
Submitted:
11 March 2025
Posted:
11 March 2025
You are already at the latest version
Abstract
Metabolic dysfunction-associated steatotic liver disease -MASLD, is the most common chronic liver disease worldwide, one of the leading causes of cirrhosis, hepatocellular carcinoma and liver transplantation in developed countries, and an important cardiovascular risk factor. It affects about 30% of the adult population and about 10% of the paediatric population. These figures may be underestimated due to the long-standing asymptomatic or sparse course of the disease, the lack of nationwide screening for MASLD in patients with risk factors for its development and the low awareness of both patients and physicians themselves. According to projections, this number could double by 2030 due to the growing obesity epidemic and the associated development of other weight-dependent metabolic complications, such as insulin resistance, pre-diabetic state, type 2 diabetes, lipid disorders and hypertension. The basis for prevention and treatment of MASLD is weight reduction with diet and regular physical activity and modern pharmacotherapy for obesity-related disease, as well as treatment aimed at reducing the cardiometabolic factors - diabetes, hyperlipidaemia and hypertension. Pharmacological treatment of hepatic steatosis, steatohepatitis or liver fibrosis alone is limited, and many drugs are currently in clinical trials. This article presents the current pharmacological options and potential pharmacotherapy pathways for the hepatic complications of MASLD - steatosis, steatohepatitis and incipient liver fibrosis.
Keywords:
Introduction
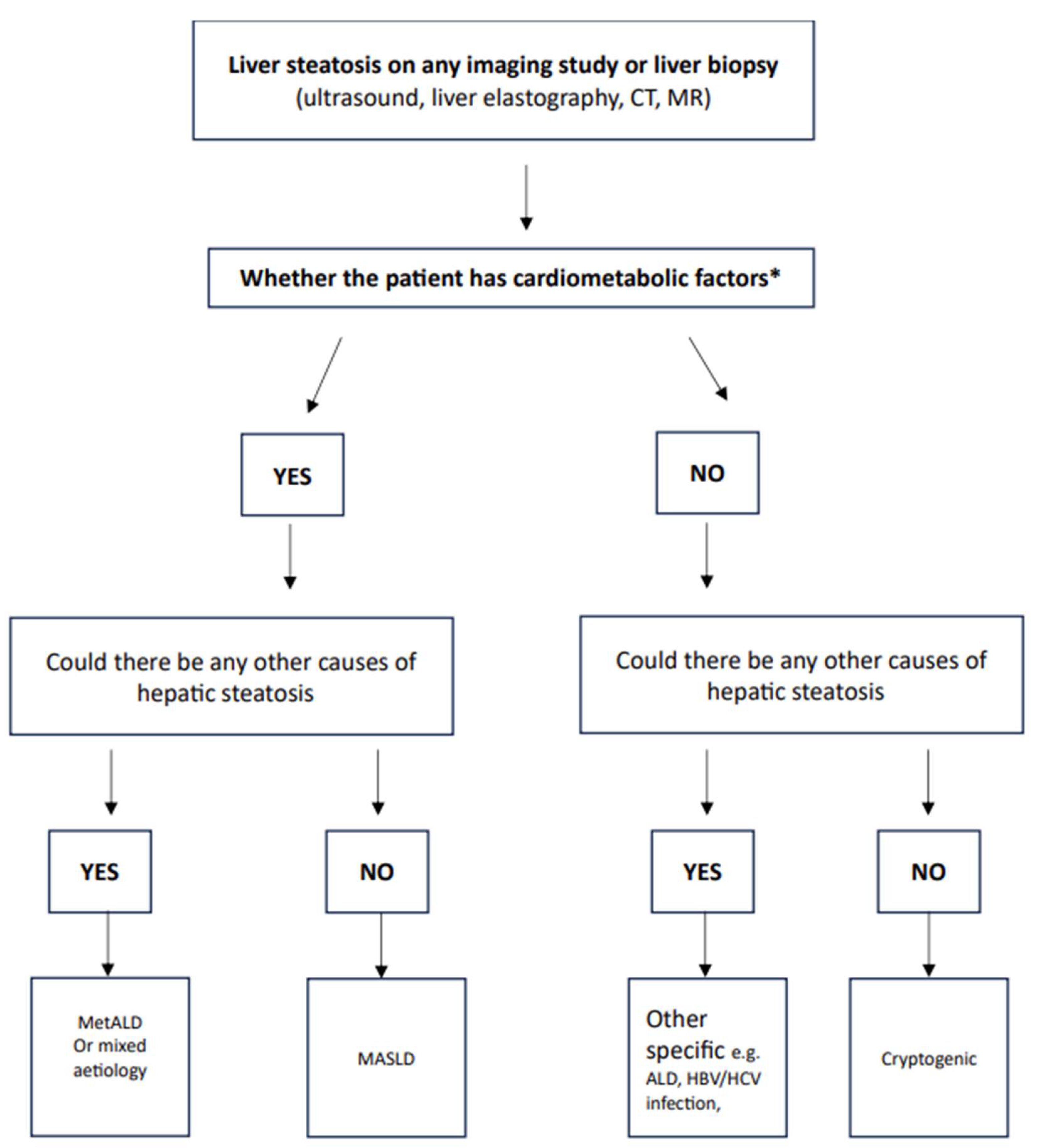
- BMI ≥25 kg/m2 or waist circumference ≥94 cm in men and ≥80 cm in women (or above normal depending on ethnicity),
- blood pressure ≥130/85 mm Hg or treatment of hypertension,
- Serum triglyceride concentration ≥1.7 mmol/l (150 mg/dl) or treatment of hypertriglyceridaemia,
- serum HDL cholesterol concentration ≤1.0 mmol/l (<40 mg/dl) in men and ≤1.3 mmol/l (<50 mg/dl) in women or treatment of hypercholesterolaemia,
- fasting glucose ≥5.6 mmol/l (100 mg/l) or 2 h after a glucose load ≥7.8 mmol/l (140 mg/dl) or HbA1c ≥5.7% (39 mmol/mol) or type 2 diabetes or treatment of type 2 diabetes.
Summary
References
- Rajewski P, Ciescinski J. The patient with steatohepatitis associated with metabolic dysfunction in clinical practice. Physician POZ. 2024;10(5).
