
Submitted:
26 March 2025
Posted:
27 March 2025
You are already at the latest version
Abstract
Background: Anxiety disorders have a 7.3% worldwide prevalence and, considering the long period of treatment, developing new efficient and safer pharmacological tools is critical. Essential oils consist of highly concentrated lipophilic compounds from plants with therapeutic potential effects—Lavandula burnatii, produced in Córdoba with high levels of active pharmaceutical ingredients. The evidence indicates that lavender essential oil could induce anxiolytic effects, however, more systematic studies are needed. Methods: To test the anxiolytic attributes of Lavandula burnatii, male Wistar rats (200-260g) were injected intraperitoneally with 2 different doses of essential oil (30 /80 mg/Kg) or vehicle (Myritol 318, a high-purity vegetable oil), once (acute) or for 7 days. One hour after the last administration, the anxiolytic effects were evaluated using the following behavioral tests: dark-light box and elevated plus maze. The open-field test was used to assess locomotor activity. Results: Our results showed that the lower dose of lavender essential oil induces anxiolytic effects since it increases the time spent in the aversive compartment in each evaluation. The acute administration has no impact on the behaviors evaluated. The higher dose is comparable with the control group and does not show significant differences. Conclusion: More studies are needed to better characterize the beneficial effects of this essential oil for anxiety disorders and to establish an adequate dosage range.
Keywords:
anxiety
; lavender essential oil
; behavior
; Lavandula burnatii
1. Introduction
The global prevalence of anxiety disorders, based on data from 87 studies conducted in 44 countries, has been estimated at 7.3% [1,2,3]. Furthermore, they are associated with significant disability [3,4], an increased risk of developing chronic diseases [5], and high rates of comorbidity with other neuropsychiatric disorders, especially those related to mood and substance abuse [6]. These disorders have a significant economic impact on society, primarily affecting the working-age population (18–64 years) and those with other psychiatric conditions [7,8,9,10].
Conventional treatment for anxiety includes benzodiazepines and selective serotonin reuptake inhibitors; however, these drugs can cause adverse effects, tolerance, and withdrawal symptoms upon discontinuation [11]. Since anxiety disorders are often chronic and require long-term treatment, it is essential that the medications used meet high standards of safety and adherence. In this context, herbal medicine emerges as a natural alternative with fewer side effects that can be used as a complementary or palliative treatment for anxiety disorders and other mental health conditions [12]. Essential oils (EOs) have a long history in pharmaceutical sciences as natural products with diverse biological applications in the medicinal, cosmetic, agrochemical, and nutritional fields [13]. Their use in aromatherapy and phytotherapy is widely recognized, especially for their effects on reducing stress and anxiety [14] and in treating central nervous system disorders [15]. Despite their popularity, the available scientific evidence presents methodological limitations in clinical studies on EOs [16,17,18]. Therefore, further studies that provide greater rigor and validity to using EO are needed.
Remarkably, there is scientific evidence supporting the anxiolytic and antidepressant effects of certain EOs, with lavender EO (LEO) being one of the most studied for its relaxing properties and its traditional use in the treatment of anxiety, stress, and depression [19]. Organizations such as the World Health Organization (WHO), the European Scientific Cooperative on Phytotherapy (ESCOP), and the European Medicines Agency (EMA) [20] have approved the therapeutic use of lavender for these disorders. Several studies have analyzed its analgesic [21], anti-inflammatory [22], anxiolytic [23], antidepressant [24], and sleep-enhancing effects [23]. Several authors report beneficial effects of LEO in humans, for example, pregnant women who used LEO during the second and third trimester of pregnancy have reported a significant improvement in anxiety and sleep quality [25]. Moreover, an improvement in social anxiety was reported in first-year university students after LEO inhalation [26], and its beneficial effect was even seen in people diagnosed with anxiety disorders when ingesting LEO [27]. However, despite numerous publications, there are very few controlled preclinical studies with a systematic scientific methodology that demonstrate clinical efficacy and provide credibility to the effect of LEO [28]. It is important to highlight that most of the data in the literature refer to human studies and aromatherapy.
Lavandula burnatii (L. burnatii, clone Super), a hybrid resulting from the cross between Lavandula angustifolia (L. angustifolia) and Lavandula latifolia, is cultivated in the province of Córdoba, Argentina. This variety has a high concentration of linalool and linalyl acetate, compounds with described anxiolytic activity [29]. L. burnatii is characterized by its robust growth, low to moderate water requirements, and excellent adaptability to the region's soils. Additionally, has an advantage since it has a 20 times higher productive yield of oil per plant than L. angustifolia, and it has the same active components (linalool and linalyl acetate) and the other components of lavender essential oil, such as limonene, perillyl alcohol, coumarin, and camphor, present in other species with relative variation in their concentrations [30] in a similar proportion. Based on the described characteristics, this study aims to evaluate the effect of L. burnatii essential oil on anxiety behavior in male rats, given the fact there is no data about this variety cultivated in our region.
2. Materials and Methods
2.1. Essential Oil
LEO: extracted from flower tops of Lavandula burnatii was provided by Dr. Cristian Moya (AROMAHERBA, Calmayo, Córdoba, Argentina). The aerial parts of L. burnatii were collected during the flowering stage from Córdoba, dried, and subjected to hydrodistillation. The oil was stored in sealed vials at 4°C.
Chemical characterization of LEO: GC-FID (Gas chromatography with flame ionization detector) was used to qualitatively characterize the LEO used in the present study. Quantitative analyses of EOs were performed using a PerkinElmer Clarus 500 equipped with an FID and a DB-5 capillary column (30 m × 0.25 mm inner diameter and 0.25 μm film thickness). A 1 μL aliquot of LEO (1/100 v/v in n-heptane) was manually injected. The oven temperature was set as follows: 60 ◦C for 5 min, ramped to 240 ◦C at 5 ◦C/min and held for 10 min. Nitrogen was used as the carrier gas at a flow rate of 1 mL/min. The injector and detector temperatures were 250◦C and 280◦C, respectively. The abundance of each volatile EO compound was expressed as a relative percentage obtained by peak area normalization.
2.2. Animals
Adult male Wistar rats (250-300 g) were obtained from the Department of Pharmacology Otto Orsingher vivarium (Facultad de Ciencias Químicas, Universidad Nacional de Córdoba, Argentina) and randomly housed in groups of 3 or 4 one week before the beginning of the experimental protocol. Throughout the experiment, animals were maintained in controlled environmental conditions (20–24°C, 12-h light/dark cycle with lights on at 07 a.m.) and had free access to food and water. Behavioral experiments were conducted between 09:00 and 14:00 h.
