
Submitted:
29 March 2025
Posted:
31 March 2025
You are already at the latest version
Abstract
Emergency Department (ED) Triage is the cornerstone of ED operations. Many different triage systems have been proposed and implemented globally. To date an ideal triage system has not been identified. As the burden on ED’s rises with overcrowding being recognized as a universal problem ED triage needs to restructure to address this reality.
Extensive and critical of the literature has identified the strengths and weaknesses of current ED triage implementations. A novel multi-layer triage system was introduced and implemented in Greek ED's combining the strengths of various triage and Early Warning Systems and scores, in an effort to minimize under-triage and the adverse downstream effects that in creates on patient outcomes. In its years of implementation, it has proven to be fast, accurate, objective, and reproducible.
Acknowledging that no triage system can be universally adapted in different settings, that the structural concepts of this triage system address most of the triage problems currently reported in the literature.
Keywords:
Triage
; Early Warning Scores
; ESI
; NEWS
; HEART
; Emergency Department
1. Introduction
Emergency department (ED) overcrowding is a global phenomenon that delays diagnostic and therapeutic interventions [8]. This time delay might crucially affect patient outcomes [1]. As ED patient volumes increase, and even more people endure constantly prolonging waiting times an accurate triage system becomes vital.
Hospital Triage is a process through which healthcare professionals actively try to identify high-acuity patients and prioritize them accordingly. These patients range from critically ill in need of immediate life-saving interventions to patients with minor medical problems and low urgency. The majority of the ED population lie in between these two extremes. Both over-triage and under-triage have a negative impact on ED flow and patient waiting times. Under-triage might leave a critical patient in the waiting room for a prolonged period of time leading to severe deterioration. Over-triage will foverflow the treatment area with lower acuity patients consuming all available treatment places and resources and thus preventing higher acuity patients from entering timely and prolonging their time in the waiting area.
Each healthcare system and even each Emergency Department has developed a triage system most fitting to their specific needs. Whatever triage system is chosen, it must meet the following requirements: it must be useful, valid and reproducible. It must also be easy to use and classify, to help medical staff determine the level of triage in the shortest possible time [7,8].
The Emergency Department of Nikaia General Hospital, Nikaia, Greece is the busiest ED in Greece with more than 1000 ED visits in a 24-hour shift. The Emergency department of Larisa General Hospital, Greece has more than 300 ED-visits in a 24-hour shift. This overflow of incomings combined with other structural vulnerabilities of the Greek emergency health care system lead to prolonged waiting times from triage to physician with right to treat, that in some cases may exceed 6 hours. In 2018 we restructured our adult patient triage protocols, introducing a multi-layer triage approach based on the Swiss cheese model[34] (Figure 1). Our goal was to combine the strengths of accredited triage and early warning systems and scores to produce a process that would ensure that prolonged waiting times would not have a negative impact on patient outcomes [33].
Based on these principles, the Hellenic Society for Emergency Medicine developed in 2024 a National Triage Proposal [11].
2. Evaluating Existing Scoring Systems
Existing scoring systems can be roughly divided into three main categories.
a. Symptom Based Triage Systems—Clinical Impression Triage Systems
The most widely used triage systems in this category are the Manchester Triage system (MTS), the Australasian triage system (ATS), the Emergency Severity Index (ESI) and the Canadian Triage and Acuity Scale (CTAS). These 5-tier scoring systems, are all well validated and widely adopted in ED’s globally.
The outlines of each triage system are presented in Table 1.
There is still no clear advantage of one triage system over another [8,10,12].
Triage accuracy by all the above systems ranges between 56% and 87% [2]. All define very precisely and concordantly the highest (1 and 2) and the lowest (5) priorities, while assigning priorities to the intermediate categories (3 and 4) was less precise for adult population [8]. ESI has been reported to have a 20%-30% under-tirage rate even for high acuity patients [4,6,9,13,14]. In our setting when using ESI alone accuracy was calculated at 63%, with an overall 23,6% under-triage rate [3]. Interpretation of vital sign deterioration has been identified as one of the factors leading to under-triage when using the ESI [5].
Summarizing the strengths of symptom-based triage systems are validated, fast, simple and reliable for higher acuity patients (Priority 1 and Priority 2) and very low acuity patients (Priority 5). Their weaknesses include a high percentage of under-triage even for high acuity patients. They remain mainly subjective (depending on the level of training of the triage personnel) and thus not reproducible.
We chose to implement the ESI triage system mainly because there are no preset response times for each triage category and it fit better with our practice and policies so far. By choosing ESI almost 80% of our high acuity patients and our very low acuity patients should be identified quickly and accurately. A second triage layer would be needed to find these under-triaged critically ill patients and sort out medium and low acuity patients. Since ESI is not symptom based, we added a number of critical presenting symptom clusters from MTS, ATS and CTAS as “Red Flag” symptoms to be recognized and prioritized accordingly.
b. Early Warning Scores (EWS)
Early warning scores are based on the concept that altered physiology often precedes patient deterioration and death. Derangements in simple physiological observations (vital signs) can identify patients at high risk of deterioration. By recording and grading multiple parameters simultaneously, subtle changes in vital signs can be used to initiate early emergency management [16,17]. Most widespread are the Rapid Acute Physiology Score (RAPS), Modified EWS (MEWS), Modified EWS with Glascow Coma Scale (GCS) (MEWS GCS), Rapid Emergency Medicine Score (REMS), Goodacre Score, Worthing Physiological Score (WPS), Groarke Score, VitalPac EWS (ViEWS), Abbreviated VitalPac EWS (AbViEWS), Glasgow Coma Scale-Age-Systolic Blood Pressure Score, Vital Sign Score (VSS), National EWS (NEWS) and Vital Sign Group (VSG) Scores.
Early warning scores can accurately predict outcomes in a number of different populations [18,21]. They have been found to be excellent predictors of cardiac arrest, ICU transfer and death on ICU, mortality within 2-days, deterioration within 2-days, and hospital admissions [18,19]. Among their advantages are accuracy, cross specialty application, impact on communication and opportunity for automation[19]. Their weak points are Sensitivity, especially compared to specialty-specific scores, Need for practitioner engagement, and need for clinical judgment.
EWS have been proposed as Emergency Department Triage tools[21]. EWS Triage outperforms symptom-based triage in high acuity patient recognition and risk stratification of mid acuity patients [20].
As there is no clear advantage to one EWS system over another [18] we have chosen to integrate NEWS 2 into our multi-layer triage system. NEWS 2 is simple, easy to use and reproducible. The vital signs are recorded on the table chart and the score is calculated (Figure 2). Once the NEWS 2 score is calculated appropriate response triggers are provided by the Royal College of Physicians (Figure 3)[22,23].
