Submitted:
11 April 2025
Posted:
11 April 2025
You are already at the latest version
Abstract
Intermediate and advanced-stage hepatocellular carcinoma (HCC) continues to present significant therapeutic challenges. Hepatic artery infusion chemotherapy (HAIC), a well-established locoregional treatment for unresectable HCC, has recently demonstrated promising clinical outcomes both as monotherapy and in combination with systemic therapies. This comprehensive review examines recent clinical advances in HAIC for HCC, with particular emphasis on evolving treatment regimens and their therapeutic efficacy.
Keywords:
hepatocellular carcinoma
; hepatic artery infusion chemotherapy
; locoregional therapy
; combination therapy
1. Introduction
Hepatocellular carcinoma (HCC) stands as a major global health burden, ranking among the most prevalent malignancies and representing the third leading cause of cancer-related mortality worldwide [1]. China bears a disproportionate share of this disease burden, contributing nearly 50% of global HCC incidence [2]. Alarmingly, the majority of patients present with intermediate or advanced-stage disease at diagnosis, rendering them ineligible for potentially curative interventions including surgical resection, liver transplantation, or ablation [2]. Current therapeutic paradigms guided by the Barcelona Clinic Liver Cancer (BCLC) staging system recommend transarterial chemoembolization (TACE) for intermediate-stage disease and systemic therapies for advanced cases [3]. However, suboptimal response rates and frequent disease progression underscore the critical need for innovative treatment strategies combining locoregional and systemic approaches [4,5].
Hepatic artery infusion chemotherapy (HAIC), also known as transcatheter arterial infusion (TAI), has re-emerged as a promising locoregional modality, driven by advancements in transcatheter techniques and optimized chemotherapeutic regimens. Modern HAIC protocols demonstrate tumor response rates exceeding 50% in selected populations, with particular efficacy in cases featuring portal vein invasion [6,7]. The therapeutic landscape has been further transformed by emerging evidence supporting synergistic effects when combining HAIC with molecular targeted agents (e.g., sorafenib, lenvatinib) and immune checkpoint inhibitors, achieving unprecedented median overall survival (OS) durations exceeding 17 months in advanced HCC cohorts [6,7]. This review critically examines contemporary clinical advances in HAIC application for HCC, with particular emphasis on evolving treatment protocols, combination strategies, and their associated therapeutic outcomes.
2. Definition and Technical Modalities
2.1. Definition
HAIC involves the direct administration of chemotherapeutic agents into the hepatic arterial system via an intra-arterial catheter. This targeted delivery mechanism achieves higher intratumoral drug concentrations compared to systemic chemotherapy while reducing extrahepatic toxicity [8]. As a specialized regional chemotherapy approach, HAIC fundamentally differs from conventional intravenous chemotherapy through its first-pass hepatic extraction advantage.
2.2. Technical Modalities
2.2.1. Surgical Pump Implantation
The surgically implanted subcutaneous pump remains the gold-standard technique in Western practice. This procedure requires laparotomy under direct visualization to ensure precise catheter placement. Specifically, the catheter is inserted retrograde into the gastroduodenal artery (GDA) and secured with sutures. During the procedure, extrahepatic arterial branches are ligated to prevent extrahepatic chemotherapeutic exposure, while accessory hepatic arteries are occluded to minimize competitive intrahepatic flow. The catheter tip is precisely positioned at the GDA-common hepatic artery (CHA) junction to optimize hepatic perfusion. Finally, the pump is connected to the catheter and implanted in a subcutaneous pocket [9,10].
While enabling repeated treatments, this technique carries significant limitations. First, the procedure requires laparotomy performed by experienced surgeons and typically requires concomitant cholecystectomy, resulting in substantial invasiveness and potential surgical complications [11]. Second, although preoperative CT can assess hepatic arterial anatomy and aberrant vessels, this technique demonstrates limited control of collateral tumor supply (e.g., subphrenic artery). Thirdly, catheter placement into arteries beyond the GDA is occasionally required, posing considerable technical difficulties [12].
2.2.2. Transfemoral Temporary Catheterization
The transfemoral temporary catheterization has been widely adopted in Chinese clinical practice [13]. This percutaneous approach involves the percutaneous insertion of a catheter in the proper hepatic artery or the tumor-feeding hepatic artery branch under digital subtraction angiography (DSA) guidance. The external end of the catheter is retained outside the skin of the arterial approach and connected with an infusion pump for chemotherapy. After the completion of a single session of chemotherapy, the catheter was removed with the puncture arterial hemostasis. It is noted that before the indwelling catheter placement, routine arterial angiography is performed to evaluate hepatic arterial anatomy and tumor blood supply. When necessary, vascular embolization is employed to address hepatic artery variations or extrahepatic collateral blood supply, thereby ensuring selective drug distribution to the liver or the tumor [14]. This procedure needs to be repeated according to the HAIC treatment schedule.
As a minimally invasive interventional procedure, this technique offers several advantages, including procedural simplicity and rapid postoperative recovery. The flexibility to adjust catheter positioning according to therapeutic requirements further enhances its clinical utility. However, certain limitations should be noted. Firstly, repeated catheterization and bedridden infusion chemotherapy may impair patient tolerance and compliance. Secondly, the tip of the indwelling catheter may become dislocated due to vomiting, coughing, or drastic positional changes, resulting in improper drug delivery. Finally, due to the limited duration of catheter placement, this approach is unsuitable for chemotherapy regimens requiring prolonged infusion or repeated short-term administration [11].
2.2.3. Percutaneous Port Systems
The percutaneous port systems represent a significant advancement in HAIC technology, with widespread clinical adoption across Asian regions. This minimally invasive procedure employs the "tip-fixation" technique to precisely position an indwelling side-holed catheter within the GDA. The catheter is strategically placed with its side-hole aligned at the origin of the common hepatic artery. Through a coaxial approach, a microcatheter is advanced via the indwelling catheter, passing through the side-hole for optimal positioning. The distal tip of the indwelling catheter is then securely anchored within the GDA using either embolization coils or an NBCA-lipiodol mixture. Finally, the proximal end of the indwelling catheter is connected to an implantable port system for drug infusion [15,16,17].
This technique integrates the advantages of previous HAIC techniques, facilitating routine angiography and necessary procedures to redistribute intrahepatic or extrahepatic blood flow, thereby enhancing the efficacy and safety of chemotherapy. Additionally, it allows for multiple treatments with a single placement, accommodating various chemotherapy regimens, improving patient comfort and compliance, and reducing overall treatment costs [18,19,20,21,22]. The main features of the above three techniques are summarized in Figure 1.
3. Pharmacological Rationale and Chemotherapeutic Agents
3.1. Pharmacological Rationale
The therapeutic foundation of HAIC stems from the differential vascular perfusion between hepatocellular malignancies and parenchymal tissue. While normal hepatocytes receive 70%–75% of their blood supply through the portal venous system, hepatic malignancies derive >90% of their perfusion from arterial circulation[23]. Therefore, it is reasonable to use the hepatic artery as an approach to deliver concentrated doses of chemotherapy to the tumor bed.
Mechanistically, HAIC capitalizes on two key pharmacokinetic advantages: first-pass hepatic extraction and enhanced tumor penetration. Studies have demonstrated that hepatic arterial infusion of floxuridine or 5-fluorouracil can achieve intrahepatic uptake rates of up to 90% and 19-90%, respectively. These rates significantly exceed those observed with conventional intravenous administration. Accordingly, intratumoral drug concentrations are also markedly elevated [9,24]. In addition, Sustained high-flow infusion creates increased interstitial pressure gradients, improving intratumoral drug distribution [25]. These synergistic mechanisms augment the efficacy of chemotherapy while mitigating extrahepatic toxicity.
3.2. Drug Selection
HAIC drug selection requires strategic integration of systemic chemotherapy principles with arterial pharmacokinetic advantages. Priority should be given to tumor-sensitive drugs and prototype drugs, with the use of combinations or sequential regimens of agents with differing mechanisms strategically designed to optimize the therapeutic efficacy[26,27]. Drugs that share similar toxic effects or exhibit cumulative hepatotoxicity, as well as those with antagonistic pharmacological effects or the potential to inactivate one another, should be avoided. The primary objective is to minimize toxicity while maximizing therapeutic efficacy against the tumor and decreasing side effects both systemically and within the liver.
