of Kawasaki disease and multisystem inflammatory syndrome in children associated with COVID-19: a comparison of two different clinical entities. Front. Pediatr. 2022, 10, 1088773. [CrossRef]
- Ogihara, Y.; Ogata, S.; Nomoto, K.; Ebato, T.; Sato, K.; Kokubo, K.; Kobayashi, H.; Ishii, M. Transcriptional regulation by infliximab therapy in Kawasaki disease patients with immunoglobulin resistance. Pediatr. Res. 2014, 76, 287-293. [CrossRef]
- Ichiyama, T.; Nishikawa, M.; Hayashi, T.; Koga, M.; Tashiro, N.; Furukawa, S. Cerebral hypoperfusion during acute Kawasaki disease. Stroke 1998, 29, 1320-1321. [CrossRef]
- Sundquist, K.; Li, X.; Hemminki, K.; Sundquist, J. Subsequent risk of hospitalization for neuropsychiatric disorders in patients with rheumatic diseases: a nationwide study from Sweden. Arch. Gen. Psychiatry 2008, 65, 501-507. [CrossRef]
- Benros, M.E.; Eaton, W.W.; Mortensen, P.B. The epidemiologic evidence linking autoimmune diseases and psychosis. Biol. Psychiatry 2014, 75, 300-306. [CrossRef]
- Eaton, W.W.; Byrne, M.; Ewald, H.; Mors, O.; Chen, C.Y.; Agerbo, E.; Mortensen, P.B. Association of schizophrenia and autoimmune diseases: linkage of Danish national registers. Am. J. Psychiatry 2006, 163, 521-528. [CrossRef]
- Khandaker, G.M.; Zammit, S.; Lewis, G.; Jones, P.B. A population-based study of atopic disorders and inflammatory markers in childhood before psychotic experiences in adolescence. Schizophr. Res. 2014, 152, 139-145. [CrossRef]