Summarizing. NEWS 2 is a validated and easy to use score[24]. By choosing to add NEWS 2 as a second layer in our triage process, we address vital signs interpretation that was one of the most common error points in the triage systems mentioned above. We decrease the probability of under-triaging high acuity patients as NEWS 2 has a better sensitivity in detecting high acuity patients that have been under triaged in the previous step. By using the integrated thresholds and triggers, patients can subjectively and reproducibly be further triaged as middle and low acuity. Adding this layer slightly prolongs the triage process. This time delay will have a minimal impact in patient outcomes as the Priority 1 and Priority 2 patients that need immediate treatment have already been transferred to the treatment area by using ESI.
c. Specific Disease Scores
Time sensitive, high mortality conditions might have atypical [25] or confusing presentations[26,27] on arrival, and minimal vital signs deterioration. Both Acute Coronary Syndromes (ACS) and Stokes are among the leading causes of death and disability and early recognition and timely intervention is critical. As stated earlier, EWS underperform compared to specialty-specific scores[28]. To detect these patients that have slipped through the first two triage layers an extra layer is added consisting of disease specific scores.
Many scores are in use to help identify patients with these conditions promptly and accurately. Most commonly used to detect ACS are the Thrombosis in Myocardial Infarction risk (TIMI) score, Global Registry of Acute Coronary Events (GRACE) score, The HEART score. Likewise the National Institutes of Health Stroke Scale (ΝΙHSS), Cincinnati Prehospital Stroke Severity Scale (CPSSS), Rapid Arterial Occlusion Evaluation (RACE), Face Arm Speech Test (FAST), Medic Prehospital Assessment for Code Stroke (MedPACS), Recognition of Stroke in the Emergency Room (ROSIER) are used for the early recognition of stroke.
The HEART score seems to perform better that other scores in detecting ACS [29,30]. In the mnemonic HEART, each letter corresponds to a key piece of the evaluation for patients with chest pain: History, ECG, Age, Risk factors, and Troponin. Each component was scored on a scale of 0–2, with total scores ranging between 0–10 (Figure 4). The calculated score corresponds to the short term probability of a major adverse cardiovascular event (MACE) and appropriate action is recommended[36] (Figure 5).
For detecting stroke in the Emergency Department In the ROSIER could be the test of choice, as it has been well evaluated and showed consistently high sensitivity[31,32]. The ROSIER scale is a 7-item stroke recognition instrument employing clinical history and neurological signs, ranging from-2 to +5. A score of +1 or higher indicates a positive diagnosis of stroke or transient ischemic attack (TIA). The scale encompasses assessment criteria such as loss of consciousness, seizure activity, asymmetric facial, arm, and leg weakness, speech disturbance, and visual field deficit. (Figure 6).
Summarizing. Adding ROSIER and HEART score as an extra layer to our triage process minimizes the chance of under triaging a life threatening, time sensitive disease. In order to perform these scores certain blood tests are necessary. Blood glucose levels and troponin are essential parts of the algorithm. These creates certain logistic needs (Point on care devices, blood sampling, personnel etc) that have a great impact on triage time. Depending on the setup, this might take from 10 to 30 minutes. In departments like ours with long waiting times there is a clear benefit as under-triaged patients might lose their therapeutic window. The number of patients that end at this arm of our triage process is small and has minimal effect on door to triage time for new incomings.
3. Proposing a Multilayer Triage System
Having an in depth understanding of our Emergency Departments strengths and weaknesses and experience on conducting Triage by ESI alone we had identified areas of improvement of our triage process. Prior to introducing our institutional multilayer triage (Figure 7) system an extensive and critical review of the literature was conducted. We combined the strong points of each score to better fit our needs. ESI would quickly and accurately identify the majority of very high acuity patients (Priority 1). ESI along with specific symptom clusters from ATS, MTS and CTAS “Red flags” were used to identify quickly and accurately our high acuity patients (Priority 2). Acknowledging that almost 20% of Priority 1 and 2 patients might be under-triaged by ESI we introduced NEWS 2 score as a second layer. Besides increasing our priority 1 and 2 detection rate this addition also helped in better interpretation of vital signs, objective and reproducible allocation of priority 3 and priority 4 patients. As an added benefit, it created an objective benchmark to which the patient’s improvement or deterioration over time and response to treatment could be compared. ACS and Stroke detection where a priority and a third layer consisting of Rosier and HEART score was added allocating patients to priority 2 or 3 or 4. Those patients who at the end of the triage process were characterized as low acuity where prioritized as priority 4 or priority 5 according to the estimated extent of investigation needed according to combined elements of the ESI (resources) and CTAS (age and comorbidities). Table 2 summarizes our priority allocation tools and scheme 1 depicts our triage process.
-
Seeking Priority 1 patients – Clinical impression
- Use the basic principles of clinical impression triage systems such as ESI
- “Is there immediate risk for life or limb?”
- If the answer is YES the patient is Priority 1
- In the answer is NO proceed to the next step
-
Seeking Priority 2 Patients – Basic History taking and clinical impression
- Use the basic principles of clinical impression triage systems such as ESI
- “Is patient’s condition serious enough or deteriorating so rapidly that there is the potential of threat to life, or organ system failure?”
- “Is the patient in severe pain?”
- “Does the patient have altered mental status?”
- “Are there any “Red Flags”?” CTAS, ATS, MTS
- If the answer is YES to any of the above questions, the Patient is Priority 2
- If the answer is NO proceed to the next step
-
Are you sure the Patient is NOT Priority 1 or 2 ? – Vital signs
- Use NEWS 2 to interpret vital signs
-
Prioritize patient according to the EWS you have chosen
- NEWS2 Score > 7 the patient is priority 2
- NEWS2 Score 5-6 or red score of 3 in any individual parameter, the patient is priority 3
- NEWS2 Score 0-4 Proceed to the next step
-
Could the patient have an atypical presentation of a time-sensitive disease? – Disease specific scores
- Use one of the accredited disease-specific scores depending on the clinical question.
- Prioritize the patient according to the score you have chosen.
-
Use the HEART score for a possible ACS
- For a HEART score 7-10 the patient is priority 2
- For a HEART score between 4-6 the patient is priority 3
- For a HEART score 0-3 proceed to the next step
-
Use Rosier score for a possible stroke
- For Rosier >1 the patient is priority 2
- For Rosier < 0 proceed to the next step
-
Will this patient require extensive work-up? – Focused history taking
- Use the basic principles of clinical impression triage systems such as ESI, CTAS
- “Will the patient, due to his age or comorbidities, require extensive work-up?”
- If the answer is YES the patient is Priority 4
- If the answer is NO the Patient is Priority 5.
4. Results
Having implemented this multi-layer triage system for our adult population for more than 3 years we have had almost no critical events in the waiting room. Less than 5% of patients in the waiting room will need to change to a higher priority category while waiting. There is a very high level of agreement of the triage category between triage personnel of different training backgrounds. Although not systematically recorded over triage is bellow 15%. Our average triage time remains at 10 minutes. Even for the most complex arms of the chart triage time never exceeds 25 minutes without prolonging our door to triage time. Having created an objective and reproducible system training, reviewing and quality control have become easier. More recently we have created and started implementing an artificial intelligence decision assistance tool built on these parameters.
