
Submitted:
23 March 2025
Posted:
24 March 2025
You are already at the latest version
Abstract
(1) Background: This study examines the relationship between hospital pharmacists' psychological contracts and their attitudes and behaviors in managing patient medication adherence. The goal is to provide a solid scientific foundation and practical recommendations for improving pharmacists' involvement in adherence management; (2) Methods: A Delphi evaluation, involving pharmacy experts from healthcare institutions, was conducted to refine the Pharmacists' Attitudes and Behaviors Toward Patient Medication Adherence Management Scale. This scale, alongside other relevant instruments, was used to survey pharmacists working in public healthcare institutions across two cities in Guizhou, China; (3) Results: The Attitudes Toward Patient Medication Adherence Management Scale exhibited strong reliability, with a Cronbach’s α coefficient of 0.796 and a KMO value of 0.899. The Behaviors Toward Patient Medication Adherence Management Scale demonstrated even higher reliability, with a Cronbach’s α of 0.986 and a KMO value of 0.963. A significant positive correlation was found between pharmacists' psychological contracts and their attitudes and behaviors toward patient medication adherence management (P < 0.01). Additionally, job burnout was identified as a partial mediator, accounting for 23.41% of the total effect; Targeted interventions to strengthen psychological contracts should be implemented to improve pharmacists' motivation and performance, ultimately boosting patient safety and treatment outcomes. (4) Conclusions: The fulfillment of pharmacists' psychological contracts plays a key role in enhancing their involvement in medication adherence management. Targeted interventions to strengthen these psychological contracts should be implemented to improve pharmacists' motivation and performance, ultimately boosting patient safety and treatment outcomes.
Keywords:
Hospital pharmacists
; Psychological contract
; Medication adherence management
; Attitudes and behaviors
; Job burnout
1. Introduction
Medication adherence remains a critical issue in healthcare, with non-adherence persisting as a widespread and enduring challenge(Osterberg, et al., 2005). The World Health Organization (WHO) estimates that 25% to 50% of patients worldwide fail to follow prescribed medication regimens. In the United States, inadequate adherence is responsible for around 125,000 deaths annually—equivalent to the combined mortality from colorectal, breast, and prostate cancers(Baryakova, et al., 2023). Poor adherence undermines treatment efficacy, leading to incomplete therapy, disease progression, and, in some cases, death. A study on patients with chronic obstructive pulmonary disease (COPD) found that poor adherence worsened symptoms, increased hospitalization and mortality, and raised healthcare costs(Ammous, et al., 2024). As healthcare models evolve and patient needs grow more complex, the role of pharmacists in enhancing medication adherence and ensuring patient safety has become increasingly important(Chisholm-Burns, et al., 2010; Glover, et al., 2024; Wu, et al., 2023).
The concept of the psychological contract refers to an employee's perception of mutual obligations between themselves and their organization, first introduced by Argyris in the 1960s(Rousseau, 1990). This implicit agreement significantly influences employee engagement(Rodwell, et al., 2022), and research highlights that fulfilling the psychological contract enhances motivation(Yu, 2022). Previous studies have shown that pharmacists’ psychological contracts positively impact their attitudes and behaviors in providing pharmaceutical services(Zhang, 2019). However, unmet organizational commitments can breach the psychological contract, leading to reduced job satisfaction, diminished motivation, and increased turnover intentions. Research on physicians shows that such breaches elicit strong negative emotions, resulting in undesirable behaviors(Hu, et al., 2023; Collins, et al., 2020). To enhance employee motivation and loyalty, organizations must prioritize psychological contracts alongside economic agreements, thereby improving healthcare quality(Yu, et al., 2020). Understanding pharmacists' psychological contracts is essential to fostering engagement, improving medication adherence, and ultimately enhancing patient care quality.
In our previous research, we developed and validated a psychological contract scale for hospital pharmacists based on data from 77 public medical institutions in Zunyi, China(Zhang, et al., 2020). This scale was proven reliable and valid, providing a robust tool for future studies. The current study aims to explore the relationship between hospital pharmacists' psychological contracts and their attitudes and behaviors toward patient medication adherence. By identifying the psychological contract factors influencing pharmacists' involvement in adherence management, this research aims to offer insights for improving their participation and ultimately enhancing patient adherence and health outcomes.
2. Materials and Methods
2.1. Scale Development
A comprehensive literature search was conducted using the keywords "Medication Adherence," "Pharmacist," "Research Progress," "Psychological Contract," and "Management" in both Chinese and English. Several databases were queried, including CNKI, Wanfang, VIP, PubMed, and Web of Science. The retrieved literature was systematically reviewed and synthesized. Based on expert consultations, a preliminary draft of the "Pharmacist's Attitudes and Behaviors Toward Patient Medication Adherence Management" scale was developed. This scale comprises two subscales: "Pharmacist's Attitudes Toward Patient Medication Adherence Management" (8 items) and "Pharmacist's Behaviors Toward Patient Medication Adherence Management" (25 items).
2.2. Delphi Expert Consultation
A Delphi consultation questionnaire was designed based on the initial scale, consisting of three sections: (1) Introduction (study background, purpose, and significance), (2) Main questionnaire (item content details), and (3) Expert demographic survey (expert information, item familiarity, and judgment criteria).
Sixteen experts were selected for the Delphi process, with inclusion criteria: (1) pharmacists in healthcare institutions, (2) associate senior title or higher, (3) bachelor's degree or above, (4) at least 5 years of experience, and (5) informed consent to participate. Exclusion criteria included external trainers.
2.3. Expert Evaluation and Data Analysis
Expert characteristics were summarized using frequencies and percentages. Expert engagement and authority were assessed through the response rate and expert authority coefficient (Cr), calculated as follows:
A Cr value ≥ 0.7 indicates good reliability. Here, Cs represents the expert's familiarity with the questionnaire (ranging from "very familiar" (0.9) to "very unfamiliar" (0.1))(Dai, et al., 2019), and Ca refers to the expert's judgment basis, which is classified into practical experience, theoretical analysis, relevant literature, and personal intuition, with corresponding values assigned as shown in Table 1 (Hu, et al., 2019).
The concentration of expert opinions was assessed using the importance score and the percentage of maximum scores. Importance was rated on a 5-point Likert scale (1 = very unimportant to 5 = very important). Consistency among expert opinions was evaluated through the coefficient of variation (CV) and Kendall’s coefficient of concordance (W). Specifically: CV < 0.3 indicates high coordination; W with P < 0.05 indicates significant agreement(de Goumoëns, et al., 2025).
Items were retained if the average importance score was ≥ 3.5 and the CV was < 0.3(Robinson, et al., 2014; Wells, et al., 2014). Expert opinions were also used to determine whether each item should be retained in the final version.
2.4. Participant Recruitment
A stratified random cluster sampling method was used to select participants from tertiary, secondary, and primary healthcare institutions in Zunyi and Bijie cities, China. Pharmacists were invited to anonymously complete a survey, which included demographic information and measures related to the "Hospital Pharmacist Psychological Contract," "Pharmacist Involvement in Patient Medication Adherence Management Attitudes and Behaviors," and "Job Burnout." Inclusion criteria included: (1) a background in pharmacy, (2) current employment as a pharmacist, and (3) voluntary participation. Trainee pharmacists were excluded from the study.
2.5. Reliability and Validity Testing
Reliability was assessed using Cronbach's α coefficient, where values between 0.5 and 0.7 indicate acceptable reliability, values above 0.7 indicate high reliability, and values above 0.9 indicate excellent reliability(Teo, et al., 2025).
Validity was assessed using exploratory factor analysis (EFA). The Kaiser-Meyer-Olkin (KMO) test and Bartlett's test of sphericity were conducted. A KMO value > 0.7 indicates suitability for factor analysis, while a significant P-value (P < 0.05) from Bartlett’s test confirms data appropriateness for analysis(Wu, 2014).