Cell cycle–nonspecific agents (eg, alkylating agents, anthracyclines, and platinum complexes) exhibit concentration-dependent cytotoxicity. These agents mandate high-intensity bolus administration protocols. For instance, oxaliplatin is usually administered short-term, high-dose infusion (85–130 mg/m² over 90–120 min). In contrast, cell cycle-specific agents (eg, 5-fluorouracil and floxuridine) are time-dependent, requiring sustained tumor exposure to achieve maximal cytotoxic effects. These agents necessitate precision-controlled infusion protocols. For instance, 5-fluorouracil is usually administered with continuous infusion (2400 mg/m² over 46 hours) [28,29]..
4. Patient Selection and Periprocedural Management
4.1. Patient Selection
HAIC is primarily indicated for HCC patients presenting with multifocal intrahepatic lesions or bulky tumors, portal vein thrombosis, Child-Pugh class A/B liver function, and an Eastern Cooperative Oncology Group (ECOG) performance status of 0–2. It may also serve as an alternative therapeutic option for advanced-stage patients with limited extrahepatic metastases [6,7].
Current clinical guidelines endorse HAIC for HCC management. The Japanese Society of Hepatology (JSH) guidelines recommend HAIC for patients with ≥4 intrahepatic lesions or vascular invasion [30]. Similarly, the Korean Liver Cancer Association-National Cancer Center (KLCA-NCC) guidelines propose HAIC for patients with portal vein invasion and no extrahepatic spread who have failed or are ineligible for first- or second-line systemic therapies [31]. Notably, the Chinese Society of Clinical Oncology (CSCO) guidelines have expanded HAIC indications to include: (1) Stage Ib–IIb patients with solitary tumors >7 cm who are ineligible for or decline surgical resection; (2) Stage III patients refractory to or declining molecular targeted therapy/systemic chemotherapy; (3) Stage IIIb patients with limited extrahepatic metastases (treatment decision at clinician's discretion); and (4) Stage IV patients unwilling or unable to undergo liver transplantation [13].
4.2. Periprocedural Management
Before the initiation of HAIC, a comprehensive patient evaluation should be conducted, encompassing detailed medical history and physical examination, laboratory analyses (hepatic/renal function, coagulation profile, complete blood count, tumor markers), and contrast-enhanced dynamic CT or MR imaging. Positron emission tomography-computed tomography (PET-CT) may supplement diagnostic workup when indicated. Liver biopsy is recommended for histopathological confirmation in cases with an inconclusive HCC diagnosis or suspected alternative hepatic malignancies.
Key preoperative parameters include liver function, performance status, and tumor burden. Regarding liver function, clinical trials predominantly enroll patients with compensated cirrhosis (Child-Pugh A to B7) for HAIC monotherapy or combination regimens [32,33]. Real-world evidence demonstrates acceptable HAIC tolerability in Child-Pugh B patients[6]. Similarly, Most trials restrict HAIC eligibility to Eastern Cooperative Oncology Group (ECOG) 0–1 [7], while observational studies extend criteria to ECOG 0–2 [6]. In terms of tumor burden, HAIC is indicated for multifocal intrahepatic lesions or bulky tumors with portal vein thrombosis. Notably, therapeutic efficacy diminishes significantly when tumor involvement exceeds ≥50% of total liver volume [34].
5. HAIC Chemotherapy Regimens and Outcomes
Current clinical HAIC protocols include FOLFOX, low-dose fluorouracil-cisplatin (FP), fluorouracil-interferon arterial infusion therapy (FAIT), New FP, and oxaliplatin-raltitrexed regimens, with efficacy outcomes varying by drug combination. The included studies of HAIC combination therapies and their characteristics are summarized in Table 1.
5.1. FOLFOX Regimen
The FOLFOX regimen is the recommended first-line systemic chemotherapy for HCC in China and has been widely adopted in HAIC treatment [13]. The standard FOLFOX regimen for HAIC includes oxaliplatin (85–130 mg/m² via 3-hour intra-arterial infusion on day 1), leucovorin (200 mg/m² via 3–5-hour intra-arterial infusion on day 1), and fluorouracil (400 mg/m² intra-arterial bolus, followed by 2400 mg/m² 46-hour continuous infusion). Treatment is typically administered every three weeks for six cycles, with adjustments made based on tumor response (Figure 2a) [7]. The FOLFOX regimen synergizes platinum concentration-dependent effects with fluorouracil time-dependent cytotoxicity, enhanced by leucovorin-mediated biochemical modulation.
HAIC monotherapy has demonstrated significant survival benefits for patients with advanced HCC. A prospective, non-randomized Phase II study compared the efficacy of HAIC and TACE in patients with massive unresectable HCC. The results showed that HAIC achieved significantly higher partial response rates and disease control rates compared to TACE (52.6% vs. 9.8%, P < 0.001; 83.8% vs. 52.5%, P < 0.01) [35]. Another randomized controlled Phase III trial evaluated HAIC versus TACE in patients with unresectable HCC without vascular invasion or extrahepatic metastasis. HAIC as a first-line treatment significantly improved OS (23.1 vs. 16.1 months, P < 0.001) and reduced the incidence of severe adverse events (AEs) (19% vs. 30%, P = 0.03) [36]. A recent randomized controlled Phase III trial comparing HAIC with sorafenib as first-line therapy for advanced HCC revealed that HAIC significantly prolonged OS compared to sorafenib (13.9 vs. 8.2 months, P < 0.001) [32]. Additionally, a Phase III, multicenter, prospective, open-label, randomized controlled trial compared postoperative adjuvant HAIC with routine follow-up in HCC patients with microvascular invasion. HAIC significantly extended median disease-free survival (20.3 vs. 10.0 months, P < 0.001) [37].
HAIC combined with targeted therapy has also emerged as a viable option for advanced HCC. An earlier randomized controlled trial compared sorafenib plus HAIC to sorafenib alone in patients with advanced HCC and portal vein invasion. The combination therapy resulted in longer OS (13.37 vs. 7.13 months, P < 0.001), longer progression-free survival (PFS) (7.03 vs. 2.6 months, P < 0.001), and a higher tumor response rate (40.8% vs. 2.46%, P < 0.001), although grade 3/4 AEs were more frequent in the combination group [38]. Another Phase II clinical trial confirmed the superior OS of sorafenib plus HAIC compared to sorafenib alone (16.3 vs. 6.5 months, P < 0.001) in advanced HCC with major portal vein tumor thrombosis [33].
HAIC combined with immunotherapy, as well as with both targeted therapy and immunotherapy, has also shown promising efficacy and safety [39,40,41,42]. A Phase II, single-center, single-arm study treated advanced, high-risk HCC patients with a combination of lenvatinib, toripalimab, and HAIC, achieving a 6-month PFS rate of 80.6%[41]. Another single-arm Phase II clinical study evaluated HAIC combined with camrelizumab and apatinib for advanced HCC, reporting an objective response rate of 77.1% and a median PFS of 10.38 months [42].
Other combination therapies, such as HAIC plus TACE or ablation, have also been explored [43,44]. A Phase II, prospective, non-randomized clinical study compared TACE combined with HAIC to TACE alone in unresectable HCC patients without extrahepatic metastasis. The combination therapy showed significant improvements in overall response rate and median PFS (68.9% vs. 45.9%, P < 0.05; 8 vs. 4.5 months, P < 0.001) [44]. Additional clinical trials of combination therapies are currently underway.
5.2. Low-Dose FP Regimen
The FP regimen, pioneered by Japanese researchers for HAIC, employs daily low-dose cisplatin (10 mg/d via 30-min intra-arterial infusion) followed by fluorouracil (250 mg/d over 3–5 hours). Administered 5 consecutive days/week with 2-day intervals per 4-week cycle (Figure 2b), this protocol utilizes cisplatin as a biochemical modulator to enhance fluorouracil's antitumor activity through intracellular reduced folate accumulation, achieving synergistic cytotoxicity. Its brief infusion requirements facilitate compatibility with percutaneous port-catheter systems [45].
