
Submitted:
22 March 2025
Posted:
24 March 2025
You are already at the latest version
Abstract
Pelvic organ prolapse (POP) is a common, multifactorial condition where pelvic organs descend into or through the vaginal canal, often compromising quality of life. Despite multiple conservative and surgical options, recurrence rates remain significant, and controversies persist regarding the optimal use of mesh, surgical techniques, and the definition of “successful” outcomes. Discrepancies in patient anatomy, tissue properties, and symptom severity underscore the limitations of a “one-size-fits-all” treatment paradigm and highlight the need for truly personalized care. Computational modeling, particularly finite element analysis (FEA), has attracted increasing attention for its ability to simulate patient-specific biomechanical forces, identify high-risk zones for surgical failure, and inform the design of innovative repair strategies. However, the literature features substantial variability in defining functional versus anatomical success, as well as inconsistent imaging methods and limited in vivo data on tissue properties, all of which make it challenging to establish uniform best practices. In this evolving context yet with too heterogeneous studies, this review summarizes in a critical way the actual methodological gaps, emphasizing the importance of standardized definitions, validated clinical endpoints for patients, and more comprehensive biomechanical characterization as the critical bases for the genesis of an effective computational surgical planning system. Emerging technologies—including machine learning, augmented reality, and multi-omics—promise to enhance diagnostic accuracy and treatment planning, fostering a paradigm shift toward truly individualized, function-oriented management. Bridging mechanical insights, patient-centered metrics, and clinical decision-making may transform POP management, reducing recurrence rates and enabling truly individualized care in gynecological practice.
Keywords:
Pelvic Organ Prolapse
; Finite Element Analysis
; Computational Modeling
; Personalized Surgical Planning
; Biomechanics
1. Introduction
Pelvic organ prolapse (POP) is a prevalent and often debilitating condition in which one or more of the pelvic organs—such as the uterus, bladder, rectum, or vaginal apex—descend from their normal anatomical position, leading to protrusion into or through the vaginal canal. This disorder can severely affect a woman’s quality of life (QoL), manifesting as pelvic pressure, urinary incontinence or urinary obstruction, defecatory dysfunction, and sexual discomfort. Worldwide estimates indicate that roughly 40% of parous women exhibit some degree of POP, with around 11–19% undergoing surgical treatment at least once in their lifetime for pelvic floor disorders. [1,2,3]. Given the anticipated growth of aging populations, these figures are expected to rise, imposing a significant economic burden on healthcare systems and stressing the need for efficacious interventions. Standard management approaches for POP range from conservative (e.g., pelvic floor muscle training, pessaries) to surgical (e.g., native tissue repair, mesh-augmented repair, sacrocolpopexy) [4,5]. Despite continuous refinements in surgical techniques, recurrence rates remain unacceptably high, and re-intervention is common [5]. In addition, controversies persist regarding the optimal use of transvaginal mesh, with concerns over mesh erosion, chronic pain, and complications that have led to restrictions or bans in certain countries [6]. Furthermore, the diversity of anatomical presentations and tissue characteristics often leads to a “one-size-fits-all” approach, which fails to account for individual anatomical and biomechanical variations among patients. These persistent challenges underscore the urgent need for more precise, personalized methods of diagnosing and treating POP. Biomechanical insights into how pelvic floor muscles, connective tissues, and ligaments interact under different loading conditions could inform more tailored and durable interventions. This has catalyzed growing interest in computational modeling techniques—particularly finite element analysis (FEA)—which have the capacity to simulate mechanical stresses and strains within the pelvic floor complex [7,8]. By integrating patient-specific imaging data, accurate material properties, and boundary conditions, FEA-based models aim to predict surgical outcomes, identify high-risk regions for failure, and guide clinicians in devising individualized treatment plans. Despite these advantages, many clinicians remain uncertain about how to incorporate computational modeling into POP management or how to collaborate with biomedical engineers and imaging specialists to generate reliable simulations. Translating engineering-driven modeling methods into daily clinical practice requires a multidisciplinary effort: data acquisition must be precise enough to reflect patient-specific anatomy, biomechanical models require clinically relevant validation, and surgeons need results they can interpret and apply to individual cases. Recognizing this gap is essential for evolving beyond standardized approaches to prolapse repair, as finite element methods could not only inform patient selection for particular interventions but also improve the accuracy and durability of surgeries. By illustrating how computational tools can bridge the current disconnect between complex pelvic floor biomechanics and individualized clinical care, the following sections highlight emerging insights and set the stage for a collaborative, data-driven future in POP management.
2. Materials and Methods
A critical review approach was chosen to highlight the conceptual and practical gaps in both the surgical and computational literature on POP. This decision was prompted by the heterogeneity of available studies: in the surgical domain, there is limited consensus on how to define functional success beyond anatomical correction, while computational research often prioritizes feasibility over integration with real-world clinical outcomes. A targeted search was performed in PubMed, and Google Scholar using the keywords “pelvic organ prolapse,” “finite element analysis,” “biomechanics,” “computational modeling,” and “patient-specific surgical planning,” without restricting the publication date and including only English-language articles. From an initial pool of 261 references, abstracts were screened for relevance to clinical strategies for POP repair, including controversies in treatment selection and success definitions, and to computational or bioinformatics methods aimed at modeling POP biomechanics or predicting outcomes. The authors, drawing on clinical and engineering expertise, retained 45 articles deemed most pertinent for critical appraisal.
Rather than employing a formal risk-of-bias assessment, an expert-driven appraisal was used to underscore four central challenges impeding the development of a unified, patient-specific computational framework. These include the lack of consensus on functional versus anatomical endpoints in clinical POP trials, inconsistencies in imaging techniques and tissue-property measurements across computational studies, limited clinical validation of finite element or machine learning–based models due to small and heterogeneous datasets, and difficulties in creating an adaptive system that can incorporate real-world outcomes over time. This critical review is organized into four sections—Efficacy of Current Treatments and Limitations in Managing Pelvic Organ Prolapse, Rationale for Predictive Tools and the Role of Finite Element Analysis, Status Quo of Computational Modeling in Pelvic Organ Prolapse, and Perspectives—to integrate findings from both surgical and computational fields. This structure allows for a focused examination of methodological shortcomings and culminates in a proposal from the authors for a multifaceted computational platform that merges clinical, biomechanical, and multi-omic data for iterative presurgical planning.