- Chen, D.T.; Chang, J.P.; Cheng, S.W.; Chang, H.C.; Hsu, J.H.; Chang, H.H.; Chiu, W.C.; Su, K.P. Kawasaki disease in childhood and psychiatric disorders: a population-based case-control prospective study in Taiwan. Brain Behav. Immun. 2022, 100, 105-111. [CrossRef]
- Robinson, C.; Lao, F.; Chanchlani, R.; Gayowsky, A.; Darling, E.; Batthish, M. Long-term hearing and neurodevelopmental outcomes following Kawasaki disease: a population-based cohort study. Brain Dev. 2021, 43, 735-744. [CrossRef]
- Kambeitz, J.; Meyer-Lindenberg, A. Modelling the impact of environmental and social determinants on mental health using generative agents. NPJ Digit. Med. 2025, 8, 36. [CrossRef]
- Werner, M.C.F.; Wirgenes, K.V.; Shadrin, A.; Lunding, S.H.; Rodevand, L.; Hjell, G.; Ormerod, M.; Haram, M.; Agartz, I.; Djurovic, S., et al. Immune marker levels in severe mental disorders: associations with polygenic risk scores of related mental phenotypes and psoriasis. Transl. Psychiatry 2022, 12, 38. [CrossRef]
- Cheol Seong, S.; Kim, Y.Y.; Khang, Y.H.; Heon Park, J.; Kang, H.J.; Lee, H.; Do, C.H.; Song, J.S.; Hyon Bang, J.; Ha, S., et al. Data resource profile: the national health information database of the National Health Insurance Service in South Korea. Int. J. Epidemiol. 2017, 46, 799-800. [CrossRef]
- Park, J.S.; Cho, Y.J.; Yun, J.Y.; Lee, H.J.; Yu, J.; Yang, H.J.; Suh, D.I.; Korean childhood Asthma, REsearch team. Leukotriene receptor antagonists and risk of neuropsychiatric events in children, adolescents and young adults: a self-controlled case series. Eur. Respir. J. 2022, 60, 2102467. [CrossRef]