- Kanwal, Fasiha, Neuschwander-Tetri, Brent A.; Loomba, Rohit; Rinella, Mary E. Metabolic dysfunction-associated steatotic liver disease: Update and impact of new nomenclature on the American Association for the Study of Liver Diseases practice guidance on nonalcoholic fatty liver disease. Hepatology 79(5):p 1212-1219, May 2024. |. [CrossRef]
- Devarbhavi H, Asrani SK, Arab JP, Nartey YA, Pose E, Kamath PS. Global burden of liver disease: 2023 update. J Hepatol. 2023 Aug;79(2):516-537. epub 2023 Mar 27. PMID: 36990226. [CrossRef]
- Rinella ME, Lazarus JV, Ratziu V, Francque SM, Sanyal AJ, Kanwal F, Romero D, Abdelmalek MF, Anstee QM, Arab JP, Arrese M, Bataller R, Beuers U, Boursier J, Bugianesi E, Byrne CD, Castro Narro GE, Chowdhury A, Cortez-Pinto H, Cryer DR, Cusi K, El-Kassas M, Klein S, Eskridge W, Fan J, Gawrieh S, Guy CD, Harrison SA, Kim SU, Koot BG, Korenjak M, Kowdley KV, Lacaille F, Loomba R, Mitchell-Thain R, Morgan TR, Powell EE, Roden M, Romero-Gómez M, Silva M, Singh SP, Sookoian SC, Spearman CW, Tiniakos D, Valenti L, Vos MB, Wong VW, Xanthakos S, Yilmaz Y, Younossi Z, Hobbs A, Villota-Rivas M, Newsome PN; NAFLD Nomenclature consensus group. A multisociety Delphi consensus statement on new fatty liver disease nomenclature. Hepatology. 2023 Dec 1;78(6):1966-1986. Epub 2023 Jun 24. PMID: 37363821; PMCID: PMC10653297. [CrossRef]
- Rinella ME, Neuschwander-Tetri BA, Siddiqui MS, Abdelmalek MF, Caldwell S, Barb D, Kleiner DE, Loomba R. AASLD Practice Guidance on the clinical assessment and management of nonalcoholic fatty liver disease. Hepatology. 2023 May 1;77(5):1797-1835. Epub 2023 Mar 17. PMID: 36727674; PMCID: PMC10735173. [CrossRef]
- Rajewski P, Ciescinski J, Rajewski P (2024) Use of Fibroscan Liver Elastography in the Rapid Diagnosis and Monitoring of MASLD Treatment. Ann Case Report. 9: 2129. [CrossRef]
- Vilar-Gomez E, Martinez-Perez Y, Calzadilla-Bertot L; et al. Weight loss through lifestyle modification signicantly reduces features of nonalcoholic steatohepatitis. Gastroenterology 2015; 149: 367-378.
- Hannah WN Jr, Harrison SA. Effect of Weight Loss, Diet, Exercise, and Bariatric Surgery on Nonalcoholic Fatty Liver Disease. Clin Liver Dis. 2016 May;20(2):339-50. epub 2016 Feb 17. PMID: 27063273. [CrossRef]
- Konerman MA et al. Pharmacotherapy for NASH: Current and emerging. J Hepatol (2017). [CrossRef]