3. Results
3.1. Efficacy of Current Treatments and Limitations in Managing Pelvic Organ Prolapse
POP can be treated conservatively or surgically, depending on symptom severity and patient preferences. Conservative measures include pelvic floor muscle training (PFMT) to strengthen supportive musculature. Several randomized controlled trials have demonstrated that PFMT is effective in reducing symptoms and/or stage of POP in middle-aged women [9]. Furthermore, an assessor-blind RCT found that PFMT significantly improved pelvic floor muscle (PFM) strength and thickness, lifted the bladder neck and rectal ampulla, narrowed the levator hiatus area, and reduced muscle length in women with POP [10]. These morphologic changes suggest that PFMT may also have a potential preventive effect on postpartum POP. However, data remain inconsistent: another RCT in primiparous postpartum women observed no significant reduction in prolapse severity with PFMT, underscoring the need for more high-quality trials [11]. So far, PFMT has been indicated as a tool for managing urinary incontinence rather than POP [12]. Pessary use, involving devices such as ring or Gellhorn pessaries, can relieve symptoms and postpone surgery, but patient compliance, routine follow-ups, and prevention of complications like vaginal ulceration remain crucial [13]. Surgical interventions range from native tissue repairs, such as anterior or posterior colporrhaphy and uterosacral ligament suspension, to more extensive options like sacrocolpopexy. Native tissue techniques seek to restore anatomy without prosthetic materials [4] yet report recurrence rates as high as 20–30% [14]. Mesh-augmented repairs were introduced to increase tissue support and potentially reduce relapse, though complications such as mesh erosion, infection, and dyspareunia have led to caution and regulatory scrutiny in multiple regions [4,15]. Sacrocolpopexy, frequently considered the gold standard for apical prolapse, can achieve durable anatomical restoration [16] but it involves significant surgical complexity and carries mesh-related risks. Reported success rates and complication profiles vary substantially among these approaches, partly due to inconsistencies in defining prolapse recurrence and “successful” outcomes [1], underscoring the need for individualized management. Despite short-term benefits, many prolapse surgeries face durability issues, and recurrence rates can exceed 20% within a few years of repair [1,2,3]. Contributing factors include incomplete restoration of pelvic support, unrecognized secondary defects, and patient-specific predispositions such as collagen abnormalities or obesity [17]. Nevertheless, the complexity of POP management extends beyond achieving anatomical correction alone. While reestablishing normal pelvic support is crucial, the ultimate therapeutic objective is to restore physiological function and enhance patient-reported outcomes, which can vary considerably among individuals. Standard anatomical assessments fail to capture these patient-specific functional nuances, thereby constraining the development of truly personalized treatment strategies. In fact, traditional evaluation systems, notably the Pelvic Organ Prolapse Quantification (POP-Q), record organ descent at a single timepoint [18] and do not capture dynamic physiological changes, such as those induced by coughing or Valsalva maneuvers. Most women and clinicians strongly support incorporating Patient-Reported Outcome Measures (PROMs) since capturing PROMs has the potential to improve individual care and long-term outcomes for women with POP [19]. However, there is a gap in evidence concerning the measurement qualities of currently used PROMs, such as validity, reliability, and responsiveness, within the POP population [20,21]. Moreover, many interventions also hinge on surgeon preference or general guidelines, rather than quantitative, patient-specific biomechanical insights. Consequently, individuals receive standardized procedures that may not reflect variations in anatomical, connective tissue, or muscular integrity, potentially yielding suboptimal results. Further controversy exists regarding the use of synthetic mesh for tissue reinforcement, as widely publicized reports of mesh erosion, infection, and chronic pain have prompted legal restrictions or outright bans in several jurisdictions [22,23]. Although mesh may be beneficial in select cases, the absence of robust predictive criteria makes it challenging to identify who is likely to benefit without incurring excessive risks. Collectively, these findings underscore that the management of pelvic organ prolapse requires more than conventional surgical or anatomical endpoints. Despite a spectrum of therapeutic options ranging from pelvic floor muscle training to mesh-augmented repairs, the goal of fully restoring functional integrity remains elusive. This persistent challenge reflects significant knowledge gaps in the interplay among biomechanical forces, individual anatomical variations, and patient-centered outcomes. Moreover, traditional assessment methods fail to account for dynamic physiological changes and functional improvements that can be paramount to patients, while treatment selection commonly relies on surgeon preference or broad guidelines rather than robust, patient-specific data. Consequently, there is a pressing need for integrative, evidence-based strategies that address both the anatomical correction and the restoration of physiological function. Such an approach would leverage quantitative biomechanical insights and validated patient-reported measures to achieve truly individualized care, reduce recurrence rates, and enhance long-term quality of life for women with POP.
3.2. Rationale for Predictive Tools and the Role of Finite Element Analysis
A growing consensus suggests that personalized approaches are essential for effectively managing POP, particularly given the high recurrence rates, mesh controversies, and the routine reliance on broadly applied guidelines [24]. Anatomical differences in pelvic floor structure, tissue quality, and biomechanical behavior can substantially affect surgical outcomes, yet clinicians often lack the patient-specific parameters needed to adjust intervention strategies [25,26]. Without rigorous methods to capture these details, the reliance on subjective assessments and generalized protocols persists, leaving surgical results unpredictable and prone to the risk of recurrence or complications. FEA has emerged as a powerful computational method for uncovering the biomechanical complexities that underlie POP [8]. By dividing the pelvic floor anatomy into discrete elements and calculating stress and strain distributions under various loads (e.g., coughing, Valsalva maneuvers, or surgical interventions), FEA can reveal subtleties that standard clinical examinations or static imaging cannot [7]. Researchers employing FEA have shown how tissue regions under elevated mechanical stress may correlate with surgical failures or future prolapse [27], suggesting a potential role for this method in identifying high-risk zones prior to intervention. Through virtual testing of repair techniques or mesh placements, FEA can also assist in choosing patient-specific solutions [25], and certain advanced models incorporate time-dependent factors, including repeated loading cycles and muscle fatigue [25]. Compared to static measurements like the well-known POP-Q system or limited two-dimensional imaging, three-dimensional FEA accounts for the multifaceted interactions among muscles, connective tissues, and organs [28]. Such models enable parametric sensitivity analyses, allowing the evaluation of subtle changes in material properties—such as collagen elasticity—or surgical variables like mesh tension. This capability identifies the factors contributing most to surgical failure or recurrence, informing more precise, tailored interventions. Despite its promise, FEA faces several hurdles, including the demand for high-quality imaging (often MRI-based) to construct anatomically accurate models and the complexity of identifying realistic material properties for anisotropic or viscoelastic tissues. Validation can be problematic due to limited intraoperative or postoperative measurements of actual tissue behavior, making it difficult to confirm model predictions. Nonetheless, incremental improvements in imaging modalities, data segmentation, material characterization, and validation frameworks suggest that routine clinical application of FEA is an attainable goal in the near future.