- Straub, L.; Bateman, B.T.; Hernandez-Diaz, S.; York, C.; Zhu, Y.; Suarez, E.A.; Lester, B.; Gonzalez, L.; Hanson, R.; Hildebrandt, C., et al. Validity of claims-based algorithms to identify neurodevelopmental disorders in children. Pharmacoepidemiol. Drug Saf. 2021, 30, 1635-1642. [CrossRef]
- Yin, W.; Wu, Y.; Wang, S.; Tang, H.; Ding, Y. Kawasaki disease involving both the nervous system and cardiovascular system: a case report and literature review. Front. Pediatr. 2024, 12, 1459143. [CrossRef]
- Lin, C.H.; Lai, J.N.; Lee, I.C.; Chou, I.C.; Lin, W.D.; Lin, M.C.; Hong, S.Y. Kawasaki disease may increase the risk of subsequent cerebrovascular disease. Stroke 2022, 53, 1256-1262. [CrossRef]
- Correction to: Update on diagnosis and management of Kawasaki disease: a scientific statement from the American Heart Association. Circulation 2025, 151, e677-e679. [CrossRef]
- Lersch, R.; Mandilaras, G.; Schrader, M.; Anselmino, F.; Haas, N.A.; Jakob, A. Have we got the optimal treatment for refractory Kawasaki disease in very young infants? A case report and literature review. Front. Pediatr. 2023, 11, 1210940. [CrossRef]
- Takekoshi, N.; Kitano, N.; Takeuchi, T.; Suenaga, T.; Kakimoto, N.; Suzuki, T.; Kada, T.T.; Shibuta, S.; Tachibana, S.; Murayama, Y., et al. Analysis of age, sex, lack of Response to intravenous immunoglobulin, and development of coronary artery abnormalities in children with Kawasaki disease in Japan. JAMA Netw. Open 2022, 5, e2216642. [CrossRef]
- Weiser, M.J.; Butt, C.M.; Mohajeri, M.H. Docosahexaenoic acid and cognition throughout the lifespan. Nutrients 2016, 8, 99. [CrossRef]
- Rowley, A.H.; Shulman, S.T. The epidemiology and pathogenesis of Kawasaki disease. Front. Pediatr. 2018, 6, 374. [CrossRef]
