
Submitted:
25 March 2025
Posted:
26 March 2025
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Since the emergence of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) in December 2019, Long COVID (LC) has become a significant global health burden. While knowledge on LC is accumulating, studies on its prevention are still lacking. We conducted a systematic review following PRISMA (Preferred Reporting Items for Systematic Reviews and Me-ta-Analyses) guidelines to investigate prevention options for LC. We identified fifteen articles on vaccines, seven on antivirals, and six on other interventions, after searching for articles in the PubMed/MEDLINE database using the MeSH terms. Most vaccine-related studies demonstrated a protective effect of COVID-19 vaccines against developing LC. COVID-19 vaccination is vital, as it not only prevents COVID-19 but also reduces severity of illness and may help prevent LC. Our review found an equivocal effect of antivirals while metformin had a protective effect in outpatients and corticosteroids in hospitalized patients against LC. Conversely, COVID-19 convalescent plasma and multiple micronutrient supplement, did not confer any protection against LC. Further studies are warranted to shed light on these topics.
Keywords:
Long COVID
; Post-Acute Sequelae of COVID-19 (PASC)
; Post-Acute COVID Syndrome (PACS)
; Post-COVID Conditions (PCC)
; COVID-19
; prevention
1. Introduction
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the causative agent of COVID-19, was first identified in December 2019 in the city of Wuhan, China. COVID-19 rapidly spread worldwide, resulting in a major global pandemic [1] that has caused over 1 million deaths in the United States (US) and 7 million deaths globally [2]. Moreover, a proportion of individuals infected with SARS-CoV-2 may experience persistent somatic symptoms, a condition known as long COVID (LC), also referred to as Post-Acute Sequelae of COVID-19 (PASC), Post-Acute COVID Syndrome (PACS), or Post-COVID Conditions (PCC). Due to the lack of biomarkers to confirm the presence of LC, along with its heterogeneous manifestations, diverse definitions of LC have been used. This has hindered accurate estimation of its burden, identification of prevention and management strategies of the condition.
The most recognized definition of LC is provided by the World Health Organization (WHO), which describes it as the continuation or development of new symptoms — over 200 different symptoms that can impact everyday functioning — occurring 3 months after the initial SARS-CoV-2 infection, lasting for at least 2 months with no other explanation [3]. In the US, the National Academic Sciences Engineering Medicine (NASEM) published a consensus definition, describing LC as an infection-associated chronic condition that occurs after SARS-CoV-2 infection, persists for at least 3 months, and can present as a continuous, relapsing and remitting, or progressive disease state affecting one or more organ systems [4]. The Centers for Disease Control and Prevention (CDC) initially defined LC as symptoms lasting 4 weeks or longer after SARS-CoV-2 infection but later revised the definition to symptoms persisting for at least 3 months after infection.
Based on data collected between 2020 and 2021 from 22 countries, approximately 6.2% of individuals of all ages experienced at least one of three LC symptom clusters — persistent fatigue with body pain or mood swings, cognitive problems, or ongoing respiratory issues — 3 months after SARS-CoV-2 infection [5]. LC negatively impacts quality of life, leading to significant health and economic strain on individuals and health care system [6]. Prevention of LC is essential to reduce this toll on individuals and the society. Studies demonstrating the impact of vaccines or antivirals on LC are accumulating, however, systematic reviews synthesizing these outcomes are lacking. We aim to shed light on interventions for prevention of LC. Our objectives are to (1) review pathogenic mechanisms and risk factors of LC, and (2) systematically review interventions, particularly vaccines and antivirals, for LC prevention, using the definition of LC as symptoms persisting for 3 months or longer after SARS-CoV-2 infection, aligning with the definitions from the WHO, NASEM, and CDC.
2. The Pathogenic Mechanism of Long Covid
Long COVID can affect multiple organs, including respiratory, cardiovascular, neurological, gastrointestinal, endocrine, musculoskeletal, reproductive, and immune systems, leading to a wide variety of symptoms [4,7,8,9]. Long-lasting symptoms after acute infection with SARS-CoV-2 are not unique; a variety of chronic conditions triggered by other infectious agents have been well described [4]. Examples include long-lasting symptoms caused by neurotrophic herpesviruses, enteroviruses, Ebola virus, MERS viruses, Borrelia spp. (implicating pathogen for Lyme disease) and chronic fatigue syndrome by Coxiella burnetii (implicating pathogen for Q fever) [4]. Moreover, there are many similarities in the pathophysiology and biological abnormalities between myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and LC, including nervous system dysfunction, cardiovascular abnormalities, immune system dysregulation, metabolic alterations, and gut microbiome alterations, suggesting potential overlapping mechanisms [10]. Insights from one condition may help understand the other [10]. At this time, the mechanisms of LC pathogenesis are not fully elucidated and can vary between individuals [4], as well as due to other external factors. For example, incidence of LC may be less common with Omicron variants compared to earlier variants [11]. Interestingly, compared to pre-Delta and Delta eras combined, gastrointestinal, metabolic, and musculoskeletal disorders have increased during the Omicron era while symptoms related to other systems like respiratory, neurological, have decreased over time. This indicates a shift in the phenotypic features of LC which is likely influenced by the evolving virus and vaccination [11].
The key mechanisms hypothesized for LC pathogenesis include persistent viral reservoirs, immune dysregulation and inflammatory responses, autoimmunity, reactivation of latent herpesviruses, microvascular and endothelial dysfunction, nervous system dysfunction, and microbiota dysbiosis.
Persistent viral reservoirs: LC consists of a broad range of symptoms lasting beyond 3 months after the infection, regardless of presence of viral particles. However, compared to individuals who do not develop LC, LC patients are more likely to have persistent viral RNA or protein in their tissues or blood, potentially establishing a reservoir [12,13,14]. In one of the studies, autopsies on 44 patients were conducted and in 11 patients they detected replication of SARS-CoV-2 in multiple anatomic sites including brain [13]. Additionally, SARS-CoV-2 proteins or RNA in specific tissues may drive LC pathogenesis such as chronic inflammation, immune dysregulation, latent pathogens reactivation, vascular abnormalities, and microbiome dysbiosis, leading to persistent symptoms [12].
Immune dysregulation and inflammatory responses: Insufficient SARS-CoV-2 antibody production and altered T cell responses during acute COVID-19 may be predictive of LC [7,15,16]. LC patients exhibit decreased CD4+ and CD8+ effector memory cells, increased expression of PD-1 (programmed cell death protein 1), highly activated innate immune cells, and a lack of naïve T and B cells, indicating persistent inflammatory response [16,17]. In fact, LC patients demonstrated persistently elevated inflammatory cytokines, such as IFN- β, IFN- λ1, IL-1β, IL-6, TNF-α, IP10, and CCL11, with some remaining elevated even months after COVID-19 infection [16,17]. Production of autoantibodies (autoAbs), such as anti-nuclear Abs (Ro/SS-A, La/SS-B, U1-snRNP, Jo-1,and P1) and anti-IFN-a2, is common in LC patients, which is negatively correlated with production of anti-SARS-CoV-2 antibodies [18]. Furthermore, some may already have autoAbs even before COVID-19 infection and COVID-19 may unmask subclinical autoimmune condition, leading to persistent inflammation and immune changes that contribute to LC [18]. Additionally, immune dysregulation promoted by SARS-CoV-2 can reactivate latent herpesviruses such as EBV and CMV, potentially worsening LC symptoms [7,9,10,19].
Microvascular and endothelial dysfunction: SARS-CoV-2 can impair microcirculation and endothelial function, leading to reduced oxygen delivery, clotting, and subsequent multiorgan damages [7,8]. Persistent microclots containing inflammatory molecules such as α2-antiplasmin and amyloid A have been observed in LC patients, potentially contributing to persistent symptoms [20].
Nervous system dysfunction: SARS-CoV-2 may cause neurological symptoms by directly invading the nervous system or triggering a systemic inflammatory response [7,21,22,23]. Additionally, impaired peripheral vasoconstriction and reduced tissue oxygen supply may contribute to neurological dysfunction [22,23]. Key characteristics of LC include neurological and cognitive dysfunction (‘brain fog’) such as fatigue, headache, memory loss, cognitive impairment, sensorimotor dysfunction, altered smell and taste, and autonomic dysfunction such as temperature dysregulation, postural orthostatic tachycardia syndrome (POTS), and orthostatic hypotension [7,10,23].
Microbiota dysbiosis: SARS-CoV-2 can disrupt gut microbiome resulting in persistent gastrointestinal (GI) symptoms (e.g. diarrhea, appetite loss, nausea, vomiting, or abdominal pain) and even respiratory (e.g. cough, sputum production, nasal congestion/runny nose, shortness of breath) and neurological symptoms (e.g. headache, dizziness, loss of taste, loss of smell, anxiety, difficulty in concentration, insomnia, poor memory, depression, blurred vision) [23,24,25,26]. The restoration of healthy microbiota could potentially reverse chronic symptoms in LC patients [27].
3. Risk Factors for Long COVID
Multiple studies have shown that females are more likely than males to develop LC [28,29,30,31]. A prospective cohort study found that female sex was associated with a 3-fold higher risk of developing LC [29]. A multicenter cohort study also described that the number of LC symptoms was significantly higher in females than in males, with a mean of 2.25 and 1.5, respectively [30]. Biological factors, such as higher estrogen levels in females, might contribute to the development of LC, as estrogen can upregulate angiotensin-converting enzyme 2 (ACE2), a receptor used by SARS-CoV-2 to enter the host cells [8,32], although the impact of ACE2 on LC remains unclear [32]. Behavioral differences, such as females being more attentive to bodily distress and more likely to seek medical care, may also contribute to the higher rate of LC in females [29,30].