3.3. Status Quo of Computational Modeling in Pelvic Organ Prolapse
3.3.1. Multi-Compartment Approaches and the Importance of Global Repair
Early computational studies focused on individual compartments, yet several investigations now emphasize multi-compartment finite element models that account for organ competition and the interplay between anterior, posterior, and apical supports [29]. By including the levator ani muscle, cardinal and uterosacral ligaments, and the paravaginal attachments, these models quantify how a defect in one region can exacerbate displacement in another. In one analysis [28], combined impairments of the levator ani and apical tissues increased cystocele severity by up to 33%, indicating that local repairs may be insufficient if coexisting support deficits remain unaddressed. Another study [30] employed two-dimensional FE simulations to demonstrate how alterations in uterine orientation (e.g., a 90° tilt) redistribute stresses toward the posterior vaginal wall, reinforcing the viewpoint that global reconstruction—particularly of the apex—is critical to reducing high-strain zones. By simulating different support defects in the same pelvic model [27,28], researchers have highlighted the concept of “organ competition,” showing that rectocele or cystocele formation can influence or conceal prolapse in adjacent compartments. These findings have guided more extensive, multi-structure surgical techniques aimed at stabilizing the entire pelvic floor rather than repairing a single defect in isolation.
3.3.2. Tissue-Specific Material Characterization and Anatomic Fidelity
The constitutive behavior of pelvic tissues has gained considerable attention, with many groups applying hyperelastic laws—such as Yeoh or Ogden—to reflect the nonlinear mechanical response of the vaginal wall, ligaments, and muscle [29,31]. One study [29] quantified how variations in mesh stiffness or suture approaches alter peak tissue displacement and stress, providing data on why continuous suturing or stiffer materials can reduce deformation but simultaneously raise local stress concentrations. Investigations measuring compliance and strain under elevated intra-abdominal pressure [32] further demonstrated that anterior tissues frequently show higher displacement than posterior tissues, corroborating clinical observations of anterior wall vulnerability. Similarly, high-resolution anatomical scans of the cardinal and uterosacral ligaments [33] revealed stress magnitudes often exceeding 1.5 MPa at these sites, suggesting that these ligaments may fail first when subjected to Valsalva-like loads. Other efforts have mapped how pregnancy-induced remodeling of the uterosacral ligament, often persisting postpartum, can predispose women to prolapse [34]. Such anatomically faithful, data-driven modeling extends the utility of FE simulations by pinpointing the precise tissue zones—ligaments, fascial layers, or levator insertions—that should be reinforced to minimize recurrence.
3.3.3. Evaluations of Surgical Technique and Mesh-Related Interventions
Simulated repairs using FE modeling have clarified the biomechanical outcomes of specific mesh anchoring techniques, suture configurations, and fixation strategies [35,36]. One mesh-related investigation [35] demonstrated that increasing mesh width from two centimeters to three can significantly reduce organ mobility but at the cost of higher local suture stress at critical zones such as the cervix; distributing sutures more evenly mitigates such stress peaks. Other teams have simulated the effect of unilateral vs. bilateral sacrospinous fixation, finding that bilateral fixation yields greater apex support and less overall displacement [37]. In uterine-preserving surgeries, some analyses suggest that leaving the uterus in situ can lead to increased regional stresses and a possible higher chance of recurrence unless tensioning and anchoring are optimized [37]. Similarly, continuous rather than simple suture anchoring around the uterosacral ligaments has demonstrated about 10% lower displacement, underscoring the potential to fine-tune mechanical stability via relatively minor changes in surgical technique [36]. Across these models, parametric sweeps of suture spacing, mesh stiffness, or anchoring points highlight how even small adjustments in tension can double or halve local stress, reinforcing the relevance of preoperative simulations for individualized procedural planning.
3.3.4. Patient-Specific Modeling, Validation, and Clinical Integration
Increasingly, patient-specific geometries derived from MRI or high-resolution scanning have been incorporated into FE models, allowing surgeons and engineers to “test” various interventions before the actual operation [31,38]. Some studies validate model outputs against dynamic MRI frames or direct measurements of tissue displacement, showing that simulated and observed data often coincide within a few millimeters [31,32]. A few have moved toward real-time or near-real-time predictions, coupling finite element methods with machine learning [39]. For instance, nodal displacements can be estimated within seconds, potentially allowing obstetric teams to identify patients at high risk for levator trauma during labor and thereby adjust delivery strategies. Moreover, validating these patient-specific simulations in prospective clinical settings fosters acceptance of computational tools as part of standard preoperative workflows. These validated models have broad applications, ranging from optimizing sacrospinous fixation angles [37] to assessing the effectiveness of partial hysterectomy in lowering mesh-related stress [40]. Collectively, contemporary FE modeling of POP elucidates the mechanical underpinnings of prolapse formation, highlights the interdependence of multiple pelvic compartments, and refines our understanding of how specific surgical maneuvers—ranging from suture anchor placement to mesh tensioning—directly alter stress distributions and organ mobility [27,28,29,30,31,32,33,34,35,36,38,39,40,40]. Studies show that single-defect or single-compartment repairs can fail if underlying apical, muscular, or fascial deficits are overlooked. Parametric analyses confirm that mesh design, suture arrangement, and ligament integrity each influence surgical outcomes by as much as 20–30% in some models. Meanwhile, patient-specific reconstructions promise finer customization of repair strategies, supported by validated data comparing simulated and observed displacements. Although challenges persist in consistently capturing tissue viscoelasticity, postpartum remodeling, and dynamic factors such as repeated loading, the collective body of work indicates that computational modeling is transitioning from an academic tool to a clinically relevant adjunct, guiding surgeons toward evidence-based, biomechanically optimized procedures for pelvic organ prolapse.