As a monotherapy, the FP-HAIC regimen demonstrated 20–71% tumor response rates and 7.3–15.9-month median OS in advanced HCC with portal vein invasion in early retrospective analyses [45,46,47,48,49,50,51,52]. The combination of FP-HAIC with targeted therapy has also been investigated. In a phase I/II trial, the FP-HAIC combined with sorafenib demonstrated a response rate of 38.9%, a disease control rate of 77.8%, a median time-to-progression of 9.7 months, and a 1-year survival rate of 88.2% [53]. Another open-label, non-comparative phase II trial using HAIC or HAIC followed by sorafenib for advanced HCC patients revealed 1-year and 2-year survival rates of 64.0% and 48.3%, respectively [54]. A recent randomized controlled phase III trial compared the FP-HAIC combined with sorafenib to sorafenib monotherapy in advanced HCC. While no statistically significant difference in OS was observed between the two groups (11.8 vs. 11.5 months, P = 0.955), subgroup analysis indicated that patients with main portal vein invasion who received the combination therapy had significantly longer median OS compared to those receiving sorafenib alone (11.4 vs. 6.5 months, P = 0.05) [55]. These evidences position FP-HAIC combination therapy as a potential survival-enhancing strategy for portal vein-involved HCC.
5.3. FAIT Regimen
The FAIT regimen was initially described in 2002 for HCC management [56]. This regimen combines intra-arterial infusion of fluorouracil with subcutaneous injection of interferon. This therapeutic protocol involves transarterial administration of fluorouracil coupled with subcutaneous interferon-α injections. Fluorouracil is delivered through continuous intra-arterial infusion according to two distinct dosing schemes: 500 mg/day or 300 mg/m²/day, administered five consecutive days weekly during the first two weeks, followed by a two-week break. Subcutaneous interferon-α is administered at 5 million IU/day, three times weekly for four weeks, with a total of 1–4 treatment cycles (Figure 2c).
Clinical investigations have documented objective response rates (ORR) of 24.6–73.0% and median OS durations of 6.9–14.7 months in HCC patients with portal vein tumor thrombosis (PVTT) treated with FAIT [57,58,59,60,61,62,63,64,65]. A phase II trial revealed significant enhancement of therapeutic outcomes through cisplatin-FAIT combination therapy, demonstrating superior ORR (45.6% vs 24.6%; P = 0.03) and extended median OS (17.6 vs 10.5 months) compared with FAIT monotherapy [62].
5.4. New FP Regimen
The new FP regimen combines cisplatin, lipiodol, and fluorouracil. The protocol involves intra-arterial administration of 50 mg cisplatin emulsified with 5–10 mL lipiodol, followed by a bolus injection of 250 mg fluorouracil and a continuous infusion of 1250 mg/m² fluorouracil over five days, with a two-day rest period (Figure 2d). Treatment is administered weekly for two or three consecutive weeks. In this regimen, the therapeutic efficacy of cisplatin is enhanced by the tumor-targeting properties of lipiodol, while the dose of fluorouracil is increased to maximize antitumor effects.
Retrospective analyses have demonstrated superior median OS in advanced HCC patients with macrovascular invasion treated with the new FP regimen compared to low-dose FP or sorafenib (24.7 vs. 16.1 months; P < 0.05; and 18.0 vs. 9.0 months; P < 0.0001, respectively) [66,67]. A multicenter single-arm phase II trial evaluating this regimen in HCC with PVTT reported a median disease-free survival of 8.6 months, OS of 27.0 months, and ORR of 75% [68]. Synergistic efficacy was observed when combined with lenvatinib, achieving an ORR of 83% in advanced HCC [69].
A non-randomized prospective cohort study comparing the new FP regimen to sorafenib in HCC with macrovascular invasion revealed significant improvements in OS (30.4 vs. 13.2 months; P = 0.013) and ORR (71% vs. 10%; P < 0.001) [70]. These outcomes are corroborated by recent large-scale multicenter retrospective studies, wherein HAIC using the new FP regimen extended median OS in locally advanced HCC versus sorafenib (12.0 vs. 7.9 months; P < 0.001) [71].
5.5. Oxaliplatin-Raltitrexed Regimen
The clinical utility of fluorouracil is constrained by its short plasma half-life, necessitating prolonged continuous infusions or repeated short-term administrations to exploit its time-dependent cytotoxic activity. These delivery modalities, however, impose significant logistical challenges for patients undergoing HAIC. Raltitrexed, a novel thymidylate synthase inhibitor, has been investigated as a potential HAIC agent for HCC. Its extended plasma half-life relative to fluorouracil may improve treatment tolerability when combined with platinum-based chemotherapeutics [72].
A single-arm phase II trial assessing oxaliplatin-raltitrexed HAIC in intermediate-to-advanced HCC documented an ORR of 51.4%, with median PFS of 6.7 months, median disease-free survival (DFS) of 5.2 months, and 1-year survival rate of 43.2%. The protocol comprised oxaliplatin (100 mg/m²) delivered via 4-hour intra-arterial infusion and raltitrexed (3 mg/m²) administered over 60 minutes, significantly reducing the total infusion duration. Treatment cycles were repeated triweekly (Figure 2e), with no grade ≥4 treatment-related adverse events (TRAEs) reported [73]. Another phase II study evaluating apatinib combined with oxaliplatin-raltitrexed HAIC in HCC patients with extrahepatic metastases refractory to first-line systemic therapy achieved an ORR of 53.8% [74].
6. Adverse Events
AEs associated with HAIC are systematically classified into chemotherapy-induced toxicities and procedural complications [9,75,76].
6.1. Chemotherapy-Induced AEs
Gastrointestinal disturbances, predominantly nausea and vomiting (incidence >30%), represent the most frequent chemotherapy-related AEs [9]. These manifestations are typically managed effectively through prophylactic antiemetic regimens. Acute epigastric pain, frequently attributable to chemotherapy-induced arterial vasospasm, may necessitate transient infusion cessation or intra-arterial lidocaine administration for symptomatic relief. Hematological toxicity, manifesting as leukopenia and thrombocytopenia, often requires granulocyte colony-stimulating factor therapy, thrombopoietin receptor agonists, or partial splenic embolization in refractory cases. Hepatobiliary toxicity, evidenced by elevated serum alanine aminotransferase and total bilirubin, mandates hepatoprotective agents such as ursodeoxycholic acid or polyene phosphatidylcholine. Nephrotoxicity prophylaxis is achieved through standardized hydration protocols during cytotoxic drug infusion. Cardiotoxicity and gastroduodenal mucosal injury, though less common, warrant systematic monitoring with adjunctive interventions including myocardial metabolic support and proton pump inhibitor therapy.
6.2. HAIC Procedure-Related AEs
HAIC procedure-associated complications are principally stratified into implantable pump-related morbidities and catheter-associated events [75,76]. Implantable pump complications (incidence: 8–18%) predominantly comprise pocket hematoma, device-related infections, pump erosion, mechanical displacement (migration/flipping), and reservoir exposure [76]. Minor hematomas are typically managed nonoperatively through compression bandages and pressure garments. Infectious complications (abscess formation or cellulitis) generally require ultrasound-guided drainage coupled with empirical antibiotic therapy; recalcitrant cases may necessitate pump explantation with delayed reimplantation [77]. Pump displacement is corrected via surgical repositioning, whereas full-thickness erosion with cutaneous penetration mandates complete device removal and alternate-site implantation. Catheter-related complications (10–26% incidence) primarily involve thrombosis (occlusion), mechanical dislodgement, or mural erosion [76,78]. These complications can usually be resolved through thrombolysis, catheter repositioning or replacement, or embolization treatment.
7. Conclusions
HAIC has demonstrated preliminary efficacy as a safe and technically feasible therapeutic modality for HCC. While widely adopted in China and select Asian nations, HAIC remains excluded from global HCC treatment guidelines. To establish HAIC as a globally recognized HCC treatment paradigm, three strategic imperatives may need to be prioritized: 1) development of consensus-driven technical guidelines through international multicenter clinical trials and Delphi-method expert panels; 2) optimization of tumor biology-informed HAIC regimens using pharmacogenomic profiling and radiomic response predictors; 3) mechanistic exploration of HAIC combined with immunotherapy/molecular targeted therapy through preclinical models correlating intratumoral drug distribution with immune microenvironment modulation. Continued innovation in HAIC may advance precision HCC management, ultimately improving oncological outcomes.