Re-structuring the triage process alone has had multiple downstream effects with a positive impact on triage accuracy. A structured training program was implemented for triage personnel. Constant and systematic training of triage personnel has been shown to have a clear impact on triage quality. Our Triage training program is being gradually adopted across Greece. Due to the new triage system, charting and recording had to be re-structured. Complete charting and strict adherence to the triage process have been identified as major contributors to high-quality triage. Re-triage at set time intervals was introduced as part of the quality control of the multilayer triage system. This created a re-Triage culture that has remained. Even during our initial needs assessment and planning of the triage system, a number of ED throughput issues were identified and addressed accordingly.
5. Conclusion
Triage is the most vital part of ED operations and can have a great impact on ED flow and patient outcomes. The perfect triage system does not exist. Comparing different triage models is very difficult as this is a multi-factorial process depending on input and output of patients, ED resources, staffing and hospital capabilities, training background of triage personnel etc. Each Emergency Department must clearly identify it’s own needs and tailor a triage process to fulfill them.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- FitzGerald G, Jelinek GA, Scott D, Gerdtz MF. Emergency department triage revisited. Emerg Med J. 2010;27:86–92.
- Tam HL, Chung SF, Lou CK. A review of triage accuracy and future direction. BMC Emerg Med. 2018; 20;18(1):58. PMID: 30572841; PMCID: PMC6302512. [CrossRef]
- El-Fellah N., Dritsa A., Dermatis P., Intas G., Papadopoulos G., Kaklamanou E., Tsiftsis D., “Knowledge of Health Care Professionals of the Emergency Department of the Hospital of N. Attica in the Emergency Severity Index Triage System”. Hellenic Journal of Nursing. 2017;56(4)358-365 (Article in Greek).
- Storm-Versloot MN, Ubbink DT, Kappelhof J, Luitse JS. Comparison of an informally structured triage system, the emergency severity index, and the manchester triage system to distinguish patient priority in the emergency department. Acad Emerg Med. 2011 Aug;18(8):822-9. PMID: 21843217. [CrossRef]
- Rashid K, Ullah M, Ahmed ST, Sajid MZ, Hayat MA, Nawaz B, Abbas K. Accuracy of Emergency Room Triage Using Emergency Severity Index (ESI): Independent Predictor of Under and Over Triage. Cureus. 2021 Dec 7;13(12):e20229. PMID: 35004046; PMCID: PMC8730791. [CrossRef]
- Mistry B, Stewart De Ramirez S, Kelen G, Schmitz PSK, Balhara KS, Levin S, Martinez D, Psoter K, Anton X, Hinson JS. Accuracy and Reliability of Emergency Department Triage Using the Emergency Severity Index: An International Multicenter Assessment. Ann Emerg Med. 2018 May;71(5):581-587.e3. Epub 2017 Nov 24. PMID: 29174836. [CrossRef]
- Alonso PS. “Comparative analysis of global triage systems: Competencies of nursing and hospital and prehospital application”. Journal Nursing Valencia 2024,1-31. ISSN 2952-3192.
- Ingielewicz A, Rychlik P, Sieminski M. Drinking from the Holy Grail-Does a Perfect Triage System Exist? And Where to Look for It? J Pers Med. 2024 May 31;14(6):590. PMID: 38929811; PMCID: PMC11204574. [CrossRef]
- Sax DR, Warton EM, Mark DG, Vinson DR, Kene MV, Ballard DW, Vitale TJ, McGaughey KR, Beardsley A, Pines JM, Reed ME; Kaiser Permanente CREST (Clinical Research on Emergency Services & Treatments) Network. Evaluation of the Emergency Severity Index in US Emergency Departments for the Rate of Mistriage. JAMA Netw Open. 2023 Mar 1;6(3):e233404. Erratum in: JAMA Netw Open. 2024 Jun 3;7(6):e2423536. doi: 10.1001/jamanetworkopen.2024.23536. PMID: 36930151; PMCID: PMC10024207. [CrossRef]
- Kuriyama A, Urushidani S, Nakayama T. Five-level emergency triage systems: variation in assessment of validity. Emerg Med J. 2017 Nov;34(11):703-710. Epub 2017 Jul 27. PMID: 28751363. [CrossRef]
- Gatsouli M., Gerakari S., Ivkovitz Z., Intas G., Kalogridaki M,. Karametos I., Lymperopoulou D., Pantazopoulos I., Paylidou E., Stavroulakis S., Notas G., Editors Tsiftsis D., Notas G., Peitsidou E., Dermatis P., Kitsakos A., Bampalis D., Tsikrika M. “Proposal of the Hellenic Society for Emergency Medicine for the pilot implementation of a National triage system in sites providing emergency care services” (Article in Greek) available on-line at https://www.hesem.gr/%cf%80%cf%81%cf%8c%cf%84%ce%b1%cf%83%ce%b7-%ce%b5%ce%bb%ce%bb%ce%b7%ce%bd%ce%b9%ce%ba%ce%ae%cf%82-%ce%b5%cf%84%ce%b1%ce%b9%cf%81%ce%b5%ce%af%ce%b1%cf%82-%ce%b5%cf%80%ce%b5%ce%af%ce%b3%ce%bf%cf%85/.
- Christ M, Grossmann F, Winter D, Bingisser R, Platz E. Modern triage in the emergency department. Dtsch Arztebl Int. 2010 Dec;107(50):892-8. Epub 2010 Dec 17. PMID: 21246025; PMCID: PMC3021905. [CrossRef]
- Zachariasse JM, van der Hagen V, Seiger N, Mackway-Jones K, van Veen M, Moll HA. Performance of triage systems in emergency care: a systematic review and meta-analysis. BMJ Open. 2019 May 28;9(5):e026471. PMID: 31142524; PMCID: PMC6549628. [CrossRef]
- Suamchaiyaphum K, Jones AR, Polancich S. The accuracy of triage classification using Emergency Severity Index. Int Emerg Nurs. 2024 Dec;77:101537. Epub 2024 Nov 10. PMID: 39527884. [CrossRef]
- Peta D, Day A, Lugari WS, Gorman V, Ahayalimudin N, Pajo VMT. Triage: A Global Perspective. J Emerg Nurs. 2023 Nov;49(6):814-825. PMID: 37925222. [CrossRef]
- Goldhill DR, McNarry AF. Physiological abnormalities in early warning scores are related to mortality in adult inpatients. British Journal of Anaesthesia. 2004;92(6):882-4.
- Ridley S. The recognition and early management of critical illness. Annals of the Royal College of Surgeons of England. 2005;87(5):315-22.