3.4. Perspectives
FEM in other fields has demonstrated considerable potential for advancing biomechanics research and clinical applications, especially when integrated with high-resolution imaging modalities such as MRI and ultrasound. Studies of corneal behavior via ultrasonic elastography has allowed for the noninvasive assessment of corneal biomechanics, offering heightened accuracy for refractive surgery outcome evaluations [41]. In tumor mechanics, incorporating solid stress and interstitial fluid pressure into FEM has enhanced the interpretation of elastographic imaging in monitoring cancer progression [42]. Beyond soft tissues, detailed MRI-based segmentation and meshing are critical in musculoskeletal FEM to capture realistic tissue responses under load [43,44]. The rapid integration of machine learning (ML) techniques with finite element analysis has further expanded these applications, enabling faster and more precise models. For instance, ML-based approaches for osteoarthritis prediction have reached R² values above 0.9 and demonstrated tangible clinical relevance [45], while Random Forest models for bone strain prediction in the acetabulum have achieved R² ≈ 0.99 [46]. Neural network finite element methods offer simulations that run in seconds rather than hours [47], suggesting that near-real-time patient-specific analyses are within reach, although ongoing work must address long-range tissue interactions and complex mechanical dependencies [48]. Looking forward, real-time FEM simulations coupled with virtual reality (VR) and augmented reality (AR) hold promise for improving surgical planning and intraoperative guidance [49,50]. New algorithms such as PolyFEM have enhanced collision detection and robust solutions for high-energy interactions [51], laying the groundwork for more reliable simulations under dynamic and potentially invasive conditions. Although clinical uptake remains variable, the application of FEM in foot biomechanics and related interventions illustrates its growing role in practical care [52] while AR tools provide real-time anatomical visualization and potential improvements in surgical precision [53]. Nonetheless, applying FEM to pelvic organ prolapse (POP) reveals important limitations inherent in a purely biomechanical framework. POP is a multidimensional disorder influenced by anatomical, physiological, and patient-centered factors—factors not always captured by standard computational predictions. In particular, while FEM can guide surgical decisions that reduce apparent organ mobility, these anatomical corrections do not necessarily correlate with the restoration of pelvic floor function that patients seek. Some clinical investigations, for example, do not confirm improved POP recurrence or symptomatic relief despite FEM-based data suggesting superior fixation strategies [54]. That is why, the central, and most challenging, question remains how to ensure that computational models do more than merely correct anatomical deficiencies, but rather optimize patient-specific functional outcomes in alignment with individual goals. As depicted in Figure 1, a future “block-chain”–style architecture for POP management would integrate multi-faceted data—dynamic imaging, tissue-properties, validated patient-reported outcome measures, and machine learning–driven risk assessments, within an iterative feedback loop. Crucially, this model must be tuned such that the ultimate endpoint is the restoration of pelvic function and well-being for each patient, rather than a single anatomical metric. Achieving that level of precision will require robust algorithms capable of incorporating each woman’s unique clinical profile, anatomical nuances, and personal preferences to predict the surgical approach most likely to fulfill her desired quality of life. By continually refining these computational predictions with real-world clinical data and patient feedback, researchers and clinicians can converge on truly patient-centered, data-driven strategies that transcend one-size-fits-all solutions and deliver durable, meaningful improvements in pelvic floor function.
4. Discussion
POP originates from complex etiologies—ranging from childbirth-related trauma to connective tissue variations—and poses substantial challenges in both diagnosis and treatment. Despite multiple surgical and conservative interventions, recurrence rates remain high, reflecting persistent uncertainties about which surgical strategies optimize both anatomical correction and functional restoration. In particular, the literature lacks consensus on how to define “successful” outcomes beyond short-term anatomical elevation, and many existing trials do not adequately capture patient-centered measures such as symptom relief, sexual function, and overall quality of life.
From a computational standpoint, FEA and related modeling techniques offer a significant opportunity to quantify tissue stresses, simulate different surgical scenarios, and develop predictive algorithms. However, these tools often focus on feasibility proofs or isolated case studies, rarely integrating comprehensive clinical datasets that could enhance model realism and facilitate reliable presurgical planning. Moreover, heterogeneous imaging modalities, variable segmentation approaches, and limited standardization of tissue-property measurements reduce the comparability of different FEA models. Consequently, current applications of computational methods in POP largely remain academic exercises rather than mainstays of routine clinical decision-making. In critically reviewing these challenges, our analysis points to four key requirements for advancing toward robust, patient-specific computational management of POP:
- Standardized Definitions of Clinical Success: Surgical success must incorporate functional endpoints, including patient-reported outcomes, not merely anatomical descriptors such as stage reduction. Harmonized definitions of recurrence and validated PROMs will facilitate more meaningful comparisons across studies and more nuanced validation of computational models.
- Comprehensive, High-Quality Data: Both clinicians and engineers need access to standardized imaging protocols (MRI-based or US 3D reconstructions) and thorough datasets that reflect different loading conditions, tissue compositions, and patient demographics. Machine-learning–or FEA-based systems can only generate reliable predictions when trained on consistent, representative clinical data.
- Adaptive Computational Frameworks: Robust models should evolve over time by incorporating new postoperative data, surgical outcomes, and possibly multi-omic information. Such an iterative “learning” system can continuously refine mesh tension settings, suture placements, or even surgical techniques as more outcome data accrue.
- Collaborative, Multidisciplinary Efforts: Engineers, data scientists, imaging experts, and clinicians must jointly design and validate computational tools. This includes aligning goals on clinically meaningful endpoints, establishing clear workflows for model deployment, and ensuring outputs are interpretable for surgeons.
Encouragingly, early validation studies suggest that patient-specific models can reduce the risk of recurrence by identifying high-stress zones that would otherwise be missed in standard surgical evaluations. Machine learning and real-time simulations further promise rapid, adaptive risk assessments based on iterative feedback loops. However, realizing these benefits at scale depends on addressing current inconsistencies in data collection, tissue characterization, and outcome definitions. As highlighted by our critical review, the path forward involves more than developing sophisticated simulations—it requires a concerted effort to link advanced computational methods with rigorously collected clinical evidence. Ultimately, moving toward a function-focused, evidence-based paradigm will likely hinge on implementing an integrated computational platform: one that unites imaging, multi-omic data, validated clinical endpoints, and machine learning–driven modeling in a real-time feedback system. Such a platform could provide surgeons with preoperative risk assessments tailored to each patient’s anatomical and functional profile, guide intraoperative decisions regarding mesh placement or tissue reinforcement, and adapt over time using postoperative results. While these aspirations remain distant from the current standard of care, the progress in imaging algorithms, computing power, and cross-disciplinary dialogue strongly indicates that personalized, computationally optimized POP management is both achievable and poised to redefine surgical practice.