- Niu, P.; Li, L.; Zhang, Y.; Su, Z.; Wang, B.; Liu, H.; Zhang, S.; Qiu, S.; Li, Y. Immune regulation based on sex differences in ischemic stroke pathology. Front. Immunol. 2023, 14, 1087815. [CrossRef]
- Engemann, K.; Pedersen, C.B.; Arge, L.; Tsirogiannis, C.; Mortensen, P.B.; Svenning, J.C. Residential green space in childhood is associated with lower risk of psychiatric disorders from adolescence into adulthood. Proc. Natl. Acad. Sci. U.S.A. 2019, 116, 5188-5193. [CrossRef]
- Vassos, E.; Agerbo, E.; Mors, O.; Pedersen, C.B. Urban-rural differences in incidence rates of psychiatric disorders in Denmark. Br. J. Psychiatry 2016, 208, 435-440. [CrossRef]
- Jiang, N.M.; Cowan, M.; Moonah, S.N.; Petri, W.A., Jr. The impact of systemic inflammation on neurodevelopment. Trends Mol. Med. 2018, 24, 794-804. [CrossRef]
- Freitas, B.C.; Beltrao-Braga, P.C.B.; Marchetto, M.C. Modeling inflammation on neurodevelopmental disorders using pluripotent stem cells. Adv. Neurobiol. 2020, 25, 207-218. [CrossRef]
- Bauer, M.E.; Teixeira, A.L. Inflammation in psychiatric disorders: what comes first? Ann. N. Y. Acad. Sci. 2019, 1437, 57-67. [CrossRef]
- Korematsu, S.; Uchiyama, S.; Miyahara, H.; Nagakura, T.; Okazaki, N.; Kawano, T.; Kojo, M.; Izumi, T. The characterization of cerebrospinal fluid and serum cytokines in patients with Kawasaki disease. Pediatr. Infect. Dis. J. 2007, 26, 750-753. [CrossRef]
- Chen, J.; Yue, Y.; Wang, L.; Deng, Z.; Yuan, Y.; Zhao, M.; Yuan, Z.; Tan, C.; Cao, Y. Altered gut microbiota correlated with systemic inflammation in children with Kawasaki disease. Sci. Rep. 2020, 10, 14525. [CrossRef]