2.6. Statistical Analysis
Data were entered into Excel and analyzed using SPSS 29.0. A P-value < 0.05 was considered statistically significant, with all tests being two-tailed. Demographic data were presented as frequencies and percentages, and scale scores as mean ± standard deviation. For binary and multi-category data, independent sample t-tests, one-way ANOVA, and Kruskal-Wallis H tests were used, with LSD and Games-Howell post hoc tests for multiple comparisons. Spearman’s correlation analysis was used to assess relationships between pharmacists’ psychological contract, job burnout, and their attitudes and behaviors toward medication adherence management. Multiple linear regression was used to identify factors influencing pharmacists' participation in medication adherence management.
3. Results
3.1. Expert Panel
3.1.1. Expert Demographics
All 16 experts in the Delphi consultation held at least a bachelor's degree, with 25% holding doctoral degrees. All experts held professional titles of associate senior or higher, and 44% had over 20 years of work experience (Table 2).
3.1.2. Expert Correlation Coefficients
As shown in Table 3, all 16 consultation questionnaires were returned, resulting in a 100% response rate. The expert authority coefficient was 0.83, indicating high expertise and reliable consultation results. The coefficient of variation for each item ranged from 0.08 to 0.60, and Kendall's coefficient of concordance was 0.198, which was statistically significant (P < 0.01).
3.2. Delphi Results
After the Delphi consultation, one item was removed from the attitude scale, and two items were modified. For the behavior scale, two items were removed, and 14 items were revised, with three new items added. The highest mean score was 4.81, and the lowest was 2.75. The highest frequency of full scores was 81.25%, and the lowest was 12.50%. The coefficient of variation ranged from 0.08 to 0.60. Detailed modifications are shown in Table 4.
A total of 196 questionnaires were distributed, with 183 returned, 180 of which were valid, yielding an effective response rate of 98.36%. The demographic information of the pharmacists is shown in Table 5.
Reliability and validity analysis indicated that the Cronbach's α coefficients for the scales on pharmacists' attitudes and behaviors toward medication adherence management, as well as for the overall questionnaire, were all greater than 0.7. The KMO values were above 0.8 (P < 0.01), as shown in Table 6 and Table 7.
3.4. Statistical Analysis Results
3.4.1. Analysis of Pharmacists' Demographic Data on Psychological Contract, Job Burnout, and Attitudes and Behaviors Toward Patient Medication Adherence Management
Significant differences in behavior scores were observed between male and female pharmacists (P < 0.05). While no overall differences were found in job burnout scores across age groups, post-hoc analysis revealed that pharmacists aged 40-49 had higher job burnout levels compared to those aged 50-59 (P < 0.05). Income level differences were noted in both psychological contract and behavior scores (P < 0.05). Detailed results are presented in Table 8.
3.4.2. Correlation Between Pharmacists' Psychological Contract, Job Burnout, and Attitudes and Behaviors Toward Patient Medication Adherence Management
Spearman’s correlation analysis was conducted to examine the relationships between pharmacists' psychological contract, job burnout, and their attitudes and behaviors toward medication adherence management. Results are displayed in Table 9.
3.4.3. Regression Analysis of Pharmacists' Attitudes and Behaviors Toward Patient Medication Adherence Management
Multiple linear regression analysis, using psychological contract and job burnout as independent variables, and attitudes and behaviors as dependent variables, revealed that both psychological contract and job burnout significantly predicted pharmacists' attitudes toward medication adherence management. Specifically, the regression coefficient for psychological contract was 0.147 (P < 0.05), and for job burnout, it was -0.140 (P < 0.01). For behaviors, psychological contract significantly predicted pharmacist involvement, with a regression coefficient of 0.489 (P < 0.01). See Table 10.
3.4.4. Mediating Effect of Job Burnout
A mediation model using psychological contract as the independent variable, job burnout as the mediator, and attitudes/behaviors as the dependent variables was tested with SPSS Process 4.1, as shown in Table 11. Results showed that psychological contract negatively affected job burnout (β = -0.2554, P < 0.01) and positively affected attitudes (β = 0.1824, P < 0.05). Job burnout negatively influenced attitudes (β = -0.2181, P < 0.01), and psychological contract positively impacted behaviors (β = 0.2955, P < 0.01).
Further testing of the mediating effect using the non-parametric percentile Bootstrap method (Table 13) indicated that in the attitude model, the indirect effect’s 95% CI did not include 0, suggesting job burnout partially mediated the relationship between pharmacists' psychological contract and attitudes toward medication adherence management (effect size = 0.0448). However, in the behavior model, the CI included 0, indicating job burnout did not mediate the relationship between psychological contract and behavior. The specific pathways are illustrated in Figure 1 and Figure 2.

Table 12.
Table of Decomposition of Total Effect, Direct Effect, and Mediated Effect.
| Model | Type of effect | Effect | standard error | t/Z | P | Boot CI Upper Limit | Boot CI lower limit | Proportion of effect |
|---|---|---|---|---|---|---|---|---|
| Attitudes | Total | 0.1914 | 0.0585 | 3.2713 | 0.0013 | 0.0759 | 0.3068 | 100.00% |
| Direct | 0.1466 | 0.0592 | 2.4753 | 0.0143 | 0.0297 | 0.2635 | 76.59% | |
| Professional burnout | 0.0448 | 0.0203 | 0.0113 | 0.0899 | 23.51% | |||
| Behaviors | Total | 0.4858 | 0.1185 | 4.0992 | 0.0001 | 0.2519 | 0.7197 | 100.00% |
| Direct | 0.4888 | 0.1229 | 3.9769 | 0.0001 | 0.2463 | 0.7314 | 100.62% | |
| Professional burnout | -0.0003 | 0.0381 | -0.0823 | 0.0724 | -0.62% |
4. Discussion
Patient medication adherence is a critical factor in the effectiveness of clinical drug therapy. However, adherence is influenced by a complex interplay of multiple factors, including the patient's age, cognitive ability, psychological state, and economic status(Dawson, 2019). In addition to patient-related factors, pharmacists play a pivotal role in the medication process. Their professional guidance and communication skills are key to improving medication adherence(Ahn, et al., 2024). Pharmacists' work attitudes and behaviors are significantly influenced by their perceptions of the psychological contract with their healthcare institutions.
This study highlights the relationship between pharmacists' psychological contracts and their attitudes and behaviors in medication adherence management. These findings align with our previous research on the connection between pharmacists' psychological contracts and their attitudes and behaviors in pharmacy services(Zhang, 2019). Specifically, when pharmacists perceive a higher level of psychological contract fulfillment, they demonstrate more positive and proactive attitudes and behaviors toward managing patient medication adherence. In turn, this commitment enhances their relationship with the hospital, fosters patient trust, and promotes better treatment outcomes, all of which contribute to a stronger doctor-patient relationship(Listed N A., 2005). Research has shown that pharmacists who improve their service attitudes can strengthen patient trust, which subsequently boosts medication adherence(de Oliveira, et al., 2006). Pharmacists with a strong psychological contract perceive medication adherence management as an essential component of their professional role, leading to increased engagement in this task(Feng, et al., 2023).
Pharmacists with a robust sense of psychological contract recognize the importance of adherence management in improving treatment outcomes, reducing healthcare costs, and enhancing patients' quality of life. As a result, they are actively involved in this area. However, when the psychological contract is breached, pharmacists may feel disillusioned, leading to a decline in their motivation to manage medication adherence. This lack of motivation can result in diminished work quality, causing patients to question the efficacy and safety of their treatment regimens, which may, in turn, reduce medication adherence. Thus, fulfilling the psychological contract between healthcare institutions and pharmacists is crucial for encouraging their active participation in medication adherence management. Healthcare organizations should prioritize fulfilling these contracts by improving communication, ensuring fair workload distribution, and offering career development support to enhance pharmacists' perception of their psychological contract. This approach will foster pharmacists' enthusiasm and initiative in managing medication adherence, ultimately improving patient adherence and strengthening the doctor-patient relationship.