All procedures were conducted following the NIH Guide for the Care and Use of Laboratory Animals and approved by the Animal Care and Use Committee CICUAL, Universidad Nacional de Córdoba, Argentina (EX-2023-00769898-UNC-ME#FCQ).
2.3. Experimental Protocol
LEO of L. burnatii was developed and supplied by Dr. Cristian Moya. The plantation is located at 850 meters above sea level, and the geographic coordinates are -32.031034 and -64.459524.
LEO was used at two different concentrations (30 and 80 mg/Kg) in a mixture of medium-chain triglycerides (Myritol 318 Pura Química, Córdoba, Argentina). The EO was stored at 4°C, and Myritol was stored at room temperature, both away from light until use.
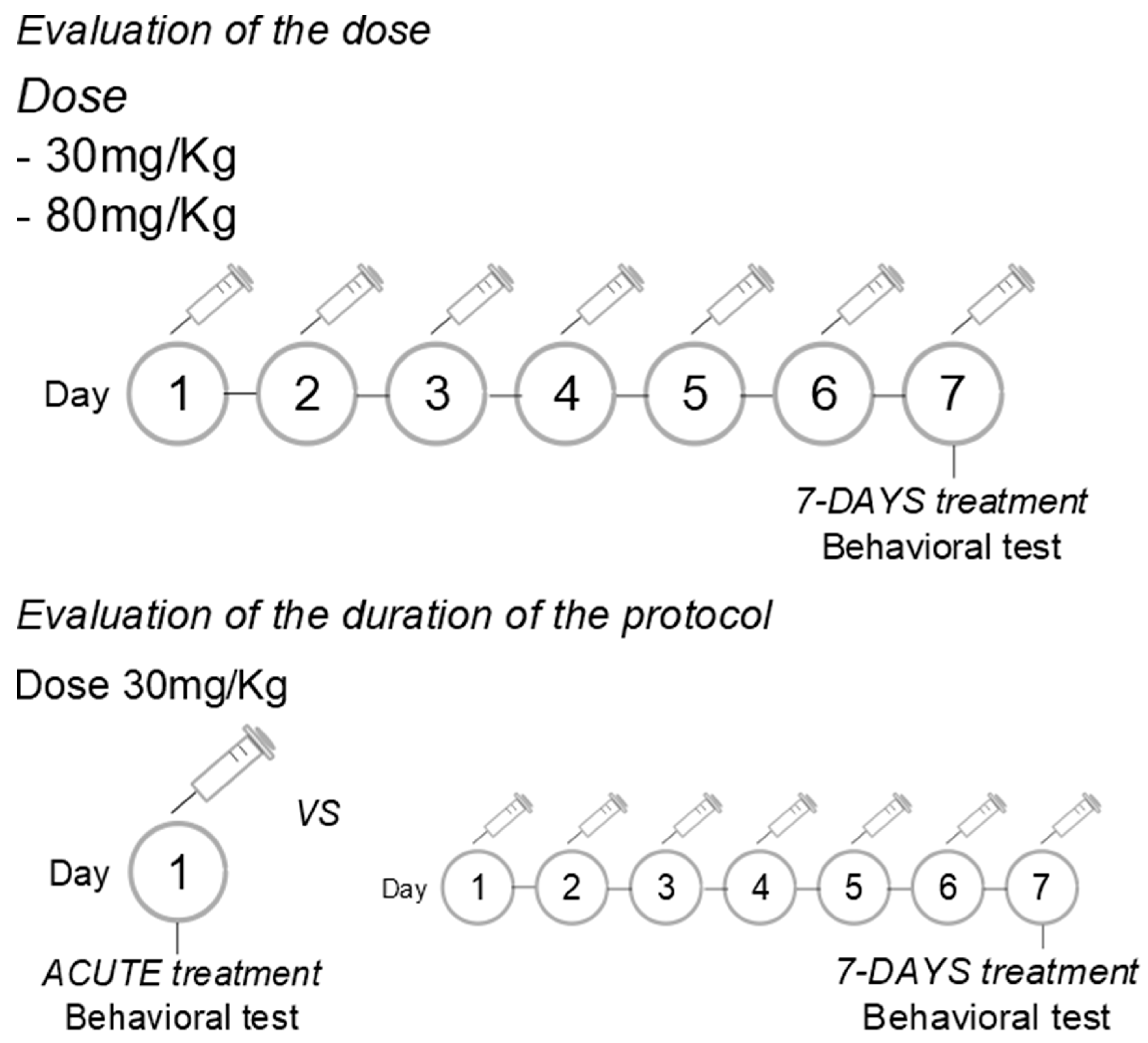
Evaluation of the dose: The LEO was administered intraperitoneally (i.p.) at doses of 30 or 80 mg/Kg, in a volume of 300 microliters, once daily for 7 consecutive days.
Evaluation of the duration of treatment: The LEO was administered in a dose of 30 mg/Kg (i.p.), in a volume of 300 microliters, acutely or once daily for 7 consecutive days. Since the dose evaluation was conducted first, we chose the dose with anxiolytic effects to assess the effective protocol of administration.
Control rats were treated with an equal volume of the vehicle (a mixture of medium-chain triglycerides). Experiments were conducted 1 h after the single or last drug/vehicle administration.
Figure 1.
Experimental protocols.
2.4. Behavioral Test
Elevated plus-maze test: The maze has two opposite arms (50 × 10 cm), crossed with two enclosed arms of the same dimension and having 40 cm high walls. The arms are connected with a central square (10 × 10 cm) giving the apparatus the shape of a plus sign. The maze was kept in a dimly lit room and elevated 50 cm above the floor. The rats were placed individually in the center of the maze, facing an open arm. Thereafter, the number of entries and time spent on the open and enclosed arms was recorded during the next 5 min. An arm entry was defined when all four paws of the rat were in the arm [31].
Dark-light test: The apparatus comprises a transparent section, called the “illuminated area” (27 × 27 × 30 cm), and a smaller, fully enclosed section, called the “dark area” (18 × 27 × 30 cm) separated by a partition with a small opening (12 × 5 cm). The light side is illuminated by a bulb. The test begins with the animal placed in the dark area, and the latency to enter the illuminated area is recorded, considering only whole-body entries. The test was measured for 5 minutes.