- Spencer W, Smith J, Date P, de Tonnerre E, Taylor DM. Determination of the best early warning scores to predict clinical outcomes of patients in the emergency department. Emerg Med J. 2019 Dec;36(12):716-721. Epub 2019 Jul 31. PMID: 31366627. [CrossRef]
- Downey CL, Tahir W, Randell R, Brown JM, Jayne DG. Strengths and limitations of early warning scores: A systematic review and narrative synthesis. Int J Nurs Stud. 2017 Nov;76:106-119. Epub 2017 Sep 13. PMID: 28950188. [CrossRef]
- Schinkel M, Bergsma L, Veldhuis LI, Ridderikhof ML, Holleman F. Comparing complaint-based triage scales and early warning scores for emergency department triage. Emerg Med J. 2022 Sep;39(9):691-696. Epub 2022 Apr 13. PMID: 35418407; PMCID: PMC9411919. [CrossRef]
- Kramer AA, Sebat F, Lissauer M. A review of early warning systems for prompt detection of patients at risk for clinical decline. J Trauma Acute Care Surg. 2019 Jul;87(1S Suppl 1):S67-S73. PMID: 31246909. [CrossRef]
- Williams B. The National Early Warning Score: from concept to NHS implementation. Clin Med (Lond). 2022 Nov;22(6):499-505. PMID: 36427887; PMCID: PMC9761416. [CrossRef]
- Royal College of Physicians. National Early Warning Score (NEWS) 2: Standardising the assessment of acute-illness severity in the NHS. Updated report of a working party. London: RCP, 2017.
- Smith GB, Prytherch DR, Meredith P, Schmidt PE, Featherstone PI. The ability of the National Early Warning Score (NEWS) to discriminate patients at risk of early cardiac arrest, unanticipated intensive care unit admission, and death. Resuscitation. 2013 Apr;84(4):465-70. Epub 2013 Jan 4. PMID: 23295778. [CrossRef]
- Khan IA, Karim HMR, Panda CK, Ahmed G, Nayak S. Atypical Presentations of Myocardial Infarction: A Systematic Review of Case Reports. Cureus. 2023 Feb 26;15(2):e35492. PMID: 36999116; PMCID: PMC10048062. [CrossRef]
- Vilela P. Acute stroke differential diagnosis: Stroke mimics. Eur J Radiol. 2017 Nov;96:133-144. Epub 2017 May 5. PMID: 28551302. [CrossRef]
- Pohl M, Hesszenberger D, Kapus K, Meszaros J, Feher A, Varadi I, Pusch G, Fejes E, Tibold A, Feher G. Ischemic stroke mimics: A comprehensive review. J Clin Neurosci. 2021 Nov;93:174-182. Epub 2021 Sep 20. PMID: 34656244. [CrossRef]
- Nishi FA, de Oliveira Motta Maia F, de Souza Santos I, de Almeida Lopes Monteiro da Cruz D. Assessing sensitivity and specificity of the Manchester Triage System in the evaluation of acute coronary syndrome in adult patients in emergency care: a systematic review. JBI Database System Rev Implement Rep. 2017 Jun;15(6):1747-1761. PMID: 28628525. [CrossRef]
- Ashburn NP, O’Neill JC, Stopyra JP, Mahler SA. Scoring systems for the triage and assessment of short-term cardiovascular risk in patients with acute chest pain. Rev Cardiovasc Med. 2021 Dec 22;22(4):1393-1403. PMID: 34957779; PMCID: PMC9038214. [CrossRef]
- Ke J, Chen Y, Wang X, Wu Z, Chen F. Indirect comparison of TIMI, HEART and GRACE for predicting major cardiovascular events in patients admitted to the emergency department with acute chest pain: a systematic review and meta-analysis. BMJ Open. 2021 Aug 18;11(8):e048356. PMID: 34408048; PMCID: PMC8375746. [CrossRef]
- Zhelev Z, Walker G, Henschke N, Fridhandler J, Yip S. Prehospital stroke scales as screening tools for early identification of stroke and transient ischemic attack. Cochrane Database Syst Rev. 2019 Apr 9;4(4):CD011427. PMID: 30964558; PMCID: PMC6455894. [CrossRef]
- Chehregani Rad I, Azimi A. Recognition of Stroke in the Emergency Room (ROSIER) Scale in Identifying Strokes and Transient Ischemic Attacks (TIAs); a Systematic Review and Meta-Analysis. Arch Acad Emerg Med. 2023 Oct 5;11(1):e67. PMID: 37840869; PMCID: PMC10568950. [CrossRef]
- Tsiftsis D., El-Fellah N., Dermatis P., “Systems and algorithms of Hospital Triage and patient acuity assessment in the Emergency department” In Book “Intensive and Emergency Medicine: Scales, Algorithms, Protocols, Limits, criteria and indicators”, 22nd Edition, Ed. George Baltopoulos. 301-9, Athens, Ekdosis Epistimon, 2019. ISBN: 978-618-83535-5-8. (Chapter in Greek).
- Reason, J. (1997). Managing the Risks of Organizational Accidents (1st ed.). Routledge. [CrossRef]
- BenAveling - File:Swiss cheese model.svg, CC BY-SA 4.0, https://commons.wikimedia.org/w/index.php?curid=133912327.
- Aung SSM, Roongsritong C. A Closer Look at the HEART Score. Cardiol Res. 2022 Oct;13(5):255-263. Epub 2022 Oct 25. PMID: 36405228; PMCID: PMC9635776. [CrossRef]
- Nor AM, Davis J, Sen B, Shipsey D, Louw SJ, Dyker AG, Davis M, Ford GA. The Recognition of Stroke in the Emergency Room (ROSIER) scale: development and validation of a stroke recognition instrument. Lancet Neurol. 2005 Nov;4(11):727-34. PMID: 16239179. [CrossRef]
- Aung SSM, Roongsritong C. A Closer Look at the HEART Score. Cardiol Res. 2022 Oct;13(5):255-263. Epub 2022 Oct 25. PMID: 36405228; PMCID: PMC9635776. [CrossRef]
Figure 1.
The multi-layer triage approach. (Based on Ben Aveling cheese model[35].)(ESI , Emergency Severity Index; NEWS 2, National Early Warning Score 2).
Figure 1.
The multi-layer triage approach. (Based on Ben Aveling cheese model[35].)(ESI , Emergency Severity Index; NEWS 2, National Early Warning Score 2).