Additionally, this study incorporated burnout as a mediating variable in the relationship between the psychological contract and participation in medication adherence management. Pharmacist burnout significantly mediated this relationship and was negatively associated with both the psychological contract and attitudes toward adherence management. The psychological contract represents an implicit agreement between pharmacists and healthcare organizations. When pharmacists feel their psychological contract is fulfilled, they experience a sense of value and significance in their work, which leads to higher job satisfaction and reduced burnout(Sui, et al., 2023). Conversely, a low perception of the psychological contract—characterized by feelings of neglect, unappreciation, or an imbalance between effort and reward—can lead to burnout. This, in turn, negatively affects their attitude toward participating in medication adherence management, compromising work performance and the quality of medication adherence support provided to patients(Mu, et al., 2020).
High levels of burnout can cause pharmacists to lose enthusiasm and motivation, diminishing their attention to medication adherence management. They may become less proactive in communicating with patients or providing necessary medication guidance and follow-up. For example, they may adopt a perfunctory attitude, offering brief and impatient responses to patients' inquiries. Emotional distress may also impair their communication with patients, reducing trust and, consequently, medication adherence(Gu, et al., 2023). Therefore, hospitals and policymakers must prioritize addressing pharmacist burnout. This can be achieved by enhancing pharmacists' perceptions of their psychological contract through respect, support, and professional development opportunities, as well as optimizing the work environment to reduce negative factors contributing to burnout. This will prevent a decline in work quality and improve medication adherence management.
This study aims to explore the psychological factors influencing pharmacists' participation in medication adherence management and examine the mediating role of burnout. It provides empirical insights into the psychological mechanisms underlying pharmacists' involvement in medication adherence management, offering theoretical support and practical guidance for healthcare organizations to develop more targeted management strategies. Based on these findings, the following recommendations are made to optimize pharmacists' motivation in medication adherence management and improve patient adherence: (1) Enhance the fulfillment of pharmacists' psychological contracts, such as strengthening trust between pharmacists and healthcare institutions, and improving communication between hospital management and pharmacists. Enhance the Fulfillment of Pharmacists' Psychological Contracts: Strengthen trust between pharmacists and healthcare institutions, improve communication between hospital management and pharmacists, and ensure psychological contract fulfillment. (2) Reduce burnout by improving working conditions, providing career development opportunities, and prioritizing pharmacists' psychological well-being. Reduce Burnout: Improve working conditions, offer career development opportunities, and prioritize pharmacists' psychological well-being to reduce burnout and enhance job satisfaction. (3) Boost pharmacists' motivation to participate in medication adherence management, e.g., fostering a sense of responsibility through training, establishing incentive mechanisms (e.g., incorporating participation in medication adherence management into performance evaluations and offering appropriate rewards), and promoting teamwork (e.g., enhancing collaboration between pharmacists and other healthcare professionals to provide comprehensive medication management services and improve adherence management outcomes). Boost Pharmacists' Motivation: Foster a sense of responsibility through training, establish incentive mechanisms (e.g., incorporating medication adherence management into performance evaluations and offering appropriate rewards), and promote teamwork (e.g., enhancing collaboration between pharmacists and other healthcare professionals to provide comprehensive medication management and improve adherence outcomes).
5. Limitations
This study has several limitations that warrant further investigation. First, only one round of the Delphi survey was conducted with a limited number of experts, which may impact the depth and comprehensiveness of the findings. Future research should involve multiple rounds of the Delphi survey and expand the expert panel to incorporate a broader range of perspectives, thereby enhancing the diversity and representativeness of the results. Second, the study focused exclusively on pharmacists in hospitals in Zunyi and Bijie, Guizhou Province, China, limiting the geographic scope of the research. Expanding the study to include regions with varying levels of economic and healthcare resources would improve the generalizability of the findings. Third, while this study explored burnout as a mediating variable in the relationship between pharmacists' psychological contracts and their involvement in medication adherence management, it may not fully capture the underlying mechanisms of pharmacists' behaviors. Future research should incorporate additional variables, such as professional responsibility and identity, to develop a more comprehensive theoretical model and enhance the explanatory power of the relationship between pharmacists' psychological contracts and engagement in medication adherence management. Lastly, this study primarily relied on quantitative surveys, which may not fully capture the complex experiences and psychological factors influencing pharmacists in real-world settings. Future research should integrate qualitative methods, such as in-depth interviews and case studies, with quantitative data to provide a more comprehensive analysis of the challenges faced by hospital pharmacists, offering deeper insights to inform decision-making.
6. Conclusions
The fulfillment of pharmacists' psychological contracts significantly influences their engagement in medication adherence management, with job burnout acting as a mediating factor. Furthermore, the psychological contract is a key determinant of pharmacist burnout. Effective management of pharmacists' psychological contracts is thus crucial for enhancing motivation, reducing burnout, improving patient adherence, and optimizing medication safety and treatment outcomes. The findings of this study offer an empirical foundation for understanding the factors that shape pharmacists' attitudes and behaviors in medication adherence management. They also provide theoretical support and practical guidance for healthcare organizations in developing strategies to manage pharmacists' psychological contracts. However, future studies should broaden the scope by exploring additional mediating variables, such as professional responsibility and identity, and investigating different types of pharmacists (e.g., community pharmacists, clinical pharmacists) and patient populations (e.g., chronically ill or elderly patients) to examine potential variations in the psychological contract's role across diverse groups. Moreover, integrating qualitative research alongside quantitative methods could offer a more nuanced understanding of the psychological factors that influence pharmacists' workplace behaviors, thus enriching our understanding of the dynamic relationship between psychological contracts and medication adherence management.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization: FT; Methodology: YL and MN; Validation: YH and JT; Formal Analysis: YL, TZ, and XJ; Investigation: YL, MN and CC; Data Curation: YG and YL; Writing—Original Draft Preparation: YL; Writing—Review and Editing: FT and JT; Visualization: FT; Project Administration: FT. All authors have read and approved the final manuscript.
Funding
This study was supported by the Special Funds for Science and Technology Cooperation in Guizhou Province and Zunyi City (Shengshikehe 2015] 53) and the Graduate Student Research Fund of Zunyi Medical University (ZYK233).
Ethical Approval
This study adheres to the Declaration of Helsinki and was approved by the Ethics Committee of Zunyi Medical University (ZMCER [2023] 1-008). All participants were fully informed of the study's purpose, and their participation was voluntary and anonymous, as detailed in the pre-questionnaire letter and survey explanation.
Informed Consent Statement
Verbal informed consent was obtained from all participants in this study.
Data Availability Statement
The datasets used and analyzed in this study can be obtained from the corresponding author upon reasonable request.
Acknowledgments
We thank all the pharmacists who actively participated in this study.
Conflicts of Interest
The authors declare no potential conflicts of interest concerning the research, authorship and/or publication of this article.