Another risk factor for LC is the severity of the illness during the acute phase. Patients with more severe symptoms — such as being hospitalized, requiring analgesics, or needing additional treatments, are at a higher risk of developing LC [33,34,35]. For example, a population-based cohort study with a total of 1,459 patients found that the prevalence of LC was higher in hospitalized patients than in non-hospitalized patients, with a prevalence rate of 72.6% and 46.2%, respectively [33]. Additionally, a cohort study by Guzman-Esquivel et al. demonstrated a positive relationship between LC and factors such as hospitalization and antibiotic use [34].
Middle age or advanced age is associated with an increased risk of developing LC [35,36]. Additionally, being overweight or obese has been linked to a higher risk of developing LC as well [35,37]. A high overall burden of comorbidities, as well as pulmonary conditions such as asthma, chronic obstructive pulmonary disease, and obstructive sleep apnea, are also positively associated with LC [33,37,38]. Furthermore, pre-infection psychological distress significantly increases the risk of LC [39]. In a large prospective cohort study using data from Nurses’ Health study (predominantly female cohorts), individuals experiencing two or more types of distress prior to infection had nearly a 50% higher risk of developing LC [39].
4. Materials and Methods
A systematic review was conducted following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines [40] to evaluate prevention strategies for LC, including vaccines and antivirals.
LC was defined as persistent symptoms lasting three or more months, affecting one or more organ systems after SARS-CoV-2 infection [4]. We searched the PubMed/MEDLINE database for articles published between December 2019 through September 2024 using the following MeSH terms: “Post-Acute COVID-19 Syndrome (PACS)” AND “prevention and control”, “PACS” AND “Vaccines”, “PACS” AND “remdesivir”, “PACS” AND “nirmatrelvir”, and “PACS” AND “molnupiravir”.
We included articles that met the following criteria: (1) study population consisting of adults aged 18 years or older, (2) LC was defined as described above, and (3) individuals who were categorized as vaccinated or treated should have received vaccines or treatment before the onset of LC. We excluded the following studies: (1) studies that either did not define LC or defined LC with symptoms lasting less than 3 months, (2) studies that did not clearly indicate the timeline of vaccinations or treatment, and (3) studies that did not report a statistical significance value. For the purpose of this review, we did not include case reports or series, review articles, and meta-analyses.
Based on the above criteria, we included 28 studies [41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63]. Of these, fifteen focused on the impact of COVID-19 vaccination on LC, seven studied the impact of antivirals on LC, and six investigated the impact of other treatments on the development of LC (Figure 1).
Additionally, we compared the impact of COVID-19 vaccines and antivirals with those when LC was defined as persistent symptoms lasting 28 days or longer, as there are significant number of studies with this definition.
5. Results
Unless specified otherwise, the findings refer to LC defined as persistent symptoms lasting 3 months or longer.
5.1. Impact of COVID-19 Vaccine on the Prevention of Long COVID
We identified fifteen articles focused on impact of COVID-19 vaccination on LC. Unless described by the authors, COVID-19 infection before January 2021 is categorized as wild-type, infection between January 2021 and June 2021 as Alpha variant, infection between July and December 2021 as Delta variant, and infection from January 2022 onwards as Omicron variant (Table 1). We specified vaccine types when the information was available (Table 1).
Of the fifteen articles, ten studies demonstrated a protective effect of vaccines against development of LC (Table 1). Among five studies [43,46,55,64,65] that did not demonstrate a statistically significant protective effect on the development of LC, one study showed a trend toward protection [65] and two reported a reduction in a few LC symptoms due to vaccination [43,46]. In this section, we describe the identified prospective studies in detail and summarize identified retrospective and cross-sectional studies, focusing on the impact of vaccines on the development of LC. A summary of each selected study is described in Table 1.
Ayoubkhani et al. [42] conducted a prospective cohort study in the United Kingdom (UK) to determine the trajectory of the LC in participants who were vaccinated after being diagnosed with COVID-19. The study included 28,356 participants, who had at least one visit between February and September 2021 (Alpha and Delta variants), a test-confirming COVID-19 diagnosis at least 12 weeks before the final visit and had received a vaccine after the diagnosis of COVID-19 but before the above study period. The odds of developing LC decreased by 12.8% after the first vaccine dose (BNT162b2, mRNA-1273, or ChAdOx1) compared to unvaccinated individuals, and then decreased by an additional 8.8% after the second vaccine dose.
Antonelli et al. [64] investigated the effect of a third dose of (booster) of monovalent vaccine compared to a second dose during the Delta and Omicron era, separately, through a prospective community-based case-control study in the UK. The study included COVID-19 patients from June 2021 to April 2022, with 1,910 patients in each group during Delta period and 7,894 in each group during the Omicron period. The booster vaccination did not reduce the risk of LC when it was defined as symptoms persisting for 12 weeks, although there was a trend towards a protective effect. The booster vaccination did reduce the risk of LC when LC was defined as symptoms persisting for 4 weeks during Delta period.
A prospective longitudinal cohort study was carried out by Richard et al. [65] in the USA using the data from the Epidemiology, Immunology, and Clinical Characteristics of Emerging Infectious Diseases with Pandemic Potential (EPICC) study. The study population consisted of 1,832 military personnel aged 18 to 44 years who tested positive for SARS-CoV-2 from February 2020 to December 2021 (wild-type, Alpha and Delta variants). Fully vaccinated individuals (two doses of BNT162b2 or mRNA-1273, or one dose of Ad26.COV2.S) were 27% less likely to develop LC, though the difference was not statistically significant (P=0.17). However, when LC was defined as symptoms persisting 4 weeks, the risk was reduced by 28% with statistical significance (P=0.02).
Nehme et al. [57] compared prevalence of LC symptoms between individuals infected with COVID-19 (Omicron variants, BA.1 and BA.2) (total 1,807) and uninfected individuals (total 882), as well as between fully vaccinated (at least two doses of mRNA-1273 or BNT162b2 before COVID-19) and unvaccinated individuals. This study included individuals who were diagnosed with Omicron infection between December 2021 and February 2022 at the Geneva University Hospitals outpatient testing center and were contacted 3 months from their test date. Overall, 11.7% of individuals infected with Omicron had LC symptoms, compared to 10.4% of individuals tested negative (P < 0.001). LC symptoms were less common in fully vaccinated individuals compared to unvaccinated individuals (adjusted prevalence, 9.7% vs. 18.1%; P < 0.001)
A prospective cohort study by Brunvoll et al. [46] included 1,420 participants diagnosed with COVID-19 between November 2020 and October 2021 (wild-type, Alpha and Delta variants) in Norway. The study found no differences in self-reported LC symptoms between fully vaccinated (at least two doses of mRNA) and unvaccinated individuals, except that vaccinated individuals reported fewer memory problems. Additionally, the study found no differences in Everyday Memory Questionnaire-13 (EMQ-13) scores between vaccinated and unvaccinated.
Abu Hamdh et al. [41] carried out a prospective cohort study in Palestine, including 669 patients diagnosed with COVID-19 between September 2021 and January 2022 (Delta variant), of whom 6.7% required hospitalization. A total of 41% patients received at least one dose of vaccine (BNT162b2, Sputnik Light, mRNA-1273, Sputnik V (2.4%), or ChAdOx1) before COVID-19 diagnosis. Vaccinated patients with at least one dose had 85% lower odds of developing LC compared to unvaccinated patients.
Another prospective study in Pakistan including a total of 481 hospitalized patients with COVID-19 between February and June 2021 (Alpha variant) [52] showed that fully or partially vaccinated patients were less likely to develop LC compared to unvaccinated patients, with an adjusted odds ratio (aOR) of 0.38 (95% CI: 0.20-0.70) and 0.44 (95% CI: 0.24-0.80), respectively. Similarly, a prospective study conducted in Brazil involving 412 hospitalized patients diagnosed with COVID-19 between May 2021 and February 2022 (Alpha, Delta, and Omega variants), demonstrated that being fully vaccinated (at least one dose of Janssen or two doses of other vaccines) reduced the odds of developing LC (aOR = 0.55, P = 0.007).
A staggered retrospective cohort at the population level was carried out by Català et al. [47] using primary care records from the United Kingdom (UK) (Clinical Practice Research Datalink [CPRD] GOLD and CPRD AURUM), Spain (The Information System for Research in Primary care [SIDIAP]), and Estonia (CORIVA database), which included over 10 million vaccinated and over 10 million unvaccinated people. Analyses included both COVID-19 infected and uninfected patients to assess vaccine effect in preventing COVID-19 and subsequent LC. Individuals were registered by January or February 2021 and follow-up through December 2022 (Alpha, Delta, Omicron Variants), and vaccinations status was staggered based on the vaccine rollout period. COVID-19 vaccine (at least one dose of BNT162b2, ChAdOx1, mRNA-1273, or Ad26.COV2.S) showed a significant protective effect against developing LC, with overall vaccine effectiveness ranging from 29% to 52%. Trinh et al. [59] conducted the same analyses as Català et al., using the Norwegian Linked Health Registries at University of Oslo, which covers the entire Norwegian population of approximately 5.4 million, and demonstrated a reproducible and significant protective effect of vaccine against developing LC with 36% effectiveness.
Luo et al. [55] performed a retrospective cohort in Hong Kong using electronic and telephone follow-up records for COVID-19 patients diagnosed between December 2021 and May 2022 (predominantly Omicron variant), with follow-up for 6 to 12 months. They found that receiving a booster vaccine (three or more doses of BNT162b2 or CoronaVac) did not reduce the risk of LC compared to fewer doses before COVID-19. However, vaccination after the infection increased the risk of reporting LC symptoms, which may be due to the side effects from vaccination. MacCallum et al. [56] conducted a population-based retrospective cohort study, using data from the Michigan COVID-19 Recovery Surveillance Study for participants diagnosed with COVID-19 between March 2020 and May 2022 (wild-type, Alpha, Delta, and Omicron variants), which found a 58% lower adjusted prevalence of 90-day LC in the fully vaccinated group (2 doses of BNT162b2, mRNA-1273, ChAdOx1, or Sinovac; or 1 dose of Ad26.COV2.S) compared to the unvaccinated group. Babicki et al. [43] conducted a retrospective study in Poland using data from the STOP-COVID registry (unknown study period), with 9.4% vaccinated before COVID-19 and 73.6% after. Full vaccination (2 doses of BNT162b2, mRNA-1273 or ChAdOx1; or 1 dose of Ad26.COV2.S) had no impact on the development of LC, although headache, arthralgia, and new diagnosis of hypertension were less common in vaccinated individuals, regardless of the timeline of vaccination.