Open-field test: The apparatus (61 x 61 x 50 cm) was made of plywood and consisted of squares, the entire apparatus was painted grey, which divided the floor into 16 squares. The animals were placed in the center of the apparatus and the ambulation (distance traveled) was measured, for 5 minutes, using Smart 3.0 software [32].
2.5. Statistical Analysis
Data were analyzed using One-way ANOVA and Tukey's post-test. Data is reported as means ± SEM. A p-value of p< 0.05 was considered significant. The analyses were performed using GraphPad Prism® 8.02 software and the images were made by using Inkscape®.
3. Results
3.1. Chemical Composition of Lavandula burnatii Essential Oil
The geographical environment significantly influences the chemical composition of EO in the plants. Factors determining the chemical composition of EOs include temperature, altitude, rainfall, and harvest season (Table 1).
3.2. Effect of Lavandula burnatii Essential Oil on Elevated Plus-Maze Test
Regarding the dose evaluation, One Way ANOVA reported a significant difference in the time spent in open arms where the 30 mg/Kg of LEO induced significantly increased time in open arms compared with the control group and 80 mg/Kg (Figure 2A; Table 2A). The time spent in open arms in 80 mg/Kg of LEO was comparable to that of the control group and did not show a significant difference. LEO does not induce significant changes in the time spent in the closed arms since the dose of 30 or 80 mg/Kg were different from the control group (Figure 2B; Table 2B).
Moreover, the 7-day protocol (30 mg/Kg of LEO) induced increased time spent in open arms (Figure 2A; Table 3A), statistically different from the acute protocol and the control groups. No significant differences were observed between these last groups. One-way ANOVA showed no significant differences in the time spent in closed arms between the groups (Figure 2B; Table 3B).
3.3. Effect of Lavandula burnatii Essential Oil on Dark-Light Test
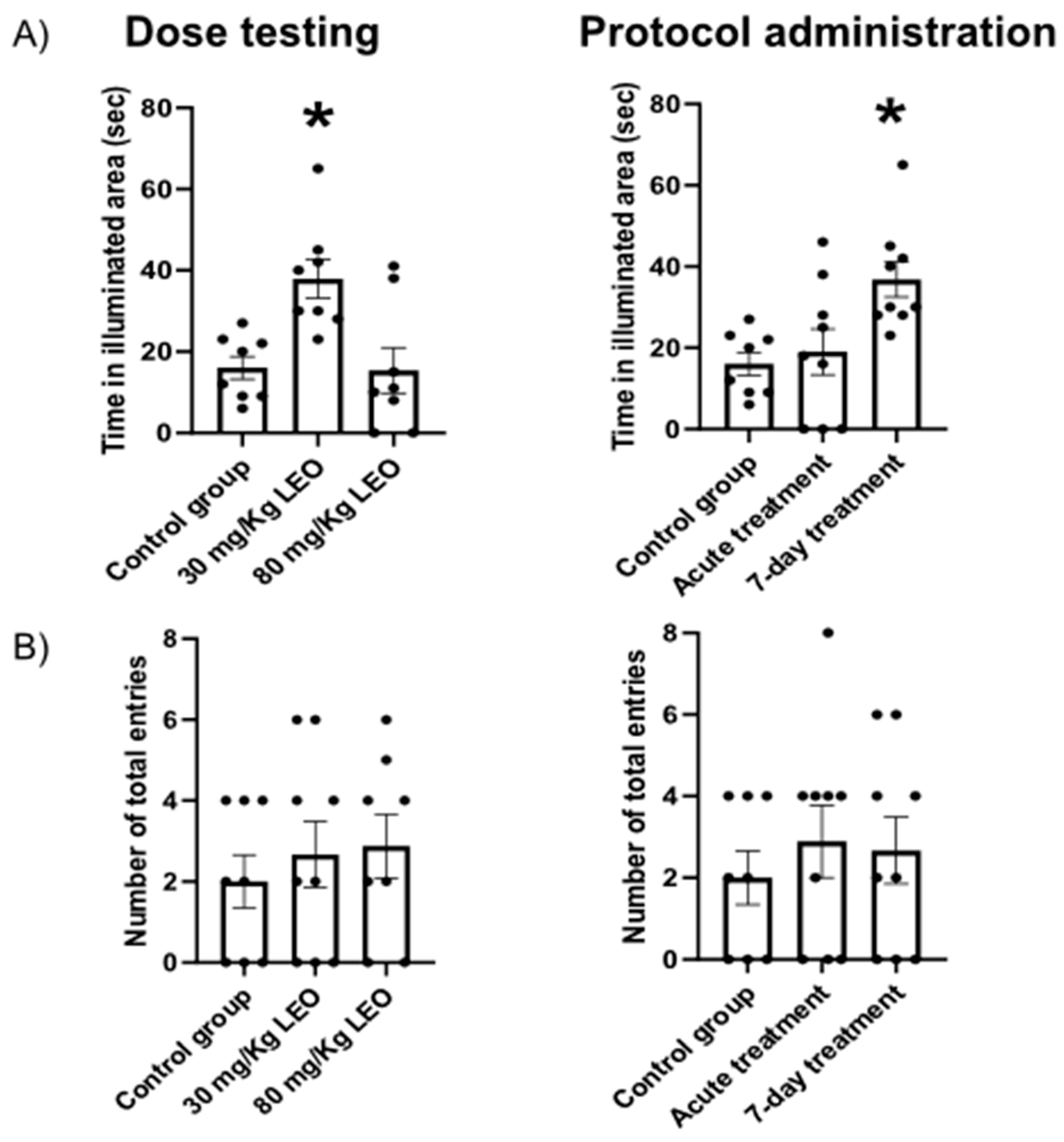
One-way ANOVA showed significant differences were the dose of 30mg/Kg of LEO showed a significant increase in the time spent in the illuminated area when compared to the dose of 80mg/Kg and the control group. No significant differences were observed between the dose of 80mg/Kg and the control group (Figure 3A; Table 4A). Both doses did not affect the number of total entries in the dark area showing no statistically significant differences when compared with the control group (Figure 3B; Table 4B).
The 7-day protocol showed a statistically significant increase in the time spent in the illuminated area compared with the acute treatment and the control group. The time spent in the illuminated area in acute treatment was comparable with the control group since no statistical difference where observed (Figure 3A; Table 5A). Both protocols of LEO (acute and 7-day) did not show a significant difference compared with the control group at the entries in the dark area (Figure 3B; Table 5B).