5. Conclusions
This critical review highlights the persistent gaps limiting the full integration of computational modeling into pelvic organ prolapse management. Current surgical strategies are hindered by inconsistencies in defining functional success, while computational studies often focus on feasibility without incorporating robust, real-world clinical datasets. Bridging these domains requires standardized imaging protocols, well-characterized tissue properties, and validated functional endpoints that capture patient-reported outcomes. By addressing these methodological barriers and engaging in cross-disciplinary collaborations, the field can progress toward an adaptive, multi-omic computational platform. Such a platform would not only enable precise presurgical planning and improved surgical outcomes but also evolve in tandem with accumulating clinical data—ultimately fostering truly individualized, function-oriented interventions for women with POP.
Author Contributions
The conceptualization of the study was carried out by Canio Martinelli, Antonio Giordano, Vincenzo Carnevale, and Alfredo Ercoli. Data curation was performed by Canio Martinelli and Patrizia Maiorano. Formal analysis was conducted by Canio Martinelli, Antonio Giordano, Luigi Alfano, and Patrizia Maiorano. The investigation process was undertaken by Canio Martinelli and Alfredo Ercoli. Methodology was developed by Canio Martinelli, Antonio Giordano, Vincenzo Carnevale, and Alfredo Ercoli. Project administration responsibilities were managed by Canio Martinelli, Antonio Giordano, and Patrizia Maiorano. Resources were provided by Canio Martinelli and Alfredo Ercoli. Validation of the study was performed by Canio Martinelli, Patrizia Maiorano, Luigi Alfano, and Alfredo Ercoli. Writing of the original draft was completed by Canio Martinelli and Patrizia Maiorano, while review and editing were conducted by Canio Martinelli, Vincenzo Carnevale, Luigi Alfano, Patrizia Maiorano, and Alfredo Ercoli.
Funding and Acknowledgments
This study did not receive any funding or financial support. The authors acknowledge the contributions of their respective institutions for providing the necessary infrastructure and support to carry out this work.
Institutional Review Board Statement
In this section, you should add the Institutional Review Board Statement and approval number, if relevant to your study. You might choose to exclude this statement if the study did not require ethical approval. Please note that the Editorial Office might ask you for further information. Please add “The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of NAME OF INSTITUTE (protocol code XXX and date of approval).” for studies involving humans. OR “The animal study protocol was approved by the Institutional Review Board (or Ethics Committee) of NAME OF INSTITUTE (protocol code XXX and date of approval).” for studies involving animals. OR “Ethical review and approval were waived for this study due to REASON (please provide a detailed justification).” OR “Not applicable” for studies not involving humans or animals.
Informed Consent Statement
Not applicable since this study does not involve humans.
Conflicts of Interest
The authors declare no conflicts of interest related to this study or the publication of this manuscript.
Abbreviations
The following abbreviations are used in this manuscript:
| POP | Pelvic Organ Prolapse |
| QoL | Quality of Life |
| PFMT | Pelvic Floor Muscle Training |
| FEA | Finite Element Analysis |
| MRI | Magnetic Resonance Imaging |
| US | Ultra Sound |
| PROMs | Patient-Reported Outcome Measures |
| POP-Q | Pelvic Organ Prolapse Quantification |
| 2D | Two-Dimensional |
| 3D | Three-Dimensional |
| ML | Machine Learning |
| VR | Virtual Reality |
| AR | Augmented Reality |
References
- Barber, M.D. Pelvic organ prolapse. BMJ 2016, i3853. [Google Scholar] [CrossRef] [PubMed]
- Hendrix, S.L.; Clark, A.; Nygaard, I.; Aragaki, A.; Barnabei, V.; McTiernan, A. Pelvic organ prolapse in the women’s health initiative: Gravity and gravidity. Am J Obstet Gynecol. 2002, 186, 1160–1166. [Google Scholar] [CrossRef] [PubMed]
- Wu, J.M.; Matthews, C.A.; Conover, M.M.; Pate, V.; Jonsson Funk, M. Lifetime Risk of Stress Urinary Incontinence or Pelvic Organ Prolapse Surgery. Obstet Gynecol. 2014, 123, 1201–1206. [Google Scholar] [CrossRef]
- Maher, C.; Feiner, B.; Baessler, K.; Schmid, C. Surgical management of pelvic organ prolapse in women. In: The Cochrane Collaboration, editor. Cochrane Database of Systematic Reviews [Internet]. Chichester, UK: John Wiley & Sons, Ltd; 2013 [cited 2025 Feb 17]. p. CD004014.pub5. Available from: https://doi.wiley.com/10.1002/14651858.CD004014.
- Smith, F.J.; Holman, C.D.J.; Moorin, R.E.; Tsokos, N. Lifetime Risk of Undergoing Surgery for Pelvic Organ Prolapse: Obstet Gynecol. 2010, 116, 1096–1100. [CrossRef]
- Danford, J.M.; Osborn, D.J.; Reynolds, W.S.; Biller, D.H.; Dmochowski, R.R. Postoperative pain outcomes after transvaginal mesh revision. Int Urogynecology J. 2015, 26, 65–69. [Google Scholar] [CrossRef]