Author Contributions
Conceptualization, W.X., Q.L. and B.L.; Data Curation, W.X., Q.L. and B.L.; writing—original draft preparation, W.X.; writing—review and editing, Q.L. and B.L.; visualization, W.X., Q.L. and B.L.; supervision, B.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
No new data were created or analyzed in this study. Data sharing is not applicable to this article.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| HCC | Hepatocellular carcinoma |
| TACE | Transarterial chemoembolization |
| HAIC | Hepatic artery infusion chemotherapy |
| GDA | Gastroduodenal artery |
| AEs | Adverse events |
| ECOG | Eastern Cooperative Oncology Group |
| ORR | Objective response rates |
| OS | Overall survival |
| PFS | Progression-free survival |
| PVTT | Portal vein tumor thrombosis |
References
- Vogel, A.; Meyer, T.; Sapisochin, G.; Salem, R.; Saborowski, A. Hepatocellular Carcinoma. Lancet 2022, 400, 1345–1362. [CrossRef]
- Zeng, H.; Chen, W.; Zheng, R.; Zhang, S.; Ji, J.S.; Zou, X.; Xia, C.; Sun, K.; Yang, Z.; Li, H.; et al. Changing Cancer Survival in China during 2003-15: A Pooled Analysis of 17 Population-Based Cancer Registries. Lancet Glob Health 2018, 6, e555–e567. [CrossRef]
- Reig, M.; Forner, A.; Rimola, J.; Ferrer-Fàbrega, J.; Burrel, M.; Garcia-Criado, Á.; Kelley, R.K.; Galle, P.R.; Mazzaferro, V.; Salem, R.; et al. BCLC Strategy for Prognosis Prediction and Treatment Recommendation: The 2022 Update. J Hepatol 2022, 76, 681–693. [CrossRef]
- Vogel, A.; Martinelli, E.; ESMO Guidelines Committee. Electronic address: clinicalguidelines@esmo.org; ESMO Guidelines Committee Updated Treatment Recommendations for Hepatocellular Carcinoma (HCC) from the ESMO Clinical Practice Guidelines. Ann Oncol 2021, 32, 801–805. [CrossRef]
- Hasegawa, K.; Takemura, N.; Yamashita, T.; Watadani, T.; Kaibori, M.; Kubo, S.; Shimada, M.; Nagano, H.; Hatano, E.; Aikata, H.; et al. Clinical Practice Guidelines for Hepatocellular Carcinoma: The Japan Society of Hepatology 2021 Version (5th JSH-HCC Guidelines). Hepatol Res 2023, 53, 383–390. [CrossRef]
- Ueshima, K.; Komemushi, A.; Aramaki, T.; Iwamoto, H.; Obi, S.; Sato, Y.; Tanaka, T.; Matsueda, K.; Moriguchi, M.; Saito, H.; et al. Clinical Practice Guidelines for Hepatic Arterial Infusion Chemotherapy with a Port System Proposed by the Japanese Society of Interventional Radiology and Japanese Society of Implantable Port Assisted Treatment. Liver Cancer 2022, 11, 407–425. [CrossRef]
- Zhao, M.; Guo, Z.; Zou, Y.-H.; Li, X.; Yan, Z.-P.; Chen, M.-S.; Fan, W.-J.; Li, H.-L.; Yang, J.-J.; Chen, X.-M.; et al. Arterial Chemotherapy for Hepatocellular Carcinoma in China: Consensus Recommendations. Hepatol Int 2024, 18, 4–31. [CrossRef]
- Ueshima, K.; Ogasawara, S.; Ikeda, M.; Yasui, Y.; Terashima, T.; Yamashita, T.; Obi, S.; Sato, S.; Aikata, H.; Ohmura, T.; et al. Hepatic Arterial Infusion Chemotherapy versus Sorafenib in Patients with Advanced Hepatocellular Carcinoma. Liver Cancer 2020, 9, 583–595. [CrossRef]
- Leal, J.N.; Kingham, T.P. Hepatic Artery Infusion Chemotherapy for Liver Malignancy. Surg Oncol Clin N Am 2015, 24, 121–148. [CrossRef]
- Van Nieuwenhove, Y.; Aerts, M.; Neyns, B.; Delvaux, G. Techniques for the Placement of Hepatic Artery Catheters for Regional Chemotherapy in Unresectable Liver Metastases. Eur J Surg Oncol 2007, 33, 336–340. [CrossRef]
- Zheng, K.; Wang, X. Techniques and Status of Hepatic Arterial Infusion Chemotherapy for Primary Hepatobiliary Cancers. Ther Adv Med Oncol 2024, 16, 17588359231225040. [CrossRef]
- Thiels, C.A.; D’Angelica, M.I. Hepatic Artery Infusion Pumps. J Surg Oncol 2020, 122, 70–77. [CrossRef]
- Zhou, J.; Sun, H.; Wang, Z.; Cong, W.; Zeng, M.; Zhou, W.; Bie, P.; Liu, L.; Wen, T.; Kuang, M.; et al. Guidelines for the Diagnosis and Treatment of Primary Liver Cancer (2022 Edition). Liver Cancer 2023, 12, 405–444. [CrossRef]
- Nagaoka, S.; Itano, S.; Nagamatsu, H.; Akiyoshi, J.; Kurogi, J.; Tajiri, N.; Kajiwara, M.; Sata, M. Temporary Indwelling Catheter System via the Left Brachial Artery: Evaluation in 83 Patients with Hepatic Tumors. AJR Am J Roentgenol 2007, 188, 652–658. [CrossRef]
- Arai, Y.; Takeuchi, Y.; Inaba, Y.; Yamaura, H.; Sato, Y.; Aramaki, T.; Matsueda, K.; Seki, H. Percutaneous Catheter Placement for Hepatic Arterial Infusion Chemotherapy. Tech Vasc Interv Radiol 2007, 10, 30–37. [CrossRef]
- Tanaka, T.; Arai, Y.; Inaba, Y.; Matsueda, K.; Aramaki, T.; Takeuchi, Y.; Kichikawa, K. Radiologic Placement of Side-Hole Catheter with Tip Fixation for Hepatic Arterial Infusion Chemotherapy. J Vasc Interv Radiol 2003, 14, 63–68. [CrossRef]
- Ganaha, F.; Sadaoka, S.; Yamada, T. Continuous Arterial Infusion Strategies Using Implanted Ports. Tech Vasc Interv Radiol 2002, 5, 170–176. [CrossRef]
- Herrmann, K.A.; Waggershauser, T.; Sittek, H.; Reiser, M.F. Liver Intraarterial Chemotherapy: Use of the Femoral Artery for Percutaneous Implantation of Catheter-Port Systems. Radiology 2000, 215, 294–299. [CrossRef]
- Meyblum, L.; Faron, M.; Deschamps, F.; Kobe, A.; Bonnet, B.; Boileve, A.; Gelli, M.; Boige, V.; Hollebecque, A.; Durand-Labrunie, J.; et al. Safety and Efficacy of Percutaneous Arterial Port Implantation for Hepatic Arterial Infusion Chemotherapy. Eur Radiol 2024. [CrossRef]
- Hu, J.; Zhu, X.; Wang, X.; Cao, G.; Wang, X.; Yang, R. Evaluation of Percutaneous Unilateral Trans-Femoral Implantation of Side-Hole Port-Catheter System with Coil Only Fixed-Catheter-Tip for Hepatic Arterial Infusion Chemotherapy. Cancer Imaging 2019, 19, 15. [CrossRef]
- Matsumoto, T.; Yamagami, T.; Yoshimatsu, R.; Morishita, H.; Kitamura, N.; Sato, O.; Hasebe, T. Hepatic Arterial Infusion Chemotherapy by the Fixed-Catheter-Tip Method: Retrospective Comparison of Percutaneous Left Subclavian and Femoral Port-Catheter System Implantation. AJR Am J Roentgenol 2014, 202, 211–215. [CrossRef]
- Yamagami, T.; Yoshimatsu, R.; Matsumoto, T.; Nishimura, T. Evaluation of Non-Target Arterial Patency after Implantation of Hepatic Arterial Catheter Using a Modified Implantation Technique with the Fixed Catheter Tip Method. Clin Radiol 2009, 64, 164–170. [CrossRef]
- Breedis, C.; Young, G. The Blood Supply of Neoplasms in the Liver. Am J Pathol 1954, 30, 969–977.