Figure 2.
Effect of Lavandula burnatii essential oil in the elevated plus maze test. A) LEO, in a dose of 30 mg/Kg, induces an increase in the time spent in open arms after a 7-day treatment, compared with 80mg/kg (left) or acute protocol (right). B) No significant differences were observed in the time spent in closed arms between the doses and the control group. N=8-10 in each group. Values are mean±SEM (*p<0.05 different from the all groups).
Figure 2.
Effect of Lavandula burnatii essential oil in the elevated plus maze test. A) LEO, in a dose of 30 mg/Kg, induces an increase in the time spent in open arms after a 7-day treatment, compared with 80mg/kg (left) or acute protocol (right). B) No significant differences were observed in the time spent in closed arms between the doses and the control group. N=8-10 in each group. Values are mean±SEM (*p<0.05 different from the all groups).
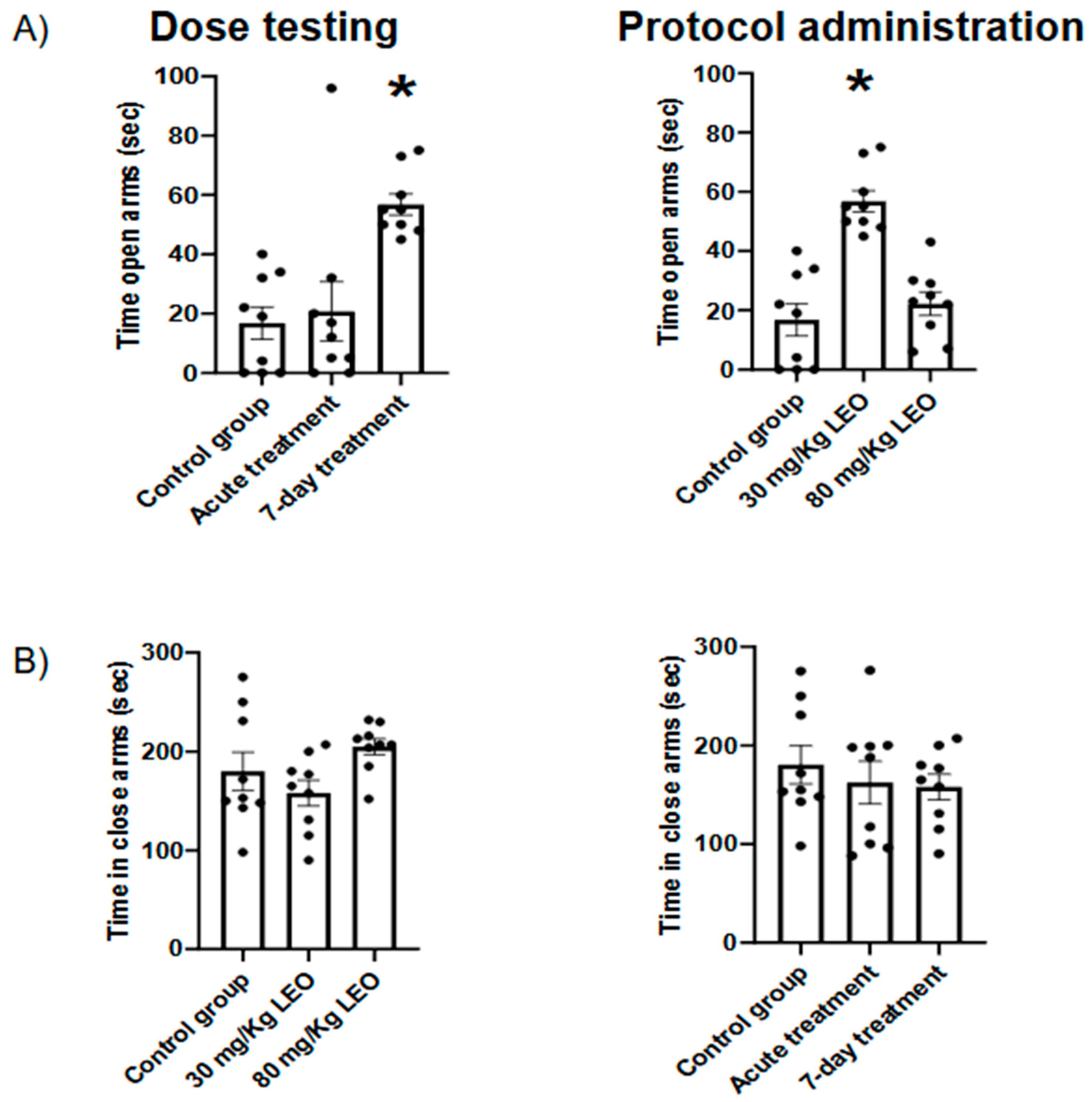
Figure 3.
Effect of Lavandula burnatii essential oil in Dark-light test. A) LEO, in a dose of 30mg/Kg, induces an increased time spent in the illuminated area after a 7-day treatment, compared with 80mg/kg (left) or acute protocol (right). B) No significant differences were observed in the total entries between the groups. N=8-10 in each group. Values are mean±SEM (*p<0.05 different from all groups).
Figure 3.
Effect of Lavandula burnatii essential oil in Dark-light test. A) LEO, in a dose of 30mg/Kg, induces an increased time spent in the illuminated area after a 7-day treatment, compared with 80mg/kg (left) or acute protocol (right). B) No significant differences were observed in the total entries between the groups. N=8-10 in each group. Values are mean±SEM (*p<0.05 different from all groups).