Woldeglorgis et al. [61] assessed LC prevalence 90 days post COVID-19 in highly vaccinated Western Australian adults between July and August 2022 (Omicron variant). Those with 0-2 vaccine doses had a 1.4-fold higher risk, and those with 3 doses had a 1.3-fold higher risk, compared to individuals with 4 or more doses. Xie et al., [62] using data from the 2022 National Health Interview Survey of the United States adults (Omicron variant), showed that those who received a booster dose had 25% lower odds of developing LC compared to unvaccinated individuals.
5.2. Impact of Antivirals on the Prevention of Long COVID
A total of seven studies met our inclusion criteria under this section. We identified one randomized trial, three prospective studies, and three retrospective studies. A summary of each study is described in Table 2.
Among the three studies that evaluated the impact of remdesivir on the prevention of LC in hospitalized patients, a randomized trial [58] found no differences between remdesivir-treated and untreated groups, while a prospective study[75] and a retrospective case-control study [53] demonstrated a protective effect of remdesivir, as described in the following details.
Nevalainen et al. [58] reported a one-year follow-up of the randomized SOLIDARITY Finland trial on the effects of remdesivir on recovery and LC symptoms. Among 181 patients recruited from 11 Finnish hospitals between July 2020 and January 2021 (wild-type) who completed the 1-year survey, no significant differences were found in self-reported recovery or LC symptoms between remdesivir-treated and untreated groups. A prospective study conducted by Boglione et al. [75] included 163 remdesivir-treated and 165 untreated patients who were hospitalized for COVID-19 during March 2020-January 2021 (wild-type and Alpha variant) at Saint Andrea hospital in Vercelli, Italy. The study showed a 36% reduction in the odds of developing LC in a remdesivir-treated group. A case control study by Fernández-de-las-Peñas et al.[53] included hospitalized COVID-19 patients from urban hospitals in Madrid, Spain, between September 2020 and March 2021 (wild-type and Alpha variant). The odds of developing LC symptoms following acute COVID-19 infection was 60% lower in patients treated with remdesivir during their acute infection compared to the patients who were not treated with remdesivir.
Among the three studies that evaluated the impact of nirmatrelvir/ritonavir on the prevention of LC, a prospective study [60] demonstrated a protective effect, while the other prospective cohort [51] and a retrospective cohort [49], did not.
A prospective cohort study conducted by Durstenfeld et al. in the United States (US) [51] involved the patients diagnosed with COVID-19 between March and August 2022 (Omicron variant), utilizing data from the Covid Citizen Science (CCS) study. This study, which included 353 treated with nirmatrelvir/ritonavir and 1,258 untreated patients, demonstrated that nirmatrelvir/ritonavir did not reduce the risk of LC at 3 months or later post COVID-19 infection, based on a propensity-adjusted model. Unlike the above study, Wang et al. [60] demonstrated a protective effect of nirmatrelvir/ritonavir in the development of LC in their prospective cohort study in China, involving COVID-19 patients discharged between April 2022 and June 2022 (Omicron variant) — nirmatrelvir/ritonavir treatment during hospitalization (178 out of 634 patients received nirmatrelvir/ritonavir) reduced the odds of developing LC by 65% at 6 months after hospital discharge. In a retrospective cohort study by Congdon et al. including 500 COVID-19 patients in New York, USA, from May to November 2022 (Omicron variant) [49], Nirmatrelvir/ritonavir was not associated with a significant reduction in the overall risk of developing LC.
Lastly, a retrospective study by Bertuccio et al. [44] showed a protective effect of antivirals, such as remdesivir, molnupiravir, or nirmatrelvir/ritonavir. Bertuccio et al. [44] included 649 outpatients with mild to moderate COVID-19 in Lombardy, Northern Italy and had at least one risk factor for disease progression between April 2021 and March 2022 (Alpha, Delta, and Omicron variants). The patients treated with antivirals, including remdesivir, molnupiravir, and nirmatrelvir/ritonavir, had a 57% reduction in the odds of developing any symptoms compared to those not treated with antivirals. Additionally, patients treated with monoclonal antibodies (mAbs) had a 52% reduction in odds of developing neuro-behavioral symptoms compared to those not treated with mAbs.
5.3. Impact of Other Treatments on the Prevention of Long COVID
Six studies met the inclusion criteria under this section, including three randomized trials, one secondary analysis of a randomized clinical trial, and two retrospective cohorts. A randomized clinical trial in outpatients [54] and a secondary analysis of a randomized clinical trial in hospitalized patients [63] found no protective effect of COVID-19 convalescent plasma (CCP) on the development of LC. In contrast, a randomized trial by Bramante et al. [45] demonstrated that metformin reduced LC risk in outpatients, and two retrospective cohort studies [48,50] demonstrated a protective effect of corticosteroids in hospitalized patients. Lastly, multiple micronutrient supplement did not demonstrate a protective effect in a randomized trial [80]. A summary of each study is described in Table 3.
Gebo et al. [54] conducted a double-blind, multicenter, randomized, controlled trial involving 1,225 symptomatic COVID-19 outpatients from June 2020 to October 2021 (wild-type, Alpha and Delta variants) across 23 sites in the USA, with a 90-day follow-up after CCP transfusion. While there was no statistically significant reduction in the odds of self-reported LC symptoms at 90 days for those who received CCP within 5 days of illness compared to the control group, a trend toward lower odds of LC was observed. Yoon et al. [63] conducted a secondary analysis of a randomized, blinded, multicenter controlled trial involving 281 hospitalized COVID-19 patients from April 2020 to March 2021 (wild-type and Alpha variant), with an 18-month follow-up. The study found no significant differences in the odds of developing LC between the CCP and placebo groups.
Bramante et al. [45] carried out a multi-site, phase 3, randomized, quadruple-blinded placebo-controlled trial to assess whether early treatment with metformin, ivermectin, or fluvoxamine could prevent LC in overweight or obese outpatients with COVID-19. Patients were enrolled within 3 days of COVID-19 diagnosis and within 7 days of symptom onset between December 2020 and January 2022 (wild-type, Alpha, Delta, and Omicron variants). The metformin group showed a 42% reduction in LC incidence compared to its control, while ivermectin or fluvoxamine showed no effect.
Two retrospective cohort studies demonstrated that corticosteroid treatment lowered the risk of developing LC — one conducted in in the Netherlands involving hospitalized COVID-19 patients between March 2020 and September 2021 (wild-type, Alpha and Delta variants) with criteria for corticosteroid use being respiratory rate > 25 breaths per minute, oxygen requirement > 5 L, or rapidly increasing oxygen requirement [50], and another in Spain in hospitalized COVID-19 patients between March and May 2020 (wild-type) [48]. The criteria for corticosteroid use were not mentioned in the study performed in Spain [48].
Two centers in Catalonia, Spain, investigated the effect of a multiple micronutrient supplement (MMS), comprising Vitamins A, B6, B12, C, D3, E, copper, folic acid, iron, selenium, and zinc, on LC incidence, in a double-blind, placebo-controlled, randomized clinical trial. The study included 246 patients with mild COVID-19 (not requiring hospital admission) between September 2021 and February 2023 (Delta and Omicron variants). The trial found no differences in LC incidence between the intervention group (MMS for 2 weeks starting on day 1 of inclusion) and the placebo groups [80].
6. Discussion
Long COVID (LC) poses significant medical, social, and economic impacts worldwide [4]. The underlying mechanisms of LC remain elusive. The hypothesized mechanisms include persistent viral reservoirs, immune dysregulation and inflammatory responses, autoimmunity, and microbiota dysbiosis. The proposed mechanisms are not mutually exclusive and may interact with each other, leading to a complex and varied clinical presentation seen in patients with LC. Risk factors such as female sex, severe illness, overweight/obesity, comorbidities, and pre-infection psychological distress are important to understand, but most are not easily modifiable. Based on that, our systematic review focused on the modifiable preventive strategies for LC.
Despite the numerous studies on LC, research on its prevention remains challenging due to the evolving nature of the virus, lack of unique biomarkers for diagnosing LC, and variations in LC definition [2]. Additionally, types of SARS-CoV-2 variants and existing immunity against COVID-19 can influence LC incidence or prevalence [11]. The definitions of LC used in studies, along with inclusion or exclusion criteria, study design and methods, and study setting (e.g. inpatient-based or outpatient), can significantly affect the effect size and outcomes of interventions as well [81]. Furthermore, LC symptoms appear to evolve over time, therefore, the study outcomes may vary depending on timing of LC assessment after COVID-19 diagnosis [81].
6.1. COVID-19 Vaccines Reduce the Risk of Long COVID
Our review found that ten out of fifteen vaccine-related studies demonstrated a significant overall protective effect of COVID-19 vaccines against developing LC, regardless of the type of SARS-CoV-2 variants. Most studies, except for two large staggered retrospective cohorts [47,59], included only patients diagnosed with COVID-19 to assess the effect of vaccines, likely underestimating the true impact of vaccines since COVID-19 vaccines reduce the risk of infection and severity of illness [82] and, consequently, LC. Still, most studies that included only patients diagnosed with COVID-19 demonstrated a protective effect of vaccines.