- Kim, D.; Zeng, M.Y.; Nunez, G. The interplay between host immune cells and gut microbiota in chronic inflammatory diseases. Exp. Mol. Med. 2017, 49, e339. [CrossRef]
- Ouabbou, S.; He, Y.; Butler, K.; Tsuang, M. Inflammation in mental disorders: is the microbiota the missing link? Neurosci. Bull. 2020, 36, 1071-1084. [CrossRef]
- Beroun, A.; Mitra, S.; Michaluk, P.; Pijet, B.; Stefaniuk, M.; Kaczmarek, L. MMPs in learning and memory and neuropsychiatric disorders. Cell. Mol. Life Sci. 2019, 76, 3207-3228. [CrossRef]
- Carrizzo, A.; Lenzi, P.; Procaccini, C.; Damato, A.; Biagioni, F.; Ambrosio, M.; Amodio, G.; Remondelli, P.; Del Giudice, C.; Izzo, R., et al. Pentraxin 3 induces vascular endothelial dysfunction through a P-selectin/matrix metalloproteinase-1 pathway. Circulation 2015, 131, 1495-1505, discussion 1505. [CrossRef]
- Park, J.A.; Shin, K.S.; Kim, Y.W. Polymorphism of matrix metalloproteinase-3 promoter gene as a risk factor for coronary artery lesions in Kawasaki disease. J. Korean Med. Sci. 2005, 20, 607-611. [CrossRef]
- Small, C.D.; Crawford, B.D. Matrix metalloproteinases in neural development: a phylogenetically diverse perspective. Neural Regen. Res. 2016, 11, 357-362. [CrossRef]
Figure 1.
Patient selection flow.
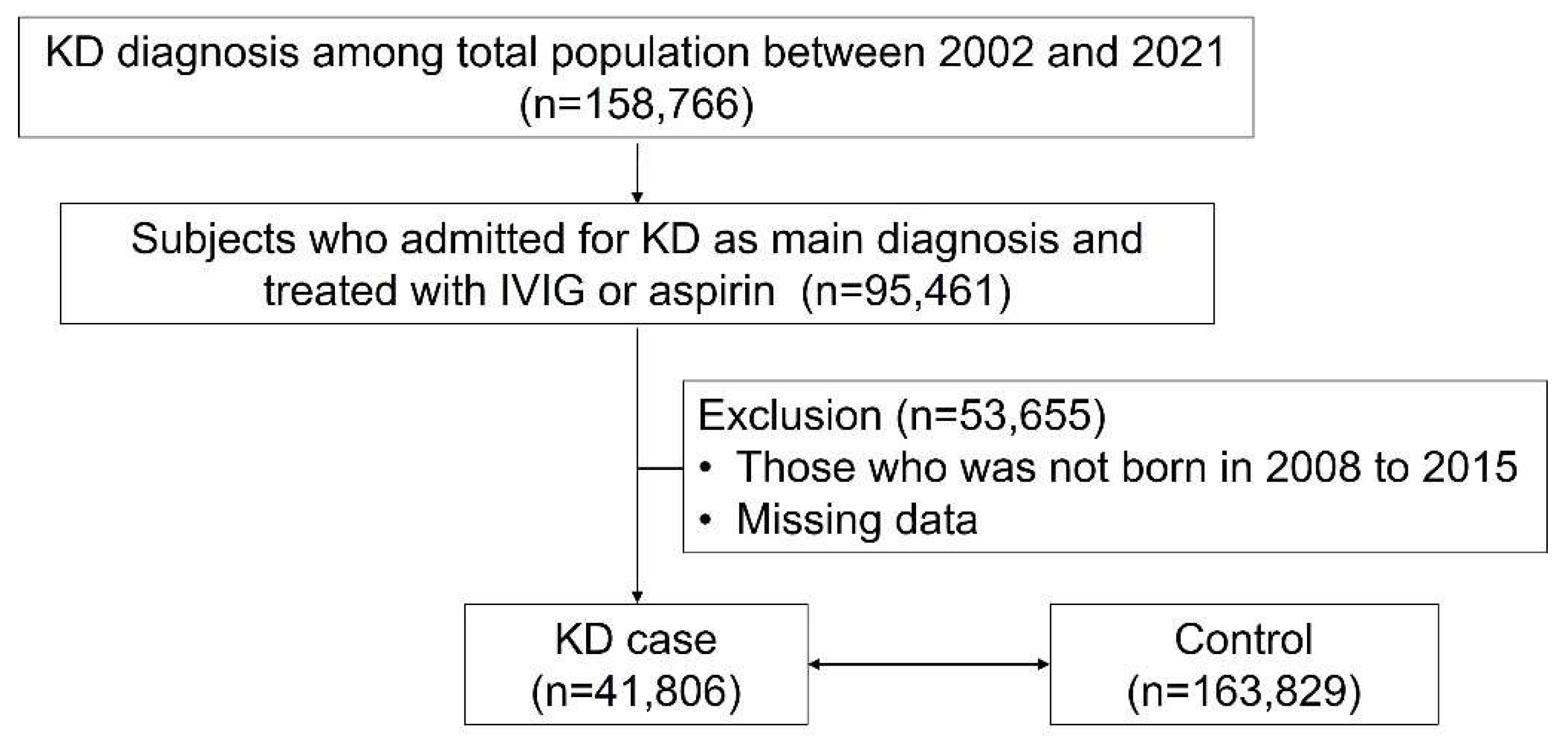
Figure 2.
Hazard ratio of psychotic disorder (a), mood disorder (b), anxiety disorder (c), sleep-related disorder (d), cognitive disorder (e), movement disorder (f), personality disorder (g), and any neuropsychiatric disorder (h) according to the demographics and Kawasaki disease.