3.4. Effect of Lavandula burnatii Essential Oil in Open Field Test
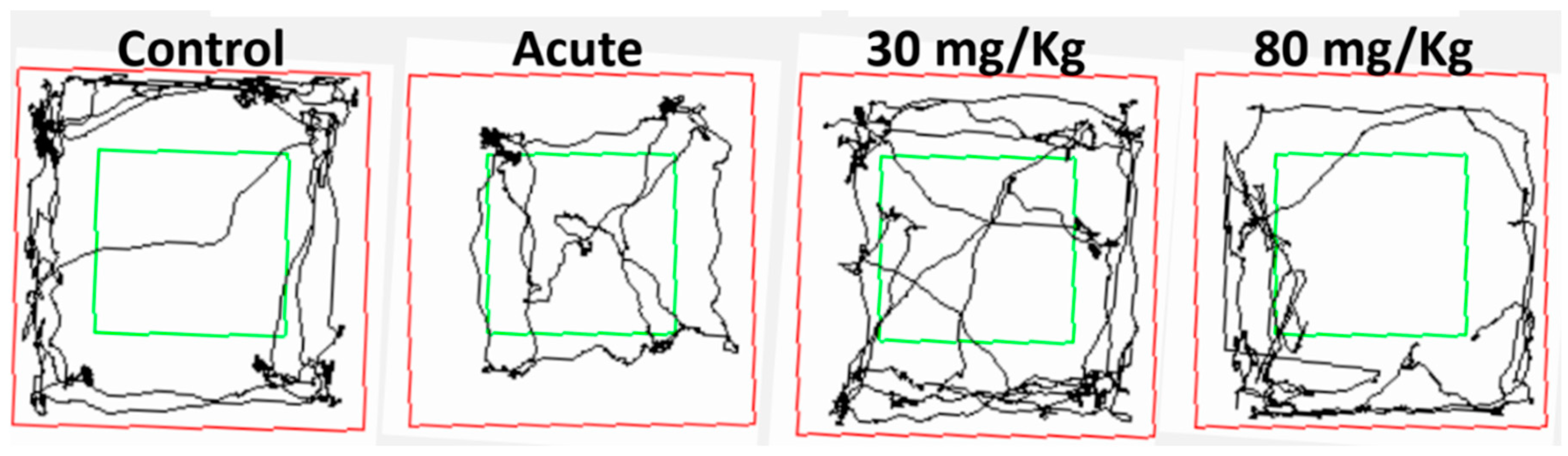
One-way ANOVA indicates no significant differences in the locomotor activity after LEO administration independently of the dose (Table 6A and Table 7) and protocol of administration (Table 6B and Table 8). Figure 4 shows the route of a representative animal from each experimental group.
Figure 4.
Illustration of the path taken during the Open-field test by one of the animals from each group. Performed using Smart 3.0 software.
Figure 4.
Illustration of the path taken during the Open-field test by one of the animals from each group. Performed using Smart 3.0 software.
4. Discussion
In the present study, we show clearly the anxiolytic effect of L. burnatii EO in rats, moreover, we presented evidence of an effective dose and two protocols of administration. Our findings were obtained using two validated tests for anxiety where the plus maze evaluates the fear of open spaces, the dark light test evaluates the aversion to illuminated spaces [31]. In this sense, we found that the dose of 30mg/kg induced a clear anxiolytic effect in the plus maze, observed as an increased time spent in the open arms, meanwhile, the higher dose showed no significant impact. Moreover, the lower dose was effective under the 7-days protocol, and no significant differences were observed with the acute administration. Similar results were obtained when the animals were evaluated in the dark light test. No significant difference was observed regarding the locomotor activity in either test, supporting the hypothesis that the difference is in the decreased fear/anxiety in the conflict test. This result is also supported by the open field evaluation showing no differences in the locomotor activity.
The results obtained in the present study are consistent with the data reported by Kumar (2013) [23], using L. angustifolia essential oil (Silexan®, standardized capsule formulation based on L. angustifolia EO) with the same dose and protocol of administration. Regarding the lack of an anxiolytic effect with the highest dose (80 mg/Kg), we can speculate that we are facing a dose-dependent response. In this sense, it has been described as the "U-shaped effect" for several drugs, where doses that are too high or too low may not cause any effect or even be harmful [33].
The beneficial effects of LEO on the central nervous system have been related to two of its main components, linalyl acetate and linalool. The results of Lopez and cols. [34] showed that L. angustifolia EO and its main therapeutic molecules (linalool and linalyl acetate) interact with glutamate receptors (NMDA), inhibiting them, and generating an anxiolytic effect. Other authors found similar results of LEO on the glutamatergic system [35,36,37,38]. Also, it has been reported that the hydroxyl group of linalool can bind to the serotonin transporter, which could explain the antidepressant effect reported in some works [39,40]. Moreover, it has been reported that Silexan® presents binding potential to serotonin-1A receptors, where its activity was significantly reduced after ingestion of LEO [41]. Schuwald et al. [42], using Silexan®, identified that the potent anxiolytic effect is due to the inhibition of voltage-gated calcium channels in synaptosomes, observed primary hippocampal neurons, and cell lines with stable overexpression. The same finding was confirmed with linalool in snail neurons, in addition to increasing potassium currents [43]. Other studies suggest that LEO reversibly inhibits GABA-induced signals. Milanos et al. [44] showed that only oxygenated metabolites of linalool at carbon 8 positively influence GABAergic currents, and hydroxylated or carboxylated derivatives at carbon 8 were ineffective, while acetylated derivatives of linalool did not produce significant changes, indicating that linalool metabolism reduces its allosteric potential at GABAA receptors compared to the original linalool molecule.
Finally, it is important to note that, according to a systematic analysis by Sattayakhom et al. [45] based on data from the MEDLINE, Scopus, and Google Scholar databases, 81.43% of EO studies have been conducted in human subjects, 18.57% in animal models, and only 1.43% in vitro cell cultures. Moreover, several of the scientific studies performed on both, animals and humans, showed significant methodological issues, such as small sample sizes, inconsistent administration methods, and a lack of placebo or control groups. In this sense, the data reported in the bibliography concerning subjects under study, the range of doses, protocols, and route of administration is wide and controversial [46,47]. We contribute to adding new systematic evidence regarding the effects of EO in the central nervous system; however, more standardized experiments are needed to confirm the benefits of lavender for brain disorders and to better understand its pharmacological and therapeutic potential.
Additionally, despite the pharmaceutical use of LEO in Europe, as far as we know, no evidence has been reported in Latin America; and the LEO formulation is not approved in all countries. In addition, we evaluated the effect of an acute dose, which had not been evaluated behaviorally until now, and we can infer from these results that repeated administration is required to observe a behavioral effect. For this reason, it becomes relevant to characterize a locally produced species of lavender thinking on a future formulation for regional use. In this sense, our study shows for the first time the therapeutic approach to L. burnatii, a Latin American endemic plant, proposing an effective dosage and administration protocol for future preclinical studies to contribute to systematic studies concerning lavender anxiolytic effects.
5. Conclusion
Our findings added new evidence supporting the previously described anxiolytic effects of LEO, highlighting the L. burnatii properties. However, further studies are still needed to determine a therapeutic dosage range, different protocol administration and the exact mechanism of action as well as possible adverse effects of LEO.