Abbreviations
The following abbreviations are used in this manuscript:
| Cr | Authority Coefficient |
| Cs | Coefficient of Familiarity |
| Ca | Coefficient of Judgment Basis |
| CV | Coefficient of Variation |
| KMO | Kaiser-Meyer-Olkin |
References
- Osterberg, L.; Blaschke, T. Adherence to medication. The New England journal of medicine 2005, 353(5), 487–97. [Google Scholar] [CrossRef] [PubMed]
- Baryakova, T. H.; Pogostin, B. H.; Langer, R.; McHugh, K. J., Overcoming barriers to patient adherence: the case for developing innovative drug delivery systems. Nature reviews. Drug discovery 2023, 22 (5), 387-409. [CrossRef]
- Ammous, O.; Kampo, R.; Wollsching-Strobel, M.; Zimmermann, M.; Andreas, S.; Friede, T.; Kroppen, D.; Stanzel, S.; Salem, S.; Windisch, W.; Mathes, T., Adherence-enhancing interventions for pharmacological and oxygen therapy in patients with COPD: a systematic review and component network meta-analyses. European respiratory review: an official journal of the European Respiratory Society 2024, 33 (173). [CrossRef]
- Chisholm-Burns, M. A.; Kim Lee, J.; Spivey, C. A.; Slack, M.; Herrier, R. N.; Hall-Lipsy, E.; Graff Zivin, J.; Abraham, I.; Palmer, J.; Martin, J. R.; Kramer, S. S.; Wunz, T., US pharmacists' effect as team members on patient care: systematic review and meta-analyses. Medical care 2010, 48 (10), 923-33. Medical care. [CrossRef]
- Glover, L. H.; Skelley, J. W.; Cimino, L. H.; Berry, R. B., Impact of a pharmacist-driven COPD clinic on outcomes related to COPD in a federally qualified health center. J Am Pharm Assoc (2003) 2024, 64 (2), 512-516. [CrossRef]
- Wu, M.; Xu, X.; Zhao, R.; Bai, X.; Zhu, B.; Zhao, Z., Effect of Pharmacist-Led Interventions on Medication Adherence and Glycemic Control in Type 2 Diabetic Patients: A Study from the Chinese Population. Patient Prefer Adherence 2023, 17, 119-129. [CrossRef]
- Rousseau, D. M., New hire perceptions of their own and their employer’s obligations: A study of psychological contracts. Journal of Organizational Behavior 1990, 11 (5), 389-400. [CrossRef]
- Rodwell, J.; Johnson, D. The state of the psychological contract, justice and engagement drive nurses' performance behaviors. International journal of environmental research and public health, 2022; 19, 20. [Google Scholar] [CrossRef]
- Yu, J., Impacts of psychological contract fulfillment on work attitudes and behaviors during the COVID-19 pandemic: Mediating role of perceived organizational support. Curr Psychol 2022, 1-10. [CrossRef]
- Zhang, T. A study on the relationship between psychological contract of pharmacists in medical institutions and attitudes and behaviors of pharmaceutical services: a case study of Zunyi City [master's thesis]. Guizhou Province: Zunyi Medical University. (2019).
- Hu, L.; Chen, C.; Zhu, J.; Zhang, Y.; Chen, Y.; Jia, Y., Relationship Between Psychological Contract Violation and Physicians' Destructive and Constructive Behaviors in Tertiary Public Hospitals: An Empirical Evidence in Beijing. J Multidiscip Healthc 2023, 16, 997-1010. [CrossRef]
- Collins, A.; Beauregard, A., The effect of breaches of the psychological contract on the job satisfaction and wellbeing of doctors in Ireland: A quantitative study. Hum Resour Health 2020, 18 (1), 89. [CrossRef]
- Yu, Y.; Chen, Z.; Zhao, Y.; Wang, Y.; Zhang, R.; Zhou, X., Medical service quality, psychological contract, and patient loyalty: An empirical study among patients in China. Medicine 2020, 99 (48), e21079. [CrossRef]
- Zhang, T.; Yin, C.; Geng, Y.; Zhou, Y.; Sun, S.; Tang, F., Development and validation of psychological contract scale for hospital pharmacists. J Multidiscip Healthc 2020, 13, 1433-1442. [CrossRef]
- Dai, F.; Wei, K.; Chen, Y.; Ju, M., Construction of an index system for qualitative evaluation of undergraduate nursing students innovative ability: A Delphi study. J Clin Nurs 2019, 28 (23-24), 4379-4388. [CrossRef]
- Hu, Q.; Qin, Z.; Zhan, M.; Wu, B.; Chen, Z.; Xu, T., Development of a trigger tool for the detection of adverse drug events in Chinese geriatric inpatients using the Delphi method. Int J Clin Pharm 2019, 41 (5), 1174-1183. [CrossRef]
- de Goumoëns, V.; Lefrançois, L. E.; Forestier, A.; Grandjean, C.; Balice-Bourgois, C.; Quillet-Cotting, J.; Thévoz, A. L.; Ramelet, A. S., Bachelor nursing competencies to care for children in hospital and home settings: A Delphi study. Nurse education today 2025, 145, 106487. [CrossRef]
- Robinson, K. R.; Leighton, P.; Logan, P.; Gordon, A. L.; Anthony, K.; Harwood, R. H.; Gladman, J. R.; Masud, T., Developing the principles of chair based exercise for older people: a modified Delphi study. BMC geriatrics 2014, 14, 65. [CrossRef]
- Wells, C.; Kolt, G. S.; Marshall, P.; Bialocerkowski, A., The definition and application of Pilates exercise to treat people with chronic low back pain: a Delphi survey of Australian physical therapists. Physical therapy 2014, 94 (6), 792-805. [CrossRef]
- Teo, V.; Weinman, J.; Yap, K. Z., A cultural adaptation and validation study of the Intentional Nonadherence Scale (INAS) among people with type 2 diabetes in Singapore. Journal of psychosomatic research 2025, 188, 111969. [CrossRef]
- Wu, S. F., Rapid screening of psychological well-being of patients with chronic illness: Reliability and validity test on WHO-5 and PHQ-9 scales. Depression Research and Treatment 2014, 2014, 239490. [CrossRef]
- Dawson, L. A., What factors affect adherence to medicines? Archives of disease in childhood. Education and practice edition 2019, 104 (1), 49-52. [CrossRef]
- Ahn, H.; Byun, B. K.; Lee, T. H.; Kang, D. W.; Park, S. K., Effects of pharmacist-led home visit services and factors influencing medication adherence improvement. PloS one 2024, 19 (11), e0314204. [CrossRef]
- Listed, N.A. Adherence strategies. Improve bedside manner, affect patient adherence. Communication makes a difference. AIDS Alert 2005, 20, 57–59. [Google Scholar]
- de Oliveira, D. R.; Shoemaker, S. J., Achieving patient centeredness in pharmacy practice: openness and the pharmacist's natural attitude. J Am Pharm Assoc (2003) 2006, 46 (1), 56-64; quiz 64-6. [CrossRef]
- Feng, Y.; Zhang, Z.; Zeng, X.; Liu, Y., The influence of internship satisfaction and the psychological contract on the career identity behavior of fresh graduates. Front Psychol 2023, 14, 1294799. [CrossRef]
- Sui, M.; Yu, Z.; Zhou, M., The impact of psychological contract, physical and mental health on burnout in grassroots civil servants: Evidence from China. Psychology research and behavior management 2023, 16, 3461-3476. [CrossRef]
- Mu, X.; Yin, C.; He, X.; Li, H.; Gong, Y.; Wei, W.; Zhang, Y.; Tang, F., Correlation between patients' medication adherence and their psychological contract with hospital pharmacists. Patient Prefer Adherence 2020, 14, 1605-1613. [CrossRef]
- Gu, Y.; Mu, X.; Zhang, Y.; Tang, Y.; Zhang, T.; Tang, F., The Effect of Patients' Psychological Contract with Pharmacists on Medication Adherence: A Qualitative Study. Patient Prefer Adherence 2023, 17, 547-555. [CrossRef]
Figure 1.
The Mediating Model of Pharmacist Burnout Between Psychological Contract and Attitude Toward Patient Medication Adherence Management. *P<0.05; **P<0.01
Figure 1.