- Barber, F.D.; Mavligit, G.; Kurzrock, R. Hepatic Arterial Infusion Chemotherapy for Metastatic Colorectal Cancer: A Concise Overview. Cancer Treat Rev 2004, 30, 425–436. [CrossRef]
- Liang, B.; Xiong, F.; Wu, H.; Wang, Y.; Dong, X.; Cheng, S.; Feng, G.; Zhou, G.; Xiong, B.; Liang, H.; et al. Effect of Transcatheter Intraarterial Therapies on the Distribution of Doxorubicin in Liver Cancer in a Rabbit Model. PLoS One 2013, 8, e76388. [CrossRef]
- Ikeda, M.; Morizane, C.; Ueno, M.; Okusaka, T.; Ishii, H.; Furuse, J. Chemotherapy for Hepatocellular Carcinoma: Current Status and Future Perspectives. Jpn J Clin Oncol 2018, 48, 103–114. [CrossRef]
- Ensminger, W.D.; Gyves, J.W. Clinical Pharmacology of Hepatic Arterial Chemotherapy. Semin Oncol 1983, 10, 176–182.
- Obi, S.; Sato, S.; Kawai, T. Current Status of Hepatic Arterial Infusion Chemotherapy. Liver Cancer 2015, 4, 188–199. [CrossRef]
- Nishikawa, H.; Osaki, Y.; Kita, R.; Kimura, T. Hepatic Arterial Infusion Chemotherapy for Advanced Hepatocellular Carcinoma in Japan. Cancers (Basel) 2012, 4, 165–183. [CrossRef]
- Kokudo, N.; Takemura, N.; Hasegawa, K.; Takayama, T.; Kubo, S.; Shimada, M.; Nagano, H.; Hatano, E.; Izumi, N.; Kaneko, S.; et al. Clinical Practice Guidelines for Hepatocellular Carcinoma: The Japan Society of Hepatology 2017 (4th JSH-HCC Guidelines) 2019 Update. Hepatol Res 2019, 49, 1109–1113. [CrossRef]
- Korean Liver Cancer Association (KLCA) and National Cancer Center (NCC) Korea 2022 KLCA-NCC Korea Practice Guidelines for the Management of Hepatocellular Carcinoma. Clin Mol Hepatol 2022, 28, 583–705. [CrossRef]
- Lyu, N.; Wang, X.; Li, J.-B.; Lai, J.-F.; Chen, Q.-F.; Li, S.-L.; Deng, H.-J.; He, M.; Mu, L.-W.; Zhao, M. Arterial Chemotherapy of Oxaliplatin Plus Fluorouracil Versus Sorafenib in Advanced Hepatocellular Carcinoma: A Biomolecular Exploratory, Randomized, Phase III Trial (FOHAIC-1). J Clin Oncol 2022, 40, 468–480. [CrossRef]
- Zheng, K.; Zhu, X.; Fu, S.; Cao, G.; Li, W.-Q.; Xu, L.; Chen, H.; Wu, D.; Yang, R.; Wang, K.; et al. Sorafenib Plus Hepatic Arterial Infusion Chemotherapy versus Sorafenib for Hepatocellular Carcinoma with Major Portal Vein Tumor Thrombosis: A Randomized Trial. Radiology 2022, 303, 455–464. [CrossRef]
- Murakami, E.; Aikata, H.; Miyaki, D.; Nagaoki, Y.; Katamura, Y.; Kawaoka, T.; Takaki, S.; Hiramatsu, A.; Waki, K.; Takahashi, S.; et al. Hepatic Arterial Infusion Chemotherapy Using 5-Fluorouracil and Systemic Interferon-α for Advanced Hepatocellular Carcinoma in Combination with or without Three-Dimensional Conformal Radiotherapy to Venous Tumor Thrombosis in Hepatic Vein or Inferior Vena Cava. Hepatol Res 2012, 42, 442–453. [CrossRef]
- He, M.-K.; Le, Y.; Li, Q.-J.; Yu, Z.-S.; Li, S.-H.; Wei, W.; Guo, R.-P.; Shi, M. Hepatic Artery Infusion Chemotherapy Using mFOLFOX versus Transarterial Chemoembolization for Massive Unresectable Hepatocellular Carcinoma: A Prospective Non-Randomized Study. Chin J Cancer 2017, 36, 83. [CrossRef]
- Li, Q.-J.; He, M.-K.; Chen, H.-W.; Fang, W.-Q.; Zhou, Y.-M.; Xu, L.; Wei, W.; Zhang, Y.-J.; Guo, Y.; Guo, R.-P.; et al. Hepatic Arterial Infusion of Oxaliplatin, Fluorouracil, and Leucovorin Versus Transarterial Chemoembolization for Large Hepatocellular Carcinoma: A Randomized Phase III Trial. J Clin Oncol 2022, 40, 150–160. [CrossRef]
- Li, S.-H.; Mei, J.; Cheng, Y.; Li, Q.; Wang, Q.-X.; Fang, C.-K.; Lei, Q.-C.; Huang, H.-K.; Cao, M.-R.; Luo, R.; et al. Postoperative Adjuvant Hepatic Arterial Infusion Chemotherapy With FOLFOX in Hepatocellular Carcinoma With Microvascular Invasion: A Multicenter, Phase III, Randomized Study. J Clin Oncol 2023, 41, 1898–1908. [CrossRef]
- He, M.; Li, Q.; Zou, R.; Shen, J.; Fang, W.; Tan, G.; Zhou, Y.; Wu, X.; Xu, L.; Wei, W.; et al. Sorafenib Plus Hepatic Arterial Infusion of Oxaliplatin, Fluorouracil, and Leucovorin vs Sorafenib Alone for Hepatocellular Carcinoma With Portal Vein Invasion: A Randomized Clinical Trial. JAMA Oncol 2019, 5, 953–960. [CrossRef]
- Tang, H.-H.; Zhang, M.-Q.; Zhang, Z.-C.; Fan, C.; Jin, Y.; Wang, W.-D. The Safety and Efficacy of Hepatic Arterial Infusion Chemotherapy Combined with PD-(L)1 Inhibitors and Molecular Targeted Therapies for the Treatment of Intermediate and Advanced Hepatocellular Carcinoma Unsuitable for Transarterial Chemoembolization. J Hepatocell Carcinoma 2023, 10, 2211–2221. [CrossRef]
- Yu, B.; Zhang, N.; Feng, Y.; Zhang, Y.; Zhang, T.; Wang, L. Tyrosine Kinase Inhibitors Plus Anti-PD-1 Antibodies with Hepatic Arterial Infusion Chemotherapy or Transarterial Chemoembolization for Unresectable Hepatocellular Carcinoma. J Hepatocell Carcinoma 2023, 10, 1735–1748. [CrossRef]
- Lai, Z.; He, M.; Bu, X.; Xu, Y.; Huang, Y.; Wen, D.; Li, Q.; Xu, L.; Zhang, Y.; Wei, W.; et al. Lenvatinib, Toripalimab plus Hepatic Arterial Infusion Chemotherapy in Patients with High-Risk Advanced Hepatocellular Carcinoma: A Biomolecular Exploratory, Phase II Trial. Eur J Cancer 2022, 174, 68–77. [CrossRef]
- Zhang, T.-Q.; Geng, Z.-J.; Zuo, M.-X.; Li, J.-B.; Huang, J.-H.; Huang, Z.-L.; Wu, P.-H.; Gu, Y.-K. Camrelizumab (a PD-1 Inhibitor) plus Apatinib (an VEGFR-2 Inhibitor) and Hepatic Artery Infusion Chemotherapy for Hepatocellular Carcinoma in Barcelona Clinic Liver Cancer Stage C (TRIPLET): A Phase II Study. Signal Transduct Target Ther 2023, 8, 413. [CrossRef]
- You, H.; Liu, X.; Guo, J.; Lin, Y.; Zhang, Y.; Li, C. Hepatic Arterial Infusion Chemotherapy and Sequential Ablation Treatment in Large Hepatocellular Carcinoma. Int J Hyperthermia 2022, 39, 1097–1105. [CrossRef]