References
- Baxter, A. J., Scott, K. M., Vos, T., & Whiteford, H. A. (2013). Global prevalence of anxiety disorders: a systematic review and meta-regression. Psychological Medicine, 43(5), 897–910. [CrossRef]
- Kessler, R. C., Berglund, P., Demler, O., Jin, R., Merikangas, K. R., & Walters, E. E. (2005). Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593. [CrossRef]
- Alonso, J., Lépine, J.-P., & ESEMeD/MHEDEA 2000 Scientific Committee. (2007). Overview of key data from the European Study of the Epidemiology of Mental Disorders (ESEMeD). The Journal of Clinical Psychiatry, 68 Suppl 2, 3–9.
- Kessler, R. C. (2007). The global burden of anxiety and mood disorders: putting the European Study of the Epidemiology of Mental Disorders (ESEMeD) findings into perspective. The Journal of Clinical Psychiatry, 68 Suppl 2(Suppl 2), 10–19.
- Scott, K. M., Bruffaerts, R., Tsang, A., Ormel, J., Alonso, J., Angermeyer, M. C., Benjet, C., Bromet, E., de Girolamo, G., de Graaf, R., Gasquet, I., Gureje, O., Haro, J. M., He, Y., Kessler, R. C., Levinson, D., Mneimneh, Z. N., Oakley Browne, M. A., Posada-Villa, J., … von Korff, M. (2007). Depression–anxiety relationships with chronic physical conditions: Results from the World Mental Health surveys. Journal of Affective Disorders, 103(1–3), 113–120. [CrossRef]
- Mathew, S. J., Price, R. B., & Charney, D. S. (2008). Recent advances in the neurobiology of anxiety disorders: Implications for novel therapeutics. American Journal of Medical Genetics Part C: Seminars in Medical Genetics, 148C(2), 89–98. [CrossRef]
- McEvoy, P. M., Grove, R., & Slade, T. (2011). Epidemiology of Anxiety Disorders in the Australian General Population: Findings of the 2007 Australian National Survey of Mental Health and Wellbeing. Australian & New Zealand Journal of Psychiatry, 45(11), 957–967. [CrossRef]
- Kessler, R. C., Ruscio, A. M., Shear, K., & Wittchen, H.-U. (2010). Epidemiology of anxiety disorders. Current Topics in Behavioral Neurosciences, 2, 21–35.
- Stein, D. J., Scott, K. M., de Jonge, P., & Kessler, R. C. (2017). Epidemiology of anxiety disorders: from surveys to nosology and back. Dialogues in Clinical Neuroscience, 19(2), 127–136. [CrossRef]
- Toft, T., Fink, P., Oernboel, E., Christensen, K., Frostholm, L., & Olesen, F. (2005). Mental disorders in primary care: prevalence and co-morbidity among disorders. Results from the Functional Illness in Primary care (FIP) study. Psychological Medicine, 35(8), 1175–1184. [CrossRef]
- Nash, J. R., & Nutt, D. J. (n.d.). Pharmacotherapy of Anxiety. In Anxiety and Anxiolytic Drugs (pp. 469–501). Springer-Verlag. [CrossRef]
- Sarris, J., Panossian, A., Schweitzer, I., Stough, C., & Scholey, A. (2011). Herbal medicine for depression, anxiety and insomnia: A review of psychopharmacology and clinical evidence. European Neuropsychopharmacology, 21(12), 841–860. [CrossRef]
- Bakkali, F., Averbeck, S., Averbeck, D., & Idaomar, M. (2008). Biological effects of essential oils – A review. Food and Chemical Toxicology, 46(2), 446–475. [CrossRef]
- Setzer, W. N. (2009). Essential oils and anxiolytic aromatherapy. Natural Product Communications, 4(9), 1305–1316.
- Wheatley, D. (2005). Medicinal plants for insomnia: a review of their pharmacology, efficacy and tolerability. Journal of Psychopharmacology, 19(4), 414–421. [CrossRef]
- Brennan, S. E., McDonald, S., Murano, M., & McKenzie, J. E. (2022). Effectiveness of aromatherapy for prevention or treatment of disease, medical or preclinical conditions, and injury: protocol for a systematic review and meta-analysis. Systematic Reviews, 11(1), 148. [CrossRef]
- Farrar, A. J., & Farrar, F. C. (2020). Clinical Aromatherapy. Nursing Clinics of North America, 55(4), 489–504. [CrossRef]
- Sattayakhom, A., Wichit, S., & Koomhin, P. (2023). The Effects of Essential Oils on the Nervous System: A Scoping Review. Molecules, 28(9), 3771. [CrossRef]
- da Porto, C., Decorti, D., & Kikic, I. (2009). Flavour compounds of Lavandula angustifolia L. to use in food manufacturing: Comparison of three different extraction methods. Food Chemistry, 112(4), 1072–1078. [CrossRef]
- Community herbal monograph on Lavandula angustifolia Mill., aetheroleum., EMA/HMPC/143181/2010 ( http://www.ema.europa.eu/ema/ ).