Figure 2.
Hazard ratio of psychotic disorder (a), mood disorder (b), anxiety disorder (c), sleep-related disorder (d), cognitive disorder (e), movement disorder (f), personality disorder (g), and any neuropsychiatric disorder (h) according to the demographics and Kawasaki disease.
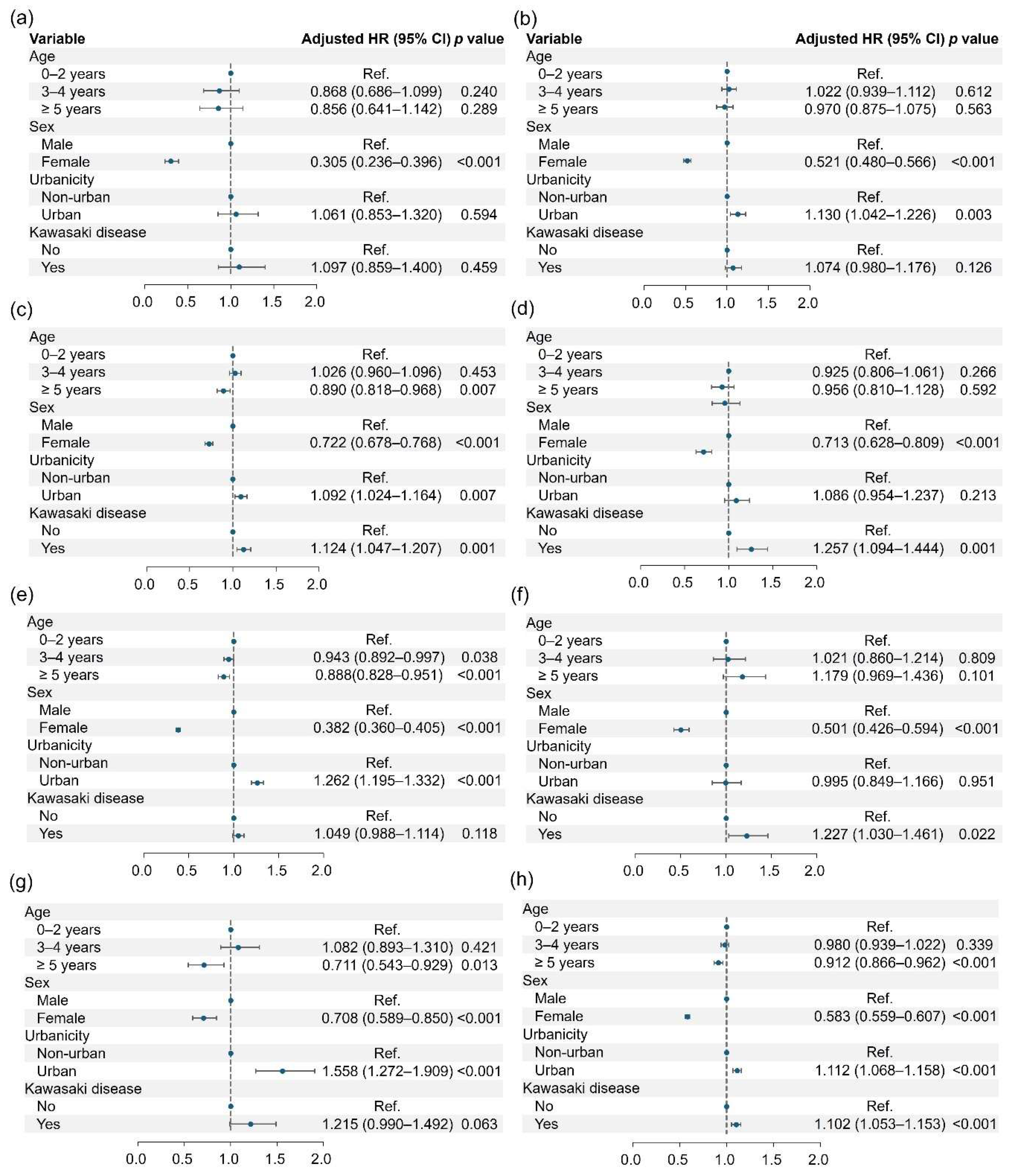
Figure 3.
Hazard ratio of intellectual disability (a), communication disorder (b), specific learning disorder (c), autism spectrum disorder (d), ADHD (e), tic disorder (f), and any neurodevelopmental disorder (g) according to the demographics and Kawasaki disease.
Figure 3.
Hazard ratio of intellectual disability (a), communication disorder (b), specific learning disorder (c), autism spectrum disorder (d), ADHD (e), tic disorder (f), and any neurodevelopmental disorder (g) according to the demographics and Kawasaki disease.
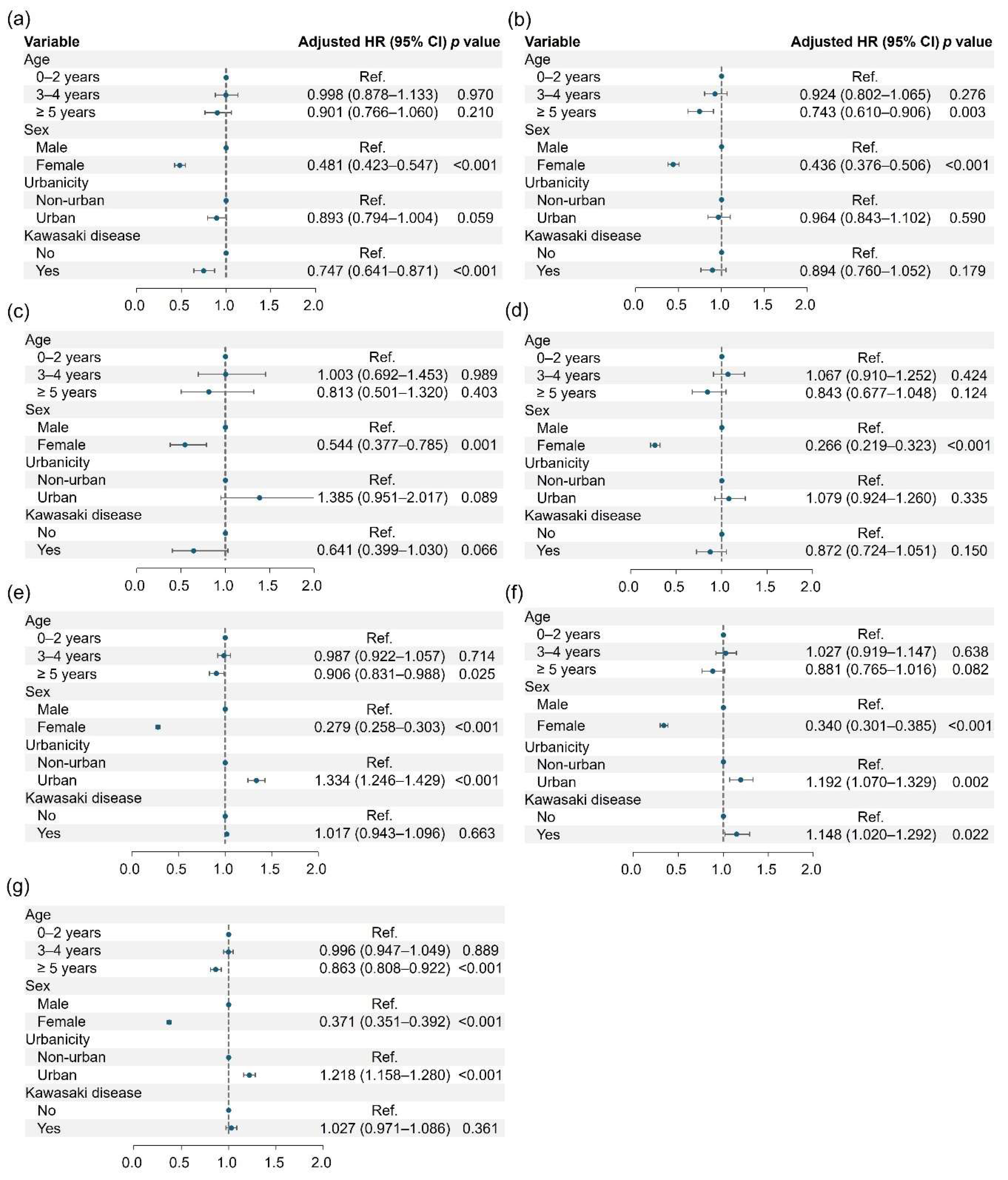

Table 1.
Baseline characteristics of the study subjects.
| Variables | KD cases (n = 41,806) |
Controls (n = 163,829) |
p |
|---|---|---|---|
| Age | |||
| Mean (years) | 2.63 ± 1.84 | 2.64 ± 1.85 | 0.119 |
| ≤ 2 years | 22,038 (52.71) | 85,992 (52.49) | 0.225 |
| 3–4 years | 13,376 (32.00) | 52,226 (31.88) | |
| ≥ 5 years | 6,392 (15.29) | 25,611 (15.63) | |
| Sex (female) | 17,643 (42.20) | 69,709 (42.55) | 0.199 |
| Urbanicity | 0.025 | ||
| Urban | 28,054 (67.11) | 108,991 (66.53) | |
| Non-urban | 13,752 (32.89) | 54,838 (33.47) |
Represented as mean ± SD or n (%). KD: Kawasaki Disease.
Table 2.
Comparison of the number of incidence cases in neuropsychiatric disorder.