- Suwała, S.; Junik, R. Assessment of the Liver Steatosisand Fibrosis Risk in Metabolic Syndrome and Its IndividualComponents, Considering the Varying Definitions Used in Clinical Practice throughout Time: A Retrospective Cross-Sectional Study. Biomedicines 2024, 12, 1739. [CrossRef]
- Cornell, S. A Review of GLP-1 Receptor Agonists in Type 2 Diabetes: A Focus on the Mechanism of Action of Once-weekly Agents. J Clin Pharm Ther 2020, 45, 17-27. [CrossRef]
- Wełnicki, M.; Gorczyca-Głowacka, I.; Mamcarz, A.; Filipiak, K.J.; Wożakowska-Kapłon, B.; Barylski, M.; Szymański, F.M.; Kasprzak, J.D.; Grabowski, M.; Dzida, G. The Use of GLP-1 Analogues in the Treatment of Diabetes in Patients with Cardiovascular Diseases. The Expert Opinion of the Working Group of Cardiovascular Pharmacotherapy of the Polish Cardiac Society. Kardiol Pol 2022, 80, 1286-1289. [CrossRef]
- Matyjaszek-Matuszek, B.; Szafraniec, A.; Porada, D. Pharmacotherapy of Obesity - State of the Art. EndocrinolPol 2018, 69. [CrossRef]
- Shao, N.; Kuang, H.Y.; Hao, M.; Gao, X.Y.; Lin, W.J.; Zou, W. Benefits of Exenatide on Obesity and Non-alcoholicFatty Liver Disease with Elevated Liver Enzymes in Patientsswith Type 2 Diabetes. Diabetes Metab Res Rev 2014, 30, 521-529. [CrossRef]
- Bi, Y.; Zhang, B.; Xu, W.; Yang, H.; Feng, W.; Li, C.; Tong, G.; Li, M.; Wang, X.; Shen, S.; et al. Effects of Exenatide, Insulin, and Pioglitazone on Liver Fat Content and Body Fat Distributions in Drug-Naive Subjects with Type 2 Diabetes. Acta Diabetol 2014, 51, 865-873. [CrossRef]
- Armstrong, M.J.; Gaunt, P.; Aithal, G.P.; Barton, D.; Hull, D.; Parker, R.; Hazlehurst, J.M.; Guo, K.; Abouda, G.; Aldersley, M.A.; et al. Liraglutide Safety and Efficacy in Patients with Non-Alcoholic Steatohepatitis (LEAN): A Multicentre, Double-Blind, Randomised, Placebo-ControlledPhase 2 Study. The Lancet 2016, 387, 679-690. [CrossRef]
- Bouchi, R.; Nakano, Y.; Fukuda, T.; Takeuchi, T.; Murakami, M.; Minami, I.; Izumiyama, H.; Hashimoto, K.; Yoshimoto, T.; Ogawa, Y. Reduction of Visceral Fat by Liraglutide Is Associated with Ameliorations of HepaticSteatosis, Albuminuria, and Micro-Inflammation in Type 2 Diabetic Patients with Insulin Treatment: A RandomizedControl Trial. Endocr J 2017, 64, 269-281. [CrossRef]
- Yan, J.; Yao, B.; Kuang, H.; Yang, X.; Huang, Q.; Hong, T.; Li, Y.; Dou, J.; Yang, W.; Qin, G.; et al. Liraglutide, Sitagliptin, and Insulin Glargine Added to Metformin: The Effect on Body Weight and Intrahepatic Lipid in Patients With Type 2 Diabetes Mellitus and Nonalcoholic Fatty LiverDisease. Hepatology 2019, 69, 2414-2426. [CrossRef]