- Gao, S.; Zhang, P.-J.; Guo, J.-H.; Chen, H.; Xu, H.-F.; Liu, P.; Yang, R.-J.; Zhu, X. Chemoembolization Alone vs Combined Chemoembolization and Hepatic Arterial Infusion Chemotherapy in Inoperable Hepatocellular Carcinoma Patients. World J Gastroenterol 2015, 21, 10443–10452. [CrossRef]
- Okuda, K.; Tanaka, M.; Shibata, J.; Ando, E.; Ogata, T.; Kinoshita, H.; Eriguchi, N.; Aoyagi, S.; Tanikawa, K. Hepatic Arterial Infusion Chemotherapy with Continuous Low Dose Administration of Cisplatin and 5-Fluorouracil for Multiple Recurrence of Hepatocellular Carcinoma after Surgical Treatment. Oncol Rep 1999, 6, 587–591. [CrossRef]
- Jeong, S.W.; Jang, J.Y.; Lee, J.E.; Lee, S.H.; Kim, S.G.; Cha, S.-W.; Kim, Y.S.; Cho, Y.D.; Kim, H.S.; Kim, B.S.; et al. The Efficacy of Hepatic Arterial Infusion Chemotherapy as an Alternative to Sorafenib in Advanced Hepatocellular Carcinoma. Asia Pac J Clin Oncol 2012, 8, 164–171. [CrossRef]
- Moriguchi, M.; Aramaki, T.; Nishiofuku, H.; Sato, R.; Asakura, K.; Yamaguchi, K.; Tanaka, T.; Endo, M.; Itoh, Y. Sorafenib versus Hepatic Arterial Infusion Chemotherapy as Initial Treatment for Hepatocellular Carcinoma with Advanced Portal Vein Tumor Thrombosis. Liver Cancer 2017, 6, 275–286. [CrossRef]
- Ando, E.; Tanaka, M.; Yamashita, F.; Kuromatsu, R.; Yutani, S.; Fukumori, K.; Sumie, S.; Yano, Y.; Okuda, K.; Sata, M. Hepatic Arterial Infusion Chemotherapy for Advanced Hepatocellular Carcinoma with Portal Vein Tumor Thrombosis: Analysis of 48 Cases. Cancer 2002, 95, 588–595. [CrossRef]
- Yamasaki, T.; Kimura, T.; Kurokawa, F.; Aoyama, K.; Ishikawa, T.; Tajima, K.; Yokoyama, Y.; Takami, T.; Omori, K.; Kawaguchi, K.; et al. Prognostic Factors in Patients with Advanced Hepatocellular Carcinoma Receiving Hepatic Arterial Infusion Chemotherapy. J Gastroenterol 2005, 40, 70–78. [CrossRef]
- Ueshima, K.; Kudo, M.; Takita, M.; Nagai, T.; Tatsumi, C.; Ueda, T.; Kitai, S.; Ishikawa, E.; Yada, N.; Inoue, T.; et al. Hepatic Arterial Infusion Chemotherapy Using Low-Dose 5-Fluorouracil and Cisplatin for Advanced Hepatocellular Carcinoma. Oncology 2010, 78 Suppl 1, 148–153. [CrossRef]
- Niizeki, T.; Sumie, S.; Torimura, T.; Kurogi, J.; Kuromatsu, R.; Iwamoto, H.; Aino, H.; Nakano, M.; Kawaguchi, A.; Kakuma, T.; et al. Serum Vascular Endothelial Growth Factor as a Predictor of Response and Survival in Patients with Advanced Hepatocellular Carcinoma Undergoing Hepatic Arterial Infusion Chemotherapy. J Gastroenterol 2012, 47, 686–695. [CrossRef]
- Nouso, K.; Miyahara, K.; Uchida, D.; Kuwaki, K.; Izumi, N.; Omata, M.; Ichida, T.; Kudo, M.; Ku, Y.; Kokudo, N.; et al. Effect of Hepatic Arterial Infusion Chemotherapy of 5-Fluorouracil and Cisplatin for Advanced Hepatocellular Carcinoma in the Nationwide Survey of Primary Liver Cancer in Japan. Br J Cancer 2013, 109, 1904–1907. [CrossRef]
- Ueshima, K.; Kudo, M.; Tanaka, M.; Kumada, T.; Chung, H.; Hagiwara, S.; Inoue, T.; Yada, N.; Kitai, S. Phase I/II Study of Sorafenib in Combination with Hepatic Arterial Infusion Chemotherapy Using Low-Dose Cisplatin and 5-Fluorouracil. Liver Cancer 2015, 4, 263–273. [CrossRef]
- Hatooka, M.; Kawaoka, T.; Aikata, H.; Inagaki, Y.; Morio, K.; Nakahara, T.; Murakami, E.; Tsuge, M.; Hiramatsu, A.; Imamura, M.; et al. Hepatic Arterial Infusion Chemotherapy Followed by Sorafenib in Patients with Advanced Hepatocellular Carcinoma (HICS 55): An Open Label, Non-Comparative, Phase II Trial. BMC Cancer 2018, 18, 633. [CrossRef]
- Kudo, M.; Ueshima, K.; Yokosuka, O.; Ogasawara, S.; Obi, S.; Izumi, N.; Aikata, H.; Nagano, H.; Hatano, E.; Sasaki, Y.; et al. Sorafenib plus Low-Dose Cisplatin and Fluorouracil Hepatic Arterial Infusion Chemotherapy versus Sorafenib Alone in Patients with Advanced Hepatocellular Carcinoma (SILIUS): A Randomised, Open Label, Phase 3 Trial. Lancet Gastroenterol Hepatol 2018, 3, 424–432. [CrossRef]
- Sakon, M.; Nagano, H.; Dono, K.; Nakamori, S.; Umeshita, K.; Yamada, A.; Kawata, S.; Imai, Y.; Iijima, S.; Monden, M. Combined Intraarterial 5-Fluorouracil and Subcutaneous Interferon-Alpha Therapy for Advanced Hepatocellular Carcinoma with Tumor Thrombi in the Major Portal Branches. Cancer 2002, 94, 435–442. [CrossRef]
- Kasai, K.; Ushio, A.; Kasai, Y.; Sawara, K.; Miyamoto, Y.; Oikawa, K.; Kuroda, H.; Takikawa, Y.; Suzuki, K. Therapeutic Efficacy of Combination Therapy with Intra-Arterial 5-Fluorouracil and Systemic Pegylated Interferon α-2b for Advanced Hepatocellular Carcinoma with Portal Venous Invasion. Cancer 2012, 118, 3302–3310. [CrossRef]
- Enjoji, M.; Morizono, S.; Kotoh, K.; Kohjima, M.; Miyagi, Y.; Yoshimoto, T.; Nakamuta, M. Re-Evaluation of Antitumor Effects of Combination Chemotherapy with Interferon-Alpha and 5-Fluorouracil for Advanced Hepatocellular Carcinoma. World J Gastroenterol 2005, 11, 5685–5687. [CrossRef]
- Ota, H.; Nagano, H.; Sakon, M.; Eguchi, H.; Kondo, M.; Yamamoto, T.; Nakamura, M.; Damdinsuren, B.; Wada, H.; Marubashi, S.; et al. Treatment of Hepatocellular Carcinoma with Major Portal Vein Thrombosis by Combined Therapy with Subcutaneous Interferon-Alpha and Intra-Arterial 5-Fluorouracil; Role of Type 1 Interferon Receptor Expression. Br J Cancer 2005, 93, 557–564. [CrossRef]
- Obi, S.; Yoshida, H.; Toune, R.; Unuma, T.; Kanda, M.; Sato, S.; Tateishi, R.; Teratani, T.; Shiina, S.; Omata, M. Combination Therapy of Intraarterial 5-Fluorouracil and Systemic Interferon-Alpha for Advanced Hepatocellular Carcinoma with Portal Venous Invasion. Cancer 2006, 106, 1990–1997. [CrossRef]