The Mediating Model of Pharmacist Burnout Between Psychological Contract and Attitude Toward Patient Medication Adherence Management. *P<0.05; **P<0.01
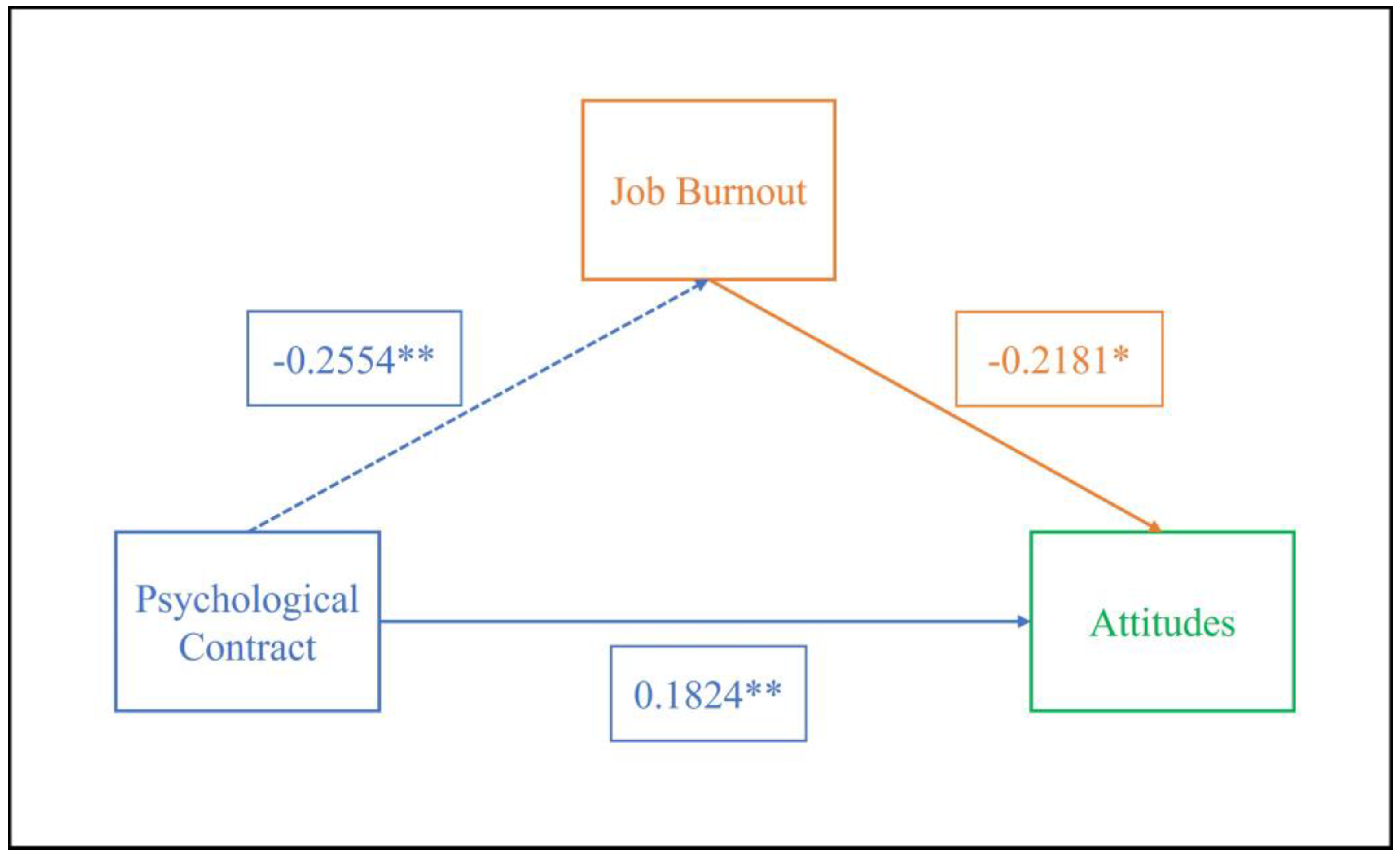
Figure 2.
The Mediating Model of Pharmacist Burnout Between Psychological Contract and Behavior Toward Patient Medication Adherence Management. **P<0.01.
Figure 2.
The Mediating Model of Pharmacist Burnout Between Psychological Contract and Behavior Toward Patient Medication Adherence Management. **P<0.01.
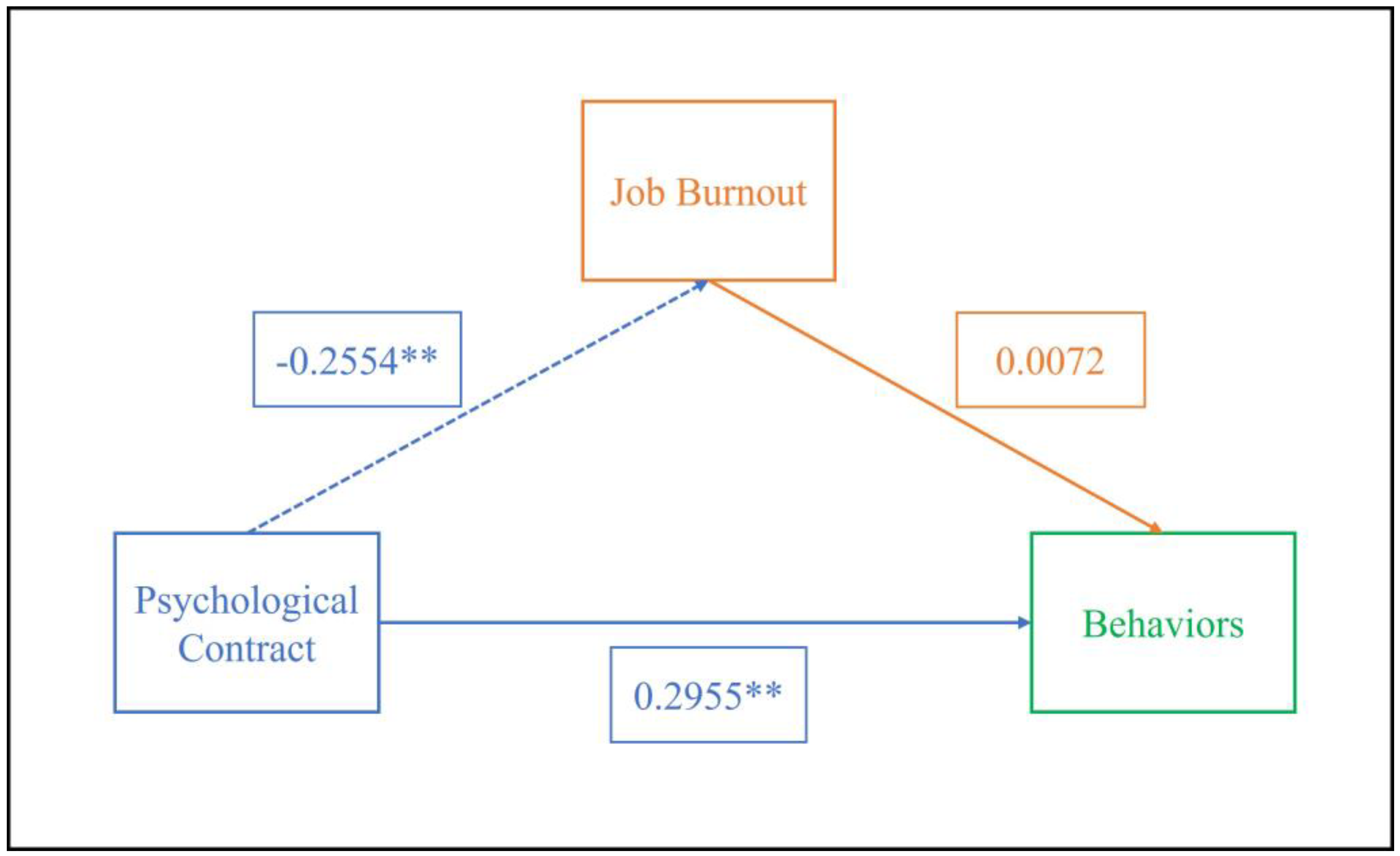
Table 1.
Expert Judgment Basis Quantification Table.
| The basis for expert review | Expert Scoring Judgment Coefficient | ||
|---|---|---|---|
| large | middle | little | |
| Practical experience | 0.5 | 0.4 | 0.3 |
| Theoretical analysis | 0.3 | 0.2 | 0.1 |
| Relevant literature | 0.1 | 0.1 | 0.1 |
| Personal intuition | 0.1 | 0.1 | 0..1 |
Table 2.