- Guo, W.; Tian, W.; Lin, L.; Xu, X. Liraglutide or Insulin Glargine Treatments Improves Hepatic Fat in Obese Patientsswith Type 2 Diabetes and Nonalcoholic Fatty Liver Disease in Twenty-Six Weeks: A Randomized Placebo-Controlled Trial. Diabetes Res Clin Pract 2020, 170, 108487. [CrossRef]
- Smits, M.M.; Tonneijck, L.; Muskiet, M.H.A.; Kramer, M.H.H.; Pouwels, P.J.W.; Pieters-van den Bos, I.C.; Hoekstra, T.; Diamant, M.; van Raalte, D.H.; Cahen, D.L. Twelve WeekLiraglutide or Sitagliptin Does Not Affect Hepatic Fat in Type2 Diabetes: A Randomised Placebo-Controlled Trial. Diabetologia 2016, 59, 2588-2593. [CrossRef]
- . Kuchay, M.S.; Krishan, S.; Mishra, S.K.; Choudhary, N.S.; Singh, M.K.; Wasir, J.S.; Kaur, P.; Gill, H.K.; Bano, T.; Farooqui, K.J.; et al. Effect of Dulaglutide on Liver Fat in Patients with Type 2 Diabetes and NAFLD: RandomisedControlled Trial (D-LIFT Trial). Diabetologia 2020, 63, 2434-2445. [CrossRef]
- Gad, A.I.; Ibrahim, N.F.; Almadani, N.; Mahfouz, R.; Nofal, H.A.; El-Rafey, D.S.; Ali, H.T.; EL-Hawary, A.T.; Sadek, A.M.E.M. Therapeutic Effects of Semaglutide on Nonalcoholic Fatty Liver Disease with Type 2 DiabetesMellitus and Obesity: An Open-Label Controlled Trial. Diseases 2024, 12, 186. [CrossRef]
- Flint, A.; Andersen, G.; Hockings, P.; Johansson, L.; Morsing, A.; Sundby Palle, M.; Vogl, T.; Loomba, R.; Plum-Mörschel, L. Randomised Clinical Trial: Semaglutide versus Placebo Reduced Liver Steatosis but Not Liver Stiffness in Subjects with Non-alcoholic Fatty Liver Disease Assessed by Magnetic Resonance Imaging. Aliment Pharmacol Ther 2021, 54, 1150-1161. [CrossRef]
- Carretero-Gómez, J.; Carrasco-Sánchez, F.J.; Fernández-Rodríguez, J.M.; Casado-Escribano, P.; Miramontes-González, J.P.; Seguí-Ripoll, J.M.; Ena, J.; Arévalo-Lorido, J.C.. Effect of Semaglutide on Fatty Liver Disease Biomarkers in Patientsswith Diabetes and Obesity. Revista Clínica Española (English Edition) 2023, 223, 134-143. [CrossRef]
- Katsarou, A.; Tsioulos, G.; Kassi, E.; Chatzigeorgiou, A. Current and Experimental Pharmacotherapy for the Management of Non-Alcoholic Fatty Liver Disease. Hormones 2024, 23, 621-636. [CrossRef]