- Duarte Thibault, M.; Chen, L.; Huebner, M.; DeLancey, J.O.; Swenson, C.W. A comparison of MRI-based pelvic floor support measures between young and old women with prolapse. Int Urogynecology J. 2023, 34, 2081–2088. [Google Scholar] [CrossRef]
- Silva, M.E.T.; Brandão, S.; Parente, M.P.L.; Mascarenhas, T.; Natal Jorge, R.M. Biomechanical properties of the pelvic floor muscles of continent and incontinent women using an inverse finite element analysis. Comput Methods Biomech Biomed Engin. 2017, 20, 842–852. [Google Scholar] [CrossRef]
- Espiño-Albela, A.; Castaño-García, C.; Díaz-Mohedo, E.; Ibáñez-Vera, A.J. Effects of Pelvic-Floor Muscle Training in Patients with Pelvic Organ Prolapse Approached with Surgery vs. Conservative Treatment: A Systematic Review. J Pers Med. 2022, 12, 806. [Google Scholar] [CrossRef]
- Hoff Brækken, I.; Majida, M.; Engh, M.E.; Bø, K. Morphological changes after pelvic floor muscle training measured by 3-dimensional ultrasonography: a randomized controlled trial. Obstet Gynecol. 2010, 115 Pt 1, 317–324. [Google Scholar] [CrossRef]
- Bø, K.; Hilde, G.; Stær-Jensen, J.; Siafarikas, F.; Tennfjord, M.K.; Engh, M.E. Postpartum pelvic floor muscle training and pelvic organ prolapse—a randomized trial of primiparous women. Am J Obstet Gynecol. 2015, 212, e1–e38. [Google Scholar] [CrossRef]
- Dumoulin, C.; Cacciari, L.P.; Hay-Smith, E.J.C. Pelvic floor muscle training versus no treatment, or inactive control treatments, for urinary incontinence in women. Cochrane Incontinence Group, editor. Cochrane Database Syst Rev [Internet]. 2018 Oct 4 [cited 2025 Feb 17];2018(10). Available from: http://doi.wiley.com/10.1002/14651858.CD005654. [CrossRef]
- Abdulaziz, M.M.; Stothers, L.; Lazare, D.; Macnab, A. An integrative review and severity classification of complications related to pessary use in the treatment of female pelvic organ prolapse. Can Urol Assoc, J. 2015, 9, 400. [Google Scholar] [CrossRef]
- De Tayrac, R.; Letouzey, V. Basic science and clinical aspects of mesh infection in pelvic floor reconstructive surgery. Int Urogynecology, J. 2011, 22, 775–780. [Google Scholar] [CrossRef] [PubMed]
- Mock, S.; Reynolds, W.S.; Dmochowski, R.R. Trans-Vaginal Mesh Revision: A Comprehensive Review on Etiologies and Management Strategies with Emphasis on Postoperative Pain Outcomes. LUTS Low Urin Tract Symptoms. 2014, 6, 69–75. [Google Scholar] [CrossRef] [PubMed]
- Nygaard, I.; Brubaker, L.; Zyczynski, H.M.; Cundiff, G.; Richter, H.; Gantz, M.; et al. Long-term outcomes following abdominal sacrocolpopexy for pelvic organ prolapse. JAMA. 2013, 309, 2016–2024. [Google Scholar] [CrossRef] [PubMed]
- Vergeldt, T.F.M.; Weemhoff, M.; IntHout, J.; Kluivers, K.B. Risk factors for pelvic organ prolapse and its recurrence: a systematic review. Int Urogynecology, J. 2015, 26, 1559–1573. [Google Scholar] [CrossRef]
- Bump, R.C.; Mattiasson, A.; Bø, K.; Brubaker, L.P.; DeLancey, J.O.; Klarskov, P.; et al. The standardization of terminology of female pelvic organ prolapse and pelvic floor dysfunction. Am J Obstet Gynecol. 1996, 175, 10–17. [Google Scholar] [CrossRef]
- Ruseckaite, R.; Jayasinghe, R.; Bavor, C.; Dean, J.; Daly, O.; Ahern, S. Evaluation and acceptability of patient-reported outcome measures in women following pelvic organ prolapse procedures. BMC Health Serv Res. 2023, 23, 624. [Google Scholar] [CrossRef]
- Conrad, S.J.; Bernard, S.; Gross, D.P.; McLean, L. Patient-Reported Outcome Measures for Pelvic Organ Prolapse: A Systematic Review Using the COnsensus-Based Standards for the Selection of Health Measurement Instruments (COSMIN) Checklist. Bjog. 2025, 132, 105–117. [Google Scholar] [CrossRef]
- Dieter, A.A.; Halder, G.E.; Pennycuff, J.F.; Singh, R.; El-Nashar, S.A.; Lipetskaia, L.; et al. Patient-Reported Outcome Measures for Use in Women With Pelvic Organ Prolapse: A Systematic Review. Obstet Gynecol. 2023, 141, 1098–1114. [Google Scholar] [CrossRef]
- Chapple, C.R.; Cruz, F.; Deffieux, X.; Milani, A.L.; Arlandis, S.; Artibani, W.; et al. Consensus Statement of the European Urology Association and the European Urogynaecological Association on the Use of Implanted Materials for Treating Pelvic Organ Prolapse and Stress Urinary Incontinence. Eur Urol. 2017, 72, 424–431. [Google Scholar] [CrossRef]
- Health C for D and, R. FDA’s Activities: Urogynecologic Surgical Mesh. FDA [Internet]. 2024 Aug 9 [cited 2025 Feb 17]; Available from: https://www.fda.
- Aboseif, C.; Liu, P. Pelvic Organ Prolapse. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 [cited 2025 Feb 17]. Available from: http://www.ncbi.nlm.nih. 5632. [Google Scholar]
- Jelovsek, J.E.; Chagin, K.; Lukacz, E.S.; Nolen, T.L.; Shepherd, J.P.; Barber, M.D.; et al. Models for Predicting Recurrence, Complications, and Health Status in Women After Pelvic Organ Prolapse Surgery. Obstet Gynecol. 2018, 132, 298–309. [Google Scholar] [CrossRef]
- Jelovsek, J.E.; Maher, C.; Barber, M.D. Pelvic organ prolapse. Lancet Lond Engl. 2007, 369, 1027–1038. [Google Scholar] [CrossRef] [PubMed]
- Luo, J.; Chen, L.; Fenner, D.E.; Ashton-Miller, J.A.; DeLancey, J.O.L. A multi-compartment 3-D finite element model of rectocele and its interaction with cystocele. J Biomech. 2015, 48, 1580–1586. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Ashton-Miller, J.A.; DeLancey, J.O.L. A 3D finite element model of anterior vaginal wall support to evaluate mechanisms underlying cystocele formation. J Biomech. 2009, 42, 1371–1377. [Google Scholar] [CrossRef]