Demographic Characteristics of Delphi Experts.
| Group | Basic Information | Number | Percentage |
|---|---|---|---|
| Gender | Male | 7 | 44% |
| Female | 9 | 56% | |
| Age | 30-39 | 5 | 31% |
| 40-49 | 7 | 44% | |
| 50-59 | 3 | 19% | |
| 60 and above | 1 | 6% | |
| Years of Experience | Less than 10 years | 0 | 0% |
| 10-20 years | 9 | 56% | |
| More than 20 years | 7 | 44% | |
| Education | Doctorate | 4 | 25% |
| Master's | 8 | 50% | |
| Bachelor's | 4 | 25% | |
| Professional Title | Senior Title | 9 | 56% |
| Associate Senior Title | 7 | 44% | |
| Research Field | Pharmacy | 1 | 6% |
| Clinical Pharmacy | 10 | 64% | |
| Hospital Pharmacy | 1 | 6% | |
| Pharmaceutical Management | 2 | 12.% | |
| Other | 2 | 12% | |
| Hospital Level | Grade III, Class A | 15 | 94% |
| Grade III, Class B | 1 | 6% |
Table 3.
Expert Activity Index, Authority Coefficient, and Opinion Coordination Level in the First Round of Consultation.
Table 3.
Expert Activity Index, Authority Coefficient, and Opinion Coordination Level in the First Round of Consultation.
| Indicator | First Round | |
|---|---|---|
| Expert Activity Index | Questionnaire Recovery Rate | 100% |
| Effective Recovery Rate | 100% | |
| Opinion Proposal Rate | 38.0% | |
| Expert Authority Coefficient | Cs | 0.70 |
| Ca | 0.90 | |
| Cr | 0.83 | |
| Expert Opinion Coordination Level | χ2 | 101.151 |
| CV | 0.08~0.60 | |
| W | 0.198** |
**P<0.01.
Table 4.
Expert Survey Results.
| Subscale | Key Indicators | Mean | Full Score Frequency | CV | Expert Comments |
|---|---|---|---|---|---|
| Pharmacist's attitude towards participating in patient medication adherence management | #1. Participating in patient medication adherence management is a requirement of pharmacists' professional ethics. | 4.63 | 62.50% | 0.10 | Modified to "professional ethics" to "responsibility" |
| 2. Participating in patient medication adherence management is not necessarily part of pharmacists' responsibilities. | 4.19 | 43.75% | 0.24 | ||
| #3. Pharmacists play a leading role in improving patient medication adherence. | 4.31 | 31.25% | 0.11 | Modified to "Pharmacists should play a leading role in patient medication adherence management." | |
| 4. Pharmacists' management of patient medication adherence plays a crucial role in treatment outcomes. | 4.38 | 43.75% | 0.14 | ||
| 5. Participating in medication adherence management is one way for pharmacists to achieve self-worth. | 4.56 | 68.75% | 0.15 | ||
| 6. Pharmacists should regularly assess patients' medication adherence. | 4.69 | 75.00% | 0.12 | ||
| 7. Pharmacists should regularly educate patients on medication adherence. | 4.81 | 81.25% | 0.08 | ||
| 8. Pharmacists should actively research and use various tools and methods to improve patient medication adherence. | 4.63 | 68.75% | 0.13 | ||
| *9. Whether patients adhere to medication is their own choice and is the responsibility of the patient or prescribing physician, not the pharmacist. | 2.75 | 25.00% | 0.60 | Delete, as it duplicates other items. | |
| The behaviors of pharmacists in participating in patient medication adherence management | 1. Establish patient health records, document medication information, and implement personalized adherence management. | 4.69 | 75.00% | 0.12 | |
| #2. Monitor patients' medication adherence through methods such as pill counting and blood drug concentration monitoring. | 4.44 | 50.00% | 0.14 | Modified to "Monitoring patient medication adherence through inquiry or monitoring methods (such as pill count, blood drug concentration monitoring, and clinical indicator testing, etc.)" | |
| #3. Assess the psychological and pathological factors in patients that may affect medication adherence. | 4.63 | 62.50% | 0.10 | Modified to “Assess psychological and pathophysiological factors (such as advanced age, memory decline, and decreased mobility) and social factors (such as previous treatment failures, medication accessibility, and financial burden related to medication use) that may affect the patient's medication adherence.” | |
| #4. Regularly inquire about objective factors that may affect patients' adherence to prescribed medications (such as side effects of the medication, financial burden related to medication use, complexity of the medication regimen, etc.). | 4.69 | 75.00% | 0.12 | Remove "financial burden related to medication use" | |
| #5. Verify the medication usage of patients with chronic diseases, especially the use of medication devices. | 4.56 | 56.35% | 0.11 | Modified to “Check the mastery of medication usage methods among patients with chronic diseases and implement necessary educational measures as needed.” | |
| 6. Assess the patient's medication adherence using compliance evaluation scales (such as MMAS, TAI, etc.) based on the patient's specific conditions. | 4.63 | 62.50% | 0.10 | ||
| #7. Conduct medication adherence education activities through patient education lectures and community outreach. | 4.50 | 56.25% | 0.14 | Modified to "Conduct medication adherence education activities through patient education lectures, community outreach, and playing medication education videos." | |
| #8. Correct the patient's misconception of stopping medication as soon as their condition shows slight improvement. | 4.75 | 75.00% | 0.09 | Modified to "correct the perception and behavior of patients discontinuing medication on their own, emphasizing the importance of regular medical visits and the dangers of arbitrarily stopping medication." | |
| #9. Implement standardized communication regarding medication therapy, covering the nature of the disease, medication options, treatment expectations, and more. | 4.50 | 56.25% | 0.14 | Modified to "Standardize communication regarding medication therapy, covering the nature of the disease, medication options, treatment expectations, safety, and cost-effectiveness." | |
| #10. Promote medication adherence-related communication among patients. | 3.75 | 31.25% | 0.35 | Modify to "Regularly organize group discussions among patients to exchange experiences on overcoming medication barriers and coping with drug side effects." | |
| 11. The pharmacist regularly communicates with the patient and their family members or caregivers to ensure that the patient is supervised in taking their medication according to the prescribed regimen. | 4.63 | 62.50% | 0.10 | ||
| #12. Collaborate with the medical team to provide feedback on patient adherence and offer recommendations for medication selection. | 4.69 | 68.75% | 0.10 | Change"offer recommendations for medication selection." to "provide recommendations for adjustments to drug treatment plans." | |
| 13. Provide patients with health consultations and guidance related to rational medication use, including diet, exercise, and stress management, and offer personalized professional services for special patient groups. | 4.38 | 43.75% | 0.14 | ||
| #14. During the patient consultation process, clarify and verify the medication instructions. | 4.44 | 56.25% | 0.16 | Modify to “During the medication guidance process, promptly correct any inappropriate medication behaviors of the patient, demonstrate the correct method, and ensure that they understand and master the proper way to take the medication.” | |
| *15. Make clear notes on the medications taken by patients who are forgetful or elderly. | 4.69 | 68.75% | 0.10 | Delete, as it duplicates other items. | |
| 16. Encourage patients to develop self-medication monitoring and cultivate awareness of self-adherence management. | 4.69 | 75.00% | 0.12 | ||
| 17. Using the Health Belief Model to enhance patients' perception of their susceptibility to illness and the severity of the disease. | 4.38 | 43.75% | 0.14 | ||
| 18. Plan, monitor, and evaluate the medication regimen, and establish a treatment plan that is tailored to the patient’s preferences. | 4.38 | 43.75% | 0.14 | ||
| #19. Use medication cards or instructional leaflets to remind and guide patients to take their medications correctly. | 4.38 | 43.75% | 0.14 | Modify to "Use drug cards or medication instruction leaflets to remind and guide patients to take their medications correctly, and make clear notes on the medications taken by forgetful or elderly patients." | |
| #20. Guide patients to use self-service medical devices (such as blood pressure monitors and glucometers) properly to promote adherence to prescribed medication regimens. | 4.31 | 31.25% | 0.11 | Modify to“Guide patients in the correct use of self-service medical devices (such as blood pressure monitors and glucometers) and instruct them on how to respond to abnormal monitoring results.” | |
| 21. Promote the use of smart pill boxes for patients who are eligible (features include real-time reminders and real-time synchronization of medication records, etc.). | 4.13 | 37.50% | 0.19 | ||
| #22. Patients are regularly reminded of medication use and drug replenishment through various communication means, including phone calls, text messages, pharmaceutical service platforms, QQ, WeChat, and others. | 4.38 | 56.25% | 0.18 | Modify to “Regularly remind patients of medication use, replenish medications, and provide professional answers to medication-related questions through communication means such as telephone, text messages, pharmaceutical service platforms, QQ, and WeChat.” | |
| *23. Research or use of artificial intelligence (AI) in managing patients' medication. | 3.69 | 12.50% | 0.25 | Delete, as it duplicates other items. | |
| #24. Keep abreast of the latest information and developments in first-line medications both domestically and internationally, and actively utilize new theories, knowledge, and technologies in the field of pharmaceutical and medical sciences to guide patients in the rational use of medications. | 4.50 | 56.25% | 0.14 | Modify to “Keep abreast of the latest information and development trends of first-line medications both domestically and internationally, and actively utilize new theories, knowledge, and technologies in the field of pharmaceutical medicine to guide rational medication use in clinical practice and for patients.” | |
| Add new entry:7. Verify the medication information of transferred patients, coordinate the medication plans, and ensure the continuity of medical care; 8. Regularly assess the patient's acceptance and implementation of personalized medication guidance or adherence reminders; 15. Based on the patient's feedback on drug efficacy or adverse reactions, promptly optimize medication guidance and intervention measures. | |||||
*indicates that the item was removed; #indicates that the item was modifie3.3. Reliability and Validity Testing.