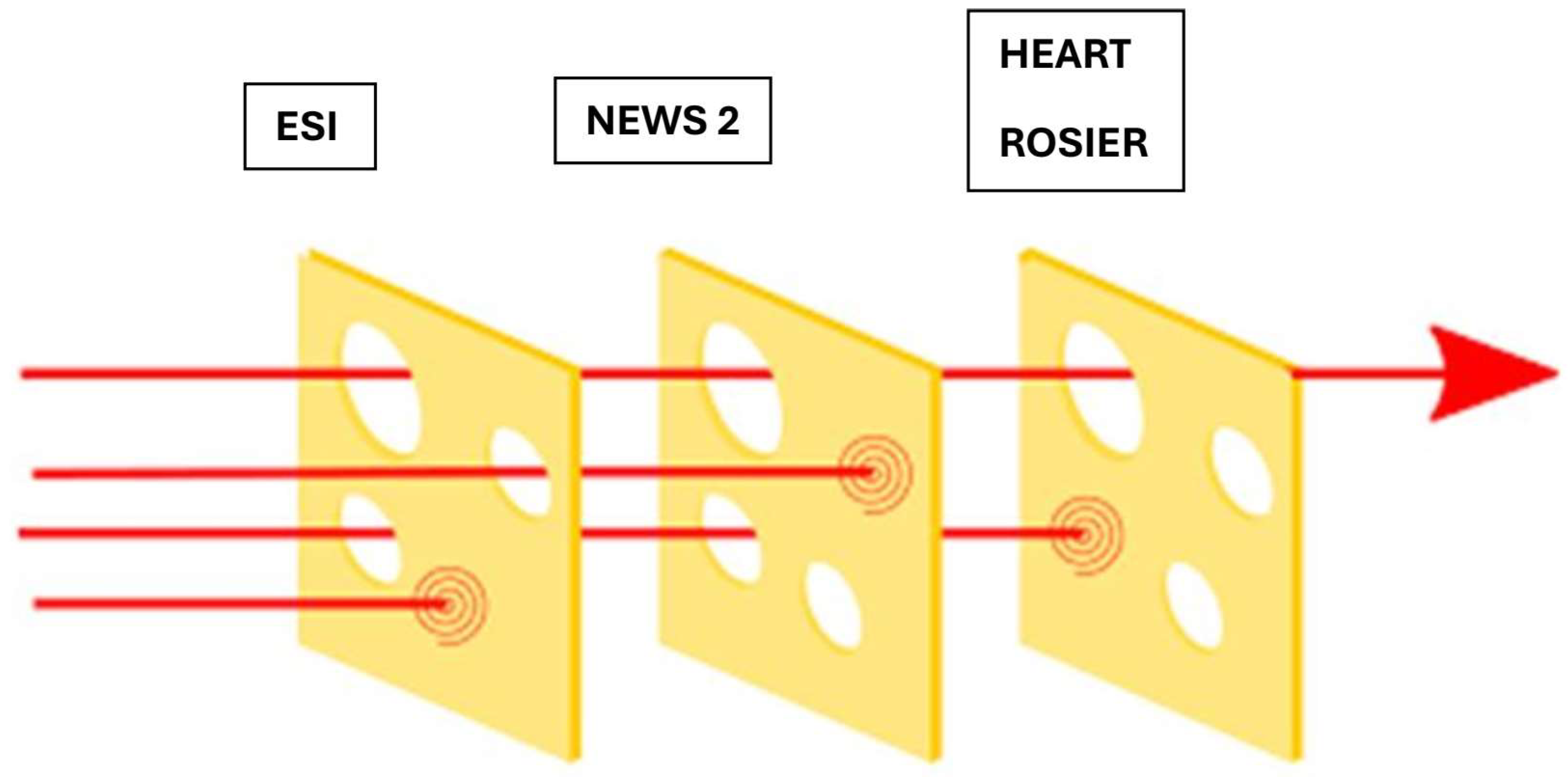
Figure 2.
NEWS 2 chart. (Royal College of Physicians. National Early Warning Score (NEWS) 2: Standardising the assessment of acute-illness severity in the NHS. Updated report of a working party. London: RCP, 2017.).
Figure 2.
NEWS 2 chart. (Royal College of Physicians. National Early Warning Score (NEWS) 2: Standardising the assessment of acute-illness severity in the NHS. Updated report of a working party. London: RCP, 2017.).
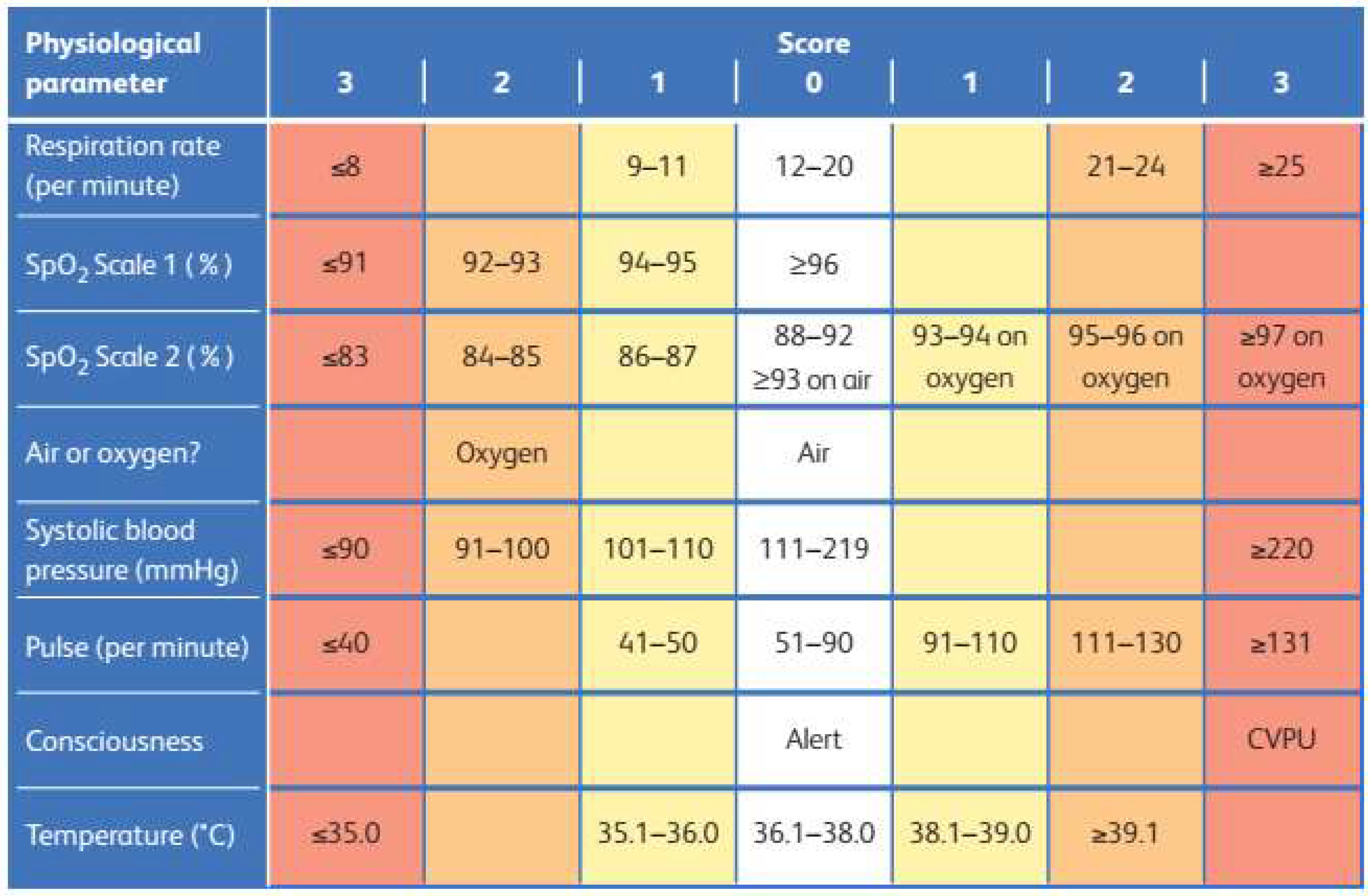
Figure 3.