- Yang, M.; Chen, C.; Wang, Z.; Long, J.; Huang, R.; Qi, W.; et al. Finite element analysis of female pelvic organ prolapse mechanism: current landscape and future opportunities. Front Med. 2024, 11, 1342645. [Google Scholar] [CrossRef]
- Xue, X.; Wang, H.; Xie, J.; Gao, Z.; Shen, J.; Yao, T. Two-dimensional biomechanical finite element modeling of the pelvic floor and prolapse. Biomech Model Mechanobiol. 2023, 22, 1425–1446. [Google Scholar] [CrossRef]
- Chen, Z.W.; Joli, P.; Feng, Z.Q.; Rahim, M.; Pirró, N.; Bellemare, M.E. Female patient-specific finite element modeling of pelvic organ prolapse (POP). J Biomech. 2015, 48, 238–245. [Google Scholar] [CrossRef]
- Liu, X.; Rong, Q.; Liu, Y.; Wang, J.; Xie, B.; Ren, S. Relationship between high intra-abdominal pressure and compliance of the pelvic floor support system in women without pelvic organ prolapse: A finite element analysis. Front Med. 2022, 9, 820016. [Google Scholar] [CrossRef]
- Xu, Z.; Chen, N.; Wang, B.; Yang, J.; Liu, H.; Zhang, X.; et al. Creation of the biomechanical finite element model of female pelvic floor supporting structure based on thin-sectional high-resolution anatomical images. J Biomech. 2023, 146, 111399. [Google Scholar] [CrossRef]
- Jean Dit Gautier, E.; Mayeur, O.; Lepage, J.; Brieu, M.; Cosson, M.; Rubod, C. Pregnancy impact on uterosacral ligament and pelvic muscles using a 3D numerical and finite element model: preliminary results. Int Urogynecology, J. 2018, 29, 425–430. [Google Scholar] [CrossRef]
- Jeanditgautier, E.; Mayeur, O.; Brieu, M.; Lamblin, G.; Rubod, C.; Cosson, M. Mobility and stress analysis of different surgical simulations during a sacral colpopexy, using a finite element model of the pelvic system. Int Urogynecology, J. 2016, 27, 951–957. [Google Scholar] [CrossRef]
- Silva, M.E.T.; Bessa, J.N.M.; Parente, M.P.L.; Mascarenhas, T.; Natal Jorge, R.M.; Fernandes, A.A. Effect of mesh anchoring technique in uterine prolapse repair surgery: A finite element analysis. J Biomech. 2021, 127, 110649. [Google Scholar] [CrossRef] [PubMed]
- Lallemant, M.; Shimojyo, A.A.; Mayeur, O.; Ramanah, R.; Rubod, C.; Kerbage, Y.; et al. Mobility analysis of a posterior sacrospinous fixation using a finite element model of the pelvic system. Garcia Aznar, J.M.; editor. PLOS ONE. 2024, 19, e0299012. [Google Scholar] [CrossRef]
- Lamblin, G.; Mayeur, O.; Giraudet, G.; Jean Dit Gautier, E.; Chene, G.; Brieu, M.; et al. Pathophysiological aspects of cystocele with a 3D finite elements model. Arch Gynecol Obstet. 2016, 294, 983–989. [Google Scholar] [CrossRef] [PubMed]
- Moura, R.; Oliveira, D.A.; Parente, M.P.L.; Kimmich, N.; Hynčík, L.; Hympánová, L.H.; et al. Patient-specific surrogate model to predict pelvic floor dynamics during vaginal delivery. J Mech Behav Biomed Mater. 2024, 160, 106736. [Google Scholar] [CrossRef]
- Lallemant, M.; Vega, A.; Chambert, J.; Jacquet, E.; Ramanah, R. Biomechanical interests of supra-cervical hysterectomy with sacrocolpopexy: first study using finite element modeling. Int Urogynecology, J. 2021, 32, 1599–1602. [Google Scholar] [CrossRef]
- Ahmed, H.M.; Salem, N.M.; Al-Atabany, W.; Al-Atabany, W. Finite Element Modelling of Corneal Biomechanics Assessment Using Ultrasonic Elastography [Internet]. In Review; 2022 [cited 2025 Feb 17]. Available from: https://www.researchsquare. 2053. [Google Scholar]
- Islam, M.T.; Righetti, R. A Novel Finite Element Model to Assess the Effect of Solid Stress Inside Tumors on Elastographic Normal Strains and Fluid Pressure. J Eng Sci Med Diagn Ther. 2019, 2, 031006. [Google Scholar] [CrossRef]
- Galbusera, F.; Cina, A.; Panico, M.; Albano, D.; Messina, C. Image-based biomechanical models of the musculoskeletal system. Eur Radiol Exp. 2020, 4, 49. [Google Scholar] [CrossRef]
- Trad, Z.; Barkaoui, A.; Chafra, M. ; Tavares JMRS. Finite Element Analysis Applications in Biomechanical Studies of the Knee Joint. In: Trad, Z.; Barkaoui, A.; Chafra, M.; Tavares JMRS, editors. FEM Analysis of the Human Knee Joint: A Review [Internet]. Cham: Springer International Publishing; 2018 [cited 2025 Feb 17]. p. 35–60. Available from. [CrossRef]
- Mononen, M.E.; Liukkonen, M.K.; Turunen, M.J. Machine Learning Model Trained with Finite Element Modeling Can Predict the Risk of Osteoarthritis: Data from the Osteoarthritis Initiative. Appl Sci. 2024, 14, 9538. [Google Scholar] [CrossRef]
- Nimmal Haribabu, G.; Basu, B. Implementing Machine Learning approaches for accelerated prediction of bone strain in acetabulum of a hip joint. J Mech Behav Biomed Mater. 2024, 153, 106495. [Google Scholar] [CrossRef]
- Goodbrake, C.; Motiwale, S.; Sacks, M.S. A neural network finite element method for contact mechanics. Comput Methods Appl Mech Eng. 2024, 419, 116671. [Google Scholar] [CrossRef]
- Shi, J.; Lin, F.; Rao, W. Learning-Based Finite Element Methods Modeling for Complex Mechanical Systems [Internet]. arXiv; 2024 [cited 2025 Feb 18]. Available from: http://arxiv.org/abs/2409.00160. arXiv:10.48550/arXiv.2409.00160.