Table 5.
Demographic Characteristics of Pharmacists Participating in the Survey.
| Basic situation | Pharmacist (%) | |
|---|---|---|
| Gender | Male | 69 (38.3%) |
| Female | 111 (61.7%) | |
| Age | 20-29 | 61 (33.9%) |
| 30-39 | 83 (46.1%) | |
| 40-49 | 21 (11.7%) | |
| 50-59 | 15 (8.3%) | |
| 60+ | 0 (0%) | |
| Marital Status | Single | 52 (28.9%) |
| Married | 127 (70.6%) | |
| Divorced/Widowed | 1 (0.5%) | |
| Highest Education | Diploma | 12 (6.7%) |
| Bachelor's | 119 (66.1%) | |
| Master's | 46 (25.6%) | |
| Doctorate | 3 (1.6%) | |
| Years of Work Experience | 1-5 | 67 (37.2%) |
| 6-10 | 39 (21.7%) | |
| 11-15 | 41 (22.8%) | |
| 16-20 | 10 (5.5%) | |
| 21-25 | 8 (4.4%) | |
| 26-30 | 2 (1.1%) | |
| 30+ | 13 (7.3%) | |
| Title | No Title | 23 (12.8%) |
| Junior Pharmacist | 6 (3.3%) | |
| Pharmacist | 57 (31.7%) | |
| Senior Pharmacist | 79 (43.9%) | |
| Deputy Chief Pharmacist | 14 (7.8%) | |
| Chief Pharmacist | 1 (0.5%) | |
| Employment Type | Full-Time | 92 (51.1%) |
| Contract | 68 (37.8%) | |
| Part-Time | 20 (11.1%) | |
| Position | Inpatient Pharmacist | 38 (21.1%) |
| Outpatient Pharmacist | 70 (38.9%) | |
| Intravenous Therapy Pharmacist | 4 (2.2%) | |
| Clinical Pharmacist | 35 (19.4%) | |
| Other | 33 (18.4%) | |
| Income Level | 0~2000 | 12 (6.7%) |
| 2000~4000 | 43 (23.9%) | |
| 4000~6000 | 72 (40.0%) | |
| 6000+ | 53 (29.4%) | |
| Hospital Level | Tertiary General Hospital | 135 (75.0%) |
| Tertiary specialized hospital | 27 (15.0%) | |
| Secondary General Hospital | 16 (8.9%) | |
| Secondary Specialist Hospital | 2 (1.1%) | |
| Primary General Hospital | 0 (0%) |
Table 6.
Reliability Test Statistics of the Scale for Pharmacists' Attitudes and Behaviors in Patient Medication Adherence Management.
Table 6.
Reliability Test Statistics of the Scale for Pharmacists' Attitudes and Behaviors in Patient Medication Adherence Management.
| Number of Items | Cronbach’s α | |
|---|---|---|
| Attitudes | 8 | 0.796 |
| Behaviors | 25 | 0.986 |
Table 7.
KMO Measure and Bartlett's Sphericity Test Results of the Pharmacist's Attitude and Behavior Scale for Participation in Patient Medication Adherence Management.
Table 7.
KMO Measure and Bartlett's Sphericity Test Results of the Pharmacist's Attitude and Behavior Scale for Participation in Patient Medication Adherence Management.
| Attitudes | Behaviors | ||
|---|---|---|---|
| KMO Sample Measure | 0.899 | 0.963 | |
| Bartlett's Test of Sphericity Significance | Approximate Chi-Square | 1002.900 | 6275.223 |
| Degree of freedom | 28 | 300 | |
| Significance probability | 0.000 | 0.000 | |
Table 8.
Analysis of the scores of pharmacists' psychological contract, job burnout, attitudes, and behaviors based on demographic data [M±SD].
Table 8.
Analysis of the scores of pharmacists' psychological contract, job burnout, attitudes, and behaviors based on demographic data [M±SD].