- Nagano, H.; Wada, H.; Kobayashi, S.; Marubashi, S.; Eguchi, H.; Tanemura, M.; Tomimaru, Y.; Osuga, K.; Umeshita, K.; Doki, Y.; et al. Long-Term Outcome of Combined Interferon-α and 5-Fluorouracil Treatment for Advanced Hepatocellular Carcinoma with Major Portal Vein Thrombosis. Oncology 2011, 80, 63–69. [CrossRef]
- Yamashita, T.; Arai, K.; Sunagozaka, H.; Ueda, T.; Terashima, T.; Yamashita, T.; Mizukoshi, E.; Sakai, A.; Nakamoto, Y.; Honda, M.; et al. Randomized, Phase II Study Comparing Interferon Combined with Hepatic Arterial Infusion of Fluorouracil plus Cisplatin and Fluorouracil Alone in Patients with Advanced Hepatocellular Carcinoma. Oncology 2011, 81, 281–290. [CrossRef]
- Monden, M.; Sakon, M.; Sakata, Y.; Ueda, Y.; Hashimura, E.; FAIT Research Group 5-Fluorouracil Arterial Infusion + Interferon Therapy for Highly Advanced Hepatocellular Carcinoma: A Multicenter, Randomized, Phase II Study. Hepatol Res 2012, 42, 150–165. [CrossRef]
- Wu, J.; Huang, W.-J.; Wang, H.-Y.; Wang, Y.-F.; Peng, B.-G.; Zhou, Q. Arterial Infusion of 5-Fluorouracil Combined with Subcutaneous Injection of Pegylated Interferon Alpha-2b in Treating Unresectable Hepatocellular Carcinoma with Portal Vein Tumor Thrombus. Med Oncol 2015, 32, 65. [CrossRef]
- Kaneko, S.; Urabe, T.; Kobayashi, K. Combination Chemotherapy for Advanced Hepatocellular Carcinoma Complicated by Major Portal Vein Thrombosis. Oncology 2002, 62 Suppl 1, 69–73. [CrossRef]
- Niizeki, T.; Iwamoto, H.; Shirono, T.; Shimose, S.; Nakano, M.; Okamura, S.; Noda, Y.; Kamachi, N.; Hiroyuki, S.; Sakai, M.; et al. Clinical Importance of Regimens in Hepatic Arterial Infusion Chemotherapy for Advanced Hepatocellular Carcinoma with Macrovascular Invasion. Cancers (Basel) 2021, 13, 4450. [CrossRef]
- Iwamoto, H.; Niizeki, T.; Nagamatsu, H.; Ueshima, K.; Tani, J.; Kuzuya, T.; Kasai, K.; Kooka, Y.; Hiraoka, A.; Sugimoto, R.; et al. The Clinical Impact of Hepatic Arterial Infusion Chemotherapy New-FP for Hepatocellular Carcinoma with Preserved Liver Function. Cancers (Basel) 2022, 14, 4873. [CrossRef]
- Nagamatsu, H.; Sumie, S.; Niizeki, T.; Tajiri, N.; Iwamoto, H.; Aino, H.; Nakano, M.; Shimose, S.; Satani, M.; Okamura, S.; et al. Hepatic Arterial Infusion Chemoembolization Therapy for Advanced Hepatocellular Carcinoma: Multicenter Phase II Study. Cancer Chemother Pharmacol 2016, 77, 243–250. [CrossRef]
- Maruta, S.; Koshima, Y.; Tsuchiya, T.; Tamura, R.; Takahashi, M.; Ohshima, T.; Ooka, Y. Combination Therapy of Lenvatinib and Hepatic Arterial Infusion Chemotherapy Using Cisplatin With Lipiodol and 5-Fluorouracil: A Potential Breakthrough Therapy for Unresectable Advanced Hepatocellular Carcinoma. Cureus 2024, 16, e66185. [CrossRef]
- Nakano, M.; Niizeki, T.; Nagamatsu, H.; Tanaka, M.; Kuromatsu, R.; Satani, M.; Okamura, S.; Iwamoto, H.; Shimose, S.; Shirono, T.; et al. Clinical Effects and Safety of Intra-Arterial Infusion Therapy of Cisplatin Suspension in Lipiodol Combined with 5-Fluorouracil versus Sorafenib, for Advanced Hepatocellular Carcinoma with Macroscopic Vascular Invasion without Extra-Hepatic Spread: A Prospective Cohort Study. Mol Clin Oncol 2017, 7, 1013–1020. [CrossRef]
- Iwamoto, H.; Niizeki, T.; Nagamatsu, H.; Ueshima, K.; Nomura, T.; Kuzuya, T.; Kasai, K.; Kooka, Y.; Hiraoka, A.; Sugimoto, R.; et al. Survival Benefit of Hepatic Arterial Infusion Chemotherapy over Sorafenib in the Treatment of Locally Progressed Hepatocellular Carcinoma. Cancers (Basel) 2021, 13, 646. [CrossRef]
- Feng, A.-W.; Guo, J.-H.; Gao, S.; Kou, F.-X.; Liu, S.-X.; Liu, P.; Chen, H.; Wang, X.-D.; Xu, H.-F.; Cao, G.; et al. A Randomized Phase II Trial of Hepatic Arterial Infusion of Oxaliplatin plus Raltitrexed versus Oxaliplatin plus 5-Fluorouracil for Unresectable Colorectal Cancer Liver Metastases. Front Oncol 2022, 12, 913017. [CrossRef]
- Chen, S.; Zhang, K.; Liu, W.; Yu, W. Hepatic Arterial Infusion of Oxaliplatin plus Raltitrexed in Patients with Intermediate and Advanced Stage Hepatocellular Carcinoma: A Phase II, Single-Arm, Prospective Study. Eur J Cancer 2020, 134, 90–98. [CrossRef]
- Chen, S.; Wang, X.; Yuan, B.; Peng, J.; Zhang, Q.; Yu, W.; Ge, N.; Weng, Z.; Huang, J.; Liu, W.; et al. Apatinib plus Hepatic Arterial Infusion of Oxaliplatin and Raltitrexed for Hepatocellular Carcinoma with Extrahepatic Metastasis: Phase II Trial. Nat Commun 2024, 15, 8857. [CrossRef]
- Allen, P.J.; Nissan, A.; Picon, A.I.; Kemeny, N.; Dudrick, P.; Ben-Porat, L.; Espat, J.; Stojadinovic, A.; Cohen, A.M.; Fong, Y.; et al. Technical Complications and Durability of Hepatic Artery Infusion Pumps for Unresectable Colorectal Liver Metastases: An Institutional Experience of 544 Consecutive Cases. J Am Coll Surg 2005, 201, 57–65. [CrossRef]
- Sharib, J.M.; Creasy, J.M.; Wildman-Tobriner, B.; Kim, C.; Uronis, H.; Hsu, S.D.; Strickler, J.H.; Gholami, S.; Cavnar, M.; Merkow, R.P.; et al. Hepatic Artery Infusion Pumps: A Surgical Toolkit for Intraoperative Decision-Making and Management of Hepatic Artery Infusion-Specific Complications. Ann Surg 2022, 276, 943–956. [CrossRef]
- Zhu, A.-L.; Liu, L.-X.; Piao, D.-X.; Lin, Y.-X.; Zhao, J.-P.; Jiang, H.-C. Liver Regional Continuous Chemotherapy: Use of Femoral or Subclavian Artery for Percutaneous Implantation of Catheter-Port Systems. World J Gastroenterol 2004, 10, 1659–1662. [CrossRef]
- Laface, C.; Laforgia, M.; Molinari, P.; Ugenti, I.; Gadaleta, C.D.; Porta, C.; Ranieri, G. Hepatic Arterial Infusion of Chemotherapy for Advanced Hepatobiliary Cancers: State of the Art. Cancers (Basel) 2021, 13, 3091. [CrossRef]
Figure 1.
Features of the techniques for HAIC.