- Gastaldelli, A.; Cusi, K.; Fernández Landó, L.; Bray, R.; Brouwers, B.; Rodríguez, Á. Effect of Tirzepatide versus Insulin Degludec on Liver Fat Content and AbdominalAdipose Tissue in People with Type 2 Diabetes (SURPASS-3 MRI): A Substudy of the Randomised, Open-Label, Parallel-Group, Phase 3 SURPASS-3 Trial. Lancet DiabetesEndocrinol 2022, 10, 393-406. [CrossRef]
- Jastreboff, A.M.; Kaplan, L.M.; Frías, J.P.; Wu, Q.; Du, Y.; Gurbuz, S.; Coskun, T.; Haupt, A.; Milicevic, Z.; Hartman, M.L. Triple-Hormone-Receptor Agonist Retatrutide for Obesity - A Phase 2 Trial. New England Journal of Medicine2023, 389, 514-526. [CrossRef]
- Mantovani, A.; Byrne, C.D.; Targher, G. Efficacy of Peroxisome Proliferator-Activated Receptor Agonists, Glucagon-like Peptide-1 Receptor Agonists, or Sodium-Glucose Cotransporter-2 Inhibitors for Treatment of Non-Alcoholic Fatty Liver Disease: A Systematic Review. Lancet Gastroenterol Hepatol 2022, 7, 367-378. [CrossRef]
- Ciardullo, S.; Vergani, M.; Perseghin, G. NonalcoholicFatty Liver Disease in Patients with Type 2 Diabetes: Screening, Diagnosis, and Treatment. J Clin Med 2023, 12, 5597. [CrossRef]
- Knowler, W.C.; Barrett-Connor, E.; Fowler, S.E.; Hamman, R.F.; Lachin, J.M.; Walker, E.A.; Nathan, D.M.; Diabetes Prevention Program Research Group Reduction in the Incidence of Type 2 Diabetes with Lifestyle Interventionor Metformin. N Engl J Med 2002, 346, 393-403. [CrossRef]
- Li, Y.; Liu, L.; Wang, B.; Wang, J.; Chen, D. Metforminin Non-Alcoholic Fatty Liver Disease: A Systematic Reviewand Meta-Analysis. Biomed Rep 2013, 1, 57-64. [CrossRef]
- Lavine, J.E.; Schwimmer, J.B.; Van Natta, M.L.; Molleston, J.P.; Murray, K.F.; Rosenthal, P.; Abrams, S.H.; Scheimann, A.O.; Sanyal, A.J.; Chalasani, N.; et al. Effect of Vitamin E or Metformin for Treatment of Nonalcoholic FattyLiver Disease in Children and Adolescents: The TONIC Randomized Controlled Trial. JAMA 2011, 305, 1659-1668. [CrossRef]
- Donal, E.; L'official, G.; Kosmala, W. New Guidelinesfor Managing Chronic Heart Failure Patients and New Needsin Echocardiography. Int J Cardiol 2022, 353, 71-72. [CrossRef]
- Kuchay, M.S.; Krishan, S.; Mishra, S.K.; Farooqui, K.J.; Singh, M.K.; Wasir, J.S.; Bansal, B.; Kaur, P.; Jevalikar, G.; Gill, H.K.; et al. Effect of Empagliflozin on Liver Fat in Patients With Type 2 Diabetes and Nonalcoholic Fatty LiverDisease: A Randomized Controlled Trial (E-LIFT Trial). Diabetes Care 2018, 41, 1801-1808. [CrossRef]