Most of our selected studies investigated the effect of full vaccination compared to no vaccination, demonstrating a protective effect of vaccination on LC. However, two studies [55,64] investigated the effect of a booster: one compared it to full vaccination and the other compared it to less than three doses, during the Delta/Omicron and Omicron periods, respectively, and did not find a statistically significant effect. In contrast, a cross-sectional study conducted in Australia [61] found a dose-response benefit of vaccination against LC during the Omicron period. While further studies are needed to elucidate this, it is possible that the effect size of booster vaccination, when compared to full vaccination, may have not be large enough to reach statistical significance in certain patient population.
Two studies did not show a benefit of vaccination in preventing LC. The study by Richard et al. [65], which did not show a statistically significant protective effect of full vaccination despite a trend toward protection, was composed of young military personnel, with only 22.9% fully vaccinated. Furthermore, the study by Brunvoll et al. [46], where no protective effect of vaccination was demonstrated except for reduction in memory problems, had only 25% of the participants vaccinated, likely because a significant portion of the participants were infected before vaccines became widely available. The unique study population and/or low vaccination rates due to vaccine unavailability during the early pandemic may have reduced the power of the studies to detect a difference.
The study by Babicki et al. [43], which found a protective effect of full vaccination on only a few symptoms, did not specify the COVID-19 eras, making it difficult to interpret the findings.
Over time, LC rates have declined, associated with viral variants, vaccination, with highest rate observed in the pre-Delta era, followed by Delta era, then Omicron era [11]. Additionally, there are significant differences in LC rates and vaccine dose requirements for protection depending on the COVID-19 eras [11]. Therefore, comparisons from different COVID-19 eras can introduce a selection bias and lead to erroneous results. For example, staggered cohorts [47,59] selected equivalent numbers of vaccinated and unvaccinated individuals from each era to avoid selection bias. However, studies [46,56], which included the patients across different COVID-19 eras, including the wild-type era, may have disproportionately selected patients from the early COVID-19 eras, when vaccines were unavailable or vaccination rates were low, and LC rates were likely high. This selection method could have introduced a bias in the estimates.
Despite differences in patient population, design, methods, and COVID-19 eras, we found that COVID-19 vaccines are generally protective against LC. While further research is required, booster vaccines may not have a significant impact on the development of LC compared to the primary vaccine series in certain populations. We found a stronger effect of vaccines when LC was defined as symptoms lasting 28 days or longer (Table S1), which implies that COVID-19 vaccines reduce both acute COVID-19 illness and LC symptoms.
6.2. Equivocal Evidence for Protective Effect of Antivirals and Other Drugs
Three studies on remdesivir demonstrated a conflicting result; a randomized study with no effect [58] but a prospective study [75] and a retrospective case-control study with a protective effect on the development of LC [53]. While a randomized study is more impactful, further studies on this topic are necessary to reach a more definite conclusion.
A prospective study of hospitalized patients in China demonstrated a protective effect of nirmatrelvir/ritonavir [60], whereas a prospective cohort and a retrospective study in the US involving outpatients did not demonstrate a protective effect [49,51]. A retrospective study in Italy found a protective effect of antivirals (molnupiravir, nirmatrelvir, and remdesivir) in outpatients [44]. In the US, the Food and Drug Administration (FDA) approved the use of nirmatrelvir/ritonavir in mild to moderate COVID-19 to prevent severe infection [83], so nirmatrelvir/ritonavir has been hardly used in inpatient settings. Differences in conclusion of the studies can be due to the use of antivirals in different settings and patient populations and study design. Additionally, studies assessed LC symptoms at different time points after COVID-19, ranging from 3 months to 1 year, which may have influenced the outcome of the studies as well.
A protective effect of antivirals against LC was more notable when LC was defined as symptoms lasting 28 days or longer, which indicates that antivirals may help reduce symptoms of acute COVID-19 illness as symptoms of acute COVID-19 can last longer than 28 days.
A randomized and a secondary analysis of a randomized study [54,63], did not demonstrate a protective effect of COVID-19 convalescent plasma transfusion on the development of LC in outpatient and hospitalized settings. However, a randomized study demonstrated a protective effect of metformin use in the obese/overweight COVID-19 outpatients [45]. In addition, two retrospective studies demonstrated a protective effect of corticosteroid use in the hospitalized COVID-19 patients on the development of LC [48,50]. Further studies would be valuable in understanding the underlying mechanisms and impact of these drugs on LC.
6.3. Nutrients and Lifestyle Factors on Long COVID
Besides vaccines, antivirals, and the above medications, other factors such as nutrients and lifestyle factors may play an important role in the development of LC. While a randomized study did not demonstrate a protective effect of multiple micronutrient supplement (MMS) on LC incidence [80], it is possible that a longer duration of MMS use could yield different results. Future studies comparing micronutrient status between patients who develop LC and those who do not would be insightful. Although it was not included in our review because it did not meet our LC definition criteria, a prospective UK cohort study examining the association between modifiable lifestyle factors prior to COVID-19 (smoking, alcohol intake, body mass index, physical activity, sedentary time, sleep duration, and dietary habits) and LC demonstrated that the risk of LC was 36% lower with favorable life style compared to unfavorable life style [84]. Additional studies on modifiable lifestyle factors to prevent LC are warranted as well, especially since lifestyle modification can be potentially achievable at low cost and with minimal adverse effects.
6.4. Limitations
Our study has several limitations. We might have missed including some studies due to our inclusion criteria, although our review was comprehensive, extending to vaccine- and antiviral-related studies that defined LC as symptoms lasting 28 days or longer. There are no randomized trials to assess the impact of vaccines on the development of LC although the majority of the studies demonstrate a robust protective effect of vaccines. There are a limited number of studies for antivirals and other treatments, therefore, drawing a conclusion requires caution. Studies ascertained LC at different time points to determine the impact of vaccines, antivirals, or other treatments, however, we do not believe that it would change the major conclusion of our study.
7. Conclusions
Long COVID is a serious global burden that has impacted millions of individuals worldwide [2]. To the best of our knowledge, our study is the first systematic review addressing various preventive strategies for LC, particularly using the LC consensus definition.
Based on the available data at this time, COVID-19 vaccines likely reduce the risk of developing LC, however, evidence for antivirals and other drugs in preventing LC is still in its nascency. Future randomized, multi-center studies would offer valuable insights to (1) strengthen the evidence on the protection provided by COVID-19 vaccines against LC, (2) understand the impact of booster vaccines, antivirals, and other drugs on LC, and (3) understand the role of lifestyle in developing LC.
Lack of biomarkers that can assist in predicting or diagnosing LC hinders us from preventing LC effectively. Studies aiming to identify biomarkers that can predict the development of LC or diagnose LC are crucial to reduce the burden of LC. As our understanding of the pathophysiology of LC matures, our diagnostic, therapeutic, and preventive options will evolve, which will eventually reduce the morbidity associated with LC.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
All authors contributed equally.
Conflicts of Interest
The authors declare no conflicts of interest.
References
- Center for Disease Control and Prevention. COVID-19 Timeline. Available at: https://www.cdc.gov/museum/timeline/covid19.html. Accessed December 7, 2024.
- Ely EW, Brown LM, Fineberg HV, National Academies of Sciences E, Medicine Committee on Examining the Working Definition for Long C. Long Covid Defined. N Engl J Med 2024.
- World Health Organization. Post COVID-19 condition (Long COVID). Available at: https://www.who.int/europe/news-room/fact-sheets/item/post-covid-19-condition. Accessed December 7, 2024.
- Committee on Examining the Working Definition for Long COVID (Washington District of Columbia). A long Covid definition : a chronic, systemic disease state with profound consequences. Washington: National Academies Press, 2024.
- Global Burden of Disease Long CC, Wulf Hanson S, Abbafati C, et al. Estimated Global Proportions of Individuals With Persistent Fatigue, Cognitive, and Respiratory Symptom Clusters Following Symptomatic COVID-19 in 2020 and 2021. JAMA 2022; 328(16): 1604-15.
- Carlile O, Briggs A, Henderson AD, et al. Impact of long COVID on health-related quality-of-life: an OpenSAFELY population cohort study using patient-reported outcome measures (OpenPROMPT). Lancet Reg Health Eur 2024; 40: 100908. [CrossRef]
- Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol 2023; 21(3): 133-46.
- Li J, Zhou Y, Ma J, et al. The long-term health outcomes, pathophysiological mechanisms and multidisciplinary management of long COVID. Signal Transduct Target Ther 2023; 8(1): 416. [CrossRef]
- Proal AD, VanElzakker MB. Long COVID or Post-acute Sequelae of COVID-19 (PASC): An Overview of Biological Factors That May Contribute to Persistent Symptoms. Front Microbiol 2021; 12: 698169. [CrossRef]
- Komaroff AL, Lipkin WI. ME/CFS and Long COVID share similar symptoms and biological abnormalities: road map to the literature. Front Med (Lausanne) 2023; 10: 1187163. [CrossRef]
- Xie Y, Choi T, Al-Aly Z. Postacute Sequelae of SARS-CoV-2 Infection in the Pre-Delta, Delta, and Omicron Eras. N Engl J Med 2024; 391(6): 515-25. [CrossRef]
- Proal AD, VanElzakker MB, Aleman S, et al. SARS-CoV-2 reservoir in post-acute sequelae of COVID-19 (PASC). Nat Immunol 2023; 24(10): 1616-27.
- Stein SR, Ramelli SC, Grazioli A, et al. SARS-CoV-2 infection and persistence in the human body and brain at autopsy. Nature 2022; 612(7941): 758-63.