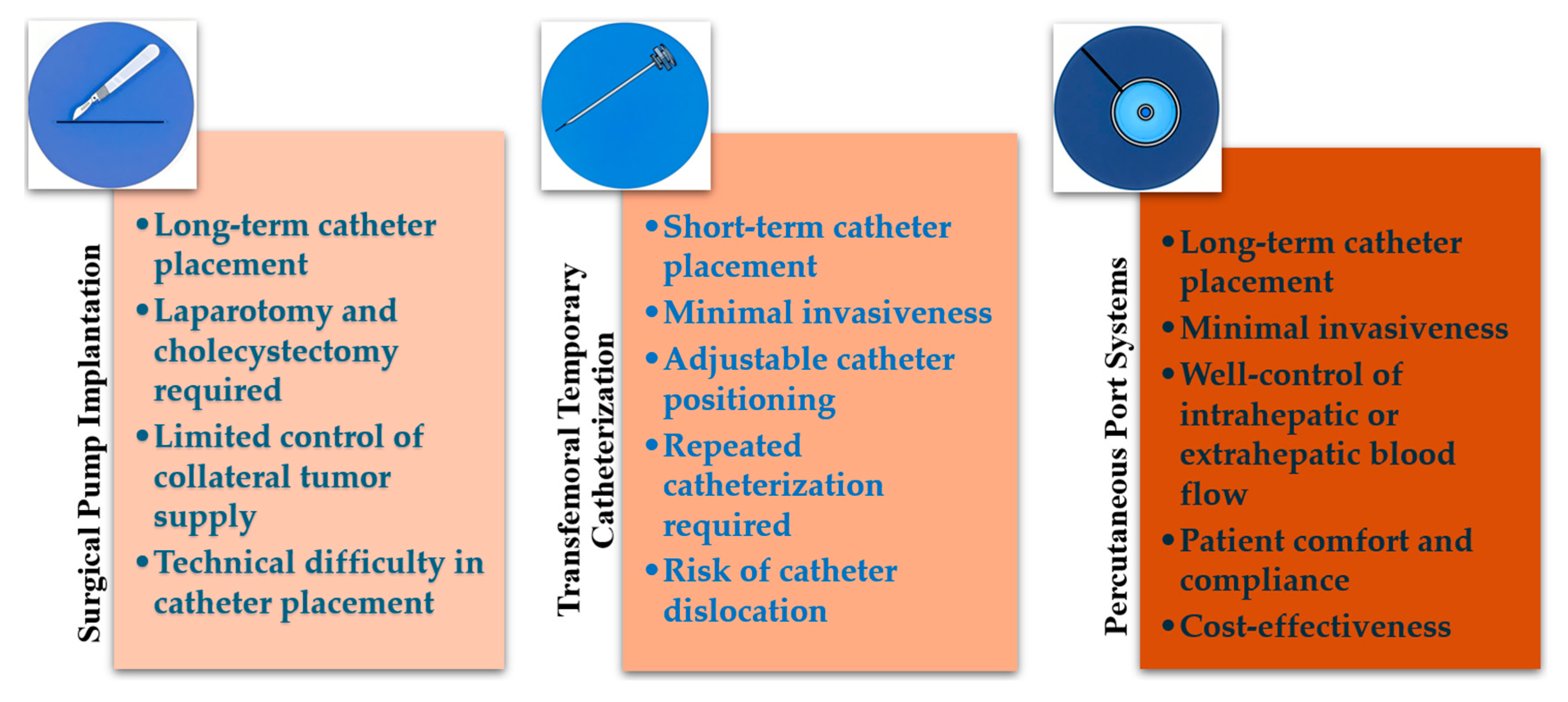
Figure 2.
Figure 2. Administrative procedures of the main regimens for HAIC: (a) FOLFOX; (b) FAIT; (c) Low-dose FP; (d) New FP; (e) Oxaliplatin-raltitrexed.
Figure 2.
Figure 2. Administrative procedures of the main regimens for HAIC: (a) FOLFOX; (b) FAIT; (c) Low-dose FP; (d) New FP; (e) Oxaliplatin-raltitrexed.


Table 1.
Summary of included studies of HAIC combination therapies.
| Study Design | Patient Population | Arm | Sample Size | Efficacy Outcomes | Author (Years) | References |
|---|---|---|---|---|---|---|
| RCT Phase II | Advanced HCC with major PVTT | HAIC(FOLFOX) + Sorafenib | 32 | OS: 16.3 months; ORR: 41%, PFS: 9.0 months |
Zeng K (2022) | [33] |
| Sorafenib | 32 | OS: 6.5 months; ORR: 3%, PFS: 2.5 months |
||||
| RCT Phase III | HCC with PVI (Vp3 and Vp4) | HAIC(FOLFOX) + Sorafenib | 125 | OS: 13.37 months; ORR: 40.8%, PFS: 7.03 months |
He M (2019) |
[38] |
| Sorafenib | 122 | OS: 7.13 months; ORR: 2.46%, PFS: 2.6 months |
||||
| Retrospective Analysis | Intermediate and Advanced HCC Unsuitable for TACE | HAIC(FOLFOX) + PD-(L)1 Inhibitors + MTT | 55 | OS: 15.0 months, PFS: 10.0 months, ORR: 43.6%, DCR: 61.8% |
Tang H-H (2023) | [39] |
| Retrospective Analysis | Unresectable HCC suitable for HAIC or TACE | HAIC(FOLFOX) + TKIs + PD-(L)1 Inhibitors |
302 | OS: Not reached, PFS: 12.4 months, ORR: 33.1%, DCR: 77.8% |
Yu B (2023) |
[40] |
| TACE + TKIs + PD-(L)1 Inhibitors |
446 | OS: 13.8 months, PFS: 8.2 months, ORR: 7.8%; DCR: 47.1% | ||||
| Single-arm Phase II | Advanced HCC unsuitable for TACE | HAIC(FOLFOX) + Lenvatinib + Toripalimab |
36 | PFS at 6 months: 80.6%, Median PFS: 10.4 months, Median OS: 17.9 months | Lai Z (2022) |
[41] |
| Single-arm Phase II | Intermediate and Advanced HCC unsuitable for TACE | HAIC-FOLFOX + Camrelizumab + Apatinib | 35 | ORR: 77.1%, DCR: 97.1%, Median PFS: 10.38 months | Zhang T-Q (2023) | [42] |
| Retrospective Analysis | Large HCC | HAIC(FOLFOX) | 135 | OS: 14.5 months, PFS: 4.6 months, ORR: 33.1% | You H (2022) |
[43] |
| HAIC(FOLFOX) and sequential ablation |
93 | OS: 22.2 months, PFS: 8.5 months, ORR: 51.4% | ||||
| RCT Phase II | Inoperable HCC without distant metastasis |
Chemoembolization alone | 39 | ORR: 45.9%, mPFS: 4.5 months | Gao S (2015) |
[44] |
| HAIC(FOLFOX) + Chemoembolization | 45 | ORR: 68.9%, mPFS: 8.0 months | ||||
| Single-arm Phase I/II | Advanced HCC | HAIC(Low-dose FP) + Sorafenib | 18 | ORR: 38.9%, DCR: 77.8%, TTP: 9.7 months, 1-year OS: 88.2% |
Ueshima K (2015) | [53] |
| Single-arm Phase II | Advanced HCC | HAIC(Low-dose FP) followed by sorafenib if non-response |
55 | 1-year OS: 64.0%, 2-year OS: 48.3% | Hatooka M (2018) | [54] |
| RCT Phase III | Advanced HCC | Sorafenib | 103 | OS: 11.5 months | Kudo M (2018) | [55] |
| HAIC(Low-dose FP) + Sorafenib | 103 | OS: 11.8 months | ||||
| Retrospective Analysis | Unresectable HCC with prior systemic therapy | HAIC(New FP) + Lenvatinib | 6 | ORR: 83%, DCR: 100% | Maruta S (2024) | [69] |
| Single-arm Phase II | Advanced HCC with extrahepatic metastasis | HAIC(Oxaliplatin-raltitrexed) + Apatinib | 39 | ORR: 53.8%; PFS: 6.2 months, OS: 11.3 months, DCR: 89.7% | Chen S (2024) | [74] |
RCT: randomized controlled trial; PVTT: portal vein tumor Thrombosis; PVI: portal vein invasion; PD-(L)1 Inhibitors: programmed death-1 or programmed death-Ligand 1 inhibitors; MTT: molecular targeted therapy; TKIs: tyrosine kinase inhibitors; OS: overall survival; ORR: objective response rate; PFS: progression-free survival; DCR: disease control rate; mPFS: median progression-free survival; TTP: time to progression.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