- Shimizu, M.; Suzuki, K.; Kato, K.; Jojima, T.; Iijima, T.; Murohisa, T.; Iijima, M.; Takekawa, H.; Usui, I.; Hiraishi, H.; et al. Evaluation of the Effects of Dapagliflozin, a Sodium-glucose Co-transporter-2 Inhibitor, on Hepatic Steatosis and Fibrosis Using Transient Elastography in Patients with Type 2 Diabetes and Non-alcoholic Fatty Liver Disease. DiabetesObes Metab 2019, 21, 285-292. [CrossRef]
- Belfort, R.; Harrison, S.A.; Brown, K.; Darland, C.; Finch, J.; Hardies, J.; Balas, B.; Gastaldelli, A.; Tio, F.; Pulcini, J.; et al. A Placebo-Controlled Trial of Pioglitazone in Subjects with Nonalcoholic Steatohepatitis. New England Journal of Medicine 2006, 355, 2297-2307. [CrossRef]
- Cusi, K.; Orsak, B.; Bril, F.; Lomonaco, R.; Hecht, J.; Ortiz-Lopez, C.; Tio, F.; Hardies, J.; Darland, C.; Musi, N.; et al. Long-Term Pioglitazone Treatment for Patients With Nonalcoholic Steatohepatitis and Prediabetes or Type 2 Diabetes Mellitus. Ann Intern Med 2016, 165, 305. [CrossRef]
- Pawlak M., Lefebyre P., Staels B.: Molecular mechanism of PPARα action and its impact on lipid metabolism, inflammation and fibrosis in non-alcoholic fatty liver disease. J. Hepatol., 2015; 62: 720-733.
- . Harrison, S.A.; Fincke, C.; Helinski, D.; Torgerson, S.; Hayashi, P. A Pilot Study of Orlistat Treatment in Obese, Non-alcoholic Steatohepatitis Patients. Aliment Pharmacol Ther2004, 20, 623-628. [CrossRef]
- Zelber-Sagi, S.; Kessler, A.; Brazowsky, E.; Webb, M.; Lurie, Y.; Santo, M.; Leshno, M.; Blendis, L.; Halpern, Z.; Oren, R. A Double-Blind Randomized Placebo-ControlledTrial of Orlistat for the Treatment of Nonalcoholic Fatty LiverDisease. Clinical Gastroenterology and Hepatology 2006, 4, 639-644. [CrossRef]
- Esmail, V.A.W.; Mohammed, M.O.; Al-Nimer, M.S.M. Short-Term Orlistat Therapy Improves Fatty InfiltrationIndices and Liver Fibrosis Scores in Patients with Non-Alcoholic Fatty Liver Disease and Metabolic Syndrome. Arab Journal of Gastroenterology 2021, 22, 1-5. [CrossRef]
- Zahmatkesh, A.; Sohouli, M.H.; Shojaie, S.; Rohani, P. The Effect of Orlistat in the Treatment of Non-Alcoholic FattyLiver in Adolescents with Overweight and Obese. Eur J Pediatr 2023, 183, 1173-1182. [CrossRef]
- Harrison, S.A.; Fecht, W.; Brunt, E.M.; Neuschwander-Tetri, B.A.. Orlistat for Overweight Subjects with Nonalcoholic Steatohepatitis. Hepatology 2009, 49, 80-86. [CrossRef]
- Xu, R.; Tao, A.; Zhang, S.; Deng, Y.; Chen, G. Association between Vitamin E and Non-AlcoholicSteatohepatitis: A Meta-Analysis. Int J Clin Exp Med 2015, 8, 3924-3934.