NEWS 2 thresholds and triggers. (Royal College of Physicians. National Early Warning Score (NEWS) 2: Standardising the assess-ment of acute-illness severity in the NHS. Updated report of a working party. London: RCP, 2017.).
Figure 3.
NEWS 2 thresholds and triggers. (Royal College of Physicians. National Early Warning Score (NEWS) 2: Standardising the assess-ment of acute-illness severity in the NHS. Updated report of a working party. London: RCP, 2017.).
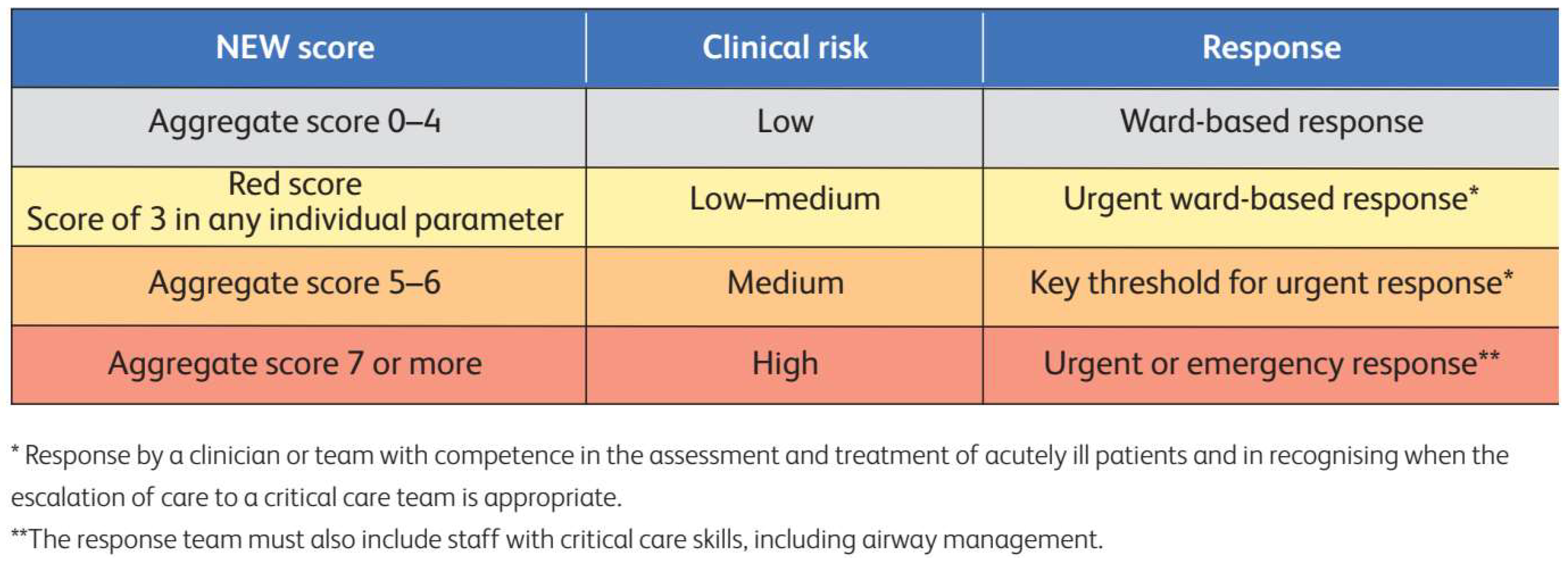
Figure 4.
The HEART score[38].
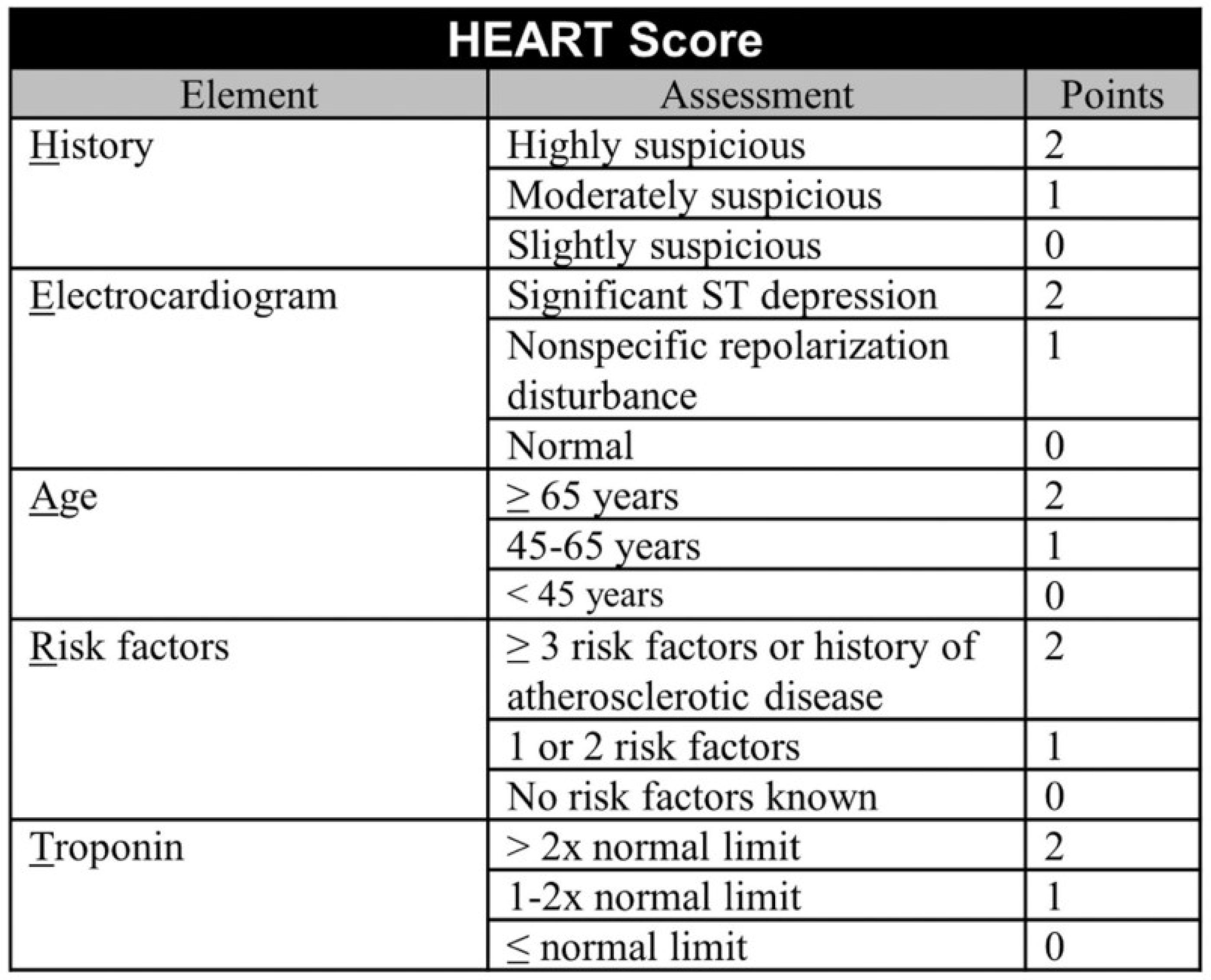
Figure 5.