| Kawasaki disease | Univariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|---|
| Case (n, %) | No | Yes | HR (95% CI) |
p | HR (95% CI) |
p |
| Psychotic disorder (-) | 163,536 (95.82) | 41,722 (99.80) | 1.000 | 1.000 | ||
| Psychotic disorder (+) | 293 (0.18) |
84 (0.20) |
1.096 (0.859–1.400) |
0.459 | 1.097 (0.859–1.400) |
0.459 |
| Mood disorder (-) |
161,639 (98.66) |
41,218 (98.59) |
1.000 | 1.000 | ||
| Mood disorder (+) |
2,190 (1.34) |
588 (1.41) |
1.068 (0.975–1.170) |
0.156 | 1.074 (0.980–1.176) |
0.126 |
| Anxiety disorder (-) |
160,403 (97.91) |
40,835 (97.68) | 1.000 | 1.000 | ||
| Anxiety disorder (+) |
3,426 (2.09) |
971 (2.32) | 1.124 (1.046–1.207) |
0.001 | 1.124 (1.047–1.207) |
0.001 |
| Sleep-related disorder (-) | 163,027 (99.51) | 41,539 (99.36) | 1.000 | 1.000 | ||
| Sleep-related disorder (+) | 802 (0.49) |
267 (0.64) | 1.254 (1.091–1.441) |
0.001 | 1.257 (1.094–1.444) |
0.001 |
| Cognitive disorder (-) | 158,718 (96.88) | 40,446 (96.75) | 1.000 | 1.000 | ||
| Cognitive disorder (+) | 5,111 (3.12) |
1,360 (3.25) |
1.046 (0.985–1.111) |
0.140 | 1.049 (0.988–1.114) |
0.118 |
| Movement disorder (-) | 163,309 (99.68) |
41,636 (99.59) |
1.000 | 1.000 | ||
| Movement disorder (+) | 520 (0.32) |
170 (0.41) |
1.222 (1.026–1.454) |
0.025 | 1.227 (1.030–1.461) |
0.022 |
| Personality disorder (-) | 163,439 (96.76) |
41,686 (99.71) | 1.000 | 1.000 | ||
| Personality disorder (+) | 390 (0.24) |
120 (0.29) | 1.219 (0.993–1.496) |
0.058 | 1.215 (0.990–1.492) |
0.063 |
| Any disorder (-) |
155,234 (94.75) | 39,400 (94.24) | 1.000 | 1.000 | ||
| Any disorder (+) |
8,595 (5.25) |
2,406 (5.76) | 1.101 (1.053–1.152) |
<0.001 | 1.102 (1.053–1.153) |
<0.001 |
Table 3.
Comparison of the number of incidence cases in neurodevelopmental disorder.
| Kawasaki disease | Univariate analysis | Multivariate analysis | ||||
|---|---|---|---|---|---|---|
| Case (n, %) | No | Yes | HR (95% CI) |
p | HR (95% CI) |
p |
| Intellectual disorder (-) | 162,817 (99.38) | 41,612 (99.54) | 1.000 | 1.000 | ||
| Intellectual disorder (+) | 1,012 (0.62) |
194 (0.46) |
0.747 (0.640–0.871) |
<0.001 | 0.747 (0.641–0.871) |
<0.001 |
| Communication disorder (-) |
163,051 (99.53) |
41,628 (99.57) |
1.000 | 1.000 | ||
| Communication disorder (+) |
778 (0.47) |
178 (0.43) |
0.897 (0.762–1.056) |
0.192 | 0.894 (0.760–1.052) |
0.179 |
| Specific learning disorder (-) | 163,708 (99.93) |
41,785 (99.95) | 1.000 | 1.000 | ||
| Specific learning disorder (+) | 121 (0.07) |
21 (0.05) | 0.643 (0.400–1.033) |
0.068 | 0.641 (0.399–1.030) |
0.066 |
| Autism spectrum disorder (-) | 163,226 (99.63) | 41,670 (99.67) | 1.000 | 1.000 | ||
| Autism spectrum disorder (+) | 603 (0.37) |
136 (0.33) | 0.876 (0.727–1.056) |
0.165 | 0.872 (0.724–1.051) |
0.150 |
| ADHD (-) |
160,512 (97.98) | 40,951 (97.95) | 1.000 | 1.000 | ||
| ADHD (+) |
3,317 (2.02) |
855 (2.05) |
1.021 (0.947–1.101) |
0.580 | 1.017 (0.943–1.096) |
0.663 |
| Tic disorder (-) |
162,608 (99.25) |
41,451 (99.15) |
1.000 | 1.000 | ||
| Tic disorder (+) |
1,221 (0.75) |
355 (0.85) |
1.154 (1.025–1.298) |
0.018 | 1.148 (1.020–1.292) |
0.022 |
| Any disorder (-) |
157,926 (96.40) | 40,262 (96.31) | 1.000 | 1.000 | ||
| Any disorder (+) |
5,903 (3.60) |
1,544 (3.69) | 1.029 (0.973–1.088) |
0.322 | 1.027 (0.971–1.086) |
0.361 |
HR: Hazard Ratio; ADHD: Attention Deficit Hyperactivity Disorder.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