- Mahmoud, A.; Mohamed, I.; Abuelazm, M.; Ahmed, A.A.S.; Saeed, A.; Elshinawy, M.; Almaadawy, O.; Abdelazeem, B. Efficacy of Orlistat in Obese Patients with Nonalcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. BaylorUniversity Medical Center Proceedings 2024, 37, 603-612. [CrossRef]
- Klein EA, Thompson Jr IM, Tangen CM; et al. Vitamin E and the risk of prostate cancer: The Selenium and Vitamin E Cancer Prevention Trial (SELECT). JAMA 2011;306:1549-1556.
- Miller 3rd ER, Pastor-Barriuso R, Dalal D; et al. Meta- analysis: High-dosage vitamin E supplementation may increase all-cause mortality. Ann Intern Med 2005;142:37-46.
- Khoo, S.; Wong, V.W.; Goh, G.B.; Fan, J.; Chan, W.K.; Seto, W.; Chow, W.C.. Suboptimal Treatment of Dyslipidemiain Patients with Nonalcoholic Fatty Liver Disease. J Gastroenterol Hepatol 2020, 35, 320-325. [CrossRef]
- Ayada, I.; van Kleef, L.A.; Zhang, H.; Liu, K.; Li, P.; Abozaid, Y.J.; Lavrijsen, M.; Janssen, H.L.A.; van der Laan, L.J.W.; Ghanbari, M.; et al. Dissecting the MultifacetedImpact of Statin Use on Fatty Liver Disease: A Multidimensional Study. EBioMedicine 2023, 87, 104392. [CrossRef]
- Rajewski P, Kwiatkowska J, Nowicka-Matuszewska A, Rajewski P. Safety of statins in chronic liver disease. Physician POZ. 2024;10(2):111-117.
- Cho, Y.; Rhee, H.; Kim, Y.; Lee, M.; Lee, B.-W.; Kang, E.S.; Cha, B.-S.; Choi, J.-Y.; Lee, Y. Ezetimibe Combination Therapy with Statin for Non- Alcoholic Fatty Liver Disease: An Open-Label Randomized Controlled Trial (ESSENTIAL Study). BMC Med 2022, 20, 93. [CrossRef]
- Gorczyca-Głowacka, I.; Wełnicki, M.; Mamcarz, A.; Filipiak, K.J.; Wożakowska-Kapłon, B.; Barylski, M.; Szymański, F.M.; Kasprzak, J.D.; Tomasiewcz, K. MetabolicAssociated Fatty Liver Disease and Cardiovascular Risk: The Expert Opinion of the Working Group on CardiovascularPharmacotherapy of the Polish Cardiac Society. Kardiol Pol2023, 81, 207-214. [CrossRef]
- Dufour, J.; Oneta, C.M.; Gonvers, J.; Bihl, F.; Cerny, A.; Cereda, J.; Zala, J.; Helbling, B.; Steuerwald, M.; Zimmermann, A. Randomized Placebo-Controlled Trial of Ursodeoxycholic Acid With Vitamin E in NonalcoholicSteatohepatitis. Clinical Gastroenterology and Hepatology2006, 4, 1537-1543. [CrossRef]
- Ratziu, V.; de Ledinghen, V.; Oberti, F.; Mathurin, P.; Wartelle-Bladou, C.; Renou, C.; Sogni, P.; Maynard, M.; Larrey, D.; Serfaty, L.; et al. A Randomized Controlled Trial ofHigh]Dose Ursodesoxycholic Acid for NonalcoholicSteatohepatitis. J Hepatol 2011, 54, 1011-1019. [CrossRef]
- Lindor KD, Kowdley KV, Heathcote EJ; et al. Ursodeoxycholic acid for treatment of nonalcoholic steatohepatitis: Results of a randomised trial. Hepatology 2004; 39: 770-778.