HEART score interpretation and stratification. (MACE = Major adverse cardiac events).
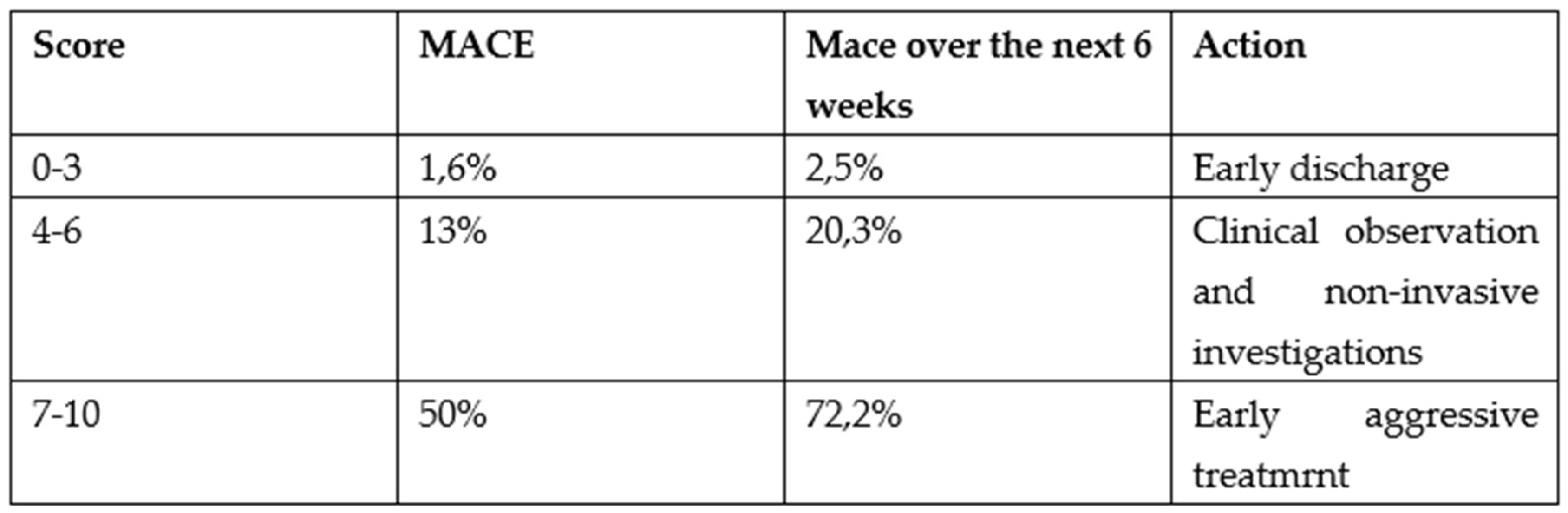
Figure 6.
Rosier score [37]. BM, blood glucose; BP, blood pressure (mm Hg); GCS, Glasgow Coma Scale; E=eye; M=motor; V=verbal component.
Figure 6.
Rosier score [37]. BM, blood glucose; BP, blood pressure (mm Hg); GCS, Glasgow Coma Scale; E=eye; M=motor; V=verbal component.
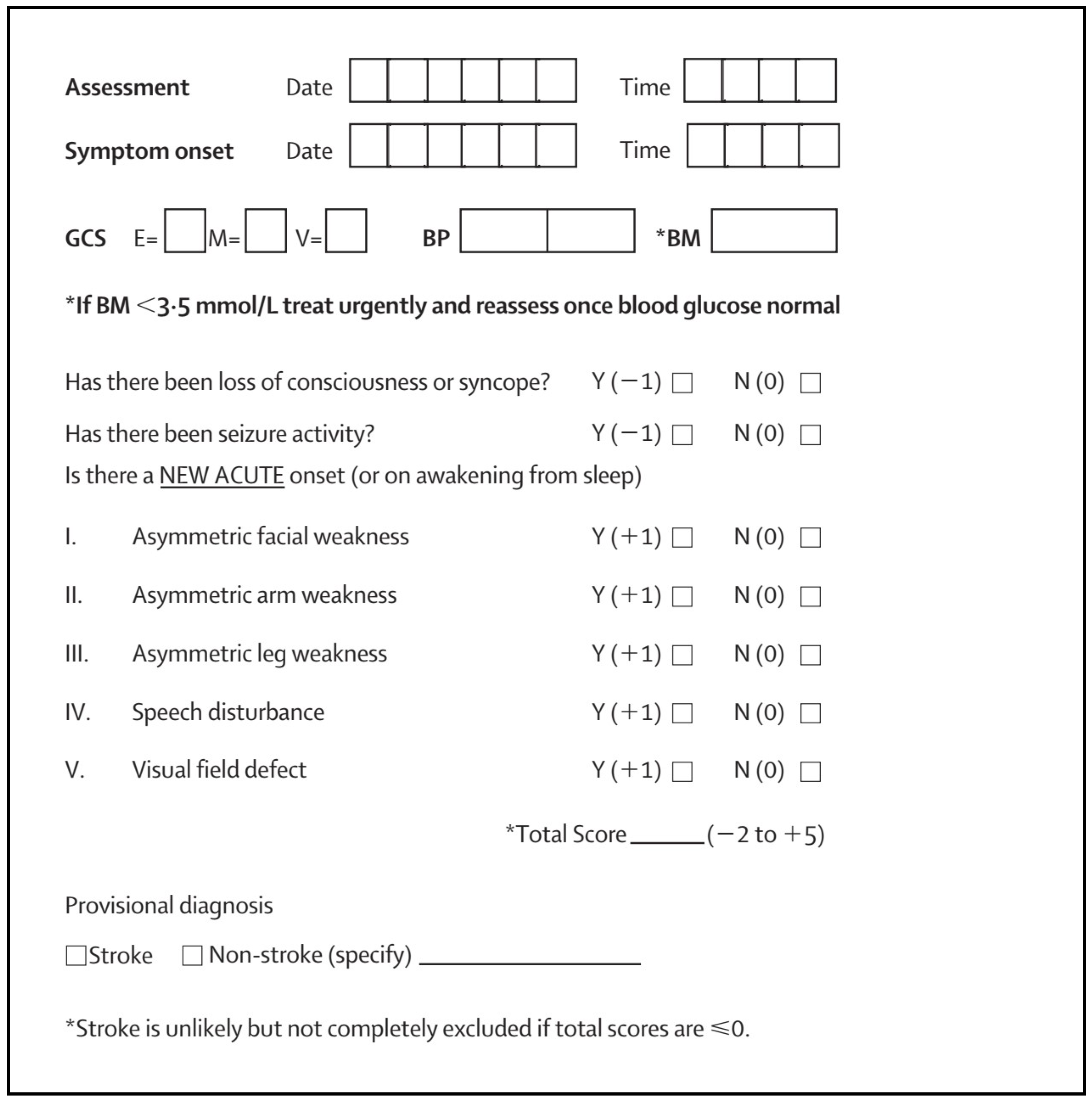
Figure 7.