- Courtecuisse, H.; Dequidt, J. Augmented reality biomechanical simulations for pelvic conditions diagnoses. In: Biomechanics of the Female Reproductive System: Breast and Pelvic Organs [Internet]. Elsevier; 2023 [cited 2025 Feb 17]. p. 455–79. Available from: https://linkinghub.elsevier. 9780. [Google Scholar]
- Motiwale, S.; Zhang, W.; Feldmeier, R.; Sacks, M.S. A neural network finite element approach for high speed cardiac mechanics simulations. Comput Methods Appl Mech Eng. 2024, 427, 117060. [Google Scholar] [CrossRef]
- Martin, L.; Jain, P.; Ferguson, Z.; Gholamalizadeh, T.; Moshfeghifar, F.; Erleben, K.; et al. A systematic comparison between FEBio and PolyFEM for biomechanical systems. Comput Methods Programs Biomed. 2024, 244, 107938. [Google Scholar] [CrossRef] [PubMed]
- Chatzistergos, P.; Behforootan, S.; Naemi, R.; Chockalingam, N. Finite Element Modeling. In: Foot and Ankle Biomechanics [Internet]. Elsevier; 2023 [cited 2025 Feb 17]. p. 365–86. Available from: https://linkinghub.elsevier. 9780. [Google Scholar]
- Zhu, J.; Su, Y.; Liu, Z.; Liu, B.; Sun, Y.; Gao, W.; et al. Real-time biomechanical modelling of the liver using LightGBM model. Int J Med Robot. 2022, 18, e2433. [Google Scholar] [CrossRef] [PubMed]
- Salman, S.; Babaoglu, B.; Kumbasar, S.; Bestel, M.; Ketenci Gencer, F.; Tuna, G.; et al. Comparison of Unilateral and Bilateral Sacrospinous Ligament Fixation Using Minimally Invasive Anchorage. Geburtshilfe Frauenheilkd. 2019, 79, 976–982. [Google Scholar] [CrossRef]
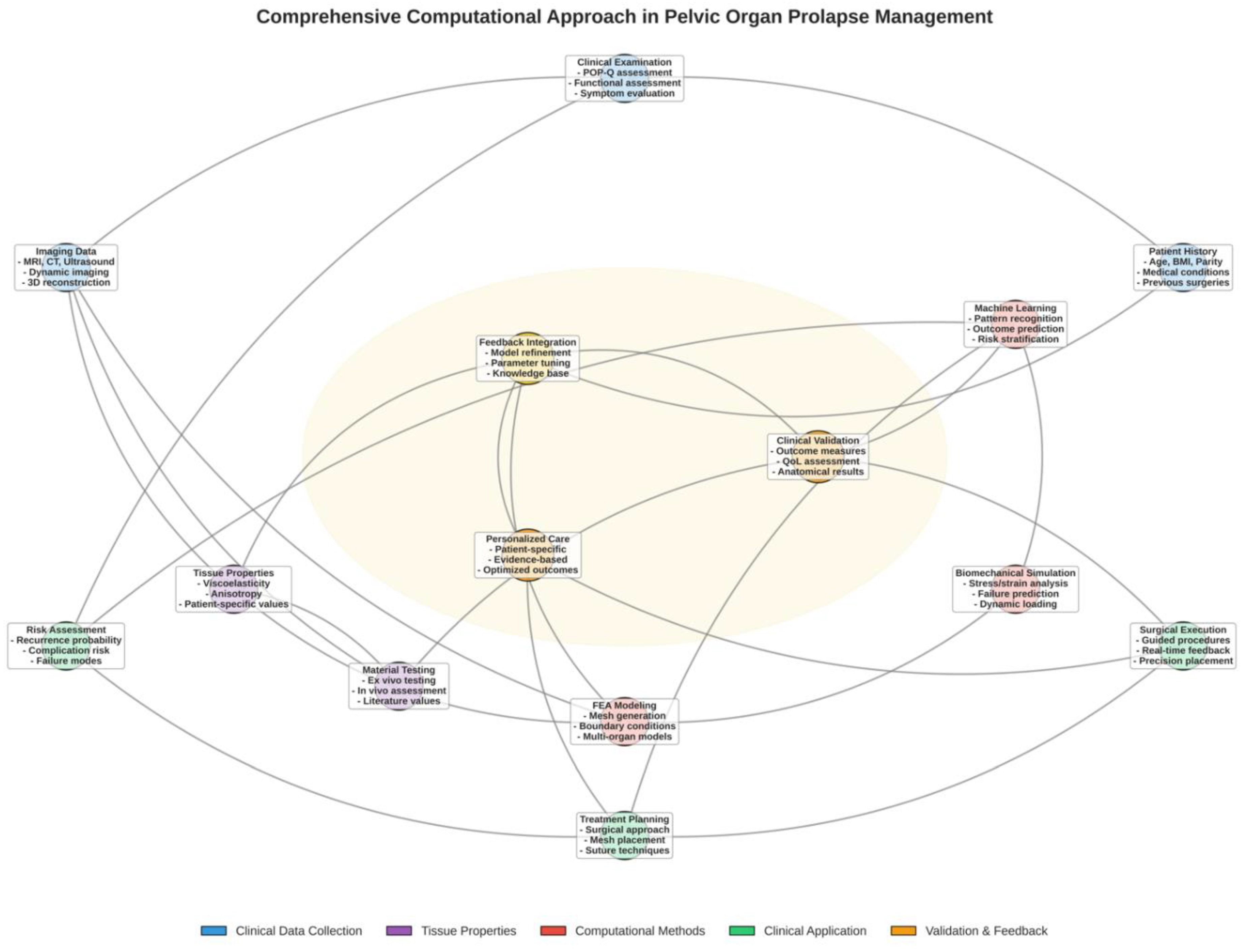
Figure 1.
Comprehensive Computational Workflow for Pelvic Organ Prolapse Management: This figure illustrates an integrated, iterative framework for pelvic organ prolapse (POP) management, organized into five domains: Clinical Data Collection (blue), Tissue Properties (purple), Computational Methods (red), Clinical Application (green), and Validation & Feedback (orange/yellow). Patient-specific data—including clinical assessments (history, physical examination, and imaging) and, where applicable, multi-omic analyses—feed into computational modeling. Finite element analysis (FEA) integrates tissue properties derived from material testing, enabling biomechanical simulations and machine learning–based risk assessments. These outputs guide surgical decision-making by informing tailored treatment plans, such as mesh placement and suture techniques. The central feedback loop (highlighted in yellow) captures how clinical outcomes continually refine computational models and risk algorithms, while personalized surgical strategies influence execution and subsequent data collection. Through this cyclical process, models evolve toward more precise, individualized interventions, potentially reducing recurrence rates and aligning management strategies with each patient’s unique anatomical and functional characteristics. This workflow represents a transition from traditional, experience-based approaches to evidence-driven, computationally optimized POP management.
Figure 1.
Comprehensive Computational Workflow for Pelvic Organ Prolapse Management: This figure illustrates an integrated, iterative framework for pelvic organ prolapse (POP) management, organized into five domains: Clinical Data Collection (blue), Tissue Properties (purple), Computational Methods (red), Clinical Application (green), and Validation & Feedback (orange/yellow). Patient-specific data—including clinical assessments (history, physical examination, and imaging) and, where applicable, multi-omic analyses—feed into computational modeling. Finite element analysis (FEA) integrates tissue properties derived from material testing, enabling biomechanical simulations and machine learning–based risk assessments. These outputs guide surgical decision-making by informing tailored treatment plans, such as mesh placement and suture techniques. The central feedback loop (highlighted in yellow) captures how clinical outcomes continually refine computational models and risk algorithms, while personalized surgical strategies influence execution and subsequent data collection. Through this cyclical process, models evolve toward more precise, individualized interventions, potentially reducing recurrence rates and aligning management strategies with each patient’s unique anatomical and functional characteristics. This workflow represents a transition from traditional, experience-based approaches to evidence-driven, computationally optimized POP management.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