- Bagheri-Nesami, M., Espahbodi, F., Nikkhah, A., Shorofi, S. A., & Charati, J. Y. (2014). The effects of lavender aromatherapy on pain following needle insertion into a fistula in hemodialysis patients. Complementary Therapies in Clinical Practice, 20(1), 1–4. [CrossRef]
- Antar, A., Abdel-Rehiem, E. S., Al-Khalaf, A. A., Abuelsaad, A. S. A., Abdel-Gabbar, M., Shehab, G. M. G., & Abdel-Aziz, A. M. (2024). Therapeutic Efficacy of Lavandula dentata’s Oil and Ethanol Extract in Regulation of the Neuroinflammation, Histopathological Alterations, Oxidative Stress, and Restoring Balance Treg Cells Expressing FoxP3+ in a Rat Model of Epilepsy. Pharmaceuticals, 18(1), 35. [CrossRef]
- Kumar, V. (2013). Characterization of anxiolytic and neuropharmacological activities of Silexan. Wiener Medizinische Wochenschrift, 163(3–4), 89–94. [CrossRef]
- Xiong, M., Li, Y., Tang, P., Zhang, Y., Cao, M., Ni, J., & Xing, M. (2018). Effectiveness of Aromatherapy Massage and Inhalation on Symptoms of Depression in Chinese Community-Dwelling Older Adults. The Journal of Alternative and Complementary Medicine, 24(7), 717–724. [CrossRef]
- Vidal-García, E., Vallhonrat-Bueno, M., Pla-Consuegra, F., & Orta-Ramírez, A. (2024). Efficacy of Lavender Essential Oil in Reducing Stress, Insomnia, and Anxiety in Pregnant Women: A Systematic Review. Healthcare, 12(23), 2456. [CrossRef]
- Solomon, D. A., Prasad, N., Beautily, V., Thenmozhi, P., Madaswamy, R., & Deepika, D. (2024). Effect of Lavender Oil on Social Anxiety Among First-Year College Students. Journal of Pharmacy and Bioallied Sciences, 16(Suppl 3), S2907–S2909. [CrossRef]
- Marchevsky, S. (2024). Real-world outcomes of long-term use of silexan in patients with anxiety disorders: a single-centre experience. International Journal of Psychiatry in Clinical Practice, 28(2), 138–141. [CrossRef]
- Faustino, T. T., Almeida, R. B. de, & Andreatini, R. (2010). Plantas medicinais no tratamento do transtorno de ansiedade generalizada: uma revisão dos estudos clínicos controlados. Revista Brasileira de Psiquiatria, 32(4), 429–436. [CrossRef]
- Wagner, J. K., Gambell, E., Gibbons, T., Martin, T. J., & Kaplan, J. S. (2024). Sex Differences in the Anxiolytic Properties of Common Cannabis Terpenes, Linalool and β-Myrcene, in Mice. NeuroSci, 5(4), 635–649. [CrossRef]
- Batiha, G. E.-S., Teibo, J. O., Wasef, L., Shaheen, H. M., Akomolafe, A. P., Teibo, T. K. A., Al-kuraishy, H. M., Al-Garbeeb, A. I., Alexiou, A., & Papadakis, M. (2023). A review of the bioactive components and pharmacological properties of Lavandula species. Naunyn-Schmiedeberg’s Archives of Pharmacology, 396(5), 877–900. [CrossRef]
- File, S. E., Lippa, A. S., Beer, B., & Lippa, M. T. (2004). Animal Tests of Anxiety. Current Protocols in Neuroscience, 26(1). [CrossRef]
- SMART v3.0.03 (Panlab Harvard Apparatus).
- Shustorovich, A., Corroon, J., Wallace, M. S., & Sexton, M. (2024). Biphasic effects of cannabis and cannabinoid therapy on pain severity, anxiety, and sleep disturbance: a scoping review. Pain Medicine, 25(6), 387–399. [CrossRef]
- López, V., Nielsen, B., Solas, M., Ramírez, M. J., & Jäger, A. K. (2017). Exploring Pharmacological Mechanisms of Lavender (Lavandula angustifolia) Essential Oil on Central Nervous System Targets. Frontiers in Pharmacology, 8. [CrossRef]
- Elisabetsky, E., Marschner, J., & Onofre Souza, D. (1995). Effects of linalool on glutamatergic system in the rat cerebral cortex. Neurochemical Research, 20(4), 461–465. [CrossRef]
- Elisabetsky, E., Silva Brum, L. F., & Souza, D. O. (1999). Anticonvulsant properties of linalool in glutamate-related seizure models. Phytomedicine, 6(2), 107–113. [CrossRef]
- Silva Brum, L. F., Emanuelli, T., Souza, D. O., & Elisabetsky, E. (2001). Effects of Linalool on Glutamate Release and Uptake in Mouse Cortical Synaptosomes. Neurochemical Research, 26(3), 191–194. [CrossRef]
- Aprotosoaie, A. C., Hăncianu, M., Costache, I., & Miron, A. (2014). Linalool: a review on a key odorant molecule with valuable biological properties. Flavour and Fragrance Journal, 29(4), 193–219. [CrossRef]
- Hritcu, L., Cioanca, O., & Hancianu, M. (2012). Effects of lavender oil inhalation on improving scopolamine-induced spatial memory impairment in laboratory rats. Phytomedicine, 19(6), 529–534. [CrossRef]
- Akhondzadeh, S., Kashani, L., Fotouhi, A., Jarvandi, S., Mobaseri, M., Moin, M., Khani, M., Jamshidi, A. H., Baghalian, K., & Taghizadeh, M. (2003). Comparison of Lavandula angustifolia Mill. tincture and imipramine in the treatment of mild to moderate depression: a double-blind, randomized trial. Progress in Neuro-Psychopharmacology and Biological Psychiatry, 27(1), 123–127. [CrossRef]
- Baldinger, P., Hoflich, A. S., Mitterhauser, M., Hahn, A., Rami-Mark, C., Spies, M., Wadsak, W., Lanzenberger, R., & Kasper, S. (2015). Effects of Silexan on the Serotonin-1A Receptor and Microstructure of the Human Brain: A Randomized, Placebo-Controlled, Double-Blind, Cross-Over Study with Molecular and Structural Neuroimaging. International Journal of Neuropsychopharmacology, 18(4), pyu063–pyu063. [CrossRef]
- Schuwald, A. M., Nöldner, M., Wilmes, T., Klugbauer, N., Leuner, K., & Müller, W. E. (2013). Lavender Oil-Potent Anxiolytic Properties via Modulating Voltage Dependent Calcium Channels. PLoS ONE, 8(4), e59998. [CrossRef]
- Vatanparast, J., Bazleh, S., & Janahmadi, M. (2017). The effects of linalool on the excitability of central neurons of snail Caucasotachea atrolabiata. Comparative Biochemistry and Physiology Part C: Toxicology & Pharmacology, 192, 33–39. [CrossRef]
- Milanos, S., Elsharif, S. A., Janzen, D., Buettner, A., & Villmann, C. (2017). Metabolic Products of Linalool and Modulation of GABAA Receptors. Frontiers in Chemistry, 5. [CrossRef]
- Sattayakhom, A., Wichit, S., & Koomhin, P. (2023). The Effects of Essential Oils on the Nervous System: A Scoping Review. Molecules, 28(9), 3771. [CrossRef]
- Umezu, T., Nagano, K., Ito, H., Kosakai, K., Sakaniwa, M., & Morita, M. (2006). Anticonflict effects of lavender oil and identification of its active constituents. Pharmacology Biochemistry and Behavior, 85(4), 713–721. [CrossRef]
- Aboutaleb, N., Jamali, H., Abolhasani, M., & Pazoki Toroudi, H. (2019). Lavender oil (Lavandula angustifolia) attenuates renal ischemia/reperfusion injury in rats through suppression of inflammation, oxidative stress and apoptosis. Biomedicine & Pharmacotherapy, 110, 9–19. [CrossRef]

Table 1.