Scheme 1: The multilayer triage flow chart.
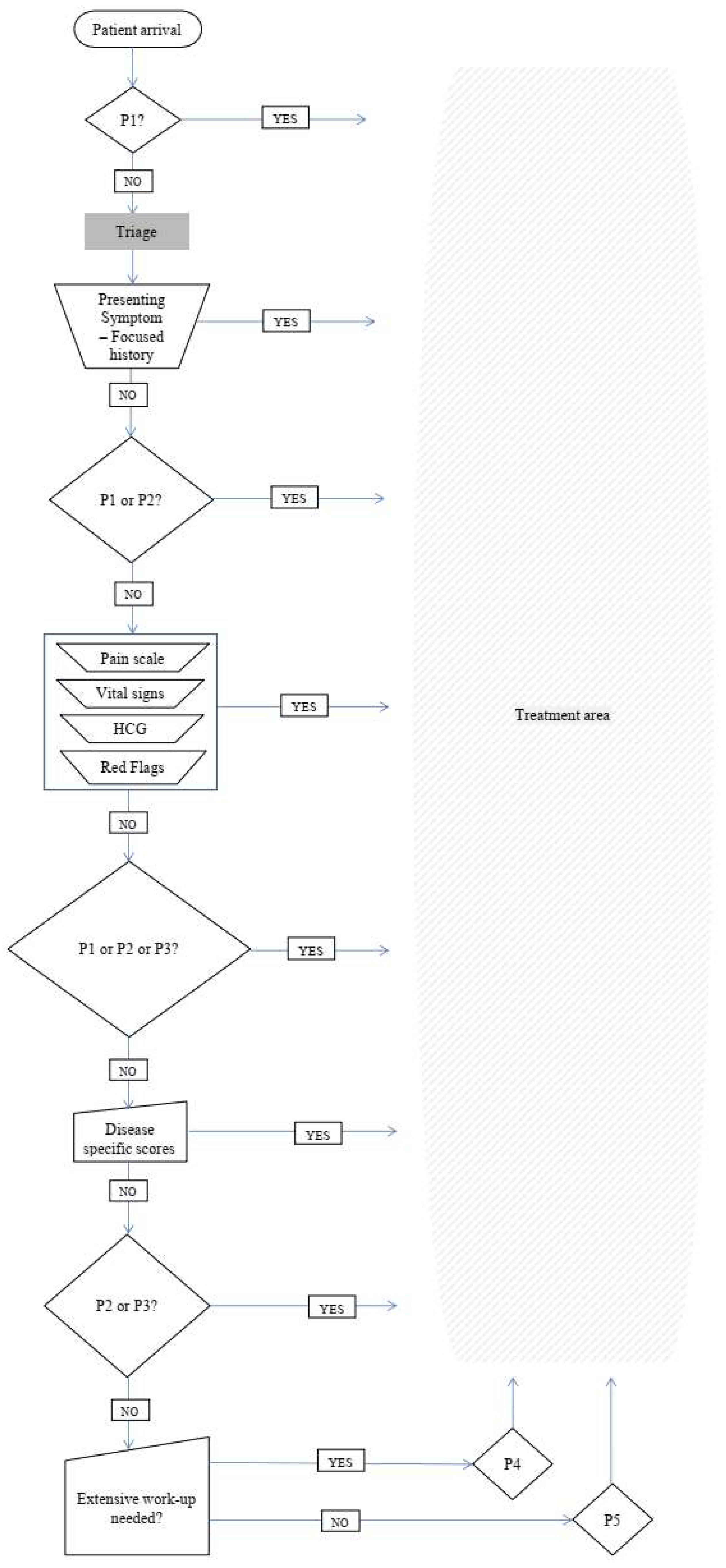

Table 1.
Characteristics of the most important five-level triage systems.
| Parameter | ATS | MTS | CTAS | ESI |
| Time to initial assessment | 10 min | ns | ns | ns |
| Time to contact with doctor with right to treat | Immediate / 10 / 30 /60 / 120 min | Immediate / 10 / 60 /120 / 240 min | Immediate / 15 / 30 /60 / 120 min | Immediate / 10 min /n. s |
| Re-triage | ns | As required | I:continuously; II: 15 min; III: 30 min; IV: 60 min; V: 120 min |
As required |
| List of diagnoses or key symptoms |
YES | 52 Key Symptoms | YES | No |
| Training material | YES | YES | YES | YES |
ATS, Australasian Triage Scale (previously National Triage Scale, NTS); CTAS, Canadian Triage and Acuity Scale; MTS, Manchester Triage Scale; ESI, Emergency Severity Index; n. s., not specified; I to V: triage priority levels.
Table 2.
.
| Patient Priority | Clinical condition | Tools used to identify |
|---|---|---|
| Priority 1 | Immediate risk for life or limb | ESI |
| Priority 2 | Serious enough or deteriorating so rapidly | ESI and/or Red Flags and/or NEWS 2>7 and/or HEART score >7 and/or Rosier >1 |
| Priority 3 | Not serious enough, but could have atypical or early presentation of a serious condition | NEWS 2=5-6 and/or HEART score =4-6 |
| Priority 4 | No serious underlying condition, but will require extensive work up | ESI and NEWS 2=0-4 and HEART =0-3 and Rosier <0 |
| Priority 5 | Acute but non-urgent or chronic problem without deterioration. Need minimum investigation | ESI and NEWS 2=0-4 and HEART =0-3 and Rosier <0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