| Group | Psychological contract | Job burnout | Attitudes | Behaviors | |
|---|---|---|---|---|---|
| Gender | ①Male | 4.89±0.737 | 2.90±0.940 | 4.11±0.441 | 3.51±1.052 |
| ②Female | 4.79±0.632 | 2.85±0.782 | 4.06±0.598 | 3.12±1.132 | |
| F | 0.949 | 0.157 | 0.263 | 5.254 | |
| P | 0.331 | 0.693 | 0.609 | 0.023 | |
| Age | ①20-29 | 4.88±0.719 | 2.81±0.856 | 4.07±0.583 | 3.48±1.165 |
| ②30-39 | 4.80±0.667 | 2.88±0.838 | 4.11±0.517 | 3.11±1.078 | |
| ③40-49 | 4.71±0.654 | 3.19±0.915 | 3.91±0.573 | 3.43±0.947 | |
| ④50-59 | 4.99±0.566 | 2.62±0.645 | 4.20±0.448 | 3.05±1.256 | |
| F | 0.671 | 1.574 | 1.021 | 1.606 | |
| P | 0.571 | 0.197 | 0.385 | 0.190 | |
| LSD/G-H | —— | ③>④* | —— | —— | |
| Marital Status | ①Single | 4.76±0.712 | 2.76±0.886 | 4.04±0.550 | 3.37±1.119 |
| ②Married | 4.86±0.662 | 2.90±0.186 | 4.10±0.541 | 3.22±1.118 | |
| ③Divorced/Widowed | 5.00±0.000 | 4.55±0.000 | 3.75±0.000 | 4.00±0.000 | |
| F | 0.380 | 2.505 | 0.452 | 0.574 | |
| P | 0.684 | 0.085 | 0.637 | 0.564 | |
| Highest Education | ①Diploma | 5.18±0.423 | 2.71±0.798 | 3.94±0.499 | 3.46±1.214 |
| ②Bachelor's | 4.82±0.688 | 2.92±0.879 | 4.05±0.526 | 3.21±1.121 | |
| ③Master's | 4.77±0.758 | 2.78±0.789 | 4.19±0.593 | 3.33±1.106 | |
| ④Doctorate | 4.79±1.068 | 2.70±0.335 | 4.21±0.402 | 3.80±0.771 | |
| F | 1.249 | 0.504 | 1.096 | 0.493 | |
| P | 0.294 | 0.680 | 0.352 | 0.687 | |
| Years of Work Experience | ①1-5 | 4.85±0.716 | 2.79±0.788 | 4.05±0.541 | 3.33±1.150 |
| ②6-10 | 4.78±0.641 | 2.90±0.791 | 4.20±0.562 | 3.08±1.088 | |
| ③11-15 | 4.85±0.625 | 2.86±0.878 | 4.05±0.567 | 3.39±1.003 | |
| ④16-20 | 4.80±0.850 | 2.81±1.078 | 4.11±0.582 | 3.40±1.408 | |
| ⑤21-25 | 4.79±0.799 | 3.80±1.053 | 3.78±0.499 | 3.61±1.158 | |
| ⑥26-30 | 3.91±0.265 | 2.84±0.996 | 3.69±0.442 | 1.68±0.849 | |
| ⑦30+ | 5.00±0.510 | 2.71±0.645 | 4.20±0.352 | 3.01±1.279 | |
| F | 0.807 | 1.862 | 1.089 | 1.260 | |
| P | 0.565 | 0.090 | 0.371 | 0.279 | |
| Title | ①No Title | 5.07±0.638 | 2.67±0.783 | 4.20±0.529 | 3.42±1.155 |
| ②Junior Pharmacist | 5.10±0.709 | 2.42±0.789 | 4.04±0.557 | 3.19±1.198 | |
| ③Pharmacist | 4.91±0.685 | 2.83±0.948 | 4.11±0.523 | 3.43±1.226 | |
| ④Senior Pharmacist | 4.65±0.673 | 2.93±0.716 | 4.05±0.567 | 3.13±1.007 | |
| ⑤Deputy Chief Pharmacist | 4.98±0.503 | 3.25±1.074 | 3.96±0.532 | 3.10±1.187 | |
| ⑥Chief Pharmacist | 5.30±0.000 | 1.86±0.000 | 4.25±0.000 | 4.04±0.000 | |
| F | 2.304 | —— | 0.488 | 0.744 | |
| H | —— | 6.117 | —— | —— | |
| P | 0.047 | 0.289 | 0.785 | 0.592 | |
| ①Full-Time | 4.78±0.663 | 2.97±0.845 | 4.09±0.583 | 3.32±1.072 | |
| Employment Type | ②Contract | 4.92±0.655 | 2.74±0.880 | 4.09±0.520 | 3.23±1.206 |
| ③Part-Time | 4.78±0.788 | 2.83±0.671 | 4.01±0.422 | 3.12±1.019 | |
| F | 0.878 | 1.432 | 0.210 | 0.314 | |
| P | 0.417 | 0.242 | 0.811 | 0.731 | |
| Position | ①Inpatient Pharmacist | 5.00±0.711 | 2.68±0.981 | 4.15±0.480 | 3.34±1.230 |
| ②Outpatient Pharmacist | 4.80±0.626 | 2.97±0.838 | 3.98±0.547 | 3.19±1.177 | |
| ③Intravenous Therapy Pharmacist | 5.37±0.919 | 2.57±0.494 | 3.91±0.449 | 3.35±1.247 | |
| ④Clinical Pharmacist | 4.62±0.612 | 2.93±0.807 | 4.17±0.561 | 3.36±0.867 | |
| ⑤Other | 4.88±0.721 | 2.86±0.746 | 4.16±0.574 | 3.24±1.123 | |
| F | 0.172 | 0.456 | 0.330 | 0.939 | |
| P | 0.070 | 0.463 | 0.269 | 0.942 | |
| Income Level | ①0-2000 | 5.26±0.842 | 2.58±1.361 | 4.30±0.428 | 3.99±1.282 |
| ②2000-4000 | 4.82±0.778 | 2.87±0.884 | 4.00±0.616 | 3.64±1.018 | |
| ③4000-6000 | 4.74±0.625 | 2.89±0.657 | 4.07±0.520 | 3.06±1.089 | |
| ④6000+ | 4.87±0.581 | 2.91±0.904 | 4.10±0.528 | 3.08±1.071 | |
| F | 0.199 | 0.882 | 0.295 | 0.008 | |
| P | 0.090 | 0.660 | 0.394 | 0.003 | |
| LSD/G-H | —— | —— | —— | ②>③# ②>④# |
|
| Hospital Level | ①Tertiary General Hospital | 4.85±0.695 | 2.84±0.833 | 4.05±0.565 | 3.34±1.028 |
| ②Tertiary specialized hospital | 4.84±0.657 | 3.23±0.916 | 4.25±0.480 | 3.31±1.406 | |
| ③Secondary General Hospital | 4.65±0.564 | 2.58±0.688 | 4.06±0.421 | 2.64±1.196 | |
| ④Secondary Specialist Hospital | 5.11±0.053 | 2.52±0.675 | 3.75±0.000 | 2.60±0.566 | |
| F | 0.001 | 0.244 | —— | 0.225 | |
| P | 0.671 | 0.064 | 0.293 | 0.094 | |
| LSD/G-H | ①<④# ③<④# |
—— | ①>④# ②>④# ③>④# |
—— |
*LSD; #DunnettT.
Table 9.
Analysis of the Correlation between Pharmacists' Psychological Contract, Professional burnout, and Their Attitudes and Behaviors in Managing Patient Medication Adherence.
Table 9.
Analysis of the Correlation between Pharmacists' Psychological Contract, Professional burnout, and Their Attitudes and Behaviors in Managing Patient Medication Adherence.
| Project | Psychological Contract | Professional burnout | Attitudes | Behaviors |
|---|---|---|---|---|
| Psychological Contract | 1 | |||
| Professional burnout | -0.272** | 1 | ||
| Attitudes | 0.221** | -0.265** | 1 | |
| Behaviors | 0.297** | -0.088 | 0.271** | 1 |
**P<0.01.
Table 10.
The Regression Analysis of Psychological Contract, Professional burnout, and Attitudes and Behaviors.
Table 10.
The Regression Analysis of Psychological Contract, Professional burnout, and Attitudes and Behaviors.
| Model | Non-standardized coefficient | standardized coefficient | t | P | VIF | ||
|---|---|---|---|---|---|---|---|
| B | standard error | β | |||||
| Attitudes | constant | 3.774 | 0.349 | 10.820 | 0.000 | ||
| Psychological Contract | 0.147 | 0.059 | 0.182 | 2.475 | 0.014 | 1.070 | |
| Professional burnout | -0.140 | 0.047 | -0.218 | -2.959 | 0.004 | 1.070 | |
| R2FP | 0.101 9.961 0.000 |
||||||
| Behaviors | constant | 0.878 | 0.724 | 1.213 | 0.227 | ||
| Psychological Contract | 0.489 | 0.123 | 0.296 | 3.977 | 0.000 | 1.070 | |
| Professional burnout | 0.009 | 0.098 | 0.007 | 0.097 | 0.923 | 1.070 | |
| R2FP | 0.086 8.360 0.000 |
||||||
Table 11.
Regression analysis between variables.
| The regression equation | The overall fit index | The significance of regression coefficients | ||||
|---|---|---|---|---|---|---|
| result variable | Predictor | R | R2 | F | β | t |
| Professional burnout | Psychological Contract | 0.2554 | 0.0652 | 12.4204 | -0.2554 | -3.5243** |
| Attitudes | Psychological Contract | 0.3181 | 0.1012 | 9.9608 | 0.1824 | 2.4753* |
| Professional burnout | -0.2181 | -2.9588** | ||||
| Behaviors | Psychological Contract | 0.2938 | 0.0863 | 8.3597 | 0.2955 | 3.9769** |
| Professional burnout | 0.0072 | 0.0966 | ||||
*P<0.05; **P<0.01.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