- Swank Z, Senussi Y, Manickas-Hill Z, et al. Persistent Circulating Severe Acute Respiratory Syndrome Coronavirus 2 Spike Is Associated With Post-acute Coronavirus Disease 2019 Sequelae. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 2023; 76(3): e487-e90. [CrossRef]
- Glynne P, Tahmasebi N, Gant V, Gupta R. Long COVID following mild SARS-CoV-2 infection: characteristic T cell alterations and response to antihistamines. J Investig Med 2022; 70(1): 61-7. [CrossRef]
- Klein J, Wood J, Jaycox JR, et al. Distinguishing features of long COVID identified through immune profiling. Nature 2023; 623(7985): 139-48. [CrossRef]
- Phetsouphanh C, Darley DR, Wilson DB, et al. Immunological dysfunction persists for 8 months following initial mild-to-moderate SARS-CoV-2 infection. Nat Immunol 2022; 23(2): 210-6. [CrossRef]
- Su Y, Yuan D, Chen DG, et al. Multiple early factors anticipate post-acute COVID-19 sequelae. Cell 2022; 185(5): 881-95 e20. [CrossRef]
- Peluso MJ, Deveau TM, Munter SE, et al. Chronic viral coinfections differentially affect the likelihood of developing long COVID. J Clin Invest 2023; 133(3). [CrossRef]
- Pretorius E, Vlok M, Venter C, et al. Persistent clotting protein pathology in Long COVID/Post-Acute Sequelae of COVID-19 (PASC) is accompanied by increased levels of antiplasmin. Cardiovasc Diabetol 2021; 20(1): 172. [CrossRef]
- Meinhardt J, Radke J, Dittmayer C, et al. Olfactory transmucosal SARS-CoV-2 invasion as a port of central nervous system entry in individuals with COVID-19. Nat Neurosci 2021; 24(2): 168-75. [CrossRef]
- Sarubbo F, El Haji K, Vidal-Balle A, Bargay Lleonart J. Neurological consequences of COVID-19 and brain related pathogenic mechanisms: A new challenge for neuroscience. Brain Behav Immun Health 2022; 19: 100399. [CrossRef]
- Turner S, Khan MA, Putrino D, Woodcock A, Kell DB, Pretorius E. Long COVID: pathophysiological factors and abnormalities of coagulation. Trends Endocrinol Metab 2023; 34(6): 321-44. [CrossRef]
- Liu Q, Mak JWY, Su Q, et al. Gut microbiota dynamics in a prospective cohort of patients with post-acute COVID-19 syndrome. Gut 2022; 71(3): 544-52. [CrossRef]
- Zollner A, Koch R, Jukic A, et al. Postacute COVID-19 is Characterized by Gut Viral Antigen Persistence in Inflammatory Bowel Diseases. Gastroenterology 2022; 163(2): 495-506 e8. [CrossRef]
- Zuo T, Zhang F, Lui GCY, et al. Alterations in Gut Microbiota of Patients With COVID-19 During Time of Hospitalization. Gastroenterology 2020; 159(3): 944-55 e8. [CrossRef]
- Mendes de Almeida V, Engel DF, Ricci MF, et al. Gut microbiota from patients with COVID-19 cause alterations in mice that resemble post-COVID symptoms. Gut Microbes 2023; 15(2): 2249146. [CrossRef]
- Asadi-Pooya AA, Akbari A, Emami A, et al. Risk Factors Associated with Long COVID Syndrome: A Retrospective Study. Iran J Med Sci 2021; 46(6): 428-36. [CrossRef]
- Bai F, Tomasoni D, Falcinella C, et al. Female gender is associated with long COVID syndrome: a prospective cohort study. Clin Microbiol Infect 2022; 28(4): 611 e9- e16. [CrossRef]
- Fernandez-de-Las-Penas C, Martin-Guerrero JD, Pellicer-Valero OJ, et al. Female Sex Is a Risk Factor Associated with Long-Term Post-COVID Related-Symptoms but Not with COVID-19 Symptoms: The LONG-COVID-EXP-CM Multicenter Study. J Clin Med 2022; 11(2). [CrossRef]
- Townsend L, Dyer AH, Jones K, et al. Persistent fatigue following SARS-CoV-2 infection is common and independent of severity of initial infection. PLoS One 2020; 15(11): e0240784. [CrossRef]
- Gagliardi MC, Tieri P, Ortona E, Ruggieri A. ACE2 expression and sex disparity in COVID-19. Cell Death Discov 2020; 6: 37. [CrossRef]
- Forster C, Colombo MG, Wetzel AJ, Martus P, Joos S. Persisting Symptoms After COVID-19. Dtsch Arztebl Int 2022; 119(10): 167-74.
- Guzman-Esquivel J, Mendoza-Hernandez MA, Guzman-Solorzano HP, et al. Clinical Characteristics in the Acute Phase of COVID-19 That Predict Long COVID: Tachycardia, Myalgias, Severity, and Use of Antibiotics as Main Risk Factors, While Education and Blood Group B Are Protective. Healthcare (Basel) 2023; 11(2). [CrossRef]
- Sudre CH, Murray B, Varsavsky T, et al. Attributes and predictors of long COVID. Nat Med 2021; 27(4): 626-31.
- Carvalho-Schneider C, Laurent E, Lemaignen A, et al. Follow-up of adults with noncritical COVID-19 two months after symptom onset. Clin Microbiol Infect 2021; 27(2): 258-63. [CrossRef]
- Vimercati L, De Maria L, Quarato M, et al. Association between Long COVID and Overweight/Obesity. J Clin Med 2021; 10(18). [CrossRef]
- Quan SF, Weaver MD, Czeisler ME, et al. Association of Obstructive Sleep Apnea with Post-Acute Sequelae of SARS-CoV-2 Infection. Am J Med 2024; 137(6): 529-37 e3. [CrossRef]
- Wang S, Quan L, Chavarro JE, et al. Associations of Depression, Anxiety, Worry, Perceived Stress, and Loneliness Prior to Infection With Risk of Post-COVID-19 Conditions. JAMA Psychiatry 2022; 79(11): 1081-91.
- Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ 2021; 372: n71.
- Abu Hamdh B, Nazzal Z. A prospective cohort study assessing the relationship between long-COVID symptom incidence in COVID-19 patients and COVID-19 vaccination. Sci Rep 2023; 13(1): 4896. [CrossRef]
- Ayoubkhani D, Bermingham C, Pouwels KB, et al. Trajectory of long covid symptoms after covid-19 vaccination: community based cohort study. Bmj 2022; 377: e069676. [CrossRef]
- Babicki M, Kapusta J, Pieniawska-Śmiech K, et al. Do COVID-19 Vaccinations Affect the Most Common Post-COVID Symptoms? Initial Data from the STOP-COVID Register-12-Month Follow-Up. Viruses 2023; 15(6). [CrossRef]
- Bertuccio P, Degli Antoni M, Minisci D, et al. The impact of early therapies for COVID-19 on death, hospitalization and persisting symptoms: a retrospective study. Infection 2023; 51(6): 1633-44. [CrossRef]
- Bramante CT, Buse JB, Liebovitz D, et al. Outpatient treatment of Covid-19 with metformin, ivermectin, and fluvoxamine and the development of Long Covid over 10-month follow-up. medRxiv 2022.
- Brunvoll SH, Nygaard AB, Fagerland MW, et al. Post-acute symptoms 3-15 months after COVID-19 among unvaccinated and vaccinated individuals with a breakthrough infection. Int J Infect Dis 2023; 126: 10-3. [CrossRef]
- Català M, Mercadé-Besora N, Kolde R, et al. The effectiveness of COVID-19 vaccines to prevent long COVID symptoms: staggered cohort study of data from the UK, Spain, and Estonia. Lancet Respir Med 2024; 12(3): 225-36. [CrossRef]
- Catalán IP, Martí CR, Sota DP, et al. Corticosteroids for COVID-19 symptoms and quality of life at 1 year from admission. J Med Virol 2022; 94(1): 205-10. [CrossRef]
- Congdon S, Narrowe Z, Yone N, et al. Nirmatrelvir/ritonavir and risk of long COVID symptoms: a retrospective cohort study. Sci Rep 2023; 13(1): 19688. [CrossRef]
- Davelaar J, Jessurun N, Schaap G, Bode C, Vonkeman H. The effect of corticosteroids, antibiotics, and anticoagulants on the development of post-COVID-19 syndrome in COVID-19 hospitalized patients 6 months after discharge: a retrospective follow up study. Clin Exp Med 2023; 23(8): 4881-8.