Lavandula burnatii essential oil characterization.
| LEO compound | Percentage of the sample (%) |
|---|---|
| Linalool | 25,18 |
| Linalyl acetate | 26,15 |
| Camphor | 10,03 |
| Cineole | 8,45 |
| Borneol | 3,81 |
| Lavandulyl acetate | 3,42 |
| Caryophyllene | 2,60 |
| Limonene | 1,63 |
| β-Farnecene | 1,35 |
| β-Ocimene | 1,26 |
| 4-Terpineol | 0,85 |
| α-Terpineol | 0,42 |
| Eugenol | 0,20 |
Table 2.
A.
| Dose - time in open arms | ||
| One-way ANOVA | ||
| F = 24.67 | P < 0.0001 | |
| Tukey's multiple comparisons test | p | |
| "Control group" vs. "30 mg/Kg of LEO" | <0.0001 | |
| "Control group" vs. "80 mg/Kg of LEO" | 0.6569 | |
| "30 mg/Kg of LEO" vs. "80 mg/Kg of LEO" | <0.0001 | |
Table 2.
B.
| Dose - time in closed arms | ||
| One-way ANOVA | ||
| F = 2.694 | P = 0.0880 | |
| Tukey's multiple comparisons test | p | |
| "Control group" vs. "30 mg/Kg of LEO" | 0.5352 | |
| "Control group" vs. "80 mg/Kg of LEO" | 0.4424 | |
| "30 mg/Kg of LEO" vs. "80 mg/Kg of LEO" | 0.0722 | |
Table 3.
A.
| Protocol administration - time in open arms | ||
| One-way ANOVA | ||
| F = 10.21 | P = 0.0006 | |
| Tukey's multiple comparisons test | p | |
| "Control group" vs. "Acute" | 0.9117 | |
| "Control group" vs. "7-day" | 0.0011 | |
| "Acute" vs. "7-day" | 0.0032 | |
Table 3.
B.
| Protocol administration - time in closed arms | ||
| One-way ANOVA RM | ||
| F = 0.4200 | P = 0.6618 | |
| Tukey's multiple comparisons test | p | |
| "Control group" vs. "Acute" | 0.7686 | |
| "Control group" vs. "7-day" | 0.6671 | |
| "Acute" vs. "7-day" | 0.9842 | |
Table 4.
A.
| Dose - time in the illuminated area | ||
| One-way ANOVA | ||
| F = 8.040 | P = 0.0026 | |
| Tukey's multiple comparisons test | p | |
| "Control group" vs. "30 mg/Kg of LEO" | 0.0069 | |
| "Control group" vs. "80 mg/Kg of LEO" | 0.9947 | |
| "30 mg/Kg of LEO" vs. "80 mg/Kg of LEO" | 0.0055 | |
Table 4.
B.
| Dose - total entries | ||
| One-way ANOVA | ||
| F = 0.3463 | P = 0.7111 | |
| Tukey's multiple comparisons test | p | |
| "Control group" vs. "30 mg/Kg of LEO" | 0.8095 | |
| "Control group" vs. "80 mg/Kg of LEO" | 0.7106 | |
| "30 mg/Kg of LEO" vs. "80 mg/Kg of LEO" | 0.9794 | |
Table 5.
A.
| Protocol administration - time in the illuminated area | ||
| One-way ANOVA | ||
| F = 6.225 | P = 0.0069 | |
| Tukey's multiple comparisons test | p | |
| "Control group" vs. "Acute" | 0.8887 | |
| "Control group" vs. "7-day" | 0.0104 | |
| "Acute" vs. "7-day" | 0.0246 | |
Table 5.
B.
| Protocol administration - total entries | ||
| One-way ANOVA | ||
| F = 0.3188 | P = 0.7302 | |
| Tukey's multiple comparisons test | p | |
| "Control group" vs. "Acute" | 0.7231 | |
| "Control group" vs. "7-day" | 0.8323 | |
| "Acute" vs. "7-day" | 0.9784 | |
Table 6.
A.
| Dose - ambulation | ||
| One-way ANOVA | ||
| F = 0.3647 | P =0.6987 | |
| Tukey's multiple comparisons test | p | |
| "Control group" vs. "30 mg/Kg of LEO" | 0.7774 | |
| "Control group" vs. "80 mg/Kg of LEO" | 0.7147 | |
| "30 mg/Kg of LEO" vs. "80 mg/Kg of LEO" | 0.9937 | |
Table 6.
B.
| Protocol administration - ambulation | ||
| One-way ANOVA | ||
| F =1.603 | P = 0.2239 | |
| Tukey's multiple comparisons test | p | |
| "Control group" vs. "Acute" | 0.2046 | |
| "Control group" vs. "7-day" | 0.7961 | |
| "Acute" vs. "7-day" | 0.5246 | |
Table 7.
Effect of Lavandula burnatii essential oil in Open-field test. This table indicates the total ambulation in the open field (cm) with different doses ( 30 and 80 mg/Kg). No significant differences were observed between the experimental groups. N=8-10 in each group. Values are mean±SEM.
Table 7.
Effect of Lavandula burnatii essential oil in Open-field test. This table indicates the total ambulation in the open field (cm) with different doses ( 30 and 80 mg/Kg). No significant differences were observed between the experimental groups. N=8-10 in each group. Values are mean±SEM.
| Treatment | Dose (mg/Kg) | Ambulation (cm) | |
| Vehicle | 1754 ± 116,2 | ||
| LEO | 30 | 1611 ± 183,3 | |
| LEO | 80 | 1589 ± 136,9 |
Table 8.
Effect of Lavandula burnatii essential oil in Open-field test. Indicates the total ambulation in the open field (cm) with different protocol administration ( acute and 7-day administration). No significant differences were observed between the experimental groups. N=8-10 in each group. Values are mean±SEM.
Table 8.
Effect of Lavandula burnatii essential oil in Open-field test. Indicates the total ambulation in the open field (cm) with different protocol administration ( acute and 7-day administration). No significant differences were observed between the experimental groups. N=8-10 in each group. Values are mean±SEM.
| Treatment | Dose (mg/Kg) | Ambulation (cm) | |
| Vehicle | 1754 ± 116,2 | ||
| LEO-Acute | 30 | 1376 ± 150,8 | |
| LEO- 7 day | 30 | 1611 ± 183,3 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