- Hrncir, T.; Hrncirova, L.; Kverka, M.; Hromadka, R.; Machova, V.; Trckova, E.; Kostovcikova, K.; Kralickova, P.; Krejsek, J.; Tlaskalova-Hogenova, H. Gut Microbiota and NAFLD: Pathogenetic Mechanisms, Microbiota Signatures, and Therapeutic Interventions. Microorganisms 2021, 9, 957. [CrossRef]
- Tang, R.; Wei, Y.; Li, Y.; Chen, W.; Chen, H.; Wang, Q.; Yang, F.; Miao, Q.; Xiao, X.; Zhang, H.; et al. Gut MicrobialProfile Is Altered in Primary Biliary Cholangitis and PartiallyRestored after UDCA Therapy. Gut 2018, 67, 534-541. [CrossRef]
- Białczyk, A.; Rajewska, A.; Junik, R.; Suwała, S. The Role of Probiotics in Managing Metabolic- Associated FattyLiver Disease: An Updated Review. Current Research in Nutrition and Food Science Journal 2024, 12, 490-501. [CrossRef]
- Asgharian, A.; Askari, G.; Esmailzade, A.; Feizi, A.; Mohammadi, V. The Effect of Symbiotic Supplementation on Liver Enzymes, c-Reactive Protein and Ultrasound Findings in Patients with Non-Alcoholic Fatty Liver Disease: A ClinicalTrial. Int J Prev Med 2016, 7, 59. [CrossRef]
- Ferolla, S.; Couto, C.; Costa-Silva, L.; Armiliato, G.; Pereira, C.; Martins, F.; Ferrari, M.; Vilela, E.; Torres, H.; Cunha, A.; et al. Beneficial Effect of SynbioticSupplementation on Hepatic Steatosis and AnthropometricParameters, But Not on Gut Permeability in a Population with Nonalcoholic Steatohepatitis. Nutrients 2016, 8, 397. [CrossRef]
- Attia, S.L.; Softic, S.; Mouzaki, M. Evolving Role for Pharmacotherapy in NAFLD/NASH. Clin Transl Sci 2021, 14, 11-19. [CrossRef]
- Suvarna, R., Shetty, S. & Pappachan, J.M. Efficacy and safety of Resmetirom, a selective thyroid hormone receptor-β agonist, in the treatment of metabolic dysfunction-associated steatotic liver disease (MASLD): A systematic review and meta-analysis. Sci Rep 14, 19790 (2024). [CrossRef]
- Kokkorakis, M. et al. Resmetirom, the first approved drug for the management of metabolic dysfunction-associated steatohepatitis: Trials, opportunities, and challenges. Metab. Clin. Exp. 2024. [CrossRef]
- Sumida, Y. & Yoneda, M. Current and future pharmacological therapies for NAFLD/NASH. J. Gastroenterol. 2018, 53, 362-376. [CrossRef]
- Szymanski F., Tomasiewicz K., Olszanecka-Glinianowicz M., Dzida G. Decalogue of MAFLD. Expert consensus on the diagnosis and treatment of steatohepatic liver disease and related metabolic disorders. 2021. Available at: www.ptchc.pl (Access date: 15.02.2022.
- Tincopa, M. A., Anstee, Q. M. & Loomba, R. New and emerging treatments for metabolic dysfunction-associated steatohepatitis. Cell Metab. 2024, 36(5), 912-926. [CrossRef]
- Rajewski, P.; Cieściński, J.; Rajewski, P.; Suwała, S.; Rajewska, A.; Potasz, M. Dietary Interventions and Physical Activity as Crucial Factors in the Prevention and Treatment of Metabolic Dysfunction-Associated Steatotic Liver Disease. Biomedicines 2025, 13, 217. [CrossRef]

| Liver complications | Extrahepatic complications |
| - progression of hepatic steatosis (S1, S2, S3) | - arteriosclerosis |
| - steatohepatitis -MASH | - ischaemic heart disease |
| - progression of hepatic fibrosis (F1, F2, F3) to cirrhosis (F4) | - chronic coronary syndrome, myocardial infarction heart muscle |
| - primary liver cancer (HCC) | - TIA |
| - liver transplantation | - ischaemic stroke |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).