- Durstenfeld MS, Peluso MJ, Lin F, et al. Association of nirmatrelvir for acute SARS-CoV-2 infection with subsequent Long COVID symptoms in an observational cohort study. J Med Virol 2024; 96(1): e29333. [CrossRef]
- Fatima S, Ismail M, Ejaz T, et al. Association between long COVID and vaccination: A 12-month follow-up study in a low- to middle-income country. PLoS One 2023; 18(11): e0294780. [CrossRef]
- Fernandez-de-Las-Penas C, Franco-Moreno A, Ruiz-Ruigomez M, et al. Is Antiviral Treatment with Remdesivir at the Acute Phase of SARS-CoV-2 Infection Effective for Decreasing the Risk of Long-Lasting Post-COVID Symptoms? Viruses 2024; 16(6). [CrossRef]
- Gebo KA, Heath SL, Fukuta Y, et al. Early antibody treatment, inflammation, and risk of post-COVID conditions. mBio 2023; 14(5): e0061823. [CrossRef]
- Luo J, Zhang J, Tang HT, et al. Prevalence and risk factors of long COVID 6-12 months after infection with the Omicron variant among nonhospitalized patients in Hong Kong. J Med Virol 2023; 95(6): e28862. [CrossRef]
- MacCallum-Bridges C, Hirschtick JL, Patel A, Orellana RC, Elliott MR, Fleischer NL. The impact of COVID-19 vaccination prior to SARS-CoV-2 infection on prevalence of long COVID among a population-based probability sample of Michiganders, 2020-2022. Ann Epidemiol 2024; 92: 17-24. [CrossRef]
- Nehme M, Vetter P, Chappuis F, Kaiser L, Guessous I, CoviCare Study T. Prevalence of Post-Coronavirus Disease Condition 12 Weeks After Omicron Infection Compared With Negative Controls and Association With Vaccination Status. Clinical infectious diseases : an official publication of the Infectious Diseases Society of America 2023; 76(9): 1567-75. [CrossRef]
- Nevalainen OPO, Horstia S, Laakkonen S, et al. Effect of remdesivir post hospitalization for COVID-19 infection from the randomized SOLIDARITY Finland trial. Nat Commun 2022; 13(1): 6152. [CrossRef]
- Trinh NT, Jödicke AM, Català M, et al. Effectiveness of COVID-19 vaccines to prevent long COVID: data from Norway. Lancet Respir Med 2024; 12(5): e33-e4. [CrossRef]
- Wang Y, Zhao D, Xiao W, et al. Paxlovid reduces the risk of Long COVID in patients six months after hospital discharge. J Med Virol 2023; 95(8): e29014. [CrossRef]
- Woldegiorgis M, Cadby G, Ngeh S, et al. Long COVID in a highly vaccinated but largely unexposed Australian population following the 2022 SARS-CoV-2 Omicron wave: a cross-sectional survey. Med J Aust 2024; 220(6): 323-30. [CrossRef]
- Xie Z, Stallings-Smith S, Patel S, Case S, Hong YR. COVID-19 booster vaccine uptake and reduced risks for long-COVID: A cross-sectional study of a U.S. adult population. Vaccine 2024; 42(16): 3529-35. [CrossRef]
- Yoon H, Li Y, Goldfeld KS, et al. COVID-19 Convalescent Plasma Therapy: Long-term Implications. Open Forum Infect Dis 2024; 11(1): ofad686. [CrossRef]
- Antonelli M, Penfold RS, Canas LDS, et al. SARS-CoV-2 infection following booster vaccination: Illness and symptom profile in a prospective, observational community-based case-control study. J Infect 2023; 87(6): 506-15. [CrossRef]
- Richard SA, Pollett SD, Fries AC, et al. Persistent COVID-19 Symptoms at 6 Months After Onset and the Role of Vaccination Before or After SARS-CoV-2 Infection. JAMA Netw Open 2023; 6(1): e2251360. [CrossRef]
- Al-Aly Z, Bowe B, Xie Y. Long COVID after breakthrough SARS-CoV-2 infection. Nat Med 2022; 28(7): 1461-7. [CrossRef]
- Azzolini E, Levi R, Sarti R, et al. Association Between BNT162b2 Vaccination and Long COVID After Infections Not Requiring Hospitalization in Health Care Workers. Jama 2022; 328(7): 676-8. [CrossRef]
- Brannock MD, Chew RF, Preiss AJ, et al. Long COVID risk and pre-COVID vaccination in an EHR-based cohort study from the RECOVER program. Nat Commun 2023; 14(1): 2914. [CrossRef]
- Di Fusco M, Sun X, Moran MM, et al. Impact of COVID-19 and effects of booster vaccination with BNT162b2 on six-month long COVID symptoms, quality of life, work productivity and activity impairment during Omicron. J Patient Rep Outcomes 2023; 7(1): 77.
- Lundberg-Morris L, Leach S, Xu Y, et al. Covid-19 vaccine effectiveness against post-covid-19 condition among 589 722 individuals in Sweden: population based cohort study. BMJ 2023; 383: e076990. [CrossRef]
- Malden DE, Liu IA, Qian L, et al. Post-COVID conditions following COVID-19 vaccination: a retrospective matched cohort study of patients with SARS-CoV-2 infection. Nat Commun 2024; 15(1): 4101. [CrossRef]
- Sigler R, Covarrubias K, Chen B, et al. Post-acute sequelae of COVID-19 in solid organ transplant recipients. Transpl Infect Dis 2023; 25(6): e14167.
- Tannous J, Pan AP, Potter T, et al. Real-world effectiveness of COVID-19 vaccines and anti-SARS-CoV-2 monoclonal antibodies against postacute sequelae of SARS-CoV-2: analysis of a COVID-19 observational registry for a diverse US metropolitan population. BMJ Open 2023; 13(4): e067611. [CrossRef]
- Taquet M, Dercon Q, Harrison PJ. Six-month sequelae of post-vaccination SARS-CoV-2 infection: A retrospective cohort study of 10,024 breakthrough infections. Brain Behav Immun 2022; 103: 154-62. [CrossRef]
- Boglione L, Meli G, Poletti F, et al. Risk factors and incidence of long-COVID syndrome in hospitalized patients: does remdesivir have a protective effect? QJM : monthly journal of the Association of Physicians 2022; 114(12): 865-71.
- Fung KW, Baye F, Baik SH, McDonald CJ. Nirmatrelvir and Molnupiravir and Post-COVID-19 Condition in Older Patients. JAMA Intern Med 2023; 183(12): 1404-6. [CrossRef]
- Ioannou GN, Berry K, Rajeevan N, et al. Effectiveness of Nirmatrelvir-Ritonavir Against the Development of Post-COVID-19 Conditions Among U.S. Veterans : A Target Trial Emulation. Ann Intern Med 2023; 176(11): 1486-97.
- Xie Y, Choi T, Al-Aly Z. Association of Treatment With Nirmatrelvir and the Risk of Post-COVID-19 Condition. JAMA Intern Med 2023; 183(6): 554-64. [CrossRef]
- Xie Y, Choi T, Al-Aly Z. Molnupiravir and risk of post-acute sequelae of covid-19: cohort study. BMJ 2023; 381: e074572. [CrossRef]
- Tomasa-Irriguible TM, Monfà R, Miranda-Jiménez C, et al. Preventive Intake of a Multiple Micronutrient Supplement during Mild, Acute SARS-CoV-2 Infection to Reduce the Post-Acute COVID-19 Condition: A Double-Blind, Placebo-Controlled, Randomized Clinical Trial. Nutrients 2024; 16(11). [CrossRef]
- Krishna B, Wills M, Sithole N. Long COVID: what is known and what gaps need to be addressed. Br Med Bull 2023; 147(1): 6-19. [CrossRef]
- Lin DY, Gu Y, Xu Y, et al. Association of Primary and Booster Vaccination and Prior Infection With SARS-CoV-2 Infection and Severe COVID-19 Outcomes. JAMA 2022; 328(14): 1415-26. [CrossRef]
- U.S. Food and Drug Administration. First Oral Antiviral for Treatment of COVID-19 in Adults. Available at: https://www.fda.gov/news-events/press-announcements/fda-approves-first-oral-antiviral-treatment-covid-19-adults. Accessed December 7, 2024.
- Wang Y, Su B, Alcalde-Herraiz M, et al. Modifiable lifestyle factors and the risk of post-COVID-19 multisystem sequelae, hospitalization, and death. Nat Commun 2024; 15(1): 6363. [CrossRef]
- Nascimento T, do Valle Costa L, Ruiz AD, et al. Vaccination status and long COVID symptoms in patients discharged from hospital. Sci Rep 2023; 13(1): 2481. [CrossRef]
Figure 1.
PRISMA diagram-selection of studies for the review.
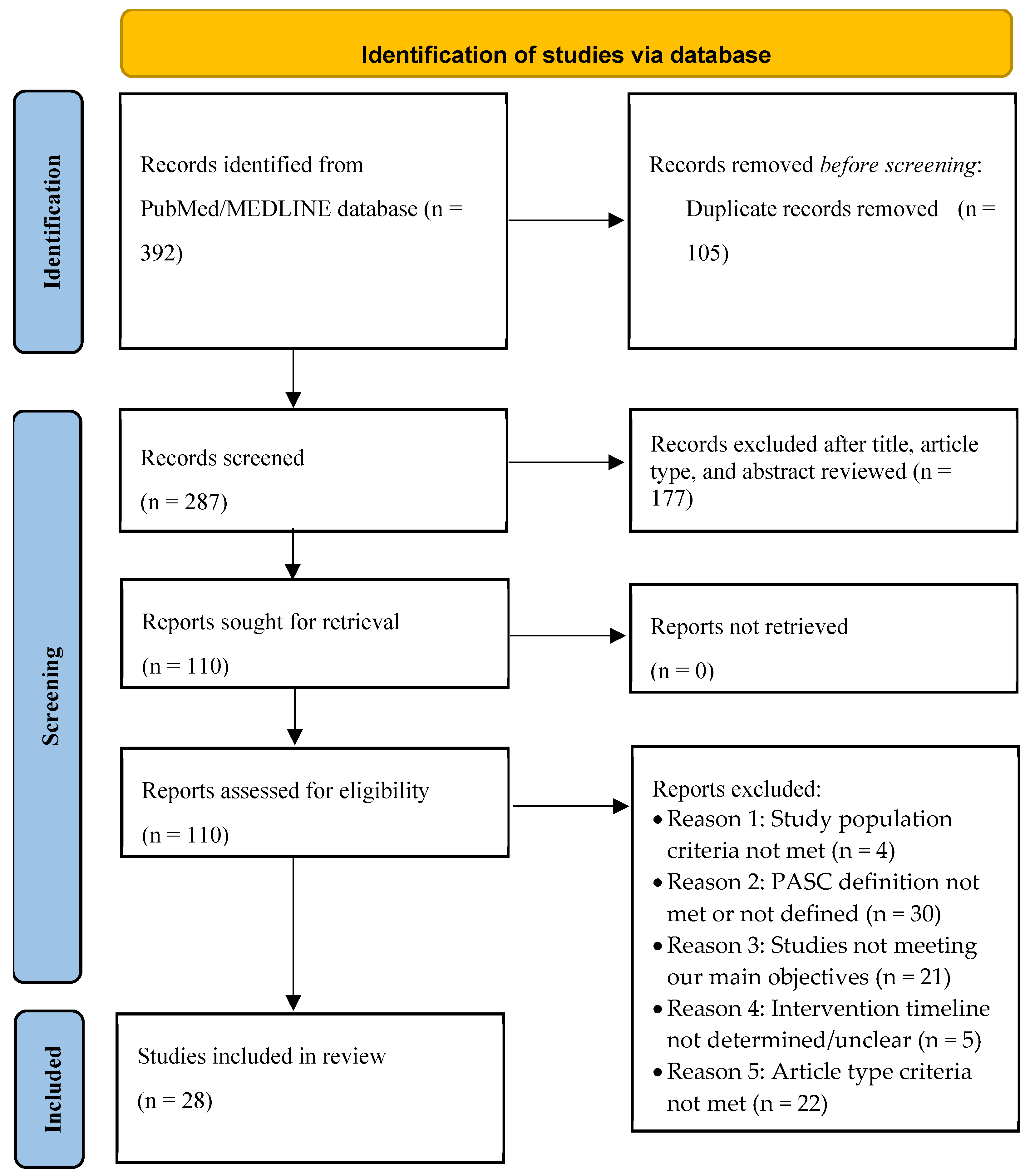

Table 1.
Impact of COVID-19 vaccine on the Prevention of Long COVID.
| Study author | Study design / Country (data) | Study period/Participants (SARS-CoV-2 variants) | LC cases | Patient N (F %) | Age (years), mean ± SD or median (IQR) |
Vaccinated (%) vaccine type vaccination time |
Vaccine impact on LC |
|---|---|---|---|---|---|---|---|
| Ayoubkhani et al. [42] | Prospective cohort / UK | Community based; Visit during Feb-Sep 2021; COVID-19 at least 12 wks before the final visit / (A, Δ) |
LC 3-10 mo after COVID-19 | COVID-19, n=28,356 (F 55.6%) | 45.9 ± 13.6 | Vaccinated (100%): BNT162b2, mRNA-1273, or ChAdOx1 after COVID-19 | Protective,1st vaccine 12.8% reduction in the odds (P < 0.001); 2nd vaccine aditional 8.8% reduction (P = 0.003) |
| Antonelli et al. [64] | Prospective case-control study / UK | Community based; June-Nov 2021 (Δ) and Dec 2021-Apr 2022 (O) / cases (third dose recipient), controls (second dose recipient) |
LC Sx ≥ 12 wks | All COVID-19, Delta:n=1,910 in each group (F 57%); Omicron: n=7,894 in each group (F 60.7%) | Delta: cases 64 ± 12.8, controls 63.7 ± 12.9; Omicron: cases 45.5 ± 16.3, controls 44.3 ± 17.7 | Vaccinated (100%): 3 doses of monovalent in cases, 2 doses in controls) before COVID-19 | No differences between cases & controls in both Δ & O eras, but a trend towards protection in vaccinated; when LC, Sx ≥ 4 wks, cases with aOR 0.56 (95% CI: 044-0.70) during Δ era. |
| Richard et al. [65] | Prospective cohort / USA | Feb 2020-Dec 2021 (wild-type, A, Δ), data from MHS EPICC study | LC Sx ≥ 3mo | COVID-19, n=1832 (F 39%) | 40.5 ± 13.7 (age range 18-44) | Fully vaccinated (22.9%) [2 doses of BNT162b2 or mRNA-1273, or one dose of Ad26.COV2.S] before COVID-19 | Trend towards Protective, RR 0.73 (95%CI: 0.47-1.14)** (When LC Sx ≥ 28d, RR 0.72 (0.54-0.96) |
|
Nehme et al. [57] |
Prospective longitudinal cohort / Switzerland | Outpatients, COVID-19 during Dec 2021-Feb 2022 (O) | LC 3 mo after COVID-19 | COVID-19, n=1807 (F 62.3%); COVID-19 negative, n=882 (F 63.9%) | COVID-19 positive, 41.6 ± 13.5 ; COVID-19 negative, 43.7 ± 14.9 | Fully vaccinated (75.5%) [at least 2 doses of mRNA-1273 (61.2%) or BNT162b2 (36.1%)] before COVID-19 | Protective, adjusted prevalence 9.7% vs. 18.1% (P < 0.001) |
| Brunvoll et al. [46] | Prospective cohort (Norweigian COVID-19 cohort) / Norway | COVID-19 during Nov 2020- Oct 2021 (wild-type, A, Δ) | LC 3 mo-15 mo after COVID-19 | COVID-19, n=1420 (F 71%) | Vaccinated, 48.3 ± 11.4 ; unvaccinated, 45.7 ± 12.3 | Fully vaccinated (25%) [at least 2 doses of mRNA vaccines at least 2 wks before COVID-19] | No differences in all components except for memory problem, fully vaccinated vs. unvaccinated, 11.9 % vs. 17.3% (P = 0.02) |
| Abu Hamdh et al. [41] | Prospective cohort / Palestine | COVID-19 during Sep 2021- Jan 2022, with FU phone interviews on d 10, 30, 60, 90 / (mainly Δ) | LC at 90 d | COVID-19, n=669 (F 57%) | 35.9 ± 11.5 | Vaccinated (41%) [BNT162b2 (17.8%), Sputnik Light (12.7%), mRNA-1273 (3.7%), Sputnik V (2.4%), ChAdOx1 (2.4%)] before COVID-19 | Protective, ≥ 1 dose vaccinated vs. unvaccinated, aOR 0.15 (95% CI: 0.09-0.24) |
|
Fatima et al. [52] |
Prospective cohort / Pakistan | Hospitalized patients with COVID-19 during Feb 2021-June 2021 / (A) | LC at 12 mo | COVID-19 patients admitted to Aga Khan University hospital, n=481 (F 38.3%) | 56.9 ± 14.3 | #Fully vaccinated (19%): 2 does of vaccines; partially vaccinated (19.2%): one dose before COVID-19 | Protective, fully vaccinated aOR 0.38 (95% CI: 0.20-0.70), partially vaccinated aOR 0.44 (95% CI: 0.24-0.80) |
| Nascimento et al. [85] | Prospective cohort / Brazil | Hospitalized patients with COVID-19 during May 2021 and Feb 2022 (A, Δ, O) | LC at 90d | COVID-19 patients, n=412 (35.4%) | 60 (IQR 48-72) | Fully vaccinated (44.9%) [1 dose Janssen or 2 doses of #other vaccines before COVID-19 | Protective, aOR for fully vaccinated 0.55 (P= 0.007) |
|
Català et al. [47] |
Staggered retrospective cohort / UK (CPRD); Spain (SIDIAP); Estonia (CORIVA) | Primary care data; registered by Jan or Feb 2021, with FU until Jan 2022 (UK), June 2022 (Spain), Dec 2022 (Estonia) / (A, Δ, O) | LC between 90 d & 365 d after COVID-19 | Over 10 million vaccinated vs. over 10 million unvaccinated (n/a). | n/a | Vaccinated with one dose (BNT162b2, ChAdOx1, mRNA-1273, or Ad26.COV2.S ) +GOLD (49.7%); *AURUM (49.4); SIDIAP (51.5%); CORIVA (19.4%) before COVID-19 | Protective: +GOLD, sHR 0.54 (95% CI: 0.44–0.67); *AURUM, 0.48 (0.34–0.68); SIDIAP, 0.71 (0.55–0.91); CORIVA, 0.59 (0.40–0.87) |
|
Trinh et al. [59] |
Staggered retrospective cohort/ Norway (Norwegian Linked Health Registries) | Primary care data; Vaccination roll out from Jan to Aug 2021, FU up to 1 yr / (A, Δ, O) |
LC between 90d & 365 d after COVID-19 | Over 2.3 million vaccinated vs. over 1.5 million unvaccinated (n/a) |
n/a | Vaccinated at least one dose (60.7%) [BNT162b2, mRNA-1273, or ChAdOx1] at least 14 d before COVID-19 | Protective, sHR 0.64 (95% CI: 0.55-0.74) |
|
Luo et al. [55] |
Retrospective cohort/ Hong Kong | Outpatient setting; COVID-19 during Dec 2021-May 2022 / (mainly O) |
LC at 6-12 mo after COVID-19 | COVID-19, n=6,242 (F 66.9%) | 47 (IQR 36-60) | Boosted (57.5%; 3 or more BNT162b2 or CoronaVac) vs. less than 3 doses, before COVID-19 | Not protective, aOR 1.105 (95% CI: 0.985-1.239) |
| MacCallum et al.[56] | Population-based retrospective cohort/ USA | Outpatient setting; COVID-19 during March 2020-May 2022 / (wild-type, A, Δ, O) |
LC at 90 d after COVID-19 | COVID-19, n=4,695 (F 54.0%) | age 18-29 (25.7%); age 30-49 (37.6%); age 50-64 (24.2%); 65+ (13.5%) | Fully vaccinated (27.9%) [2 doses of BNT162b2, mRNA-1273, ChAdOx1, or Sinovac; or 1 dose of Ad26.COV2.S] before COVID-19 | Protective, aPR 0.42 (95% CI: 0.34-0.53) |
|
Babicki et al. [43] |
Retrospective cohort/ Poland (STOP-COVID registry) | Unspecified study period, FU visits at 3 mo and 12 mo after COVID-19/ (n/a) | LC at 1 yr after COVID-19 | COVID-19, n=801 (F 65.4%) | 53.5 ± 12.8 | Fully vaccinated (83%) [2 doses of BNT162b2, mRNA-1273 or ChAdOx1 or 1 dose of Ad26.COV2.S], 73.6% vaccinated after COVID-19, 9.4% before COVID-19 | No differences, except that headache (17.4% vs. 29.4%, P=0.001), arthralgia (5.4% vs. 10.3%, P=0.032), dysregulation of HTN (11.6% vs. 18.4%, P=0.030) were more common in unvaccinated. |
| Woldegiorgis et al.[61] | Cross-sectional survey/ Australia | COVID-19 during July-Aug 2022, FU in 90 d / (O) | LC at 90 d after COVID-19 | COVID-19, n=11,697 (F 52.0%) | age 18-29 (20.9%); age 30-39 (21.0%); age 40-49 (18.7%); 50-59 (18.0%); 60-69 (11.6%); 70+ ( 9.7%) |
#Vaccinated, 0-2 (6%); three doses (76.3%); four doses (17.7%) before COVID-19 |
Protective, compared to vaccines 4 or more, 3 doses aRR 1.3 (95% CI: 1.1-1.5); 0-2 doses aRR 1.4 (1.2-1.8) |
|
Xie et al. [62] |
Cross-sectional survey/ USA | Outpatient setting; 2022 National Health Interview Survey / (O) |
LC 3 mo or longer post-infection | COVID-19, n=8,757(weighted 87,509,670) (F 53.3%) | age 18-29 (23.8%); age 30-39 (21.3%); age 40-49 (18.2%); age 50-64 (23.2%); 65+ (13.5%) | #Vaccinated, one dose (17.3%); initial series (33.3%); booster (27.2%) before COVID-19 | Protective, a booster vs. unvaccinated, aOR 0.75 (95% CI: 0.61-0.93) |
**not statistically significant; # Vaccine type not specified. Abbreviations; LC, Long COVID; N (n), number; F, female; UK, United Kingdon; USA, the United States of America; MHS EPICC, military health system Epidemiology, Immunology, and Clinical Characteristics of Emerging Infectious Diseases With Pandemic; CPRD, Clinical Practice Research Datalink; +GOLD, CPRD GOLD; *ARUM, CPRD ARUM; SIDIAP, The Information System for Research in Primary care; FU, follow-up; d, days; wks, weeks; mo, months; yrs, years; n/a, not available; CI, confidence interval; P, P-value; aOR, adjusted odds ratio; sHR, sub-distribution hazard ratio; aPR, adjusted prevalence ratio; aRR, adjusted risk ratio; HTN, hypertension; Jan, January; Feb, February; Aug, August; Sep, September; Oct, October; Nov, November; A, Alpha; Δ, Delta; O, Omicron.
Table 2.
Impact of Antivirals on the Prevention of Long COVID.
| Study author | Study design/ Country | Study period/Participants/ (SARS-CoV-2 variants) | LC cases | Patient N (F %) | Age, mean±SD or median (IQR) | Antivirals (treated %) | Antiviral impact on LC |
|---|---|---|---|---|---|---|---|
| Nevalainen et al. [58] | Randomized trial / Finland | Hospitalized patients with COVID-19 during July 2020 - Jan 2021/ (wild-type, A) | LC at 1 yr after COVID-19 | Treated 114 (F 35.1%); untreated 94 (F 36.2%). | Treated, 57.2 ± 13.5; untreated, 59.7 ± 13.2 | Remdesivir (200mg on the 1st day, then 100mg daily for a maximum 10 days.) |
No differences between remdesivir-treated & untreated with wide CI |
| Boglione et al. [75] | Prospective cohort / Italy | Hospitalized patients with COVID-19 during March 2020-Jan 2021(wild-type, A) | LC symptoms ≥ 12 wks | Total 449 (F 22%); Remdesvir-treated 163; untreated 165 |
65 (IQR 56-75.5) | Remdesivir | Protective, OR 0.64 (95% CI: 0.41-0.78) |
|
Fernández-de-las-Peñas et al. [53] |
Retrospective, Case-control study / Madrid, Spain | Hospitalized patients with COVID-19 during Sep 2020-March 2021 / (wild-type, A) | LC at 3 mo or later following COVID-19 | Treated, 216 (F 43.5%); untreated, 216 (F 43.5%) | Treated, 55.4 ± 12.6; Untreated, 55.6 ± 12.7 | Remdesivir (200mg on the 1st day, then 100mg daily for a maximum 10 days.) |
Protective, OR 0.401 (95 CI: 0.256-0.628) |
| Durstenfeld et al. [51] | Prospective cohort / USA | Vaccinated, outpatients with their first SARS-CoV-2 positive between March and Aug 2022 / (O) | LC at 90 d or later following COVID-19 | Treated, 353 (F 53.3%); untreated, 1258 (F 64.9%) | Treated, 62.1 ± 12.7; Untreated, 55.1 ± 13.6 | Nirmatrelvir/ritonavir |
No association, aOR 1.15 (95% CI: 0.80-1.64) |
| Wang et al. [60] | Prospective cohort / Shanghai, China | Admitted with COVID-19, then discharged between April and June 2022 / (O) | LC at 6 mo since discharged | COVID-19, 634 (F 54.4%) | 74.1 ± 11.4 | Nirmatrelvir/ritonavir | Protective, OR 0.349 (95 CI: 0.205-0.595) |
| Congdon et al. [49] | Retrospective cohort / New York, USA | Phone interviews between May 2022 & Nov 2022; COVID-19 four mo before the phone interview / (Δ, O) | LC at 4 mo after COVID-19 | Treated, 250 (F 66.4%); untreated, 250 (F 73.6%). Hospitalized (1%). | 50.6 | Nirmatrelvir/ritonavir | No reduction of overall risk of LC (Incidence 44% vs. 50%, P=0.21; aOR 0.83, 95% CI: 0.57-1.2). |
|
Bertuccio et al. [44] |
Retrospective cohort / Italy | Outpatients with mild to moderate COVID-19 during April 2021- March 2022 / (A, 3.5%; Δ, 2.2%; O 94.3%) | LC at 3 mo after COVID-19 | COVID-19, 649 (F 48.4%) |
67 (IQR 54-76) | 77 with antivirals (Molnupiravir, 41.6%; Nirmatrelvir/ritonavir, 13.0%; remdesivir, 45.5%); 141 with mAbs (Bamlanivimab/ Etesevimab, 44.7%; Casirivimab, 16.3%; Sotrovimab, 39.0%) |
Antiviral Protective, aOR 0.43 (95% CI: 0.21-0.87) for any symptoms; mAbs Protective, aOR 0.48 (0.25-0.92) for neuro-behavioral symptoms; |
Abbreviations; LC, Long COVID; N (n), number; F, female; USA, the United States of America; FU, follow-up; d, days; wks, weeks; mo, months; yrs, years; mAbs, monoclonal antibodies; CI, confidence interval; P, P-value; aOR, adjusted odds ratio; Jan, January; Aug, August; Sep, September; Nov, November; A, Alpha; Δ, Delta; O, Omicron.
Table 3.
Impact of Other treatments on the Prevention of Long COVID.
| Study author | Study design/ Country (Data) | Study period/Participants/ (SARS-CoV-2 variants) |
LC cases | Patient N (F %) | Age (years), mean ± SD or median (IQR) |
Treatment (treated %) | Treatment impact on LC |
|---|---|---|---|---|---|---|---|
| Gebo et al. [54] | Randomized clinical trial/ USA | Outpatients with COVID-19 between June 2020 & Oct 2021 / (wild-type, A, Δ) | LC at 90 d after CCP | 882 (F 57.4%) | 43 ± n/a | CCP | No association, aOR 0.75 (95% CI: 0.46-1.23) |
|
Yoon et al. [63] |
A secondary analysis of randomized clinical trial/ USA (CONTAIN-RCT) | Hospitalized with COVID-19 between April 2020 & March 2021 / (wild-type, A) | LC at 18 mo post-randomization | 281 (F 44.5%) | 59 (IQR 50-67) | CCP | No association, aOR 0.95 (95% CI: 0.54-1.67) |
|
Bramante et al. [45] |
Randomized clinical trial / USA | Enrolled from Dec 2020 to Jan 2022 / (wild-type, A, Δ, O) | LC at 10 mo after randomization | 1,125 (F 56%) | 45 (IQR 37-54) | #Metformin, ivermectin, fluvoxamine | Only metformin was protective, HR 0.58 (95% CI: 0.38-0.88); Ivermectin, HR 0.99 (0.59-1.64); fluvoxamine, HR 1.36 (0.79-2.39) |
| Davelaar et al. [50] | Retrospective cohort/ The Netherlands | Hospitalized with COVID-19 between March 2020 & Sep 2021 / (wild-type, A, Δ) | LC at 6 mo after discharged | 123 (F 38.2%) | 62.1 ± 9.5 | Corticosteroids | Protective, aOR 0.32 (95% CI: 0.11-0.90) |
| Catalán et al. [48] | Retrospective cohort / Spain | Telephone survey between March 2021 & April 2021 for patients hospitalized with COVID-19 one yr earlier / (wild-type) | LC at 1 yr after discharged | 76 (F 38%) | Treated, 68.5 (IQR 60.2-75.5); untreated, 61.5 (IQR 52.7-72.5) | Corticosteroids | Protective: headache, 6.3% vs. 25% (P=0.032); dysphagia, 11.4% vs. 0% (P=0.049); depression (22.7% vs. 3.1 %, P=0.016), chest pain (11.4% vs. 0%, P= 0.049); bodily pain (SF-36*: 100 vs. 75, P=0.017), mental health (SF-36*: 86 vs. 76, P=0.027) |
| Tomasa-Irriguible et al. [80] | Randomized clinical trial / Catalonia, Spain |
Outpatients with COVID-19 between Sep 2021 & Feb 2023 / (Δ, O) | LC at 6 mo | 246 (F 68.3%) | 46.8 ± 16.3 | Multiple micronutrient supplement |
No reduction of incidence of LC (intervention 27.7% vs. placebo 25%; P=0.785) |
#Metformin: 500mg on day 1, then 500mg twice daily for 4 days, then 500mg in the mornings and 1000mg in the evenings through 14 days; Ivermectin 390-470mcg/kg/day for 3 days; Fluvoxamine: 50mg on day 1, then 50mg twice daily through 14 days; SF-36*: Short Form-36 quality of life questionnaire. Abbreviations; LC, Long COVID; N (n), number; F, female; USA, the United States of America; FU, follow-up; d, days; wks, weeks; mo, months; yr(s), year(s); n/a, not available; CCP, COVID-19 convalescent plasma; CI, confidence interval; P, P-value; aOR, adjusted odds ratio; HR, hazard ratio; Oct, October; Dec, December; Jan, January; Sep, September; Feb, February; A, Alpha; Δ, Delta; O, Omicron.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



